Embed Size (px)
Citation preview
Rheumatoid ArthritisRheumatoid Arthritis
Grassi W et al. Grassi W et al. Eur J RadiolEur J Radiol. 1998;27(suppl 1):S18–S24.. 1998;27(suppl 1):S18–S24.
RHEUMATOID ARTHRITISRHEUMATOID ARTHRITIS
OverviewOverview
Chronic inflammatory disease of unknown etiologyChronic inflammatory disease of unknown etiology
Complex, multifactorial pathogenesisComplex, multifactorial pathogenesis
Fluctuating clinical course; unpredictable prognosisFluctuating clinical course; unpredictable prognosis
Characterized byCharacterized by– Progressive destruction of synovial joints with lossProgressive destruction of synovial joints with loss
of cartilage and boneof cartilage and bone– Damaged ligaments and tendonsDamaged ligaments and tendons– Loss of physical function and quality of lifeLoss of physical function and quality of life– Premature deathPremature death
Sangha O. Sangha O. RheumatologyRheumatology. 2000;39(suppl 2):3–12.. 2000;39(suppl 2):3–12.MacGregor AJ, Silman AJ. In: Klippel JH, Dieppe PA, eds. MacGregor AJ, Silman AJ. In: Klippel JH, Dieppe PA, eds. Rheumatology. Rheumatology. Vol 1. 2nd ed. Vol 1. 2nd ed. London: Mosby;1998:2.1–2.6.London: Mosby;1998:2.1–2.6.
RHEUMATOID ARTHRITISRHEUMATOID ARTHRITIS EpidemiologyEpidemiology Affects approximately 1% of the global adult populationAffects approximately 1% of the global adult population Estimated annual incidenceEstimated annual incidence
– Males: 0.1–0.2 per 1000Males: 0.1–0.2 per 1000– Females: 0.2–0.4 per 1000Females: 0.2–0.4 per 1000
Occurs 2 to 3 times more often in women than in menOccurs 2 to 3 times more often in women than in men Incidence largely consistent racially and geographicallyIncidence largely consistent racially and geographically Peak age of onset between the ages of 45 and 65 yearsPeak age of onset between the ages of 45 and 65 years
RHEUMATOID ARTHRITISRHEUMATOID ARTHRITIS
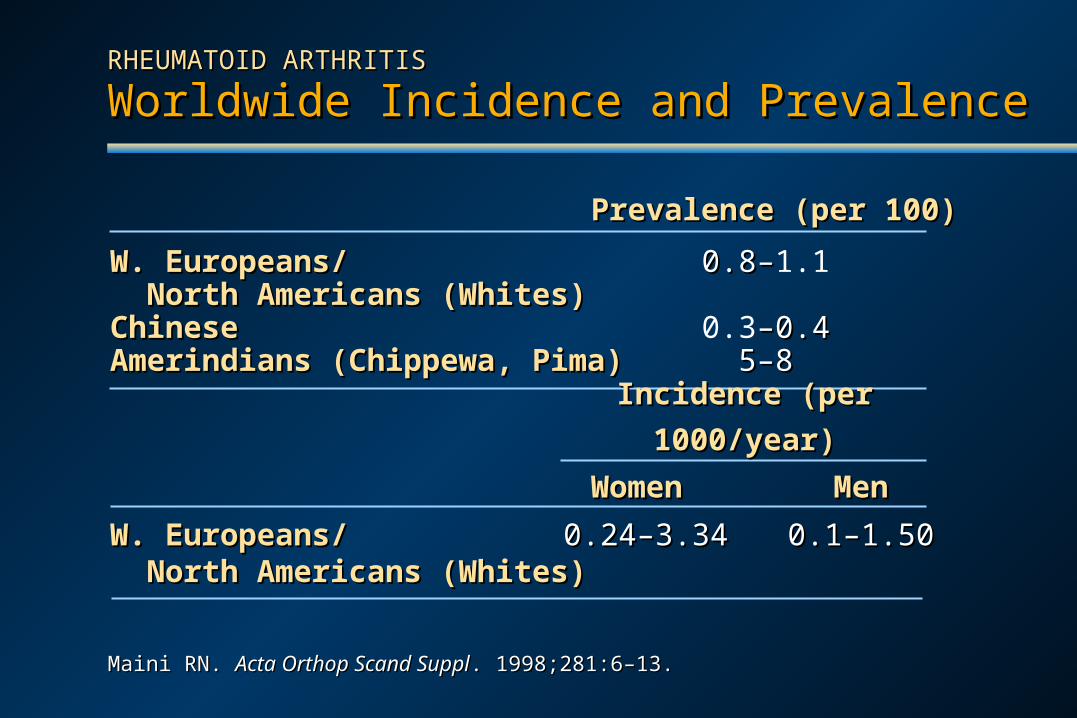
Worldwide Incidence and PrevalenceWorldwide Incidence and Prevalence
Maini RN. Maini RN. Acta Orthop Scand SupplActa Orthop Scand Suppl. 1998;281:6–13.. 1998;281:6–13.
Prevalence (per 100)Prevalence (per 100)
W. Europeans/W. Europeans/ 0.8–0.8–1.1 North Americans (Whites)North Americans (Whites)ChineseChinese 0.3–0.4–0.4Amerindians (Chippewa, Pima)Amerindians (Chippewa, Pima) 5–85–8
W. Europeans/W. Europeans/ 0.24–3.340.24–3.34 0.1–1.500.1–1.50 North Americans (Whites)North Americans (Whites)
WomenWomen Men Men
Incidence (per 1000/year)Incidence (per 1000/year)
Patients usually experience moderate disability withinPatients usually experience moderate disability within2 years of diagnosis and are severely disabled by 10 years2 years of diagnosis and are severely disabled by 10 years
Approximately 30% of patients are unable to work withinApproximately 30% of patients are unable to work within10 years of RA onset10 years of RA onset
Patients experience feelings of helplessness and other Patients experience feelings of helplessness and other psychological distress due to their increasing dependence psychological distress due to their increasing dependence upon help from othersupon help from others
Patients may be prevented from carrying out social rolesPatients may be prevented from carrying out social roles
Alarcón GS. Alarcón GS. Rheum Dis Clin North AmRheum Dis Clin North Am. 1995;21:589–604.. 1995;21:589–604.Wolfe F, Hawley D. Wolfe F, Hawley D. J RheumatolJ Rheumatol. 1998;25:2108–2117. . 1998;25:2108–2117. Pincus T. Pincus T. DrugsDrugs. 1995;50(suppl 1):1–14.. 1995;50(suppl 1):1–14.
RHEUMATOID ARTHRITISRHEUMATOID ARTHRITIS
Social and Psychological BurdenSocial and Psychological Burden
Estimated costs of RA were $8.74 billion in 1994,Estimated costs of RA were $8.74 billion in 1994,0.3% of the gross domestic product (GDP)0.3% of the gross domestic product (GDP)
Direct medical costs are $5,919/case/yearDirect medical costs are $5,919/case/year
Indirect costsIndirect costs– 3 to 4 times higher than direct costs3 to 4 times higher than direct costs– $11,750 per person-year in patients with early RA $11,750 per person-year in patients with early RA
Lifetime costs of RA rival those of coronary arteryLifetime costs of RA rival those of coronary arterydisease or strokedisease or stroke
Yelin E. Yelin E. J Rheumatol SupplJ Rheumatol Suppl. 1996;44:47–61.. 1996;44:47–61.Yelin E, Wanke LA. Yelin E, Wanke LA. Arthritis RheumArthritis Rheum. 1999;42:1209–1218. . 1999;42:1209–1218. Allaire SH et al. Allaire SH et al. PharmacoeconomicsPharmacoeconomics. 1994;6:513–522.. 1994;6:513–522.Merkesdal S et al. Merkesdal S et al. ArthritisArthritis RheumRheum. 2001;44:528–534.. 2001;44:528–534.
RHEUMATOID ARTHRITISRHEUMATOID ARTHRITIS
Economic Burden (US)Economic Burden (US)
RHEUMATOID ARTHRITISRHEUMATOID ARTHRITIS
Economic Burden (Europe)Economic Burden (Europe) In West Germany, the costs of RA were >40 billion DMIn West Germany, the costs of RA were >40 billion DM
(US $17.6 billion) in 1994 for treatment alone(US $17.6 billion) in 1994 for treatment alone In the UK, average RA outpatient cost/case/year was £798In the UK, average RA outpatient cost/case/year was £798
(US $1,126) and £1,253 (US $1,769) per inpatient in 1997(US $1,126) and £1,253 (US $1,769) per inpatient in 1997 RA per capita costs average:RA per capita costs average:
– 49% of cost of cancer49% of cost of cancer– 68% of cost of stroke68% of cost of stroke– 82% of cost of coronary heart disease82% of cost of coronary heart disease– 5X cost of motor vehicle accidents5X cost of motor vehicle accidents
Knorr U. Knorr U. VersicherungsmedizinVersicherungsmedizin. 1994.. 1994.Rothfuss J. Rothfuss J. Akt RheumatolAkt Rheumatol. 1997.. 1997.Lubeck DP et al. Lubeck DP et al. Arthritis RheumArthritis Rheum. 1986;29:488–493.. 1986;29:488–493.Lorig KR et al. Lorig KR et al. Arthritis RheumArthritis Rheum. 1993;36:439–446.. 1993;36:439–446.
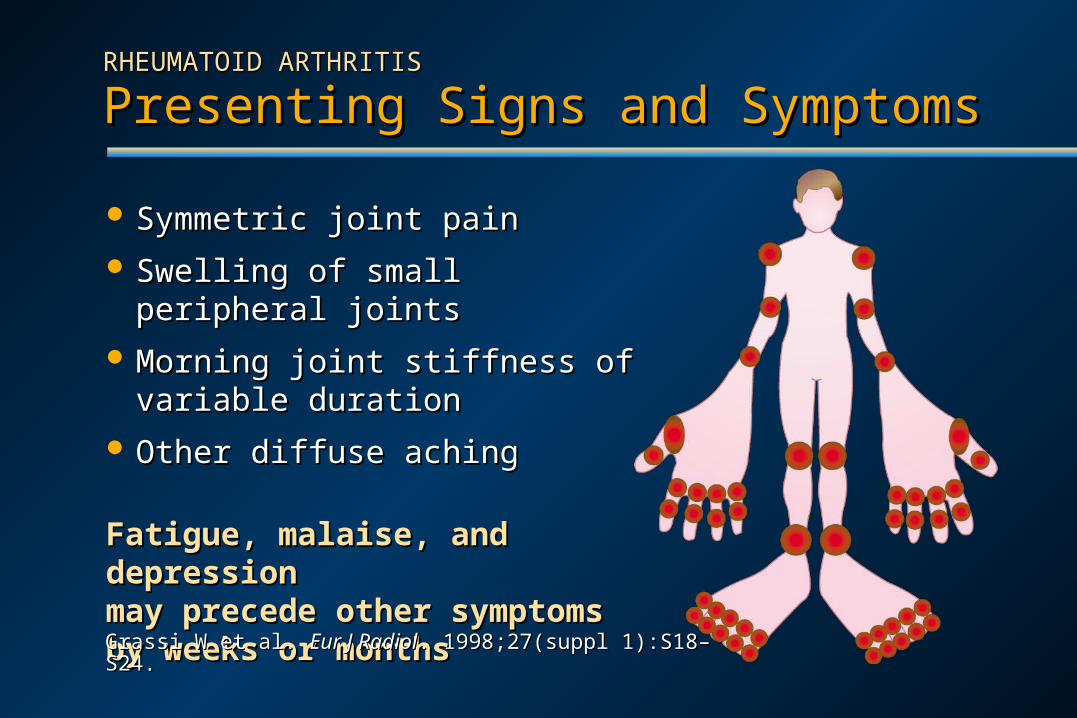
Symmetric joint painSymmetric joint pain
Swelling of small peripheral jointsSwelling of small peripheral joints
Morning joint stiffness of variable Morning joint stiffness of variable durationduration
Other diffuse achingOther diffuse aching
Fatigue, malaise, and depressionFatigue, malaise, and depressionmay precede other symptomsmay precede other symptomsby weeks or monthsby weeks or months
Grassi W et al. Grassi W et al. Eur J RadiolEur J Radiol. 1998;27(suppl 1):S18–S24.. 1998;27(suppl 1):S18–S24.
RHEUMATOID ARTHRITISRHEUMATOID ARTHRITIS
Presenting Signs and SymptomsPresenting Signs and Symptoms
Rosenberg A. In: Cotran RS, Kumar V, Collins T, eds. Rosenberg A. In: Cotran RS, Kumar V, Collins T, eds. Robbins Pathologic Basis of Disease.Robbins Pathologic Basis of Disease. 6th ed. Philadelphia, PA: WB Saunders; 1999:1215–1268.6th ed. Philadelphia, PA: WB Saunders; 1999:1215–1268.
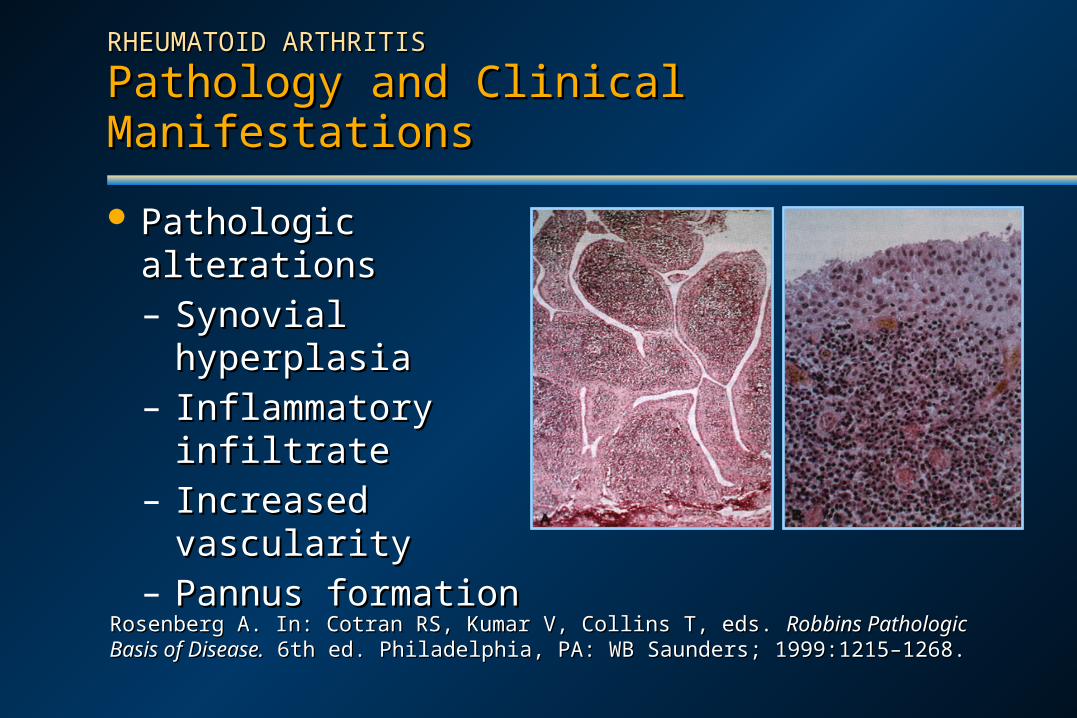
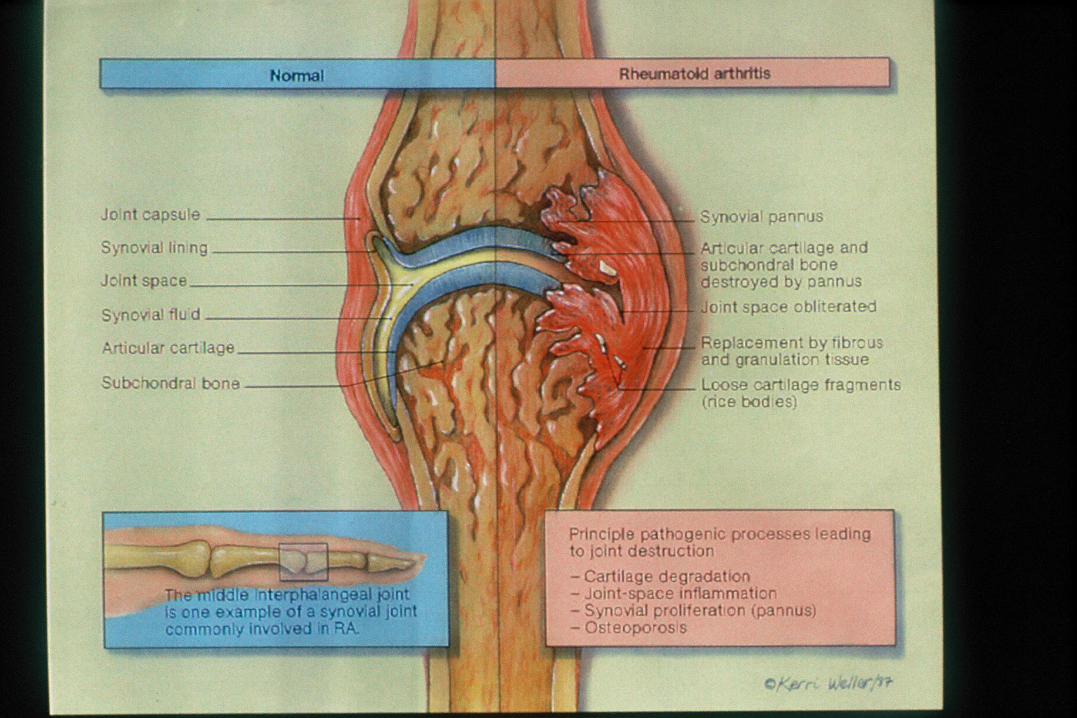
RHEUMATOID ARTHRITISRHEUMATOID ARTHRITIS
Pathology and Clinical ManifestationsPathology and Clinical Manifestations
Pathologic alterationsPathologic alterations– Synovial hyperplasiaSynovial hyperplasia– Inflammatory infiltrateInflammatory infiltrate– Increased vascularityIncreased vascularity– Pannus formationPannus formation


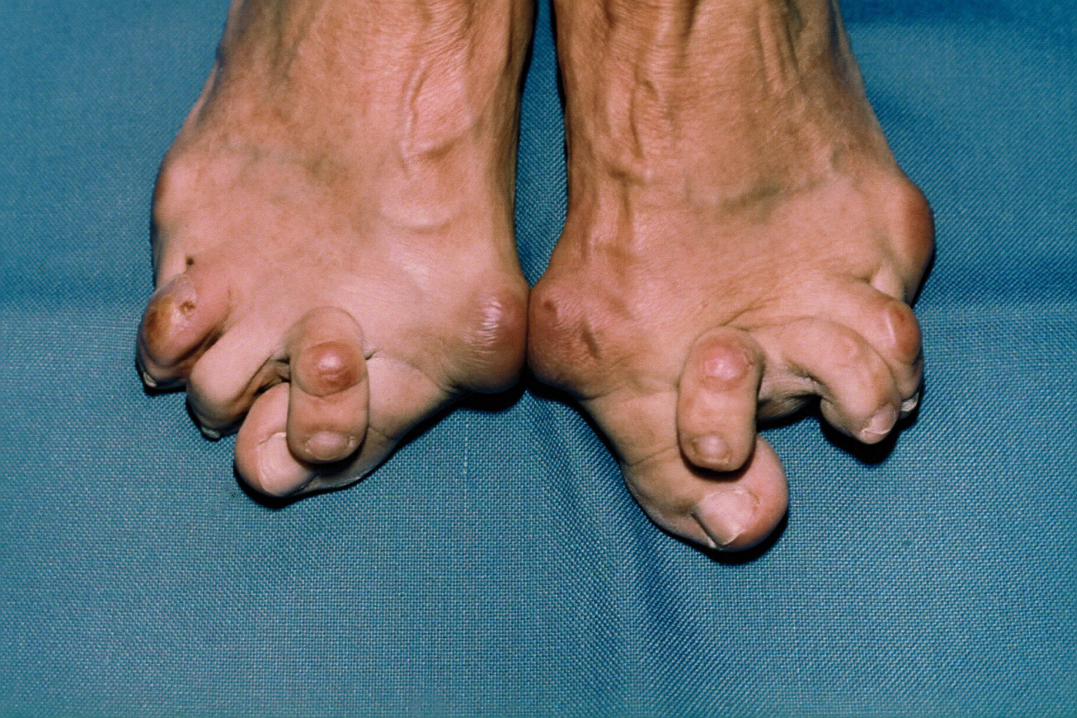
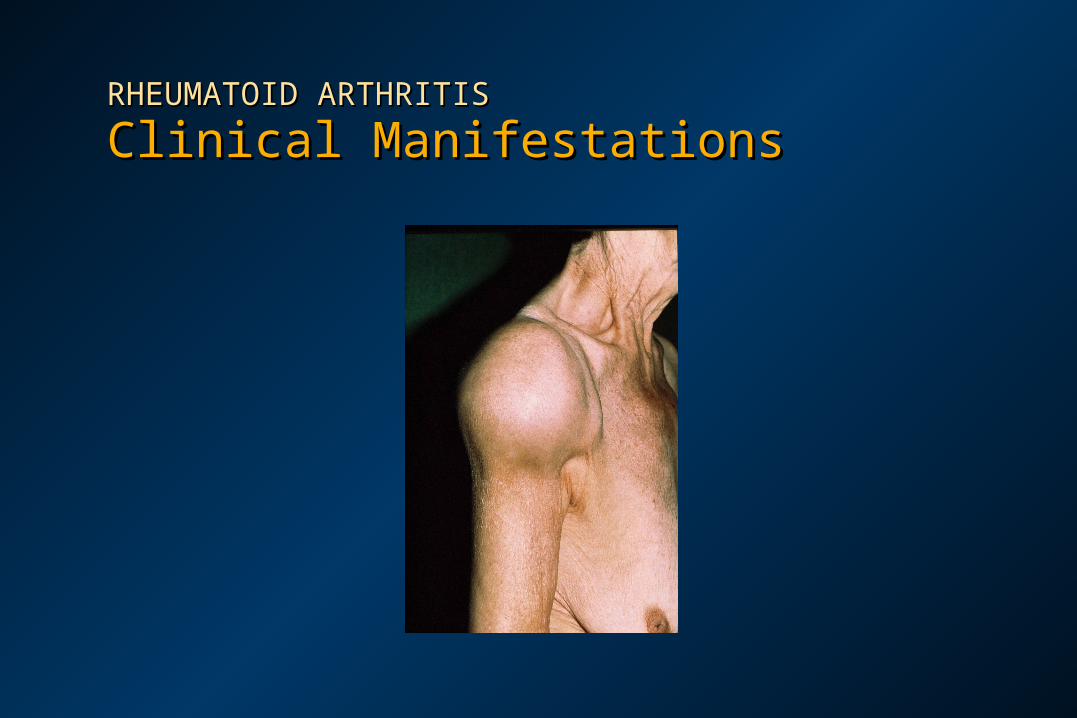
RHEUMATOID ARTHRITISRHEUMATOID ARTHRITIS
Clinical ManifestationsClinical Manifestations
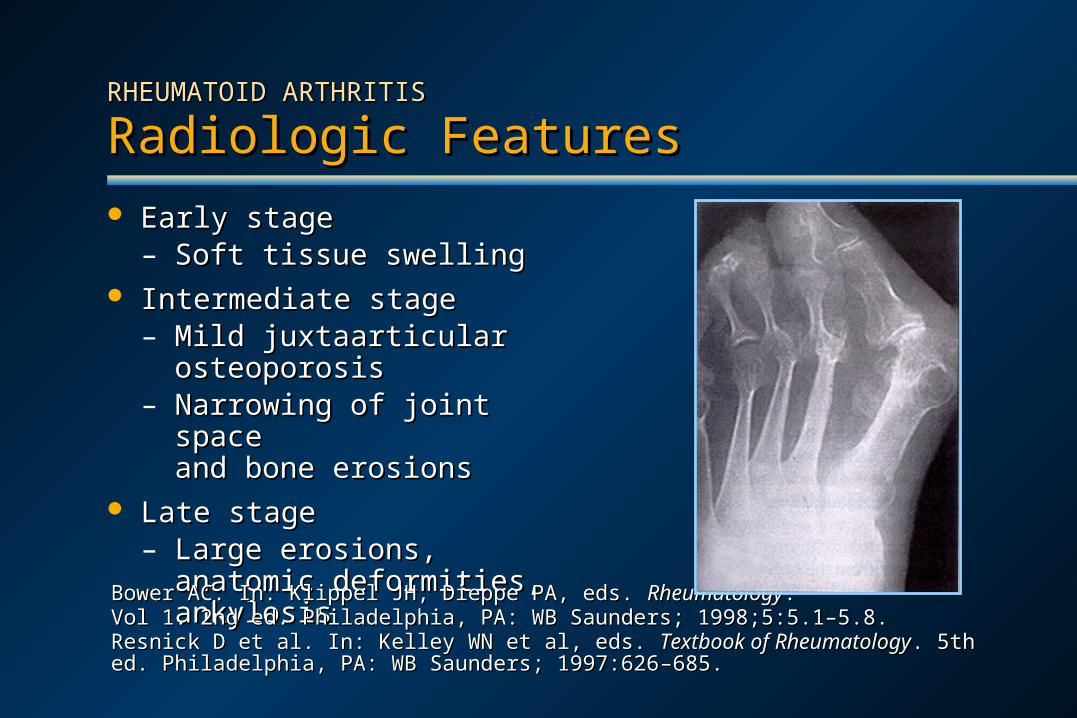
Early stageEarly stage– Soft tissue swellingSoft tissue swelling
Intermediate stageIntermediate stage– Mild juxtaarticularMild juxtaarticular
osteoporosisosteoporosis– Narrowing of joint spaceNarrowing of joint space
and bone erosionsand bone erosions Late stageLate stage
– Large erosions, anatomic Large erosions, anatomic deformities, ankylosisdeformities, ankylosis
Bower AC. In: Klippel JH, Dieppe PA, eds. Bower AC. In: Klippel JH, Dieppe PA, eds. RheumatologyRheumatology. . Vol 1. 2nd ed. Philadelphia, PA: WB Saunders; 1998;5:5.1–5.8.Vol 1. 2nd ed. Philadelphia, PA: WB Saunders; 1998;5:5.1–5.8.Resnick D et al. In: Kelley WN et al, eds. Resnick D et al. In: Kelley WN et al, eds. Textbook of RheumatologyTextbook of Rheumatology. 5th ed. Philadelphia, PA: . 5th ed. Philadelphia, PA: WB Saunders; 1997:626WB Saunders; 1997:626––685.685.
RHEUMATOID ARTHRITISRHEUMATOID ARTHRITIS
Radiologic FeaturesRadiologic Features

RHEUMATOID ARTHRITISRHEUMATOID ARTHRITIS
Radiologic FeaturesRadiologic Features
Harris ED Jr. In: Kelley WN et al, eds. Harris ED Jr. In: Kelley WN et al, eds. Textbook of RheumatologyTextbook of Rheumatology. 5th ed. Philadelphia, PA: . 5th ed. Philadelphia, PA: WB Saunders; 1997:898–932.WB Saunders; 1997:898–932.Pincus T. In: Klippel JH, Dieppe PA, eds. Pincus T. In: Klippel JH, Dieppe PA, eds. Rheumatology. Rheumatology. Vol 1. 2nd ed. London: Mosby; Vol 1. 2nd ed. London: Mosby; 1998;2:10.1–10.8.1998;2:10.1–10.8.
RHEUMATOID ARTHRITISRHEUMATOID ARTHRITIS
Laboratory FindingsLaboratory Findings Rheumatoid factor positive in up to 80% of patientsRheumatoid factor positive in up to 80% of patients Antinuclear antibody positive in 80% of patientsAntinuclear antibody positive in 80% of patients Acute phase reactants (ESR, CRP) Acute phase reactants (ESR, CRP) in almost all patients in almost all patients
at some pointat some point Chemistries normal, except slight Chemistries normal, except slight in albumin, in albumin, total total
protein, and protein, and iron iron Hematologic findingsHematologic findings
– Mild anemia in 25% to 35% of patientsMild anemia in 25% to 35% of patients– Normal or slight Normal or slight in white cell count in white cell count– ThrombocytosisThrombocytosis
ESR = erythrocyte sedimentation rate; CRP = C-reactive protein.ESR = erythrocyte sedimentation rate; CRP = C-reactive protein.
RHEUMATOID ARTHRITISRHEUMATOID ARTHRITIS
ComplicationsComplications
Rheumatoid nodulesRheumatoid nodules Cardiovascular: vasculitis, pericarditisCardiovascular: vasculitis, pericarditis Pulmonary: pulmonary nodules, interstitial fibrosis, pleuritisPulmonary: pulmonary nodules, interstitial fibrosis, pleuritis Ocular: scleritis, conjunctivitisOcular: scleritis, conjunctivitis Neurologic: compression neuropathy, vasculitisNeurologic: compression neuropathy, vasculitis Skin: distal leg ulcers, palmar erythemaSkin: distal leg ulcers, palmar erythema Hematologic: granulocytopenia (Felty’s syndrome), Hematologic: granulocytopenia (Felty’s syndrome),
hyperviscosityhyperviscosity Renal/hepatic: amyloidosis, Renal/hepatic: amyloidosis, liver enzymes liver enzymesHarris ED Jr. In: Kelley WN et al, eds. Harris ED Jr. In: Kelley WN et al, eds. Textbook of RheumatologyTextbook of Rheumatology. 5th ed. Philadelphia, PA:. 5th ed. Philadelphia, PA:WB Saunders; 1997:898–932.WB Saunders; 1997:898–932.Grassi W et al. Grassi W et al. Eur J Radiol. Eur J Radiol. 1998;27(suppl 1):S18–S24.1998;27(suppl 1):S18–S24.
Diagnosis of Rheumatoid ArthritisDiagnosis of Rheumatoid ArthritisAmerican College of Rheumatology CriteriaAmerican College of Rheumatology Criteria
Arnett FC et al. Arnett FC et al. Arthritis RheumArthritis Rheum. 1988;31:315–324.. 1988;31:315–324.
At least 4 of the following criteriaAt least 4 of the following criteria
Morning stiffness >1 hourMorning stiffness >1 hour
Arthritis of Arthritis of 3 joint areas3 joint areas
Arthritis of hand jointsArthritis of hand joints
Symmetric arthritisSymmetric arthritis
Rheumatoid nodulesRheumatoid nodules
Serum rheumatoid factorSerum rheumatoid factor
Radiographic changesRadiographic changes
Must be presentMust be presentfor at least 6 weeksfor at least 6 weeks
RHEUMATOID ARTHRITISRHEUMATOID ARTHRITIS
Clinical CourseClinical Course
Clinical course unpredictable but mostly progressiveClinical course unpredictable but mostly progressive
Unfavorable prognostic markers Unfavorable prognostic markers
– – Male sexMale sex – Eosinophilia– Eosinophilia
– – Low socioeconomic status Low socioeconomic status – Elevated ESR or CRP– Elevated ESR or CRP
– – Subcutaneous nodules Subcutaneous nodules – High RF factor titer – High RF factor titer
– – Systemic signsSystemic signs – Antinuclear antibodies– Antinuclear antibodies
– – Persistent synovitisPersistent synovitis – Cryoglobulins– Cryoglobulins
– – ThrombocytosisThrombocytosis – Shared epitope (?)– Shared epitope (?)
Disease activity reduced faster and radiographic evidence ofDisease activity reduced faster and radiographic evidence ofjoint damage lessened with early diagnosis and treatmentjoint damage lessened with early diagnosis and treatment
Albers JMC et al. Albers JMC et al. Ann Rheum DisAnn Rheum Dis. 2001;60:453–458.. 2001;60:453–458.Grassi W et al. Grassi W et al. Eur J RadiolEur J Radiol. 1998;27(suppl 1):S18–S24. . 1998;27(suppl 1):S18–S24.
TREATMENT OF RHEUMATOID ARTHRITISTREATMENT OF RHEUMATOID ARTHRITIS
Goals of TherapyGoals of Therapy
Relieve symptoms, including fatigue, pain, swelling, Relieve symptoms, including fatigue, pain, swelling, and stiffnessand stiffness
Prevent joint destruction, loss of joint function, Prevent joint destruction, loss of joint function, deformity, disability, and early deathdeformity, disability, and early death
Preserve quality of lifePreserve quality of life
Achieve clinical remissionAchieve clinical remission
Albers JMC et al. Albers JMC et al. Ann Rheum DisAnn Rheum Dis. 2001;60:453–458.. 2001;60:453–458.Grassi W et al. Grassi W et al. Eur J RadiolEur J Radiol. 1998;27(suppl 1):S18–S24.. 1998;27(suppl 1):S18–S24.
TREATMENT OF TREATMENT OF RHEUMATOID ARTHRITISRHEUMATOID ARTHRITIS
Conventional PharmacotherapyConventional PharmacotherapyDisease Modifying Antirheumatic Drugs (DMARDs)Disease Modifying Antirheumatic Drugs (DMARDs)
AzathioprineAzathioprine
D-penicillamineD-penicillamine
HydroxychloroquineHydroxychloroquine
Injectable gold saltsInjectable gold salts(oral gold)(oral gold)
LeflunomideLeflunomide
Methotrexate (MTX)Methotrexate (MTX)
SulfasalazineSulfasalazine










