Embed Size (px)
Citation preview

Catherine A. Staples, MD #{149}Eun-Young Kang, MD #{149}Joanne L. Wright, MD #{149}Peter Phillips, MDNestor L. Muller, MD, PhD
Invasive Pulmonary Aspergillosis in AIDS:Radiographic, CT, and Pathologic Findings’
409
PURPOSE: To review the radio-graphic and computed tomographic(CT) manifestations of invasive pul-monary aspergillosis and to correlatethe imaging and pathologic findingsin patients with acquired immunode-ficiency syndrome (AIDS).
MATERIALS AND METHODS: Chestradiographs, CT scans, and pathologicspecimens were reviewed retrospec-lively in 10 AIDS patients with provedinvasive pulmonary aspergillosis.
RESULTS: The most common radio-graphic finding was the presence ofthick-walled cavitary lesions. Lesscommon findings included nodules,
consolidation, and pleural effusion.CT depicted more nodules and cavi-ties than did radiography. The pre-dominant pathologic abnormalitiesconsisted of tissue invasion and ab-scess formation and angioinvasionwith or without infarction. All pa-tients had infection with Aspergillusfu migatus as well as other pathogens,the most common being cytomegalo-virus and Pseudomonas aeruginosa.
CONCLUSION: Thick-walled cavi-tary lesions are the most commonradiologic manifestation of invasivepulmonary aspergillosis in AIDS.The findings are more numerous andbetter defined on CT scans. The ra-diologic findings reflect a spectrumof pathologic abnormalities.
Index terms: Acquired immunodeficiency syn-
drome (AIDS), 68.2518 #{149}Aspergillosis,
68.2056 S Lung, infection, 68.2056
Radiology 1995; 196:409-414
I NVASIVE aspergillosis is uncommonin patients with acquired immu-
nodeficiency syndrome (AIDS) pre-sumably because the immune deficitsin these patients affect mainly the T
cells rather than granulocytes and
macrophages (1-10). In 1994, Miller etal (10) reviewed the radiographic andclinical features of confirmed or pre-sumed pulmonary aspergillosis in 36patients with AIDS. These includedsix new patients, as well as the 30 pa-tients who previously were reportedin the literature. The most commonradiographic manifestations includedcavitary upper lobe disease, focal con-solidation, and bilateral patchy or dif-fuse air-space consolidation. Verylittle information, however, is avail-able about the pathologic findings inthese patients (10). To our knowledge,
descriptions of the radiologic featuresof AIDS-related thoracic aspergillosisin the radiology literature are limitedto isolated case reports (8,9).
Our purpose was to review the ra-diographic and computed tomo-graphic (CT) findings of pulmonaryaspergillosis in patients with AIDSand to correlate the imaging andpathologic findings.
MATERIALS AND METHODS
Review of the medical and laboratoryrecords at our institution was performedto identify AIDS patients with proved pul-monary aspergillosis between August 1988and December 1993. To allow comparisonbetween the radiographic, CT, and patho-logic findings, only those patients withgross lung specimens obtained at surgeryor at autopsy were induded in the study.The medical charts were reviewed for per-tinent clinical data that included age, sex,
risk factors for infection with human im-munodeficiency virus (HIV), length inyears of HIV seropositivity, symptoms atinitial examination, associated illnesses,and use of corticosteroids. Also tabulatedwere the CD4 cell counts and the presenceof neutropenia (neutrophil count < 2,000).
The study group included 10 homo-sexual men, one of whom was also an in-travenous drug abuser. The mean age was37.6 years (range, 30-47 years). Preopera-
tive or premortal diagnosis was made insix patients by detection of an Aspergillusorganism in specimens obtained from oneor more sites by means of thoracentesis(n = 2), bronchoalveolar lavage (n = 2),
fine-needle aspiration biopsy (n = 2), andsputum culture (n = 1). Confirmation ofthe diagnosis was based on the identifica-tion of organisms in pathologic specimensobtained by means oflobectomy or pneumo-nectomy (n = 2) or autopsy (n = 8) (Table 1).All cases were due toAspergillusfumigatus.
Chest radiographs obtained at presenta-tion were reviewed retrospectively by twochest radiologists (C.A.S., N.L.M.) whoreached a final decision by consensus.Two to six radiographs (mean, four radio-graphs) were evaluated over an average of10 weeks (range, 2-40 weeks) in all pa-tients. The observers assessed the number,size, and the minimum and maximumwall thickness of pulmonary cavities andthe presence of noncavitary nodules, ir-regular linear opacities, ground-glassopacities, and air-space consolidation. Thepresence of airway abnormalities, lymph-adenopathy, pleural and pericardial effu-sions, and pneumothoraces was also as-sessed. Disease distribution was dividedinto upper and lower lung zone predomi-nance. Previous radiographs were as-sessed to identify cystic lesions or otherstructural abnormalities that predated sub-sequent radiographic abnormalities re-lated to aspergillosis.
CT scans were available in seven pa-tients. The CT examinations were per-formed with either a GE 9800 scanner (n =
3) or a 9800 HiLite Advantage scanner
I From the Departments of Radiology (C.A.S.), Pathology (J.L.W.), and Infectious Diseases (PP.),University of British Columbia and St Paul’s Hospital, Vancouver, and the Department of Radiology,University of British Columbia and Vancouver Hospital and Health Sciences Centre, 855 W 12thAve. Vancouver, British Columbia, Canada V5Z 1M9 (E.Y.K., N.L.M.). Received September 2, 1994;revision requested October 26; revision received February 21, 1995; accepted February 22. Addressreprint requests to N.L.M.
C RSNA, 1995
Abbreviations: AIDS = acquired immunodefi-ciency syndrome, CMV = cytomegalovirus,HIV = human immunodeficiency virus, PCP =
Pneumocystis carinii pneumonia.

410 #{149}Radiology August 1995
Table 1Summasy of Clinical Findings
PatientNo/Age
(y)Years with
HIV Positivity
CD4 CellCount
(cells/mm3) NeutropeniaSteroid
Therapy
Previous DiseaseThat Caused
Preexisting CystMethod ofDiagnosis
AssociatedPulmonary
Disease
DeathAttributed toAspergillosis
1/38 3 . . . No Yes PCP Lobectomy Granulomatous PCP No
2/30 6 200 No No PCP Thoracentesis, pneu-monectomy
Streptococcal infec-tion (pleural fluid)
No
3/47 9 10 No Yes . . . Thoracentesis,autopsy
CMV Yes
4/45 2 . . . No No PCP Bronchoscopy,autopsy
CMV, Kaposi sar-coma, tuberculosis,M kansasii
Yes
5/30 4 . . . Yes No . . . Fine-needle aspira-tion biopsy,autopsy
CMV Yes
6/33 7 20 Yes No Septic emboli Bronchoscopy, fine-needle aspirationbiopsy, autopsy
CMV Yes
7/42 10 0 Yes No Pyogenic infection Sputum culture,autopsy
CMV, Pseudomonasinfection
Yes
8/40 7 . . . Yes Yes . . . Autopsy CMV, Pseudomonasinfection
Yes
9/39 3 . . . No Yes . . . Autopsy Streptococcal pneu-monia
No
10/32 3 . . . Yes No . . . Autopsy CMV Yes
(n = 4) (GE Medical Systems, Milwaukee,Wis). Thin-section CT scans (1.5-mm colli-
mation with a high-spatial-frequency re-construction algorithm) were obtained infour patients and conventional 10-mm col-limation scans in three patients. Intrave-nous contrast material was used in onepatient. The CT scans were reviewed ret-rospectively by the two observers afterreview of the chest radiographs and thendirectly compared with the radiographs.
Pathologic specimens were obtained inall 10 patients. They induded specimens ob-tamed at lobectomy (n = 1), pneumonectomy(n = 1), or autopsy (n = 8) (Table 1). Allpathologic specimens were reviewed by anexperienced lung pathologist (J.LW.).
The diagnosis of tissue invasion wasbased on the presence of Aspergillus or-ganisms within alveolar spaces associatedwith tissue necrosis. Aspergillus pneumo-nia was defined as a diffuse area of in-volvement with pronounced inflamma-tory reaction and abundant tissuenecrosis. An Aspergillus abscess was char-acterized by the presence of a localizedarea of tissue necrosis that contained As-pergillus organisms, was well demarcatedfrom the adjacent parenchyma, and did ordid not have a fibrotic capsule. Angioinva-sive aspergillosis was characterized by in-filtration of the walls of small to medium-size pulmonary arteries by fungal hyphae.It could be associated with thrombus for-mation and hemorrhagic infarction due tovascular obstruction.
Clinical Data
RESULTS
The patients were known to be HIVpositive for an average of 5.4 years(range, 2-10 years) before the diagno-sis of invasive aspergillosis. One or
more risk factors for the developmentof aspergillosis were present in eightof 10 patients (Table 1).
All patients were symptomatic atpresentation. The most commonsymptoms included cough (n = 8),fever (n = 4), and shortness of breath(n = 7). All patients have died. Theaverage interval between presentationwith radiographic findings of invasiveaspergillosis and autopsy (n = 8) or sur-gical resection (n = 2) was 11 weeks.Death could be directly attributed toaspergillosis in seven patients.
Chest Radiographic Findings
The most common radiographicfinding was thick-walled, cavitarylesions and was seen in eight (80%) of10 patients (Table 2). The cavitarynodules or masses were 2-10 cm indiameter (mean, 6.2 cm) and had anaverage minimal wall thickness of 3mm (range, 2-8 mm) and averagemaximal wall thickness of 9.4 mm(range, 5-15 mm). The cavitary lesionsinvolved mainly the upper lobes in six(75%) of eight patients and the lower
lung zones in two patients. The cavi-ties were multiple in three patients(Fig 1). An intracavitary mass wasnoted on the radiographs in two pa-tients (Fig 2).
Less common radiographic findingsat initial examination included non-cavitary nodules in four (40%) of 10patients, consolidation in six patients(60%), pleural effusion in two patients(20%), and irregular linear opacities inone patient (10%) (Table 2). A pneu-
mopericardium and a hydropneumo-thorax were identified in one patient.Lymphadenopathy, airway lesions,and ground-glass opacities were notidentified on any chest radiograph.
Five patients had cystic or cavitarylesions before the development of
aspergillosis. These lesions includedcysts related to previous Pneumocystiscarinii pneumonia (PCP) (Fig 2) inthree patients, to septic emboli in onepatient, and to necrotizing pyogenicpneumonia in one patient (Table 1).The other five patients had no evi-dence of cystic lesions on previousradiographs.
CT Findings
The interval between chest radiog-raphy at initial examination and CT
(performed in seven patients) was0-10 days (median, 3 days). CT dem-
onstrated additional cavitary lesionsin three patients and noncavitarynodules in four patients (Table 2). Thecavities were better delineated from
surrounding abnormalities on the CTscan than on the radiograph (Fig 2).
Calcification of a cavity wall and anintracavitary mass were noted at CT
in one patient (patient 1). No air cres-cents and no evidence of bronchiecta-sis were seen on the radiographs orCT scans in any of the patients.
Pathologic Findings andCorrelation with Imaging Findings
Lung specimens obtained at lobec-tomy or pneumonectomy (patients 1

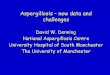
Figure 1. Patient 6. Cavitary aspergillosis in a 33-year-old man. (a) Posteroanterior chest ra-
diograph shows three, large, irregular, thick-walled cavities in the left upper lobe; a small ill-defined cavity in the right upper lobe; and nodules. The patient had previous cystic lesions
that increased in size and wall thickness with the aspergillosis. (b) Photograph of the left up-per lobe at autopsy shows multiple cavities that range in size from 0.3 to 5.0 cm. The smaller lesions
appear centered on airways (arrow). At pathologic examination, the patient had Aspergillus abscesseswith necrosis and tissue invasion. No bacteria were present in the lungs at autopsy.
Volume 196 #{149}Number 2 Radiology #{149}411
Table 2
Predominant Chest Radiographic, CT, and Pathologic Findings in AIDS Patients with Aspergillosis
PatientNo.
RadiographicFindings CT Findings Pathologic Findings
1 One cavity with intracavitary mass, irregular Two cavities, intracavitary mass, irregular Abscess, adjacent angioinvasion, intracavi-linear opacities linear areas of high attenuation tary mass
2 One cavity, consolidation, hydropneumo- One cavity, consolidation, hydropneumo- Abscess, empyema
thorax thorax3 Single cavity and single nodule, patchy con-
solidation, pneumopericardium, hydro-Five cavities, 10 nodules, patchy consolida-
tion, pneumopericardium, hydropneumo-Small airway invasion with necrosis; abscess;
tissue invasion of pleura, heart, and pen-
4pneumothorax
One cavity with intracavitary mass, patchythorax
Five nodules, one cavity with intracavitarycardium
Tissue invasion, abscess, intracavitary mass
consolidation mass, patchy consolidation
5 Consolidation with cavity Consolidation with cavity, one nodule Pneumonia, abscess, subpleural nodulartissue invasion
6 Four cavities, three nodules Four cavities, three nodules Tissue invasion, necrosis with abscesses,multiple intracavitary masses
7 Two cavities, patchy consolidation Four cavities, two nodules, patchy consoli-dation
Angioinvasion with large infarct in rightupper lobe, multiple bilateral infarcts 1-3cm in diameter, pneumonia
8 Three cavities, nodule Not performed Angioinvasion with several infarcts, onelarge airway destroyed
9 Consolidation in right lung, wedge opacity Not performed Angioinvasion, infarction
10of lingula
Three nodules Not performed Angioinvasion with several lung infarcts,small airway lesions
and 2) and autopsy (patients 3-10)were available in the 10 patients. Atpathologic examination, all 10 pa-tients had invasive aspergillosis. All
10 patients had associated pulmonarydiseases that included infection withcytomegalovirus (CMV) in seven pa-tients; streptococcal infection in twopatients; infection with a Pseudomonasorganism in two patients; granuloma-
tous PCP in one patient; and Kaposisarcoma, tuberculosis, and infection
with Mycobacterium kansasii in onepatient (Table 1). Eight of these 10patients had cavitary lesions with or
without associated noncavitary nod-ules and areas of consolidation, andone patient (patient 3) had invasion
into the lung, as well as of the pleura,pericardium, and heart.
The cavitary lesions seen on theradiographs and CT scans in the eightpatients represented pulmonary in-
farcts (n = 2) or abscesses (n = 6).
Two patients with abscesses also hadinvasion of nonvascular tissue with A
I umigatus, with necrosis. Intracavitarymasses of fungal hyphae and necrotictissue were seen at pathologic exami-nation in three patients. In two ofthese three patients, the intracavitarymasses had been identified on theradiograph.
Seven of the 10 patients had non-cavitary nodules on radiographs and
CT scans that were shown at patho-logic examination to represent in-farcts (n = 3) or nonvascular tissueinvasion with A fumigatus, with orwithout associated necrosis (n = 4).
Nodules in pathologic specimens cor-related with nodular lesions on chestradiographs and on CT scans (Table2). In two patients (patients 6 and 10),additional micronodules not depictedwith radiography and CT were due toinvolvement of the airways with A
fumigatus at the level of the distal res-piratory bronchioles and alveolar
ducts (Fig 1). In all seven patientswith nodular lesions in pathologicspecimens, CMV inclusions were alsoidentified.
In the six patients with areas of
consolidation on radiographs and CTscans, the causes of the consolidationat pathologic examination were multi-
factorial and included pneumonia,angioinvasion with infarction, diffusealveolar damage, and airway involve-ment at the level of the distal respira-tory bronchioles and alveolar ducts(Table 2). In five of the six patients
with consolidation, the organismidentified was A fumigatus, whereas in

a. b.
C.
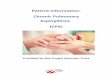
Figure 2. Patient 1. Cavitary aspergillosis in a 38-year-old man. (a) Posteroantenor chest ra-diograph shows perihilar irregular linear opacities and patchy areas of consolidation. A thin-walled cyst is seen in the left upper lobe. PCP was diagnosed with bronchoscopy. (b) Sevenmonths later, the chest radiograph shows an irregular cavity in the left upper lobe at the siteof the previously noted cyst. A cavitary mass is noted centrally within the cavity. A few pen-hilar linear opacities are seen. (c) Thin-section CT scan through the upper lobes shows an in-regular, thick-walled cavity with an intracavitany mass, which is also cavitated. A few, irregu-
lar linear areas of increased attenuation and subpleural cysts are seen in both lung apices.After left upper lobectomy, the predominant pathologic findings were an Aspergillus abscesswith an intracavitary mass and adjacent angioinvasion.
412 #{149}Radiology August 1995
the other patient, no organism wasidentified at pathologic examination.Coexisting infections with Pseudomo-nas and Streptococcus organisms were
present within the areas of consolida-tion in three patients.
Patient 1 also had prominent, ir-regular linear opacities on the chestradiograph and linear areas of in-
creased attenuation on the CT scan.This could be directly correlated with
granulomatous PCP in the pathologicspecimen. There was no evidence tosuggest that aspergillosis was respon-
sible for the irregular linear pattern.Patient 2 also had an Aspergillus
empyema. Patient 3 had pneumoperi-cardium and pericardial effusion andthickening. This latter patient had a2-cm defect in the pericardium thatcommunicated with the left lowerlobe. Multiple shallow ulcerationswere seen at pathologic examinationthat correlated with multiple subpleu-ral nodules at CT (Fig 3). In this pa-tient, A furningatus was also present inthe pericardium and myocardium.
DISCUSSION
Neutropenia and treatment withcorticosteroids are well established
risk factors for the development ofinvasive aspergillosis (10). Invasiveaspergillosis also occurs in patientswith advanced AIDS.
Cystic pulmonary lesions in pa-tients with AIDS have also been sug-
gested as a possible risk factor for thedevelopment of pulmonary aspergil-losis (4-10). In our study, five of 10patients had cystic or cavitary lesionsthat predated the location and subse-quent development of cavitary asper-gillosis.
Several forms of pulmonary asper-gillosis have been described, includ-ing allergic noninvasive, semi-inva-sive, and invasive (6). These variousforms usually occur in distinct sub-populations, although virtually allforms have been described in patients
with AIDS (5,7,10,11). A range ofpathologic manifestations was alsoobserved in the present study andincluded angioinvasion, pneumonia,abscess formation, tissue invasion
without obvious vascular invasion,
chronic necrotizing cavitary aspergil-losis, empyema, and myocardial inva-
sion. Several patients had more thanone manifestation.
The results of previous clinicalstudies have shown that the radio-graphic manifestations of invasiveaspergillosis in patients with AIDS areheterogeneous; the most commonabnormalities reported include cavi-
tary lesions (29%-42%), focal alveolar
or nodular opacities (22%-57%), andbilateral interstitial or alveolar infil-trates (23%-55%) (1,2,10). The fre-quency of cavitary lesions was higherin our study; they were seen in 80%
of patients on the chest radiographsand in 100% on CT scans. Similar toprevious reports, cavities showed anupper lobe predominance (10). Thefrequencies of noncavitary pulmo-nary nodules (40%) and consolidation(60%) were similar to those of previ-ous reports, but interstitial infiltrates
were distinctly uncommon in our se-ries. Irregular linear opacities seen inonly one patient were due to granulo-matous PCP at pathologic examina-tion.
CT scans, available in seven pa-tients, better delineated abnormalitiessuch as cavity wall thickness and
yielded additional information in allseven patients. Pleural and pencardialeffusions, nodules, and cavities with
or without intracavitary masses were
identified more commonly with CTthan with radiography. One case ofmediastinal lymphadenopathy wasmissed on the corresponding radio-graphs. All patients, however, hadabnormal chest radiographs. Further-
more, the interval time between chestradiography and CT may have ac-counted for some of the differencesbetween the radiographic and CTfindings.
All cavitary lesions examined
pathologically could be attributed di-rectly to aspergillosis and were eithercaused by infarcts, necrosis, or ab-scesses. Intracavitary masses on the
chest radiograph correlated with thepresence of intracavitary masses of

b. C.
Volume 196 #{149}Number 2 Radiology #{149}413
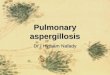
Figure 3. Patient 3. Invasive pleuropulmonary, penicardial, and myocardial aspengillosis in a47-year-old man. (a) Posteroantenor chest radiograph shows a left hydropneumothorax, ill-defined subpleural nodules, and patchy consolidation in the left lower lobe. (b) ConventionalCT scan through lower lung zones shows consolidation in the lingula and multiple nodules inthe left lower lobe. A subpleural nodule has cavitated and ruptured into the pleural space (ar-row). Note the pneumopencardium. (c) Low-power photomicrograph from a small area of
consolidation shows tissue necrosis that involves a small airway and subtends alveolar ductsand alveoli. Scattered Aspergillus organisms could be identified in the necrotic tissue. (Hema-
toxylin-eosin stain; original magnification, x 34.)
necrotic lung and Afumingatus at
pathologic examination. Noncavitarynodular lesions apparent on radio-graphs were also correlated directlywith infarcts or tissue invasion in allseven pathologic specimens withnodules. CMV inclusions were seen atpathologic examination in all sevenpatients with nodules. Although arecent report by McGuinness et al (12)noted masses and nodules in 57% ofcases of CMV infection confirmedwith cytopathologic examination,CMV was not the cause of nodules inour series. Mycobacterial infection,Kaposi sarcoma, and pneumonia dueto Pseudomonas organisms may have
accounted for some of the nodules inthree patients.
The pathogenesis of the consolida-tion in six patients with availablepathologic correlation was heteroge-neous and included tissue invasionwith A fumigatus centered on distal
respiratory bronchioles and alveolar
ducts, pneumonia due to A fumigatus,infarction, diffuse alveolar damage,
pyogenic pneumonia, and pneumo-
nia with no obvious cause in one pa-tient. Associated CMV inclusions
were identified in four patients butdid not contribute substantially toconsolidation. In three patients withconsolidation on radiographs butwithout pathologic correlation, infec-tion with Pseudomonas organisms and
streptococcal pneumonia likely con-
tributed to the abnormalities.Invasion of the pleura was uncom-
mon in our series and occurred inonly two patients. The two patientswith invasive pleuritis and empyema
had effusions apparent on radio-
graphs.Our study has several limitations.
First, all patients had concomitant
pulmonary complications other thanaspergillosis. These associated infec-tions likely contributed to the radio-graphic features of nodules, consoli-dation, and linear opacities in somepatients. These infections, however,apparently did not cause cavitary le-sions. The high frequency of associ-ated infection probably reflects theadvanced stage of AIDS in these pa-
tients. Associated illnesses were alsoprevalent in other series (10). Second,
to directly compare the radiographicand CT findings with the macroscopicand histologic findings in pathologicspecimens, the study was limited topatients who had undergone lobec-tomy, pneumonectomy, or autopsy.This likely biased the study to pa-tients with severe complications.
Third, only four patients underwent
thin-section CT. This may account for
the lack of visualization of airway ab-normalities in patients with histologic
evidence of airway invasion.Although the presence of thick-
walled irregular cavitary lesions in
patients with AIDS should suggestthe possibility of invasive aspergillo-
sis, other conditions must be consid-ered in the differential diagnosis. PCP
usually produces thin-walled cysts
but occasionally may produce thick-walled cavities (13). Pyogenic ab-scesses, septic emboli, lymphoma, andbronchogenic carcinoma may alsocause similar findings. Fungal infec-tions other than invasive pulmonary

414 #{149}Radiology August 1995
aspergillosis may also produce cavi-tary lesions in patients with AIDS(13). The differential diagnosis of non-cavitary nodules includes other dis-seminated fungal infections and my-cobacterial infection, as well as AIDS-related malignancies.
In conclusion, invasive aspergillosisis an increasingly common infectionwith a high mortality in patients withadvanced AIDS. Single or multipleupper lobe cavities with thick irregu-lar walls are strongly suggestive ofinvasive aspergillosis. When invasiveaspergillosis is suspected, CT may behelpful to better define the natureand extent of the abnormalities. #{149}
References1. Klapholz A, Solomon N, Perlman DC, Tala-
vera W. Aspergillosis in the acquired im-munodeficiency syndrome. Chest 1991;
100:1614-1618.
2. Singh N, Yu VL, Rihs JD. Invasive aspen-gillosis in AIDS. South Med J 1991; 84:822-827.
3. Fairley CK, Kent SJ, Street A, Mijch A, HoyJ. Invasive aspergillosis in AIDS. Aust NZJ Med 1991; 21:747-749.
4. Lortholary 0, Meyohas MC, Dupont B,Cadranelj, Salmon-Ceron D. Invasiveaspergillosis in patients with acquired tin-munodeficiency syndrome: report of 33cases. AmJ Med 1993; 95:177-187.
5. Denning DW, Follansbee SE, Scolaro M,.Norris 5, Edelstein H, Stevens DA. Pul-monary aspergillosis in the acquired imm#{252}-nodeficiency syndrome. N EnglJ Med1991; 324:654-662.
6. Fraser RS. Pulmonary aspergillosis:pathologic and pathogenetic features.Pathol Annu 1993; 28(pt 1):231-277.
7. Wright JL, Lawson L, Chan N, Filipenko D.An unusual form of pulmonary aspergillo-sis in two patients with the acquired tin-munodeficiency syndrome. AmJ ClinPathol 1993; 100:57-59.
8. Morrison DL, Granton jT, Kesten 5, BalterMS. Cavitary aspergillosis as a complica-tion of AIDS. Can Assoc RadiolJ 1993; 44:35-38.
9. Torrents C, Alvarez-Castells A, Vicente deVera P, Coll S, Solduga C, Puy R. Post-
pneumocystis aspergilloma in AIDS: CTfeatures. J Comput Assist Tomogr 1991;15:304-307.
10. Miller WTJr, Sais GJ, Frank I, Gefter WB,AronchickJM, Miller WT. Pulmonary as-pergillosis in patients with AIDS. Chest1994; 105:37-44.
11. Perves NK, Kleinerman J, Kattan M, et aLPseudomembranous necrotizing bronchialaspergillosis. Am Rev Respir EMs 1985; 131:%1-963.
12. McGuinness C, Scholes jV, Garay SM, Leit-man BS, McCauley DI, Naidich DP. Cyto-megalovirus pneumonitis: spectrum of CTparenchymal findings with pathologic cor-relation in 21 AIDS patients. Radiology1994; 192:451-459.
13. Kuhlman JE, Kavuru M, Fishman EK,
Siegelman SS. Pneumocystis carinii pneu-monia: spectrum of parenchymal CT find-ings. Radiology 1990; 175:711-714.