Embed Size (px)
Citation preview

Quand faut-il implanter un PM après un TAVI?
Nicolas Lellouche MD, PhDCardiology Unit
Hôpital Henri MondorCréteil, France
1

•Trans Aortic Valve Implantation (TAVI) is a new technology with increasing indication to treat symptomatic severe aortic stenosis
•However numerous complicationsare associated with this procedure
INTRODUCTION

0,0%
5,0%
10,0%
15,0%
20,0%
25,0%
30,0%
New Pacemaker
New pace-maker (Corevalve+Edwards)
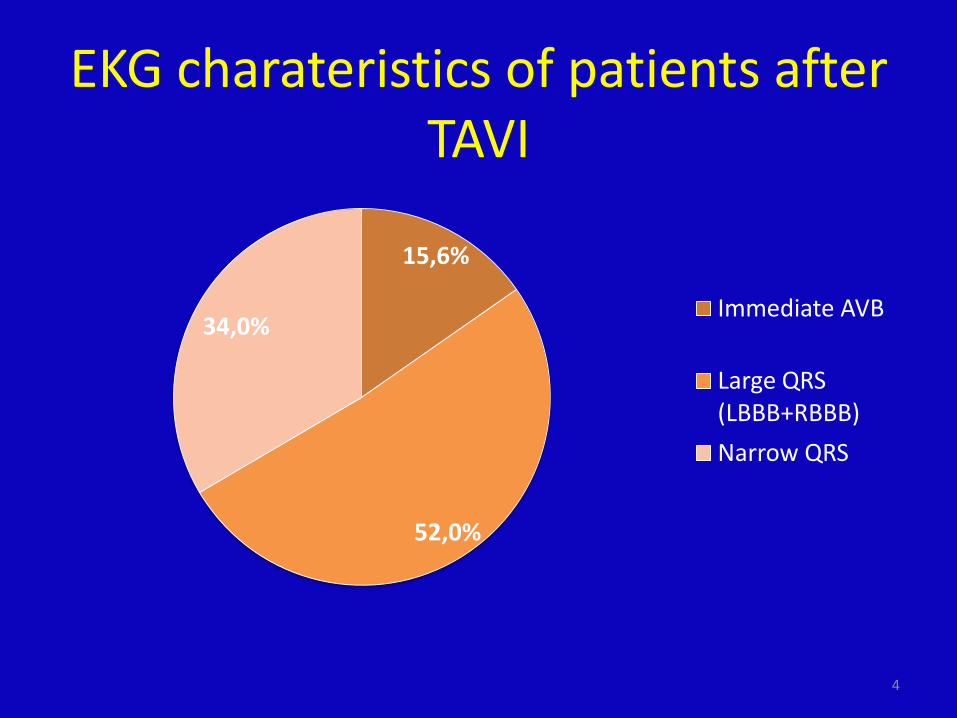
EKG charateristics of patients after TAVI
4
15,6%
52,0%
34,0%Immediate AVB
Large QRS (LBBB+RBBB)Narrow QRS

-Facteurs pronostics de survenue de BAV de haut degré
-Critères d’implantation en post TAVI: pas de problème pour les classiques: BAV 3 ou 2: problématique de la récupération; Plus discutable pour BBG ± BAV1-Problème du BBG avec risque d’aggravation de la fonction VG= indication de la resynchronisation
PROBLEMATIQUE

Major Predictors for AVB after TAVI
• Pre existing RBBB • Non coronary cusp calcification• Depth of biosprothesis implantation• QRS duration after TAVI (QRSd).
Mouillet et al Catheterization and Cardiovascular Interventions 81:882–887 (2013)
Tchetche et al EuroIntervention 2012;8:556-562
Baan et al
Piazza et al EuroIntervention (2008) ;4:242-249
Latsios et al Catheterization and Cardiovascular Interventions 76:431-439 (2010)
Bleiziffer et al jacc cardiac intervention 2010; 3:524-530

7
Faut-il implanter un PM en préventif chez un patient avec BBdt?
Entre 30-40% de taux d’implantation des BBD

Post TAVI QRS duration best predictor of delayed AVB.
Q R S _ p o s t_ c o re va lve _ J 0
0 2 0 4 0 6 0 8 0 1 0 0
1 0 0
8 0
6 0
4 0
2 0
0
1 0 0 -S p e c if ic ity
Sens
itivity AUC = 0.765
P<0.0001
Safety Cut-off= QRS duration = 128 ms 100 % Se
Mouillet, Lellouche et al Catheterization and Cardiovascular Interventions 81:882–887 (2013)

Patient at risk with QRS ≤ 128 ms after TAVI (n) 24 21 11 4 2 2 2 1 0
Patient at risk with QRS>128 ms after TAVI (n) 55 26 18 4 1 1 1 0 0
Follow up free from AVB after TAVI
QRS≤128 ms
QRS >128 ms
Period Free from AVB after TAVI
0 5 10 15 20 25 30 35 40
100
90
80
70
60
50
40
30
20
10
0
Follow up time (months)
Free
dom
from
PPI
(%)
P = 0,0016
Mouillet, Lellouche et al Catheterization and Cardiovascular Interventions 81:882–887 (2013)

Intérêt de l’EEP en post TAVI

MéthodeCritères d’inclusion: - tout patient eligible au TAVICritères d’exclusion: - pace maker
COREVALVE
EDWARDSSAPIEN
Bilan préopératoire:- ECG rythme, PR, QRS, axe- Scanner cardiaque: calcifications- ETT: valulopathie, taille anneau aortique (min et max)- antécédents
EEP
préT
AVI
EEP
post
TAVI
imm
édia
t
SEESSi 1 FR
sinon: scope 5
jours
EE
P po
stTA
VI
tard
if PM si- BAV II ou IIIà J2 (ES) ou J5 (CV)- HV3 > 80 ms
J0 J5J2J0, J1, J2, J3, J4, J5
ECG M1 M6ECG
CONTRÔLE PMExamen clinique
FR BAV transitoire :- Corevalve- BBD préexistant - BBG de novo- BAV II ou III per implantation- HV2 > 70 ms
HV1 HV2 HV3

CLINICAL CHARACTERISTICSMale 34 (41)Age, years 83 +/-9Coronary artery disease 29 (35)oronary angioplasty 12 (14)CABG 8 (9)Dyspnea class NYHA >II 68 (81)Hypertension 55 (65)Diabetes 19 (23)COPD 6 (7)Creatinine (µmol/l) 107+/- 10Evaluated mortality - Euroscore (%) 15.4 +/-10ELECTROCARDIOGRAM AT BASELINESinus rhythm 76 (90)PR interval (ms) 179 +/- 281st Degree AVB 1 (13)QRS duration (ms) 104 +/- 30RBBB 9 (10)LBBB 12 (14)QRS Axis 6 +/- 43MORPHOLOGICAL FINDINGSAortic annulus
minimal diameter (mm) 22 +/- 3maximal diameter (mm) 27 +/- 3
Aortic valv area (cm²) 0.7 +/- 0.2Mean gradient (mmHg) 49 +/- 15LVEF (%) 55 +/-13TAVR PROCEDURE Prosthesis model, Corevalve® 56 (67)Femoral access 61 (73)Aortic access 9 (11)Subclaviar access 10 (12)Other access 4 (4)POST OPERATIVE CHARACTERISTICSElectrosystolic stimulating 77 (92)PPM implantation 28 (33)PPM implantation for AVB 17 (20)PPM implantation based on EP 9 (11)Death 9 (11)Hospitalisation length (without PPM) 10 +/-6Hospitalisation length (with PPM) 10 +-/6
Table 1: Patient‘s baseline characteristics. N =84 patients
27 PM implantés (34%)

Clinical Parameter Secondary endpointn=13/76
UNIVARIATE ANALYSIS MULTIVARIATE ANALYSISOR [95% CI] p OR [95% CI] p
POPULATION CHARACTERISTICSMale, n (%) 7 (53.8) 2.03 [0.60-6.77] 0.25Age, mean+/-SD 86.4 +/- 4 1.09 [0.98-1.21] 0.09 NSCPI, n (%) 5 (41.6) 1.24 [0.35-4.36] 0.73NYHA >2, n (%) 11 (91.6) 1.45 [0.16-13.03] 0.74HTA, n (%) 9 (75) 1.28 [0.31-5.31] 0.73Diabete, n (%) 3 (25) 1.00 [0.24-4.18] 1BPCO, n (%) 1 (8.3) 0.81 [0.09-7.49] 0.86Créatinine, mean +/- SD 135+/-85 1.00 [0.99-1.01] 0.25ECG AT BASELINERS, n (%) 12 (92.3) 1.26 [0.14-11.47] 0.83BBD, n (%) 6 (46.1) 17.14 [3.49-84.20] <0.001 - NSPR 191 +/-55 1.01 [0.99-1.02] 0.24QRS 115 +/-32 1.01 [0.99-1.03] 0.11 - NSBAV 1, n (%) 2 (15.4) 1.20 [0.22-6.46] 0.82BBG, n (%) 1 (7.7) 0.57 [0.06-5.02] 0.61Axe QRS -8 +/-44 0.99 [0.97-1.01] 0.23 - NSAORTIC VALVE CHARACTERISTICSDiam min 23+/-4 1.08 [0.88-1.33] 0.44Diam max 27 +/-4 1.05 [0.86-1.28] 0.63Euroscore 18 +/- 11 1.04 [0.97-1.10] 0.21SAO 0.66 +/-0.23 0.46 [0.01-28.61] 0.71DP 52 +/-16 1.01 [0.96-1.06] 0.57FEVG 61 +/-11 1.06 [0.98-1.14] 0.09 - NSINTERVENTIONModel Corevalve, n (%) 12 (92.3) 7.89 [0.96-64.56] 0.054 - NSBAV per op 9 (69.2) 8.65 [2.29-32.6] 0.001 NSTransient perop AVB 3 (23.1) 1.80 [0.41-7.83] 0.43Persistant perop AVB 6 (46.1) 12.64 [2.85-55.99] 0.001 NSEVOLUTIONHV1 > 70ms 0HV2 > 70ms 3 (46.8) 0.86 [0.17-4.19] 0.85HV3 > 70ms 1 (33.3) 1.28 [0.10-15.13] 0.84HV2 - HV 1 ms 14 +/-19 1.00 [0.95-1.04] 0.99HV3 – HV1 ms 13 +/-5.5 0.96 [0.88-1.05] 0.40PR J5 235 +/- 88 1.01 [0.99-1.02] 0.13 NSQRS J5 145 +/-10 1.02 [0.99-1.05] 0.07 NSQRS axis -6 +/- 54 0.99 [0.97-1.01] 0.43BBG de novo 7 (53.8) 1.41 [0.42-4.70] 0.57BAV post op et< j5 12 (92.3) 139.2 [14.89-1301.28] <0.001 70.66 [5.91-
844.59]0.001
Table 3Table : Survenue de BAV II ou III dans le suivi(M1 M6): facteurs prédictifs

Figure 1: evolution of HV interval before and after TAVR according to prosthesis type.

15
The value of electrophysiologic study in decision-making regarding the need for pacemaker implantation after TAVI.Tovia-Brodie O1, Ben-Haim Y1, Joffe E2, Finkelstein A1, Glick A1, Rosso R1, Belhassen B1, Michowitz Y3,4.AbstractPURPOSE: The purpose of this study was to evaluate electrophysiologic study (EPS) in risk stratification of relative indications for pacemaker implantation (PMI) after transcatheter aortic valve implantation (TAVI).METHODS: We reviewed files of all patients who had a left bundle branch block (LBBB) and underwent EPS after TAVI between 3/2009 and 5/2015. The indications for EPS were new-onset LBBB and the presence of an old or a new-onset LBBB associated with either PR prolongation after TAVI ( ∆PR >20 ms) or with "slow" atrial fibrillation (<100/min). Pacemakers were implanted when significant infranodal disease was demonstrated. The control group comprised of 55 consecutive patients who underwent TAVI and had an indication for an EPS per our definitions. These patients were discharged without further intervention. All patients were followed during 1 year for the composite endpoint of mortality or PMI after hospital discharge.RESULTS: Indications for EPS were new LBBB (n = 8, 30.8%), new LBBB + ∆PR >20 ms (n = 9, 34.6%), baseline LBBB + ∆PR >20 ms (n = 7, 26.9%) and new LBBB + slow AF <100 bpm (n = 2, 7.7%). Multilevel conduction disturbances involving the AV node (n = 19, 73.1%), the His (n = 3, 11.5%), and the infra-His system (n = 4, 15.4%) were found. Post discharge, there were 5 (9%) deaths and 3 (5.5%) PMI in the control group compared to none in the EPS group corresponding to event-free survival of 85 and 100%, respectively (p = 0.04).CONCLUSIONS: Patients with LBBB with or without ∆PR >20 ms are at a higher risk of mortality and late PMI at 1-year follow-up. EPS can be used to safely identify patients in whom a PMI is needed.

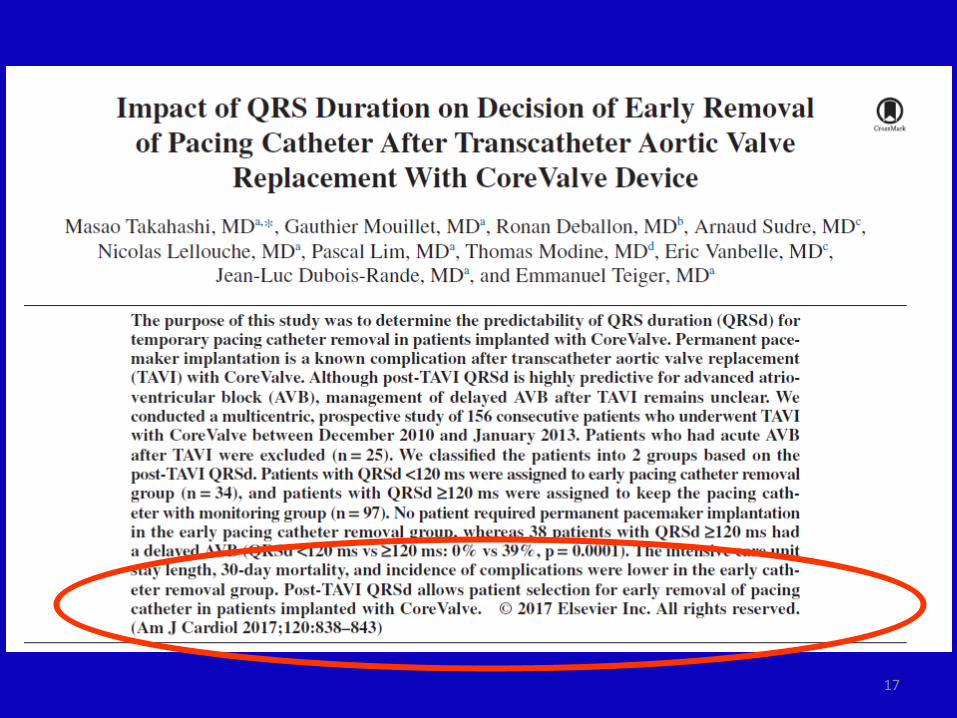
QRSd <120 ms QRSd ≥120 ms Complete AVB
EKG recording
• high degree conduction trouble
• Early PM implantation
• Low risk for AVB • pacing catheter was
removed. • Carefull Follow-up under
monitoring was performed during 48 hours or more if necessary.
• Unknown risk for AVB • Kept on demand pacing
catheter• Carefull Follow-up under
monitoring was performed during 48 hours or more if necessary.
PROPOSITION DE CAT APRES TAVI
17

18
Délai d’implantation
-Stabilisation des troubles conductifs à J5 mais ce délai est associé à des risques de complication liés à l’hospitalisation
-Donc Privilégier stratégie d’implantation précoce+++Pour les troubles conductifs de haut degré

19
Intérêt du pace sans sonde pour implantation dans la foulée du TAVI?

Récupération des troubles conductifs

– Evaluation du pourcentage de stimulation ?• Mode de stimulation, modèle de stimulateur• BAVc paroxystique ?
21
Boerlage-Van Dijk, PACE 2014121 patients, 23 implantés d’un PM 22% considérés comme ayant une conduction A-V normale à 1 anMais conduction « normale » si pourcentage de stimulation < 20%
Patient porteur de PM ou évolution des troubles conductifs sans PM (BAV1±BBG)

Reevaluation of the indications for permanent pacemaker implantation after transcatheter aortic valve implantation.Bjerre Thygesen J1, Loh PH, Cholteesupachai J, Franzen O, Søndergaard L.Author information1Department of Cardiology, Rigshospitalet, University Hospital of Copenhagen, Denmark. [email protected].
Abstract
AIMS: Conduction abnormalities (CA) requiring permanent pacemaker (PPM) are a well-known complication after transcatheter aortic valve implantation (TAVI). This study aimed to determine the incidence of TAVI-related PPM and reevaluate the indications for PPM after the periprocedural period.METHODS AND RESULTS: A total of 258 consecutive patients underwent TAVI with the Medtronic CoreValve (MCV), whereas 24 patients were excluded from the study. TAVI-related PPM was defined as PPM implantation ≤30 days after the procedure and due to atrioventricular block (AVB). Third-degree AVB, second-degree type-II, or advanced second-degree AVB were considered as absolute indications for PPM. The incidence of TAVI-related PPM implantation was 27.4%. Forty-six patients (19.7%) had an absolute indication for PPM, but CA had resolved in 50% beyond the periprocedural period. Electrocardiographic analysis of the patients who did not have a TAVI-related PPM implantation showed that the PR and QRS intervals increased following TAVI, reaching a peak on days 4-6 and 7-9, respectively, before decreasing to near baseline levels.CONCLUSION: Although the incidence of periprocedural PPM implantation following TAVI was high, most CAs following TAVI tend to resolve after the periprocedural period. This suggests that delaying the decision for PPM implantation after TAVI may reduce the PPM rate.

Abstract
Background/objectivesTo determine pacemaker (PM) dependency at follow-up visit in patients who underwent new permanent pacemaker implantation (PPI) following transcatheter aortic valve implantation (TAVI).MethodsSingle center prospective observational study including 167 patients without previous PM implantation who underwent TAVI with the self-expanding Medtronic CoreValve System (MCS) between November 2005 and February 2011. PM dependency was defined by the presence of a high degree atrioventricular block (HDAVB; second [AV2] and third degree [AV3B]), or a slow (< 30 bpm) or absent ventricular escape rhythm during follow-up PM interrogation.ResultsA total of 36 patients (21.6%) received a new PM following TAVI. The indication for PM was AV2B (n = 2, 5.6%), AV3B (n = 28, 77.8%), postoperative symptomatic bradycardia (n = 3, 8.3%), brady–tachy syndrome (n = 1, 2.8%), atrial fibrilation with slow response (n = 1, 2.8%) and left bundle branch block (n = 1, 2.8%). Long term follow-up was complete for all patients and ranged from 1 to 40 months (median (IQR): 11.5 (5.0–18.0 months). Of those patients with a HDAVB, 16 out of the 30 patients (53.3%) were PM independent at follow-up visit (complete or partial resolution of the AV conduction abnormality). Overall, 20 out of the 36 patients (55.6%) who received a new PM following TAVI were PM independent at follow-up.ConclusionPartial and even complete resolution of peri-operative AV conduction abnormalities after MCS valve implantation occurred in more than half of the patients.

• Etude observationnelle multicentrique
• Objectif principal : Définir la persistance ou non de troubles conductifs de haut
grade au-delà de 7 jours après une procédure de TAVI
• Objectif secondaire :Valider les facteurs associés à l’évolution vers un BAV de
haut degré au long cours dans les suites d’une procédure de TAVI
Etude STIM TAVI
24

• Patients implantés d’un PM pendant l’hospitalisation pour la procédure de TAVI– Rythme sinusal– Pas d’indication de resynchronisation– PM Sorin avec réglage en AAI SafeR
• 250 patients, suivis pendant 1an
• Durée prévisible de l’étude : 2 ans
• Résultats de l’étude courant 2018
Etude STIM TAVI
25

26
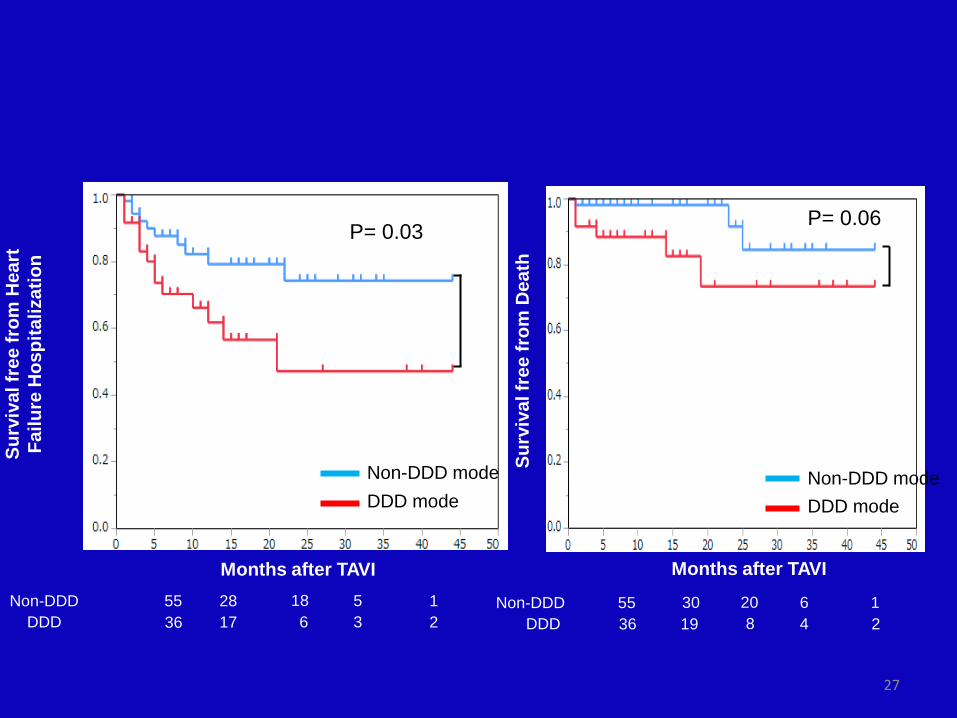
Background. Although high-degree atrioventricular conduction disturbance (AVCD) after transcatheter aortic valve implantation (TAVI) can require permanent pacemaker implantation (PPI), recovery of the AVCD is often observed. Specific pacemaker algorithms are now available which favor spontaneous atrioventricular conduction. Thus, this study aimed to assess the impact of pacemaker mode programming on clinical outcomes in patients with high-degree AVCD after TAVI.Methods and Results. Of 1621 consecutive multi-centric TAVI patients, 269 (16.4%) required PPI. We retrospectively included 91 patients with persistent high-degree AVCD at hospital discharge. Pacemaker dependency was defined as absence, inadequate intrinsic ventricular rhythm, or ventricular pacing time > 95% on pacemaker interrogation during follow-up. During a mean follow-up duration of 13 months, the pacemaker dependency rate was 52.8%. Patients with conventional DDD mode (N=36: 40.0%) had significantly more chronic kidney disease, larger implanted valve size, and more pacemaker dependency. Multivariate analysis showed that conventional DDD mode programming was independently associated with pacemaker dependency (odds ratio=3.63, P=0.03). Moreover, conventional DDD patients had a significant higher incidence of heart failure hospitalization (Hospitalization: DDD vs. others = 38.9% vs. 18.2%, P=0.04) and decreased left ventricular ejection fraction (ΔLVEF: DDD vs. the others = -10.1% [SD 11.0] vs. 0.5% [SD 12.7%], P=0.01). Conclusion. Up to half of patients implanted for high-degree AVCD after TAVI had conduction recovery. Patients with conventional DDD mode programming at hospital discharge had more pacemaker dependency and a worse cardiac prognosis. Thus, pacemaker mode should be systematically set to promote spontaneous atrioventricular conduction in patients with PPI after TAVI.
Impact du mode de programmation de stimulation à la sortie du patient
27
Surv
ival
free
from
Hea
rtFa
ilure
Hos
pita
lizat
ion
Months after TAVI
P= 0.03
DDD modeNon-DDD mode
Non-DDD 55DDD 36
2817
186
53
12
DDD modeNon-DDD mode
Surv
ival
free
from
Dea
th
Months after TAVI
P= 0.06
Non-DDD 55DDD 36
3019
208
64
12

PLACE DE LA RESYNCHRONISATION EN POST-TAVI

EKG charateristics of patients after TAVI
29
15,6%
52,0%
34,0%Immediate AVB
Large QRS (LBBB+RBBB)Narrow QRS

Mortality according to QRS duration
Meguro, Lellouche et al, AJC 2012

Heart Failure event according to QRS duration
Meguro, Lellouche et al, AJC 2012

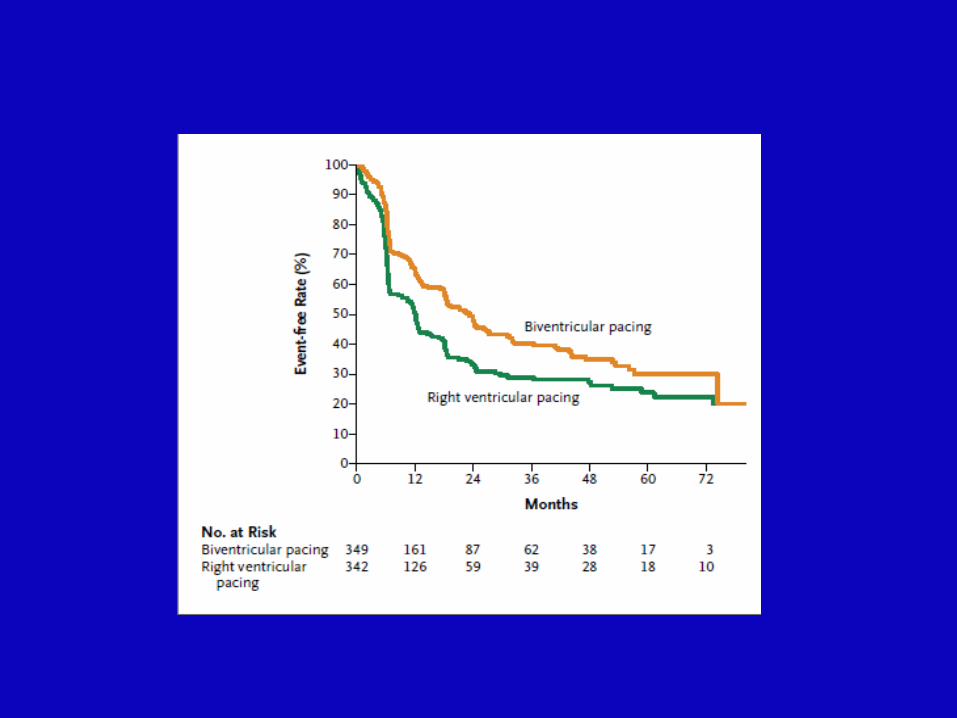
BLOCK-HF
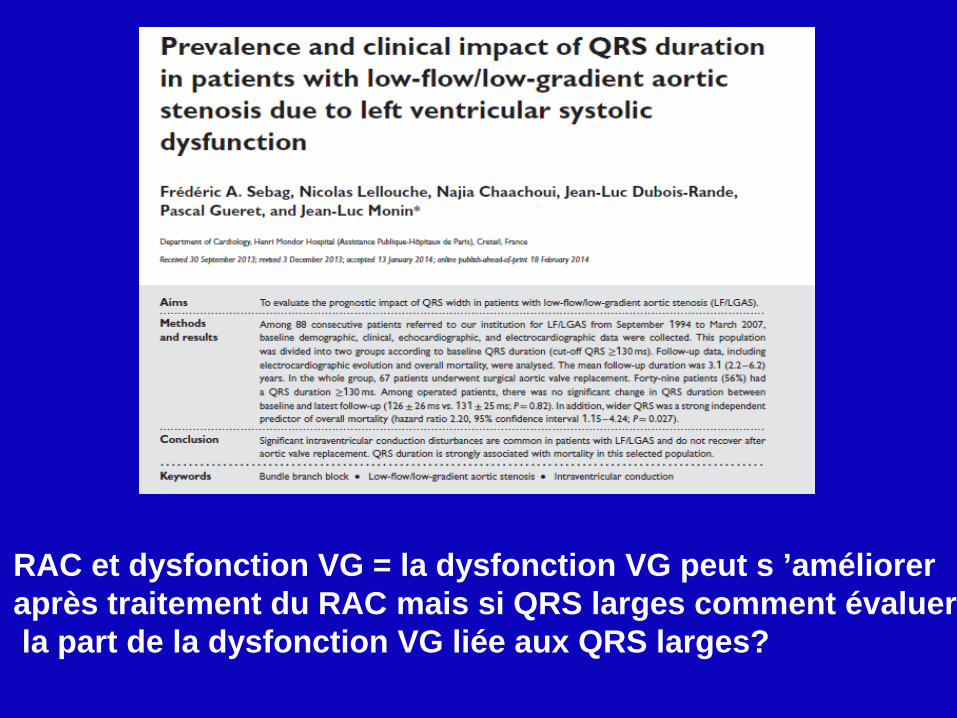
RAC et dysfonction VG = la dysfonction VG peut s ’améliorer après traitement du RAC mais si QRS larges comment évaluerla part de la dysfonction VG liée aux QRS larges?
-Si FEVG < 35% en pré TAVI et indication à PM pose d’un triple chambre
-Si FEVG entre 35-50% en pré TAVI et indication PM double ou triple chambre?
-Si apparition d’un BBG post TAVI sans réelle indication de PM contrôle patient avec bilan entre 1 et 3 mois puis rediscuter de l’indication d’une resynchronisation Cf recommandations européennes
En pratique TAVI et resynchronisation

Conclusion-L’implantation d’un PM est relativement fréquente après TAVI (10-20%) mais est en diminution
-Pas d’implantation prophylactique des BB droit pré TAVI ouBAV1 et/ou BBG post TAVI
-QRS fins post-TAVI hautement associé à l’absence de futurs troubles conductifs
-EEP peu intéressante
-Récupération des troubles conductifs après TAVI fréquents (50%) d’où intérêt de préserver la conduction Intrinsèque ventriculaire sur le mode du PM
-Indication de la resynchronisation pas clairement définie (récupération de la FEVG après TAVI?)

Thank you for your attention!!!
37