Embed Size (px)
Citation preview
Quarantine Stations and the Control of M. tuberculosis
Institute of Medicine January 20, 2005
Sarah Royce, MD, MPH, ChiefTuberculosis Control Branch
California Dept Health [email protected]
(510) 540 2345
2
3
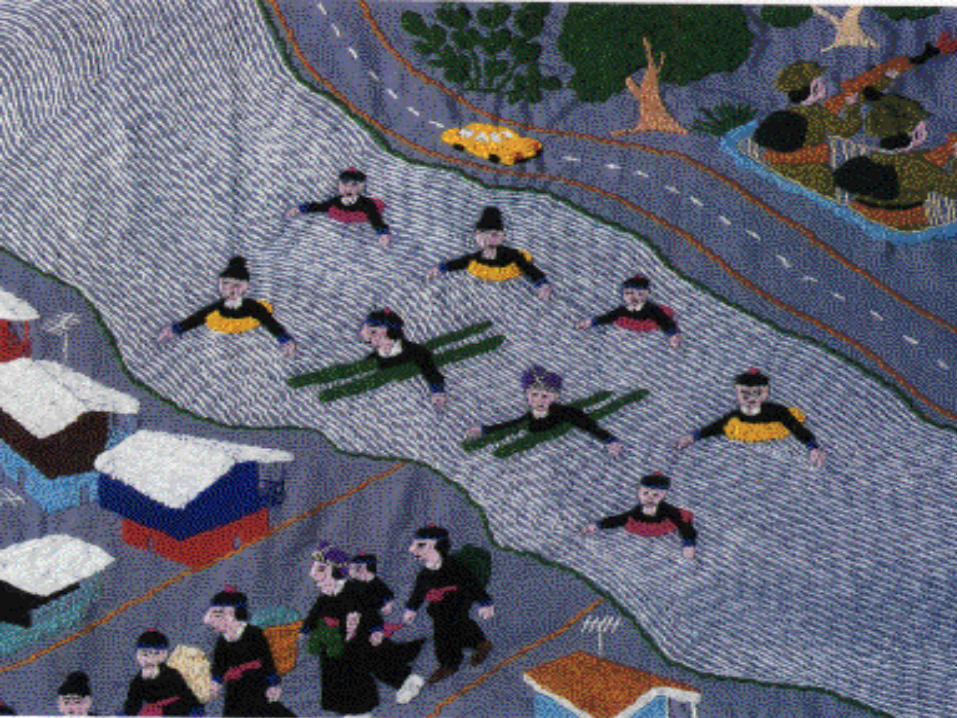
Arriving in America: Family lands in capital, the first of 16,000 Hmong coming to the US after waiting as refugees in Thailand
--Sacramento Bee, June 20, 2004
4
End of the Journey for a 41 Year Old Hmong Refugee, 2004THAILAND4/26: Normal CXR in immigration exam 5/12: Hospitalized, cavity on CXR, smear
positive sputum negative on TB RxCALIFORNIA6/16: Bangkok to LA to Sacramento6/17: Hospitalized: smear positive sputum6/25: Died7/27: M. tuberculosis, multidrug-resistant
5
Importation of M. tuberculosis, a Test of Public Health Protection at
our Nation’s Borders
• TB is “bread and butter” for quarantine stations
• “Getting it right” for TB will help quarantine stations prepare for emerging pathogens or bioterrorism agents
6
Quarantine Stations, with Health Department Partners, as a Public
Health Intervention*• Preventing TB cases and deaths
– Overseas TB screening– Domestic follow up
• Q stations, at our nation’s borders, – Bridge international and domestic
components– Maximize the public health benefits
* IOM Statement of Task
7
Overview
• California TB epidemiology• Purpose of overseas TB screening• Process• Outcomes—averting TB cases and deaths• Challenges• Roles of quarantine stations in maximizing
the benefits of this public health intervention
8
Impact of the Global TB Epidemic on California, 2003
• California reports the most TB cases of any state (3,227)
• 75% born outside the US• Most MDR-TB cases of any state (33
incident, nearly 70 prevalent cases)• Over 80% of MDR TB cases are in persons
born outside the US

9
Purpose of Overseas TB Screening of Immigrants and
Refugees
• Identify persons with suspected TB• Restrict entry of cases of infectious,
active TB disease• Facilitate entry of rest, so US health
departments can evaluate and treat

10
Overseas TB Screening AlgorithmChest radiograph
> 15 years old
Active TB
AFB sputum smears (3)
Inactive TB No TB
Infectious TB Class A
Noninfectious TB Class B1
All (-) (at least one +)
Class B2

11
Limits--Today’s Overseas Exams•Embassies select panel MDs•QA visits to 5% of panel MDs/y•Algorithm sensitivity,specificity•Rx w/o culture, susceptibility
12
13
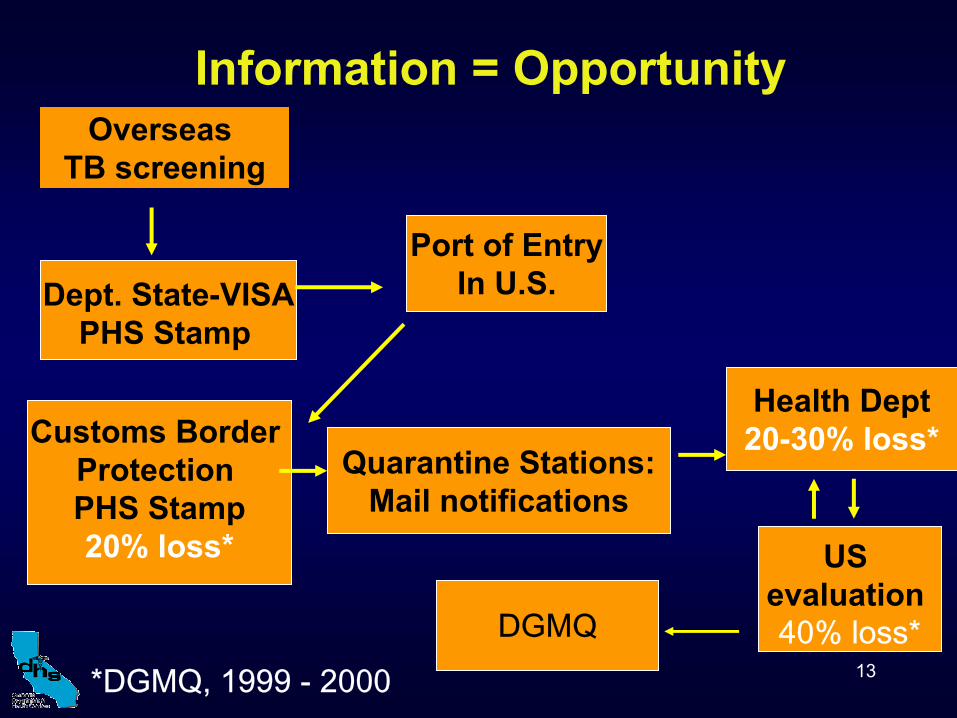
Information = OpportunityOverseas
TB screening
Dept. State-VISAPHS Stamp
Port of EntryIn U.S.
Customs Border Protection PHS Stamp20% loss*
Health Dept20-30% loss*
US evaluation40% loss*
Quarantine Stations:Mail notifications
*DGMQ, 1999 - 2000DGMQ

14
Domestic TB categorization
+ TB skin or blood test
NoneLatent TB infection
Abnormal chest x-ray,+ culture
CoughingActive TB Disease
N/ANoneNeither
LaboratorySymptoms
15
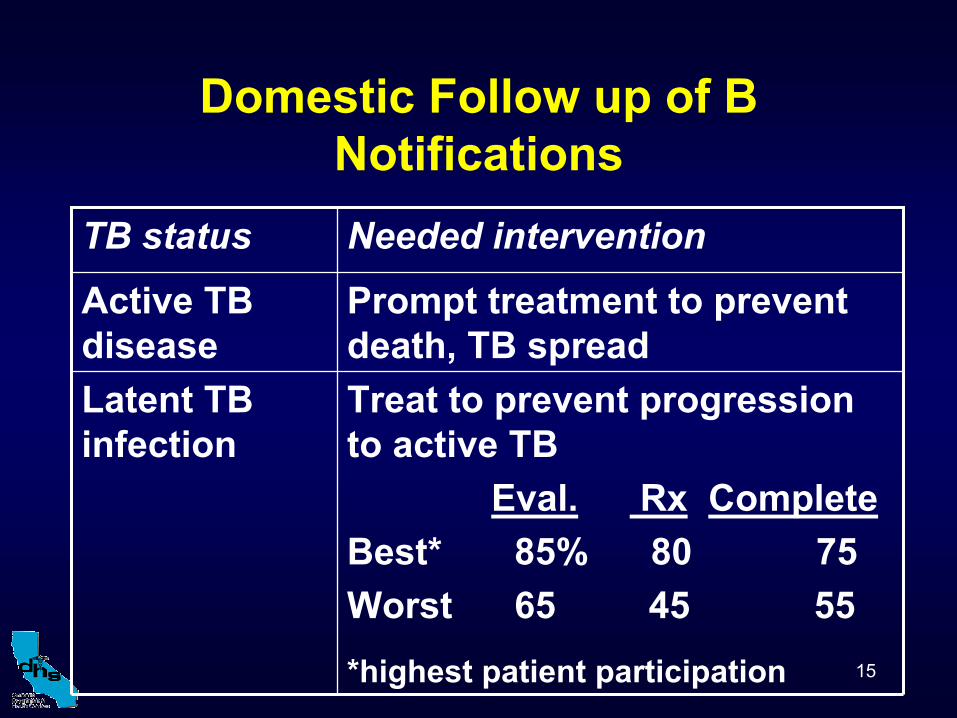
Domestic Follow up of B Notifications
*highest patient participation
Treat to prevent progression to active TB
Eval. Rx CompleteBest* 85% 80 75Worst 65 45 55
Latent TB infection
Prompt treatment to prevent death, TB spread
Active TB disease
Needed interventionTB status

16
B notification patients entering California, annually (1, 2)
4000100Total
198049.5Already treated, or no TB
188047Latent TB infection
140*3.5Active TB disease
#%TB status on entry
*20 smear positive, 2-6 MDR TB cases
17
B notification as Active Case Finding (1, 3)
• 5x higher yield of confirmed TB cases than contact investigation (3.5% vs. 0.7%)
• B notification patients are detected earlier--Within 3 months after arrival, vs. 5 months for TB cases* without B notification
* TB diagnosis within 1 year of arrival

18
Cost Effectiveness of Domestic Treatment of 4000 B notification
Patients Entering California/Year, Followed for 20 years (4)
savings494638Best*
savings280317Worst
Net cost perQALY
QALYsgained
TB deaths averted
TB cases averted
* Health depts with highest patient participation

19
Summary of Challenges
• Staffing, authority for quality assurance of overseas exams
• Timely, complete notification to domestic health departments
• Data available to assess/improve system• US health departments maximizing the
prevention of TB cases, deaths

20
IOM TB Report (5)
Federal TB Task Force (6,7)
• Improve quality of overseas TB exams
• Optimize follow-up of immigrants and refugees arriving in US with suspected TB
21
Q Station Roles: Improve Quality of
Overseas TB Exams
• Perform QA program visits overseas
• Provide ongoing consultation to panel MDs
• When things go wrong …
– Elicit feedback from US health departments
– Investigate, remediate systems failures

22
Q Station Roles: Optimize US Follow-up
• Oversee data collection, entry and use
• Assist US health departments to assess performance, set and reach objectives
• Identify, manage highest priority entrants
23
Quarantine Station Needs
1. A functional information system2. Sustainable funding3. Legal framework to enable effective
public health interventions
24
1. Electronic Data Network
• Improve timeliness, completeness • Close loop to allow assessment and to
direct interventions: individual, policy• Implement in Q stations, US health depts• Eventually: link overseas panel MDs,
expand to include ill arriving passengersFunding?
25
2. Start-up, Sustainable Funding: Options
• User fees
– Panel MD, immigrant applicant
– Airline ticket surcharge
• Emergency preparedness or CDC funding
• International organizations
• Medicaid

26
3. Legal Framework
• Medicaid coverage for immigrants during first 5 years in the US (made ineligible with 1996 Welfare Reform Act)
• Establish user fees, CDC authority for panel physicians
• Overseas TB screening for students, workers, visitors who plan to stay > 6 months
27
Summary: Overseas TB Screening, Domestic Follow up
• Life (and cost) saving• Q stations play a key role in improving
– both overseas, domestic components – bridges with overseas colleagues
• Need information system, funding and legal authority
• Health department partners who can provide feedback to improve overseas exams, and fully realize public health benefits of preventing TB and saving lives

28Estimates from U.S. Department of Homeland Security, 2003
Status adjusters in U.S.:679,305
Immigrants and refugees 411,266
Undocumented migrants ~ 275,000 ????
Non-immigrant visas27,907,139
N= ~ 59,000,000
Visitors without visas~ 30,000,000
Migrants “Entering” U.S., 2002
29
Civil Surgeons
Quarantine station staff could:
• Ensure quality of domestic TB exams for persons adjusting their immigration status*
• Select, train, accredit, oversee civil surgeons*
• Foster health department linkages
*Requires transfer of authority to CDC
30
References
1. Sciortino et al. Int J Tuberc Lung Dis 3(9):778-7852. deReimer et al. Arch Intern Med 158:753-760.3. Sprinson et al. Int J Tuberc Lung Dis 7(12):S363-S368.4. Porco et al. submitted for publication5. Institute of Medicine. Ending Neglect: The Elimination of
TB in the US. 20006. US Dept of Health and Human Services, CDC, 2003.
Federal TB Task Force Plan in Response to the IOM Report. (pp. 12-14)
7. US Dept of Health and Human Services, CDC, 2002. CDC’s Response to Ending Neglect.. (pp 30-33)