Embed Size (px)
Citation preview

Pulmonary Edema
Pulmonary Medicine

Pulmonary Edema

Pulmonary Medicine
Pulmonary Edema

Copyright © 2011 Hindawi Publishing Corporation. All rights reserved.
This is a focus issue published in volume 2011 of “Pulmonary Medicine.” All articles are open access articles distributed under theCreative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided theoriginal work is properly cited.

Editorial Board
N. Ambrosino, ItalyMichel Aubier, FranceA. Azuma, JapanM. Safwan Badr, USALeif Bjermer, SwedenDemosthenes Bouros, GreeceDina Brooks, CanadaAndrew Bush, UKDenis Caillaud, FranceStefano Centanni, ItalyPascal O. Chanez, FranceEdwin Chilvers, UKKazuo Chin, JapanBruno Crestani, FranceRoberto Walter Dal Negro, ItalyJean-Charles Dalphin, FranceP. Dekhuijzen, The Netherlands
Burton F. Dickey, USAEric Duiverman, The NetherlandsJim Egan, IrelandArmin Ernst, USAR. Farre, SpainDimitris Georgopoulos, GreeceJorrit Gerritsen, The NetherlandsNicole S. L. Goh, AustraliaHartmut Grasemann, CanadaAndrew Greening, UKAndrew J. Halayko, CanadaFelix Herth, GermanyAldo T. Iacono, USAS. L. Johnston, UKMarc A. Judson, USARomain Kessler, FranceKazuyoshi Kuwano, Japan
Joseph P. Lynch, USAJudith C. W. Mak, Hong KongHisako Matsumoto, JapanLuisetti Maurizio, ItalyM. S. Niederman, USAAkio Niimi, JapanT. Penzel, GermanyMilos Pesek, Czech RepublicIrwin Reiss, GermanyLuca Richeldi, ItalyAndrew Sandford, CanadaOm P. Sharma, USACharlie Strange, USAE. R. Swenson, USAJun Tamaoki, JapanJeremy P. T. Ward, UKEmiel Wouters, The Netherlands

Contents
Amiloride-Sensitive Sodium Channels and Pulmonary Edema, Mike Althaus, Wolfgang G. Clauss,and Martin FroniusVolume 2011, Article ID 830320, 8 pages
The Curious Question of Exercise-Induced Pulmonary Edema, Melissa L. Bates, Emily T. Farrell,and Marlowe W. EldridgeVolume 2011, Article ID 361931, 7 pages
Effects of Ischemic Acute Kidney Injury on Lung Water Balance: Nephrogenic Pulmonary Edema?,Rajit K. Basu and Derek WheelerVolume 2011, Article ID 414253, 6 pages
Standardization of Methods for Early Diagnosis and On-Site Treatment of High-Altitude PulmonaryEdema, Qiquan ZhouVolume 2011, Article ID 190648, 7 pages
Pulmonary Edema in Healthy Subjects in Extreme Conditions, Erika Garbella, Giosue Catapano,Lorenza Pratali, and Alessandro PingitoreVolume 2011, Article ID 275857, 9 pages

Hindawi Publishing CorporationPulmonary MedicineVolume 2011, Article ID 830320, 8 pagesdoi:10.1155/2011/830320
Review Article
Amiloride-Sensitive Sodium Channels and Pulmonary Edema
Mike Althaus, Wolfgang G. Clauss, and Martin Fronius
Institute of Animal Physiology, Justus-Liebig University of Giessen, Wartweg 95, 35392 Giessen, Germany
Correspondence should be addressed to Mike Althaus, [email protected]
Received 10 September 2010; Accepted 1 December 2010
Academic Editor: Andrew Sandford
Copyright © 2011 Mike Althaus et al. This is an open access article distributed under the Creative Commons Attribution License,which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
The development of pulmonary edema can be considered as a combination of alveolar flooding via increased fluid filtration,impaired alveolar-capillary barrier integrity, and disturbed resolution due to decreased alveolar fluid clearance. An importantmechanism regulating alveolar fluid clearance is sodium transport across the alveolar epithelium. Transepithelial sodium transportis largely dependent on the activity of sodium channels in alveolar epithelial cells. This paper describes how sodium channelscontribute to alveolar fluid clearance under physiological conditions and how deregulation of sodium channel activity mightcontribute to the pathogenesis of lung diseases associated with pulmonary edema. Furthermore, sodium channels as putativemolecular targets for the treatment of pulmonary edema are discussed.
1. Introduction
According to Fick’s law, the anatomy of the human lungpermits optimal gas exchange due to a large surface area anda thin diffusion barrier. The large surface area is generatedby the division of airways into smaller gas exchange units(alveoli). Alveoli consist of two cell types, alveolar type 1(AT1) and type 2 (AT2) cells. AT1 cells are large, flat cellsthat build the bulk of the alveolar surface. In contrast, AT2cells are smaller cuboidal cells, which are active secretorycells and are responsible for the secretion of surface activeproteins and lipids, which are referred to as surfactant.Both cell types form tight junctions and thereby build apolar organised epithelium with an apical, “air-faced”, and abasolateral, “blood-faced,” side. At the basolateral side, a thinbasal lamina separates the alveolar epithelium from the smallinterstitium and the capillaries of the lung. For effective gasexchange to take place, O2 and CO2 must cross the alveolarepithelium, the basal lamina, and the endothelial cells thatform the capillaries. Therefore, these layers are referred toas the alveolar-capillary barrier. This barrier has a distanceof less than 1 μm, a diffusion distance that is thin enough toallow efficient gas exchange. Thus, the anatomy of the mam-malian lung and the structure of the alveoli satisfy Fick’s lawof diffusion in terms of requirements for a large surface areaand thin diffusion distance and establish the physical require-ments for optimal gas exchange of air breathing mammals.
The consequence of the proximity of the capillaries to thealveolar epithelium, however, is that small amounts of liquidare permanently forced into the alveolar airspaces due toblood pressure. This fluid contributes to alveolar lining fluid,facilitating diffusion of dissolved gases such as O2 and CO2.However, increased fluid volume in the alveoli characterisedleads to an extension of the gas diffusion distance. Therefore,mechanisms must exist which remove infiltrated fluid fromthe alveoli—a process referred to as alveolar fluid clearance.For this, the reabsorption of Na+ from the alveoli, especiallyvia the activity of Na+ channels in the pulmonary epithelium,is of particular importance and will be discussed in furtherdetail below.
2. Na+ Channels and Their Role in AlveolarFluid Clearance
As described above, AT1 and AT2 cells are linked togetherby tight junctions. The formation of tight junctions betweenthese epithelial cells not only results in a tight linkage ofthe cells to one another, but also limits the free diffusionof transmembrane protein complexes. Thus, the proteinrepertoire of the apical membrane of the alveolar epitheliumdiffers from that of the basolateral membrane. This issue isof particular importance for transepithelial Na+ transport,a mechanism that is crucial for alveolar fluid clearance.Transepithelial Na+ transport occurs primarily through

2 Pulmonary Medicine
Air-faced side
H2O
Blood-faced side
Tight
junction
Na+ channels
K+ channelsNa+/K+ ATPase
K+
Na+
Na+ Na+
Aquaporins
Aquaporins
K+
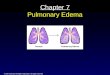
Figure 1: Transepithelial Na+ transport drives alveolar fluidclearance. Na+ enters the cell interior passively following anelectrochemical gradient via Na+ channels, which are located at theapical membrane of alveolar epithelial cells. The Na+ ions are thenactively pumped out of the cells by the Na+/K+-ATPase in exchangefor K+ ions, which leave the cell afterwards via basolaterally localizedpotassium channels. Thus, there is a net movement of Na+ ionsfrom the apical (air-faced) to the basolateral (blood/interstitium-faced) side of the alveolar epithelium. This creates osmotic forces,and, consequently, water follows out of the airspaces across theepithelium either paracellularly via tight junctions or transcellularlyvia aquaporins. The figure has been modified from [2].
the interplay of two transport systems: Na+permeable ionchannels, such as the epithelial Na+ channel (ENaC), locatedat the apical membrane, as well as the basolaterally localizedNa+/K+-ATPase (Figure 1). The Na+ ions enter the cells,following an electrochemical gradient, at the apical mem-brane via Na+ channels and are extruded at the basolateralside by the activity of the Na+/K+-ATPase. This leads to anet movement of Na+ from the apical to the basolateralside of the alveolar epithelium. This transepithelial Na+
transport in turn creates osmotic forces which drive themovement of water from the apical to the basolateral side.Water crosses the alveolar epithelium either paracellularlyvia tight junctions or transcellularly via water channels, oraquaporins, which are expressed in alveolar type 1 cells [1].Water is eventually removed from the lungs via the lymphaticor capillary system.
Thus, alveolar fluid clearance is a direct consequenceof transepithelial ion and, particularly, Na+ transport(Figure 1). This correlation was demonstrated in a study byHummler et al., where knock-out mice that did not expressthe alpha subunit of the epithelial Na+ channel (ENaC)in the alveolar epithelium died after birth due to defectiveneonatal fluid clearance and fluid accumulation in the lungs[3]. Consistent with this study, lung-specific knockdown ofαENaC using siRNA decreased baseline fluid clearance in ratsin vivo [4].
These examples underline the fact that Na+ channels inthe pulmonary epithelium play a key role in driving alveolarfluid clearance and, thus, the regulation of the fluid contentof the airspaces in the lung.
3. Na+ Channels in the Pulmonary Epithelium
Several types of Na+ channels have been described in alveolarepithelial cells, including channels sensitive to the diureticamiloride as well as cyclic nucleotide gated cation channels[5, 6]. Amiloride-sensitive Na+ channels in particular arethought to represent the major pathway for apical Na+ entryinto alveolar epithelial cells [7, 8]. Their contribution to alve-olar fluid clearance has been demonstrated in studies, whichshow that amiloride is able to block active Na+ transport andfluid clearance in isolated lung models [9–13] and in vivoin animal studies. This finding was recently confirmed byusing genetically engineered mice with mutations conferringhypo- or hyperactivity of the amiloride-sensitive epithelialsodium channel (ENaC). Those studies demonstrated thatthe fluid content of the lungs is highly dependent on theactivity of amiloride-sensitive Na+ channels, thus illustratingthe major contribution of these channels to alveolar fluidclearance [14–16].
Two distinct types of amiloride-sensitive Na+ channelshave been described in alveolar epithelial cells: highly selec-tive Na+ channels (HSCs), which are characterized by a highselectivity towards Na+, and nonselective cation channels(NSCs), with no selectivity for Na+ over K+ [5, 6, 17–19].The HSCs are also referred to as “epithelial Na+ channel(ENaC)-like” Na+ channels [20]. The classical ENaC consistsof three subunits, α, β and γ[21], which might assemble as aheterotrimer to build a Na+-permeable channel spanning thecell membrane [22]. When these three subunits of ENaC arecoexpressed in Xenopus laevis oocytes, the resulting expressedchannel has almost identical characteristics to the HSCsidentified from lung cells [18, 23, 24]. Therefore, the HSCobserved in lung epithelia might be ENaC consisting of theα, β and γ subunits [6, 18, 25, 26]. In contrast to the HSCs,the structure and subunit composition of NSCs are still notcompletely understood [19, 20]. It is speculated that NSCsmight solely be formed by the α subunit of ENaC [27].In order to clarify these topics, it is important to identifythe precise structure and subunit stoichiometry in whichthe classical ENaC subunits might assemble to form eitherselective or nonselective ion channels. In this regard, it isalso noteworthy that an additional subunit of ENaC (δ)has been described in humans [28] which has at least twofunctionally different splice isoforms [29, 30] that are alsoexpressed in the human lung (unpublished observations)and lung epithelial cells [31, 32]. The δ subunit of ENaCcan replace the α subunit, forming Na+ channels togetherwith β and γ subunits when heterologously expressed inXenopus laevis oocytes [28]. Interestingly, these channelshave different biophysical properties when compared tochannels containing the α subunit [31]. To what extent,the δ ENaC subunits might be involved in, for example,forming NSCs and how these subunits might play a rolein amiloride-sensitive pulmonary transepithelial Na+ trans-port and alveolar fluid clearance however, remain to beelucidated.
It should be mentioned that there is also a fraction ofactive Na+ transport and alveolar fluid clearance which isinsensitive to amiloride [33]. However, which Na+ channels

Pulmonary Medicine 3
Normal situation
H2O
H2O
Alveolarepithelium
Na+ channels
Na+/K+ ATPase
Na+
Na+ Na+
(a)
Pulmonary edema
Inflammatory mediators
Hypoxia
5-HT Reactive speciesO
NET-1
Barrier damage
H2O
H2O
Alveolarepithelium
Na+ channels
Na+/K+ ATPase
Immune cells(macrophages/neutrophils)
Na+
Na+
(b)
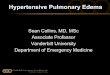
Figure 2: Impaired Na+ channel activity is associated with the development of pulmonary edema. (a) under normal conditionstransepithelial Na+ transport mediated via Na+ channels in the alveolar epithelium drives water reabsorption from the airspaces to theinterstitium. This mechanism counteracts water filtration into the airspaces and keeps the fluid layer covering the alveolar epithelium low.(b) a variety of factors that inhibit Na+ channels in the alveolar epithelium have been identified under diseases associated with pulmonaryedema such as HAPE or ALI/ARDS: hypoxia, inflammatory mediators which are released by activated immune cells (such as macrophagesor neutrophils), endothelin 1 (ET-1), reactive species such as nitric oxide (NO), or factors which are released due to hypoxia or epithelialstress such as serotonin (5-HT). The decreased activity of Na+ channels leads to decreased water reabsorption and fluid accumulation in theairspaces. Under pathological conditions such as HAPE or ALI/ARDS, there is additionally increased fluid filtration into the airspaces dueto impaired epithelial barrier integrity. The consequence of both impaired Na+ and thus water reabsorption and increased fluid filtrationis the development of pulmonary edema. The figure has been modified from [2]. For clarity, aquaporins and potassium fluxes/channels, asindicated in Figure 1, have been omitted.
or Na+-coupled transporters are involved in amiloride-insensitive transport across the alveolar epithelium remainsunknown (for detailed review see [33]).
Aside from the identification of the precise structureand composition of Na+ channels in the distal lung, animportant aspect is the question as to where in the distallung these channels are expressed. As described earlier, thealveolar epithelium consists of two cell types: AT1 and AT2cells. Although AT1 cells represent less than 10% of thecells in the lung, they form more than 98% of the lungsurface area [1]. In this regard, the classical paradigm wasthat AT1 cells are “biologically inert” cells that just contributeto the thin alveolar-capillary barrier whereas the “biologicallyactive” cells are AT2 cells [1]. Following that paradigm,until recently, the general view was that transepithelial Na+
absorption takes place solely by AT2 cells. However, giventhat AT2 cells correspond to less than 2% of the total lungsurface area, it seems surprising that these cells alone manageto drive alveolar fluid clearance by transepithelial Na+-transport. The idea of AT2 cells as the Na+ transporting cellin the distal lung is largely rooted in the fact that these cellshave been experimentally approachable for more than 30years [34] and have been intensively investigated. In contrast,techniques to isolate and investigate pure populations of AT1cells have only recently been developed [1, 35, 36]. Sincethen, there have been experimental hints that isolated AT1cells also express Na+ channels (HSC and NSC) [8, 37, 38]. It
should be mentioned that studies with AT2 cells have shownthat the expression of Na+ channels in isolated alveolarcells is highly sensitive to culture conditions [39], and thismakes it difficult to integrate data from isolated cells into aphysiological context. However, more recent data from theEaton group delivered hints for the existence of HSCs andNSCs in AT1 cells of lung slice preparations [40, 41]. Thus, itseems that AT1 and AT2 cells both express the Na+ channelrepertoire which makes them suitable for transepithelialNa+ transport. Therefore, the classical paradigm of pureAT2-driven Na+ absorption changes into the view that Na+
absorption takes place across the entire alveolar epitheliummediated by Na+ channels which are expressed both in AT1and AT2 cells.
4. Na+ Channels and the Development ofPulmonary Edema
Although many open questions remain concerning theprecise Na+ channel structure and spatial expression, thecorrelation between Na+ channel activity in AT1 and AT2cells and alveolar fluid clearance implies that there maybe a link between dysregulated Na+ channel activity andthe development of pulmonary edema due to impairedresolution of fluid (Figure 2). Evidence for this assumptioncomes from transgenic mice with loss-of-function muta-tions of amiloride-sensitive HSCs [14, 16]. These studies

4 Pulmonary Medicine
demonstrated that hypoactive Na+ channels in the lung notonly lead to impaired alveolar fluid clearance but also area predisposing factor for the development of pulmonaryedema [14].
The physiological importance of this association isevident when one considers the development of high-altitudepulmonary edema (HAPE). Mountaineers at high altitudeare faced with physical problems: decreased atmosphericpressure, hypoxia, and pulmonary hypertension due tohypoxic vasoconstriction. The lower atmospheric pressureleads to an increased pressure gradient between the airspacesof the lung and the body interior. Thus, the describedleakage of fluid—as a result of blood pressure—is enhanced.In addition, pulmonary blood vessels respond to hypoxiawith vasoconstriction, a mechanism that usually preventsnonventilated alveoli from being perfused. The pulmonaryblood pressure further increases fluid filtration into thelungs. In addition, there is also an impairment of barrierintegrity under HAPE which augments alveolar flooding(as reviewed in [42]). The situation becomes even moreproblematic, since there is also an impairment of fluidresolution due to impaired Na+-transport, and the activityof Na+ channels in particular. This phenomenon is interalia due to hypoxia-induced inhibition of Na+ channels[43, 44]. The decreased Na+ channel activity in hypoxiclungs is likely due to hypoxia-induced Na+ channel retrievalfrom the alveolar epithelial cell surface without affectingtotal expression of Na+ channels in the lung [45]. However,experimental studies concerning the latter issue deliveredcontroversial results [45–48], which might be due to thedifferent degrees of hypoxia employed in the used models.Nevertheless, the overall effect of hypoxia is an impairedtransepithelial Na+ transport, which is—at least in part—dueto impaired Na+ channel activity in the alveolar epithelium.This eventually leads to a reduction of fluid reabsorptionfrom the alveoli and thus contributes to the development ofpulmonary edema.
Taken together, the conditions leading to HAPE demon-strate how pulmonary edema can develop as a combi-nation of both increased fluid filtration and impairmentof transepithelial Na+ transport, especially epithelial Na+
channel activity (Figure 2). In this regard, there is alsoan association between transepithelial Na+ transport anda human lung disease which is referred to as acute lunginjury (ALI) or acute respiratory distress syndrome (ARDS[49]). Apart from pronounced inflammation and epithelialdamage, pulmonary edema is a hallmark of this disease[50, 51]. The formation of pulmonary edema in ALI/ARDSoccurs due to damage to the alveolar-capillary barrier, whichleads to fluid leakage into the alveoli and also due to defectivealveolar fluid clearance mechanisms [49]. Thus, in additionto increased edema formation due to epithelial damage,there is also an impairment of the resolution of edema dueto diminished alveolar fluid clearance, which is dependenton the efficacy of transepithelial Na+ transport [51]. Thereis a correlation between transepithelial Na+ transport andedema clearance in ALI/ARDS patients: patients that havea functional transepithelial Na+ transport exhibit improvedpulmonary edema resolution and have a better clinical
outcome compared to patients with defective transepithelialNa+ transport [51].
Thus, in the described pathophysiological situations,HAPE and ALI/ARDS, there is a link between transepithelialNa+ transport, Na+ channels in particular, and the devel-opment of pulmonary edema. Following that line, a varietyof factors have been identified which might account fora decreased activity of Na+ channels under these patho-physiological conditions (Figure 2). Increased synthesis ofnitric oxide (NO) due to, for example, upregulation ofnitric oxide synthases, has been demonstrated in ALI/ARDS[52, 53]. Furthermore, NO decreased the activity of Na+
channels (HSC and NSC) in alveolar epithelial cells [23,41, 54, 55]. Thus, there might be a link between thedevelopment or persistence of edema in ALI/ARDS and NO-mediated inhibition of Na+ channels. By contrast, defectiveNO synthesis is observed under HAPE [42]. However, thisputatively beneficial effect with respect to Na+ channelactivity might be outweighed by exaggerated pulmonaryhypertension and thus increased fluid filtration into thealveoli [42].
Another factor which might account for impaired Na+
channel activity and pulmonary edema is endothelin 1 (ET-1). ET-1 is a vasoconstrictor which regulates pulmonaryvascular tone [56]. Increased levels of ET-1 have beendemonstrated in HAPE [57] and ALI/ARDS [58]. In addi-tion, ET-1 inhibits epithelial Na+ channels in vitro [59] anddecreases alveolar fluid clearance in rats [60]. Thus, ET-1not only leads to enhanced fluid filtration due to pulmonaryhypertension, but might also represent a key factor thatimpairs the activity of Na+ channels and thus impairs theresolution of pulmonary edema in patients with HAPE orALI/ARDS.
Both examples, NO and ET-1, demonstrate how dysreg-ulated Na+ channel activity might occur under conditions asHAPE or ALI/ARDS. Apart from ET-1 and NO, a variety ofother factors have been identified which may also contributeto a decreased activity of Na+ channels and hence edemadevelopment (Figure 2): inflammatory mediators such asinterleukin-1beta [61] or tumor necrosis factor-alpha [62]or factors, such as serotonin, which are released as a resultof hypoxia or epithelial stress [63].
Thus, apart from hypoxia, there are intrinsic factorsthat occur in diseases associated with pulmonary edemawhich might contribute to disturbed fluid clearance, andhence edema resolution, by interference with Na+ channels inthe alveolar epithelium (Figure 2). Therefore, Na+ channelscan be regarded as key players with respect to edemaformation and might be promising targets for the treatmentof pulmonary edema.
5. Na+ Channels as Molecular Targets forthe Treatment of Pulmonary Edema?
The described examples, HAPE and ALI/ARDS, demonstratethat pathological situations in the lung which are associatedwith pulmonary edema can be correlated with an impairedactivity of Na+ channels and transepithelial Na+ transport.Consequently, it might be questioned whether enhancement

Pulmonary Medicine 5
of Na+ channel activity would enhance edema resolution andimprove the clinical outcome of patients with pulmonaryedema.
Experimental evidence that enhanced Na+ channel activ-ity might indeed improve edema resolution comes fromstudies using transgenic mice with hyperactive Na+ channels[64]. These mice carry a mutation in the β-subunit ofthe epithelial Na+ channel, ENaC, which leads to impairedchannel retrieval, and thus, persistence of ENaC at the cellsurface [65, 66]. This mutation is the genetic reason fora hereditary form of hypertension referred to as Liddle’ssyndrome [67]. Consistent with the association of Na+
channel activity and alveolar fluid clearance, baseline fluidclearance was increased in mice carrying the β-Liddlemutation compared to wild types [64]. Moreover, these micewere able to resolute hydrostatic pulmonary edema (inducedby volume overload due to saline infusion) much betterthan wild-type mice [64]. These results demonstrate thatincreasing Na+ channel activity might be a putative tool topotentiate alveolar fluid clearance and thereby enhance theresolution of pulmonary edema.
In this regard, β-adrenergic agonists are prominentactivators of Na+ channels in the alveolar epithelium andtherefore stimulators of alveolar fluid clearance (for detailedreview see [7]). This finding has been confirmed recently inmutant mice with low expression of epithelial Na+ channels(β-ENaC) which show no increase in alveolar fluid clearanceupon β-agonist treatment [16].
Consistent with the idea of β-agonists as potential thera-peutic tools, β-adrenergic agonist treatment improved fluidclearance and edema resolution in experimental modelsof ALI/ARDS [68–71]. The activation of transepithelialNa+ transport and alveolar fluid clearance by β-adrenergicagonists was also shown to reduce extravascular lung waterin patients who were part of the so-called BALTI trial (beta-agonist lung injury trial, BALTI), a clinical trial that addressedthe possibility of β-agonist treatment in ALI/ARDS [72].Recent data also suggest that β-agonist treatment mightrestore Na+ absorption and epithelial Na+ channel activityto normal levels in hypoxic alveolar epithelial cells from rats[73]. Consistently, β-adrenergic agonist inhalation reducedthe incidence of HAPE likely by stimulated fluid absorption[74].
The described studies with β-adrenergic agonists demon-strate that activation of Na+ transport, inter alia by stimulat-ing Na+ channels, might indeed be a promising strategy toimprove edema resolution. Thus, Na+ channels might indeedrepresent molecular targets for the treatment of pulmonaryedema. However, it is important to note that in diseases likeHAPE or ALI/ARDS there are three steps that account forthe development of pulmonary edema: (i) alveolar floodingdue to increased fluid filtration (ii) disturbances in theepithelial barrier integrity, and (iii) impaired fluid clearancedue to impaired transepithelial Na+ transport. Althoughthere are experimental studies demonstrating that edemaformation can be the result of diminished Na+ transportdespite of an intact epithelial barrier [75], especially edemaresolution driven by transepithelial Na+ transport can onlytake place over an intact epithelial barrier. Barrier leakage
is beside impaired Na+ transport a characteristic of HAPE[76] or ALI/ARDS [7]. Whereas damage to the alveolarepithelium is the major cause of barrier disruption inpatients with ALI/ARDS, it is speculated that an impairmentof barrier integrity under HAPE—independently of Na+
channel activity—might be the result of enhanced leakinessof alveolar epithelial tight junctions [77]. Independent ofits cause, barrier damage is an important factor that has tobe carefully taken into consideration [78]. Therefore, Na+
channels cannot be the only molecular target for putativetherapeutic tools regarding the treatment of pulmonaryedema under conditions such as HAPE or ALI/ARDS.Reducing the cause of fluid filtration into the alveoli andrestoring especially the epithelial barrier integrity has to bea prerequisite for enhanced Na+ transport to be effective foredema resolution.
This correlation has already been implicated in the BALTItrial [72]. The reduction of extravascular lung water by β-adrenergic agonist treatment was only apparent 72 h afterthe beginning of treatment [72]. This observation mightdemonstrate that for effective edema resolution to take place,an improvement in barrier integrity is necessary. Followingthat line, there are interesting data suggesting a role of β-adrenergic agonists in stimulating barrier integrity in vitro[79] and in patients with ALI/ARDS [80].
Therefore, future therapeutic strategies to improveedema resolution must focus on (i) a reduction of alveolarflooding, for example, by reduction of hypoxia and pul-monary hypertension (ii) restoration of barrier integrity andfinally (iii) enhancement of transepithelial Na+ transport,for example, by stimulating Na+ channels in the alveolarepithelium.
6. Concluding Remarks
Taken together, Na+ channels in alveolar epithelial cellsrepresent important mediators of alveolar fluid clearance.Understanding the precise structure and regulation of Na+
channels under physiological conditions in the lung as wellas their dysregulation under pathological conditions suchas HAPE or ALI/ARDS is a prerequisite for understandingthe pathogenesis of lung diseases associated with pulmonaryedema and the development of new therapeutic strategies.It is important to point out that Na+ transport mediatedalveolar fluid clearance can only take place across an intactepithelial barrier. Thus, the challenge of future therapeuticapproaches to treat pulmonary edema will be to minimizeedema formation due to barrier damage or increasedfiltration and to enhance edema resolution by stimulatingNa+ transport and, particularly, Na+ channels in the alveolarepithelium.
Acknowledgments
The authors thank Sarah Kessler and Dr. Rory E. Morty(University of Giessen Lung Center, Giessen, Germany) forhelpful comments as well as Kevin D. Urness (University ofEdmonton, Alberta, Canada) and Blake Haller (Hendrix Col-lege, Arkansas, US) for language editing of the manuscript.

6 Pulmonary Medicine
References
[1] L. Dobbs, M. Johnson, J. Vanderbilt, L. Allen, and R.Gonzalez, “The great big alveolar TI cell: evolving conceptsand paradigms,” Cellular Physiology and Biochemistry, vol. 25,no. 1, pp. 55–62, 2010.
[2] M. Althaus, R. E. Morty, W. Clauss, and M. Fronius, “DerEpitheliale Natrium Kanal. 15 Jahre Kanalarbeiten,” Biologiein unserer Zeit, vol. 39, no. 5, pp. 320–326, 2009.
[3] E. Hummler, P. Barker, J. Galzy et al., “Early death due todefective neonatal lung liquid clearance in αENaC-deficientmice,” Nature Genetics, vol. 12, no. 3, pp. 325–328, 1996.
[4] T. Li and H. G. Folkesson, “RNA interference for α-ENaCinhibits rat lung fluid absorption in vivo,” American Journalof Physiology, vol. 290, no. 4, pp. L649–L660, 2006.
[5] D. C. Eaton, MY. N. Helms, M. Koval, F. B. Hui, and L. Jain,“The contribution of epithelial sodium channels to alveolarfunction in health and disease,” Annual Review of Physiology,vol. 71, pp. 403–423, 2009.
[6] S. Matalon, A. Lazrak, L. Jain, and D. C. Eaton, “Invitedreview: biophysical properties of sodium channels in lungalveolar epithelial cells,” Journal of Applied Physiology, vol. 93,no. 5, pp. 1852–1859, 2002.
[7] M. A. Matthay, H. G. Folkesson, and C. Clerici, “Lungepithelial fluid transport and the resolution of pulmonaryedema,” Physiological Reviews, vol. 82, no. 3, pp. 569–600,2002.
[8] M. D. Johnson, H. F. Bao, M. N. Helms et al., “Functional ionchannels in pulmonary alveolar type I cells support a role fortype I cells in lung ion transport,” Proceedings of the NationalAcademy of Sciences of the United States of America, vol. 103,no. 13, pp. 4964–4969, 2006.
[9] M. Althaus, M. Fronius, Y. Buchackert et al., “Carbon monox-ide rapidly impairs alveolar fluid clearance by inhibitingepithelial sodium channels,” American Journal of RespiratoryCell and Molecular Biology, vol. 41, no. 6, pp. 639–650, 2009.
[10] G. Basset, C. Crone, and G. Saumon, “Significance of activeion transport in transalveolar water absorption: a study onisolated rat lung,” Journal of Physiology, vol. 384, pp. 311–324,1987.
[11] Y. Berthiaume, N. C. Staub, and M. A. Matthay, “Beta-adrenergic agonists increase lung liquid clearance in anes-thetized sheep,” Journal of Clinical Investigation, vol. 79, no.2, pp. 335–343, 1987.
[12] H. A. Ghofrani, M. G. Kohstall, N. Weissmann et al., “Alveolarepithelial barrier functions in ventilated perfused rabbitlungs,” American Journal of Physiology, vol. 280, no. 5, pp.L896–L904, 2001.
[13] A. Norlin, N. Finley, P. Abedinpour, and H. G. Folkesson,“Alveolar liquid clearance in the anesthetized ventilated guineapig,” American Journal of Physiology, vol. 274, no. 2, pp. L235–L243, 1998.
[14] M. Egli, H. Duplain, M. Lepori et al., “Defective respi-ratory amiloride-sensitive sodium transport predisposes topulmonary oedema and delays its resolution in mice,” Journalof Physiology, vol. 560, no. 3, pp. 857–865, 2004.
[15] M. Mall, B. R. Grubb, J. R. Harkema, W. K. O’Neal, andR. C. Boucher, “Increased airway epithelial Na+ absorptionproduces cystic fibrosis-like lung disease in mice,” NatureMedicine, vol. 10, no. 5, pp. 487–493, 2004.
[16] N. Randrianarison, C. Clerici, C. Ferreira et al., “Low expres-sion of the β-ENaC subunit impairs lung fluid clearance in themouse,” American Journal of Physiology, vol. 294, no. 3, pp.L409–L416, 2008.
[17] S. G. Brown, M. Gallacher, R. E. Olver, and S. M. Wilson, “Theregulation of selective and nonselective Na+ conductancesin H441 human airway epithelial cells,” American Journal ofPhysiology, vol. 294, no. 5, pp. L942–L954, 2008.
[18] M. T. Clunes, A. G. Butt, and S. M. Wilson, “A glucocorticoid-induced Na+ conductance in human airway epithelial cellsidentified by perforated patch recording,” Journal of Physiol-ogy, vol. 557, no. 3, pp. 809–819, 2004.
[19] S. J. Ramminger, K. Richard, S. K. Inglis, S. C. Land,R. E. Olver, and S. M. Wilson, “A regulated apical Na+
conductance in dexamethasone-treated H441 airway epithelialcells,” American Journal of Physiology, vol. 287, no. 2, pp. L411–L419, 2004.
[20] A. P. Albert, A. M. Woollhead, O. J. Mace, and D. L. Baines,“AICAR decreases the activity of two distinct amiloride-sensitive Na+-permeable channels in H441 human lungepithelial cell monolayers,” American Journal of Physiology, vol.295, no. 5, pp. L837–L848, 2008.
[21] C. M. Canessa, L. Schild, G. Buell et al., “Amiloride-sensitiveepithelial Na+ channel is made of three homologous subunits,”Nature, vol. 367, no. 6462, pp. 463–467, 1994.
[22] J. Jasti, H. Furukawa, E. B. Gonzales, and E. Gouaux,“Structure of acid-sensing ion channel 1 at 1.9 A resolutionand low pH,” Nature, vol. 449, no. 7160, pp. 316–323, 2007.
[23] M. Althaus, A. Pichl, W. G. Clauss et al., “Nitric oxide inhibitshighly selective sodium channels and the Na+/K+-ATPase inH441 cells,” American Journal of Respiratory and Critical CareMedicine, vol. 44, no. 1, pp. 53–65, 2011.
[24] A. Lazrak and S. Matalon, “cAMP-induced changes of apicalmembrane potentials of confluent H441 monolayers,” Ameri-can Journal of Physiology, vol. 285, no. 2, pp. L443–L450, 2003.
[25] O. J. Mace, A. M. Woollhead, and D. L. Baines, “AICARactivates AMPK and alters PIP 2 association with the epithelialsodium channel ENaC to inhibit Na+ transport in H441 lungepithelial cells,” Journal of Physiology, vol. 586, no. 18, pp.4541–4557, 2008.
[26] A. M. Wollhead, J. W. Scott, D. G. Hardie, and D. L. Baines,“Phenformin and 5-aminoimidazole-4-carboxamide-1-β-D-ribofuranoside (AICAR) activation of AMP-activated proteinkinase inhibits transepithelial Na+ transport across H441 lungcells,” Journal of Physiology, vol. 566, no. 3, pp. 781–792, 2005.
[27] L. Jain, XI. J. Chen, B. Malik, O. Al-Khalili, and D. C. Eaton,“Antisense oligonucleotides against the α-subunit of ENaCdecrease lung epithelial cation-channel activity,” AmericanJournal of Physiology, vol. 276, no. 6, pp. L1046–L1051, 1999.
[28] R. Waldmann, G. Champigny, F. Bassilana, N. Voilley, and M.Lazdunski, “Molecular cloning and functional expression ofa novel amiloride-sensitive Na+ channel,” Journal of BiologicalChemistry, vol. 270, no. 46, pp. 27411–27414, 1995.
[29] T. Giraldez, D. Afonso-Oramas, I. Cruz-Muros et al., “Cloningand functional expression of a new epithelial sodium channelδ subunit isoform differentially expressed in neurons of thehuman and monkey telencephalon,” Journal of Neurochem-istry, vol. 102, no. 4, pp. 1304–1315, 2007.
[30] D. Wesch, P. Miranda, D. Afonso-Oramas et al., “Theneuronal-specific SGK1.1 kinase regulates δ-epithelial Na+
channel independently of PY motifs and couples it to phos-pholipase C signaling,” American Journal of Physiology, vol.299, no. 4, pp. C779–C790, 2010.
[31] H.-L. Ji, X.-F. Su, S. Kedar et al., “δ-subunit confers novelbiophysical features to αβγ-human epithelial sodium channel(ENaC) via a physical interaction,” Journal of BiologicalChemistry, vol. 281, no. 12, pp. 8233–8241, 2006.

Pulmonary Medicine 7
[32] H. G. Nie, L. Chen, D. Y. Han et al., “Regulation of epithelialsodium channels by cGMP/PKGII,” Journal of Physiology, vol.587, no. 11, pp. 2663–2676, 2009.
[33] H. O’Brodovich, P. Yang, S. Gandhi, and G. Otulakowski,“Amiloride-insensitive Na+ and fluid absorption in the mam-malian distal lung,” American Journal of Physiology, vol. 294,no. 3, pp. L401–L408, 2008.
[34] Y. Kikkawa and K. Yoneda, “The type II epithelial cell of thelung. I. Method of isolation,” Laboratory Investigation, vol. 30,no. 1, pp. 76–84, 1974.
[35] J. Chen, Z. Chen, T. Narasaraju, N. Jin, and L. Liu, “Isolationof highly pure alveolar epithelial type I and type II cells fromrat lungs,” Laboratory Investigation, vol. 84, no. 6, pp. 727–735,2004.
[36] L. G. Dobbs, R. Gonzalez, M. A. Matthay, E. P. Carter, L.Allen, and A. S. Verkman, “Highly water-permeable type Ialveolar epithelial cells confer high water permeability betweenthe airspace and vasculature in rat lung,” Proceedings of theNational Academy of Sciences of the United States of America,vol. 95, no. 6, pp. 2991–2996, 1998.
[37] Z. Borok, J. M. Liebler, R. L. Lubman et al., “Na transportproteins are expressed by rat alveolar epithelial type I cells,”American Journal of Physiology, vol. 282, no. 4, pp. L599–L608,2002.
[38] M. D. Johnson, J. H. Widdicombe, L. Allen, P. Barbry, and L.G. Dobbs, “Alveolar epithelial I cells contain transport proteinsand transport sodium, supporting an active role for type I cellsin regulation of lung liquid homeostasis,” Proceedings of theNational Academy of Sciences of the United States of America,vol. 99, no. 4, pp. 1966–1971, 2002.
[39] L. Jain, X. J. Chen, S. Ramosevac, L. A. Brown, and D. C. Eaton,“Expression of highly selective sodium channels in alveolartype II cells is determined by culture conditions,” AmericanJournal of Physiology, vol. 280, no. 4, pp. L646–L658, 2001.
[40] M. N. Helms, J. Self, F. B. Hui, L. C. Job, L. Jain, and D.C. Eaton, “Dopamine activates amiloride-sensitive sodiumchannels in alveolar type I cells in lung slice preparations,”American Journal of Physiology, vol. 291, no. 4, pp. L610–L618,2006.
[41] M. N. Helms, L. Jain, J. L. Self, and D. C. Eaton, “Redoxregulation of epithelial sodium channels examined in alveolartype 1 and 2 cells patch-clamped in lung slice tissue,” Journal ofBiological Chemistry, vol. 283, no. 33, pp. 22875–22883, 2008.
[42] U. Scherrer, E. Rexhaj, P. Y. Jayet, Y. Allemann, and C. Sartori,“New insights in the pathogenesis of high-altitude pulmonaryedema,” Progress in Cardiovascular Diseases, vol. 52, no. 6, pp.485–492, 2010.
[43] C. Clerici and M. A. Matthay, “Hypoxia regulates geneexpression of alveolar epithelial transport proteins,” Journal ofApplied Physiology, vol. 88, no. 5, pp. 1890–1896, 2000.
[44] M. Jain and J. I. Sznajder, “Effects of hypoxia on the alveolarepithelium,” Proceedings of the American Thoracic Society, vol.2, no. 3, pp. 202–205, 2005.
[45] C. Planes, M. Blot-Chabaud, M. A. Matthay, S. Couette, T.Uchida, and C. Clerici, “Hypoxia and β-agonists regulate cellsurface expression of the epithelial sodium channel in nativealveolar epithelial cells,” Journal of Biological Chemistry, vol.277, no. 49, pp. 47318–47324, 2002.
[46] C. Planes, B. Escoubet, M. Blot-Chabaud, G. Friedlander, N.Farman, and C. Clerici, “Hypoxia downregulates expressionand activity of epithelial sodium channels in rat alveolarepithelial cells,” American Journal of Respiratory Cell andMolecular Biology, vol. 17, no. 4, pp. 508–518, 1997.
[47] M. L. Vivona, M. Matthay, M. B. Chabaud, G. Friedlander,and C. Clerici, “Hypoxia reduces alveolar epithelial sodiumand fluid transport in rats reversal by β-adrenergic agonisttreatment,” American Journal of Respiratory Cell and MolecularBiology, vol. 25, no. 5, pp. 554–561, 2001.
[48] R. Wodopia, H. S. Ko, J. Billian, R. Wiesner, P. Bartsch, and H.Mairbaurl, “Hypoxia decreases proteins involved in epithelialelectrolyte transport in A549 cells and rat lung,” AmericanJournal of Physiology, vol. 279, no. 6, pp. L1110–L1119, 2000.
[49] R. E. Morty, O. Eickelberg, and W. Seeger, “Alveolar fluidclearance in acute lung injury: what have we learned fromanimal models and clinical studies?” Intensive Care Medicine,vol. 33, no. 7, pp. 1229–1240, 2007.
[50] L. B. Ware and M. A. Matthay, “The acute respiratory distresssyndrome,” The New England Journal of Medicine, vol. 342, no.18, pp. 1334–1349, 2000.
[51] L. B. Ware and M. A. Matthay, “Alveolar fluid clearance isimpaired in the majority of patients with acute lung injuryand the acute respiratory distress syndrome,” American Journalof Respiratory and Critical Care Medicine, vol. 163, no. 6, pp.1376–1383, 2001.
[52] A. Kobayashi, S. Hashimoto, K. Kooguchi et al., “Expressionof inducible nitric oxide synthase and inflammatory cytokinesin alveolar macrophages of ARDS following sepsis,” Chest, vol.113, no. 6, pp. 1632–1639, 1998.
[53] C. Sittipunt, K. P. Steinberg, J. T. Ruzinski et al., “Nitric oxideand nitrotyrosine in the lungs of patients with acute respira-tory distress syndrome,” American Journal of Respiratory andCritical Care Medicine, vol. 163, no. 2, pp. 503–510, 2001.
[54] Y. Guo, M. D. DuVall, J. P. Crow, and S. Matalon, “Nitricoxide inhibits Na+ absorption across cultured alveolar type IImonolayers,” American Journal of Physiology, vol. 274, no. 3,pp. L369–L377, 1998.
[55] L. Jain, XI. J. Chen, L. A. Brown, and D. C. Eaton, “Nitric oxideinhibits lung sodium transport through a cGMP-mediatedinhibition of epithelial cation channels,” American Journal ofPhysiology, vol. 274, no. 4, pp. L475–L484, 1998.
[56] M. Yanagisawa, H. Kurihara, S. Kimura et al., “A novel potentvasoconstrictor peptide produced by vascular endothelialcells,” Nature, vol. 332, no. 6163, pp. 411–415, 1988.
[57] C. Sartori, L. Vollenweider, B. M. Loffler et al., “Exaggeratedendothelin release in high-altitude pulmonary edema,” Circu-lation, vol. 99, no. 20, pp. 2665–2668, 1999.
[58] C. Mitaka, Y. Hirata, T. Nagura, Y. Tsunoda, and K. Amaha,“Circulating endothelin-1 concentrations in acute respiratoryfailure,” Chest, vol. 104, no. 2, pp. 476–480, 1993.
[59] T. S. Pavlov, A. Chahdi, D. V. Ilatovskaya et al., “Endothelin-1 inhibits the epithelial Na+ channel through βPix/14-3-3/Nedd4-2,” Journal of the American Society of Nephrology, vol.21, no. 5, pp. 833–843, 2010.
[60] M. M. Berger, C. S. Rozendal, C. Schieber et al., “The effectof endothelin-1 on alveolar fluid clearance and pulmonaryedema formation in the rat,” Anesthesia and Analgesia, vol.108, no. 1, pp. 225–231, 2009.
[61] J. Roux, H. Kawakatsu, B. Gartland et al., “Interleukin-1βdecreases expression of the epithelial sodium channel α-subunit in alveolar epithelial cells via a p38 MAPK-dependentsignaling pathway,” Journal of Biological Chemistry, vol. 280,no. 19, pp. 18579–18589, 2005.
[62] T. Yamagata, Y. Yamagata, T. Nishimoto et al., “The regulationof amiloride-sensitive epithelial sodium channels by tumornecrosis factor-alpha in injured lungs and alveolar type IIcells,” Respiratory Physiology and Neurobiology, vol. 166, no. 1,pp. 16–23, 2009.

8 Pulmonary Medicine
[63] A. Goolaerts, J. Roux, M. T. Ganter et al., “Serotonin decreasesalveolar epithelial fluid transport via a direct inhibition of theepithelial sodium channel,” American Journal of RespiratoryCell and Molecular Biology, vol. 43, no. 1, pp. 99–108, 2010.
[64] N. Randrianarison, B. Escoubet, C. Ferreira et al., “β-Liddle mutation of the epithelial sodium channel increasesalveolar fluid clearance and reduces the severity of hydrostaticpulmonary oedema in mice,” Journal of Physiology, vol. 582,no. 2, pp. 777–788, 2007.
[65] H. Abriel, J. Loffing, J. F. Rebhun et al., “Defective regulationof the epithelial Na+ channel by Nedd4 in Liddle’s syndrome,”Journal of Clinical Investigation, vol. 103, no. 5, pp. 667–673,1999.
[66] D. Firsov, L. Schild, I. Gautschi, A. M. Merillat, E. Schnee-berger, and B. C. Rossier, “Cell surface expression of theepithelial Na channel and a mutant causing Liddle syndrome:a quantitative approach,” Proceedings of the National Academyof Sciences of the United States of America, vol. 93, no. 26, pp.15370–15375, 1996.
[67] S. Kellenberger and L. Schild, “Epithelial sodium chan-nel/degenerin family of ion channels: a variety of functionsfor a shared structure,” Physiological Reviews, vol. 82, no. 3,pp. 735–767, 2002.
[68] V. Chamorro-Marın, M. Garcıa-Delgado, A. Touma-Fernandez, E. Aguilar-Alonso, and E. Fernandez-Mondejar,“Intratracheal dopamine attenuates pulmonary edema andimproves survival after ventilator-induced lung injury in rats,”Critical Care, vol. 12, no. 2, article R39, 2008.
[69] D. F. McAuley, J. A. Frank, X. Fang, and M. A. Matthay,“Clinically relevant concentrations of β-adrenergic ago-nists stimulate maximal cyclic adenosine monophosphate-dependent airspace fluid clearance and decrease pulmonaryedema in experimental acid-induced lung injury,” CriticalCare Medicine, vol. 32, no. 7, pp. 1470–1476, 2004.
[70] F. J. Saldıas, A. Comellas, K. M. Ridge, E. Lecuona, and J.I. Sznajder, “Isoproterenol improves ability of lung to clearedema in rats exposed to hyperoxia,” Journal of AppliedPhysiology, vol. 87, no. 1, pp. 30–35, 1999.
[71] F. J. Saldıas, E. Lecuona, A. P. Comellas, K. M. Ridge, D.H. Rutschman, and J. I. Sznajder, “β-adrenergic stimulationrestores rat lung ability to clear edema in ventilator-associatedlung injury,” American Journal of Respiratory and Critical CareMedicine, vol. 162, no. 1, pp. 282–287, 2000.
[72] G. D. Perkins, D. F. McAuley, D. R. Thickett, and F. Gao, “Theβ-agonist lung injury trial (BALTI): a randomized placebo-controlled clinical trial,” American Journal of Respiratory andCritical Care Medicine, vol. 173, no. 3, pp. 281–287, 2006.
[73] B. Loeh, E. Baloglu, A. Ke, P. Bartsch, and H. Mairbaurl,“β -adrenergic stimulation blunts inhibition of epithelial iontransport by hypoxia of rat alveolar epithelial cells,” CellularPhysiology and Biochemistry, vol. 25, no. 1, pp. 123–134, 2010.
[74] C. Sartori, Y. Allemann, H. Duplain et al., “Salmeterol forthe prevention of high-altitude pulmonary edema,” The NewEngland Journal of Medicine, vol. 346, no. 21, pp. 1631–1636,2002.
[75] C. Planes, N. H. Randrianarison, R. P. Charles et al., “ENaC-mediated alveolar fluid clearance and lung fluid balancedepend on the channel-activating protease 1,” The EMBOMolecular Medicine, vol. 2, no. 1, pp. 26–37, 2010.
[76] S. Hoschele and H. Mairbaurl, “Alveolar flooding at high alti-tude: failure of reabsorption?” News in Physiological Sciences,vol. 18, no. 2, pp. 55–59, 2003.
[77] R. J. Kaner and R. G. Crystal, “Pathogenesis of high altitudepulmonary edema: does alveolar epithelial lining fluid vascu-lar endothelial growth factor exacerbate capillary leak?” HighAltitude Medicine and Biology, vol. 5, no. 4, pp. 399–409, 2004.
[78] R. Lucas, A. D. Verin, S. M. Black, and J. D. Catravas,“Regulators of endothelial and epithelial barrier integrity andfunction in acute lung injury,” Biochemical Pharmacology, vol.77, no. 12, pp. 1763–1772, 2009.
[79] J. R. Spurzem, J. Gupta, T. Veys, K. R. Kneifl, S. I. Rennard,and T. A. Wyatt, “Activation of protein kinase A acceleratesbovine bronchial epithelial cell migration,” American Journalof Physiology, vol. 282, no. 5, pp. L1108–L1116, 2002.
[80] G. D. Perkins, F. Gao, and D. R. Thickett, “In vivo and in vitroeffects of salbutamol on alveolar epithelial repair in acute lunginjury,” Thorax, vol. 63, no. 3, pp. 215–220, 2008.

Hindawi Publishing CorporationPulmonary MedicineVolume 2011, Article ID 361931, 7 pagesdoi:10.1155/2011/361931
Review Article
The Curious Question of Exercise-Induced Pulmonary Edema
Melissa L. Bates,1 Emily T. Farrell,1 and Marlowe W. Eldridge1, 2
1 Critical Care Division, Department of Pediatrics, The University of Wisconsin, H6/551 600 Highland Avenue, Madison,WI 53792, USA
2 Departments of Biomedical Engineering and Kinesiology, The University of Wisconsin, H6/551 600 Highland Avenue, Madison,WI 53792, USA
Correspondence should be addressed to Melissa L. Bates, [email protected]
Received 16 November 2010; Revised 21 January 2011; Accepted 29 January 2011
Academic Editor: Kazuo Chin
Copyright © 2011 Melissa L. Bates et al. This is an open access article distributed under the Creative Commons AttributionLicense, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properlycited.
The question of whether pulmonary edema develops during exercise on land is controversial. Yet, the development of pulmonaryedema during swimming and diving is well established. This paper addresses the current controversies that exist in the field ofexercise-induced pulmonary edema on land and with water immersion. It also discusses the mechanisms by which pulmonaryedema can develop during land exercise, swimming, and diving and the current gaps in knowledge that exist. Finally, this paperdiscusses how these fields can continue to advance and the areas where clinical knowledge is lacking.
1. The Challenge of Lung Fluid Handlingduring Exercise
During exercise, the transport of oxygen across the pul-monary membrane increases from ∼4 mL/kg/min at restto over 75 mL/kg/min in endurance athletes performingmaximal exercise [1]. A couple of key anatomical andphysiological features allow this almost twentyfold increasein the transport of oxygen from the alveolar region to thecapillary network. The interface between the alveolus andcapillary is exquisitely thin such that the diffusion distancebetween the alveolus and a red blood cell is only 1 μm[2]. The surface area for gas exchange is immense (∼1 ×104 cm2), and the delicate, thin-walled vasculature has thecapacity to be distended and recruited in order to accept a5-fold increase in the cardiac output during exercise. Duringhigh intensity exercise, in the face of increased blood flowand elevated capillary pressures, the lung is faced with thechallenge of keeping the respiratory membrane intact and thealveolar surface dry.
Like in other tissues, fluid flux across the lung vasculatureis thought to be determined by the balance between thevascular hydrostatic and oncotic pressures relative to theinterstitial space. The Starling equation illustrates this as
Jv = Kf ([Pc − Pi]− σ[πc − πi]), (1)
where Jv is the net fluid absorption or filtration from thevasculature, Kf is a filtration coefficient that describes thepermeability of the capillary to fluid and is determinedin part by the capillary surface area, Pc and Pi are thecapillary and interstitial hydrostatic pressures, πc and πiare the capillary and interstitial oncotic pressures, and σis a reflection coefficient that corrects the oncotic pressurefor the permeability of the capillary to large proteins.Considering the variables in the Starling equation, exercise-induced pulmonary edema could occur by the followingmechanisms:
(i) an increase in the capillary hydrostatic pressure,
(ii) an increase in Kf as a result of capillary wall damageor increased capillary surface,
(iii) an inability of the lymphatics to sufficiently clearwater extruded from the vessels.
Although the lung is perfused at much lower pressurescompared to the systemic vasculature (12 versus 120 mmHg,systolic at rest), the lung must still accommodate a morethan doubling of the pulmonary artery driving pressure.This increase in pulmonary artery pressure is largely deter-mined by the increased left atrial pressure that resultsfrom increased venous return to a limited atrial volume.

2 Pulmonary Medicine
Indeed, eighty percent of the increase in pulmonary arterypressure is explained by an increase in left atrial pressure[3]. Elevated pulmonary artery and left atrial pressures,coupled with a decreased intrathoracic pressure duringinspiration, translate to increased capillary transmural pres-sures and the exudation of fluid from the capillary tothe airspace.
In the resting human, fluid transitions from the vascularspace to the interstitium at a rate of 0.3 mL/kg/hr [4] and iscleared by the lymphatic system. Studies in exercising sheepdemonstrate that lung lymphatic flow can increase 7–10-fold. This increase requires hyperpnea to occur and translatesto 150–210 mL/hr of fluid clearance in a 70 kg human [5]. Itwas once thought that the simple negative pressure gradientbetween the lymphatics and the thoracic duct, caused bydecreased thoracic pressure during the inspiratory phaseof exercise hyperpnea, causes the increase in lymph flow.However, the real mechanism of increased lymph flow maybe more elegant. Similar to the systemic veins, the lunglymphatics are valved. Much like skeletal muscle contractionreturns venous blood to the heart through a series of valvedvessels (termed the “skeletal muscle pump”), inspiratory andexpiratory pressure oscillations may serve to pump bloodthrough the pulmonary lymphatics [6–8]. Additionally, thelymphatics may have peristaltic properties. The collectinglymphatics have a smooth muscle layer that can have periodiccontractions, elevating the internal pressure several mmHg[9]. They also have alpha and beta adrenergic receptors,and the application of catecholamines can increase thelymphatic pressure to 20–30 mmHg [10, 11]. Circulatingcatecholamines are increased with exercise [12] and mayplay a role in lymphatic function. However, their effect onlymphatic flow is not known.
2. Does Exercise-Induced PulmonaryEdema Exist?
The question of whether pulmonary edema develops duringexercise is controversial. Systematic experimental attempts todocument postexercise pulmonary edema yield conflictingdata, but several clinical case reports exist in the literature.Clinically relevant edema has been reported in an elitecyclist participating in a transcontinental race [10], threerunners participating in marathon and ultramarathon races[13, 14], and in a single individual after cross-country skiingin the cold [15]. In a single case report, an apparentlyhealthy man developed pulmonary edema after exercise[16]. Interestingly, a clinical examination revealed mitralvalve prolapsed, and the authors suggest that this structuralabnormality likely contributed to the edema formation.There may be a role for unrecognized valve dysfunctionin other cases. Indeed, in patients with left ventricularsystolic dysfunction, mitral valve dysfunction is associatedwith increased pulmonary vascular pressure, capillary barrierdisruption, and exercise-induced pulmonary edema [17]. Todate, there have been no comprehensive studies quantifyingthe annual incidence of postexercise pulmonary edema inindividuals with and without previously identified cardiacabnormalities.
The impetus to suspect a high prevalence of subclinicalinterstitial edema postexercise comes primarily from dataobtained using the multiple inert gas elimination technique(MIGET). The MIGET quantifies the degree to whichventilation and perfusion in the lung are well matched (V/Q)[18, 19]. V/Q mismatch increases with moderate to heavyexercise and persists even after exercise termination andthe return to baseline cardiopulmonary function [20, 21].Hopkins has proposed that the “most plausible” explanationfor this is the formation of interstitial pulmonary edema,causing peribronchial and perivascular cuffing.
Several of the case reports mentioned in this paper pointto exercise-induced pulmonary edema as a cause of exercise-induced arterial hypoxemia, which occurs in at least 50%of healthy individuals exercising at sea level [22]. In thesereports, where clinical signs of alveolar flooding were noted,hypoxemia is probably the result of edema. However, in mostexercising individuals, the issue is less clear. V/Q mismatch,the major piece of evidence for exercise-induced pulmonaryedema, is probably a minimal contributor to gas exchangedeficits. The proportion of the alveolar-arterial oxygendifference explained by V/Q mismatch does not change fromrest to heavy exercise [23], leaving diffusion limitation andright-to-left shunt as the remaining possible culprits [23, 24].Indeed, the increase in V/Q mismatch does not impact gasexchange because the increase in ventilation exceeds thatof perfusion, resulting in few very low V/Q compartments.Hopkins suggests that the reason gas exchange abnormalitiesare not predicted by V/Q mismatch is because interstitialand peribronchial edema does not progress to the point ofalveolar edema and flooding in most individuals [25].
The limitation of translating V/Q measurements fromthe realm of explanation to causation is that the V/Qabnormalities measured by MIGET have never been relatedto direct measures of pulmonary edema in the same indi-viduals postexercise. A recent study used a rapid infusion ofsaline (20 mL/kg) to increase interstitial lung water withoutelevating cardiac output. Although an increase in lungwater was verified by impedence cardiography, there was noevidence of V/Q mismatch [26]. Importantly, there was noevidence of change in the index of ventilation distribution(LogSDV and the mean of V) despite changes in spirometricmeasurements consistent with the development of interstitialedema. In a study of subjects with a history of high altitudepulmonary edema (HAPE), V/Q mismatch with exerciseat 3,800 m was no different than controls with no historyof HAPE. Additional resting V/Q inequality has only beenobserved in participants of Operation Everest II at simulatedaltitudes ≥20,000 ft [27]. Finally, performing repeated boutsof exercise, an activity that would be expected to successivelycompound interstitial edema, does not increase V/Q mis-match [28].
Several studies have relied on the use of direct imagingmodalities (MRI, CT, etc.) and thoracic impedance todemonstrate pulmonary edema postexercise with mixedresults. Some studies using CT and MRI have found evidenceof increased lung water after sustained, heavy exercise [29,30], but these findings have not been consistently replicated.There are several potential pitfalls to using imaging and

Pulmonary Medicine 3
thoracic impedance to measure exercise-induced edema.Both can be confounded by the increase in total thoracicwater caused by the increased blood volume in the lungimmediately postexercise. Magnetic resonance and CT imag-ing require a change in posture which alters the distributionof blood flow and may confound the ability to visualizeedema. Additionally, MRI is time consuming; during thetime required to complete the imaging, low level edemamay resolve. Computed tomography can be impractical touse in research studies because of risks associated with X-ray radiation exposure [31]. Finally, some have argued thatdirect imaging is not sensitive enough to visualize interstitialedema; in order to visualize edema, it must have progressedto the point of alveolar flooding [25]. Certainly, overtalveolar flooding with exercise is rare. The major challenge todemonstrating subclinical pulmonary edema lies in the lackof a reliable, sensitive, gold standard measurement.
The best evidence for exercise-induced pulmonaryedema comes from studies looking for capillary stressfailure in postexercise bronchalveolar lavage fluid (BALF).Pulmonary capillary stress failure and hemorrhage are esti-mated to occur at capillary transmural pressures ≥40 mmHg[32]. Capillary stress failure and frank alveolar bleedinghave been well documented in exercising thoroughbredrace horses, which can achieve estimated capillary pressures≥100 mmHg [33, 34]. Eldridge et al. found evidence ofcapillary disruption in athletes after three short bouts ofintense sea level and high altitude exercise by examiningthe BALF for the presence of red blood cells [35]. Red cellswere found in all athletes’ BALF postexercise, but not in theBALF of resting controls. Although the BALF of each athletewas positive for red cells, the number of red cells found(5.4 × 104/mL) was orders of magnitude lower than thosefound in humans with a clinical diagnosis of high altitudepulmonary edema (2.6 × 106/mL) or exercising horses (30–60× 106/mL) [36, 37]. Still, these data provide evidence thatthe respiratory membrane is disrupted with intense exercisein healthy, active adults.
The lesson learned from many of these studies is thatthe normal lung appears well designed for sea-level exercise.In most individuals, water exudation into the interstitium isbalanced by an increase in lymph flow, preventing the devel-opment of clinical pulmonary edema marked by dyspnea,end expiratory crackles, and the production of bloody, frothysputum. Despite the case reports that exist in the literature,the development of clinically important pulmonary edemawith exercise remains a rare event. It has been suggestedthat the rare individuals who do develop exercise-inducedpulmonary edema had an unknown underlying pathologythat made them more likely to develop pulmonary edemawith exertion [38].
3. What Can We Learn from ImmersionPulmonary Edema?
Exercise in water places a unique set of stresses on the res-piratory system. Immersion pulmonary edema with breath-hold diving, SCUBA diving, and cold water exercise has beenwell documented in the literature [39–41]. In a survey of 460
active SCUBA divers, 1.1% had a history consistent with thedevelopment of immersion pulmonary edema [42]. A surveyof triathletes from the group USA Triathlon revealed that1.4% of the members had symptoms suggestive of pul-monary edema after completing an event that containeda swimming component [43] In 2009, the ProfessionalAssociation of Diving Instructors reported that 900,000 newdiving certifications are issued by its members each year [44].If 1% of the population experiences immersion pulmonaryedema, then 900,000 new divers per year translates to 9,000new individuals at risk for immersion pulmonary edema.
Different populations seem to be at risk for the devel-opment of immersion edema, depending on the type ofimmersion activity. Cases in athletes swimming at the surfacetend to occur in young, fit individuals performing intenseexercise. The maneuvers performed by elite breath-holdand military divers make them susceptible to pulmonarybarotrauma and alveolar hemorrhage. Some have speculatedthat SCUBA divers, some of whom tend to be older, mayhave undiagnosed left ventricular dysfunction that wouldcontribute to the development of edema [45]. However,SCUBA divers are subjected to many of the same stressorsas breath-hold divers and surface swimmers and their edemamay not depend entirely upon pre-existing cardiovascularpathology. The cause of immersion pulmonary edema isprobably multifactorial.
Immersion in upright, seated research participants redi-rects ∼0.7 L of blood to the thorax and increases pul-monary artery systolic pressure [46]. This is augmentedby immersion in cold water, which redirects blood flowto the thorax in order to preserve body temperature, andcaused by vasoconstriction in the trunk and extremities [47].Exercise further increases thoracic blood volume and leftatrial, pulmonary artery, and capillary pressures, althoughthere is substantial variability in pulmonary artery pressurewith immersion exercise. Peacher et al. found a large degreeof intersubject variability in pulmonary artery pressurewith surface immersion exercise (16.0–39.6 mmHg) [48],although the rise in pulmonary artery pressure was higherthan what is typically observed during land exercise [49].These investigators speculated that this high variability mayexplain why some individuals are more susceptible to edemaformation than others when performing the same activity.For example, in a case report of 30 Israeli soldiers performinga 2.4 km open water time trial, 8/30 developed overt edemamarked by frothy sputum, dyspnea, and hemoptysis [50].There is debate as to whether pulmonary artery pressurecontinues to rise during exercise as conflicting studies haveshown it to both increase and decrease with increasingexercise duration [47, 48].
The addition of diving further increases blood redirec-tion to the thorax in order to combat the effect of theincreased pressure on lung volume. As predicted by Boyle’sLaw, the barometric pressure rises during descent, while thelung volume shrinks. Blood is redirected from the peripheryto the thorax [51]. This increases the vascular hydrostaticpressure and counteracts the increased airway pressures.Ferrigno and Lundgren predict that the effects of “lungsqueeze” during a breath-hold dive would be sufficient to

4 Pulmonary Medicine
elevate the capillary hydrostatic pressure 11–32 mmHg [52].These pressures, certainly beyond the 40 mmHg needed todisrupt capillary integrity, are sufficient to cause edema givenlong enough exposure.
Ventilation may also contribute to the formation ofedema, although knowledge in this area is limited. There areno direct studies of the importance of ventilation in edemaformation, and most of what is known is inferred from otherareas. For example, hyperventilation is required to increasefluid clearance by the lymphatics [5]. With high intensityexercise, minute ventilation tends to be lower during proneswimming compared to treadmill running, and the abilityto increase minute ventilation is limited by the need tocoordinate breathing with swimming stroke [53]. This maylimit the lymphatics’ ability to clear fluid. Submersion to theneck causes a 3-fold decline in the expiratory reserve volumeand, as a result, low lung volume breathing [54]. Hydrostaticcompression of the thorax increases inspiratory resistance[55] and decreases maximum expiratory flow rates at lungvolumes <60% of total lung capacity [56]. The additionof a regulator during SCUBA diving can further increasethe respiratory effort needed to overcome the regulator’sresistance by >20 cm H2O [57]. These limitations demandan increase in the work of breathing, and the enhancednegative intrathoracic pressure during inhalation supportsfluid filtration and edema formation.
Finally, glottal closure or SCUBA regulator failure maycontribute to edema formation. In a study of seven men sub-mersed supine in only 1 ft of water while breathing througha rigid metal tube, three of the men terminated the studywithin the first 30 seconds of the initial submersion [54]with the complaint that the breathing tube was obstructed. Itwas later discovered that they were experiencing involuntaryglottal closure, which could be overcome by not attempt-ing to inhale during the first 15 seconds of submersion.Similar to the development of flash pulmonary edema inpatients with laryngospasm or upper airway obstruction[58, 59], breathing against an involuntarily closed glottisor a malfunctioning SCUBA regulator may generate largenegative intrathoracic pressures and disrupt the integrity ofthe respiratory membrane.
4. What Gaps Still Exist in Our Knowledge?
Collaboration with investigators studying immersion pul-monary edema may provide new abilities to answer thequestion of whether subclinical pulmonary edema forms inathletes ubiquitously with intense, land exercise. The majorobstacle limiting our ability to more definitively answer thequestion using current approaches is the lack of a sufficientlysensitive method of detection. Certainly, if edema forms inthe most exercising individuals on land, it is subclinical. Untila more sensitive detection method is developed, evidence forand against the formation of edema with land exercise willcontinue to be met with skepticism.
It is surprising that the rapid infusion of saline doesnot produce V/Q inequality, considering that spirometricmeasurements of midexpiratory flow are altered in a mannerconsistent with interstitial edema [26]. It is possible that
the edema affects the lung uniformly, but it is also pos-sible that the MIGET measurement is not able to detectpulmonary edema with sufficient sensitivity. Nonetheless,we know that edema develops in a substantial fraction ofdivers performing water exercise. Several recent studies havebeen conducted in which invasive pulmonary hemodynamicmeasurements were made in human research participantsperforming hyperbaric water exercise [47, 48], offeringinsight into the mechanism of edema formation duringsubmersion. Pulmonary edema has been observed in thelaboratory in humans performing immersion exercise andhas been verified by observing blood in the conductingairways below the vocal cords [39]. To determine whetherMIGET is able to quantify V/Q inequality in patientswith pulmonary edema, it would be valuable to makemeasurements in patients with varying degrees of activeedema, which could be generated in the laboratory withimmersion exercise. MIGET measurements have been madein immersion [60], but not in individuals with immersionpulmonary edema.
While immersion pulmonary edema is currently a veryexciting and active field of research, investigators studyingimmersion pulmonary edema have inferred that elevationsin pulmonary artery and left atrial pressure must be themajor cause of immersion pulmonary edema. Yet, they havenot directly linked hemodynamic measures to quantifiededema formation. It is important that future mechanisticstudies include a quantitative measurement of edema for-mation to truly define the importance of any mechanism.Because immersion pulmonary edema is more overt, it maybe possible to quantify it using magnetic resonance imaging.The development of comprehensive mathematical modelsusing data from research participants with immersion pul-monary edema may be able to be extrapolated to predict theedema formation that would occur with land exercise.
Another opportunity to advance both fields may lie ina return to the use of animal models. The majority ofmeasurements using MIGET have been made in exercisinghuman research participants. However, Hopkins et al. pre-viously established the Yucatan miniswine as a valid modelfor the investigation of V/Q mismatch with exercise [61].Like humans, the miniswine develops reproducible V/Qinequality with exercise. A simple, but useful, question to askwould be if the V/Q inequality in the miniswine is associatedwith an increase in lung water by simple assessment ofthe lung’s wet to dry weight in exercising and nonexercis-ing animals. V/Q measurements could also be related tointerstitial thickness and other morphometric measurementswith and without exercise. Since pigs have been describedas developing perivascular edema with intense exercise,it is conceivable that there might be a relation betweenMIGET measurements and histological findings [62] in theminiswine.
Studies of immersion edema in humans have recentlyfocused on hemodynamic measurements, although there islittle data regarding changes in the other Starling forces.Hyperbaric hyperoxia without immersion or exercise induceslung function changes consistent with edema formation[63]. How, for example, do the gas mixtures breathed

Pulmonary Medicine 5
by divers affect fluid filtration? We know little about theeffect of immersion exercise on the reflection and filtrationcoefficients and less about the degree to which the lymphaticsmay be overwhelmed by fluid filtration during immersionexercise. Studies conducted using an exercising sheep modelreveal the importance of the lymphatics in keeping theairspaces dry on land, although we still know very little abouthow they are regulated on land and in water. We know thatadrenergic stimulation has the ability to increase pressurewithin the lymphatics by 30 mmHg, but we have littleinsight into how adrenergic mediators affect fluid clearanceby the lymphatics. We also do not know how the changesin pulmonary mechanics and ventilation with immersionaffect lymphatic function. Isolated lung and intact, largeanimals could be used to investigate the importance of thefiltration and reflection coefficients and the regulation of thelymphatics.
5. Why Is It Important Clinically to StudyExercise-Induced Pulmonary Edema?
Each of these smaller gaps in our knowledge contributes toa larger gap; we have no real comprehensive mathematicalmodels of fluid handling during exercise or understandingof the risk factors for the development of exercise-inducedpulmonary edema. For example, we know that sex, smalllung volume, low basal nitric oxide production, geneticsusceptibility (specifically polymorphisms in the angiotensinconverting enzyme gene), and a decreased hypoxic venti-latory response predispose individuals to exercise-inducedpulmonary edema at altitude [35, 64–69], but we do notknow the risk factors associated with land or immersion exer-cise. Mathematical models are valuable both to understandhow fluid balance is maintained in the healthy lung, andalso to predict fluid shifts in patients with cardiopulmonarypathology. Some have speculated that the rare patientswho develop pulmonary edema with exercise on land musthave some previously undetected left heart dysfunction[38]. Considering the association between heart failureand pulmonary edema, surely these patients would havewarranted examination by echocardiography. How subtlemust that dysfunction be to result in edema with exercise andwhy was it not detected when these patients presented withpulmonary edema?
Water exercise is widely recommended for the elderlyand patients with heart failure and systemic hypertensionbecause of its low impact nature and the ability to tailoraquatic exercise to accommodate different fitness levels [70–72]. Yet we know nothing of the effect of immersion andexercise on lung fluid balance in these populations. Couldlow intensity water exercise contribute to edema formationin these groups? More studies are needed to begin to answerthese questions.
References
[1] L. Hermansen, B. Ekblom, and B. Saltin, “Cardiac output dur-ing submaximal and maximal treadmill and bicycle exercise,”Journal of Applied Physiology, vol. 29, no. 1, pp. 82–86, 1970.
[2] E. R. Weibel, Morphometry of the Human Lung, AcademicPress, New York, NY, USA, 1963.
[3] J. T. Reeves and A. E. Taylor, “Pulmonary hemodynamics andfluid exchange in the lungs during exercise,” in Handbook ofPhysiology: Section 12: Exercise: Regulation and Integration ofMultiple Systems, L. B. Rowell and J. T. Shepherd, Eds., pp.585–613, The American Physiological Society, 1996.
[4] J. West, Respiratory Physiology: The Essentials, LippincottWilliams & Wilkins, 2008.
[5] T. Koizumi, R. J. Roselli, R. E. Parker, C. I. Hermo-Weiler, M.Banerjee, and J. H. Newman, “Clearance of filtered fluid fromthe lung during exercise: role of hyperpnea,” American Journalof Respiratory and Critical Care Medicine, vol. 163, no. 3, pp.614–618, 2001.
[6] R. E. Drake, D. K. Adcock, R. L. Scott, and J. C. Gabel,“Effect of outflow pressure upon lymph flow from dog lungs,”Circulation Research, vol. 50, no. 6, pp. 865–869, 1982.
[7] J. C. Parker and A. E. Taylor, “Comparison of capsular andintra-alveolar fluid pressures in the lung,” Journal of AppliedPhysiology Respiratory Environmental and Exercise Physiology,vol. 52, no. 6, pp. 1444–1452, 1982.
[8] R. E. Parker, R. J. Roselli, and K. L. Brigham, “Effectsof prolonged elevated microvascular pressure on lung fluidbalance in sheep,” Journal of Applied Physiology, vol. 58, no.3, pp. 869–875, 1985.
[9] G. Schmid-Schonbein and B. Zweifach, “Fluid pump mecha-nisms in initial lymphatics,” News in Physiological Sciences, vol.9, pp. 67–71, 1994.
[10] A. M. Luks, H. T. Robertson, and E. R. Swenson, “Anultracyclist with pulmonary edema during the Bicycle RaceAcross America,” Medicine and Science in Sports and Exercise,vol. 39, no. 1, pp. 8–12, 2007.
[11] T. Ohhashi, Y. Kawai, and T. Azuma, “The response oflymphatic smooth muscles to vasoactive substances,” PflugersArchiv European Journal of Physiology, vol. 375, no. 2, pp. 183–188, 1978.
[12] M. H. Irving, B. J. Britton, W. G. Wood, C. Padgham, andM. Carruthe, “Effect of β adrenergic blockade on plasmacatecholamines in exercise,” Nature, vol. 248, no. 5448, pp.531–533, 1974.
[13] A. J. Ghio, C. Ghio, and M. Bassett, “Exercise-inducedpulmonary hemorrhage after running a marathon,” Lung, vol.184, no. 6, pp. 331–333, 2006.
[14] J. K. McKechnie, W. P. Leary, and T. D. Noakes, “Acutepulmonary oedema in two athletes during a 90-km runningrace,” South African Medical Journal, vol. 56, no. 7, pp. 261–265, 1979.
[15] P. T. Wilmshurst, “Pulmonary oedema induced by emotionalstress, by sexual intercourse, and by exertion in a coldenvironment in people without evidence of heart disease,”Heart, vol. 90, no. 7, pp. 806–807, 2004.
[16] F. H. Zimmerman and A. H. Mogtader, “Ruptured chordaetendineae and acute pulmonary edema induced by exercise.Occurrence in a young man with mitral valve prolapse,”Journal of the American Medical Association, vol. 258, no. 6,pp. 812–813, 1987.
[17] L. A. Pierard and P. Lancellotti, “The role of ischemic mitralregurgitation in the pathogenesis of acute pulmonary Edema,”New England Journal of Medicine, vol. 351, no. 16, pp. 1627–1634, 2004.
[18] P. D. Wagner, “Estimation of distributions of ventila-tion/perfusion ratios,” Annals of Biomedical Engineering, vol.9, no. 5-6, pp. 543–556, 1981.

6 Pulmonary Medicine
[19] P. D. Wagner, “The multiple inert gas elimination technique(MIGET),” Intensive Care Medicine, vol. 34, no. 6, pp. 994–1001, 2008.
[20] S. R. Hopkins, “Exercise induced arterial hypoxemia: the roleof ventilation-perfusion inequality and pulmonary diffusionlimitation,” in Hypoxia and Exercise, R. C. Roach, P. D. Wagner,and P. H. Hackett, Eds., pp. 17–30, 2006.
[21] S. R. Hopkins, D. C. McKenzie, R. B. Schoene, R. W. Glenny,and H. T. Robertson, “Pulmonary gas exchange duringexercise in athletes I. Ventilation-perfusion mismatch anddiffusion limitation,” Journal of Applied Physiology, vol. 77, no.2, pp. 912–917, 1994.
[22] J. A. Dempsey and P. D. Wagner, “Exercise-induced arterialhypoxemia,” Journal of Applied Physiology, vol. 87, no. 6, pp.1997–2006, 1999.
[23] P. D. Wagner, G. E. Gale, R. E. Moon, J. R. Torre-Bueno, B.W. Stolp, and H. A. Saltzman, “Pulmonary gas exchange inhumans exercising at sea level and simulated altitude,” Journalof Applied Physiology, vol. 61, no. 1, pp. 260–270, 1986.
[24] A. T. Lovering, L. M. Romer, H. C. Haverkamp, D. F. Pegelow,J. S. Hokanson, and M. W. Eldridge, “Intrapulmonaryshunting and pulmonary gas exchange during normoxicand hypoxic exercise in healthy humans,” Journal of AppliedPhysiology, vol. 104, no. 5, pp. 1418–1425, 2008.
[25] S. R. Hopkins, “Point: pulmonary edema does occur inhuman athletes performing heavy sea-level exercise,” Journalof Applied Physiology, vol. 109, pp. 1270–1272, 2010.
[26] G. K. Prisk, I. M. Olfert, T. J. Arai, P. D. Wagner, and S. R.Hopkins, “Rapid intravenous infusion of 20 ml/kg saline doesnot impair resting pulmonary gas exchange in the healthyhuman lung,” Journal of Applied Physiology, vol. 108, no. 1, pp.53–59, 2010.
[27] P. D. Wagner, J. R. sutton, J. T. Reeves, A. Cymerman, B.M. Groves, and M. K. Malconian, “Operation Everest II:pulmonary gas exchange during a simulated ascent of Mt.Everest,” Journal of Applied Physiology, vol. 63, no. 6, pp. 2348–2359, 1987.
[28] C. M. St. Croix, C. A. Harms, S. R. McClaran et al., “Effectsof prior exercise on exercise-induced arterial hypoxemia inyoung women,” Journal of Applied Physiology, vol. 85, no. 4,pp. 1556–1563, 1998.
[29] C. Caillaud, O. Serre-Cousine, F. Anselme, X. Capdevilla,and C. Prefaut, “Computerized tomography and pulmonarydiffusing capacity in highly trained athletes after performinga triathlon,” Journal of Applied Physiology, vol. 79, no. 4, pp.1226–1232, 1995.
[30] D. C. McKenzie, T. J. O’Hare, and J. Mayo, “The effect ofsustained heavy exercise on the development of pulmonaryedema in trained male cyclists,” Respiratory Physiology andNeurobiology, vol. 145, no. 2-3, pp. 209–218, 2005.
[31] W. A. Sheel and D. C. McKenzie, “Counterpoint: pulmonaryedema does not occur in human athletes performing heavysea-level exercise,” Journal of Applied Physiology, vol. 109, no.4, pp. 1272–1273, 2010.
[32] J. B. West, K. Tsukimoto, O. Mathieu-Costello, and R.Prediletto, “Stress failure in pulmonary capillaries,” Journal ofApplied Physiology, vol. 70, no. 4, pp. 1731–1742, 1991.
[33] M. Manohar, E. Coney, and E. Hutchens, “Pulmonary vascularpressure in near-maximally exercised horses,” Equine Practice,vol. 15, pp. 16–21, 1993.
[34] M. Manohar, T. E. Goetz, E. Hutchens, and E. Coney,“Effects of graded-exercise on pulmonary AND systemichemodynamics in horses,” Equine Practice, vol. 17, pp. 17–23,1995.
[35] M. W. Eldridge, R. K. Braun, K. Y. Yoneda, and W. F.Walby, “Effects of altitude and exercise on pulmonary capillaryintegrity: evidence for subclinical high-altitude pulmonaryedema,” Journal of Applied Physiology, vol. 100, no. 3, pp. 972–980, 2006.
[36] D. C. Poole, C. A. Kindig, G. Fenton, L. Ferguson, B. R. Rush,and H. H. Erickson, “Effects of external nasal support onpulmonary gas exchange and EIPH in the horse,” Journal ofEquine Veterinary Science, vol. 20, no. 9, pp. 579–585, 2000.
[37] R. B. Schoene, P. H. Hackett, W. R. Henderson et al., “High-altitude pulmonary edema: characteristics of lung lavagefluid,” Journal of the American Medical Association, vol. 256,no. 1, pp. 63–69, 1986.
[38] S. R. Hopkins, “Last word on point: counterpoint: pulmonaryedema does occur in human athletes performing heavy sea-level exercise,” Journal of Applied Physiology, vol. 109, no. 4, p.1281, 2010.
[39] P. Lindholm, A. Ekborn, D. Oberg, and M. Gennser, “Pul-monary edema and hemoptysis after breath-hold diving atresidual volume,” Journal of Applied Physiology, vol. 104, no.4, pp. 912–917, 2008.
[40] J. B. Slade, T. Hattori, C. S. Ray, A. A. Bove, and P. Cianci,“Pulmonary edema associated with scuba diving: case reportsand review,” Chest, vol. 120, no. 5, pp. 1686–1694, 2001.
[41] P. T. Wilmshurst, A. Crowther, M. Nuri, and M. M. Webb-Peploe, “Cold-induced pulmonary oedema in scuba diversand swimmers and subsequent development of hypertension,”Lancet, vol. 1, no. 8629, pp. 62–65, 1989.
[42] M. Pons, D. Blickenstorfer, E. Oechslin et al., “Pulmonaryoedema in healthy persons during scuba-diving and swim-ming,” European Respiratory Journal, vol. 8, no. 5, pp. 762–767,1995.
[43] C. C. Miller III, K. Calder-Becker, and F. Modave, “Swimming-induced pulmonary edema in triathletes,” American Journal ofEmergency Medicine, vol. 28, no. 8, pp. 941–946, 2010.
[44] PADI Statistics, “Professional, Association, of, Diving, andInstructors,” November 2010, http://www.padi.com/scuba/uploadedFiles/About PADI/PADI Statistics/padi%20statistics%20jun2010.pdf.
[45] C. Edmonds, “Scuba divers’ pulmonary oedema. A review,”Diving and Hyperbaric Medicine, vol. 39, no. 4, pp. 226–231,2009.
[46] R. Begin, M. Epstein, M. A. Sackner, R. Levinson, R.Dougherty, and D. Duncan, “Effects of water immersion tothe neck on pulmonary circulation and tissue volume in man,”Journal of Applied Physiology, vol. 40, no. 3, pp. 293–299, 1976.
[47] T. E. Wester, A. D. Cherry, N. W. Pollock et al., “Effects of headand body cooling on hemodynamics during immersed proneexercise at 1 ATA,” Journal of Applied Physiology, vol. 106, no.2, pp. 691–700, 2009.
[48] D. F. Peacher, S. R. H. Pecorella, J. J. Freiberger et al., “Effectsof hyperoxia on ventilation and pulmonary hemodynamicsduring immersed prone exercise at 4.7 ATA: possible impli-cations for immersion pulmonary edema,” Journal of AppliedPhysiology, vol. 109, no. 1, pp. 68–78, 2010.
[49] N. B. Slonim, A. Ravin, O. J. Balchum, and S. H. Dressler, “Theeffect of mild exercise in the supine position on the pulmonaryarterial pressure of five normal human subjects 1,” The Journalof Clinical Investigation, vol. 33, pp. 1022–1030, 1954.
[50] D. Weiler-Ravell, A. Shupak, I. Goldenberg et al., “Pulmonaryoedema and haemoptysis induced by strenuous swimming,”British Medical Journal, vol. 311, no. 7001, pp. 361–362, 1995.
[51] G. O. Dahlback, E. Jonsson, and M. H. Liner, “Influence ofhydrostatic compression of the chest and intrathoracic blood

Pulmonary Medicine 7
pooling on static lung mechanics during head out immersion,”Undersea Biomedical Research, vol. 5, no. 1, pp. 71–85, 1978.
[52] M. Ferrigno and C. Lundgren, “Human breath-hold diving,”in The Lung at Depth, C. Lundgren and J. Miller, Eds., pp. 529–585, Dekker, New York, NY, USA, 1999.
[53] W. D. McArdle, R. M. Glaser, and J. R. Magel, “Metabolicand cardiorespiratory response during free swimming andtreadmill walking,” Journal of Applied Physiology, vol. 30, no.5, pp. 733–738, 1971.
[54] S. K. Hong, E. Y. Ting, and H. Rahn, “Lung volumes atdifferent depths of submersion,” Journal of Applied Physiology,vol. 15, pp. 550–553, 1960.
[55] A. D. Ray, D. R. Pendergast, and C. E. G. Lundgren,“Respiratory muscle training reduces the work of breathing atdepth,” European Journal of Applied Physiology, vol. 108, no. 4,pp. 811–820, 2010.
[56] C. Prefaut, E. Lupi, and N. R. Anthonisen, “Human lungmechanics during water immersion,” Journal of Applied Physi-ology, vol. 40, no. 3, pp. 320–323, 1976.
[57] J. Clarke and M. Rainone, “Evaluation of the scubapro MK10and MK20 SCUBA regulators for use in cold water,” Tech. Rep.Report NEDU TR No. 1-96), Command NSS, Panama City,Fla, USA, 1996.
[58] P. S. L. Da Silva, H. M. Neto, M. M. Takeuchi Andrade, andC. V. De Mattos Neves, “Negative-pressure pulmonary edema:a rare complication of upper airway obstruction in children,”Pediatric Emergency Care, vol. 21, no. 11, pp. 751–754, 2005.
[59] J. P. Guinard, “Laryngospasm-induced pulmonary edema,”International Journal of Pediatric Otorhinolaryngology, vol. 20,no. 2, pp. 163–168, 1990.
[60] T. Derion, H. J. B. Guy, K. Tsukimoto et al., “Ventilation-perfusion relationships in the lung during head-out waterimmersion,” Journal of Applied Physiology, vol. 72, no. 1, pp.64–72, 1992.
[61] S. R. Hopkins, C. M. Stary, E. Falor, H. Wagner, P. D.Wagner, and M. D. McKirnan, “Pulmonary gas exchangeduring exercise in pigs,” Journal of Applied Physiology, vol. 86,no. 1, pp. 93–100, 1999.
[62] W. Schaffartzik, J. Arcos, K. Tsukimoto, O. Mathieu-Costello,and P. D. Wagner, “Pulmonary interstitial edema in the pigafter heavy exercise,” Journal of Applied Physiology, vol. 75, no.6, pp. 2535–2540, 1993.
[63] J. M. Clark, C. J. Lambertsen, R. Gelfand et al., “Effectsof prolonged oxygen exposure at 1.5, 2.0, or 2.5 ATA onpulmonary function in men (Predictive Studies V),” Journalof Applied Physiology, vol. 86, no. 1, pp. 243–259, 1999.
[64] P. Bartsch, H. Mairbaurl, M. Maggiorini, and E. R. Swenson,“Physiological aspects of high-altitude pulmonary edema,”Journal of Applied Physiology, vol. 98, no. 3, pp. 1101–1110,2005.
[65] T. Busch, P. Bartsch, D. Pappert et al., “Hypoxia decreasesexhaled nitric oxide in mountaineers susceptible to high-altitude pulmonary edema,” American Journal of Respiratoryand Critical Care Medicine, vol. 163, no. 2, pp. 368–373, 2001.
[66] P. H. Hackett, R. C. Roach, R. B. Schoene, G. L. Harrison,and W. J. Mills Jr., “Abnormal control of ventilation in high-altitude pulmonary edema,” Journal of Applied Physiology, vol.64, no. 3, pp. 1268–1272, 1988.
[67] H. N. Hultgren, B. Honigman, K. Theis, and D. Nicholas,“High-altitude pulmonary edema at a ski resort,” WesternJournal of Medicine, vol. 164, no. 3, pp. 222–227, 1996.
[68] D. R. Woods and H. E. Montgomery, “Angiotensin-convertingenzyme and genetics at high altitude,” High Altitude Medicineand Biology, vol. 2, no. 2, pp. 201–210, 2001.
[69] D. R. Woods, A. J. Pollard, D. J. Collier et al., “Inser-tion/deletion polymorphism of the angiotensin I-convertingenzyme gene and arterial oxygen saturation at high altitude,”American Journal of Respiratory and Critical Care Medicine,vol. 166, no. 3, pp. 362–366, 2002.
[70] K. L. Cox, V. Burke, L. J. Beilin, J. R. Grove, B. A. Blanksby,and I. B. Puddey, “Blood pressure rise with swimming versuswalking in older women: the sedentary women exerciseadherence trial 2 (SWEAT 2),” Journal of Hypertension, vol. 24,no. 2, pp. 307–314, 2006.
[71] K. Meyer and J. Bucking, “Aqua exercises and swimmingin heart failureWassertherapie bei herzinsuffizienz,” DeutscheZeitschrift fur Sportmedizin, vol. 56, no. 12, pp. 403–409, 2005.
[72] K. Meyer and J. Bucking, “Exercise in heart failure: shouldaqua therapy swimming be allowed?” Medicine and Science inSports and Exercise, vol. 36, no. 12, pp. 2017–2023, 2004.

Hindawi Publishing CorporationPulmonary MedicineVolume 2011, Article ID 414253, 6 pagesdoi:10.1155/2011/414253
Review Article
Effects of Ischemic Acute Kidney Injury on Lung Water Balance:Nephrogenic Pulmonary Edema?
Rajit K. Basu1, 2 and Derek Wheeler1, 2
1 Division of Critical Care Medicine, Cincinnati Children’s Hospital Medical Center, 3333 Burnet Avenue,Cincinnati, OH 45229, USA
2 Cincinnati Children’s Hospital Medical Center, 3333 Burnet Avenue, Cincinnati, OH 45229, USA
Correspondence should be addressed to Rajit K. Basu, [email protected]
Received 17 December 2010; Accepted 28 March 2011
Academic Editor: Charlie Strange
Copyright © 2011 R. K. Basu and D. Wheeler. This is an open access article distributed under the Creative Commons AttributionLicense, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properlycited.
Pulmonary edema worsens the morbidity and increases the mortality of critically ill patients. Mechanistically, edema formation inthe lung is a result of net flow across the alveolar capillary membrane, dependent on the relationship of hydrostatic and oncoticpressures. Traditionally, the contribution of acute kidney injury (AKI) to the formation of pulmonary edema has been attributed tobulk fluid accumulation, increasing capillary hydrostatic pressure and the gradient favoring net flow into the alveolar spaces. Recentresearch has revealed more subtle, and distant, effects of AKI. In this review we discuss the concept of nephrogenic pulmonaryedema. Pro-inflammatory gene upregulation, chemokine over-expression, altered biochemical channel function, and apoptoticdysregulation manifest in the lung are now understood as “extra-renal” and pulmonary effects of AKI. AKI should be counted asa disease process that alters the endothelial integrity of the alveolar capillary barrier and has the potential to overpower the abilityof the lung to regulate fluid balance. Nephrogenic pulmonary edema, therefore, is the net effect of fluid accumulation in the lungas a result of both the macroscopic and microscopic effects of AKI.
1. Introduction
Pulmonary edema, a state of abnormal fluid accumulationin the alveolar space of the lung, can interfere with normaloxygenation and ventilation. At baseline, the heart, lungs,and vascular system work in concert to facilitate fluidmovement through the capillary and lymphatic beds ofthe lung ensuring adequate oxygen transport with limitedtransudation of fluid from the lung interstitium into thealveolar space. In disease states causing acute lung injury(ALI), both direct and indirect, this harmony can bedisrupted.
Pulmonary edema affects the morbidity and overall mor-tality of critically ill patients. Patients with pulmonary edemahave longer hospital stays, duration of mechanical ventila-tion, and rates of pneumonia in both adults and children [1–3]. In adult and pediatric populations, pulmonary edema cancomplicate the hospital course of any patient, but has notableeffects on those with primary respiratory failure, transplant
surgery, cardiothoracic surgery, or traumatic brain inj-ury. More recently, clinicians are appreciating the impact ofacute kidney injury (AKI) on ventilation and water balancein the lung. As clinical and experimental evidence continuesto mount for organ crosstalk, the relationship betweenthe kidney and the lung in critical illness emerges aspathologically significant [4].
The purpose of this brief narrative is to discuss the poten-tial impact of AKI on lung homeostasis, specifically waterbalance. Numerous laboratory models of isolated AKI havedemonstrated deleterious effects on lung pathology and sup-port the existence of kidney-lung crosstalk. Using this back-ground, we propose the concept of nephrogenic pulmonaryedema. Though fluid overload is often seen in patients withacute renal failure, we highlight the evidence pointing to astate of pulmonary edema induced by extrarenal microscopiceffects of kidney injury. Timely identification of these effectsof AKI may aid in the treatment of this disease process whichhas significant associated morbidity and mortality [5].

2 Pulmonary Medicine
Fluid overload
Qf = Kf [( − PT )− σ(πc − πT )]
Cd14, Lcn-2, CXCL-2, IL-6, TNF-α
caspase-3
↑↑ Aquaporin-1, 5
↓
↓↓
↓↓
↓↓
↓↓
↓↓↓↓↓↓
Na/K-ATPase
↓ ENaC↓ Total body protein
relative hypoproteinemia
NOS, HO-1
πT
πc
PT
Pc
Pc
↑↑ Proinflammatory mediators:
↑↑ Proapoptotic mediators:
↓ Antioxidant expression:
Figure 1: Nephrogenic pulmonary edema. Acute kidney injury triggers numerous mechanisms which alter the homeostasis of pulmonaryinterstitial and alveolar fluid balance. Qf : net flow across the alveolar-capillary membrane; Kf : filtration coefficient; PC : capillary hydrostaticpressure; PT : interstitial fluid hydrostatic pressure; σ : reflection coefficient of the alveolar-capillary membrane; πC : capillary oncotic pressure;πT : interstitial oncotic pressure; NOS: nitric oxide synthase; HO-1: heme-oxygenase-1; Lcn-2: lipocalin-2; CXCL-2: chemokine ligand-2;IL-6: interleukin-6; TNF-α: tumor necrosis factor-α; Na/K-ATPase: sodium-potassium ATPase; ENaC: endothelial sodium channel. It isimportant to note that negative changes in the reflection coefficient likely also increase the filtration coefficient leading to a net increase influid flow across the alveolar-capillary membrane.
2. Pathophysiology
Pulmonary edema occurs when net flow across the alveolar-capillary membrane is positive. Under normal conditions,fluid in the alveolar space is drained by pulmonary lymphaticvessels and then contained within the interstitial space. If thealveolar epithelial barrier is disrupted or if the interstitialfluid volume of the lungs increases by more than 50%,flooding of the alveolar space can occur [6]. The movementof fluid is dependent on both hydrostatic and oncoticpressures and is modeled by the Starling equation
Qf = Kf [(PC − PT)− σ(πC − πT)], (1)
where Qf is the net flow across the alveolar-capillarymembrane; Kf is the filtration coefficient (dependent onthe permeability and the surface area of the membrane);PC is the capillary hydrostatic pressure; PT is the interstitialfluid hydrostatic pressure; σ is the reflection coefficient ofthe alveolar-capillary membrane (σ = 1 if the membraneis impermeable to protein, and σ = 0 if the membrane iscompletely permeable to protein); πC is the capillary oncoticpressure; πT is the interstitial oncotic pressure [7]. In normalconditions, capillary hydrostatic pressure (PC) approximatesinterstitial fluid hydrostatic pressure (PT), (PC � PT), suchthat net fluid movement (Qf ) is low and fluid stays in thecapillary lumen. Similarly, capillary oncotic pressure (πC) isnormally greater than interstitial oncotic pressure (πT), andsince the reflection coefficient (σ) is generally near 1 (0.7–0.95), Qf is generally low. Implicit in the equation is that anyforce or mechanism that creates a large difference betweenthe hydrostatic forces and the oncotic forces will increase Qf ,
and thus flux of fluid from the capillary bed into the alveolarspace. The lung has safety measures in place to prevent suchleakage. The lymphatic system has high capacitance and flowto clear excess fluid from the interstitium. The capillaryendothelium between the interstitium and the alveolar bedscan tolerate increasing amounts of hydrostatic and interstitialfluid pressure [8]. However, in conditions of excess lungwater such as pulmonary edema, overall oncotic pressurebecomes dilute (thereby increasing the discrepancy betweenthe hydrostatic and the oncotic pressures) favoring net flowof fluid into the alveolar space (Figure 1).
Aside from bulk fluid and protein effects, changes atthe microscopic level change permeability of the alveolarcapillary endothelium. Decreased expressions of sodiumtransport molecules, such as the epithelial sodium channel(ENaC), the sodium-potassium-ATPase pump (Na+/K+-ATPase), or the cystic fibrosis transmembrane conductanceregulator (CFTR), all contribute to increased alveolar fluidaccumulation in experimental models of pulmonary edema[9, 10]. ENaC promotes sodium absorption from the alveolarspace into the lung epithelial cells. Similarly, the sodiumATPase pump allows for sodium extrusion from the alveolus.Aberrant expression of either has significant ramificationsfor fluid balance as water passively follows sodium. Addi-tionally, the regulation of fluid clearance by endogenouscatecholamines, particularly the β-adrenergic system, hasbeen highlighted [11].
Variations in vascular preload, capillary endothelialintegrity, and aberrations in osmotic pressure can alter theinterstitial-alveolar fluid balance. Increased vascular preloadleading to pulmonary edema is commonly observed in

Pulmonary Medicine 3
patients with left-sided cardiogenic shock and disorders ofincomplete pulmonary vascular drainage. In these situa-tions, the capacitance of the interstitial lymphatic systemis overwhelmed, the PC � PT , and fluid spills from thevascular space down a hydrostatic gradient. Acutely negativeintrathoracic pressure raises left ventricular stroke work andlikely leads to backup of fluid into the pulmonary bed(increasing PC) in postobstructive pulmonary edema. Theintegrity of the alveolar capillary endothelium is alteredin acute respiratory distress syndrome (ARDS), sepsis,and stress states [12, 13]. Bacterial contribution to typeII pneumocyte surfactant production has been linked toincreased capillary permeability in sepsis [14]. Such diseasestates alter the reflection coefficient (σ), decreasing the abilityof oncotic pressure to balance hydrostatic pressure in theStarling equation. Neurogenic pulmonary edema, commonlyobserved in intracranial hypertension, may both alter thesympathetic catecholamine regulation of the systemic circu-lation, thereby diverting blood to the alveolar capillary bed(↑ PC), and disrupt capillary integrity [15]. Finally, acuteor chronic disease states commonly carry the comorbidityof hypoproteinemia. Low circulating serum total proteinlevels directly reduce the capillary oncotic pressure, favoringfluid efflux from the luminal space. The interstitial-alveolarinterface in the lung is under tight control and can beaffected by disease states that cause dysregulation in totalbody fluid status, levels of inflammatory mediators, andaberrant protein homeostasis.
3. AKI and Fluid Balance
Acute kidney injury complicates critical illness in manyways. Concomitant with the diagnosis of AKI was fluidoverload, which has been found retrospectively to indepen-dently increase morbidities such as duration of mechanicalventilation and hospital length of stay, and overall mortality[16–18]. Fluid overload carries increased risk of morbidity inmortality in both adults and children [19]. On retrospectivereview, children with greater degrees of fluid overload hadhigher mortality on initiation of renal replacement therapy[20].
The kidney is central to many homeostatic mechanismsin the body, and as AKI progresses dysregulation occurs invarious locations in the body. The kidney communicateswith the lung in several ways: regulating acid-base balance,increasing oxygen carrying capacity through erythropoiesis,and regulating blood pressure through the renin-angioten-sin-aldosterone axis. All of these processes may be altered inAKI. The deleterious connection between the kidney and thelung in disease states, first reported by Bass and Singer in1950, was assumed to be secondary to uremia and fluid over-load [21]. However, despite the use of dialysis to limit uremiaand to control fluid balance, high mortality rates continue inpatients with both AKI and ALI [22]. In progressive ALI andARDS, impaired global oxygenation will necessarily decreaserenal oxygenation leading to a vicious cycle of progressivelung and kidney injury [23]. The crosstalk between the kid-ney and the lung in the critically ill patient is of extremeimportance to all critical care physicians [4].
4. AKI and ALI
The impact of AKI on the lung can be seen on many levels.One of the major effects of AKI is to effect lung waterbalance. While fluid overload from anuric or oliguric AKIcan upset the hydrostatic-oncotic balance in the pulmonaryinterstitium, inflammation and endothelial injury whichmay be triggered by AKI also upset this equilibrium. Thecontributions of the latter, inflammation, changes in expres-sion of regulators of the pulmonary fluid and electrolytechemical gradient, and altered regulation of oxidative stress,may be greater than previously appreciated.
AKI triggers gene expression changes which may alterlung vascular stability. Global gene expression mapping oflung tissues in experimental murine kidney ischemia iden-tifies proinflammatory and proapoptotic gene upregulationin the lung transcriptome [24]. Proinflammatory genessuch as Cd14, lipocalin-2, chemokine ligand-2 (CXCL2),and IL-6 are all upregulated after ischemia [24]. Thesemediators, notably IL-6, trigger acute phase responses toantigens and initiate the inflammatory cascade. Subsequentinjury is caused by many mechanisms including: disruptionof endothelial integrity, aberrant signaling of the coagula-tion and contact cascades, and direct cellular toxicity invital organs. Reduction of the IL-6 effect using chemicalinhibition of IL-6 or use of IL-6-deficient mice reduceslung inflammation after ischemic AKI [25]. Caspase-3, amarker of cellular apoptotic activity, is upregulated in typeII pneumocytes after experimental AKI [26]. Macrophages,mediators of global injury and repair, may be involved; useof macrophage activation inhibitor decreases the amount ofpulmonary capillary leakage in murine ischemia [27].Uremiamay contribute to such upregulation, as lung inflammationand apoptosis are abrogated after nephrectomy [28]. Inrepeated animal models of AKI, proinflammatory mediatorsare expressed within hours of injury. Circulating inflamma-tory cytokines may affect lung capillary endothelium, chang-ing permeability. Apoptosis of either capillary endothelialcells or pneumocytes responsible for producing surfactantwill also change the permeability of the interstitial-alveolarinterface in the lung. Cytokine, chemokine, and apoptoticdysregulation is therefore a prime suspect of ALI after AKIand demonstrates kidney-lung crosstalk.
Fluid and electrolyte conduction in the lung is altered inAKI. Rabb and colleagues published the seminal work des-cribing the downregulation of pulmonary ENaC, Na/KATPase, and aquaporin-5 after ischemic injury and nephrec-tomy in rats [29]. As the primary interstitial solute, sodium isthe central determinant of fluid shift based on osmolar gra-dients. Changes in sodium balance on either side of thecapillary membrane, therefore, may have marked effects onfluid shifts between the interstitium and the alveolar bed.Aquaporin-1 message upregulation, in a sheep model of car-diopulmonary bypass and hypothermic circulatory arrest,was correlated with increased rates of pulmonary edema[30]. Similarly, aquaporin-5 has been identified in sepsis as acontributor to dysregulation in tissue and vascular permea-bility [31]. In experimental models, osmotically driven waterpermeability between the alveolar and capillary components

4 Pulmonary Medicine
of the lung is changed tenfold by deletion of aquaporin-1or aquaporin-5 [32]. While changes in aquaporin expressionmay have only minor clinical ramification, the evidencefor kidney-lung crosstalk is robust [33]. Aberrant salt andwater handling by the lung is altered in even mild modelsof experimental kidney ischemia. The impact of this onpulmonary edema formation is obvious.
Oxidative stress plays a role in the kidney-lung crosstalkseen during AKI. Hepatic levels of superoxide dismutase,glutathione, and catalase are decreased after ischemic AKIin mice, which may decrease host response to oxidativestress [34]. Additionally, TNF-α levels were significantlyhigher in ischemic mice than in sham controls pointing to asystemic oxidative/inflammatory response of AKI [35]. Thenitric oxide signaling pathway is critical to oxidative balanceand is altered in AKI. Patients with chronic kidney diseasehave lower basal production of nitric oxide compared tocontrols, and mice subjected to subtotal nephrectomy havelower levels of nitric oxide synthase [36, 37]. Finally, micelacking heme-oxygenase-1 (HO-1), critical for reducingoxidative stress and generation of antioxidant metabolites,have increased levels of inflammation after ischemic AKIversus sham controls [38]. Nitric oxide, HO-1, and TNF-αall affect lung capillary stability [39–41]. Therefore, thealteration in these regulators of oxidative balance after AKIcan affect lung vascular stability.
The conclusion that significant lung pathology resultsfrom ischemic AKI models must be tempered by the factthat, in practice, renal hypoperfusion without concurrentpulmonary hypoperfusion is rare. Indeed, it is rarely knownif ischemia to the kidney occurs before or after ischemia tothe lungs. Models of hemorrhagic and septic shock do notadequately address this issue. Additionally, in the commoncase of decreased renal preload (i.e., prerenal azotemia),the microscopic effects on the lung have not been clearlydescribed. Still, the findings described above highlight thepotential contribution of the injured renal endothelium tolung injury and edema formation.
5. Nephrogenic Pulmonary Edema
In the context of ischemic AKI and kidney-lung crosstalk,we propose the concept of nephrogenic pulmonary edema.Resting on the evidence of experimental extrarenal effects ofAKI and the acknowledged clinical effects of oliguric volumeoverload, nephrogenic pulmonary edema (NPE) could rep-resent net aberrant fluid handling at the interstitial-alveolarlung interface. On a microscopic level, NPE could resultas a consequence of damage of pulmonary endotheliumby AKI-mediated upregulated inflammation, disruption ofpulmonary sodium transport, and activation of apoptosis inpulmonary cells responsible for maintaining the homeostaticintegrity of lung water balance. AKI should be countedamongst the numerous disease processes that alter boththe volume load in the pulmonary capillary bed and theendothelial integrity of the alveolar capillary barrier.
Experimental manifestations of kidney injury are mani-fest in multiple extrarenal locations [42]. Experimental AKIhas deleterious effects on the central nervous system affecting
glial cell viability, blood-brain barrier permeability, andneurocognitive status [43]. Systolic ventricular function isnegatively affected by ischemic kidney injury [44]. Leukocytetrafficking is aberrant, and a host of proinflammatorygenomic and proteomic responses occur after experimentalAKI [24, 45]. The experimental evidence for lung injury afterAKI is robust [4].
Critically ill patients with acute lung injury with AKIhave worse morbidity and mortality. Fluid overload anduremia may be regulated by extracorporeal therapy such asdialysis, but lung injury and kidney injury are progressiveand mortality rates in patients with both disease processeshave not significantly improved with these therapies. Useof stratification criteria has retrospectively demonstratedimproved outcomes for patients with less severe AKI [46];biomarker research seeks to identify kidney injury in its earlystages. Appreciation of the impact of kidney injury duringthis epoch, before the onset of oliguria and fluid overload,may be critical. The impact of kidney-lung crosstalk on themolecular level may be creating a milieu of lung inflam-mation, mediated by proinflammatory, oxidative, chemical,and apoptotic signals. Ultimately, the accumulated signalsoverpower the ability of the lung to regulate fluid balance,leading to nephrogenic pulmonary edema.
References
[1] T. Kendirli, A. Kavaz, Z. Yalaki, B. Ozturk Hismi, E. Derelli,and E. Ince, “Mechanical ventilation in children,” TurkishJournal of Pediatrics, vol. 48, no. 4, pp. 323–327, 2006.
[2] A. Vasudevan, R. Lodha, and S. K. Kabra, “Acute lung injuryand acute respiratory distress syndrome,” Indian Journal ofPediatrics, vol. 71, no. 8, pp. 743–750, 2004.
[3] D. Schuller, J. P. Mitchell, F. S. Calandrino, and D. P. Schuster,“Fluid balance during pulmonary edema; is fluid gain amarker or a cause of poor outcome?” Chest, vol. 100, no. 4,pp. 1068–1075, 1991.
[4] G. J. Ko, H. Rabb, and H. T. Hassoun, “Kidney-lung crosstalkin the critically ill patient,” Blood Purification, vol. 28, no. 2,pp. 75–83, 2009.
[5] E. A. Hoste and M. Schurgers, “Epidemiology of acute kidneyinjury: how big is the problem?” Critical Care Medicine, vol.36, supplement 4, pp. S146–S151, 2008.
[6] A. C. Guyton and J. E. Hall, Textbook of Medical Physiology,Saunders, Philadelphia, Pa, USA, 9th edition, 1996.
[7] M. P. Chase and D. S. Wheeler, “Pediatric critical caremedicine,” in Basic Science and Clinical Evidence, D. S.Wheeler, H. R. Wong, and T. P. Shanley, Eds., vol. 1, Springer,London, UK, 1st edition, 2007.
[8] R. H. Demling, C. LaLonde, and K. Ikegami, “Pulmonaryedema: pathophysiology, methods of measurement, and clini-cal importance in acute respiratory failure,” New Horizons, vol.1, no. 3, pp. 371–380, 1993.
[9] Y. Berthiaume, H. G. Folkesson, and M. A. Matthay, “Lungedema clearance: 20 Years of progress invited review: alveolaredema fluid clearance in the injured lung,” Journal of AppliedPhysiology, vol. 93, no. 6, pp. 2207–2213, 2002.
[10] G. M. Verghese, L. B. Ware, B. A. Matthay, and M. A.Matthay, “Alveolar epithelial fluid transport and the resolutionof clinically severe hydrostatic pulmonary edema,” Journal ofApplied Physiology, vol. 87, no. 4, pp. 1301–1312, 1999.

Pulmonary Medicine 5
[11] D. Mehta, J. Bhattacharya, M. A. Matthay, and A. B. Malik,“Integrated control of lung fluid balance,” American Journal ofPhysiology, vol. 287, no. 6, pp. L1081–L1090, 2004.
[12] D. M. Berkowitz, P. A. Danai, S. Eaton, M. Moss, and G. S.Martin, “Accurate characterization of extravascular lung waterin acute respiratory distress syndrome,” Critical Care Medicine,vol. 36, no. 6, pp. 1803–1809, 2008.
[13] A. B. Groeneveld, “Vascular pharmacology of acute lung inj-ury and acute respiratory distress syndrome,” Vascular Phar-macology, vol. 39, no. 4-5, pp. 247–256, 2002.
[14] K. T. Oldham, K. S. Guice, P. S. Stetson, and R. R. Wolfe,“Bacteremia-induced suppression of alveolar surfactant pro-duction,” Journal of Surgical Research, vol. 47, no. 5, pp. 397–402, 1989.
[15] H. I. Chen, “From neurogenic pulmonary edema to fatembolism syndrome: a brief review of experimental and clin-ical investigations of acute lung injury and acute respiratorydistress syndrome,” Chinese Journal of Physiology, vol. 52,supplement 5, pp. 339–344, 2009.
[16] E. A. Hoste and W. De Corte, “Epidemiology of AKI in theICU,” Acta Clinica Belgica, vol. 2, pp. 314–317, 2007.
[17] E. A. J. Hoste and J. A. Kellum, “Incidence, classification, andoutcomes of acute kidney injury,” Contributions to Nephrology,vol. 156, pp. 32–38, 2007.
[18] R. Thadhani, M. Pascual, and J. V. Bonventre, “Acute renalfailure,” The New England Journal of Medicine, vol. 334, no.22, pp. 1448–1460, 1996.
[19] S. M. Bagshaw and D. N. Cruz, “Fluid overload as a biomarkerof heart failure and acute kidney injury,” Contributions toNephrology, vol. 164, pp. 54–68, 2010.
[20] R.K. Basu, An Update and Review of Acute Kidney Injury inPediatrics, Pediatric Critical Care Medicine, 2010.
[21] H. E. Bass and E. Singer, “Pulmonary changes in uremia,”Journal of the American Medical Association, vol. 144, no. 10,pp. 819–823, 1950.
[22] R. L. Mehta, M. T. Pascual, C. G. Gruta, S. Zhuang, and G. M.Chertow, “Refining predictive models in critically ill patientswith acute renal failure,” Journal of the American Society ofNephrology, vol. 13, no. 5, pp. 1350–1357, 2002.
[23] J. W. Kuiper, A. B. J. Groeneveld, A. S. Slutsky, and F. B. Plotz,“Mechanical ventilation and acute renal failure,” Critical CareMedicine, vol. 33, no. 6, pp. 1408–1415, 2005.
[24] D. N. Grigoryev, M. Liu, H. T. Hassoun, C. Cheadle, K. C.Barnes, and H. Rabb, “The local and systemic inflammatorytranscriptome after acute kidney injury,” Journal of the Ameri-can Society of Nephrology, vol. 19, no. 3, pp. 547–558, 2008.
[25] C. L. Klein, T. S. Hoke, W. F. Fang, C. J. Altmann, I. S. Douglas,and S. Faubel, “Interleukin-6 mediates lung injury followingischemic acute kidney injury or bilateral nephrectomy,” KidneyInternational, vol. 74, no. 7, pp. 901–909, 2008.
[26] H. R. Jang and H. Rabb, “The innate immune response inischemic acute kidney injury,” Clinical Immunology, vol. 130,no. 1, pp. 41–50, 2009.
[27] A. A. Kramer, G. Postler, K. F. Salhab, C. Mendez, L. C. Carey,and H. Rabb, “Renal ischemia/reperfusion leads to macrop-hage-mediated increase in pulmonary vascular permeability,”Kidney International, vol. 55, no. 6, pp. 2362–2367, 1999.
[28] T. S. Hoke, I. S. Douglas, C. L. Klein et al., “Acute renalfailure after bilateral nephrectomy is associated with cytokine-mediated pulmonary injury,” Journal of the American Societyof Nephrology, vol. 18, no. 1, pp. 155–164, 2007.
[29] H. Rabb, Z. Wang, T. Nemoto, J. Hotchkiss, N. Yokota, and M.Soleimani, “Acute renal failure leads to dysregulation of lung
salt and water channels,” Kidney International, vol. 63, no. 2,pp. 600–606, 2003.
[30] S. Tabbutt, D. P. Nelson, N. Tsai et al., “Induction of aqua-porin-1 mRNA following cardiopulmonary bypass and reper-fusion,” Molecular Medicine, vol. 3, no. 9, pp. 600–609, 1997.
[31] M. Arul, M. A. Chinnaiyan, M. Huber-Lang et al., “Molecularsignatures of sepsis: multiorgan gene expression profiles ofsystemic inflammation,” American Journal of Pathology, vol.159, no. 4, pp. 1199–1209, 2001.
[32] A. S. Verkman, M. A. Matthay, and Y. Song, “Aquaporin waterchannels and lung physiology,” American Journal of Physiology,vol. 278, no. 5, pp. L867–L879, 2000.
[33] Y. Song, N. Fukuda, C. Bai, T. Ma, M. A. Matthay, and A. S.Verkman, “Role of aquaporins in alveolar fluid clearance inneonatal and adult lung, and in oedema formation followingacute lung injury: studies in transgenic aquaporin null mice,”Journal of Physiology, vol. 525, part 3, pp. 771–779, 2000.
[34] M. Serteser, T. Koken, A. Kahraman, K. Yilmaz, G. Akbu-lut, and O. N. Dilek, “Changes in hepatic TNF-alpha lev-els, antioxidant status, and oxidation products after renalischemia/reperfusion injury in mice,” Journal of SurgicalResearch, vol. 107, no. 2, pp. 234–240, 2002.
[35] G. Akbulut, O. N. Dilek, A. Kahraman, T. Koken, and M.Serteser, “The correlation between renal tissue oxidative stressparameters and TNF-alpha levels in an experimental modelof ischemia-reperfusion injury in mice,” Ulusal Travma ve AcilCerrahi Dergisi, vol. 11, no. 1, pp. 11–16, 2005.
[36] R. Wever, P. Boer, M. Hijmering et al., “Nitric oxide pro-duction is reduced in patients with chronic renal failure,”Arteriosclerosis, Thrombosis, and Vascular Biology, vol. 19, no.5, pp. 1168–1172, 1999.
[37] N. D. Vaziri, Z. Ni, F. Oveisi, K. Liang, and R. Pandian,“Enhanced nitric oxide inactivation and protein nitration byreactive oxygen species in renal insufficiency,” Hypertension,vol. 39, no. 1, pp. 135–141, 2002.
[38] M. J. Tracz, J. P. Juncos, A. J. Croatt et al., “Deficiency of hemeoxygenase-1 impairs renal hemodynamics and exaggeratessystemic inflammatory responses to renal ischemia,” KidneyInternational, vol. 72, no. 9, pp. 1073–1080, 2007.
[39] F. Jiang, S. J. Roberts, S. R. Datla, and G. J. Dusting, “NOmodulates NADPH oxidase function via heme oxygenase-1 inhuman endothelial cells,” Hypertension, vol. 48, no. 5, pp. 950–957, 2006.
[40] L. A. Morio, K. A. Hooper, J. Brittingham et al., “Tissue injuryfollowing inhalation of fine particulate matter and hydrogenperoxide is associated with altered production of inflamma-tory mediators and antioxidants by alveolar macrophages,”Toxicology and Applied Pharmacology, vol. 177, no. 3, pp. 188–199, 2001.
[41] P. Vigne, E. Feolde, A. Ladoux, D. Duval, and C. Frelin,“Contributions of NO synthase and heme oxygenase to cGMPformation by cytokine and hemin treated brain capillaryendothelial cells,” Biochemical and Biophysical Research Com-munications, vol. 214, no. 1, pp. 1–5, 1995.
[42] C. M. Feltes, J. Van Eyk, and H. Rabb, “Distant-organ changesafter acute kidney injury,” Nephron Physiology, vol. 109, no. 4,pp. p80–p84, 2008.
[43] M. Liu, Y. Liang, S. Chigurupati et al., “Acute kidney injuryleads to inflammation and functional changes in the brain,”Journal of the American Society of Nephrology, vol. 19, no. 7,pp. 1360–1370, 2008.
[44] K. J. Kelly, “Distant effects of experimental renal ischemia/reperfusion injury,” Journal of the American Society of Nephrol-ogy, vol. 14, no. 6, pp. 1549–1558, 2003.

6 Pulmonary Medicine
[45] S. Miyazawa, H. Watanabe, C. Miyaji, O. Hotta, and T.Abo, “Leukocyte accumulation and changes in extra-renalorgans during renal ischemia reperfusion in mice,” Journal ofLaboratory and Clinical Medicine, vol. 139, no. 5, pp. 269–278,2002.
[46] S. M. Bagshaw, C. George, I. Dinu, and R. Bellomo, “Amulti-centre evaluation of the RIFLE criteria for early acutekidney injury in critically ill patients,” Nephrology DialysisTransplantation, vol. 23, no. 4, pp. 1203–1210, 2008.

Hindawi Publishing CorporationPulmonary MedicineVolume 2011, Article ID 190648, 7 pagesdoi:10.1155/2011/190648
Review Article
Standardization of Methods for Early Diagnosis andOn-Site Treatment of High-Altitude Pulmonary Edema
Qiquan Zhou
Department of High Altitude Disease, College of High Altitude Military Medicine, Third Military Medical University,and Key Laboratory of High Altitude Medicine, Ministry of Education, Chongqing 400038, China
Correspondence should be addressed to Qiquan Zhou, [email protected]
Received 15 November 2010; Revised 16 March 2011; Accepted 28 March 2011
Academic Editor: Hartmut Grasemann
Copyright © 2011 Qiquan Zhou. This is an open access article distributed under the Creative Commons Attribution License,which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
High-altitude pulmonary edema (HAPE) is a life-threatening disease of high altitude that often affects nonacclimatized apparentlyhealthy individuals who rapidly ascend to high altitude. Early detection, early diagnosis, and early treatment are essential tomaintain the safety of people who ascend to high altitude, such as construction workers and tourists. In this paper, I discuss variousmethods and criteria that can be used for the early diagnosis and prediction of HAPE. I also discuss the preventive strategies andoptions for on-site treatment. My objective is to improve the understanding of HAPE and to highlight the need for prevention,early diagnosis, and early treatment of HAPE to improve the safety of individuals ascending to high altitude.
1. Introduction
High-altitude pulmonary edema (HAPE) is a specific diseaseof high altitude. It has a high incidence and is often seriousbecause of its rapid progresses. It is also life-threatening iftreatment is not started in a timely manner [1, 2].
Many studies [3, 4] have shown that HAPE is a majordisease that often affects nonacclimatized healthy individualswho ascend to high altitudes. Therefore, early diagnosisof HAPE is essential to initiate early treatment of HAPEand maintain the safety of people who ascent to highaltitude. Although international and Chinese criteria havebeen established for HAPE [5], its early detection anddiagnosis are difficult, except in the presence of typicalpulmonary edema. Following the magnitude 7.1 earthquakethat struck Yushu (Yushu Tibetan Autonomous Prefecture,Qinghai Province, China) on April 14, 2010, approximately50,000 rescuers assembled in the region. This region liesat an altitude ranging from 3700 m to 4900 m, the averagealtitude is 4,493 m. Although the incidence of HAPE is only2–4%, the sudden influx of nonacclimatized rescuers to theregion meant that HAPE was one of the most commonlife-threatening diseases at that time, even considering theeffects of the earthquake, which caused 1944 deaths, with 216people missing and 12,135 injured.
HAPE can also induce psychological disorders in affectedindividuals. Therefore, it is essential to highlight the earlydiagnosis and on-site treatment of HAPE. Under the supportof the National Science and Technology Program, we haveconducted an extensive range of studies on HAPE intendedto find effective methods for early diagnosis and clinicaltreatment of HAPE and, thus, improve the health and safetyof individuals who rapidly ascend to high altitude.
2. Methods for the Early Diagnosis of HAPE
It is generally not difficult for physicians to diagnose typicalHAPE, which is based on medical history, symptoms, andsigns including white, yellow, or pink frothy sputum, moistrales on pulmonary auscultation, and flocculent shadowson chest X-rays. However, atypical HAPE is much moredifficult to diagnose. Patients usually develop atypical HAPEat altitude <3000 m, which may occur several days or longerafter ascending to altitude. Symptoms differ from thoseof typical HAPE, such as less sputum or an absence ofsputum and nonspecific findings on chest X-rays. Basedon a previous study [6], the development of HAPE can beclassified into two stages from the onset to the presenceof typical symptoms. The early stage is characterized by

2 Pulmonary Medicine
interstitial pulmonary edema while the late stage is character-ized by alveolar pulmonary edema. Patients with interstitialpulmonary edema do not usually exhibit serious dyspneaor typical signs such as pink frothy sputum, extensivemoist rales, or wheezy phlegm. Thus, these patients aresusceptible to misdiagnosis and delayed treatment. Li et al.[7] investigated the characteristics of HAPE in 482 patients.They examined the clinical symptoms and signs, andperformed routine blood tests, electrocardiography, colorDoppler echocardiography, chest X-rays, and computedtomography (CT) of the patients. They found that HAPEpatients exhibited significant differences in these parameterscompared with non-HAPE patients, and that the symptomsand signs were more obvious in HAPE patients than innon-HAPE patients. In addition, studies have revealed thatoxygen treatment is more effective in HAPE than in otherforms of lung injury. Therefore, some researchers haveproposed that tentative oxygen treatment can be used for theearly diagnosis of HAPE. Nevertheless, the most importantexaminations for the early diagnosis of HAPE are chestX-rays or CT. On chest X-rays, HAPE often presents asdecreased pulmonary transmittance, increased or obscurelung markings, and ground glass-like changes in the lung,or patchy shadows. On CT scans, increased and enlargedlung markings, ground glass-like changes in the lung,nodule-like shadows, scattered or isolated alveolar edemaof terminal bronchioles, and slim reticulate shadows can beobserved.
3. Diagnosis and Grading of HAPE
3.1. Criteria for Early Diagnosis of HAPE. According to theclinical symptoms, signs, and findings of blood routine tests,electrocardiography, color Doppler echocardiography, chestX-rays, and CT, the following criteria for HAPE have beendeveloped [7]:
(1) recent ascent to high altitude (>3000 m); the presenceof palpitations, chest tightness, dyspnea and coughwith or without white foamy sputum;
(2) local, unilateral, or bilateral coarse breath sounds,with or without local moist rales, central cyanosis,tachycardia (>100/min), and tachypnea (>24/min);
(3) chest X-ray findings including decreased pulmonarytransmittance, increased or obscure lung markings,ground glass-like changes or patchy shadows in thelung; CT findings including increased and enlargedlung markings, ground glass-like changes, nodule-like shadows, scattered or isolated alveolar edema ofterminal bronchioles and slim reticulate shadows;
(4) routine blood test findings include an increased whiteblood cell count and an increased neutrophil count;
(5) arterial blood gas analysis showing continuoushypoxemia accompanied by mild respiratory alkalo-sis;
(6) electrocardiographic findings including sinus tachy-cardia, clockwise rotation and sharp P waves;
(7) persistent pulmonary hypertension on echocardiog-raphy;
(8) symptoms resolve rapidly following rest, oxygentreatment, pulmonary artery pressure lowering treat-ment, and diuresis.
For the diagnosis of HAPE, criteria 1, 2 and 3 must bemet. These findings, together with those in 4, 5, 6, 7, and/or8, are then used to confirm HAPE. Using these criteria,the severity of disease can be determined, which is criticalfor individualized therapy. With early diagnosis and earlytreatment, HAPE can be controlled at the early stage and thesymptoms be markedly improved.
3.2. Criteria for the Grading of HAPE. Once HAPE is diag-nosed, its severity should be graded to provide individualizedtherapy. Therefore, when a patient with suspected HAPE isadmitted, the grade of HAPE should be confirmed as soon aspossible according to the criteria for early diagnosis [8].
3.2.1. Mild. Dyspnea and cough with white foamy sputummay occur after intermediate manual labor. Lung auscul-tation shows local moist rales in a unilateral lung. Therespiratory rate is often <24 breaths/min, and heart rate<100 beats/min. There is no arrhythmia. Chest X-rays showsthe area of flocculent shadows occupies <1/4 of the lung.The shadows are confined to the right lower lobe and arespotty or patchy. CT scans reveal increased and enlarged lungmarkings. Routine blood tests are normal.
3.2.2. Moderate. Dyspnea, chest pain, chest tightness, andcough with a large amount of white foamy sputum occurafter mild manual labor. Extensive moist rales are notedin the bilateral lower lung or unilateral lung on lungauscultation. The respiratory rate is >24 breaths/min whilethe heart rate is >110 beats/min and is accompanied byarrhythmia. Chest X-rays show patchy or flocculent shadowscovering >1/2 of the lung, and CT scans show ground glass-like changes or nodule-like shadows. The white blood cellcount and neutrophil count are slightly increased.
3.2.3. Severe. Patients can not lie in the supine or proneposition. They may have a pale complexion, cold sweat onthe forehead, serious dyspnea, and a heavy cough with alarge amount of white or pink foamy sputum. Rales of small,intermediate, and large bubbles are extensive in the bilaterallungs and are accompanied by the sound of boiling water.The respiratory rate is >30 breaths/min, while the heart rateis >120 beats/min and is accompanied by arrhythmia. ChestX-rays reveal asymmetric cloudy shadows covering >1/2 ofthe bilateral lungs, and CT scans indicate scattered or isolatedalveolar edema of the terminal bronchioles. The white bloodcell count is 10× 109/L.
3.2.4. Extremely Severe. The symptoms and signs are moreserious than those in severe HAPE. Patients are at high risk

Pulmonary Medicine 3
of dying. They have a pale complexion, weak breathing, anda large amount of foam is discharged from the nose andmouth. A gurgling sound is audible in the bilateral lungs. Theheart sounds are weak, and blood pressure is decreased. Thepatient is also likely to have high-altitude cerebral edema.Heart failure and secondary pulmonary infection are verylikely. Chest X-rays reveal flocculent shadows in unilateral orbilateral lungs, enlargement of the heart, and the pulmonaryartery is particularly clear. CT scans show diffuse alveolaredema in unilateral or bilateral lungs. The number of whiteblood cells is > 16× 109/L.
4. Guidelines for On-Site Treatment of HAPE
4.1. Guidelines for the Treatment of HAPE. In terms of phar-macotherapy, there is no consensus on the types of drugs,their doses, or administration routes for HAPE. Thus, it isimperative to develop guidelines to standardize and optimizethe treatment of HAPE. Based on the experience of severalmountain sickness treatment centers and the efficacy ofcurrently available drugs and strategies, in combination withrecent advances in the treatment of HAPE, our researchgroup proposed four regimens for early diagnosis and treat-ment of HAPE and conducted a prospective, randomized,controlled study to investigate their efficacy. A total of 400patients with HAPE were divided into four groups andtreated as follows: patients in group A received oxygeninhalation, dexamethasone, and aminophylline; patients ingroup B-C were treated as in group A, in addition to diuresiswith furosemide in group B, blood pressure-lowering withnifedipine in group C, or L-arginine in group D. The efficacyand safety of these therapeutic regimens were compared.The treatment showing greatest therapeutic efficacy wassubsequently used to prepare the guidelines for the treatmentof HAPE. Overall, all four regimens were effective for thetreatment of HAPE [9]. However, in terms of the time toresolution of symptom and signs, the time to resolutionof chest X-ray findings, and duration of hospitalization,regimen B was superior to the other regimens. Interestingly,there were no marked differences between regimens A,C, and D. Furthermore, there were no differences in theincidence of adverse effects between regimens A, B, andD, or in the liver and kidney functions between all fourregimens. These findings suggest that a regimen composedof oxygen inhalation, dexamethasone, aminophylline, andfurosemide is effective, well tolerated, simple to follow, andthus offers a basic, standardized regimen for the treatment ofHAPE
Once the regimen has been selected, timely initiationof individualized treatment is a key factor that contributestowards its therapeutic efficacy. Our experience of on-sitetreatment of more than 300 patients with HAPE has shownthat on-site individualized treatment is feasible, withoutincreasing the risk for death [10]. Following the Yushu earth-quake, the efficacy of this regimen was further confirmed asthe prognosis after on-site treatment was significantly betterthan that after blind evacuation, which usually results in pooroutcomes.
4.2. Principles of Individualized Treatment of HAPE. Theprinciples of individualized treatment of HAPE are highlydependent on the severity of HAPE [11].
4.2.1. Mild. Bed rest, intermittent oxygen inhalation or sub-cutaneous oxygen treatment, oral aminophylline (250 mg),prednisone (10 mg), furosemide (20 mg), atropine or aniso-damine (5 mg) twice daily, and other treatments for specificsymptoms are recommended.
4.2.2. Moderate. Absolute bed rest, continuous oxygen in-halation or subcutaneous oxygen treatment are necessary.Drugs are mainly administered intramuscularly, accompa-nied by oral and intravenous medication. Aminophylline(250 mg), prednisone (10 mg), furosemide (20 mg), atropineor anisodamine (5 mg) three to four times daily, and othertreatments for specific symptoms are recommended.
4.2.3. Severe. Absolute bed rest, preferably in a semirecum-bent position and continuous high-flow oxygen inhalationwith defoaming agents in a humidifier bottle are nec-essary. Drugs are mainly administered intravenously andintramuscularly. Atropine (2–5 mg/0.5 h) or anisodamine(20–40 mg/0.5 h), dexamethasone (10 mg/4 h), furosemide(40 mg/8 h), gentamicin (80000 IU/8 h); or dexamethasone(200 mg), furosemide (40 mg), atropine or anisodamine(10 mg), and gentamicin (160000 IU) in 10% glucose solu-tion (500 mL) three times daily are recommended. Symp-tomatic treatments may include intramuscular morphine(10 mg) for patients with dysphoria, intramuscular cedilanid(0.4–0.8 mg) for patients with heart failure, and vitamin C,ATP solution, coenzyme A, and cytochrome C, as deemednecessary.
4.2.4. Extremely Severe. On-site treatment is preferred, fol-lowed by escalation therapy during evacuation once thepatient’s condition has stabilized. The procedures for thetreatment of extremely severe HAPE are similar to those ofsevere HAPE, except for the treatment of complications. Forpatients with cerebral edema, the doses of dexamethasoneand diuretics should be increased and airway maintenanceis necessary. Hyperbaric oxygen treatment or oxygen inhala-tion through a ventilator is also recommended. Hypothermiais beneficial for the brain. For patients with serious heartfailure, half or two-thirds of the recommended dose ofdigitalis should be administered in combination with anappropriate dose of a sedative. The daily dose of glucoseshould be <400 g to maintain low energy consumption andto promote osmotic diuresis. The treatments should beescalated during evacuation once the patient’s condition hasstabilized.
The following factors are particularly important duringevacuation. (1) Mode of transport: the patient should betransported in a vehicle that can provide rapid and steadyevacuation. Such transportation options include helicopter,motor truck, heavy-duty medical car, and miniambulance.The vehicle’s speed should be carefully controlled, particu-larly in undulating conditions, to ensure the patient remains

4 Pulmonary Medicine
in a horizontal position and excess movement is avoided.(2) Accompanying personnel: the patient should be ideallyaccompanied by one nurse and one physician, or at least onemedical staff who can provide effective on-site treatment,The personnel should continuously monitor and recordthe patient’s vital signs and perform treatment as deemednecessary. (3) Patient position: the patient should be keptin a semirecumbent position, and airway maintenance isessential. However, the supine position is recommended forpatients in a coma. Head vibration and bumps should beavoided to prevent cerebral hernia. (4) For deceased patients,the time of death and the patients symptoms and signs atdeath should be recorded, and the body should remain in astable position.
4.2.5. Symptomatic Treatment. For patients with suspectedheart failure, treatment with digitalis (e.g., cedilanid anddigoxin) is recommended to improve myocardial contrac-tility. For patients with low blood pressure, dextran andhydroxyethyl starch 40 is recommended for blood volumeexpansion. For patients with secondary infections, penicillinor other antibiotics can be administered. For patients withdysphoria, sedatives can be given according to the diseasestate.
In summary, patients with mild to moderate HAPEshould receive basic treatment plus any supplementarytreatment required. Patients with severe and extremely severeHAPE should also receive treatment for any symptoms.Basic treatment consists of bed rest, oxygen inhalation, andintravenous administration of aminophylline, dexametha-sone, and furosemide. Supplementary treatments includeantibiotics, vitamin C, and cytochrome C, for example.
4.3. Pathophysiological Evidence for the On-Site
Treatment of HAPE
4.3.1. Bed Rest. Physical activity may lead to contractionof pulmonary vessels resulting in an increase in pulmonaryartery pressure and a decrease in arterial partial pressure ofoxygen. Therefore, absolute bed rest can reduce muscularactivity and contraction of blood vessels and, thus, providestable pulmonary artery pressure. In some studies [12], bedrest alone was used for the treatment of mild HAPE.
4.3.2. Oxygen Inhalation. Oxygen inhalation can decreasethe pulmonary artery pressure. Evidence shows that inhala-tion of 100% oxygen can significantly decrease the increasedpulmonary artery pressure and is accompanied by improve-ments in symptoms [13]. In addition, oxygen inhalation canincrease arterial oxygen saturation and improve tissue oxy-gen supply, thus alleviating hypoxia. For patients with severeHAPE, hyperbaric oxygen is preferred. Some researchers[14, 15] have proposed mechanical ventilation for patientswith respiratory distress. Hyperbaric oxygen treatment notonly increases the oxygen concentration and subsequentlythe alveolar and arterial partial pressure of oxygen, but alsoincreases pulmonary ventilation and alveolar pressure, whichinhibit fluid exudation. Oxygen inhalation can also rectify
respiratory alkalosis, which prevents the transportation ofperipheral blood to the lung.
4.3.3. Nitric Oxide Inhalation. Experimental studies haveshown that hypoxia results in reduced nitric oxide levels,a principle cause of pulmonary vasoconstriction and thatinhalation of nitric oxide can reduce hypoxic pulmonaryhypertension, improve the patient’s ventilation to perfusionratio, improve hypoxemia, and improve HAPE in patientswith signs and symptoms, as well as decrease hospitalizationtime with few adverse effects. Accordingly, we suggest thatnitric oxide inhalation should be considered in the treatmentof HAPE. It should be administered via a nasal catheter ata dose of 10 ppm (0.001%) at a flow rate of 3–5 L/min for30 min in normal air or in oxygen.
4.3.4. Aminophylline. Aminophylline is a classic bronchod-ilator and has long been used in the treatment of HAPE.Aminophylline can dilate the bronchus, decrease hypoxicpulmonary hypertension, enhance diaphragm function, sup-press lipid peroxidation and hypoxia-induced pulmonaryvascular inflammation, enhance cardiac function and diure-sis, clear bronchial mucus, and subsequently resolve moistrales. Unlike other bronchodilators, aminophylline can dilateboth the bronchus and vascular smooth muscle; hence, itis preferred over other bronchodilators for the treatment ofHAPE.
4.3.5. Anticholinergics. Some hospitals use anisodamine(654-2) instead of aminophylline for the treatment of HAPE.Anisodamine can improve pulmonary vascular spasms, de-crease pulmonary vascular resistance and hypoxic pulmo-nary hypertension, improve the pulmonary microcircula-tion, and maintain smooth pulmonary blood flow. As aresult, anisodamine inhibits intravascular coagulation and,thus, reduces the risk of pulmonary embolism.
4.3.6. Nifedipine. Nifedipine is a calcium channel blockerthat inhibits release of catecholamines from sympatheticnerve endings. Therefore, it is an effective vasodilator,reduces hypoxic pulmonary hypertension, increases arterialoxygen tension, improves the symptoms and signs of HAPE,lowers right atrial pressure, and increases cardiac output.Therefore, nifedipine targets many of the effects of HAPE.
4.3.7. Dehydration and Diuresis. Hypoxia can lead to redis-tribution of systemic blood and abrupt increases in pul-monary blood volume. Furosemide and chlorothiazide notonly promote diuresis and dehydration, but also increaserenal blood flow and reduce left ventricular filling pressure.Thus, blood in the lungs is transported to the periphery,improving pulmonary congestion. In addition, oral aceta-zolamide can play a significant role in the treatment ofHAPE because it can increase urine output in patientswith HAPE or fluid retention. Acetazolamide is a carbonicanhydrase inhibitor that inhibits carbonic anhydrase activityin the brain, kidney, and blood. In the kidney, acetazolamidereduces the formation of hydrogen and bicarbonate ions and

Pulmonary Medicine 5
inhibits sodium bicarbonate reabsorption to increase urineoutput and, thus, reduce sodium and water retention. In thebrain, acetazolamide inhibits brain choroid plexus carbonicanhydrase activity to reduce cerebrospinal fluid productionrate and hence reduce intracranial pressure.
4.3.8. Dexamethasone. Dexamethasone is an analog ofadrenocortical hormones that can improve the functionsof capillary endothelial cells and alveolar epithelial cells,decrease pulmonary capillary permeability, protect alveolarepithelial type II cells, promote the secretion of pulmonarysurfactant, increase renal blood flow, and decrease thesecretion of antidiuretic hormone. Thus, dexamethasone isa key drug in the treatment of HAPE.
5. Early Prediction of HAPE
HAPE is a disease that is very difficult to predict. Althoughmuch research has been done in attempts to predict HAPE,no consensus has been reached regarding markers for theearly prediction of HAPE. However, many studies have sug-gested that HAPE could be predicted based on physiologicalfunctions, molecular biology, or genetic predisposition.
5.1. Physiological Parameters
5.1.1. Oxygen Saturation. Respiratory gas exchange disordersmay predict serious hypoxemia and even acute mountainsickness in individuals who rapidly ascend to high altitude.Thus, monitoring arterial oxygen saturation (SaO2) can beused to predict HAPE. Studies have shown that 80–100% ofpatients with serious hypoxemia develop HAPE. Accordingly,Roach et al. [16] speculated that noninvasive measurementof SaO2 was a simple and convenient way to predict theonset of HAPE. Similarly, Burtscher et al. [17] suggested thatmeasurement of SaO2 could be used to predict the onsetof acute mountain sickness. In a prospective cohort study,Shen et al. [18] found that there were significant individualdifferences in the changes in oxygen saturation with increasesin altitude. They found that when the SaO2 decreased by>30% at low altitude, the susceptibility to HAPE increasedmarkedly and about 62% of the participants developedHAPE. Thus, they speculated that a decrease in SaO2 > 30%offers a biomarker to predict susceptibility to HAPE.
5.1.2. Maximal Oxygen Uptake. Zhang et al. [19] used sub-maximal bench stepping to directly calculate maximal oxy-gen uptake (VO2max), which was then applied to predictHAPE. They conducted this study in soldiers ascending tohigh altitude. They found that soldiers with a VO2max ≥3 L/min at sea level were less likely to develop HAPE thanthose with a VO2max < 3 L/min.
5.1.3. Forced Vital Capacity (FVC). Wang and Zhou [20]measured FVC, body surface area, and thoracic volume inan effort to predict HAPE in individuals ascending to highaltitude. They found that a FVC/body surface area <3 L/m3,FVC/thoracic volume <400 L/m3, lung/body index >30, and
lung/thorax index >0.24 were associated with increased riskfor HAPE.
5.1.4. Pulmonary Diffusion Function. Geng et al. [21] investi-gated the diffusion of carbon monoxide (CO) in the lung of27 subjects who rapidly ascended from 2260 m to 4700 m.They found that CO diffusion was correlated with thedevelopment of acute mountain sickness. In 10 patients withHAPE, the diffusing capacity of CO (DLCO) increased withincreasing altitude, but the amplitude of this increase wasgreater in subjects without HAPE. Thus, they speculatedthat insufficient DLCO was a cause of acute mountainsickness and that DLCO is an objective parameter to predictadaptability to high altitude and the occurrence of HAPE.
5.1.5. Urine Volume after a Water Load. Huang et al. [22]measured urine volume within 2.5 h after participantsadministered 1000 mL of water at sea level in an effort topredict HAPE. They found that urine volume in subjectswho developed acute mountain response was significantlylower than that in the control group. In addition, the urinevolumes at 1, 1.5, 2, and 2.5 h after hydration and the totalurine volume within 1.5, 2, and 2.5 h after hydration werenegatively associated with AMS. They concluded that greaterurine volume within 2.5 h after hydration at sea level wasassociated with milder symptoms of acute mountain sicknessafter ascending to high altitude. Therefore, urine volumeafter hydration might be a marker for acute mountainsickness.
5.1.6. Blood Pressure and Blood pH. Zhou et al. [23] mea-sured the pH of blood in individuals before they ascendedto high altitude, in addition to PaCO2, and PaO2. Inthat study, the blood pH was significantly associated withsusceptibility to HAPE, and there was a significant differencein blood pH value between subjects who developed HAPEand without HAPE. They found that during intense physicallabor following a rapid ascent to 4000 m, the likelihood ofdeveloping acute mountain sickness was significantly greateramong individuals with blood pH > 7.45 than among thosewith blood pH < 7.45. However, they found no significantdifferences in PaCO2 or PaO2 between these two groups ofsubjects. Thus, they concluded that blood pH, but not PaCO2
or PaO2, could be used as a predictor of HAPE.
5.1.7. Ventilatory Function. Zhou et al. [24] investigatedthe ventilatory functions in 113 newly recruited soldiers atsea level, and then the soldiers were transferred to 3658 mby airplane. Two and three days after ascending to highaltitude, the investigators scored the symptoms of acutemountain sickness and evaluated the relationship betweenventilatory functions and symptom scores. They found thatFVC, peak expiratory flow, and forced expiratory volumein 1 second in soldiers with HAPE were significantly lowerthan those in soldiers without HAPE. Thus, they speculatedthat ventilatory functions at sea level could be used to screensubjects susceptible to HAPE.

6 Pulmonary Medicine
5.1.8. Cardiopulmonary Exercise Test. Wu and Li [25] investi-gated whether a cardiopulmonary exercise test could be usedto predict HAPE. They found that subjects with poor cardiacand ventilatory responses to hypoxia were more susceptibleto HAPE. They assessed several parameters, including theheart rate to oxygen saturation ratio (ΔHR/ΔSaO2) and theminute ventilation to oxygen saturation ratio (ΔVE/ΔSaO2),to establish a mathematical model that could predict HAPE.They established a discriminant model based on Z = b1X1 +b2X2, in which coefficients b1 = 0.00769, b2 = 0.0810, andZ0 = 0.472 (discrimination threshold). In this model, Z > Z0
is defined as non-AMS and Z < Z0 is defined as AMS. Thediscriminant model had a high sensitivity (93.9%) and a highaccuracy (92.2%) for the prediction of HAPE.
5.2. Endocrine Parameters. Endocrine parameters may alsobe used to predict HAPE. For example, Cai and Yang [26]used radioimmunoassays to measure the blood levels of18 endocrine parameters, including thyroid stimulatinghormone, adrenocorticotropic hormone, and corticotropinhormone, and found that plasma cortisol <20 µg/L and urine17-hydroxy corticosteroid (17-OHCS) levels <17 µmoL/dLcould predict HAPE with an accuracy >95%.
5.3. Molecular Biological Parameters. Luo et al. [27–29]compared the sequences of the mitochondrial genome inHAPE patients and rats at high altitude versus sequencesfrom healthy individuals at high altitude and animals atsea level, and identified single-nucleotide polymorphismsin nine genes in mitochondrial DNA (T6680C, C3970T,G3010A, A13497G, c15508T, G4164G, G1598A, C16111T,and T7684C). All of the affected genes encoded proteins con-trolling mitochondrial electron transport. Based on single-nucleotide polymorphism of mitochondrial DNA T6680C,DNA C3970T, and DNA G3010A, they developed a kit thatcan be used to predict susceptibility to HAPE. This kit canbe used to screen subjects for susceptibility to HAPE beforeascending to high altitude.
In another study, Qiu et al. [30] compared geneticparameters of patients with HAPE, as well as people living inTibetan and Han Chinese migrants. They found that humanleucocyte antigen (HLA) DR6, particularly DR6(1402), wasassociated with increased susceptibility to HAPE. Thus, theyspeculated that susceptibility to HAPE was not only related togenetic factors but was also influenced by some susceptibilitygenes.
6. Early Prevention of HAPE
Prevention of HAPE, as well as its associated symptomsand signs, is important to reduce its incidence amongthose ascending to high altitude. To achieve this, thefollowing factors are particularly important. (1) Maintainbody warmth with appropriate insulation and avoid upperrespiratory tract infection. Several days before ascending tohigh altitude, bathing should be avoided to reduce exposureto cold temperatures. (2) Avoid fatigue. Physical activity athigh altitude should be performed at an intensity of no more
than 60–80% of that at sea level and duration of activityshould be <6 h. Similarly, the body must be given sufficienttime to rest both before and during the time at high altitude.(3) Stop alcohol intake. Fifteen days before ascending to highaltitude, the consumption of alcohol should be stopped. (4)Emotional stress. Unwanted emotional tension should beavoided, while optimism and aggressiveness should be main-tained. (5) Patients with upper respiratory tract infectionshould be carefully monitored before and during the time athigh altitude. However, delaying the ascent until the infectionhas been fully resolved is preferable. (6) Oxygen must beavailable at high altitude, either by maintaining high oxygenlevels in living quarters or by supplying compressed oxygentanks for use during physical activity. (7) Food and watersanitation. Diets containing high levels of carbohydrates andprotein and low levels of fat are recommended. The intake ofvitamins can also be increased. (9) The use of drugs such asRhodiola rosea, Zangtianlu, Codonopsis compound tablets,Shenqi pollen tablets, and acetazolamide during the time athigh altitude can also reduce the risk of HAPE.
For people working at high altitude, such as constructionworkers, preventative measures are particularly important.As outlined above, it is essential to provide sufficientnutrients, rest, and insulation against the cold, as well as tolimit labor intensity and duration of labor to avoid fatigue.Shift-work is also recommended and may entail 20–30 daysof work at high altitude followed by a period of rest atlow altitude to provide more effective resting conditions.Shift-work also reduces the incidence of chronic mountainsickness induced by long periods of physically demandingwork at high altitude. It is also essential to ensure there isan adequate medical team to enable early detection, diag-nosis, and treatment, should mountain sickness of HAPEoccur.
Finally, individuals planning on ascending to high alti-tude should receive education regarding the prevention andtreatment of HAPE and take appropriate measures [31] todecrease the risk of developing HAPE: maintain a positiveattitude after ascending to high altitude take measures toprevent HAPE, and consider the possible treatments beoptimistic but do not fear high altitude maintain bodytemperature avoid hyperphagia stop smoking and alcoholconsumption conduct appropriate excise but avoid strenuousexercise and fatigue do not worry about trouble sleeping buttry to maintain good sleep quality pay attention to cough,particularly cough event of bloody sputum and considerseeking treatment consider bed rest and oxygen inhalationbe aware that headache, vomiting, and unsteady walking aresymptoms of HAPE and should be checked by a physician;treatment should be started as soon as possible, even if thesymptoms are mild, as timely and comprehensive treatmentfavors positive outcomes.
References
[1] Z. Q. Hu, “High altitude pulmonary edema,” National MedicalJournal of China, vol. 9, pp. 727–729, 1963.
[2] T. Singh, “High altitude pulmonary edema,” Lancet, vol. 1, pp.229–231, 1965.

Pulmonary Medicine 7
[3] B. Basnyat, D. Subedi, J. Sleggs et al., “Disoriented and ataxicpilgrims: an epidemiological study of acute mountain sicknessand high altitude cerebral edema at a sacred lake at 4300 m inthe Nepal Himalayas,” Wilderness & Environmental Medicine,vol. 11, no. 2, pp. 89–93, 2000.
[4] Y. Ren, Z. Fu, W. Shen et al., “Incidence of high altitudeillnesses among unacclimatized persons who acutely ascendedto Tibet,” High Altitude Medicine & Biology, vol. 11, no. 1, pp.39–42, 2010.
[5] T. Y. Wu, “Evaluation of criteria for the diagnosis of highaltitude diseases,” Journal of High Altitude Medicine, vol. 5, no.3, pp. 3–8, 1995.
[6] Q. Q. Zhou, Y. J. Luo, H. Li et al., “Epidemiologicalstudy of mountain sickness complicated with multiple organdysfunction syndrome on the Qinghai-Tibetan Plateau: reportof 103 cases,” Scientific Research and Essays, vol. 5, no. 17, pp.2506–2516, 2010.
[7] S. Z. Li, Y. L. Wang, C. C. Yan et al., “Diagnostic criteria forhigh altitude pulmonary edema in the early stage,” MilitaryMedical Journal of South China, vol. 24, no. 3, pp. 161–165,2010.
[8] J. Y. Yang, W. Y. Wei, X. P. Wang et al., “Grading andon-site treatment of acute high altitude pulmonary edema:experience from 54 patients,” Chinese Journal of Tuberculosisand Respiratory Diseases, vol. 9, no. 2, pp. 92–94, 1986.
[9] S. Z. Li, B. H. Zheng, C. C. Yan et al., “Four therapeutic regi-mens for high altitude pulmonary edema: result comparisonand preliminary study of standardized treatment,” MedicalJournal of National Defending Forces in Southwest China, vol.20, no. 7, pp. 771–774, 2010.
[10] J. Y. Yang and F. S. Wang, “On-site treatment of acute highaltitude deseases,” People’s Military Surgeon, vol. 3, pp. 8–10,1993.
[11] D. M. Zhang, Q. Q. Zhou, and J. Y. Yang, “A clinical analysis of306 cases acute high altitude pulmonary edema treated on thespot in high altitude regions,” West China Medical Journal, vol.16, no. 2, pp. 208–209, 2001.
[12] K. Zafren, J. T. Reeves, and R. Schoene, “Treatment of high-altitude pulmonary edema by bed rest and supplementaloxygen,” Wilderness & Environmental Medicine, vol. 7, no. 2,pp. 127–132, 1996.
[13] M. Xinbing, L. Suzhi, G. Yuqi et al., “Haemodynamic changesin high altitude pulmonary edema and effects of oxygenbreathing,” Chinese Journal of Pathophysiology, vol. 19, no. 8,pp. 1106–1108, 2003.
[14] X. Yuanda, J. Mei, X. Zheng lun et al., “Noninvasive ventilationfor treatment of acute respiratory failure secondary to severeacute respiratory syndrome,” Chinese Journal of Respiratoryand Critical Care Medicine, vol. 9, no. 6, pp. 575–579, 2010.
[15] S. Q. Ma, S. Z. Wu, Z. P. Yang et al., “Treatment of highaltitude pulmonary edema combined with secondary adultrespiratory distress syndrome and monitoring of oxygendynamics,” Medical Journal of National Defending Forces inNorthwest China, vol. 31, no. 2, pp. 89–91, 2010.
[16] R. C. Roach, E. R. Greene, R. B. Schoene, and P. H. Hackett,“Arterial oxygen saturation for prediction of acute mountainsickness,” Aviation Space and Environmental Medicine, vol. 69,no. 12, pp. 1182–1185, 1998.
[17] M. Burtscher, M. Flatz, and M. Faulhaber, “Prediction of sus-ceptibility to acute mountain sickness by SaO2 values duringshort-term exposure to hypoxia,” High Altitude Medicine &Biology, vol. 5, no. 3, pp. 335–340, 2004.
[18] Q. Shen, Y. J. Sun, Y. Qi et al., “Magnitude of SaO2 decreasingwith increasing altitude as a biomarker to predict HAPE
occurred at high altitude,” Journal of Medical Research, vol. 38,no. 7, pp. 29–31, 2009.
[19] X. Z. Zhang, S. P. Zhang, Z. J. Zhou et al., “Application ofmaximal oxygen uptake at sea level in the prediction of acutemountain sickness: an experimental study,” Medical Journal ofNational Defending Forces in Northwest China, vol. 17, no. 4,pp. 279–280, 1996.
[20] L. A. Wang and Q. Q. Zhou, “Predictive importance of forcedvital capacity to susceptive population of acute mountainsickness,” West China Medical Journal, vol. 18, no. 2, p. 231,2003.
[21] D. Geng, R. L. Ge, Z. G. Wang et al., “Measurement ofpulmonary diffusion capacity as a method evaluating acutemountain response in men exposed rapidly to high altitude,”Journal of High Altitude Medicine, vol. 5, no. 1, pp. 53–54,1995.
[22] Q. Y. Huang, Y. Q. Gao, F. Y. Liu et al., “Correlation betweenthe amount of urine excreted after water lod at sea level andthe symptomatic scores of AMS,” Journal of High AltitudeMedicine, vol. 13, no. 3, pp. 2–4, 2003.
[23] B. Zhou, Q. Q. Zhou, and J. Y. Yang, “Prediction of blood acid-base scale to the susceptible population with acute mountainsickness,” West China Medical Journal, vol. 21, no. 4, pp. 284–285, 2004.
[24] Q. Q. Zhou, Y. Q. Gao, Q. Y. Huang et al., “Predictive effect oflung functional determination of the population susceptibleto acute mountain sickness,” Medical Journal of NationalDefending Forces in Northwest China, vol. 25, no. 1, pp. 13–15,2004.
[25] T. Y. Wu and W. S. Li, “Cardiopulmonary exercise test forthe evaluation of acute mountain sickness,” Chinese Journal ofApplied Physiology, vol. 8, no. 4, pp. 289–293, 1992.
[26] W. C. Cai and J. Y. Yang, “Role of 18 endocrine parametersin the prediction of acute mountain sickness in susceptiblepopulation,” Ningxia Medical Journal, vol. 12, no. 6, pp. 348–350, 1990.
[27] Y. Luo, W. Gao, Y. Gao et al., “Mitochondrial genome analysisof Ochotona curzoniae and implication of cytochrome coxidase in hypoxic adaptation,” Mitochondrion, vol. 8, no. 5-6, pp. 352–357, 2008.
[28] Y. Luo, S. Tang, W. Gao et al., “Genotyping mitochondrialDNA single nucleotide polymorphisms by PCR ligase detec-tion reactions,” Clinical Chemistry and Laboratory Medicine,vol. 48, no. 4, pp. 475–483, 2010.
[29] W. Gao, Y. Gao, G. Zhang, L. Song, B. Sun, and J. Shi,“Hypoxia-induced expression of HIF-1alpha and its targetgenes in umbilical venous endothelial cells of Tibetans andimmigrant Han,” Comparative Biochemistry and PhysiologyPart C, vol. 141, no. 1, pp. 93–100, 2005.
[30] C. C. Qiu, T. C. Zhu, Y. J. Sun et al., “Molecular genetic studyof different susceptibility to high altitude pulmonary edema,”Chinese Journal of Applied Physiology, vol. 21, no. 3, p. 11, 2005.
[31] Q. Q. Zhou, “How to practice scientific remedy in highaltitude—about medical rescue after intense earthquake inYushu Qinghai,” Chinese Journal of New Drugs, vol. 19, no. 8,pp. 1–3, 2010.

Hindawi Publishing CorporationPulmonary MedicineVolume 2011, Article ID 275857, 9 pagesdoi:10.1155/2011/275857
Review Article
Pulmonary Edema in Healthy Subjects in Extreme Conditions
Erika Garbella,1, 2 Giosue Catapano,1 Lorenza Pratali,3 and Alessandro Pingitore2, 3
1 Clinical Physiology Institute, CNR, Via Moruzzi 1, 56124 Pisa, Italy2 Fondazione G. Monasterio, CNR, Regione Toscana, Via Moruzzi 1, 56124 Pisa, Italy3 Extreme Center, Scuola Superiore S. Anna, Piazza Martiri della Liberta 33, 56127 Pisa, Italy
Correspondence should be addressed to Alessandro Pingitore, [email protected]
Received 16 November 2010; Accepted 27 April 2011
Academic Editor: David J. Feller-Kopman
Copyright © 2011 Erika Garbella et al. This is an open access article distributed under the Creative Commons Attribution License,which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
There are several pieces of evidence showing occurrence of pulmonary edema (PE) in healthy subjects in extreme conditionsconsisting of extreme psychophysical demand in normal environment and psychophysical performances in extreme environment.A combination of different mechanisms, such as mechanical, hemodynamic, biochemical, and hypoxemic ones, may underlie PEleading to an increase in lung vascular hydrostatic pressure and lung vascular permeability and/or a downregulation of the alveolarfluid reabsorption pathways. PE can be functionally detected by closing volume measurement and lung diffusing capacity test todifferent gases or directly visualized by multiple imaging techniques. Among them chest ultrasonography can detect and quantifythe extravascular lung water, creating “comet-tail” ultrasound artefacts (ULCs) from water-thickened pulmonary interlobularsepta. In this paper the physiopathological mechanisms of PE, the functional and imaging techniques applied to detect and quantifythe phenomenon, and three models of extreme conditions, that is, ironman athletes, climbers and breath-hold divers, are described.
1. Introduction
Pulmonary edema (PE) is a life-threatening condition thatmay lead to acute respiratory failure. There are severalpieces of evidence showing the occurrence of PE in healthysubjects in extreme environment and/or under extremepsychophysical stress [1–3]. Human extreme conditions canbe considered in terms of extreme psychophysical demandin normal environment, such as for ironman athletes,or in terms of psychophysical performances in extremeenvironment, such as for climbers or breath-hold deepdivers (Figure 1). Susceptibility to PE has been shown to berelated to pulmonary hemodynamics and ventilatory drive(precisely reduced hypoxic ventilatory response), that leadto a greater hypoxic stimulus and/or a pulmonary hemo-dynamic hyperresponse to the above-mentioned extremeconditions. Finally, a combination of different and not well-defined yet mechanisms, such as mechanical, hemodynamic,biochemical, and hypoxemic ones, may underlie PE, leadingto a greater increase in lung vascular hydrostatic pressure(either heterogeneous or not), an increase in lung vascularpermeability, and/or a downregulation of the alveolar fluidreabsorption pathways.
PE can be functionally detected by an increase in closinglung volume (the volume at which small airways startclosing), reflecting an early small airways compression dueto pulmonary interstitial fluid accumulation [4]. Anotherfunctional method is the lung diffusing capacity test (DL)to different gases (carbon monoxide, CO and nitric oxide,NO), being expression of the alveolar-capillary membraneintegrity [5]. Moreover PE can be directly visualized bymultiple imaging techniques, such as chest radiography,computed tomography (CT), magnetic resonance (MR),and chest ultrasonography [2, 6]. Among these, chestultrasonography detects and quantifies extravascular lungwater, creating “comet-tail” ultrasound artefacts (ULCs)from water-thickened pulmonary interlobular septa [7]. Thistechnique is suitable, versatile, not invasive, nonionizingand hand portable, a fundamental option when studyingsubjects directly on the field and not in a dedicated imaginglaboratory.
In this paper the physiopathological mechanisms of PE,the functional and imaging techniques applied to detect andquantify the phenomenon, and three models of extremeconditions, that is, ironman athletes, climbers and breath-hold divers, are described.

2 Pulmonary Medicine
Chestultrasonography
Clim
bers
ath
igh
alti
tude
Gor
ak-s
hep
(513
0m
)
(a)
Models of extremeconditions
(b)
Ultrasound lung comets(ULCs)
(c)
Iron
man
atlh
etes
atse
ale
vel
Pis
a(3
0m
)
(d) (e) (f)
Div
ers
un
der
sea
Shar
m-E
l-Sh
eik
(−11
2m
)
(g) (h) (i)
Figure 1: Three different models of extreme conditions: climbers at 5130 meters above sea level; ironman athletes at sea level; breath-holddiver at –112 meters under sea level. In all the above-mentioned conditions subjects were monitored by chest ultrasonography that showedthe presence of ULCs.
2. Physiopathology
The pulmonary blood-gas barrier is continuously subjectto mechanical stress. Precisely its integrity depends onbalance between circumferential tension (related to thecapillary transmural pressure and the radius of capillary’scurvature), longitudinal tension in the alveolar wall elements(related to the inflation of the lung), and surface tensionof the alveolar lining layer [8, 9]. Therefore, “stress failure”describes mechanically induced breaks in the blood-gasbarrier. In the last years, West and others have reporteda great deal of experimental data describing the effectsof mechanical stress on the lung [10–12]. Vulnerability topulmonary capillary stress failure varies between species andincreases at high lung inflation [13]. Exercise increases thepotential risk of pulmonary capillary stress failure. In factincrease in pulmonary arterial pressure together with active
expiration and increased lung inflation resulting from itexert mechanical forces on the pulmonary microvasculature.Moreover pulmonary capillary stress failure is associatedwith an increased permeability to protein and red bloodcells, as shown by their increased concentration in thebronchoalveolar lavage fluid [14]. Another physiologicalmechanism that potentially augments pulmonary capillarypressure is the uneven vasoconstriction of the pulmonaryarteries, resulting in heterogeneous distribution of theblood flow within the vascular bed and thus in a regionalcapillaries’ overperfusion (i.e., in areas with the least arterialvasoconstriction) [15, 16]. Moreover, once the drop ofalveolar oxygen tension is detected by oxygen sensors locatedin the pulmonary vasculature, it follows vasoconstrictionof both small pulmonary arteries and pulmonary veins[17–19]. Physiologically, inhibition of voltage-dependentpotassium channels, membrane depolarization, and calcium

Pulmonary Medicine 3
entry through L-type calcium channels are involved in theresponse to acute hypoxia of smooth-muscle cells in thepulmonary vasculature, that begins within few seconds [18,20]. However it remains to be determined if constitutivelydecreased mRNA expression or an acquired transcriptionaldefect of voltage-dependent potassium channels proteinis at the origin of oedema susceptibility. On the otherhand the regional hypoxic vasoconstriction, that leads toa nonhomogeneous distribution of pulmonary blood flow,thus possibly to lung edema, could be explained eitherby an uneven distribution of alveolar ventilation or aheterogeneous oxygen sensing within pulmonary vasculaturesmooth muscle cells [21–24]. Furthermore, also a consti-tutionally pulmonary vascular hyperreactivity to hypoxiaseems to have an important role behind lung edema. Infact hypoxia has been shown to impair, in predisposed sub-jects, systemic endothelial function, resulting in decreasedbioavailability of NO and its second messenger cGMP, thatis likely to contribute to the enhanced hypoxic pulmonaryvasoconstriction [14, 25, 26]. Moreover other factors maybe involved in vascular hyperreactivity to hypoxia, suchas a sustained elevation of cytoplasmic calcium concen-tration, sympathetic activity, hypersecretion in the pul-monary circulation of vasoconstrictor mediators (e-selectin,endothelin-1), and reduced activity of protective enzymaticproducts of hemooxigenase-1 (inhibitors of hypoxia-inducedvasoconstrictive and proinflammatory pathways) [27–31].Finally another factor that may be involved in alveolar fluidaccumulation and PE severity is a downregulation of thesodium-water transport pathway that leads to reduction innet alveolar fluid reabsorption [32].
Besides the local pulmonary mechanisms of PE, sys-temic factors may also predispose to PE. Exercise-associatedhyponatremia, due to altered body fluid homeostasis, rep-resents emerging potential cause of both PE and cerebraledema [33]. Several mechanisms have been considered.Hyponatremia may be the consequence of either sodiumdepletion, as in salty sweaters without adequate salt intake,or sodium dilution, secondary to excessive water intake[34, 35]. Interestingly a variant of the syndrome of inap-propriate antidiuretic hormone secretion, with a hyper-secretion of arginine vasopressin, has also been implicatedas a mechanism of exercise-associated hyponatremia [36].Sodium depletion would lead to hypoosmolar hyponatremiaaccompanied by hypovolemia and urine concentration,whereas dilutional hyponatremia is accompanied by euv-olemia or hypervolemia and dilute urine. Moreover, theabove-mentioned dilutional hyponatremia contrasts withthe one mediated by inappropriate arginine vasopressonsecretion, that is characterized by less than maximally diluiteurine, natriuresis marked by a urinary Na concentration,and measurable plasma levels of arginine vasopressin [35].Further a nonosmotic stimulation of arginine vasopressinis the enhanced release of muscle-derived interleukin (IL) 6during glycogen depletion, as documented by administrationof recombinant IL-6 in healthy subjects [37].
Perivascular inflammatory cell infiltration as well asincreased serum levels of proinflammatory IL-1β and IL-6has been reported in clinical cases of primary pulmonary
hypertension but it is not fully clear up to now therole of pulmonary inflammation in the pathogenesis ofacute PE in healthy subjects under extreme psychophysicalconditions. Exhaustive endurance exercise leads to systemicinflammatory response secondary to metabolic, hormonal,thermal stress, and muscle damage thus potentially affectingmicrovascular endothelial function and lung tissue integrity.Moreover, in endurance athletes the activation of the inflam-matory cascade within six hours from the end of strenuousexercise has been associated with a reduction in ventilatoryperformance [38].
3. Pulmonary Function Tests
It is well known that prolonged heavy exercise increaseslung ventilo-perfusive heterogeneity and affects the efficiencyof gas exchange [21, 39]. The effect of repeated exerciseon pulmonary gas exchange has been used to elucidate theimportance of structural versus functional mechanisms asa cause for the gas exchange impairment during exercise.Several authors have suggested that sustained exercise ofmaximum or near maximum effort might result in astructural injury (stress failure) of the alveolar-capillarymembrane, likely when pulmonary arterial pressures is over40 mmHg [10, 11, 39, 40]. Moreover stress failure maylead to increased fluid permeability and to edema. Finally,PE seems to worsen gas exchange in terms of arterialblood oxygen content (decrease in oxygen partial pressureand/or haemoglobin saturation), only at advanced stages,that is during alveolar edema [41]. Instead, early subclinicalphases of interstitial edema can be functionally detected byincrease in closing volume and/or reduction in DLCO [4,5]. Indeed DLCO reflects the alveolar-capillary membraneintegrity condition, being the expression of the CO passagethrough the alveolar-capillary membrane and into theplasma and the erythrocytes, as defined by the Roughton andForster equation. DLCO is thus expected to be persistentlyreduced in case of thickening of the alveolar-capillary wall(interstitial oedema), while temporarily increased duringblood shift and persistently and consistently increased incase of alveolar haemorrhage [42]. Moreover, DLNO isthought to represent the true membrane diffusing capacityas it is not dependent from pulmonary capillary bloodvolume and flow because of its very high affinity forhaemoglobin. Therefore, DLNO/DLCO ratio can be used todifferentiate between thickened alveolocapillary membrane(DLNO and DLCO are both decreased; DLNO/DLCO ratiois normal) and decreased perfusion of ventilated alveoli(DLNO less decreased than DLCO, DLNO/DLCO ratio ishigh) showing the presence of ventilo-perfusive mismatch[5]. Finally the rationale for measuring closing volume todetect early PE is that increased pulmonary extravascularfluid would be expected to early compress airways andthus increase the volume at which small airways close [43].The method based on Guy’s single breath techniques, thatdoes not require foreign inert gases or 100% of oxygen,can be used to measure closing volume with hand-portableequipment directly at the place of the extreme performance[44].

4 Pulmonary Medicine
4. Imaging Techniques
Radiographic, CT, or MRI imaging resulted equally effectivein detecting PE induced by exhaustive endurance sports [2].Since increased blood flow after exercise may be misdiag-nosed as edema, time elapse of at least 30 minutes betweenthe end of exercise and the postexercise imaging has beensuggested to allow normalization of pulmonary capillaryblood flow and volume [45]. Despite a large range time ofPE evaluation after exercise (from 2 minutes to 2 hours),no differences in the frequency of edema have been reportedsuggesting that PE occurs during and not following exercise[2]. However, since the lung has been shown to recoverrapidly from hydrostatic-induced pulmonary damage, thatis, when pulmonary capillary transmural pressure backsto normal, the incidence of edema formation may beunderestimated by imaging techniques and it may be difficultto be quantified after exercise. By the way, in early stageof high-altitude PE (HAPE) chest radiographs showed apatchy, peripheral distribution of edema that becomes morehomogeneous and diffuses in advanced cases and duringrecovery [46].
Immersion PE has been seen in the dependent lung onCT scans (in special forces combat swimmers at the lateraldecubitus position and in elite breath-hold divers at thelevel of the superior as well as parahilar zones bilaterally)whereas recurrent HAPE has showed patchy distributionof pulmonary infiltrates bilaterally on chest radiographsand on CT scans. These last findings strongly support theheterogeneous distribution of elevated capillary pressures,that in summary is likely to rely on an unevenly distributedhypoxic vasoconstriction in either pulmonary arteries orveins, or both.
The technical developments and the use of high-field-strength MR have improved the image quality, with a bettersignal-to-noise ratio, and the speed of acquisition of MRimaging, overwhelming the motion artefact due to heart andlung movements and susceptibility due to the presence ofair in the lung. MR can give in the same exam informationregarding both tissue characterization (in this context thepresence of pulmonary fluid accumulation) and perfusion.In the clinical practice lung MR has comparable sensitivity toCT for the detection of lung diseases with MR having lowerspatial but greater contrast resolution than CT [2, 47]. MRarterial spin labeling measures of pulmonary perfusion havebeen used to detect the ventilo-perfusive mismatch, that isknown to increase under strenuous exercise, relating spatialperfusion heterogeneity to the exercise-induced changesin ventilation distribution. When exposed to normobarichypoxia, HAPE-susceptible subjects have showed a more het-erogeneous regional pulmonary blood flow than individualswithout HAPE. These novel data suggest that uneven hypoxicpulmonary vasoconstriction is an important feature of sub-jects developing HAPE [16]. Despite the high accuracy of CTand MR in detecting PE, both techniques suffer of limitationsconsisting of high costs, low availability, exam complexity,duration, and, only for CT, ionizing exposure, that makethem not suitable for studying healthy subjects on the field.Differently, chest ultrasonography is a highly performable
imaging technique for its low time exam consuming, lowcost, high versatility and availability. The “ultrasound comet-tail image” is an echographic image detectable by a cardiacultrasound probe positioned over the chest. This imageconsists of multiple comet tails fanning out from the lungsurface. They originate from water-thickened interlobularsepta, and they give quantification of the extravascular lungwater excess. They also provide an indirect measurementof pulmonary wedge pressure and a sensitive and accuratedetection of even early subclinical interstitial edema. In a pigmodel of oleic-acid-induced lung injury, that mimics humanAcute Respiratory Distress Syndrome, ULCs unmaskedaccumulation of extravascular lung water, then verifiedhistologically, very early in the course of lung injury, evenat a stage when no changes in hemogasanalytic parameterscould be observed [48]. In clinical practice there is a greatpotential for this hand-portable technology that allows toquantify lung edema in real time, noninvasively, and with aradiation-free method [49]. In a head-to-head simultaneouscomparison study of chest radiographs and ULCs, a linearcorrelation between echocardiographic comet score andradiologic lung water score (r = .78; P < .01) was found[6]. Further, ULCs have been proven useful in the differentialdiagnosis of dyspnoea of uncertain cause at the EmergencyRoom and for risk stratification in patients with heart failureor admitted with acute coronary syndrome [50–53]. Thetechnique requires ultrasound scanning of the anterior rightand left chest, from the second to the fifth intercostal space. Itis simple (with a learning curve of less than 10 examinations)and fast to perform (requiring less than 3 minutes), and itis independent of the cardiac acoustic window. It requiresvery basic 2D technology imaging, even without a secondharmonic or Doppler. The great advantage of this methodis the versatility that allows to study free divers and climbersin their natural home, the sea and the mountains.
5. Extreme Psychophysical Performance inNormal Environment
Ironman race is also called ultratriathlon and consists ofthe following three different endurance sports: swim (2.4miles, 3.86 km), bike ride (112 miles, 180 km), and marathon(26.2 miles, 42.2 km). This multidisciplinary sport demandsan extraordinary psicophysical performance in terms ofboth endurance and exercise intensity. Reversible changesin the cardiovascular system, consisting of biohumoral andfunctional signs of cardiac damage have been documentedafter an ironman race. In particular there is an increase incardiac troponins and B-type natriuretic peptide in presenceof impairment of regional and global cardiac performance[54]. Indeed exhaustive endurance exercise induces ultra-structural damage of muscle tissue and release of metabolic,hormonal, thermal, and oxidative stress factors, which cangive rise to systemic inflammatory and immune systemresponse [55, 56]. Particularly after a triathlon race there isevidence of augmented proinflammatory interleukins (suchas IL-8, IL-6, TNF-alpha, IL-1B), that are also markers ofincreased vascular permeability and bronchial inflammation[57–59].

Pulmonary Medicine 5
100
95
90
85
80
75
70
0 3440 4800 5130 1350
Quotes (m s.I.)
97± 1.5
91± 2.1
81.8± 4.5
84.1± 3
97± 1.7
P < .001
P < .001P < .001
O2
satu
rati
on(%
)
(a)
O2 saturation (%)
60
50
40
30
20
10
0
70 75 80 85 90 95 100
R = −0.7;P < .001
Lun
gco
met
s
(b)
Absent
“Black lung”
(c)
Mild Moderate
“Black and white lung”
(d)
Severe
“White lung”
(e)
Figure 2: Progressive O2 saturation reduction at increasing altitude above sea level. Inverse correlation between O2 saturation and lungcomets. Increase number of ULCs from sea level to 5130 meters above sea level (Pratali et al. [64]).
The likelihood of developing clinical PE is at least 65% inpresence of maximum or near-maximum effort, whereas it islow or absent in presence of submaximal exercise. In this con-text interstitial PE has been detected by various imaging tech-niques, such as TC scan, MR, chest ultrasonography, as wellas by a decline in lung function (particularly of vital capacityand flow rates at mid and low lung volumes) and impairmentof the pulmonary blood gas-barrier gas exchange, that isreduction in DL [10, 60, 61]. Furthermore the increase insmall airways flow resistance, likely related to extravascu-lar lung water accumulation, has been associated to theincrease in systemic cytokine levels [58, 62]. In our studyon ultratriathlon athletes a significant increase in ULCs,partially reduced after 12 hours, has been documented afterexhaustive exercise. In parallel at the acute phase there wasa significant decrease in spirometric indices of big and smallairways flows and lung volume (remaining within the normalrange values) and in ventilatory performance, and that resultwas also influenced by the inflammatory cascade [63].
6. Psychophysical Performances inExtreme Environment
Combination of mechanical, hemodynamic, biochemical,and hypoxemic mechanisms seems to be behind the PE
in both hypoxic hypo- and hyperbaric conditions (high-altitude and breath-hold deep diving), leading to an increasein both lung vascular hydrostatic pressure (either heteroge-neous or not) and permeability.
Breath-hold diving causes hyperbaric and hypoxic stresson the cardiopulmonary system [65, 66]. Peripheral “bloodshift” into the intrathoracic cavity is a well-known physio-logical response which prevents chest wall from collapsingat depth, particularly at low lung volumes [67, 68]. Boththe acute increase in pulmonary arterial pressure due toblood shift and the reduction in gas-lung volume withdepth challenge the pulmonary capillary system. Increasedintravascular pressure and especially transcapillary pressuremay stretch the wall, weaken its integrity, and reduce naturalvessel ability to sustain high mechanical stress [69]. A furtherincrease in capillary pressure may cause the rupture ofthe alveolar-endothelial membrane, till leading to alveolarhaemorrhage [8, 40, 70].
An additional potential mechanism responsible for suchstress is the pulmonary vasoconstriction secondary tobreath-holding hypoxia, with similarity to HAPE. BehindHAPE, physical exertion associated with hypoxic vasocon-striction may lead to an uneven redistribution of pulmonarycapillary blood and ventilation, further leading to ventilo-perfusive mismatch that ultimately affects pulmonary gas

6 Pulmonary Medicine
Rest After diving 24 hoursafter diving
0
50
100
(a)
Baseline
(b)
Early after diving
(c)
24 hours after diving
(d)
Figure 3: Chest ultrasonography revealed an increased number of ULCs within 10 minutes after immersion in 45% of 14 top-level breath-hold deep divers, which resolved completely after 24 hours (Frassi et al. [71]).
exchange [21, 72]. West proposed that stress failure mightbe the initial factor for HAPE as seen in experimental animalmodels [73, 74]. According to this hypothesis recent studieshave shown that the initial leak in HAPE is likely notinflammatory but related to increased hydrostatic pressure,with an alveolar increase in inflammatory mediators onlyat advanced stages, secondary to the high-pressure injury tothe blood-gas barrier and/or PE formation [14]. In contrast,another study documented an increase in inflammatorymediators (IL-1B, IL-6, IL-8, and TNF-alpha) in broncoalve-olar lavage fluid already at the early stage of HAPE [75]. Inour study on recreational climbers, Chest ultrasonographyrevealed a high prevalence of clinically silent ULCs, thatincreased during ascent. In fact ULCs were present in83% of subjects at 3440 m above sea level and in 100%of subjects at 4790 m above sea level, always with normalleft and right ventricular function. Furthermore, ULCswere mirrored by decreased oxigen saturation (Figure 2),whereas no statistically significant correlation with systolicpulmonary arterial pressure rise during ascent was observed.Finally, ULCs decreased at descent [64].
Besides perplexities about mechanisms underlying PEin extreme environment and hypoxic conditions anotherproblem is how early interstitial PE can be detected andmeasured. For example, there is the evidence that 92% ofrecreational climbers presenting chest rales or interstitial
edema on the chest radiograph after ascent had increasedclosing volume. Furthermore 74% of climbers with noclinical or radiological evidence had probable subclinicaledema, having an increase in closing volume at altitude (withno change in vital capacity) [4].
Chest ultrasonography revealed an increased number ofULCs within 10 minutes after immersion (depth range 31to 112 meters) in 45% of 14 top-level breath-hold deepdivers, which resolved completely after 24 hours (Figure 3).Of these, 2 had specific clinical symptoms, indicating arelatively high prevalence of subclinical extravascular lungwater accumulation after breath hold deep diving [71]. Inanother study we measured DLCO to investigate the blood-gas barrier integrity after deep (30 meters) breath-holddiving at different time points (basely, within 2 minutespost dive, after 10 and 25 minutes). The early but transientincrease in DLCO after diving in all subjects supported thehypothesis of intrathoracic capillary pooling of red bloodcells (blood shift). Persistence at 25 minutes of high valueof DLCO in one subject could be attributed to extravasationof blood into the alveoli by CT scan. In other 5 subjects, alate (at 25 minutes) decrease in DLCO more than 10% belowthe baseline, together with symptoms of dizziness in 3 ofthem, strongly suggested the presence of interstitial edema[3]. Furthermore we evaluated whether a hyperbaric stresscondition associated to a prevalent hypoxic condition, as

Pulmonary Medicine 7
induced by a maximal static breath holding at 10 metersdepth, may influence the integrity of the alveolar-capillarymembrane and lung ventilo-perfusive heterogeneity. Accord-ingly we employed both DLCO and DLNO measurementbasely, at 2-10-25 minutes after dive. We found an early (at2 minutes) but transient increase in DLCO, likely indicatingthe persistence of capillary pooling of red blood cells fol-lowing emersion (blood shift). This hypothesis was furthersupported by a parallel stable trend of DLNO, as expectedbeing DLNO not affected by blood volume and flow. FinallyDLNO significantly increased at 10 minutes likely secondaryto pulmonary blood redistribution and thus probably reflect-ing a condition of ventilo-perfusive mismatch. Significantdecrease of both DLNO and DLCO at 25 minutes stronglysupported the hypothesis of alveolar-capillary membranedistress until interstitial fluid accumulation that is thecondition affecting lung diffusive function [76].
7. Conclusions
Lung fluid accumulation in healthy subjects during theabove-mentioned extreme conditions is a complex andmultifactor phenomenon, still with unanswered questions.In particular whether the acute, reversible increase inlung fluid content is an innocent and benign part of theadaptation to extreme physiological condition or ratherthe clinically relevant marker of an individual vulnerabilityto life-threatening PE remains to be established in futurestudies. Thus the question if encouraging more conservativehabits is right or not remains open. Chest ultrasonographyis a low-cost highly feasible and versatile, nonionizing andnoninvasive technique, with the undiscussed advantage tobe used on the field early after exercise and repeated inthe followup on a large sample of subjects. Further, chestultrasonography has the potential to detect even subclinicalepisodes of lung fluid accumulation, thus it can providenew features on physiological mechanisms, incidence, andprogression of this phenomenon with the final goal toidentify vulnerable subjects.
References
[1] P. Bartsch, H. Mairbaurl, M. Maggiorini, and E. R. Swenson,“Pulmonary circulation and hypoxia. Physiological aspects ofhigh-altitude pulmonary edema,” Journal of Applied Physiol-ogy, vol. 98, no. 3, pp. 1101–1110, 2005.
[2] G. S. Zavorsky, “Evidence of pulmonary oedema triggered byexercise in healthy humans and detected with various imagingtechniques,” Acta Physiologica, vol. 189, no. 4, pp. 305–317,2007.
[3] R. Prediletto, E. Fornai, G. Catapano et al., “Time course ofcarbon monoxide transfer factor after breath-hold diving,”Undersea and Hyperbaric Medicine, vol. 36, no. 2, pp. 93–101,2009.
[4] G. Cremona, R. Asnaghi, P. Baderna et al., “Pulmonaryextravascular fluid accumulation in recreational climbers: aprospective study,” The Lancet, vol. 359, no. 9303, pp. 303–309,2002.
[5] I. van der Lee, P. Zanen, J. C. Grutters, R. J. Snijder, and J. M.van den Bosch, “Diffusing capacity for nitric oxide and carbonmonoxide in patients with diffuse parenchymal lung disease
and pulmonary arterial hypertension,” Chest, vol. 129, no. 2,pp. 378–383, 2006.
[6] Z. Jambrik, S. Monti, V. Coppola et al., “Usefulness of ultra-sound lung comets as a nonradiologic sign of extravascularlung water,” American Journal of Cardiology, vol. 93, no. 10,pp. 1265–1270, 2004.
[7] E. Picano, F. Frassi, E. Agricola, S. Gligorova, L. Gargani, andG. Mottola, “Ultrasound lung comets: a clinically useful signof extravascular lung water,” Journal of the American Society ofEchocardiography, vol. 19, no. 3, pp. 356–363, 2006.
[8] K. Tsukimoto, O. Mathieu-Costello, R. Prediletto, A. R. Elliott,and J. B. West, “Ultrastructural appearances of pulmonarycapillaries at high transmural pressures,” Journal of AppliedPhysiology, vol. 71, no. 2, pp. 573–582, 1991.
[9] J. B. West, “Invited review: pulmonary capillary stress failure,”Journal of Applied Physiology, vol. 89, no. 6, pp. 2483–2489,2000.
[10] Y. Namba, S. S. Kurdak, Z. Fu, O. Mathieu-Costello, and J.B. West, “Effect of reducing alveolar surface tension on stressfailure in pulmonary capillaries,” Journal of Applied Physiology,vol. 79, no. 6, pp. 2114–2121, 1995.
[11] S. R. Hopkins, R. B. Schoene, W. R. Henderson, R. G. Spragg,T. R. Martin, and J. B. West, “Intense exercise impairs theintegrity of the pulmonary blood-gas barrier in elite athletes,”American Journal of Respiratory and Critical Care Medicine,vol. 155, no. 3, pp. 1090–1094, 1997.
[12] J. B. West, “Vulnerability of pulmonary capillaries duringexercise,” Exercise and Sport Sciences Reviews, vol. 32, no. 1,pp. 24–30, 2004.
[13] Z. Fu, M. L. Costello, K. Tsukimoto et al., “High lung volumeincreases stress failure in pulmonary capillaries,” Journal ofApplied Physiology, vol. 73, no. 1, pp. 123–133, 1992.
[14] E. R. Swenson, M. Maggiorini, S. Mongovin et al., “Pathogene-sis of high-altitude pulmonary edema: inflammation is not anetiologic factor,” Journal of the American Medical Association,vol. 287, no. 17, pp. 2228–2235, 2002, Erratum in: Journal ofthe American Medical Association, vol. 288, no. 9, p. 1064, 2002.
[15] S. R. Hopkins, J. Garg, D. S. Bolar, J. Balouch, and D. L.Levin, “Pulmonary blood flow heterogeneity during hypoxiaand high-altitude pulmonary edema,” American Journal ofRespiratory and Critical Care Medicine, vol. 171, no. 1, pp. 83–87, 2005.
[16] S. R. Hopkins and L. L. David, “Heterogeneous pulmonaryblood flow in response to hypoxia: a risk factor for highaltitude pulmonary edema?” Respiratory Physiology and Neu-robiology, vol. 151, no. 2-3, pp. 217–228, 2006.
[17] E. K. Weir, J. Lopez-Barneo, K. J. Buckler, and S. L. Archer,“Acute oxygen-sensing mechanisms,” New England Journal ofMedicine, vol. 353, no. 19, pp. 2042–2055, 2005.
[18] F. Murray, P. A. Insel, and J. X. Yuan, “Role of O2-sensitiveK+ and Ca2+ channels in the regulation of the pulmonarycirculation: potential role of caveolae and implications forhigh altitude pulmonary edema,” Respiratory Physiology andNeurobiology, vol. 151, no. 2-3, pp. 192–208, 2006.
[19] Y. Gao and J. U. Raj, “Role of veins in regulation of pulmonarycirculation,” American Journal of Physiology, vol. 288, no. 2, pp.L213–L226, 2005.
[20] C. V. Remillard and J. X. Yuan, “High altitude pulmonaryhypertension: role of K+ and Ca2+ channels,” High AltitudeMedicine and Biology, vol. 6, no. 2, pp. 133–146, 2005.
[21] A. Podolsky, M. W. Eldridge, R. S. Richardson et al., “Exercise-induced VA/Q inequality in subjects with prior high-altitudepulmonary edema,” Journal of Applied Physiology, vol. 81, no.2, pp. 922–932, 1996.

8 Pulmonary Medicine
[22] B. R. Walker, “Evidence for uneven distribution of L-typecalcium channels in rat pulmonary circulation,” AmericanJournal of Physiology, vol. 269, no. 6, pp. H2051–H2056, 1995.
[23] E. K. Weir, H. L. Reeve, D. N. Cornfield, M. Tristani-Firouzi,D. A. Peterson, and S. L. Archer, “Diversity of response invascular smooth muscle cells to changes in oxygen tension,”Kidney International, vol. 51, no. 2, pp. 462–466, 1997.
[24] X. R. Yang, M. J. Lin, K. P. Yip et al., “Multiple ryanodinereceptor subtypes and heterogeneous ryanodine receptor-gated Ca2+ stores in pulmonary arterial smooth muscle cells,”American Journal of Physiology, vol. 289, no. 2, pp. L338–L348,2005.
[25] M. M. Berger, C. Hesse, C. Dehnert et al., “Hypoxia impairssystemic endothelial function in individuals prone to high-altitude pulmonary edema,” American Journal of Respiratoryand Critical Care Medicine, vol. 172, no. 6, pp. 763–767, 2005.
[26] H. Duplain, C. Sartori, M. Lepori et al., “Exhaled nitric oxidein high-altitude pulmonary edema: role in the regulationof pulmonary vascular tone and evidence for a role againstinflammation,” American Journal of Respiratory and CriticalCare Medicine, vol. 162, no. 1, pp. 221–224, 2000.
[27] S. Koyama, T. Kobayashi, K. Kubo et al., “The increased sym-pathoadrenal activity in patients with high altitude pulmonaryedema is centrally mediated,” Japanese Journal of Medicine, vol.27, no. 1, pp. 10–16, 1988.
[28] H. Duplain, L. Vollenweider, A. Delabays, P. Nicod, P. Bartsch,and U. Scherrer, “Augmented sympathetic activation duringshort-term hypoxia and high-altitude exposure in subjectssusceptible to high-altitude pulmonary edema,” Circulation,vol. 99, no. 13, pp. 1713–1718, 1999.
[29] S. Goerre, M. Wenk, P. Bartsch et al., “Endothelin-1 in pul-monary hypertension associated with high-altitude exposure,”Circulation, vol. 91, no. 2, pp. 359–364, 1995.
[30] C. Sartori, L. Vollenweider, B. M. Loffler et al., “Exaggeratedendothelin release in high-altitude ulmonary edema,” Circula-tion, vol. 99, no. 20, pp. 2665–2668, 1999.
[31] W. Durante, N. Christodoulides, K. Cheng, K. J. Peyton, R. K.Sunahara, and A. I. Schafer, “cAMP induces heme oxygenase-1gene expression and carbon monoxide production in vascularsmooth muscle,” American Journal of Physiology, vol. 273, no.1, pp. H317–H323, 1997.
[32] C. Sartori and M. A. Matthay, “Alveolar epithelial fluid trans-port in acute lung injury: new insights,” European RespiratoryJournal, vol. 20, no. 5, pp. 1299–1313, 2002.
[33] S. Richter, C. Betz, and H. Geiger, “Severe hyponatremia withpulmonary and cerebral edema in an ironman triathlete,”Deutsche Medizinische Wochenschrift, vol. 132, no. 36, pp.1829–1832, 2007.
[34] D. B. Speedy, J. G. Faris, M. Hamlin, P. G. Gallagher, andR. G. Campbell, “Hyponatremia and weight changes in anultradistance triathlon,” Clinical Journal of Sport Medicine, vol.7, no. 3, pp. 180–184, 1997.
[35] A. J. Siegel, “Exercise-associated hyponatremia: role ofcytokines,” American Journal of Medicine, vol. 119, no. 7, pp.S74–S78, 2006.
[36] T. Hew-Butler, C. Almond, J. C. Ayus et al., “Consen-sus statement of the 1st International Exercise-AssociatedHyponatremia Consensus Development Conference, CapeTown, South Africa 2005,” Clinical Journal of Sport Medicine,vol. 15, no. 4, pp. 208–213, 2005.
[37] G. Mastorakos, J. S. Weber, M. A. Magiakou, H. Gunn,and G. P. Chrousos, “Hypothalamic-pituitary-adrenal axisactivation and stimulation of systemic vasopressin secretion by
recombinant interleukin-6 in humans: potential implicationsfor the syndrome of inappropriate vasopressin secretion,”Journal of Clinical Endocrinology and Metabolism, vol. 79, no.4, pp. 934–939, 1994.
[38] A. Rivier, J. Pane, P. Chanez et al., “Release of cytokinesby blood monocytes during strenuous exercise,” InternationalJournal of Sports Medicine, vol. 15, no. 4, pp. 192–198, 1994.
[39] J. B. West, “Understanding pulmonary gas exchange:ventilation-perfusion relationships,” American Journal ofPhysiology, vol. 287, no. 6, pp. L1071–L1072, 2004.
[40] J. B. West, K. Tsukimoto, O. Mathieu-Costello, and R.Prediletto, “Stress failure in pulmonary capillaries,” Journal ofApplied Physiology, vol. 70, no. 4, pp. 1731–1742, 1991.
[41] C. M. Croix, C. A. Harms, S. R. McClaran et al., “Effectsof prior exercise on exercise-induced arterial hypoxemia inyoung women,” Journal of Applied Physiology, vol. 85, no. 4,pp. 1556–1563, 1998.
[42] A. P. Greening and J. M. Hughes, “Serial estimations ofcarbon monoxide diffusing capacity in intrapulmonary haem-orrhage,” Clinical Science, vol. 60, no. 5, pp. 507–512, 1981.
[43] G. W. Gray, I. D. B. Rennie, C. S. Houston, and A. C. Bryan,“Phase IV volume of the single breath nitrogen washout curveon exposure to altitude,” Journal of Applied Physiology, vol. 35,no. 2, pp. 227–230, 1973.
[44] H. J. Guy, P. A. Gaines, P. M. Hill, P. D. Wagner, and J. B.West, “Computerized, noninvasive tests of lung function: aflexible approach using mass spectrometry,” American Reviewof Respiratory Disease, vol. 113, no. 6, pp. 737–744, 1976.
[45] G. Manier, J. Moinard, and H. Stoıcheff, “Pulmonary diffusingcapacity after maximal exercise,” Journal of Applied Physiology,vol. 75, no. 6, pp. 2580–2585, 1993.
[46] P. Vock, M. H. Brutsche, A. Nanzer, and P. Bartsch, “Variableradiomorphologic data of high altitude pulmonary edema,”Chest, vol. 100, no. 5, pp. 1306–1311, 1991.
[47] G. Lutterbey, J. Gieseke, M. von Falkenhausen, N. Morakka-bati, and H. Schild, “Lung MRI at 3.0 T: a comparison ofhelical CT and high-field MRI in the detection of diffuse lungdisease,” European Radiology, vol. 15, no. 2, pp. 324–328, 2005.
[48] L. Gargani, V. Lionetti, C. Di Cristofano, G. Bevilacqua, F.A. Recchia, and E. Picano, “Early detection of acute lunginjury uncoupled to hypoxemia in pigs using ultrasound lungcomets,” Critical Care Medicine, vol. 35, no. 12, pp. 2769–2774,2007.
[49] O. Frobert, J. Moesgaard, E. Toft, S. H. Poulsen, and P. Sogaard,“Influence of oxygen tension on myocardial performance.Evaluation by tissue Doppler imaging,” Cardiovascular Ultra-sound, vol. 2, article 22, 2004.
[50] G. R. Rajan, “Ultrasound lung comets: a clinically usefulsign in acute respiratory distress syndrome/acute lung injury,”Critical Care Medicine, vol. 35, no. 12, pp. 2869–2870, 2007.
[51] G. Volpicelli, “Significance of comet tail artifacts at lungultrasound,” American Journal of Emergency Medicine, vol. 25,no. 8, pp. 981–982, 2007.
[52] F. Frassi, L. Gargani, P. Tesorio, M. Raciti, G. Mottola, and E.Picano, “Prognostic value of extravascular lung water assessedwith ultrasound lung comets by chest sonography in patientswith dyspnea and/or chest pain,” Journal of Cardiac Failure,vol. 13, no. 10, pp. 830–835, 2007.
[53] P. Capozza, L. Gargani, and G. Bedetti, “Cardiac-chest ultra-sound risk score in acute coronary syndromes: the prognosticvalue of the echographic deadly quartet,” European HeartJournal, 2008.
[54] D. Konig, O. Neubauer, L. Nics et al., “Biomarkers of exercise-induced myocardial stress in relation to inflammatory and

Pulmonary Medicine 9
oxidative stress,” Exercise Immunology Review, vol. 13, pp. 15–36, 2007.
[55] E. Fehrenbach and M. E. Schneider, “Trauma-inducedsystemic inflammatory response versus exercise-inducedimmunomodulatory effects,” Sports Medicine, vol. 36, no. 5,pp. 373–384, 2006.
[56] D. Konig, K. H. Wagner, I. Elmadfa, and A. Berg, “Exerciseand oxidative stress: significance of antioxidants with referenceto inflammatory, muscular, and systemic stress,” ExerciseImmunology Review, vol. 7, pp. 108–133, 2001.
[57] K. Suzuki, J. Peake, K. Nosaka et al., “Changes in markers ofmuscle damage, inflammation and HSP70 after an Ironmantriathlon race,” European Journal of Applied Physiology, vol. 98,no. 6, pp. 525–534, 2006.
[58] C. Rong, H. Bei, M. Yun, W. Yuzhu, and Z. Mingwu, “Lungfunction and cytokine levels in professional athletes,” Journalof Asthma, vol. 45, no. 4, pp. 343–348, 2008.
[59] D. Gomez-Merino, C. Drogou, C. Y. Guezennec et al.,“Comparison of systemic cytokine responses after a longdistance triathlon and a 100-km run: relationship to metabolicand inflammatory processes,” European Cytokine Network, vol.17, no. 2, pp. 117–124, 2006.
[60] N. S. Hill, C. Jacoby, and H. W. Farber, “Effect of an endurancetriathlon on pulmonary function,” Medicine and Science inSports and Exercise, vol. 23, no. 11, pp. 1260–1264, 1991.
[61] G. Manier, J. Moinard, P. Techoueyres, N. Varene, and H.Guenard, “Pulmonary diffusion limitation after prolongedstrenuous exercise,” Respiration Physiology, vol. 83, no. 2, pp.143–153, 1991.
[62] C. Rong, H. Bei, M. Yun, W. Yuzhu, and Z. Mingwu, “Lungfunction and cytokine levels in professional athletes,” Journalof Asthma, vol. 45, no. 4, pp. 343–348, 2008.
[63] E. Garbella, F. Frassi, A. Piarulli et al., “Lung tissue damageand pulmonary function impairment after extreme physicalexercise (ultra triathlon). Possible implication of systemicinflammation,” in Proceedings of the 6th Italian NationalCongress of Pneumology (SIMER-UIP), Milan, Italy, 2010.
[64] L. Pratali, M. Cavana, R. Sicari, and E. Picano, “Fre-quent subclinical high-altitude pulmonary edema detected bychest sonography as ultrasound lung comets in recreationalclimbers,” Critical Care Medicine, vol. 38, no. 9, pp. 1818–1823,2010.
[65] G. Ferretti, “Extreme human breath-hold diving,” EuropeanJournal of Applied Physiology, vol. 84, no. 4, pp. 254–271, 2001.
[66] J. A. Andersson, M. H. Liner, E. Runow, and E. Schagatay,“Diving response and arterial oxygen saturation during apneaand exercise in breath-hold divers,” Journal of Applied Physiol-ogy, vol. 93, no. 3, pp. 882–886, 2002.
[67] K. E. Schaefer, R. D. Allison, I. H. Dougherty et al., “Pul-monary and circulatory adjustments determining the limits ofdepths in breathhold diving,” Science, vol. 162, no. 3857, pp.1020–1023, 1968.
[68] M. Arborelius Jr., U. I. Balldin, B. Lilja, and C. E. Lundgren,“Hemodynamic changes in man during immersion with thehead above water,” Aerospace Medicine, vol. 43, no. 6, pp. 592–598, 1972.
[69] J. B. West and O. Mathieu-Costello, “Stress failure of pul-monary capillaries: role in lung and heart disease,” The Lancet,vol. 340, no. 8822, pp. 762–767, 1992.
[70] A. Boussuges, C. Pinet, P. Thomas, E. Bergmann, J. M. Sainty,and D. Vervloet, “Haemoptysis after breathhold diving,”European Respiratory Journal, vol. 13, no. 3, pp. 697–699, 1999.
[71] F. Frassi, A. Pingitore, D. Cialoni, and E. Picano, “Chest sonog-raphy detects lung water accumulation in healthy elite apnea
divers,” Journal of the American Society of Echocardiography,vol. 21, no. 10, pp. 1150–1155, 2008.
[72] J. B. West, American College of Physicians, and AmericanPhysiological Society, “The physiologic basis of high-altitudediseases,” Annals of Internal Medicine, vol. 141, no. 10, pp. 789–800, 2004.
[73] C. Bai, J. She, A. Goolaerts et al., “Stress failure plays a majorrole in the development of high-altitude pulmonary oedemain rats,” European Respiratory Journal, vol. 35, no. 3, pp. 584–591, 2010.
[74] J. B. West, G. L. Colice, Y. J. Lee et al., “Pathogenesis of high-altitude pulmonary oedema: direct evidence of stress failureof pulmonary capillaries,” European Respiratory Journal, vol.8, no. 4, pp. 523–529, 1995.
[75] K. Kubo, M. Hanaoka, T. Hayano et al., “Inflammatorycytokines in BAL fluid and pulmonary hemodynamics inhigh-altitude pulmonary edema,” Respiration Physiology, vol.111, no. 3, pp. 301–310, 1998.
[76] R. Prediletto, E. Garbella, E. Fornai et al., “Time course ofDLNO/DLCO after induced hypoxic and hyperbaric stress inbreath-hold divers,” Chest, vol. 138, p. 561A, 2010.