-
4/28/2015 Neurogenicpulmonaryedema
http://www.uptodate.com/contents/neurogenicpulmonaryedema?topicKey=PULM%2F1610&elapsedTimeMs=4&view=print&displayedView=full#
1/12
UpToDate OfficialreprintfromUpToDate
www.uptodate.com2015UpToDate
AuthorsMatthewWemple,MDMatthewHallman,MDAndrewMLuks,MD
SectionEditorPollyEParsons,MD
DeputyEditorGeraldineFinlay,MD
Neurogenicpulmonaryedema
Alltopicsareupdatedasnewevidencebecomesavailableandourpeerreviewprocessiscomplete.Literaturereviewcurrentthrough:Mar2015.|Thistopiclastupdated:Apr02,2014.
INTRODUCTIONNeurogenicpulmonaryedema(NPE)isanincreaseinpulmonaryinterstitialandalveolarfluidthatisduetoanacutecentralnervoussysteminjuryandusuallydevelopsrapidlyaftertheinjury[1].Itissometimesclassifiedasaformoftheacuterespiratorydistresssyndrome(ARDS),butitspathophysiologyandprognosisaredifferent.
Theclinicalfeatures,differentialdiagnosis,diagnosis,etiology,pathogenesis,andtreatmentofNPEarereviewedhere.ARDSandnoncardiogenicpulmonaryedemaduetoothercausesarediscussedelsewhere.(See"Acuterespiratorydistresssyndrome:Clinicalfeaturesanddiagnosisinadults"and"Noncardiogenicpulmonaryedema".)
CLINICALPRESENTATIONNPEcharacteristicallypresentswithinminutestohoursofaseverecentralnervoussysteminsultsuchassubarachnoidhemorrhageortraumaticbraininjury.However,morerapidonset(immediate)anddelayedonset(hourstodays)havebeendescribed[24].Resolutionusuallyoccurswithinseveraldays[5].
Dyspneaisthemostcommonsymptom,althoughmildhemoptysisispresentinmanypatients.Thephysicalexaminationgenerallyrevealstachypnea,tachycardia,andbasilarrales.Chestradiographstypicallyshowanormalsizeheartwithbilateralalveolaropacities,althoughunilateralopacitieshavealsobeendescribed[68].HemodynamicmeasurementsareusuallynormalbythetimeNPEisdiagnosed,includingthebloodpressure,cardiacoutput,andpulmonarycapillarywedgepressure.
ThereisabroadrangeofseveritiesofNPEandmildcasesmayneverbedetected.WhileNPEcanbefulminantandcontributetodeath,mortalityismorecommonlyduetotheneurologicinsultthatprecipitatedtheonsetofNPE.
DIFFERENTIALDIAGNOSISTheclinicalfindingsofNPEmaybeconfusedwithaspirationpneumonitis.Reliabledifferentiationbetweenthesesyndromesisdifficultbecausetheyarebothcommoninsettingsofalteredconsciousness,suchaspostictalstates.NPEtendstodevelopmorerapidlythanaspirationpneumonia,whilefeverandfocalopacities,particularlyinthelowerlungzones,favoraspiration.Inaddition,NPEtendstoresolvemorerapidlythanlunginjuryrelatedtoaspiration,particularlyifaspirationpneumoniadevelops.
Othercausesofpulmonaryedemashouldalsobeconsidered,suchasheartfailureandacuterespiratorydistresssyndrome.(See"Evaluationofthepatientwithsuspectedheartfailure"and"Acuterespiratorydistresssyndrome:Clinicalfeaturesanddiagnosisinadults".)
DIAGNOSISDefinitivediagnosisofNPEisdifficultbecausetheclinicalsignsandroutinediagnostictestsarenonspecific.Thus,NPEisaclinicaldiagnosisbasedupontheoccurrenceofpulmonaryedemaintheappropriatesettingandintheabsenceofamorelikelyalternativecause.ThefollowingcriteriaforthediagnosisandclassificationofNPEhavebeenproposed,buthavenotbeenwidelyaccepted[9]:
BilateralopacitiesPaO /FiO ratio
-
4/28/2015 Neurogenicpulmonaryedema
http://www.uptodate.com/contents/neurogenicpulmonaryedema?topicKey=PULM%2F1610&elapsedTimeMs=4&view=print&displayedView=full#
2/12
ETIOLOGYTheprimaryprecipitantsofNPEareepilepticseizures,traumaticbraininjury,andcerebralhemorrhages(table1)[3,10].
EpilepticseizuresAmongallpatientswithepilepsytheoccurrenceofNPEisrare.However,severalcaseseriesreportedthatuptoonethirdofpatientswithfatalstatusepilepticushadclinicalevidenceofNPE,whileanautopsystudyfoundthat87percentofpatientswithepilepsyandunexplainedsuddendeathhadNPE[1012].ItisuncertainwhetherNPEwastheproximatecauseofdeathinthesestudies,butitisclearthattheNPEismorelikelywithincreasingseizureseverity.
NPEduetoepilepticseizuresgenerallyoccursduringthepostictalperiodanditmayoccurrepeatedlyinagivenindividual[3,13,14].(See"Convulsivestatusepilepticusinadults:Classification,clinicalfeatures,anddiagnosis".)
TraumaticbraininjuryBluntorpenetratingheadinjuryandneurosurgicalprocedurescancauseNPE[2,3,15].TheNPEisusuallyassociatedwithelevatedintracranialpressure(ICP),butraisedICPisnotanecessarycondition[16].TheincidenceofNPEintraumaticbraininjuryhasbeenestimatedat20percent,andappearstoincreasewithincreasingseverityofinjury[17].(See"Evaluationandmanagementofelevatedintracranialpressureinadults".)
CerebralhemorrhageNPEcancomplicateupto43percentofcasesofsubarachnoidhemorrhage[4,7,1821].Inaseriesof78casesoffatalsubarachnoidhemorrhage,31percenthadantemortemclinicalevidenceofNPEand71percenthadpathologicalevidenceofNPEatautopsy[18].Onsetistypicallywithinminutestohoursofthehemorrhagealthoughlateonsetdaysafterhemorrhageorrecurrenceafterapparentresolutionhavealsobeendescribed[22].NPEhasalsobeenreportedduringcoilembolizationofarupturedcerebralaneurysm[23].ThemostimportantriskfactorsforNPEfollowingsubarachnoidhemorrhagearetheclinicalandradiographicseveritiesofthehemorrhagesaswellasavertebralarterysourceofthehemorrhage[1,21].NPEcanalsobeseeninupto35percentofpatientswithintracerebralhemorrhage,withtheprimaryriskfactorsinsuchpatientsbeinghigherAcutePhysiologyandChronicHealthEvaluation(APACHE)IIscoresandincreasedlevelsofseruminflammatorymarkers[24].(See"Clinicalmanifestationsanddiagnosisofaneurysmalsubarachnoidhemorrhage".)
Otherlesscommonetiologiesarelistedinthetable(table1)[2528].
PATHOGENESISTheneurologicalstructuresthatarecriticaltothedevelopmentofNPEareknown.However,themechanismbywhichlesionsinthesestructuresleadtoNPEisnotwellunderstood.
NeurologicstructuresThemedullaoblongataandhypothalamusareconsideredthecriticalanatomicstructuresinvolvedinthepathogenesisofNPE.Theimportanceofthemedullaissupportedbytheobservationthatbilaterallesionsinthenucleusofthesolitarytract,areapostremaandlesionsintheA1andA5neuroadrenergicneurons(allofwhichareinthemedulla)cancausesystemichypertensionandNPE[2932].
Themedullaoblongataprobablyactsviathesympatheticcomponentoftheautonomicnervoussystem,assuggestedbythefollowingevidencefromanimalmodels[3335]:
Inadditiontotheroleofthemedullaoblongata,theoriesregardingthepathogenesisofNPEhavecenteredonthepotentialcontributionsofthehypothalamus,elevatedintracranialpressure,andactivationofthesympathoadrenalsystem[29,30,3345].Experimentalmodelshaveshown,forexample,thatinducinghypothalamiclesionsprecipitatesNPE[46],whileacaseseriesof22patientswithNPEfoundthathalfof
(ARDS)(eg,aspiration,massivebloodtransfusion,sepsis)
Alphaadrenergicblockade(eg,withphentolamine)canpreventthedevelopmentofNPE
NPEcanbepreventedbyspinalcordtransectionatorabovetheC7level,belowwhichsympatheticfibersleavethelateralpartofthecordtoformtheparaspinalsympathetictrunks
NPEcanbepreventedbydenervationbytransectionofthesplanchnicsympatheticfiberstothelungs
NPEmaybeproducedbystimulationofthecordattheC7C8level,withthecordandsympatheticnervesintact
-
4/28/2015 Neurogenicpulmonaryedema
http://www.uptodate.com/contents/neurogenicpulmonaryedema?topicKey=PULM%2F1610&elapsedTimeMs=4&view=print&displayedView=full#
3/12
themhadradiographicevidenceofhypothalamicinjury,afindingassociatedwithworseoutcome[47].
MechanismsofedemaformationNPErequiresacentralnervoussysteminjuryorevent(eg,seizure)thatalterstheStarling'sforcesinawaythatincreasesthemovementoffluidfromthecapillariestothepulmonaryinterstitium,increasesthepermeabilityofthepulmonarycapillaries,orboth(figure1).
CapillaryhydrostaticpressureIncreasedcapillaryhydrostaticpressureistheStarling'sforcethatismostlikelytocontributetoNPE,sinceitisunlikelythatacentralnervoussysteminjuryoreventcouldchangecapillaryorinterstitialoncoticpressurerapidly[3].ThisissupportedbytheobservationthatalveolarfluidhasalowfluidtoserumproteinratioearlyduringthecourseofNPE,consistentwithhydrostaticpulmonaryedema[48].
Experimentalstudiesusinganimalmodelsanduncontrolledobservationsinhumanssuggestseveralmechanismsbywhichpulmonarycapillaryhydrostaticpressuremayincreaseacutely:
DespitetheevidencethatincreasedpulmonarycapillaryhydrostaticpressureplaysaroleinNPE,therearelikelyadditionalcontributors.ThisnotionisbaseduponreportsofNPEoccurringwithlittleornoelevationinthepulmonarycapillarywedgepressureandintheabsenceofleftatrialorsystemichypertension[49].
PulmonarycapillarypermeabilityIncreasedpulmonarycapillarypermeabilitymaycontributetoNPE.ThisideaissupportedbythefindingofproteinrichedemafluidinanimalmodelsandsomepatientswithNPE,aswellastheobservationthatNPEcanoccurintheabsenceofthehemodynamicalterationsassociatedwithpulmonaryedema[4,48,62,63].
Asanexample,astudyusedthermalgreendyetechniquestomeasureextravascularlungwaterin18patientswitheitherheadtraumaorsubarachnoidhemorrhageand13controlpatients(traumapatientswithoutheadinjury)[4].Nineofthe18patientswithbraininjurieshadpulmonaryedema,definedasextravascularlungwatervaluesgreaterthantwostandarddeviationsabovethecontrolgroupmean.Thepulmonaryedemawasindependentofintracranialorpulmonaryvascularpressure,suggestingincreasedvascularpermeability.
Themechanismbywhichneuralinfluencesproducechangesinpulmonaryvascularpermeabilityhavenotbeenelucidatedwell.However,severalhypothesesexist:
Pulmonaryvenoconstrictionmayoccurwithintracranialhypertensionorsympatheticstimulation.Thisincreasesthepulmonarycapillaryhydrostaticpressure,producingpulmonaryedema[33,4952].Alphaadrenergicantagonistsmayattenuatetheeffect[53].
Excessivesystemicvenoconstrictionmayoccurleadingtoasignificantincreaseinvenousreturntotherightheartandpulmonarycirculation.Supportforthisconceptcomesfromanimalstudiesinwhichprophylacticphlebotomy(15percentofbloodvolume)priortoCNSinsultpreventeddevelopmentneurogenicpulmonaryedema[54].
Leftventricularperformancemaydeteriorateforseveralreasons:directmyocardialdamageorstunningsecondarytobraininjury,increasedafterloadduetosystemichypertension,andnegativeinotropicandchronotropicinfluencesofexcessivevagaltone[52,55,56].Thiscancausepassiveelevationoftheleftatrialandpulmonarycapillarypressures,leadingtopulmonaryedema[38,39,55,5761].
Epinephrineornorepinephrinemaydirectlyincreasevascularpermeability.SupportingthisideaaretheobservationsfromanimalmodelsthatalphaadrenergicblockadecanprotectagainstNPEandsympatheticstimulationcanproduceit[53].However,thehypothesisisimperfectbecausedirectinfusionofthesesubstancesintothepulmonarycirculationdoesnotproducesuchaneffect[64].
Alphaadrenergicagonistsreleasedinresponsetobraininjurymaycausethereleaseofasecondmediator,whichincreasesvascularpermeability(eg,endorphins,histamine,bradykinin)[3].
Aninitialrapidincreaseinpulmonaryvascularpressure(eg,duetopulmonaryvasospasmand/orincreasedsystemicvenousreturn)maycausepulmonarymicrovascularinjurywithasubsequentincreaseinpermeability[65].Thistheory,sometimescalledthe"blasttheory"issupportedbystudiesinrabbitsshowingthatpulmonarycapillariesaredamagedwhenpressuresexceed40mmHg[66].ItisalsosupportedbytheobservationthatpatientswithNPEfrequentlyhavemildhemoptysisorpulmonary
-
4/28/2015 Neurogenicpulmonaryedema
http://www.uptodate.com/contents/neurogenicpulmonaryedema?topicKey=PULM%2F1610&elapsedTimeMs=4&view=print&displayedView=full#
4/12
Inflammatorymechanismsmayalsocontributetoincreasedcapillarypermeability[45].Evidenceforinflammatoryresponsestoseverebraininjuryinclude:
Whethertheseobservedinflammatoryresponsespredisposetoedemaformationremainsasubjectofdebate.
TREATMENTTheoutcomeofpatientswithNPEisusuallydeterminedbythecourseoftheneurologicinsultandnottheNPE.Thus,treatmentshouldfocusontheneurologicaldisorderwhileNPEismanagedinasupportivefashion.ManyepisodesofNPEarewelltoleratedandmostresolvewithin48to72hours.
SupportivecareMostpatientswithNPEarehypoxemicandrequiresupplementaloxygen.Somepatientsmayrequiremechanicalventilation.
WhilemostpatientswithNPEarehypoxemicandrequiresupplementaloxygen,thereisinsufficientevidencetosupportspecificoxygenationgoals.Maintenanceofanoxyhemoglobinsaturation88percentorPaO
55mmHgisgenerallyacceptableinundifferentiatedlunginjury,butspecifictargetsinNPEshouldalsotakeintoconsiderationtheeffectthatrelativehypoxemiamayhaveontheunderlyingneurologicalinjury.
Oxygenationgoalsmaybeachievedinsomepatientswithnoninvasivemeasuressuchasoxygenbynasalcannulasimplefacemask,nonrebreathermask,orhighflowdeliverysystems,butmechanicalventilationmaybenecessaryinothercircumstances.Mechanicalventilationandthedecisiontointubateapatientarediscussedseparately.(See"Overviewofmechanicalventilation"and"Noninvasivepositivepressureventilationinacuterespiratoryfailureinadults"and"Thedecisiontointubate".)
MechanicalventilationinpatientswithNPEissimilartothatinpatientswithothercausesofrespiratoryfailure,althoughtherearesomeimportantdifferences:
IfICPelevationisaclinicalconcern,ICPmonitoringmaybeconsideredtoguidemechanicalventilation.
Singlecasereportsdocumenttheuseofproneventilation,inhalednitricoxide,andextracorporealmembranousoxygenation(ECMO)inpatientswithNPEandseverehypoxemia,butthereisnosystematicevidencesupportingabenefitfromthesepracticesinsuchcircumstances[7779].BecauseECMOcarriestheriskofintracranialhemorrhage,extremecaremustbetakenwithitsapplicationinpatientswithcentralnervoussysteminjury.(See"Proneventilation"and"Extracorporealmembraneoxygenation(ECMO)inadults".)
Maintenanceoflowcardiacfillingpressureswithdiureticsandlimitationofintravenousfluidsmaydecreasepulmonaryedema.However,caremustbetakentoavoidcompromiseofcardiacoutputandcerebralperfusion.Pulmonaryarterycatheterizationwashistoricallythoughthelpfulinguidingtherapy,buthassincefallenoutof
hemorrhage[2].ThehypothesisisimperfectbecausetherapiddevelopmentofacutepulmonaryhypertensionisnotanecessaryconditionforNPE[67,68]andinanimalmodelselevatedpulmonaryvascularpressuresdonotinvariablyleadtoNPE[69].
Excesscatecholaminescanthemselvesleadtothereleaseofinflammatorymediators[70,71].
S100B,aserumbiomarkerofbraininjury,hasbeenshowntoinducethereleaseofproinflammatorycytokinesinalveolartype1likecellsinvitro[72].
Braininjuryhasbeenassociatedwithincreasedintracranialproductionofproinflammatorymediatorsandsubsequentreleaseofthesemediatorsintothesystemiccirculation[73,74].
AratmodelofSAHdocumentedincreasedexpressionofendothelialactivationmarkersonpulmonaryendothelialcells,andincreasedpulmonaryTNFexpression,whichwasattenuatedbyadministrationoftheimmunemodulatorIFN.
2
Highlevelsofpositiveendexpiratorypressure(PEEP)canreducecerebralvenousreturnandworsenintracranialhypertension[75,76].(See"Positiveendexpiratorypressure(PEEP)",sectionon'Intracranialdisease'.)
Hypercapnia,whichisoftentoleratedinpatientswithARDS,cancausecerebralvasodilation,therebyincreasingcerebralbloodflowandpotentiallyincreasingICP[1].(See"Permissivehypercapnia",sectionon'Contraindications'.)
-
4/28/2015 Neurogenicpulmonaryedema
http://www.uptodate.com/contents/neurogenicpulmonaryedema?topicKey=PULM%2F1610&elapsedTimeMs=4&view=print&displayedView=full#
5/12
favoraspartofroutinefluidmanagement[5].(See"Pulmonaryarterycatheterization:Indications,contraindications,andcomplicationsinadults".)
TheutilityoflessinvasivemethodsofassessingcardiacfunctionandpulmonaryedematoguidetreatmentinNPEisnotwellstudied.Simultaneousassessmentofcardiacoutput,extravascularlungwater,globalenddiastolicvolume,andpulmonaryvascularpermeabilityusinglessinvasivehemodynamicmonitorshasbeenproposedasamethodtoguidemanagementdecisions,butthedataareinsufficienttosupportspecificrecommendations[80].Small,limitedstudieshavealsoevaluatedtheutilityoflungultrasoundexamsinNPE[81].
MedicationsAvarietyofmedicationshavebeenusedtotreatpatientswithNPE,buttheireffectivenessisunproven.Theseinclude:
AlphaadrenergicantagonistshavebeenshowntopreventNPEorhastenitsresolutioninanimalmodels,whilearecentreportdemonstratedrapidimprovementsinoxygenationfollowingadministrationofphentolamineinasinglepatientwithNPEduetoarupturedarteriovenousmalformation[53].However,unopposedalphaadrenergicantagonistsmayprecipitatesystemichypotensionandcerebralhypoperfusion,andintheabsenceofdatafromcontrolledtrials,routineuseoftheseagentscannotberecommendedatthistime.(See"Antihypertensivetherapytopreventrecurrentstrokeortransientischemicattack"and"Evaluationandmanagementofelevatedintracranialpressureinadults".)
OutcomesAlthoughmanyepisodesofNPEarewelltoleratedandmostcasesresolvewithin48to72hours,thedevelopmentofNPEisassociatedwithworselongtermoutcomes.Asanexample,arecentobservationalstudyof108patientswithnontraumaticintracranialhemorrhage,foundthatcomparedtothosewithoutNPE,thosewhodevelopedNPEhadahigheroneyearmortalityof(37versus14percent)[24].
SUMMARYANDRECOMMENDATIONS
Betaadrenergicantagonistsarethoughttoincreaselymphflow,decreaseedemaandreducehistamineinducedaugmentationofpulmonaryvascularpermeability[3]
Dobutamine,whichmayincreasecardiacoutput,decreasespulmonarycapillarywedgepressure,andpromotediuresis[82,83]
Chlorpromazinemayblockalphaadrenergicreceptorstoreduceedema[84]
Neurogenicpulmonaryedema(NPE)isanincreaseinpulmonaryinterstitialandalveolarfluidthatisduetoanacutecentralnervoussysteminjury.Itusuallydevelopsrapidlyfollowingtheinjury.(See'Introduction'above.)
NPEcharacteristicallypresentswithinminutestohoursofaseverecentralnervoussysteminsult.Dyspneaisthemostcommonsymptom,althoughmildhemoptysisispresentinmanypatients.Thephysicalexaminationgenerallyrevealstachypnea,tachycardia,andbasilarrales.Chestradiographstypicallyshowanormalsizeheartwithbilateralalveolarfilling,whilehemodynamicmeasurementsareusuallynormal.(See'Clinicalpresentation'above.)
NPEisaclinicaldiagnosisbasedupontheoccurrenceofpulmonaryedemaintheappropriatesettingandintheabsenceofamorelikelyalternativecause.(See'Differentialdiagnosis'aboveand'Diagnosis'above.)
TheprimaryprecipitantsofNPEareepilepticseizures,traumaticbraininjury,andcerebralhemorrhages(table1).(See'Etiology'above.)
ThetreatmentofNPEshouldfocusontreatingtheneurologicaldisorderwhileNPEismanagedinasupportivefashion.ManyepisodesofNPEarewelltoleratedandmostresolvewithin48to72hours.(See'Treatment'above.)
MostpatientswithNPEarehypoxemicandrequiresupplementaloxygen.Somepatientsmayrequiremechanicalventilation,whichdiffersfromthatforothercausesofrespiratoryfailureintwoways:permissivehypercapniaandhighlevelsofpositiveendexpiratorypressure(PEEP)shouldbeused
-
4/28/2015 Neurogenicpulmonaryedema
http://www.uptodate.com/contents/neurogenicpulmonaryedema?topicKey=PULM%2F1610&elapsedTimeMs=4&view=print&displayedView=full#
6/12
ACKNOWLEDGMENTTheeditorialstaffatUpToDate,Inc.wouldliketoacknowledgeFrankDrislane,MD,andJessMandel,MD,whocontributedtoanearlierversionofthistopicreview.
UseofUpToDateissubjecttotheSubscriptionandLicenseAgreement.
REFERENCES
1.
BaumannA,AudibertG,McDonnellJ,MertesPM.Neurogenicpulmonaryedema.ActaAnaesthesiolScand200751:447.
2.
SimmonsRL,MartinAMJr,HeisterkampCA3rd,DuckerTB.Respiratoryinsufficiencyincombatcasualties.II.Pulmonaryedemafollowingheadinjury.AnnSurg1969170:39.
3.
ColiceGL,MatthayMA,BassE,MatthayRA.Neurogenicpulmonaryedema.AmRevRespirDis1984130:941.
4.
MackersieRC,ChristensenJM,PittsLH,LewisFR.Pulmonaryextravascularfluidaccumulationfollowingintracranialinjury.JTrauma198323:968.
5.
LagerkranserM,PehrssonK,SylvnC.Neurogenicpulmonaryoedema.Areviewofthepathophysiologywithclinicalandtherapeuticimplications.ActaMedScand1982212:267.
6.
EllSR.Neurogenicpulmonaryedema.Areviewoftheliteratureandaperspective.InvestRadiol199126:499.
7.
FontesRB,AguiarPH,ZanettiMV,etal.Acuteneurogenicpulmonaryedema:casereportsandliteraturereview.JNeurosurgAnesthesiol200315:144.
8.
DurgaP,JonnavithulaN,PanigrahiMK,ManthaS.Unilateralneurogenicpulmonaryoedema:Anunusualcauseforpostoperativerespiratorydysfunctionfollowingclippingofrupturedintracranialaneurysm.IndianJAnaesth201256:58.
9.
DavisonDL,TerekM,ChawlaLS.Neurogenicpulmonaryedema.CritCare201216:212.10.
SimonRP.Neurogenicpulmonaryedema.NeurolClin199311:309.11.
Ohlmacher,AP.Acutepulmonaryedemaasaterminaleventincertainformsofepilepsy.AmJMedSci
1910139:417.12.
LeestmaJE,WalczakT,HughesJR,etal.Aprospectivestudyonsuddenunexpecteddeathin
epilepsy.AnnNeurol198926:195.13.
MulroyJJ,MickellJJ,TongTK,PellockJM.Postictalpulmonaryedemainchildren.Neurology1985
35:403.14.
DarnellJC,JaySJ.Recurrentpostictalpulmonaryedema:acasereportandreviewoftheliterature.
Epilepsia198223:71.15.
QinSQ,SunW,WangHB,ZhangQL.Neurogenicpulmonaryedemainheadinjuries:analysisof5
cases.ChinJTraumatol20058:172.16.
PoppAJ,ShahDM,BermanRA,etal.Delayedpulmonarydysfunctioninheadinjuredpatients.J
Neurosurg198257:784.17.
BrattonSL,DavisRL.Acutelunginjuryinisolatedtraumaticbraininjury.Neurosurgery199740:707.18.
WeirBK.Pulmonaryedemafollowingfatalaneurysmrupture.JNeurosurg197849:502.19.
MuroiC,KellerM,PangaluA,etal.Neurogenicpulmonaryedemainpatientswithsubarachnoid
hemorrhage.JNeurosurgAnesthesiol200820:188.20.
FriedmanJA,PichelmannMA,PiepgrasDG,etal.Pulmonarycomplicationsofaneurysmalsubarachnoid
hemorrhage.Neurosurgery200352:1025.21.
SolenskiNJ,HaleyECJr,KassellNF,etal.Medicalcomplicationsofaneurysmalsubarachnoid
hemorrhage:areportofthemulticenter,cooperativeaneurysmstudy.ParticipantsoftheMulticenterCooperativeAneurysmStudy.CritCareMed199523:1007.
cautiously.(See'Supportivecare'above.)
AvarietyofmedicationshavebeenusedtotreatpatientswithNPE,buttheirefficacyinthissettinghasnotbeenestablished.(See'Medications'above.)
AlthoughmanyepisodesofNPEarewelltoleratedandresolve,thedevelopmentofNPEisassociatedwithworselongtermoutcomes
-
4/28/2015 Neurogenicpulmonaryedema
http://www.uptodate.com/contents/neurogenicpulmonaryedema?topicKey=PULM%2F1610&elapsedTimeMs=4&view=print&displayedView=full#
7/12
22.
FisherA,AboulNasrHT.Delayednonfatalpulmonaryedemafollowingsubarachnoidhemorrhage.Casereport.JNeurosurg197951:856.
23.
KimJE,ParkJH,LeeSH,LeeY.NeurogenicpulmonaryedemafollowingintracranialcoilembolizationforsubarachnoidhemorrhageAcasereport.KoreanJAnesthesiol201263:368.
24.
JunttilaE,AlaKokkoT,OhtonenP,etal.Neurogenicpulmonaryedemainpatientswithnontraumaticintracerebralhemorrhage:predictorsandassociationwithoutcome.AnesthAnalg2013116:855.
25.
SimonRP,GeanMartonAD,SanderJE.Medullarylesioninducingpulmonaryedema:amagneticresonanceimagingstudy.AnnNeurol199130:727.
26.
WrightRS,FeuermanT,BrownJ.Neurogenicpulmonaryedemaaftertrigeminalnerveblockade.Chest198996:436.
27.
LeeDS,KobrineA.Neurogenicpulmonaryedemaassociatedwithrupturedspinalcordarteriovenousmalformation.Neurosurgery198312:691.
28.
PragerP,NolanM,AndrewsIP,WilliamsGD.Neurogenicpulmonaryedemainenterovirus71encephalitisisnotuniformlyfatalbutcausesseveremorbidityinsurvivors.PediatrCritCareMed20034:377.
29.
ChenHI,SunSC,ChaiCY.Pulmonaryedemaandhemorrhageresultingfromcerebralcompression.AmJPhysiol1973224:223.
30.
ChenHI,ChaiCY.Integrationofthecardiovagalmechanisminthemedullaoblongataofthecat.AmJPhysiol1976231:454.
31.
NathanMA,ReisDJ.Fulminatingarterialhypertensionwithpulmonaryedemafromreleaseofadrenomedullarycatecholaminesafterlesionsoftheanteriorhypothalamusintherat.CircRes197537:226.
32.
BlessingWW,WestMJ,ChalmersJ.Hypertension,bradycardia,andpulmonaryedemaintheconsciousrabbitafterbrainstemlesionscoincidingwiththeA1groupofcatecholamineneurons.CircRes198149:949.
33.
MaronMB,DawsonCA.Pulmonaryvenoconstrictioncausedbyelevatedcerebrospinalfluidpressureinthedog.JApplPhysiolRespirEnvironExercPhysiol198049:73.
34.
MalikAB.Mechanismsofneurogenicpulmonaryedema.CircRes198557:1.35.
HakimTS,vanderZeeH,MalikAB.Effectsofsympatheticnervestimulationonlungfluidandprotein
exchange.JApplPhysiolRespirEnvironExercPhysiol197947:1025.36.
GAMBLEJE,PATTONHD.Pulmonaryedemaandhemorrhagefrompreopticlesionsinrats.AmJ
Physiol1953172:623.37.
REYNOLDSRW.PULMONARYEDEMAASACONSEQUENCEOFHYPOTHALAMICLESIONSIN
RATS.Science1963141:930.38.
MAIREFW,PATTONHD.Neuralstructuresinvolvedinthegenesisofpreopticpulmonaryedema,
gastricerosionsandbehaviorchanges.AmJPhysiol1956184:345.39.
MAIREFW,PATTONHD.Roleofthesplanchnicnerveandtheadrenalmedullainthegenesisof
preopticpulmonaryedema.AmJPhysiol1956184:351.40.
GarciaUriaJ,HoffJT,MirandaS,NishimuraM.ExperimentalneurogenicpulmonaryedemaPart2:The
roleofcardiopulmonarypressurechange.JNeurosurg198154:632.41.
DarraghTM,SimonRP.Nucleustractussolitariuslesionselevatepulmonaryarterialpressureandlymph
flow.AnnNeurol198517:565.42.
GrafCJ,RossiNP.Catecholamineresponsetointracranialhypertension.JNeurosurg197849:862.43.
InobeJJ,MoriT,UeyamaH,etal.Neurogenicpulmonaryedemainducedbyprimarymedullary
hemorrhage:acasereport.JNeurolSci2000172:73.44.
KeeganMT,LanierWL.Pulmonaryedemaafterresectionofafourthventricletumor:possibleevidence
foramedullamediatedmechanism.MayoClinProc199974:264.45.
SedJ,ZichaJ,KunesJ,etal.Mechanismsofneurogenicpulmonaryedemadevelopment.PhysiolRes
200857:499.46.
BrownRHJr,BeyerlBD,IsekeR,LavyneMH.Medullaoblongataedemaassociatedwithneurogenic
pulmonaryedema.Casereport.JNeurosurg198664:494.47.
ImaiK.Radiographicalinvestigationsoforganiclesionsofthehypothalamusinpatientssufferingfrom
neurogenicpulmonaryedemaduetoseriousintracranialdiseases:relationshipbetweenradiographicalfindingsandoutcomeofpatientssufferingfromneurogenicpulmonaryedema.NoShinkeiGeka200331:757.
-
4/28/2015 Neurogenicpulmonaryedema
http://www.uptodate.com/contents/neurogenicpulmonaryedema?topicKey=PULM%2F1610&elapsedTimeMs=4&view=print&displayedView=full#
8/12
48.
SmithWS,MatthayMA.Evidenceforahydrostaticmechanisminhumanneurogenicpulmonaryedema.Chest1997111:1326.
49.
HoffJT,NishimuraM,GarciaUriaJ,MirandaS.Experimentalneurogenicpulmonaryedema.Part1:Theroleofsystemichypertension.JNeurosurg198154:627.
50.
KadowitzPJ,JoinerPD,HymanAL.Influenceofsympatheticstimulationandvasoactivesubstancesonthecaninepulmonaryveins.JClinInvest197556:354.
51.
ElBermaniAW.Innervationofthemicrocirculation.AnnNYAcadSci1982384:21.52.
MacmillanCS,GrantIS,AndrewsPJ.Pulmonaryandcardiacsequelaeofsubarachnoidhaemorrhage:
timeforactivemanagement?IntensiveCareMed200228:1012.53.
SchraufnagelDE,ThakkarMB.Pulmonaryvenoussphincterconstrictionisattenuatedbyalpha
adrenergicantagonism.AmRevRespirDis1993148:477.54.
SedJ,ZichaJ,NedvdkovJ,KunesJ.Theroleofsympatheticnervoussysteminthedevelopmentof
neurogenicpulmonaryedemainspinalcordinjuredrats.JApplPhysiol(1985)2012112:1.55.
BahloulM,ChaariAN,KallelH,etal.Neurogenicpulmonaryedemaduetotraumaticbraininjury:
evidenceofcardiacdysfunction.AmJCritCare200615:462.56.
MayerSA,LinJ,HommaS,etal.Myocardialinjuryandleftventricularperformanceaftersubarachnoid
hemorrhage.Stroke199930:780.57.
LloydTCJr.Effectofincreasedintracranialpressureonpulmonaryvascularresistance.JApplPhysiol
197335:332.58.
BrashearRE,RossJC.Hemodynamiceffectsofelevatedcerebrospinalfluidpressure:alterationswith
adrenergicblockade.JClinInvest197049:1324.59.
CAMPBELLGS,HADDYFJ.Circulatorychangesandpulmonarylesionsindogsfollowingincreased
intracranialpressure,andtheeffectofatropineuponsuchchanges.AmJPhysiol1949158:96.60.
WrayNP,NicotraMB.Pathogenesisofneurogenicpulmonaryedema.AmRevRespirDis1978
118:783.61.
MayerSA,FinkME,HommaS,etal.Cardiacinjuryassociatedwithneurogenicpulmonaryedema
followingsubarachnoidhemorrhage.Neurology199444:815.62.
KowalskiML,DidierA,KalinerMA.Neurogenicinflammationintheairways.I.Neurogenicstimulation
inducesplasmaproteinextravasationintotheratairwaylumen.AmRevRespirDis1989140:101.63.
McClellanMD,DauberIM,WeilJV.Elevatedintracranialpressureincreasespulmonaryvascular
permeabilitytoprotein.JApplPhysiol(1985)198967:1185.64.
RosellS.Neuronalcontrolofmicrovessels.AnnuRevPhysiol198042:359.65.
TheodoreJ,RobinED.Speculationsonneurogenicpulmonaryedema(NPE).AmRevRespirDis1976
113:405.66.
WestJB,MathieuCostelloO.Stressfailureofpulmonarycapillaries:roleinlungandheartdisease.
Lancet1992340:762.67.
BowersRE,McKeenCR,ParkBE,BrighamKL.Increasedpulmonaryvascularpermeabilityfollows
intracranialhypertensioninsheep.AmRevRespirDis1979119:637.68.
TouhoH,KarasawaJ,ShishidoH,etal.Neurogenicpulmonaryedemaintheacutestageofhemorrhagic
cerebrovasculardisease.Neurosurgery198925:762.69.
LandoltCC,MatthayMA,AlbertineKH,etal.Overperfusion,hypoxia,andincreasedpressurecause
onlyhydrostaticpulmonaryedemainanesthetizedsheep.CircRes198352:335.70.
RasslerB,ReissigC,BriestW,etal.Pulmonaryedemaandpleuraleffusioninnorepinephrine
stimulatedratshemodynamicorinflammatoryeffect?MolCellBiochem2003250:55.71.
vanGoolJ,vanVugtH,HelleM,AardenLA.Therelationamongstress,adrenalin,interleukin6and
acutephaseproteinsintherat.ClinImmunolImmunopathol199057:200.72.
PiazzaO,LeggieroE,DeBenedictisG,etal.S100Binducesthereleaseofproinflammatorycytokines
inalveolartypeIlikecells.IntJImmunopatholPharmacol201326:383.73.
MasciaL.Acutelunginjuryinpatientswithseverebraininjury:adoublehitmodel.NeurocritCare2009
11:417.74.
HutchinsonPJ,O'ConnellMT,RothwellNJ,etal.Inflammationinhumanbraininjury:intracerebral
concentrationsofIL1alpha,IL1beta,andtheirendogenousinhibitorIL1ra.JNeurotrauma200724:1545.
75. ColiceGL.Neurogenicpulmonaryedema.ClinChestMed19856:473.
-
4/28/2015 Neurogenicpulmonaryedema
http://www.uptodate.com/contents/neurogenicpulmonaryedema?topicKey=PULM%2F1610&elapsedTimeMs=4&view=print&displayedView=full#
9/12
76.
CohenNH.VentilatormanagementintheNICU.In:CriticalCare,KellyB(Ed),AmericanAcademyofNeurologyCourse,AnnualMeeting,1994.
77.
FletcherSJ,AtkinsonJD.Useofproneventilationinneurogenicpulmonaryoedema.BrJAnaesth200390:238.
78.
HwangGJ,SheenSH,KimHS,etal.Extracorporealmembraneoxygenationforacutelifethreateningneurogenicpulmonaryedemafollowingruptureofanintracranialaneurysm.JKoreanMedSci201328:962.
79.
ProdhanP,CasavantD,MedlockMD,etal.Inhalednitricoxideinneurogeniccardiopulmonarydysfunction:implicationsfororgandonation.TransplantProc200436:2570.
80.
MutohT,KazumataK,KobayashiS,etal.Serialmeasurementofextravascularlungwaterandbloodvolumeduringthecourseofneurogenicpulmonaryedemaaftersubarachnoidhemorrhage:initialexperiencewith3cases.JNeurosurgAnesthesiol201224:203.
81.
MerenkovVV,KovalevAN,GorbunovVV.Bedsidelungultrasound:acaseofneurogenicpulmonaryedema.NeurocritCare201318:391.
82.
KnudsenF,JensenHP,PetersenPL.Neurogenicpulmonaryedema:treatmentwithdobutamine.Neurosurgery199129:269.
83.
DeehanSC,GrantIS.Haemodynamicchangesinneurogenicpulmonaryoedema:effectofdobutamine.IntensiveCareMed199622:672.
84.
WohnsRN,TamasL,PierceKR,HoweJF.Chlorpromazinetreatmentforneurogenicpulmonaryedema.CritCareMed198513:210.
Topic1610Version8.0
-
4/28/2015 Neurogenicpulmonaryedema
http://www.uptodate.com/contents/neurogenicpulmonaryedema?topicKey=PULM%2F1610&elapsedTimeMs=4&view=print&displayedView=full#
10/12
GRAPHICS
Causesofneurogenicpulmonaryedema
MajorcausesEpilepticseizures,particularlystatusepilepticus
Cerebralhemorrhage
Headinjury
MinorcausesGuillainBarrsyndrome
Multiplesclerosiswithmedullaryinvolvement
Nonhemorrhagicstrokes
Trigeminalnerveblock
Bulbarpoliomyelitis
Vertebralarteryligation
Rupturedspinalarteriovenousmalformation
Airembolism
Braintumors
Electroconvulsivetherapy
Inductionofgeneralanesthesia
Colloidcyst
Hydrocephalus
Reyesyndrome
Bacterialmeningitis
Viralmeningoencephalitis
Cervicalspinalcordinjury
Graphic57483Version2.0
-
4/28/2015 Neurogenicpulmonaryedema
http://www.uptodate.com/contents/neurogenicpulmonaryedema?topicKey=PULM%2F1610&elapsedTimeMs=4&view=print&displayedView=full#
11/12
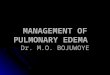
Capillaryhemodynamicforces
Schematicrepresentationofthecapillaryandinterstitialfluidhydraulic(P)andoncotic()pressurescontrollingfluidmovementacrossthecapillarywallbetweentheplasmaandtheinterstitialfluid.Thearrowspointinthedirectionoffluidmovementinducedbyeachoftheforces.
Graphic66819Version1.0
-
4/28/2015 Neurogenicpulmonaryedema
http://www.uptodate.com/contents/neurogenicpulmonaryedema?topicKey=PULM%2F1610&elapsedTimeMs=4&view=print&displayedView=full#
12/12
Disclosures:MatthewWemple,MDNothingtodisclose.MatthewHallman,MDNothingtodisclose.AndrewMLuks,MDNothingtodisclose.PollyEParsons,MDNothingtodisclose.GeraldineFinlay,MDNothingtodisclose.Contributordisclosuresarereviewedforconflictsofinterestbytheeditorialgroup.Whenfound,theseareaddressedbyvettingthroughamultilevelreviewprocess,andthroughrequirementsforreferencestobeprovidedtosupportthecontent.AppropriatelyreferencedcontentisrequiredofallauthorsandmustconformtoUpToDatestandardsofevidence.Conflictofinterestpolicy
Disclosures