Embed Size (px)
Citation preview

1
Greg Sackett, M.S., CHPMedical Physicist
Radiation Safety Issues for Radiologic Technologists
Radiation Worker Risks?
2
Patient Risks?
l Acute Effects?l Delayed Effects?l Patient Questions?
Radiation Dose Limits
l Dose limits are used to provide a basis for radiation worker safety
l Whole body limits are designed to reduce stochastic risk (i.e. cancer) to less than 1 in 10,000/yr (10-4 yr-1)
l Risk Equivalent to “Safe” Occupations l Additional limits are designed to reduce
deterministic effects (i.e. cataracts)

3
NCRP Dose Limits
Category mrem/yr
Effective dose (whole body) 5000
Lifetime Effective dose 1000 x age
Lens of eye 15,000
Organs, skin, extremities 50,000
Public (frequent exposure) 2% of rad worker (100 mrem)
Public (infrequent exposure) 10% of rad worker (500 mrem)
Embryo/Fetus Total 500
Embryo/Fetus monthly 50
Regulatory Dose Limits
Body Part NRC/KS Limit (mrem/yr)
MO Limit (mrem/yr)
Whole Body 5000 5000
Lens of Eye 15000 5000
Extremities 50000 75000
Pregnant Worker 500 500
Public 100 100

4
Typical Occupational Exposures
Category Avg. Annual Dose (mrem)
Uranium miners 1200
Nuclear power operations 600
Airline crews 170
Rad and NM Techs 100
Radiologists (Non-Interventionalist)
70
Scatter - The Source of Operator Exposure
l Staff do not receive exposure from the primary x-ray beam
l Exposure comes from scattered radiation as soon as the beam strikes an object (usually the patient or table)– Larger patients = more scatter– Higher kVp/mAs = more scatter– Larger field of view = more scatter
5
Cardinal Principles of Radiation Protection*
TimeDistanceShielding
*External Exposure Hazards Only
Time
The amount of exposure an individual receives is directly proportional to the time of exposure. Therefore, minimize the amount of time spent with a radiation source.
Exposure = Exposure Rate x Time

6
Time
l Time of fluoro procedures should be kept to a minimum
l Fluoro should alternate on-off, rather than constant on
l “Pulsed Progressive” fluoro can reduce patient and caregiver dose by 90% or more
l Fluoroscopes have 5 minute reset timers to remind users of time elapsed
Distance
(Doubling the distance from the source will decrease the exposure by four)
7
Distance
l X-ray, CT, LINAC – staff should be outside the room (or behind shielding) when machine is on
l Fluoro – remain as far away from patient as possible when fluoro is on
l Just two steps back can greatly reduce exposure
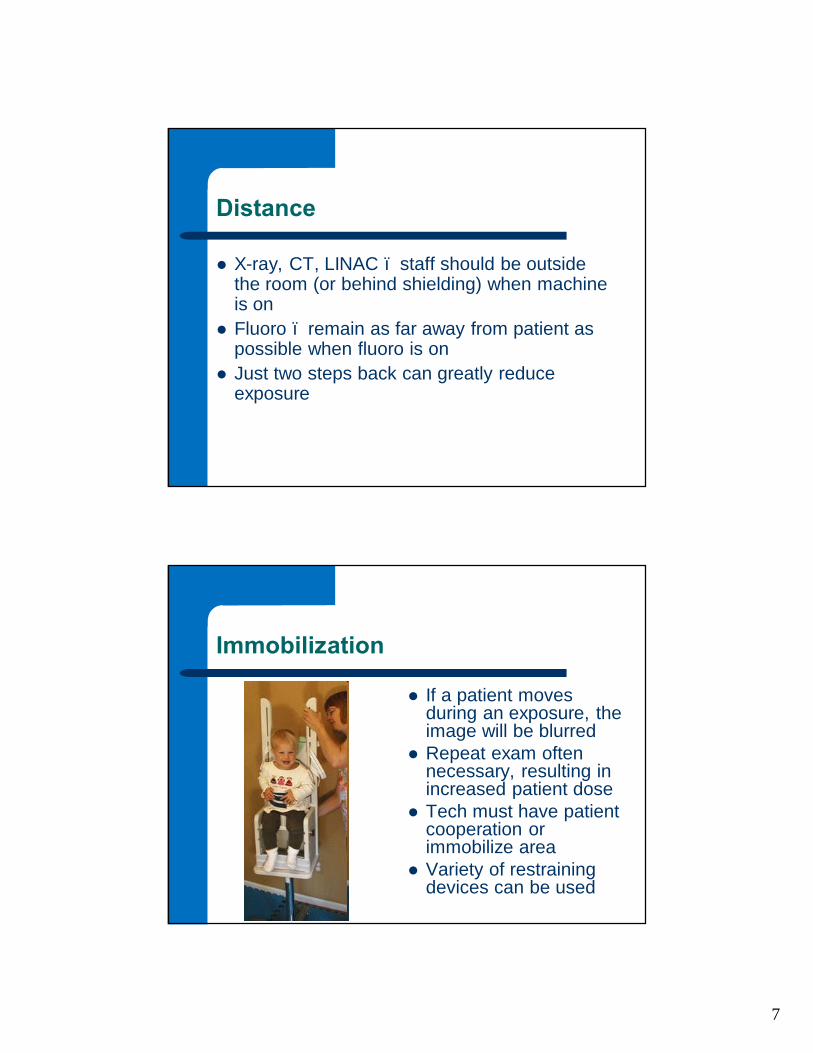
Immobilization
l If a patient moves during an exposure, the image will be blurred
l Repeat exam often necessary, resulting in increased patient dose
l Tech must have patient cooperation or immobilize area
l Variety of restraining devices can be used

8
Patient Holding
l Mechanical devices should be used
l If mechanical device impractical, then relative or friend of patient should hold
l Non-radiology workers could be used as last resort
l Protective apparel should always be worn by holder
l In some states, techs holding patients is illegal or log books are required
Shielding
Any object between you and a source of radiation will provide some shielding. In general, the more dense an object or material, the better the shield.

9
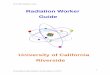
Protective Apparell Must be worn during fluoro and
possibly mobile imagingl Lead aprons do not stop 100% of x-
raysl Recommended to contain at least
0.5mm lead equivalentl CV and Interventionals should use
wrap-around apronsl Aprons must be inspected annually
for leaks and stored appropriatelyl Correction factors may be applied
for personnel dose calculations
Apron Effectiveness

10
Additional Shielding
l Drapes and equipment aprons
l Ceiling mounted face shields (can reduce exposure by up to 40 times!)
l Mobile shields for stationary staff like anesthesia techs (can virtually eliminate exposure)
Radiation Safety by Modality
l Fluoroscopyl Interventionall Mammographyl CTl Surgeryl Mobile

11
Fluoroscopy
l Personnel exposure directly related to “beam on” time
l Tube should be below patient
l Techs should use ALARA principles to reduce dose– Time– Distance– Shielding
Interventional Radiology and Cardiology
l Exposures higher due to longer “beam on” time for procedures and cineradiography
l Extremity exposures often significant
12
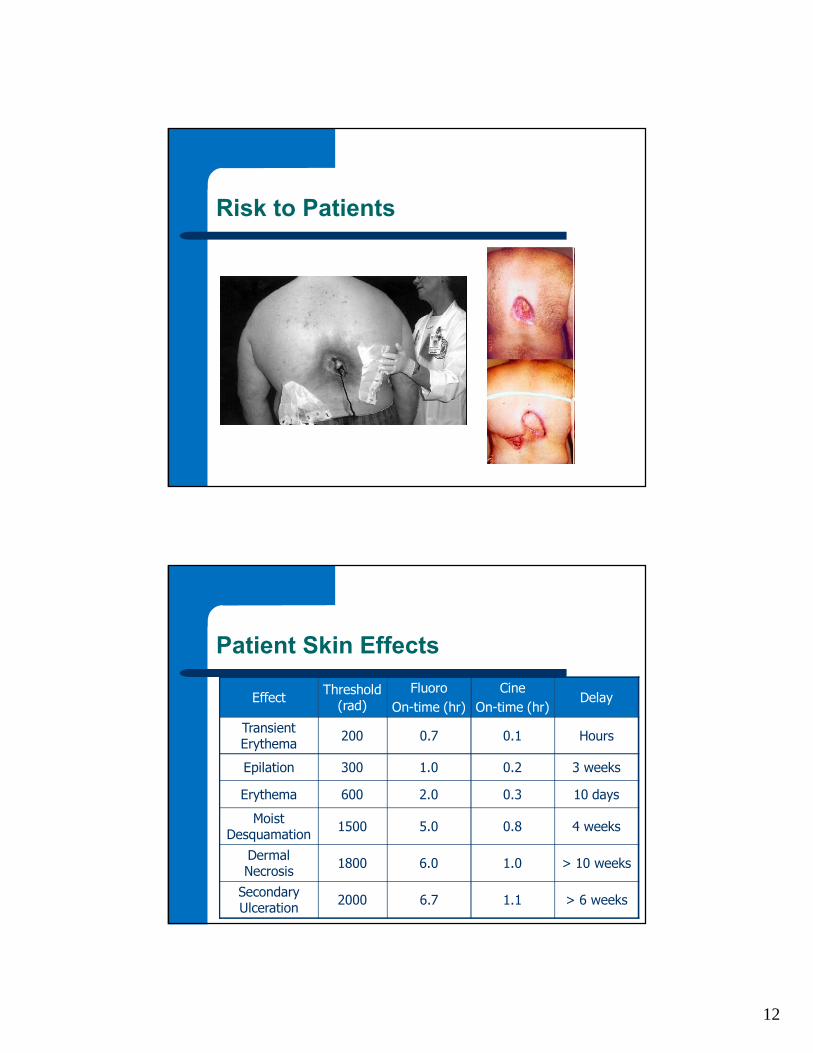
Risk to Patients
Patient Skin Effects
Effect Threshold (rad)
FluoroOn-time (hr)
Cine On-time (hr)
Delay
Transient Erythema 200 0.7 0.1 Hours
Epilation 300 1.0 0.2 3 weeks
Erythema 600 2.0 0.3 10 days
Moist Desquamation 1500 5.0 0.8 4 weeks
Dermal Necrosis 1800 6.0 1.0 > 10 weeks
Secondary Ulceration 2000 6.7 1.1 > 6 weeks

13
Typical Patient Dose
Procedure Patient DoseTIPS 217 rad
Nephrostomy 25.8 rad
Neuroembolization—Head 198 rad
Neuroembolization—Spine 374 rad
IVC Filter Placement 19.3 rad
Biliary Drainage 78.1 rad
Hepatic Embolization 196 rad
Percutaneous CoronaryIntervention
200 rad
PTCA & CA 141 rad
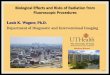
Projections
Vertical PA 30° from Vertical

14
Projections
Horizontal Vertical AP(not recommended)
Proximity of C-Arm to Patient
l Place detector as close to patient as possible– Will reduce patient
dose and scatterl Place tube as far from
patient as possible– Do not remove
spacer cones

15
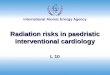
Collimation
• Collimate tightly to the area of interest.• Reduces the patient’s
total entrance skin exposure.
• Improves image contrast.
• Scatter radiation to the operator will also decrease.
Collimation
l Always collimate as much as possible
l If the video image is circular you aren’t collimating
16
Mammography
l Low personnel exposures
l Normal walls and barriers adequate
l Dosimetry probably not required
Mammography Dose
l Primary impact on patient dose is number of views (ESE~800 mrem/view)
l Therefore, for screening, no more than 2 views per breast recommended (4 for implants)
l Tomosynthesis doses are higher but will likely prevent additional views
l Thyroid shields are not required
17
Computed Tomography
l Personnel exposures low
l Collimated beam results in low scatter
l Personnel can remain in room if necessary with lead aprons
CT Patient Doses
l Only 5% of all exams are CT, yet CT accounts for ~35% of patient dose
l Approximately 3000 to 5000 mrad for head scan
l 2000 to 4000 mrad for body imaging
l Highly collimated beam allows for avoidance of radiosensitive organs
l Patient shielding not usually necessary

18
CT Patient Doses
l Patient doses can be large (> 6 Gy)
l Dependent upon protocol techniques (so they should be reviewed)
l Machine reported CTDI is NOT the actual patient dose
CT Patient Doses
l

19
CT Dose
l Low noise, high resolution images result in high patient dose
l Goal is to produce best possible image with reasonable dose
l Key is proper review of protocols
Surgery
l Surgery personnel often concerned about doses
l Actual doses are generally low and staff are often not provided dosimetry
l Pain Clinic physicians may be the exception

20
Surgery
l Who runs the equipment?
l Portable c-arm safety techniques are similar to interventional rooms
l If image quality acceptable, use low dose settings
Mobile Radiography
l Usually low personnel doses
l Exposure cord long enough for tech to be out of scatter area
l Be aware of location of tube/image receptor
l Beware of other staff/patients/visitors

21
Mobile Radiography
l It is often not practical to stand more than 6 feet away
l Techs should wear apronsl Criteria for where to stand:
– Must be able to quickly access patient
– Must be able to communicate with patient
– Must be able to communicate with x-ray operator
Occupational Radiation Monitoring
l Required if worker expected to exceed 10% of annual limits (500 mrem)
l Some states require all machine users to wear dosimeters
l Dosimeters offer no protection, just record exposure

22
Dosimeter Location
l During fluoro procedures, dosimeter should be worn on the collar outside the lead apron
l For non-fluoro users, the NCRP recommends wearing the badge at the waist or chest
l Fetal badges should be worn at the waist, under a lead apron
Dosimetry Reports
l Dose data must be maintained indefinitely
l Reports deep dose, eye dose and shallow (skin) dose
l Maintains current, quarterly, annual and lifetime doses

23
X-Rays and Pregnancy
l Human body is most sensitive to radiation effects before birth
l Pregnant Patients?l Effects
– Time Dependent– Dose Dependent
Pregnant Workers
l Radiation workers who become pregnant are rarely at any significant risk of exposure
l Pregnant worker WILL be concerned about her exposure
l Training should be provided to inform her of potential risks and available options

24
• Pregnant worker may declare pregnancy to RSO
• Entitles worker to lower dose limits (500 mrem, 50 mrem/month)
• Additional monitoring (monthly)
• Possible change of duties• Cannot be forced to declare
pregnancy
Declared Pregnancy
Discussing Risk with Patients
Keys:l Tell the truth;l Use positive or neutral terms
and no jargon;l Use examples to help the
patient understand;l Don’t speculate, discuss only
the procedure being performed;l Do not attack the patient’s
beliefs or a source of misinformation;
l Ask if you are being understood.

25
Discussing Risk with Patients
l Risk of cancer induction is age dependent
l Remember to emphasize the BENEFITS of the procedure
l If you can’t answer question, refer to Radiologist or RSO
Radiation Safety Officer
l Many institutions have an RSO
l Required by Radioactive Materials License
l Often a Radiologist
26
Radiation Safety Officer Duties
l Ensure workplace safe for patients and staff
l Ensure compliance with state/federal regulations
l Provide safety training to staff
l Counsel patientsl Maintain records
Reducing Occupational Exposure
l 95% of tech doses come from fluoro and mobile radiography
l Use Time, Distance and Shielding to keep doses ALARA
l Pay attention to fluoro timesl Be aware of direction of primary beaml Use provided aprons and shields
27
Reducing Unnecessary Patient Dose
l Unnecessary examinations– Radiologist controlled
l Repeat Examinations– Tech controlled
l Radiographic Technique– High kVp/Low mAs
reduces patient dose– May result in lower
contrast
QUESTIONS?