Embed Size (px)
Citation preview

Pediatric Pulmonology 44:1025–1032 (2009)
Pulmonary Function Changes in Children AfterTranscatheter Closure of Atrial Septal Defect
Yu-Sheng Lee, MD,1,2,3 Mei-Jy Jeng, MD, PhD1,2,3, Pei-Chen Tsao, MD,1,2 Chia-Feng Yang, MD,1
Wen-Jue Soong, MD,1,2,3* Betau Hwang, MD,3,4 and Ran-Bin Tang, MD1,3
Summary. This study was performed to assess changes in pulmonary function test (PFT) and
pulmonary outcome after transcatheter closure of atrial septal defect (ASD) in pediatric patients.
A total 55 pediatric patients undergoing transcatheter ASD closure received PFTat baseline (day
before ASD closure), and at 3 days and 6 months after procedure. Forced vital capacity (FVC),
forced expired volume in 1 sec (FEV1), FEV1 to FVC ratio (FEV1/FVC), peak expiratory flow (PEF),
and mean forced expiratory flow during the middle half of FVC (FEF25–75) were measured.
Individually, subjects were classified by spirometry as normal, obstructive or restrictive, to evaluate
the effect of transcatheter closure on pulmonary outcome. These 55 children had significantly
reduced mean PEF and FEF25–75 (84�24%, P¼ 0.040 and 76�22%, P¼0.010, respectively) at
baseline, with FEF25–75 reduced significantly at 3 days and 6 months (78�24%, P¼0.010 and
81� 24%, P¼0.040, respectively) after transcatheter closure. Six months after transcatheter
closure of ASD, significant improvement was observed in mean FVC (94�19% vs. 98� 15%,
P¼0.034) and FEV1 (90�20% vs. 96� 19%, P¼ 0.008). Assessed individually, better pulmonary
outcome was found in patients without pulmonary hypertension (PH) (w2¼8.333, P¼ 0.044). PFT
disturbance was observed in significant flow limitation in the peripheral airway of ASD patients.
Improved PFTwas found after transcatheter closure and better pulmonary outcome was observed
in patients without PH. ASD children need monitoring pulmonary function and should receive
transcatheter closure before PH develops. Pediatr Pulmonol. 2009; 44:1025–1032.
� 2009 Wiley-Liss, Inc.
Key words: atrial septal defect; pulmonary function; pulmonary hypertension;
spirometry.
INTRODUCTION
Congenital atrial septal defect (ASD) is commonamong congenital heart diseases (CHD) in children,and can occur in several different anatomic levels ofthe atrial septum. According to location, ASD can beclassified as secundum, primum, and sinus venosus types.Secundum ASD accounts for 6–10% of CHD at birth,1
often as an isolated lesion.The left-to-right blood shunting ASD allows may
induce right heart volume overload. Long term exposureto right heart volume overload may cause right atrium andventricle dilatations and increase pulmonary blood flow, inturn leading to pulmonary hypertension (PH) and rightside heart failure.2 Pathologic pulmonary hemodynamicsprenatally and postnatally lead to abnormalities inlung structure,3 and these changes result in pulmonaryfunction abnormalities. Despite a large spectrum ofchanges in pulmonary function test (PFT) parametershave been reported in patients with ASD,4–11 the resultsof these studies are conflicting. The most prominentpulmonary abnormality is lung volume restriction.7,10–12
Some authors report changes in residual volume, func-tional residual capacity,10,11,13 and non-uniform changes
1Department of Pediatrics, Taipei Veterans General Hospital, Taipei,
Taiwan.
2Institute of Emergency and Critical Care Medicine, School of Medicine,
National Yang-Ming University, Taipei, Taiwan.
3Faculty of Medicine, Department of Pediatrics, School of Medicine,
National Yang-Ming University, Taipei, Taiwan.
4Department of Pediatrics, Taipei City Hospital, Zhongxiao Branch, Taipei,
Taiwan.
*Correspondence to: W.J. Soong, MD, Division of General Pediatrics,
Department of Pediatrics, Taipei Veterans General Hospital, Number 201,
Section 2 Shih-Pai Road, Taipei 112, Taiwan.
E-mail: [email protected]
Received 11 November 2008; Revised 9 May 2009; Accepted 10 May
2009.
DOI 10.1002/ppul.21100
Published online 16 September 2009 in Wiley InterScience
(www.interscience.wiley.com).
Grant sponsor: Taipei Veterans General Hospital; Grant number: V97A-
018.
� 2009 Wiley-Liss, Inc.

in lung elasticity.9,10,14,15 On the other hand, otherstudies demonstrate normal or decreased airwaypatency.4,5,7,8,10,11
Closure of the interatrial defect is the treatment ofchoice for ASD with significant pulmonary to systemicflow ratio, even if the patient has few or no symptoms.16
Surgical repair of an ASD is a widely accepted low-riskprocedure,17 but carries with it risk of morbidity,discomfort, and thoracotomy scar.18 Percutaneous trans-catheter closure of ASD, first described by King et al.,19
has became a secure, efficient, and cost effective option fordefect management.20–22 Improvements in PFT para-meters occur following the closure of the left-to-rightshunt of ASD in the pulmonary circulation. Whileprevious studies have compared PFT indices before andafter open heart surgery for ASD,7–9 there is no publisheddata regarding the changes of PFT parameters aftertranscatheter closure in pediatric ASD patients. Our aim inthis study was therefore to assess the changes in PFTand pulmonary outcome in pediatric patients after trans-catheter closure of ASD.
MATERIALS AND METHODS
This was a prospective study conducted in ourinstitution, and the study protocol was approved by theinstitutional review board of our hospital. Pediatricpatients with secundum ASD referred for percutaneoustranscatheter closure were eligible for study. All patientswere asymptomatic while enrolled and were excluded ifthey had history of asthma or other acute respiratoryillness during the 4 weeks before testing. None of thesepatients received previous thoracic surgery, nor were theyassociated with chest wall deformity, congenital anomaly,or other additional CHD. All patients’ parents or guardianssigned individual informed consent before enrollment,and all procedures were in accordance with the ethicalguidelines of our institution.
Background demographic and clinical characteristicsfor this study were collected and recorded as follows:gender, body height, body weight, and size of ASDdetected by echocardiography. All patients received a
complete two-dimensional and color Doppler trans-thoracic echocardiography to assess cardiac anatomyusing an Acuson 128XP ultrasound system with atransducer appropriate to their size and body weightbefore and after successful transcatheter closure. Hemo-dynamic study and transcatheter ASD closure wereperformed under sedation and local anesthesia. Standardright heart catheterization was performed, and pulmonaryartery, right ventricle, and right and left atrial pressureswere obtained with standard fluid-filled catheters. Meanpulmonary artery pressure (MPAP), right ventriclesystolic pressure (RVSP), and ratio of pulmonary tosystemic flow (Qp/Qs) were recorded. The size, location,and relation of the ASD to surrounding structures wereassessed by transesophageal echocardiography (TEE).Qp/Qs flow ratio was calculated by oxymetry using theFick principle. The defect was demonstrated angio-graphically and the stretched diameter measured aspreviously described.23 An Amplatzer septal occluder(AGA Medical Corporation, Plymouth, MN) was thenimplanted using previously reported techniques.24
Absence of residual shunt or obstruction created by thedevice was confirmed by TEE.
These ASD patients received PFT at baseline (daybefore transcatheter closure of ASD), and at 3 days and6 months after the procedure. Spirometry was performedaccording to the American Thoracic Society (ATS) andEuropean Respiratory Society (ERS) criteria for childrento ensure quality.25,26 The same equipment (Exhalyzer’sSpiroware, Eco Medics AG, Duernten, Switzerland) wasused to measure PFT in all patients. Spirometry wascarried out with the patient standing, rest allowed betweeneach repeated test. At least three trials were performed byeach patient and the curve with the largest forced vitalcapacity (FVC) and forced expired volume in 1 sec (FEV1)was chosen as the best trial. The FVC, FEV1, FEV1 to FVCratio (FEV1/FVC), peak expiratory flow (PEF), and meanforced expiratory flow during the middle half of the FVC(FEF25–75) were measured. Predicted value was basedon the spirometric reference equations for children inTaiwan.27 PFT results were expressed as percentage ofpredicted values.
Pulmonary outcome was assessed individually based onPFT data. The children at baseline, and 6 months afterpercutaneous transcatheter ASD closure were classifiedas either normal (FVC and FEV1 �80% of predictedvalue with normal FEV1/FVC), obstructive (FEV1/FVC<80%), or restrictive (FVC<80% of predicted value withnormal FEV1/FVC).
Statistical Analysis
All data were expressed as the mean� SD. Univariantcorrelation between continuous variables was calcu-lated by Pearson’s coefficient. Difference among PFT
ABBREVIATIONS
ASD Atrial septal defect
CHD Congenital heart disease
FEF25–75 Mean forced expiratory flow during the middle half of
the forced vital capacity
FEV1 Forced expired volume in 1 sec
FVC Forced vital capacity
FEV1/FVC The FEV1 to FVC ratio
PEF Peak expiratory flow
PFT Pulmonary function test
PH Pulmonary hypertension
RVSP Right ventricle systolic pressure
TEE Transesophageal echocardiography
Pediatric Pulmonology
1026 Lee et al.

parameters and the reference standard at baseline, 3 days,and 6 months after percutaneous transcatheter ASDclosure was analyzed by two-tailed, independent t-test.PFT parameters between baseline, 3 days, and 6 monthsafter procedure were compared by repeated measuredone-way analysis of variance (ANOVA), and multiplecomparisons of means were performed when a significantdifference between groups was apparent. The effect oftranscatheter closure of ASD was analyzed by Chi-squaretest, and Fisher’s exact test was performed when cells’expected count <5. A value of P< 0.05 was consideredstatistically significant. The statistical program SPSSversion 15.0 was used for data analysis (SPSS Inc.,Chicago, IL).
RESULTS
From August 2005 to December 2007, 55 pediatricpatients, 24 (43.6%) males and 31 (56.4%) females, wereenrolled in this study. None had evidence of primarypulmonary disease. Mean age of patients at baseline was9.5� 3.1 years old. Mean diameter of secundum ASD was10.2� 5.8 mm as detected by transthoracic echocardio-graphy. Mean Qp/Qs was 2.1� 0.8, and 10 (18.2%)patients were >2. Mean MPAP before transcatheterclosure of ASD was 19.1� 5.8 mmHg, and 9 (16.4%)patients had MPAP >25 mmHg, defined as PH.28 Thoughpatients with PH had higher RVSP than those without PH,the age, body height, body weight, secundum ASDdiameter, and Qp/Qs were not statistically differentbetween the subgroup with and without PH. The baselineclinical, echocardiographic, and hemodynamic charac-teristics of the 55 patients included in the study aresummarized in Table 1. No correlation was found betweenPFT measurements at baseline and after closure of defectand age at transcatheter closure, body height, body weight,ASD diameter, Qp/Qs, MPAP, or RVSP.
Compared to the reference standard at baseline,these 55 children had reduced mean FVC, FEV1, PEF,and FEF25–75, but only mean PEF and FEF25–75 weresignificantly reduced. At 3 days and 6 months aftertranscatheter closure of ASD, these children still hadlower mean FVC, FEV1, PEF, and FEF25–75, with onlymean FEF25–75 statistically significant. The 46 patientswithout PH had no significant difference in mean FVC,FEV1, PEF, and FEF25–75 at baseline, 3 days and 6 monthsafter transcatheter closure of ASD. But the nine patientswith PH had significant lower mean FEF25–75 at baseline,3 days after, and 6 months after transcatheter closure ofASD. The comparison of PFT parameters and thereference standard in these ASD patients before and afterpercutaneous transcatheter closure is summarized inTable 2.
In the whole group when compared with baseline, PFTparameters did not significantly change 3 days after
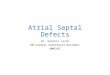
procedure. Six months after transcatheter ASD closure,significant improvement of PFT parameters was observedin mean FVC (94� 9% vs. 98� 15%, P¼ 0.034) andFEV1 (90� 20% vs. 96� 19%, P¼ 0.008). Mean PEFand FEF25–75 tended to increase after transcatheterclosure of ASD, but did not reach statistical significance.ASD patients without PH showed no significant improve-ment in PFT parameters at 3 days and 6 months aftertranscatheter closure. ASD patients with PH showed nosignificant difference 3 days after transcatheter closure ofASD but FVC (92� 18% vs. 98� 18%, P¼ 0.012) andFEV1 (89� 21% vs. 95� 19%, P¼ 0.013) were improvedsignificantly at 6 months after transcatheter closure.The changes of PFT parameters at baseline, 3 days, and6 months after transcatheter closure of ASD in thesepatients and in the subgroup with or without PH are shownin Figure 1.
Pulmonary classification of ASD patients at baselineand 6 months after transcatheter closure of ASD is shownin Table 3. Of the 55 children completing spirometry tests,34 (61.8%) had normal PFT, 9 (16.4%) had obstructivedefect, and 12 (21.8%) had restrictive defect before
Pediatric Pulmonology
TABLE 1— Baseline Clinical, Echocardiographic, andHemodynamic Characteristics of the Study Patients
Mean� SD N (%)
Patients 55
Mean pulmonary artery pressure
(mmHg)
19.1� 5.8
PH (�) 17.3� 4.1 46 (83.6%)
PH (þ) 30.3� 1.5* 9 (16.4%)
Gender
Male 24 (43.6%)
Female 31 (56.4%)
Age (years) 9.5� 3.1
PH (�) 8.7� 2.0
PH (þ) 9.5� 4.2
Body height (cm) 134.3� 19.0
PH (�) 129.6� 16.6
PH (þ) 132.0� 11.8
Body weight (kg) 33.1� 12.2
PH (�) 30.6� 9.9
PH (þ) 38.5� 18.8
Secundum ASD diameter,
TTE (mm)
10.2� 5.8
PH (�) 10.0� 3.4
PH (þ) 15.1� 4.9
Qp/Qs 2.1� 0.1
PH (�) 2.0� 0.6
PH (þ) 2.2� 0.3
Right ventricle systolic
pressure (mmHg)
32.4� 6.7
PH (�) 29.8� 5.3
PH (þ) 37.8� 6.1*
PH (�), without pulmonary hypertension; PH (þ), with pulmonary
hypertension; TTE, transthoracic echocardiography; Qp/Qs, the ratio of
pulmonary to systemic flow.
*P< 0.05.
Pulmonary Function in ASD Children 1027

transcatheter closure. Three children with reduced FVCalso had a minimal obstructive component because theirFVC were<80% of predicted values and their FEV1/FVCwere <80%, so they were classified with restrictivedefect. Of the 46 ASD patients without PH, 28 (60.1%)had normal pulmonary function, nine (19.6%) hadobstructive defect, and nine (19.6%) had restrictive defect.Of the nine ASD patients with PH, six (66.7%) wereclassified as normal, and three (33.3%) had restrictivedefect. Six months after transcatheter closure of ASD,patients with normal pulmonary function increased from34 (61.8%) to 43 (78.2%); patients with air flowobstruction decreased from 9 (16.4%) to 6 (10.9%);and patients with restrictive defect also decreased, from12 (21.8%) to 6 (10.9%). Significant improvement wasobserved 6 months after transcatheter closure of ASD(w2¼ 12.429, P¼ 0.011). Better pulmonary outcome aftertranscatheter closure was observed in the 46 patientswithout PH (w2¼ 8.333, P¼ 0.044): patients with normalPFT increased from 28 (68.1%) at baseline to 37 (80.4%)6 months after procedure; and six of nine patients withair flow obstruction and three of nine with restrictivedefect at baseline were reclassified as normal. There wasno significant difference in pulmonary classification inpatients with PH (w2¼ 3.000, P¼ 0.333) after trans-catheter closure of ASD: six with normal pulmonaryclassification before closure were still normal afterclosure; and three patients with restrictive defect remainedin the same classification 6 months after ASD closure.
DISCUSSION
To our knowledge, this is the first study to show thechanges of PFT parameters after transcatheter closure ofASD in pediatric patients. As a whole, these children with
Pediatric Pulmonology
TABLE 2— Comparison of PFT Parameters in ASD Patientsand the Reference Standard at Baseline and AfterTranscatheter ASD Closure
PFT parameters Baseline 3 days after 6 months after
FVC 94� 19 94� 19 98� 15
PH (�) 97� 17 98� 19 102� 14
PH (þ) 92� 18 93� 17 98� 18
FEV1 90� 20 91� 20 96� 19
PH (�) 93� 18 94� 19 100� 16
PH (þ) 89� 21 91� 21 95� 19
PEF 84� 24* 86� 28 86� 25
PH (�) 85� 21 88� 27 90� 30
PH (þ) 79� 18 81� 23 84� 10
FEF25–75 76� 22* 78� 24* 81� 24*
PH (�) 77� 19 79� 10 82� 10
PH (þ) 75� 23* 79� 26* 80� 26*
FEV1/FVC 85� 8 85� 8 87� 7
PH (�) 85� 6 84� 6 87� 8
PH (þ) 85� 8 86� 6 85� 6
Values are expressed as mean� SD.
ASD, atrial septal defect; PFT, pulmonary function test; PH (�),
without pulmonary hypertension; PH (þ), with pulmonary hyper-
tension; FVC, forced vital capacity; FEV1, forced expired volume in
1 sec; FEV1/FVC, FEV1 to FVC ratio; PEF, peak expiratory flow;
FEF25–75, forced expiratory flow between 25% and 75% of vital
capacity.
*P< 0.05.
Fig. 1. The changes of pulmonary function parameters in
ASD patients at baseline, 3 days after, and 6 months
after transcatheter closure. * indicate FVC; * indicate FEV1;
& indicate PEF; & indicate FEF25–75 ASD, atrial septal defect;
PFT, pulmonary function test; FVC, forced vital capacity; PH,
pulmonary hypertension; FEV1, forced expired volume in 1 sec;
PEF, peak expiratory flow; FEF25–75, forced expiratory flow
between 25% and 75% of vital capacity. *P<0.05.
1028 Lee et al.

ASD had a significant reduction in mean PEF andFEF25–75 at baseline, and only mean FEF25–75 signifi-cantly lower than the reference standard after trans-catheter closure of ASD. There was no significantimprovement in mean FEF25–75 after correction whencompared with baseline. This result means that an elementof airflow obstruction in the central and peripheral airwaywas observed at baseline, consistent with previousstudies.8,11,13,29 The peripheral airway obstruction per-sisted even after transcatheter closure of ASD. Thelimitation of peripheral airway airflow may be due toincreased pulmonary blood flow, engorged capillarynetwork, or abnormalities in the elastic properties of thelung.3,10,30 Lung biopsy was not performed in our patients,so it is difficult to draw any conclusion on anatomicalabnormalities. We assume that high pulmonary bloodflow resulted in pulmonary vascular changes leading toprogressive remodeling of the lung parenchyma andeven fibrotic changes.14,31 Children with ASD suffer fromimpaired lung function partly because of the pathologichemodynamics of the lungs and partly because ofhistological changes in lung tissue. Changes of thepulmonary vascularity and the lung parenchyma maynot be reversed after transcatheter closure of ASD, stillcausing flow limitation in the peripheral airway. Absenceof significant changes in the peripheral airway indicatethat pulmonary vascularity and lung parenchyma pro-blems were not resolved, either because they are stillstructured or because the changes take more than 6 monthsto be reverted.
The mean FVC and FEV1 improved significantly6 months after transcatheter closure, which reflects thepossibility that lung volume and central airway patencymay be improved after transcatheter closure of ASD. Sulcet al.8 reported the same improvement in central airwayobstruction after heart surgery for ASD. Airway obstruc-tion is well-recognized in children with CHD.32,33 The
increased shunting of blood flow in ASD leads to enlargedright-sided heart chambers, dilated main pulmonaryarteries, and increased pulmonary vascularity. Thiscompetition for space between heart chambers, vessels,and airways within the thoracic cavity increases airwayresistance. Previous studies have reported that trans-catheter closure of ASD may restore right ventriclevolume and decrease pulmonary blood flow,34,35 so wespeculate that the improved FVC and FEV1 may be dueto abolition of left-to-right blood shunting, leading tovolume reduction after correction of defect.
Patients with ASD are at risk of developing PH36–38
caused by chronic exposure of the pulmonary vessels toincreased blood flow, which may produce histologicalchanges in the intima and media of the pulmonary arteriesand arterioles and result in luminal narrowing. Consistentwith previous reports of PH in 6–17% of patients withASD,39–41 the incidence of ASD with PH in our series was16.4%. Similar to previous reports in adults,37,42 we sawno correlation between degree of PH and defect size. ASDchildren with PH had significant decreases in mean PEFand FEF25–75 over the reference standard, and meanFEF25–75 did not return to normal even after transcatheterclosure. Furthermore, there were significant increases inmean FVC and FEV1 after transcatheter closure in ASDpatients with PH, increases not observed in patientswithout PH. This result suggests that lung volume andcentral airway patency might be reversed after trans-catheter closure of ASD, but flow limitation in theperipheral airways caused by changes in the pulmonaryvessels and lung parenchyma as a consequence oflong standing increased pulmonary blood flow persistsespecially in ASD patients with PH.
The present study demonstrates the PFT parameterstended to increase at 3 days soon after transcatheterclosure of ASD, though did not reach statistical signifi-cance. The insignificant difference of PFT parameters
Pediatric Pulmonology
TABLE 3— Pulmonary Classification in ASD Patients at Baseline and 6 Months AfterPercutaneous Transcatheter ASD Closure: N (%)
6 months after
Total
PFT
classification
Normal, 43
(78.2%)
Obstructive, 6
(10.9%)
Restrictive,
6 (10.9%)
Baseline
Normal 34 (61.8%) PH (�) 28 28 (60.1%)
PH (þ) 6 6 (66.7%)
Obstructive 9 (16.4%) PH (�) 6 3 9 (19.6%)
PH (þ)
Restrictive 12 (21.8%) PH (�) 3 3 3 9 (19.6%)
PH (þ) 3 3 (33.3%)
Total PH (�) 37 (80.4%) 6 (13.0%) 3 (36.5%) 46
PH (þ) 6 (66.7%) 3 (33.3%) 9
PH (�), without pulmonary hypertension; PH (þ), with pulmonary hypertension.
Whole group: P< 0.05; PH (�): P< 0.05.
Pulmonary Function in ASD Children 1029

between baseline and 3 days after shunt closure in ourstudy may imply that transcatheter closure of ASD doesnot deteriorate pulmonary function. Habre et al.42 reportedthat surgical repair of septal defect leads to improveairway mechanics significantly immediate after correctionof left-to-right shunt. The inconsistency of our findingswith the previous results may be due to the diversity ofcongenital cardiac lesions, the different method to closeseptal defect, and the dissimilar technique to evaluate PFTindices.
In addition to group results, we also classified each ASDchild individually based on spirometry result. Most of ourstudy population was classified with normal pulmonaryfunction at baseline. Twenty-one (38.2%) of 55 patientshad abnormal PFT at baseline, either restrictive orobstructive defects, and 12 (21.8%) had abnormal lungfunction after transcatheter closure of ASD. No specificpulmonary function defect was typical for ASD. The mostprominent PFT abnormality of ASD patients beforecorrection in our study was restrictive defect, consistentwith previous studies.7,10,11 The frequency of abnormalPFT in our study was lower than that reported by Sulcet al.8 in ASD patients before (18, or 69.2% of 26 ASDpatients) and after (12 or 50% of 24 patients) heart surgery.We infer that the difference in frequency of abnormal PFTbefore shunt correction may be due to the fact that ourstudy population was younger than that studied by Sulcet al. (9.5� 3.1 years vs. 11.8� 3.8 years, respectively).The younger the patients, the shorter the chronic exposureto volume overload and increased pulmonary blood flow,which may impact PFT. Moreover, the correction methodof ASD in our study was transcatheter closure, whereasheart surgery was the method for correction in the previousstudy. Surgical closure of ASD seems to result inpersisting right heart dysfunction up to several years;percutaneous transcatheter closure seems to lead fasterresolution of right heart dilatation.43,44 The surgicalprocedure itself might damage the lungs because thepatient receiving ASD surgery is exposed to thoracotomy,cardiopulmonary bypass and ventilation during theoperation period, any one of which might cause consid-erable structural or functional cardiopulmonary changes.Transcatheter closure of ASD is ideal because it involvesneither the anatomical nor the functional pulmonarychanges associated with heart surgery.
For the whole study population, the pulmonary outcomeimproved significantly 6 months after transcatheterclosure of ASD, indicated by the increased percentageof ASD children with normal pulmonary function. Thisimprovement of pulmonary outcome after transcatheterASD closure may be of clinical importance. The subgroupwithout PH saw significantly improved pulmonary out-come. In our opinion, PH may be an important pulmonaryprognostic factor for patients with ASD undergoingtranscatheter closure. The increased flow and chronic
changes in pulmonary circulation lead to alternations inpulmonary vessels and in the composition of lung tissuewhich may impair PFT even after correction. This resultimplies that transcatheter ASD closure should optimallybe performed before PH develops, even if the patientis asymptomatic, to improve pulmonary outcome. Other-wise, abnormal PFT, especially flow limitation in theperipheral airway, may not improve after shunt closure.
We use spirometry as the clinical modality toevaluate changes in PFT after transcatheter closure inASD children. Spirometry has proven invaluable as ascreening test of general respiratory health and is the mostfrequent PFT obtained by clinicians caring for childrenwith respiratory disease. We found a significant decreasein FEF25–75 among ASD children, and reduced FEF25–75
was still significant in patients with PH. A decreasedFEF25–75 may have marked clinical significance, andevaluation of spirometry in all ASD children at risk of lowFEF25–75 may be useful in identifying those children atgreatest risk of respiratory limitations.
Our study has some limitations. The follow-up PFTwasperformed only at 3 days and 6 months after transcatheterclosure of ASD. Extended long term PFT follow-up aftertranscatheter closure may be needed to clarify pulmonaryoutcome after shunt closure in pediatric patients. The PFTparameters determined in our study were limited andstudies of pulmonary volume and diffusion capacity maybe indicated to fully characterize the pulmonary functiondisturbance in ASD patients after transcatheter closure.
CONCLUSION
Our study shows that prominent pulmonary functiondisturbance is observed in the peripheral airway in ASDchildren before and after transcatheter closure of ASD,and improved PFT and pulmonary outcome can be foundafter shunt closure. ASD children should receive trans-catheter closure before PH develops because changes dueto volume overload and increased pulmonary blood flowmay lead to pulmonary function disturbance whichmay not return to normal even after closure of ASD.Spirometry should be used to provide regular assessmentof PFT in ASD children before and after transcatheterclosure, especially in those with PH.
REFERENCES
1. Dickinson DF, Arnold R, Wilkinson JL. Congenital heart disease
among 160 480 liveborn children in Liverpool 1960 to 1969.
Implications for surgical treatment. Br Heart J 1981;46:55–
62.
2. Graham TP Jr. Ventricular performance in congenital heart
disease. Circulation 1991;84:2259–2274.
3. Rabinovitch M, Keane JF, Norwood WI, Castaneda AR, Reid L.
Vascular structure in lung tissue obtained at biopsy correlated
with pulmonary hemodynamic findings after repair of congenital
heart defects. Circulation 1984;69:655–667.
Pediatric Pulmonology
1030 Lee et al.

4. Cowen ME, Jeffrey RR, Drakeley MJ, Mercer JL, Meade JB,
Fabri BM. The results of surgery for atrial septal defect in patients
aged fifty years and over. Eur Heart J 1990;11:29–34.
5. Davies H, Gazetopoulos N. Lung function in patients with left-to-
right shunts. Br Heart J 1967;29:317–326.
6. Lubica H. Pathologic lung function in children and adolescents
with congenital heart defects. Pediatr Cardiol 1996;17:314–315.
7. Schofield PM, Barber PV, Kingston T. Preoperative and post-
operative pulmonary function tests in patients with atrial septal
defect and their relation to pulmonary artery pressure and
pulmonary:systemic flow ratio. Br Heart J 1985;54:577–582.
8. Sulc J, Andrle V, Hruda J, Hucin B, Samanek M, Zapletal A.
Pulmonary function in children with atrial septal defect before
and after heart surgery. Heart 1998;80:484–488.
9. Sulc J, Samanek M, Zapletal A. Lung function in atrial septal
defect after heart surgery. Int J Cardiol 1992;37:15–21.
10. De Troyer A, Yernault JC, Englert M. Mechanics of breathing in
patients with atrial septal defect. Am Rev Respir Dis 1977;115:
413–421.
11. Yoshioka T, Kunieda T, Naito M, Fukunaga Y, Okubo S,
Nakanishi N. Effects of pulmonary hemodynamics on lung
function in adult patients with atrial septal defect. Jpn Circ J 1985;
49:960–966.
12. Bedell GN, Adams RW. Pulmonary diffusing capacity during rest
and exercise. A study of normal persons and persons with atrial
septal defect, pregnancy, and pulmonary disease. J Clin Invest
1962;41:1908–1914.
13. Wood TE, McLeod P, Anthonisen NR, Macklem PT. Mechanics
of breathing in mitral stenosis. Am Rev Respir Dis 1971;104:52–
60.
14. Wallgren G, Geubelle F, Koch G. Studies of the mechanics of
breathing in children with congenital heart lesions. Acta Paediatr
1960;49:415–425.
15. Griffin AJ, Ferrara JD, Lax JO, Cassels DE. Pulmonary
compliance. An index of cardiovascular status in infancy. Am
J Dis Child 1972;123:89–95.
16. Brochu MC, Baril JF, Dore A, Juneau M, De Guise P, Mercier LA.
Improvement in exercise capacity in asymptomatic and mildly
symptomatic adults after atrial septal defect percutaneous closure.
Circulation 2002;106:1821–1826.
17. Horvath KA, Burke RP, Collins JJ, Jr., Cohn LH. Surgical
treatment of adult atrial septal defect: early and long-term results.
J Am Coll Cardiol 1992;20:1156–1159.
18. Butera G, De Rosa G, Chessa M, Rosti L, Negura DG, Luciane P,
Giamberti A, Bossone E, Carminati M. Transcatheter closure of
atrial septal defect in young children: results and follow-up. J Am
Coll Cardiol 2003;42:241–245.
19. King TD, Thompson SL, Steiner C, Mills NL. Secundum atrial
septal defect. Nonoperative closure during cardiac catheter-
ization. JAMA 1976;235:2506–2509.
20. Bruch L, Parsi A, Grad MO, Rux S, Burmeister T, Krebs H,
Kleber FX. Transcatheter closure of interatrial communications
for secondary prevention of paradoxical embolism: single-center
experience. Circulation 2002;105:2845–2848.
21. Fischer G, Stieh J, Uebing A, Hoffmann U, Morf G, Kramer HH.
Experience with transcatheter closure of secundum atrial septal
defects using the Amplatzer septal occluder: a single centre study
in 236 consecutive patients. Heart 2003;89:199–204.
22. Pedra CA, Pedra SR, Esteves CA, Cassar R, Pontes SC, Jr., Braga
SL, Fontes VF. Transcatheter closure of secundum atrial septal
defects with complex anatomy. J Invasive Cardiol 2004;16:117–
122.
23. Rao PS, Langhough R, Beekman RH, Lloyd TR, Sideris EB.
Echocardiographic estimation of balloon-stretched diameter
of secundum atrial septal defect for transcatheter occlusion. Am
Heart J 1992;124:172–175.
24. Fischer G, Kramer HH, Stieh J, Harding P, Jung O. Transcatheter
closure of secundum atrial septal defects with the new self-
centering Amplatzer Septal Occluder. Eur Heart J 1999;20:541–
549.
25. Miller MR, Hankinson J, Brusasco V, Burgos F, Casaburi
R, Coates A, Crapo R, Enright P, van der Grinten CP,
Gustafsson P, Jensen R, Johnson DC, MacIntyre N, McKay
R, Navajas D, Pedersen OF, Pellegrino R, Viegi G, Wanger
J. Standardisation of spirometry. Eur Respir J 2005;26:319–
338.
26. Beydon N, Davis SD, Lombardi E, Allen JL, Arets HG, Aurora P,
Bisgaard H, Davis GM, Ducharme FM, Eigen H, Gappa M,
Gaultier C, Gustafsson PM, Hall GL, Hantos Z, Healy MJ, Jones
MH, Klug B, Lodrup Carlsen KC, McKenzie SA, Marchal F,
Mayer OH, Merkus PJ, Morris MG, Oostveen E, Pillow JJ,
Seddon PC, Silverman M, Sly PD, Stocks J, Tepper RS, Vilozni
D, Wilson NM. An official American Thoracic Society/European
Respiratory Society statement: pulmonary function testing in
preschool children. Am J Respir Crit Care Med 2007;175:1304–
1345.
27. Chang HL, Jeng MJ, Tsao PC, Kou YR, Soong WJ. Spirometric
Reference Equations for Healthy Children Aged 3 to 6 Years. ATS
2005 San Diego International Conference 2005:Abstract Page:
A183.
28. Barst RJ, McGoon M, Torbicki A, Sitbon O, Krowka MJ,
Olschewski H, Gaine S. Diagnosis and differential assessment of
pulmonary arterial hypertension. J Am Coll Cardiol 2004;43:
40S–47S.
29. Giannelli S, Jr., Ayres SM, Buehler ME. Effect of pulmonary
blood flow upon lung mechanics. J Clin Invest 1967;46:1625–
1642.
30. Rosengart R, Fisbein M, Emmanouilides GC. Progressive
pulmonary vascular disease after surgical correction (Mustard
procedure) of transposition of great arteries with intact ventricular
septum. Am J Cardiol 1975;35:107–111.
31. Corno A, Giamberti A, Giannico S, Marino B, Rossi E,
Marcelletti C, Kirklin JK. Airway obstructions associated with
congenital heart disease in infancy. J Thorac Cardiovasc Surg
1990;99:1091–1098.
32. deLorimier AA, Harrison MR, Hardy K, Howell LJ, Adzick NS.
Tracheobronchial obstructions in infants and children. Experience
with 45 cases. Ann Surg 1990;212:277–289.
33. Schoen SP, Kittner T, Bohl S, Braun MU, Simonis G, Schmeisser
A, Strasser RH. Transcatheter closure of atrial septal defects
improves right ventricular volume, mass, function, pulmonary
pressure, and functional class: a magnetic resonance imaging
study. Heart 2006;92:821–826.
34. de Lezo JS, Medina A, Romero M, Pan M, Segura J, Caballero E,
Pavlovic D, Ortega JR, Franco M, Delgado A, Ojeda S, Mesa D,
Lafuente M. Effectiveness of percutaneous device occlusion for
atrial septal defect in adult patients with pulmonary hypertension.
Am Heart J 2002;144:877–880.
35. Konstantinides S, Geibel A, Olschewski M, Gornandt L,
Roskamm H, Spillner G, Just H, Kasper W. A comparison of
surgical and medical therapy for atrial septal defect in adults. N
Engl J Med 1995;333:469–473.
36. Vogel M, Berger F, Kramer A, Alexi-Meshkishvili V, Lange PE.
Incidence of secondary pulmonary hypertension in adults
with atrial septal or sinus venosus defects. Heart 1999;82:30–
33.
37. Sachweh JS, Daebritz SH, Hermanns B, Fausten B, Jockenhoevel
S, Handt S, Messmer BJ. Hypertensive pulmonary vascular
disease in adults with secundum or sinus venosus atrial septal
defect. Ann Thorac Surg 2006;81:207–213.
38. Craig RJ, Selzer A. Natural history and prognosis of atrial septal
defect. Circulation 1968;37:805–815.
Pediatric Pulmonology
Pulmonary Function in ASD Children 1031

39. Cherian G, Uthaman CB, Durairaj M, Sukumar IP, Krishnaswami
S, Jairaj PS, John S, Krishnaswami H, Bhaktaviziam A.
Pulmonary hypertension in isolated secundum atrial septal defect:
high frequency in young patients. Am Heart J 1983;105:952–
957.
40. Steele PM, Fuster V, Cohen M, Ritter DG, McGoon DC. Isolated
atrial septal defect with pulmonary vascular obstructive disease—
long-term follow-up and prediction of outcome after surgical
correction. Circulation 1987;76:1037–1042.
41. Murphy JG, Gersh BJ, McGoon MD, Mair DD, Porter CJ, Ilstrup
DM, McGoon DC, Puga FJ, Kirklin JW, Danielson GK. Long-
term outcome after surgical repair of isolated atrial septal defect.
Follow-up at 27 to 32 years. N Engl J Med 1990;323:1645–
1650.
42. Habre W, Schutz N, Pellegrini M, Beghetti M, Sly PD, Hantos Z,
Petak F. Preoperative pulmonary hemodynamics determines
changes in airway and tissue mechanics following surgical repair
of congenital heart diseases. Pediatr Pulmonol 2004;38:470–476.
43. Dhillon R, Josen M, Henein M, Redington A. Transcatheter
closure of atrial septal defect preserves right ventricular function.
Heart 2002;87:461–465.
44. Ning SB, Fazal H, Cook D, Wood MM, Duncan WJ, Rowe RD.
Right ventricular size and ventricular septal motion after repair of
atrial septal defect in children. Can J Surg 1984;27:395–398.
Pediatric Pulmonology
1032 Lee et al.