Embed Size (px)
Citation preview
234
EURRAD 00 15 1
European Journal of Radiology, 12 (1991) 234-231 Elsevier
Radiographic findings in pulmonary tuberculosis: the influence of human immunodeficiency virus infection
J. GutiCrrez ‘, R. Miralles ‘, J. Co11 ‘, C. Alvarez 2, M. Sanz2 and J. Rubih-Prat ’
Departments of ‘Medicine and 2Radiology, Hospital de1 Mar, Universidad Autbnoma de Barcelona, Spain
(Received 6 August 1990; accepted after revision 20 December 1990)
Key words: Thorax, tuberculosis; Thorax, radiography; Thorax, AIDS; Tuberculosis, influence of HIV
Abstract
The chest radiographs and medical records of 166 patients diagnosed as having clinically active pulmonary tuberculosis were reviewed. Forty-nine patients (group I) were seropositives to human immunodeficiency virus (HIV), and 117 patients (group II) did not have known risk factors for HIV infection. Roentgenographic abnormalities were analysed in the two groups, according to nine different radiographic patterns previously defined. The seropositive group had a significantly higher proportion of hilar and/or mediastinal adenopathy (P < O.OOl), infiltrates confined to the lower lung fields (P < 0.05), and miliary tuberculosis (P < 0.005). Otherwise, single cavitation and destructive pattern were more frequent in the group II. These data suggest that patients with pulmonary tuberculosis and HIV infection are much more likely to have atypical radiographic findings.
Introduction
Pulmonary tuberculosis is still frequent in our geographic area and remains a public health problem. It is usually associated with lower socioeconomic con- ditions, alcoholism, starvation, chronic diseases and parenteral drug addiction [I]. In the last few years, patients infected by the human immunodeficiency virus (HIV) are also considered as a risk group for pulmonary tuberculosis [2-51. Infections due to Mycobacterium tuberculosis are in part related to the immunologic con- dition of the host, and in these subjects extrapulmonary and atypical forms of tuberculosis seems to be more common [ 6,7].
Recently, a high incidence of atypical radiographic appearance of pulmonary tuberculosis in HIV-infected patients has been reported [4,7-g]. Because of this, suspicious diagnosis based on X-ray chest examination and consequently the starting of antituberculous ther- apy may be delayed in these patients.
In this study, radiological findings in patients
Address for reprints: Prof. J Rubies-Prat, Department of Medicine, Hospital de1 Mar, Paseo Maritimo 25-29,08003 Barcelona, Spain.
0720-048X/91/$03.50 0 1991 Elsevier Science Publishers B.V.
infected by HIV and suffering from pulmonary tuber- culosis are analysed, and compared with another group of patients with pulmonary tuberculosis with no known risk factors for HIV infection.
Patients and Methods
The chest radiographs and medical records of 166 patients diagnosed as having clinically active pulmo- nary tuberculosis were reviewed. The criteria for inclu- sion in the study were a positive culture for Myco- bacteriun tuberculosis in Lowenstein medium, and/or a positive Ziehl-Neelsen stain for acid-fast bacilli, in samples obtained from the sputum, bronchial washing, or pleural biopsy, followed by clinical improvement after antituberculous therapy.
Forty-nine patients (34 men and 15 women) aged 20 to 50 years (mean 29) were seropositive to HIV (ELISA and Western Blot) (group I). One hundred and seven- teen patients (98 men and 19 women) aged 18 to 88 years (mean 5 1) did not have known risk factors for HIV infection (group II). The first group included all the patients seropositive to HIV, and the second group was recruited from the case list of the tuberculosis registry

235
of our hospital (within the last 5 years), and they were selected at random (a fourth part of each year). Their medical records were reviewed in order to exclude the presence of any risk factor for HIV infection and other clinical features, suggesting acquired immunodeficiency syndrome (AIDS).
In all cases, roentgenographic abnormalities were analysed by two radiologists, who did not know the patient’s group. Nine different radiographic patterns were defined [4,8,10]: (1) Typical infiltrate limited to the upper lobe; (2) single cavitation; (3) atypical intil- trate (pulmonary infiltrate that was diffuse throughout all lung fields or that was confined to the middle lung fields); (4) hilar and/or mediastinal adenopathy; (5) in- filtrate confined to the lower lung fields (infiltrate that is in contact with the pulmonary base); (6) miliary tuberculosis; (7) destructive pattern (diffuse fibrotic lesion and destruction of pulmonary parenchyma); (8) pleural effusion and/or pleural thickness; and (9) normal chest radiograph. One or more radiographic features may be present in the same patient. Statistical differences in the radiographic findings of tuberculosis between the two groups were determined using the Chi- square test and the Yates correction when necessary.
Results
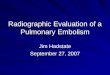
Table 1 shows the prevalence of the different radio- graphic patterns in the two groups. The seropositive group had a significantly higher proportion of hilar and/or mediastinal adenopathy (P < 0.001) (Fig. l),
TABLE 1
Radiographic findings in pulmonary tuberculosis in 49 HIV-sero- positive patients (group I) and in 117 patients with no known risk factors for HIV infection (group II)
Radiographic features Group I Group II P
n % n %
I. Typical infiltrate in upper lobe
2. Single cavitation 3. Atypical infiltrate 4. Hilar and/or
mediastinal adenopathy 5. Infiltrate confined
to the lower lung fields 6. Miliary 7. Destructive pattern 8. Pleural effusion and/or
pleural thickness 9. Normal chest radiograph
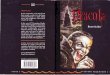
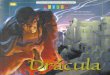
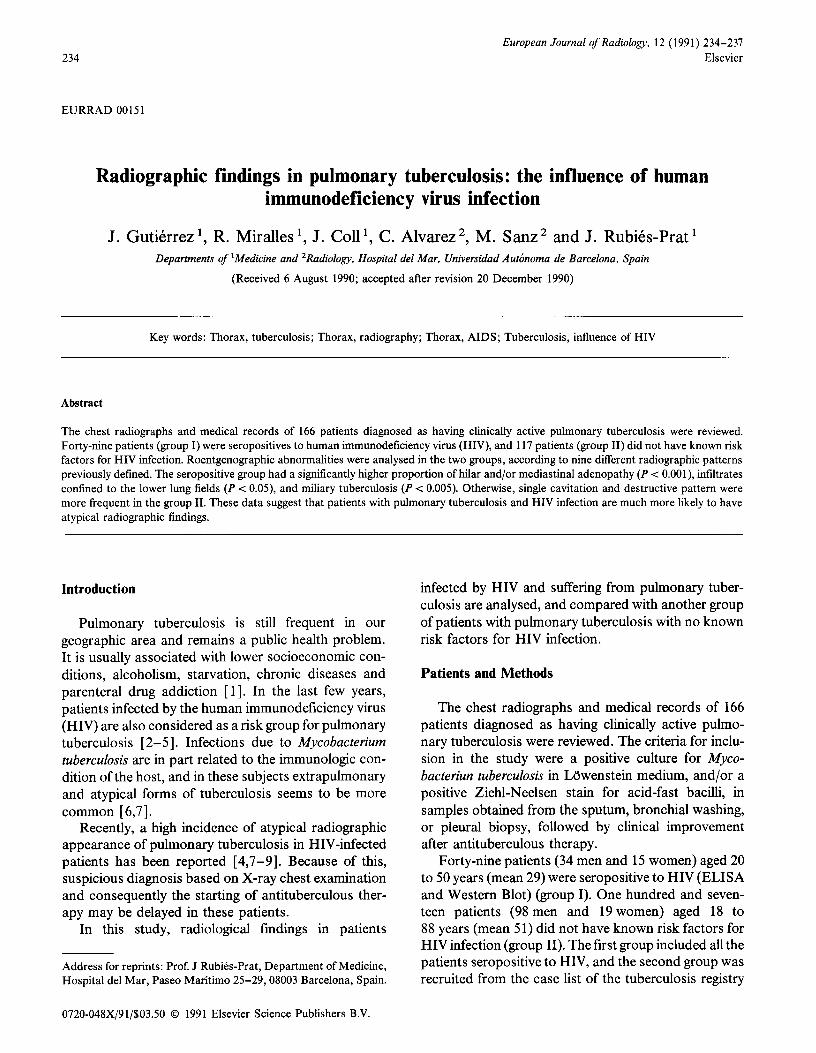
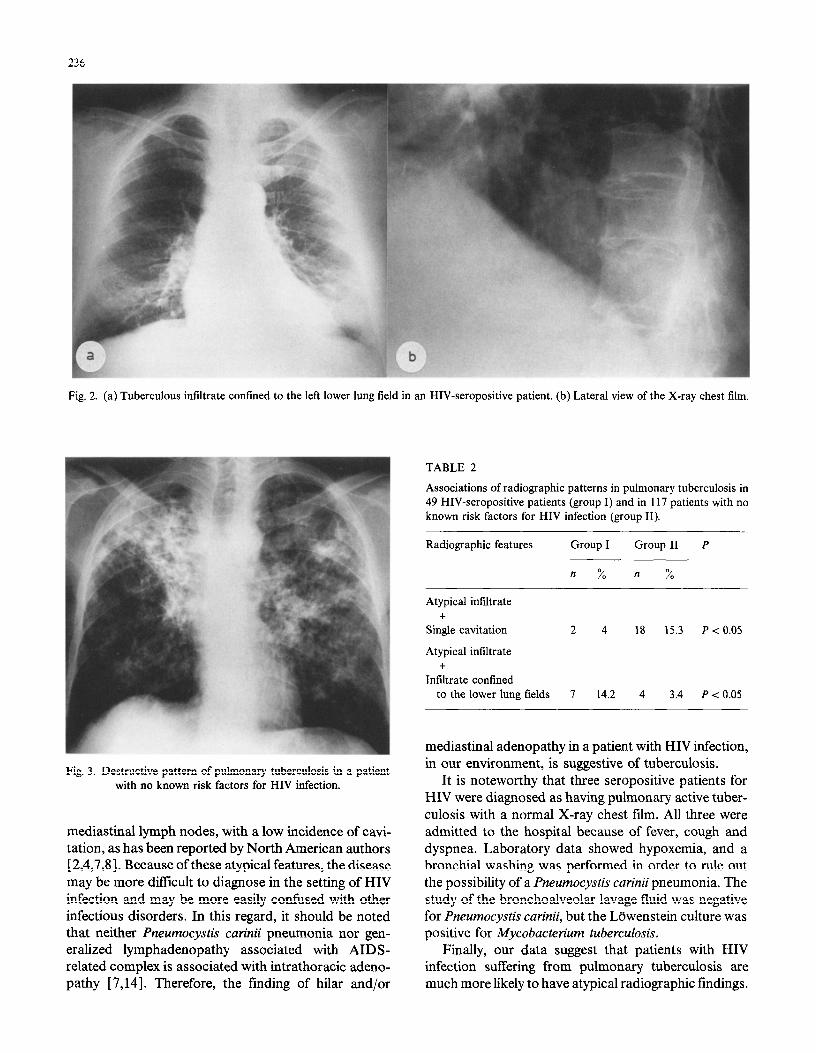
infiltrate confined to the lower lung fields (P < 0.05) (Fig. 2a and b), and miliary tuberculosis (P < 0.005). Otherwise single cavitation and destructive pattern were more frequent in the group II (Fig. 3). Two types of radiographic abnormality were observed in 114 patients (30 in group I and 84 in group II). Nineteen patients had three radiographic abnormalities (4 in group I and 15 in group II). No patient showed more than three abnormal radiographic features. The asso- ciations of the different abnormal radiographic patterns are shown in the Table 2. It is noteworthy that the X-ray chest film was normal in three HIV-seropositive patients with pulmonary tuberculosis.
Discussion
The prevalence of tuberculosis in Barcelona is 58.3 per 100000 population, this high prevalence being in part related to a high prevalence of parenteral drug abusers infected by HIV [ 111. Our center is a municipal hospital localized in the district of Barcelona with the highest prevalence of tuberculosis in the town. It has been reported that the incidence of tuberculosis in patients infected by HIV is raised in geographic areas in which the prevalence of tuberculosis is high [ 121, as occurs in our country [ 5,131. Chest roentgenography is the most useful method to suspect or exclude the pres- ence of tuberculosis, physicians being more familiar with the classical radiographic manifestations of pul- monary tuberculosis [ lo]. In the present study, tubercu- losis in HIV-infected patients shows a high frequency of atypical infiltrates in the lower lobes and hilar and
10 20.4 40 34.1 NS 5 10.2 35 29.9 P< 0.01
15 30.6 43 36.7 NS
16 32.6 4 3.4 P < 0.001
9 18.3 9 7.6 P < 0.05 6 12.2 1 0.8 P < 0.005 5 10.2 28 23.9 P < 0.05
5 10.2 26 22.2 NS 3 6.1 0 0 -
Fig. 1. Mediastinal tuberculous lymphadenopathy (diagnosed by biopsy after mediastinoscopy) in an AIDS patient. NS: not significant.
236
Fig. 2. (a) Tuberculous infiltrate confined to the left lower lung field in an HIV-seropositive patient. (b) Lateral view of the X-ray chest film.
Fig. 3. Destructive pattern of pulmonary tuberculosis in a patient with no known risk factors for HIV infection.
mediastinal lymph nodes, with a low incidence of cavi- tation, as has been reported by North American authors [ 2,4,7,8]. Because of these atypical features, the disease may be more difficult to diagnose in the setting of HIV infection and may be more easily confused with other infectious disorders. In this regard, it should be noted that neither Pneumocystis curinii pneumonia nor gen- eralized lymphadenopathy associated with AIDS- related complex is associated with intrathoracic adeno- pathy [ 7,141. Therefore, the finding of hilar and/or
TABLE 2
Associations of radiographic patterns in pulmonary tuberculosis in 49 HIV-seropositive patients (group I) and in 117 patients with no known risk factors for HIV infection (group II).
Radiographic features Group I Group II P
n % n %
Atypical infiltrate +
Single cavitation 2 4 18 15.3 P < 0.05
Atypical infiltrate +
Infiltrate confined to the lower lung fields 7 14.2 4 3.4 P < 0.05
mediastinal adenopathy in a patient with HIV infection, in our environment, is suggestive of tuberculosis.
It is noteworthy that three seropositive patients for HIV were diagnosed as having pulmonary active tuber- culosis with a normal X-ray chest film. All three were admitted to the hospital because of fever, cough and dyspnea. Laboratory data showed hypoxemia, and a bronchial washing was performed in order to rule out the possibility of a Pneumocystis carinii pneumonia. The study of the bronchoalveolar lavage fluid was negative for Pneumocystis carinii, but the Ldwenstein culture was positive for Mycobacterium tuberculosis.
Finally, our data suggest that patients with HIV infection suffering from pulmonary tuberculosis are much more likely to have atypical radiographic findings.

Clinicians and radiologists may recognize it, and start an early antituberculosis therapy with the consequent benefit for the patient and for the community.
References
Reichman LB, Felton CP, Edsall JR. Drug dependence, a possi- ble new risk factor for tuberculosis disease. Arch Intern Med 1979; 139: 337-339. Sunderam G, McDonald RJ, Maniatis T, Oleske J, Kapila R, Reichman LB. Tuberculosis as a manifestation of the acquired immunodeficiency syndrome (AIDS). JAMA 1986; 256: 362-366. Handwerger S, Mildvan D, Senie R, McKinley FW. Tuberculo- sis and the acquired immunodeficiency syndrome at a New York City hospital: 1978-1985. Chest 1987; 91: 176-180. Pitchenik AE, Burr J, Suarez M, Fertel D, Gonzalez G, Moas C. Human T-cell lymphotropic virus-III (HTLV-III) sero- positivity and related disease among 71 consecutive patients in whom tuberculosis was diagnosed. Am Rev Respir Dis 1987; 135: 875-879. Gate11 JM, Soriano E, Mallolas J, Mariscal D. Tuberculosis and the new CDC case definition for AIDS. Lancet 1988; i: 832.
6 Alvarez S, McCabe WR. Extrapulmonary tuberculosis revisited: a review of experience at Boston city and other hospitals. Medi- cine (Balt) 1984; 63: 25-55.
7 Chaisson RE, Schecter GF, Theuer ChP, Rutherford GW,
8
9
10
11
12
13
14
231
Echenberg DF, Hopewell PC. Tuberculosis in patients with the acquired immunodeficiency syndrome. Am Rev Respir Dis 1987; 136: 570-574. Pitchenik AE, Rubinson HA. The radiographic appearance of tuberculosis in patients with the acquired immune deficiency syndrome (AIDS) and pre-AIDS. Am Rev Respir Dis 1985; 131: 393-396. Louie E, Rice LB, Holzman RS. Tuberculosis in non-Haitian patients with acquired immunodeficiency syndrome. Chest 1986; 90: 542-545. Woodring JH, Vandiviere HM, Fried AM, Dillon ML, Williams TD, Melvin IG. Update: the radiographic features of pulmonary tuberculosis. AJR 1986; 146: 497-506. Programa de prevencib i control de la tuberculosis a la ciutat de Barcelona. Resultats de l’any 1988. Servei d’Epidemiologia i Estadistiques Vitals. Institut Municipal de la Salut. Ajuntament de Barcelona. Barcelona, Septiembre 1989. Pitchenik AE, Cole C, Russell BW, Fischl MA, Spira TJ, Snider DE. Tuberculosis, atypical Mycobacteriosis, and the acquired immunodeficiency syndrome among Haitian and non-Haitian patients in south Florida. Ann Intern Med 1984; 101: 641-645. Miralles R, Garces JM, Gall&, M, Gutitrrez-Cebollada J, Torn& J, Lopez-Colomes JL, Yazbeck H, Prats F. Sindrome de inmunodeficiencia adquirida: estudio descriptive y analisis de la supervivencia en 73 cases. Med Clin (Bare) 1990; 94: 401-405. Abrams DI, Ziegler JL. The AIDS-related complex. In: De Vita V, Hellman S, Rosenberg SA, eds. AIDS-etiology diagnosis, treatment and prevention. Philadelphia: Lippincott, 1985.



![Severe pulmonary radiological manifestations are ... · radiographic manifestations of pulmonary TB [15]. Other studies, however, have failed to demonstrate that DM impacts radiographic](https://img.pdfslide.us/doc/110x75/5fd15363a2500027f4297b60/severe-pulmonary-radiological-manifestations-are-radiographic-manifestations.jpg)





![Standardized radiographic interpretation of thoracic ... · culosis depends largely on chest imaging [1 ]. Pulmonary tuber-culosis has been classically classified as primary tuberculosis](https://img.pdfslide.us/doc/110x75/607490a4c43e164edd032250/standardized-radiographic-interpretation-of-thoracic-culosis-depends-largely.jpg)