Embed Size (px)
Citation preview
Radical Changes For Our Future: In and Outside the OR
Radical Changes For Our Future: In and Outside the OR
Keith P. Lewis, RPh, MDChairman, Department of Anesthesiology
Keith P. Lewis, RPh, MDChairman, Department of Anesthesiology
Boston University School of Medicine
May 20, 2006
Boston University School of Medicine
May 20, 200612:00-12:30pm12:00-12:30pm
2nd Annual Ellison Pierce Symposium Positioning Your ORs For The Future
What Upcoming Changes Will Have A Major Impact on the Way We Practice?
What Upcoming Changes Will Have A Major Impact on the Way We Practice?
The Arrival of Rapid Neuromuscular Reversal
The Arrival of Rapid Neuromuscular Reversal
• Sugammadex – Org 25969 (GC derivative)
• Selective relaxant binding agent
• Rapid reversal of rocuronium/vecuronium
• Dose dependant reversal of moderate/deep blockade
• Safe reversal in less than 2 minutes!
• Sugammadex – Org 25969 (GC derivative)
• Selective relaxant binding agent
• Rapid reversal of rocuronium/vecuronium
• Dose dependant reversal of moderate/deep blockade
• Safe reversal in less than 2 minutes!
Why is Sugammadex So Different?Why is Sugammadex So Different?
• No muscle tone to full muscle tone in 2 min
• Encapsulate rather than antagonize
• Relative absence of side effects
• Implications for the difficult airway
• Reversal of a “mistake”
• “Basically its like putting an eraser on your pencil”*
• No muscle tone to full muscle tone in 2 min
• Encapsulate rather than antagonize
• Relative absence of side effects
• Implications for the difficult airway
• Reversal of a “mistake”
• “Basically its like putting an eraser on your pencil”*
*Dr. Groudine, Albany

Org 25969 (Sugammadex)Org 25969 (Sugammadex)
Coming to a Theater Near You: 1 YearComing to a Theater Near You: 1 Year
Major Changes in SurgeryMajor Changes in Surgery
• 70% of all surgical cases are now ambulatory
• 31.5 million cases/year in 2700 centers
• Shift to → more complex surgery, more office-based and minimally invasive
• Providing extended analgesia has limited the growth after painful procedures
• New SAFE (Short Acting Fast Emergence) agents readily available
• 70% of all surgical cases are now ambulatory
• 31.5 million cases/year in 2700 centers
• Shift to → more complex surgery, more office-based and minimally invasive
• Providing extended analgesia has limited the growth after painful procedures
• New SAFE (Short Acting Fast Emergence) agents readily available
Continuous Post-op Infusions in the Outpatient Setting
Continuous Post-op Infusions in the Outpatient Setting
• Pain control is often the reason for admission after ambulatory procedures
• Shift from neuroaxial to peripheral nerve blocks due to Black Box Warning (1997) of spinal hematoma and LMWH
• Self-administering local anesthetics via wound and perineural catheters (1998)
• Equipment for successful continuous peripheral nerve blocks now available
• Pain control is often the reason for admission after ambulatory procedures
• Shift from neuroaxial to peripheral nerve blocks due to Black Box Warning (1997) of spinal hematoma and LMWH
• Self-administering local anesthetics via wound and perineural catheters (1998)
• Equipment for successful continuous peripheral nerve blocks now available
The Application of Continuous Regional Anesthesia (CRA)
The Application of Continuous Regional Anesthesia (CRA)
• Femoral nerve or psoas compartment block for ACL
• Continuous interscalene brachial plexus for shoulders
• Patient-controlled interscalene brachial plexus block with improved PT, ↓ opioid, ↑patient satisfaction (Borgeat et al. Ay 1997;87:1343-71)
• Continuous sciatic nerve block for foot/ankle procedures
• Continuous wound perfusion: iliac bone crest harvesting
• Femoral nerve or psoas compartment block for ACL
• Continuous interscalene brachial plexus for shoulders
• Patient-controlled interscalene brachial plexus block with improved PT, ↓ opioid, ↑patient satisfaction (Borgeat et al. Ay 1997;87:1343-71)
• Continuous sciatic nerve block for foot/ankle procedures
• Continuous wound perfusion: iliac bone crest harvesting
This All Creates the Need for a Multidisciplinary TeamThis All Creates the Need
for a Multidisciplinary Team
• Shift of in-patient services to outpatient setting
• Traditionally the surgeon takes control
• Active role of anesthesiologist
• Resources from third party payors
• Shift of in-patient services to outpatient setting
• Traditionally the surgeon takes control
• Active role of anesthesiologist
• Resources from third party payors
Safety ConcernsSafety Concerns
• Discharge with an insensate extremity
• Risk of bodily injury
• 2382 long acting PNB’s with ropivicaine
-one patient fell going to car (0.2%)
• Catheter migration/dislodgement
• 24/7/365
• Discharge with an insensate extremity
• Risk of bodily injury
• 2382 long acting PNB’s with ropivicaine
-one patient fell going to car (0.2%)
• Catheter migration/dislodgement
• 24/7/365
New and Better Old Drugs Better New and Better Old Drugs Better
• Liposomes: sealed sacs in the micron range that contain water soluble drugs that can be slowly dispersed
• Postoperative analgesia for up to 4 days
• Microspheres 10-150 microns with duration of 10 hours to 5.5 days
• Dexamethasone increases duration of block in sheep up to 16 days
• Liposomes: sealed sacs in the micron range that contain water soluble drugs that can be slowly dispersed
• Postoperative analgesia for up to 4 days
• Microspheres 10-150 microns with duration of 10 hours to 5.5 days
• Dexamethasone increases duration of block in sheep up to 16 days
Where is Surgery Going?Where is Surgery Going?
Open Surgery
Laparoscopic Surgery
Robotic Camera Operation
Robotic Surgery
Telerobotic Surgery
Miniature Robots
Open Surgery
Laparoscopic Surgery
Robotic Camera Operation
Robotic Surgery
Telerobotic Surgery
Miniature Robots
Increasing Usage of Robotic SurgeryIncreasing Usage of Robotic Surgery
• Radical retropubic prostatectomy
• Cardiac surgery (valve, IMA)
• Uterine fibroids
• Esophageal resection
• Thoracic surgery
• Bariatric procedures
• Radical retropubic prostatectomy
• Cardiac surgery (valve, IMA)
• Uterine fibroids
• Esophageal resection
• Thoracic surgery
• Bariatric procedures
Smaller, Less Expensive TechnologiesSmaller, Less Expensive Technologies
• Light weight system: 250,000
• Table mounted, modular and compact, 2-0
• Feels like a laparoscopic hand with robotic capabilities
• Enter the room at any moment
• Weight: 12 years, 1200 pounds
• Surgeon console on sterile field
• Light weight system: 250,000
• Table mounted, modular and compact, 2-0
• Feels like a laparoscopic hand with robotic capabilities
• Enter the room at any moment
• Weight: 12 years, 1200 pounds
• Surgeon console on sterile field
• Smallest/least painful incisions
• No external incisions:
Utilize pre-existing orifice
Stomach to peritoneum
Insufflate peritoneal cavity
Specimen out through mouth
• Smallest/least painful incisions
• No external incisions:
Utilize pre-existing orifice
Stomach to peritoneum
Insufflate peritoneal cavity
Specimen out through mouth
What Will Our Patients Want?
Flexible transgastric peritoneoscopy: a novel approach to diagnostic and therapeutic interventions in the peritoneal cavity. Kalloo AN et al, Gastrointest Endosc. 2004 Jul;60(1):114-7.
Will there be widespread use in urology?
Will it become the standard of care?
Will there be widespread use in urology?
Will it become the standard of care?
“There is no such thing as science fiction, only scientific eventuality”
Steven Speilberg
“There is no such thing as science fiction, only scientific eventuality”
Steven Speilberg
The Key To Our Success Will Be….
The Key To Our Success Will Be….
Preventing Errors Before They HappenPreventing Errors Before They Happen
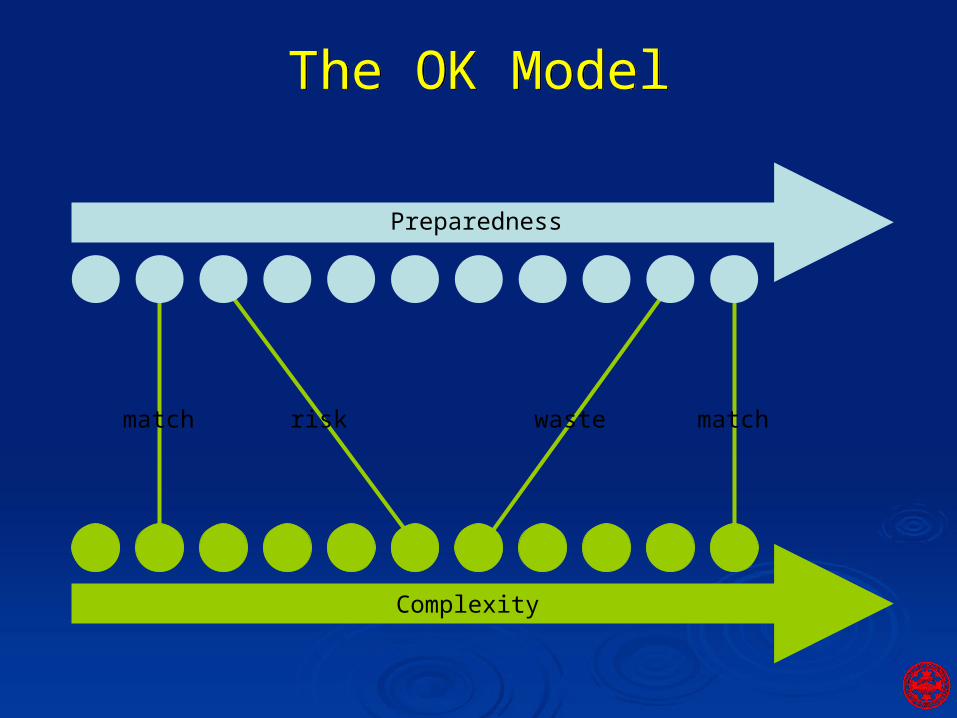
wasterisk matchmatch
Complexity
Preparedness
The OK ModelThe OK Model
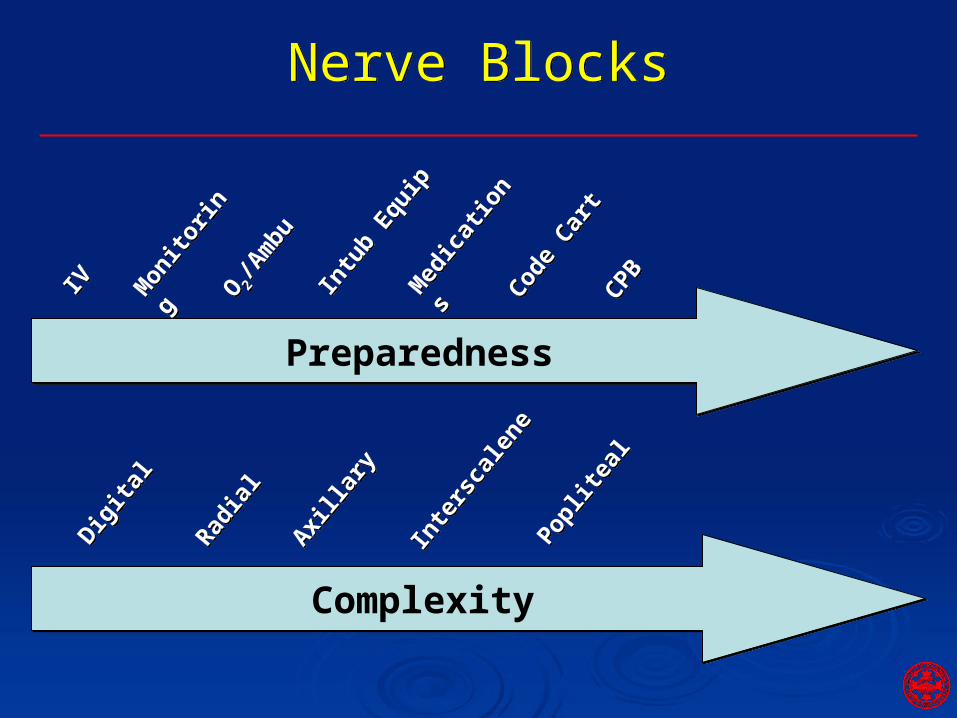
ComplexityComplexity
Digita
l
Digita
l
Radia
l
Radia
l
Axilla
ry
Axilla
ry
Inte
rsca
lene
Inte
rsca
lene
Poplit
eal
Poplit
eal
PreparednessPreparedness
IVIV Mon
itorin
g
Mon
itorin
gO 2
/Am
bu
O 2/A
mbu
Intu
b Equ
ip
Intu
b Equ
ipM
edic
atio
ns
Med
icat
ions
Code
Cart
Code
Cart
CPBCPB
Nerve BlocksNerve Blocks
Ultrasound/Imaging to Minimize Risk
Ultrasound/Imaging to Minimize Risk
• Identify nerves and surrounding structures
• Avoid intravascular injection
• Avoid nerve stimulation
• Avoid paresthesias
• Monitor spread of local anesthetic
• 95% success rate
• Identify nerves and surrounding structures
• Avoid intravascular injection
• Avoid nerve stimulation
• Avoid paresthesias
• Monitor spread of local anesthetic
• 95% success rate
Ultrasonography and PNB’sUltrasonography and PNB’s
• Available at bedside
• Portable
• Non-invasive
• Can be used in the OR
• Affordable
• Available at bedside
• Portable
• Non-invasive
• Can be used in the OR
• Affordable
Anesthesiology: Ultrasound Guided Vascular Access
Anesthesiology: Ultrasound Guided Vascular Access
• Identify target vessel
• Determine size, location, patency
• Identify abnormal anatomy and variations
• Minimize unsuccessful needle sticks
• Improves efficiency and proficiency
• Avoid vital structures– Unintended arterial punctures
– Pneumothorax
– Hematoma
• Reduce patient discomfort and anxiety
• Identify target vessel
• Determine size, location, patency
• Identify abnormal anatomy and variations
• Minimize unsuccessful needle sticks
• Improves efficiency and proficiency
• Avoid vital structures– Unintended arterial punctures
– Pneumothorax
– Hematoma
• Reduce patient discomfort and anxiety
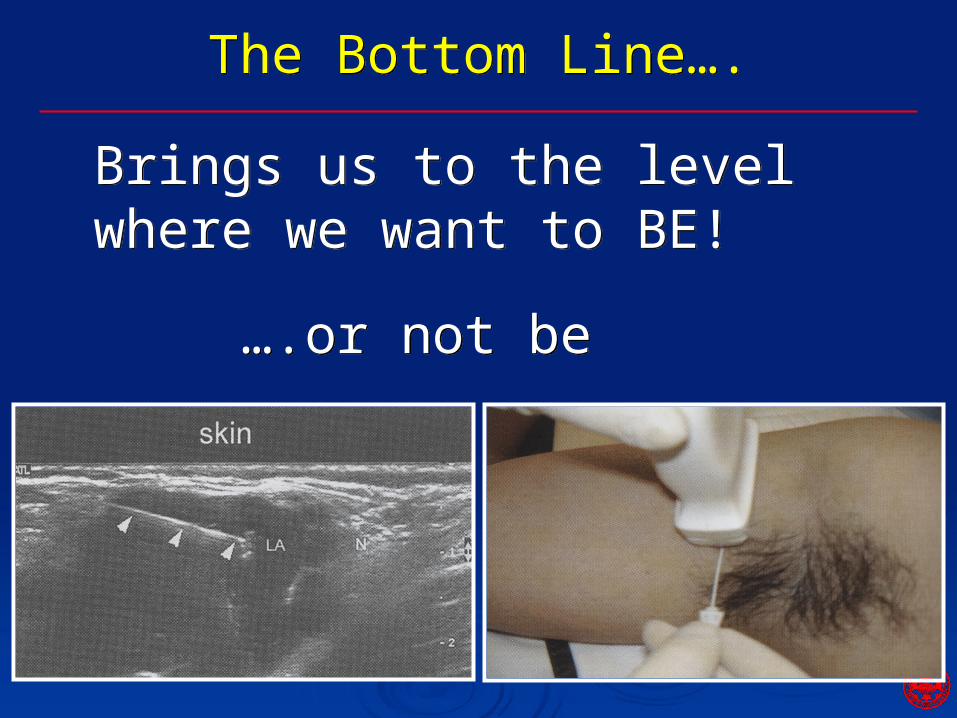
The Bottom Line….The Bottom Line….
Brings us to the level where we want to BE!Brings us to the level where we want to BE!
….or not be….or not be
Earlier and Earlier DischargeEarlier and Earlier Discharge
• Total knee arthroplasty LOS 4-5 days
• Utilize ambulatory continuous femoral nerve block
• Multimodel analgesia regimen at home
• In place for 4 days
• Good pain control and minimal sleep disturbances
• Patients discharged POD 1
• What’s Next: Nissen, CEA, Thyroid??
• Total knee arthroplasty LOS 4-5 days
• Utilize ambulatory continuous femoral nerve block
• Multimodel analgesia regimen at home
• In place for 4 days
• Good pain control and minimal sleep disturbances
• Patients discharged POD 1
• What’s Next: Nissen, CEA, Thyroid??
Anesth Anal 2006;102:82-90
Wireless MonitoringWireless Monitoring
• Facilitate transport and early ambulation
• Wireless nondisposable biomedical sensor prototype (WisMos)
• Same accuracy as with a wired sensor
• Standard OR equipment with no interference
• WisMos Prototype: Displays 3 invasive BPs, and 2-channel, 5 lead ECG’s
• Future version: pulse oximetry and 2 Temps
• Facilitate transport and early ambulation
• Wireless nondisposable biomedical sensor prototype (WisMos)
• Same accuracy as with a wired sensor
• Standard OR equipment with no interference
• WisMos Prototype: Displays 3 invasive BPs, and 2-channel, 5 lead ECG’s
• Future version: pulse oximetry and 2 Temps
Oyr: Anesth Analg 2006;102-478-83
Airways with a ViewAirways with a View
• ETT with an embedded tiny video camera
• Continuous visual control of intubation procedure
• Effective ventilation when in place
• Continuous monitoring of ETT position
• Application to first responders, ER, resuscitation and telemedicine
• ETT with an embedded tiny video camera
• Continuous visual control of intubation procedure
• Effective ventilation when in place
• Continuous monitoring of ETT position
• Application to first responders, ER, resuscitation and telemedicine
We Will Figure Out How Inhalation Agents Work?
We Will Figure Out How Inhalation Agents Work?
• Certain nematodes shares 60% of the genes in humans
• Isoflurane delivered via a gas chamber - distance traveled, speed, top speed, roaming range, track patterns
• Number of genes associated with isoflurane response narrowed to 10 mutations
• Finding may help design more specific anesthetic agents without affecting other brain functions leading to untoward effects
• Certain nematodes shares 60% of the genes in humans
• Isoflurane delivered via a gas chamber - distance traveled, speed, top speed, roaming range, track patterns
• Number of genes associated with isoflurane response narrowed to 10 mutations
• Finding may help design more specific anesthetic agents without affecting other brain functions leading to untoward effects
Meiler, ASA 2005
Alternative to Inhaled Anesthetics: Xenon
Alternative to Inhaled Anesthetics: Xenon
• Rapid induction/recovery and CV stability
• Lowest blood-gas coefficient (0.115)
• Similar recovery time with propofol/remifentanil
• Beneficial cardiovascular effects
• Rapid induction/recovery and CV stability
• Lowest blood-gas coefficient (0.115)
• Similar recovery time with propofol/remifentanil
• Beneficial cardiovascular effects
Br. J Anesth 2005;94:198-202
AnesthesiologyMay Go
Molecular
AnesthesiologyMay Go
Molecular
The Operating Room & Perioperative Clinical Genomics
The Operating Room & Perioperative Clinical Genomics
“The OR is the last physiology laboratory in medicine”
“The OR is the last physiology laboratory in medicine”
Perioperative Genomics:Perioperative Genomics:
• Polymorphisms (genetic variations) have been categorized
• May become part of OR arsenal to ENSURE PATIENT SAFETY
• Marathon Runner: O2 consumption ↑ 15X, CO2 exhalation ↑ 8X, HR 200, catecholamines double
• CPB: 10X ↑ in catecholamines (dopamine, norepinephrine, epinephrine)
• Bottom Line: Examine DNA changes to PREDICT negative surgical outcome
• Polymorphisms (genetic variations) have been categorized
• May become part of OR arsenal to ENSURE PATIENT SAFETY
• Marathon Runner: O2 consumption ↑ 15X, CO2 exhalation ↑ 8X, HR 200, catecholamines double
• CPB: 10X ↑ in catecholamines (dopamine, norepinephrine, epinephrine)
• Bottom Line: Examine DNA changes to PREDICT negative surgical outcome
Adverse Outcomes StudiedAdverse Outcomes Studied
• Myocardial ischemia
• Postoperative arrhythmias
• Vein graft restenosis
• Neurocognitive dysfunction
• Stroke
• Bleeding/Thrombosis
• Sepsis
• Death
• Myocardial ischemia
• Postoperative arrhythmias
• Vein graft restenosis
• Neurocognitive dysfunction
• Stroke
• Bleeding/Thrombosis
• Sepsis
• Death
Will Cardiology Consults Become Extinct?
Will Cardiology Consults Become Extinct?
Avoid hypertension, tachycardia, volume overload and consider invasive monitoring including a PAC. Strongly recommended the use of perioperative B-blockers to minimize cardiovascular risk. Straight local or block would be preferred to GA.
Avoid hypertension, tachycardia, volume overload and consider invasive monitoring including a PAC. Strongly recommended the use of perioperative B-blockers to minimize cardiovascular risk. Straight local or block would be preferred to GA.
Where Will We Be in 2025?Where Will We Be in 2025?
• Critical care beds hit 50% in teaching hospitals
• Robotics, information intensive layouts, voice activation
• Credentialing based on demonstrated competence
• Turf wars
• Imaging and invasive catheters over surgery
• Genetic-molecular medicine
• Drugs with little or no risk
• Critical care beds hit 50% in teaching hospitals
• Robotics, information intensive layouts, voice activation
• Credentialing based on demonstrated competence
• Turf wars
• Imaging and invasive catheters over surgery
• Genetic-molecular medicine
• Drugs with little or no risk
ASA Task Force 2004
Opportunities for the FutureOpportunities for the Future
• Hospital leaders in the future
• Diversification of practice paradigm
• Interventional pain management
• Outpatient palliative care
• The rapid changes are already taking place
• Are you capable of changing and adapting yourself for the future?
• Hospital leaders in the future
• Diversification of practice paradigm
• Interventional pain management
• Outpatient palliative care
• The rapid changes are already taking place
• Are you capable of changing and adapting yourself for the future?
The answer must be YES since your are…The answer must be YES since your are…
attending “Positioning Your OR’s For the Future”attending “Positioning Your OR’s For the Future”

Moving ForwardMoving Forward
Let’s take charge of:
OUR FUTURE!
…as opposed to having our future taken charge of by
others
Let’s take charge of:
OUR FUTURE!
…as opposed to having our future taken charge of by
others
http://www.dennisbike.com/images/up%20the%20garden%20climb,jacques-maynes%20taking%20charge%20of%20the%20pace_std.jpg

Thank You for attending our symposium!
Thank You for attending our symposium!
Ether MonumentEther Monument