Embed Size (px)
Citation preview

Clinical Science and Molecular Medicine (1974) 47, 317-330.
QUANTITATIVE RADIOISOTOPE RENOGRAPHY : THE DERIVATION OF PHYSIOLOGICAL DATA BY
DECONVOLUTION ANALYSIS USING A SINGLE-INJECTION TECHNIQUE
J . REEVE AND J . C . W . CRAWLEY
Radioisotopes Division, Clinical Research Centre, Harrow, Middlesex
(Received 7 April 1974)
SUMMARY
1. An improved method is presented for quantifying all the information relating to individual kidney function that is contained in the renogram.
2. From the convolution theorem, functions are derived which are equivalent to the renograms that would be obtained by simultaneous injections of the indicator into each renal artery, fractionated according to renal blood flow.
3. The ‘pulse-input’ renograms so derived can have the blood background sub- tracted by a process of ‘kinetic discrimination’, which dispenses with the prior in- jection of human serum albumin.
4. The ‘pulse-input’ renograms with blood background subtracted are analysed by the techniques used in conventional indicator dilution methods.
5. The value of this approach in clinical and experimental work is illustrated by comparison of examples drawn from 400 consecutive studies of patients with normal data.
Key words : renography, Hippuran, deconvolution.
Since its introduction by Taplin, Meredith, Kade & Winter (1956), renography has become widely practised as a simple test of renal function. The development of the human serum 1311-labelled albumin blood background-subtraction technique by Hall & Monks (1 966) and empirical methods for the estimation of overall effective renal plasma flow (ERPF) (Blaufox & Merrill, 1966; Ram, Evans & Chisholm, 1967) have made it possible to estimate ERPF to individual kidneys from the renogram. In addition, the three-probe renogram contains quantitative information sufbcient to define two other characteristics of the observed kidneys. The first is a spectrum of transit times (or transfer function) for Hippuran from renal artery to ureter, and the second is an estimate of the fraction of Hippuran entering with the initial circulation that is retained within the kidney at any time up to the end of the test. The renogram contains no other information that is directly related to renal function.
Middlesex HA1 3UJ. Correspondence: Dr J. Reeve, Radioisotopes Division, Clinical Research Centre, Watford Road, Harrow,
317

318 J. Reeve and J. C. W. Crawley By analogy with conventional indicator dilution techniques, a pulse injection of l 3 lI-labelled
Hippuran into each renal artery combined with either outflow or residue detection of the tracer as it passes through the kidneys would provide mathematical functions showing the distribution of transit times through each kidney (Zierler, 1965). Studies of this type in dogs have been published by Chinard (1 956), who used p-aminohippuric acid (PAH) (a physiological analogue of Hippuran) and by Farmelant, Bakos & Burrows (1969), who used '311-labelled Hippuran. A single study on man using PAH has been published by Schoutens & Raynaud (1968). Coe & Burke (1965) and Van Stekelenburg, Al, Truijens, Van Vals & Kooman (1966) presented techniques for estimating a mean transit time of Hippuran through the kidney from the renogram as distinct from the distribution of transit times. Colin, Mercenier, Lenaers, Kornitzer & Cleempoel(l965) derived spectra of transit times from renograms recorded from exteriorized dog kidneys with a deconvolution technique, which, however, constrained the calculated transit time spectrum to a monomodal positively skewed distribution. Meldolesi, Roncari, Fidanza & Conte (1969) derived similar curves from their analyses of renograms with blood background subtracted obtained in man. The deconvolution techniques employed by Brown & Britton (1970) and Floyrac, Itti, Planiol & Pourcelot (1972) avoid fitting the transit time spectrum to a preconceived model, and are therefore more generally applicable. Others have built compartmental models in an attempt to quantify the renogram (Turco, Ghemi, Cavalli & Segre, 1969; Martin & Monot, 1969).
General acceptance of any of these approaches in clinical or experimental work has been retarded by the number of assumptions inherent in the various analyses and doubts as to the precision with which calculated parameters can be estimated. We describe here a develop- ment of the stochastic approach, which involves fewer assumptions than compartmental modelling and also provides a calculated renogram with blood background subtraction without the use of human serum '311-labelled albumin. Illustrations from among the 400 patients studied so far by this method are used to define both the potential and the limitations of quantitative renography as a clinical and experimental tool.
MATERIALS A N D M E T H O D S All studies were performed on patients referred to a routine hospital renography service, together with eight informed normal volunteers. Kidney location was by a plain radiograph of the abdomen. Patients were prepared and data collected by the use of 5 cm crystals, as recom- mended by Britton & Brown (1971), with the exception that in the majority of cases the 'blood curve' was recorded from the head with a 7.5 cm crystal. Data were recorded both in analogue form and, in most cases, in digital form by using a Didac multiscaler (Intertechnique Ltd), radioactivity counts being summed at 20 s intervals and recorded on magnetic or paper tape for subsequent analysis in an ICL 1903A computer. A dose of approximately 0.5 pCi/kg body weight of '311-labelled Hippuran was used, preceded in some cases by a 0-1 pCi/kg dose of human serum '311-labelled albumin. In most cases, overall ERPF was measured by the tech- nique of Ram el al. (1967).
THEORY AND C O M P U T A T I O N S A standard renogram is a time-dependent, composite function of three other functions: a probability density function describing the retention of Hippuran within the kidney after

Deconvolution analysis of the renogram 3 19 proximal tubular uptake at zero time; a function describing the blood input of Hippuran to the kidney and surrounding tissues; a function representing the transit of Hippuran through non-renal tissues, usually referred to as ‘blood background‘. It is necessary to separate these functions if quantification of the information concerning renal function is to be successful.
As the kidney is composed of several million discrete nephrons, a renogram necessarily described the behaviour of a population of similar, but not identical, units. Hence a stochastic approach to the transit of Hippuran from blood to bladder is most appropriate.
Direct observation of the spectrum of transit times from blood to ureter would require that a pulse injection of Hippuran be made into the renal artery, combined with ureteric outflow detection. However, indirect measurement of the spectrum presents no theoretical difficulty in this context. If a physiological study is conducted in the steady state (and the principle of linear superposition thereby made acceptable), the response of an organ or network to a pulse injection may be derived if the response to any other known input can be observed. Under such conditions the observed renogram with blood background subtracted, Q(t), is the convoluted integral of the ‘pulse-input’ renogram, H(t), and the blood curve, Z(t) (Stephenson, 1948; Zierler, 1965). The pulse-input renogram is obtained from the two observed functions by deconvoluting function I(t) from function Q(t), a procedure which is now finding widespread application in the life sciences (Veall, 1971; Simon, 1972). The spectrum of intrarenal transit times h(t) is the negative differential of the pulse-input renogram H(t) (Zierler, 1965). The third function, ‘blood background’, was initially separated by Britton & Brown’s (1971) modification of the technique of Hall & Monks (1966). It was found, however, that if the deconvolution procedure is applied to the standard renogram, it is possible to obtain the renogram with blood background subtracted without the prior injection of labelled human serum albumin.
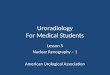
The deconvoluted function thus derived corresponds to the overall retention curve that would be observed if a pulse injection of Hippuran were delivered in proportion to apparent blood flow to all the tissues in the field of view of the renal detector. In every case this composite function, H,(t)+H,(t), which is determined jointly by both venous and urinary outflow of Hippuran, shows a sharp initial fall. This is assumed to represent the vascular outflow function H&) over the first minute of the test, since there is a minimum delay of at least 75 s associated with the passage of Hippuran or of PAH through tubular cell and nephron (Chinard, 1956; Wedeen, 1969; Schoutens & Raynaud, 1968). Differentiation of the complete function after inversion yields the overall spectrum of transit times h,(t) +h,(t), and an example from a study on a normal subject is shown in Fig. 1. The two distinct populations of transit times are clearly evident, there being a fast initial outflow phase followed by a second slower phase, with a mean transit time (0 in normal subjects ranging between 2 and 4 min (Fig. 1). This is assumed to represent the urinary exit of tracer, h,(t). Therefore it is possible to separate h,(t) from h,(t) by a process of kinetic discrimination.
The simplest approach to extracting the urinary component would be to subtract the initial vascular component h,(t) from the spectrum of transit times h,(t) +h,(t), and then (working backwards) to integrate the remaining functions h,(t) to derive a pulse-input renogram with blood background subtraction H,(t). Convolution of H,(t) with the blood curve I(t) then yields the blood background subtraction (BBS) renogram. The integration requires the addition of a constant, which is taken as the value of the final point on the pulse-input renogram H,(t)+ H”(t).
C

320 J. Reeve and J. C. W. Crawley
Time (min)
FIG. 1. Overall spectrum of transit times for Hippuran [hv(t)+h.(t)] through renal and non-renal tissues in the view of a detector, as calculated for a normal subject (data points). See text for explanation of the method used to resolve the functioning renal component from the combined spectrum. ____ , h,(t); - - - -, hdt ) .
However, the renogram also contains information related to blood inflow, of potential importance in clinical situations such as suspected renal artery stenosis and proliferative glomerulonephritis. The following elaboration of the subtraction procedure was adopted in an attempt to extract this information. It was observed that the vascular phase of the spectrum of transit times h,(t) can reasonably be fitted by a single exponential. A least squares fit is there- fore performed on the logarithms of those points obtained from the initial downslope of the combined spectrum of transit times curve h,(t) + h,(t), and the resulting exponential subtracted from the original curve over the vascular phase period up to a maximum of 100 s. In the case of delayed inflow it can be expected that the subtracted curve on the affected side will commence with an extended negative phase representing delay to arterial input (inflow and outflow to the kidney being represented by negative and positive respectively in the transit time spectrum derived by this method).

Deconvolution analysis of the renogram 321
Many methods have been used to deconvolute one function from another. Where the input function [blood curve, I(t)] is a continuously falling curve, the use of the algorithm (described empirically by Scholer & Code, 1954) in eqn. (1) has proved satisfactory and economical of computer time,
k = 2
where n is the number of observational points.
To obtain the spectrum of transit times h(t), the function H(t) was differentiated simply by recording the difference between successive points (eqn. 2).
h(i++)=Hi-H(i+I) (2)
As the two procedures of deconvolution and differentiation have a magnifying effect on the ‘noise’ inherent in the raw data, both the blood curve and renograms were subjected to a smoothing process on the recorded points obtained from the second minute onwards before further analysis, according to the formula in eqn. (3).
(A=QorI>
This is mathematically equivalent to two degrees of smoothing by the simple technique of replacing each point by the average value of itself and its two neighbours. However, if the resulting smoothed value exceeded two standard deviations from the original value, the latter was allowed to stand. The transit time spectra were also smoothed by this technique.
Having derived the pulse-input renograms, the percentage share of ERPF was estimated by comparing the relative amplitudes of the functions H,,(t) over the first minute (H, Zeft and H, right). This is mathematically equivalent to Britton & Brown’s (1968) relative slope method. Mean transit time (0 for each kidney was estimated as the area under the curve (from zero time until the function reached zero amplitude) divided by its initial amplitude (Zierler, 1965), as in eqn. (4),
€,(min) = CHJ(H,n) (4) where n = 3, the number of points recorded per minute.
taken as being from the first positive point until the curve again became negative (eqn. 5). As a check on the fitst calculation, € was also estimated from the distribution of transit times,
Additionally, the second and third moments were calculated, and from thein the variance of the distribution, the relative standard deviation (RSD) about € and the degree of skewness of the distribution (Kendall & Stuart, 1963). Relative uptake by each kidney was also checked by

322 J. Reeve and J. C. W. Crawley measuring the ratio of the areas under each transit time curve, each area corresponding to the difference between the maximum and minimum of their respective pulse-input renograms.
The parameters derived from this distribution curve are still sensitive to residual ‘noise’ in the data, so were only deemed acceptable if they fell within f 5% of the same values derived from the smoothed and doubly smoothed versions of the same curve. The first negative and subsequent values were ignored because their inclusion would lead to spurious values in the calculation of second and third moments, and, secondly, oscillations about zero are to be expected as a result of statistical ‘noise’.
To investigate the effects of random variations in radioactivity count rate on the calculated parameters, the data from a study on a normal individual were subjected to a randomization procedure to produce twenty-one sets of data. Each data point was modified according to the formcla in eqn. (6),
A’, =Ai + Fi JA, (6) where Fi was a pseudo random number calculated so that a large number of F values had a Gaussian distribution with a mean of zero and SD i 1.0. These twenty-one simulated renograms were then analysed as described above.
(The authors will supply a copy of the computer program used in these studies to interested workers.)
RESULTS
The results of the investigation into the effects of random variation in radioactivity count rate on the calculated parameters are summarized in Table 1. Similar analyses of renograms from individuals with reduced ERPF values or increasing transit time spectra with increased spread would clearly indicate less precision in the estimated values of the parameters of interest.
When these studies were commenced, the blood disappearance curve was estimated by pre- cordial radioactivity counting. This was abandoned in favour of head radioactivity counting because deconvolution sometimes resulted in the appearance of a long tail on the pulse-input functions derived from normal renograms. On the other hand, the flatter head curve usually results in the terminal portion of the pulse-input retention curve being slightly negative, so that a positive tail on this curve is much more likely to signify some delay to outflow.
Three patients were studied who had had unilateral nephrectomies previously. In no case was the apparent share of overall ERPF taken by the non-existent kidney greater than 5%.
In twelve studies on hypertensive patients a comparison was made between the parameters derived from analysis of the renogram by the ‘kinetic discrimination’ method with those derived from the same renogram, using an otherwise identical computer program with blood background subtracted by the method of Britton & Brown (1968). This group of patients was drawn from a larger group of thirty-three hypertensive individuals with no evidence of uni- lateral renal disease. In the group as a whole these parameters had approximately normal distri- butions. There was excellent correlation between the two methods in the calculation of per- centage ERPF to the left kidney (correlation coefficient 0.97, n = 12) and the BBS renograms were closely comparable after the first minute. Mean estimate of i for the group of twenty-four kidneys was 10 s longer by the ‘kinetic discrimination’ method, the correlation coefficient for the paired estimates being 0.86. These means were compared by the method of paired compari-

Deconvolution analysis of the renogram TABLE 1. Effect of statistical variations in observed radioactivity count rate
upon parameters calculated from a normal renogram (a) Observed and calculated radioactivity count rates at peak time.
323
Radioactivity (counts/20 s) at 2.7 min
Head 750 Left kidney (total) 9100
Left kidney (-blood background) 8240 Right kidney (- blood background) 4840
Right kidney (total) 5500
(b) Coefficients of variation in parameters calculated from this renogram. Mean values are shown in parentheses.
Parameter
Coefficient of variation (%)
Left Right
ERPF (%) 6 8 (55.9) -
RSD about t‘ (%) 7.7 (27.4) 4.3 (34.9) i (min) 3.1 (3.82) 1.7 (3.05)
Skewness (meanf 1 SD) -0.37 k 0.10 - 0.06 k 0.09
sons (Bailey, 1959) and the difference between them found to be significant (0.02 > P> 0.01). The mean of the estimates of RSD about din this group of patients was 37% for the human serum 1311-labelled albumin method compared with 32% for the ‘kinetic discrimination’ method. The difference between the means was more significant (0.005 >P> 0.001) and the correlation coefficient for the paired estimates was 0.8 1.
The normal volunteers were studied under the same conditions as those applying to the patients. The results of these studies are summarized in Table 2. Noteworthy is the considerable variation in mean transit time between subjects, contrasting with the near identity of the transit times calculated for a normal individual’s left and right kidneys in the same study.
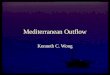
The shape of the blood curve can play a critical role in determining the shape of the renogram. This is illustrated by the following study (Fig. 2). Calculated BBS renograms have been derived from the following combinations : a normal blood curve and one from a patient with reduced ERPF (140 ml/min), each convoluted with a normal pulse-input renogram and one from a patient with severe hypertension. It will be seen that where f is prolonged and the RSD about f increased, the appearance of the renogram can depend very substantially on the steepness of the downward slope of the blood curve, which in turn is partially dependent on the value of the ERPF.
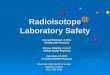
A clinical illustration of the value of deconvolution in the analysis of the continuously rising renogram is illustrated in Fig. 3. A clear-cut case of unilateral obstruction is here contrasted with that of a patient presenting with oliguria (250 ml/day) and two continuously rising renograms, where the diagnosis lay between acute tubular necrosis and bilateral obstruction.

324 J. Reeve and J. C. W. Crawley
TABLE 2. Summarized results from normal subjects
Difference Difference between L between and R RSD L and R RSD about about mean
Transit time transit times mean transit transit times (min) (min) time (%) PA)
Mean 2.86") - 25") - Range 1-65467 0-0.55 16-38 0-1 1 (twice SD)
4r
Log normal distribution assumed for a group of normal individuals. ( I ) Normal distribution assumed.
0 1 2 3 4 5 6 7 8 9 1 0 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 2 3 4 5 6 7 8 9 1 0 1 1 1 2
T i m e h i d
FIG. 2. BI=Blood curve from a normal subject; B2=blood curve from a hypertensive subject with ERPF 140 dimin. (a) Renograms R I and R2 are calculated by convoluting the pulse-input renogram H(t)from the same normal subject with blood curves B1 and B2. (b) Renograms R1 and R2 are calculated by performing the same operations on the pulseinput renogram from the hypertensive subject. Redrawn from a flat-bed graph plot in which data points (3/min) are con- nected by a continuous line. Renograms are smoothed as described in the text.

Deconvolution analysis of the renogram 325
( 0 )
.$ 20 Patient F.W. t , X
n
‘0 R. K. L.K.
Y
10 20 30 40 T i m ( min)
Patient D.W.
H ( t ) L . K .
Patient F.W. \
Time (min)
Fm. 3. (a) Blood background-subtractedrenograms and blood curve (F3) from a patient (D.W.) with left urinary tract obstruction and one (F.W.) with acute tubular necrosis. (b) Pulse-input renograms calculated by deconvolution. L.K. =left kidney; R.K. = right kidney.
The problem was resolved in favour of the former diagnosis by the demonstration of slow but definite excretion of tracer that for a calculated pulse input was more than 90% complete at 40 min.
An investigation was carried out into what factors other than the shape of the blood curve determined the appearance time of the renogram peak, a parameter of considerable value in traditional methods of analysis. The results from thirty-three studies in hypertensive patients without evidence of unilateral renal disease by the human serum 1311-labelled albumin sub- traction method were subjected to regression analysis. Peak time (PT) regressed significantly on both i and on the RSD about f, but was clearly much more closely related to the product of the two, namely the standard deviation (SD) about the mean transit time, which obeyed an approximately normal distribution. The linear regression equation relating PT to SD was PT = b.sD-k (b = 3-1 &O-18, k = 0.5f0.8, P<O-OOl; figures are expressed as meansftwo standard deviations).
These findings indicate that time to peak is determined principally by the interaction of three

326 J. Reeve and J. C. W. Crawley factors: the mean transit time, the degree of homogeneity of the spectrum of transit times and the slope of the blood curve.
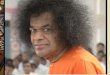
Apart from the discovery of a just significant negative regression of ERPF on diastolic blood pressure, statistical analysis of a further thirty-three renograms in hypertensive patients with symmetrical renograms failed to demonstrate close relationships between other para- meters of the renogram and diastolic blood pressure. Nevertheless, by inspection a group of hypertensive patients with symmetrical renograms differed from the majority (whose pulse- input renograms were indistinguishable from normal) by the tardiness with which the h a 1 20% or so of the drop to zero was completed (Fig. 4). The pronounced effect of ‘noise’ in this
I I I I I I 1 I I I I I 3 6 9 12 15 3 6 9 12 15
Time ( m i d
FIG. 4. Right: pulse-input renogram and spectrum of transit times for a hypertensive patient whose renograms were normal. Left: representative results from a group of hypertensive patients with symmetrically abnormal renograms.
group made the estimation of iand RSD difficult. However, after subjecting the tail of the pulse- input retention curves to further smoothing, it became clear that in this group as a whole RSD was increased above normal and there was a tendency toward a longer i and positive skewness.
In cases of unilateral renal disease the close relationship between the two i values and RSD values about the mean are no longer seen. An analysis of a proven case of renal artery stenosis published by Britton & Brown (1968) is shown in Fig. 5. Noteworthy is the increase of 1-43 min in f on the side with stenosis, and the 29% increase in the RSD about i. These findings are comparable with those of Farmelant et al. (1969) in dogs with clamped renal arteries. No delay to inflow was demonstrated on the affected side in this case.

Deconvolution analysis of the renogram 327
(a1
2 4 6 8 1 0 1 2 2 4 6 8 1 0 1 2 Time ( m i d Time (min)
4 6 8 10 12 Time (min)
FIG. 5. (a) Blood background-subtracted renograms ; (b) pulse-input renograms ; (c) spectra of transit times derived from results on a patient with left renal artery stenosis, published by Britton & Brown (1968). Peak radioactivity count rate calculated for right BBS renogram = 8000 counts/20 s.
DISCUSSION The concept of the renogram with blood background subtracted as the convoluted integral of the blood-input function and a theoretical ‘pulse-input’ renogram employed here is mathe- matically closely related to the theories underlying the analytical methods of Meldolesi et al. (1969), Brown & Britton (1970) and Floyrac et al. (1972). All four approaches lead to the formulation of a Volterra integral equation relating three functions, two of which are directly observed or easily derived, making the third obtainable by deconvolution.
With the approach presented in this paper, two significant advances are introduced. First, a pulse-input renogram is provided, which represents the negative integral of the spectrum of transit times. Because every integration procedure introduces a constant of integration, simple integration of the transit time spectrum yields no information about the physical analogue of this constant, namely Hippuran which remains within the field of view until the end of the study. By deconvoluting the blood curve from the renogram itself rather than from the calculated curve of unilateral Hippuran outflow rate, a pulse-input renogram is obtained which provides visually distinctive and easily quantified indication in cases where obstruction or prolonged hold-up is a possibility (Fig. 3).
The second advance lies in dispensing with the preliminary injection of human serum 13’1- labelled albumin for the purpose of deriving a ‘blood background’ subtraction renogram. This has two important consequences. First, radiation dosage is very much reduced, a point of particular importance for studies in children. A 40pCi dose of 1311-labelled Hippuran would be expected to give a radiation dose to the whole body of less than 12 mrem (Henk, Cottrall & Taylor, 1967), which could be further reduced by prior removal of free iodide from the Hippuran, or prior blocking of the thyroid. To this dosage a further 10 pCi of 13’I-labelled albumin would add 35 mrem (Hall & Monks, 1966). Secondly, advantages are offered where frequent serial studies are required. With the human serum 311-labelled albumin technique the investigator has two choices : either to give repeated injections of 1311-labelled albumin and

328 J. Reeve and J. C. W. Crawley
accept an ever-increasing background count, or to accept the inaccuracies due to using a single initial dose of 13’I-labelled albumin consequent upon its slow redistribution in the extracellular fluid between studies.
To est,ablish any deconvolution technique as providing reliable quantitative information concerning renal function, the common assumptions inherent in its theoretical foundations must be shown to be valid. These assumptions are as follows. First, it is assumed that the externally recorded ‘blood pool’ curve is representative of the blood concentration of Hippuran. Secondly, in common with all quantitative approaches in renography, it is assumed that blood flow to the kidney and the extraction ratio of Hippuran are constant throughout the test. Thirdly, it is assumed that over the first 13 min at least no Hippuran leaves the kidney via the ureters. Finally, it is assumed that the technique used for subtracting the non-renal contribution of counts recorded is valid. If all these assumptions are made acceptable, then the confidence that can be placed in the results depends solely on the degree of precision of the measurements of kidney activity and the accuracy of the deconvolution method employed (the convolution theorem itself has been formally proven : Volterra, 1959). Strictly speaking, the first assumption can never be entirely true. In practice, counts recorded from the left subclavicular region or from the head will include some from extravascular Hippuran. This will have the effect of making the observed curve fall less steeply than it should. The result is that when normal renograms are deconvoluted, the derived pulse-input renograms regularly show a negative ‘overshoot’ (Fig. 4b), resulting in an underestimate of mean transit time. However, the effect on the spectrum of transit times is less marked. This apparent disadvantage does carry with it a useful feature in that spurious diagnoses of obstruction or prolonged hold-up are there- by made unlikely (Fig. 3b).
The third assumption is supported by two lines of evidence. First, by the autoradiographic evidence of Wedeen (1969) and more directly by the dog studies of Chinard (1956) and the thirty or more studies in man of Schoutens & Raynaud (1968), who found that after injection of PAH and inulin, PAH never appeared at the ureter more than a few seconds before inulin. This does not necessarily imply that the pulse-input renogram will have a horizontal first portion, as the intrarenal transport may affect the observed count rate.
The technique of deconvolution used in these studies involves no ‘fitting’ of observed data to theoretical curves, as is necessary, for example, in methods employing Laplace transforms. However, like all other methods, it does have disadvantages, which have been investigated in a theoretical paper by Hart & Sondheimer (1970). Essentially, if ‘noise’-free data are available, accuracy is improved by increasing the number of elements in each data array (i.e. summing radioactivity counts for shorter intervals). However, ‘noise’ superimposed on the data has the opposite effect. Therefore in these studies the summing time of 20 s represents a compromise. Hart & Sondheimer (1970) showed that the main inaccuracies are likely to occur in the first four or five values of the deconvoluted renogram, a period when practically none of the Hippuran has IeR the kidneys. Nevertheless, it is clearly desirable to aim for the optimum compromise between low radiation dose to the patient and high radioactivity count rate from the detecting system. In some clinical situations therefore it may prove justified to increase the dose of Hippuran fourfold in order to reduce the summing time to half. This would not only enable a more accurate deconvolution, but considerably improve the confidence that could be placed in the accuracy of the blood background subtraction.
In this context it should be noted that estimates of relative renal blood flow are necessarily crude unless the effects of variation in kidney depth are considered (Tauxe & Burke, 1968).

Deconvolution analysis of the renogram 329 If the error of some +20% due to this cause is to be reduced, it is necessary either to set the detectors well back (compensating for lost counts with an increased dose of Hippuran) or to use a double-isotope technique such as that of Dolan & Tauxe (1968) in order to apply an empirical correction.
The differences between the analyses of the twelve renograms in which blood background was subtracted by two different methods requires comment. Inspection of the transit-time spectra derived from deconvolution of human serum 1311-labelled albumin BBS renograms sometimes revealed an early peak at 20 s. This represents apparently incomplete blood back- ground subtraction, and would have the effect of shortening f and increasing RSD about f. This is thought to be the explanation of the small discrepancies observed.
Because data collection has been automated and digital computing facilities are readily available, it has been possible to study 400 unselected patients, the last 250 with the single- injection technique. The ease and safety of the procedure make it an ideal tool for sequential studies, and a group of hypertensive patients with bilaterally abnormal renograms are currently being followed closely to observe the measurable effects of treatment on the homogeneity of nephron performance.
Comparison of the analysis presented here with others is clearly of importance in establishing the general validity of this approach. A series of paired studies on the same data is in progress to assess the degree of agreement between the results of analyses by this method and that of Brown k Britton (1972).
In conclusion, the techniques presented here provide quantification of all the information contained in the renogram. In addition, BBS renograms are calculated to aid in the traditional methods of renogram interpretation. Given access to off-line computer facilities, the require- ment for only relatively simple equipment and a single injection are practical advantages, and the multiscaler may be dispensed with if points are noted from a graphical output, at some cost in time and convenience. The straightforward derivation of information concerning flow rate of glomerular filtrate from proximal tubule to ureter offers numerous possibilities for further physiological studies.
ACKNOWLEDGMENTS
The authors acknowledge the skilled technical assistance of Miss D. Worth, Mr M. Bond and Mr D. Hinge, and the helpful co-operation of the technical staff of the Division of Computing and Statistics. They particularly thank Mr P. Vitek for his programming work on the magnetic tape interface, without which only a fraction of this work would have been possible. They also thank Dr N. Veal1 for considerable encouragement, the medical staff who kindly referred their patients, and Dr C. K. McPherson and Miss S. Chinn for statistical advice. J.R. is an MRC Clinical Research Fellow.
REFERENCES BAILEY, N.T.J. (1959) Statistical Methods in Biology. English Universities Press Ltd, London. BLAUFOX, M.D. & MERRILL, J.P. (1966) Simplified hippuran clearance. Measurement of renal function in man
BRITTON, K.E. & BROWN, N.J.G. (1968) A Practical Approach to Rudioisotope Renography, Medical Monograph
BRITTON, K.E. & BROWN, N.J.G. (1971) Clinical Renography. Lloyd-Luke, London. BROWN, N.J.G. & BFUTTON, K.E. (1970) Distribution of intrarenal transit times in man. JournaZ of Nuclear
with simplified hippuran clearance. Nephron, 3,274-281.
no. 1, Nuclear Enterprises Ltd, Edinburgh.
Medicine, 11,305.

330 J. Reeve and J. C. W. Crawley BROWN, N.J.G. & BRITTON, K.E. (1972) The theory of renography and analysis of results. In: Radionuclides in
Nephrology, pp. 315-324. Ed. Blaufox, M. & Funck-Brentano, J.-L. Grune & Stratton, New York. CHINARD, F.P. (1956) Relative renal excretion patterns of p-aminohippurate (PAH) and glomerular substances.
American Journal of Physiology, 185,413417. COE, F.L. & BURKE, G. (1965) Renal transit time; its measurement by the 13'1 hippuran renogram. Journal of
Nuclear Medicine, 6 , 269-274. COLIN, F., MERCENIER, P., LENAERS, A., KORMTZER, M. & CLEEMPOEL, H. (1965) etude expkrimentale du
rhogramme. Archiv f i r Kreislauforschmg, 46,289-306. DOLAN, C.T. & TAUXE, W.N. (1968) Estimation of organ depth by a double isotope technique. American Journal
of Clinical Pathology, 50, 83-88. FARMELANT, M.H., BAKOS, K. & BURROWS, B.A. (1969) Physiological determinants of renal tubular passage
times. Journal of Nuclear Medicine, 10, 641-645. FLOYRAC, R., I ~ I , R., PLANIOL, TH. & POURCELOT, L. (1972) Le nCphrogramme et la distribution des temps de
transit. Annales de Physique Biologique et Mkdicale, 6, 1-6. HALL, F.M. & MONKS, G.K. (1966) The renogram: A method of separating vascular and renal components.
Investigative Radiology, 1,220-224. HART, H.E. & SONDHEIMER, J.H. (1970) Discrete formulation and error minimisation in applying the integro-
differential equation approach to mono-compartment data. Computers in Biology and Medicine, 1, 59-74. HENK, J.M., COTTRALL, M.F. & TAYLOR, D.M. (1967) Radiation dosimetry of the 13'I-Hippuran renogram.
British Journal of Radiology, 40,327-334. KENDALL, M.G. & STUART, A. (1963) The Aduanced Theory of Statistics, vol. 1, Distribution Theory. C. Griffin
& Co., London. MARTIN, J. & MONOT, C. (1969) Analysis of a mathematical model of renal function. In: Radioisotopes in the
Diagnosis of Diseases of the Kidneys and Urinary Tract, pp. 508-520. Ed. Timmermans, L. & Merchie, G. Excerpta Medica Foundation, Amsterdam.
MELDOLESI, U., RONCARI, G., FIDANZA, M.A. & CONTE, L. (1969) First attempts of clinical application of a method for the quantitative interpretation of renograms with radio-hippuran. Journal of Nuclear Biology and Medicine, 13,94102.
RAM, M.D., EVANS, K. & CHISHOLM, G.D. (1967) A simple injection method for measurement of effective renal plasma flow. British Journal of Urology, 39,425428.
SCHOLER, J.F. &CODE, C.F. (1954) Rate of absorption of water from stomach and small bowel of human beings. Gastroenterology, 27, 565-577.
SCHOUTENS, A. & RAYNAUD, C. (1968) ktude de la permkabilite du nkphron de l'homme aux tlectrolytes. Nephron, 5 , 217-241.
SIMON, W. (1972) Mathematical Techniques for Physiology and Medicine. Academic Press, New York. STEPHENSON, J.L. (1948) Theory of the measurement of blood flow by the dilution of an indicator. Bulletin of
TAPLIN, G.V., MEREDITH, O.M., KADE, H. & WINTER, C.C. (1956) The radioisotope renogram. Journal of
TAUXE, W.N. & BURKE, E.C. (1968) Kidney depth and isotope renography. Journal of Nuclear Medicine, 9,
TURCO, G.L., GHEMI, F., CAVALLI, P.L. & SEGRE, G. (1969) Quantitation of renography with digital computing techniques in normal subjects, and in cases of hypertension and renal ptosis. In: Radioisotopes in the Diagnosis of Diseases of the Kidneys and Urinary Tracf, pp. 528-533. Ed. Timmermans, L. & Merchie, G. Excerpta Medica Foundation, Amsterdam.
VAN STEKELENBURG, L.H.M., AL, N., TRUIJENS, J.H.J., VAN VALS, G.H. & KOOMAN, A. (1966) A quantitative theory of radioisotope renography with h i p p ~ r a n - ~ ~ ~ I . Physics in Medicine and Biology, 11,451460.
VBALL, N. (1971) Theoretical aspects of dynamic clinical studies with radioisotopes. In: Dynamic Studies with Radioisotopes in Medicine, pp. 3-12. International Atomic Energy Agency, Vienna.
VOLTERRA, V. (1959) Theory of Functionals and of Integral and Zntegro-differential Equations. Dover, New York. WEDEEN, R.P. (1969) Autoradiography of hippuran lz5I in rat kidney: the intrarenal basis of the radioisotope
renogram. In: Radioisotope in the Diagnosis of Diseases of the Kidneys and Urinary Tract, pp. 461-466. Ed. Timermans, L. & Merchie, G. Exerpta Medica Foundation, Amsterdam.
ZIERLER, K.L. (1965) Equations for measuring blood flow by external monitoring of radioisotopes. Circulation Research, 16, 309-321.
Mathematical Biophysics, 10, 117-121.
Laboratory and Clinical Medicine, 48,886901.
225-226.