Embed Size (px)
DESCRIPTION
Pulmonary Circulation Vol. 1 Issue 1 2011
Citation preview

Pulmonary Circulation
Journal of the Pulmonary Vascular Research Institute
Real-time imaging of a computational model of cell networking (please see COVER PHOTO inside)
ISSN : 2045-8932E-ISSN : 2045-8940
Volume 1, Number 1 (January-March 2011)
www.PulmonaryCirculation.org

COVER PHOTO: Computational model of coordinated pulmonary artery endothelial cell networking behavior during capillary formation. Real-time imaging of pulmonary vascular endothelial cells cultured within a specialized 3D extra-cellular matrix microenvironment formed the basis of this project. (Sabin+Jones LabStudio, University of Pennsylvania Departments of Pathology & Laboratory Medicine & Architecture, Nonlinear Systems Biology and Design. Credits: Jenny E. Sabin & Peter Lloyd Jones (instructors); Shuni Feng, Joshua Freese, and Jeffrey Nesbit.)
The Journal reserves the right to reject any advertisement considered unsuitable to the set policies of the Journal.
The appearance of advertising or product information in the various sections in the Journal does not constitute an endorsement or approval by the Journal and/or the Publisher of the quality or value of the said product or of claims made for it by its manufacturer.
Copyright
The entire contents of each issue of Pulmonary Circulation are protected under Indian and international copyright laws. The Journal, however, grants to all users a free, irrevocable, worldwide, perpetual right of access to, and a license to copy, use, distribute, perform and display the work publicly and to make and distribute derivative works in any digital medium for any reasonable noncommercial purpose, subject to proper attribution of authorship and ownership of the rights. The Journal also grants the right to make small numbers of printed copies for their personal noncommercial use.
Individual authors retain ownership to the copyrights of their particular articles. As a mandatory part of the manuscript submission process, the author assigns First Serial Rights to the Publisher, Medknow Publications and Media Pvt. Ltd., and agrees that any subsequent publication of his or her article will end with this parenthetical statement: “(This article was first published in Pulmonary Circulation, Volume, Number [year], pages).”
Permissions
For information on how to request permissions to reproduce articles from this journal, please visit www.pulmonarycirculation.org.
Disclaimer
The information and opinions presented in the Journal reflect the views of the authors providing them and not of the Journal or its Editorial Board or the Publisher. Publication does not constitute endorsement by the Journal. Neither Pulmonary Circulation nor the Publisher nor anyone else involved in the creation, production, or delivery of Pulmonary Circulation or the materials contained therein, assumes any liability or responsibility for the accuracy, completeness, or usefulness of any information provided in Pulmonary Circulation, nor shall they be liable for any direct, indirect, special, consequential or punitive damages arising from the use of Pulmonary Circulation. Neither Pulmonary Circulation nor the Publisher nor any party in the preparation of material contained in Pulmonary Circulation represents or warrants that the information contained herein is in every respect accurate or complete, and they are not responsible for any errors or omissions or for the results obtained from the use of such material. Readers are encouraged to confirm the information contained herein with other sources.
Addresses
Editorial OfficeLondon, UKPulmon ary Vascular Research Institute (PVRI)Nikki KrolEmail: [email protected]: www.pvri.infoJournal website: www.pulmonarycirculation.org
Published byMedknow Publications and Media Pvt. Ltd.B5-12, Kanara Business Centre,Off Link Road, Ghatkopar (East)Mumbai – 400075, IndiaPhone: 91-22-66491818Email: [email protected]: www.medknow.com
Printed byWill be inserting the printer’s name before it goes for print.???
The Journal
Pulmonary Circulation (print ISSN 2045-8932, online ISSN 2045-8940) is a peer-reviewed journal published on behalf of the Pulmonary Vascular Research Institute (PVRI). Published quarterly in the months of January, April, July and October, the Journal publishes original research articles and review articles related to the pulmonary circulation, pulmonary vascular medicine, and pulmonary vascular disease.
Abstracting and indexing information
The Journal is indexed/listed with Caspur, DOAJ, EBSCO Publishing’s Electronic Databases, Expanded Academic ASAP, GenamicsJournalSeek, Google Scholar, Hinari, Index Copernicus, OpenJGate, PrimoCentral, ProQuest, SCOLOAR, SIIC databases, Summon by Serial Solutions, and Ulrich’s International Periodical Directory.
Information for authors
There are no page charges for manuscript submissions. For details lease check http://www.pulmonarycirculation.org/contributors.asp. All manuscripts must be submitted online at www.journalonweb.com/pc.
Subscription information
Free print copies of the Journal are sent to all Fellows of the PVRI.”
A year’s subscription to Pulmonary Circulation comprises 4 regular issues and one supplemental issue. Prices include postage. The annual subscription rate for nonmembers is:
Institutional: USD 100.00 (or INR 1000.00)Personal: USD 50.00 (INR 500.00)
For mode of payment and other details, please visit www.medknow.com/subscribe.asp.
Additional and special supplements may be published from time to time, and they carry additional charges.
Claims for missing issues will be serviced if received within 60 days of the cover date for domestic subscribers, and within 3 months for subscribers outside India. Duplicate copies cannot be sent to replace issues not delivered because of failure to notify the Publisher, at the address shown below, of a change of address.
The Journal is published and distributed by Medknow Publications and Media Pvt. Ltd. Copies are sent to subscribers directly from the Publisher’s address. It is illegal to acquire copies from any other source. If a copy is received for personal use, one cannot resell the copy or give it away for commercial or library use.
The copies of Pulmonary Circulation to the members of the PVRI are sent by ordinary post. Neither the Publisher nor the PVRI nor the Journal’s Editorial Board will be responsible for any non-receipt of copies. If any member/subscriber wishes to receive his or her copies by registered post or courier, kindly contact the Publisher’s office. If a copy is returned due to an incomplete, incorrect, or changed address of a member/subscriber on 2 consecutive occasions, then the person’s name is deleted from the mailing list of the Journal. Providing a complete, correct and up-to-date address is the responsibility of the member/subscriber.
Nonmembers: Please send change of address information to [email protected].
Advertising
The Journal accepts both display and classified advertising. For prices and page positions, contact either Karen Gordon ([email protected], or 312/996-5023) or Dr. Jason Yuan ([email protected], or 312/355-5911). Frequency discounts and special positions are available. Inquiries about advertising may also be sent to Medknow Publications, [email protected].
GENERAL INFORMATION

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 i
Pulmonary CirculationAn official journal of the Pulmonary Vascular Research Institute
Editors-in-Chief Jason X.-J. Yuan, MD, PhD (Chicago, USA)
Nicholas W. Morrell, MD (Cambridge, UK)Harikrishnan S., MD (Trivandrum, India)
Senior Editor Executive Editor Ghazwan Butrous, MD (Canterbury, UK) Harikrishnan S., MD (Trivandrum, India)
ISSN 2045-8932, E-ISSN 2045-8940
Kurt R. Stenmark, MD (Denver, USA)Kenneth D. Bloch, MD (Boston, USA)Stephen L. Archer, MD (Chicago, USA)Marlene Rabinovitch, MD (Stanford, USA)Joe G.N. Garcia, MD (Chicago, USA)
Stuart Rich, MD (Chicago, USA)Martin R. Wilkins, MD (London, UK)Hossein A. Ghofrani, MD (Giessen, Germany)Candice D. Fike, MD (Nashville, USA)Werner Seeger, MD (Giessen, Germany)
Editors
Editorial Board
Scientific Advisory Board
Robert F. Grover, MD, PhD. (Denver, USA) John B. West, MD, PhD, DSc (San Diego, USA) Charles A. Hales, MD (Boston, USA) Magdi H. Yacoub, MD, DSc, FRS (London, UK) Joseph Loscalzo, MD (Boston, USA)
Steven H. Abman, MD, USASerge Adnot, MD, FranceVera D. Aiello, MD, BrazilAlmaz Aldashev, MD, PhD, Kyrgyz RepublicDiego F. Alvarez, MD, PhD, USARobyn J. Barst, MD, USAEvgeny Berdyshev, PhD, USAMichael A. Bettmann, MD, USAJahar Bhattacharya, MD, PhD, USAKonstantin G. Birukov, MD, USAMurali Chakinala, MD, USANavdeep S. Chantal, PhD, USARichard N. Channick, MD, USAHunter C. Champion, MD, USAShampa Chatterjee, PhD, USAXiansheng Cheng, MD, ChinaNaomi C. Chesler, PhD, USAAugustine M.K. Choi, MD, USAPaul A. Corris, MD, UKDavid N. Cornfield, MD, USAMichael J. Cuttica, MD, USAHiroshi Date, MD, PhD, JapanRegina M. Day, USASteven M. Dudek, MD, USARaed A. Dweik, MD, USAYung E. Earm, MD, PhD, KoreaJeffrey D. Edelman, MD, USAOliver Eickelberg, PhD, GermanyC. Gregory Elliott, MD, USASerpil Erzurum, MD, USAA. Mark Evans, PhD, UKKaren A. Fagan, MD, USABarry L. Fanburg, MD, USAHarrison W. Farber, MD, USAJeffrey A. Feinstein, MD, USA Jeffrey Fineman, MD, USAPatricia W. Finn, MD, USASonia C. Flores, PhD, USAPaul R. Forfia, MD, USARobert Frantz, MD, USAM. Patricia George, MD, USAMark W. Geraci, MD, USAStefano Ghio, MD, ItalyMark N. Gillespie, PhD, USA
Reda Girgis, MD, USAMark T. Gladwin, MD, USAMardi Gomberg-Maitland, MD, USAAndy Grieve, PhD, GermanyAlison M. Gurney, PhD, UKElizabeth O. Harrington, PhD, USAC. Michael Hart, MD, USAPaul M. Hassoun, MD, USAAbraham G. Hartzema, USAJianguo He, MD, ChinaJan Herget, MD, PhD, Czech RepublicNicholas S. Hill, MD, USAMarius M. Hoeper, MD, GermanyEric A. Hoffman, PhD, USAYuji Imaizumi, PhD, JapanDunbar Ivy, MD, USAJeffrey R. Jacobson, MD, USARoger Johns, MD, PhD, USAPeter L. Jones, PhD, USANaftali Kaminski, MD, USAChandrasekharan C. Kartha, MD, India Steven M. Kawut, MD, USAAnn M. Keogh, MD, AustraliaNick H. Kim, MD, USASung Joon Kim, MD, PhD, KoreaJames R. Klinger, MD, USAStella Kourembanas, MD, USAMichael J. Krowka, MD, USAThomas J. Kulik, MD, USAR. Krishna Kumar, MD, DM, IndiaSteven Kymes, PhD, USADavid Langleben, MD, CanadaTimothy D. Le Cras, PhD, USA Normand Leblanc, PhD, USAFabiola Leon-Velarde, MD, PeruIrena Levitan, PhD, USAJose Lopez-Barneo, MD, PhD, SpainWenju Lu, MD, PhD, ChinaRoberto Machado, MD, USAMargaret R. MacLean, PhD, UKMichael M. Madani, MD, USAAyako Makino, PhD, USAAsrar B. Malik, PhD, USAJess Mandel, MD, USA
Michael A. Matthay, MD, USAMarco Matucci-Cerinic, MD, PhD, ItalyPaul McLoughlin, PhD, IrelandIvan F. McMurtry, PhD, USADolly Mehta, PhD, USAMarilyn P. Merker, PhD, USABarbara O. Meyrick, PhD, USAEvangelos Michelakis, MD, CanadaOmar A. Minai, MD, USALiliana Moreno, PhD, USATimothy A. Morris, MD, USAKamal K. Mubarak, MD, USASrinivas Murali, MD, USAFiona Murray, PhD, USAKazufumi Nakamura, MD, PhD, JapanNorifumi Nakanishi, MD, PhD, JapanRobert Naeije, MD, BelgiumViswanathan Natarajan, PhD, USAJohn H. Newman, MD, USAAndrea Olschewski, MD, AustriaHorst Olschewski, MD, AustriaStylianos E. Orfanos, MD, Greece Ronald J. Oudiz, MD, USAHarold Palevsky, MD, USA Lisa A. Palmer, PhD, USAMyung H. Park, MD, USAQadar Pasha, PhD, IndiaAndrew J. Peacock, MD, UKJoanna Pepke-Zaba, MD, UKNicola Petrosillo, MD, ItalyBruce R. Pitt, PhD, USANanduri R. Prabhakar, PhD, USA Ioana R. Preston, MD, USATomas Pulido, MD, MexicoSoni S. Pullamsetti, PhD, GermanyGoverdhan D. Puri, MD, India Rozenn Quarck, PhD, BelgiumDeborah A. Quinn, MD, USAJ. Usha Raj, MD, USAAmer Rana, PhD, USAThomas C. Resta, PhD, USA Ivan M. Robbins, MD, USASharon I. Rounds, MD, USA Nancy J. Rusch, PhD, USA
Tarek Safwat, MD, EgyptSami I. Said, MD, USAJulio Sandoval, MD, MexicoMaria V.T. Santana, MD, Brazil Bhagavathula K. Sastry, MD., IndiaAnita Saxena, MD, IndiaMarc J. Semigran, MD, USARalph T. Schermuly, MD, GermanyDean Schraufnagel, MD, USAPaul T. Schumacker, PhD, USAPravin B. Sehgal, MD, PhD, USAJames S.K. Sham, PhD, USASteven D. Shapiro, MD, USALarisa A. Shimoda, PhD, USARobin H. Steinhorn, MD, USATroy Stevens, PhD, USADuncan J. Stuart, MD, CanadaYuchiro J. Suzuki, PhD, USAVictor F. Tapson, MD, USAMerryn H. Tawhai, PhD, New ZealandDick Tibboel, MD, PhD, The NetherlandsChristoph Thiemermann, MD, PhD, UKMary I. Townsley, PhD, USARichard C. Trembath, MD, UKRubin M. Tuder, MD, USACarmine D. Vizza, MD, Italy Norbert F. Voelkel, MD, USAPeter D. Wagner, MD, USAWiltz W. Wagner, Jr., PhD, USAJian Wang, MD, USAJian-Ying Wang, MD, USAJun Wang, MD, PhD, ChinaXingxiang Wang, MD, ChinaJeremy P.T. Ward, PhD, UKAaron B. Waxman, MD, USANorbert Weissmann, PhD, GermanyJames D. West, PhD, USAR. James White, MD, USASean W. Wilson, PhD, USAMichael S. Wolin, PhD, USATianyi Wu, MD, ChinaLan Zhao, MD PhD, UKNanshan Zhong, MD, ChinaBrian S. Zuckerbraun, MD, USA
Sheila G. Haworth, MD (London, UK)Patricia A. Thistlethwaite, MD, PhD (San Diego, USA)Chen Wang, MD, PhD (Beijing, China)Antonio A. Lopes, MD, PhD (Sao Paulo, Brazil)
Editorial Staff Nikki Krol (London, UK), [email protected] Karen Gordon (Chicago, USA), [email protected] Paul Soderberg (Phoenix, USA), [email protected]

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 ii
Pulmonary CirculationAn official journal of the Pulmonary Vascular Research Institute
| January-March 2011 | Vol 1 | No 1 |
CONTENTS
General Information Inside front cover
Editors and Board Members i
Welcome
Pulmonary Circulation: A new venue for communicating your findings, ideas and perspectivesJason X.-J. Yuan, Nicholas W. Morrell, Harikrishnan S., Ghazwan Butrous 1
Review Articles
Progenitor cells in pulmonary vascular remodelingMichael E. Yeager, Maria G. Frid, Kurt R. Stenmark 3
Protein trafficking dysfunctions: Role in the pathogenesis of pulmonary arterial hypertensionPravin B. Sehgal, Jason E. Lee 17
Is peroxisome proliferator-activated receptor gamma (PPAR) a therapeutic target for the treatment of pulmonary hypertension?
David E. Green, Roy L. Sutliff , C. Michael Hart 33
Functional ion channels in human pulmonary artery smooth muscle cells: Voltage-dependent cation channels
Amy L. Firth, Carmelle V. Remillard, Oleksandr Platoshyn, Ivana Fantozzi, Eun A. Ko, Jason X.-J. Yuan 48
Research Articles
Oxidative injury is a common consequence of BMPR2 mutationsKirk L. Lane, Megha Talati, Eric Austin, Anna R. Hemnes, Jennifer A. Johnson, Joshua P. Fessel, Tom Blackwell, Ray L. Mernaugh, Linda Robinson, Candice Fike, L. Jackson Roberts II, James West 72
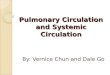
STIM2 contributes to enhanced store-operated Ca2+ entry in pulmonary artery smooth muscle cells from patients with idiopathic pulmonary arterial hypertension
Michael Y. Song, Ayako Makino, Jason X.-J. Yuan 84
Rab7STAT3
EGFR
12 VDCC- 1α C
Kv1.1
Kv1.5Kv1.6
MaxiK-β4
VDCC-β3SCN8A
LEFT TO RIGHT: pages 19, 126, 80, 30, and 53

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 iii
Doppler-defined pulmonary hypertension in medical intensive care unit patients: Retrospective investigation of risk factors and impact on mortality
Jason A. Stamm, Bryan J. McVerry, Michael A. Mathier, Michael P. Donahoe, Melissa I. Saul, Mark T. Gladwin 95
Expression of mutant BMPR-II in pulmonary endothelial cells promotes apoptosis and a release of factors that stimulate proliferation of pulmonary arterial smooth muscle cells
Xudong Yang, Lu Long, Paul N. Reynolds, Nicholas W. Morrell 103
Short Research Report
Combination use of sildenafil and simvastatin increases BMPR-II signal transduction in rats with monocrotaline-mediated pulmonary hypertension
Tuguang Kuang, Jun Wang, Amy Zeifman, Baosen Pang, Xiuxia Huang, Elyssa D. Burg, Jason X.-J. Yuan, Chen Wang 111
Case Reports
Severe pulmonary artery hypertension following intracardiac repair of tetralogy of Fallot: An unusual finding
Bhupesh Kumar, Goverdhan D. Puri, RohitManoj, Kirti Gupta, Shyam K. S. 115
Clinical demonstration of efficiency and reversibility of hypoxic pulmonary vasoconstriction in a patient presenting with unilateral incomplete bronchial occlusion
Syeda Jafri, Pasupathy Sivasothy, Francis Wells, Nicholas W. Morrell 119
Snapshot
Diagnostic and therapeutic algorithm for pulmonary arterial hypertensionAnkit A. Desai, Roberto F. Machado 122
Announcement
The PVM History Initiative of the PVRIGhazwan Butrous
Contributions to Pulmonary Circulation 127
Call for Papers Inside back cover
STIM11.0
1.5
2.0
aliz
ed to
NPH
)
IPAHNPH 1 2 1 2
b
75
kD
0.0
0.5
1
STIM
1 Pr
otei
n Le
vel
(Nor
ma
NPH IPAH
β-tub
1.5
2.0
oN
PH)
*
STIM2
IPAHNPH 1 2 1 2
c
50
kD
0.0
0.5
1.0
1
STIM
2 Pr
otei
n L
evel
(N
orm
aliz
ed to
NPH IPAH
STIM2
β-tub
75
50
CONTENTS continued
LEFT TO RIGHT: pages 88, 39, 120, and 106

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 iv
Author Institution Mapping (AIM)
Please note that not all the institutions may get mapped due to non-availability of the requisite information in the Google Map. For AIM of other issues, please check the Archives/Back Issues page on the journal’s website.

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 1
Pulmonary CirculationPulmonary Circulation: A new venue for communicating your fi ndings, ideas and
perspectives
Welcome
Pulmonary circulation is the flow of blood from the right ventricle through the pulmonary artery to the lungs, where carbon dioxide (CO2) is exchanged for oxygen (O2), and back through the pulmonary vein to the left atrium. The pulmonary vasculature includes the arteries from the main pulmonary to the precapillary arterioles, the capillaries, and the vein from the capillary to the left atrium. – Wikipedia.
The pulmonary circulation, once referred to as the lesser circulation, is now a circulatory system that medical and research professionals (as well as patients) can no longer ignore. Based on the World Health Organization’s (WHO) annual report in 2010, pulmonary vascular disease (e.g., pulmonary hypertension, pulmonary embolism) affects more than two million people in the world. The survival from idiopathic pulmonary arterial hypertension (IPAH), a rare form of pulmonary hypertension that predominantly affects younger women, is similar to cancer and is worse than many ischemic cardiovascular diseases.
In PubMed, “pulmonary vascular disease” generates almost 90,000 publications, while “pulmonary artery” generates more than 62,000 hits. “Hypertension” yields 321,623 publications, of which 38,486 are related to pulmonary hypertension. “Artery” generates 597,907 hits, of which 78,734 publications are related to “pulmonary artery.” “Heart” generates 956,653 publications, of which there are 153,194 publications related to “left heart” and 73,071 publications related to “right heart.” These data indicate that approximately 15% of the publications in the cardiovascular field are related to pulmonary circulation.
There are many journals currently available in the fields of cardiology, cardiovascular physiology, cardiovascular disease, systemic circulation and systemic hypertension, as well as lung biology, respiratory physiology and pathophysiology. For many years, physicians, investigators and trainees with an interest in the field of pulmonary circulation and pulmonary vascular disease published their work in general medical journals (e.g., Journal of Clinical Investigation, Nature Medicine, New England Journal Medicine and Lancet), general heart and circulation journals (e.g., Circulation, Circulation Research, American
Journal of Physiology Heart and Circulatory Physiology), general lung and respiratory journals (e.g., Chest, European Respiratory Journal, American Journal of Respiratory and Critical Care Medicine, American Journal of Respiratory Cellular and Molecular Medicine) and pharmacological and physiological journals (e.g., American Journal of Physiology Lung Cellular and Molecular Physiology, Journal of Applied Physiology, American Journal of Pathology and British Journal of Pharmacology). We should be rightly proud of the great and extensive contributions made during the last century by physicians and investigators in the pulmonary circulation field and published in the prestigious journals mentioned above. However, journals specifically aiming at the pulmonary circulation and pulmonary vascular diseases are not available at present.
After discussion with many colleagues in the field, there was widely held enthusiasm for a new and specialized journal for: (a) physicians, surgeons and practitioners in pulmonary and critical care medicine, cardiology, cardiothoracic surgery, heart/lung transplant surgery, pediatric pulmonology and pediatric cardiology, whose clinical responsibilities include taking care of patients with pulmonary vascular diseases; (b) basic science investigators whose primary research interests center on pulmonary circulation, pulmonary vascular physiology and pathophysiology, pulmonary vascular diseases, lung vascular biology and acute lung injury; and (c) cardiopulmonary subspecialty fellows, postdoctoral research fellows, medical and graduate students who are interested in developing an academic career in the clinical management of patients with pulmonary vascular disease and in clinical, translational and basic research on pulmonary circulation. Providing a high-quality venue for these investigators and clinicians to publish articles relevant to the pulmonary circulation is the major goal for this new journal, Pulmonary Circulation.
As evidenced in this current issue, Pulmonary Circulation will publish (i) original articles in basic and clinical research, (ii) review articles on clinical and research topics, (iii) progress in clinical trials, (iv) new techniques and technology and (v) case reports. Pulmonary Circulation will publish articles on the topics related to (a) molecular and cell biology, structure and morphology,

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 2
physiology and pathophysiology and translational research topics of the pulmonary circulation, (b) the state-of-the-art techniques and their potential applications in diagnosis and treatment of pulmonary vascular diseases, (c) clinical diagnosis and treatment and surgical interventions of pulmonary vascular diseases and (d) techniques and technology applied to research on pulmonary vasculature and to clinical management of pulmonary vascular diseases.
We believe that Pulmonary Circulation will appeal to two main audiences. The primary group is the physicians, surgeons, clinical scientists, basic science researchers and cardiopulmonary and critical care practitioners, whose clinical activity and research interests are primarily focused on pulmonary vascular disorders. In addition, postdoctoral fellows, medical students and graduate students will comprise another major audience for the journal. This is also a journal for libraries in medical schools and universities that contain biomedical science departments, and also in veterinary medical schools. A second group is the investigators in pharmaceutical companies who conduct clinical and basic research on developing diagnostic and therapeutic approaches for patients with pulmonary vascular disease and other cardiopulmonary diseases.
The journal is sponsored and published by the Pulmonary Vascular Research Institute (PVRI, www.pvri.info), an international and not-for-profit medical research organization devoted to increasing awareness and knowledge of pulmonary vascular disease. The journal is printed and distributed by Medknow Publishing Ltd. (Mumbai, India). We sincerely appreciate the support and effort put forth by the colleagues at PVRI and Medknow to achieve the goal; it would not have happened without the support and encouragement from the members and fellows of PVRI and the staff of Medknow.
The editorial board of Pulmonary Circulation is composed of three editors-in-chief (Jason Yuan, Nick Morrell and Harikrishnan S.), a senior editor (Ghazwan Butrous), an executive editor (Harikrishnan S), 14 editors (Kurt Stenmark, Ken Bloch, Stephen Archer, Marlene Rabinovitch, Skip Garcia, Stuart Rich, Martin Wilkins, Ardi Ghofrani, Candice Fike, Werner Seeger, Glennis Haworth, Patty Thistlethwaite, Chen Wang and Antonio Lopes), five scientific advisory board members (Bob Grover, Charles Hales, Joe Loscalzo, John West and Magdi Yacoub) and 170 members from countries across the globe – the United States, Canada, Mexico, Brazil, Peru, the United Kingdom, Germany, France, Belgium, The Netherlands, Kyrgyz Republic, Spain, Ireland, Austria, Czech Republic, Italy, Greece, Egypt, India, Japan, Korea, China, Australia and New Zealand. Furthermore, there are two editorial
assistants, Nikki Krol and Karen Gordon, who work in the journal’s editorial offices in London, UK and Chicago, USA, respectively.
We truly appreciate the support and enthusiasm of all the members on the editorial board for establishing this journal, and the fantastic encouragement of our colleagues in the field. We look forward to working with you all to make the new journal a communication medium that you and your colleagues would like to use to convey your research findings, scientific perspectives and clinical experience with the physicians and investigators in the world.
In order to establish a journal with high impact and broad visibility, the quality of the papers it publishes and the reputation of its authors (laboratories and research groups) are the key, especially in the journal’s early days. Therefore, we strongly urge you to submit your next manuscript to Pulmonary Circulation. All manuscripts, of course, will go through the peer-review process; the editorial office will make sure to process your manuscript as fast as possible. We will try our best to make Pulmonary Circulation an interesting and informative journal that you would like to read, to cite and to recommend to your students and colleagues.
“Those who know don’t lecture; those who lecture don’t know... The wise are heard through their silence, always self-full through selflessness,” Lao Tzu said more than two thousands of years ago. It is time for us to be silent so we can hear from you, the good, the bad and either or neither.
Jason X.-J. Yuan1, Nicholas W. Morrell2, Harikrishnan S.3, Ghazwan Butrous4
1Departments of Medicine and Pharmacology, The Institute for Personalized Respiratory Medicine, University of Illinois at Chicago,
Chicago, IL 60611, USA; 2Department of Medicine, Division of Respiratory Medicine, University of Cambridge School of Clinical
Medicine, Addenbrooke’s Hospital, Cambridge, CB2 0QQ, UK; 3Department of Cardiology, Sree Chitra Tirunal Institute for Medical
Sciences and Technology, Thiruvananthapuram - 695 011, Kerala, India; 4University of Kent, Canterbury, CT2 7LR, UK
E-mail: [email protected]
Yuan, et al.: A new journal for pulmonary vascular disease
Access this article online
Quick Response Code:Website: www.pulmonarycirculation.org
DOI: 10.4103/2045-8932.78094
Pulm Circ 2011;1:1-2

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 3
Progenitor cells in pulmonary vascular remodeling
Michael E. Yeager1, Maria G. Frid2, Kurt R. Stenmark2
1Department of Pediatrics and Critical Care, University of Colorado at Denver and Health Sciences Center, 2Developmental Lung Biology Laboratory, Denver, Colorado, USA
ABSTRACT
Pulmonary hypertension is characterized by cellular and structural changes in the walls of pulmonary arteries. Intimal thickening and fi brosis, medial hypertrophy and fi broproliferative changes in the adventitia are commonly observed, as is the extension of smooth muscle into the previously non-muscularized vessels. A majority of these changes are associated with the enhanced presence of α-SM-actin+ cells and infl ammatory cells. Atypical abundances of functionally distinct endothelial cells, particularly in the intima (plexiform lesions), and also in the perivascular regions, are also described. At present, neither the origin(s) of these cells nor the molecular mechanisms responsible for their accumulation, in any of the three compartments of the vessel wall, have been fully elucidated. The possibility that they arise from either resident vascular progenitors or bone marrow–derived progenitor cells is now well established. Resident vascular progenitor cells have been demonstrated to exist within the vessel wall, and in response to certain stimuli, to expand and express myofi broblastic, endothelial or even hematopoietic markers. Bone marrow–derived or circulating progenitor cells have also been shown to be recruited to sites of vascular injury and to assume both endothelial and SM-like phenotypes. Here, we review the data supporting the contributory role of vascular progenitors (including endothelial progenitor cells, smooth muscle progenitor cells, pericytes, and fi brocytes) in vascular remodeling. A more complete understanding of the processes by which progenitor cells modulate pulmonary vascular remodeling will undoubtedly herald a renaissance of therapies extending beyond the control of vascular tonicity and reduction of pulmonary artery pressure.
Key Words: Fibrocyte, pericyte, angiogenesis, inflammation
Access this article online
Quick Response Code:Website: www.pulmonarycirculation.org
DOI: 10.4103/2045-8932.78095
Pulm Circ 2011;1:3-16
Address correspondence to:Prof. Kurt R. StenmarkPediatric Critical Care Medicine,Developmental Lung Biology Research and, Cardiovascular Pulmonary Research Laboratories,University of Colorado, Denver, Research Complex 2, 12700 E. 19th Avenue, Mail Stop B131, Aurora, Colorado 80045 USAE-mail: [email protected]
INTRODUCTION
Pulmonary hypertension is characterized by cellular and structural changes in the walls of the pulmonary arteries. Intimal thickening and fibrosis, medial hypertrophy, and fibroproliferative changes in the adventitia are commonly observed, as is the extension of smooth muscle into previously non-muscularized vessels. A majority of these changes are associated with the enhanced presence of α-SM-actin+ cells and inflammatory cells.[1-4] Atypical abundances of functionally distinct endothelial cells, particularly in the intima (plexiform lesions) and also in the perivascular regions, are now described.[5,6] At present, neither the origin(s) of these cells nor the molecular mechanisms responsible for their accumulation in any of the three compartments of the vessel wall, have been fully elucidated.
Regarding their origin, it has been postulated that α-SM-actin-expressing cells accruing in systemic and pulmonary vascular lesions are exclusively derived from resident vascular smooth muscle cells (SMC) and / or from adventitial fibroblasts via ‘de-differentiation’ of the former or ‘differentiation’ of the latter [Figure 1]. Over the past decade, however, this concept has been expanded by new experimental data, suggesting many alternative sources of α-SM-actin-expressing cells (SM-like cells or myofibroblasts), in various vascular diseases, including pulmonary hypertension. For instance, the possibility that both epithelial and endothelial cells have the capability of transitioning into a mesenchymal, SM-like phenotype has been raised [Figure 1].[7-9] Resident vascular progenitor cells have been demonstrated to exist
Review Ar t ic le

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 4
within the vessel wall, and in response to certain stimuli, to expand and express myofibroblastic, endothelial or even hematopoietic markers.[10-14] Multipotent resident lung vascular progenitors have also been demonstrated to reside within the Hoechstlow lung side population of the cells.[15,16] Bone marrow–derived or circulating progenitor cells have also been seen to be recruited to sites of vascular injury and to assume both endothelial and SM-like phenotypes [17-19] [Figure 1]. Here, we review the data supporting a contributory role for vascular progenitors (including endothelial progenitor cells, smooth muscle progenitor cells, pericytes, and fibrocytes) in systemic and pulmonary vascular remodeling. A more complete understanding of the processes by which progenitor cells modulate pulmonary vascular remodeling, will undoubtedly herald a renaissance of therapies extending beyond the control of vascular tonicity and reduction of pulmonary artery pressure.
Origin and phenotypic characterization of circulating endothelial, smooth muscle, and fibroblast / myofibroblast (i.e., fibrocytes) progenitors Circulating endothelial precursorsCurrently, endothelial progenitor cells (EPCs) represent the most widely studied adult human progenitor cell subpopulation. Their discovery in 1997, by Asahara et al., marks a milestone in our understanding of the development of blood vessels in an adult.[20] EPCs are most commonly thought to be of bone marrow origin, but have recently been reported to also reside in the vascular adventitia,[21,22] and perhaps may also even exist in endothelium lining of blood vessels.[14,23-26] At present, however, the definition of EPC remains controversial and is not yet consistent.[27] Most commonly, marker combinations for identifying the putative circulating EPC comprise certain hematopoietic lineage markers, such as, CD133, CD34, VEGFR-2, Tie-2, and UEA-1 lectin.[24,25,27-29] However, recent studies have provided growing evidence supporting the inclusion of some circulating myeloid cells as functional EPCs, which can contribute to endothelial regeneration and ischemic or tumor angiogenesis. These cells are characterized by the expression of CD14; the subpopulations include CD14+ / CD34low, CD14+ / VEGFR-2+, CD14+ / VEGFR2+ / CXCR2+, and CD14low / CD16+ / Tie-2+.[30,31] Thus, it seems that circulating pools of functional EPCs correspond to a rather heterogeneous cell population of multiple origins, phenotypes, and tissue distribution. The common features of these cells, arguably, encompass the expression of the progenitor and endothelial markers (i.e., CD34, VEGFR2, CD31, VE-cadherin, von Willebrand Factor), colony forming capacity, and differentiation toward the endothelial lineage, with formation of angiogenic structures in vitro as well as in vivo.[25,27,30] The function of these EPCs in vivo is not known
and may depend on the interplay with the inflammation and the tissue microenvironment. Investigators have also explored the growth properties and colony forming unit (CFU) potential of these cells, which have been found to be useful as biomarkers for outcomes in acute lung injury, as well as in cardiovascular diseases, including pulmonary hypertension.[32-35]
Circulating smooth muscle precursorsAnother vascular progenitor subtype, the smooth muscle progenitor cell (SPCs), has not been studied as intensively as the EPC. It has been shown that, similar to the EPCs, these progenitor cells can reside in the bone marrow, can circulate, or can be found in the peripheral tissues. Circulating SPCs can be distinguished by the expression of markers of mesenchymal / smooth muscle lineage, such as, endoglin (CD105), α-SM-actin (α -SMA), calponin, SM-myosin heavy chain (SM-MHC), SM22, or platelet-derived growth factor receptor-β (PDGFR-β).[36-39] Bone marrow–derived cells expressing smooth muscle markers have been observed in the remodeled intima of patients who have undergone sex-mismatched bone marrow transplants.[18,40] Furthermore, in a murine model, a subpopulation of sorted c-Kitneg / Sca-1+ / Linneg / PDGFR-β+ cells was reported to acquire the phenotype of mature SMCs in the presence of a platelet-derived growth factor-BB (PDGF-BB).[38] They are speculated to promote atherosclerotic plaque formation by producing extracellular matrix proteins.[39,41]
Yeager, et al.: Progenitor cells in pulmonary vascular remodeling
Figure 1: Potential origins of fi broblasts / myofi broblasts in the vessel wall. Several potential origins for tissue myofi broblasts have been proposed: (1) In several organs, α-SMA-expressing myofi broblasts are believed to originate from tissue-resident fi broblasts; (2) In the vasculature, myofi broblasts may arise through de-differentiation of resident SMC; (3) Epithelial cells can give rise to fi broblasts / myofi broblasts in the lung and other organs through a process of endothelial-mesenchymal transdifferentiation (EMT); (4) In the lung, endothelial-to-mesenchymal (EnMT) transition may provide another mechanism to generate myofi broblasts; (5) In various fi brotic lesions in tissue injury/ repair processes, bone marrow-derived circulating progenitor cells are proposed, to contribute to the pool of myofi broblasts (Adapted from Hinz et al.) [8]

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 5
Interestingly, similar to EPCs, human myeloid CD14+ SPCs have also been recently identified as a circulating CD14+ / CD105+ subpopulation.[37]
Circulating fibroblast precursors: fibrocytesAnother cell type that has received much attention as a potential vascular progenitor is the fibrocyte. Fibrocytes are bone marrow–derived mesenchymal progenitors that co-express hematopoietic stem cell antigens, markers of the monocyte lineage, and fibroblast products.[42-46] These cells produce extracellular matrix (ECM) components as well as ECM-modifying enzymes and can further differentiate into myofibroblasts both in vitro and in vivo, under permissive microenvironmental conditions.[43] Fibrocytes express the common leukocyte antigen CD45 as well as monocyte markers CD11a and b, and are variably reported to express CD14 and CD34. Upon stimulation, these cells express type 1 collagen, fibronectin, vimentin, and MMP-9. This expression pattern has led several investigators to hypothesize that fibrocytes, like some dendritic cell subsets, derive from precursors of the monocyte lineage. In fact, these cells express the major histocompatability complex class I and class II and the co-stimulatory molecules CD80 and CD86. Fibrocytes also exhibit antigen-presenting activity, and activate both the CD4 and CD8 T-lymphocytes.[43,46,47] The combination of collagen production and expression of CD45 (or one of the hematopoietic or myeloid antigens, CD11b, CD13 or CD34) is considered as sufficient criteria to discriminate fibrocytes from leukocytes, dendritic cells, endothelial cells, and tissue resident fibroblasts in vivo and in vitro. Fibrocytes can be distinguished from circulating or tissue resident mesenchymal stem / stromal cells, because the latter cells do express fibroblast products, but do not express CD34 or CD45, or the monocyte markers.[48]
Several factors effect the differentiation of fibrocytes from CD14+ monocyte precursors into mature mesenchymal cells. PDGF, interleukin (IL)-4, and IL-13 promote the differentiation of CD14+ mononuclear cells into fibrocytes.[49] By contrast, serum amyloid-P (SAP) inhibits the differentiation of CD14+ mononuclear cells into fibrocytes.[49,50] Recent studies also suggest that TH-1 derived cytokines such as IL-12 and interferon-γ may inhibit fibrocyte differentiation. On the other hand, TH-2 products, such as IL-4 and IL-13, stimulate fibrocyte differentiation as does TGF-β. Further differentiation into cells, ultrastructurally, phenotypically, and functionally similar to mature fibroblasts and / or myofibroblasts is promoted by stimulation with TGF-β or endothelin.[49] The resulting cell population produces more collagen and fibronectin than the relatively immature fibrocyte. In certain circumstances, the fibrocyte begins to express α-SM-actin, while downregulating the leukocyte marker expression, and assumes a myofibroblast phenotype.
Resident endothelial, smooth muscle, and fibroblast / myofibroblast progenitorsResident intimal progenitorsIn addition to a circulating source of EPCs and mesenchymal cells, there is increasing evidence to suggest that cells with progenitor characteristics exist within the vessel wall. Pioneering research uncovering endothelial cell division and proliferation by tritiated thymidine uptake is now nearing its fortieth anniversary.[51] A few years later, it was determined that endothelial proliferation could increase during injury and that the replicating endothelial cells appeared in clusters termed ‘high turnover regions’.[52] Following the discovery of circulating EPCs, it was demonstrated that EPCs exist in the wall of the human embryonic aorta, which can differentiate into mature endothelial cells and form vascular-like structures under in vitro conditions.[26,53] Further studies revealed the presence of a complete hierarchy of EPCs in the wall of the human adult blood vessels as well as umbilical cord.[26,54] Recently, it was shown that large- and middle-sized human arteries and veins in several organs contain EPCs in a distinct zone of the vascular wall (termed ‘vascular wall-resident EPCs’, VW-EPCs), and that the region was named the ‘vasculogenic zone’ [Figure 2]. This zone was located between the outer media and the adventitial layers.[10,14] Interestingly, the VW-EPCs were reported to differentiate not only into mature endothelial cells, but also into hematopoietic and local immune cells such as macrophages. In the vessel wall these cells were not CD34+, but CD31-, and they also expressed VEGFR-2 and Tie-2. Only a few cells in this zone of the vascular wall were positive for a leukocytic antigen CD45. Most intriguingly, recent findings suggested that some circulating EPCs might in fact derive from the intimal vascular endothelial layer,[54] perhaps in regions such as the ‘vasculogenic zones’. If confirmed, such a phenomenon would make
Yeager, et al.: Progenitor cells in pulmonary vascular remodeling
Figure 2: Hypothetical scheme illustrating the concept of the ‘vasculogenic zone’. This vascular mural zone at the border between the media and adventitia contains EPCs and probably also multipotent mesodermal stem cells. EPCs present in this zone are proposed to differentiate into endothelial cells and form capillary-like sprouts from the vascular wall, whereas, the multipotent mesodermal stem cells in this zone may serve as precursors of macrophages, fi broblasts, and SMC (Adapted from Zengin et al.) [14]

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 6
Yeager, et al.: Progenitor cells in pulmonary vascular remodeling
unclear the current distinctions between resident and circulating progenitors, and potentially also between the processes of angiogenesis and vasculogenesis.
Resident adventitial progenitorsOther investigators have reported that non-EPC progenitor cells reside in the adventitia of the vessel wall and are capable of giving rise to vascular wall cells including SMCs. Hu et al. reported that stem cell antigen-1 (Sca-1)+ cells, with a potential to differentiate into SMC, reside in the aortic adventitia of adult mice.[55] Subsequent studies by Passman et al. have confirmed the presence of Sca-1+ progenitor cells at the medial-adventitial border. In vivo, these adventitial Sca-1+ cells do not express SMC marker proteins. They do, however, express transcription factors thought to be required for SMC differentiation, including the serum response factor (SRF) and myocardin family members, and in vitro they readily differentiate into SM-like cells. It is possible that these cells, when activated in response to injury, contribute to the accumulation of SM-like cells in the vessel wall.[56]
Resident medial / adventitial border progenitorsIn addition to progenitors located within distinct medial or adventitial compartments, studies have suggested that there exists a progenitor cell subset at the medial / adventitial border, in the medium to large arteries and veins. This CD34+ / CD31-cell type can apparently give rise to KDR+ / Tie2+ endothelial cells and capillary sprouts.[10,14] Interestingly, additional cells within these ‘vasculogenic zone’ cells are CD45+, pointing to the possibility of a vascular wall resident HSC population, at least in the human internal thoracic artery segments studied. Strengthening these findings, Pasquinelli et al. have determined that the thoracic aorta segments contain a mesenchymal stromal cell (MSC) population capable of differentiation into the endothelium.[57] Of late, this group has provided evidence that MSCs within the vasculogenic zone are morphologically and immunophenotypically stem-like. By flow cytometry, MSCs can be identified by the expression of mesenchymal antigens CD29, CD44, CD90, CD73, CD105, and CD166, and lack of expression of the hematopoietic lineage markers CD45 and CD34.[58] In addition, the vasculogenic zone MSCs robustly express ‘stemness’ markers OCT-4, Notch-1, and Stro-1, and exclude the Hoechst dye, as mentioned a little further in the text, for other SP cells. Further confirmation using robust lineage-tracking systems is needed to fully elucidate the true potential of progenitor cell subsets within the vasculogenic zone. Nevertheless, it is conceivable that in medium-to-large-sized vessels, the wall itself contains the progenitor cell potential for renewal of all vessel cell types, and possibly immune and / or inflammatory cell types.
Pericytes as resident progenitor cellsPericytes were discovered over one hundred years ago [59,60] and are subendothelial cells resident in large vessels down through to the microvasculature. Currently, the true nature of their origin remains complex and poorly understood. Their location in vessels can vary, from a peri-endothelial localization to the media, adventitia, and in association with the vasa vasorum.[61] They are best characterized in the microvasculature, where they play important roles in capillogenesis, microvascular tone, as well as providing structural integrity.[62] New investigations into these enigmatic cells have revealed a possible progenitor cell role. Although it has been known for some time that pericytes are able to differentiate into osteoprogenitor cells,[63] they seem to figure prominently in aortic calcification during atherosclerosis.[64] The characteristic expression pattern of pericytes has been reviewed elsewhere,[65] but a thorough characterization of the specific pericyte markers associated with the bona fide multipotent progenitor potential remains to be defined. Interestingly, it has been suggested that pericytes and vasculogenic zone MSCs may be closely related.[65] The distribution of pericytes throughout the vasculature suggests that perhaps pericytes or MSCs are vascular progenitor cells that are competent to renew a variety of cell types, while simultaneously maintaining a ‘lineage-allegiance’ [65] responsive to the needs of the tissue of residence. A better understanding of the mechanisms of control that facilitate pericyte (and vessel wall MSC) progenitor competence, particularly in the context of vascular remodeling, could open a new era of therapy targeting the vessel wall to repair itself.
Lung side population cells as progenitors of endothelial and mesenchymal cellsAnother source of resident lung vascular progenitors, which may play a role in the pathogenesis of pulmonary arterial hypertension, is the Hoechstlow CD45neg side population of cells, also termed as ‘SP’. The term side population (SP) is based on the cytometric profile in which there is a side arm of cells protruding from the main Hoechst stained population and is referred to as Hoechstlow [Figure 3]. The Hoechst vital dye is taken up by live cells and fluoresces in red and blue when excited by a UV laser. An ABCG2 multidrug resistance (MDR) transporter mechanism allows the cells to pump out the dye, thus leading to a lower fluorescence intensity.[66,67] ABCG2 as well as other MDR transporters are believed to be a hallmark of primitive cell types, HSC, and cancer cells.[66-71] The murine lung SP cell populations (Hoechstlow CD45neg) have been isolated and characterized in vitro as an enriched tissue-specific source of organ-specific pulmonary precursors, having mesenchymal stem cell properties as well as both endothelial and epithelial lineage potential.[15,16,72-75] The origin of lung SP was

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 7
examined by bone marrow transplantation analyses and it was determined that the CD45pos fraction was derived from the bone marrow, while the origin of the CD45neg population was undefined.[75] These studies form the basis for the identification of the SP, or ABCG2, as a resident adult tissue-specific stem cell marker.
The vascular potential of the lung SP is defined in vitro by their ability to express VE-Cadherin, bind isolectin B4, take up diLDL, and their ability to form angiogenic tubes in matrigel.[15] More recent studies defined the mesenchymal stem cell potential of this Hoechstlow CD45neg in both mixed populations of cells as well as with single cell clones. These cells express high levels of telomerase, relative to the liver tissue, which does not decrease significantly over time.[16] These cells express characteristic mesenchymal markers (CD44, CD90, CD105, CD106, CD73, and Sca-I) and lack any hematopoietic markers (CD45, c-kit, CD11b, CD34, and CD14). The clonal analyses demonstrated that a single lung SP could assume the phenotype of mesenchymal lineages such as bone, cartilage, and fat.[16] Although the true role of these cells in vivo is yet to be determined, as this cell population has both vascular endothelial and mesenchymal stem cell characteristics, it is likely that they differentiate to endothelial, smooth muscle, and myofibroblast lineages, depending on the microenvironment. Thus, the lung SP may play a role in the remodeling associated with pulmonary hypertension.
Contribution of circulating vascular progenitors to systemic vascular remodelingThe contribution of circulating progenitor cells to vascular remodeling has been studied more extensively in systemic
vascular disease than in pulmonary vascular disease. Many of these studies serve as the rationale for investigations in pulmonary circulation, and thus, a brief review of this study is critical for a better understanding of progenitor cells in pulmonary vascular remodeling.
As mentioned earlier, in contrast to the initial conventional assumption that damaged organs are repaired only by migration and proliferation of adjacent resident cells, accumulating the evidence supports the idea that multifunctional progenitor cells are mobilized into the circulation and are recruited specifically into the sites of tissue regeneration. Many reports have demonstrated that bone marrow-derived EPCs significantly contribute to neovascularization and re-endothelialization after acute vascular injury.[20,76] Furthermore, several animal and clinical studies have demonstrated that transplantation of autologous EPCs or unfractionated bone-marrow cells is effective for the treatment of ischemic cardiovascular disease.[19,77] On the other hand, there is increasingly good evidence demonstrating that bone marrow cells or circulating progenitor cells can participate not only in the maintenance or restoration of vascular homeostasis, but also in the pathogenesis of various vascular diseases. The role of EPC cells in vascular healing has been well demonstrated and recently reviewed and will not be discussed further.[78,79] However, the role of progenitor cells in pathological angiogenesis and intimal lesion formation is briefly reviewed here, because of its relevance to the mechanisms involved in vascular remodeling in pulmonary hypertension.
Angiogenesis has been implicated in the pathogenesis of a variety of systemic disorders, including diabetic retinopathies, tumors, rheumatoid arthritis, and cirrhosis.[80,81] EPCs have been shown to contribute to the pathological angiogenesis observed in these conditions.[11,82,83] Tumor angiogenesis, in particular, is associated with the recruitment of hematopoietic and circulating EPCs.[84] In fact, experimental evidence has demonstrated that hematopoietic progenitors expressing vascular endothelial growth factor receptor-1 (VEGFR1) are required for regulation of tumor metastasis.[85] In this manner, injection of bone marrow cells promoted injury-associated retinal angiogenesis.[86] Furthermore, endothelial cells that accumulate in the neointimal lesions in allografts and originate from circulating and bone marrow-derived progenitors, are responsible for the formation of microvessels in the setting of transplant atherosclerosis.[11] These observations raise the possibility that transplantation of endothelial progenitor or bone marrow cells may, under certain circumstances, promote tumor formation, diabetic retinopathy, and atherosclerosis, by augmenting disease-associated pathological angiogenesis. However, some clinical studies
Yeager, et al.: Progenitor cells in pulmonary vascular remodeling
Figure 3: Identifi cation of increased markers of c-kit+ cells in the blood and pulmonary artery of chronically hypoxic animals. Increased numbers of c-kit+ cells are present in the blood of chronically hypoxic calves compared to controls. Immunohistochemistry (brown peroxidase signal) revealed greater number of c-kit+ cells (arrows) in the vessel wall of the distal PA from hypoxic animals compared to controls. The c-kit+ cells were localized, contiguous to, and within, the vasa vasorum in the adventia (Adapted from Davie et al.) [106]

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 8
have demonstrated that the number of circulating EPCs correlates inversely with the risk factors of coronary artery disease.[33] In addition, the levels of circulating EPCs have been reported to predict the occurrence of cardiovascular events.[87] These observations have prompted some investigators to suggest that the physiological levels of circulating EPCs, in fact, function to prevent atherosclerosis, without promoting unfavorable angiogenesis.
The observations that a majority of cells in neointimal lesions express certain SM-markers (typically α-SM-actin [88]) has led to the general assumption that SMCs in the adjacent medial layer migrate into the subendothelial space, and proliferate and synthesize the extracellular matrix, thereby contributing to neointimal formation.[89] However, many recent pathological studies have demonstrated that neointimal SM-like cells are phenotypically distinct from medial SMCs. For example, unlike SMCs in the normal vascular media that express a differentiated contractile phenotype, neointimal SM-like cells are characterized by a large number of synthetic and secretory organelles. These ‘synthetic’ SM-like cells secrete extracellular matrix components and express lower levels of SM-specific contractile proteins.[90] These synthetic SM-like cells proliferate and migrate significantly in response to various growth factors present in the injured vessel wall.[91] In fact, much effort has been devoted to understanding the regulators of the vascular SM phenotype that control the transition from a quiescent differentiated SMC, under normal conditions, to proliferative de-differentiated SM-like, in the presence of pathological stimuli. Intriguingly, however, it was reported that some neointimal SM-like cells express a number of hematopoietic lineage makers along with certain SM markers.[92] Macrophage-like SM-like cells with phagocytic activity have been obtained from human arteries.[93] Although it has been assumed that resident medial SMC ‘transdifferentiate’ into macrophage-like cells, recent studies have demonstrated that some ‘synthetic’ SM-like cells with characteristics of macrophages, are derived from circulating blood cells rather than from medial SMC.[22,94] Taking advantage of both genetically modified mice as well as the use of a chimeric mouse model of parabiosis, recent studies have demonstrated convincingly that in a variety of systemic vascular injuries, bone marrow-derived cells home to the damaged vessels and contribute to both vascular repair and pathological remodeling, by differentiating into cells expressing mesenchymal or SMC characteristics.[22,95] Smooth muscle progenitor cells may in fact contribute to plaque formation through the production of extracellular matrix proteins.[39]
In addition to EPCs and SM progenitor cells, fibrocytes have also been described as being present in the diseased
systemic vessel wall. Fibrocytes (procollagen-1+ / CD34+) have recently been identified in the fibrous cap of human atherosclerotic lesions.[96,97] Moreover, subendothelial αSMA+ myofibroblasts, co-expressing CD68 or CD34, have been found in the lipid-rich areas of the atherosclerotic intima in the human aorta and in the fibrous cap of human carotid arteries, suggesting that these cells are fibrocytes.[96,98] Furthermore, one of the subsets of monocytes that is preferentially recruited into the arterial wall during experimentally induced arteriosclerosis in mice, represents the murine counterpart of the human inflammatory subset of CD14+ / CD16neg mononuclear cells, which express the MCP-1 receptor, CCR2.[99] These observations are consistent with the elegant new studies from Varco et al. demonstrating that intimal hyperplasia in an ovine carotid artery patch graft model is partially due to hematopoetic circulating progenitor cells, fibrocytes that acquire mesenchymal features as they mature at the site of injury.[100] Thus, a CD14+ / CD16- / CCR2+ subpopulation may be involved in atherogenesis and may contain fibrocyte precursors that contribute to lesion formation. In addition to diseases of the proper vessels, fibrocytes are associated with pathological vascular remodeling in the context of a diverse set of disease states including obliterative bronchiolitis,[101] asthma,[102] pulmonary fibrosis,[103] and ischemic cardiomyopathy.[104] Collectively, these observations are supported by epidemiological data showing that MCP-1 plays a major role in the pathogenesis of atherosclerosis and disease progression, and may promote recruitment of fibrocytes to the vessel wall.[105]
Contribution of circulating vascular progenitors to pulmonary vascular remodelingAnimal studiesBased on the observations in systemic vascular diseases, Davie et al. were among the first to examine the possibility that circulating progenitor cells contribute to pulmonary vascular remodeling.[106] They tested the hypothesis that hypoxia would stimulate mobilization of bone marrow (BM)-derived c-Kit+ cells (c-Kit is a transmembrane tyrosine kinase receptor for the stem cell factor and a generally accepted marker for BM-derived hematopoietic stem cells (HSC)) into the circulation, and create an environment, specifically in the pulmonary artery, which facilitates circulating c-Kit+ cell adhesion, and thus, increase the number of c-Kit+ cells within the remodeled pulmonary artery. The study demonstrated that chronic hypoxia significantly increased the number of c-Kit+ cells in the circulation and decreased their numbers in the BM, thus supporting the previously reported idea that ischemic stimuli led to the mobilization of BM-derived stem cells [Figure 3A].[106,107] Of relevance is the fact that genes regulated by hypoxia, including erythropoietin and VEGF, have been implicated in the generation and differentiation of hemangioblasts, the precursors of both HSC and
Yeager, et al.: Progenitor cells in pulmonary vascular remodeling

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 9
primitive endothelial cells.[108] Moreover, VEGF has been shown to mediate the mobilization of BM-derived HSCs and EPCs, which promote tumor blood vessel growth.[84] An increase in the number of c-Kit+ cells in the remodeled adventitia as well as in the expanding vasa vasorum of hypoxic pulmonary arteries compared with the relatively acellular pulmonary adventitia of normoxic animals was also observed [Figure 3]. Elevated expression of proteins that serve critical roles in recruitment, retention and differentiation of progenitor cells (such as VEGF, fibronectin, thrombin, and osteopontin) were observed in regions enriched in c-Kit+ cells. Each of these molecules has been implicated in inflammatory cell responses, including adhesion, migration, division, and differentiation of cells, including monocytes, macrophages, and progenitor cells. Indirect evidence that the c-Kit+ cells might contribute to the expansion of the vasa vasorum and accumulation of fibroblasts / myofibroblasts in the vessel wall was provided by in vitro observations that peripheral blood MNCs derived from hypoxic calves exhibited the potential to differentiate into endothelial as well as SM-like cell phenotypes, depending on the culture conditions.
In this study, it was also demonstrated that a marked
expansion of the vasa vasorum occurred in the setting of chronic hypoxic pulmonary hypertension [Figure 4], as based on cell localization studies [Figure 4C] and studies in systemic vascular disease, the expanding vasa vasorum acted as a conduit for delivery of inflammatory leukocytes and progenitor cells (c-Kit+) to the vessel wall.[98] Shortly after publication of these data came other reports supporting the idea that circulating progenitor cells contribute to remodeling in various models of pulmonary hypertension. Hayashida et al. used green fluorescent protein-BM-transplanted (GFP-BMT) chimeric mice to investigate the possible role of BM-derived cells in hypoxia-induced pulmonary vascular remodeling.[109] These investigators demonstrated that hypoxia induced the recruitment of significant numbers of GFP+ BM-derived cells into the pulmonary artery wall, including the adventitia. Very few cells were observed in the control mice. The investigators quantified the number of GFP+ cells that co-expressed α-SMA in the lung tissues of both the control and pulmonary hypertensive mice and found significant increases in the numbers of GFP+ / α-SMA+ cells in the pulmonary media and adventitia. They found that the number of GFP+ / α-SMA+ cells increased with time in parallel with the progression of pulmonary
Yeager, et al.: Progenitor cells in pulmonary vascular remodeling
Figure 4: Expansion of the vasa vasorum in hypoxic pulmonary hypertension. Increase in the density of vasa vasorum (arrows) in proximal (a) and distal (b) vessels from hypoxic animals, compared with proximal (c) and distal (d) vessels from normoxic animals. Vasa (arrows) in hypoxic proximal and distal arteries express platelet endothelial cell adhesion molecule (PECAM)-1 (e and f, respectively). Quantitative morphometric analysis demonstrated that the volume density (Vv) of the vasa vasorum is signifi cantly greater in the adventitia and media of the pulmonary arteries of chronically hypoxic animals, at every level along the longitudinal axis of the pulmonary circulation than in the controls. Monocytes (CD11b) appear preferentially next to the vasa (eNOS+cells) in hypoxic vessels

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 10
hypertension. Collectively, the Davie et al. and Hayashida et al. studies provide evidence that BM-derived cells, which are mobilized and accumulate in the pulmonary arteries, contribute to pulmonary vascular remodeling in hypoxia-induced pulmonary hypertension.[106,109]
Subsequently, additional reports have emerged supporting the role of specific progenitor cells, including fibrocytes and bone marrow-derived mesenchymal progenitors, in the pulmonary vascular remodeling process. Circulating fibrocytes have been implicated in the pathogenesis of lung fibrosis in several mouse models, including irradiation- and bleomycin-induced lung injury.[102,103,110,111] Fibrocytes have also been shown to contribute to the subepithelial fibrosis observed in the airways of mice with experimentally induced asthma.[112] In experimental animal models (rat and neonatal calf) with pulmonary hypertension, Frid et al. reported that exposure of these animals to chronic hypoxia led to a robust accumulation of fibrocytes in the adventitia of pulmonary, but not systemic vessels.[17] Using confocal microscopy, the investigators found that at least 40% of the monocyte-like cells accumulating in the pulmonary artery adventitia co-expressed the leukocytic marker CD45 and the mesenchymal marker, type 1 pro-collagen, consistent with a fibrocyte phenotype [Figure 5]. A significant but lesser proportion of cells co-expressed CD45 and α-SM-actin, thus indicating the transition of the recruited
circulating fibrocytes toward the myofibroblast phenotype [Figure 6]. In vivo labeling of circulating monocytic cells with liposome-encapsulated DiI (a red fluorochrome) provided additional evidence that, in response to chronic hypoxic exposure, the circulating cells were recruited specifically to the pulmonary vessels and not to the systemic vessels, and consequently expressed fibroblast antigens (type 1 procollagen) in the remodeled pulmonary vessel wall. Most importantly, the investigators demonstrated a causal link between fibrocyte accumulation and vascular wall remodeling, by showing that depletion of circulating monocytes / fibrocytes, using two different strategies (gadolinium chloride- and chlodronate-encapsulated liposomes), abrogated hypoxia-induced perivascular remodeling in the rat model of hypoxic pulmonary hypertension. These results are consistent with studies in other organ systems, where inhibition of fibrocyte accumulation resulted in reduced collagen deposition and reduced accumulation of myofibroblasts.[100,104,113,114] However, it must be noted that fibrocytes themselves are pro-inflammatory cells and produce a number of cytokines and growth factors that can induce angiogenesis, fibroblast hyperplasia, and release of ECM molecules from the resident tissue fibroblasts.[115] Therefore, the correlations between fibrocyte accumulation and tissue remodeling may also reflect the paracrine effects of these cells on resident vascular wall cells.
Yeager, et al.: Progenitor cells in pulmonary vascular remodeling
Figure 5: Hypoxia-induced pulmonary remodeling is characterized by monocyte/fi brocyte accumulation in the adventitia and media. (a) Sustained hypoxia induces a robust appearance of mononuclear CD45+ cells (indirectly labeled with red fl uorochrome) in the pulmonary arterial adventitia (these lesions are marked by triple large arrowheads in the ‘Hypoxia’ columns). (b) A large proportion (around 40%) of the CD45 + leukocytic cells (red fl uorescence) accumulating in the remodeled pulmonary arterial adventitia of hypoxic hypertensive calves co-express type 1 pro-collagen (green fl uorescence), suggestive of a fi brocyte phenotype. Scale bars, 5 μm. (Adapted from: Frid et al.).[17]

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 11
A recent study on two distinct rodent models of pulmonary hypertension highlights the potential contribution of BM-derived progenitor cells and the efforts to unravel their contribution to pulmonary vascular remodeling. Angelini et al., using GFP + transgenic mice, determined that chronic hypoxia caused the recruitment of cells positive for Sca-1 and c-kit, but negative for CD31 and CD34, to neovascularized small vessels.[116] Recent studies by Spees et al. examined the potential, specifically of the bone marrow of BM-derived progenitor cells, to contribute to the repair and remodeling observed in the lung and heart during monocrotaline (MCT)-induced progressive pulmonary hypertension.[117] Female rats transplanted with GFP+ male (Y-chromosome+) BM cells were used as models. In the control, in the untreated GFP+-BMT chimeric rats, approximately 15% of the cells in the lung were GFP+, whereas, in the MCT-treated chimeric rats, the number of GFP+ cells increased to 35–45%. The pulmonary GFP+ cells in both cases were a mix of hematopoietic inflammatory and non-hematopoietic cells. A large number of BM-derived GFP+ cells in the lung were fibroblasts and myofibroblasts and thus may have contributed to lung fibrosis following irradiation and MCT treatment. The possibility that cell fusion could have been playing a role in the differentiation of BM-derived cells into mesenchymal cells was addressed. However, as indicted by fluorescence in situ hybridization (FISH) assays, the incidence of cell fusion in the lung was very low, ruling this out as a major contributing mechanism. Importantly, the investigators also showed the presence of BM-derived cells in the right ventricle of MCT-treated chimeric rats. Therefore, as in the case of many fibrotic diseases, these results identify BM-derived progenitors as important players in vascular pathology and suggest that strategies aimed at the inhibition of the recruitment of these cells may constitute important therapeutic options in the treatment of pulmonary vascular disease.
Human studiesNewly emerging data in humans with PH support the role of progenitor cells in the vascular remodeling that characterizes these patients. Patients with chronic obstructive pulmonary disease (COPD) often exhibit striking vascular remodeling in the pulmonary muscular arteries in precapillary vessels. The hallmark of remodeling in this group of patients is the thickening of the intima due to the accumulation of SM-like cells. Peinado et al. presented evidence that CD133+ EPCs participate in this process.[118] They demonstrated an increased number of CD133+ cells infiltrating the hyperplastic intima of pulmonary arteries very close to the areas of the denuded endothelium. The number of recruited progenitor cells correlated with the thickness of the arterial wall, suggesting a potential association with
the severity of the remodeling process.[118] Subsequently, in vitro studies by the same group demonstrated that the CD133+ cells might acquire the morphology and phenotype of not only the endothelial cells, but also the SM-like cells. CD133+ cells, co-incubated with the isolated human pulmonary artery, were shown to migrate into the intima and differentiate into SMC. Progenitor cell differentiation was produced without fusion, with mature SMC. Thus, CD133+ cells exhibit a certain degree of plasticity, with an ability to differentiate into both endothelial and SM-like cells, which re-enforces the idea regarding their potential role in pulmonary hypertension in COPD.
Firth et al., reported that endarterectomized tissues from patients with chronic thromboembolic pulmonary hypertension (CTEPH) contained mesenchymal progenitor cells that were CD44 (+) CD73 (+), CD90 (+), CD166 (+); > 80% CD29 (+); 45–99% CD105 (+); CD34 (-), and CD45 (-).[119] Furthermore, they showed that sorted progenitor
Figure 6: Hypoxia promotes the emergence of cells co-expressing leukocytic (CD11b) and the myofi broblast marker α-SM-actin. (a) A robust infl ux of CD11b+ cells (red) in the PA adventitia of chronically hypoxic rats correlates with a signifi cant number of α-SMA+ myofi broblasts in that region. A – Adventitia; M – Media. (b) Double-label immunofl uorescent staining for CD11b (red) and α-SMA (green), followed by deconvolution confocal microscopy analysis of the ‘boxed’ area in A, demonstrate cells that co-express both markers (arrowheads), or express only one of the markers (α-SMA, single arrow or CD11b, triple arrows). (c) Signifi cant numbers of α-SMA+ myofi broblasts (brown staining in the adventitia (labeled (‘A’)) are present in distal PAs of the chronically hypoxic calves. (d) Double-label immunofl uorescent staining, followed by deconvolution confocal microscopy, demonstrate that some of the α-SMA+ myofi broblasts (green) co-express a macrophage marker CD68 (red) (arrowheads). DAPI (blue) labels cell nuclei. M, media; A, adventitia. Scale bars: 50 μm (a, c); 5 μm (b, d). (Adapted from: Frid et al.)[17]
Yeager, et al.: Progenitor cells in pulmonary vascular remodeling

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 12
cells from these tissues were able to give rise to adipocytes, and underwent osteogenic differentiation. The progenitor cells typically co-expressed the intermediate filaments vimentin and smooth muscle alpha-actin, suggesting that they had identified a myofibroblast cell predominant in the endarterectomized tissue.
Evidence of endothelial progenitor dysfunction has recently been provided by Toshner et al. In this study, the endothelial cells within the plexiform lesions were determined to express CD31, CD133, c-kit, CXCR4, and SDF-1.[120] Furthermore, fluorescence-activated cell sorter (FACS) analysis showed an increase in CD133 + CD34 + VEGFR2+ circulating angiogenic progenitors in PAH compared to controls. In addition, late-outgrowth endothelial progenitor cells from patients with PAH demonstrated increased proliferation, migration, and angiogenic capacity compared to controls. This study points to the significant contribution of circulating progenitors to vascular remodeling, most particularly development of endothelial cells containing obliterative lesions.
It has also been recently reported that the numbers of apoptosis-resistant, highly proliferative circulating CD133+ cells increase in human idiopathic PAH.[5,121] The investigators raised the possibility that these cells contributed to the intimal lesions observed in these patients. Importantly, a recent study by Majka et al. demonstrated increased numbers of CD133+ cells in and around the pulmonary vascular lesions in both idiopathic PAH (iPAH) and familial PAH (fPAH)2 [Figure 7]. The increases in CD133+ and CD45+ cells raised questions as to how these cells affected resident cell function and the remodeling process in general. One possibility was that cell–cell fusion events were present and contributed to the remodeling process. Cell fusion could result in genetic changes, which conferred selective growth advantages as well as microsatellite instability, point mutations, allelic imbalance, and loss of heterozygosity.[122-124] The result of such changes were uncoupling from normal checkpoint apoptosis, germline mutation, and hypermethylation, which could, in part, explain the presence of the apoptosis-resistant cells in PAH. Majka et al. therefore analyzed ploidy in cells comprising vascular lesions, as any cell fusion event would result in at least twice the chromosomal content (4N) 2. The investigators did not detect any chromosomal content amplification in either iPAH or fPAH specimens, thus suggesting that genetic instability and proliferative advantage of cells in the hypertensive tissues were not the result of aneuploidy. Thus, it was speculated by the authors that if a neoplastic ‘switch’ had occurred in the cells that characterized the vascular lesions in PAH, it did not involve genes typical to those usually observed in lung cancer.[125,126] The possibility that fibrocytes were also present in the remodeled vessel wall of patients with severe
PAH was raised, although not demonstrated as conclusively as was their presence and contribution to airway remodeling in patients with asthma.[112]
A recent study has shown significant accumulation of c-Kit+ cells in the pulmonary arterial lesions of IPAH patients in an adventitial perivascular distribution.[127] These cells comprised both a mast cell and a potential progenitor population of cells. A marked expansion of the vasa vasorum was noted, with c-Kit+ cells present in this expanding vasculature. The findings were very similar to those reported by Davie et al. and supported the notion raised in that study that c-Kit+ and vasa vasorum could be therapeutic targets in PH.
Chemokine signaling involved in progenitor cell recruitmentAt present, the molecular mechanisms controlling the recruitment, retention, and differentiation of circulating
Figure 7: CD133 positive cells accumulate and proliferate in the pulmonary artery intima of PAH patients. Immunostaining with antibodies to smooth muscle actin (SMA) demonstrates the accumulation of mesenchymal cells in the intima (a) DAPI staining demonstrates total cell accumulation (b) CD133+ cells comprise a portion of the cells accumulating in the intima (c) Ki67 immunostaining on the same section, re-photographed, demonstrate that the majority of proliferating cells are CD133+ (d) High magnifi cation views of (c) and (d) are shown in panels (e) and (f), respectively.
Yeager, et al.: Progenitor cells in pulmonary vascular remodeling

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 13
progenitor cells into the vessel wall remain largely undefined. It is clear, however, that chemokines play an important role in the vascular remodeling process, through the guidance of circulating mononuclear cells to the injury site and activation of resident vascular cells.[128,129] Considering the cell type-specific expression of chemokine receptors and the substantial overlap in ligand-receptor specificity, an interactive network of chemokines and chemokine receptors has emerged, which exhibits enormous plasticity in different types of injury / repair processes. A growing number of chemokine / chemokine receptor pairs with confined effects in vascular diseases have been described.[130] For instance, in systemic circulation, SDF-1 has been shown to regulate vascular repair by CXCR4-dependent SM-progenitor cell recruitment, which contributes to the maladaptive response to injury.[131] Furthermore, three distinct chemokine / chemokine receptor pairs (MCP-1 / CCR2, RANTES / CCR5, and Fractalkine / CX3CR1) have been shown to direct lesional leukocyte infiltration.[132] In addition, MCP-1 / CCR2 and Fractalkine / CX3CR1 increase expansion of neointimal SM-like cells.[133] Thus, to ultimately pharmacologically modulate the maladaptative responses in arterial remodeling, it will be essential to identify specific chemokine / chemokine receptor pairs that play specific roles in the remodeling process. It is possible that these will be vessel- and disease-specific and may, in fact, vary over time.
Recent studies have begun to address specific chemokine / chemokine receptor pairs involved in inflammatory / progenitor cell recruitment to the pulmonary arteries in models of pulmonary hypertension. Advancement in this area has come about through the use of laser capture microdissection (LCM), to evaluate vessel-specific changes, as it is becoming increasingly clear that an analysis of the whole lung tissue may not accurately reflect the specific changes in gene and protein expression in the vessel wall itself.[134-136] Of late, with the use of the LCM technique, sustained hypoxia-induced upregulation of a wide range of inflammatory mediators, growth-, differentiation-, adhesion- and fibrosis-associated molecules in a pulmonary artery-specific fashion [137] was demonstrated. The study demonstrated the upregulation of a number of chemokines and receptors, as well as adhesion molecules, which preceded the influx of the inflammatory cells and the onset of perivascular fibrosis. These included CXCL12 (SDF-1) / CXCR4, VCAM-1, ICAM-1, TGF-β, and 5-LO. Interestingly, over time, the pulmonary artery inflammatory microenvironment became more complex, with the appearance of other cytokine, adhesion, growth and differentiation mediators (such as IL-6, MCP-1, PDGF-BB), which was consistent with the increasing number and persistent presence of monocytes and other inflammatory cells in the perivascular regions.
Upon removal of the hypoxic stimulus, expression of specific chemokine / chemokine receptors and adhesion molecules rapidly returned to control levels, which preceded the disappearance of inflammatory cells and ultimately reversal of vascular remodeling and resolution of pulmonary hypertension. Importantly, administration of antagonists of SDF-1 / CXCL-12 and CXCR4 has been shown to prevent vascular remodeling and accumulation of c-kit+ / Sca-1+ progenitor cells in the vessel wall of chronically hypoxic mice.[138,139] Additionally, inhibition of SDF-1 / CXCR4 signaling reversed the established remodeling in these mice. These studies highlight the impact of progenitor cells in the pulmonary hypertensive process and hint at their potential therapeutic importance for pulmonary hypertension. Similarly, in patients with idiopathic PAH, increases in fractalkine, RANTES, and PDGF expression, particularly within the pulmonary arterial wall, have been observed.[136,140,141] Further studies are essential to define more precisely the chemokine / chemokine receptor pairs involved in the pulmonary vascular remodeling process. This information will be critical to the development of new therapeutic interventions.
SUMMARY
In summary, substantial experimental evidence points to the role of the circulating progenitor cells in vascular pathology, which characterizes chronic PH. More study is needed to determine the types of progenitor cells involved in vascular remodeling and their specific functions, once they take up residence in the vessel wall. Much study is needed to determine the factors involved in their recruitment and retention. Additionally, studies are needed to determine factors involved in controlling their proliferative and differentiation states. Studies are also needed to address the role of resident lung and vascular progenitor cells in the remodeling process. Collectively, these experiments may yield opportunities for critical new treatment strategies.
REFERENCES
1. Humbert M, Morrell NW, Archer SL, Stenmark KR, MacLean MR, Lang IM, et al. Cellular and molecular pathobiology of pulmonary arterial hypertension. J Am Coll Cardiol 2004;43:13S-24S.
2. Majka SM, Skokan M, Wheeler L, Harral J, Gladson S, Burnham E, et al. Evidence for cell fusion is absent in vascular lesions associated with pulmonary arterial hypertension. Am J Physiol Lung Cell Mol Physiol 2008;295:L1028-39.
3. Pietra GG, Capron F, Stewart S, Leone O, Humbert M, Robbins IM, et al. Pathologic assessment of vasculopathies in pulmonary hypertension. J Am Coll Cardiol 2004;43:25S-32S.
4. Yi ES, Kim H, Ahn H, Strother J, Morris T, Masliah E, et al. Distribution of obstructive intimal lesions and their cellular phenotypes in chronic pulmonary hypertension. A morphometric and immunohistochemical study. Am J Respir Crit Care Med 2000;162:1577-86.
Yeager, et al.: Progenitor cells in pulmonary vascular remodeling

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 14
5. Masri FA, Xu W, Comhair SA, Asosingh K, Koo M, Vasanji A, et al. Hyperproliferative apoptosis-resistant endothelial cells in idiopathic pulmonary arterial hypertension. Am J Physiol Lung Cell Mol Physiol 2007;293:L548-54.
6. Tuder RM, Marecki JC, Richter A, Fij alkowska I, Flores S. Pathology of pulmonary hypertension. Clin Chest Med 2007;28:23-42.
7. Arciniegas E, Frid MG, Douglas IS, Stenmark KR. Perspectives on endothelial-to-mesenchymal transition: potential contribution to vascular remodeling in chronic pulmonary hypertension. Am J Physiol Lung Cell Mol Physiol 2007;293:L1-8.
8. Hinz B, Phan SH, Thannickal VJ, Galli A, Bochaton-Piallat ML, Gabbiani G. The myofibroblast: One function, multiple origins. Am J Pathol 2007;170:1807-16.
9. Kalluri R, Neilson EG. Epithelial-mesenchymal transition and its implications for fi brosis. J Clin Invest 2003;112:1776-84.
10. Ergun S, Tilki D, Klein D. Vascular wall as a reservoir for diff erent types of stem and progenitor cells. Antioxid Redox Signal 2010.
11. Hu Y, Davison F, Zhang Z, Xu Q. Endothelial replacement and angiogenesis in arteriosclerotic lesions of allograft s are contributed by circulating progenitor cells. Circulation 2003;108:3122-7.
12. Stenmark KR, Davie N, Frid M, Gerasimovskaya E, Das M. Role of the adventitia in pulmonary vascular remodeling. Physiology (Bethesda) 2006;21:134-45.
13. Torsney E, Xu Q. Resident vascular progenitor cells. J Mol Cell Cardiol 2011;50:304-11.
14. Zengin E, Chalajour F, Gehling UM, Ito WD, Treede H, Lauke H, et al. Vascular wall resident progenitor cells: A source for postnatal vasculogenesis. Development 2006;133:1543-51.
15. Irwin D, Helm K, Campbell N, Imamura M, Fagan K, Harral J, et al. Neonatal lung side population cells demonstrate endothelial potential and are altered in response to hyperoxia-induced lung simplifi cation. Am J Physiol Lung Cell Mol Physiol 2007;293:L941-51.
16. Martin J, Helm K, Ruegg P, Varella-Garcia M, Burnham E, Majka S. Adult lung side population cells have mesenchymal stem cell potential. Cytotherapy 2008;10:140-51.
17. Frid MG, Brunett i JA, Burke DL, Carpenter TC, Davie NJ, Reeves JT, et al. Hypoxia-induced pulmonary vascular remodeling requires recruitment of circulating mesenchymal precursors of a monocyte / macrophage lineage. Am J Pathol 2006;168:659-69.
18. Liu C, Nath KA, Katusic ZS, Caplice NM. Smooth muscle progenitor cells in vascular disease. Trends Cardiovasc Med 2004;14:288-93.
19. Sata M. Role of circulating vascular progenitors in angiogenesis, vascular healing, and pulmonary hypertension: Lessons from animal models. Arterioscler Thromb Vasc Biol 2006;26:1008-14.
20. Asahara T, Murohara T, Sullivan A, Silver M, van der Zee R, Li T, et al. Isolation of putative progenitor endothelial cells for angiogenesis. Science 1997;275:964-7.
21. Sirker AA, Astroulakis ZM, Hill JM. Vascular progenitor cells and translational research: the role of endothelial and smooth muscle progenitor cells in endogenous arterial remodelling in the adult. Clin Sci (Lond) 2009;116:283-99.
22. Tanaka K, Sata M. Contribution of circulating vascular progenitors in lesion formation and vascular healing: Lessons from animal models. Curr Opin Lipidol 2008;19:498-504.
23. Alvarez DF, Huang L, King JA, ElZarrad MK, Yoder MC, Stevens T. Lung microvascular endothelium is enriched with progenitor cells that exhibit vasculogenic capacity. Am J Physiol Lung Cell Mol Physiol 2008;294:L419-30.
24. Rabelink TJ, de Boer HC, de Koning EJ, van Zonneveld AJ. Endothelial progenitor cells: More than an infl ammatory response? Arterioscler Thromb Vasc Biol 2004;24:834-8.
25. Urbich C, Dimmeler S. Endothelial progenitor cells: Characterization and role in vascular biology. Circ Res 2004;95:343-53.
26. Yoder MC. Is endothelium the origin of endothelial progenitor cells? Arterioscler Thromb Vasc Biol 2010;30:1094-103.
27. Yoder MC, Ingram DA. The defi nition of EPCs and other bone marrow cells contributing to neoangiogenesis and tumor growth: Is there common ground for understanding the roles of numerous marrow-derived cells in the neoangiogenic process? Biochim Biophys Acta 2009;1796:50-4.
28. Barber CL, Iruela-Arispe ML. The ever-elusive endothelial progenitor cell: Identities, functions and clinical implications. Pediatr Res 2006;59:26R-32R.
29. Peichev M, Naiyer AJ, Pereira D, Zhu Z, Lane WJ, Williams M, et al. Expression of VEGFR-2 and AC133 by circulating human CD34(+) cells identifi es a population of functional endothelial precursors. Blood
2000;95:952-8.30. Hristov M, Zernecke A, Bidzhekov K, Liehn EA, Shagdarsuren E, Ludwig
A, et al. Importance of CXC chemokine receptor 2 in the homing of human peripheral blood endothelial progenitor cells to sites of arterial injury. Circ Res 2007;100:590-7.
31. Venneri MA, De Palma M, Ponzoni M, Pucci F, Scielzo C, Zonari E, et al. Identifi cation of proangiogenic TIE2-expressing monocytes (TEMs) in human peripheral blood and cancer. Blood 2007;109:5276-85.
32. Burnham EL, Taylor WR, Quyyumi AA, Rojas M, Brigham KL, Moss M. Increased circulating endothelial progenitor cells are associated with survival in acute lung injury. Am J Respir Crit Care Med 2005;172:854-60.
33. Hill JM, Zalos G, Halcox JP, Schenke WH, Waclawiw MA, Quyyumi AA, et al. Circulating endothelial progenitor cells, vascular function, and cardiovascular risk. N Engl J Med 2003;348:593-600.
34. Smadja DM, Gaussem P, Mauge L, Israël-Biet D, Dignat-George F, Peyrard S, et al. Circulating endothelial cells: A new candidate biomarker of irreversible pulmonary hypertension secondary to congenital heart disease. Circulation 2009;119:374-81.
35. Smadja DM, Mauge L, Sanchez O, Silvestre JS, Guerin C, Godier A, et al. Distinct patt erns of circulating endothelial cells in pulmonary hypertension. Eur Respir J 2010;36:1284-93.
36. Simper D, Stalboerger PG, Panett a CJ, Wang S, Caplice NM. Smooth muscle progenitor cells in human blood. Circulation 2002;106:1199-204.
37. Sugiyama S, Kugiyama K, Nakamura S, Kataoka K, Aikawa M, Shimizu K, et al. Characterization of smooth muscle-like cells in circulating human peripheral blood. Atherosclerosis 2006;187:351-62.
38. Zernecke A, Schober A, Bot I, von Hundelshausen P, Liehn EA, Möpps B, et al. SDF-1alpha / CXCR4 axis is instrumental in neointimal hyperplasia and recruitment of smooth muscle progenitor cells. Circ Res 2005;96:784-91.
39. Campagnolo P, Wong MM, Xu Q. Progenitor Cells in Arteriosclerosis: Good or Bad Guys? Antioxid Redox Signal 2010:Epub (09 / 4 / 2010).
40. Caplice NM, Bunch TJ, Stalboerger PG, Wang S, Simper D, Miller DV, et al. Smooth muscle cells in human coronary atherosclerosis can originate from cells administered at marrow transplantation. Proc Natl Acad Sci U S A 2003;100:4754-9.
41. Bentzon JF, Falk E. Circulating smooth muscle progenitor cells in atherosclerosis and plaque rupture: Current perspective and methods of analysis. Vascul Pharmacol 2010;52:11-20.
42. Abe R, Donnelly SC, Peng T, Bucala R, Metz CN. Peripheral blood fi brocytes: diff erentiation pathway and migration to wound sites. J Immunol 2001;166:7556-62.
43. Bellini A, Matt oli S. The role of the fi brocyte, a bone marrow-derived mesenchymal progenitor, in reactive and reparative fi broses. Lab Invest 2007;87:858-70.
44. Bucala R, Spiegel LA, Chesney J, Hogan M, Cerami A. Circulating fi brocytes defi ne a new leukocyte subpopulation that mediates tissue repair. Mol Med 1994;1:71-81.
45. Ebihara Y, Masuya M, Larue AC, Fleming PA, Visconti RP, Minamiguchi H, et al. Hematopoietic origins of fi broblasts: II. In vitro studies of fi broblasts, CFU-F, and fi brocytes. Exp Hematol 2006;34:219-29.
46. Herzog EL, Bucala R. Fibrocytes in health and disease. Exp Hematol 2010;38:548-56.
47. Balmelli C, Ruggli N, McCullough K, Summerfi eld A. Fibrocytes are potent stimulators of anti-virus cytotoxic T cells. J Leukoc Biol 2005;77:923-33.
48. He Q, Wan C, Li G. Concise review: Multipotent mesenchymal stromal cells in blood. Stem Cells 2007;25:69-77.
49. Pilling D, Gomer R. Regulatory Pathways for Fibrocyte Diff erentiation. In: World Scientifi c Publishing Company. Singapore; 2007.
50. Pilling D, Buckley CD, Salmon M, Gomer RH. Inhibition of fi brocyte diff erentiation by serum amyloid P. J Immunol 2003;171:5537-46.
51. Schwartz SM, Benditt EP. Cell replication in the aortic endothelium: A new method for study of the problem. Lab Invest 1973;28:699-707.
52. Schwartz SM, Benditt EP. Clustering of replicating cells in aortic endothelium. Proc Natl Acad Sci U S A 1976;73:651-3.
53. Alessandri G, Girelli M, Taccagni G, Colombo A, Nicosia R, Caruso A, et al. Human vasculogenesis ex vivo: embryonal aorta as a tool for isolation of endothelial cell progenitors. Lab Invest 2001;81:875-85.
54. Ingram DA, Mead LE, Moore DB, Woodard W, Fenoglio A, Yoder MC. Vessel wall-derived endothelial cells rapidly proliferate because they contain a complete hierarchy of endothelial progenitor cells. Blood 2005;105:2783-6.
55. Hu Y, Zhang Z, Torsney E, Afzal AR, Davison F, Metzler B, et al. Abundant progenitor cells in the adventitia contribute to atherosclerosis of vein graft s
Yeager, et al.: Progenitor cells in pulmonary vascular remodeling

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 15
in ApoE-defi cient mice. J Clin Invest 2004;113:1258-65.56. Passman JN, Dong XR, Wu SP, Maguire CT, Hogan KA, Bautch VL, et al.
A sonic hedgehog signaling domain in the arterial adventitia supports resident Sca1+ smooth muscle progenitor cells. Proc Natl Acad Sci U S A 2008;105:9349-54.
57. Pasquinelli G, Tazzari PL, Vaselli C, Foroni L, Buzzi M, Storci G, et al. Thoracic aortas from multiorgan donors are suitable for obtaining resident angiogenic mesenchymal stromal cells. Stem Cells 2007;25:1627-34.
58. Pasquinelli G, Pacilli A, Alviano F, Foroni L, Ricci F, Valente S, et al. Multidistrict human mesenchymal vascular cells: Pluripotency and stemness characteristics. Cytotherapy 2010;12:275-87.
59. Eberth C. Handbuch der Lehre von den Geweben des Menschen und der Thiere. Leipzig: W. Engelman; 1871.
60. Rouget C. Sur la contractilite des capillaires sanguins. CR Acad Sci 1879;88:916-8.
61. Andreeva ER, Pugach IM, Gordon D, Orekhov AN. Continuous subendothelial network formed by pericyte-like cells in human vascular bed. Tissue Cell 1998;30:127-35.
62. Shepro D, Morel NM. Pericyte physiology. FASEB J 1993;7:1031-8.63. Sato K, Urist MR. Induced regeneration of calvaria by bone morphogenetic
protein (BMP) in dogs. Clin Orthop Relat Res 1985:301-11.64. Bostrom K, Watson KE, Horn S, Wortham C, Herman IM, Demer LL.
Bone morphogenetic protein expression in human atherosclerotic lesions. J Clin Invest 1993;91:1800-9.
65. Kovacic JC, Boehm M. Resident vascular progenitor cells: An emerging role for non-terminally diff erentiated vessel-resident cells in vascular biology. Stem Cell Res 2009;2:2-15.
66. Bunting KD. ABC transporters as phenotypic markers and functional regulators of stem cells. Stem Cells 2002;20:11-20.
67. Zhou S, Schuetz JD, Bunting KD, Colapietro AM, Sampath J, Morris JJ,et al. The ABC transporter Bcrp1 / ABCG2 is expressed in a wide variety of stem cells and is a molecular determinant of the side-population phenotype. Nat Med 2001;7:1028-34.
68. Al-Hajj M, Wicha MS, Benito-Hernandez A, Morrison SJ, Clarke MF. Prospective identifi cation of tumorigenic breast cancer cells. Proc Natl Acad Sci U S A 2003;100:3983-8.
69. Goodell MA, Brose K, Paradis G, Conner AS, Mulligan RC. Isolation and functional properties of murine hematopoietic stem cells that are replicating in vivo. J Exp Med 1996;183:1797-806.
70. Hirschmann-Jax C, Foster AE, Wulf GG, Nuchtern JG, Jax TW, Gobel U, et al. A distinct ‘ side population’ of cells with high drug effl ux capacity in human tumor cells. Proc Natl Acad Sci U S A 2004;101:14228-33.
71. Tadjali M, Zhou S, Rehg J, Sorrentino BP. Prospective isolation of murine hematopoietic stem cells by expression of an Abcg2 / GFP allele. Stem Cells 2006;24:1556-63.
72. Giangreco A, Shen H, Reynolds SD, Stripp BR. Molecular phenotype of airway side population cells. Am J Physiol Lung Cell Mol Physiol 2004;286:L624-30.
73. Kott on DN, Summer R, Fine A. Lung stem cells: New paradigms. Exp Hematol 2004;32:340-3.
74. Summer R, Kott on DN, Sun X, Fitzsimmons K, Fine A. Translational physiology: Origin and phenotype of lung side population cells. Am J Physiol Lung Cell Mol Physiol 2004;287:L477-83.
75. Summer R, Kott on DN, Sun X, Ma B, Fitzsimmons K, Fine A. Side population cells and Bcrp1 expression in lung. Am J Physiol Lung Cell Mol Physiol 2003;285:L97-104.
76. Murasawa S, Asahara T. Endothelial progenitor cells for vasculogenesis. Physiology (Bethesda) 2005;20:36-42.
77. Khakoo AY, Finkel T. Endothelial progenitor cells. Annu Rev Med 2005;56:79-101.
78. Ben-Shoshan J, George J. Endothelial progenitor cells as therapeutic vectors in cardiovascular disorders: From experimental models to human trials. Pharmacol Ther 2007;115:25-36.
79. Shantsila E, Watson T, Lip GY. Endothelial progenitor cells in cardiovascular disorders. J Am Coll Cardiol 2007;49:741-52.
80. Ferrara N. Vascular endothelial growth factor and the regulation of angiogenesis. Recent Prog Horm Res 2000;55:15-35.
81. Folkman J. Seminars in Medicine of the Beth Israel Hospital, Boston. Clinical applications of research on angiogenesis. N Engl J Med 1995;333:1757-63.
82. Asahara T, Masuda H, Takahashi T, Kalka C, Pastore C, Silver M, et al. Bone marrow origin of endothelial progenitor cells responsible for postnatal vasculogenesis in physiological and pathological neovascularization. Circ Res 1999;85:221-8.
83. Grant MB, May WS, Caballero S, Brown GA, Guthrie SM, Mames RN, et al. Adult hematopoietic stem cells provide functional hemangioblast activity during retinal neovascularization. Nat Med 2002;8:607-12.
84. Lyden D, Hatt ori K, Dias S, Costa C, Blaikie P, Butros L, et al. Impaired recruitment of bone-marrow-derived endothelial and hematopoietic precursor cells blocks tumor angiogenesis and growth. Nat Med 2001;7:1194-201.
85. Kaplan RN, Riba RD, Zacharoulis S, Bramley AH, Vincent L, Costa C, et al. VEGFR1-positive haematopoietic bone marrow progenitors initiate the pre-metastatic niche. Nature 2005;438:820-7.
86. Otani A, Kinder K, Ewalt K, Otero FJ, Schimmel P, Friedlander M. Bone marrow-derived stem cells target retinal astrocytes and can promote or inhibit retinal angiogenesis. Nat Med 2002;8:1004-10.
87. Schmidt-Lucke C, Rossig L, Fichtlscherer S, Vasa M, Britt en M, Kämper U, et al. Reduced number of circulating endothelial progenitor cells predicts future cardiovascular events: Proof of concept for the clinical importance of endogenous vascular repair. Circulation 2005;111:2981-7.
88. Kearney M, Pieczek A, Haley L, Losordo DW, Andres V, Schainfeld R, et al. Histopathology of in-stent restenosis in patients with peripheral artery disease. Circulation 1997;95:1998-2002.
89. Ross R. Atherosclerosis - an inflammatory disease. N Engl J Med 1999;340:115-26.
90. Campbell GR, Campbell JH. The phenotypes of smooth muscle expressed in human atheroma. Ann N Y Acad Sci 1990;598:143-58.
91. Owens GK, Kumar MS, Wamhoff BR. Molecular regulation of vascular smooth muscle cell diff erentiation in development and disease. Physiol Rev 2004;84:767-801.
92. Zohlnhofer D, Richter T, Neumann F, Nührenberg T, Wessely R, Brandl R, et al. Transcriptome analysis reveals a role of interferon-gamma in human neointima formation. Mol Cell 2001;7:1059-69.
93. Matsumoto K, Hirano K, Nozaki S, Takamoto A, Nishida M, Nakagawa-Toyama Y, et al. Expression of macrophage (Mphi) scavenger receptor, CD36, in cultured human aortic smooth muscle cells in association with expression of peroxisome proliferator activated receptor-gamma, which regulates gain of Mphi-like phenotype in vitro, and its implication in atherogenesis. Arterioscler Thromb Vasc Biol 2000;20:1027-32.
94. Tanaka K, Sata M, Hirata Y, Nagai R. Diverse contribution of bone marrow cells to neointimal hyperplasia aft er mechanical vascular injuries. Circ Res 2003;93:783-90.
95. Iwata H, Sata M. Potential contribution of bone marrow-derived precursors to vascular repair and lesion formation: Lessons from animal models of vascular diseases. Front Biosci 2007;12:4157-67.
96. Medbury H. Role of Fibrocytes in Atherogenesis. In. Singapore: World Scientifi c Publishing Company; 2007.
97. Medbury HJ, Tarran SL, Guiff re AK, Williams MM, Lam TH, Vicarett i M, et al. Monocytes contribute to the atherosclerotic cap by transformation into fi brocytes. Int Angiol 2008;27:114-23.
98. Andreeva ER, Pugach IM, Orekhov AN. Subendothelial smooth muscle cells of human aorta express macrophage antigen in situ and in vitro. Atherosclerosis 1997;135:19-27.
99. Tacke F, Randolph GJ. Migratory fate and differentiation of blood monocyte subsets. Immunobiology 2006;211:609-18.
100. Varcoe RL, Mikhail M, Guiff re AK, Pennings G, Vicarett i M, Hawthorne WJ, et al. The role of the fi brocyte in intimal hyperplasia. J Thromb Haemost 2006;4:1125-33.
101. Andersson-Sjoland A, Erjefalt JS, Bjermer L, Eriksson L, Westergren-Thorsson G. Fibrocytes are associated with vascular and parenchymal remodelling in patients with obliterative bronchiolitis. Respir Res 2009;10:103.
102. Westergren-Thorsson G, Larsen K, Nihlberg K, Andersson-Sjöland A, Hallgren O, Marko-Varga G, et al. Pathological airway remodelling in infl ammation. Clin Respir J 2010;4:1-8.
103. Keeley EC, Mehrad B, Strieter RM. Fibrocytes: Bringing new insights into mechanisms of infl ammation and fi brosis. Int J Biochem Cell Biol 2010;42:535-42.
104. Haudek SB, Xia Y, Huebener P, Lee JM, Carlson S, Crawford JR, et al. Bone marrow-derived fi broblast precursors mediate ischemic cardiomyopathy in mice. Proc Natl Acad Sci U S A 2006;103:18284-9.
105. McDermott DH, Yang Q, Kathiresan S, Cupples LA, Massaro JM, Keaney JF Jr, et al. CCL2 polymorphisms are associated with serum monocyte chemoattractant protein-1 levels and myocardial infarction in the Framingham Heart Study. Circulation 2005;112:1113-20.
106. Davie NJ, Crossno JT, Jr., Frid MG, Hofmeister SE, Reeves JT, Hyde DM, et al. Hypoxia-induced pulmonary artery adventitial remodeling and
Yeager, et al.: Progenitor cells in pulmonary vascular remodeling

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 16
neovascularization: contribution of progenitor cells. Am J Physiol Lung Cell Mol Physiol 2004;286:L668-78.
107. Takahashi T, Kalka C, Masuda H, Chen D, Silver M, Kearney M, et al. Ischemia- and cytokine-induced mobilization of bone marrow-derived endothelial progenitor cells for neovascularization. Nat Med 1999;5:434-8.
108. Ramirez-Bergeron DL, Simon MC. Hypoxia-inducible factor and the development of stem cells of the cardiovascular system. Stem Cells 2001;19:279-86.
109. Hayashida K, Fujita J, Miyake Y, Kawada H, Ando K, Ogawa S, et al. Bone marrow-derived cells contribute to pulmonary vascular remodeling in hypoxia-induced pulmonary hypertension. Chest 2005;127:1793-8.
110. Gomperts BN, Strieter RM. Fibrocytes in lung disease. J Leukoc Biol 2007;82:449-56.
111. Lama VN, Phan SH. The extrapulmonary origin of fi broblasts: Stem / progenitor cells and beyond. Proc Am Thorac Soc 2006;3:373-6.
112. Schmidt M, Sun G, Stacey MA, Mori L, Mattoli S. Identification of circulating fi brocytes as precursors of bronchial myofi broblasts in asthma. J Immunol 2003;171:380-9.
113. Ishida Y, Kimura A, Kondo T, Hayashi T, Ueno M, Takakura N, et al. Essential roles of the CC chemokine ligand 3-CC chemokine receptor 5 axis in bleomycin-induced pulmonary fi brosis through regulation of macrophage and fi brocyte infi ltration. Am J Pathol 2007;170:843-54.
114. Phillips RJ, Burdick MD, Hong K, Lutz MA, Murray LA, Xue YY, et al. Circulating fi brocytes traffi c to the lungs in response to CXCL12 and mediate fi brosis. J Clin Invest 2004;114:438-46.
115. Wang JF, Jiao H, Stewart TL, Shankowsky HA, Scott PG, Tredget EE. Fibrocytes from burn patients regulate the activities of fi broblasts. Wound Repair Regen 2007;15:113-21.
116. Angelini DJ, Su Q, Kolosova IA, Fan C, Skinner JT, Yamaji-Kegan K, et al. Hypoxia-induced mitogenic factor (HIMF / FIZZ1 / RELM alpha) recruits bone marrow-derived cells to the murine pulmonary vasculature. PLoS One 2010;5:e11251.
117. Spees JL, Whitney MJ, Sullivan DE, Lasky JA, Laboy M, Ylostalo J, et al. Bone marrow progenitor cells contribute to repair and remodeling of the lung and heart in a rat model of progressive pulmonary hypertension. FASEB J 2008;22:1226-36.
118. Peinado VI, Ramirez J, Roca J, Rodriguez-Roisin R, Barbera JA. Identifi cation of vascular progenitor cells in pulmonary arteries of patients with chronic obstructive pulmonary disease. Am J Respir Cell Mol Biol 2006;34:257-63.
119. Firth AL, Yao W, Ogawa A, Madani MM, Lin GY, Yuan JX. Multipotent mesenchymal progenitor cells are present in endarterectomized tissues from patients with chronic thromboembolic pulmonary hypertension. Am J Physiol Cell Physiol 2010;298:C1217-25.
120. Toshner M, Voswinckel R, Southwood M, Al-Lamki R, Howard LS, Marchesan D, et al. Evidence of dysfunction of endothelial progenitors in pulmonary arterial hypertension. Am J Respir Crit Care Med 2009;180:780-7.
121. Asosingh K, Aldred MA, Vasanji A, Drazba J, Sharp J, Farver C, et al. Circulating angiogenic precursors in idiopathic pulmonary arterial hypertension. Am J Pathol 2008;172:615-27.
122. Gao Q, Reynolds GE, Innes L, Pedram M, Jones E, Junabi M, et al. Telomeric transgenes are silenced in adult mouse tissues and embryo fi broblasts but are expressed in embryonic stem cells. Stem Cells 2007;25:3085-92.
123. Niv Y. Microsatellite instability and MLH1 promoter hypermethylation in colorectal cancer. World J Gastroenterol 2007;13:1767-9.
124. Yeager ME, Golpon HA, Voelkel NF, Tuder RM. Microsatellite mutational analysis of endothelial cells within plexiform lesions from patients
with familial, pediatric, and sporadic pulmonary hypertension. Chest 2002;121:61S.
125. Jacobsen BM, Harrell JC, Jedlicka P, Borges VF, Varella-Garcia M, Horwitz KB. Spontaneous fusion with, and transformation of mouse stroma by, malignant human breast cancer epithelium. Cancer Res 2006;66:8274-9.
126. Varella-Garcia M. Stratifi cation of non-small cell lung cancer patients for therapy with epidermal growth factor receptor inhibitors: the EGFR fl uorescence in situ hybridization assay. Diagn Pathol 2006;1:19.
127. Montani D, Perros F, Gambaryan N, Dorfmuller P, Girerd B, Simonneau G, et al. Bone Marrow Derived C-kit Positive Cells in Pulmonary Hypertension. Am J Respir Crit Care Med 2010;181:A2289.
128. Charo IF, Ransohoff RM. The many roles of chemokines and chemokine receptors in infl ammation. N Engl J Med 2006;354:610-21.
129. Schober A. Chemokines in vascular dysfunction and remodeling. Arterioscler Thromb Vasc Biol 2008;28:1950-9.
130. Saederup N, Chan L, Lira SA, Charo IF. Fractalkine defi ciency markedly reduces macrophage accumulation and atherosclerotic lesion formation in CCR2- / - mice: Evidence for independent chemokine functions in atherogenesis. Circulation 2008;117:1642-8.
131. Schober A, Knarren S, Lietz M, Lin EA, Weber C. Crucial role of stromal cell-derived factor-1alpha in neointima formation aft er vascular injury in apolipoprotein E-defi cient mice. Circulation 2003;108:2491-7.
132. Raines EW, Ferri N. Thematic review series: The immune system and atherogenesis. Cytokines aff ecting endothelial and smooth muscle cells in vascular disease. J Lipid Res 2005;46:1081-92.
133. Liu P, Patil S, Rojas M, Fong AM, Smyth SS, Patel DD. CX3CR1 defi ciency confers protection from intimal hyperplasia after arterial injury. Arterioscler Thromb Vasc Biol 2006;26:2056-62.
134. Fink L, Kohlhoff S, Stein MM, Hänze J, Weissmann N, Rose F, et al. cDNA array hybridization aft er laser-assisted microdissection from nonneoplastic tissue. Am J Pathol 2002;160:81-90.
135. Kwapiszewska G, Wygrecka M, Marsh LM, Schmitt S, Trösser R, Wilhelm J, et al. Fhl-1, a new key protein in pulmonary hypertension. Circulation 2008;118:1183-94.
136. Perros F, Dorfmuller P, Souza R, Durand-Gasselin I, Godot V, Capel F, et al. Fractalkine-induced smooth muscle cell proliferation in pulmonary hypertension. Eur Respir J 2007;29:937-43.
137. Burke D, Howells J, Trevillion L, McNulty PA, Jankelowitz SK, Kiernan MC. Threshold behaviour of human axons explored using subthreshold perturbations to membrane potential. J Physiol 2009;587:491-504.
138. Gambaryan N, Perros F, Montani D, Cohen-Kaminsky S, Mazmanian M, Renaud JF, et al. Targeting of c-kit+ hematopoietic progenitor cells prevents hypoxic pulmonary hypertension. Eur Respir J 2010.
139. Young KC, Torres E, Hatzistergos KE, Hehre D, Suguihara C, Hare JM. Inhibition of the SDF-1 / CXCR4 axis att enuates neonatal hypoxia-induced pulmonary hypertension. Circ Res 2009;104:1293-301.
140. Dorfmuller P, Zarka V, Durand-Gasselin I, Monti G, Balabanian K, Garcia G, et al. Chemokine RANTES in severe pulmonary arterial hypertension. Am J Respir Crit Care Med 2002;165:534-9.
141. Perros F, Montani D, Dorfmuller P, Durand-Gasselin I, Tcherakian C, Le Pavec J, et al. Platelet-derived growth factor expression and function in idiopathic pulmonary arterial hypertension. Am J Respir Crit Care Med 2008;178:81-8..
Source of Support: NIH SCCOR Grant (HL084923) and NIH Program Project Grant (HL014985), Confl ict of Interest: None declared.
Yeager, et al.: Progenitor cells in pulmonary vascular remodeling
“Quick Response Code” link for full text articles
The journal issue has a unique new feature for reaching to the journal’s website without typing a single letter. Each article on its first page has a “Quick Response Code”. Using any mobile or other hand-held device with camera and GPRS/other internet source, one can reach to the full text of that particular article on the journal’s website. Start a QR-code reading software (see list of free applications from http://tinyurl.com/yzlh2tc) and point the camera to the QR-code printed in the journal. It will automatically take you to the HTML full text of that article. One can also use a desktop or laptop with web camera for similar functionality. See http://tinyurl.com/2bw7fn3 or http://tinyurl.com/3ysr3me for the free applications.

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 17
Review Ar t ic le
INTRODUCTION
To quote the first sentence of the recent comprehensive review by Stenmark and colleagues[1] on animal models for pulmonary hypertension, “Pulmonary hypertension is not a disease per se but rather a pathophysiological parameter defined by a mean pulmonary arterial pressure exceeding the upper limits of normal, i.e. ≥25 mmHg at rest”. Intrinsic to this understanding is that this chronic disease will perforce have many steps in its pathogenesis that follow one or, perhaps, more than one “initiating” event(s), likely different for different etiologies, which cascade through
Protein traffi cking dysfunctions: Role in the pathogenesis of pulmonary arterial
hypertensionPravin B. Sehgal1,2, Jason E. Lee1
Departments of 1Cell Biology & Anatomy, and 2Medicine, New York Medical College, Valhalla, New York, USA
ABSTRACT
Earlier electron microscopic data had shown that a hallmark of the vascular remodeling in pulmonary arterial hypertension (PAH) in man and experimental models includes enlarged vacuolated endothelial and smooth muscle cells with increased endoplasmic reticulum and Golgi stacks in pulmonary arterial lesions. In cell culture and in vivo experiments in the monocrotaline model, we observed disruption of Golgi function and intracellular traffi cking with trapping of diverse vesicle tethers, SNAREs and SNAPs in the Golgi membranes of enlarged pulmonary arterial endothelial cells (PAECs) and pulmonary arterial smooth muscle cells (PASMCs). Consequences included the loss of cell surface caveolin-1, hyperactivation of STAT3, mislocalization of eNOS with reduced cell surface/caveolar NO and hypo-S-nitrosylation of traffi cking-relevant proteins. Similar Golgi tether, SNARE and SNAP dysfunctions were also observed in hypoxic PAECs in culture and in PAECs subjected to NO scavenging. Strikingly, a hypo-NO state promoted PAEC mitosis and cell proliferation. Golgi dysfunction was also observed in pulmonary vascular cells in idiopathic PAH (IPAH) in terms of a marked cytoplasmic dispersal and increased cellular content of the Golgi tethers, giantin and p115, in cells in the proliferative, obliterative and plexiform lesions in IPAH. The question of whether there might be a causal relationship between traffi cking dysfunction and vasculopathies of PAH was approached by genetic means using HIV-nef, a protein that disrupts endocytic and trans-Golgi traffi cking. Macaques infected with a chimeric simian immunodefi ciency virus (SIV) containing the HIV-nef gene (SHIV-nef), but not the non-chimeric SIV virus containing the endogenous SIV-nef gene, displayed pulmonary arterial vasculopathies similar to those in human IPAH. Only macaques infected with chimeric SHIV-nef showed pulmonary vascular lesions containing cells with dramatic cytoplasmic dispersal and increase in giantin and p115. Specifi cally, it was the HIV-nef–positive cells that showed increased giantin. Elucidating how each of these changes fi ts into the multifactorial context of hypoxia, reduced NO bioavailability, mutations in BMPR II, modulation of disease penetrance and gender effects in disease occurrence in the pathogenesis of PAH is part of the road ahead.
Key Words: Pulmonary vascular remodeling, intracellular organelles, Golgi apparatus
multiple pathways flowing both in series and parallel, culminating in the pathophysiological changes at the organ, tissue, cellular and subcellular levels evident as the eventual proliferative, obliterative and plexiform pulmonary arterial lesions characteristic of pulmonary arterial hypertension (PAH) [Figure 1]. The focus of this review is on those aspects of the cell biology in PAH that relate to vascular remodeling.[2]
Access this article online
Quick Response Code:Website: www.pulmonarycirculation.org
DOI: 10.4103/2045-8932.78097
Pulm Circ 2011;1:17-32
Address correspondence to:Dr. Pravin B. SehgalDepartments of Cell Biology & Anatomy,Rm. 201 Basic Sciences Building, Valhalla, New York 10595, USAE-mail: [email protected]

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 18
Sehgal and Lee: Protein traffi cking dysfunctions in PAH
We were attracted to the question of dysfunctional intracellular trafficking in PAH by observations of an inverse relationship between the levels of the plasma membrane raft/caveolar protein caveolin-1 (cav-1) and development of PAH in the rat/monocrotaline model.[3] The observations by Zhao and colleagues that cav-1-/- mice spontaneously developed pulmonary hypertension and dilated cardiomyopathy,[4,5] and reports that cav-1 and cav-2 were reduced in the cells in plexiform lesions in patients with severe PAH[6], heightened interest in this inverse relationship. Our initial focus in PAH was in terms of the structure and function of plasma membrane rafts and caveolae and the trafficking of vasorelevant proteins to such specialized subcellular regions on the cell surface and
effects on the transmission of ligand-activated cell surface signals to the cell interior [e.g. the hyperactivation of the IL-6/STAT3 and IL-6/ERK pathways inversely with loss of cav-1 from plasma membrane rafts in pulmonary arterial endothelial cells (PAECs)].[3] In recent years, this focus has expanded to a consideration of broader dysfunctions in anterograde and retrograde vesicular trafficking in the development of PAH.[7,8] Numerous studies have elucidated the molecular and vesicular machineries involved in the trafficking of vasorelevant growth factor and cytokine receptors (as examples, the trafficking of BMPR I and BMPR II, VEGFR, IL-6R and gp130, etc.) from the endoplasmic reticulum (ER) through the Golgi apparatus (abbreviated to “Golgi”) and thence to the plasma
Ctrl-A
IPAH-B
Plex
Oblit
Prolif
IPAH-A
IPAH-B
Ctrl-A
IPAH-B
Plex
Oblit
Prolif
IPAH-A
IPAH-B
200 μm 50 μm 25 μm
Figure 1: Representative histopathologic changes observed in idiopathic pulmonary hypertension. Sections of human lungs (Ctrl-A, IPAH-A and IPAH-B) were stained using H&E and imaged using a ×40 objective in visible light. Elastin autofl uoresence was simultaneously imaged in green and the visible light and autofl uoresence images merged. Representative images showing neointimal proliferation (Prolif), obliterative (Oblit) and plexiform (Plex) lesions are illustrated. Side sets on the right show higher magnifi cation views of the boxed areas within panels in the middle column. (Adapted from ref. 2.)

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 19
Sehgal and Lee: Protein traffi cking dysfunctions in PAH
membrane or via the alternative pathways that “bypass” the Golgi [Figure 2].[7-10] The secretion of cytokines and growth factors by different cell types is also intricately regulated by distinct vesicular trafficking pathways and molecules in different types of cells.[10] Moreover, numerous studies have elucidated the obligatory involvement of membrane-associated pathways (clathrin- or caveolin-mediated endocytic pathways) in the inward transcription-targeted signaling initiated by growth factors, cytokines and ligands (e.g. signaling by transforming growth factor beta (TGF-β), bone morphogenetic proteins (BMPs), interleukin-6 (IL-6), epidermal growth factor (EGF), platelet-derived growth factor (PDGF), vascular endothelial growth factor (VEGF), Notch-3 and Wnt.[11-16] With several of these receptors and ligands implicated in the pathogenesis of PAH,[17-20] it becomes increasingly important to consider the potential involvement of dysfunctional membrane- and protein-
trafficking pathways in the pathogenesis of this disease. The observations that some mutant BMPR II species, such as those observed in patients with familial PAH, failed to traffic normally from the ER to the Golgi and thence to the plasma membrane[20] highlight the importance of investigating the role of protein trafficking dysfunctions in the pathogenesis of PAH.
SPATIAL CELL BIOLOGY – AT THE SUBCELLULAR LEVEL
A constant refrain in our perspective on the involvement of various molecules and mediators of interest in the pathogenesis of PAH is the question of where exactly inside the cell is that particular molecule located.[7,8] Is it in the correct place inside the cell or is its location
Figure 2: Dysfunctional intracellular traffi cking in the pathobiology of pulmonary arterial hypertension. (a) Productive transcriptional signaling from the plasma membrane to the nucleus along the BMP/Smad1/5, TGFβ/Smad2 and IL-6/PY-STAT-3 signaling pathways is membrane associated. IL-6/STAT3 and ERK1/2 signaling is inversely related to loss of caveolar/raft cav-1. (b) Golgi blockade mechanisms in PAH. MCTP and hypoxia lead to a trapping of vesicle tethers, SNAREs and SNAPs in the Golgi of affected pulmonary arterial endothelial cells. This leads to a block in anterograde traffi cking of vasorelevant cargo proteins such as cav-1 and eNOS and reduced caveolar NO production. The intracellularly sequestered eNOS produces NO which may potentially S-nitrosylate cysteine-rich proteins like NSF, further inhibiting traffi cking. Golgi-trapped dominant negative BMPR 2 mutants may also potentially block traffi cking of cargo proteins to the plasma membrane. (Adapted from ref. 8.)
Golgi megalocytosis
eNOS
NSFNSF
Sequestered
Trapped tethers,
SNARES and SNAPsMonocrotaline
Hypoxia
Sequestered
eNO
S
Blocked anterograde trafficking
caveolarNO
NO
ER
Endocytosis
ER
Lysosomes
IL-6/PY-STAT3, BMP/Smad 1/5, TGFβ/Smad 2Nuclear Signaling
[STAT3, EGFR, TGFβR]
Rab7 EEA1, Rab5
Smad2SARA
PY-STAT3BMPR1,2
Nef
STAT3
EGFR
Turnover
Smad1/5
Nucleus
C la t h r in
a
b
BMPs
Ang1
TGFβ
IL-6
BMPR2 mutants ?
Tie2
BMPR1,2
gp130
TGFβR Tie2
cav-1
IL-6/PY-STAT3,ERK1/2
PY-STAT3
?NSFNSF
Thrombogeniccell surface
? altered vesicular trafficking Caveolar
Promitogenic; ant iapoptot ic
Caveolarcav-1eNOS
BMPR2Tie2
PECAM-1

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 20
Sehgal and Lee: Protein traffi cking dysfunctions in PAH
aberrant? As a consequence of aberrant location, is the function aberrant? As one example, when investigators report the increase in eNOS in PAECs in, for example, the monocrotaline/rat model of PAH,[21] we wondered exactly where within the cell was the eNOS located. Was it at the cell surface and available for function or was it trapped in a non-functional intracellular compartment? As another example, do mutant BMPR II species[20] have dominant negative effects on the intracellular trafficking of other molecules, including eNOS, other receptors and membrane-associated signaling pathways?
INSIGHTS FROM PRIOR LITERATURE
In 1914, Cajal reported finding a compact juxtanuclear “apparato reticular de Golgi” in endothelial cells and the fragmentation and pulverization of this Golgi apparatus in cells (neuronal cells) subjected to hypoxia.[22] The pulmonary hypertension literature over the last four decades contains numerous pieces of data indicative of defects in intracellular trafficking in the cellular elements in pulmonary arterial lesions.[7,8] Noteworthy among these are histologic and electron microscopic (EM) studies reporting “plump” and “enlarged” endothelial and smooth muscle cells with increased vacuolation, Golgi stacks and ER in hypoxic and primary PAH.[23-30] Particularly evocative are the EM studies reporting extensive rough ER with dilated cisternae in a cell within a plexiform lesion in idiopathic PAH,[26] and a cell showing distended globular and granular structures.[28] Meyrick and Reid[25] reported “hypertrophied smooth muscle cells (with) a significant increase in relative areal proportions of Golgi apparatus and rough sarcoplasmic reticulum in the tunica media of the hilar artery of rats with hypoxia-induced PAH” and further commented that such rats have “thickened endothelial cells (with) a more extensive Golgi apparatus than normal and many have swollen cisternae of rough endoplasmic reticulum”. Increased accumulations of Weibel-Palade bodies (which are vesicular structures involved in the exocytosis of Factor VIII) were reported in endothelial cells in hypoxic rats with PAH[29] and in human primary PAH.[27] Mette and colleagues[30] reported marked accumulations of vesicular cytoplasmic structures in cells in pulmonary vascular lesions of patients with PAH with HIV infection. Taken together, these prior observations point to dysfunctions in intracellular membrane trafficking in cells located within lesions in PAH.
A major line of research extending back to the observations of Harris et al. in 1944,[31,32] Bull in 1955[33] and the EM studies of Klienerman and Merkow in 1966[34] and of Afzelius and Schoental in 1967[35] is also particularly insightful. These and subsequent investigators[36-39] studied the effects of pyrrolizidene alkaloids on various cell
types and tissues. One of these alkaloids, monocrotaline (MCT), is the basis for a widely used, and widely debated, experimental model of PAH in rats, pigs and dogs.[1,36-39]
Harris et al.[31,32] and Bull[33] reported that pyrrolizidene alkaloid treated liver cells (which themselves metabolically activate the alkaloid) continued to grow in size but not divide. This phenotype was termed “megalocytosis” by Bull in 1955.[33] PAECs and alveolar type II cells in lungs of rats exposed to MCT that developed PAH showed increased vacuolation, increased ER and extensive Golgi complexes.[34,37-40] Afzelius and Schoental[35] pointed out that “one of the most striking features of the enlarged cells is the lack of normal distribution of organelles”. Specifically, Afzelius and Schoental[35] linked the “large size of the Golgi complexes” to defects in “sorting out of organelles into separate regions” as well as a defect in entry of cells into mitosis, yielding “growing, but non-dividing cells”.
In 1991, Reindel and Roth[40] extended the above insightful observations to changes in bovine pulmonary artery endothelial and smooth muscle cells in culture exposed to the bioactive monocrotaline pyrrole (MCTP). Ultrastructurally, the hypertrophic MCTP-treated bovine pulmonary artery endothelial cells (BPAECs) had enlarged cell profiles with enlarged nuclei and “prominent” Golgi apparatus and endoplasmic reticulum.[40] In the last 20 years, these investigators as well as the research groups of Segall and Wilson pioneered extensive cell culture studies of the MCTP-induced megalocytosis in pulmonary vascular cells.[39,41,42] A landmark observation by the Segall and Wilson groups has been the identification of specific Cys-containing and Cys-free proteins that are covalently derivatized by MCTP when human PAECs were exposed by radioisotope labeled MCTP – this list included proteins that help fold newly synthesized proteins in the lumen of the ER (such as the protein disulfide isomerases, ERp57 and PDI) as well as cell surface proteins such as galectin-1.[41,42]
The above data in the prior literature taken together point to dysfunctions in intracellular membrane trafficking in cells exposed to bioactive pyrrolizidene alkaloids.
Following the discovery of the relationship between mutations in BMPR II and idiopathic PAH (IPAH) (both the familial and sporadic types) beginning approximately 10 years ago,[43] it was realized that several of the relevant mutant BMPR II species failed to traffic correctly to the plasma membrane.[20,44,45] Subsequent detailed studies have identified PAH disease-related BMPR II mutants that remain sequestered in the ER, sequestered in the Golgi or even those that traffic to the plasma membrane and yet exhibit defective signaling.[20,44,45] These data raise the question of potential dominant negative effects of such BMPR II mutants on the intracellular trafficking of other vasorelevant molecules. Mice harboring such mutant

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 21
Sehgal and Lee: Protein traffi cking dysfunctions in PAH
BMPR II genes have proven informative in exploring the pathogenesis of PAH.[1,46,47] However, the incomplete penetrance of disease parameters in even the BMPR II knockout model[46] suggests that additional environmental and genetic factors influence PAH pathogenesis.[1,20]
The observations by Zhao and colleagues in 2002 that cav-1-/- mice spontaneously developed pulmonary hypertension and dilated cardiomyopathy[4,5] highlight the ability of defects in trafficking scaffolding proteins to initiate a cascade of changes including pulmonary hypercellularity, interstitial fibrosis, thickening of the alveolar septa and reduced exercise tolerance.[48-50]
In pioneering observations Flores and colleagues[51] reported in 2006 that macaques infected with a chimeric simian immunodeficiency virus (SIV) in which the endogenous SIV-nef had been replaced by the HIV-nef gene (dubbed SHIV-nef virus) developed pulmonary arterial lesions similar to those seen in IPAH. These lesions included complex plexiform-like lesions characterized by medial hypertrophy and luminal obliteration. Such lesions included cells that were nef−, Factor VIII−, and/or smooth muscle-specific actin-positive. Such lesions were not observed in macaques infected with the non-chimeric SIV virus. In parallel, Flores and colleagues[51] reported that HIV-nef–positive cells were also observed in pulmonary vascular lesions in HIV-positive patients but not in patients with IPAH. The fact that HIV-nef is a protein that is well known to interfere with and modulate endocytic and Golgi trafficking pathways, and has been best investigated in terms of its effects on intracellular trafficking pathways involved in major histocompatibility complex (MHC) antigen presentation,[9,52-55] again point to dysfunctional protein trafficking as, at the very least, part of the overall process leading to pulmonary vascular lesions.
The above brief overview of the prior PAH literature highlights previously published data that clearly pointed to the occurrence of protein trafficking dysfunctions in PAH. The seminal hypothesis of Afzelius and Schoental[35]
linking Golgi dysfunction to organellar defects on the one hand and to entry into mitosis and effects on cell proliferation on the other hand represents an important link in discussions of how trafficking defects can underlie effects on cell size and cell proliferation. Organelles such as the Golgi apparatus stand at the interface between trafficking and cell proliferation.
DISRUPTION OF ENDOTHELIAL CELL CAV-1/RAFT SCAFFOLDING IN PAH
In 2002, we observed that normal IL-6 signaling in different cell types to the cell interior was dependent on
the integrity of cholesterol-rich plasma membrane raft microdomains.[12,56] In 2004, we reported that in the MCT/rat model although PAH and right ventricular hypertrophy developed by 2 weeks after MCT, a reduction in cav-1 levels in the lung was apparent within 48 hrs, declining to 30% of control levels by 2 weeks, accompanied by an increase in the activation of the transcription factor, PY -STAT3, which also began within 48 hrs.[3] Immunofluorescence studies showed a loss of cav-1 in PAECs within 48 hrs after MCT but an increase in PY-STAT3. At the single-cell level in pulmonary arteries of MCT-treated rats, the particular PAECs that showed reduced cav-1 were the ones that showed increased PY-STAT3 and nuclear immunostaining for proliferating cell nuclear antigen (PCNA). Cell fractionation studies showed that there was a loss of cav-1 from detergent-resistant membrane raft fraction concomitant with hyperactivation of PY-STAT3. Additionally, PAECs treated with MCTP in culture developed megalocytosis associated with hypo-oligomerization and reduction of cav-1, hyperactivation of PY-STAT3 and ERK1/2, and stimulation of DNA synthesis. These data suggested the occurrence of defects in the trafficking of cav-1 to plasma membrane rafts in MCTP-treated cells with a consequent promitogenic cascade of events.[3]
Lisanti and colleagues[50] confirmed and extended the above observations in the rat/MCT model and showed that the decline in cav-1 and cav-2 and development of PAH as well as the activation of PY-STAT3 and upregulation of cyclins D1 and D3 could be blocked by a cav-1-mimetic peptide (AP-Cav) administered 30 min after MCT administration. The loss of cav-1 from cells in plexiform lesions in severe IPAH,[6] in rats with PAH following experimental myocardial infarction,[49] those administered SU5419[6] and the ability of the cholesterol reducing agent, simvastatin, to reduce the severity of PAH in the MCT/rat model[57,58] further supported interest in the mechanisms underlying the trafficking and loss of cav-1 in PAECs in PAH.
In studies that recapitulated the earlier work of Riendel and Roth and of the Segall and Wilson research groups on the effects of MCTP on pulmonary vascular cells in culture,[39,40] we observed that pulmonary vascular cells exposed to MCTP displayed megalocytosis within 24–48 hrs of exposure with the trapping of cav-1 in the enlarged Golgi apparatus. In these studies, the Golgi apparatus was observed using immunostaining for a Golgi tether/scaffolding protein called GM130 [Figure 3].[3,59] Subsequent studies showed that this phenotype in PAECs was characterized by a cascade of changes including increased DNA synthesis but reduced entry into mitosis, increased PY-STAT3, an incomplete unfolded protein response, reduced cdc2 but increased

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 22
p21, and various alterations in cyclins D1, D3, E, A and B1.[59-62] It was noteworthy that eNOS was also lost from the plasma membrane and now increasingly sequestered in the Golgi and in intracellular vesicular structures.[62-64] The increased sequestration of cav-1 in the Golgi membranes was apparent within 6–8 hrs after MCTP exposure, that is, in advance of any other phenotypic alteration. Similar alterations were also observed in PAECs exposed to hypoxia.[62] These observations led to the hypothesis that defective trafficking of proteins through the Golgi apparatus might represent an event in how MCTP and hypoxia affected pulmonary vascular cells and that this trafficking disruption might also be of relevance in the human disease (Golgi blockade hypothesis).[59]
BMPR II has been reported to be located in lipid rafts, including caveolae, in human and rat pulmonary arterial endothelium.[65] Additionally, cav-1 has been shown to regulate the caveolar localization and transcriptional activation function of BMPR II in mouse aortic smooth muscle cells.[66] BMPR II interacted with cav-1 and downregulation of cav-1 using an siRNA approach decreased BMP-dependent Smad phosphorylation and gene regulation. Reduction in cav-1 or a dominant-negative mutant of cav-1 reduced BMPR II plasma membrane localization. A reduction in cav-1 also reduced the association between BMPR II and BMPR I.[66] In MCTP-treated PAECs, BMPR II was increasingly trapped in the Golgi membranes together with increased trapping of cav-1 and eNOS,[62] and such cells displayed altered functional BMP/Smad signaling.[67,68]
However, several puzzling questions about the relationship between cav-1 and development of PAH prompt a more
detailed look at the subcellular/intracellular events that might be at play. On the one hand, overexpression of wild-type (wt) cav-1 in PAECs inhibited IL-6/STAT3 transcriptional signaling,[15] and thus, the inverse relationship between cav-1 levels and PY-STAT3 levels in PAECs in rats exposed to MCT or in the cav-1 knockout mouse appears reasonable. In the latter case, an interpretation would be that disruption of cav-1/rafts per se produced the hyperactivation of IL-6/PY-STAT3 because cav-1 in rafts is inhibitory to such signaling. On the other hand, the Antennapedia-Cav-1 membrane-permeable small peptide used by Jasmin et al.[50] that inhibited MCT-induced PAH and also inhibited the loss of cav-1 (and cav-2) and the increase in PY-STAT3 corresponds to the scaffolding domain of cav-1 and should have also disrupted cav-1 rafts and had the opposite effects – if the effects were solely due to events at the level of the plasma membrane caveolae. It is known from our prior work that raft disruption by other means (such as using the cholesterol binding compounds, filipin III or β-methylcyclodextrin) inhibited IL-6/STAT3 signaling, even in cells low in cav-1 (in such cells, “plasma membrane rafts” are formed by other proteins such as flotillin-1 or flotillin-2).[12,56] One possible way to resolve these seemingly contradictory observations is to extend the discussion to intracellular trafficking pathways. The cav- 1/caveosome retrograde trafficking has been shown to inhibit TGF-β/Smad transcriptional signaling by shunting the activated Smad molecules toward lysosomal degradation, while clathrin/endocytic trafficking leads to transcriptionally productive signaling.[11] Similarly, the majority of activated PY-STAT3 in the cytoplasm is associated with the early endosome compartment[13,69] and overexpression of cav-1 increasingly targets STAT3
GM130/DAPI
Control MCTP MCTP
Figure 3: Golgi enlargement and fragmentation in primary bovine PAECs in culture exposed to MCTP for 4 days. BPAEC cultures in a 6-well plate were exposed to MCTP and megalocytosis was allowed to develop for 4 days.[3,7,8] The cultures were then fi xed and immunostained for the Golgi tether, GM130, and for nuclei using 4’,6-diamidino-2-phenylindole (DAPI). Scale bar=4 μm.
Sehgal and Lee: Protein traffi cking dysfunctions in PAH

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 23
toward the lysosomal compartment.[15] The possibility of cav-1 levels affecting intracellular retrograde signaling pathways has not been explored in the context of PAH. To add to the puzzle are more recent observations of Zhou et al.[5] showing that lungs in the cav-1-/- mouse display persistent eNOS activation and that the PAH observed can be reduced by a superoxide scavenger (MnTMPyP) or a NOS inhibitor (L-NAME). However, it was not evaluated where exactly within the endothelial and/or bronchial epithelial cells was the eNOS located. Additionally, Patel et al.[70] reported increased cav-1 in PASMCs in patients with IPAH and interpreted their cell culture experiments to indicate that increased cav-1 and caveolae “contribute to IPAH-PASMC pathophysiology”. Moreover, Patel et al.[70] suggest that “disruption of caveolae in PASMC may provide a novel therapeutic approach to attenuate disease manifestations of IPAH”, which would be the opposite of the inference of an inverse relationship between cav-1 and PAH from the studies summarized above. Perhaps, the many unanswered puzzles at hand relate to cell type, disease heterogeneity, lesion heterogeneity and the multiple different levels at which cav-1 can affect intracellular trafficking pathways and functions of vasoactive molecules (such as eNOS and BMPR II). There is a clear need for a more detailed understanding of the subcellular events that connect cav-1–mediated trafficking and regulatory pathways to the development of PAH.
The above considerations led us to evaluate various molecules and cellular organelles involved in both Golgi to plasma membrane (anterograde; exocytosis) and plasma membrane to cell interior (retrograde; endocytosis) trafficking in pulmonary vascular cells, both in pulmonary vascular cells in culture under various experimental conditions and in cells in pulmonary vascular disease lesions in IPAH and in the MCT/rat and SHIV-nef/macaque models.
BRIEF OVERVIEW OF VESICULAR TRAFFICKING MACHINERIES AND MOLECULES
Intracellular protein trafficking involves the selective scission of vesicles from membranous organelles, followed by the selective and targeted capture of such vesicles by other membrane organelles and membrane fusion.[7-10,62,64,71,72] This process requires molecules on the surface of vesicles and on acceptor membranes that recognize each other with specificity (the tethers and SNAREs (soluble N-ethylmaleimide-sensitive factor attachment protein receptor)], molecules that are involved in the recruitment of an ATPase to the SNARE complexes [the SNAPs (soluble N-ethylmaleimide-sensitive factor attachment protein) and NSF (N-ethylmaleimide-
sensitive factor)] and an additional hierarchy of molecules belonging to the complexin and Sec-Munc (SM) family of proteins that provide an additional layer of regulation [Figures 4 and 5]. Several reviews provide considerable details about these molecules and mechanisms and show that this is an exciting new area of considerable ongoing research in cell biology today.[8,10,71,72]
Figure 4 is a brief compilation of the molecules that are part of the discussion relating to pathogenesis of PAH. “Tethers” represent cell surface molecules on respective vesicle and target membrane surfaces that search for and mediate binding of cognately recognized molecules at long distance (up to 50 nm) [Figure 5]. Each organelle and vesicle type contains several such tethers. In the Golgi, these tethers include giantin, p115 and Golgi matrix 130 kDa (GM130). In addition to tethering, these molecules also mediate more specific functions in the respective organelle (such as structural scaffolding, phosphorylation-mediated organelle fragmentation and apoptosis). Tether interactions draw the vesicle and target membrane surface closer to each other, and at distances of 25 nm or less, groups of proteins called SNAREs come together as part of a four-helix complex called a trans-SNARE complex [Figure 5]. One of the helices is contributed by the SNARE on the vesicle membrane, while the other three are contributed by two or three SNAREs on the target membrane. There are 38 different SNAREs in human cells and these mediate specific interactions with cognate molecules [Figures 4 and 5]. Thus, the combinations of specific SNAREs provide the addressing mechanisms (like Zip Codes) for vesicular trafficking. The SNAREs are classified as Q- and R-SNARES depending upon their
N-ethymaleimide sensitive factor (NSF): NO-sensitive
Golgi tethers: giantin, p115, GM130, others
SNAP: soluble NSF accepting protein
SNARE: SNAP receptor
Complexins and SM family of proteins; sorting nexins
Q-SNARE=t-SNARE; R-SNARE=v-SNARE (38 SNAREs in human cells)
Q-SNARE family members
Qa: syntaxin 1 (STX1), STX2, STX3, STX4, STX5, STX7, STX11, STX13, STX16, STX 17 and STX18
Qb: GS27 (Golgi SNARE of 27 kDa), GS28, Vti1a (vesicle transport through interaction with t-SNARE homolog 1a) and Vti1b
Qc: STX6, STX8 and STX10, GS15, BET1 and SLT1 (SNARE-like tail-anchor protein 1)
Qb,c: SNAP23, SNAP25, SNAP29 and SNAP47
R: VAMP1 (vesicle-associated membrane protein 1), VAMP2, VAMP3, VAMP4, VAMP5, VAMP7, VAMP8, ERS24 (SEC22b) and YKT6
Figure 4: Tethers, SNAREs, SNAPs, NSF and additional molecules involved in vesicular traffi cking
Sehgal and Lee: Protein traffi cking dysfunctions in PAH

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 24
underlying amino acid motifs (Q-SNAREs are typically t- or target-SNAREs, while R-SNAREs are typically v- or vesicle SNAREs).
The trans-SNARE complex drives the membrane fusion reaction [Figure 5]. However, this membrane fusion event is regulated by the family of complexin and Sec-Munc proteins.[71,72] Subsequent to membrane fusion, the now cis-SNARE complex recruits a soluble cytosolic protein called a SNAP (α-, β- or γ-SNAP) (not to be confused with SNAP proteins identified by numerical designations such as SNAP23, etc.; the latter are SNARE proteins). Of the SNAP proteins, α-SNAP is the most ubiquitous (present in PAECs and PASMCs) and this protein, in turn, recruits the cytosolic ATPase called NSF to the cis-SNARE complex. NSF, in an energy dependent manner, leads to the disassembly of the four-helix complex into its component SNAREs, preparing this machinery for another round of membrane fusion. Thus, in PAECs and PASMCs, α -SNAP and NSF participate in virtually all vesicular trafficking. Moreover, it is noteworthy that the ATPase activity of NSF is inhibited by NO through S-nitrosylation at multiple Cys residues.[73] Finally, a range of additional GTPases (the dynamin family and the Rab family of GTPases)
are involved in the process of scission of the newly forming vesicle for organellar membranes with different membrane trafficking pathways requiring different GTPases in a selective manner.[9-11]
Dysfunctions of Golgi tethers, SNAREs, -SNAP and NSF in pulmonary vascular cells exposed to MCTP, hypoxia, NO scavenging and senescencePAECs exposed to MCTP in cell culture had shown increased trapping of cav-1 in Golgi membranes as early as 6 hrs after MCTP.[62] In this experimental system, a combination of immunofluorescence and cell-fractionation studies revealed the considerable accumulation of diverse Golgi trafficking mediator proteins in the enlarged/circumnuclear Golgi apparatus by 1–2 days after exposure to MCTP or the NO scavenger, c-PTIO [Figures 3 and 6]. These proteins included GM130, p115, giantin, golgin 84, syntaxin-4, -6, Vti1a, Vti1b, GS15, GS27, GS28, SNAP23 and α-SNAP. Strikingly, NSF, the ATPase required in all vesicular trafficking, was increasingly sequestered in non-Golgi vesicular elements and was depleted from Golgi membranes.[64] The sequestration of a large collection of trafficking-mediator molecules in the Golgi was accompanied by intracellular accumulation of eNOS
Figure 5: The SNARE cycle in membrane fusion. Initial interaction between a vesicle and its target membrane is mediated by cognate tethers. Membrane fusion is then mediated by the formation of a quaternary-α-helical trans-SNARE complex consisting of one v- (or R -) SNARE on the vesicle and two or three t- (or Q-) SNAREs on the target membrane. After membrane fusion, the cis-SNARE complex is disassembled by the ATPase NSF which is recruited to the cis-SNARE complex from the cytosol by α-SNAP. (Adapted from ref. 8.)
Sehgal and Lee: Protein traffi cking dysfunctions in PAH

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 25
and reduced caveolar NO production as assayed using live-cell DAF2-DA imaging.[62-64] The reduced levels of caveolar NO in MCTP-treated cells were consistent with the observation of reduced S -nitrosylation of NSF, eNOS and cav-1 in such cells.[63,64] Thus, although total eNOS levels were either unchanged (on a total cell protein basis) after MCTP or were increased, this eNOS was mislocalized to the incorrect intracellular compartment and was thus hypofunctional. These effects were evident in cultures of both bovine and human PAECs [Figures 3 and 6].[74,75]
An enlarged Golgi, as evidenced by increased circumnuclear accumulation of GM130 and giantin, was observed in PAECs in rat lungs within 4 days after administration of MCT to rats.[62] Thus, this Golgi alteration was observed at a time when there was no evidence of PAH which takes 10–14 days to develop.[3,62] Because the changes in the Golgi preceded development of PAH, the data suggested that such changes might lie in the pathway of causality
leading to the disease and were not a consequence of increased pulmonary arterial pressure per se.
PAECs exposed to hypoxia (1.5% v/v oxygen in room air) for 4 days also showed a similar phenotype.[63] The cells were enlarged and contained enlarged circumnuclear Golgi with increased trapping of GM130, p115, syntaxin 6, GS28, together with cav-1 and eNOS in Golgi membranes. In such cells, the eNOS was mislocalized away from the plasma membrane. Senescent PAECs also exhibited a similar phenotype with enlarged cells with increased GM130, giantin, p115, GS28, syntaxin 6, Vti1a in the enlarged Golgi with marked intracellular mislocalization of eNOS and cav-1.[63]
Various investigators had previously suggested that at least some instances of PAH might include reduced bioavailability of NO.[75] We observed that scavenging NO from cultures of bovine PAECs or human PAECs
Figure 6: Golgi fragmentation and dispersal in human PAECs after exposure to MCTP or the NO scavenger, c-PTIO. Primary HPAEC cultures in 6-well plates were exposed to MCTP once or to c-PTIO (100 μM) continuously for 48 hrs. The integrity of the Golgi was assayed by immunotagging for the Golgi tether, giantin, together with DAPI staining for demarcating nuclei. NIH Image J software using Otsu segmentation analyses were used to determine Golgi structures with fragment number greater than 1[75] and are enumerated as % cells with dispersed Golgi. Scale bar=20 μm
Primary human PAEC (48 hr after exposure)Control MCTP c-PTIO
n =
% Disp
205
33%
323
82%
125
100%
Gia
ntin
DA
PIGia
ntin
Hig
h m
ag
Sehgal and Lee: Protein traffi cking dysfunctions in PAH

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 26
and PASMCs led to marked Golgi fragmentation [Figure 6].[74,75] However, although MCTP exposure reduced entry of PAECs into mitosis, exposure of PAECs to the NO scavenger, c-PTIO, markedly increased the entry of endothelial cells into mitosis.[74] Thus, a hypo-NO state was promitogenic, at least for PAECs in culture.
Inhibition of functional endocytosis and an unusual secretory phenotypeIn functional ligand uptake assays, we observed that PAECs exposed to MCTP showed intact uptake and sequestration of C5-ceramide to the Golgi membranes but a marked inhibition of the endocytic uptake of LDL (clathrin-mediated endocytosis), transferrin (clathrin-mediated endocytosis) and cholera toxin (caveolar endocytosis).[74] In comparison, NO scavenging using c-PTIO inhibited the uptake of all four tracers.[74] Both MCTP and c-PTIO reduced the cell surface concentrations of low density lipoprotein receptor (LDLR), TfnR, BMPR II, Tie-2 and PECAM-1, albeit to differing extents. Neither MCTP nor c-PTIO affected the uptake and subcellular localization of LysoTracker, ERTracker or MitoTracker. Thus, there was clear selectivity in the effects of these agents on intracellular trafficking.
However, both MCTP and c-PTIO generated an unusual secretory phenotype in PAECs.[74] After an initial inhibition of the secretion of exogenously expressed soluble HRP over the first day following exposure to either MCTP or c-PTIO,[62,74] there was a marked increase in secretion over and above that seen in untreated PAECs.[74] This marked increase in secretion was sustained for the duration of the 5-day assay despite development of clear megalocytosis. This unusual secretory phenotype recalls (1) the senescence-associated secretory phenotype reported recently by Campisi and colleagues[77,78] in which senescent breast cancer cells secrete growth factors (including IL-6 and IL-8) which then recruit and enhance the function of infiltrating immune cells leading to increased tumorigenicity with increasing age and (2) the thesis, often stated, that the endothelial cells in pulmonary vascular lesions release cytokines and growth factors that then lead to the migration of smooth muscle cells into previously non-muscular arteries or even the conversion of arterial pericytes into smooth muscle cells.[3,17,18] The spectrum of cytokines and growth factors secreted by, for example, say, human PAECs in response to a hypo-NO state[74-76] would be important to elucidate as part of delineating a “PAH-associated persistent secretory phenotype” of the affected endothelial cells.
Dysfunctions of Golgi tethers, SNAREs and SNAPs in IPAHThe histological and EM data in IPAH reviewed in the section “Insights from Prior Literature” already included
evidence of alterations in the structure of the Golgi apparatus and of various membrane organelles such as the endoplasmic reticulum in cells of IPAH lesions. Given this prior information, we asked whether we could extend this to identifying dysfunctions of specific Golgi tethers, SNAREs and α SNAP. A technical limitation in carrying out these analyses was the availability, at the moment, of only archived formalin-fixed, paraffin-embedded tissue from patients with IPAH. For now, we have been limited to evaluating only those tethers, SNAREs and α SNAP for which the respective antibodies can react with tissue antigens still immunoreactive despite the fixation, embedding and long-term storage.[2,75]
Sections of lung tissue corresponding to the IPAH patients and lesions shown in part in Figure 1 were subjected to immunofluorescence imaging for the Golgi tethers, giantin and p115.[2] Compared to pulmonary vascular cells in controls without PAH, there was an increase in the amounts of these Golgi tethers on a per cell basis in lung tissue from patients with IPAH, accompanied by marked cytoplasmic dispersal of giantin- and p115-bearing vesicular elements in the vascular cells in the proliferative, obliterative and plexiform lesions[2] [Figures 7 and 8]. High-resolution subcellular 3D imaging of immunotagged giantin confirmed marked Golgi fragmentation and increased cell size of individual cells in pulmonary arterial lesions in IPAH compared to compact Golgi in controls.[75] Immunofluorescence tagging followed by high-resolution 3D imaging of subcellular structures also revealed increased levels of the SNARE Vti1a and α-SNAP cells in IPAH lesions in dispersed cytoplasmic vesicular elements.[75]
Dysfunctions of Golgi tethers, SNAREs and SNAPs in the SHIV-nef/macaque modelThe SHIV-nef–infected macaque model has proven informative in helping address the question whether Golgi and trafficking dysfunctions might lie in the chain of causality of pulmonary vasculopathies. Flores and colleagues[51] had previously shown that macaques infected with the chimeric SHIV-nef virus, but not those infected with the non-chimeric SIV virus, developed pulmonary vasculopathies similar to those seen in IPAH. Figure 9 shows the pulmonary vascular histopathology observed in SHIV-nef–infected macaques to that observed in IPAH in the proliferative, obliterative and plexiform lesions in a manner that is directly comparable to the histopathology shown in Figure 1 for IPAH.[2] Since HIV-nef had been previously shown to interfere with endocytic and Golgi trafficking, the data implied that these vasculopathies might be initiated by such trafficking defects.[9,52-55] The question remained whether cells in pulmonary vascular lesions in SHIV-nef–infected macaques did indeed display Golgi defects. This was addressed by
Sehgal and Lee: Protein traffi cking dysfunctions in PAH

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 27
quantitative immunofluorescence assays as well as high-resolution 3D imaging of subcellular organelles in cells in SHIV-nef–induced pulmonary vasculopathies compared to those in SIV-infected or uninfected macaques.[2,75] Only macaques infected with the chimeric SHIV-nef virus showed pulmonary vascular lesions containing cells with dramatic increase in and cytoplasmic dispersal of the Golgi tethers, giantin and p115 [Figures 10 and 11]. High-resolution 3D subcellular imaging confirmed the extensive fragmentation of the Golgi in such cells. Moreover, it was specifically only those cells that contained endocytic nef that showed enlarged dispersed vesicular Golgi elements [Figure 12].[2,75] In contrast, giantin and p115 immunostaining of pulmonary vascular cells in SIV-infected or uninfected macaques showed a discrete compact Golgi.
GiantinHuman
Ctr
l -A
IPA
H-B
p115
Ctr
l -A
IPA
H-B
a
b
DAPI
Figure 7: Increased accumulation of the Golgi matrix proteins/tethers, giantin and p115, in cellular elements in pulmonary arterial vasculopathies in human IPAH. (a) Representative images of respective vasculopathies probed for giantin or p115 compared to representative controls. Scale bar=85 μm. (b) Representative higher magnifi cation images of giantin and p115 immunostaining from analyses as in Figure 7a. Scale bar=10 μm. (Adapted from ref. 2.)
2
4
6
8
10
12
14
2
4
6
8
10
12
14
PAHCtrl
a. Giantin b. p115
*
**
* *
PAEC Art. wall Plex Oblt PAEC
145
175
201
284
219
193
116
135n
Human IPAH
Int.
pixe
l int
ensi
ty/c
ell (
A.U
.)
PAEC: SMA-neg; vWF-pos; Art wall cells: SMA-pos; vWF neg; Plex and Oblit: various
Figure 8: Summary of the quantitative immunomorphometry data for the Golgi tethers, giantin and p115, in cellular elements in pulmonary arterial vasculopathies in IPAH. Integrated pixel intensity/cell was computed using Image J software by outlining individual cells within immunofl uorescence images corresponding to luminal endothelium (PAEC), cells in arterial walls, in plexiform lesions and in obliterative lesions and was expressed in arbitrary units (A.U.). Images for quantitation were derived from sections in the set of the human control and IPAH patients as in ref. 2. All the per cell data (n as indicated in the fi gure) were pooled into either control or IPAH and evaluated using Student’s two-tailed t-test. Asterisks indicate P<0.0001 for groups compared with the corresponding control groups; cells in plexiform lesions and in the obliterative lesions were compared with the control PAEC group. In Panel b, there was little detectable p115 signal in the control PAECs evaluated. (Adapted from ref. 2.)
Additionally, both Vti1a and α-SNAP were increased in per cell amounts and localized to cytoplasmic vesicular structures in cells in the pulmonary vascular lesions in SHIV-nef–infected macaques.[75] These data, especially the more recent high-resolution 3D imaging studies,[75] provide evidence in support of an underlying trafficking defect in nef-containing cells in this model of pulmonary vasculopathy. Flores and colleagues are currently engaged in the isolation of HIV virus from AIDS patients with PAH or without PAH and carrying out genetic sequence analyses of the respective HIV-nef genes in order to help identify mutations that predispose toward PAH.[79]
It has been recently reported that exposure of porcine pulmonary artery rings and human PAECs in culture to HIV-nef protein for 24 hrs led to decreased vasorelaxation, decreased eNOS expression, decreased eNOS antigen by immunohistochemistry and reduced NO bioavailability.[80] It is an exciting possibility that reduced NO bioavailability subsequent to endosomal uptake of HIV-nef might mechanistically contribute to Golgi fragmentation in a manner similar to that observed after NO scavenging[64,74-76] and it can be tested in future studies using the subcellular 3D imaging approach.
Sehgal and Lee: Protein traffi cking dysfunctions in PAH

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 28
Figure 9: Representative histopathologic changes observed in pulmonary vascular lesions in SHIV-nef–infected macaques. Sections of lungs from macaques infected with the chimeric SHIV-nef virus (SHIV-A) or a non-chimeric SIV virus (SIV-F) were stained using H&E and imaged using a ×40 objective in visible light. Elastin autofl uoresence was simultaneously imaged in green and the visible light and autofl uoresence images merged. Representative images showing neointimal proliferation (Prolif), obliterative (Oblit) and plexiform (Plex) lesions are illustrated. Side sets on the right show higher magnifi cation views of the boxed areas within each panel in the middle column. (Adapted from ref. 2.)
SIV-F
SHIV-AProlif
Plex
Oblit
SHIV-A
SHIV-A
SIV-F
SHIV-AProlif
Plex
Oblit
SHIV-A
SHIV-A
200 µm 50 µm 25 µm
Defective trafficking of mutants of BMPR IIThe pioneering studies of Morrell and colleagues[20,43,45] and of Nishihara and colleagues[44] have drawn attention to the observations that several of the mutants of BMPR II found in patients with PAH show defective trafficking in their traverse from the ER to the Golgi and thence to the plasma membrane. Using green fluorescent protein (GFP) -tagged constructs of wt and mutant BMPR II species, Rudarakanchana et al.[45] and Nishihara et al.[44] showed the failure of several such mutants to traffic to the plasma membrane. BMPR II proteins containing mutations in the conserved Cys residues in the ligand binding remained increasingly trapped in the ER and the Golgi apparatus,
while those with mutations in the kinase domain appeared to traffic to the plasma membrane but displayed reduced BMP/Smad signaling. However, all mutants investigated showed a gain in function involving upregulation of p38MAPK-dependent proproliferative pathways.[20,81]
Chemical chaperones (thapsigargin, glycerol or sodium 4-phenylbutyrate) increased the trafficking of the C118W BMPR II mutant to the cell surface, accompanied by enhanced BMP/Smad signaling.[82] However, several parts of the puzzle of how mutations in BMPR II eventually lead to PAH disease manifestations include (1) the incomplete and delayed penetrance,[17-20] (2) the gender dependence,[17-20,83] (3) the postulated roles of additional
Sehgal and Lee: Protein traffi cking dysfunctions in PAH

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 29
unknown genetic and/or environmental factors,[17-20] and (4) that in some cases of PAH, there are reduced levels of BMPR II and reduced BMP/Smad signaling even though there are no mutations in BMPR II.[84]
The consequences of mutations in BMPR II on the traf f icking of other vasorelevant proteins (such as eNOS) and receptors (such as gp130 or IL-6R or VEGFR) in trans have not been adequately investigated. Moreover, since Smad signaling is obligatorily dependent on membrane-associated endocytic pathways for transcriptional signaling,[11,13,69] it is important to consider the dependence of this inward signaling on the integrity of the underlying vesicular transport and fusion machineries. Perhaps, defects in the retrograde
SIV
-F
Macaque
SHIV
-D
p115Giantin
SIV
-FSH
IV -D
a
b
DAPI
Figure 10: Increased accumulation of the Golgi matrix proteins/tethers, giantin and p115, in cellular elements in pulmonary arterial vasculopathies in the chimeric SHIV-infected macaque model. (a) Representative images of respective vasculopathies probed for giantin or p115 compared to representative controls. Scale bar=85 μm. (b) Representative higher magnifi cation images of giantin and p115 immunostaining from analyses as in Figure 10a. Scale bar=10 μm. The SIV-F, p115 segment in the upper right is the same as in Figure 9, SIV-F at the top of the middle column. (Adapted from ref. 2.)
2
4
6
8
10
12
14
16
18
Int.
pixe
l int
ensi
ty/c
ell (
A.U
.)
n 18 90 46 31 140 25 199
F G H A B C DSHIVCtrl
PAECs: p115
SHIVCtrl **
**
** **
E
27
SIV SIV SIV
Uni
nfec
ted
Macaque
Figure 11: Quantitative immunomorphometry data for the Golgi tether, p115, in PAECs in SHIV-nef–infected macaques. Integrated pixel intensity/cell was computed using Image J software by outlining individual cells within immunofl uorescence images corresponding to luminal endothelium (PAEC) in sections from each of the control/SIV- and SHIV-infected macaques (n=4 in each group) and was expressed in arbitrary units (A.U.) (mean±SE; n is number of cells quantitated). PAECs in group Ctrl-E had little or no detectable p115. Post-hoc between-group comparisons were carried out using the Tukey–Kramer Multiple Comparison test with an alpha setting of 0.05 (NCSS 2007). Double asterisks indicate that the particular group was different from all control/SIV groups. (Adapted from ref. 2.)
membrane-associated trafficking pathways might explain defects in BMP/Smad signaling in IPAH despite a wt BMPR II. The reduced expression of eNOS antigen in arterial endothelium in lungs of BMPR II mutant transgenic mice subjected to hypoxia[85] suggests a multifactorial pathophysiology. As this review makes clear, reduced NO bioavailability, hypoxia and mutations in BMPR II all affect intracellular trafficking pathways.
Estradiol and trans-Golgi traffickingThere is a gender bias in the development of IPAH with the female to male ratio recently quoted as 1.64–3.88:1.[83] Familial PAH due to mutations in BMPR II also appears to have an earlier onset in women.[17-20,82] However, it has been long known that in the case of the MCT/rat model, the situation is the opposite – estradiol-17β and related compounds inhibit the development of PAH.[86,87] In this context, it is worth noting the studies of Greenfield et al.[88] who investigated the mechanisms by which estrogen therapy reduced the risk of Alzheimer’s disease in post-menopausal women, β-amyloid burden in animal models of Alzheimer’s disease, and secretion of β-amyloid peptides by neuronal cells. These investigators observed that estradiol-17β stimulates trans-Golgi network (TGN) biogenesis including increased TGN phospholipids levels, recruitment of soluble Rab 11 to the TGN and regulating traffic within the late secretory pathway.[88]
Sehgal and Lee: Protein traffi cking dysfunctions in PAH

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 30
Giantin/DAPI Nef/DAPI Merge
f
a
b
b
a
Giantin Nef Merge
a
b
SHIV
-A
Hig
h m
ag
Figure 12: HIV-nef–positive vascular cell elements have increased giantin. (a) Lung sections from a SHIV-nef–infected macaque with increased giantin in the obliterative vascular lesion probed for HIV-nef and giantin. Scale bar=25 μm. (b) Higher magnifi cation images of the insets depicted in Figure 12a. Scale bar=4 μm. Respective 3D intracellular immunoimaging is in ref. 75. (Adapted from ref. 2.)
Earlier, Hendrix et al.[89] reported the effects of estrogens and progestins and their antagonists in modulating the intracellular trafficking of integral membrane proteins. We have recently discovered two specific estrogen-binding proteins in the Golgi apparatus of human PAECs and PASMCs that await further characterization(Lee JE, Sehgal PB, unpublished data). There is thus a growing nexus of data pointing to the ability of estrogens in regulating intracellular trafficking, in particular, through the Golgi. The ability of estrogens to regulate intracellular trafficking remains unexplored in the context of PAH.
A LOOK AHEAD
We have been struck by the presence of almost all of our current ideas already extant in the PAH and related literature extending back over the last four decades. The EM data of Heath and colleagues,[26-28] and others clearly pointed to defects in intracellular trafficking in cells in pulmonary vascular lesions in IPAH. From our perspective, we have added a vocabulary long established in cell biology
in terms of the molecules and machineries that mediate and regulate intracellular trafficking and targeted vesicular transport to consideration of role(s) in the pathogenesis PAH. In doing so, our focus remains on the subcellular mechanisms at the level of cytoplasmic organelles and trafficking, which might contribute to the net consequence of vascular remodeling observed in PAH. We clearly envisage such contributions to be at multiple levels in terms of anterograde and retrograde trafficking and in the regulation of cell motility and cell mitosis. Consequences of such dysfunctions would be widespread changes in the cell surface texture and landscape of the affected cells, leading to global changes in cell surface receptors, cell surface ligands, signaling pathways, the unusual secretory phenotype, prothrombogenicity and lumen closure [Figure 2]. A separate major line of research with a focus on subcellular organellar biology not addressed in the present review involves the role of mitochondria in pulmonary vascular remodeling.[90] Elucidating how each of these changes fits into the multifactorial context of hypoxia, reduced NO bioavailability, mutations in BMPR II, modulation of disease penetrance and gender
Sehgal and Lee: Protein traffi cking dysfunctions in PAH

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 31
effects in disease occurrence in the pathogenesis of PAH is part of the road ahead.
REFERENCES
1. Stenmark KR, Meyrick B, Galie N, Mooi WJ, McMurtry IF. Animal models of pulmonary arterial hypertension: The hope for etiological discovery and pharmacological cure. Am J Physiol Lung Cell Mol Physiol 2009;297:L1013-32.
2. Sehgal PB, Mukhopadhyay S, Patel K, Xu F, Almodóvar S, Tuder RM, et al. Golgi dysfunction is a common feature in idiopathic human pulmonary hypertension and vascular lesions in SHIV-nef-infected macaques. Am J Physiol Lung Cell Mol Physiol 2009;297:L729-37.
3. Mathew R, Huang J, Shah M, Patel K, Gewitz M, Sehgal PB. Disruption of endothelial-cell caveolin-1alpha/raft scaff olding during development of monocrotaline-induced pulmonary hypertension. Circulation 2004;110:1499-506.
4. Zhao YY, Lui Y, Stan RV, Fan L, Gu Y, Dalton N, et al. Defects in caveolin-1 cause dilated cardiomyopathy and pulmonary hypertension in knockout mice. Proc Natl Acad Sci U S A 2002;99:11375-80.
5. Zhao YY, Zhao YD, Mirza MK, Huang JH, Potula HH, Vogel SM, et al. Persistent eNOS activation secondary to caveolin-1 defi ciency induces pulmonary hypertension in mice and humans through PKG nitration. J Clin Invest 2009;119:2009-18.
6. Achcar RO, Demura Y, Rai PR, Taraseviciene-Stewart L, Kasper M, Voelkel NF, et al. Loss of caveolin and heme oxygenase expression in severe pulmonary hypertension. Chest 2006;129:696-705.
7. Sehgal PB, Mukhopadhyay S. Pulmonary arterial hypertension: A disease of tethers, SNAREs, and SNAPs. Am J Physiol Heart Circ Physiol 2007;293:H77-85.
8. Sehgal PB, Mukhopadhyay S. Dysfunctional intracellular traffi cking in the pathobiology of pulmonary arterial hypertension. Am J Respir Cell Mol Biol 2007;37:31-7.
9. Bonifacino JS, Glick BS. The mechanisms of vesicle budding and fusion. Cell 2004;116:153-66.
10. Jahn R, Scheller RH. SNAREs—engines for membrane fusion. Nat Rev Mol Cell Biol 2006;7:631-43.
11. Di Guglielmo GM, Le Roy C, Goodfellow AF, Wrana JL. Distinct endocytic pathways regulate TGF-beta receptor signaling and turnover. Nat Cell Biol 2003;5:410-21.
12. Sehgal PB, Guo GG, Shah M, Kumar V, Patel K. Cytokine signaling: STATs in plasma membrane raft s. J Biol Chem 2002;277:12067-74.
13. Shah M, Patel K, Mukhopadhyay S, Xu F, Guo G, Sehgal PB. Membrane-associated STAT3 and PY-STAT3 in the cytoplasm. J Biol Chem 2006;281:7302-8.
14. Xu F, Mukhopadhyay S, Sehgal PB. Live cell imaging of interleukin-6-induced targeting of the “transcription factor” STAT3 to sequestering endosomes in the cytoplasm. Am J Physiol Cell Physiol 2007;293:C1374-82.
15. Mukhopadhyay S, Shah M, Xu F, Patel K, Tuder RM, Sehgal PB. Cytoplasmic provenance of STAT3 and PY-STAT3 in the endolysosomal compartments in pulmonary arterial endothelial and smooth muscle cells: Implication in pulmonary arterial hypertension. Am J Physiol Lung Cell Mol Physiol 2007;294:L449-68.
16. Le Borgne R. Regulation of Notch signaling by endocytosis and endosomal sorting. Curr Opin Cell Biol 2006;18:213-22.
17. Tuder RM, Marecki JC, Richter A, Fij lkowska I, Flores S. Pathology of pulmonary hypertension. Clin Chest Med 2007;28:23-42.
18. Rabinovitch M. Molecular pathogenesis of pulmonary hypertension. J Clin Invest 2008;118:2372-9.
19. Runo JR, Loyd JE. Primary pulmonary hypertension. Lancet 2003;361:1533-44.
20. Morrell NW. Role of bone morphogenetic protein receptors in the development of pulmonary hypertension. Adv Exp Med Biol 2010;661:251-64.
21. Resta TC, Gonzales RJ, Dail WG, Sanders TC, Walker BR. Selective upregulation of arterial endothelial nitric oxide synthase in pulmonary hypertension. Am J Physiol Heart Circ Physiol 1997;41:H806-13.
22. Cajal SR. Algunas variaciones fi silógicas y patalógicas del aparato reticular de Golgi. Trab Del Lab De Inv Biol Madrid 1914;12:127-227.
23. Jaenke RS, Alexander AF. Fine structural alterations of bovine peripheral pulmonary arteries in hypoxia-induced hypertension. Am J Pathol
1973;73:377-98. 24. Meyrick B, Reid L. The eff ect of continued hypoxia on rat pulmonary
arterial circulation. An ultrastructural study. Lab Invest 1978;38:188-200. 25. Meyrick B, Reid L. Hypoxia-induced structural changes in the media and
adventitia of the rat hilar pulmonary artery and their regression. Am J Pathol 1980;100:151-78.
26. Smith P, Heath D. Electron microscopy of the plexiform lesion. Thorax 1979;34:177-86.
27. Heath D, Smith P, Gosney J, Mulcahy D, Fox K, Yacoub M, et al. The pathology of the early and late stages of primary pulmonary hypertension. Br Heart J 1987;58:204-13.
28. Smith P, Heath D, Yacoub M, Madden B, Caslin A, Gosney J. The ultrastructure of plexogenic pulmonary arteriopathy. J Pathol 1990;160:111-21.
29. King AP, Smith P, Heath D. Ultrastructure of rat pulmonary arterioles aft er neonatal exposure to hypoxia and subsequent relief and treatment with monocrotaline. J Pathol 1995;177:71-81.
30. Mett e SA, Palevsky HI, Pietra GG, Williams TM, Bruder E, Prestipino AJ, et al. Primary pulmonary hypertension in association with human immunodefi ciency virus infection. A possible viral etiology for some forms of hypertensive pulmonary arteriopathy. Am Rev Respir Dis 1992;145:1196-200.
31. Harns PN, Anderson RC, Chen KK. The action of senecionine, integerrimine, jacobine, longilobine and spartiodine, especially on the liver. J Pharmacol Exp Ther 1942;69:69-77.
32. Harns PN, Anderson RC, Chen KK. The action of monocrotaline and retronecine. J Pharmacol Exp Ther 1942;75:78-82.
33. Bull LB. The histological evidence of liver damage from pyrrolizidene alkaloids: Megalocytosis of the liver cells and inclusion globules. Aust Vet J 1955;31:33-40.
34. Merkow L, Kleinerman J. An electron microscopic study of pulmonary vasculitis induced by monocrotaline. Lab Invest 1966;15:547-64.
35. Afzelius BA, Schoental R. The ultrastructure of the enlarged hepatocyes induced in rats with a single oral dose of retrorsine, a pyrrolozidine (Senecio) alkaloid. J Ultrastruct Res 1967;20:328-45.
36. Todorovich-Hunter L, Johnson DJ, Ranger P, Keeley FW, Rabinovitch M. Altered elastin and collagen synthesis associated with progressive pulmonary hypertension induced by monocrotaline. A biochemical and ultrastructural study. Lab Invest 1988;58:184-95.
37. Rosenberg HC, Rabinovitch M. Endothelial injury and vascular reactivity in monocrotaline pulmonary hypertension. Am J Physiol 1988;255:H1484-91.
38. Sugita T, Stenmark KR, Wagner WW Jr, Henson PM, Henson JE, Hyers TM, et al. Abnormal alveolar cells in monocrotaline induced pulmonary hypertension. Exp Lung Res 1983;5:201-15.
39. Wilson DW, Segall HJ. Changes in type II cell populations in monocrotaline pneumotoxicity. Am. J. Pathol. 1990; 136:1293-1299.
40. Reindel JF, Roth RA. The eff ects of moncrotaline pyrrole on cultured bovine pulmonary artery endothelial smooth muscle cells. Am J Pathol 1991;138:707-19.
41. Lamé MW, Jones AD, Wilson DW, Dunston SK, Segall HJ. Protein targets of monocrotaline pyrrole in pulmonary artery endothelial cells. J Biol Chem 2000;275:29091-9.
42. Lamé MW, Jones AD, Wilson DW, Segall HJ. Monocrotaline pyrrole targets proteins with and without cysteine residues in the cytosol and membranes of human pulmonary artery endothelial cells. Proteomics 2005;5:4398-413.
43. Lane KB, Machado RD, Pauciulo MW, Thomson JR, Phillips JA 3rd, Loyd JE, et al. Heterozygous germline mutations in BMPR2, encoding a TGF-β receptor, cause familial primary pulmonary hypertension. Nat Genet 2000;26:81-4.
44. Nishihara A, Watabe T, Imamura T, Miyazono K. Functional heterogeneity of bone morphogenetic protein receptor-II mutants found in patients with primary pulmonary hypertension. Mol Biol Cell 2002;13:3055-63.
45. Rudarakanchana N, Flanagan JA, Chen H, Upton PD, Machado R, Patel D, et al. Functional analysis of bone morphogenetic protein type II receptor mutations underlying primary pulmonary hypertension. Hum Mol Genet 2002;11:1517-25.
46. Hong KH, Lee YJ, Lee E, Park SO, Han C, Beppu H, et al. Genetic ablation of the BMPR2 gene in pulmonary endothelium is suffi cient to predispose to pulmonary arterial hypertension. Circulation 2008;118:722-30.
47. West J. Cross talk between Smad, MAPK, and actin in the etiology of pulmonary arterial hypertension. Adv Exp Med Biol 2010;661:265-78.
48. Razani B, Wang XB, Engelman JA, Batt ista M, Lagaud G, Zhang XL, et al. Caveolin-2-defi cient mice show evidence of severe pulmonary dysfunction
Sehgal and Lee: Protein traffi cking dysfunctions in PAH

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 32
without the disruption of caveolae. Mol Cell Biol 2002;22:2329-44. 49. Jasmin JF, Mercier I, Hnasko R, Cheung MW, Tanowitz HB, Dupuis J,
et al. Lung remodeling and pulmonary hypertension aft er myocardial infarction: Pathogenic role of reduced caveolin expression. Cardiovasc Res 2004;63:747-55.
50. Jasmin JF, Mercier I, Dupuis J, Tanowitz HB, Lisante MP. Short-term administration of a cell-permeable caveolin-1 peptide prevents the development of monocrotaline¬induced pulmonary hypertension and right ventricular hypertrophy. Circulation 2006;114:912-20.
51. Marecki JC, Cool CD, Parr JE, Beckley VE, Luciw PA, Tarantal AF, et al. HIV-1 Nef is associated with complex pulmonary vascular lesions in SHIV-nef-infected macaques. Am J Respir Crit Care Med 2006;174:437-45.
52. Chaudhri R, Lindwasser OW, Smith WJ, Hurley JH, Bonifacino JS. CD4 downregulation by HIV-1 Nef is dependent on clathrin and involves a direct interaction of Nef with AP2 clathrin adaptor. J Virol 2007;81:3877-90.
53. Collett e Y, Aroid S, Picard C, Janvier K, Benichou S, Benarous R, et al. HIV-2 and SIV nef proteins target diff erent src family SH3 domains than does HIV-1 Nef because of a triple amino acid substitution. J Biol Chem 2000;275:4171-6.
54. Hiyoshi M, Suzu S, Yoshidomi Y, Hassan R, Harada H, Sakashita N, et al. Interaction between Hck and HIV-1 Nef negatively regulates cell surface expression of M-CSF receptor. Blood 2008;111:243-50.
55. Roeth JF, Williams M, Kasper MR, Filzen TM, Collins KL. HIV-1 Nef disrupts MHC-1 traffi cking by recruiting AP-1 to the MHC-1 cytoplasmic tail. J Cell Biol 2004;167:903-13.
56. Shah M, Patel K, Fried VA, Sehgal PB. Interactions of STAT3 with caveolin-1 and heat shock protein 90 in plasma membrane raft and cytosolic complexes. Preservation of cytokine signaling during fever. J Biol Chem 2002;277:45662-9.
57. Nishimura T, Faul JL, Berry GJ, Vaszar LT, Qui D, Pearl RG, et al. Simvastatin att enuates smooth muscle neointimal proliferation and pulmonary hypertension in rats. Am J Respir Crit Care Med 2002;166:1403-8.
58. Nishimura T, Vaszar LT, Faul JL, Zhao G, Berry GJ, Shi L, et al. Simvastatin rescues rats from fatal pulmonary hypertension by inducing apoptosis of neointimal smooth muscle cells. Circulation 2003;108:1640-5.
59. Shah M, Patel K, Sehgal PB. Monocrotaline pyrrole-induced endothelial cell megalocytosis involves a Golgi blockade mechanism. Am J Physiol Cell Physiol 2005;288:C850-62.
60. Mukhopadhyay S, Sehgal PB. Discordant regulatory changes in monocrotaline ¬induced megalocytosis of lung arterial endothelial and alveolar epithelial cells. Am J Physiol Lung Cell Mol Physiol 2006;290:L1216-26.
61. Mukhopadhyay S, Shah M, Patel K, Sehgal PB. Monocrotaline pyrrole-induced megalocytosis of lung and breast epithelial cells: Disruption of plasma membrane and Golgi dynamics and an enhanced unfolded protein response. Toxicol Appl Pharmacol 2006;211:209-20.
62. Sehgal PB, Mukhopadhyay S, Xu F, Patel K, Shah M. Dysfunction of Golgi tethers, SNAREs, and SNAPs in monocrotaline-induced pulmonary hypertension. Am J Physiol Lung Cell Mol Physiol 2007;290:L1526-42.
63. Mukhopadhyay S, Xu F, Sehgal PB. Aberrant cytoplasmic sequestration of eNOS in endothelial cells aft er monocrotaline, hypoxia, and senescence: Live-cell caveolar and cyotplasmic NO imaging. Am J Physiol Heart Circ Physiol 2007;292:H1373-89.
64. Mukhopadhyay S, Lee J, Sehgal PB. Depletion of the ATPase NSF from Golgi membranes with hypo-S-nitrosylation of vasorelevant proteins in endothelial cells exposed to monocrotaline pyrrole. Am J Physiol Heart Circ Physiol 2008;295:H1943-55.
65. Ramos M, Lame MW, Segall HJ, Wilson DW. The BMP type II receptor is located in lipid raft s, including caveolae, of pulmonary endothelium in vivo and in vitro. Vasc Pharmacol 2006;44:50-9.
66. Wertz JW, Bauer PM. Caveolin-1 regulates BMPR II localization and signaling in vascular smooth muscle cells. Biochem Biophys Res Commun 2008;375:557-61.
67. Ramos M, Lame MW, Segall HJ, Wilson DW. Monocrotaline pyrrole induces Smad nuclear accumulation and altered signaling expression in human pulmonary arterial endothelial cells. Vasc Pharmacol 2007;46:439-48.
68. Ramos MF, Lame MW, Segall HJ, Wilson DW. Smad signaling in the rat model of monocrotaline pulmonary hypertension. Toxicol Pathol 2008;36:311-20.
69. Sehgal PB. Paradigm shift s in the cell biology of STAT signaling. Semin Cell Dev Biol 2008;19:329-40.
70. Patel HH, Zhang S, Murray F, Suda RY, Head BP, Yokoyama U, et al.
Increased smooth muscle cell expression of caveolin-1 and caveolae contribute to the pathophysiology of idiopathic pulmonary arterial hypertension. FASEB J 2007;21:2970-9.
71. Maximov A, Tang J, Yang X, Pang ZP, Sudhof TC. Complexin controls the force transfer from SNARE complexes to membranes in fusion. Science 2009;323:516-21.
72. Giraudo CG, Garcia-Diaz A, Eng WS, Chen Y, Hendrickson WA, Melia TJ, et al. Alternative zippering as an on-off switch for SNARE-mediated fusion. Science 2009;323:512-6.
73. Matsushita K, Morrell CN, Cambein B, Yang SX, Yamakuchi M, Bao C, et al. Nitric oxide regulates exocytosis by S-nitrosylation of N-ethlymaleimide sensitive factor. Cell 2003;115:139-50.
74. Lee J, Reich R, Xu F, Sehgal PB. Golgi, traffi cking, and mitotis dysfunctions in pulmonary arterial endothelial cells exposed to monocrotaline pyrrole and NO scavenging. Am J Physiol Lung Cell Mol Physiol 2009;297:715-28.
75. Lee JE, Patel K, Almodovar S, Tuder RM, Flores SC, Dehgal PB. Dependence of Golgi apparatus on nitiric oxide in vascular cells; implications in pulmonary artirial hypertension. Am J Physiol Heart Circ Physiol 2011 [In Press].
76. Zuckerbraun BS, Shiva S, Ifedigbo E, Mathier MA, Mollen KP, Rao J, et al. Nitrite potently inhibits hypoxic and infl ammatory pulmonary arterial hypertension and smooth muscle proliferation via xanthine oxidoreductase-dependent nitric oxide generation. Circulation 2010;121:98-109.
77. Orialo AV, Bhaumik D, Gengler BK, Scott GK, Campisi J. Cell surface-bound IL 1alpha is an upstream regulator of the senescence-associated IL-6/IL-8 cytokine network. Proc Natl Acad Sci U S A 2009;106:17031-6.
78. Rodier F, Coppé JP, Patil CK, Hoeij makers WA, Muñoz DP, Raza SR, et al. Persistent DNA damage signalling triggers senescence-associated infl ammatory cytokine secretion. Nat Cell Biol 2009;11:973-9.
79. Almodovar S, Cicalini S, Petrosillo N, Flores SC. Pulmonary hypertension associated with HIV infection: Pulmonary vascular disease: The global perspective. Chest 2010;137:6S-12S.
80. Duff y P, Wang X, Lin PH, Yao Q, Chen C. HIV Nef protein causes endothelial dysfunction in porcine pulmonary arteries and human pulmonary artery endothelial cells. J Surg Res 2009;156:257-64.
81. Yang X, Long Lu, Southwood M, Rudarakanchana N, Upton PD, Jeff ery TK, et al. Dysfunctional Smad signaling contributes to abnormal smooth muscle cell proliferation in familial pulmonary arterial hypertension. Circ Res 2005;96:1053-63.
82. Sobolewski A, Rudarakanchana N, Upton PD, Yang J, Crilley TK, Trembath RC, et al. Failure of bone morphogenetic protein receptor traffi cking in pulmonary arterial hypertension: Potential for rescue. Hum Mol Genet 2008;17:3180-90.
83. Sakao S, Tanabe N, Tatsumi K. The estrogen paradox in pulmonary arterial hypertension. Am J Physiol Lung Cell Mol Physiol 2010;299:L435-8.
84. Atkinson C, Stewart S, Upton PD, Machado R, Thomson JR, Trembath RC, et al. Primary pulmonary hypertension is associated with reduced pulmonary vascular expression of type II bone morphogenetic protein receptor. Circulation 2002;105:1672-8.
85. Frank DB, Lowery J, Anderson L, Brink M, Reese J, de Caestecker M. Increased susceptibility to hypoxic pulmonary hypertension in Bmpr2 mutant mice is associated with endothelial dysfunction in the pulmonary vasculature. Am J Physiol Lung Cell Mol Physiol 2008;294:L98-109.
86. Farhat MY, Chen MF, Bhatt i T, Iqbal A, Cathapermal S, Ramwell PW. Protection by oestradiol against the development of cardiovascular changes associated with monocrotaline pulmonary hypertension in rats. Br J Pharmacol 1993;110:719-23.
87. Tofovic SP, Zhang X, Jackson EK, Dacic S, Petrusevska G. 2-methoxyestradiol mediates the protective eff ects of estradiol in monocrotaline-induced pulmonary hypertension. Vascul Pharmacol 2006;45:358-67.
88. Greenfi eld JP, Leung LW, Cai D, Kaasik K, Gross RS, Rodriguez-Boulan E, et al. Estrogen lowers Alzheimer beta-amyloid generation by stimulating trans-Golgi network vesicle biogenesis. J Biol Chem 2002;277:12128-36.
89. Hendrix EM, Myatt L, Sellers S, Russell PT, Larsen WJ. Steroid hormone regulation of rat myometrial gap junction formation: Eff ects on cx43 levels and traffi cking. Biol Reprod 1995;52:547-60.
90. Dromparis P, Sutendra G, Michelakis ED. The role of mitochondria in pulmonary vascular remodeling. J Mol Med 2010;88:1003-10.
Source of Support: NIH R01 HL-087176 and F31 HL-107013, Confl ict of Interest: None.
Sehgal and Lee: Protein traffi cking dysfunctions in PAH

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 33
INTRODUCTION
Pulmonary hypertension (PH) is a rare and progressive disorder with a prevalence of 15 cases per million.[1] The hemodynamic definition of PH requires elevation of the mean pulmonary artery pressure >25 mm Hg at rest or 30 mm Hg with exercise and a mean pulmonary-capillary wedge pressure or left ventricular end-diastolic pressure ≤15 mm Hg. The World Health Organization (WHO) now classifies PH into five groups with similar disease mechanisms, histopathologic features and responses to treatment.[2] Current concepts suggest that PH pathogenesis involves three primary processes: vasoconstriction, cellular proliferation/vascular remodeling, and thrombosis.[3] Evolving evidence
Is peroxisome proliferator-activated receptor gamma (PPAR) a therapeutic target for the
treatment of pulmonary hypertension?David E. Green1, Roy L. Sutliff 1 , C. Michael Hart1
1Department of Medicine, Emory University, Atlanta Veterans Affairs Medical Center, Decatur, Georgia, USA
ABSTRACT
Pulmonary hypertension (PH), a progressive disorder associated with signifi cant morbidity and mortality, is caused by complex pathways that culminate in structural and functional alterations of the pulmonary circulation and increases in pulmonary vascular resistance and pressure. Diverse genetic, pathological, or environmental triggers stimulate PH pathogenesis culminating in vasoconstriction, cell proliferation, vascular remodeling, and thrombosis. We conducted a thorough literature review by performing MEDLINE searches via PubMed to identify articles pertaining to PPARγ as a therapeutic target for the treatment of PH. This review examines basic and preclinical studies that explore PPARγ and its ability to regulate PH pathogenesis. Despite the current therapies that target specifi c pathways in PH pathogenesis, including prostacyclin derivatives, endothelin-receptor antagonists, and phosphodiesterase type 5 inhibitors, morbidity and mortality related to PH remain unacceptably high, indicating the need for novel therapeutic approaches. Consequently, therapeutic targets that simultaneously regulate multiple pathways involved in PH pathogenesis have gained attention. This review focuses on peroxisome proliferator-activated receptor gamma (PPARγ), a member of the nuclear hormone receptor superfamily of ligand-activated transcription factors. While the PPARγ receptor is best known as a master regulator of lipid and glucose metabolism, a growing body of literature demonstrates that activation of PPARγ exerts antiproliferative, antithrombotic, and vasodilatory effects on the vasculature, suggesting its potential effi cacy as a PH therapeutic target.
Key Words: Peroxisome proliferator-activated receptor gamma, pulmonary hypertension, therapy
Review Ar t ic le
suggests that peroxisome proliferator-activated receptor gamma (PPARγ), a member of the nuclear hormone receptor superfamily of ligand-activated transcription factors, can favorably modulate cellular proliferation, vascular tone and coagulation. This review provides an overview of PPARγ and considers how PPARγ impacts these primary processes involved in PH pathogenesis.
A thorough literature review was conducted to identify articles pertaining to PPAR as a therapeutic target for the treatment of PH. We performed MEDLINE searches through PubMed in the National Library of Medicine to identify relevant articles. Articles accepted for review
Access this article online
Quick Response Code:Website: www.pulmonarycirculation.org
DOI: 10.4103/2045-8932.78101
Pulm Circ 2011;1:33-47
Address correspondence to:Dr. C. Michael HartAtlanta VA Medical Center (151),1670 Clairmont Road,Decatur, Georgia 30033, USAE-mail: [email protected]

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 34
included full text journal articles, clinical trials, reviews, guidelines, and randomized controlled trials. Articles not accepted for review included letters, editorials and correspondence, and manuscripts published before 1985.
PPAR AND PH
Overview of PPAR biologyPeroxisome proliferator-activated receptors (PPARs) belong to subfamily 1 of the nuclear hormone receptor superfamily (Nuclear Receptors Nomenclature Committee, 1999). There are three distinct isotypes of PPARs (α, β/δ, and γ) that are expressed throughout the body and possess similar structural and functional features. PPARs are responsive to the lipid status of the cell and act as ligand-activated transcription factors. PPAR isotypes are distinguished by their tissue distribution, ligand specificity and target genes. PPARα is most highly expressed in tissues with high catabolic rates such as the liver, kidney, heart, brown adipose tissue, and the intestine.[4,5] PPARβ/δ has the broadest expression pattern with the expression in many cases dependent on the degree of cell proliferation and differentiation.[4,6,7] PPARγ exists as two isoforms that differ in their N terminus. PPARγ2 is found in adipose and PPARγ1 is more widely expressed in tissues such as the brain, vascular tissues, small intestine, and lymphatic tissues.[4,8] Each PPAR isotype is preferentially activated by a wide range of naturally occurring or metabolized lipids derived from the diet or from intracellular signaling pathways, which include n-3 and n-6 family polyunsaturated fatty acids (PUFAs) and eicosanoid products of cyclooxygenase and lipoxygenase.
As illustrated in Figure 1, transcriptional regulation by PPARs requires the formation of heterodimers with retinoid X receptor (RXR) isotypes. PPARs typically form heterodimers with RXRalpha (RXRα). PPAR:RXR heterodimers bind to DNA at sites composed of the hexameric direct repeat sequence, AGGTCA, separated by a single nucleotide. Gene regulation involves ligand-induced conformational changes in the PPAR receptor which mediate interaction with specific coactivator (e.g. steroid receptor coactivator-1 and p300) and corepressor molecules. Coactivator proteins possess either histone acetyltransferase activity or recruit other proteins with this activity to the transcription start site. Acetylation of histone proteins alters chromatin structure, facilitating the binding of RNA polymerase and the initiation of transcription.[9] PPARγ can also repress gene expression by interfering with the clearance of corepressors from selected promoters.[10] Due to their numerous metabolic and therapeutic actions, PPARs have become pharmacological targets. For example, PPARα agonists
Figure 1: Schematic illustration of PPARγ-mediated gene regulation. PPARγ ligands originating from outside or inside the cell bind to the PPARγ receptor, stimulating formation of a heterodimer with the retinoid X receptor (RXR). The PPARγ–RXR heterodimer binds to PPAR response elements (PPRE) comprising hexameric repeats of the sequence, AGGTCA-X-AGGTCA. This active heterodimer recruits coactivators to and/or derecruits corepressor molecules from the transcriptional start site, leading to increased transcription of selected genes. Activation of PPARγ can also inhibit the expression of genes regulated by specifi c proinfl ammatory transcription factors such as NF-kB, AP-1, and STAT
such as fibrate medications are used in the treatment of dyslipidemia and may have anti-inflammatory effects. PPARβ/δ selective agonists such as GW0742 augment high density lipoprotein (HDL) cholesterol and have been implicated in promoting tissue repair.[9-12] On the other hand, PPARγ agonists such as rosiglitazone and pioglitazone, used to treat type 2 diabetes, have beneficial effects in vascular disease in animal models.[11,12] These reports emphasize that ligands for PPAR receptors can exert diverse biological effects in numerous organs and tissues. Among these PPAR receptors, PPARγ is of particular interest in the pulmonary circulation.
The role of altered PPAR expression in PHPPARγ is abundantly expressed in many cell types in the lung, including those of the pulmonary vascular wall such as endothelial and smooth muscle cells. Several studies indicate that expression of PPARγ is reduced by conditions associated with PH. Ameshima and colleagues were the first to demonstrate that compared to normal or chronic obstructive pulmonary disease (COPD) patients, patients with PH had significantly reduced or absent expression of PPARγ in precapillary arteriolar plexiform lesions.[13] PPARγ expression was markedly reduced in endothelial cells isolated from PH patients when compared to normal patients (unpublished observation). These clinical findings have also been corroborated using in vivo experimental models of PH. For example, PPARγ expression was reduced in pulmonary vascular lesions in the rat model of hypoxia-induced PH.[13,14] Similarly, using in vitro cell culture models, increased shear
Green, et al.: PPAR and pulmonary hypertension

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 35
stress or hypoxia was demonstrated to directly alter PPARγ expression. Exposure of ECV304 endothelial cells to increased fluid shear stress decreased PPARγ expression.[13] Similarly, exposure of endothelial cells to 1% hypoxia decreased expression of PPARγ.[15] Collectively, these findings suggest that PPARγ expression is reduced in PH and that cells exposed to conditions that promote PH have decreased PPARγ expression. These reductions in PPARγ could contribute to an abnormal, proliferative, and apoptosis-resistant endothelial cell phenotype.
To further examine the role of PPARγ in pulmonary vascular biology, more recent studies have employed PPARγ knockout mice. Because global deletion of PPARγ results in embryonic lethality,[16] investigators have examined experimental animals with tissue-targeted deletion of PPARγ. For example, Guignabert and co-workers reported that targeted deletion of PPARγ in the vascular endothelium of mice (ePPARγ-/-) results in spontaneous PH with right ventricular hypertrophy and muscularization of small distal pulmonary arteries.[17] The ePPARγ-/- mice exposed to chronic hypoxia (10% O2) for 3 weeks developed a similar degree of PH as wild-type control mice. However, following cessation of hypoxia, PH persisted longer in the ePPARγ-/- mice compared to wild-type mice exposed to hypoxia, suggesting that reduced endothelial PPARγ signaling is sufficient to cause mild PH and impair recovery from chronic hypoxia exposure.[17] Targeted deletion of PPARγ from smooth muscle (smPPARγ-/-) also resulted in spontaneous PH in mice.[18] Microarray analysis of bovine pulmonary artery endothelial cells following treatment with a PPARγ antagonist revealed alterations in the expression of numerous genes including those that might stimulate cell cycle progression and proliferation.[19] Taken together, these reports suggest that loss of PPARγ function in pulmonary vascular wall cells stimulates PH pathogenesis.
PPAR activation ameliorates experimental PHMounting experimental evidence indicates that PPARγ stimulation ameliorates PH development in animal models of PH. Monocrotaline (MCT)-induced PH and vascular remodeling in the rat were attenuated by treatment with the PPARγ ligands, pioglitazone or troglitazone.[20] Interestingly, PPARγ ligands also inhibited MCT-induced vascular wall thickening and staining for proliferating cell nuclear antigen, suggesting that PPARγ ligands suppressed cell proliferation and vascular remodeling.[20] In Wistar-Kyoto rats exposed to continuous hypobaric hypoxia for 3 weeks, treatment with rosiglitazone attenuated hypoxia-induced right ventricular hypertrophy and vascular smooth muscle cell (VSMC) proliferation, as well as pulmonary vascular collagen and elastin deposition, infiltration of c-Kit–positive cells into the adventitia, and matrix metalloproteinase-2 (MMP-2) activity. In this
study, rosiglitazone failed to attenuate hypoxia-induced increases in pulmonary artery pressure, an observation attributed to the inability of PPARγ ligands to modulate Rho kinase signaling, a critical mediator of pulmonary vasoconstriction.[21] Hansmann and colleagues reported that ApoE knockout mice fed high fat diets developed significant increases in right ventricular systolic pressure, pulmonary vascular remodeling and right ventricular hypertrophy and that administration of PPARγ ligands in this model attenuated PH.[22] An elegant series of experiments in this model provided evidence that PPARγ ligands attenuated PH by inhibiting platelet derived growth factor (PDGF) signaling.
Male C57Bl/6 mice exposed to chronic hypoxia (10% O2) for 3 weeks developed PH that was attenuated by treatment with the PPARγ agonist, rosiglitazone (10 mg/kg/day by gavage) during the final 10 days of hypoxia exposure.[15] Rosiglitazone treatment also reduced hypoxia-induced right ventricular hypertrophy and muscularization of small pulmonary arterioles. From a therapeutic perspective, this study also demonstrated that rosiglitazone could reverse the established PH by introducing rosiglitazone treatment only after animals developed PH.[15] The mechanisms of these therapeutic effects were attributed to PPARγ-mediated reductions in Nox4 expression, oxidative stress, and PDGF signaling in the lung. Collectively, these reports indicate that PPARγ ligands attenuated pulmonary vascular remodeling and hypertension caused by a variety of stimuli in experimental models. The effect of alterations in PPARγ expression and activation on PH in various experimental models is summarized in Table 1. These studies have begun to identify specific pathways modulated by PPARγ in the pathogenesis of PH. Additional evidence, reviewed below, suggests that PPARγ has the potential to regulate a diverse spectrum of pathways and mediators implicated in PH. The ensuing section will consider how targeting PPARγ can potentially modulate additional pathways fundamental to the pathogenesis of PH.
ASPECTS OF PH PATHOGENESIS THAT ARE POTENTIALLY REGULATED BY PPAR
Vascular tone in PHCommon mechanisms in the pathogenesis of PH are endothelial dysfunction, reduced endothelial production of vasodilators, and increased production of vasoconstrictors leading to vasoconstriction and increased pulmonary vascular resistance. Recent advances in PH therapeutics have sought to promote vascular function by restoring vasodilator levels. For example, circulating levels of the
Green, et al.: PPAR and pulmonary hypertension

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 36
vasodilator, prostacyclin, are decreased in PH,[23] and the administration of prostacyclin or its analogues represents a significant advance in PH therapy.[24] Nitric oxide (NO)-mediated vasorelaxation is also impaired in PH.[25] Phosphodiesterase type 5 inhibitors which prolong NO-mediated increases in cGMP are now employed in selected patients with PH.[24] Conversely, levels of vasoconstrictors such as endothelin-1 (ET-1) and thromboxane (TXA2) are increased in PH patients.[26] By blocking these vasoconstrictive effects, both endothelin receptor antagonists and calcium channel blockers comprise additional strategies in the current PH therapeutic armamentarium. In addition to altering vascular tone, these agents may also modulate structural changes in the pulmonary vasculature and vascular remodeling, sequelae of vascular injury and increased intraluminal pressure or flow. While the current therapies target individual mediators or mechanisms in PH pathogenesis, PPARγ may simultaneously modulate several of these pathways involved in PH pathogenesis as described below.
ProstacyclinAs a critical regulator of pulmonary vascular function, the endothelial-derived mediator, prostacyclin, is a potent vasodilator that inhibits platelet aggregation and exerts anti-inflammatory, anti-thrombotic, and anti-proliferative vascular effects.[27] Overexpression of prostacyclin synthase protected mice from chronic hypoxia-induced PH, whereas prostacyclin-receptor deficient mice were sensitized to hypoxia-induced PH.[28] Prostacyclin synthase expression was reduced in the pulmonary arteries of patients with severe PH compared to normal subjects, and the vascular endothelium was found to be the major site of lung vascular prostacyclin synthase expression.[29] In patients with PH, prostacyclin derivatives decreased urinary isoprostane metabolites, an index
of oxidative stress, without altering TXA2.[30] Currently, augmenting prostacyclin levels constitutes a therapeutic strategy in PH, but the precise cellular mechanisms responsible for prostacyclin-mediated benefits remain to be defined. The classical signaling pathway activated by prostacyclin involves binding the G-protein coupled cell surface prostacyclin receptor (IP), which when activated, stimulates adenyl cyclase and increases cellular cAMP content. However, prostacyclin and its analogues can also activate PPAR receptors including PPARδ and PPARγ to mediate biological effects.[31,32] Activation of the PPARγ receptor with thiazolidinedione also reduced systemic vascular production of the potent vasoconstrictor, thromboxane,[33] and attenuated iNOS and Cox-2 upregulation.[34] These reports emphasize that PPARγ can regulate prostanoid production and that additional studies will be required to determine if PPARγ can regulate prostacyclin and its metabolites in the pulmonary circulation.
Nitric oxideIn addition to prostacyclin, NO represents an additional endothelium-derived vasodilator whose bioavailability is reduced in PH.[35,36] Downregulation of the enzyme that produces nitric oxide, endothelial nitric oxide synthase (eNOS), has been described in PH in some studies,[37] whereas others report unchanged or increased levels of the enzyme. (More consistent evidence demonstrates that endothelium-derived, NO-mediated vasodilation is impaired in models of PH.) Thus, it is likely that reductions in NO bioavailability in PH are more closely related to post-translational alterations in eNOS regulation and/or enhanced NO degradation rather than reduced eNOS expression. The critical role of NO bioavailability in PH is supported by the evidence that genetic deletion of eNOS enhanced susceptibility to hypoxia-induced PH,[38]
Table 1: Current evidence linking PPAR and pulmonary hypertensionAuthor Year Ref.
No.Observation
Decreased PPARγ expression is associated with PH
Ameshima 2003 13 PPARγ expression reduced in lung tissue from PH patientsShear stress decreased PPARγ expression in ECV304 cells
Hansmann 2008 18 Targeted smooth muscle PPARγ deletion in mice caused PH
Guignabert 2009 17 Targeted endothelial PPARγ deletion in mice caused PHNisbet 2010 15 Hypoxia decreased PPARγ in HPASMC and HPAECKim 2010 14 Hypoxia decreased lung PPARγ in rat model
PPARγ activation reduced PHMatsuda 2005 19 MCT-induced PH in rats attenuated by PPARγ ligandsCrossno 2007 20 Hypoxia-induced vascular remodeling in rats attenuated by PPARγ ligandsHansmann 2008 22 High fat diet-induced PH in Apo-E defi cient mice attenuated by PPARγ ligands
Nisbet 2010 15 Hypoxia-induced PH and vascular remodeling in mice attenuated by PPARγ ligands
Kim 2010 14 Hypoxia-induced PH in rats attenuated by PPARγ ligands
Green, et al.: PPAR and pulmonary hypertension

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 37
a defect reversed by adenoviral-mediated transfection of the pulmonary vasculature with eNOS.[39] Furthermore, overexpression of eNOS attenuated hypoxia-induced PH.[40] In addition, NO inhalation improves pulmonary hemodynamics and quality of life in a subset of patients with PH,[41] and recent advances in cell-based eNOS gene transfer to the lung have demonstrated that eNOS can reverse the established PH in animal models and facilitate restoration of the pulmonary microvasculature.[42]
NO is produced constitutively in vascular endothelial cells from the amino acid, L-arginine, by the Type III, eNOS isoform. Enzyme activity is largely regulated by intracellular Ca2+, cofactor availability, and eNOS post-translational modifications including phosphorylation and interaction with other proteins such as caveolin and heat shock protein 90 (hsp90).[43] Derangements in eNOS phosphorylation and interactions between eNOS and caveolin have been reported in PH. PPARγ ligands can affect these post-translational pathways.[44,45] PPARγ increased endothelial NO release by reducing the inhibitory interaction between eNOS and caveolin, increasing interactions between eNOS and the molecular chaperone, hsp90, and enhancing phosphorylation of eNOS on serine 1177, all post-translational modifications associated with enhanced eNOS activity.[46,47] PPARγ agonists can increase NO bioavailability by blunting the degradation of inducible nitric oxide synthase (iNOS) and by decreasing serum levels of asymmetric dimethylarginine (ADMA), the endogenous inhibitor of NOS.[48-50]
Once produced, endothelial-derived NO reduces: 1) vascular tone,[51] 2) platelet activation and aggregation,[52] 3) stimulated vascular smooth muscle proliferation,[53] and 4) leukocyte adherence.[54] To exert these biological effects, NO must diffuse into the vascular wall where its activity may be limited by local concentrations of superoxide. Superoxide combines at diffusion-limited rates with NO, forming the potent oxidant, peroxynitrite, thereby reducing the vascular protective effects of NO and enhancing oxidative stress. Peroxynitrite also oxidizes the NOS cofactor, tetrahydrobiopterin.[55] Deficiency of tetrahydrobiopterin alters electron flow through eNOS to molecular oxygen rather than arginine, producing superoxide rather than NO, a condition referred to as eNOS uncoupling. Enhanced superoxide production in the vascular wall may, therefore, reduce NO bioavailability through multiple mechanisms. As a result, NO bioavailability can be regulated not only by the rate of NO formation, but also by the rate of NO degradation. Thus, increased superoxide generation constitutes an important mechanism of NO inactivation and endothelial dysfunction in the vascular wall. Current evidence indicates that PPARγ can stimulate endothelial NO release and simultaneously
reduce superoxide generation in vascular endothelial cells, suggesting that PPARγ ligands could enhance NO bioavailability and the vascular protective effects of NO to favorably modulate vasoconstriction and PH.[46,47]
Endothelin-1The potent vasoconstricting polypeptide, ET-1, has been implicated in PH pathogenesis. ET-1 receptors are upregulated in the lung in both animal models and patients with PH.[25] ET-1, as well as endothelium-derived reactive oxygen species (ROS), attenuated NO-dependent pulmonary vasodilation, following exposure to chronic hypoxia in isolated rat lungs.[56] ET-1–induced pulmonary vasoconstriction was markedly reduced by administration of Cu/Zn superoxide dismutase and was completely attenuated in gp91phox deficient mice.[57] These findings suggest that NADPH oxidase and superoxide play an important role in pulmonary vascular effects of ET-1. ET-1 receptor antagonists have been employed in patients with PH to improve functional status and other indices of PH related morbidity,[56] further suggesting that ET-1 is an important mediator of pulmonary vascular dysregulation. Emerging evidence in several disease states indicates that PPARγ activation attenuates ET-1 signaling. PPAR ligands inhibited ET-1 secretion by vascular endothelial cells in vitro.[57-60] Similarly, in non-diabetic patients with metabolic syndrome, treatment with rosiglitazone reduced several markers of vascular inflammation including plasma levels of ET-1 and improved markers of metabolic control, while lowering blood pressure and improving flow-mediated vasodilation.[61] PPARγ activation also reduced hypertrophy and anti-apoptotic effects caused by ET-1 in cardiac myocytes in vitro through altered nuclear factor of activated T cells (NFAT) signaling. Treatment with PPARγ ligands in several rat models of hypertension reduced ET-1 expression in cardiac and vascular tissues.[62] Collectively, these findings suggest that PPARγ activation can attenuate expression of ET-1 in cardiovascular tissues in response to a variety of stimuli and can attenuate ET-1-mediated signaling in selected models. Potential pathways by which PPARγ regulates vascular tone are illustrated in Figure 2.
Abnormal vascular remodeling, inflammation, and cell proliferation in PHRemodeling of the pulmonary vasculature can reduce its cross-sectional diameter and compliance, increase pulmonary vascular resistance, and contribute to sustained PH. Studies examining the molecular mechanisms underlying pulmonary vascular remodeling have implicated growth factor pathways as well as matrix remodeling in the development and progression of PH.[63] Inflammation also plays a significant role in altered pulmonary vascular function during the development
Green, et al.: PPAR and pulmonary hypertension

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 38
of PH.[64] Inflammatory markers are elevated in PH, and the plexiform lesions that characterize severe PH are surrounded by macrophages, T and B lymphocytes, and dendritic cells.[65] These cells may exacerbate PH by releasing growth factors, ROS and additional cytokines.[66] Chemokines such as CX3CL1, CCL5 and MCP-1 which recruit inflammatory cells are elevated in PH patients.[67-69] Therefore, agents that target the generation of these oxidative and inflammatory stimuli in the pulmonary vascular wall may reduce vascular dysfunction and attenuate the development or progression of PH. Relationships between PPARγ and these complex pathways implicated in PH pathogenesis are illustrated in Figure 3.
NADPH oxidases NADPH oxidases, a major source of superoxide production in the vasculature, have been implicated in PH and contribute to endothelial dysfunction and vascular cell proliferation.[70,71] Originally described in phagocytic cells, the gp91phox-based NADPH oxidase is a multicomponent, membrane-associated, enzyme that catalyzes the one electron reduction of oxygen to superoxide, using NADH or NADPH as the electron donor.[70] The classical phagocytic NADPH oxidase is composed of several components or subunits including the membrane-bound gp91phox (Nox2) and p22phox subunits as well as the cytosolic p47phox and p67phox subunits that, when stimulated, combine with the small G-protein, rac, and translocate to the membrane to activate the enzyme complex. On the other hand, in nonphagocytic cells, the catalytic moiety of NADPH oxidases is composed of one or more Nox2 homologues, Nox 1, 3, 4, 5, Duox1 or Duox2.[72] These Nox homologues associate with the membrane-bound p22phox subunit and are differentially regulated and targeted to distinct subcellular loci, suggesting that these oxidases serve unique roles in cell function. Nox1 and 3 are activated through interactions with rac and the p47phox and p67phox homologues, NOXA1 and NOXO1.
Current evidence indicates that Nox4 expression is increased in hypoxia-induced PH in the mouse and in the pulmonary vasculature of patients with PH.[15,73] Nox4 is highly expressed in vascular wall cells including smooth muscle and endothelial cells where it is constitutively active.[74] Furthermore, hypoxia increased Nox4 expression and pulmonary artery smooth muscle cell (PASMC) proliferation,[73] and Nox4 stimulated the proliferation of endothelial and smooth muscle cells.[75] Hypoxia stimulated Nox4 expression and cell proliferation in the mouse lung in vivo and in human pulmonary artery endothelial cell (HPAEC) and human pulmonary artery smooth muscle cell (HPASMC) in vitro.[15] Treatment with rosiglitazone during the last 10 days of hypoxia exposure reduced Nox4 levels and ROS production and attenuated
hypoxia-induced PH, right ventricular hypertrophy and vascular remodeling. Similarly, rosiglitazone attenuated hypoxia-induced Nox4 expression and proliferation in human PAEC and PASMC in vitro. Taken together, these findings suggest that NADPH oxidases are important mediators of cell proliferation and vasoconstriction in PH that can be regulated by PPARγ [summarized in Figure 4].
Figure 3: Potential pathways by which PPARγ regulates vascular remodeling, cell proliferation and hypertrophy in PH. PPARγ has the potential to regulate a complex variety of pathways that are involved in remodeling of the pulmonary vasculature during the development of PH. Arrowheads at the end of lines denote stimulatory effects, whereas perpendicular lines denote inhibitory effects. *Pathway components that are inhibited by PPARγ, +pathway components that are stimulated by PPARγ. (BMP-2 – Bone morphogenetic protein-2; BMPR-2 – BMP-2 receptor; EPC – endothelial progenitor cell; ET-1 – Endothelin – 1; ET-R – Endothelin-1 receptor; ROS – Reactive oxygen species; TF – Infl ammatory transcription factors (e.g. NF-κB); TGF-β – Transforming growth factor beta; TGFβR - TGF-β receptor)
Green, et al.: PPAR and pulmonary hypertension
Figure 2: Potential pathways by which PPARγ regulates vascular tone. Activation of PPARγ potentially modulates several pathways involved in the regulation of vascular tone. In addition, prostacyclin or its analogues may activate PPARγ. Arrowheads at the end of lines denote stimulatory effects, whereas perpendicular lines denote inhibitory effects. (ADMA – Asymmetric dimethyl arginine; cAMP – Cyclic adenosine nucleotide monophosphate; cGMP – Cyclic guanosine nucleotide monophosphate; eNOS – Endothelial nitric oxide synthase; ET-1 – Endothelin-1; ET-R – Endothelin-1 receptor; NO – Nitric oxide; IP receptor – Prostacyclin receptor)

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 39
Although increases in Nox4 mRNA levels were associated with increased Nox4 activity,[76] detailed understanding of Nox4 transcriptional regulation remains to be established. Nox4 induction has been reported in response to diverse stimuli including hypoxia in kidney and ischemia in brain.[71] In smooth muscle cells, activators of Nox4 transcription include urokinase, plasminogen activator, angiotensin II, transforming growth factor-beta 1 (TGF)-β1, and tumor necrosis factor (TNF)-α.[77] In contrast, in endothelial cells, oscillatory shear stress[78] and PPARγ activation[79] suppressed Nox4 mRNA levels. However, few studies have examined regulatory elements in the Nox4 promoter. Hypoxia stimulated activation of the Nox4 promoter in part through nuclear factor (NF)-κB-mediated signaling and enhanced p65 binding to the Nox4 promoter which increased Nox4 expression and activity.[80] Furthermore, treatment with rosiglitazone inhibited hypoxia-induced Nox4 expression and activity, proliferation, and p65–Nox4 promoter interaction.[80] HIF-1α and the E2F family transcription factors also activated the Nox4 promoter although their regulation by PPARγ at this site has yet to be confirmed.[81] Based on evidence that Nox4 stimulates smooth muscle and endothelial cell proliferation, these findings suggest that activation of PPARγ can attenuate the proliferation of pulmonary vascular wall cells that may participate in the pathogenesis of PH.[82] Coupled with the ability of NADPH oxidases to attenuate NO bioavailability, Nox4, in particular, and NADPH oxidases, in general, may be an important target of PPARγ amelioration of PH.
PDGF signalingPDGF participates in PH pathogenesis. Two genes (A and
B) produce three biologically active forms of PDGF protein (AA, AB, and BB).[83,84] These proteins activate one or more PDGF receptors (αα, αβ, or ββ) to stimulate cell migration and survival. Ligand binding promotes PDGF receptor tyrosine autophosphorylation and subsequent activation of several downstream signaling pathways including Src, phosphatidylinositol 3 kinase (PI3K), phospholipase Cγ, and Ras. These signaling pathways are largely activated by recruitment of these enzymes to PDGF-R SH-2 domains. The composition of the downstream signaling pathways activated by PDGF and their integration into specific cellular responses continue to be defined.[85] Although the expression of PDGF and its receptors is limited in the vascular wall at baseline, several pathological stimuli, including alterations in blood pressure and shear stress, induce peptide and receptor expression.[84] PDGF receptor expression was increased in the lungs of patients with PH, and the PDGF receptor antagonist, imatinib, reversed MCT- or hypoxia-induced PH in rodents and improved pulmonary vascular resistance and exercise capacity in a patient with severe idiopathic PH.[86-88] PPARγ ligands attenuated hypoxia-induced PDGF activation in a mouse model of PH in vivo.[15] Coupled with reports that NO inhibits PDGF signaling and that PPARγ ligands inhibit PDGF-stimulated VSMC migration in vitro,[89-91] these studies suggest that PPARγ can regulate important proliferative signaling pathways in experimental PH, including those activated by PDGF.
PDGF receptor activity can also be regulated by phosphatase and tensin homologue deleted on chromosome 10 (PTEN), a dual specificity phosphatase that dep hosphorylates both lipid and protein substrates.[92] PTEN catalyzes the removal of the phosphate moiety from the 3-position of the phosphatidylinositol ring, converting the second messenger, PI(3,4,5)P3, to PI(4,5)P2.[93] PTEN and PI3K thereby have opposing actions on cellular levels of PI(3,4,5)P3. PTEN also dephosphorylates the PDGF receptor. Because PDGF receptor activation mediates cell proliferation and migration in part through stimulation of PI3K, PTEN can inhibit PDGF signaling both at the receptor and through lowering of PI(3,4,5)P3 levels, thereby lowering the activity of PI3K-related downstream mediators such as the protein kinase B, Akt, which mediates survival, growth, and proliferative signals by inhibiting apoptosis.
PTEN activity is regulated at the transcriptional and post-translational level. At the transcriptional level, pathological stimuli such as ischemia reduced PTEN expression and promoted hypertrophy and remodeling.[94,95] Limited evidence suggests that NF-κB activation may lead to suppression of PTEN expression.[96,97] On the other hand, the PTEN promoter contains two PPAR response elements, and several studies demonstrated that PPARγ ligands
Figure 4: The effects of PPARγ activation on chronic hypoxia-induced PH and PDGF signaling. PPARγ activation decreases oxidative stress and hypoxic vasoconstriction by blunting hypoxia-induced increases NADPH oxidase expression and decreases in NO, respectively. PPARγ stimulated PTEN expression blocks PDGF-mediated vascular smooth muscle cell proliferation. Arrowheads at the end of lines denote stimulatory effects, whereas perpendicular lines denote inhibitory effects
Green, et al.: PPAR and pulmonary hypertension

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 40
stimulated PTEN expression.[98,99] Furthermore, PTEN overexpression reduced VSMC proliferation and migration and inhibited injury-induced vascular remodeling in vivo.[100,101] PTEN activity is inhibited by ROS which reversibly oxidize cysteine residues in the phosphatase active site.[102,103] In fact, NADPH oxidase-derived ROS facilitated PDGF signaling by inhibiting PTEN.[104] These reports suggested that chronic hypoxia caused sustained PI3K/Akt activation, in part, through the generation of NADPH oxidase-derived ROS that stimulated PDGF and inhibited PTEN signaling pathways. A recent report confirmed that chronic hypoxia increased PDGF receptor activation and reduced PTEN expression in the lung.[15] Furthermore, treatment with rosiglitazone attenuated hypoxia-induced PDGF receptor activation and restored PTEN levels in hypoxic mice to levels comparable to control animals. The ability of PPARγ ligands to simultaneously stimulate PTEN expression and lower oxidative stress-induced PTEN inactivation while attenuating PH provides a unique strategy to lower PDGF receptor phosphorylation and activation and reduce cellular PI(3,4,5)P3 levels. These integrated effects may contribute to the ability of PPARγ to attenuate pulmonary VSMC proliferation and hypertrophy as well as vascular remodeling caused by chronic hypoxia. A hypothetical schema depicting relationships between PPARγ, NADPH oxidase, PDGF, and PTEN is provided in Figure 4.
ALTERED BONE MORPHOGENETIC PROTEIN (BMP) AND TGF-β1 SIGNALING IN PH
BMP and TGF-β1 belong to the TGF beta superfamily of growth factors which are involved in multiple cellular processes including proliferation, differentiation, inflammation, and immunity.[105,106] All TGF-β superfamily ligands are generated as inactive dimeric precursor proteins that are subsequently cleaved by proteases, activated and secreted.[105] The ligands bind to one of two types of serine/threonine kinase receptors (type I and II) causing Smad substrate recruitment, phosphorylation, transduction of intracellular signals and nuclear translocation.[106-108] Approximately 70% of patients with familial pulmonary arterial hypertension and 11–40% with idiopathic pulmonary arterial hypertension (IPAH) have germline mutations in bone morphogenetic protein receptor-2 (BMPR-2), a receptor needed for normal vascular development.[109] BMPR-2 expression is decreased in some PH cases without identified BMPR mutation.[110] In comparison to unaffected patients, IPAH patients have altered cellular growth responses to TGF-β1 and BMP signals which favor VSMC proliferation.[106,111] Specifically, in IPAH patients, TGF-β1 induces a heightened SMC
proliferative response and BMP signaling fails to confer an expected antiproliferative and proapoptotic effect.[49] TGF-β1 signaling is responsible for pulmonary artery remodeling in rat models as evidenced by the attenuation of SMC migration and muscularization of small pulmonary arteries that occurred upon the inhibition of the TGF-β1 receptor activin like kinase-5 (ALK-5).[112]
Cell culture experiments reveal that TGF-β1 promotes smooth muscle proliferation via an autocrine induction of PDGF and Nox4.[113] Mechanistically, Nox4-derived ROS may cause transient oxidative inactivation of counterbalancing phosphatases involved in kinase-based cell growth cascades, effectively promoting cell cycle transition and proliferation. Nox4 and TGF-β1 signaling are closely linked and both increase in response to hypoxia and mediate proliferation of HPASMC in vitro.[15,114] Specifically, TGF-β1 was found to be the proximal mediator of HPASMC proliferation through a cascade involving sequential signaling of phosphatidylinositol 3-kinase (PI3K) and serine/threonine kinase (Akt) phosphorylation, insulin-like growth factor binding protein-3 (IGFBP-3), and Nox 4.[114] Dominant negative mutations of the TGF-β type II receptor ameliorated hypoxia-induced pulmonary vascular remodeling in mice, supporting the role of TGF-β1 in promoting PH through enhanced cellular proliferation.[115,116]
Several lines of evidence suggest that PPARγ activation can modulate TGF-β1 signaling through Smad-dependent and Smad-independent mechanisms. For example, both natural (15d-PGJ2) and synthetic (ciglitazone and rosiglitazone) PPARγ ligands inhibited the profibrotic effects of TGF-β1 on human lung fibroblasts in a Smad-independent manner as evidenced by blunted myofibroblast differentiation and collagen I synthesis.[117] Adenoviral PPARγ gene overexpression similarly decreased fibroblast to myofibroblast differentiation, collagen I and III production in alkali burned mouse corneas.[118] In this study, PPARγ overexpression also reduced TGF-β1mRNA transcription in fibroblasts, cultured macrophages, and epithelial cells. In other studies, PPARγ agonists prevented TGF-β1 induced mesangial and hepatic stellate cell activation and extracellular matrix secretion.[119,120] Finally, PPARγ activation inhibited TGF-β1–mediated Smad 3 phosphorylation and induction of connective tissue growth factor expression, a key regulator of extracellular matrix production and neointima formation following vascular injury.[121] These findings emphasize that PPARγ modulation of TGF-β1 signaling is cell type and context specific and that PPARγ agonists may blunt abnormal TGF-β1/BMP-2 signaling and resultant pulmonary vascular remodeling in PH. Additional pathways by which PPARγ regulates cellular proliferation and vascular remodeling are summarized in Figure 4.
Green, et al.: PPAR and pulmonary hypertension

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 41
Matrix alterationsPH involves remodeling of pulmonary vessels with muscularization of nonmuscular distal arterioles, proliferation and migration of VSMC, and increased production of extracellular matrix proteins including fibronectin, collagen, and elastin.[122,123] Alterations in matrix composition may be related to increased matrix degradation resulting from an imbalance in the matrix metalloproteinases-tissue inhibitor of metalloproteinases system (MMP-TIMP) with deposition of collagen, elastin, fibronectin, and tenascin-C.[122] Inhibition of MMPs and elastase prevented the progression and actually induced regression of vascular remodeling in an experimental model of PH.[122] In addition, the elastase inhibitor, elafin, protected mice from chronic hypoxia-induced PH.[124] Recent evidence indicates that the PPARγ ligand, rosiglitazone, attenuated and reversed vascular remodeling in rat and mouse models of chronic hypoxia-induced PH.[15,21] Rosiglitazone decreased collagen production and elastin deposition and increased MMP-2 activity. Treatment with PPARγ ligands has also been associated with attenuation of matrix deposition in disorders other than PH.[125-127] Taken together, these reports suggest that therapeutic mechanisms of PPARγ activation in PH could involve attenuation of matrix deposition and remodeling in the pulmonary vasculature.
InflammationSeveral lines of evidence implicate inflammation in the pathobiology of PH. Despite the heterogeneity of disease conditions that lead to PH, similar inflammatory cells types can be found in the plexiform vascular lesions in patients with IPAH and PH associated with connective tissue disease and HIV. Perivascular mononuclear cell infiltrates comprising macrophages, T and B lymphocytes, and dendritic cells are reported in patients with PH.[64,66,68] Circulating markers of inflammation are also increased in patients with PH.[128] Proinflammatory cytokines and growth factors such as IL-1, IL-6, PDGF, epidermal growth factor (EGF), and vascular endothelial growth factor (VEGF) are increased and contribute to mitogenic and chemoattractant events in the vascular wall in PH.[64] Chemokines that mediate inflammation by recruiting leukocytes, monocytes, and T cells to the vascular wall are increased in patients with PH. Chemokines, including fractalkine (CX3CL1), regulated upon activation, normal T-cell expressed and secreted (RANTES), and monocyte chemotactic protein-1 (MCP-1), also promote pulmonary vascular remodeling in PH.[64,68] Fracktalkine is directly associated with pulmonary artery SMC proliferation in MCT-induced PH in the rat,[129] and both RANTES[68] and MCP-1[130] may indirectly contribute to mitogenesis and vasoconstriction by inducing endothelin converting enzyme-1 (ECE-1) and ET-1.
The stimulation of these inflammatory pathways and their modulation by PPARγ likely occurs at the level of transcriptional regulation. The transcription factor, NFAT, is upregulated in the pulmonary artery walls and circulating inflammatory cells of PH patients. NFAT, a master activator of T cells, regulates the expression of many inflammatory genes. In PAH, increases in NFAT confer a proliferative and apoptosis resistant phenotype on PASMC by increasing bcl-2, mitochondrial hyperpolarization, and downregulating voltage-gated potassium channels (Kv1.5).[131] Common stimuli of PH such as hypoxia cause inflammatory responses in the pulmonary vasculature. PPARγ is expressed in T cells, macrophages, leukocytes, and dendritic cells, suggesting that its activation could modulate inflammation in the pulmonary vasculature that contributes to the development of PH. Studies demonstrate that PPARγ ligands attenuate inflammation in numerous models.[132] PPARγ activation reduced macrophage recruitment and inflammatory mediator production, impaired dendritic cell priming of T cells, as well as T lymphocyte proliferation and viability. PPARγ ligands also induced regulatory T cells which downregulate immune responses.[133,134] Current evidence indicates that these anti-inflammatory effects of PPARγ are mediated not through transactivation of specific target genes, rather through physical binding to other proinflammatory transcription factors such as NF-kB, AP-1, and STAT, leading to suppression of these proinflammatory transcriptional pathways. The precise mechanisms of these transrepression effects remain to be completely defined but may involve ligand-dependent SUMOylation of PPARγ which targets the receptor to corepressor complexes on the promoters of inflammatory genes preventing proteosomal degradation of the corepressors and thereby causing inhibition of inflammatory gene expression.[10]
ApoptosisApoptosis is an important process whereby selected cells are programmed for death and removal.[135] Apoptosis counterbalances cell proliferation and mitotic division in a cascade of events involving caspase activation and protein cleavage, nuclear DNA fragmentation, cytoplasmic condensation, cell fragment sequestration and formation of apoptotic bodies.[136] Ineffective apoptosis contributes to the pathology of diseases including some malignancies, autoimmunity and persistent infections. Deregulated apoptosis, on the other hand, may be implicated in atherosclerosis and other cardiovascular diseases.[136] Triggers for apoptosis include, but are not limited to Fas death receptor stimulation by Fas ligand, recognition of cells with DNA damage, abnormal cellular migration and proliferation, ROS, angiotensin type 2, and BMP-2.[135]
Green, et al.: PPAR and pulmonary hypertension

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 42
The pulmonary artery SMCs of patients with PAH demonstrated increased tendency to proliferate and exhibited resistance to normal apoptotic signals such as bone morphogenetic protein-2 (BMP-2).[137] Accordingly, germline mutations in BMPR-2 significantly contribute to disease pathogenesis in 70% of patients with familial PAH.[109] Impaired apoptosis and proliferation of PASMC may result from increases in the apoptosis inhibitor, survivin, and the sequential occurrences: hyperpolarization of mitochondria, increased HIF-1α transcription and nuclear translocation, and decreased Kv1.5 voltage-gated potassium channel expression.[131] These derangements in the regulation of apoptosis in pulmonary vascular wall cells likely contribute to the increased cell proliferation and migration characteristic of the remodeled pulmonary vasculature in PH.[135] PPARγ agonists promote apoptosis of proliferating VSMCs in an extracellular signal-related kinase 1/2 (ERK 1/2) - independent manner that may involve interferon regulatory factor-1 (IRF-1) or activation of the proapoptotic genes, p53 and Gadd 45.[138,139] PPARγ agonists also induce apoptosis in endothelial cells in a PPARγ-dependent manner.[140] Similarly, pulmonary artery endothelial cells derived from patients with IPAH displayed a proliferative, apoptosis-resistant phenotype associated with enhanced STAT 3 signaling, and PPAR ligands reduced STAT 3 signaling.[141,142] Taken together, these studies indicate that multiple pathways can lead to an apoptosis-resistant phenotype in pulmonary vascular wall cells during the development of PH and that PPARγ may counterbalance these proliferative pathways by stimulating apoptosis.
Progenitor cell recruitmentEndothelial progenitor cells (EPCs) are bone marrow-derived cells that are mobilized into the systemic circulation in response to ischemia or vascular injury.[143] The role of EPCs in vascular repair, vascular homeostasis, and formation of new blood vessels continues to be defined.[144] Clinical trials suggest that EPCs may serve as markers of vascular dysfunction and cardiovascular disease.[145,146] Because endothelial dysfunction participates in the pathogenesis of PH, EPCs may play a role in pulmonary vascular disease.[147] The endogenous erythropoietin system recruits EPCs to the lung in experimental PH in mice.[148] Furthermore, mesenchymal stem cells overexpressing eNOS or EPCs expressing adrenomedullin attenuated MCT-induced PH in rats.[149] These reports suggest that migration of EPCs to the pulmonary vasculature during experimental PH can exert beneficial effects. PPARγ agonists facilitate the differentiation of angiogenic progenitor cells into EPC.[150] PPARγ agonists also increased the number and migratory activity of EPC in patients with type 2 diabetes and impaired endothelial function and increased EPC migratory activity and reduced EPC apoptosis in
mice.[151] Collectively, these reports suggest that PPARγ ligands might stimulate EPC to reduce pulmonary vascular dysfunction and reduce PH.
Thrombosis in PHPulmonary artery thrombosis is a common pathologic finding occurring in 48–56% of patients with IPAH.[152,153] Thrombosis can also be found in other forms of PH associated with collagen vascular disease, HIV, portal hypertension, drugs and anorexigens. Thrombotic lesions in IPAH can be eccentric or concentric and usually occur in situ in peripheral muscular arteries where they form lesions that result from mural organization of thrombi.[49,153] Thrombosis is in large part due to abnormal platelet activation and endothelial dysfunction which results in coagulation and loss of counterbalancing antifibrinolytic mechanisms.[152,153] Shear stress from elevated pulmonary pressures may contribute to endothelial injury and release of mediators of coagulation.[49] Accordingly, patients with IPAH have increased serum levels of coagulation mediators including plasminogen activator inhibitor type-1 (PAI-1),[154] Von Willebrand factor (vWF),[155] fibrinopeptide A,[156] and factor VIIIc.[157] The abnormal platelet activation in PH can be attributed to increases in platelet-derived thromboxane (TXA2) and decreased levels of endothelial derived prostacyclin (PGI2) and nitric oxide synthase (eNOS).[158] Collectively, these imbalances favor coagulation and platelet aggregation which ultimately predisposes patients with PH to the development of thrombosis.
PPARγ agonists modulate platelets’ immunoregulatory and proinflammatory functions and favorably affect vascular patency. Platelets release a variety of proinflammatory mediators and cytokines including prostaglandin E1, TGF-β, IL-1B, PAI-1, and CD 40.[48] For example, the CD 40 ligand is a transmembrane protein expressed on stimulated CD4+ T cells and platelets,[159,160] whose expression can be reduced by PPARγ ligands.[48,161] CD 40 ligand is associated with platelet activation and increased risk for cardiovascular disease.[48,159,160] Upon platelet activation, the CD 40 ligand is released and promotes the expression of vasoactive, inflammatory, and thrombotic mediators including cyclooxygenase-2 (COX-2), prostaglandins, TNF-α, IFN-γ, tissue factor, MMPs, selected interleukins, chemokines, and multiple adhesion molecules.[48,159-161] Thus, CD 40 receptor–ligand binding links platelet activation and vascular inflammation to hemostasis and increased risk for intravascular thrombosis. In vitro, thiazolidinediones decreased platelet CD 40 ligand expression and release.[159] In vivo experiments confirmed that diabetic mice treated with pioglitazone had decreased CD 40 expression after platelet activation.[162] These studies demonstrate that PPARγ agonists modulate platelet immunoregulatory and hemostatic function by attenuating CD 40 expression.
Green, et al.: PPAR and pulmonary hypertension

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 43
Since PPARγ belongs to a nuclear receptor superfamily of transcription factors, historically PPARγ expression was thought to be limited to nucleated cells. However, Akbiyik and colleagues reported that platelets contain PPARγ.[159] Given that platelets have no nucleus and express no PPARγ mRNA, PPARγ agonists may affect platelet function through non-transcriptional pathways such as modulation of intracellular signaling or platelet–protein interactions. For example, two studies reported that pioglitazone delayed the onset of iatrogenic arterial thrombosis in animal models.[163,164] The mechanisms for these PPARγ effects may include attenuation of platelet activation as evidenced by reductions in soluble and platelet bound P-selectin,[48,162] CD 40 ligand,[49,159] and TXA2,[49,159] or to direct effects of PPARγ ligands on vascular endothelium and its production of platelet regulators. PPARγ agonists also decreased adenosine diphosphate and arachidonic acid-induced platelet aggregation,[159,163] ATP production,[163] and increased nitric oxide-mediated activation of fibrinolysis and inhibition of coagulation.[163,165] Other proposed anti-thrombotic mechanisms involve PPARγ-induced increases in prostacyclin,[164] thrombomodulin,[163] as well as decreases in PAI-1 and fibrinogen.[166,167] In summary, PPARγ ligands likely decrease platelet activation and aggregation through direct effects on platelets and cells of the vascular wall that stimulate endothelial and platelet-derived vasodilatory mediators to maintain vascular patency and blood flow.
CONCLUSIONS AND FUTURE DIRECTIONS
The evidence reviewed above suggests that PPARγ can participate in the regulation of numerous pathways implicated in PH pathogenesis. Activation of PPARγ can reduce vasoconstriction, vascular remodeling and inflammation, and thrombosis that contribute to the generation and progression of PH. Studies employing animal models of PH have demonstrated that tissue-targeted deletion of PPARγ in vascular wall cells can promote PH while activation of PPARγ with exogenous ligands attenuated PH or vascular remodeling in MCT- or hypoxia-induced rodent models of PH.[14,15,17,20-22] The limitations of these animal models have been recently reviewed emphasizing that the performance of pharmacological tools in the treatment of common experimental models of PH in rodents may not accurately translate to the treatment of human PAH.[168] The investigation of PPARγ ligands in recently reported rodent models which more closely reproduce pathological changes seen in the pulmonary arteries of patients with advanced PAH provides an experimental strategy that might circumvent some of the limitations of common existing models.[169]
Based on the findings in this review, the next step in the evaluation of PPARγ as a therapeutic target in PH would appear to be clinical trials employing PPARγ ligands in patients with PH. The abundant evidence reviewed above that PPARγ ligands can favorably modulate many pathological pathways and mediators involved in PH would support this position. In addition, the current availability of synthetic thiazolidinedione PPARγ ligands (rosiglitazone and pioglitazone) for the treatment of type 2 diabetes in the United States suggests that clinical trials could be expedited. However, recent findings surrounding potential adverse cardiovascular events in diabetic patients taking rosiglitazone emphasize the need for caution before employing this agent in PH patients with preexisting cardiopulmonary disease.[170,171] In contrast, clinical studies with pioglitazone in diabetic patients have reported a lowered risk for adverse cardiovascular endpoints.[172-175] These reports emphasize that individual PPARγ ligands may regulate unique patterns of gene expression that differentially modulate cell and tissue function. Thus, the therapeutic potential of strategies targeting PPARγ will be optimized by future studies that must determine not only the relevant molecular pathways that are altered by PPARγ in a ligand-specific manner, but also the cellular site of action of any ligand and its relative dependence on the PPARγ receptor. Evidence supporting successful therapy of PH with existing PPARγ ligands could also stimulate the development of novel pharmacological PPARγ ligands with enhanced therapeutic efficacy and/or reduced side effects.
ACKNOWLEDGMENTS
The authors acknowledge grant support from the Research Service of the Atlanta Veterans Affairs Medical Center and the National Institutes of Health (R01 DK 074518). Dr. Green is supported by an NHLBI T32 training grant (HL076118-06).
REFERENCES
1. Humbert M, Sitbon O, Chaouat A, Bertocchi M, Habib G, Gressin V, et al. Pulmonary arterial hypertension in France: Results from a national registry. Am J Respir Crit Care Med 2006;173:1023-30.
2. Simonneau G, Robbins IM, Beghett i M, Channick RN, Delcroix M, Denton CP, et al. Updated clinical classifi cation of pulmonary hypertension. J Am Coll Cardiol 2009;54:S43-54.
3. McLaughlin VV, Archer SL, Badesch DB, Barst RJ, Farber HW, Lindner JR, et al. ACCF/AHA 2009 expert consensus document on pulmonary hypertension: A report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents and the American Heart Association: Developed in collaboration with the American College of Chest Physicians, American Thoracic Society, Inc., and the Pulmonary Hypertension Association. Circulation 2009;119:2250-94.
4. Desvergne B, Wahli W. Peroxisome proliferator-activated receptors: Nuclear control of metabolism. Endocr Rev 1999;20:649-88.
5. Mandard S, Müller M, Kersten S. Peroxisome proliferator-activated receptor alpha target genes. Cell Mol Life Sci 2004;61:393-416.
6. Barak Y, Liao D, He W, Ong ES, Nelson MC, Olefsky JM, et al. Eff ects of peroxisome proliferator-activated receptor delta on placentation,
Green, et al.: PPAR and pulmonary hypertension

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 44
adiposity, and colorectal cancer. Proc Natl Acad Sci U S A 2002;99:303-8.7. Peters JM, Lee SS, Li W, Ward JM, Gavrilova O, Everett C, et al. Growth,
adipose, brain, and skin alterations resulting from targeted disruption of the mouse peroxisome proliferator-activated receptor beta(delta). Mol Cell Biol 2000;20:5119-28.
8. Zhu Y, Qi C, Korenberg JR, Chen XN, Noya D, Rao MS, et al. Structural organization of mouse peroxisome proliferator-activated receptor gamma (mPPAR gamma) gene: Alternative promoter use and diff erent splicing yield two mPPAR gamma isoforms. Proc Natl Acad Sci U S A 1995;92:7921-5.
9. Rosen ED, Sarraf P, Troy AE, Bradwin G, Moore K, Milstone DS, et al. PPAR gamma is required for the diff erentiation of adipose tissue in vivo and in vitro. Mol Cell 1999;4:611-7.
10. Pascual G, Fong AL, Ogawa S, Gamliel A, Li AC, Perissi V, et al. A SUMOylation-dependent pathway mediates transrepression of infl ammatory response genes by PPAR-gamma. Nature 2005;437:759-63.
11. Li AC, Brown KK, Silvestre MJ, Willson TM, Palinski W, Glass CK. Peroxisome proliferator-activated receptor gamma ligands inhibit development of atherosclerosis in LDL receptor-defi cient mice. J Clin Invest 2000;106:523-31.
12. Xu HE, Lambert MH, Montana VG, Parks DJ, Blanchard SG, Brown PJ, et al. Molecular recognition of fatt y acids by peroxisome proliferator-activated receptors. Mol Cell 1999;3:397-403.
13. Ameshima S, Golpon H, Cool CD, Chan D, Vandivier RW, Gardai SJ, et al. Peroxisome proliferator-activated receptor gamma (PPARgamma) expression is decreased in pulmonary hypertension and aff ects endothelial cell growth. Circ Res 2003;92:1162-9.
14. Kim EK, Lee JH, Oh YM, Lee YS, Lee SD. Rosiglitazone att enuates hypoxia-induced pulmonary arterial hypertension in rats. Respirology 2010;15:659-68.
15. Nisbet RE, Bland JM, Kleinhenz DJ, Mitchell PO, Walp ER, Sutliff RL, et al. Rosiglitazone attenuates chronic hypoxia-induced pulmonary hypertension in a mouse model. Am J Respir Cell Mol Biol 2010;42:482-90.
16. Barak Y, Nelson MC, Ong ES, Jones YZ, Ruiz-Lozano P, Chien KR, et al. PPAR gamma is required for placental, cardiac, and adipose tissue development. Mol Cell 1999;4:585-95.
17. Guignabert C, Alvira CM, Alastalo TP, Sawada H, Hansmann G, Zhao M, et al. Tie2-Mediated loss of peroxisome proliferator-activated receptor-{gamma} in mice causes PDGF-receptor {beta}-dependant pulmonary arterial muscularization. Am J Physiol Lung Cell Mol Physiol 2009;297:L1082-90.
18. Hansmann L, Groeger S, von Wulff en W, Bein G, Hackstein H. Human monocytes represent a competitive source of interferon-alpha in peripheral blood. Clin Immunol 2008;127:252-64.
19. Tian J, Smith A, Nechtman J, Podolsky R, Aggarwal S, Snead C, et al. Eff ect of PPARgamma inhibition on pulmonary endothelial cell gene expression: Gene profi ling in pulmonary hypertension. Physiol Genomics 2009;40:48-60.
20. Matsuda Y, Hoshikawa Y, Ameshima S, Suzuki S, Okada Y, Tabata T, et al. [Eff ects of peroxisome proliferator-activated receptor gamma ligands on monocrotaline-induced pulmonary hypertension in rats]. Nihon Kokyuki Gakkai Zasshi 2005;43:283-8.
21. Crossno JT Jr, Garat CV, Reusch JE, Morris KG, Dempsey EC, McMurtry IF, et al. Rosiglitazone att enuates hypoxia-induced pulmonary arterial remodeling. Am J Physiol Lung Cell Mol Physiol 2007;292:L885-97.
22. Hansmann G, de Jesus Perez VA, Alastalo TP, Alvira CM, Guignabert C, Bekker JM, et al. An antiproliferative BMP-2/PPARgamma/apoE axis in human and murine SMCs and its role in pulmonary hypertension. J Clin Invest 2008;118:1846-57.
23. Christman BW, McPherson CD, Newman JH, King GA, Bernard GR, Groves BM, et al. An imbalance between the excretion of thromboxane and prostacyclin metabolites in pulmonary hypertension. N Engl J Med 1992;327:70-5.
24. Farber HW, Loscalzo J. Pulmonary arterial hypertension. N Engl J Med 2004;351:1655-65.
25. Giaid A, Saleh D. Reduced expression of endothelial nitric oxide synthase in the lungs of patients with pulmonary hypertension. N Engl J Med 1995;333:214-21.
26. Li H, Chen SJ, Chen YF, Meng QC, Durand J, Oparil S, et al. Enhanced endothelin-1 and endothelin receptor gene expression in chronic hypoxia. J Appl Physiol 1994;77:1451-9.
27. Olschewski H, Rose F, Schermuly R, Ghofrani HA, Enke B, Olschewski A, et al. Prostacyclin and its analogues in the treatment of pulmonary hypertension. Pharmacol Ther 2004;102:139-53.
28. Hoshikawa Y, Voelkel NF, Gesell TL, Moore MD, Morris KG, Alger LA, et al., Prostacyclin receptor-dependent modulation of pulmonary vascular remodeling. Am J Respir Crit Care Med 2001;164:314-8.
29. Tuder RM, Cool CD, Geraci MW, Wang J, Abman SH, Wright L, et al. Prostacyclin synthase expression is decreased in lungs from patients with severe pulmonary hypertension. Am J Respir Crit Care Med 1999;159:1925-32.
30. Robbins IM, Morrow JD, Christman BW. Oxidant stress but not thromboxane decreases with epoprostenol therapy. Free Radic Biol Med 2005;38:568-74.
31. Gupta RA, Tan J, Krause WF, Geraci MW, Willson TM, Dey SK, et al. Prostacyclin-mediated activation of peroxisome proliferator-activated receptor delta in colorectal cancer. Proc Natl Acad Sci U S A 2000;97:13275-80.
32. Lim H, Dey SK. A novel pathway of prostacyclin signaling-hanging out with nuclear receptors. Endocrinology 2002;143:3207-10.
33. Peredo HA, Mayer MA, Carranza A, Puyó AM. Pioglitazone and losartan modify hemodynamic and metabolic parameters and vascular prostanoids in fructose-overloaded rats. Clin Exp Hypertens 2008;30:159-69.
34. Tesse A, Al-Massarani G, Wangensteen R, Reitenbach S, Martínez MC, Andriantsitohaina R. Rosiglitazone, a peroxisome proliferator-activated receptor-gamma agonist, prevents microparticle-induced vascular hyporeactivity through the regulation of proinfl ammatory proteins. J Pharmacol Exp Ther 2008;324:539-47.
35. Adnot S, Raffestin B, Eddahibi S, Braquet P, Chabrier PE. Loss of endothelium-dependent relaxant activity in the pulmonary circulation of rats exposed to chronic hypoxia. J Clin Invest 1991;87:155-62.
36. Steinhorn RH, Russell JA, Lakshminrusimha S, Gugino SF, Black SM, Fineman JR. Altered endothelium-dependent relaxations in lambs with high pulmonary blood fl ow and pulmonary hypertension. Am J Physiol Heart Circ Physiol 2001;280:H311-7.
37. McQuillan LP, Leung GK, Marsden PA, Kostyk SK, Kourembanas S. Hypoxia inhibits expression of eNOS via transcriptional and postt ranscriptional mechanisms. Am J Physiol 1994;267:H1921-7.
38. Fagan KA, Fouty BW, Tyler RC, Morris KG Jr, Hepler LK, Sato K, et al. The pulmonary circulation of homozygous or heterozygous eNOS-null mice is hyperresponsive to mild hypoxia. J Clin Invest 1999;103:291-9.
39. Champion HC, Bivalacqua TJ, Greenberg SS, Giles TD, Hyman AL, Kadowitz PJ. Adenoviral gene transfer of endothelial nitric-oxide synthase (eNOS) partially restores normal pulmonary arterial pressure in eNOS-defi cient mice. Proc Natl Acad Sci U S A 2002;99:13248-53.
40. Ozaki M, Kawashima S, Yamashita T, Ohashi Y, Rikitake Y, Inoue N, et al. Reduced hypoxic pulmonary vascular remodeling by nitric oxide from the endothelium. Hypertension 2001;37:322-7.
41. Channick RN, Newhart JW, Johnson FW, Williams PJ, Auger WR, Fedullo PF, et al. Pulsed delivery of inhaled nitric oxide to patients with primary pulmonary hypertension: An ambulatory delivery system and initial clinical tests. Chest 1996;109:1545-9.
42. Zhao YD, Courtman DW, Ng DS, Robb MJ, Deng YP, Trogadis J, et al. Microvascular regeneration in established pulmonary hypertension by angiogenic gene transfer. Am J Respir Cell Mol Biol 2006;35:182-9.
43. Pritchard KA Jr, Ackerman AW, Gross ER, Stepp DW, Shi Y, Fontana JT, et al. Heat shock protein 90 mediates the balance of nitric oxide and superoxide anion from endothelial nitric-oxide synthase. J Biol Chem 2001;276:17621-4.
44. Konduri GG, Ou J, Shi Y, Pritchard KA Jr. Decreased association of HSP90 impairs endothelial nitric oxide synthase in fetal lambs with persistent pulmonary hypertension. Am J Physiol Heart Circ Physiol 2003;285:H204-11.
45. Murata T, Sato K, Hori M, Ozaki H, Karaki H. Decreased endothelial nitric-oxide synthase (eNOS) activity resulting from abnormal interaction between eNOS and its regulatory proteins in hypoxia-induced pulmonary hypertension. J Biol Chem 2002;277:44085-92.
46. Calnek DS, Mazzella L, Roser S, Roman J, Hart CM. Peroxisome proliferator-activated receptor gamma ligands increase release of nitric oxide from endothelial cells. Arterioscler Thromb Vasc Biol 2003;23:52-7.
47. Polikandriotis JA, Mazzella LJ, Rupnow HL, Hart CM. Peroxisome proliferator-activated receptor gamma ligands stimulate endothelial nitric oxide production through distinct peroxisome proliferator-activated receptor gamma-dependent mechanisms. Arterioscler Thromb Vasc Biol 2005;25:1810-6.
48. Borchert M, Schöndorf T, Lübben G, Forst T, Pfützner A. Review of the pleiotropic eff ects of peroxisome proliferator-activated receptor gamma agonists on platelet function. Diabetes Technol Ther 2007;9:410-20.
49. Morrell NW, Adnot S, Archer SL, Dupuis J, Jones PL, MacLean MR, et al.
Green, et al.: PPAR and pulmonary hypertension

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 45
Cellular and molecular basis of pulmonary arterial hypertension. J Am Coll Cardiol 2009;54:S20-31.
50. Wakino S, Hayashi K, Tatematsu S, Hasegawa K, Takamatsu I, Kanda T, et al. Pioglitazone lowers systemic asymmetric dimethylarginine by inducing dimethylarginine dimethylaminohydrolase in rats. Hypertens Res 2005;28:255-62.
51. Palmer RM, Ferrige AG, Moncada S. Nitric oxide release accounts for the biological activity of endothelium-derived relaxing factor. Nature 1987;327:524-6.
52. Azuma H, Ishikawa M, Sekizaki S. Endothelium-dependent inhibition of platelet aggregation. Br J Pharmacol 1986;88:411-5.
53. Garg UC, Hassid A. Nitric oxide-generating vasodilators and 8-bromo-cyclic guanosine monophosphate inhibit mitogenesis and proliferation of cultured rat vascular smooth muscle cells. J Clin Invest 1989;83:1774-7.
54. Bath PM, Hassall DG, Gladwin AM, Palmer RM, Martin JF. Nitric oxide and prostacyclin. Divergence of inhibitory eff ects on monocyte chemotaxis and adhesion to endothelium in vitro. Arterioscler Thromb 1991;11:254-60.
55. Kuzkaya N, Weissmann N, Harrison DG, Dikalov S. Interactions of peroxynitrite, tetrahydrobiopterin, ascorbic acid, and thiols: Implications for uncoupling endothelial nitric-oxide synthase. J Biol Chem 2003;278:22546-54.
56. Jernigan NL, Walker BR, Resta TC. Endothelium-derived reactive oxygen species and endothelin-1 att enuate NO-dependent pulmonary vasodilation following chronic hypoxia. Am J Physiol Lung Cell Mol Physiol 2004;287:L801-8.
57. Liu JQ, Zelko IN, Erbynn EM, Sham JS, Folz RJ. Hypoxic pulmonary hypertension: Role of superoxide and NADPH oxidase (gp91phox). Am J Physiol Lung Cell Mol Physiol 2006;290:L2-10.
58. Delerive P, Martin-Nizard F, Chinett i G, Trott ein F, Fruchart JC, Najib J, et al. Peroxisome proliferator-activated receptor activators inhibit thrombin-induced endothelin-1 production in human vascular endothelial cells by inhibiting the activator protein-1 signaling pathway. Circ Res 1999;85:394-402.
59. Martin-Nizard F, Furman C, Delerive P, Kandoussi A, Fruchart JC, Staels B, et al. Peroxisome proliferator-activated receptor activators inhibit oxidized low-density lipoprotein-induced endothelin-1 secretion in endothelial cells. J Cardiovasc Pharmacol 2002;40:822-31.
60. Fukunaga Y, Itoh H, Doi K, Tanaka T, Yamashita J, Chun TH, et al. Thiazolidinediones, peroxisome proliferator-activated receptor gamma agonists, regulate endothelial cell growth and secretion of vasoactive peptides. Atherosclerosis 2001;158:113-9.
61. Wang TD, Chen WJ, Cheng WC, Lin JW, Chen MF, Lee YT. Relation of improvement in endothelium-dependent fl ow-mediated vasodilation aft er rosiglitazone to changes in asymmetric dimethylarginine, endothelin-1, and C-reactive protein in nondiabetic patients with the metabolic syndrome. Am J Cardiol 2006;98:1057-62.
62. Iglarz M, Touyz RM, Amiri F, Lavoie MF, Diep QN, Schiff rin EL. Eff ect of peroxisome proliferator-activated receptor-alpha and -gamma activators on vascular remodeling in endothelin-dependent hypertension. Arterioscler Thromb Vasc Biol 2003;23:45-51.
63. Jeff ery TK, Morrell NW. Molecular and cellular basis of pulmonary vascular remodeling in pulmonary hypertension. Prog Cardiovasc Dis 2002;45:173-202.
64. Hassoun PM, Mouthon L, Barberà JA, Eddahibi S, Flores SC, Grimminger F, et al. Infl ammation, growth factors, and pulmonary vascular remodeling. J Am Coll Cardiol 2009;54:S10-9.
65. Tuder RM, Groves B, Badesch DB, Voelkel NF. Exuberant endothelial cell growth and elements of infl ammation are present in plexiform lesions of pulmonary hypertension. Am J Pathol 1994;144:275-85.
66. Tuder RM, Voelkel NF. Pulmonary hypertension and infl ammation. J Lab Clin Med 1998;132:16-24.
67. Balabanian K, Foussat A, Dorfmüller P, Durand-Gasselin I, Capel F, Bouchet-Delbos L, et al. CX(3)C chemokine fractalkine in pulmonary arterial hypertension. Am J Respir Crit Care Med 2002;165:1419-25.
68. Dorfmüller P, Zarka V, Durand-Gasselin I, Monti G, Balabanian K, Garcia G, et al. Chemokine RANTES in severe pulmonary arterial hypertension. Am J Respir Crit Care Med 2002;165:534-9.
69. Sanchez O, Marcos E, Perros F, Fadel E, Tu L, Humbert M, et al. Role of endothelium-derived CC chemokine ligand 2 in idiopathic pulmonary arterial hypertension. Am J Respir Crit Care Med 2007;176:1041-7.
70. Griendling KK, Sorescu D, Ushio-Fukai M. NAD(P)H oxidase: Role in cardiovascular biology and disease. Circ Res 2000;86:494-501.
71. Bedard K, Krause KH. The NOX family of ROS-generating NADPH oxidases: Physiology and pathophysiology. Physiol Rev 2007;87:245-313.
72. Lambeth JD. Nox/Duox family of nicotinamide adenine dinucleotide (phosphate) oxidases. Curr Opin Hematol 2002;9:11-7.
73. Mitt al M, Roth M, König P, Hofmann S, Dony E, Goyal P, et al. Hypoxia-dependent regulation of nonphagocytic NADPH oxidase subunit NOX4 in the pulmonary vasculature. Circ Res 2007;101:258-67.
74. Ambasta RK, Kumar P, Griendling KK, Schmidt HH, Busse R, Brandes RP. Direct interaction of the novel Nox proteins with p22phox is required for the formation of a functionally active NADPH oxidase. J Biol Chem 2004;279:45935-41.
75. Djordjevic T, BelAiba RS, Bonello S, Pfeilschift er J, Hess J, Görlach A. Human urotensin II is a novel activator of NADPH oxidase in human pulmonary artery smooth muscle cells. Arterioscler Thromb Vasc Biol 2005;25:519-25.
76. Serrander L, Cartier L, Bedard K, Banfi B, Lardy B, Plastre O, et al. NOX4 activity is determined by mRNA levels and reveals a unique patt ern of ROS generation. Biochem J 2007;406:105-14.
77. Lambeth JD, Kawahara T, Diebold B. Regulation of Nox and Duox enzymatic activity and expression. Free Radic Biol Med 2007;43:319-31.
78. Sorescu GP, Song H, Tressel SL, Hwang J, Dikalov S, Smith DA, et al. Bone morphogenic protein 4 produced in endothelial cells by oscillatory shear stress induces monocyte adhesion by stimulating reactive oxygen species production from a nox1-based NADPH oxidase. Circ Res 2004;95:773-9.
79. Hwang J, Kleinhenz DJ, Lassègue B, Griendling KK, Dikalov S, Hart CM. Peroxisome proliferator-activated receptor-gamma ligands regulate endothelial membrane superoxide production. Am J Physiol Cell Physiol 2005;288:C899-905.
80. Lu X, Murphy TC, Nanes MS, Hart CM. PPAR{gamma} regulates hypoxia-induced Nox4 expression in human pulmonary artery smooth muscle cells through NF-{kappa}B. Am J Physiol Lung Cell Mol Physiol 2010;299:L559-66.
81. Zhang L, Sheppard OR, Shah AM, Brewer AC. Positive regulation of the NADPH oxidase NOX4 promoter in vascular smooth muscle cells by E2F. Free Radic Biol Med 2008;45:679-85.
82. Chen K, Kirber MT, Xiao H, Yang Y, Keaney JF Jr. Regulation of ROS signal transduction by NADPH oxidase 4 localization. J Cell Biol 2008;181:1129-39.
83. Fredriksson L, Li H, Eriksson U. The PDGF family: Four gene products form fi ve dimeric isoforms. Cytokine Growth Factor Rev 2004;15:197-204.
84. Raines EW. PDGF and cardiovascular disease. Cytokine Growth Factor Rev 2004;15:237-54.
85. Tallquist M, Kazlauskas A. PDGF signaling in cells and mice. Cytokine Growth Factor Rev 2004;15:205-13.
86. Balasubramaniam V, Le Cras TD, Ivy DD, Grover TR, Kinsella JP, Abman SH. Role of platelet-derived growth factor in vascular remodeling during pulmonary hypertension in the ovine fetus. Am J Physiol Lung Cell Mol Physiol 2003;284:L826-33.
87. Ghofrani HA, Seeger W, Grimminger F. Imatinib for the treatment of pulmonary arterial hypertension. N Engl J Med 2005;353:1412-3.
88. Schermuly RT, Dony E, Ghofrani HA, Pullamsett i S, Savai R, Roth M, et al. Reversal of experimental pulmonary hypertension by PDGF inhibition. J Clin Invest 2005;115:2811-21.
89. Goetze S, Xi XP, Kawano H, Gotlibowski T, Fleck E, Hsueh WA, et al. PPAR gamma-ligands inhibit migration mediated by multiple chemoatt ractants in vascular smooth muscle cells. J Cardiovasc Pharmacol 1999;33:798-806.
90. Marx N, Schönbeck U, Lazar MA, Libby P, Plutzky J. Peroxisome proliferator-activated receptor gamma activators inhibit gene expression and migration in human vascular smooth muscle cells. Circ Res 1998;83:1097-103.
91. Law RE, Goetze S, Xi XP, Jackson S, Kawano Y, Demer L, et al. Expression and function of PPARgamma in rat and human vascular smooth muscle cells. Circulation 2000;101:1311-8.
92. Gericke A, Munson M, Ross AH. Regulation of the PTEN phosphatase. Gene 2006;374:1-9.
93. Maehama T, Dixon JE. The tumor suppressor, PTEN/MMAC1, dephosphorylates the lipid second messenger, phosphatidylinositol 3,4,5-trisphosphate. J Biol Chem 1998;273:13375-8.
94. Schwartzbauer G, Robbins J. The tumor suppressor gene PTEN can regulate cardiac hypertrophy and survival. J Biol Chem 2001;276:35786-93.
95. Tong H, Chen W, Steenbergen C, Murphy E. Ischemic preconditioning activates phosphatidylinositol-3-kinase upstream of protein kinase C. Circ Res 2000;87:309-15.
96. Han SW, Roman J. Fibronectin induces cell proliferation and inhibits apoptosis in human bronchial epithelial cells: Pro-oncogenic eff ects mediated by PI3-kinase and NF-kappa B. Oncogene 2006;25:4341-9.
Green, et al.: PPAR and pulmonary hypertension

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 46
97. Wang Q, Zhou Y, Wang X, Chung DH, Evers BM. Regulation of PTEN expression in intestinal epithelial cells by c-Jun NH2-terminal kinase activation and nuclear factor-kappaB inhibition. Cancer Res 2007;67:7773-81.
98. Farrow B, Evers BM. Activation of PPARgamma increases PTEN expression in pancreatic cancer cells. Biochem Biophys Res Commun 2003;301:50-3.
99. Patel L, Pass I, Coxon P, Downes CP, Smith SA, Macphee CH. Tumor suppressor and anti-infl ammatory actions of PPARgamma agonists are mediated via upregulation of PTEN. Curr Biol 2001;11:764-8.
100. Huang J, Kontos CD. Inhibition of vascular smooth muscle cell proliferation, migration, and survival by the tumor suppressor protein PTEN. Arterioscler Thromb Vasc Biol 2002;22:745-51.
101. Huang J, Niu XL, Pippen AM, Annex BH, Kontos CD. Adenovirus-mediated intraarterial delivery of PTEN inhibits neointimal hyperplasia. Arterioscler Thromb Vasc Biol 2005;25:354-8.
102. Lee SR, Yang KS, Kwon J, Lee C, Jeong W, Rhee SG. Reversible inactivation of the tumor suppressor PTEN by H2O2. J Biol Chem 2002;277:20336-42.
103. Leslie NR, Bennett D, Lindsay YE, Stewart H, Gray A, Downes CP. Redox regulation of PI 3-kinase signalling via inactivation of PTEN. EMBO J 2003;22:5501-10.
104. Kwon J, Lee SR, Yang KS, Ahn Y, Kim YJ, Stadtman ER, et al. Reversible oxidation and inactivation of the tumor suppressor PTEN in cells stimulated with peptide growth factors. Proc Natl Acad Sci U S A 2004;101:16419-24.
105. Goumans MJ, Liu Z, ten Dij ke P. TGF-beta signaling in vascular biology and dysfunction. Cell Res 2009;19:116-27.
106. Upton PD, Morrell NW. TGF-beta and BMPR-II pharmacology--implications for pulmonary vascular diseases. Curr Opin Pharmacol 2009;9:274-80.
107. Miyazono K. Transforming growth factor-beta signaling in epithelial-mesenchymal transition and progression of cancer. Proc Jpn Acad Ser B Phys Biol Sci 2009;85:314-23.
108. Richter A, Yeager ME, Zaiman A, Cool CD, Voelkel NF, Tuder RM. Impaired transforming growth factor-beta signaling in idiopathic pulmonary arterial hypertension. Am J Respir Crit Care Med 2004;170:1340-8.
109. Cogan JD, Vnencak-Jones CL, Phillips JA 3rd, Lane KB, Wheeler LA, Robbins IM, et al. Gross BMPR2 gene rearrangements constitute a new cause for primary pulmonary hypertension. Genet Med 2005;7:169-74.
110. Du L, Sullivan CC, Chu D, Cho AJ, Kido M, Wolf PL, et al. Signaling molecules in nonfamilial pulmonary hypertension. N Engl J Med 2003;348:500-9.
111. Humbert M, Morrell NW, Archer SL, Stenmark KR, MacLean MR, Lang IM, et al. Cellular and molecular pathobiology of pulmonary arterial hypertension. J Am Coll Cardiol 2004;43:13S-24S.
112. Long L, Crosby A, Yang X, Southwood M, Upton PD, Kim DK, et al. Altered bone morphogenetic protein and transforming growth factor-beta signaling in rat models of pulmonary hypertension: Potential for activin receptor-like kinase-5 inhibition in prevention and progression of disease. Circulation 2009;119:566-76.
113. Sturrock A, Cahill B, Norman K, Huecksteadt TP, Hill K, Sanders K, et al. Transforming growth factor-beta1 induces Nox4 NAD(P)H oxidase and reactive oxygen species-dependent proliferation in human pulmonary artery smooth muscle cells. Am J Physiol Lung Cell Mol Physiol 2006;290:L661-73.
114. Ismail S, Sturrock A, Wu P, Cahill B, Norman K, Huecksteadt T, et al. NOX4 mediates hypoxia-induced proliferation of human pulmonary artery smooth muscle cells: The role of autocrine production of transforming growth factor-{beta}1 and insulin-like growth factor binding protein-3. Am J Physiol Lung Cell Mol Physiol 2009;296:L489-99.
115. Ambalavanan N, Nicola T, Hagood J, Bulger A, Serra R, Murphy-Ullrich J, et al. Transforming growth factor-beta signaling mediates hypoxia-induced pulmonary arterial remodeling and inhibition of alveolar development in newborn mouse lung. Am J Physiol Lung Cell Mol Physiol 2008;295:L86-95.
116. Chen G, Khalil N. TGF-beta1 increases proliferation of airway smooth muscle cells by phosphorylation of map kinases. Respir Res 2006;7:2.
117. Burgess HA, Daugherty LE, Thatcher TH, Lakatos HF, Ray DM, Redonnet M, et al. PPARgamma agonists inhibit TGF-beta induced pulmonary myofi broblast diff erentiation and collagen production: Implications for therapy of lung fibrosis. Am J Physiol Lung Cell Mol Physiol 2005;288:L1146-53.
118. Saika S, Yamanaka O, Nishikawa-Ishida I, Kitano A, Flanders KC, Okada Y, et al. Eff ect of Smad7 gene overexpression on transforming growth factor
beta-induced retinal pigment fi brosis in a proliferative vitreoretinopathy mouse model. Arch Ophthalmol 2007;125:647-54.
119. Zou R, Xu G, Liu XC, Han M, Jiang JJ, Huang Q, et al. PPARgamma agonists inhibit TGF-beta-PKA signaling in glomerulosclerosis. Acta Pharmacol Sin 2010;31:43-50.
120. Zhao C, Chen W, Yang L, Chen L, Stimpson SA, Diehl AM. PPARgamma agonists prevent TGFbeta1/Smad3-signaling in human hepatic stellate cells. Biochem Biophys Res Commun 2006;350:385-91.
121. Fu M, Zhang J, Zhu X, Myles DE, Willson TM, Liu X, et al. Peroxisome proliferator-activated receptor gamma inhibits transforming growth factor beta-induced connective tissue growth factor expression in human aortic smooth muscle cells by interfering with Smad3. J Biol Chem 2001;276:45888-94.
122. Cowan KN, Jones PL, Rabinovitch M. Elastase and matrix metalloproteinase inhibitors induce regression, and tenascin-C antisense prevents progression, of vascular disease. J Clin Invest 2000;105:21-34.
123. Stenmark KR, Fagan KA, Frid MG. Hypoxia-induced pulmonary vascular remodeling: Cellular and molecular mechanisms. Circ Res 2006;99:675-91.
124. Zaidi SH, You XM, Ciura S, Husain M, Rabinovitch M. Overexpression of the serine elastase inhibitor elafi n protects transgenic mice from hypoxic pulmonary hypertension. Circulation 2002;105:516-21.
125. Hao GH, Niu XL, Gao DF, Wei J, Wang NP. Agonists at PPAR-gamma suppress angiotensin II-induced production of plasminogen activator inhibitor-1 and extracellular matrix in rat cardiac fibroblasts. Br J Pharmacol 2008;153:1409-19.
126. Makino N, Sugano M, Satoh S, Oyama J, Maeda T. Peroxisome proliferator-activated receptor-gamma ligands att enuate brain natriuretic peptide production and aff ect remodeling in cardiac fi broblasts in reoxygenation aft er hypoxia. Cell Biochem Biophys 2006;44:65-71.
127. Peng Y, Liu H, Liu F, Liu Y, Li J, Chen X. Troglitazone inhibits synthesis of transforming growth factor-beta1 and reduces matrix production in human peritoneal mesothelial cells. Nephrology (Carlton) 2006;11:516-23.
128. Bakouboula B, Morel O, Faure A, Zobairi F, Jesel L, Trinh A, et al. Procoagulant membrane microparticles correlate with the severity of pulmonary arterial hypertension. Am J Respir Crit Care Med 2008;177:536-43.
129. Perros F, Dorfmüller P, Souza R, Durand-Gasselin I, Godot V, Capel F, et al. Fractalkine-induced smooth muscle cell proliferation in pulmonary hypertension. Eur Respir J 2007;29:937-43.
130. Molet S, Furukawa K, Maghazechi A, Hamid Q, Giaid A. Chemokine- and cytokine-induced expression of endothelin 1 and endothelin-converting enzyme 1 in endothelial cells. J Allergy Clin Immunol 2000;105:333-8.
131. Bonnet S, Rochefort G, Sutendra G, Archer SL, Haromy A, Webster L, et al. The nuclear factor of activated T cells in pulmonary arterial hypertension can be therapeutically targeted. Proc Natl Acad Sci U S A 2007;104:11418-23.
132. Szanto A, Nagy L. The many faces of PPARgamma: Anti-infl ammatory by any means? Immunobiology 2008;213:789-803.
133. Hontecillas R, Bassaganya-Riera J. Peroxisome proliferator-activated receptor gamma is required for regulatory CD4+ T cell-mediated protection against colitis. J Immunol 2007;178:2940-9.
134. Wohlfert EA, Nichols FC, Nevius E, Clark RB. Peroxisome proliferator-activated receptor gamma (PPARgamma) and immunoregulation: Enhancement of regulatory T cells through PPARgamma-dependent and -independent mechanisms. J Immunol 2007;178:4129-35.
135. Gurbanov E, Shiliang X. The key role of apoptosis in the pathogenesis and treatment of pulmonary hypertension. Eur J Cardiothorac Surg 2006;30:499-507.
136. Haunstett er A, Izumo S. Apoptosis: Basic mechanisms and implications for cardiovascular disease. Circ Res 1998;82:1111-29.
137. Zhang S, Fantozzi I, Tigno DD, Yi ES, Platoshyn O, Thistlethwaite PA, et al. Bone morphogenetic proteins induce apoptosis in human pulmonary vascular smooth muscle cells. Am J Physiol Lung Cell Mol Physiol 2003;285:L740-54.
138. Okura T, Nakamura M, Takata Y, Watanabe S, Kitami Y, Hiwada K. Troglitazone induces apoptosis via the p53 and Gadd45 pathway in vascular smooth muscle cells. Eur J Pharmacol 2000;407:227-35.
139. Aizawa Y, Kawabe J, Hasebe N, Takehara N, Kikuchi K. Pioglitazone enhances cytokine-induced apoptosis in vascular smooth muscle cells and reduces intimal hyperplasia. Circulation 2001;104:455-60.
140. Bishop-Bailey D, Hla T. Endothelial cell apoptosis induced by the peroxisome proliferator-activated receptor (PPAR) ligand 15-deoxy-Delta12, 14-prostaglandin J2. J Biol Chem 1999;274:17042-8.
141. Masri FA, Xu W, Comhair SA, Asosingh K, Koo M, Vasanji A, et al.
Green, et al.: PPAR and pulmonary hypertension

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 47
Hyperproliferative apoptosis-resistant endothelial cells in idiopathic pulmonary arterial hypertension. Am J Physiol Lung Cell Mol Physiol 2007;293:L548-54.
142. Park EJ, Park SY, Joe EH, Jou I. 15d-PGJ2 and rosiglitazone suppress Janus kinase-STAT inflammatory signaling through induction of suppressor of cytokine signaling 1 (SOCS1) and SOCS3 in glia. J Biol Chem 2003;278:14747-52.
143. Asahara T, Murohara T, Sullivan A, Silver M, van der Zee R, Li T, et al. Isolation of putative progenitor endothelial cells for angiogenesis. Science 1997;275:964-7.
144. Rosenzweig A. Circulating endothelial progenitors--cells as biomarkers. N Engl J Med 2005;353:1055-7.
145. Hill JM, Zalos G, Halcox JP, Schenke WH, Waclawiw MA, Quyyumi AA, et al. Circulating endothelial progenitor cells, vascular function, and cardiovascular risk. N Engl J Med 2003;348:593-600.
146. Werner N, Kosiol S, Schiegl T, Ahlers P, Walenta K, Link A, et al. Circulating endothelial progenitor cells and cardiovascular outcomes. N Engl J Med 2005;353:999-1007.
147. Sata M. Role of circulating vascular progenitors in angiogenesis, vascular healing, and pulmonary hypertension: Lessons from animal models. Arterioscler Thromb Vasc Biol 2006;26:1008-14.
148. Satoh K, Kagaya Y, Nakano M, Ito Y, Ohta J, Tada H, et al. Important role of endogenous erythropoietin system in recruitment of endothelial progenitor cells in hypoxia-induced pulmonary hypertension in mice. Circulation 2006;113:1442-50.
149. Nagaya N, Kangawa K, Kanda M, Uematsu M, Horio T, Fukuyama N, et al. Hybrid cell-gene therapy for pulmonary hypertension based on phagocytosing action of endothelial progenitor cells. Circulation 2003;108:889-95.
150. Wang CH, Ciliberti N, Li SH, Szmitko PE, Weisel RD, Fedak PW, et al. Rosiglitazone facilitates angiogenic progenitor cell diff erentiation toward endothelial lineage: A new paradigm in glitazone pleiotropy. Circulation 2004;109:1392-400.
151. Gensch C, Clever YP, Werner C, Hanhoun M, Böhm M, Laufs U. The PPAR-gamma agonist pioglitazone increases neoangiogenesis and prevents apoptosis of endothelial progenitor cells. Atherosclerosis 2007;192:67-74.
152. Chaouat A, Weitzenblum E, Higenbott am T. The role of thrombosis in severe pulmonary hypertension. Eur Respir J 1996;9:356-63.
153. Herve P, Humbert M, Sitbon O, Parent F, Nunes H, Legal C, et al. Pathobiology of pulmonary hypertension. The role of platelets and thrombosis. Clin Chest Med 2001;22:451-8.
154. Welsh CH, Hassell KL, Badesch DB, Kressin DC, Marlar RA. Coagulation and fi brinolytic profi les in patients with severe pulmonary hypertension. Chest 1996;110:710-7.
155. Hoeper MM, Sosada M, Fabel H. Plasma coagulation profi les in patients with severe primary pulmonary hypertension. Eur Respir J 1998;12:1446-9.
156. Eisenberg PR, Lucore C, Kaufman L, Sobel BE, Jaffe AS, Rich S. Fibrinopeptide A levels indicative of pulmonary vascular thrombosis in patients with primary pulmonary hypertension. Circulation 1990;82:841-7.
157. Altman R, Scazziota A, Rouvier J, Gurfi nkel E, Favaloro R, Perrone S, et al. Coagulation and fi brinolytic parameters in patients with pulmonary hypertension. Clin Cardiol 1996;19:549-54.
158. Tuder RM, Chacon M, Alger L, Wang J, Taraseviciene-Stewart L, Kasahara Y, et al. Expression of angiogenesis-related molecules in plexiform lesions in severe pulmonary hypertension: Evidence for a process of disordered angiogenesis. J Pathol 2001;195:367-74.
159. Akbiyik F, Ray DM, Gett ings KF, Blumberg N, Francis CW, Phipps RP. Human bone marrow megakaryocytes and platelets express PPARgamma,
and PPARgamma agonists blunt platelet release of CD40 ligand and thromboxanes. Blood 2004;104:1361-8.
160. Schönbeck U, Libby P. CD40 signaling and plaque instability. Circ Res 2001;89:1092-103.
161. Henn V, Slupsky JR, Gräfe M, Anagnostopoulos I, Förster R, Müller-Berghaus G, et al., CD40 ligand on activated platelets triggers an infl ammatory reaction of endothelial cells. Nature 1998;391:591-4.
162. Bodary PF, Vargas FB, King SA, Jongeward KL, Wickenheiser KJ, Eitzman DT. Pioglitazone protects against thrombosis in a mouse model of obesity and insulin resistance. J Thromb Haemost 2005;3:2149-53.
163. Li D, Chen K, Sinha N, Zhang X, Wang Y, Sinha AK, et al. The eff ects of PPAR-gamma ligand pioglitazone on platelet aggregation and arterial thrombus formation. Cardiovasc Res 2005;65:907-12.
164. Smyth SS, Jennings JL. PPARgamma agonists: A new strategy for antithrombotic therapy. J Thromb Haemost 2005;3:2147-8.
165. Cylwik D, Mogielnicki A, Buczko W. L-arginine and cardiovascular system. Pharmacol Rep 2005;57:14-22.
166. Fonseca VA, Reynolds T, Hemphill D, Randolph C, Wall J, Valiquet TR, et al. Eff ect of troglitazone on fi brinolysis and activated coagulation in patients with non-insulin-dependent diabetes mellitus. J Diabetes Complications 1998;12:181-6.
167. Kato K, Yamada D, Midorikawa S, Sato W, Watanabe T. Improvement by the insulin-sensitizing agent, troglitazone, of abnormal fi brinolysis in type 2 diabetes mellitus. Metabolism 2000;49:662-5.
168. Stenmark KR, Meyrick B, Galie N, Mooi WJ, McMurtry IF. Animal models of pulmonary arterial hypertension: The hope for etiological discovery and pharmacological cure. Am J Physiol Lung Cell Mol Physiol 2009;297:L1013-32.
169. Abe K, Toba M, Alzoubi A, Ito M, Fagan KA, Cool CD, et al. Formation of plexiform lesions in experimental severe pulmonary arterial hypertension. Circulation 2010;121:2747-54.
170. Nissen SE, Wolski K. Eff ect of rosiglitazone on the risk of myocardial infarction and death from cardiovascular causes. N Engl J Med 2007;356:2457-71.
171. Rosen CJ. The rosiglitazone story--lessons from an FDA Advisory Committ ee meeting. N Engl J Med 2007;357:844-6.
172. Dormandy JA, Charbonnel B, Eckland DJ, Erdmann E, Massi-Benedett i M, Moules IK, et al. Secondary prevention of macrovascular events in patients with type 2 diabetes in the PROactive Study (PROspective pioglitAzone Clinical Trial In macroVascular Events): A randomised controlled trial. Lancet 2005;366:1279-89.
173. Erdmann E, Dormandy JA, Charbonnel B, Massi-Benedett i M, Moules IK, Skene AM, et al. The eff ect of pioglitazone on recurrent myocardial infarction in 2,445 patients with type 2 diabetes and previous myocardial infarction: Results from the PROactive (PROactive 05) Study. J Am Coll Cardiol 2007;49:1772-80.
174. Lincoff AM, Wolski K, Nicholls SJ, Nissen SE. Pioglitazone and risk of cardiovascular events in patients with type 2 diabetes mellitus: A meta-analysis of randomized trials. JAMA 2007;298:1180-8.
175. Wilcox R, Bousser MG, Bett eridge DJ, Schernthaner G, Pirags V, Kupfer S, et al. Eff ects of pioglitazone in patients with type 2 diabetes with or without previous stroke: Results from PROactive (PROspective pioglitAzone Clinical Trial In macroVascular Events 04). Stroke 2007;38:865-73.
Source of Support: Atlanta Veterans Affairs Medical Center and the National Institutes of Health (R01 DK 074518). NHLBI T32 training grant
(HL076118-06), Confl ict of Interest: None declared.
Green, et al.: PPAR and pulmonary hypertension
Staying in touch with the Journal
1) Table of Contents (TOC) email alert Receive an email alert containing the TOC when a new complete issue of the journal is made available online. To register for TOC alerts go to
www.pulmonarycirculation.org/signup.asp.
2) RSS feeds Really Simple Syndication (RSS) helps you to get alerts on new publication right on your desktop without going to the journal’s website.
You need a software (e.g. RSSReader, Feed Demon, FeedReader, My Yahoo!, NewsGator and NewzCrawler) to get advantage of this tool. RSS feeds can also be read through FireFox or Microsoft Outlook 2007. Once any of these small (and mostly free) software is installed, add www.pulmonarycirculation.org/rssfeed.asp as one of the feeds.

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 48
Functional ion channels in human pulmonary artery smooth muscle cells: Voltage-dependent
cation channelsAmy L. Firth1, Carmelle V. Remillard2, Oleksandr Platoshyn2, Ivana Fantozzi2, Eun A. Ko3, Jason X.-J. Yuan2,3
1The Salk Institute for Biological Studies, La Jolla, California, USA, 2Department of Medicine, University of California, San Diego, La Jolla, California, USA, and 3Department of Medicine (Section of Pulmonary, Critical Care, Sleep and Allergy),
Institute for Personalized Respiratory Medicine, University of Illinois at Chicago, Chicago, Illinois, USA
ABSTRACT
The activity of voltage-gated ion channels is critical for the maintenance of cellular membrane potential and generation of action potentials. In turn, membrane potential regulates cellular ion homeostasis, triggering the opening and closing of ion channels in the plasma membrane and, thus, enabling ion transport across the membrane. Such transmembrane ion fl uxes are important for excitation–contraction coupling in pulmonary artery smooth muscle cells (PASMC). Families of voltage-dependent cation channels known to be present in PASMC include voltage-gated K+ (Kv) channels, voltage-dependent Ca2+-activated K+ (Kca) channels, L- and T- type voltage-dependent Ca2+ channels, voltage-gated Na+ channels and voltage-gated proton channels. When cells are dialyzed with Ca2+-free K+- solutions, depolarization elicits four components of 4-aminopyridine (4-AP)-sensitive Kvcurrents based on the kinetics of current activation and inactivation. In cell-attached membrane patches, depolarization elicits a wide range of single-channel K+ currents, with conductances ranging between 6 and 290 pS. Macroscopic 4-AP-sensitive Kv currents and iberiotoxin-sensitive Kca currents are also observed. Transcripts of (a) two Na+ channel α-subunit genes (SCN5A and SCN6A), (b) six Ca2+ channel α−subunit genes (α1A, α1Β, α1Χ, α1D, α1E and α1G) and many regulatory subunits (α2δ1, β1-4, and γ6), (c) 22 Kv channel α−subunit genes (Kv1.1 - Kv1.7, Kv1.10, Kv2.1, Kv3.1, Kv3.3, Kv3.4, Kv4.1, Kv4.2, Kv5.1, Kv 6.1-Kv6.3, Kv9.1, Kv9.3, Kv10.1 and Kv11.1) and three Kv channel β-subunit genes (Kvβ1-3) and (d) four Kca channel α−subunit genes (Sloα1 and SK2-SK4) and four Kca channel β-subunit genes (Kcaβ1-4) have been detected in PASMC. Tetrodotoxin-sensitive and rapidly inactivating Na+ currents have been recorded with properties similar to those in cardiac myocytes. In the presence of 20 mM external Ca2+, membrane depolarization from a holding potential of -100 mV elicits a rapidly inactivating T-type Ca2+ current, while depolarization from a holding potential of -70 mV elicits a slowly inactivating dihydropyridine-sensitive L-type Ca2+ current. This review will focus on describing the electrophysiological properties and molecular identities of these voltage-dependent cation channels in PASMC and their contribution to the regulation of pulmonary vascular function and its potential role in the pathogenesis of pulmonary vascular disease.
Key Words: Ca2+ channel, K+ channel, membrane potential, Na+ channel, pulmonary hypertension
Access this article online
Quick Response Code:Website: www.pulmonarycirculation.org
DOI: 10.4103/2045-8932.78103
Pulm Circ 2011;1:48-71
Address correspondence to:Prof. Jason X.-J. YuanDepartment of Medicine (Section of Pulmonary, Critical Care and Sleep and Allergy), Institute for Personalized Respiratory Medicine,University of Illinois at Chicago, COMRB Rm. 3131 (MC 719),909 South Wolcott Avenue, Chicago, Illinois 60612, USAE-mail: [email protected]
INTRODUCTION
Intracellular ion homeostasis, cell volume and membrane excitability are all important mechanisms regulated by the membrane permeability to cations and anions. It is this transmembrane ion flux that is the predominant factor in controlling excitation–contraction (EC) coupling mechanisms in pulmonary artery smooth muscle cells
(PASMC). Electromechanical and pharmacomechanical coupling processes are the two major EC coupling mechanisms. Of these, it is the electric excitability that plays an important role in EC coupling in the pulmonary vasculature,[1,2] predominantly controlled
Review Ar t ic le

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 49
by the transmembrane ion flux in PASMC. Indeed, many vasoactive substances also alter the membrane potential (Em) in these cells.[3,4] Expression and functionality of ion channels in the plasma membrane is also important in modulation of cell motility, migration and proliferation by governing the cytoplasmic free Ca2+ concentration ([Ca2+]cyt).
A rise in [Ca2+]cyt in PASMC triggers pulmonary vasoconstriction[5] and stimulates cell proliferation[6] and migration,[7] leading to pulmonary vascular remodeling.[8] The mechanisms involved in the regulation of [Ca2+]cyt directly control vasomotor tone and vascular wall thickness; two major determinants of pulmonary vascular resistance (PVR). Because PVR is inversely proportional to the fourth power of the radius (r) of the pulmonary arterial lumen (PVR=8Lη/πr4), a very small change in r would thus cause a large change in PVR. As a consequence, pulmonary vasoconstriction will also increase PVR by reducing the arterial radius. Pulmonary arterial pressure (PAP), a diagnostic criterion for PAH, is a product of PVR and cardiac output. Pulmonary vasoconstriction and vascular medial hypertrophy caused by excessive PASMC proliferation and migration contribute considerably to the elevated PVR in patients with pulmonary hypertension. Indeed, dysfunction of a number of ion channels has been implicated in a variety of cardiopulmonary diseases, such as pulmonary arterial hypertension,[8,9] spontaneous genetic systemic arterial hypertension[10-13] and heart failure.[14] Therefore, defining the molecular identities and electrophysiological properties of plasmalemmal ion channels in human PASMC will help to enhance our understanding of normal EC coupling mechanisms, to
define the pathogenic roles of ion channels in pulmonary vascular disease and to develop new therapeutic approaches for patients with pulmonary hypertension.
As mentioned above, EC coupling requires a change in membrane potential to alter vascular tone. Ion channels are sarcolemmal pores selectively permeable to either cations (Na+, Ca2+, K+) or anions (Cl-). Both anions and cations are distributed on either side of the cell membrane, and their transmembrane movement is based on their electrochemical gradient, a potential- and concentration-based driving force for the ions, i.e. flowing from more-concentrated to less-concentrated zones and, for cations, from positive or less-negative sites to those with a more negative membrane potential. In human cells, Na+ (~140 mM) and Ca2+ (~2 mM) are the dominant cations in the external fluid (concentrations similar to those found in blood plasma), whereas K+ (~140 mM) is the dominant cation in the cell cytoplasm. Cl-, the most dominant anion in vascular smooth muscle cells,[15] is unevenly distributed between the cytosol and the extracellular fluids, and plays an important role in controlling osmolarity, cell volume, excitability and ion homeostasis [Table 1]. Additionally, ion channels expressed in the plasma membrane also play important roles in the regulation of secretion, migration, proliferation, differentiation and apoptosis. In vascular smooth muscle cells, the resting Em is predominantly regulated by the permeability and the concentration gradients of K+ across the plasma membrane. The reason that the resting Em (-40 to -55 mV) in vascular smooth muscle cells is not equal to the K+ equilibrium potential (approximately -85 mV) indicates that other cation (e.g., Na+ and Ca2+) and anion (e.g., Cl-) channels also
Firth, et al.: Ion channels in human PASMC
Table 1: Ionic composition of extracellular and intracellular solutions used for measurement of various ion channel currentsCurrent Na+ Ca2+ K+ Mg2+ Cl- Cs+ ATP EGTA Glu HEPES pH
Type mM mM mM mM mM mM mM mM mM mM
INa (whole cell)Bath 141 - 4.7 3 151.7 - - 1 10 10 7.4Pipette 10 - - 4 143 135 5 10 - 10 7.2
ICa (whole cell)Bath 110 20 4.7 1.2 157.1 - - - 10 10 7.4Pipette 10 - - 4 143 135 5 10 - 10 7.2
IK(V) (whole cell)Bath 141 - 4.7 3 151.7 - - 1 10 10 7.4Pipette 10 0 135 4 143 - 5 10 - 10 7.2
IK(Ca) (whole cell)Bath 141 1.8 4.7 1.2 151.7 - - - 10 10 7.4Pipette 10 0 (8.8) 135 4 143 - 5 - (10) - 10 7.2
IK(Ca) (cell attached)Bath 141 1.7 4.7 1.2 151.7 - - - 10 10 7.4Pipette 10 - 125 4 129 - 5 0.1 - 10 7.2
IK(V) (cell attached)Bath 141 1.8 4.7 1.2 151.7 - - - 10 10 7.4Pipette 5 0 137 1.2 143.2 - 5 0.1 0 10 7.2

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 50
Firth, et al.: Ion channels in human PASMC
contribute to regulating the Em. This review will provide an in-depth summary of the molecular identities and electrophysiological properties of voltage-dependent cation channels in PASMC, focusing on Na+ and Ca2+ channels, which are opened by membrane depolarization and responsible for cell excitation, and voltage-gated Kv and Kca channels, which are responsible for controlling resting Em and repolarization when the cells are stimulated.
Passive cell membrane properties of human PASMCThe whole-cell patch clamp configuration[16] may be likened to an electrical circuit [Figures 1 and 2a]. A capacitor is made with two charged surfaces separated by a dielectric substance. The pipette itself is such a dielectric substance with two charged surfaces and, therefore, is represented by a capacitor in the circuit. Pipette capacitance (Cp, measured in Farads, F) is complicated in character, but its contribution to the overall circuit is usually minimized electronically by injecting a current transient designed to pre-charge the glass surface to the new desired potential. The pore of the pipette presents a resistance to current flow that may be easily measured before seal formation (Re, measured in Ohms, Ω). During whole-cell access, however, this resistance is increased by further resistance to current flow due to the contents or geometry of the cell itself (“series resistance” or “access resistance,” Ra), i.e. resistance to filling the entire cytosolic space with the desired amount of charge or potential due to interaction of charges with proteins or due to limited flux through long cell processes or narrow cell geometry.
Once the cytosolic space of the cell is voltage clamped, the cell membrane also presents its own capacitance. Unlike the pipette, the cell membrane is of relatively uniform thickness and uniform dielectric content (lipids); therefore, in most cells, the specific membrane capacitance (Cm), which is normalized by the area of the plasma membrane, is ~1 μF/cm2,[17] and a measure of the cell capacitance is a good indicator of cell size. The cell membrane itself is a very good dielectric, presenting a resistance of several gigaOhms (gigaΩ) when the membrane channels are closed at rest, in effect stopping the flow of charge across the membrane. However, the membrane resistance (Rm) is strongly influenced by the presence of ion conductances through the membrane ion channels.
Ion channels are selectively permeable to specific cations, and have a gating mechanism that may be controlled by voltage or other methods. Ion channels produce a conductance (g, measured in Siemens, S) that is dependent on the transmembrane electrical potential energy (∆E, or Em, measured in Volts, V), and defined by Ohm’s law, Ix=gE, where Ix is the conductance or current
through that particular type of channel. Because Ohm’s law defines resistance as the inverse of conductance, the overall membrane resistance is the inverse of the sum of all the conductances present on the membrane. The simple measurement of overall membrane resistance is therefore a good indicator of the amount of current carried through all the open channels on the membrane. As many membrane channels are voltage dependent, the membrane resistance likewise varies with membrane potential.
By employing a small hyperpolarizing command voltage step (Vcomm), for example from -70 mV to -85 mV (close to
VcomI
Cell-attached Whole-cell
a
Am
plitu
deVcom
I
-70 mV
+80 mV
Open probability
Closedduration
Openduration
Activation DeactivationInactivation
b
c
K+K+
Ca2+
Na+
K+
K+
K+K+
Ca2+
Cell-attached
Whole-cell
Am
plitu
de
Approachcell
Attachto cell
Makeseal
Break intocell
Figure 1: Patch-clamp electrophysiology. (a) Formation of the giga seal and the subsequent cell-attached and whole-cell configurations. (b) Enhanced view of the membrane–pipette arrangements in the cell-attached and whole-cell confi gurations. In a cell-attached patch, unitary currents are produced by ion fl ux through single channels. Three different channel types are shown. In the whole-cell mode, the macroscopic current recorded is the summation of all the currents generated by similar channels throughout the cell. (c) Measured parameters. Single-channel recordings can provide information relating to the amplitude the unitary currents, the open probability of the channels and the amount of time the channel(s) spend in open (open duration) or closed (closed duration) confi gurations. Macroscopic currents are characterized by the current amplitude, activation, inactivation and deactivation during a pulse protocol

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 51
Firth, et al.: Ion channels in human PASMC
the equilibrium potential for K+), current transient (Itran) is induced [Figure 2b]. The cell membrane capacitance (Cm) can then be determined by pClamp software based on the equation: Cm=(integral of Itran)/)Vcomm). The membrane input resistance (Rm) is then calculated from the equation: Rm=(Rtotal×Rseal)/(Rseal -Rtotal), where Rseal and Rtotal are the resistance determined, respectively, from the steady currents of Itran in response to Vcomm (-5 mV) before and after break-in. As shown in Figure 2c, Cm can range from 15 pF to 45 pF, with an average Cm of 34±5 pF measured in 220 PASMC. The specific membrane capacitance can be calculated from the mean values of Cm and cell surface
(capacitative) area; for PASMC, this is in the region of 1.25 μF/cm2, similar to the 1.3 μF/cm2 reported in rat caudal artery smooth muscle cells.[18] Rm under resting conditions is usually very high in the vascular smooth muscle cells.[19] Indeed, the calculated Rm in PASMC ranges from 1 GΩ to 12 GΩ, with an average Rm of 5±1 GΩ (n=171) [Figure 2d]. Importantly, the duration of PASMC in cell culture conditions does not significantly alter the values for Cm and Rm [Figure 2e and f].
Membrane potential can be measured in the current-clamp (I=0) mode. The resting Em in cultured human PASMC is approximately -45±5 mV [Figure 3a], and is slightly less negative than that observed in freshly dissociated PASMC from animals.[20,21] As previously mentioned, Em is less negative than the EK (approximately -85 mV), which suggests that Em in these cells is also controlled by the permeability of other ions (e.g., Na+, Ca2+ and Cl-). The equilibrium potentials for Na+, Ca2+ and Cl- are believed to be +66, +122 and -26 mV, respectively, in native vascular smooth muscle cells.[15] In some PASMC, spontaneous electrical activity has been observed under resting conditions [Figure 3b], suggesting that these cells are electrically excitable.[22] This spontaneous electrical activity in PASMC is dependent upon the presence of extracellular Ca2+ [Figure 3b].[2,23-25]
Evolution and diversity of the pore-forming voltage-gated cation channelsIon-selective voltage-gated cation channels generate electrical activity in cells by undergoing rapid conformational changes from an impermeable structure to a highly permeable pore in the membrane through which ions can pass. Based on inherent similarities
Figure 3: Electrically active human pulmonary artery smooth muscle cells (PASMC). (a) Histogram showing the wide distribution of resting Em in human PASMC. Em was measured in the current clamp (I=0) mode. (b) Spontaneous action potentials recorded in human PASMC are abolished when external Ca2+ is removed. Electrical activity is restored upon return to normal physiological Ca2+ (1.8 mM)
Em (m
V)
-60
-40
-20
0
20
-75 -70 -65 -60 -55 -50 -45 -40 -35 -30 -25 -20 -15 -10
1 min0Ca
b
a
Resting E m (mV)
Cel
l Num
ber
0
10
20
30 mean Em = -45.2 mV
Cel
l Num
ber
010203040506070
Cm (pF)
0 1 2 3 4 5 6 7 8 0 1 2 3 4 5 6 7 80
10
20
30
40
50
5 1015 2025 30354045 50 1 2 3 4 5 6 7 8 9101112
Time in culture (day)
Cm
(pF)
Rm (G Ω)
Rm
(GΩ
)C
ell N
umbe
r
0
10
20
30
40
50
012345678
Time in culture (day)
-70 mV-80 mV
200 pA1 ms
Seal
Break-in
b
c
e
d
a
f
Cell
Cm
Rm
CpRe Electrode
Figure 2: Passive membrane properties of human pulmonary artery smooth muscle cells (PASMC). (a) The cell and pipette form a circuit in the whole-cell patch-clamp confi guration. Membrane capacitance (Cm) and resistance (Rm) are indicators of cell size and transmembrane ion fl ux, respectively. (b) Cm is often used to indicate that the membrane is ruptured. In the cell-attached confi guration (“Seal”), Cm, measured as the surface area under the transient spikes, is small. Upon whole-cell access (“Break-in”), Cm is greatly increased. (c and d) Frequency distribution of Cm and Rm within a cell population. (e and f) Cm (n=220) and Rm (n=171) of human PASMC do not vary over time in culture

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 52
Firth, et al.: Ion channels in human PASMC
in the transmembrane domain structure of Na+, Ca2+ and K+ channel pore-forming α subunits, it is widely agreed upon that voltage-gated cation channels share a common ancestor. The basic building block of all these channels is a one-domain (1D) two-transmembrane segment (2TM) protein with an ion-selective pore/loop region between the transmembrane segments,[26] reminiscent of prokaryotic and eukaryotic K+-selective inward rectifier channels [Figure 4]. Indeed, K+ channels are the oldest of the voltage-gated cation channels as examples of these have been found in both prokaryotic and eukaryotic organisms.[27] Over time, multiple gene duplications and modifications elaborated this channel by the addition of four transmembrane segments, forming 1D six-transmembrane segment (6TM) protein that constitutes the basic pore-forming α−unit of mammalian voltage-gated cation channels. From this point, the evolution of voltage-gated ion channels diverged, with ion selectivity being a key element to channel diversification. Figure 4 provides a simple phylogenetic tree of voltage-gated cation channels based on sequence identity and domain arrangement.
K+ channels evolved into the most diverse family of channels, mainly due to the sheer number of α−subunits and possible α4β4 subunit combinations. Four superfamilies of human K+ channels have maintained the 1D-6TM motif, and multiple α−subunits have surfaced for each: ether-a-go-go (eag, erk, elk; 3 isoforms in human), KQT (5 isoforms in humans), Kca (maxi-Kca and SKca; 6 isoforms in humans) and Kv (11 subfamilies and ≥30 isoforms) (see Coetzee et al. for review[28]). The sequence identity varies greatly within (e.g., 35–88% identity between Kv1 and Kv9) and between (e.g., 8–17% identity between Kv and Kca) the families.[28] Chromosomal site analysis of the known human isoforms also suggests that K+ channels have existed for a long time. Genes encoding 1D-6TM K+ channels are found on at least 13 human chromosomes, with little evidence of clustering of genes except in the case of a few Kv channels (Figure 5 depicts the chromosomal location of channel pore-forming and regulatory subunits identified in human PASMC). Kv channel α−subunits alone can be found on 10 chromosomes within the human genome.
Na+ and Ca2+ channels evolved after K+ channels were well established.[27] A few theories have been put forth to explain the development of four-domain (4D) -6TM channels from 1D-6TM channels:[26] (a) two rounds of gene duplication of 1D-6TM K+ channels (1D÷2D, 2D÷4D) and mutations within the pore region to alter ion selectivity created the 4D-6TM Ca2+ and Na+ channels.[26] Coupled with mutations within the pore to alter ion selectivity, this evolutionary cascade would have produced the 4D-6TM Ca2+ and Na+ channels. (b) 1D- and 4D-6TM channels
have a common 1D-6TM cyclic-nucleotide gated (CNG) channel ancestor, with S4 and pore regions similar to voltage-gated K+, Ca2+ and Na+ channels. In addition to structural similarities, CNG channels also exhibit some voltage sensitivity and are permeable to both monovalent and divalent cations, making it an ideal common precursor.[26] (c) More recently, Durell and Guy[29] showed that a Ca2+ channel with a 1D-6TM motif could be detected in the akylaphilic bacterium Bacillus halodurans\pard plain. This suggests that more mutations conferring Ca2+ selectivity in bacterial 1D-6TM channels occurred before any gene duplication occurred and prior to the development of lower eukaryotes (protozoans), where 4D-6TM Ca2+ channels have been identified.[26,29]
The first 4D-6TM proteins were voltage-dependent Ca2+ channels (VDCC), with early gene identification revealing multiple channels within the same tissue or cell. Eventually, Ca2+ channels were classified as low-voltage activated (LVA) or high-voltage activated (HVA) VDCC (see below and Catterall[30] for review). Ca2+ influx via VDCC has already been established as an effector or trigger in numerous cellular processes, with the different channel subtypes sometimes playing different roles. The variety of functional roles for VDCC correlates well with the significant structural diversity between the 10 VDCC α subunits currently identified (α1A-1I, α1S).[30] Although the six isoforms identified in human PASMC represent each of the five
Figure 4: Proposed phylogenetic tree depicting the evolution of voltage-dependent cation channels. Pore-forming unit isoforms representing each channel are shown in parentheses. (TM – Transmembrane domain; D – Domain; KT – Two-pore domain K+ channel; KIR – Inward rectifi er K+ channel; KATP – ATP-sensitive K+ channel; HVA – High-voltage activated; LVA – Low-voltage activated; Kv – Voltage-gated K+ channel; KQT – Long-QT K+ channel; Kca – Ca2+-activated K+ channel; SK – small-conductance Ca2+-activated K+ channel)
(α1C, D, F, S)
4 D
eag Kv KQT KCa
Shaker(Kv1)
Shab(Kv2)
Shaw(Kv3)
Shal(Kv4)
silent(Kv5-6,Kv8-9)
other(Kv10,Kv11)
Slo(α1)
SK(1-4)
HVACaL CaT
(α1G-I)
1 D
Ca(bac) 1.1
LVA
1 D
CaN(α1B)
CaR(α1E)
CaP/Q(α1A)
Na(SCN1A-11A)
6 TM
2 TM2 D
KT KIR/KATP1 D
?
S1 S2

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 53
Ca2+ channel subtypes, there is only electrophysiological evidence for the L- and T-type channels in PASMC[31,32] (also see below). As for voltage-gated K+ channels, the associated genes are encoded on at least five human chromosomes, with no grouping of α−subunits encoding for similar currents on the same chromosome. For example, α1C and α1D, both encoding for L-type VDCC in human PASMC, are located on chromosomes 12 and 3, respectively, while those encoding for T-, N-, R- and P/Q-type channels are scattered on chromosomes 17, 9, 1 and 19, respectively [Figure 5]. Furthermore, while the structure of T-type VDCC is very similar to that of LVA channels, the sequence identity between them is <25%, implying that the HVA and LVA subfamilies represent radically different evolutionary branches.[26]
Like T-type Ca2+ currents (ICa(T)), Na+ currents are rapidly activating transient currents activated at more negative membrane potentials. In lower eukaryotes, Ca2+ was the primary charge carrier;[26] purely Na+-dependent action potentials were not common until the advent of the
early metazoans. This has led to speculation that low-voltage activated and rapidly activating Na+ channels evolved from Ca2+ channels in parallel with the evolution of the first nervous systems. Sequence analysis has shown that ligand-binding sites (e.g., carboxy-terminal calmodulin-binding site) may be conserved within the 4D-6TM voltage-gated Ca2+ and Na+ channels, suggesting a similar evolutionary precursor.[33,34] Of particular interest is a putative calmodulin (CaM)-binding site located in the carboxy-terminal regions of both Na+ and Ca2+ channels.[33,34] Cloning of the first LVA channels verified that voltage-dependent Na+ channels did evolve from T-type VDCC.[35] Eleven known Na+ channel α−subunit genes (SCN1A-11A) bearing strong biophysical and sequence (~75% sequence identity) similarities have been identified in the skeletal, cardiac and uterine muscles and in the human brain,[26,36,37] and bear approximately 75% sequence identity to each other.[26] Because the isoforms bear strong similarities, even when expressed in heterologous systems, voltage-gated Na+ channels are not generally grouped into families like their Ca2+
Firth, et al.: Ion channels in human PASMC
Figure 5: Chromosomal location of ion channel genes expressed in human pulmonary artery smooth muscle cells (PASMC). All isoforms of pore-forming and regulatory subunits of Na+, voltage-dependent Ca2+ channels, Kv, and Kca channels identifi ed in human PASMC are shown. Chromosomal location is based on the primer sequences described in Table 2
Chromosomal Location of Ion Channel Genes Expressedin Human Pulmonary Artery Smooth Muscle Cells
50 millionnucleotidepairs
1 μm
VDCC-α1G
1
K -SK3
Kvβ-2
VDCC-α1E
2 3
MaxiK-β2MaxiK- 3β
Kvβ -1
12 VDCC- 1α C
Kv1.1
Kv1.5Kv1.6
MaxiK-β4
11
Kv3.1
Kv1.4
10
VDCC-β2
MaxiK-α 1
16
Kv6.3
VDCC-α1A
Kv3.3
KCa-SK4Kv1.7VDCC-γ6
20
Kv2.1Kv6.1Kv9.1
SCN2A
SCN1B
SCN3A SCN2B
SCN7A
SCN4A
SCN9A
SCN11A
Kv5.1Kv9.3
Kv10.1(Kv6.3)* 9
Kv11.1
VDCC-α1 B
VDCC 4β
VDCC-α1D
VDCC-β3SCN8A
VDCC-β1
17Kvβ-3
19
Kv1.3Kv3.4
Kv1.10Kv1.2
5
KCa
Ca
-SK2
MaxiK-β1X
Kv4.1
7
VDCC-α2δ1
Kv4.2
Kv6.2
18

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 54
-80 mV
-60 mV
-40 mV
-20 mV
0 mV
+20 mV
+40 mV
+60 mV
+80 mV
-70 mV
10 ms50 pA
0 mV
-120 mV
-20 mV
-70 mV
5 ms50 pA
Cont
V (mV)I/
I max
(%)
0
25
50
75
100
-120 -80 -40 0
g Na/g
Na,
max
(%)
0
25
50
75
100
NMG Wash
50 pA
WashTTXCont
5 ms
5 ms
V (mV)
-500I (pA)
0 mV
-70 mV
50 pA
a
b
ca
b
-80 mV
-80 mV
TP
ms
I (%)
02 3 4
8 16 24
5
100
ms
I (%)
0
100
-80 -40 80 40
Figure 6: Electrophysiological and pharmacological properties of voltage-gated Na+ currents (INa(V)) in human pulmonary artery smooth muscle cells (PASMC). Cells are dialyzed with a Cs+-containing pipette solution [Table 1]. (a) Representative currents were elicited by depolarizing the cell to from a holding potential of –70 mV to test potentials between –80 mV and +80 mV (protocol at bottom). Upper left inset: Steady-state activation and inactivation of currents occurred within <5 ms and <16 ms, respectively. Lower right inset: Summarized INa(V) I-V relationship. (b) Currents were evoked by a step depolarization to 0 mV from different conditioning potentials (-120 mV and -20 mV) applied for 10 s prior to the test depolarization (left). Voltage-dependent steady-state availability (I/Imax) and normalized conductance-voltage relationship (gNa/gNa, max) of the peak INa(V) amplitude. The I/Imax and gNa/gNa, max curves were best fi tted using exponential and Boltzman equations, respectively. (c) INa(V) is completely suppressed by equimolar replacement of extracellular Na+ with N-methyl-D-glucamine (NMG) or extracellular application of 1 μM tetrodotoxin. Currents were elicited by step depolarizations from –70 mV to 0 mV
currents determined by the overlap between the activation and inactivation curves are in the voltage range of -60 to -20 mV in human PASMC cultured in growth medium [Figure 6b, right panel]; these values are similar to those in other vascular smooth muscle cells, suggesting the participation of Na+ currents in the regulation of resting Em in human PASMC.
Firth, et al.: Ion channels in human PASMC
and K+ counterparts. The SCN5A and 6A isoforms expressed in PASMC are typically found in cardiac and uterine muscle. Unlike K+ and Ca2+ channel α−subunit genes, all Na+ channel α−subunit genes map within four chromosomes (2, 3, 12 and 17) containing homeobox (HOX) gene clusters.[37] HOX genes have been predicted to have existed in ancestral chordates, suggesting that the initial expansion of Na+ channels is associated with multiple chromosome duplications occurring after the divergence from invertebrate to pre-vertebrate chordates. The fact that many of the SCN genes are clustered on two chromosomes also suggests that intrachromosomal duplications also occurred over time.
Voltage-gated Na+ ChannelsIn a variety of excitable cells, including smooth muscle cells, voltage-gated Na+ channels are responsible for generating action potentials. Activation of the channels induces membrane depolarization and thus increases [Ca2+]cyt by promoting Ca2+ influx through the sarcolemmal VDCC and the reverse mode Na+/Ca2+ exchanger.[38,39] While the activation of Na+ channels may underlie the spontaneous action potentials observed in cardiac and skeletal muscle myocytes,[40] removal of extracellular Ca2+ abolished spontaneous action potentials in PASMC [Figure 3b], suggesting that the electrical excitability of PASMC is induced by multiple ion channel functions. Furthermore, voltage-gated Na+ channels may serve as a pathway for Ca2+ entry under physiological and pathophysiological conditions.[41,42]
Biophysical properties of voltage-gated Na+ currents (INa)The inward INa(V) observed in PASMC possesses similar biophysical and pharmacological characteristics to those previously identified in other human vascular smooth muscle cells:[39,43-46] sensitivity to tetrodotoxin (≤1 μM for total inhibition), -60 to -50 mV activation threshold, -15 to 10 mV peak amplitude potential, -70 to -65 mV half-inactivation voltage (τinact ≤4 ms) and -25 to -15 mV half-activation voltage (τact ~1 ms). In cultured human PASMC dialyzed with Cs+-containing solution, a rapidly inactivating inward Na+ current is observed in the absence of extracellular Ca2+ [Figure 6a]. As mentioned above, the current activates at potentials close to -60 mV and peaks at approximately +10 mV [Figure 6a]. These currents also inactivate rapidly, with the half-inactivation (V0.5) occurring at approximately -65 mV and complete inactivation occurs at -20 mV [Figure 6b]. Equimolar replacement of external Na+ with N-methyl-D-glucamine (NMDG) or extracellular application of 1 μM tetrodotoxin (TTX) is sufficient to abolish the currents [Figure 6c], suggesting that the currents in PASMC are carried by Na+ influx through the TTX-sensitive, voltage-gated Na+ channels similar to those described in neurons and cardiomyocytes.[40] The window

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 55
NH2NH2 COOH
NH2
β1 S1 S2 S6S3 S4 S5 S1 S2 S6S3 S4 S5 β2S1 S2 S6S3 S4 S5 S1 S2 S6S3 S4 S5+
+
+
+
+
+
+
+
COOH
a
COOH
Voltage-dependent Na + Channel
α subunit β subunitβ subunit
b
0.1
c
M 6A4A 5ASCN
bp300 Br
PA300
Br
PA
2Bbp
200
300
M 2A1A 1BSCN
M 3A 3BSCN
bpBr
PA
300
300
650GAPDH
11AM 9A7A 8A 10ASCN
300bp
300
Br
PA
M
SCN6A
SCN7A
SCN1B
SCN2B
SCN10A
SCN11A
SCN2A
SCN5A
SCN9A
SCN1A
SCN4A
SCN8A
SCN3A
SCN3B
Figure 7: Molecular identity of voltage-gated Na+ channels in human pulmonary artery smooth muscle cells (PASMC). (a) Structural arrangement of Na+ channel α-, β1- and β2-subunits. (b) The mRNA expression of cloned Na+ channels in human brain (Br) and PASMC (PA). Polymerase chain reaction (PCR)-amplifi ed products displayed for the transcripts of SCN2A, SCN4A, SCN5A, SCN6A and β-actin. “-RT”, PCR performed with no reverse transcriptase (RT). “M”, 100 bp DNA ladder. (c) A phylogenetic tree showing the inferred evolutionary relationships among different Na+ channel genes
Voltage-gated Na+ channel genes expressed in human PASMCA complex of three glycoprotein subunits form functional Na+ channels: a pore-forming α−subunit and two β-subunits that modulate channel gating and membrane expression [Figure 7a].[47] The α−subunit alone can form a functional channel and is composed of four domains, each containing six transmembrane segments (S1–S6) and a pore loop (P region). Each S4 segment is believed to act as a voltage sensor, while the S5-pore loop-S6 segments form the transmembrane pore itself. Using reverse transcriptase-polymerase chain reaction (RT-PCR), seven Na+ channel-related gene transcripts (SCN1B, 2A, 2B, 4A, 8A, 9A and 11A) have been detected in PASMC [Figure 7b]. Transcripts for SCN5A and SCN6A have
not yet been detected in PASMC. All of these isoforms are expressed in the brain [Figure 7b]. The combined functional and molecular identification of Na+ currents and channels in human PASMC suggest that voltage-gated Na+ channel activity and expression may relate to PASMC excitability, contractility, proliferation and differentiation.
Phenotypical change of voltage-gated Na+ channel expression in freshly dissociated and cultured VSMCVoltage-gated TTX-sensitive Na+ currents (INa(V)) have been described in several types of human vascular smooth muscle cells cultured from the aorta[43,44] and coronary[39,46] and pulmonary[43,45] arteries. On only rare occasions have INa(V) been recorded in freshly dissociated human vascular
Firth, et al.: Ion channels in human PASMC

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 56
smooth muscle cells, although they are readily detected when the same cells are cultured.[46] Although it may be due to a technical problem (e.g., the rapid inactivation of the currents and the large size of most freshly dissociated smooth muscle cells to record INa(V)), the relative inability to detect INa(V) in freshly dissociated, but not cultured, cells from the same vascular bed may bear some relation to cell dedifferentiation and proliferation.[46] More specifically, voltage-gated Na+ channel expression and activity may be required to facilitate the transition from a “contractile” to “synthetic” or “proliferative” phenotype.[48,49] However, INa(V) have been recorded in both freshly dispersed rabbit[24] and cultured human[45] PASMC. This raises the possibility that the development and expression of functional voltage-gated Na+ channels in cultured cells acts as a trigger for cell differentiation and proliferation, possibly via enhanced [Ca2+]cyt, as discussed below.
Functional properties of voltage-gated Na+ channels in human PASMCNa+ channels appear to play an important role in the regulation of [Ca2+]cyt and sarcolemmal Ca2+ influx by different mechanisms. Firstly, in cardiac myocytes, enhanced TTX-sensitive INa(V) causes a localized transient increase in [Na+]cyt, thereby activating reverse-mode Na+/Ca2+ exchange and increasing [Ca2+]cyt with the subsarcolemmal space between the plasma membrane and SR.[41] The Ca2+ newly introduced into the cytoplasm can then trigger further Ca2+ release from the SR (which ultimately will cause contraction and stimulate proliferation and migration) or replenish SR Ca2+ pools by Ca2+-ATPase-mediated re-uptake.[42,50] Secondly, TTX-sensitive Na+ channels are promiscuous, i.e. they can allow permeation of other cations (such as Ca2+) under certain conditions (e.g., absence of extracellular Na+, presence of tracing doses of steroids such as ouabain and digoxin).[42,51] Ca2+ influx through promiscuous Na+ channels can contribute to local and global cardiac Ca2+ signaling, especially in heart failure patients treated with digoxin.[52] In addition to its modulating [Ca2+]cyt, the permeability of Na+ channels to Ca2+ may also play a role in the contractile-to-proliferative cellular transition. Thirdly, voltage-gated Na+ channels are essential in the generation of action potentials in many excitable cells, thereby regulating [Ca2+]cyt based on evidence from expressed SCN5A channels,[33,53] we can speculate that Ca2+/CaM-mediated regulation of voltage-gated Na+ channels may play an important role in the coupling of human PASMC excitation and contraction.
VDCCIn excitable cells, the opening of VDCC is a critical mechanism responsible for muscle contraction induced by neuronal and humoral stimulation. There are at least five types of VDCC described in neurons and
cardiomyocytes: L-type, T-type, P/Q-type, R-type and N-type.[54,55] These Ca2+ channels have been sorted based on their electrophysiological, pharmacological, kinetic and molecular properties. VDCC have also been separated into two groups based on their activation voltage. HVA VDCC include all but T-type channels, with the latter classified as LVA VDCC. HVA channels activate at membrane potentials between -50 mV and -20 mV, while LVA channels activate at more negative potentials approximating -70 mV. Typically, only currents generated by L- and T-type channels have been measured in cardiovascular tissues, while all current types have been recorded in neuronal tissues.[54]
Whole-cell VDCC currents (ICa)In human PASMC, a large, slowly inactivating inward Ca2+ current is observed when cells are held at -70 mV and depolarized to 0 mV [Figure 8a]. The current activates close to -20 mV, with a maximal activation of approximately +15 mV. Removal of extracellular Ca2+ abolishes the currents, confirming that the currents are due to Ca2+ influx. Nifedipine, a dihydropyridine blocker of VDCC, is also able to significantly inhibit the currents. The currents present in PASMC are, therefore, mainly due to Ca2+ influx through dihydropyridine-sensitive L-type Ca2+ channels. Less frequently, and while being held at a very negative potential (-100 mV), depolarization to a test potential to -20 mV can elicit a rapidly activating transient inward Ca2+ current [Figure 8b and c]. This transient
epyT-T epyT-L
0 mv-70 mv
-20 mv
-100 mv
a b
50 ms100 pA
Time (ms)
I/I m
ax (%
)
00 5 10 15 0 80 160 24020 25
20
40
60
80
100
Time (ms)
I / I m
ax (%
)
0
20
40
60
80
100
L
T
cT
L
Figure 8: Electrophysiological and pharmacological properties of L- and T-type voltage-dependent Ca2+ currents (ICa) in human pulmonary artery smooth muscle cells (PASMC). Cells were dialyzed with a Cs+-containing pipette solution [Table 1]. (a) A representative current (L-type ICa), elicited by depolarizing a cell from a holding potential of -70 mV to 0 mV. (b) A representative current (L-type ICa), elicited by depolarizing a cell from a holding potential of -100 mV to -20 mV. (c) Activation (left) and inactivation (right) kinetics of L-type and T-type ICa
Firth, et al.: Ion channels in human PASMC

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 57
current activates and inactivates rapidly in comparison with the L-type current [Figure 8a], with a threshold potential for activation of approximately -36 mV at a holding potential of -90 mV. The biophysical properties of these currents are very similar to the T-type Ca2+ current observed in aortic[56] and renal artery[57] smooth muscle cells, rat PASMC[58] and cardiomyocytes.[59]
Endogenously expressed genes that encode VDCC in human PASMCAs for voltage-gated Na+ channels, the pore-forming VDCC α1-subunits (10 identified isoforms) are composed of four, six transmembrane segment domains [Figure 9a] that, when expressed alone, can create functional channels.[47] The pore-forming S5-loop-S6 segments and the voltage-sensing S4 segments are integral to the function of α1-subunits. Three different regulatory subunits are also part of the greater Ca2+ channel complex.[54,60-62] β−subunits (four isoforms with their associated subtypes) play multiple roles in regulating channel membrane expression of α1-subunits, current kinetics and biophysical properties. Extracellular α2δ-subunits (two isoforms plus their subtypes) that are attached to the plasma membrane via a disulfide linkage can influence current amplitude and inactivation rates, and likely play a major role in stabilizing the incorporation of the Ca2+ channel complex into the plasma membrane. Finally, γ-subunits (six known isoforms) may modulate channel assembly and channel subtype-specific current kinetics, both effects being highly dependent on the nature of the co-expressed β− and α2δ-subunits [Figure 9a]. At the RNA level, transcripts for six pore-forming α1-subunits have been detected in human PASMC, encoding for all five VDCC types: α1A (P/Q-type), α1B (N-type), α1C and α1D (L-type), α1E (R-type) and α1G (T-type) [Figure 9b]. Additionally, a variety of regulatory subunit isoforms are also present, including α2δ1 [Figure 9c], β1-4 [Figure 9d] and γ6 [Figure 9e] in human PASMC. From the current molecular and electrophysiological evidence, it may be speculated that the α1C-subunit may encode the L-type VDCC while the α1G encodes for the T-type VDCC in human PASMC.
Voltage-gated K+ ChannelsFunctionally, both voltage-gated (Kv) channels and Ca2+-activated K+ (Kca) channels (see below) are sensitive to voltage changes. In other words, these channels are activated by membrane depolarization and are deactivated by membrane hyperpolarization. A fundamental difference between Kv and Kca channels is their response to Ca2+: in vascular smooth muscle cells, Kv channels are inhibited by cytoplasmic Ca2+[21,63] and Kca channels are activated by cytosolic Ca2+.[19,64] The existence of other types of K+ channels, such as inward rectifier (KIR), ATP-sensitive (KATP) and tandem-pore (KT) channels, has also been
demonstrated in vascular smooth muscle cells.[19,65,66] This review focuses only on the voltage-dependent channels; Kv and Kca channels.
Classification based on unitary conductanceMacroscopic currents of Kv (IK(V)) and Kca (IK(Ca)) channels can be readily dissociated based on their pharmacological properties and Ca2+-dependence. Additionally, the single-channel conductance for each of these channels can also serve to distinguish them from each other. The traces shown in Figure 10 are representative cell-attached recordings from PASMC, where multiple channel subtype openings can be recorded from the same patch using identical Ca2+-containing perfusion solutions. As shown in Figure 10a, large amplitude K+ currents (a) and several small amplitude currents (b–f) can be recorded in a cell-attached membrane patch. In addition to the various amplitudes of the recorded K+ currents, the duration of the channel openings varies in human PASMC. Examples of long-lasting channel and “flickery” openings are shown in Figures 10b and c. In cell-attached patches of PASMC, multiple amplitudes of outward K+ currents can be elicited by steadily holding the patch at different potentials. Representative openings for channels with seven different conductance levels are shown in Figure 11. The large amplitude current (225 pS and 189 pS) openings are likely generated by the activation of large-conductance Kca channels,[67] while the 33 pS, 81 pS and 6 pS channels may represent unitary currents through different Kv channels or small to intermediate conductance Kca channels.
In addition to its regulation of current amplitude, membrane potential can also affect the gating properties of these channels, e.g. the open probability (Popen). For the 189 pS channel shown in Figure 10, Popen increased with membrane depolarization from 0.0005 at 0 mV to 0.014 at +50 mV and 0.27 at +90 mV. Similarly Popen for the 33 pS channel increased from 0.04 at +60 mV to 0.43 at +90 mV, from 0.009 at +40 mV to 0.01 at +90 mV for the 141 pS channel and from 0.007 at +40 mV to 0.02 at +90 mV for the 6 pS channel. Therefore, both the single channel amplitude and the open probability of Kca and Kv channels are influenced by membrane potential in human PASMC.
Whole-cell voltage-gated K+ (Kv) currentsIn order to record optimal whole-cell (macroscopic) Kv currents (IK(V)), cells are commonly perfused with Ca2+-free bath solution (plus 1 mM EGTA) and dialyzed with Ca2+-free pipette solution (plus 10 mM EGTA). Depolarizing the cells from a holding potential of -70 mV to a series of test potentials ranging from -60 mV to +80 mV elicits outward K+ currents, with a threshold potential of activation at approximately -45 mV. Four families of whole-cell IK(V) currents can be distinguished
Firth, et al.: Ion channels in human PASMC

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 58
Firth, et al.: Ion channels in human PASMC
α2 subunit
NH2
a
COOHNH2
COOHβ subunit
NH2
NH2
COOH
COOH
δsubunit
S1 S2 S6S3 S4 S5 S1 S2 S6S3 S4 S5 S1 S2 S6S3 S4 S5 S1 S2 S6S3 S4 S5+
+
+
+
+
+
+
+
Voltage-dependent Ca2+ Channel
γ subunit α subunit
b (α -subunits)
α1G α1H α1IMbp300200
α1Fα1Dα1Cα1SMbp400200
bp α1A α1B α1EM
300400 hPASMC
L-type T-type R-type
N-type
P/Q-ty
pe
400200100
300200 hBrain
400200
c
γ1M γ2 γ4γ3 γ5 γ6bp
200300 hPASMC
/2α /2 /2α /21δ1δMbp 3δ3δ
100200
β1 β2 β3 β4Mbp
200300
α 2 2δ -subunits d β -subunits e γ-subunits
200300 hBrain
300100 200
300
650GAPDHM
0.1f
CACNG2 ( γ2)
CACNA1S ( α 1S)CACNA1C ( α 1C)CACNA1D ( α 1D)CACNA1F ( α 1F)CACNA1B ( α 1B)CACNA1A ( α 1A)CACNA1E ( α 1E)
CACNA1G ( α 1G)CACNA1H ( α 1H)CACNA1I ( α 1I)
CACNB4 ( β4)CACNB2 ( β2)CACNB1 ( β1)CACNB3 ( β3)
CACNA2D1 ( α 2δ1)
CACNG3 ( γ3)
CACNG4 ( γ4)
CACNA2D3 ( α 2δ3)CACNG1 ( γ1)CACNG6 ( γ6)CACNG5 ( γ5)
Figure 9: Molecular identity of voltage-dependent Ca2+ channels (VDCC) in pulmonary artery smooth muscle cells (PASMC). (a) Structural arrangement of Ca2+ channel α-, β-, α2β- and γ-subunits. (b–e) The mRNA expression of α (1A-1F, 1S), α2δ (δ1 and δ3), β (1-4) and γ (1-6) subunits for L-, T-, P/Q-, N- and R-type VDCC in human PASMC (hPASMC) and brain tissues (hBrain). “M,” 100 bp DNA ladder. (f) A phylogenetic tree showing the inferred evolutionary relationships among different Ca2+ channel genes

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 59
based on their activation and inactivation kinetics: (i) rapidly activating and slowly inactivating IK(V) [Figure 12a], (ii) rapidly activating and non-inactivating IK(V) [Figure 12b], (iii) slowly activating and non-inactivating
Firth, et al.: Ion channels in human PASMC
f
e
ab c
f
f
d
a
c
5 pA10 ms
a
50 ms5 pA
5 ms5 pA
5 ms5 pA
c
c
c
b
2 pA50 ms
2 pA50 ms
a b
a
b
Figure 10: Single-channel K+ currents in cell-attached patches of human pulmonary artery smooth muscle cells (PASMC). (a) Recordings from a human PASMC showing the variability of current amplitudes (a-f) within the same patch. The horizontal broken line indicates the level of currents when the channels are closed. Unitary Kv (b) and Kca (c) openings can be sustained (a) or fl ickery (b). (c). View of fl ickery and sustained iK(Ca) on expanded time scales
Cel
l Num
ber
0
3
6
9
12
15
18
21
150-199
>200
Slop
e-co
nduc
tanc
e (p
S)
0
50
100
150
200
250
300
20-3010-19< 10
Range ofConductance (pS)
50-99
100-149
Figure 11: Range of single-channel conductances of K+ channels observed in human pulmonary artery smooth muscle cells (PASMC). Floating bar graph showing modes, medians and ranges of the seven conductance classes identifi ed in human PASMC. The number of cells exhibiting particular channel conductances is indicated by the gray-shaded bars
IK(V) [Figure 12c] and (iv) rapidly activating and rapidly inactivating IK(V) [Figure 12d]. Activation time constants (τact) can be separated into two components corresponding to the rapidly and slowly activating currents (<3 ms and >3 ms, respectively) [Figure 12e, top panel]. Inactivation constants (τinact) are much more variable, as shown in Figure 12e, bottom panel, with the midpoint between rapid and slow inactivation being approximately 100 ms. The half-activation occurs at +25 mV for each type of current. In PASMC, the family of Kv channels can thus be grossly divided into two categories: (a) delayed rectifier Kv channels generating slowly activating and non- or slowly inactivating currents and (b) rapidly activating and rapidly inactivating currents originating from the activation of transient “A”-type currents similar to those observed in phasic smooth muscle, cardiomyocytes and neurons.[68-71]
Extracellular application of 5 mM 4-AP, a common Kv channel inhibitor, reversibly decreases Kv currents [Figure 13]. While the slow inactivation kinetics of three of the different currents are typical of most native delayed-rectifier K+ currents recorded in vascular SMCs,[19,25] the 4-AP-sensitive rapidly activating and inactivating current may represent a different class of K+ current less commonly observed in vascular SMC. Based on its rapid inactivation (<100 ms) kinetics, this component closely resembles the transient IA-type current that has been observed in phasic smooth muscle cells,[71,72] cardiac cells[68] and neurons.[70] Heteromeric assembly of K+ channel α−subunits may account for the notable diversity of K+ currents within the same cell system. When the electrophysiological properties of PASMC Kv currents are compared with those generated by cloned Kv channel α-subunits,[28,73-75] it is clear that the native channels’ properties are intermediaries of those different clones forming the functional channels.

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 60
Firth, et al.: Ion channels in human PASMC
Figure 13: Inhibitory effect of 4-amynopyridine (4-AP) on macroscopic voltage-gated K+ (Kv) currents (IK(V)) in pulmonary artery smooth muscle cells (PASMC). Rapidly activating and slowly inactivating (a), rapidly activating and non-inactivating (b) and rapidly activating and rapidly inactivating (c) were elicited by step depolarizations between -80 mV and +80 mV from a holding potential of -70 mV. Representative traces are shown before (Cont), during (4-AP) and after (washout) the application of 5 mM 4-AP. I-V curves of 4-AP-sensitive currents (subtraction of the currents recorded during 4-AP from the control currents) are presented in the middle panels for each current type. The 4-AP-sensitive current components depicted to the right were obtained by digital subtraction (Cont – 4-AP)
Cont 4-AP Washa
b
c
Cont 4-AP Wash
Cont 4-AP Wash
Cont 4-AP Wash
Subtraction
Subtraction
V (mV)
I (pA
)
0-40 40 800
-40 40 800
-40 40 800
-40 40 800
400
600
V (mV)I (
pA)
0200400600800
1000
Subtraction
V (mV)
I (pA
)
0
200
400
600
800
I (pA
)
200
400
600
800
V (mV)
Subtractiond
a
b
-40 0 40 800
300
600
900
1200
I (pA
)
V (mV)
-40 0 40 800
500
10001500
2000
c
-40 0 40 800
100200300400500
d
-40 0 40 800
100200300400500
I (pA
)
V (mV)
I (pA
)
V (mV)
I (pA
)
V (mV)
Activation Time Constant (ms)0 1 2 3 4 5 6 7 8 9 10 11 12
Cel
l Num
ber
01020304050
Inactivation Time Constant (ms)0 50 100 150 200 250 300
Cel
l Num
ber
05
10152025
e
τact(ms)0 3 6 9
τ ina
ct(m
s)
0100200300
2400
50100
40050
4001
2100
50100
1400
50400
200 pA
50 ms
200 pA
50 pA
200 pA
Figure 12: Whole-cell voltage-gated K+ (Kv) currents (IK(V)) in human pulmonary artery smooth muscle cells (PASMC). (a–d) Four different types of Kv currents were elicited by step depolarizations from a holding potential of –70 mV to test potentials between -80 mV and +80 mV in 20 mV increments. Representative families of currents (left panels), enlarged trace segments showing steady-state activation (middle, top panels) and inactivation (middle, bottom panels) and I-V curves are presented for each type of current. (e) Activation (top) and inactivation (bottom) time constants are plotted as a function of cell number. The majority of currents activated rapidly (within 1-4 ms). The range of inactivation constants is more varied, refl ecting the different current types
The behavior of single channels within a patch provides some evidence for the heteromeric assembly of the pore-forming units [Figure 10]. Cloned Kv channels have a wide range of single-channel conductances that do not always match with the conductance of native Kv channels. For example, the single-channel conductances for Kv1.1, Kv1.2 and Kv1.5 channels expressed in heterologous expression systems are reported to be 10 pS, 9–17 pS and 8 pS, respectively.[28,76,77] The conductance of native Kv channels in vascular SMC at physiological K+ concentrations (5 mM internal, 140 mM external) ranges between 5 pS and 11 pS,[72,78] and between 15 pS and 70 pS in symmetrical (140 mM) K+ conditions.[79-81] While the differences between native and cloned Kv conductances may relate to differences in the expression systems (e.g., pulmonary

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 61
artery vs. HEK 293 cells), splicing or post-translational modifications, it is quite likely that native Kv channels are heterotetramers.
The association of multiple β−subunits with the functional α−tetramer may further influence the biophysical properties of native currents,[73] including those in human PASMC. Cytoplasmic Kv channel β−subunits associate with the S6 segment and carboxy-terminal region of Kvα−subunits via their own highly conserved carboxy terminus.[82] The most dramatic functional effect of Kv channel β-subunit association with Kv channel α is to confer inactivation onto the non-inactivating channels [Figure 14] and to confer redox and O2 sensitivity onto the Kv channels.[83,84] In extreme cases, they convert non-inactivating Kv currents into rapidly inactivating transient currents.[85] In the case of the Kv channel β1-subunit, this occurs via the pore-blocking effect of an amino-terminal inactivation ball domain similar to that found on the “subunit.[85] Other β-subunits modulate current kinetics by shifting the activation curve, slowly deactivating the current, enhancing slow inactivation or altering peak current amplitude by acting as an open-channel blocker.[82,86] Finally, Kv channel β−subunits may participate in α-subunit assembly and transport to the plasma membrane, and enhance the interaction of α-subunits with protein kinases.[82,87] Given the diversity of roles and properties of Kv α− and β-subunits, it is not altogether surprising that Kv channel activity is central to numerous processes that rely on membrane potential regulation, such as hypoxic pulmonary vasoconstriction,[21,88-90] cell proliferation[6,91] and myogenic reactivity.[92]
Kv channel genes expressed in human PASMCAs mentioned above, native Kv channels are believed to be heteromeric tetramers composed of the pore-forming α-subunits and regulatory cytoplasmic β-subunits (α4/β4)[28,93] [Figure 15a]. Transcripts of Kv channel genes detected by RT-PCR on mRNA isolated from human PASMC and brain tissues are shown for each Kv channel subunit in Table 2. Brain tissue is commonly used as a positive control for the mRNA expression of ion channels due to its high expression of the majority of known ion channels. In human PASMC, at least 22 Kvα-subunits and 3 Kvβ-subunits [Figure 15b] have been identified. It is currently unknown as to how many of these transcripts are transcribed leading to expression of a functional channel/protein in PASMC. Figure 15c shows a phylogenetic diagram of Kv channels.
Macroscopic Ca2+-activated K+ currentsTo record Kca currents, cells need to be superfused with 1.8 mM Ca2+-containing bath solution and dialysed with an EGTA-free pipette solution. Depolarization from a
Figure 14: Co-transfection of Kvβ-subunits affects KCNA5 channel kinetics. HEK-293 cells were transfected with wild-type KCNA5 alone (KCNA5) or in the presence of Kvβ1.3-HA (KCNA5/Kvβ1.3). Representative current recordings (a) and I-V curves (b) are shown (pulse protocol, lower panel). (c) Averaged currents (left) and normalized currents (right) at +60 mV in cells transiently transfected with WT KCNA5 alone (KCNA5) or WT KCNA5 + Kvβ1.3-HA (KCNA5/ Kvβ1.3)
KCNA5 KCNA5/Kvβ1.3
-70 mV
+60 mV
-80 mV
1 nA50 ms V (mV)
-80 -40 0 40
I (nA
)
3
6
9
12
Time (ms)0 100 200 300
I at +
60 m
V (n
A)
0
3
6
9
12
Time (ms)0 100 200 300
I/Im
ax (%
)
0
20
40
60
80
100
KCNA5
KCNA5+Kvβ1.3
KCNA5
KCNA5+Kvβ1.3
KCNA5
KCNA5+Kvβ1.3
a b
c
Firth, et al.: Ion channels in human PASMC
holding potential of -70 mV to a series of test potentials ranging from -60 mV to +80 mV will elicit both Kca and Kv currents. The noisy currents dominant at positive potentials are representative of whole-cell Kca currents (IK(Ca)) observed in freshly dissociated animal vascular smooth muscle cells.[21,69] In direct comparison with IK(V), IK(Ca) activate slowly with relatively little inactivation. Extracellular application of known inhibitors of Kca channels such as 1 mM TEA, 50 nM iberiotoxin or 50 nM charybdotoxin can significantly block the noisy IK(Ca) while having a negligible effect on IK(V). These findings in PASMC are consistent with observations in systemic vascular smooth muscle cells.[19,78,80] Dialysis of PASMC with a high (500 μM) Ca2+ pipette solution (containing 8.8 mM EGTA and 10 mM CaCl2) yields slowly activating outward currents that are significantly inhibited by extracellular application of the Kca channel blockers iberiotoxin and charybdotoxin. The slow activation kinetics of the IK(Ca) is consistent with the kinetics of the currents measured in cells transfected with the maxi-K+ channel gene, hSlo-α1.[94,95]
In cell-attached patches of PASMC, increased [Ca2+]cyt by FCCP (which depolarizes and releases Ca2+ from mitochondria[96]) causes a significant increase in the steady-state open probability of the large-conductance IK(Ca) [Figure 16a]. Extracellular application of dihydroepiandrosterone, an agent that opens Kca channels via cAMP/cGMP-independent pathways,[97] also increases the Popen of large-conductance IK(Ca)

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 62
Firth, et al.: Ion channels in human PASMC
a Voltage-gated K + Channel
c
MKvβ3P B
Kvβ2P B
Kvβ1P B
200bp
b
b
MKv1.5P B
Kv1.6P B
Kv1.7P B
Kv1.10P B
200bp
MKv1.1P B
Kv1.2P B
Kv1.3P B
Kv1.4P B
bp
200
a
a
COOH
S1 S2 S6S3 S4 S5
NH2β subunit
α subunit bα
α α
α
Κ+
open inactivated
β
β
β
β
α
β
MKv11.1P B
bp200
iM
Kv9.3P B
Kv9.1P B
bp200
hM
Kv5.1P B
200bp
f
200
bpM
Kv6.2P B
Kv6.1P B
Kv6.3P B
g
200
bpM
Kv4.2P B
Kv4.1P B
Kv4.3P B
ecM
Kv3.3P B
Kv3.1P B
Kv3.4P B
200bp
dM
Kv2.1P B
400
bpM
Kv2.2P B
bp
200
GAPDH
600
j
KCNB1 (Kv2.1)
KCNA10 (Kv1.10)
KCNA7 (Kv1.7)
KCNA4 (Kv1.4)KCNA3 (Kv1.3)KCNA1 (Kv1.1)KCNA2 (Kv1.2)
KCNA6 (Kv1.6)
KCNA5 (Kv1.5)
KCNC4 (Kv3.4)KCNC1 (Kv3.1)KCNC3 (Kv3.3)
KCNG3 (Kv6.3)KCNG3 (Kv10.1)
KCNV2 (Kv11.1)KCNF1 (Kv)
KCNS1 (Kv9.1)KCNS3 (Kv9.3)
KCNG2 (Kv6.2)KCNG1 (Kv6.1)
KCNAB2 (Kv β2.1)KCNAB1 (Kv β1.1)KCNAB3 (Kv β3)KCND3 (Kv4.3)KCND2 (Kv4.2)KCND1 (Kv4.1)
KCNB2 (Kv2.2)
0.1
Figure 15: Molecular identity of voltage-gated K+ (Kv) channels in pulmonary artery smooth muscle cells (PASMC). (a) Structural arrangement of Kv channel α- and β-subunits (a), the tetrameric association of α-subunits (b) and the ball-and-chain inactivation mechanism for IK(V) (b). (b) The mRNA expression of reverse transcriptase-polymerase chain reaction products using Kv1 (a), Kvβ (b), Kv2 (c), Kv3 (d), Kv4 (e), Kv5 (f), Kv6 (g), Kv9 (h) and Kv11 (i) primers in human PASMC (P) and brain (b) tissues. “M,” 100 bp DNA ladder. (c) A phylogenetic tree showing the inferred evolutionary relationships among different Kv channel genes

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 63
Firth, et al.: Ion channels in human PASMC
Control FCCP Washouta
10 pA100 ms
10 pA100 ms
Control DHEA Washoutb
WashoutCPA (5 μM)Controlc
3 pA100 ms
FCCP
[Ca2+
] cyt
(nM
)
0200400600800
[Ca2+
] cyt
(nM
)
0200400600800
[Ca2+
] cyt
(nM
)
0200400600800
1 min
***
CPA
1 min
Cont WashCPA
***
[Ca2+
] cyt
(nM
)
0200400600800
FCCP WashCont
a
b
a
b
Figure 16: Single-channel Ca2+-activated K+ (Kca) currents (iK(Ca)) in cell-attached membrane patches of human pulmonary artery smooth muscle cells (PASMC). (a) FCCP (5 μM) enhances large-amplitude iK(Ca) open probability (Popen) (a) by causing a transient [Ca+]cyt (b) increase. (b) dihydroepiandrosterone (0.1 mM) also enhances the large-amplitude iK(Ca) Popen. (c) Cyclopiazonic acid (5 μM), an inhibitor of sarcoplasmic reticulum (SR) Ca2+ pump, increases the activity of a smaller amplitude iK(Ca) (a) by causing SR Ca2+ release from the SR to the cytosol (b)
Molecular identities of Kca channels in human PASMCUnlike the mainly heterotetrameric Kv channels, Kca channels are predominantly homomeric tetramers composed of the pore-forming α-subunits and the auxiliary β-subunits [Figure 17a].[95] Several human Kca channel α-subunits that encode the large (maxi-Kca)- and small (SKca)-conductance Kca channels have been cloned and characterized in vascular SMC.[98,99] In addition to the pore-forming α-subunit, several β-subunits have also been identified.[99] Maxi-Kca α1 (hSlo-α1) is highly expressed in human PASMC [Figure 17a]. Four β-subunits (Maxi-Kca β1-4) are also detected by RT-PCR in PASMC [Figure 17b]. Three (SK2-4) pore-forming subunits are observed at the mRNA level for SKca channels [Figure 17c].
Table 3 shows the biophysical and pharmacological properties, along with the molecular identifies of, voltage-dependent cation channels in human PASMC. The information shown in Table 3 is certainly incomplete and it is important to conduct more studies to reveal all voltage-dependent cation channels that are functionally expressed in animal and human PASMC.
Contribution of Cation Channels to the Regulation of Em and [Ca2+]cyt in Human PASMCA rise in [Ca2+]cyt in PASMC causes pulmonary vasoc-onstriction and stimulates PASMC proliferation.[100-108]. Changes in Em regulates [Ca2+]cyt in PASMC. Em is primarily determined by the concentration gradients across the plasma membrane of electrically charged ions, mainly Na+, Ca2+, K+ and Cl+, and their relative permeability. At rest, the concentration of intracellular K+ (~140 mM) is much greater than that of the extracellular space (~5 mM) because of Na+-K+ ATPase pump activity, and the K+ permeability across the plasma membrane is far greater than that of Na+, Ca2+ and Cl-.[15,106] Therefore, the resting Em is mainly determined by the permeability of K+ (EK ≈ -85 mV) and the activity of Na+-K+ ATPase. Extracellular application of 5 mM 4-AP, which is known to reduce IK(V) [Figure 13], can reversibly cause membrane depolarization in human PASMC, whereas iberiotoxin, an inhibitor of Kca channels, has little effect on Em. Increasing extracellular K+ concentration (e.g., from 4.7 mM to 60 mM) also shifts the K+ equilibrium potential and depolarizes Em. It can, therefore, be proposed that 4-AP-sensitive Kv channels are active and contribute to the regulation of the resting Em in PASMC.[25] Em is an important determinant of [Ca2+]cyt in SMC because of the voltage dependence of Ca2+ influx via voltage-dependent L-type VDCC[106,109] and the reverse mode of Na+/Ca2+ exchanger.[110,111] Consistent with its inhibitory effect on Kv channels and depolarizing effect on PASMC membrane,
[Figure 16b]. Cyclopiazonic acid causes Ca2+ mobilization from intracellular stores and, when applied in the cell-attached configuration, can increase Popen of a smaller-conductance IK(Ca) (47 pS) [Figure 16c] at +70 mV. It can therefore be inferred that two types of Kca channels, a large- and a small- or intermediate-conductance channel, are functionally expressed in human PASMC, and that they are synergistically regulated by membrane potential and [Ca2+]cyt.

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 64
Table 2: Oligonucleotide sequences of the RT-PCR primersStandard names (Accession no.)*
Size(bp)
Predicted sense/antisense Location(nt)
Gene(chromosome)
Voltage-gated Na+ channelsSCN2A
(X65361)629 5'-ACATCTGTGTGAAGGCTGGTAG-3'/
5'-CAGTAAGGACTGGTGTGGAGAA-3'1157-11791763-1785
2q23-q24
SCN4A(M81758)
684 5'-GCCGTTCAACGACACCAACACC-3'/5'-GATGTGTCCAGGCTGCCATTGC-3'
932-9541593-1615
17q23.1-q25.3
SCN5A(M77235.1
466 5’ -AGAAGATGGTCCCAGAGCAATG-3'/5’-CTCGAAGCCATCTACACACGGA-3’
1647-16692090-2112
3p21
SCN6A(M91556)
507 5'-CAGATGAGGCCAAGACCATACA-3'/5'-ATCGAAGAAGAGCCATTCCTGC-3'
1422-14441906-1928
2q21-q23
-actin(M10277)
661 5'-GACGGGGTCACCCACACTGTGCCCATCTA-3'/5'-CTAGAAGCATTTGCGGTGGACGATGGAGG-3'
2134-21622971-3000
7p22-p12
-actin(X00351)
314 5'-CACTCTTCCAGCCTTCCTTC-3'/5'-CTCGTCATACTCCTGCTTGC-3'
820-8401113-1133
7p22-p12
Voltage-gated Ca2+ channelsL-type1S
(NM_000069)246 5'-GGGAGCGAGGAGAGTAATCC-3'/
5'-CTCAGGAACTGGCTTCTTGG-3' 46-65
272-2911q32
1C(NM_000719
357 5'-TCTTTCACCCCAATGCCTAC-3'/5'-CCTCCTGGTTGTAGCAGGTC-3'
1875-18942212-2231
12p13.3
1D(XM_003238)
258 5'-GCCAGATTGGTTGACACAGA-3'/ 5'-CAGTGCCTGGTCACTTTGAA-3'
1819-18382057-2076
3p14.3
1F(NM_005183
251 5'-CTACTTCCTGGGATCCGACA-3'/ 5'-ACACCCAGGGCAGTTCATA-3'
863-8821095-1113
Xp11.23
T-type1G
(AF029229)250 5'-TTCCCAAAGATGCACCTCAT-3'/
5'-TGTGCCTGGGTACTTGACTG-3'494-513724-743
17q22
1H(NM_021096)
5'-ACCGTGTTCCAGATCCTGAC-3'/ 5'-TGAAGAGCACATAGTTGCCG-3'
3144-31633251-3270
22q13.1
1I(XM_010005)
270 5'-CCGTGGTTTGAATGTGTCAG-3'/ 5'-GTCCAGGGAGTACTCGACCA-3'
235-254485-504
22q13.1
N-type1B
(XM_015804)254 5'-CCCAGGCAGTGGAAGAAATA-3'/
5'-TGCTCCTGGAAGGTGATGAT-3' 2041-20602275-2294
9q34
P/Q-type1A
(XM_051369)250 5'-TTGCCCTACAGAAAGCCAAG-3'/
5'-TCCAAGTGCGTCTTCATGTC-3'2458-24772688-2707
19p13.2-p13.1
R-type1E
(XM_001815)253 5'-GTGGCAAGTTACATCGAGCA-3'/
5'-CAATTCCAGGTGGCTCCTAA-3' 988-10071221-1240
1q25-q31
21(XM_167505)
178 5'-AGTGGATGGCCTGTGAAAAC-3'/ 5'-ACAAGTCCCAGTTCCAATGC-3'
1231-12501389-1408
7q21-q22
23(XM_035446)
167 5'-CCTGTGCCAACAAAGGATTT-3'/ 5'-CTTTTGTGCCTGAGGGAGAG-3'
555-574702-721
3p21.1
1(XM_054993)
253 5'-CTGGCTAAGCGCTCAGTTCT-3'/ 5'-GGGACTTGATGAGCCTTTGA-3'
976-9951209-1228
17q21-q22
2(NM_000724)
241 5'-CCACAACCACAGAGACGAGA-3'/5'-AACACAAAAGGGCAAAACTC-3'
2097-21162318-2337
10p12
3(XM_028766)
248 5'-AGGAGATCTGGGAACCCTTC-3'/5'-GTGACTCGGGTGATGGAGAT-3'
406-425634-653
12q13
4(AF216867)
262 5'-CGCACCCTGAGAGTCTTTGT-3'/5'-CCACCTGGACTCGACACAC3'
342-361585-603
2q22-q23
1(XM_008262)
250 5'-GATTTGTACCAAGCGCATCC-3'/ 5'-TCGCAGCAGATAGTCCCTCT-3'
236-255466-485
17q24
2(NM_006078)
249 5'-GGCTGTTTGATCGAGGTGTT-3'/5'-TGCATCCTCTGGGAAGTGAT-3'
5-24242-261
22q13.1
3(NM_006539)
259 5'-CCTTGGGGGAAGTGTACAGA-3'/ 5'-CAAGGAGGGAAGAATGTGGA-3'
1327-13461566-1585
1612-p13.1
4(NM_014408)
299 5'-CTACAGCCGCAAGAACAACA-3'/5'-AAGGAGAAGAGGAAGACGCC-3'
407-426686-705
17q24
5(AF361351)
337 5'-CGATGAGATGCTCAACAGGA-3'/ 5'-CTGATCATAGTCGGGGCACT-3'
471-490788-807
17q24
6(AF361352)
271 5'-TTGGGGTGCCTCTGTATCAT-3'/5'-GCAGTGTGAGCAGCAGAAAG-3'
460-479711-730
19q13.4
Firth, et al.: Ion channels in human PASMC

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 65
Table 2 continuedStandard names(Accession no.) *
Size(bp)
Predicted sense/ antisense Location(nt)
Gene(chromosome)
Voltage-gated K+ channelsKv1.1 (KCNA1)
(NM_000217)258 5'-CGGGGTCATCCTGTTTTCTA-3'/
5'-CCCTCAGTTTCTCGGTGGTA-3'1005-10241243-1262
12p13
Kv1.2 (KCNA2)(NM_004974)
200 5'-ATGAGAGAATTGGGCCTCCT-3'/ 5'-CCCACTATCTTTCCCCCAAT-3'
986-10051166-1185
1p13
Kv1.3 (KCNA3)(NM_002232)
259 5'-TCTGCCTATGCCCTTGTTTT-3'/5'-TTCCTCCCAGGATGTACTGC-3'
1711-17301950-1969
1p21-p13.3
Kv1.4 (KCNA4)(NM_002233)
571 5'-TGGCGGCTACAGTTCAGTC-3'/5'-ATCATTCAACAACCCACCAT-3'
1640-16582191-2210
11q13.4-q14.1
Kv1.5 (KCNA5)(NM_002234)
201 5'-ACTTGCGGAGGTCCCTTTAT-3'/5'-GGAGGGAGGAAAGGAGTGAA-3'
2013-20322194-2213
12p13
Kv1.6 (KCNA6)(NM_002235)
197 5'-CAGAGGAATCGTGTTGCAGA-3'/5'-TGCCCATAAAATGGGAAGAA-3'
3380-33993557-3576
12p13
Kv1.7 (KCNA7)(NM_031886)
300 5'-CTTCCAGGGGCATGTTATTTTA-3'/5'-CTCAATGGAACTCAATTCAGCA-3'
2254-22752532-2553
19q13.3
Kv1.10 (KCNA10)(NM_005549)
201 5'-TGGGGTTGCTCATCTTCTTT-3'/ 5'-CACACAGAGTGCCCACAATC-3'
1124-11431305-1324
1p13.1
Kv1 (KCNAB1)(NM_003471)
197 5'-AGGCTGCAGCTCGAGTATGT-3'/ 5'-ACCGGTGGGATCATATTGAA-3'
701-720878-897
3q26.1
Kv2 (KCNAB2)(NM_003636)
195 5'-TGGGCAATAAACCCTACAGC-3'/5'-CAGCGACTTGGGAGATCATT-3'
1242-12611417-1436
1p36.3
Kv3 (KCNAB3)(NM_004732)
200 5'-GTGGTGTTCGGGTATCCTGT-3'/5'-TGATCTCCTCCAACCTTTGC-3'
257-276437-456
17p13.1
Kv2.1 (KCNB1)(NM_004975)
383 5'-ACAGAGCAAACCAAAGGAAGAAC-3'/5'-CACCCTCCATGAAGTTGACTTTA-3'
1656-16782016-2038
20q13.2
Kv3.1 (KCNC1)(NM_004976)
387 5'-GGAGGCCTTCCTTACCTACATC-3'/5'-CCTATCCTCTCGGCGTAGTAGA-3'
791-8121156-1177
11p15
Kv3.3 (KCNC3)(NM_004977)
199 5'-TGCTGCTCATCATCTTCCTG-3'/5'-GACCACGTCTTGGGGTACAT-3'
1641-16601820-1839
19q13.3-q13.4
Kv3.4 (KCNC4)(NM_004978)
196 5'-CTACCTGGAGGTGGGACTGA-3'/5'-CAGGGCCAGGAAGATGATAA-3'
1131-11501307-1326
1p21
Kv4.1 (KCND1)(NM_004979)
199 5'-GAGAAGACAACGTGCCATGA-3'/5'-TGACTGAGGCAGTGGAGTTG-3'
1456-14751635-1654
Xp11.23-p11.3
Kv4.2 (KCND2)(NM_012281)
201 5'-GCCAATGTGTCAGGAAGTCA-3'/5'-TTCTGGGGTGGTTACTGGAG-3'
1857-18762038-2057
7q31-q32
Kv4.3 (KCND3)(NM_004980)
275 5'-CATGGCCATCATCATCTTTG-3'/5'-CCCTGCGTTTATCAGCTCTC-3'
1465-14841720-1739
1p13.3
Kv5.1 (KCNF1)(NM_002236)
195 5'-GCCAGCGACGACATAGAGAT-3'/5'-CGGGTCCCTGTCAAAGTAGA-3'
303-322478-497
2p25
Kv6.1 (KCNG1)(NM_002237)
191 5'-CTACTGGTGGGCTGTCATCA-3'/5'-TCACCCTCTCTTGCTCCTGT-3'
1242-12611413-1432
20q13
Kv6.2 (KCNG2)(NM_012283)
254 5'-CTGCTGCTGCTGTTCCTCTG-3'/5'-AAAGGTGTGGAAGATGGAGGT-3'
347-366581-601
18q22-q23
Kv6.3 (KCNG3)(NM_133329)(Identical gene to Kv10.1)
227 5'-TGCATAGGTTGGTTCACTGC-3'/5'-GGCAAGCTTAATCACCCAAA-3'
682-701890-909
16q24
Kv9.1 (KCNS1)(NM_002251)
202 5'-ATACCAGCCCTTCTGCACAC-3'/5'-AGGCCAGATGATTCCCTCTT-3'
4234-42534416-4435
20q12
Kv9.3 (KCNS3)(NM_002252)
200 5'-CAGTGAGGATGCACCAGAGA-3'/5'-TTGCTGTGCAATTCTCCAAG-3'
1652-16711832-1851
2p24
Kv10.1 (KCNG3)(AF-348982)(Identical gene to Kv6.3)
227 5'-TGCATAGGTTGGTTCACTGC-3'/5'-GGCAAGCTTAATCACCCAAA-3'
682-701890-909
2p21
Kv11.1(NM_133497.1)
210 5'-CCTTCCTCTGCATTGCTTTT-3'/5'-CTTGTCTTGGGGTGAGCTGT-3'
1425-14441615-1634
9p24.2
Voltage-dependent Ca2+-activated K+ channelsMaxiKca-1
(NM_002247)442 5’-CTACTGGGATGTTTCACTGGTGT-3'/
5’-TGCTGTCATCAAACTGCATA-3'2210-22322634-2653
10q22
MaxiKca-1(NM_004137)
363 5’-TCTACTGCTTCTCCGCAC-3'/5’-GAGCAGGCAATGACTTCA-3'
557-574902-919
5q34
MaxiKca-2(NM_005832)
449 5’-GGGACTGGCTATGATGGT-3'/5’-GTGAATGGAACAGCACGTTG-3'
502-519931-950
3q26.2-q27.1
Firth, et al.: Ion channels in human PASMC

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 66
extracellular application of 4-AP also reversibly increases [Ca2+]cyt in PASMC and causes pulmonary vasoconstriction [Figure 18]. Membrane depolarization generated by raising the extracellular K+ concentration from 4.7 mM to 60 mM results from an ~20 mV shift of EK toward less-negative potentials. As a result of this rightward shift in EK and the subsequent depolarization of Em, [Ca2+]cyt is elevated [Figure 18b], an effect significantly attenuated by the removal of extracellular Ca2+. Membrane depolarization-mediated elevation of [Ca2+]cyt is therefore mainly due to Ca2+ influx through nifedipine-sensitive VDCC in human PASMC.
Both excitable and quiescent cells possess a negative
MaxiKca-3(NM_014407)
351 5’-GCTCAACAGTGCTCTGGACA-3'/5’-TGGCCACCGTCTTAAGATTT-3'
1013-10321344-1363
3q26.3-q27.1
MaxiKca-4(NM_014505)
300 5’-CTGAGTCCAACTCTAGGGCG-3'/5'-TGGTCAGGACCACAATGAGA-3'
612-631892-911
12q14.1-q15
Kca-SK1(NM_002248)
357 5’-CTTCCTCTCCATTGGCTACG-3'/5’-TTCCCTTGCTCGATCTTCAC-3'
1301-13201638-1657
19p13.1
Kca-SK2(NM_021614)
451 5’-CAAGCAAACACTTTGGTGGA-3'5’-TGTTCAGGTTCCCAGGATTC-3'
1880-18992311-2330
5q22.3
Kca-SK3(NM_002249)
349 5’-CTTGATCATCGCCTACCACA-3'/5'-GCGGGTGTTGAAGTTGATCT-3'
1344-13631673-1692
1q21.3
Kca-SK4(NM_002250)
399 5’-GCCCTGGAGAAACAGATTGA-3'/5’-AGAGCTGGAGGTCGTCCATA-3'
1567-15861946-1965
19q13.2
*The accession numbers in GenBank for the sequence used in designing the primers
Table 2 continuedStandard names(Accession no.)*
Size(bp)
Predicted sense/antisense Location(nt)
Gene(chromosome)
Firth, et al.: Ion channels in human PASMC
resting Em. Em is known to control electrical excitability (e.g., generation and propagation of action potentials), muscle contraction, apoptosis[112-114] and gene expression.[115,116] From the latter functions, it is apparent that the mechanisms controlling Em and [Ca2+]cyt are interrelated. Membrane depolarization elevates [Ca2+]cyt mainly by activating VDCC[19,25,109,117,118] and the reverse-mode Na+/Ca2+ exchanger[110,111,119] in the plasma membrane. In smooth muscle cells, the voltage window of sarcolemmal L-type voltage-gated Ca2+ channels for sustained elevation of [Ca2+]cyt ranges from -40 mV to -20 mV, and peaks at -30 mV,[109] similar to what has been observed in human PASMC. The Na+/Ca2+ exchanger has a reversal potential (ENa-Ca) of approximately -47 mV at rest, based
Table 3: Biophysical properties and molecular identities of voltage-dependent cation channels expressed in human PASMCTypes of currents Activation threshold Blocked by (EC50) Gene transcripts identifi ed
INa -34 mV Tetrodotoxin SCN5ASCN6A
ICa -24 mV (HVA)-50 mV (LVA)
NickelNifedipine
L-type (1C, 1D)T-type (1G)P/Q-type (1A)N-type (1B)R-type (1E)21β1, β2, β3, β4γ6
IK(V) -55 mV 4-AP Kv1.1, 1.2, 1.3, 1.4, 1.5, 1.6, 1.7, 1-10Kv2.1Kv3.1, 3.3, 3.4Kv4.1, 4.2Kv5.1Kv6.1, 6.2, 6.3Kv9.1, 9.3Kv10.1Kv11.1Kvβ1, β2, β3
IK(Ca) -25 mV IberiotoxinCharybdotoxin
Maxi-Kca α1Maxi-Kca β1, β2, β3, β4SK2, 3, 4

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 67
modulating Na+/Ca2+ exchange activity, (ii) non-selective permeation of Ca2+ ions through Na+ channels and (iii) rapid Na+-induced depolarization and subsequent VDCC activation.
While Na+ and Ca2+ channel activation has a tendency to depolarize cells and enhance [Ca2+]cyt, K+ channel activation hyperpolarizes the membrane and decreases sarcolemmal Ca2+ influx. Because of their voltage- and/or Ca2+-dependence, K+ channels are key elements in the maintenance of Em to the “near-resting” level. This review reflects on data that an inhibition of Kv channels with 4-AP induces membrane depolarization and increases [Ca2+]cyt by opening the nifedipine-sensitive L-type VDCC
Firth, et al.: Ion channels in human PASMC
on the equation: ENa-Ca=3ENa-2ECa,[111] where ENa is the
Na+ equilibrium potential (approximately +66 mV) and ECa is the Ca2+ equilibrium potential (approximately +122 mV). Membrane depolarization to potentials less negative than ENa-Ca would activate the reverse-mode Na+/Ca2+ exchanger and promote Ca2+ influx.[110,111,119] Thus, the sustained membrane depolarization in PASMC may produce a constant Ca2+ influx through voltage-gated Ca2+ channels[106,109] and an inward Ca2+ transportation via the reverse mode of Na+/Ca2+ exchange, and contribute to maintain the elevated [Ca2+]cyt that is crucial for PASMC contraction and proliferation. As discussed earlier, Na+ channel activation by membrane depolarization can also modulate [Ca2+]cyt by (i) controlling [Na+]cyt, thereby
C
C
n
a Ca2+-activated K+ Channel(Large-conductance
e
c Ca2+-activated K+ Channel(Small/intermediate Conductance)
S7
S10 S9
S8
COO H
NH2
S1 S3 S4 S5S0
Ca2+
α subunit
β subunit
S2 S6
S1 S3 S4 S5+
S2 S6+
COO HNH2
d
b
SK-Ca1 2 3 4M
500
300hPASM
bp
hBrai n500
300
M650
GAPDH
bp
300
500
Maxi K-Caα 1 1β 2β 3β 4βM
hPASM
300500 hBrai
GAPDH
650
M
+
+
KCNMB3 (MaxiK -β3)
KCNMB1 (MaxiK -β1)
KCNMB4 (MaxiK -β4)
KCNMB2 (MaxiK -β2)
KCNMA1 (MaxiK -α1)
KCNN4 (SK-4)
KCNN1 (SK-1)
KCNN2 (SK-2)
KCNN3 (SK-3)
0.1
Figure 17: Molecular identity of Ca2+-activated K+ (Kca) channels in human pulmonary artery smooth muscle cells (PASMC). (a) Structural arrangement of Kca channel α- and β-subunits. The putative binding site for Ca2+ is shown on the C-terminal region of the α-subunit. (b–d) The mRNA expression of reverse transcriptase-polymerase chain reaction products for maxi Kca channel α1 and β1-4 subunits (b) and small- (SK1-3) and intermediate- (SK4) channels (c and d) are shown in human PASMC and brain tissues. “M,” 100 bp DNA ladder. (e) A phylogenetic tree showing the inferred evolutionary relationships among different Kca channel genes

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 68
in human PASMC. An increase in [Ca2+]cyt is believed to play an important role in stimulating cell growth by activating protein kinases and transcription factors that are essential for the progression of cell cycle.[115,116,120-122] Kv channels in PASMC may play an important role in modulating pulmonary vascular contractility and remodeling via regulating Em and [Ca2+]cyt. Indeed, the roles of both Kca and Kv channels as feedback modulators of myogenic tone and agonist-induced vascular tone in systemic[123-125] and pulmonary arteries[63,126-132] are well documented.
CONCLUSIONS
In PASMC, EC-coupling is mainly achieved by a rise in [Ca2+]cyt, which is controlled by two related mechanisms, voltage-sensitive Ca2+ influx (electromechanical coupling) and ligand-mediated Ca2+ influx and mobilization (pharmacomechanical coupling). Membrane potential (Em) and ion diffusion across the plasma membrane are
dominantly regulated by the function and expression of ion-selective channels embedded in the plasma membrane. In addition, the activity of plasmalemmal ion channels and homeostasis of intracellular ions play important roles in the regulation of cell excitability, contraction, gene expression, proliferation, differentiation and apoptosis.[22,102,133] Electromechanical coupling mechanisms cause tonic and phasic vasomotor tone in blood vessels[106,134] and participate in regulating cell proliferation[6] and protein/gene expression.[135] An understanding of the electrophysiological properties and molecular composition of voltage-dependent ion channels in human PASMC may provide important information for the development of effective therapeutic approaches for patients with pulmonary vascular diseases.
Pulmonary vasoconstriction and vascular remodeling (i.e., intimal and medial hypertrophy due to smooth muscle cell proliferation and migration) greatly contribute to the elevated pulmonary vascular resistance in patients with
Firth, et al.: Ion channels in human PASMC
Ca2+ Ca2+
K+ K+
K channels+
Voltage-dependentCa channels (VDCC)2+
DepolarizationHyperpolarization
OpenClose
[Ca ]2+
cyt
VasoconstrictionVasodilation
K+
K+
K+ K+
K+
K+
(Artery and arteriole)
OpenK channels+ Close
K channels+
Open Close
ba
Open VDCC
Increase [Ca ]2+cyt
PASMC Contraction
Close VDCC
Decrease [Ca ]2+cyt
PASMC Relaxation
a
b
c
d
Figure 18: Inhibition of K+ channels causes membrane depolarization and causes pulmonary vasoconstriction. (a) Closure of K+ channels in pulmonary artery smooth muscle cells (PASMC) causes membrane depolarization, which subsequently opens voltage-dependent Ca2+ channels (VDCC), enhances Ca2+ infl ux, increases [Ca2+]cyt and induces pulmonary vasoconstriction. Opening of K+ channels, on the other hand, causes membrane hyperpolarization (close to the K+ equilibrium potential), decreases VDCC activity and causes pulmonary vasodilation. (b) Representative records of whole-cell K+ currents (a), membrane potential (Em, b) and [Ca2+]cyt (c) in PASMC before (control), during (4-AP) and after (wash) extracellular application of 5 mM 4-amynopyridine (4-AP), an inhibitor of Kv channels. (d) A representative record of tension measurement in an isolated mouse pulmonary arterial ring before, during and after 4-AP treatment is shown

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 69
pulmonary hypertension.[136,137] Because both Em and Ca2+ are recognized as important modulators of both vascular tone and cell growth, it is plausible that ion channels also play a role in these processes, particularly those ion channels that regulate and can be regulated by Em and Ca2+. Dysfunctional K+ channels have been demonstrated to be involved in the pathogenesis of idiopathic pulmonary arterial hypertension.[8,9] There is no direct evidence to suggest alterations in Na+ channel gene expression or function in pulmonary hypertension-induced vascular remodeling. Nonetheless, Na+ channel-mediated regulation of [Ca2+]cyt may be important in the modulation of cell proliferation. Similarly, VDCC upregulation or “gain-in-function” has not been directly involved in the pathogenesis of pulmonary arterial hypertension, although any abnormalities in its expression or function may alter the remodeling process. However, recent observations have reported an increase in store-operated Ca2+ channel activity during human PASMC proliferation,[138] suggesting that alternative Ca2+ influx pathways may be involved in the pulmonary vascular remodeling process. Targeting Ca2+ - (and Na+-) permeable channels in the plasma membrane of pulmonary vascular smooth muscle cells and myofibroblasts is an efficient approach to develop a novel therapy for patients with pulmonary arterial hypertension.
ACKNOWLEDGMENTS
This work was supported by grants from the National Heart, Lung and Blood Institute of the National Institutes of Health (HL 066012 and HL 098053). We would like to thank Mehran Mandegar, Jian Wang, Tiffany Sison and Elyssa D. Burg for their excellent work for generating the unpublished data shown in this review.
REFERENCES
1. Casteels R, Kitamura K, Kuriyama H, Suzuki H. Excitation-contraction coupling in the smooth muscle cells of the rabbit main pulmonary artery. J Physiol 1977;271:63-79.
2. Madden JA, Dawson CA, Harder DR. Hypoxia-induced activation in small isolated pulmonary arteries from the cat. J Appl Physiol 1985;59:113-9.
3. Beech DJ. Actions of neurotransmitt ers and other messengers on Ca2+ channels and K+ channels in smooth muscle cells. Pharmacol Ther 1997;73:91-119.
4. Wang Q, Large WA. Action of histamine on single smooth muscle cells dispersed from the rabbit pulmonary artery. J Physiol 1993;468:125-39.
5. Devine CE, Somlyo AV, Somlyo AP. Sarcoplasmic reticulum and excitation-contraction coupling in mammalian smooth muscles. J Cell Biol 1972;52:690-718.
6. Platoshyn O, Golovina VA, Bailey CL, Limsuwan A, Krick S, Juhaszova M, et al. Sustained membrane depolarization and pulmonary artery smooth muscle cell proliferation. Am J Physiol Cell Physiol 2000;279:C1540-9.
7. Pauly RR, Bilato C, Sollott SJ, Monticone R, Kelly PT, Lakatt a EG, et al. Role of calcium/calmodulin-dependent protein kinase II in the regulation of vascular smooth muscle cell migration. Circulation 1995;91:1107-15.
8. Yuan JX, Aldinger AM, Juhaszova M, Wang J, Conte JV Jr, Gaine SP, et al. Dysfunctional voltage-gated K+ channels in pulmonary artery smooth muscle cells of patients with primary pulmonary hypertension. Circulation 1998;98:1400-6.
9. Yuan XJ, Wang J, Juhaszova M, Gaine SP, Rubin LJ. Attenuated K+ channel gene transcription in primary pulmonary hypertension. Lancet 1998;351:726-7.
10. Cox RH, Folander K, Swanson R. Diff erential expression of voltage-gated K+ channel genes in arteries from spontaneously hypertensive and Wistar-Kyoto rats. Hypertension 2001;37:1315-22.
11. Liu Y, Hudetz AG, Knaus HG, Rusch NJ. Increased expression of Ca2+-sensitive K+ channels in the cerebral microcirculation of genetically hypertensive rats. Evidence for their protection against cerebral vasospasm. Circ Res 1998;82:729-37.
12. Martens JR, Gelband CH. Alterations in rat interlobar artery membrane potential and K+ channels in genetic and nongenetic hypertension. Circ Res 1996;79:295-301.
13. Martens JR, Gelband CH. Ion channels in vascular smooth muscle: Alterations in essential hypertension. Proc Soc Exp Biol Med 1998;218:192-203.
14. Beuckelmann DJ, Näbauer M, Erdmann E. Alterations of K+ currents in isolated human ventricular myocytes from patients with terminal heart failure. Circ Res 1993;73:379-85.
15. Jones AW. Content and fl uxes of electrolytes. In: Bohr DF, Somlyo AP, Sparks HV, editors. Handbook of Physiology, The Cardiovascular System Vascular Smooth Muscle. Baltimore, MD: Williams and Wilkins; 1980. p. 253-99.
16. Hamill OP, Marty A, Neher E, Sakmann B, Sigworth FJ. Improved patch-clamp techniques for high-resolution current recording from cells and cell-free membrane patches. Pfl ugers Arch 1981;391:85-100.
17. Hille B. Ionic channels of excitable membranes. 2nd ed. Sunderland, Massachusett s: Sinauer Associates Inc.; 1992.
18. Toro L, Gonzalez-Robles A, Stefani E. Electrical properties and morphology of single vascular smooth muscle cells in culture. Am J Physiol 1986;251:C763-73.
19. Nelson MT, Quayle JM. Physiological roles and properties of potassium channels in arterial smooth muscle. Am J Physiol 1995;268:C799-822.
20. Post JM, Hume JR, Archer SL, Weir EK. Direct role for potassium channel inhibition in hypoxic pulmonary vasoconstriction. Am J Physiol 1992;262:C882-90.
21. Post JM, Gelband CH, Hume JR. [Ca2+]i inhibition of K+ channels in canine pulmonary artery. Novel mechanism for hypoxia-induced membrane depolarization. Circ Res 1995;77:131-9.
22. Somlyo AP, Somlyo AV. Smooth muscle: Excitation-contraction coupling, contractile regulation, and the cross-bridge cycle. Alcohol Clin Exp Res 1994;18:138-43.
23. Kuriyama H, Suzuki H. Electrical property and chemical sensitivity of vascular smooth muscles in normotensive and spontaneously hypertensive rats. J Physiol 1978;285:409-24.
24. Okabe K, Kitamura K, Kuriyama H. The existence of a highly tetrodotoxin sensitive Na channel in freshly dispersed smooth muscle cells of the rabbit main pulmonary artery. Pfl ugers Arch 1988;411:423-8.
25. Yuan XJ. Voltage-gated K+ currents regulate resting membrane potential and [Ca2+]i in pulmonary arterial myocytes. Circ Res 1995;77:370-8.
26. Anderson PA, Greenberg RM. Phylogeny of ion channels: Clues to structure and function. Comp Biochem Physiol B Biochem Mol Biol 2001;129:17-28.
27. Strong M, Chandy KG, Gutman GA. Molecular evolution of voltage-sensitive ion channel genes: On the origns of electrical excitability. Mol Biol Evol 1993;10:221-42.
28. Coetzee WA, Amarillo Y, Chiu J, Chow A, Lau D, McCormack T, et al. Molecular diversity of K+ channels. Ann N Y Acad Sci 1999;868:233-85.
29. Durell SR, Guy HR. A putative prokaryote voltage-gated Ca2+ channel with only one 6TM motif per subunit. Biochem Biophys Res Comm 2001;281:741-6.
30. Catt erall WA. From ionic currents to molecular mechanisms: The structure and function of voltage-gated sodium channels. Neuron 2000;26:13-25.
31. Shimoda LA, Sham JS, Shimoda TH, Sylvester JT. L-type Ca2+ channels, resting [Ca2+]i, and ET-1-induced responses in chronically hypoxic pulmonary myocytes. Am J Physiol Lung Cell Mol Physiol 2000;279:L884-94.
32. Zhou C, Wu S. T-type calcium channels in pulmonary vascular endothelium. Microcirculation 2006;13:645-56.
33. Mori M, Konno T, Ozawa T, Murata M, Imoto K, Nagayama K. Novel interaction of the voltage-dependent sodium channel (VDSC) with calmodulin: Does VDSC acquire calmoduln-mediated Ca2+ sensitivity? Biochemistry 2000;39:1316-23.
34. Zühlke RD, Pitt GS, Deisseroth K, Tsien RW, Reuter H. Calmodulin
Firth, et al.: Ion channels in human PASMC

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 70
supports both inactivation and facilitation of L-type calcium channels. Nature 1999;399:159-62.
35. Spaff ord JD, Spencer AN, Gallin WJ. Genomic organization of a voltage-gated Na+ channel in a hydrozoan jellyfi sh: Insights into the evolution of voltage-gated Na+ channel genes. Receptors Channels 1999;6:493-506.
36. Goldin AL. Resurgence of sodium channel research. Annu Rev Physiol 2001;63:871-94.
37. Plummer NW, Meisler MH. Evolution and diversity of mammalian sodium channel genes. Genomics 1999;57:323-31.
38. Arnon A, Hamlyn JM, Blaustein MP. Na+ entry via store-operated channels modulates Ca2+ signaling in arterial myocytes. Am J Physiol Cell Physiol 2000;278:C163-73.
39. Boccara G, Choby C, Frapier JM, Quignard JF, Nargeot J, Dayanithi G, et al. Regulation of Ca2+ homeostasis by atypical Na+ currents in cultured human coronary myocytes. Circ Res 1999;85:606-13.
40. Fozzard HA, January CT, Makielski JC. New studies of the excitatory sodium currents in heart muscle. Circ Res 1985;56:475-85.
41. Leblanc N, Hume JR. Sodium current induced release of calcium from cardiac sarcoplasmic reticulum. Science 1990;248:372-6.
42. Santana LF, Gómez AM, Lederer WJ. Ca2+ fl ux through promiscuous cardiac Na+ channels: Slip-mode conductance. Science 1998;279:1027-33.
43. Choby C, Mangoni ME, Boccara G, Nargeot J, Richard S. Evidence for tetrodotoxin-sensitive sodium currents in primary cultured myocytes from human, pig and rabbit arteries. Pfl ugers Arch 2000;440:149-52.
44. Cox RH, Zhou Z, Tulenko TN. Voltage-gated sodium channels in human aortic smooth muscle cells. J Vasc Res 1998;35:310-7.
45. James AF, Okada T, Horie M. A fast transient outward current in cultured cells from human pulmonary artery smooth muscle. Am J Physiol 1995;268:H2358-65.
46. Quignard JF, Ryckwaert F, Albat B, Nargeot J, Richard S. A novel tetrodotoxin-sensitive Na+ current in cultured human coronary myocytes. Circ Res 1997;80:377-82.
47. Felix R. Channelopathies: Ion channel defects linked to heritable clinical disorders. J Med Genet 2000;37:729-40.
48. Li S, Sims S, Jiao Y, Chow LH, Pickering JG. Evidence from a novel human cell clone that adult vascular smooth muscle cells can convert reversibly between noncontractile and contractile phenotypes. Circ Res 1999;85:338-48.
49. Sashihara S, Tshuji S, Matsui T. Oncogenes and signal transduction pathways involved in the regulation of Na+ channel expression. Crit Rev Oncog 1998;9:19-34.
50. Aggarwal R, Shorofsky SR, Goldman L, Balke CW. Tetrodotoxin-blockable calcium currents in rat ventricular myocytes: A third type of cardiac cell sodium current. J Physiol 1997;505:353-69.
51. Cole WC, Chartier D, Martin M, Leblanc N. Ca2+ permeation through Na+ channels in guinea pig ventricular myocytes. Am J Physiol 1997;273:H128-37.
52. Deschenes I, Neyroud N, DiSilvestre D, Marban E, Yue DT, Tomaselli GF. Isoform-specifi c modulation of voltage-gated Na(+) channels by calmodulin. Circ Res 2002;90:E49-57.
53. Tan HL, Kupershmidt S, Zhang R, Stepanovic S, Roden DM, Wilde AA, et al. A calcium sensor in the sodium channel modulates cardiac excitability. Nature 2002;415:442-7.
54. Catt erall WA. Structure and regulation of voltage-gated Ca2+ channels. Annu Rev Cell Dev Biol 2000;16:521-55.
55. Randall AD. The molecular basis of voltage-gated Ca2+ channel diversity: Is it time for T? J Membr Biol 1998;161:207-13.
56. Sturek M, Hermsmeyer K. Calcium and sodium channels in spontaneously contracting vascular muscle cells. Science 1986;233:475-8.
57. Hansen PB, Jensen BL, Andreasen D, Skøtt O. Diff erential expression of T- and L-type voltage dependent calcium channels in renal resistance vessels. Circ Res 2001;89:630-8.
58. Muramatsu M, Tyler RC, Rodman DM, McMurtry IF. Possible role of T-type Ca2+ channels in L-NNA vasoconstriction of hypertensive rat lungs. Am J Physiol 1997;272:H2612-21.
59. Balke CW, Rose WC, Marban E, Wier WG. Macroscopic and unitary properties of physiological ion fl ux through T-type Ca2+ channels in guinea-pig heart cells. J Physiol 1992;456:247-65.
60. Restituito S, Cens T, Rousset M, Charnet P. Ca2+ channel inactivation heterogeneity reveals physiological unbinding of auxiliary b subunits. Biophys J 2001;81:89-96.
61. Varadi G, Mori Y, Mikala G, Schwartz A. Molecular determinants of Ca2+ channel function and drug action. Trends Pharmacol Sci 1995;16:43-9.
62. Walker D, De Waard M. Subunit interaction sites in voltage-dependent
Ca2+ channels: Role in channel function. Trends Neurosci 1998;21:148-54.63. Gelband CH, Gelband H. Ca2+ release from intracellular stores is an initial
step in hypoxic pulmonary vasoconstriction of rat pulmonary artery resistance vessels. Circulation 1997;96:3647-54.
64. Peng W, Hoidal JR, Karwande SV, Farrukh IS. Eff ect of chronic hypoxia on K+ channels: Regulation in human pulmonary vascular smooth muscle cells. Am J Physiol 1997;272:C1271-8.
65. Koh SD, Monaghan K, Sergeant GP, Ro S, Walker RL, Sanders KM, et al. TREK-1 regulation by nitric oxide and cGMP-dependent protein kinase. An essential role in smooth muscle inhibitory neurotransmission. J Biol Chem 2001;276:44338-46.
66. Mandegar M, Yu Y, Platoshyn O, Lapp BR, Rubin LJ, Yuan JX. Expression and function of tandem-pore K+ channels in human pulmonary artery smooth muscle cells. Am J Respir Crit Care Med 2002;195:B53.
67. Peng W, Karwande SV, Hoidal JR, Farrukh IS. Potassium currents in cultured human pulmonary arterial smooth muscle cells. J Appl Physiol 1996;80:1187-96.
68. Barry DM, Nerbonne JM. Myocardial potassium channels: Electrophysiological and molecular diversity. Annu Rev Physiol 1994;58:363-94.
69. Beech DJ, Bolton TB. Two components of potassium current activated by depolarization of single smooth muscle cells from the rabbit portal vein. J Physiol 1989;418:293-309.
70. Rogawski MA. The A-current: How ubiquitous a feature of excitable cells is it? Trends Neurosci 1985;8:214-9.
71. Vogalis F, Lang RJ. Identifi cation of single transiently opening (‘A-type’) K channels in guinea-pig colonic myocytes. Pfl ugers Arch 1994;429:160-4.
72. Beech DJ, Bolton TB. A voltage-dependent outward current with fast kinetics in single smooth muscle cells isolated from rabbit portal vein. J Physiol 1989;412:397-414.
73. Coppock EA, Tamkun MM. Diff erential expression of Kv channel a- and b-subunits in the bovine pulmonary arterial circulation. Am J Physiol Lung Cell Mol Physiol 2001;281:L1350-60.
74. Hulme JT, Coppock EA, Felipe A, Martens JR, Tamkun MM. Oxygen sensitivity of cloned voltage-gated K+ channels expressed in the pulmonary vasculature. Circ Res 1999;85:489-97.
75. Patel AJ, Honoré E. Molecular physiology of oxygen-sensitive potassium channels. Eur Respir J 2001;18:221-7.
76. Clément-Chomienne O, Ishii K, Walsh MP, Cole WC. Identifi cation, cloning and expression of rabbit vascular smooth muscle Kv1.5 and comparison with native delayed rectifi er K+ current. J Physiol 1999;515:653-67.
77. Hart PJ, Overturf KE, Russell SN, Carl A, Hume JR, Sanders KM, et al. Cloning and expression of a Kv1.2 class delayed rectifi er K+ channel from canine colonic smooth muscle. Proc Natl Acad Sci U S A 1993;90:9659-63.
78. Volk KA, Matsuda JJ, Shibata EF. A voltage-dependent potassium current in rabbit coronary artery smooth muscle cells. J Physiol 1991;439:751-68.
79. Aiello EA, Malcolm AT, Walsh MP, Cole WC. b-Adrenoceptor activation and PKA regulate delayed rectifi er K+ channels of vascular smooth muscle cells. Am J Physiol 1998;275:H448-59.
80. Gelband CH, Hume JR. Ionic currents in single smooth muscle cells of the canine renal artery. Circ Res 1992;71:745-58.
81. Ishikawa T, Hume JR, Keef KD. Modulation of K+ and Ca2+ channels by histamine H1-receptor stimulation in rabbit coronary artery cells. J Physiol 1993;468:379-400.
82. Martens JR, Kwak YG, Tamkun MM. Modulation of Kv channel a/b subunit interactions. Trends Cardiovasc Med 1999;9:253-8.
83. Gulbis JM, Mann S, MacKinnon R. Structure of a voltage-dependent K+ channel beta subunit. Cell 1999;97:943-52.
84. Pérez-García MT, López-López JR, González C. Kvb1.2 subunit coexpression in HEK293 cells confers O2 sensitivity to Kv4.2 but not to Shaker channels. J Gen Physiol 1999;113:897-907.
85. Rett ig J, Heinemann SH, Wunder F, Lorra C, Parcej DN, Dolly JO, et al. Inactivation properties of voltage-gated K+ channels altered by presence of b-subunit. Nature 1994;369:289-94.
86. Rasmusson RL, Wang S, Castellino RC, Morales MJ, Strauss HC. The b subunit, Kvb1.2, acts as a rapid open channel blocker of NH2 terminal deleted Kv1.4 a-subunits. Adv Exp Med Biol 1997;430:29-37.
87. Gong J, Xu J, Bezanilla M, van Huizen R, Derin R, Li M. Diff erential stimulation of PKC phosphorylation of potassium channels by ZIP1 and ZIP2. Science 1999;285:1565-9.
88. Park MK, Bae YM, Lee SH, Ho WK, Earm YE. Modulation of voltage-dependent K+ channel by redox potential in pulmonary and ear arterial smooth muscle cells of the rabbit. Pfl ugers Arch 1997;434:764-71.
89. Smirnov SV, Robertson TP, Ward JP, Aaronson PI. Chronic hypoxia is
Firth, et al.: Ion channels in human PASMC

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 71
associated with reduced delayed rectifi er K+ current in rat pulmonary artery muscle cells. Am J Physiol 1994;266:H365-70.
90. Yuan XJ, Goldman WF, Tod ML, Rubin LJ, Blaustein MP. Hypoxia reduces potassium currents in cultured rat pulmonary but not mesenteric arterial myocytes. Am J Physiol 1993;264:L116-23.
91. Yu Y, Platoshyn O, Zhang J, Krick S, Zhao Y, Rubin LJ, et al. c-Jun decreases voltage-gated K+ channel activity in pulmonary artery smooth muscle cells. Circulation 2001;104:1557-63.
92. Knot HJ, Nelson MT. Regulation of membrane potential and diameter by voltage-dependent K+ channels in rabbit myogenic cerebral arteries. Am J Physiol 1995;269:H348-55.
93. Chandy KG, Gutman GA. Voltage-gated K+ channels. In: North RA, editor. Ligand- and Voltage-Gated Ion Channels. Boca Raton, FL: CRC; 1995. p. 1-71.
94. Alioua A, Tanaka Y, Wallner M, Hofmann F, Ruth P, Meera P, et al. The large-conductance, voltage-dependent, and calcium-sensitive K+ channel, Hslo, is a target of cGMP-dependent protein kinase phosphorylation in vivo. J Biol Chem 1998;273:32950-6.
95. Toro L, Wallner M, Meera P, Tanaka Y. Maxi-Kca, a unique member of the voltage-gated K channel superfamily. News Physiol Sci 1998;13:112-7.
96. Krick S, Platoshyn O, McDaniel SS, Rubin LJ, Yuan JX. Augmented K+ currents and mitochondrial membrane depolarization in pulmonary artery myocyte apoptosis. Am J Physiol Lung Cell Mol Physiol 2001;281:L887-94.
97. Farrukh IS, Peng W, Orlinska U, Hoidal JR. Eff ect of dehydroepiandrosterone on hypoxic pulmonary vasoconstriction: A Ca2+-activated K+-channel opener. Am J Physiol 1998;274:L186-95.
98. Neylon CB, Lang RJ, Fu Y, Bobik A, Reinhart PH. Molecular cloning and characterization of the intermediate-conductance Ca2+-activated K+ channel in vascular smooth muscle: Relationship between Kca channel diversity and smooth muscle cell function. Circ Res 1999;85:e33-43.
99. Tanaka Y, Meera P, Song M, Knaus HG, Toro L. Molecular constituents of maxi Kca channels in human coronary smooth muscle: Predominant a + b subunit complexes. J Physiol 1997;502:545-57.
100. Stull JT, Kamm KE, Taylor DA. Calcium control of smooth muscle contractility. Am J Med Sci 1988;296:241-5.
101. Berridge MJ. Calcium signalling and cell proliferation. Bioessays 1995;17:491-500.
102. Means AR. Calcium calmodulin and cell cycle regulation. FEBS Lett 1994;347:1-4.
103. Dolmetsch RE, Lewis RS, Goodnow CC, Healy JI. Diff erential activation of transcription factors induced by Ca2+ response amplitude and duration. Nature 1997;386:855-8.
104. Ginty DD. Calcium regulation of gene expression: Isn’t that spatial? Neuron 1997;18:183-6.
105. Johnson CM, Hill CS, Chawla S, Treisman R, Bading H. Calcium controls gene expression via three distinct pathways that can function independently of the Ras/mitogen-activated protein kinases (ERKs) signaling cascade. J Neurosci 1997;17:6189-202.
106. Nelson MT, Patlak JB, Worley JF, Standen NB. Calcium channels, potassium channels, and voltage dependence of arterial smooth muscle tone. Am J Physiol 1990;259:C3-18.
107. Short AD, Bian J, Ghosh TK, Waldron RT, Rybak SL, Gill DL. Intracellular Ca2+ pool content is linked to control of cell growth. Proc Natl Acad Sci U S A 1993;90:4986-90.
108. He H, Lam M, McCormick TS, Distelhorst CW. Maintenance of calcium homeostasis in the endoplasmic reticulum by Bcl-2. J Cell Biol 1997;138:1219-28.
109. Fleischmann BK, Murray RK, Kotlikoff MI. Voltage window for sustained elevation of cytosolic calcium in smooth muscle cells. Proc Natl Acad Sci U S A 1994;91:11914-8.
110. Kohomoto O, Levi AJ, Bridge JH. Relation between reverse sodium-calcium exchange and sarcoplasmic reticulum calcium release in guinea pig ventricular cells. Circ Res 1994;74:550-4.
111. Blaustein MP, Lederer WJ. Sodium/calcium exchange: Its physiological implications. Physiol Rev 1999;79:763-854.
112. Franklin JL, Sanz-Rodriguez C, Juhasz A, Deckwerth TL, Johnson EM Jr. Chronic depolarization prevents programmed death of sympathetic neurons in vitro but does not support growth: Requirement for Ca2+ infl ux but not Trk activation. J Neurosci 1995;15:643-64.
113. Koike T, Martin DP, Johnson EM Jr. Role of Ca2+ channels in the ability of membrane depolarization to prevent neuronal death induced by trophic-factor deprivation: Evidence that levels of internal Ca2+ determine nerve growth factor dependence of sympathetic ganglion cells. Proc Natl Acad
Sci U S A 1989;86:6421-5.114. Yu SP, Yeh CH, Sensi SL, Gwag BJ, Canzoniero LM, Farhangrazi ZS, et al.
Mediation of neuronal apoptosis by enhancement of outward potassium current. Science 1997;278:114-7.
115. Rosen LB, Ginty DD, Weber MJ, Greenberg ME. Membrane depolarization and calcium infl ux stimulate MEK and MAP kinase via activation of Ras. Neuron 1994;12:1207-21.
116. Sheng M, McFadden G, Greenberg ME. Membrane depolarization and calcium induce c-fos transcription via phosphorylation of transcription factor CREB. Neuron 1990;4:571-82.
117. Tsien RW, Tsien RY. Calcium channels, stores, and oscillations. Annu Rev Cell Biol 1990;6:715-60.
118. Van Breemen C, Saida K. Cellular mechanisms regulating [Ca2+]i smooth muscle. Annu Rev Physiol 1989;51:315-29.
119. Sham JS, Cleemann L, Morad M. Gating of the cardiac Ca2+ release channel: The role of Na+ current and Na+-Ca2+ exchange. Science 1992;255:850-3.
120. Chao TS, Byron KL, Lee KM, Villereal M, Rosner MR. Activation of MAP kinases by calcium-dependent and calcium-independent pathways. Stimulation by thapsigargin and epidermal growth factor. J Biol Chem 1992;267:19876-83.
121. Dynlacht BD. Regulation of transcription by proteins that control the cell cycle. Nature 1997;389:149-52.
122. Husain M, Jiang L, See V, Bein K, Simons M, Alper SL, et al. Regulation of vascular smooth muscle cell proliferation by plasma membrane Ca(2+)-ATPase. Am J Physiol 1997;272:C1947-59.
123. Brayden JE, Nelson MT. Regulation of arterial tone by activation of calcium-dependent potassium channels. Science 1992;256:532-5.
124. Jaggar JH, Mawe GM, Nelson MT. Voltage-dependent K+ currents in smooth muscle cells from mouse gallbladder. Am J Physiol 1998;274:G687-93.
125. Khan SA, Mathews WR, Meisheri KD. Role of calcium-activated K+ channels in vasodilation induced by nitroglycerine, acetylcholine and nitric oxide. J Pharmacol Exp Ther 1993;267:1327-35.
126. Barman SA. Pulmonary vasoreactivity to endothelin-1 at elevated vascular tone is modulated by potassium channels. J Appl Physiol 1996;80:91-8.
127. Barman SA. Potassium channels modulate canine pulmonary vasoreactivity to protein kinase C activation. Am J Physiol 1999;277:L558-65.
128. Hasunuma K, Rodman DM, McMurtry IF. Eff ects of K+ channel blockers on vascular tone in the perfused rat lung. Am Rev Respir Dis 1991;144:884-7.
129. Peng W, Hoidal JR, Farrukh IS. Regulation of Ca2+-activated K+ channels in pulmonary vascular smooth muscle cells: Role of nitric oxide. J Appl Physiol 1996;81:1264-72.
130. Shimoda LA, Sylvester JT, Sham JS. Inhibition of voltage-gated K+ current in rat intrapulmonary arterial myocytes by endothelin-1. Am J Physiol 1998;274:L842-53.
131. Yuan XJ, Sugiyama T, Goldman WF, Rubin LJ, Blaustein MP. A mitochondrial uncoupler increases Kca currents but decreases Kv currents in pulmonary artery myocytes. Am J Physiol 1996;270:C321-31.
132. Zhao YJ, Wang J, Rubin LJ, Yuan XJ. Inhibition of Kv and Kca channels antagonizes NO-induced relaxation in pulmonary artery. Am J Physiol 1997;272:H904-12.
133. Yu SP, Choi DW. Ions, cell volume, and apoptosis. Proc Natl Acad Sci U S A 2000;97:9360-2.
134. Somlyo AV, Somlyo AP. Electromechanical and pharmacomechanical coupling in vascular smooth muscle. J Pharmacol Exp Ther 1968;159:129-45.
135. Morgan KG. Calcium and vascular smooth muscle tone. Am J Med 1987;82:9-15.
136. Stenmark KR, Mecham RP. Cellular and molecular mechanisms of pulmonary vascular remodeling. Annu Rev Physiol 1997;59:89-144.
137. Rubin LJ, Rich S. Primary Pulmonary Hypertension. New York, NY: Marcel Dekker Inc.; 1997.
138. Golovina VA, Platoshyn O, Bailey CL, Wang J, Limsuwan A, Sweeney M, et al. Upregulated TRP and enhanced capacitative Ca2+ entry in human pulmonary artery myocytes during proliferation. Am J Physiol Heart Circ Physiol 2001;280:H746-55.
Firth, et al.: Ion channels in human PASMC
Source of Support: National Heart, Lung and Blood Institute of the National Institutes of Health (HL 066012 and HL 098053), Confl ict of
Interest: None declared.

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 72
INTRODUCTION
Pulmonary arterial hypertension (PAH) is a disease characterized by progressively worsening pulmonary vascular resistance, leading to right heart failure and death. The heritable form is usually caused by mutations in the type 2 receptor for the bone morphogenic protein pathway, BMPR2.[1,2]
BMPR2 is a 1038 amino acid single-pass transmembrane receptor, consisting of an extracellular ligand-binding domain, a short transmembrane domain, a kinase domain and a long, relatively uncharacterized, cytoplasmic tail. In the canonical signaling pathway, dimers of BMPR2 bind dimers of type 1 receptor (there are three possible)
Oxidative injury is a common consequence of BMPR2 mutations
Kirk L. Lane1, Megha Talati1, Eric Austin2,4, Anna R. Hemnes1, Jennifer A. Johnson1, Joshua P. Fessel1, Tom Blackwell1, Ray L. Mernaugh3, Linda Robinson1, Candice Fike4, L. Jackson Roberts II1,5, James West1
Departments of 1Medicine, 2Genetics, 3Biochemistry, 4Pediatrics and 5Pharmacology, Vanderbilt University Medical Center, Nashville, Tennessee, USA
ABSTRACT
Hereditary pulmonary arterial hypertension (PAH) is usually caused by mutations in BMPR2. Mutations are found throughout the gene, and common molecular consequences of different types of mutation are not known. Knowledge of common molecular consequences would provide insight into the molecular etiology of the disease. The objective of this study was to determine the common molecular consequences across classes of BMPR2 mutation. Increased superoxide and peroxide production and alterations in genes associated with oxidative stress were a common consequence of stable transfection of the vascular smooth muscle cells, with three distinct classes of BMPR2 mutation, in the ligand binding domain, the kinase domain and the cytoplasmic tail domain. Measurement of oxidized lipids in whole lung from transgenic mice expressing a mutation in the BMPR2 cytoplasmic tail showed a 50% increase in isoprostanes and a two-fold increase in isofurans, suggesting increased reactive oxygen species (ROS) of mitochondrial origin. Immunohistochemistry on BMPR2 transgenic mouse lung showed that oxidative stress was vascular-specifi c. Electron microscopy showed decreased mitochondrial size and variability in the pulmonary vessels from BMPR2-mutant mice. Measurement of oxidized lipids in urine from humans with BMPR2 mutations demonstrated increased ROS, regardless of disease status. Immunohistochemistry on hereditary PAH patient lung confi rmed oxidative stress specifi c to the vasculature. Increased oxidative stress, likely of mitochondrial origin, is a common consequence of BMPR2 mutation across mutation types in cell culture, mice and humans.
Key Words: Born morphogenetic protein receptor II, idiopathic and heritable pulmonary arterial hypertension, signal transduction
Research Ar t ic le
in the presence of the BMP ligand. The kinase domain in BMPR2 phosphorylates the type 1 receptor, which then phosphorylates SMAD1, 5 or 8. Phosphorylated SMAD complexes with SMAD4 and enters the nucleus as a transcription factor.[3] The cytoplasmic tail domain binds and signals through LIMK,[4] a regulator of actin cytoskeletal organization, but may have other functions as well.
BMPR2 mutations in PAH patient families are widely distributed throughout the gene and, to date, a common molecular consequence of BMPR2 mutation has not
Access this article online
Quick Response Code:Website: www.pulmonarycirculation.org
DOI: 10.4103/2045-8932.78107
Pulm Circ 2011;1:72-83
Address correspondence to:Dr. James WestDivision of Allergy, Pulmonary and Critical Care Medicine,Vanderbilt University Medical Center,1161 21st Avenue South, Suite T-1218 (MCN),Nashville, Tennessee 37232-2650, USAEmail: [email protected]

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 73
been found. Mutations in the cytoplasmic tail domain do not appear to affect SMAD signaling.[5,6] While it has been suggested that increased p38 or p42/44 MAPK phosphorylation was a common consequence of BMPR2 mutation,[7,8] it seems likely with additional experimentation that BMPR2 mutation derepresses MAPK activation, but does not consistently cause induction.[9] There is thus no known common downstream consequence of different classes of BMPR2 mutation.
Determining the common molecular consequences of the different types of BMPR2 mutation has important implications for PAH. While penetrance and age of onset may vary between mutations,[6,10] all patients develop the same disease regardless of location of their mutation, which implies a common molecular etiology. Understanding the common molecular consequences of different categories of BMPR2 mutation is thus critical to understanding the molecular etiology of PAH.
To address this, we stably transfected vascular smooth muscle cells with three categories of BMPR2 mutation, all derived from hereditary PAH (HPAH) families. Stable transfections of a cell line were used to avoid the problems with interpreting the effects of genetic, environmental, historical and cell origin variation inherent in the study of patient-derived cells. We used a C118W mutation in the ligand binding domain, an R332X mutation in the kinase domain and a 2579–2580delT frameshift in the cytoplasmic tail domain. mRNA from transfected vascular smooth muscle cells was used for gene array analyses, with follow-up measurements in cell culture, transgenic mice and human samples.
MATERIALS AND METHODS
Generation of A7r5 linesWild-type human BMPR2 was polymerase chain reaction (PCR) cloned into pCI-Neo and sequence verified. Next, three different mutation types were created using the Stratagene QuickChange Site-Directed Mutagenesis kit (Agilent Technologies, Santa Clara, CA, USA). Mutations were all derived from human patient families, and included T354G (or C118W) in the ligand binding domain, a C994T (or R332X) mutation in the kinase domain and a 2570–2580delT frameshift resulting in a cytoplasmic tail truncation.
Constructs were stably transfected into A7R5 vascular smooth muscle cells using 5 g/plate Fugene-6 (Promega, Madison, WI, USA) according to the manufacturer’s protocol in p100 plates. Initial selection used 1.6 mg/ml G418S for 7 days, followed by maintenance at 800 g/ml.
Western blotsCultured cells were rinsed twice with cold phosphate-buffered saline (PBS) and then resuspended in RIPA buffer with 2 phosphatase inhibitors (SigmaP 5726, P2850) and a protease inhibitor (Sigma P8340). Lysates were placed on ice for 30 min and then spun at 13,000 rpm for 15 min at 4oC.
Protein was quantified using the Bradford Protein Assay (Bio-Rad, Hercules CA, USA). The gel system was the 8–16% Tris-glycine gel method using Invitrogen and the chemiluminescent detection by ECL Plus Kit (GE Healthcare, Piscataway, NJ, USA, Invitrogen, Carlsbad, CA, USA). The imaging system used was Alpha Innotech’s FluorChem HD2. The transfer membrane was PVDF (GE Healthcare). Antibodies were used pSMAD(Cell Sig 9511), pp38(Cell Sig 9211), pp42/44(Cell Sig 4376), pcofilin (Cell Sig 3313) and -actin (Abcam 8227).
A7r5 gene expression arraysRNA was isolated from A7R5 cells using a Qiagen RNeasy mini kit (Valencia, CA, USA). RNA quality was confirmed using a Bioanalyzer RNA 6000 kit (Agilent Technologies, Santa Clara, CA, USA). High-quality RNA from three plates was pooled for each array, and two arrays were used for each mutation type (native or no mutation, CD, KD and ED BMPR2 mutations).
First and second strand complementary DNA was synthesized using standard techniques. Biotin-labeled antisense complimentary RNA was produced by an in vitro transcription reaction. Affymetrix rat genome 230 2.0 microarrays were hybridized with 20 μg cRNA. Target hybridization, washing, staining and scanning probe arrays were performed following an Affymetrix GeneChip Expression Analysis Manual.
The array results have been submitted to the NCBI gene expression and hybridization array data repository (GEO, http://www.ncbi.nlm.nih.gov/geo/), as series GSE21583.
Gene expression array analysisAffymetrix Cel files were loaded into dChip array analysis software.[11] The overall signal strength from the arrays was normalized to the median array, and the expression levels were determined using the perfect match/mismatch (PM/MM) algorithm. Expression values were base 2 log-transformed for comparisons. Comparisons between mutant lines and native lines used the following criteria: (1) the larger average expression must be at least 7 (128 before log-transformation) in order to avoid values entirely within experimental noise, (2) the sum of the standard deviations of the two groups was subtracted from the absolute value of the difference between
Lane, et al.: BMPR2 mutations lead to oxidative injury

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 74
the groups, and this value needed to exceed 0.4. This corresponds to roughly a 95% confidence of a minimum 1.3x change, but, on a practical basis, required a much larger average fold change (as only those genes with no error would have an average 1.3x change). This low-fold change requirement is suitable for gene ontology group analyses, which was our goal. A false discovery rate was determined by mixing group identifiers and performing the same analysis.
The resulting lists of genes were imported into a Gene Ontology Tree Machine,[12] where they were sorted into statistically significant Gene Ontology Consortium groups by hypergeometric test internal to the software.
Murine arrays reanalyzed here are part of a recently completed study (companion paper) of actin-organization in Rosa26-BMPR2R899X mice. The arrays referenced here consist of two arrays on control (Rosa26-only) and two in mutant mice (Rosa26-BMPR2R899X) activated for 1 week, with normal right ventricular systolic pressure (RVSP). These arrays have been submitted to the NCBI gene expression and hybridization array data repository (GEO, http://www.ncbi.nlm.nih.gov/geo/), as series GSE21573.
Amplex red assayCells were plated in flat bottom white polystyrene 96 well plates (Costar cat #3912) the day prior to the experiment at a concentration of 3×104/well. At the start of the experiment, the media was aspirated and replaced with 100 microliters reaction mixture (50 micromolar Amplex Red reagent [Invitrogen] and 0.1 U/mL HRP in Krebs-Ringer phosphate buffer). Then, the fluorescence was immediately assayed using an Optima fluorescence microplate reader (BMG-Labtech, Offenburg, Germany), with excitation at 544 nm and emission at 590 nm. Fluorescence was read every 10 min for a 1-h period. Values reported are the slope of the resulting line, with the slope of the negative control (empty wells) subtracted.
Luminol assayCells were plated at 2.5 x 105 cells/plate in 12-well plates (Falcon polystyrene) the day prior to the assay. At the start of the assay, cells were washed once with ice-cold PBS and the media was replaced with Krebs Ringer phosphate buffer (2 ml/well). Luminol was added to a final concentration of 40 micromolar and the plates were immediately placed in the Xenogen IVIS imager and images were captured for 15 s. The luminescence was assayed with Xenogen-Living Image 4.0 software, with background (wells with no cells but otherwise identically treated) subtracted.
Transgenic mouse linesRosa26-rtTA2 and TetO7CMV-BMPR2R899X transgenic lines were generated by the University of Cincinnati Trangenic Mouse Core on a FVB/N background, as previously described.[5] Breeding colonies of these lines are maintained independently within the (redacted) Division of Animal Care, and were crossed to produce double transgenic Rosa26-rtTA2 X TetO7CMV-BMPR2R899X mice for these studies.
For gene expression studies, Rosa26-rtTA2 mice or Rosa26-rtTA2 X TetO7CMV-BMPR2R899X mice at 12 weeks of age had transgene expression induced for 1 week by addition of doxycycline at 1 g/kg to chow. For lipid oxidation studies, Rosa26-rtTA2 mice or Rosa26-rtTA2 X TetO7CMV-BMPR2R899X mice at approximately 5 months of age had transgene expression induced for 4 weeks by the addition of doxycycline at 1 g/kg to the chow. Animals used for these studies had normal RVSP, as assessed by right heart catheterization (as previously described).[5]
All studies were approved by the (redacted) Vanderbilt University Animal Care and Use Committee.
Electron micrographyLungs from Rosa26-rtTA2 (control) mice or Rosa26-rtTA2 X TetO7CMV-BMPR2R899X mice were inflated and fixed in 2.5% glutaraldehyde in 0.1M cacodylate buffer and then washed and post-fixed in 1% aqueous osmium tetroxide. Following fixation, the samples were dehydrated through a graded series of ethanols to 100%. The samples were then embedded in Spurr resin. Thin sections of the cured resin were viewed using an FEI CM12 transmission electron microscope operated at 80 KeV. Lung sections containing small vessels were selected (away from broncus and large arteries) for EM. Pulmonary vessels were identified by the presence of blood, which was not flushed for this experiment. Mitochondrial long axis was measured in cells surrounding vessels in three control mice and three BMPR2-mutant mice by a blinded observer.
Immunohistochemical analysis of 15-F2t-isoprostane and isoketals protein adducts in human lungImmunolocalization of 15-F2t-IsoP was performed on archival paraffin-embedded human lung tissue obtained from control (n=3), HPAH patients (n=3) with BMPR2 mutations. Each of the HPAH cases had a known BMPR2 mutation. Lung sections were deparaffinized, rehydrated and treated with 0.3% hydrogen peroxide for 20 min to block endogenous peroxidase. Sections were incubated with 10% normal rabbit serum in 0.1 M PBS (pH 7.4) for 10 min at room temperature to block non-specific binding of the secondary antibody, followed by incubation
Lane, et al.: BMPR2 mutations lead to oxidative injury

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 75
Lane, et al.: BMPR2 mutations lead to oxidative injury
chromatography/negative ion chemical ionization mass spectrometry with selected ion monitoring. IsoFs were detected at m/z 585, F2-IsoPs at m/z 569 and the [2H4] 15-F2t-IsoP internal standard at m/z 573. Quantification was accomplished by measuring the areas under the portions of the curves for the selected ion currents for IsoFs and F2-IsoPs, respectively, and comparing with the area under the curve for the selected ion current corresponding to the internal standard. Using stable isotope dilution calculations, the amount of IsoFs and F2-IsoPs in each sample was determined and normalized to tissue wet weight.
Quantification of F2-isoprostanes in human urineThe subjects were approached in a clinic or by telephone for enrolment in this study and planning for sample acquisition. In brief, subjects were asked to provide consent prior to study enrolment. They were then given, in person or by subsequent mailing, a box that contained a copy of the consent form already signed by the subject as well as a cold pack for storage and two 50 ml conical tubes. Each tube contained 0.5 ml of 500 mM ascorbic acid for urine preservation per established protocols (1 mg/mL). Each research box came with a set of instructions along with the supplies, with orders to collect the urine sample as a 12-h overnight urine sample. In the morning after collection, the subject filled completely the two 50 ml conical tubes with urine, sealed them and placed the tubes in the package with a cold pack for return by overnight mail to the group’s research laboratory (in approved biosample transport packing). The subject called the Research Coordinator upon sending the sample, which was tracked until receipt. All samples were aliquoted into conical tubes and stored at -80°C within 24 h of collection. This study was approved by the (redacted) Human Subjects IRB.
To quantify F2-IsoPs, 0.2 mL urine was added to 2–3 mL deionized water. Internal standard was added, the pH was adjusted to 3 with 1N HCl and analysis was carried out as described above. A separate 1 mL sample from each subject was sent to the core clinical lab for quantification of creatinine.
RESULTS
Different BMPR2 mutations do not cause consistent changes in known downstream pathwaysA7r5 rat vascular smooth muscle cells were stably transfected with three categories of human BMPR2 mutation: a cytoplasmic domain (CD) mutation, a kinase domain (KD) mutation, and a ligand binding or extracellular domain (ED) mutation. Quantitative reverse
with 15-F2t-IsoP antibody (Oxford Biomedical Research, MI; dilution 1:100 of 6 mg/ml protein concentration) overnight at 4°C. The sections were then incubated with biotinylated goat secondary antibody (1:400 dilution; Vector Laboratories Inc., Burlingame, CA, USA) for 1 h at room temperature followed by incubation with HRP-conjugated Streptavidin. Diaminobenzidine (DAB) was used as a substrate for HRP. The sections were dehydrated and mounted in Cytoseal XYL (Richard-Allan Scientific, MI, USA) for the light microscopic examination.
Immunolocalization of isoketal protein adducts was performed on the control and HPAH human lung sections, or on murine lung sections, as mentioned above. Tissue sections were deparaffinized, rehydrated and treated with 0.3% hydrogen peroxide as described previously. Sections were incubated with 0.1 M PBS (pH 7.4) containing 5% normal mouse serum and 5% bovine serum albumin for 30 min at room temperature to block the non-specific binding of the secondary antibody. Sections were incubated with 5 ug/ml D11 ScFv (isoketal antibody) for 2 h at room temperature and then incubated with HRP-labeled anti-E Tag (1:500 dilution, GE Healthcare, Pittsburgh, PA, USA) for 2 h at room temperature. DAB was used as a substrate for HRP. The sections were dehydrated and mounted in Cytoseal XYL (Richard-Allan Scientific) for the light microscopic examination.
Quantification of isofurans and F2-isoprostanes in mouse lung tissueLungs were harvested from mice, snap frozen in liquid nitrogen and stored at -80°C until analysis. Tissues were homogenized and lipids were extracted and analyzed as previously described.[13] Briefly, tissues were homogenized in 2:1 chloroform:methanol containing 0.005% butylated hydroxytoluene (BHT). Following quantitative extraction, 0.9% saline was added to precipitate the proteins. Samples were centrifuged at 2000 rpm for 10 min, the upper aqueous phase was removed and the lower organic phase was decanted and evaporated to dryness under nitrogen. Equal parts of methanol containing 0.005% BHT and 15% KOH were added and the samples were incubated at 37°C for 30 min. The pH was adjusted to 3 with 1N HCl, and 1 ng of a [2H4] 15-F2t-IsoP internal standard (Cayman Chemical Company, Ann Arbor, MI, USA) was added. Lipids were partially purified by sequential loading/washing/elution from a C-18 followed by a silica Sep-Pak (Waters Associates, Milford, MA, USA), derivatized to pentafluorobenzyl esters, and further purified by silica thin-layer chromatography. The portion of the thin-layer chromatography plate corresponding to the highest concentration of IsoFs and F2-IsoPs (determined by the relative mobility of a PGF2α methyl ester standard) was scraped free. Lipids were extracted, derivatized to trimethylsilyl ethers and analyzed by gas

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 76
transcriptase PCR was performed to confirm mutant BMPR2 expression comparable with wild-type levels (not shown). We found decreased SMAD1 phosphorylation in KD and ED mutants, but not in CD mutants [Figure 1]. We found increased cofilin phosphorylation,[4] presumably secondary to LIMK dysfunction, in CD, but not in KD and ED mutants. These changes were not dramatic (~40–60%), but were in keeping with our goal of using roughly physiologic stoichiometry between mutant and wild-type mutation.
Both p38 and p42/44 phosphorylation showed a great deal of variation from plate to plate in all samples and no consistent changes between mutation types; this was true even after extensive experimentation with timepoints and conditions.
Different BMPR2 mutations cause dysregulation of energy metabolism or reactive oxygen species (ROS)-related gene expressionTo determine the common molecular consequences of different classes of BMPR2 mutation, Affymetrix gene expression array analysis was performed on native A7r5 cells, or cells stably transfected with CD, KD or ED mutations. RNA from three plates was pooled for each array, and two arrays were used per condition. Using requirements for a minimum expression threshold and minimum change in statistically relevant levels of expression (described in Methods), we found 296 probe sets altered between CD and native arrays, representing 249 named genes, with a false discovery rate of 3.7% (Lane and West, unpublished data). With the same conditions, we found 415 probe sets representing 390 genes altered between the ED and the native arrays (Lane and West, unpublished data). Forty-five percent of the alterations on the CD arrays were in common with alterations in the ED arrays. The KD mutation was a strong outlier, with 8444 probe sets altered using the same criteria, with a 0% false discovery rate. This probably represents a wholesale change in the cell differentiation state. When we previously expressed a very similar mutation in the smooth muscle of live mice, we also had a broad dedifferentiation of smooth muscle.[14]
Most of the genes with common altered regulation across mutation types could be grouped into cell cycle or apoptosis, migration or actin organization and energy metabolism or ROS-related genes. Cell-cycle changes related to BMPR2 mutation have been extensively studied.[15] We recently completed a study on the physiologic relevance of dysregulation of actin organization by BMPR2,[16] and thus were most interested in the indicators of altered energy metabolism and increased ROS suggested by the arrays.
Indicators of altered energy metabolism and increased ROS included altered glycolysis genes, decreased mitochondrial ribosomal genes, increased expression of ROS-responsive genes and suggestions of a shift to glutaminolysis, including increased sterol activity and alterations in citrate synthase and glutamine-related genes [Figure 2]. Depicted in Figure 2 are alterations common to all three mutations; each mutation included alterations in additional energy metabolism genes with similar consequences.
Different BMPR2 mutations cause increased peroxide and superoxide in cultureGene expression arrays are an excellent tool for generating a broad overview of the pathways altered in an experiment but, by their nature, are almost useless for determining the functional consequences of alterations in those pathways. To determine whether BMPR2 mutations actually resulted in alterations in ROS production, we directly assayed production of ROS in A7r5 culture by standard methods. The Amplex red assay was used to determine the levels
Figure 1: Western blot for phosphorylation of BMPR2 activity targets Smad1, p38, p42/44 and cofi lin show no consistent changes across the extracellular domain (ED), kinase domain (KD) and cytoplasmic domain (CD) BMPR2 mutation types. Densitometry (lower panel) indicates a signifi cant decrease in Smad1 phosphorylation in KD and ED mutants, but not CD, and a signifi cant increase in cofi lin phosphorylation in CD, but not KD and ED mutants. Signifi cance is P<0.05 by ANOVA with post hoc t-test
Lane, et al.: BMPR2 mutations lead to oxidative injury

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 77
of peroxide;[17] the luminol assay was used to determine the levels of the more labile superoxide.[18] Both assays indicated about a two-fold increase in ROS production across mutation types [Figure 3], although the increase in superoxide was less robust in the CD mutation.
Cytoplasmic domain BMPR2 mutation alters gene expression in transgenic mice in a manner suggesting increased ROSBecause BMPR2 mutation produces increased ROS in cell culture, we were interested in whether this would be true in vivo as well. The CD mutation was used because it had the weakest effect in culture, and would be the most stringent test of in vivo effect. We recently crossed the BMPR2R899X mutation, previously published with smooth muscle expression,[5] into a universal, Rosa26-driven promoter.[16] This has the advantage that molecular phenotype is far easier to discern because this Rosa26-BMPR2R899X model does not have the dilution-effect problems of smooth muscle-only models.
As a first step, we performed a retrospective analysis of the existing arrays from these animals to determine whether there were signs of altered ROS. We compared gene expression in Rosa26-BMPR2R899X mice with transgene activated for 1 week (long before RVSP increases) to control mice also fed doxycycline, by Affymetrix array. Gene expression data from Rosa26-BMPR2R899X mice suggest elevated ROS of mitochondrial origin. The mice showed an increase in the oxidative stress response genes, including glutathione peroxidase,[19] two lysyl oxidases[20] and hydroxyprostaglandin dehydrogenase.[21] However, many NADPH complex genes were downregulated, with approximately two-fold downregulation of Nox2, Nox4, Ncf1 (p47phox) and Ncf4 (p40phox). More broadly, of the 832 genes with at least 3x change in regulation, 386 or 46% fell into the cellular metabolic process gene ontology[22] group, which was thus statistically overrepresented at P=0.005 by hypergeometric test. This suggests that BMPR2 mutations promote widespread alteration in energy metabolism.
Mice with a cytoplasmic domain BMPR2 mutation have increased levels of oxidized lipids in whole lungWhile expression arrays suggested broad defects in energy metabolism in vivo, and increased ROS specifically, we wished to directly test the hypothesis that ROS were increased in vivo. Because of their volatility, direct measurement of ROS from animal tissues is extremely error-prone.[18] However, presence of oxidized lipids is an indicator of increased ROS over time. Unlike ROS, lipid oxidation is quite stable, and is the most accurate measure of in vivo oxidant stress.[23]
Lane, et al.: BMPR2 mutations lead to oxidative injury
Figure 2: Gene expression changes common to three classes of BMPR2 mutation are consistent with a shift to catabolism and glutaminolysis. Glutaminolysis is normally accompanied by increased glutamine uptake and citrate synthase activity, resulting in increased sterol synthesis and reactive oxygen species. Catabolism is associated with decreased importance of mitochondria in energy production, consistent with decreased mitochondrial functional genes seen in the arrays. Green indicates upregulated genes; red indicates downregulated genes
Figure 3: Multiple BMPR2 mutation types show increased reactive oxygen species formation. (a) Cytoplasmic domain (CD), extracellular domain (ED) and kinase domain (KD) mutations all show increased peroxide formation by the Amplex Red assay when stably transfected into A7r5 vascular smooth muscle cells compared with cells stably transfected with wild-type BMPR2, or untransfected cells. (b) Assay of superoxide levels by luminol shows increased levels in ED and KD mutations as compared with wild-type BMPR2. Superoxide levels in CD-mutant A7R5 cells were too noisy across experiments to distinguish from wild-type BMPR2

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 78
We thus measured the levels of oxidized lipids in whole lung from either control (transactivator-only) or BMPR2R899X mice, both fed doxycycline for 6 weeks, and all with normal RVSP. Free radical-mediated lipid peroxidation was assessed by measurement of F2-isoprostanes (IsoPs) and isofurans (IsoFs) by GC/MS. Elevated cellular oxygen concentration, which occurs as a result of mitochondrial dysfunction, favors the formation of IsoFs and suppresses the formation of IsoPs.[24] We found approximately a 50% increase in the levels of IsoPs and a 100% increase in the levels of IsoFs in BMPR2-mutant mice compared with controls [Figure 4a and b]. The ratio of IsoF to IsoP increased from 2.3 to 3.2, P=0.02, suggesting that much of the increase was due to mitochondrial dysfunction.
Mitochondria in BMPR2-mutant mice are smaller, with less variable sizeMany defects in mitochondrial energy metabolism result in alterations in the mitochondria that are visible by electron microscopy.[25,26] We therefore performed electron microscopy on the lung from Rosa26-BMPR2R899X mice. A blinded observer measured lengths of the long-axis of mitochondria in pulmonary vascular cells, and found that mitochondria from mutant mice were roughly 40% smaller on average, and with three-fold less variability in size than mitochondria from pulmonary vascular cells in controls [Figure 4c and d].
Oxidized lipids in BMPR2-mutant mice are localized to the vasculatureBoth gene array and lipid peroxidation data from BMPR2R899X mice were from whole lung. Because expression of the mutant transgene is universal, it was possible that increase in lipid oxidation was also universal. To determine localization, we used antibodies to isoketals[27] for immunohistochemistry. We found that in control mouse lung, isoketal staining was primarily found in likely alveolar macrophages [Figure 5a]. In Rosa26-BMPR2R899X-mutant mice with transgene activated for 4 weeks, but in which RVSP is still normal, there is an increase in vascular but not alveolar isoketal staining [Figure 5b and c]. After an increase in the RVSP, staining is found throughout the area of the lesions [Figure 5d].
Human BMPR2 mutation carriers have increased oxidized lipids, regardless of disease statusTo determine whether increased oxidative stress was present in human BMPR2 mutation carriers, we collected urine from five controls and 17 individuals with BMPR2 mutations, including nine with PAH and eight that were currently asymptomatic, representing six different mutations. We found that HPAH patients had roughly two-fold higher urine isoprostane levels than controls, in agreement with previous studies of urine isoprostanes
in idiopathic (IPAH) patients[28] [Figure 6]. However, we discovered that unaffected BMPR2 mutation carriers (UMC) also have increased urine isoprostanes, to a degree statistically indistinguishable from those affected with disease. There was no relationship between isoprostane levels and mutation type, age or treatment.
As all BMPR2 mutation carriers have abnormal exercise tests,[29] we hypothesize that all have lung pathology. For reasons that are not yet clear in either mice or humans, BMPR2 mutation does not produce sufficient lung pathology for some to develop clinical disease. The increase in ROS seen in asymptomatic BMPR2 mutation carriers may thus be associated with developing disease, but because of the difficulty in obtaining lung samples from asymptomatic individuals, this cannot be directly tested.
Oxidized lipids in human BMPR2-related PAH are localized to the vasculatureIn control lung, immunohistochemical analysis revealed the presence of IsoFs [Figure 7a and b] and 15-F2t-IsoP [Figure 7e and f] in a few endothelial and smooth muscle cells of the large and small arteries, respectively. 15-F2t-IsoP was also present in the elastin surrounding these vessels. In HPAH lung, the intensity and number of endothelial and smooth muscle cells exhibiting immunoreactivity to IsoFs [Figure 7c and d] and 15-F2t-IsoP [Figure 7g and h] were increased in the large and small arteries as compared with controls. Immunoreactivity to 15-F2t-IsoP antibody was diffused as compared with IsoFs antibody.
DISCUSSION
In this study, we show for the first time that increased production of ROS, likely of mitochondrial origin, is a common consequence of BMPR2 mutation in cultured smooth muscle cells, mice and humans. We demonstrate increased ROS directly in cell culture [Figure 3] and through increased lipid oxidation in mice [Figure 4] and humans [Figure 6]. We confirm that the increase in ROS is vascular-specific in both mice and humans [Figures 5 and 7]. Our data suggest that the increased ROS is of mitochondrial origin (gene array data on cell culture and mice; ratio of IsoF to IsoP in mice; electron microscopy in mice). We further show that the increased ROS precedes the development of elevated RVSP in both mice and humans, indicating that it is likely important to pathogenesis, not just a response to high pressure.
There has been an explosion of interest in the relationship between ROS and pulmonary hypertension recently, with
Lane, et al.: BMPR2 mutations lead to oxidative injury

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 79
Lane, et al.: BMPR2 mutations lead to oxidative injury
Figure 4: Mice with cytoplasmic domain mutation show increased oxidized lipids, including (a) increases in isoprostane and isofuran levels (signifi cant at indicated levels by unpaired t-test) and (b) an increase in the ratio of isofuran:isoprostane levels (P=0.02 by rank-sum test, appropriate for data not normally distributed). n=6 per group (each symbol corresponds to an individual mouse). (c) Mitochondria in BMPR2-mutant mice are smaller, with less variability in size, than those in controls. (d) Example electron micrography fi elds from BMPR2-mutant mice showing smaller mitochondria
64 papers on the topic from 2003 to 2010. The majority of these are in the context of persistent pulmonary hypertension of the neonate or hypoxia-induced PAH animal models, in which the increased ROS appears to be at least in part through NOS uncoupling.[30] Recently, Xu et al. found that IPAH patients had increased glucose
uptake, decreased mitochondrial numbers and an apparent shift to “Warburg effect” aerobic glycolysis metabolism in their lungs.[31,32] While the authors hypothesized that their findings were secondary to dysregulation of NO, these findings are highly supportive of our current results.

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 80
Lane, et al.: BMPR2 mutations lead to oxidative injury
Figure 5: BMPR2-mutant mice have elevated pulmonary vascular isoketals. (a) The control mouse has positive staining limited to macrophages (red arrows). (b, c) Increased isoketal levels are limited to the vasculature in lungs of BMPR2R899X mice that do not yet have elevated RVSP. (d) BMPRR899X mouse with elevated RVSP and adventitial remodeling shows increased isoketal staining throughout the remodeled area
Figure 6: (a) Humans with BMPR2 mutations have increased isoprostane oxidized lipids in urine, regardless of disease status. UMC, unaffected BMPR2 mutation carriers; HPAH, hereditary pulmonary arterial hypertension (also BMPR2 mutation+). Comparisons are by ANOVA with post hoc t-test
The data from this earlier study combined with our own results suggests that a common consequence of BMPR2 mutation, and indeed of any PAH, is a shift in cellular metabolism away from production of energy and toward the production of proteins, lipids, etc., necessary for proliferation, similar to the shift in energy metabolism found in cancers.[31] This mechanism is thus very similar to the likely mechanism for spontaneous PAH in fawn-hooded rats.[33] Under this hypothesis, increased ROS is a marker of a pathologic shift in energy metabolism, rather than being directly pathologic itself.
On the other hand, there are multiple mechanisms by which the increased ROS could be directly pathologic. There is a strong crosstalk between mitochondrial ROS and NADPH,[34] and thus NO metabolism through BH4 depletion.[35] High levels of ROS can cause DNA damage, potentially leading to genetic instability.[36] Increased ROS could cause cross-linking of lipids or collagen, directly leading to increased vascular stiffness.[37,38] ROS can also more directly drive inflammatory processes,[39] including through induction of NF-kappaB.
While this study does not directly address the protein–protein interactions by which BMPR2 mutation results in the observed mitochondrial defects, a strong hypothesis can be formed by combining the data from this study with our previous studies and the literature. BMPR2 has multiple points of direct interaction with cytoskeletal regulatory elements, including binding of LIMK, SRC and TCTEX, among others.[40] We have recently shown in mice that BMPR2 mutation causes broad-based defects in f-actin-related pathways and cytoskeletal trafficking;[16] this is supported by the arrays in this study (Lane and West, unpublished data). These are the central pathways regulating mitochondrial fission and fusion;[41] defects in mitochondrial fission and fusion have already been implicated in pulmonary hypertension and oxidant stress.[42]
Limitations of our study include use of urine, the only available substrate from asymptomatic BMPR2 mutation carriers, to assess lipid oxidation in human patients. Additional limitations to our study include the use of systemic vascular smooth muscle cells for cell culture, although confirmation of cell culture results in both animal and human experiments somewhat ameliorates this. Further, we were only able to examine ROS in one mutation type because of the time and expense of animal studies. Finally, while the direct mechanism linking BMPR2 to mitochondrial defects seems very likely to be through altered f-actin dynamics, we have not directly shown that yet.
Our central finding is that increased oxidative injury is a common consequence of BMPR2 mutations, probably

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 81
Lane, et al.: BMPR2 mutations lead to oxidative injury
Figure 7: (a–d) Localization of isoketals in human lung from control and hereditary pulmonary arterial hypertension (HPAH) with BMPR2 mutation. In (a) large and (b) small vessels from control lung, localization of isoketals was observed in few endothelial cells (ECs) (black arrows) and smooth muscle cells (SMCs) (blue arrows). In (c) large and (d) small vessels from HPAH lung, the intensity of immunoreactivity and localization of isoketals was signifi cantly increased in ECs and SMCs. (e–h) Localization of 8-isoprostane (8-IP) in human lung from control and HPAH with BMPR2 mutation. In (e) large and (f) small vessels from control lung localization of 8-IP was observed in ECs (black arrows) and SMCs (blue arrows). Immunoreactivity of 8-IP was also observed in elastin surrounding the vessels. In (g) large and (h) small vessels from HPAH lung, the intensity of immunoreactivity and localization of isoketals was signifi cantly increased. Magnifi cation ×600

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 82
because of a shift in mitochondrial metabolism. Identification of disease genes carries with it the promise of understanding molecular etiology and thus identification of important targets for intervention. The functional significance to this study is that mechanisms for attacking the Warburg effect in cancer patients could be addressed to PAH patients. Use of dichloroacetate,[43] blood glucose control[44,45] or other small-molecule drugs targeted at aerobic glycolysis[46] provide potential treatment options entirely distinct from the current therapies. Interventions against mitochondrial dysfunction and increased ROS may allow resolution of the vascular injury that is the hallmark of PAH.
REFERENCES
1. Lane KB, Machado RD, Pauciulo MW, Thomson JR, Phillips JA 3rd, Loyd JE, et al. Heterozygous germline mutations in BMPR2, encoding a TGF-beta receptor, cause familial primary pulmonary hypertension. Nat Genet 2000;26:81-4.
2. Cogan JD, Vnencak-Jones CL, Phillips JA 3rd, Lane KB, Wheeler LA, Robbins IM, et al. Gross BMPR2 gene rearrangements constitute a new cause for primary pulmonary hypertension. Genet Med 2005;7:169-74.
3. ten Dij ke P, Korchynskyi O, Valdimarsdott ir G, Goumans MJ. Controlling cell fate by bone morphogenetic protein receptors. Mol Cell Endocrinol 2003;211:105-13.
4. Folett a VC, Lim MA, Soosairajah J, Kelly AP, Stanley EG, Shannon M, et al. Direct signaling by the BMP type II receptor via the cytoskeletal regulator LIMK1. J Cell Biol 2003;162:1089-98.
5. West J, Harral J, Lane K, Deng Y, Ickes B, Crona D, et al. Mice expressing BMPR2R899X transgene in smooth muscle develop pulmonary vascular lesions. Am J Physiol Lung Cell Mol Physiol 2008;295:L744-55.
6. Sankelo M, Flanagan JA, Machado R, Harrison R, Rudarakanchana N, Morrell N, et al. BMPR2 mutations have short lifetime expectancy in primary pulmonary hypertension. Hum Mutat 2005;26:119-24.
7. Rudarakanchana N, Flanagan JA, Chen H, Upton PD, Machado R, Patel D, et al. Functional analysis of bone morphogenetic protein type II receptor mutations underlying primary pulmonary hypertension. Hum Mol Genet 2002;11:1517-25.
8. Yang J, Davies RJ, Southwood M, Long L, Yang X, Sobolewski A, et al. Mutations in bone morphogenetic protein type II receptor cause dysregulation of Id gene expression in pulmonary artery smooth muscle cells: implications for familial pulmonary arterial hypertension. Circ Res 2008;102:1212-21.
9. Herpin A, Cunningham C. Cross-talk between the bone morphogenetic protein pathway and other major signaling pathways results in tightly regulated cell-specifi c outcomes. FEBS J 2007;274:2977-85.
10. Austin ED, Phillips JA, Cogan JD, Hamid R, Yu C, Stanton KC, et al. Truncating and missense BMPR2 mutations diff erentially aff ect the severity of heritable pulmonary arterial hypertension. Respir Res 2009;10:87.
11. Li C, Wong WH. Model-based analysis of oligonucleotide arrays: expression index computation and outlier detection. Proc Natl Acad Sci U S A 2001;98:31-6.
12. Zhang B, Schmoyer D, Kirov S, Snoddy J. GO Tree Machine (GOTM): a web-based platform for interpreting sets of interesting genes using Gene Ontology hierarchies. BMC Bioinformatics 2004;5:16.
13. Morrow JD, Scruggs J, Chen Y, Zackert WE, Roberts LJ 2nd. In vivo Evidence that the E2-isoprostane, 15-E2t-isoprostane (8-iso-prostaglandin E2) is formed. J Lipid Res 1998;39:1589-93.
14. Tada Y, Majka S, Carr M, Harral J, Crona D, Kuriyama T, et al. Molecular eff ects of loss of BMPR2 signaling in smooth muscle in a transgenic mouse model of PAH. Am J Physiol Lung Cell Mol Physiol 2007;292:L1556-63.
15. Morrell NW. Pulmonary hypertension due to BMPR2 mutation: a new paradigm for tissue remodeling? Proc Am Thorac Soc 2006;3:680-6.
16. Johnson J, Hemnes A, Lane K, Robinson L, Gladson S, West J. ACE2 Reverses Established Pulmonary Arterial Hypertension in BMPR2R899X Mice. Paper presented at: American Thoracic Society International
Conference. New Orleans, Louisiana;2010.17. Zhou M, Diwu Z, Panchuk-Voloshina N, Haugland RP. A stable
nonfl uorescent derivative of resorufi n for the fl uorometric determination of trace hydrogen peroxide: applications in detecting the activity of phagocyte NADPH oxidase and other oxidases. Anal Biochem 1997;253:162-8.
18. Münzel T, Afanas’ev IB, Kleschyov AL, Harrison DG. Detection of superoxide in vascular tissue. Arterioscler Thromb Vasc Biol 2002;22:1761-8.
19. Förstermann U. Oxidative stress in vascular disease: causes, defense mechanisms and potential therapies. Nat Clin Pract Cardiovasc Med 2008;5:338-49.
20. Johnson CD, Balagurunathan Y, Dougherty ER, Afshari CA, He Q, Ramos KS. Insight into redox-regulated gene networks in vascular cells. Bioinformation 2007;1:379-83.
21. Tai HH, Cho H, Tong M, Ding Y. NAD+-linked 15-hydroxyprostaglandin dehydrogenase: structure and biological functions. Curr Pharm Des 2006;12:955-62.
22. The Gene Ontology in 2010: extensions and refi nements. Nucleic Acids Res 2010;38:D331-5.
23. Milne GL, Yin H, Brooks JD, Sanchez S, Jackson Roberts L 2nd, Morrow JD. Quantifi cation of F2-isoprostanes in biological fl uids and tissues as a measure of oxidant stress. Methods Enzymol 2007;433:113-26.
24. Fessel JP, Jackson Roberts L. Isofurans: novel products of lipid peroxidation that defi ne the occurrence of oxidant injury in sett ings of elevated oxygen tension. Antioxid Redox Signal 2005;7:202-9.
25. Brooks C, Wei Q, Cho SG, Dong Z. Regulation of mitochondrial dynamics in acute kidney injury in cell culture and rodent models. J Clin Invest 2009;119:1275-85.
26. Ong SB, Subrayan S, Lim SY, Yellon DM, Davidson SM, Hausenloy DJ. Inhibiting mitochondrial fi ssion protects the heart against ischemia/reperfusion injury. Circulation 2010;121:2012-22.
27. Davies SS, Amarnath V, Roberts LJ 2nd. Isoketals: highly reactive gamma-ketoaldehydes formed from the H2-isoprostane pathway. Chem Phys Lipids 2004;128:85-99.
28. Robbins IM, Morrow JD, Christman BW. Oxidant stress but not thromboxane decreases with epoprostenol therapy. Free Radic Biol Med 2005;38:568-74.
29. Grunig E, Weissmann S, Ehlken N, Fij alkowska A, Fischer C, Fourme T, et al. Stress Doppler echocardiography in relatives of patients with idiopathic and familial pulmonary arterial hypertension: results of a multicenter European analysis of pulmonary artery pressure response to exercise and hypoxia. Circulation 2009;119:1747-57.
30. Firth AL, Yuan JX. Bringing down the ROS: a new therapeutic approach for PPHN. Am J Physiol Lung Cell Mol Physiol 2008;295:L976-8.
31. Vander Heiden MG, Cantley LC, Thompson CB. Understanding the Warburg eff ect: the metabolic requirements of cell proliferation. Science 2009;324:1029-33.
32. Xu W, Koeck T, Lara AR, Neumann D, DiFilippo FP, Koo M, et al. Alterations of cellular bioenergetics in pulmonary artery endothelial cells. Proc Natl Acad Sci U S A 2007;104:1342-7.
33. Rehman J, Archer SL. A proposed mitochondrial-metabolic mechanism for initiation and maintenance of pulmonary arterial hypertension in fawn-hooded rats: the Warburg model of pulmonary arterial hypertension. Adv Exp Med Biol 2010;661:171-85.
34. Daiber A. Redox signaling (cross-talk) from and to mitochondria involves mitochondrial pores and reactive oxygen species. Biochim Biophys Acta 2010;1797:897-906.
35. Chen CA, Druhan LJ, Varadharaj S, Chen YR, Zweier JL. Phosphorylation of endothelial nitric-oxide synthase regulates superoxide generation from the enzyme. J Biol Chem 2008;283:27038-47.
36. Naka K, Muraguchi T, Hoshii T, Hirao A. Regulation of reactive oxygen species and genomic stability in hematopoietic stem cells. Antioxid Redox Signal 2008;10:1883-94.
37. Goh SY, Cooper ME. Clinical review: The role of advanced glycation end products in progression and complications of diabetes. J Clin Endocrinol Metab 2008;93:1143-52.
38. Hunter KS, Albietz JA, Lee PF, Lanning CJ, Lammers SR, Hofmeister SH, et al. In vivo measurement of proximal pulmonary artery elastic modulus in the neonatal calf model of pulmonary hypertension: development and ex-vivo validation. J Appl Physiol 2010;108:968-75.
39. Yao H, Yang SR, Kode A, Rajendrasozhan S, Caito S, Adenuga D, et al. Redox regulation of lung infl ammation: role of NADPH oxidase and NF-kappaB signalling. Biochem Soc Trans 2007;35:1151-5.
Lane, et al.: BMPR2 mutations lead to oxidative injury

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 83
40. West J. Cross talk between Smad, MAPK, and actin in the etiology of pulmonary arterial hypertension. Adv Exp Med Biol 2010;661:265-78.
41. Bereiter-Hahn J, Vöth M, Mai S, Jendrach M. Structural implications of mitochondrial dynamics. Biotechnol J 2008;3:765-80.
42. Archer SL, Gomberg-Maitland M, Maitland ML, Rich S, Garcia JG, Weir EK. Mitochondrial metabolism, redox signaling, and fusion: a mitochondria-ROS-HIF-1alpha-Kv1.5 O2-sensing pathway at the intersection of pulmonary hypertension and cancer. Am J Physiol Heart Circ Physiol 2008;294:H570-8.
43. Michelakis ED, Webster L, Mackey JR. Dichloroacetate (DCA) as a potential metabolic-targeting therapy for cancer. Br J Cancer 2008;99:989-94.
44. Shanmugam M, McBrayer SK, Rosen ST. Targeting the Warburg eff ect
in hematological malignancies: from PET to therapy. Curr Opin Oncol 2009;21:531-6.
45. Rippe C, Lesniewski L, Connell M, Larocca T, Donato A, Seals D. Short-term Calorie Restriction Reverses Vascular Endothelial Dysfunction in Old Mice by Increasing Nitric Oxide and Reducing Oxidative Stress. Aging Cell 2010;9:304-12.
46. Granchi C, Bertini S, Macchia M, Minutolo F. Inhibitors of Lactate Dehydrogenase Isoforms and their Therapeutic Potentials. Curr Med Chem 2010;17:672-97.
Source of Support: NIH, Confl ict of Interest: None declared. AQ 1
Lane, et al.: BMPR2 mutations lead to oxidative injury
New features on the Journal’s website
Optimized content for mobile and hand-held devices
HTML pages have been optimized of mobile and other hand-held devices (such as iPad, Kindle, iPod) for faster browsing speed.Click on [Mobile Full text] from Table of Contents page.This is simple HTML version for faster download on mobiles (if viewed on desktop, it will be automatically redirected to full HTML version)
E-Pub for hand-held devices
EPUB is an open e-book standard recommended by The International Digital Publishing Forum which is designed for reflowable content i.e. the text display can be optimized for a particular display device.Click on [EPub] from Table of Contents page.There are various e-Pub readers such as for Windows: Digital Editions, OS X: Calibre/Bookworm, iPhone/iPod Touch/iPad: Stanza, and Linux: Calibre/Bookworm.
E-Book for desktop
One can also see the entire issue as printed here in a ‘flip book’ version on desktops.Links are available from Current Issue as well as Archives pages. Click on View as eBook
AQ 1: details required such as grant number???

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 84
STIM2 contributes to enhanced store-operated Ca2+ entry in pulmonary artery
smooth muscle cells from patients with idiopathic pulmonary arterial hypertension
Michael Y. Song1, Ayako Makino2,3, Jason X.-J. Yuan1-3
1Biomedical Sciences Graduate Program and 2Department of Medicine, University of California, San Diego, La Jolla, California, USA; 3Department of Medicine, University of Illinois at Chicago, Chicago, Illinois, USA
ABSTRACT
Pulmonary vasoconstriction and vascular remodeling are two major causes for elevated pulmonary vascular resistance and pulmonary arterial pressure in patients with idiopathic pulmonary arterial hypertension (IPAH). An increase in cytosolic free Ca2+ concentration ([Ca2+]cyt) in pulmonary artery smooth muscle cells (PASMC) is a major trigger for pulmonary vasoconstriction and an important stimulus for PASMC proliferation, which causes pulmonary vascular remodeling. Store-operated Ca2+ entry (SOCE), induced by depletion of stored Ca2+ in the sarcoplasmic reticulum (SR), can increase [Ca2+]cyt in PASMC, independent of other means of Ca2+ entry. Stromal interaction molecule (STIM) proteins, STIM1 and STIM2, were both recently identifi ed as sensors for store depletion and also signaling molecules to open store-operated Ca2+ channels. We previously reported that SOCE was signifi cantly enhanced in PASMC from IPAH patients compared to PASMC from normotensive control subjects. Enhanced SOCE plays an important role in the pathophysiological changes in PASMC associated with pulmonary arterial hypertension. In this study, we examine whether the expression levels of STIM1 and STIM2 are altered in IPAH-PASMC compared to control PASMC, and whether these putative changes in the STIM1 and STIM2 expression levels are responsible for enhanced SOCE and proliferation in IPAH-PASMC. Compared to control PASMC, the protein expression level of STIM2 was signifi cantly increased in IPAH-PASMC, whereas STIM1 protein expression was not signifi cantly changed. In IPAH-PASMC, the small interfering RNA (siRNA)-mediated knockdown of STIM2 decreased SOCE and proliferation, while knockdown of STIM2 in control PASMC had no effect on either SOCE or proliferation. Overexpression of STIM2 in the control PASMC failed to enhance SOCE or proliferation. These data indicate that enhanced protein expression of STIM2 is necessary, but not suffi cient, for enhanced SOCE and proliferation of IPAH-PASMC.
Key Words: Ca2+ signaling, Orai, Stromal interaction molecule, vascular remodeling, vasoconstriction
Access this article online
Quick Response Code:Website: www.pulmonarycirculation.org
DOI: 10.4103/2045-8932.78106
Pulm Circ 2011;1:84-94
Address correspondence to:Prof. Jason X.-J. YuanDepartment of Medicine,Section of Pulmonary, Critical Care and Sleep Medicine,University of Illinois at Chicago, COMRB Rm. 3131 (MC 719)909 South Wolcott Avenue, Chicago, Illinois 60612, USAE-mail: [email protected]
INTRODUCTION
Increased pulmonary vascular resistance, due to sustained vasoconstriction, vascular remodeling, in situ thrombosis, and increased vascular wall stiffness, is the major cause for elevated pulmonary arterial pressure in patients with pulmonary arterial hypertension (PAH).[1,2] Studies from a pulmonary angiogram show that patients with idiopathic pulmonary arterial hypertension (IPAH) and hypoxia-induced pulmonary hypertension (HPH) have
a significant decrease in the blood flow to small- and medium-sized pulmonary arteries. Decreased blood flow to small and medium-sized pulmonary arteries results mainly from a decrease in the diameter of the artery lumen, due to sustained pulmonary vasoconstriction and vascular remodeling — two major causes that lead to increased pulmonary vascular resistance and pulmonary
Research Ar t ic le

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 85
hypertension. HPH and IPAH share many pathological and histological traits, such as, concentric vascular remodeling and medial hypertrophy. In fact, rats subjected to chronic hypoxia are used as in vivo models for studying the pathogenic and therapeutic mechanisms of pulmonary arterial hypertension, and rat pulmonary artery smooth muscle cells (PASMC) treated with hypoxia are common in vitro models for studying the cellular and molecular sequences of events involved in pulmonary vascular remodeling. Pulmonary vascular remodeling due to excessive proliferation of PASMC and sustained pulmonary vasoconstriction due to contraction of PASMC contribute greatly to the elevated pulmonary vascular resistance in patients and animals with IPAH and HPH.
An increase in cytosolic Ca2+ concentration ([Ca2+]cyt) in PASMC is a major trigger for pulmonary vasoconstriction and an important stimulus for cell proliferation and migration that contributes to pulmonary vascular remodeling. Removal of extracellular Ca2+ or reduction of extracellular free [Ca2+] with the Ca2+ chelator (e.g., EGTA and EDTA) not only significantly inhibits agonist-induced vasoconstriction in the isolated pulmonary arterial rings, but also significantly attenuates PASMC proliferation when cultured in growth factor-containing media. Both blockade of Ca2+ influx and depletion of intracellular Ca2+ stores in the sarcoplasmic reticulum (SR) or endoplasmic reticulum attenuate PASMC contraction and proliferation. Our preliminary studies show that resting [Ca2+]cyt is increased and that agonist-induced rise in [Ca2+]cyt is significantly enhanced in patients with IPAH when compared with normotensive control subjects.[3] Furthermore, chronic hypoxia also increases [Ca2+]cyt in PASMC.[4,5] Therefore, increased proliferation and contraction of PASMC in IPAH and HPH patients are likely related to the increase in [Ca2+]cyt and enhancement of the mechanisms that mediate Ca2+ influx.
Store-operated Ca2+ entry (SOCE) is an important mechanism that mediates Ca2+ influx and raises [Ca2+]cyt when the intracellular stores are depleted by agonist- or ligand-induced Ca2+ mobilization.[6,7] Depletion of intracellular Ca2+ stores, predominantly the sarcoplasmic reticulum (SR) in PASMC, activates a Ca2+ influx through the store-operated Ca2+ channels (SOC) expressed on the plasma membrane. Stromal interacting molecule (STIM) proteins, which include two isoforms, STIM1 and STIM2, are single transmembrane proteins that have been identified as the sensors of store depletion.[8,9] STIM1 and STIM2 are expressed on the SR membrane of PASMC. An EF-hand domain near the N-terminus of STIM1 and STIM2 serves as the sensor of Ca2+ concentration in the SR lumen. STIM1 and STIM2 are locked in an inactive conformation when Ca2+ is bound to the EF-hand domain, but when Ca2+ is depleted in the SR the conformation of STIM1 and
STIM2 changes to active conformation.[9,10] The active STIM1 (and STIM2) can oligomerize and translocate to ER-PM junctions, activate ER-PM junctions Ca2+ channels, and elicit SOCE. In HEK cells, overexpression of STIM1 can reconstitute a robust inwardly rectifying Ca2+ current following store depletion.[11] Similar studies have shown that STIM2 can reconstitute SOCE in the absence of STIM1, although at a lower magnitude of Ca2+ influx.[12,13] While STIM2 has lower activity in activating Ca2+ channels (or store-operated Ca2+ channels) on the plasma membrane, it is more sensitive to small changes in SR Ca2+ concentration.[14,15]
Our preliminary data indicate that both receptor-operated and store-operated Ca2+ entry play an important role in normal PASMC proliferation and migration.[16,17] Inhibition of SOCE with, for example, Ni2+, 1-[β-[3-(4-methoxyphenyl)pro-poxy]-4-methoxyphenethyl]-1H-imidazole hydrochloride (SKF96365), or La3+, markedly attenuates PASMC proliferation.[3,18-20] Furthermore, SOCE, induced by the passive depletion of Ca2+ stores using cyclopiazonic acid (CPA), an inhibitor of Ca2+-Mg2+ ATPase (SERCA) on the SR membrane is significantly enhanced, and the mRNA and protein expression of the canonical transient receptor potential (TRPC) channels are upregulated in the PASMC from IPAH patients in comparison to normotensive controls.[21,22] We have previously shown that upregulated TRPC channels (e.g., TRPC3 and TRPC6) contribute in enhancing SOCE in IPAH-PASMC, it is not known whether STIM1 and / or STIM2 are also involved in enhancing SOCE in IPAH-PASMC. Specifically, it is not known whether the protein expression of STIM1 and / or STIM2 changes in IPAH -PASMC and whether any observed changes in protein expression are responsible for enhanced SOCE and proliferation in IPAH-PASMC. In this study, we compare the protein expression levels of STIM1 and STIM2 in IPAH-PASMC and control PASMC, and investigated the functional role of any putative changes in protein expression level of STIM 1 and STIM2 on SOCE and proliferation in PASMC.
MATERIALS AND METHODS
PASMC isolation and cultureSprague-Dawley rats (125–250 g) were decapitated; the right and left branches of the main pulmonary artery as well as the intrapulmonary arteries and surrounding tissues were removed and placed in Hanks’ solution (HBSS), comprised of Hanks’ balanced salt (Irvine Scientific, Santa Ana, CA) supplemented with 14.98 mM N-2-hydroxyethylpiperazine-N’-2-ethanesulfonic acid (HEPES), 4.17 mM NaH2CO3, 0.4 mM MgS04, 10,000 U/ml penicillin, 10 mg/ml streptomycin, and 0.02 mM CaCl2. The connective tissues were gently removed under a
Song, et al.: STIM2 and SOCE in PASMC

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 86
dissecting microscope using sterile conditions. The isolated PA was incubated in 1 ml HBSS containing 1.7 mg collagenase (Worthington Biochemical, Freehold, NJ) for 20 minutes. The adventitia was carefully stripped off and the endothelium was scraped off with a fine forceps. The resulting PA smooth muscle tissue was incubated at 37°C for 20–25 hours in 10% fetal bovine serum culture medium (FBSCM), comprised of Dulbecco’s modified Eagle’s medium (DMEM, Sigma Chemical, St. Louis, MO) supplemented with 7 mM NaH2CO3 and 10 mM HEPES at pH 7.2, and fortified with fetal bovine serum (10%, Irvine Scientific). The overnight incubation of the smooth muscle tissues in 10% FBSCM, before enzymatic digestion, improved the yield of the cells. The tissue was then incubated with 1.7 mg collagenase (Worthington), 0.5 mg elastase (Sigma), and 1 mg bovine serum albumin (Sigma) in 1 ml HBSS at 37°C for 40 minutes. After 15–20 minutes, the tissue was triturated three to five times with a fire polished Pasteur pipette, to speed the digestion. The incubation mixtures were then diluted 20-fold by adding 20% FBSCM to stop the digestion. The cell suspensions were centrifuged for 5 minutes at 1,500 rpm, at room temperature, and the supernatant was removed. The resulting pellets were resuspended in 2–3 ml of 10% FBSCM and triturated with fire-polished Pasteur pipettes to separate the cells. Aliquots (3–6 drops) of the cell suspensions were drawn off and placed on cover slips in Petri dishes with 2 ml of 10% FBSCM. The cells were fed every 48 hours with 10% FBSCM and incubated in a humidified atmosphere of 5% CO, in air, at 37°C for three to seven days. After l0–20 days, the primary cultured cells had reached a confluence on the cover slips. At this time, the cells were treated with trypsin (1 mg/ml, Sigma) in HBSS and then replated on the cover slips in Petri dishes, with the addition of 2 ml of 10% FBSCM. Six to twelve hours later, the 10% FBSCM in the Petri dishes was replaced by fresh 10% FBSCM, to remove the dead and unattached cells.
Human PASMC were isolated from the lobectomized or resected lungs of normotensive control patients and from explanted lungs of patients with IPAH. The mean pulmonary arterial pressure of the IPAH patients was 52 mmHg. Patients undergoing lobectomy for
bronchogenic carcinoma, who had no evidence of pulmonary hypertension by physical examination, electrocardiogram (ECG), echocardiogram, or pathological
examination of resected lung tissue, and four patients with obstructive disease, who had normal pulmonary arterial pressures, were the sources of tissue for the normotensive control experiments. Lung tissue, removed from patients in the operating room, was immediately placed in cold (4°C) saline and taken to the laboratory for dissection. The muscular pulmonary arteries were incubated in Hanks’ balanced salt solution (20 minutes) containing
2 mg/ml collagenase (Worthington Biochemical). The adventitia was stripped, and the endothelium removed. The remaining smooth muscle was digested with 2.0 mg/ml collagenase, 0.5 mg/ml elastase, and 1 mg/ml bovine albumin (Sigma Chemical Co.) at 37°C, to make a cell suspension of PASMC. The cell suspension was plated onto 25 mm cover slips, and incubated in a humidified atmosphere of 5% CO2 in air, at 37°C, in 10% fetal bovine serum, DMEM, for one week. The cells were isolated from arteries that were between 100–500 μm in diameter.
After isolation, all PASMC were cultured in M199 supplemented with 10% FCS, 100 μg/ml endothelial cell growth supplement (ECGS), 100 IU/ml penicillin, 100 μg/ml streptomycin, and 50 mg/L D-valine. The cells were plated on the cover slips and coated with 2% gelatin. Approval to use the human lung tissues and cells was granted by the University of California, San Diego (UCSD) Institutional Review Board.
All cells were incubated in a humidified environment at 37°C and 5% CO2. The medium was changed 24 hours after initial seeding and every 48 hours subsequently. When the cells reached 80–90% confluency, they were gently washed with phosphate buffered saline (PBS), incubated briefly with 3 mL of 0.025% trypsin / EDTA solution until detachment (3–5 minutes), and then incubated with an equal amount of trypsin neutralizing solution or serum. The cell suspension was then transferred to a sterile 15 ml round bottom tube, centrifuged at room temperature for 5 minutes, at 200 times gravity, and then resuspended in the appropriate growth media and seeded. Human PASMC between passages 3 and 8 were used for experiments, and rat PASMC were used during the first passage.
Measurement of cytosolic Ca2+ concentration ([Ca2+]cyt)Cells on 25 mm cover slips were placed in a recording chamber on the stage of an inverted Nikon Eclipse / TE 200 microscope with the TE-FM epifluorescence attachment. [Ca2+]cyt was measured in each cell using the membrane-permeable Ca2+-sensitive fluorescent indicator, Fura-2-AM (Invitrogen). The cells were incubated at room temperature for 30 minutes in modified Krebs solution (MKS) containing 4 μM Fura-2-AM. The loaded cells were then washed with modified Krebs solution (MKS) for 30 minutes, to remove the excess extracellular dye and to allow the intracellular esterases to cleave the cytosolic Fura-2-AM into the active Fura-2 that was trapped in the cytosolic compartment. Fura-2 fluorescence was observed as a 510-nm-wavelength light emission with excitation wavelengths of 340 and 380 nm, with a use of the digital fluorescence imaging system from Intracellular Imaging. In all the experiments, multiple cells were imaged in a single field, and one arbitrarily chosen peripheral cytosolic
Song, et al.: STIM2 and SOCE in PASMC

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 87
area from each cell was spatially averaged. [Ca2+]cyt was expressed as a Fura-2 fluorescence emission ratio, excited at 340 and 380 nm (F340/F380), and then normalized to initial F340/F380 (F/F0).
The MKS had an ionic composition of 140 mM NaCl, 4.7 mM KCl, 1.8 mM CaCl2, 1.2 mM MgCl2, 10 mM glucose, and 10 mM HEPES. The pH was adjusted to 7.4 with 10 N NaOH. The recording chamber was continuously perfused with MKS at a flow rate of 2 ml / minute using a mini-pump (Model 3385; Control, Friendswood, TX). The [Ca2+]cyt measurements were carried out at 32°C using an automatic temperature controller (TC-344B, Warner Instruments, Holliston, MA).
Western blotThe cells were lysed (Lysate buffer: 0.5% sodium deoxycholate, 0.1% SDS, 1% triton-X, 0.1% protease inhibitor cocktail) and centrifuged at 16,000 g for 10 minutes at 4°C. The supernatants were used as protein samples. The samples were separated through an SDS-polyacrylamide gel and transferred to the nitrocellular membranes. The membranes were incubated with anti-STIM1, STIM2, antibodies (1:1,000), and followed by a secondary antibody (1:4,000) application. The immunoblots were detected with the ECL Western blotting detection reagents (Perkin-Elmer, Norton, OH). Band intensity quantified with ImageJ64, normalized to β-tubulin control, and expressed as arbitrary units. All antibodies were purchased from Pro-Sci or Sigma.
Transfection of PASMCPulmonary artery smooth muscle cells were transfected with siRNA against STIM2 (Santa Cruz sc-76589) or scramble siRNA-A (Santa Cruz sc-37007) as control using the Amaxa Nucleofector electroporation system. Sixteen microliters of a 10 μM solution of siRNA was used per 2 x 105 cells, in each reaction. Overexpression of STIM2 (Plasmid 18868: pEX-CMV-SP-STIM2 (15-746)) was performed by the Amaxa Nucleofector electroporation system. The STIM2 plasmid was ordered from Addgene, as provided by Dr. Tobais Meyer. Protein expression was examined, SOCE was measured, and cell proliferation was determined by cell counting, 48 hours following transfection.
PASMC proliferation assayPulmonary artery smooth muscle cells proliferation was determined by counting cells using the Bio-Rad TC10 Automated Cell Counter. Forty-eight hours after treatment (with siRNA or cDNA), the PASMC were counted and divided into three groups, with equal number of cells. These three groups of PASMC were then re-plated (0 hour) and counted after 24, 48, and 72 hours, respectively.
Statistical analysis The composite data are expressed as mean±SE. Statistical analysis was performed using the unpaired Student’s t-test. Differences were considered to be significant when *P<0.05, **P<0.01, and ***P<0.005.
RESULTS
Higher expression levels of STIM2, but not STIM1, in PASMC from IPAH patientsAs previously described, PASMC from IPAH patients show enhanced SOCE compared to control PASMC.[18,22-24] However, it is not known whether the expression level of the proteins that mediate SOCE by sensing store depletion is altered in the PASMC from IPAH patients. PASMC were isolated and cultured either from non-pulmonary hypertensive patients (NPH-PASMC) or patients with IPAH (IPAH-PASMC). The protein levels of STIM1 and STIM2 were examined in IPAH-PASMC and NPH-PASMC whole cell lysate. In order to compare the protein expression levels of STIM1 and STIM2 between IPAH-PASMC and NPH-PASMC, we measured the protein concentration in the whole cell lysates and standardized protein loading with β-tubulin as a loading control. As shown in Figure 1a, there was no significant morphological difference between NPH-PASMC and IPAH-PASMC. The protein expression level of STIM2, however, was significantly upregulated in IPAH-PASMC compared to NPH-PASMC [Figure 1b and c]. Surprisingly, the STIM1 protein expression level was not significantly changed in IPAH-PASMC; however, it seemed that the level of the STIM1 protein expression had a trend to be lower in IPAH-PASMC than in NPH-PASMC [Figure 1c]. These data suggest that STIM2, rather than STIM1, may be important in enhancing SOCE in PASMC from IPAH patients, in addition to the upregulated TRPC channels, which we previously reported.[21,22]
Decreasing protein expression level of STIM2 in PASMC from IPAH patients with siRNA In order to further examine the functional role of STIM2 in PASMC from IPAH patients, small interfering RNA (siRNA) was used to decrease the protein expression level of STIM2 in PASMC. IPAH-PASMC were transfected with different concentrations (4, 8 or 16 μl) of 10 μM siRNA targeting STIM2 (siSTIM2) or 16 μl of 10 μM scrambled siRNA (control siRNA). Protein expression levels of STIM2 were examined with Western blot 48 hours following transfection. FACS analysis showed over 75% transfection efficiency with Enhanced Green Fluorecence Protein (EGFP) in PASMC (data not shown). siSTIM2 significantly decreased protein expression of STIM2 in IPAH-PASMC [Figure 2]; 4, 8, and 16-μl siSTIM2 decreased STIM2 protein expression levels in IPAH-PASMC by roughly 20,
Song, et al.: STIM2 and SOCE in PASMC

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 88
1.8 mM extracellular Ca2+. Consistent with our previously reported findings,[22,24] IPAH-PASMC exhibited significantly larger (P=0.010) SOCE than NPH-PASMC [Figure 3a and b]. The siRNA-mediated knockdown of STIM2 in IPAH-PASMC led to a significant decrease (P=0.023) in the amplitude of SOCE [Figure 3b and c]. There was no significant difference in the magnitude of SR Ca2+ release, or a rise in [Ca2+]cyt due to Ca2+ leakage from the SR in NPH-PASMC, IPAH-PASMC treated with scramble siRNA, or IPAH-PASMC treated with siRNA-STIM2 (siSTIM2). Furthermore, there was no statistically significant difference (P=0.224) in SOCE between NPH-PASMC and IPAH-PASMC treated with siRNA-STIM2 [Figure 3b]. Western blot experiments also confirmed that the protein level of STIM2 was higher in IPAH-PASMC than in NPH-PASMC, and that siRNA-STIM2 effectively decreased the protein expression level of STIM2 in IPAH-PASMC [Figure 3c]. These data suggest that the increased protein expression level of STIM2 is necessary for enhanced SOCE in IPAH-PASMC.
STIM2 is necessary for the increased proliferation of PASMC from IPAH patientsProliferation of PASMC was determined by counting cells at the 0 hour (i.e., two days after the cells were plated onto the Petri dishes) and 24, 48, and 72 hours later. At the 0 hour, the control (NPH) PASMC group and IPAH-PASMC group had roughly the same number of cells [Figure 4a]. After 72 hours, the numbers of NPH-PASMC and IPAH-PASMC were both significantly increased [Figure 4a and b]; however, the increase in the IPAH-PASMC number was much greater that in the NPH-PASMC [Figure 4b]. Knockdown of STIM2 with siRNA had little effect on the change in the NPH-PASMC number after 72 hours [Figure 4c, left panel]. However, knockdown of STIM2 with siRNA in the IPAH-PASMC significantly decreased the increase
a NPH-PASMC IPAH-PASMC
STIM11.0
1.5
2.0
aliz
ed to
NPH
)
IPAHNPH 1 2 1 2
b
75
kD
0.0
0.5
1
STIM
1 Pr
otei
n Le
vel
(Nor
ma
NPH IPAH
β-tub
1.5
2.0
oN
PH)
*
STIM2
IPAHNPH 1 2 1 2
c
50
kD
0.0
0.5
1.0
1
STIM
2 Pr
otei
n L
evel
(N
orm
aliz
ed to
NPH IPAH
STIM2
β-tub
75
50
0 20.40.60.8
11.2
β-tub
STIM2
C 4 8 16 μlsiSTIM2
ba
75
50
kD
0.
1 2 3 4
STIM
2 Pr
otei
n Le
vel
(Nor
mal
ized
to C
ontro
l)
4C 16 μl8siSTIM2
Figure 1: Protein expression of STIM2, but not STIM1, is increased in IPAH patients’ PASMC. (a) Photograph showing that PASMC isolated from normotensive control subjects (NPH) and IPAH patients are morphologically comparable. (b and c) Representative Western blot images (left panels) and summarized data (right panels) for STIM1 (b) and STIM2 (c) proteins in PASMC isolated from IPAH patients’ lung tissues or normotensive control patient lung tissues (NPH). β-tubulin was used as a loading control. Summarized data of STIM1 (b, right panel) or STIM2 (c, right panel) protein expression level (mean±SE) in IPAH-PASMC (n=6) and NPH-PASMC (n=6). Graph shows protein expression of STIM1 and STIM2 normalized to an average level in NPH-PASMC. *P<0.05 versus NPH. STIM2 protein expression level was increased in IPAH-PASMC, but STIM1 protein expression level was not changed in IPAH-PASMC
Figure 2: Dose-dependent knockdown of STIM2 in IPAH patients’ PASMC with siRNA. (a) Representative Western blot image of STIM2 protein in IPAH-PASMC treated with siRNA against STIM2 (siSTIM2; with doses of 4, 8, and 16 μl) or control scrambled siRNA (indicated by ‘C’). β-tubulin (β-tub) was used as a loading control. (b) Quantifi cation of STIM2 protein expression level in IPAH-PASMC treated with control scrambled siRNA (‘C’) or 4, 8, and 16 μl of siRNA-STIM2. Values were normalized to the β-tub level at the start and then normalized to the level of cells treated with control scrambled siRNA. The STIM2 protein expression level in IPAH-PASMC was decreased in a dose-dependent manner by siRNA targeting STIM2
60, and 80%, respectively, compared to scrambled siRNA control [Figure 2a and b]. The 16 μl dose of 10 μM of siSTIM2 and scrambled siRNA (control siRNA) was chosen as the dose to knockdown STIM2 in the experiments shown a little later in the text.
STIM2 is necessary for enhanced SOCE in PASMC from IPAH patientsChange in [Ca2+]cyt was measured as the ratio of F340 / F380 (F) and normalized to the initial F340 / F380 ratio (F0), measured in PASMC superfused with physiological salt solution (PSS). SOCE was induced by the passive depletion of SR Ca2+ using 10 μM cyclopiazonic acid (CPA) in the absence of extracellular Ca2+, followed by re-addition of
Song, et al.: STIM2 and SOCE in PASMC

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 89
2 5 2 52 5 IPAH +siSTIM2NPH IPAHa
0.5
1.0
1.5
2.0
2.5
Rat
io (F
/F0)
0.5
1.0
1.5
2.0
2.5
Rat
io (F
/F0)
0.5
1.0
1.5
2.0
2.5
Rat
io (F
/F0)
10 min10 min 10 min
0 Ca2+CPA
0 Ca2+CPA
0 Ca2+CPA
IPAH +siSTIM2NPH IPAH
0.7
0.8
0.9
1
(F/F
0)
NPH IPAH IPAHsiSTIM2
STIM2
**
75
cb
kD
NPH
IPAH
IPAH +siSTIM2**
0.5
0.6
1
Cha
nge
in R
atio
SOCE
Figure 3: Upregulated protein expression of STIM2 is necessary for enhanced SOCE in IPAH patients’ PASMC. (a) Representative records show CPA-induced changes in [Ca2+]cyt in the absence or presence of extracellular Ca2+ in NPH-PASMC (NPH, left panel), IPAH-PASMC (IPAH, middle panel), and IPAH-PASMC treated with siRNA targeting STIM2 (IPAH + siSTIM2, right panel). SOCE (indicated by the CPA-induced increase in [Ca2+]cyt when extracellular Ca2+ is restored) is induced by the passive depletion of SR Ca2+ using 10 μM CPA. NPH-PASMC (left panel) and IPAH-PASMC (middle panel) were treated with scrambled siRNA as a control. (b) Summary data (mean±SE) showing changes in CPA-induced increase in [Ca2+]cyt, immediately following the re-addition of Ca2+ after store depletion (indicative of SOCE) in NPH-PASMC (black bar), IPAH-PASMC (red bar), and IPAH-PASMC, treated with siRNA-STIM2 (blue bar). **P<0.01 (NS, not signifi cant) versus NPH. (c) Western blot image of STIM2 protein expression in NPH-PASMC (NPH), IPAH-PASMC (IPAH), and IPAH-PASMC, treated with siRNA-STIM2 (IPAH + siSTIM2). NPH-PASMC (black) and IPAH-PASMC (red) were treated with scrambled siRNA
in cell number after 72 hours (P<0.001) [Figure 4c, right panel, and d]. The siRNA-STIM2-mediated knockdown of STIM2 appeared to attenuate IPAH-PASMC growth at an early time (24 hours) and lasted for at least 72 hours [Figure 4d]. These data indicated that upregulated STIM2 was necessary for the enhanced proliferation of IPAH-PASMC. Inhibition of STIM2 was an effective method to attenuate excessive proliferation of IPAH-PASMC; STIM2 could be a potential target for developing a novel therapeutic approach for patients with IPAH.
Overexpression of STIM2 is not sufficient to enhance SOCE in normal PASMCIn order to further examine the functional role of STIM2 in IPAH-PASMC, STIM2 was transiently transfected into NPH-PASMC, to determine whether overexpression of STIM2 was sufficient to enhance SOCE and increase proliferation in normal PASMC. STIM2 was overexpressed in NPH-PASMC in a dose-dependent manner [Figure 5]. One microgram of STIM2-cDNA significantly enhanced the protein expression of STIM2 both in HEK-293 cells (data not shown) and NPH-PASMC [Figure 5], and was used to overexpress STIM2 for the experiments described herewith.
Change in [Ca2+]cyt was measured as the ratio of F340 / F380 (F) and normalized to the initial F340 / F380 ratio (F0),
as described earlier. SOCE was induced by the passive depletion of SR Ca2+ with 10 μM CPA in NPH-PASMC, superfused with Ca2+-free solution followed by restoration of extracellular Ca2+ (1.8 mM). Overexpression of STIM2 in NPH-PASMC (48 hours after STIM2 transfection) had no significant effect on either the amplitude of the rise in [Ca2+]cyt due to Ca2+ release from the SR [Figure 6b, right panel] or the amplitude of SOCE [Figure 6b, right panel] when compared to the NPH-PASMC transfected with the control vector. In fact, overexpression of STIM2 caused a slight (but not statistically significant) decrease in the peak amplitude of SOCE [Figure 6b, right panel]. These data suggest that overexpression of STIM2 is not sufficient to enhance SOCE in normal PASMC.
Overexpression of STIM2 is not sufficient to increase proliferation in normal PASMCIn order to examine whether overexpression of STIM2 in normal PASMC would enhance cell proliferation, we measured and compared cell number changes in NPH-PASMC, transfected with a control vector and NPH-PASMC transfected with STIM2. As shown in Figure 7, overexpression of STIM2 failed to enhance the proliferation of NPH-PASMC; the increases in cell number were comparable between the control vector-transfected NPH-PASMC and STIM2-transfected NPH-PASMC. In these experiments, proliferation of PASMC was determined by
Song, et al.: STIM2 and SOCE in PASMC

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 90
1
2
3
4
5
Cel
l Num
ber
(x10
5 )
1
2
3
4
5
(x10
5 )
***
*****
0 hrs72 hrs
a b
01
3
4
5
105 )
NPH
01
Incr
ease
inC
ell N
umbe
r
IPAHNPH
3
4
5
105 )
IPAH
NS
IPAHNPHc
0
1
2
1
Incr
ease
in C
ell N
umbe
r (x
1
siS2siC0
1
2
1
Incr
ease
in C
ell N
umbe
r
(x1
siS2siC
**
4
5
IPAH siC
d
0
1
2
3
4
0 24 48 72
Cel
l Num
ber
(x10
5 )
Time (hrs)
IPAH +siS2
Figure 4: Knockdown of STIM2 mitigates enhanced proliferation in IPAH patients’ PASMC. (a) Summary data (mean±SE) showing cell numbers for NPH-PASMC and IPAH-PASMC before (0 hour) and after 72 hours of culture in the growth media. *** P<0.001 versus 0 hour. (b) Summary data showing the increase in cell numbers after 72 hours in NPH-PASMC (blue) and IPAH-PASMC (red). ** P<0.01 versus NPH. IPAH patients’ PASMC showed a signifi cantly greater increase in cell number after 72 hours compared to NPH-PASMC. (c) Summary data showing the increase in cell number after 72 hours in NPH-PASMC (left panel) and IPAH-PASMC (right panel) treated with either scrambled siRNA (siC) or siRNA against STIM2 (siS2). Decreasing the protein expression level of STIM2 did not affect the increase in cell number after 72 hours in NPH-PASMC (left panel), but signifi cantly inhibited the increase in cell number after 72 hours in IPAH-PASMC (right panel). ** P<0.01 versus siC. (d) Summary data showing the total number of IPAH-PASMC cultured in growth media at 0, 24, 48, and 72 hours. The cells were treated with scrambled siRNA (square symbols) or siRNA against STIM2 (circle symbols). IPAH-PASMC treated with siRNA-STIM2 had a slower rate of proliferation than IPAH-PASMC treated with scrambled siRNA. The growth curves in IPAH-PASMC treated with scrambled siRNA and siRNA against STIM2 were signifi cantly different
1
1.52
2.5
3
M2
Prot
ein
Leve
lm
aliz
ed to
β-tu
b)
β-tub
STIM2
C 1 2 4 μgsiSTIM2
75
50
ba
kD
0
0.5
1 2 3 4
STI
(Nor
m
1C 42STIM2
50
1.0
1.5
2.0
Rat
io (F
/F0)
1.0
1.5
2.0
Rat
io (F
/F0)
Rat
io (F
/F0)
Rat
io (F
/F0)
10 min 10 min 2MITSlortnoC
CPA CPA
a
0.50.5
0.6
0.8
1
0.6
0.8
1
0 Ca2+CPA0 Ca2+CPA
b
0
0.2
0.4
0
0.2
0.4
SR Ca2+ Release SOCE
Control STIM2
Figure 5: Dose-dependent overexpression of STIM2 in NPH-PASMC transiently transfected with siRNA. (a) Representative Western blot image of STIM2 protein in NPH-PASMC. STIM2 was overexpressed using 1, 2, or 4 μg of DNA. Vector DNA was used as a control (‘C’). β-tubulin (β-tub) was used as a loading control. (b) Quantifi cation of STIM2 protein expression level in NPH-PASMC transfeted with vector DNA (‘C’) and 1, 2, or 4 μg of STIM2-DNA. Values were normalized to β-tubulin. STIM2 protein expression level was increased in a dose-dependent manner in NPH-PASMC transfected with STIM2
Figure 6: Overexpression of STIM2 is not suffi cient to enhance SOCE in normal PASMC. (a) Representative records showing changes in [Ca2+]cyt before, during, and after the application of CPA (10 μM), in the absence or presence of extracellular Ca2+ in the vector control (left panel) and STIM2-transfected (right panel) NPH-PASMC. SOCE was induced by the passive depletion of SR Ca2+, using CPA. (b) Summary data (mean±SE) showing changes in [Ca2+]cyt immediately following the addition of CPA in the absence of extracellular Ca2+, which refl ects SR Ca2+ release (SR Ca2+ Release, left panel), in control (black) and STIM2-transfected (red) NPH-PASMC. There was no difference in magnitude of SR Ca2+ release between the two groups. Summary data (mean±SE) showing changes in [Ca2+]cyt immediately following the re-addition of Ca2+ after CPA-induced store depletion (indicative of SOCE, right panel) in control (black) and STIM2-overexpressing PASMC (red). There was no difference in magnitude of SOCE between the two groupscounting the cells at time 0 and 72 hours. Transfection
of PASMC with either STIM2 cDNA or the control vector was performed 48 hours prior to time 0. At time 0, PASMC transfected with STIM2 or the control vector had the same number of cells to start with. After 72 hours, both the control vector- and STIM2-transfected PASMC proliferated,
but the increase in cell number was similar between NPH-PASMC transfected with a control vector and STIM2 [Figure 7]. These data suggest that overexpression of STIM2 is not sufficient to enhance the proliferation of normal PASMC.
Song, et al.: STIM2 and SOCE in PASMC

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 91
Figure 9: Protein expression of Orai2 was increased in IPAH patients’ PASMC. (a) Representative Western blot image for Orai2 protein from IPAH-PASMC and NPH-PASMC. β-tubulin (β-tub) was used as a loading control. (b) Summarized data (mean±SE) comparing protein expression level of Orai2 in IPAH-PASMC to NPH-PASMC. Values were normalized to β-tubulin. IPAH patients’ PASMC had signifi cantly higher protein expression level of Orai2 compared to NPH-PASMC. *** P<0.001 versus NPH
0.4
0.8
1.2
1.6
2
Ora
i2 P
rote
in L
evel
(Nor
mal
ized
toN
PH)
***
Orai2
β-tub
IPAHNPH 1 2 1 2
25
50
ba
kD
0
0.4
1NPH IPAH
Chronic hypoxia increases protein expression of Orai2 and STIM2 in rat PASMCChronic hypoxia causes pulmonary hypertension by increasing PASMC proliferation, migration, and contraction through, at least partially, a Ca2+-dependent mechanism.[25,26] Chronic hypoxia has been reported to inhibit voltage-gated K+ (KV) channels, cause membrane depolarization, open
0 hra b
2
4
6
8
10
12
Cel
l Num
ber
(x10
4 )
1
2
3
4
5
6
Incr
ese
in C
ell N
umbe
r(x
104 )
0 72 hrs
**
0
2
1
0
1
1STIM2Vector STIM2Vector
Figure 7: Overexpression of STIM2 does not increase NPH-PASMC proliferation. (a) Summary data for NPH-PASMC proliferation after 72 hours. Cell number was counted at time zero (0 hours: white bar) and 72 hours (72 hours: black bar) and shown as the multiple of 104. After 72 hours, both vector control and STIM2-overexpressing NPH-PASMC increased in cell number. *P<0.05 versus open bars (0 hour). (b) Summary data (mean±SE) showing the increase in cell number after 72 hours in NPH-PASMC. STIM2-overexpressing PASMC (STIM2) did not show a greater increase in cell number after 72 hours compared to control (vector). Cell counts were repeated four times (n=4)
2.5 **HypNora
0
0.5
1
1.5
2
Ora
i2 P
rote
in L
evel
(Nor
mal
ized
to N
or)
HN
Orai2
β-tub
1 2 1 2
1 2 1 2
25
50
kD
1HypNo r
STIM2
1
1.5
2
2.5
Prot
ein
Leve
lm
aliz
ed to
Nor
) **
HypNorb
75
kD
β-tub
0
0.5
1
STIM
2 (N
orm
Nor Hyp
50
Figure 8: Hypoxia increases protein expression of STIM2 and Orai2 in rat PASMC. (a) and (b). Representative Western blot images (left panels) and summarized data (mean±SE) showing protein levels (right panels) for Orai2 (a) and STIM2 (b) protein in rat PASMC exposed to normoxia (Nor, room air supplemented with 5% CO2) or hypoxia (Hyp, 3% O2 and 5% CO2 balanced in N2 for 48 hours). β-tubulin (β-tub) was used as a loading control. Values were normalized to β-tubulin. Hypoxia increased the protein expression of Orai2 and STIM2 in rat PASMC. ** P<0.01 versus Nor
voltage-gated Ca2+ channels, and increase [Ca2+]cyt in PASMC by increased Ca2+ influx through voltage-gated Ca2+ channels. Chronic hypoxia has also been shown to upregulate the TRPC channels in rat PASMC and increase [Ca2+]cyt via enhanced receptor-operated and store-operated Ca2+ influx.[4,5,27-29] To investigate whether the upregulation of STIM2 is also involved in hypoxia-mediated pulmonary vasoconstriction and vascular remodeling, we exposed rat PASMC to hypoxia (PO2=22 mmHg for 48 hours) and examined the protein expression level of STIM2 and Orai2; in these experiments, we used β-tubulin as the loading control. As shown in Figure 8, chronic hypoxia significantly upregulated Orai2 [Figure 8a] and STIM2 [Figure 8b] protein expression levels in normal rat PASMC. These data are consistent with our earlier findings, where STIM2 protein expression levels were increased in PASMC from IPAH patients. Furthermore, increased protein expression of Orai2 in hypoxia-treated rat PASMC might also explain our finding that STIM2 alone is insufficient to enhance SOCE and proliferation in normal PASMC.
Upregulated Orai2 protein expression in PASMC from IPAH patientsAs shown in Figure 3 and our previously published data,[17,22,24,30] PASMC from IPAH patients showed enhanced SOCE compared to control PASMC. In addition, IPAH-PASMC showed elevated protein expression of STIM2, but not STIM1 [Figure 1]. Furthermore, while increased protein expression levels of STIM2 were necessary for enhanced SOCE in IPAH-PASMC, overexpression of STIM2 alone was not sufficient to enhance SOCE in NPH-PASMC. Therefore, we examined whether the protein expression of Orai2, a store-operated Ca2+ channel protein, was increased in PASMC from IPAH patients. As shown in Figure 9, the Orai2 protein expression level was significantly higher in IPAH-PASMC than in NPH-PASMC. Taken together, these data suggest that upregulated Orai2, in addition to upregulated STIM2 (this study) and TRPC3 / 6,[22,24] may
Song, et al.: STIM2 and SOCE in PASMC

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 92
also be important in enhancing SOCE in PASMC from IPAH patients.
DISCUSSION
A rise in [Ca2+]cyt is a major trigger for pulmonary vasoconstriction and is an important stimulus for PASMC proliferation, which leads to pulmonary vascular remodeling.[31,32] Human and animal PASMC functionally express many signal transduction proteins and kinases (e.g., calmodulin, CaMK, MAPK, and calcineurin) and transcription factors (e.g., CREB, c-Fos/c-Jun, c-Myc, NFAT, NF-κB) that are sensitive to changes in [Ca2+]cyt or Ca2+-calmodulin (CaM).[33] An increase in [Ca2+]cyt can rapidly increase [Ca2+] in the nuclei[6,34-36] and stimulate nuclear events that are related to cell proliferation. In the cell cycle, it has been well-demonstrated that there are at least four steps that are regulated by Ca2+ or Ca2+ /CaM: the transition from the G0 to the G1 phase, the transition from the G1 to the S phase, the transition from the S to the M phase, and the whole process in the M phase.[37-40] In isolated pulmonary arterial rings, removal of extracellular Ca2+ abolished high K+-mediated pulmonary vasoconstriction and significantly inhibited agonist-mediated pulmonary vasoconstriction.[31,41,42] In cultured PASMC, reduction of free Ca2+ concentration in the culture medium significantly inhibited cell proliferation in the presence of growth factors, while depletion of intracellularly stored Ca2+ in the sarcoplasmic or endoplasmic reticulum also significantly attenuated smooth muscle cell proliferation.[43-45] In addition, Ca2+ is an important signal in initiating and guiding cell migration.[46-51] These observations indicate that intracellular Ca2+ signaling, regulated by Ca2+ influx through Ca2+-permeable channels; Ca2+ extrusion via Ca2+-Mg2+ ATPase (Ca2+ pumps) in the plasma membrane; Ca2+ release through IP3 / ryanadine receptors; and Ca2+ uptake via the Ca2+–Mg2+ ATPase (SERCA) on the SR / ER membrane, play an important role in the regulation of smooth muscle cell contraction, migration, and proliferation. Significantly, the upregulated expression of Ca2+-permeable channels and enhanced Ca2+ influx through these channels would thus cause sustained vasoconstriction, stimulate smooth muscle cell migration and proliferation, and ultimately cause vascular wall thickening.
IPAH-PASMC demonstrated significantly enhanced SOCE and proliferated faster compared to NPH-PASMC.[22,24,30] In this study, we have shown that STIM2 is necessary but insufficient for the enhancement of SOCE in IPAH-PASMC. Many studies have shown that STIM1 can enhance SOCE when overexpressed in a variety of cell types.[8,10,12,52,53] This lead us to hypothesize that STIM1 protein expression will be upregulated in IPAH-PASMC. Surprisingly STIM2, but not STIM1 protein expression,
is increased in IPAH-PASMC compared to NPH-PASMC. These findings are consistent with the observations which show that protein expression of STIM2 is upregulated in rat PASMC subjected to hypoxia (48 hours). These data suggest that STIM2 may be the important isoform for pathophysiological increase in SOCE in PASMC from IPAH patients.
Further examination showed that STIM2 played an important functional role in both augmented SOCE and enhanced proliferation in IPAH-PASMC. Increased protein expression of STIM2 in IPAH-PASMC was necessary for increased SOCE compared to NPH-PASMC. When the STIM2 protein expression level in IPAH-PASMC was decreased to the level similar to NPH-PASMC, IPAH-PASMC no longer exhibited enhanced SOCE or enhanced proliferation. However, overexpression of STIM2 alone could not enhance SOCE or proliferation in NPH-PASMC, suggesting that STIM2 did not act alone in eliciting the pathophysiological changes in PASMC associated with IPAH. Taken together, these findings suggested that STIM2 was necessary, but not sufficient, for the enhanced proliferation and SOCE found in IPAH-PASMC. Functional interaction of STIM2 with STIM1 and / or Orai and TRPC channels might also be important.
As mentioned earlier, STIM2 overexpression had no effect on SOCE or proliferation in NPH-PASMC, while knockdown of STIM2 in IPAH-PASMC decreased both SOCE and the proliferation. Therefore, it seems that STIM2 was functionally active only in IPAH-PASMC and had no or little function in NPH-PASMC. Several explanations could explain how STIM2 was ‘turned on’ in IPAH, but not in NPH-PASMC. STIM2 could be activated by phosphorylation or another form of post-translational modification. It is widely accepted that Rho/Rho-associated protein kinase (ROCK) signaling is involved in Ca2+ sensitization, proliferation, contraction, and migration in PASMC.[54] Researchers have demonstrated that the Rho/ ROCK signaling pathway plays a significant role in the pathogenesis of different experimental models of PAH as well as PAH in patients.[55-60] Perhaps the pathogenesis of IPAH involves RhoA / ROCK signaling though STIM2.
A second explanation for how STIM2 is only active in IPAH-PASMC, but not NPH-PASMC, involves store-operated channels (SOC) on the plasma membrane. Strong evidence suggests that Orai1 interacts with STIM1 and functions as an SOC. Orai1 was discovered through genome-wide RNAi screening. A mutation in Orai1 in patients with severe combined immune deficiency eliminates the Ca2+ release-activated Ca2+ currents (ICRAC), which can then be reconstituted by expressing the wild-type Orai1.[61,62] Orai1 spans the plasma membrane four times, with both the C- and N- termi, in the cytoplasm. Co-expression of STIM1
Song, et al.: STIM2 and SOCE in PASMC

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 93
with Orai1 in the HEK293 cells results in large increases in SOCE and ICRAC compared to the vector control cells.[12,13] The co-immunoprecipitation data shows that STIM1 and Orai1 interact and store depletion significantly increases the amount to an interaction.[63] Furthermore, other isoforms of Orai (e.g., Orai2 and Orai3) are also believed to play a role in SOCE.[62] Our laboratory has previously demonstrated that TRPC channels also function as SOC and are important in PASMC physiology and pathophysiology.[22-24,31,64] TRPC channels are important in the regulation of vascular tone, as they regulate the Ca2+ influx required for agonist-induced vasoconstriction and mitogen-mediated smooth muscle cell proliferation. Moreover, the ability of the TRPC channels to alter [Ca2+]cyt without a change in the membrane potential, lends them the ability to modulate vasoconstriction and vasorelaxation through a voltage-independent mechanism. Agonist- and hypoxia-induced pulmonary vasoconstriction is believed to be, at least in part, mediated through the Ca2+ influx, through the TRPC1 and TRPC6 channels.[23,65] Upregulated TRPC channel expression, enhanced SOCE, and increased [Ca2+]cyt are associated with the enhanced proliferation of PASMC isolated from IPAH patients.[21,22] Therefore, increased SOCE and proliferation in the IPAH-PASMC may be functions of both increased protein expression of STIM2 and increased protein expression of SOC, such as, Orai1/2 or TRPC1/3/6, or TRPC in the plasma membrane. Corroborating this idea, we found enhanced protein expression of Orai2 in both the hypoxia-treated rat PASMC and IPAH-PASMC. It is, however, unknown whether STIM2 can functionally interact with both the Orai2 and TRPC channels, to enhance SOCE in PASMC from IPAH patients; this is a research project we are currently pursuing.
In conclusion, upregulated protein expression of STIM2, a Ca2+ sensor that senses the level of Ca2+ in the sarcoplasmic reticulum and mediates SOCE by recruiting and activating SOC in the plasma membrane, is necessary for the augmented SOCE and enhanced proliferation in PASMC from IPAH patients. Downregulation of STIM2 protein expression and / or inhibition of STIM2 protein function in PASMC may be an important target for developing therapeutic approaches for IPAH. As upregulation of STIM2 alone, in normal PASMC, is not sufficient to enhance SOCE, it is likely that STIM2 functionally and physically interacts with other proteins (e.g., Orai2, TRPC3 / TRPC6) involved in forming SOC to regulate SOCE in normal PASMC and cause enhanced SOCE and proliferation in PASMC from IPAH patients.
ACKNOWLEDGMENTS
We thank Amy Zeifman for her critical review of the manuscript, and Anthony Ngo and Dr. Ling Zhu for their technical assistance.
This study has been supported, in part, by grants from the National Institutes of Health (HL066012 and HL 098053 to JX-JY and DK 083506 to AM). M.Y. Song is supported by a pre-doctoral training grant from the National Institutes of Health (T32 DK07202).
REFERENCES
1. Morrell NW, Adnot S, Archer SL, Dupuis J, Jones PL, MacLean MR, et al. Cellular and molecular basis of pulmonary arterial hypertension. J Am Coll Cardiol 2009;54:S20-31.
2. Hassoun PM, Mouthon L, Barbera JA, Eddahibi S, Flores SC, Grimminger F, et al. Infl ammation, growth factors, and pulmonary vascular remodeling. J Am Coll Cardiol 2009;54:S10-9.
3. Firth AL, Mandel J, Yuan JX. Idiopathic pulmonary arterial hypertension. Dis Model Mech 2010;3:268-73.
4. Lu W, Wang J, Peng G, Shimoda LA, Sylvester JT. Knockdown of stromal interaction molecule 1 att enuates store-operated Ca2+ entry and Ca2+ responses to acute hypoxia in pulmonary arterial smooth muscle. Am J Physiol Lung Cell Mol Physiol 2009;297:L17-25.
5. Lu W, Wang J, Shimoda LA, Sylvester JT. Diff erences in STIM1 and TRPC expression in proximal and distal pulmonary arterial smooth muscle are associated with diff erences in Ca2+ responses to hypoxia. Am J Physiol Lung Cell Mol Physiol 2008;295:L104-13.
6. Berridge MJ, Bootman MD, Roderick HL. Calcium signalling: dynamics, homeostasis and remodelling. Nat Rev Mol Cell Biol 2003;4:517-29.
7. Cahalan MD. STIMulating store-operated Ca2+ entry. Nat Cell Biol 2009;11:669-77.
8. Abdullaev IF, Bisaillon JM, Potier M, Gonzalez JC, Motiani RK, Trebak M. Stim1 and Orai1 mediate CRAC currents and store-operated calcium entry important for endothelial cell Proliferation. Circ Res 2008;23:1289-99.
9. Zhang SL, Yu Y, Roos J, Kozak JA, Deerinck TJ, Ellisman MH, et al. STIM1 is a Ca2+ sensor that activates CRAC channels and migrates from the Ca2+ store to the plasma membrane. Nature 2005;437:902-5.
10. Luik RM, Wang B, Prakriya M, Wu MM, Lewis RS. Oligomerization of STIM1 couples ER calcium depletion to CRAC channel activation. Nature 2008;454:538-42.
11. Ross PE, Cahalan MD. Ca2+ infl ux pathways mediated by swelling or stores depletion in mouse thymocytes. J Gen Physiol 1995;106:415-44.
12. Soboloff J, Spassova MA, Hewavitharana T, He LP, Xu W, Johnstone LS, et al. STIM2 is an inhibitor of STIM1-mediated store-operated Ca2+ entry. Curr Biol 2006;16:1465-70.
13. Soboloff J, Spassova MA, Tang XD, Hewavitharana T, Xu W, Gill DL. Orai1 and STIM reconstitute store-operated calcium channel function. J Biol Chem 2006;281:20661-5.
14. Darbellay B, Arnaudeau S, Ceroni D, Bader CR, Konig S, Bernheim L. Human muscle economy myoblast diff erentiation and excitation-contraction coupling use the same molecular partners, STIM1 and STIM2. J Biol Chem;285:22437-47.
15. El Boustany C, Katsogiannou M, Delcourt P, Dewailly E, Prevarskaya N, Borowiec AS, et al. Diff erential roles of STIM1, STIM2 and Orai1 in the control of cell proliferation and SOCE amplitude in HEK293 cells. Cell Calcium;47:350-9.
16. Yu Y, Sweeney M, Zhang S, Platoshyn O, Landsberg J, Rothman A, et al. PDGF stimulates pulmonary vascular smooth muscle cell proliferation by upregulating TRPC6 expression. Am J Physiol Cell Physiol 2003;284:C316-30.
17. Sweeney M, Yu Y, Platoshyn O, Zhang S, McDaniel SS, Yuan JX. Inhibition of endogenous TRP1 decreases capacitative Ca2+ entry and att enuates pulmonary artery smooth muscle cell proliferation. Am J Physiol Lung Cell Mol Physiol 2002;283:L144-55.
18. Cahalan MD, Zhang SL, Yeromin AV, Ohlsen K, Roos J, Stauderman KA. Molecular basis of the CRAC channel. Cell Calcium 2007;42:133-44.
19. Burg ED, Platoshyn O, Tsigelny IF, Lozano-Ruiz B, Rana BK, Yuan JX. Tetramerization domain mutations in KCNA5 aff ect channel kinetics and cause abnormal traffi cking patt erns. Am J Physiol Cell Physiol 2009;298:C496-509.
20. Firth AL, Remillard CV, Yuan JX. TRP channels in hypertension. Biochim Biophys Acta 2007;1772:895-906.
21. Yu Y, Fantozzi I, Remillard CV, Landsberg JW, Kunichika N, Platoshyn O, et al. Enhanced expression of transient receptor potential channels in idiopathic pulmonary arterial hypertension. Proc Natl Acad Sci USA 2004;101:13861-6.
Song, et al.: STIM2 and SOCE in PASMC

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 94
22. Yu Y, Keller SH, Remillard CV, Safrina O, Nicholson A, Zhang SL, et al. A functional single-nucleotide polymorphism in the TRPC6 gene promoter associated with idiopathic pulmonary arterial hypertension. Circulation 2009;119:2313-22.
23. Krick S, Platoshyn O, Sweeney M, McDaniel SS, Zhang S, Rubin LJ, et al. Nitric oxide induces apoptosis by activating K+ channels in pulmonary vascular smooth muscle cells. Am J Physiol Heart Circ Physiol 2002;282:H184-93.
24. Brevnova EE, Platoshyn O, Zhang S, Yuan JX. Overexpression of human KCNA5 increases IK(V) and enhances apoptosis. Am J Physiol Cell Physiol 2004;287:C715-22.
25. Yuan JX, Rubin LJ. Pathogenesis of pulmonary arterial hypertension: the need for multiple hits. Circulation 2005;111:534-8.
26. Sweeney M, Yuan JX. Hypoxic pulmonary vasoconstriction: role of voltage-gated potassium channels. Respir Res 2000;1:40-8.
27. Peng G, Lu W, Li X, Chen Y, Zhong N, Ran P, et al. Expression of store-operated Ca2+ entry and transient receptor potential canonical and vanilloid-related proteins in rat distal pulmonary venous smooth muscle. Am J Physiol Lung Cell Mol Physiol 2010;299:L621-30.
28. Shimoda LA, Wang J, Sylvester JT. Ca2+ channels and chronic hypoxia. Microcirculation 2006;13:657-70.
29. Lin MJ, Leung GP, Zhang WM, Yang XR, Yip KP, Tse CM, et al. Chronic hypoxia-induced upregulation of store-operated and receptor-operated Ca2+ channels in pulmonary arterial smooth muscle cells: A novel mechanism of hypoxic pulmonary hypertension. Circ Res 2004;95:496-505.
30. Zhang S, Dong H, Rubin LJ, Yuan JX. Upregulation of Na+/Ca2+ exchanger contributes to the enhanced Ca2+ entry in pulmonary artery smooth muscle cells from patients with idiopathic pulmonary arterial hypertension. Am J Physiol Cell Physiol 2007;292:C2297-305.
31. Golovina VA, Platoshyn O, Bailey CL, Wang J, Limsuwan A, Sweeney M, et al. Upregulated TRP and enhanced capacitative Ca2+ entry in human pulmonary artery myocytes during proliferation. Am J Physiol Heart Circ Physiol 2001;280:H746-55.
32. Mandegar M, Fung YC, Huang W, Remillard CV, Rubin LJ, Yuan JX. Cellular and molecular mechanisms of pulmonary vascular remodeling: Role in the development of pulmonary hypertension. Microvasc Res 2004;68:75-103.
33. Berridge MJ. Calcium signalling and cell proliferation. Bioessays 1995;17:491-500.
34. Allbritt on NL, Oancea E, Kuhn MA, Meyer T. Source of nuclear calcium signals. Proc Natl Acad Sci U S A 1994;91:12458-62.
35. Wu G, Xie X, Lu ZH, Ledeen RW. Sodium-calcium exchanger complexed with GM1 ganglioside in nuclear membrane transfers calcium from nucleoplasm to endoplasmic reticulum. Proc Natl Acad Sci 2009;106:10829-34.
36. Faury G, Usson Y, Robert-Nicoud M, Robert L, Verdett i J. Nuclear and cytoplasmic free calcium level changes induced by elastin peptides in human endothelial cells. Proc Natl Acad Sci U S A 1998;95:2967-72.
37. Rodriguez-Mora OG, LaHair MM, McCubrey JA, Franklin RA. Calcium/calmodulin-dependent kinase I and calcium/calmodulin-dependent kinase kinase participate in the control of cell cycle progression in MCF-7 human breast cancer cells. Cancer Res 2005;65:5408-16.
38. Kahl CR, Means AR. Regulation of cell cycle progression by calcium/calmodulin-dependent pathways. Endocr Rev 2003;24:719-36.
39. Karcher RL, Roland JT, Zappacosta F, Huddleston MJ, Annan RS, Carr SA, et al. Cell cycle regulation of myosin-V by calcium/calmodulin-dependent protein kinase II. Science 2001;293:1317-20.
40. Planas-Silva MD, Means AR. Expression of a constitutive form of calcium/calmodulin dependent protein kinase II leads to arrest of the cell cycle in G2. EMBO J 1992;11:507-17.
41. Platoshyn O, Golovina VA, Bailey CL, Limsuwan A, Krick S, Juhaszova M, et al. Sustained membrane depolarization and pulmonary artery smooth muscle cell proliferation. Am J Physiol Cell Physiol 2000;279:C1540-9.
42. McDaniel SS, Platoshyn O, Wang J, Yu Y, Sweeney M, Krick S, et al. Capacitative Ca2+ entry in agonist-induced pulmonary vasoconstriction. Am J Physiol Lung Cell Mol Physiol 2001;280:L870-80.
43. Waldron RT, Short AD, Meadows JJ, Ghosh TK, Gill DL. Endoplasmic reticulum calcium pump expression and control of cell growth. J Biol Chem 1994;269:11927-33.
44. Ufret-Vincenty CA, Short AD, Alfonso A, Gill DL. A novel Ca2+ entry mechanism is turned on during growth arrest induced by Ca2+ pool depletion. J Biol Chem 1995;270:26790-3.
45. Waldron RT, Short AD, Gill DL. Thapsigargin-resistant intracellular calcium pumps. Role in calcium pool function and growth of thapsigargin-
resistant cells. J Biol Chem 1995;270:11955-61.46. Wei C, Wang X, Chen M, Ouyang K, Zheng M, Cheng H. Flickering
calcium microdomains signal turning of migrating cells. Can J Physiol Pharmacol;88:105-10.
47. Wei C, Wang X, Chen M, Ouyang K, Song LS, Cheng H. Calcium fl ickers steer cell migration. Nature 2009;457:901-5.
48. Pfl eiderer PJ, Lu KK, Crow MT, Keller RS, Singer HA. Modulation of vascular smooth muscle cell migration by calcium/ calmodulin-dependent protein kinase II-delta 2. Am J Physiol Cell Physiol 2004;286:C1238-45.
49. Lundberg MS, Curto KA, Bilato C, Monticone RE, Crow MT. Regulation of vascular smooth muscle migration by mitogen-activated protein kinase and calcium/calmodulin-dependent protein kinase II signaling pathways. J Mol Cell Cardiol 1998;30:2377-89.
50. Bilato C, Curto KA, Monticone RE, Pauly RR, White AJ, Crow MT. The inhibition of vascular smooth muscle cell migration by peptide and antibody antagonists of the alphavbeta3 integrin complex is reversed by activated calcium/calmodulin- dependent protein kinase II. J Clin Invest 1997;100:693-704.
51. Pauly RR, Bilato C, Sollott SJ, Monticone R, Kelly PT, Lakatta EG, et al. Role of calcium/calmodulin-dependent protein kinase II in the regulation of vascular smooth muscle cell migration. Circulation 1995;91:1107-15.
52. Burg ED, Remillard CV, Yuan JX. Potassium channels in the regulation of pulmonary artery smooth muscle cell proliferation and apoptosis: Pharmacotherapeutic implications. Br J Pharmacol 2008;153 Suppl 1:S99-S111.
53. Potier M, Gonzalez JC, Motiani RK, Abdullaev IF, Bisaillon JM, Singer HA, et al. Evidence for STIM1- and Orai1-dependent store-operated calcium infl ux through ICRAC in vascular smooth muscle cells: Role in proliferation and migration. Faseb J 2009;23:2425-37.
54. Wirth A. Rho kinase and hypertension. Biochim Biophys Acta 2010;1802:1276-84.
55. Connolly MJ, Aaronson PI. Key role of the RhoA/Rho kinase system in pulmonary hypertension. Pulm Pharmacol Ther 2011;24:14.
56. Ward JP, McMurtry IF. Mechanisms of hypoxic pulmonary vasoconstriction and their roles in pulmonary hypertension: New fi ndings for an old problem. Curr Opin Pharmacol 2009;9:287-96.
57. Oka M, Fagan KA, Jones PL, McMurtry IF. Therapeutic potential of RhoA/Rho kinase inhibitors in pulmonary hypertension. Br J Pharmacol 2008;155:444-54.
58. Homma N, Nagaoka T, Karoor V, Imamura M, Taraseviciene-Stewart L, Walker LA, et al. Involvement of RhoA/Rho kinase signaling in protection against monocrotaline-induced pulmonary hypertension in pneumonectomized rats by dehydroepiandrosterone. Am J Physiol Lung Cell Mol Physiol 2008;295:L71-8.
59. Oka M, Homma N, McMurtry IF. Rho kinase-mediated vasoconstriction in rat models of pulmonary hypertension. Methods Enzymol 2008;439:191-204.
60. Nagaoka T, Gebb SA, Karoor V, Homma N, Morris KG, McMurtry IF, et al. Involvement of RhoA/Rho kinase signaling in pulmonary hypertension of the fawn-hooded rat. J Appl Physiol 2006;100:996-1002.
61. Feske S, Gwack Y, Prakriya M, Srikanth S, Puppel SH, Tanasa B, et al. A mutation in Orai1 causes immune defi ciency by abrogating CRAC channel function. Nature 2006;441:179-85.
62. Mercer JC, Dehaven WI, Smyth JT, Wedel B, Boyles RR, Bird GS, et al. Large store-operated calcium selective currents due to co-expression of Orai1 or Orai2 with the intracellular calcium sensor, Stim1. J Biol Chem 2006;281:24979-90.
63. Yeromin AV, Zhang SL, Jiang W, Yu Y, Safrina O, Cahalan MD. Molecular identifi cation of the CRAC channel by altered ion selectivity in a mutant of Orai. Nature 2006;443:226-9.
64. Du L, Sullivan CC, Chu D, Cho AJ, Kido M, Wolf PL, et al. Signaling molecules in nonfamilial pulmonary hypertension. N Engl J Med 2003;348:500-9.
65. Kunichika N, Landsberg JW, Yu Y, Kunichika H, Thistlethwaite PA, Rubin LJ, et al. Bosentan inhibits transient receptor potential channel expression in pulmonary vascular myocytes. Am J Respir Crit Care Med 2004;170:1101-7.
Source of Support: National Institutes of Health (HL066012 & HL 098053 to JX-JY and DK 083506 to AM), Pre-doctoral training to MY Song
(T32 DK07202) from the National Institutes of Health, Confl ict of Interest: None declared.
Song, et al.: STIM2 and SOCE in PASMC

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 95
INTRODUCTION
Pulmonary hypertension (PH) in the medical intensive care unit patient population is not well characterized. PH in the intensive care unit may be due to pre-existing pulmonary vascular disease or may occur acutely as a response to de novo cardiac, lung, or vascular injury.[1] Prior investigation of PH in critically ill patients has been limited to the description of PH in association with certain disorders such as acute respiratory distress syndrome
Doppler-defi ned pulmonary hypertension in medical intensive care unit patients:
Retrospective investigation of risk factors and impact on mortality
Jason A. Stamm1, Bryan J. McVerry1, Michael A. Mathier2, Michael P. Donahoe1, Melissa I. Saul3, Mark T. Gladwin1,4
1Department of Pulmonary, Allergy, and Critical Care Medicine and 2Cardiovascular Institute, University of Pittsburgh Medical Center, 3Department of Biomedical Informatics and 4Vascular Medicine Institute, University of Pittsburgh School of Medicine,
Pittsburgh, Pennsylvania, USA
ABSTRACT
Pulmonary hypertension (PH) is poorly characterized in the critically ill. No prior studies describe the burden of or outcomes associated with PH in a general medical intensive care unit population. We hypothesize that PH is an important comorbidity prevalent in the modern medical intensive care unit. We undertook a preliminary investigation to defi ne the consequences of Doppler-defi ned PH in the critically ill. A single-center retrospective case–control study of medical intensive care patients admitted over a 1-year period was conducted. Eligible patients had an echocardiogram within 4 days of admission. PH was defi ned to include both pulmonary arterial and venous hypertension and required a tricuspid regurgitant jet velocity ≥3 m/sec. Cases and controls were compared for comorbidities, illness severity, diagnoses, and mortality. Multivariable regression was performed to identify clinical features associated with PH and mortality. 299 (21% of admissions) patients had an eligible echocardiogram. Patients with PH (N=126) had a higher unadjusted mortality than did controls (N=173) (37% vs. 25%, P=0.04) and PH remained signifi cantly associated with mortality after controlling for other clinical factors (HR=1.59, 95% CI=1.03–2.44, P=0.036). Low ejection fraction (OR=2.21, 95% CI=1.19–4.11, P=0.012) and pulmonary embolism (OR=4.28, 95% CI=1.59–11.5, P=0.004) were independently associated with PH. Doppler-defi ned PH is associated with mortality in the critically ill. Prospective studies are needed to defi ne the prevalence of pulmonary venous hypertension versus pulmonary arterial hypertension, and the clinical consequences of each, in a general medical intensive care unit population.
Key Words: Critical illness, echocardiography, pulmonary arterial hypertension, pulmonary venous hypertension
Research Ar t ic le
(ARDS), pulmonary embolism, or after cardiothoracic surgery.[2-9] Much less is known of the overall incidence of PH in an unselected critically ill population; moreover, the association of PH with clinical outcomes in a general medical intensive care unit population has not been previously reported.
Access this article online
Quick Response Code:Website: www.pulmonarycirculation.org
DOI: 10.4103/2045-8932.78104
Pulm Circ 2011;1:95-102
Address correspondence to:Dr. Mark T. GladwinDivision of Pulmonary, Allergy and Critical Care Medicine,University of Pittsburgh Medical Center, NW 628 Montefi ore Hospital, 3459 Fifth Avenue, Pittsburgh, Pennsylvania 15213, USAE-mail: [email protected]

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 96
In an effort to better define risk factors and clinical outcomes of PH in a general medical intensive care unit patient population, we retrospectively reviewed admissions to a tertiary care medical intensive care unit to examine the hypotheses that PH is common in the modern medical intensive care unit population and that the presence of PH adversely impacts mortality. The information gained from this study will provide the background necessary to plan further prospective epidemiologic and therapeutic trials of PH in a critically ill medical population. The results of this investigation were presented in abstract form at the 2010 American Thoracic Society meeting.
MATERIALS AND METHODS
Study design and study populationA retrospective case–control study of patients admitted to one tertiary academic medical center over a 1-year period (July 2008 through June 2009) was conducted. All patients over the age of 18 years, admitted to the medical intensive care unit, and who had an echocardiogram performed within the first 4 days of intensive care unit admission, were eligible. This time period was chosen to optimize enrollment while limiting the number of patients who develop PH as a result of prolonged critical illness, such as those who progress to end stage heart, liver, or renal disease. These patients likely represent a different cohort from those who develop PH early in their intensive care unit stay. This study was approved by the University’s Institutional Review Board.
Data collectionBaseline demographics, intensive care unit admission diagnoses, and mortality were obtained from the electronic medical record. Echocardiograms were performed in the course of routine clinical care and were interpreted by academic cardiology attending physicians. Patients with echocardiogram quantification of tricuspid regurgitant (TR) jet velocity and ejection fraction had the following data extracted from the medical record: pre-existing comorbidities, laboratory data, use of mechanical ventilation, renal replacement therapy, systemic or pulmonary vasoactive medications, red blood cell transfusion, and right heart catheterization data (if available). Discharge diagnoses for the following disorders were also extracted via review of ICD-9 diagnostic codes: acute respiratory distress syndrome (518.5 and 518.82),[10] pulmonary embolus (415.1, 415.11, and 415.19), sepsis (995.91 and 995.92) and acute myocardial infarction (410.0–410.9).
DefinitionsDoppler-defined PH was defined as a TR jet velocity ≥3 m/sec by echocardiography, a value that was
selected based on accepted guidelines and population-based echocardiographic investigation.[11,12] A TR jet velocity <3 m/sec defined the control patients. Therefore, all the eligible patients of the study underwent echocardiography and our definitions of case and control can be considered as a comparison between patients with “high versus low” TR jet velocity. Comorbidities were classified as present if noted in an admission history or a consultation performed in the intensive care unit. Immunosuppression was defined as known infection with the human immunodeficiency virus or chronic use of any immunosuppressant medication, including prednisone ≥10 mg/day. Renal replacement therapy was defined as any intermittent or continuous renal replacement therapy. Pulmonary vasodilator use was defined via physician order for any pulmonary vasodilator medication while the patient was admitted to the intensive care unit.
Statistical analysisUnivariate analysis of baseline demographics and mortality between those who did and did not undergo echocardiography was performed via appropriate methods. Baseline characteristics and clinical outcomes were expressed as mean±standard deviation (continuous variables) or as percent (categorical variables). Univariate analysis of variables between groups with and without Doppler-defined PH were compared using Student’s t-tests or Wilcoxon rank sum tests, as appropriate, for continuous variables, and using chi-square tests for categorical variables. Multivariable logistic regression analysis using Doppler-defined PH as the dependent outcome was performed in an effort to identify the relevant variables. Time of survival was calculated from date of intensive care unit admission until death. Data were censored at the date of hospital discharge. Survival was assessed using the Kaplan–Meier method and the log-rank test in univariate analysis, and with the Cox proportional hazard method for multivariable analysis. For all regression analyses, variables found to have a P value ≤0.20 in univariate analysis were included in a backward elimination process to arrive at the final model. Age was forced into all survival models. Logistic regression model discrimination was assessed via the Hosmer and Lemeshow test. The proportional hazard assumption was assessed using Schoenfeld residuals. A two-sided P value of ≤0.05 was considered statistically significant. All statistical analyses were performed with Stata, version 10 (StataCorp LP, College Station, TX, USA).
RESULTS
Patient characteristicsExactly 1431 patients were admitted to our medical intensive care unit during the study period. The primary
Stamm, et al.: Doppler-defi ned PH in MICU patients

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 97
reasons for intensive care unit admission were sepsis (15%), respiratory failure (13%), pneumonia (7%), heart disease (6%), gastrointestinal disease (6%), renal failure (3%), malignancy-related (3%), neurologic disease (3%), complications of chronic liver disease (3%), complications of diabetes mellitus (2%), drug or alcohol related (<1%), or other miscellaneous disorders (38%). Of these patients, 449 (31%) had echocardiography performed within 4 days of admission to the intensive care unit and were significantly older (61±17 vs. 57±18 years, P<0.001), more likely females (52 vs. 43% P=0.002), and had a higher unadjusted mortality (28 vs. 19%, P=0.001) compared to those patients who did not undergo echocardiography. Of the 449 echocardiography studies, 299 (67%) reported both a TR jet velocity and left ventricular ejection fraction and composed the study sample [Figure 1]. Overall, 28% (126 of 449) of all medical intensive care unit patients who underwent echocardiography had Doppler-defined PH, while 42% (126 of 299) of the patients eligible for the study had Doppler-defined PH. Baseline characteristics and admission diagnoses of patients with and without Doppler-defined PH are similar [Table 1]. The distribution of TR jet velocities in the study cohort (mean 2.88±0.57 m/sec) is displayed in Figure 2. Only 17 of the 299 study eligible patients (6%) had a pre-existing diagnosis of PH. The prevalence of other comorbid conditions in the study population was as follows: systemic hypertension (55%), coronary artery disease (28%), chronic obstructive pulmonary disease (22%), congestive heart failure (19%),
Stamm, et al.: Doppler-defi ned PH in MICU patients
Table 1: Characteristics of patients with Doppler-defi ned pulmonary hypertension and controlsPulmonary hypertension Controls P value
Patients 126 173Age (years)a 63±17 61±18 0.52Gender (male) 43% 51% 0.17TR jet (m/sec)a 3.4±0.4 2.5±0.4 <0.0001Estimated sPAP (mmHg)a,b 57±11 36±7 <0.0001Admission diagnosis 0.47
Renal failure related 2% 3%Malignancy related 2% 2%Cirrhosis related <1% 5%Neurology related 2% 1%Diabetes mellitus related <1% 2%Drug overdose <1% <1%Gastrointestinal related 5% 4%Heart disease related 11% 9%Pneumonia 5% 5%Respiratory failure 23% 12%Sepsis 20% 26%Other 27% 30%
Hospital LOS (days)a 17±13 17±15 0.98MICU LOS (days)a 8±9 7±9 0.63Mortality 37% 25% 0.039
LOS - Length of stay; MICU - Medical intensive care unit; TR - Tricuspid regurgitant; sPAP - Systolic pulmonary artery pressure; aData presented as mean±standard deviation; bSystolic pulmonary artery pressure as estimated by echocardiography using a modifi ed Bernoulli equation [systolic pulmonary artery pressure ≈ 4 (tricuspid regurgitant jet velocity)2 + estimated right atrial pressure, where right atrial pressure is estimated using respiratory variation of the inferior vena cava]
immunosuppression (19%), chronic kidney disease (17%), and interstitial lung disease (5%).
Right heart catheterizationTwenty-one of 299 patients (7%) underwent right heart catheterization during the study admission (11 in Doppler-defined PH group and 10 in control group). The mean
Figure 1: Study fl ow diagram. Pulmonary hypertension defi ned as TR jet ≥3 m/sec (LVEF – Left ventricular ejection fraction; MICU –Medical intensive care unit; PH – Pulmonary hypertension; TR – tricuspid regurgitant)
All MICU admissions over one year period (N=1431)
Collect demographics, length of stay, mortality
Excluded if no echocardiogram within 4 days of MICU admission (N=982)
Excluded if either TR jet (N=150) and/or LVEF (N=13) not reported
Collect comorbidities, lab data, types of supportive care provided, diagnoses
Echocardiogram performed within 4 days of MICU admissions (N=449)
Qualifying echocardiogram with reported TR jet and LVEF (N=299)
Study patients with PH (N=126) or controls (N=173)

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 98
Multivariable regression analysis of Doppler-defined PH risk factorsThe following clinical characteristics were included in a regression analysis of Doppler-defined PH risk factors: age, gender, low ejection fraction, history of interstitial lung disease, lowest serum bicarbonate value, and diagnosis of pulmonary embolus. Partial pressure of arterial oxygen and brain natriuretic peptide values were excluded due to multiple missing values. Pulmonary vasodilator was considered a consequence rather than an indicator of PH and was not included in the regression model. When controlling for these clinical features, low ejection fraction, lowest serum bicarbonate, and diagnosis of pulmonary embolus remained independently associated with Doppler-defined PH [Table 2].
Risk factors for mortalityOf the examined variables, the following were significantly associated with in-hospital mortality in univariate analysis: age (P<0.001), chronic obstructive pulmonary disease (P=0.049) or interstitial lung disease (P=0.003), Doppler-defined PH (P=0.039), highest serum creatinine (P=0.004), lowest platelet count (P<0.001), diagnosis of sepsis (P=0.005), renal replacement therapy (P=0.002), mechanical ventilation (P<0.001), and use of either vasopressors (P<0.001) or pulmonary vasodilators (P=0.008) [Table 3].
Survival analysisKaplan–Meier survival analysis yielded significantly lower survival in those with Doppler-defined PH (log rank test P=0.05) [Figure 3]. The following clinical characteristics were included in a Cox proportional hazard analysis of variables associated with in-hospital mortality: age, gender, pre-existing history of chronic obstructive pulmonary disease or interstitial lung disease, Doppler-defined PH, low left ventricular ejection fraction, highest
Stamm, et al.: Doppler-defi ned PH in MICU patients
Figure 3: Kaplan–Meier survival curve of those with (PH) and without (control) Doppler-defi ned pulmonary hypertension. Log-rank test=0.05. Time of survival calculated as date of intensive care unit admission until death or hospital discharge (censoring)
Figure 2: Distribution of tricuspid regurgitant (TR) jet velocities in medical intensive care unit population. Mean TR jet velocity = 2.88±0.57 m/sec; median TR jet velocity=2.80 m/sec
duration between echocardiogram and catheterization was 10±10 days. The positive predictive value of a TR jet velocity ≥3 m/sec to diagnose PH, defined as a mean pulmonary artery pressure ≥25 mmHg, was 91% while the negative predictive value was 20% in this critically ill cohort. A moderate correlation existed between estimated and measured values of systolic pulmonary artery pressures (r=0.65, P=0.002).
Risk factors for Doppler-defined PHThe distribution of measured ejection fraction was markedly skewed; categorization of the ejection fraction variable around the 25th percentile (ejection fraction<50%) revealed that 29 patients (23%) in the PH group and 22 patients (13%) in the control group had a depressed left ventricular ejection fraction (P=0.019). Laboratory data associated with Doppler-defined PH included lowest recorded partial pressure of arterial oxygen (P=0.01), lowest recorded serum bicarbonate value (P=0.04), and a trend toward association with highest recorded brain natriuretic peptide (P=0.07). Multiple patients did not have blood gas (21% of study cohort) or brain natriuretic peptide (74% of study cohort) testing performed during their intensive care unit admission. Pulmonary vasodilator, used in a total of 12 patients (11 sildenafil and 1 bosentan), was significantly associated with the Doppler-defined PH (P<0.001). Of the reviewed diagnostic codes, only pulmonary embolus (Doppler-defined PH in 71% of those with a pulmonary embolus compared to 40% of those without a pulmonary embolus, P=0.005) was significantly associated with Doppler-defined PH. Those with ARDS displayed a trend toward reduced PH (Doppler-defined PH in 28% of those with compared to 43% of those without ARDS, P=0.14). Mechanical ventilation, vasopressor use, and renal replacement therapy were not associated with Doppler-defined PH [Table 2].

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 99
serum creatinine, lowest platelet count, diagnosis of sepsis, renal replacement therapy, mechanical ventilation and vasopressor use. When controlling for these clinical features, Doppler-defined PH remained significantly associated with mortality (HR=1.59, 95% CI=1.03–2.44, P=0.036) [Table 3].
DISCUSSION
This is the first report to indicate that Doppler-defined PH is common in a general medical intensive care unit population, with 126 of 449 patients (28%) undergoing echocardiography having evidence of PH, as defined by a TR jet velocity ≥3 m/sec. It is important to note that Doppler-defined PH in this investigation includes both pulmonary venous and pulmonary arterial hypertension, given the diagnostic reliance on echocardiography. The presence of Doppler-defined PH is associated with an increased risk of death, an effect that remains even after controlling for other clinical variables associated with mortality. Risk factors for the development of Doppler-defined PH in the medical intensive care unit include low left ventricular ejection fraction and a diagnosis of pulmonary embolism.
The definition of PH as a TR jet velocity ≥3 m/sec, which corresponds approximately to a systolic pulmonary artery pressure of ≥40 mmHg, is consistent with prior literature in other patient populations[13,14] and is in accordance with recent evidenced-based guidelines.[11] The distribution of TR jet velocities in a general intensive care unit population has not been previously reported. A TR jet velocity of 2.64 m/sec is reported to be 2 standard deviations above the mean in a normal population.[12] The mean TR jet velocity of 2.88 m/sec in our patient population is markedly higher than that seen in non-critically ill patients and suggests that PH is prevalent in the critically ill.
PH is a known complication of certain diseases commonly seen in the medical intensive care unit, such as ARDS and pulmonary embolism.[2-6,15] However, less is known of the burden of PH in a general medical critical care population. Our finding that at least 28% of patients undergoing echocardiography have an elevated TR jet velocity suggests that the burden of PH in a general medical intensive care unit population may be significant. Our retrospective study design inherently results in selection bias, however, and likely inflates the apparent burden of PH in the critically ill. Similarly, as not all
Table 2: Clinical variables and their association with pulmonary hypertensionUnivariate Multivariable regression
P value OR (95% CI) P value
Comorbid conditionsLow LVEFa 0.019 2.21 (1.19–4.12) 0.012COPD 0.31Interstitial lung disease 0.18Coronary artery disease 0.92Systemic hypertension 0.12Congestive heart failure 0.56Chronic kidney disease 0.74Immunosuppression 0.65
Laboratory abnormalitiesLowest pHb 0.58Lowest PaO2
b 0.01Lowest platelet countb 0.69Highest serum creatinineb 0.89Lowest bicarbonateb 0.04 6.92 (1.00–48.0) 0.050Highest BNPb 0.07
Therapeutic interventionsRenal replacement therapy 0.32Systemic vasopressor use 0.82Pulmonary vasodilator use <0.001Mechanical ventilation 0.92Blood transfusion 0.48
DiagnosesARDS 0.14Pulmonary embolus 0.005 4.28 (1.59–11.5) 0.004Sepsis 0.38Acute myocardial infarction 0.44
ARDS - Acute respiratory distress syndrome; BNP - Brain natriuretic peptide; CI - Confi dence interval; COPD - Chronic obstructive pulmonary disease; LVEF - left ventricular ejection fraction; OR - Odds ratio; PaO2 - Partial pressure of arterial oxygen; aLow LVEF defi ned as <50% by study qualifying echocardiogram; bLab values recorded during intensive care unit admission
Stamm, et al.: Doppler-defi ned PH in MICU patients

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 100
patients admitted to the intensive care unit underwent echocardiography, the actual prevalence could not be determined with this study.
Our findings that depressed left ventricular ejection fraction and a diagnosis of pulmonary embolism are risk factors for the development of PH are consistent with the reports in literature.[9,16] While in accordance with prior reports, only a minority of patients with PH in our study had either a pulmonary embolus (12%) or depressed ejection fraction (23%), suggesting that these disorders were not the predominant comorbidities in our cohort. Admittedly, given the reliance on non-invasively measured pulmonary vascular pressures, a reduced left ventricular ejection fraction does not necessarily relate to post-capillary PH and, conversely, those with normal left ventricular function can still have post-capillary PH.[17] The association between low arterial partial pressure of oxygen and PH has been previously reported[5,6] and may reflect hypoxia-mediated pulmonary vasoconstriction. Multiple patients in our cohort did not undergo arterial blood gas
Table 3: Clinical variables and their association with mortalityUnivariate Multivariable Cox regression
P value HR (95% CI) P value
Age (years) <0.001 1.03 (1.01–1.05) <0.001Gender (male) 0.11Pulmonary hypertensiona 0.039 1.59 (1.03–2.44) 0.036Comorbid conditions
Low LVEFb 0.059 1.62 (0.97–2.72) 0.067COPD 0.049Interstitial lung disease 0.003Coronary artery disease 0.45Systemic hypertension 0.93Congestive heart failure 0.96Chronic kidney disease 0.99Immunosuppression 0.86
Laboratory abnormalitiesLowest pHc 0.021Lowest PaO2
c 0.87Lowest platelet countc <0.001 0.38 (0.22–0.65) <0.001Highest serum creatininec 0.004Lowest bicarbonatec 0.35Highest BNPc 0.42
Therapeutic interventionsRenal replacement therapy 0.002Systemic vasopressor use <0.001 1.96 (1.11–3.43) 0.019Pulmonary vasodilator use 0.008Mechanical ventilation <0.001 2.65 (1.13–6.22) 0.026Blood transfusion 0.24
DiagnosesARDS 0.50Pulmonary embolus 0.33Sepsis 0.005Acute myocardial infarction 0.22
ARDS - Acute respiratory distress syndrome; BNP - Brain natriuretic peptide; CI - Confi dence interval; COPD - Chronic obstructive pulmonary disease; LVEF - Left ventricular ejection fraction; OR - Odds ratio; PaO2 - Partial pressure of arterial oxygen; aDefi ned as a tricuspid regurgitant jet velocity ≥3 m/sec in study qualifying echocardiogram; bLow LVEF defi ned as <50% by study qualifying echocardiogram; cLab values recorded during intensive care unit admission
measurement, limiting further interpretation. Our finding that low serum bicarbonate is an independent risk factor for PH is also consistent with prior literature. Teplinsky and coworkers reported that metabolic acidemia leads to increased pulmonary arterial pressures and depressed left ventricular stroke volume in a canine model.[18] Although acidemia may result in increased pulmonary arterial pressure, our finding of a lack of an association between blood pH and Doppler-defined PH in those patients who underwent arterial blood gas analysis suggests that the result obtained could also be due to chance.
The diagnosis of ARDS was not associated with Doppler-defined PH in our study. Although PH is commonly reported in the ARDS literature, the heterogeneous definitions of acute lung injury used in these studies and the selective use of diagnostic right heart catheterization make extrapolations between studies difficult and determination of true prevalence impossible.[3-5,19] Our use of ICD-9 diagnostic codes to define ARDS is similar to that used in other studies but resulted in few patients being
Stamm, et al.: Doppler-defi ned PH in MICU patients

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 101
diagnosed with ARDS.[10] Thus, our study may have lacked sensitivity in detecting ARDS and be underpowered.
We found a significant association between Doppler-defined PH and increased mortality. Moreover, Doppler-defined PH remained an independent predictor of death when controlling for other clinical variables associated with mortality. While not previously reported in a general medical critical care population, PH is independently associated with mortality in multiple other disorders, including pulmonary embolism,[9,15] congestive heart failure,[20] and chronic obstructive pulmonary disease.[21] The ARDS literature suggests a correlation between the presence of PH and worse outcomes,[3,5,22] although this finding has not been seen in all studies.[4] Bull and colleagues recently reported in a secondary analysis of a modern cohort of patients with acute lung injury, who underwent right heart catheterization, that an elevated transpulmonary gradient or pulmonary vascular resistance (both hemodynamic measures of pulmonary vascular dysfunction) predicted increased morbidity and mortality, while independent hemodynamic measurements, such as mean pulmonary artery or pulmonary artery occlusion pressure, were not associated with worse outcomes.[19] While intriguing, only a randomized study will be able to address the unresolved issue of whether PH is casually related to mortality or is simply a marker of disease severity.
The results of right heart catheterization in a subset of patients demonstrated that the presence of PH by echocardiography is a reliable predictor of true elevated mean pulmonary arterial pressures in the critically ill, with a positive predictive value of over 90%. However, the absence of an elevated TR jet velocity does not rule out PH, based on the lower negative predictive value found in our study. While the total number of right heart catheterization studies is low and should be interpreted with caution, echocardiography estimated systolic pulmonary artery pressures showed good correlation with invasive measurements.
The results of our investigation demonstrate robust external validity. Features that were found to be associated with Doppler-defined PH, including hypoxemia, reduced ejection fraction, and pulmonary embolus, are known risk factors for PH.[5,9,16,20] Clinical markers of increased mortality in the critically ill, including advanced age, requirement for mechanical ventilation, systemic vasopressor support, and renal replacement therapy, were found to predict mortality in our study cohort.[23,24]
Despite the strengths of our analysis and the validity of our data, the study has several limitations worth
consideration. The single center retrospective design, and in particular, the inability to control which patients received an echocardiogram, introduces significant selection bias. Clearly, the patients in this study who underwent echocardiography were older and had higher mortality than those patients who did not; thus, our results cannot be extrapolated to all medical intensive care unit patients. Although echocardiography is a diagnostic tool available to most intensivists, the reliance on routine clinical echocardiography in this study prohibits further characterization of the contribution of left and right heart disease to the diagnosis of PH, information that may be obtained from invasive hemodynamic measurements and/or specialized echocardiographic techniques. Finally, the reliance on the electronic medical record for clinical information, with the attendant issues of missing data, accuracy, and use of ICD-9 codes, is a documented source of potential study error.[25,26]
In conclusion, in this initial hypothesis-generating investigation, we have shown that Doppler-defined PH in a general medical intensive care unit population is common and associated with an increased risk of mortality. Future prospective studies should attempt to more clearly define the prevalence of and risk factors for PH in a medical intensive care unit population. In addition, the balance of pulmonary venous versus pulmonary arterial hypertension, with clinical associations of each, needs to be defined. Given the lack of current knowledge regarding the balance and outcomes associated with pulmonary arterial versus pulmonary venous hypertension, empiric therapy of Doppler-detected PH in the critically ill with targeted pulmonary vascular medications cannot be recommended at this time. If pulmonary arterial hypertension independently predicts worsened outcomes in the critically ill, therapeutic trials of hemodynamic goal-directed therapy, using pulmonary vascular targeted medication and aimed at reducing pulmonary artery pressures and improving right ventricular function, may be indicated.
ACKNOWLEDGMENT
The authors would like to thank Thomas Richards, PhD, for his thoughtful review of the study’s statistical plan and results.
REFERENCES
1. Zamanian RT, Haddad F, Doyle RL, Weinacker AB. Management strategies for patients with pulmonary hypertension in the intensive care unit. Crit Care Med 2007;35:2037-50.
2. Zapol WM, Snider MT. Pulmonary hypertension in severe acute respiratory failure. N Engl J Med 1977;296:476-80.
3. Sloane PJ, Gee MH, Gott lieb JE, Albertine KH, Peters SP, Burns JR, et al. A multicenter registry of patients with acute respiratory distress syndrome.
Stamm, et al.: Doppler-defi ned PH in MICU patients

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 102
Physiology and outcome. Am Rev Respir Dis 1992;146:419-26.4. Suchyta MR, Clemmer TP, Elliott CG, Orme JF Jr, Weaver LK. The adult
respiratory distress syndrome. A report of survival and modifying factors. Chest 1992;101:1074-9.
5. Squara P, Dhainaut JF, Artigas A, Carlet J. Hemodynamic profi le in severe ARDS: Results of the European Collaborative ARDS Study. Intensive Care Med 1998;24:1018-28.
6. Vieillard-Baron A, Schmitt JM, Augarde R, Fellahi JL, Prin S, Page B, et al. Acute cor pulmonale in acute respiratory distress syndrome submitt ed to protective ventilation: Incidence, clinical implications, and prognosis. Crit Care Med 2001;29:1551-5.
7. Wynne R, Bott i M. Postoperative pulmonary dysfunction in adults aft er cardiac surgery with cardiopulmonary bypass: Clinical signifi cance and implications for practice. Am J Crit Care 2004;13:384-93.
8. Subramaniam K, Yared JP. Management of pulmonary hypertension in the operating room. Semin Cardiothorac Vasc Anesth 2007;11:119-36.
9. Kucher N, Rossi E, De Rosa M, Goldhaber SZ. Prognostic role of echocardiography among patients with acute pulmonary embolism and a systolic arterial pressure of 90 mm Hg or higher. Arch Intern Med 2005;165:1777-81.
10. Reynolds HN, McCunn M, Borg U, Habashi N, Cott ingham C, Bar-Lavi Y. Acute respiratory distress syndrome: Estimated incidence and mortality rate in a 5 million-person population base. Crit Care 1998;2:29-34.
11. Badesch DB, Champion HC, Sanchez MA, Hoeper MM, Loyd JE, Manes A, et al. Diagnosis and assessment of pulmonary arterial hypertension. J Am Coll Cardiol 2009;54:S55-66.
12. McQuillan BM, Picard MH, Leavitt M, Weyman AE. Clinical correlates and reference intervals for pulmonary artery systolic pressure among echocardiographically normal subjects. Circulation 2001;104:2797-802.
13. Arcasoy SM, Christie JD, Ferrari VA, Sutt on MS, Zisman DA, Blumenthal NP, et al. Echocardiographic assessment of pulmonary hypertension in patients with advanced lung disease. Am J Respir Crit Care Med 2003;167:735-40.
14. Allanore Y, Borderie D, Meune C, Cabanes L, Weber S, Ekindjian OG, et al. N-terminal pro-brain natriuretic peptide as a diagnostic marker of early pulmonary artery hypertension in patients with systemic sclerosis and eff ects of calcium-channel blockers. Arthritis Rheum 2003;48:3503-8.
15. Vieillard-Baron A, Page B, Augarde R, Prin S, Qanadli S, Beauchet A, et al. Acute cor pulmonale in massive pulmonary embolism: Incidence, echocardiographic pattern, clinical implications and recovery rate. Intensive Care Med 2001;27:1481-6.
16. Konstantinides S, Geibel A, Heusel G, Heinrich F, Kasper W. Heparin
plus alteplase compared with heparin alone in patients with submassive pulmonary embolism. N Engl J Med 2002;347:1143-50.
17. Hoeper MM, Barberà JA, Channick RN, Hassoun PM, Lang IM, Manes A, et al. Diagnosis, assessment, and treatment of non-pulmonary arterial hypertension pulmonary hypertension. J Am Coll Cardiol 2009;54:S85-96.
18. Teplinsky K, O’Toole M, Olman M, Walley KR, Wood LD. Eff ect of lactic acidosis on canine hemodynamics and left ventricular function. Am J Physiol 1990;258:H1193-9.
19. Bull TM, Clark B, McFann K, Moss M; National Institutes of Health/National Heart, Lung, and Blood Institute ARDS Network. Pulmonary vascular dysfunction is associated with poor outcomes in patients with acute lung injury. Am J Respir Crit Care Med 2010;182:1123-8.
20. Grigioni F, Potena L, Galiè N, Fallani F, Bigliardi M, Coccolo F, et al. Prognostic implications of serial assessments of pulmonary hypertension in severe chronic heart failure. J Heart Lung Transplant 2006;25:1241-6.
21. Oswald-Mammosser M, Weitzenblum E, Quoix E, Moser G, Chaouat A, Charpentier C, et al. Prognostic factors in COPD patients receiving long-term oxygen therapy. Importance of pulmonary artery pressure. Chest 1995;107:1193-8.
22. Villar J, Blazquez MA, Lubillo S, Quintana J, Manzano JL. Pulmonary hypertension in acute respiratory failure. Crit Care Med 1989;17:523-6.
23. Ware LB. Prognostic determinants of acute respiratory distress syndrome in adults: Impact on clinical trial design. Crit Care Med 2005;33:S217-22.
24. Vincent JL, Ferreira F, Moreno R. Scoring systems for assessing organ dysfunction and survival. Crit Care Clin 2000;16:353-66.
25. Ward NS. The accuracy of clinical information systems. J Crit Care 2004;19:221-5.
26. Howard AE, Courtney-Shapiro C, Kelso LA, Goltz M, Morris PE. Comparison of 3 methods of detecting acute respiratory distress syndrome: Clinical screening, chart review, and diagnostic coding. Am J Crit Care 2004;13:59-64.
Source of Support: None declared. Confl ict of Interest: Dr. Mathier reports receiving consulting fees (all less than US$10,000) from Actelion,
Gilead, and United Therapeutics. Dr. Gladwin further reports receiving grant support from the Institute of Transfusion Medicine and the Hemophilia Center of Western Pennsylvania, and federal funding by the NHLBI, NIDDK
and NIAMS of the National Institutes of Health (HL098032, HL096973, DK085852, AR058910). None of Dr. Gladwin’s grant resources were used in
this project and there is no funding source for this study.
Stamm, et al.: Doppler-defi ned PH in MICU patients
Author Help: Online submission of the manuscripts
Articles can be submitted online from http://www.journalonweb.com. For online submission, the articles should be prepared in two files (first page file and article file). Images should be submitted separately.
1) First Page File: Prepare the title page, covering letter, acknowledgement etc. using a word processor program. All information related to your identity should
be included here. Use text/rtf/doc/pdf files. Do not zip the files.2) Article File: The main text of the article, beginning with the Abstract to References (including tables) should be in this file. Do not include any informa-
tion (such as acknowledgement, your names in page headers etc.) in this file. Use text/rtf/doc/pdf files. Do not zip the files. Limit the file size to 1 MB. Do not incorporate images in the file. If file size is large, graphs can be submitted separately as images, without their being incorporated in the article file. This will reduce the size of the file.
3) Images: Submit good quality color images. Each image should be less than 2048 kb (2 MB) in size. The size of the image can be reduced by decreas-
ing the actual height and width of the images (keep up to about 6 inches and up to about 1800 x 1200 pixels). JPEG is the most suitable file format. The image quality should be good enough to judge the scientific value of the image. For the purpose of printing, always retain a good quality, high resolution image. This high resolution image should be sent to the editorial office at the time of sending a revised article.
4) Legends: Legends for the figures/images should be included at the end of the article file.

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 103
Expression of mutant BMPR-II in pulmonary endothelial cells promotes apoptosis and a
release of factors that stimulate proliferation of pulmonary arterial smooth muscle cells
Xudong Yang1, Lu Long1, Paul N. Reynolds1, Nicholas W. Morrell1
1Department of Medicine, University of Cambridge School of Clinical Medicine, Addenbrooke’s and Papworth Hospitals, Cambridge, United Kingdom
ABSTRACT
Mutations in the bone morphogenetic protein type II receptor gene (BMPR-II) are the major cause of heritable pulmonary arterial hypertension (PAH). Although both endothelial and smooth muscle cell BMPR-II dysfunction have been seen to contribute to pulmonary hypertension in vivo, little is known about the impact of BMPR-II mutation on the interaction between these two important cell types. We employed adenoviral vectors to overexpress wild type or mutant (kinase-defi cient mutation, D485G) BMPR-II in human pulmonary arterial endothelial cells (PAECs). PAECs transfected with mutant BMPR-II demonstrated increased susceptibility to apoptosis. Conditioned media from PAECs transfected with mutant BMPR-II increased the proliferation of pulmonary arterial smooth muscle cells (PASMCs), when compared with conditioned media from PAECs transfected with wild-type BMPR-II. PAECs transfected with mutant BMPR-II released higher levels of TGF-β1 and FGF2 into the conditioned media than the wild-type BMPR-II-transfected cells. Conditioned media from PAECs expressing mutant BMPR-II also showed increased activation of luciferase activity in a TGF-β bioassay. The increased proliferation observed in PASMCs exposed to conditioned media from PAECs expressing mutant BMPR-II was inhibited by neutralizing the antibodies to TGF-β1, or small molecule inhibitors of ALK-5 (SD208) or FGFR1 (SU5402). We conclude that mutation in BMPR-II increases susceptibility to apoptosis of PAECs and leads to secretion of growth factors that stimulate the proliferation of PASMCs. These processes may contribute to the remodeling of pulmonary arteries observed in patients with familial or heritable PAH.
Key Words: Fibroblast growth factor, pulmonary vasculature, transforming growth factor beta
Access this article online
Quick Response Code:Website: www.pulmonarycirculation.org
DOI: 10.4103/2045-8932.78100
Pulm Circ 2011;1:103-10
Address correspondence to:Prof. Nicholas W. Morrell,Department of Medicine,University of Cambridge School of Clinical Medicine,Addenbrooke’s Hospital, Box 157,Hills Road, Cambridge CB2 0QQ, United Kingdom.E-mail: [email protected]
INTRODUCTION
Pulmonary arterial hypertension (PAH) is a progressive disease characterized by a marked increase in pulmonary arterial pressure and right ventricular hypertrophy. Without treatment, progression of pulmonary hypertension leads to right ventricular failure and death in ~three years from diagnosis.[1] Mutations in the gene, encoding the bone morphogenetic protein type II receptor (BMPR-II),[2,3] have been found in ~70% of families with heritable or familial PAH;[4]and up to 25% of the patients with apparently sporadic or idiopathic PAH (IPAH) harbor mutation.[5]
BMPR-II is highly expressed on the vascular endothelium of the pulmonary arteries and at a low level in PASMCs and fibroblasts in the lung.[6]
Endothelial cells (ECs) are recognized as major regulators of vascular function, balancing the production of vasoconstrictors versus vasodilators, activators versus inhibitors of smooth muscle cell (SMC) growth and migration, prothrombotic versus antithrombotic mediators, and proinflammatory versus anti-inflammatory signals.[7,8]
Research Ar t ic le

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 104
Recent studies have shown that apoptosis of ECs induces the release of mediators that cause vascular SMC proliferation.[9] Endothelial dysfunction in PAH may allow excessive release of paracrine factors that act either as growth factors to induce PASMC proliferation or as chemokines to recruit circulating inflammatory cells.[10-12] Exposure of pulmonary arterial SMCs (PASMCs) to the culture medium from pulmonary arterial ECs (PAECs) induces PASMC proliferation, and this effect is exaggerated when PAECs from patients with PAH are used.[10] However, the role of endothelial dysfunction caused by the mutation of BMPR-II on PASMC hyperplasia remains unclear.
In the present study, we examined the impact of introducing a kinase-inactive, disease-relevant BMPR-II mutant into the PAECs and demonstrated that this promotes apoptosis of the PAECs. This was associated with an increased release of TGF-β1 and FGF2 from the PAECs transfected with mutant BMPR-II. Furthermore, the conditioned media from mutant BMPR-II-transfected PAECs stimulated a heightened proliferation of PASMCs, an effect that could be inhibited with a neutralizing antibody to TGF-β1 or an ALK-5 inhibitor, or a small molecule inhibitor of the fibroblast growth factor receptor-1 (FGFR1). These findings demonstrated that the mutation in BMPR-II promoted the apoptosis of PAECs and stimulated the release of growth factors, with pro-proliferative effects on PASMCs. These findings provided a mechanism by which the BMPR-II mutation drove the cellular processes that contributed to pulmonary vascular remodeling in patients with heritable PAH.
MATERIALS AND METHODS
Cell culture and experimental designHuman pulmonary artery endothelial cells (PAECs; n=3) and an EGM-2 Bullet Kit were purchased from Lonza (UK). PAECs were grown in 5% fetal bovine serum (FBS) / EGM-2 and used between passage 5~6.[13] The cells were plated at 2.5105 cells in 60-mm culture dishes or 0.5104 cells in eight-well chamber slides, for adenoviral transfection. The control and mutant human pulmonary artery smooth muscle cells (PASMCs, n=3 in each group) were explant-derived from the peripheral pulmonary arteries (<2 mm external diameter), as previously described (14). The Papworth Hospital (UK) Ethical Review Committee approved the study, and the subjects or their relatives gave an informed written consent. The cells were maintained in 10% FBS / Dulbecco’s modified Eagle Medium (DMEM) and used between passages 4~6. The smooth muscle phenotype of isolated cells was confirmed, as previously described.[14]
Adenoviral transfectionThe generation and transfection of the adenoviral constructs was described as previously expressed.[13] In brief, the PAECs were plated in 60-mm dishes or eight-well chamber slides in cultured medium, overnight. After washing in serum-free EGM-2 twice, the cells were transfected with overexpress wild-type (Wt) or mutant (kinase-deficient mutation, D485G) of BMPR-II constructs for 48 hours at 50 pfu / cell, in serum-free EGM-2.
Apoptosis assayApoptosis was assessed by a morphological assay after H-33342 and propidium iodide (PI) staining, as previously described.[14] Flow cytometric analysis was also used to determine apoptotic cells, using an FITC Annexin V staining kit (BD Biosciences, UK) according to the manufacturer’s protocol. Briefly, after 48 hours of adenoviral infection, PAECs were washed thrice with serum-free EGM-2 (SFE2). The cells were maintained in serum-free EGM-2, after the last wash, for 24 hours. A serum-free EGM-2 without growth factors (SF) was used as the positive control for apoptosis. The cells were harvested by brief trysinization and washed twice with cold PBS. Five microliters of Annexin V-fluorescein isothiocyanate (FITC) and PI were added to every 100 μl of cell suspension, for 15 minutes, at room temperature, in the dark, and then 400 μl of 1x binding buffer were added to each sample before analysis. FACS analysis was carried out using a Becton Dickinson FACS Scan analyzer (BD Biosciences, UK).
Conditioned mediumAfter a 24-hour incubation in serum-free EGM-2, the medium in 60-mm dishes was collected from the PAECs transfected with adenoviral BMPR-II constructs (Wt and D485G), and designated as CMWt and CMMut, respectively. The medium from nontransfected PAECs incubating in serum-free EGM-2 alone for 24 hours was used as the control (CMControl). Conditioned media were centrifuged at 15,000 g for 5 minutes at 4°C. The supernatants were then aliquoted and stored at -80°C and thawed for use in subsequent experiments.
Proliferation of PASMCs in response to conditioned mediumPulmonary arterial smooth muscle cell proliferation was quantified by cell number counting and by 3H-thymidine incorporation assay, as previously described.[14] In brief, PASMCs were plated at 1.5104 cells / well in 24-well plates, overnight. The following day, the cultured medium (CM) was replaced with 0.5% FBS in CM, with or without pretreatment, with a neutralizing antibody to TGF-β1 (NA-TGF, 10 μg/ml; R and D Systems, UK). Further experiments involved incubation with the ALK-5 receptor
Yang, et al.: BMPR-II mutation and endothelial apoptosis

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 105
inhibitor, SD208, (0.5 μM; TOCRIS, UK), or SU5402 (10 μM; Calbiochem, UK), a small molecule inhibitor of FGFR1. The 3H-thymidine was added for the last six hours. The cell counts were carried out on day 2 or 3, and day 5. The conditioned medium was replenished on day 3. Each experiment was repeated at least thrice.
Enzyme-linked immunosorbent assay (ELISA)Sandwich ELISA kits (R and Sytems, UK) were used to measure the amount of TGF-β1 or FGF2 in the conditioned medium following the manufacturer’s protocol. The samples were read using a spectrophotometer at an absorbance of 405 nm.
Luciferase activity assayMink lung epithelial cells (MLECs-clone 320) were used to quantify the active TGF-β1 in a conditioned medium.[15] The MLECs (provided by Dr. D.B. Rifkin, Department of Cell Biology, New York University Medical Center) were stably transfected with human plasminogen activator inhibitor-1 promoter-luciferase construct (PAI-L). Mature TGF-β got bound to the receptors of the MLECs resulting in a dose-dependent increase in luciferase activity. Briefly, the cells were seeded at 1.5104 / well in 96-well plates, in 10% FBS/DMEM with geneticin (0.25mg/ml), for three hours. Next the medium was replaced by 100 μl of the control or conditioned medium for 20 hours. The cells were lysed in 100 μl / well of lysis buffer. The luciferase activity was assayed according to the manufacture’s instruction (Roche, UK).
StatisticsData were expressed as mean±SEM and analyzed with GraphPad Prism version 5.01 (GraphPad Software). Comparisons were made by Students t-test or ANOVA, as appropriate, and a value of P<0.05 indicated the statistical significance.
RESULTS
Overexpression of mutant BMPR-II causes apoptosis of PAECsWe used two methods (nuclear morphology and flow cytometry) to investigate the effects of overexpressing mutant BMPR-II (D485G) on apoptosis of PAECs. First we compared the PAEC number in non-transfected cells and in PAECs transfected with wild-type (Wt) or D485G BMPR-II (Mut) for 48 hours. There was a trend toward reduced cell number in cells transfected with Mut [Figure 1a and b]. The nuclear morphology and quantification demonstrated that after incubation in serum-free EGM-2 (SFE2) for 24 hours, the PAECs transfected with mutant BMPR-II exhibited a higher nuclear condensed cell number (27.9±5.7%) compared
with Wt (7.4±1.9%) and control cells (4.8±2.1%) [Figure 1c and d]. The increased apoptosis was further demonstrated by flow cytometric analysis. The percentage of apoptotic cells (early and late-stage apoptosis) was increased following the incubation of cells in SFE2 without growth factors (SF) [Figure 2a and b]. The transfection of cells with the Wt construct did not change the percentage of apoptotic cells compared with SFE2 (12.6±3.2%) [Figure 2c]. In contrast, transfection of PAECs with the D485G construct increased the percentage of apoptotic PAECs significantly (25.7±7.1%) [Figure 2d]. The differences are shown graphically in [Figure 2e].
Conditioned media from PAECs transfected with mutant BMPR-II stimulate proliferation of PASMCs We employed 3H-thymidine uptake and cell counting to examine the growth rates of PASMCs (n=3) exposed to a conditioned medium. PASMCs incubated with a conditioned medium from PAECs transfected with Wt BMPR-II (CMWt) showed similar 3H-thymidine incorporation and growth rates compared to PASMCs exposed to conditioned media from non-transfected PAECs (CM control) [Figure 3a and b]. In contrast PASMCs exposed to conditioned media from PAECs transfected with mutant BMPR-II (CMMut) exhibited increased 3H-thymidine incorporation and increased rates of proliferation [Figure 3a and b].
PAECs expressing mutant BMPR-II release higher levels of TGF-1 and FGF2Increased endothelial release of FGF2 was reported in PAECs from idiopathic PAH patients [12] and increased release of TGF-β1 was observed in endothelial cells undergoing apoptosis.[9] Both of these growth factors were known to play important roles in pulmonary vascular remodeling. We questioned whether conditioned media from PAECs transfected with mutant BMPR-II contained increased levels of these mediators. Employing ELISAs to detect the amount of TGF-β1 and FGF2 in the three sets of conditioned media, we observed higher levels of TGF-β1 and FGF2 in the media conditioned by PAECs transfectd with mutant BMPR-II, compared to WT transfected cells and non-transfected cells [Figure 4a and b]. In addition, we measured the TGF-β1 activity of the conditioned media using the MLEC bioassay. This assay further confirmed the finding of increased TGF-β1 activity in the media conditioned by PAECs transfected with mutant BMPR-II [Figure 4c].
Pro-proliferative effects of mutant PAEC conditioned media are inhibited by inhibitors of ALK-5 and FGFR1In order to confirm the functional significance of the observed increased levels of TGF-β1 and FGF2 in
Yang, et al.: BMPR-II mutation and endothelial apoptosis

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 106
Figure 1: Pulmonary artery endothelial cell morphology and number, 48 hours following adenoviral transfection with wild type (Wt) or D485G (Mut) BMPR-II constructs, or non-transfected (Control) conditions (a and b). Following H-33342 staining for nuclear morphology (c) (red arrows indicates apoptotic cells) quantifi cation demonstrated that after incubation in serum-free EGM-2 for 24 hours, the PAECs transfected with mutant BMPR II exhibited a higher nuclear condensed cell number (27.9±5.7%) compared to wild-type cells (7.4±1.9%) and NS (4.8±2.1%) (d)
Yang, et al.: BMPR-II mutation and endothelial apoptosis
a
Control MutWt
80
100p=0.062
p=0.349
ell)
b
Control
Control
Wt Mut
Mut
0
20
40
60
Cel
l num
ber
(x10
3 /w
e
c
Wt
d�� P= 0.0013
Control Wt Mut
30
25
20
15
10
5
0
% o
f tot
alap
opto
tic c
ells
conditioned media from PAECs transfected with mutant BMPR-II, we performed further experiments employing
inhibitors of TGF-β and FGF2 signaling. Thus pretreatment of control PASMCs with an anti-TGF-β1 neutralizing

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 107
SF0.9%
7.2%SFE20.8%
2.9%a b
70.4%
21.5%
88.5%
7.8%
Prop
idiu
m Io
dide
c
Control
Wt1%
Mut2.5%
90.1%
2.7%
66.1%
12.7%d
6.2% 17.7%
Annexin V
�� P<0.05 ( n=4)e
20
25
30
35
�
�
Control Control Wt Mut0
5
10
15
% o
f tot
al a
popt
otic
cel
ls
SF SFE 2
antibody resulted in the inhibition of PASMC proliferation to PAEC mutant conditioned media [Figure 5a]. Similar effects were observed with an inhibitor of the TGF-β type 1 receptor (ALK-5), SD208 [Figure 5b]. A small molecule inhibitor of the FGFR1 receptor, SU5402, also markedly inhibited the pro-proliferative effect of conditioned media from PAECs transfected with mutant BMPR-II [Figure 5b]. The results of experiments using 3H-thymidine incorporation were mirrored by experiments employing
cell counting [Figure 6a]. In the latter studies we also determined the effect of conditioned media on PASMCs isolated from PAH patients known to harbor mutations in BMPR-II (N903S; W9X; R899X). Although there was a trend to higher rates of proliferation in mutant PASMCs (~25%) compared with PASMCs from the control subjects, this was not statistically significant (P=0.062) [Figure 6a and b]. Conditioned media from PAECs transfected with mutant BMPR-II had a similar effect to
Figure 2: Apoptosis was further measured by fl ow cytometric analysis. (a, b, c, and d) Represents scatter plots of propidium iodide (PI) (y-axis) versus Annexin V-FITC (x-axis). Lower left quadrants (absence of both markers) indicate viable cells; upper left quadrants (PI positive) indicate cellular necrosis. The total apoptotic cells (early and late-stage apoptosis) are represented by the right side of the panel (Annexin V staining alone or together with PI) in which the total cell death number from the Mut is signifi cantly higher (25.7±7.1%) than the Wt (12.6±3.2%) (e)
Yang, et al.: BMPR-II mutation and endothelial apoptosis

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 108
25�
P= 0.011a
10
15
20
(1x1
000c
pm/w
ell)
CMControl CMWt CMMut0
53 H-th
ymid
ine
upta
ke
b�� P= 0.0012
�P=0.012
40
50
CMWt
CMMut��
0 /
wel
l)3 P 0.012
10
20
30CMControl
�
Cel
l num
ber (
x1
0 1 2 3 4 50 Days
bP= 0.01825 �
a P= 0.014880 �
10
15
20
FGF2
(pg/
ml)
�
40
60
80 �
CMControl CMW CMMut0
5
10
Leve
l of
0
20
CMControl CMWt CMMut
c
P= 0.001117500
20000
ase
activ
ityR
elat
ive
luci
fera
nits
)(a
rbitr
ary
un
CMMut0
2500
5000�
TGF- 1 CMControl CMWT
TGF-
1(pg
/ml)
Leve
l of
T
that observed in control PASMCs, as did the inhibitors of ALK-5 and FGFR1
DISCUSSION
In this study we provide evidence that overexpression of mutant BMPR-II confers increased susceptibility to apoptosis in PAECs. These data support the observation that siRNA knockdown of BMPR-II also promotes endothelial apoptosis.[16] Endothelial apoptosis is considered to be a key trigger to disease initiation in the pathobiology of pulmonary hypertension.[7] The subsequent ingress of serum factors into the vessel wall leads to the activation of growth factors and of endogenous vascular elastases.[17] Here we report that an additional factor contributing to vascular remodeling may be the release of pro-proliferative growth factors from PAECs undergoing apoptosis.
Apoptotic cells are known to secrete TGF-β and this has also been shown for PAECs.[9] A previous report has also found that the released TGF-β from PAECs could
stimulate proliferation of PASMCs.[9] In the present study we provide a link between BMPR-II mutation, endothelial apoptosis, and the secretion of growth factors from PAECS that can contribute to the proliferation of the underlying mesenchymal cells. In our study, overexpression of mutant BMPR-II in PAECs led to the release of both TGF-β1 and FGF2 and increased PAEC apoptosis. Increased endothelial apoptosis has also been noted in the lungs of heterozygous BMPR-II null mice exposed to inflammatory stimuli.[18]
Serum-free media conditioned by PAECs transfected with mutant BMPR-II and subjected to co-culture with control PASMCs, caused an abnormal proliferation of PASMCs. This pro-proliferative effect could be inhibited by a neutralizing antibody to TGF-β1 or an ALK-5 inhibitor (SD208), or a small molecule inhibitor (SU5402) of fibroblast growth factor receptor-1 (FGFR1). These findings provide a mechanism by which the BMPR-II mutation drives the cellular processes that contribute to pulmonary vascular remodeling in patients with heritable PAH.
Recent studies have demonstrated that BMP signaling represents an inhibitory pathway, which prevents excessive pulmonary arterial muscularization by
Figure 3: 3H-thymidine uptake (a) and cell number (b) of PASMCs (n=3) in conditioned medium (CM) from PAECs. The PASMCs seeded in 0.5% FBS / CMMut for 24 hours show a signifi cant increase in the DNA synthesis compared to the CM from control cells or CM from Wt transfected cells (a). Cell numbers were also increased after two days of incubation in 0.5% FBS/CMMut, a difference that was maintained at day 5 (b)
Figure 4: The level of TGF-β1 or FGF2 in the three types of conditioned medium were measured by ELISA. Both growth factors were higher in the conditioned media (CM) from the Mut cells compared to the CM from the control, or Wt transfected cells (a,b). Luciferase assays in the mink lung epithelial cells, stably expressing the human PAI-1 promoter, confi rmed that CM from mutant transfected PAECs (CM Mut) contained more active TGF-β than CM from untransfected (control) cells or CM from PAECs transfected with WT BMPR-II (CM WT) (c). TGF-β1 was used as a positive control in this assay
Yang, et al.: BMPR-II mutation and endothelial apoptosis

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 109
reducing PASMC growth and increasing apoptosis.[14,19-21] In contrast, BMPs in general promote proliferation and are anti-apoptotic in endothelial cells.[13,16,22] Knockdown of BMPR-II with siRNA increases the susceptibility of PAECs to apoptosis.[16] The contrasting effects of BMPs in pulmonary vascular ECs and the underlying PASMCs provide a hypothesis for pulmonary vascular damage and remodeling in heritable PAH. A critical reduction in BMPR-II function in the endothelium may promote increased endothelial apoptosis, which compromises the integrity of the endothelial barrier and contributes to endothelial dysfunction. This view is almost certainly an oversimplification. In particular, BMP9 was recently identified as a ligand for a receptor complex, comprising of ALK-1 and BMPR-II.[23] In contrast to other BMPs, BMP9 appears to inhibit the proliferation of PAECs.[24] Therefore, the importance of diverse BMP ligands to the endothelial response in vivo remains to be elucidated.
bControl PASMCs(n=3)250 Control Mutant PASMCs(n=3)
150
200�
�
upta
ke(%
of C
MN
S)
P< 0.05
CMControl CMWt +SU5402 +SD2080
50
100
� ��
�
3 H-th
ymid
ine
u
CMMut
P= 0.0015
4
5
e
��
a
1
2
3
3H
-thym
idin
e up
tak
(1x1
000c
pm/w
ell)
0.5%FCS NA-TGF- 10
3
CMMut
CMControl
CMWt
CMMut
CMMut+SU5402-*
- CMMut+SD208
Control PASMC(n=3)
100
125
a
��
50
75
100
*
*
���� P<0.01
0 1 2 3 4 525 *
*
Days
Mutant PASMC(n=3)
125
150
b
0 3 )��
��
75
100
*
*Cel
l num
ber (
1x1
0 3 )C
ell n
umbe
r (1x
1
�� P<0.01
0 1 2 3 4 525
50
*
Days
Apoptosis and engulfment of apoptotic cells is known to be accompanied by the robust release of TGF-β.[25] Our group has previously shown that PASMCs isolated from patients with idiopathic PAH or heritable PAH
Figure 5: Graphs showing 3H-thymidine uptake in normal PASMCs following treatment with conditioned media (CM) from control PAECS, or PAECs transfected with WT or Mut BMPR-II constructs. A specifi c TGF-β1 neutralizing antibody signifi cantly reversed the CM Mut-induced DNA synthesis in PASMCs (a). Similar effects were observed with an inhibitor of the TGF-β type 1 receptor (ALK-5), SD208, and the FGFR1 inhibitor, SU5402 (b)
Figure 6: Graphs showing control (a) and BMPR II mutant (b) PASMC numbers following treatment with conditioned media (CM) from control PAECS, or PAECs transfected with WT or Mut BMPR-II constructs. The mutant PASMCs harbored one of the following mutations: N903S; W9X; or R899X. Increased proliferation was observed in both control and mutant PASMCs in the presence of CM from PAECs transfected with mutant (Mut) BMPR-II. There was a trend toward higher rates of proliferation (Figure 6b) in mutant PASMCs (~25%) compared to the control PASMCs, but this did not reach statistical signifi cance (P=0.062). The results in the control and mutant PASMCs were otherwise similar and the heightened growth response to CM Mut could be abrogated by SU5402 or SD208 in both cell types
Yang, et al.: BMPR-II mutation and endothelial apoptosis

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 110
exhibit an exaggerated growth response to TGF-β1 compared to control cells.[20] We therefore questioned whether the growth of PASMCs harboring BMPR-II mutations would be more susceptible than control cells to the pro-proliferative effects of conditioned media from PAECs transfected with mutant BMPR-II. Conditioned media from mutant transfected PAECS caused an increased proliferation of both control and BMPR-II mutant PASMCs. Although there was a trend towards heightened proliferation of PASMCs from patients harboring BMPR-II mutations, this did not reach statistical significance.
Taken together, our findings further strengthen the view that BMPR-II mutation promotes PAEC apoptosis and provide evidence that part of the endothelial dysfunction includes an increased release of growth factors that support proliferation of the underlying mesenchymal cells. Our data further suggests that BMPR-II mutation in PAECs leads to altered cross-talk between endothelial and smooth muscle cells that could contribute to the pathobiology of pulmonary hypertension.
ACKNOWLEDGMENTS
This project was funded by the British Heart Foundation (Program grant RG256 to NWM) and the European Commission, under the Sixth Framework Program (Contract No LSHM-CT-2005-018725, PULMOTENSION).
REFERENCES
1. Runo JR, Loyd JE. Primary pulmonary hypertension. Lancet 2003;361:1533-44.
2. Lane KB, Machado RD, Pauciulo MW, Thomson JR, Phillips JA 3rd, Loyd JE, et al. Heterozygous germline mutations in BMPR2, encoding a TGF-beta receptor, cause familial primary pulmonary hypertension. Nat Genet 2000;26:81-4.
3. Deng Z, Haghighi F, Helleby L, Vanterpool K, Horn EM, Barst RJ, et al. Fine mapping of PPH1, a gene for familial primary pulmonary hypertension, to a 3-cM region on chromosome 2q33. Am J Respir Crit Care Med 2000;161:1055-9.
4. Machado RD, Aldred MA, James V, Harrison RE, Patel B, Schwalbe EC, et al. Mutations of the TGF-beta type II receptor BMPR2 in pulmonary arterial hypertension. Hum Mutat 2006;27:121-32.
5. Thomson JR, Machado RD, Pauciulo MW, Morgan NV, Humbert M, Elliott GC, et al. Sporadic primary pulmonary hypertension is associated with germline mutations of the gene encoding BMPR-II, a receptor member of the TGF-beta family. J Med Genet 2000;37:741-5.
6. Atkinson C, Stewart S, Upton PD, Machado R, Thomson JR, Trembath RC, et al. Primary pulmonary hypertension is associated with reduced pulmonary vascular expression of type II bone morphogenetic protein receptor. Circulation 2002;105:1672-8
7. Morrell NW, Adnot S, Archer SL, Dupuis J, Jones PL, MacLean MR, et al. Cellular and molecular basis of pulmonary arterial hypertension. J Am Coll Cardiol 2009;54:S20-31.
8. Sakao S, Tatsumi K, Voelkel NF. Endothelial cells and pulmonary arterial hypertension: apoptosis, proliferation, interaction and transdiff erentiation. Respir Res 2009;10:95.
9. Sakao S, Taraseviciene-Stewart L, Wood K, Cool CD, Voelkel NF. Apoptosis of pulmonary microvascular endothelial cells stimulates vascular smooth muscle cell growth. Am J Physiol Lung Cell Mol Physiol 2006;291:L362-8.
10. Eddahibi S, Guignabert C, Barlier-Mur AM, Dewachter L, Fadel E, Dartevelle P, et al. Cross talk between endothelial and smooth muscle cells in pulmonary hypertension: Critical role for serotonin-induced smooth muscle hyperplasia. Circulation 2006;113:1857-64.
11. Sanchez O, Marcos E, Perros F, Fadel E, Tu L, Humbert M, et al. Role of endothelium-derived CC chemokine ligand 2 in idiopathic pulmonary arterial hypertension. Am J Respir Crit Care Med 2007;176:1041-7.
12. Izikki M, Guignabert C, Fadel E, Humbert M, Tu L, Zadigue P, et al. Endothelial-derived FGF2 contributes to the progression of pulmonary hypertension in humans and rodents. J Clin Invest 2009;119:512-23.
13. Southwood M, Jeff ery TK, Yang X, Upton PD, Hall SM, Atkinson C, et al. Regulation of bone morphogenetic protein signalling in human pulmonary vascular development. J Pathol 2008;214:85-95.
14. Yang X, Long L, Southwood M, Rudarakanchana N, Upton PD, Jeff ery TK, et al. Dysfunctional Smad signaling contributes to abnormal smooth muscle cell proliferation in familial pulmonary arterial hypertension. Circ Res 2005;96:1053-63.
15. Van Waarde MA, van Assen AJ, Kampinga HH, Konings AW, Vujaskovic Z. Quantifi cation of transforming growth factor-beta in biological material using cells transfected with a plasminogen activator inhibitor-1 promoter-luciferase construct. Anal Biochem 1997;247:45-51.
16. Teichert-Kuliszewska K, Kutryk MJ, Kuliszewski MA, Karoubi G, Courtman DW, Zucco L, et al. Bone morphogenetic protein receptor-2 signaling promotes pulmonary arterial endothelial cell survival: Implications for loss-of-function mutations in the pathogenesis of pulmonary hypertension. Circ Res 2006;98:209-17.
17. Rabinovitch M. EVE and beyond, retro and prospective insights. Am J Physiol 1999; 277:L5-12.
18. Song Y, Coleman L, Shi J, Beppu H, Sato K, Walsh K, et al. Infl ammation, endothelial injury, and persistent pulmonary hypertension in heterozygous BMPR2-mutant mice. Am J Physiol Heart Circ Physiol 2008;295:H677-90.
19. Zhang S, Fantozzi I, Tigno DD, Yi ES, Platoshyn O, Thistlethwaite PA, et al. Bone morphogenetic proteins induce apoptosis in human pulmonary vascular smooth muscle cells. Am J Physiol Lung Cell Mol Physiol 2003;285:L740-54.
20. Morrell NW, Yang X, Upton PD, Jourdan KB, Morgan N, Sheares KK, et al. Altered growth responses of pulmonary artery smooth muscle cells from patients with primary pulmonary hypertension to transforming growth factor-beta(1) and bone morphogenetic proteins. Circulation 2001;104:790-5.
21. Yang J, Davies RJ, Southwood M, Long L, Yang X, Sobolewski A, et al. Mutations in bone morphogenetic protein type II receptor cause dysregulation of Id gene expression in pulmonary artery smooth muscle cells: implications for familial pulmonary arterial hypertension. Circ Res 2008;102:1212-21.
22. Valdimarsdott ir G, Goumans MJ, Rosendahl A, Brugman M, Itoh S, Lebrin F, et al. Stimulation of Id1 expression by bone morphogenetic protein is suffi cient and necessary for bone morphogenetic protein-induced activation of endothelial cells. Circulation 2002;106:2263-70.
23. David L, Mallet C, Mazerbourg S, Feige JJ, Bailly S. Identifi cation of BMP9 and BMP10 as functional activators of the orphan activin receptor-like kinase 1 (ALK1) in endothelial cells. Blood 2007;109:1953-61.
24. Upton PD, Davies RJ, Trembath RC, Morrell NW. Bone morphogenetic protein (BMP) and activin type II receptors balance BMP9 signals mediated by activin receptor-like kinase-1 in human pulmonary artery endothelial cells. J Biol Chem 2009;284:15794-804.
25. McDonald PP, Fadok VA, Bratton D, Henson PM. Transcriptional and translational regulation of infl ammatory mediator production by endogenous TGF-β in macrophages that have ingested apoptotic cells. J Immunol 1999;163:6164-72.
Source of Support: British Heart Foundation (Program grant RG256 to NWM) and the European Commission, under the Sixth Framework Program (Contract No LSHM-CT-2005-018725, PULMOTENSION),
Confl ict of Interest: None declared.
Yang, et al.: BMPR-II mutation and endothelial apoptosis

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 111
Dysfunctional bone morphogenetic protein (BMP) signaling has been found in patients with pulmonary arterial hypertension (PAH); however, the exact role of BMP signaling in the treatment of PAH remains unknown. The BMP receptor type II (BMPR-II) is a member of the TGF-β family of signaling molecules. Functional receptors are heterodimers composed of a BMPR-II subunit and a serine–threonine kinase type I subunit, of which there are three members: BMPR-Ia, BMPR-Ib and Alk2.[1,2] Both BMPR-II and BMPR-Ia/Ib are highly expressed in the pulmonary vascular smooth muscle and endothelium. The discovery of heterozygous mutations of the BMPR-II gene (BMPR2) in patients with hereditary (or familial) PAH and patients with idiopathic PAH [3,4] represented a significant advance in the understanding of the genetic contributions to PAH.
The two main pathways downstream of BMP signaling are the Smad-dependent pathway, which uses Smad-signaling proteins, and the Smad-independent pathway, which involves p38, MAPK, ERK and JNK proteins.[1,5,6] In the Smad pathway, activation of the receptor complex by ligand binding results in the recruitment and phosphorylation of regulatory Smad proteins (Smads-1, 5 or 8). These Smad proteins recruit Smad-4, and the resulting complex is translocated to the nucleus, where it regulates transcription of target genes containing the Smad-binding sequence. Although BMP signaling may provide a common pathway in PAH pathogenesis, it is unclear whether current treatments
Combination use of sildenafi l and simvastatin increases BMPR-II signal transduction in rats
with monocrotaline-mediated pulmonary hypertension
Tuguang Kuang1, Jun Wang1,2, Amy Zeifman3, Baosen Pang1, Xiuxia Huang1, Elyssa D. Burg4, Jason X.-J. Yuan1,3, Chen Wang1,2,5
1Department of Pulmonary and Critical Care Medicine, Beijing Chao-Yang Hospital, Capital Medical University and Beijing Institute of Respiratory Medicine, China, 2Department of Physiology, Capital Medical University, Beijing, China, 3Department of Medicine,
University of Illinois, Chicago, Illinois, USA, 4National Institutes of Health, Bethesda, Maryland, USA, 5Beijing Hospital of the Ministry of Health, Beijing, China
Shor t Research Repor t
targeting different pathways lead to an increase in BMP signal transduction in the lung tissues. A treatment that targets a common underlying cause of PAH, such as BMP dysfunction, may prove efficacious.
Both sildenafil, a phosphodiesterase-5 inhibitor, and simvastatin, a cholesterol-lowering drug, have therapeutic effects on PAH. In our previous studies, we investigated three different therapeutic regimens for treating pulmonary hypertension (PH) in rats injected with monocrotaline (MCT) using sildenafil, simvastatin and a combined sildenafil and simvastatin treatment. MCT injections cause a significant increase in the mean pulmonary arterial pressure (PAP) and pulmonary vascular medial thickening. The time course for the MCT-induced increase in mean PAP is associated with the MCT-induced increase in pulmonary vascular wall thickness, occurring after 2 weeks of the injection of MCT.[7] Although all treatment regimens have an effect on right ventricular systolic pressure (RVSP) in rats with MCT-mediated PH, the combined drug treatment of both sildenafil and simvastatin is more effective in reducing RVSP than either drug alone.[7]
The purpose of this study was to investigate the changes in BMP signaling, including both Smad and ERK downstream
Access this article online
Quick Response Code:Website: www.pulmonarycirculation.org
DOI: 10.4103/2045-8932.78102
Pulm Circ 2011;1:111-4
Address correspondence to:Prof. Chen WangBeijing Chao-Yang Hospital, Capital Medical University,8 Gongtinan Road, Chaoyang District, Beijing - 100 020, China.E-mail: [email protected]

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 112
pathways, in rats with MCT-induced PH treated with sildenafil and simvastatin.
We first examined whether key BMP molecules (BMPR-II, BMPR-Ia and BMP-2) were changed in lung tissues over a 4-week time course in rats subcutaneously injected with MCT (50 mg/kg or 25 ml/kg of 2% MCT). Interestingly, animals at both weeks 1 and 2 (after injection of MCT) had significantly increased levels of BMPR-II (3.655±1.008 in week 1 group and 2.164±0.508 in week 2 group compared to 1.874±0.121 in the saline injected control), BMPR-Ia (1.451±0.334 in week 1 group and 1.082±0.106 in week 2 group compared to 0.625±0.188 in the saline injected control animals), and BMP-2 (1.500±0.243 in the week 1 group and 1.428±0.056 in week 2 group vs. 0.696±0.068 in the saline injected control group); however, by the third week, BMPR-II had declined to levels below those of the control group and, by the fourth week, BMP-2 had also declined to below the control levels [Figure 1]. Our observations indicate that MCT injection caused a transient increase in the mRNA and protein expression of BMP-2, BMPR-II and BMPR-Ia, which correlates with a transient increase in Smad1 phosphorylation.[7] The changes in BMP signaling molecules correlate well with the observed MCT-induced PH at 3 and 4 weeks.[7] Thus, both hemodynamic indicators of PAH and underlying molecular abnormalities (e.g., BMP-signaling molecules and Smad) correlate with each other in rats during the development of MCT-induced PH.
Then, we examined the effects of sildenafil, simvastatin and combination treatment on BMPR-Ia, BMPR-II and BMP-2 mRNA levels in our MCT model of PH. Compared with rats in the sham group (normotensive saline-injected rats), lung tissue BMPR-Ia, BMPR-II and BMP-2 mRNA levels detected by real-time reverse transcriptase polymerase chain reaction (RT-PCR) in the MCT-injected control group decreased significantly (BMPR-Ia: 0.50±0.09 compared with 0.39±0.11; BMPR-II: 1.75±0.28 compared with
0.40±0.02; BMP-2: 0.68±0.02 compared with 0.37±0.05 arbitrary unit) [Figure 2A(a–c)]. Either sildenafil or simvastatin treatment alone prevented decreases in BMPR-Ia, BMPR-II and BMP-2 mRNA levels, but the combination therapy was more effective at preventing the decrease in BMPR-II and BMPR-Ia [Figure 2B(b and c)]. The level of BMP-2 in the combination group, while being higher than that in the MCT-injected control animals, was not significantly different from either treatment alone [Figure 2B(a)].
BMP signaling, including BMP-2 and its receptors, plays an important role in maintaining the normal structure of the pulmonary vasculature through its regulation of apoptosis and suppression of cell proliferation.[8-10] In the pulmonary vasculature, BMP-2 is predominantly expressed in endothelial cells, with a low level of expression in vascular smooth muscle cells, whereas BMPR-II localizes to endothelial cells, smooth muscle cells and adventitial fibroblasts.[8] In both apical and basal membranes of the arteriolar endothelium, BMPR-II colocalizes with caveolin-1,[11] indicating that BMPR-II may have a hemodynamic regulatory role because caveolae also contains hemodynamically relevant signaling molecules, including eNOS,[12,13] the serotonin transporter,[14-16] transient receptor potential (TRP) channels[17,18] and endothelin receptors.[19,20]
In our study, the expression of BMP-2, BMPR-Ia and BMPR-II mRNAs during the 4-week course of MCT-induced PH increased significantly in the first week after MCT injection. At week 2, these levels were still above baseline, although they had started to decline from week 1. This initial increase was followed by a significant decrease 3–4 weeks after MCT injection. We did not study BMP signaling or pulmonary artery smooth muscle cell (PASMC) proliferation in MCT-treated rats beyond 4 weeks after injection; however, within the 4-week time course, we observed an important difference
Figure 1: Bone morphogenetic protein (BMP) signaling proteins in rat lung initially increase and then decrease after monocrotaline (MCT) injection. mRNA was collected from whole lung from rats injected with MCT at the indicated time points after injection. The week 0 group was injected with saline and RNA was isolated the next day. mRNA was used in reverse transcriptase-polymerase chain reaction to quantify BMP-2 (a), BMPR-Ia (b) and BMPR-II (c) mRNA levels. All BMP signaling molecule mRNA levels were normalized against Glyceraldehyde 3-phosphate dehydrogenase (GAPDH) mRNA levels. Data are presented in arbitrary units (a.u.) as mean±SD; n=8/group; **P<0.01 vs. 0 week control group
Kuang, et al.: Sildenafi l and simvastatin increase BMP signaling
MCT Injection (wks)0 1 2 3 4 0 1 2 3 4 0 1 2 3 4
BM
P-2
mR
NA
(a.u
.)
0.0
0.3
0.6
0.9
1.2
1.5
1.8
MCT Injection (wks)
BM
PRIa
mR
NA
(a.u
.)
0.0
0.3
0.6
0.9
1.2
1.5
1.8
MCT Injection (wks)
BM
PRII
mR
NA
(a.u
.)
0
1
2
3
4**
**
**
**
**
**
**
** **
a b c

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 113
between MCT-induced PAH and clinical PAH caused by defective BMP signaling. In many patients, dysfunctional BMP signaling due to BMPR-II mutations and/or downregulated BMPR-Ia causes PAH.[21-24] However, in the MCT model, there was an initial increase in BMP signaling molecules as previously noted. The subsequent decline in these correlated with the development of elevated RVSP, right ventricular hypertrophy (RVH) and remodeling.[7] An initial increase in BMP signaling molecules in models of PAH is not without precedent, however, as hypoxia induces an initial rise (~3 weeks) in BMP4 in mouse lung followed by a decrease in BMP4 mRNA after week 3.[25] It may be that initial MCT-induced endothelial injury causes the subsequent rise in BMP signaling. Lung tissue p-Smad1, a downstream signaling molecule involved in proapoptotic BMPR-II signaling, paralleled the changes of BMP2, BMPR-Ia and BMPR-II mRNAs, consistent with the observation of previous studies.[26,27] This pattern suggests that acute injury to the pulmonary vascular endothelium may stimulate BMPR-II, BMPR-Ia and BMP-2 expression in lung vascular endothelial cells, whereas chronic injury results in a decline of these molecules.
BMPR-II signaling in pulmonary artery endothelial cells (PAEC) promotes cell survival and protects against apoptosis, whereas it is proapoptotic (through Smad
signaling) in PASMC.[10,28] It is therefore tempting to speculate that PAEC respond to MCT injury initially by increasing BMP signaling to promote endothelial protection; the subsequent MCT-induced decline in BMP-signaling molecules may then tip the balance toward an increase in PASMC proliferation, which overtakes the already injured endothelium, thus leading to muscularization and PH by week 3 after MCT injection. Indeed, the pulmonary vascular remodeling associated with clinical PAH is believed to result largely from increased proliferation and decreased apoptosis of PASMC that could be caused by defects in the proapoptotic BMPR-II/Smad signaling pathway.[6,21-23,28,29]
Our results suggest that targeting BMPR-II deficiencies in PAH may provide a useful therapeutic approach to treat the disease. Current PAH medications do not target the BMP pathway, but a more complete understanding of BMPR-II signaling in the MCT model of PH, such as provided here, will prove useful in future investigations aimed at developing interventions that target this pathway.
The levels of lung tissue BMPR-II, BMPR-Ia and BMP-2 mRNA and p-Smad1 protein were much higher in both the sildenafil and the simvastatin groups compared with
Figure 2: Combined sildenafi l and simvastatin treatment prevents the monocrotaline (MCT)-induced decrease in bone morphogenetic protein (BMP)-signal pathway molecules to a greater extent than either drug alone. mRNA was collected from whole lung tissue from saline-injected sham treated rats, MCT-injected control rats and rats treated with sildenafi l, simvastatin or both. mRNA levels of BMP-2 (Aa), BMPR-Ia (Ab) and BMPR-II (Ac) were determined using reverse transcriptase-polymerase chain reaction and normalized to GAPDH. Increases in BMP-2 (a), BMPR-Ia (b) and BMPR-II (c) are shown in (B) as the change compared with the levels in the MCT-injected control group. Data are presented in arbitrary units (A) as mean±SD; n=8/group; **P<0.01 vs. sham-injected (A) or vs. MCT-injected control (B); ++ P<0.01 vs. combination group (B)
Kuang, et al.: Sildenafi l and simvastatin increase BMP signaling
BM
P-2/
GA
PDH
0.0
0.2
0.4
0.6
0.8
**
Cha
nge
in B
MP-
2 Pr
otei
n
0.0
0.2
0.4
0.6
0.8
1.0
1.2
****
**
++
MCT MCT+Sildenafil
MCT+Simvastatin
MCT+Sildenafil+Simvastatin
Sham-treated MCT-treated
BM
PRIa
/GA
PDH
0.0
0.2
0.4
0.6
0.8
BM
PRII
/GA
PDH
0.0
0.5
1.0
1.5
2.0
**
**
Cha
nge
in B
MPR
Ia P
rote
in
0.00.30.60.91.21.51.82.1
Cha
nge
in B
MPR
II P
rote
in
0.00.40.81.21.62.02.42.8
++
**
**
**
++
++
++
****
**
++++
b
a a b c
a b c

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 114
the MCT-injected control group, indicating that either drug alone inhibits the decrease in the expression of the BMP signaling molecules. The inhibition of the loss of BMPR-II signaling may be an important mechanism underlying the prevention of PASMC overproliferation and pulmonary vascular remodeling in the sildenafil or simvastatin treatment groups. The low levels of matrix metalloproteinases (MMPs) may be due to the concomitant increase in BMP-signal transduction, as the reduction in BMP signaling has been shown to reduce MMP activity.[30] Furthermore, reductions in BMP signaling and/or MMP activity confer resistance to apoptosis,[30] indicating that sildenafil and simvastatin may reduce PASMC proliferation at least in part by maintaining BMP signaling molecules.
Because combination treatment was able to prevent the decrease in lung tissue BMPR-II and BMPR-Ia to a greater extent than either treatment alone, it is likely that the additive effect of combination treatment in preventing the development of PH involves BMP signaling.
ACKNOWLEDGMENTS
We would like to thank Dr. Ling Zhu for her helpful comments in preparing this manuscript. This work was supported in part by grants from the National Natural Science Foundation of China (NSFC-30810103904) and 973 Program (2009CB522107).
REFERENCES
1. Nohe A, Keating E, Knaus P, Petersen NO. Signal transduction of bone morphogenetic protein receptors. Cell Signal 2004;16:291-9.
2. Yu PB, Beppu H, Kawai N, Li E, Bloch KD. Bone morphogenetic protein (BMP) type II receptor deletion reveals BMP ligand-specifi c gain of signaling in pulmonary artery smooth muscle cells. J Biol Chem 2005;280:24443-50.
3. Machado RD, Pauciulo MW, Thomson JR, Lane KB, Morgan NV, Wheeler L, et al. BMPR2 haploinsuffi ciency as the inherited molecular mechanism for primary pulmonary hypertension. Am J Hum Genet 2001;68:92-102.
4. Newman JH, Wheeler L, Lane KB, Loyd E, Gaddipati R, Phillips JA 3rd, et al. Mutation in the gene for bone morphogenetic protein receptor II as a cause of primary pulmonary hypertension in a large kindred. N Engl J Med 2001;345:319-24.
5. Nohe A, Hassel S, Ehrlich M, Neubauer F, Sebald W, Henis YI, et al. The mode of bone morphogenetic protein (BMP) receptor oligomerization determines different BMP-2 signaling pathways. J Biol Chem 2002;277:5330-8.
6. Mandegar M, Fung YC, Huang W, Remillard CV, Rubin LJ, Yuan JX. Cellular and molecular mechanisms of pulmonary vascular remodeling: Role in the development of pulmonary hypertension. Microvasc Res 2004;68:75-103.
7. Kuang T, Wang J, Pang B, Huang X, Burg ED, Yuan JX, et al. Combination of sildenafi l and simvastatin ameliorates monocrotaline-induced pulmonary hypertension in rats. Pulm Pharmacol Ther 2010;23:456-64.
8. Takahashi H, Goto N, Kojima Y, Tsuda Y, Morio Y, Muramatsu M, et al. Downregulation of type II bone morphogenetic protein receptor in hypoxic pulmonary hypertension. Am J Physiol Lung Cell Mol Physiol 2006;290:L450-8.
9. Fukui N, Zhu Y, Maloney WJ, Clohisy J, Sandell LJ. Stimulation of BMP-2 expression by pro-infl ammatory cytokines IL-1 and TNF-a in normal and osteoarthritic chondrocytes. J Bone Joint Surg Am 2003;85-A:59-66.
10. Zhang S, Fantozzi I, Tigno DD, Yi ES, Platoshyn O, Thistlethwaite PA, et al. Bone morphogenetic proteins induce apoptosis in human pulmonary vascular smooth muscle cells. Am J Physiol Lung Cell Mol Physiol 2003;285:L740-54.
11. Ramos M, Lame MW, Segall HJ, Wilson DW. The BMP type II receptor is located in lipid raft s, including caveolae, of pulmonary endothelium in vivo and in vitro. Vascul Pharmacol 2006;44:50-9.
12. Garcia-Cardena G, Oh P, Liu J, Schnitzer JE, Sessa WC. Targeting of nitric oxide synthase to endothelial cell caveolae via palmitoylation: Implications for nitric oxide signaling. Proc Natl Acad Sci U S A 1996;93:6448-53.
13. Shaul PW, Smart EJ, Robinson LJ, German Z, Yuhanna IS, Ying Y, et al. Acylation targets emdothelial nitric-oxide synthase to plasmalemmal caveolae. J Biol Chem 1996;271:6518-22.
14. Fiorica-Howells E, Hen R, Gingrich J, Li Z, Gershon MD. 5-HT2A receptors: Location and functional analysis in intestines of wild-type and 5-HT2A knockout mice. Am J Physiol Gastrointest Liver Physiol 2002;282:G877-93.
15. Dreja K, Voldstedlund M, Vinten J, Tranum-Jensen J, Hellstrand P, Sward K. Cholesterol depletion disrupts caveolae and diff erentially impairs agonist-induced arterial contraction. Arterioscler Thromb Vasc Biol 2002;22:1267-72.
16. Bhatnagar A, Sheffler DJ, Kroeze WK, Compton-Toth B, Roth BL. Caveolin-1 interacts with 5-HT2A serotonin receptors and profoundly modulates the signaling of selected Gaq-coupled protein receptors. J Biol Chem 2004;279:34614-23.
17. Lockwich TP, Liu X, Singh BB, Jadlowiec J, Weiland S, Ambudkar IS. Assembly of Trp1 in a signaling complex associated with caveolin-scaff olding lipid raft domains. J Biol Chem 2000;275:11934-42.
18. Bergdahl A, Gomez MF, Dreja K, Xu SZ, Adner M, Beech DJ, et al. Cholesterol depletion impairs vascular reactivity to endothelin-1 by reducing store-operated Ca2+ entry dependent on TRPC1. Circ Res 2003;93:839-47.
19. Chun M, Liyanage UK, Lisanti MP, Lodish HF. Signal transduction of a G protein-coupled receptor in caveolae: Colocalization of endothelin and its receptor with caveolin. Proc Natl Acad Sci U S A 1994;91:11728-32.
20. Okamoto Y, Ninomiya H, Miwa S, Masaki T. Cholesterol oxidation switches the internalization pathway of endothelin receptor type A from caveolae to clathrin-coated pits in Chinese hamster ovary cells. J Biol Chem 2000;275:6439-46.
21. Long L, Crosby A, Yang X, Southwood M, Upton PD, Kim DK, et al. Altered bone morphogenetic protein and transforming growth factor-b signaling in rat models of pulmonary hypertension: Potential for activin receptor-like kinase-5 inhibition in prevention and progression of disease. Circulation 2009;119:566-76.
22. Schwappacher R, Weiske J, Heining E, Ezerski V, Marom B, Henis YI, et al. Novel crosstalk to BMP signalling: cGMP-dependent kinase I modulates BMPR receptor and Smad activity. EMBO J 2009;28:1537-50.
23. Morrell NW. Pulmonary hypertension due to BMPR2 mutation: A new paradigm for tissue remodeling? Proc Am Thorac Soc 2006;3:680-6.
24. Davies RJ, Morrell NW. Molecular mechanisms of pulmonary arterial hypertension: Role of mutations in the bone morphogenetic protein type II receptor. Chest 2008;134:1271-7.
25. Frank DB, Abtahi A, Yamaguchi DJ, Manning S, Shyr Y, Pozzi A, et al. Bone morphogenetic protein 4 promotes pulmonary vascular remodeling in hypoxic pulmonary hypertension. Circ Res 2005;97:496-504.
26. Ramos MF, Lame MW, Segall HJ, Wilson DW. Smad signaling in the rat model of monocrotaline pulmonary hypertension. Toxicol Pathol 2008;36:311-20.
27. Morty RE, Nejman B, Kwapiszewska G, Hecker M, Zakrzewicz A, Kouri FM, et al. Dysregulated bone morphogenetic protein signaling in monocrotaline-induced pulmonary arterial hypertension. Arterioscler Thromb Vasc Biol 2007;27:1072-8.
28. Eickelberg O, Morty RE. Transforming growth factor b/bone morphogenic protein signaling in pulmonary arterial hypertension: Remodeling revisited. Trends Cardiovasc Med 2007;17:263-9.
29. Rubin LJ. Pulmonary arterial hypertension. Proc Am Thorac Soc 2006;3:111-5.
30. El-Bizri N, Guignabert C, Wang L, Cheng A, Stankunas K, Chang CP, et al. SM22a-targeted deletion of bone morphogenetic protein receptor 1A in mice impairs cardiac and vascular development, and infl uences organogenesis. Development 2008;135:2981-91.
Kuang, et al.: Sildenafi l and simvastatin increase BMP signaling
Source of Support: National Natural Science Foundation of China (NSFC-30810103904) and 973 Program (2009CB522107), Confl ict of
Interest: None declared.

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 115
Severe pulmonary artery hypertension following intracardiac repair of tetralogy of
Fallot: An unusual fi ndingBhupesh Kumar1, Goverdhan D. Puri1, RohitManoj2, Kirti Gupta3, Shyam K. S.4
Department of 1Anesthesia & Intensive Care, 2Cardiology, 3Histopathology, and 4Cardiac Surgery, Postgraduate Institute of Medical Education and Research, Chandigarh, India
ABSTRACT
Although mild increase in pulmonary vascular resistance following intracardiac repair of tetralogy of Fallot is often seen in the early postoperative period, it usually subsides without any sequel. Persistent severe pulmonary artery hypertension after total correction is rare. We report a child with tetralogy of Fallot and Down’s syndrome, who developed severe pulmonary hypertension and low cardiac output syndrome following an intracardiac repair, which was resistant to specifi c pulmonary vasodilators and increasing ionotropes. The post correction echocardiogram suggested an intact ventricular septal defect patch, no residual gradient across the right ventricular outfl ow tract, with free pulmonary regurgitation. The child had a poor outcome. A postmortem biopsy revealed histopathological signs of pulmonary hypertension.
Key Words: Down’s syndrome, intracardiac repair, severe pulmonary artery hypertension, tetralogy of Fallot
Access this article online
Quick Response Code:Website: www.pulmonarycirculation.org
DOI: 10.4103/2045-8932.78099
Pulm Circ 2011;1:115-8
Address correspondence to:Dr. Bhupesh KumarDepartment of Anesthesia and Intensive Care,Postgraduate Institute of Medical Education and Research,Chandigarh - 12, India.E-mail: [email protected]
INTRODUCTION
A mild increase in pulmonary vascular resistance is often seen after a successful total correction of tetralogy of Fallot (TOF) in the early postoperative period. This is usually reversed with time, without producing untoward consequences. Persistence of severe pulmonary artery hypertension (PAH) following corrective surgery for TOF is rare.[1] We present a case of TOF with Down’s syndrome (DS), where there was development of severe PAH and low cardiac output syndrome following intracardiac repair (ICR), leading to a negative outcome. We also discuss the possible causes of PAH in this setting.
CASE REPORT
A seven-year-old male child, weighing 18 kg, presented to our Cardiac Surgical Outpatient Department, with a history of tachypnea and cyanosis since birth. His perinatal period was uneventful. General physical examination revealed features of DS with mental retardation and
delayed developmental milestones, besides cyanosis and clubbing. The pulse rate was 82 per minute and blood pressure was 100 / 60 mmHg. On auscultation there was a 3 / 6 ejection systolic murmur in the pulmonary area, and normal breath sounds. Routine blood examination was normal except for hemoglobin of 15.3 gm%. Electrocardiogram revealed features of right ventricular hypertrophy. Chest X-ray showed pulmonary oligemia and a boot-shaped heart. The echocardiogram revealed a 15 mm perimembranous ventricular septal defect (VSD) with 50% aortic override, severe right ventricular outflow tract (RVOT) obstruction (peak gradient 110 mmHg), with infundibular, valvular, and supravalvular (small main pulmonary artery) stenosis. A small-sized (3 mm) patent ductus arteriosus (PDA), with a left-to-right shunt, and a left superior vena cava (LSVC) was draining into the coronary sinus. The right and left ventricular systolic function was normal. A preoperative catheterization study showed equal pressures in right ventricle (RV), left
Case Repor t

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 116
ventricle (LV), and aorta. The pulmonary artery (PA) was not entered. The coronary anatomy was normal and there were no aortopulmonary collaterals.
He underwent intracardiac repair with pericardial patch augmentation of the RVOT and main pulmonary artery, together with PDA ligation, and cardiopulmonary bypass (CPB). Total CPB time and aortic cross clamp time were 132 and 92 minutes, respectively. Termination of CPB was achieved using adrenaline 0.1 – 0.15 μg/kg/minute, dopamine 8 μg/kg/minute, and nitroglycerin 0.5 μg/kg/minute. Immediately after CPB, needle insertion in the RV and PA showed a pressure of 55 / 4 and 48 / 16 mmHg, respectively, with a corresponding systemic pressure of 65 / 44 mmHg. In the postoperative period, he developed features of low cardiac output syndrome with increase in ionotropic requirement. The postoperative ECG revealed atrioventricular block. Echocardiogram on day two showed dilated RA and RV, intact VSD patch, with no RVOT obstruction, and mild right pulmonary artery (RPA) origin stenosis. The catheterization study done on postoperative day two revealed the presence of severe PAH (RV systolic pressure - 55 / 8 mmHg, with a corresponding systemic pressure of 82 / 43 mmHg) with no gradient across the RVOT. Pulmonary artery angiogram showed mild RPA origin stenosis [Figure 1] and free pulmonary regurgitation. LSVC draining to the LA was ruled out [Figure 2]. He was started on sildenafil 0.5 mg / kg every six hours and Thyroxin 12.5 μg once daily, besides an increase in inotropes. Furthermore, the postoperative course was characterized by hypotension in spite of maximal inotropes. Finally the patient had a cardiopulmonary arrest on postoperative day four and could not be revived. The subsequent postmortem lung biopsy revealed features of pulmonary hypertension, with medial hypertrophy and intimal proliferation in the intra-acinar arterioles corresponding to grade II of the Heath-Edwards grading system of pulmonary hypertension [Figure 3].
DISCUSSION
The poor clinical results following ICR of TOF are usually due to incomplete correction of the defect. It could be failure to relieve pulmonary stenosis, creation of free pulmonary insufficiency, inadequate closure of VSD, undetected branch pulmonary artery stenosis or absent left pulmonary artery and pre-existing pulmonary hypertension or left ventricular failure.
In the present case, the poor outcome was due to severe PAH together with the development of low cardiac output syndrome, as suggested by the postoperative catheterization study.
Kumar, et al.: Severe PAH after tetralogy of Fallot repair
Figure 1: Catheterization study showing mild RPA origin stenosis
Figure 2: Catheterization study showing LSVC opening to CS
Severe PAH following correction of TOF is rare, with a prevalence of about 1%.[1] In some isolated cases, it may be due to previously undetected pulmonary agenesis, pulmonary thrombosis, inadequate closure of the ventricular septal defect, with relief of the pulmonic stenosis, or too large a shunt from a previous Blalock, or, more likely, a Pott’s anastomosis.[2-4]In the present case pressure measurement on the operating table, after coming off CPB, showed high RV (55 / 4 mmHg) and PA (48 / 16 mmHg) pressure, with a corresponding systemic pressure of 65 / 44 mmHg. It was accepted, as there was no significant gradient across the RVOT, and the PA pressure was thought to settle in due course. Furthermore, a search for the cause of persistent severe PAH with a postoperative echo and catheterization study showed only mild RPA origin stenosis, which did not explain the finding of severe

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 117
pulmonary hypertension. However, our patient had DS with a small PDA, which might have contributed to the development of PAH.
Children with DS are at an increased risk of developing PAH due to multiple factors: Congenital heart disease (CHD) with persistent left-to-right shunts, chronic upper airway obstruction, abnormal pulmonary vasculature growth, alveolar hypoventilation, recurrent pulmonary infections, thinner media of the pulmonary arterioles, and diminished number of alveoli.[5-9]
An autopsy study in patients with DS has shown a reduction in the alveolar count, persistence of the fetal double capillary network in the lung, and a reduction in the cross-sectional area of the vascular bed.[6] The increased incidence of persistent pulmonary hypertension in DS is also thought to be due to intrinsic factors, such as abnormal production of NO, and less pulmonary vasodilatation response to NO in DS patients versus control.[10,11]
In addition, following the surgical correction of pulmonary stenosis, significant increase in the pulmonary arterial flow might have enhanced the shear stress on the pulmonary endothelium, causing increased biosynthesis and release of circulating endothelin-1 (ET-1).[12] The elevated plasma levels of ET-1 might be responsible for aggravation of the pre-existing pulmonary hypertension.[13]
A low cardiac output syndrome may be the cause for development of pulmonary hypertension, or, it may occur as a sequel of pulmonary hypertension. Often it is difficult to differentiate between cause and effect. Postoperative low cardiac output may be due to inadequate myocardial protection, ventricle compromised by surgical incision, residual RVOT obstruction, and free pulmonary regurgitation, especially in presence of PAH or residual branch pulmonary stenosis. In a minority of patients it may occur despite a good surgical repair and preserved biventricular systolic function. In such a case echocardiography may show evidence of the restrictive physiology.[14]However, it is a transient phenomenon and
Kumar, et al.: Severe PAH after tetralogy of Fallot repair
Figure 3: (a and b) Histological section showing prominence of the intracinar arterioles with medial hypertrophy corresponding to Grade I pulmonary hypertension (Heath-Edwards grading system), (H and E ×100 (a), ×200 (b). (c) Elastic von-Gieson’s (EVG) stain highlighting the prominent intracinar arterioles (EVG ×100). (d and e) Muscle hypertrophy along with proliferation of intimal cells in the arterioles corresponding to Grade II pulmonary hypertension (Masson’s trichrome ×100 (d), ×400 (e)
a
c d e
b

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 118
Kumar, et al.: Severe PAH after tetralogy of Fallot repair
usually recovers in 72 hours or so. Persistent LSVC with dilated coronary sinus may also cause left ventricular filling impairment that is difficult to recognize in the postoperative period, and may lead to impaired LV performance.[15]
Post CPB thyroid hormone suppression in children has shown to contribute to the development of postoperative low cardiac output syndrome and PAH. Perioperative thyroid supplement may lead to an improved cardiac output. The aim of the supplement should be to restore the serum T3 level to within the normal limit. The recommended replacement dose of T3 is 0.1 – 0.4 μg/kg/dose at 8 – 12 hour intervals.[16]
Our case developed a low cardiac output syndrome resistant to maximum ionotropic support and administration of thyroid hormone. In such a situation, where there is a failing myocardium unresponsive to ionotrops, providing a period of rest to the myocardium on ECMO may be helpful. This facility was not available to us.
The development of severe PAH due to low cardiac output is unlikely in the present case, as pulmonary artery pressure measurement immediately after coming off CPB also showed severe PAH. However, the persistent postoperative low cardiac output may have contributed to the persistence of PAH and failure of response to the specific pulmonary vasodilator (sildenafil). Inhaled NO, a potent selective pulmonary vasodilator, and its demonstrated synergistic effect with sildenafil, could have been useful, but we could not use it because of its unavailability. The subsequent postmortem lung biopsy with features of medial hypertrophy and intimal proliferation in the intra-acinar arterioles also did not correlate with the recent onset of PAH.
To conclude, severe pulmonary hypertension may occur in a patient with TOF if associated with DS. Development of low cardiac syndrome in these patients can produce a
vicious cycle by aggravating the pre-existing PAH, which may lead to a poor outcome.
REFERENCES
1. Roisman ML, Beller BM, O’Keefe JD. Irreversible pulmonary hypertension aft er correction of tetralogy of Fallot. Chest 1972;62:34-8.
2. Gotsman MS, Beck W, Barnard CN, O’Donovan TG, Schrire V. Results of repair of tetralogy of Fallot. Circulation 1969;40:803-21.
3. Ferencz C. Pulmonary vascular bed in tetralogy of Fallot. I Changes with pulmonic stenosis. I1 Changes following a systemic pulmonary arterial anastomosis. Bull John Hopkins Hosp 1960;108:81.
4. Aum D, Khoury GH, Ongley PA, Swan HJ, Kincaid OW. Congenital stenosis of the pulmonary artery branches. Circulation 1984;29:680-7.
5. Cua CL, Blankenship A, North J, Hayes AL, Nelin LD. Increased incidence of idiopathic persistent pulmonary hypertension in Down syndrome neonates. Pediatr Cardiol 2007;28:250-4.
6. Chi TP, Krovetz JL. The pulmonary vascular bed in children with Down syndrome. J Pediatr 1975;86:533-8.
7. Jacobs IN, Gray RF, Todd NW. Upper airway obstruction in children with Down syndrome. Arch Otolaryngol Head Neck Surg 1996;122:945-50.
8. Shah PS, Hellman J, Adatha I. Clinical characteristics and follow up of Down syndrome infants without congenital heart disease who presented with persistent pulmonary hypertension of newborn. Perinatal Med 2004;32:168-70.
9. Byard RW. Forensic issues in Down syndrome fatalities. J Forensic Legal Med 2007;14:475-81.
10. Cappelli-Bigazzi M, Santoro G, Batt aglia C, Palladino MT, Carrozza M, Russo MG, et al. Endothelial cell function in patients with Down’s syndrome. Am J Cardiol 2004;94:392-5.
11. Cannon BC, Feltes TF, Fraley JK. Nitric oxide in the evaluation of congenital heart disease with pulmonary hypertension: Factors related to nitric oxide response. Pediatr Cardiol 2005;26:565-9.
12. Ma ZS, Ma SJ, Dong MF, Wang JT, Wang LX. Eff ect of Captopril on Pulmonary Artery Pressure Following Corrective Surgery for Tetralogy of Fallot. J Card Surg 2009;24:553-5.
13. Hiramoto Y, Shioyama W, Kuroda T, Masaki M, Sugiyama S, Okamoto K, et al. Eff ect of Bosentan on plasma endothelin-1 concentration in patients with pulmonary arterial hypertension. Circ J 2007;71:367-9.
14. Cullen S, Shore D, Redington A. Characterization of right ventricular diastolic performance after complete repair of tetralogy of Fallot. Restrictive physiology predicts slow postoperative recovery. Circulation 1995;91:1782-9.
15. Dibardino DJ, Fraser CD Jr, Dickerson HA, Heinle JS, McKenzie ED, Kung G. Left ventricular infl ow obstruction associated with persistent left superior vena cava and dilated coronary sinus. J Thorac Cardiovasc Surg 2004;127:959-62.
16. Shann F. Drug Doses. 11th ed. Parkville, Australia: Collective Pty Ltd; 2001. p. 40.
Source of Support: None declared. Confl ict of Interest: None declared.

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 119
Clinical demonstration of effi ciency and reversibility of hypoxic pulmonary
vasoconstriction in a patient presenting with unilateral incomplete bronchial occlusion
Syeda Jafri1, Pasupathy Sivasothy1, Francis Wells2, Nicholas W. Morrell1
Department of 1Medicine, Addenbrooke’s Hospital, Cambridge, and 2Department of Cardiothoracic Surgery, Papworth Hospital, Cambridge, UK
ABSTRACT
Although hypoxic pulmonary vasoconstriction is a well-recognized physiological phenomenon it is unusual to observe and assess its effi ciency in clinical practice. Here, we report the case of a 50-year-old female who presented with unilateral incomplete bronchial occlusion due to a carcinoid tumor involving the left main bronchus in the absence of atelectasis. Ventilation-perfusion imaging revealed absent ventilation and perfusion to the left lung. She underwent bronchotomy and removal of the tumor. One month after the operation a further ventilation-perfusion lung scan revealed complete restoration of ventilation to the left lung and almost complete recovery of the perfusion. This unusual case demonstrates the marked effi ciency of hypoxic pulmonary vasoconstriction at the level of a single lung and its reversible nature following relief of regional hypoxia.
Key Words: Bronchotomy, carcinoid, hypoxic pulmonary vasoconstriction, ventilation-perfusion lung scan
Access this article online
Quick Response Code:Website: www.pulmonarycirculation.org
DOI: 10.4103/2045-8932.78098
Pulm Circ 2011;1:119-21
Address correspondence to:Prof. Nicholas W. Morrell,Department of Medicine, University of Cambridge School of Clinical Medicine,Box 157, Addenbrooke’s Hospital,Hills Road, Cambridge CB2 0QQ, United Kingdom.E-mail: [email protected]
INTRODUCTION
The first systematic description of hypoxic pulmonary vasoconstriction is widely attributed to von Euler and Liljestrand.[1] These investigators were also the first to suggest that this phenomenon serves to protect individuals from systemic hypoxemia by reducing venous admixture from poorly ventilated regions of the lung. The efficiency of hypoxic vasoconstriction varies between species and between individuals.[2-4] In populations residing for generations at a high altitude, where excessive hypoxic pulmonary vasoconstriction would be detrimental, the response is often minimal. In addition, the magnitude of the response has been reported to be greater in small lung regions and weaker if a larger proportion of the lung is hypoxic.[2] Most experimental reports of the efficiency of hypoxic pulmonary vasoconstriction in Man have been necessarily limited to a time course of minutes in normal subjects.[4,5] Here we report an unusual clinical case that
demonstrates almost complete, reversible, redistribution of blood flow in an entire lung.
CASE REPORT
A 50-year-old Caucasian female presented to the Accident and Emergency Department for evaluation of acutely worsening breathlessness of seven days’ duration, with a background of chronic shortness of breath for the past few weeks. Her primary care practitioner had initiated an inhaled beta-2-receptor agonist, because of suspected asthma, with no benefit. She also felt more breathless when lying on her left side associated with mild chest discomfort. On chest auscultation she was noted to have reduced breath sounds in the left hemithorax, but her presenting chest radiograph was normal [Figure 1a].
Case Repor t

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 120
She had never smoked. She denied any significant family history. Vital signs were within normal limits and oxygen saturations were greater than 95%. Initial investigations, including full blood count and electrolytes, were normal. Although, when rising from the examination couch, she suddenly complained of severe shortness of breath and chest pain, with oxygen saturations falling to 89%. An urgent ventilation-perfusion (VQ) lung scintigram was arranged to exclude pulmonary embolism. The VQ scan showed complete absence of ventilation and perfusion to the left lung [Figure 1b and c].
In view of the striking findings on the VQ scan an urgent computed tomographic (CT) scan of the chest was performed, which revealed a mass obstructing the left main bronchus close to the origin. There was no evidence of atelectasis on the CT. Bronchoscopy was undertaken the following day, which confirmed the CT findings and
identified a fleshy mass almost completely occluding the lumen of the left main bronchus. Biopsies were taken, histology of which were consistent with a bronchial carcinoid tumor.
Two hours after bronchoscopy she became more breathless and her oxygen saturation fell to 85%. A repeat chest radiograph now showed complete collapse of the left lung. She was referred to Papworth Hospital for urgent thoracic surgical assessment. It was decided that the carcinoid tumor was amenable to resection by bronchotomy, involving removal of a segment of the left main bronchus involved with the tumor. This procedure preserved the distal lung without need for pneumonectomy. The operation was successful with complete resection of the tumor and re-expansion of the atelectatic lung. She made an uneventful recovery from surgery.
Jafri, et al.: Hypoxic vasoconstriction
Figure 1: Chest radiograph (a) anterior perfusion and (b) ventilation; (c) lung scintigrams demonstrating loss of ventilation and perfusion to the left lung at initial presentation
Figure 2: Chest radiograph (a) anterior perfusion and (b) ventilation; (c) lung scintigrams demonstrating restoration of ventilation and perfusion to the left lung one month following surgery

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 121
One month later she attended for follow-up and was virtually symptom-free. A repeat chest radiograph [Figure 2a] showed the presence of surgical staples at the site of bronchial anastomosis, but otherwise normal lung fields. A repeat VQ scan showed almost complete recovery of ventilation and perfusion to the left lung [Figure 2b and c].
DISCUSSION
The case we describe is unusual in that the patient presented initially with almost complete obstruction of the left main bronchus due to an endobronchial carcinoid tumor, but without associated atelectasis. Atelectasis occurs when the ventilation-perfusion ratio falls to a level at which the rate of gas removal by the blood flow exceeds the rate of gas entering the obstructed lung.[6] Our patient must have had a critically low ventilation-perfusion ratio in the left lung at presentation with an alveolar PO2 that would have approximated mixed venous PO2. This would have provided the stimulus for hypoxic pulmonary vasoconstriction. Although we do not know how long this situation has been present — as a carcinoid is a slow growing tumor — it is likely that the hypoxic stimulus may have been present for some weeks. One can expect a degree of chronic hypoxic vascular remodeling to have occurred under these circumstances. The efficiency of hypoxic pulmonary vasoconstriction can be judged from the lung scintigrams to be nearly complete, in that there has been an almost complete absence of perfusion to the left lung and her peripheral oxygen saturation has been initially measured at greater than 95%. In the absence of this response she may have suffered marked systemic hypoxemia.
Following bronchoscopy and biopsy the obstruction of air flow to the left lung was further compromised and atelectasis occurred, prompting surgical referral and intervention.
At a follow-up one month after surgery the repeat lung scintigram revealed matched restoration of ventilation and blood flow to the left lung. Thus, despite a period of several weeks of hypoxic pulmonary vasoconstriction, probably associated with some chronic pulmonary vascular remodeling, the relief of alveolar hypoxia allowed restoration of blood flow to the left lung. Reversal of both acute and chronic hypoxic vasoconstriction and remodeling is reported in animal models, but rarely observed in clinical practice.
REFERENCES
1. Von Euler US, Liljestrand G. Observations on the pulmonary aterial blood pressure in the cat. Acta Physiol Scand. 1946;12:301-20.
2. Marshall BE, Marshall C, Benumof J, Saidman LJ. Hypoxic pulmonary vasoconstriction in dogs: Eff ects of lung segment size and oxygen tension. J Appl Physiol. 1981;51:1543-51.
3. Barer GR, Howard P, Shaw JW. Stimulus-response curves for the pulmonary vascular bed to hypoxia and hypercapnia. J Physiol. 1970;211:139-55.
4. Morrell NW, Nij ran KS, Biggs T, Seed WA. Magnitude and time course of acute hypoxic pulmonary vasoconstriction in man. Respir Physiol. 1995;100:271-81.
5. Morrell NW, Nij ran KS, Biggs T, Seed WA. Changes in regional pulmonary blood fl ow during lobar bronchial occlusion in man. Clin Sci (Lond). 1994;86:639-44.
6. Dantzker DR, Wagner P.D., West J.B. Instability of lung units with low V/Q ratios during oxygen breathing. J Appl Physiol. 1975;38:886-95.
Source of Support: None declared. Confl ict of Interest: None declared.
Jafri, et al.: Hypoxic vasoconstriction
Author Help: Reference checking facility
The manuscript system (www.journalonweb.com) allows the authors to check and verify the accuracy and style of references. The tool checks the references with PubMed as per a predefined style. Authors are encouraged to use this facility, before submitting articles to the journal.
• The style as well as bibliographic elements should be 100% accurate, to help get the references verified from the system. Even a single spelling error or addition of issue number/month of publication will lead to an error when verifying the reference.
• Example of a correct style Sheahan P, O’leary G, Lee G, Fitzgibbon J. Cystic cervical metastases: Incidence and diagnosis using fine needle aspiration biopsy.
Otolaryngol Head Neck Surg 2002;127:294-8. • Only the references from journals indexed in PubMed will be checked. • Enter each reference in new line, without a serial number.• Add up to a maximum of 15 references at a time.• If the reference is correct for its bibliographic elements and punctuations, it will be shown as CORRECT and a link to the correct
article in PubMed will be given.• If any of the bibliographic elements are missing, incorrect or extra (such as issue number), it will be shown as INCORRECT and link to
possible articles in PubMed will be given.

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 122
Snapshot
PULMONARY ARTERIAL HYPERTENSION DIAGNOSTIC ALGORITHM
Pulmonary hypertension (PH) is defined as a mean pulmonary artery pressure (mPAP) ≥25 mmHg, irrespective of etiology. In contrast to PH, the definition of pulmonary arterial hypertension (PAH) requires the exclusion of elevated pulmonary venous pressure, an established cause of PH, as reflected by a normal wedge pressure or left ventricular end-diastolic pressure (LVEDP) (≤15 mmHg). If PH is suspected in a patient, suitable screening tests are conducted to confirm the presence of PH and delineate the etiology to appropriately tailor an optimal therapeutic regimen. The diagnostic algorithm [Figure 1] reflects an integration of assessment pathways that help differentiate patients with WHO groups II–IV of pulmonary hypertension from WHO group I PAH as well as the subgroups of PAH. Caution is advised to apply the algorithm to any individual patient as the evaluation process of any patient with suspected PH requires a variety of investigations intended to confirm PH and the specific PAH subtype and, once confirmed, evaluate the functional and hemodynamic impairments of those patients. Right heart catheterization is universally considered to be an indispensable part of the diagnostic assessment.
PAH RX ALGORITHM
The treatment algorithm is based on a consensus of the PH community based on the majority of randomized controlled clinical trials (RCTs) for PAH. The grading system is based on the recently published consensus
for these drug trials.[1] Additionally, most trials were conducted in idiopathic or heritable PAH and PAH associated with scleroderma or anorexigen use; hence, the therapeutic effect on other PAH subpopulations may not be equal. Although there are no RCTs to substantiate the use of the following therapies, oral anticoagulation, diuretics in cases of fluid retention and supplemental oxygen in cases of hypoxemia (oxygen saturation <92%) are still considered the first line of treatment in patients with PAH. Acute vasoreactivity testing should be performed in all patients with PAH. Vasoreactivity is defined as reduction of mPAP ≥10 mmHg to reach an mPAP ≤40 mmHg with a normalized or increased cardiac output with acute pulmonary vasodilator challenge (either inhaled nitric oxide, adenosine or intravenous epoprostenol). Vasoreactive patients should be treated with high-dose calcium channel blockers with maintenance of response, defined as WHO functional class I or II with near-normal hemodynamic status, being confirmed by repeat right heart catheterization and clinical assessment after 3–6 months of treatment. Non-responders to acute vasoreactivity testing are defined both hemodynamically as well as by functional class II–IV, and should be considered candidates for other treatments as shown in Figure 2. The choice of the agent is dependent on a variety of factors, including route of administration, side-effect profile, patient preference and the physician's experience and clinical judgment. Continuous IV epoprostenol is the first-line therapy for IPAH and HPAH patients in WHO functional class IV because of its demonstrated survival benefit. Combination therapy should be considered for patients who fail monotherapy.
Diagnostic and therapeutic algorithm for pulmonary arterial hypertension
Ankit A. Desai1, Roberto F. Machado1
1Department of Medicine (Section of Pulmonary, Critical Care, Sleep and Allergy Medicine and Section of Cardiology), Institute for Personalized Respiratory Medicine, University of Illinois, Chicago, Illinois, USA
Access this article online
Quick Response Code:Website: www.pulmonarycirculation.org
DOI: 10.4103/2045-8932.78096
Pulm Circ 2011;1:122-4
Address correspondence to:Dr. Ankit A. DesaiDepartment of Medicine, University of IllinoisCOMRB 3128 (MC 719), 909 South Wolcott Avenue, Chicago, Illinois 60612, USAEmail: [email protected]

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 123
Figure 2: PAH treatment algorithm. (PAH - Pulmonary arterial hypertension; FC - Functional class; ERA - Endothelin receptor antagonist; PDE-I - Phosphodiesterase type 5 inhibitor; IV - Intravenous; PO - Oral; SC - Subcutaneous; NA - Not approved; WHO - World Health Organization; PAP - Pulmonary arterial pressure; RCT - Randomized controlled trial. Strength of recommendation: A - Strong recommendation; B - Moderate recommendation; C - Weak recommendation; D - Negative recommendation; E/A - Strong recommendation on the basis of expert opinion only; E/B - Moderate recommendation on the basis of expert opinion only; E/C - Weak recommendation on the basis of expert opinion only; E/D - Negative recommendation on the basis of expert opinion only)
Desai and Machado: Diagnostic and therapeutic algorithms for PAH
Figure 1: PAH diagnostic algorithm. (ABG - Arterial blood gas; ALK-1 - Activin-receptor-like kinase; ANA - Anti-nuclear antibodies; BMPR2 - Bone morphogenetic protein receptor 2; CHD - Congenital heart disease; CMR - Cardiac magnetic resonance; CT - Computed tomography; CTD - Connective tissue disease; ECG - Electrocardiogram; FMHx - Family medical history; HHT - Hereditary hemorrhagic telangiectasia; HRCT - High-resolution computed tomography; LFTs - Liver function tests; LH - Left heart; PAP - Pulmonary arterial pressure; LVEDP - Left ventricular end-diastolic pressure; PAH - Pulmonary arterial hypertension; IPAH - Idiopathic pulmonary arterial hypertension; PCH - Pulmonary capillary hemangiomatosis; PE - Pulmonary thromboembolic disease; PFT - Pulmonary function test; PH - Pulmonary hypertension; PVOD - Pulmonary veno-occlusive disease; RHC - Right heart catheterization; TEE - Transesophageal echocardiography; TTE - Transthoracic echocardiography; US - Ultrasonography; V/Q - Ventilation/perfusion lung scan; WHO - World Health Organization)
REFERENCES
1. Barst RJ, Gibbs JS, Ghofrani HA, Hoeper MM, McLaughlin VV, Rubin LJ,
et al. Updated evidence-based treatment algorithm in pulmonary arterial hypertension. J Am Coll Cardiol 2009;54:78-84.
2. Rich S, Kaufmann E, Levy PS. The eff ect of high doses of calcium-channel blockers on survival in primary pulmonary hypertension. N Engl J Med

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 124
Desai and Machado: Diagnostic and therapeutic algorithms for PAH
1992;327:76-81. 3. Rich S, Brundage BH. High-dose calcium channel-blocking therapy for
primary pulmonary hypertension: evidence for long-term reduction in pulmonary arterial pressure and regression of right ventricular hypertrophy. Circulation 1987;76:135-41.
4. Raff y O, Azarian R, Brenot F, Parent F, Sitbon O, Petitpretz P, et al. Clinical signifi cance of the pulmonary vasodilator response during short-term infusion of prostacyclin in primary pulmonary hypertension. Circulation 1996;93:484-8.
5. Barst RJ, Maislin G, Fishman AP. Vasodilator therapy for primary pulmonary hypertension in children. Circulation 1999;99:1197-208.
6. Sitbon O, Humbert M, Jaïs X, Ioos V, Hamid AM, Provencher S, et al. Long-term response to calcium channel blockers in idiopathic pulmonary arterial hypertension. Circulation 2005;111:3105-11.
7. Yung D, Widlitz AC, Rosenzweig EB, Kerstein D, Maislin G, Barst RJ. Outcomes in children with idiopathic pulmonary arterial hypertension. Circulation 2004;110:660-5.
8. Rich S, Seidlitz M, Dodin E, Osimani D, Judd D, Genthner D, et al. The short-term eff ects of digoxin in patients with right ventricular dysfunction from pulmonary hypertension. Chest 1998;114:787-92.
9. Fuster V, Steele PM, Edwards WD, Gersh BJ, McGoon MD, Frye RL. Primary pulmonary hypertension: natural history and the importance of thrombosis. Circulation 1984;70:580-7.
10. Frank H, Mlczoch J, Huber K, Schuster E, Gurtner HP, Kneussl M. The eff ect of anticoagulant therapy in primary and anorectic drug-induced pulmonary hypertension. Chest 1997;112:714-21.
11. Johnson SR, Mehta S, Granton JT. Anticoagulation in pulmonary arterial hypertension: a qualitative systematic review. Eur Respir J 2006;28:999-1004.
12. Channick RN, Simonneau G, Sitbon O, Robbins IM, Frost A, Tapson VF, Eff ects of the dual endothelin-receptor antagonist bosentan in patients with pulmonary hypertension: a randomised placebo-controlled study. Lancet 2001;358:1119-23.
13. Rubin LJ, Badesch DB, Barst RJ, Galie N, Black CM, Keogh A, et al. Bosentan therapy for pulmonary arterial hypertension. N Engl J Med 2002;346:896-903.
14. Galiè N, Beghett i M, Gatzoulis MA, Granton J, Berger RM, Lauer A, et al. Bosentan therapy in patients with Eisenmenger syndrome: a multicenter, double-blind, randomized, placebo-controlled study. Circulation 2006;144:48-54.
15. Galiè N, Rubin Lj, Hoeper M, Jansa P, Al-Hiti H, Meyer G, et al. Treatment of patients with mildly symptomatic pulmonary arterial hypertension with bosentan (EARLY study): a double-blind, randomised controlled trial. Lancet 2008;371:2093-100.
16. Galiè N, Brundage BH, Ghofrani HA, Oudiz RJ, Simonneau G, Safdar Z, et al. Tadalafi l therapy for pulmonary arterial hypertension. Circulation 2009;119:2894-903.
17. Galiè N, Hinderliter AL, Torbicki A, Fourme T, Simonneau G, Pulido T, et al. Eff ects of the oral endothelin-receptor antagonist bosentan on echocardiographic and doppler measures in patients with pulmonary arterial hypertension. J Am Coll Cardiol 2003;41:1380-6.
18 Galiè N, Olschewski H, Oudiz RJ, Torres F, Frost A, Ghofrani HA, et al. Ambrisentan for the treatment of pulmonary arterial hypertension: results of the ambrisentan in pulmonary arterial hypertension, randomized, double-blind, placebo-controlled, multicenter, effi cacy (ARIES) study 1 and 2. Circulation 2008;117:3010-9.
19. Galié N, Badesch D, Oudiz R, Simonneau G, McGoon MD, Keogh AM, et al. Ambrisentan therapy for pulmonary arterial hypertension. J Am Coll Cardiol 2005;46:529-35.
20. Oudiz RJ, Galiè N, Olschewski H, Torres F, Frost A, Ghofrani HA, et al. Long-term ambrisentan therapy for the treatment of pulmonary arterial hypertension. J Am Coll Cardiol 2009;54:1971-81.
21. Galiè N, Ghofrani HA, Torbicki A, Barst RJ, Rubin LJ, Badesch D, et al. Sildenafi l citrate therapy for pulmonary arterial hypertension. N Engl J Med 2005;353:2148-57.
22. Galiè N, Humbert M, Vachiéry JL, Vizza CD, Kneussl M, Manes A, et al.
Eff ects of beraprost sodium, an oral prostacyclin analogue, in patients with pulmonary arterial hypertension: a randomized, double-blind, placebo-controlled trial. J Am Coll Cardiol 2002;39:1496-502.
23. Barst RJ, McGoon M, McLaughlin V, Tapson V, Rich S, Rubin L, et al. Beraprost therapy for pulmonary arterial hypertension. J Am Coll Cardiol 2003;41:2119-25.
24. Olschewski H, Simonneau G, Galiè N, Higenbott am T, Naeij e R, Rubin LJ, et al. Inhaled iloprost for severe pulmonary hypertension. N Engl J Med 2002;347:322-9.
25. McLaughlin VV, Benza RL, Rubin LJ, Channick RN, Voswinckel R, Tapson VF, et al. Addition of inhaled treprostinil to oral therapy for pulmonary arterial hypertension: a randomized controlled clinical trial. J Am Coll Cardiol 2010;55:915-22.
26. Higenbott am TW, Butt AY, Dinh-Xaun AT, Takao M, Cremona G, Akamine S. Treatment of pulmonary hypertension with the continuous infusion of a prostacyclin analogue, iloprost. Heart 1998;79:175-9.
27. Rubin LJ, Mendoza J, Hood M, McGoon M, Barst R, Williams WB, et al. Treatment of primary pulmonary hypertension with continuous intravenous prostacyclin (epoprostenol). Results of a randomized trial. Ann Intern Med 1990;112:485-91.
28. Barst RJ, Rubin LJ, Long WA, McGoon MD, Rich S, Badesch DB, et al. A comparison of continuous intravenous epoprostenol (prostacyclin) with conventional therapy for primary pulmonary hypertension. The Primary Pulmonary Hypertension Study Group. N Engl J Med 1996;334:296-301.
29. Tapson VF, Gomberg-Maitland M, McLaughlin VV, Benza RL, Widlitz AC, Krichman A, et al. Safety and effi cacy of IV treprostinil for pulmonary arterial hypertension: a prospective, multicenter, open-label, 12-week trial. Chest 2006;129:683-8.
30. Gomberg-Maitland M, Tapson VF, Benza RL, McLaughlin VV, Krichman A, Widlitz AC, et al. Transition from intravenous epoprostenol to intravenous treprostinil in pulmonary hypertension. Am J Respir Crit Care Med 2005;172:1586-9.
31. Simonneau G, Barst RJ, Galie N, Naeij e R, Rich S, Bourge RC, et al. Continuous subcutaneous infusion of treprostinil, a prostacyclin analogue, in patients with pulmonary arterial hypertension: a double-blind, randomized, placebo-controlled trial. Am J Respir Crit Care Med 2002;165:800-4.
32. McLaughlin VV, Gaine SP, Barst RJ, Oudiz RJ, Bourge RC, Frost A, et al. Effi cacy and safety of treprostinil: an epoprostenol analog for primary pulmonary hypertension. J Cardiovasc Pharmacol 2003;41:293-9.
33. McLaughlin VV, Benza RL, Rubin LJ, Channick RN, Voswinckel R, Tapson VF, et al. Addition of inhaled treprostinil to oral therapy for pulmonary arterial hypertension: a randomized controlled clinical trial. J Am Coll Cardiol 2010;55:1915-22.
34. Simonneau G, Rubin LJ, Galiè N, Barst RJ, Fleming TR, Frost AE, et al. Addition of sildenafi l to long-term intravenous epoprostenol therapy in patients with pulmonary arterial hypertension: a randomized trial. Ann Intern Med 2008;149:521-30.
35. Humbert M, Barst RJ, Robbins IM, Channick RN, Galiè N, Boonstra A, et al. Combination of bosentan with epoprostenol in pulmonary arterial hypertension: BREATHE-2. Eur Respir J 2004;24:353-9.
36. Hoeper MM, Leuchte H, Halank M, Wilkens H, Meyer FJ, Seyfarth HJ, et al. Combining inhaled iloprost with bosentan in patients with idiopathic pulmonary arterial hypertension. Eur Respir J2006;28:691-4.
37. McLaughlin VV, Oudiz RJ, Frost A, Tapson VF, Murali S, Channick RN, et al. Randomized study of adding inhaled iloprost to existing bosentan in pulmonary arterial hypertension. Am J Respir Crit Care Med 2006;174:1257-63.
38. McLaughlin VV, Benza RL, Rubin LJ, Channick RN, Voswinckel R, Tapson VF, et al. Addition of inhaled treprostinil to oral therapy for pulmonary arterial hypertension: a randomized controlled clinical trial. J Am Coll Cardiol 2010;55:1915-22.
Source of Support: NIH grant (HL098454), Confl ict of Interest: None declared.

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 125
Announcement
The PVM History Initiative of the PVRI
“Declare the past, diagnose the present, foretell the future.”
—The Father of Medicine himself, Hippocrates (460-357 BC), who gave us the Hippocratic Oath
While the Pulmonary Vascular Research Institute (PVRI) has always been, and remains, dedicated to the cutting-edge present and future of our field, I am proud to announce a new History Initiative that will also recognize the long and amazing past of pulmonary vascular medicine (PVM).
As our understanding of PVM increases by leaps and bounds in this Information Age, it becomes ever more important to increase our understanding and appreciation of our field all the way back to the legendary Shen Nung, the Father of Chinese Medicine, who lived c. 2800 BC, or roughly two millennia before Hippocrates.
Pulmonary vascular medicine is of course of relevance to all people everywhere, and the critical advances in our field have occurred in all lands. The intent of our PVRI History Initiative is not merely to compile names and dates and chronologies of achievement, it is also to glean nuggets of wisdom with which all of us might enrich our present and our future. Here are its seven key features and functions.1. Maintain a History Initiative website where scientists
and scholars of PVM can share information, interact with each other, and contribute original articles.
2. Encourage research projects on the history of PVM. This includes our establishment of a Research Fellowship for the history of pulmonary hypertension and pulmonary vascular medicine.
3. Reprint milestone historical articles and books that played an important role in the development of our current concept and understanding of PVM. These publications will include authentic papers with commentary detailing their value in the research, diagnosis and treatment of pulmonary hypertension.
4. Presenting history in terms of individuals with whom people can identify, as opposed to relating it in terms of huge impersonal events, makes it more human and easier to grasp. So we will establish a “Who’s Who in Pulmonary Vascular Medicine®,” a biographical index or database of people past and present who increased
or enhanced our knowledge and understanding of PVM. Each biography of 500-2,000 words will include the person’s life highlights, main achievements and milestones, and major publications. This biographical index will be hosted on the PVRI website’s special historical section, while selected articles from it will be published in Pulmonary Circulation.
5. Commission and encourage the writing of biographies and autobiographies of PVM scientists living and deceased. Where possible, this will include interviewing scientists about their careers and achievements, as well as their reflections and predictions.
6. Establish a new image archive of historical artifacts or objects relating to PVM. This includes images, graphs, diagrams, instruments, and any other materials that have been used to increase our understanding of PVM. For this image archive, we are looking for images with commentary and references.
7. Regularly publish original articles and biographies in a special section of our quarterly journal, Pulmonary Circulation. In the next issue, Vol. 1, No. 2, we will feature a paper on the discovery of the pulmonary circulation by Ibn al-Nafis, who accurately described the pulmonary circulation in the 13th Century, daring to correct Galen’s earlier error. This will be followed in subsequent issues by papers on such 16th-Century physicians as Michael Servetus, Realdus Columbus, and others (Figure 1).
Whether you are an established or younger scientist working in PVM today, or a professional in the History of Medicine, we welcome your research or review articles on the ancient and modern history of pulmonary vascular medicine.
We also invite you to discuss this project with us, welcome your comments, and sincerely hope you will join us as both a frequent contributor and a regular reader of our History Initiative.
Ghazwan Butrous, Managing Director, PVRI
Senior Editor, Pulmonary CirculationE-mail:[email protected]

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 126
Butrous: History Initiative
Figure 1: The main players in the description of pulmonary circulation from antiquity till the end of the 17th Century (solid arrows represent direct infl uence, dotted arrows represent doubtful or partial infl uence).
“As our understanding of PVM increases by leaps and bounds in this Information Age, it becomes ever more important to increase our
understanding and appreciation of our field all the way back to the legendary Shen Nung, the Father of Chinese Medicine, who lived c. 2800 BC,
or roughly two millennia before Hippocrates.”
—Ghazwan Butrous
“When hearing something unusual, do not preemptively reject it, for that would be folly. Indeed, horrible things may be true, and familiar and praised things may prove to be lies. Truth is truth unto itself, not because crowds of people say it is truth.”
—Ibn al-Nafis (1210-1288), in his Sharh’ al Qanun

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 127
articles to letters to the editor - from clinicians, clinical scientists, investigators, and any other professional working in the pulmonary circulation, pulmonary vascular medicine, or pulmonary vascular disease.
Authorship criteriaAuthorship should be based on substantial contributions to each of these 3 components: concept and design of study or acquisition of data or analysis and interpretation of data; crafting the article or revising it critically for important intellectual content; and final approval of the version to be published.
Participation solely in the acquisition of funding or the collection of data does not justify authorship. General supervision of the research group is not sufficient for authorship. Each contributor should have participated sufficiently in the work to take public responsibility for appropriate portions of the content of the manuscript.
The order of naming the contributors should be based on the relative contribution of each contributor toward the study and the writing of the manuscript. Once submitted, the order cannot be changed without the written consent of all the contributors.
The Journal does not require the publication in its articles of statements of who did what during the preparation of a multiple-author article. For such articles, the authors may make special mention of particular authors’ efforts in the article’s Acknowledgments.
The corresponding authorTeams of authors must nominate one individual to be the Corresponding Author who first communicates with the Journal’s editorial office for all matters related to the manuscript (especially any revisions and final approval of the proof pages [“galley proofs”]), and who thereafter will field reader inquiries (his or her name, mailing address and email address having been published on the first page of the article).
Contribution Components Defined
*Components added by Journal staff from information provided by authors
AbstractA succinct description of the article’s main points.
*Access this article online (box)Created by the editors, not the authors.
AcknowledgementsIn this optional section you may specify: contributions that need acknowledging but do not justify authorship, such as general support by a departmental chair or individuals who helped collect blood samples and tissue specimen; contributions of technical help; and contributions of financial and material support, which should specify the nature of the support. If the manuscript was presented as part at a meeting, then the organization, place and exact date on which it was presented should be included.
Affiliations. Institutions of the authors (e.g., universities, research institutes), named beneath the by-line, identified by superscripted numbers.
*Article typeThe word or words identifying a contribution above and to the left of the title, where appropriate (e.g., for articles, not for letters to the editor—all defined below in “Your Contribution Type”).
By-lineThe authors’ names—without the word “by.”
CaptionsSometimes called legends, these are the lines of text beneath a figure describing the figure. If a figure came from an existing source, then the caption must end with this parenthetical statement: “(Adapted from [source]),” as in: “(Adapted from ref. 53)”
ConclusionsThe significance of your findings.
*Correspondence (box)The name, physical mailing address, and email address of the individual authorized by all the authors of the manuscript to communicate with the Journal’s editorial office for all matters related to the manuscript, and to receive communications from readers of the Journal.
Contributions to Pulmonary Circulation
General Comments
Identity and naturePulmonary Circulation (ISSN 2045-8932, E-ISSN 2045-8940) is a peer-reviewed international quarterly journal, with editorial offices in Chicago USA, Trivandrum India, Cambridge UK, and London UK, and with contributing editors and editorial board members from more than 20 countries. Each quarter’s issue is published in the last week of the previous quarter. Each issue’s full text is available online (www.pulmonarycirculation.org).
FocusPulmonary Circulation is designed to be the main communicating medium connecting clinicians and researchers who are interested in the pulmonary circulation and pulmonary vascular disease. It is expected to serve the interests of people in all parts of the world.
AffiliationThe Journal is a publication of the Pulmonary Vascular Research Institute (PVRI), an independent international medical research organization devoted to increasing awareness and knowledge of pulmonary vascular disease (www.pvri.info).
IndexingPulmonary Circulation is indexed/listed with Caspur, DOAJ, EBSCO Publishing’s Electronic Databases, Expanded Academic ASAP, Genamics JournalSeek, Google Scholar, Hinari, Index Copernicus, OpenJGate, PrimoCentral, ProQuest, SCOLOAR, SIIC databases, Summon by Serial Solutions and Ulrich’s International Periodical Directory
FeesPulmonary Circulation charges authors no fee of any kind, neither for submission nor for processing or publication of manuscripts, nor even for the reproduction of color photographs.
CopyrightWhile other journals require authors to transfer copyright ownership of their articles to them, Pulmonary Circulation follows the modern trend of open-access journals to allow authors to retain ownership of their own articles, as specified by the ICMJE (International Committee of Medical Journal Editors). To ensure originality, we merely require authors to assign us First Serial Rights (first publication in a periodical); and we ask only that for any subsequent publication of their articles (as in an anthology or a textbook) the following parenthetical statement appear at the end of it: “(This article was first published in Pulmonary Circulation, volume, number [year] pages.)”
AccessThe Journal allows free access (open access) to its contents and permits authors to self-archive the final accepted version of articles on any OAI-compliant institutional/subject-based repository. To achieve faster and greater dissemination of knowledge and information, the Journal publishes articles online as “Ahead of Print” immediately on acceptance.
ReprintsPulmonary Circulation provides no free reprints. Reprints may be purchased directly from Medknow, the world’s largest publisher of open-access journals (www.medknow.com).
LanguagesThe Journal is published in English, and there are simultaneous editions (both hard copies and online) in other languages.
For precision in key-word searches online, and as a matter of stylistic consistency, the Journal editors use American English.• Spellings and words, for example: “pediatrics” rather than “paediatrics,”
“caption” rather than “legend,” and (conceivably) “hood and trunk” rather than “bonnet and boot.”
• Punctuation, for example: “sample,” rather than ‘sample’,
Details of how to compose your manuscript in American English automatically are provided in “The Writing Process,” below.
Author Requirements
Author perspectivesPulmonary Circulation welcomes all contributions - from original research
Inst ruct ions for Authors

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 128
DiscussionDiscussion of your findings or results—the body of the article.
FiguresWith the exception of tables, “figures” are all non-text components of a manuscript—graphs, photographs, line drawings, etc. (Specifications for figures are given below in “The Manuscript Preparation Process.”)
Footnotes Used only in tables to define symbols.
IntroductionPreliminary remarks to introduce the article’s major subjects and rationale.
Key words3-5 words that describe the content of the manuscript but that are not included in the title of the manuscript.
Materials and methodsDescription of any materials or methods you used which a researcher would need to know in order to duplicate your results.
PermissionsPermission to use copyrighted text or trademarked material. Please see “Legal Requirements,” below.
ReferencesThe published sources cited in an article, in the text indicated by a superscripted number, all appearing at the end of the article in the order in which the article cited them (not alphabetically by author names). Pulmonary Circulation employs the same format of reference citation as The New England Journal of Medicine.
ResultsYour findings.
Running head (a.k.a. Running headline)The line that appears as a header for each page of an article after the first page, identifying the article with condensed versions of its authors and its titles. (Detailed below in “The Manuscript Preparation Process.”)
Sources of support, conflicts of interestDisclosures of any funding sources and potential conflicts of interest. Please see “Legal Requirements,” below.
TableA boxed arrangement of data, usually in columns and rows, each table with its own title, its own caption, and, if necessary, its own footnotes to explain any symbols used in the table. Tables with more than 10 columns and/or 25 rows may not be accepted.
TitleThe descriptive name of an article. (Detailed below in “The Manuscript Preparation Process.”
Your Contribution
Letter to the editorDescriptionLetters to the Editor pertain directly to an article published in the journal within the preceding 8 weeks. Authors of the original article cited in the letter will be invited to reply. Letters to the Editor should be submitted via the online manuscript submission process described below.
Suggested length300 words
ComponentsText only
Guest editorialDescriptionAn informal (“plain English”) statement of opinions or a position on an issue relevant to Pulmonary Circulation readers, by a Journal reader or readers.
Suggested length500 words
ComponentsText only
EditorialDescription An informal (“plain English”) statement of opinions or a position on an issue relevant to Pulmonary Circulation readers, by a Journal editor or editorial board member.
Suggested length500 words
ComponentsText only
Editor’s HighlightDescriptionA Journal editor’s “behind the scenes” or “sneak preview” focus on a particular topic
Suggested length1,000 words
ComponentsText, possibly with figures
Special ReportDescriptionA short clinical research paper describing the observations from a small cohort of patients.
Suggested length1,500 words
ComponentsKey Words, text (including a brief Abstract, background and rationale, brief description of methodology, Results, and Discussion); up to 20 references; figures and tables
Case ReportDescriptionNew, interesting and rare cases can be reported. They should be unique, describing a great diagnostic or therapeutic challenge and providing a learning point for the readers. Cases with clinical significance or implications will be given priority.
Suggested lengthUp to 1,500 words (excluding Abstract and References)
ComponentsAbstract, Key Words, Introduction, Discussion, Reference (no more than 10), ideally with tables and figures
Field ReportDescriptionA clinical article that could be described by any of these titles: Guidelines and Consensus, Clinical Trials, Clinical Debates, Personal Perspectives, Clinical Practice,
Suggested length1,500 words
ComponentsAs necessitated by the article’s contents
Review ArticleDescriptionA comprehensive review on a topic related to the pulmonary circulation and/or pulmonary vascular disease. Review articles usually are invited by the editors; but unsolicited manuscripts will also be considered for publication. It is expected that these articles will be written by individuals who have done substantial work on the subject or are considered experts in the field.
Suggested lengthUp to 15,000 words excluding Abstract, figure captions, tables, and References
ComponentsAbstract, Introduction, Discussion (text), Conclusions (including future directions), References (up to 200), figures (ideally 3-8 schematic diagrams, color images, flow charts, etc.), and tables
Contributions to Pulmonary Circulation

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 129
Original Research ArticleDescriptionPulmonary Circulation considers all types of original research articles including clinical and basic research conducted in human subjects and laboratory animals and in vitro, randomized controlled trials, intervention studies, studies of screening and diagnostic tests, outcome studies, cost effectiveness analyses, case-control series, and surveys with high response rates.
Suggested lengthUp to 6,000 words
ComponentsAbstract, Key Words, Introduction, Materials and Methods, Results, Discussion, References, figures and tables
Study design for an original design articleSelection and Description of Participants: Clearly describe your selection of the observational or experimental participants (patients or laboratory animals, including controls), including eligibility and exclusion criteria and a description of the source population.
Technical informationIdentify the methods, apparatus (give the manufacturer’s name and address in parentheses), and procedures in sufficient detail to allow other workers to reproduce the results. Give references to established methods, including statistical methods (see below); provide references and brief descriptions for methods that have been published but are not well known; describe new or substantially modified methods, give reasons for using them, and evaluate their limitations. Identify precisely all drugs and chemicals used, including generic name(s), dose(s), and route(s) of administration.
Reports of randomized clinical trials should present information on all major study elements, including the protocol, assignment of interventions (methods of randomization, concealment of allocation to treatment groups), and the method of masking (blinding), based on the CONSORT Statement (www.consort-statement.org).
Reporting guidelines for specific study designs
Initiative Type of Study Source
Consort randomized controlled trials
http://www.consort-statement.org
Stard studies of diagnostic accuracy
http://www.consort-statement.org/stardstatement.htm
Quorom systematic reviews and meta-analyses
http://www.consort-statement.org/Initiatives/MOOSE/moose.pdf
Strobe observational studies in epidemiology
http://www.strobe-statement.org
Moose meta-analyses of observational studies in epidemiology
http://www.consort-statement.org/Initiatives/MOOSE/moose.pdf
StatisticsWhenever possible quantify findings and present them with appropriate indicators of measurement error or uncertainty (such as confidence intervals). Authors should report losses to observation (such as, dropouts from a clinical trial). When data are summarized in the Results section, specify the statistical methods used to analyze them. Avoid non-technical uses of technical terms in statistics, such as “random” (which implies a randomizing device), “normal,” “significant,” “correlation,” and “sample.” Define statistical terms, abbreviations, and most symbols. Specify the computer software used. Use upper italics (P=0.048). For all P values include the exact value, not less than 0.05 or 0.001. Mean differences in continuous variables, proportions in categorical variables and relative risks including odds ratios and hazard ratios, should be accompanied by their confidence intervals.
ResultsPresent your results in a logical sequence in the text, tables, and figures, giving the main or most important findings first. Do not repeat in the text all the data in the tables or figures; emphasize or summarize only important
observations. Extra or supplementary materials and technical detail can be placed in an appendix where it will be accessible but will not interrupt the flow of the text; alternatively, it can be published only in the electronic version of the journal.
When data are summarized in the Results section, give numeric results not only as derivatives (for example, percentages) but also as the absolute numbers from which the derivatives were calculated, and specify the statistical methods used to analyze them. Restrict tables and figures to those needed to explain the argument of the paper and to assess its support. Use graphs as an alternative to tables with many entries; do not duplicate data in graphs and tables. Where scientifically appropriate, analyses of the data by variables such as age and sex should be included.
DiscussionInclude summary of key findings (primary outcome measures, secondary outcome measures, results as they relate to a prior hypothesis); strengths and limitations of the study (study question, study design, data collection, analysis and interpretation); interpretation and implications in the context of the totality of evidence (“Is there a systematic review to refer to, if not, could one be reasonably done here and now?” or “What this study adds to the available evidence,” or, “Effects on patient care and health policy, possible mechanisms,” etc.); controversies raised by this study; and future research directions (for this particular research collaboration, underlying mechanisms, or clinical research).
General CommentsDo not repeat in detail data or other material given in the Introduction or the Results section. In particular, contributors should avoid making statements on economic benefits and costs unless their manuscript includes economic data and analyses. Avoid claiming priority and alluding to work that has not been completed. New hypotheses may be stated if needed; however, they should be clearly labeled as such.
The ProcessesThe writing processSince all manuscripts published by Pulmonary Circulation must conform to the latest version of the ICMJE’s (International Committee of Medical Journal Editors) “Uniform Requirements for Manuscripts Submitted to Biomedical Journals” (www.icmje.org), we at Pulmonary Circulation strongly recommend that you write your article according to those requirements (as opposed to first writing it and then checking to see if it conforms).
Please write, or compose, your manuscript in a Word or WordPerfect document that has the settings shown below for Text under “The Manuscript Preparation Process.”
The manuscript preparation processAll submissions must be made online through our website (www.journalonweb.com/pc).
First-time authors will have to register at the website. (Registration is free but mandatory.)
Instructions for submission are also available at the Journal’s website (www.pulmonarycirculation.org).
For “simpler” contributions (i.e., those having no figures or abstracts, such as a letter to the Editor or a guest editorial), you need to prepare only a Manuscript file (described below) to be submitted.
For “full article” contributions, please prepare the required 4 separate files for submission at the same time. (You may certainly send them at different times; but Journal policy specifies that no article is put into production until its 4 files have been received). The 4 are: the MANUSCRIPT file (including all tables and all captions); the FIGURES file (all non-text components other than tables—graphs, photos, color images, illustrations, etc.); the SIGNS file; and the LEGALITIES file.
Your MANUSCRIPT file (“the text file”) [1st of the 4 files to be submitted for an article-type contribution]• The acceptable format is Word.• Maximum file size is 1 MB (.rtf or.doc). • Please do not zip the files, nor use a pdf, and kindly do not incorporate
figures in this file. • Begin with a cover page (a.k.a. title page) showing: the total number of
pages, total number of figures, and word counts for the text (excluding
Contributions to Pulmonary Circulation

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 130
the References, tables and Abstract); type of contribution (original article, case report, review article, clinical trial, letter to editor, etc.); article title and running head (see below); names of all authors (with their highest academic degrees); name(s) of affiliations (department(s) and/or institution(s) to which the work should be credited); criteria for inclusion in the list of authors (please see Authorship Criteria, above.); and the name and contact information of the corresponding author.
• Following your References section, please type the information that Journal staff will put in the little box (Sources of Support and Conflicts of Interest, if any). Your published article will end there, with that little box; however, here in your Manuscript File to be submitted, please follow that (the information to be boxed) with these two things, in this order:
Each actual table with its own title and its own caption; and thenAll figure captions.
Title (of article)Only the first word of your title is capitalized, with 3 exceptions: the word following a colon is capitalized; acronyms are all capital letters; and any word which is always capitalized is capitalized in the title (e.g., “Smith,” “United Kingdom,” etc.).• Table titles follow this same rule.
By-line (the authors’ names—without the word “by”)• Spell out the first name and use an initial with a period for middle name:
“John Q. Public”• 2 authors: use only the word “and”: “Abdul al-Nafis and Mary T. Smith” • 3 or more authors: use commas, and between the last 2 the word “and”
preceded by a comma: “John Q. Public, Abdul al-Nafis, and Mary T. Smith”
Running HeadThe line that appears as a header for each page of an article after the first page, identifying the article with condensed versions of its authors and its titles, usually consisting of not more than 50 characters (including spaces). Example:
Article:
Functional ion channels in human pulmonary artery smooth muscle cells: Voltage-dependent cation channels
Amy L. Firth, Carmelle V. Remillard, Oleksandr Platoshyn, Ivana Fantozzi, Eun A. Ko, and Jason X.-J. Yuan
Running head:
Firth et al.: Ion channels in human PASMC
• Because “et” means “and,” it is not preceded by a comma in the running head.
Text (all word components from Abstract to Conclusions)• Language setting (Tools, Language): English (US).• Document size: US Letter (8.5 x 11).• Font type and size: Times New Roman (or equivalent serif font—not a
sans-serif or “block letter” font like Helvetica or Arial), 11-pt.• Paragraphs: Single-spaced; no paragraph indents; double-space between
paragraphs.• Spacing: Please do not use either the “Spacing Before” or “Spacing After”
functions in the paragraph formatting options (both setting should read “0 pt.”).
• Kerning: please do not kern your text (expand or condense words or lines).
• Justification: Left-justified text a.k.a. flush left a.k.a. quad left (do not justify margins).
• Page numbers: Use automatic page numbers in the footer. • When submitting your manuscript, please do not send the file with
“Track Changes.”
Tables and Table CaptionsTables should be self-explanatory and should not duplicate textual material. The tables along with their numbers should be cited at the relevant place in the text. • All tables for your article, and each one’s caption, should be placed (in
the same Word or WordPerfect document as the text) at the very end of the manuscript’s text, after the References.
• Place each table on its own separate manuscript page.• Tables must be numbered consecutively in the order of their first citation
in the text.
• The table number should be Arabic, followed by a period and a brief title.• Type the table caption double-spaced. • For both the table title and the table caption, use the same size type as
the text (11-pt.).• Explain in a footnote beneath the table’s caption all non-standard
abbreviations that are used in each table. • Supply a brief column heading for each column in a table.• Do not use vertical lines between columns. Use horizontal lines above
and below the column headings and at the bottom of the table only. Use extra space to delineate sections within the table.
• Obtain permission for all borrowed, adapted, and modified tables and provide a credit line in the footnote.
• Please remember that tables prepared with Excel are not accepted unless embedded within your text document.
Figure captions• Your figure captions must be carefully numbered to reflect the numbers
you assigned to your figures (which are submitted separately from your manuscript—in your Figures file, described below).
• For your figure captions, please type them in the order in which they are cited in your text, and so number them here: 1, 2, 3, etc.
• When symbols, arrows, numbers, or letters are used to identify parts of a figure, identify and explain each one in the caption.
• Explain any internal scale (magnification) and identify the method of staining in photomicrographs.
• If your figure was inspired by a published figure of any kind, please end your caption with a parenthetical credit line: (Adapted from [source].)
• If a figure has been published elsewhere, please submit written permission from the copyright owner to reproduce the material—in your Legalities file, described below.
References• References should be numbered consecutively in the order in which they
are first mentioned in the text (not in alphabetic order). • Identify references in text, tables, and legends by Arabic numerals in
superscript within brackets after the punctuation marks. • References cited only in tables or figures’ captions should be numbered
in accordance with the sequence established by the first identification in the text of the particular table or figure.
• List all authors for each reference; do not use “et al.”• The format of references—examples of which may be seen in any
previous issue of Pulmonary Circulation—is based on the formats used by the National Library of Medicine (NLM) in Index Medicus and The New England Journal of Medicine.
• Please verify all references against original sources, as the accuracy of reference data is the responsibility of the author.
Your FIGURES file (all non-text components of your manuscript other than tables)[2nd of the 4 files to be submitted for an article-type contribution]• All figures must be submitted electronically.• Acceptable formats are: jpg, gif, png.• Maximum file size is 4 MB.• Please do not zip the files. • Submit high-quality figures, either color or black-and-white.• Figures should be actual size.• Figures should be numbered consecutively according to the order in
which they are first cited in the text. • Labels, numbers, and symbols should be clear and of uniform size. The
lettering for figures should be large enough to be legible. • Symbols, arrows, or letters used in photomicrographs should contrast
with the background.• Titles and detailed explanations belong in the captions for figures,
not on the figures themselves (i.e., in your Manuscript file, not in this Figures file).
• Line art should not contain hair-thin lines (which are easily lost in reproductions).
• Line art must be saved at a resolution of at least 1200 dpi; photographs, CT scans, radiographs, etc, should be saved at a resolution of at least 300 dpi. Figures saved at 72 dpi are not acceptable.
• When graphs, scatter-grams or histograms are submitted, the numerical data on which they are based should also be supplied.
• The Journal reserves the right to crop, rotate, reduce, or enlarge photographs.
Contributions to Pulmonary Circulation

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 131
• If needed, videos can also be uploaded (mpg, mpeg, mp4, wmv; maximum file size 20 MB).
Your SIGNS file [3rd of the 4 files to be submitted for an article-type contribution]
As an umbrella term, Pulmonary Circulation uses the word “sign” as it is used in the discipline of semiotics: “something that stands for something.”
With the exception of numbers (which are symbols of amounts), this file must list and define all signs you use in your manuscript—in the text and in figure and table captions—including especially:
• acronyms (e.g., PASMC, -SNAP, PPAR, WHO, BMPR2, BMPRII, etc.);• abbreviations (e.g., ctl., ibid., Disp., b.i.d. [bis in die, “twice daily”], etc.);
and• symbols (e.g., mV, Rm(G), Qa, Kv, etc.).There is no need to alphabetize your list of signs.
Your LEGALITIES file [4th of the 4 files to be submitted for an article-type contribution]• A statement affirming that the manuscript has been read and approved
by all the authors, that the requirements for authorship have been met, and that each author believes that the manuscript represents honest original work.
• Rights and permissions. (Please see Legal Requirements, below.)• Ethical considerations. (Please see Legal Requirements, below.)• Sources of support of each author. (Please see Legal Requirements,
below.)• Conflicts of interest of each author. (Please see Legal Requirements,
below.)
The submission processTo submit your first manuscript to Pulmonary Circulation, simply follow these 10 easy steps. (For subsequent submissions, you already have your log-in name and password.)
STEP 1: Make sure you have your file or your 4 files ready to send (for text-only contributions, your Manuscript file; for article-type contributions, your Manuscript file, your Signs file, your Figures file, and your Legalities file).
STEP 2: Access www.journalonweb.com/pc
STEP 3: Create a login name and set a password through a few simple steps.
STEP 4: Log in as author using your login name and password.
STEP 5: Enter the Article Type, Title, Key Words (3-5) and Abstract. (The Abstract, which should not exceed 2,000 characters, can be typed in or cut-and-pasted in the slot in the website.)
STEP 6: Upload the files applicable to your contribution (either “Manuscript” only, or “Manuscript,” “Figures,” “Signs,” “Legalities”) by browsing to locate the files in your computer.
STEP 7: Click “Next” to include suggested reviewers if you want, or to skip this step, click “Next.”
STEP 8: Next page is the Preview page. Preview using links to all the files you have submitted.
STEP 9: Click the “Submit the Manuscript” button at the end of the page.
STEP 10: You will receive a notification in your email (please check your “junk” email folder if you don’t see the mail in a few minutes).
The receiving processAll manuscripts received are duly acknowledged as having been received and successfully opened.
Before being sent out for review of its contents, each manuscript is checked for its compliance with the Legal Requirements detailed below. Manuscripts that ignore those requirements are returned.
The review processA received manuscript will be reviewed for possible publication with the understanding that it is being submitted solely to Pulmonary Circulation and has not been published anywhere, simultaneously submitted, or already accepted for publication elsewhere.
Pulmonary Circulation editors review all submitted manuscripts initially for suitability for formal peer review. Manuscripts with insufficient originality, ethical or legal problems, serious scientific or technical flaws, or lack of a significant message, are rejected before proceeding to formal peer-review.
A manuscript deemed to be acceptable for review is then sent to reviewers (who many include ones named by the author in the Manuscript Preparation Process).
The disposition processA reviewed manuscript is assigned to an editor who, based on the comments from the reviewers, makes a final decision on its disposition—rejection, acceptance, or acceptance with amendments.
The editor conveys to the author the comments and/or suggestions received from reviewers. The author may be requested to provide a point-by-point response to reviewers’ comments and to submit a revised version of the manuscript. This process is repeated until reviewers, editors, and authors are all satisfied with the manuscript.
The editing processManuscripts accepted for publication are copy-edited for grammar, punctuation, and other considerations.
Page proofs are sent to the corresponding author.
The corresponding author is expected to return the corrected proofs within a specified time period. It may not be possible to incorporate corrections received after that period.
The publishing and printing processAn article will be published online and will remain online for 2 weeks, after which it will go for printing.
The tracking and troubleshooting processRegistered authors can keep track of their articles after logging into the website.
Instructions are also available at our website (www.pulmonarycirculation.org).
If you experience any problems during any of these various processes, please don’t hesitate to email the nearest of our editorial offices: the USA ([email protected]); India ([email protected]); and the UK ([email protected]).
Style Requirements
DashesNone of the dashes ever has either a space before it or a space after it (hyphen: “a one-page article”; en dash: “4–23”; em dash: “The subjects—who were mice—responded well.”). The only exception: multiple hyphens (“In both mid- and long-range plans . . .”).
EllipsesAn ellipsis always has spaces between the 3 periods (“. . .”). While ellipses may be used in informal documents (e.g., emails) to indicate pregnant pauses, their use in scholarly journals is restricted to quotations to indicate that text has been deleted:
“The test was conducted in X township of Y province of Z region in Thailand.”
“The test was conducted . . . in Thailand.”
ItalicsLatin terms are never italicized—et al., per, e.g., etc. Words giving directions are italicized:
Table 2 continued
See Case Studies, below.
NumbersFor conversational-type usage, spell out numbers from one to eleven, then use numbers—12, etc. For describing data, always use numbers: “We had two stages, the first involving 2 units, the second involving 4.6 units.”
In Pulmonary Circulation, all numbers of 4 or more digits use commas:
Contributions to Pulmonary Circulation

Pulmonary Circulation | January-March 2011 | Vol 1 | No 1 132
2451,39915,000,987
Scientific namesThe genus name is always capitalized and always italicized. The species (and subspecies) name is always italicized but never capitalized, even when country names are used:
Homarus americanus (Maine lobster)
For naming species of the same genus, the genus name is spelled out only for the first one:
“Species of lobster include Homarus americanus, sometimes called the American lobster, and H. gammarus, the European lobster.”
All categories above genus are never italicized and always capitalized (as, for the Maine lobster):Kingdom AnimaliaPhylum ArthropodaClass MalacostracaOrder DecapodaFamily Nephropidae
Units of measureUse the International System of Units, SI (from French Système international d'unités), the modern form of the metric system. A more conventionally used measurement may follow in parentheses. Make all conversions before manuscript submission.
Zip CodesFor US states, a physical mailing address is—by US Postal regulations—the one and only place that Zip Codes may be used (e.g., NJ, AK, NM); in every other usage, including the body of your manuscript, a state should be spelled out or, if parenthetical, abbreviated: “Massachusetts,” “(Boston, Mass.)”
For the answer to any other question about a Pulmonary Circulation style requirements, simply email:Nikki Krol ([email protected]) at the Pulmonary Vascular Research Institute in London (the PVRI).
Legal Requirements
Rights and permissions It is the responsibility of the authors to obtain permissions for reproducing any copyrighted text or trademarked material used in their articles. A copy of all permissions obtained must accompany the manuscript.• If a photograph of individuals is used, their pictures must be accompanied
by written permission from them to publish the photograph.
Ethical considerationsThe Journal will not publish any manuscript found to be ethically unacceptable. When reporting studies on humans, indicate whether the procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional or
regional) and with the Helsinki Declaration of 1975, as revised in 2008 (available at www.wma.net). For prospective studies involving human participants, authors are expected to mention approval of a regional or national or institutional or independent Ethics Committee or Review Board, obtaining informed consent from adult research participants and obtaining assent for children aged over 7 years participating in the trial. Ensure confidentiality of subjects by refraining from using participants’ names, initials or hospital numbers, especially in illustrative material. When reporting experiments on animals, indicate whether the institution’s or a national research council’s guide for, or any national law on the care and use of laboratory animals, was followed. Documentation of approval by a local Ethics Committee (for both human and animal studies) must be supplied by the authors on demand.
Patients’ right to privacy Identifying information should not be published in written descriptions, photographs, sonograms, CT scans, etc., and pedigrees unless the information is essential for scientific purposes and the patient (or parent or guardian, wherever applicable) gives written informed consent for publication. Authors should remove patients’ names from figures unless they have obtained written informed consent from the patients. When informed consent has been obtained, it should be indicated in the article and a copy of the consent should be included in your Legalities file.
Warranties of originality and compliance• Manuscripts are considered only on the legal understanding that they
contain original material never before published in article form in any venue.
• Manuscripts are considered only on the legal understanding that they are in full compliance with any applicable NIH or other funding agency requirements.
Sources of supportAll sources of support for the research described in your article must be identified. Such sources include but are not limited to grants, fellowships and scholarships. (See Note following “Conflicts of Interest.”)
Conflicts of interestAll authors must disclose any and all conflicts of interest they may have with an institution or product that is mentioned in the manuscript and/or is important to the outcome of the study presented. Authors must also disclose:• Any income which may be perceived as a conflict of interest (including
but not limited to employment by an industrial concern, consulting fees, and honoraria); and
• Any conflict of interest with products that compete with those mentioned in their manuscripts (including but not limited to any relationship with pharmaceutical companies, device manufacturers, or other corporations whose products or services are related to an article’s subject matter).
NOTE: Both Sources of Support and Conflicts of Interest are published in a box following an article’s References. For example:
Sources of Support: National Institutes of Health (grant ID number). Conflicts of Interest: None declared.
Contributions to Pulmonary Circulation

Call for Papers
Pulmonary
CirculationFirst Peer-Reviewed Journal Dedicated to
Pulmonary Vascular Disease
For more information see:http://www.pulmonarycirculation.org/
Submit your manuscript at:http://www.journalonweb.com/PC/
Editors-in-Chief
Senior Editor
Editors
Executive Editor
Scientific Advisory Board
Jason X.-J. Yuan, MD, PhDNicholas W. Morrell, MDHarikrishnan S., MD
Kurt R. Stenmark, MDKenneth D. Bloch, MDStephen L. Archer, MDMarlene Rabinovitch, MDJoe G.N. Garcia, MDStuart Rich, MDMartin R. Wilkins, MDHossein A. Ghofrani, MDCandice D. Fike, MDWerner Seeger, MDSheila G. Haworth, MDPatricia A. Thistlethwaite, MD, PhDChen Wang, MD, PhDAntonio A. Lopes, MD
Ghazwan Butrous, MD
Harikrishnan S., MD
Robert F. Growver, MD, PhDCharles A. Hales, MDJoseph Loscalzo, MDJohn B. West, MD, PhD, DScMagdi H. Yacoub, MD, DSc, FRS
Pulmonary Circulation is the only journal devoted to the fieldof pulmonary circulation publishing ,
, and in pulmonaryvascular disease and lung injury. The new journal stands at the
forefront of the critical collaboration between basic scientists andclinicians in research on the pulmonary circulatory system and
clinical diagnosis and treatment of pulmonary vascular diseases
original research articlesreview articles case reports perspectives
Pulmonary Vascular Research Institute (PVRI)is an international, non-profit medical research organizationdedicated to increasing the awareness and knowledge ofpulmonary vascular diseases and facilitating advances
in the treatment of affected people worldwide
First dedicated journal on the pulmonary circulationImmediate publication on acceptanceNo charge for processing manuscript
No charge for color photographsNo charge for publication
Open access
Clinical trialsClinical researchDrug developmentBasic science researchEpidemiology and biomedical informaticsDiagnostic and therapeutic guidelines

CONTENTS
Welcome
Pulmonary Circulation: A new venue for communicating your findings, ideas and perspectivesJason X.-J. Yuan, Nicholas W. Morrell, Harikrishnan S., Ghazwan Butrous 1
Review Articles
Progenitor cells in pulmonary vascular remodelingMichael E. Yeager, Maria G. Frid, Kurt R. Stenmark 3
Protein trafficking dysfunctions: Role in the pathogenesis of pulmonary arterial hypertensionPravin B. Sehgal, Jason E. Lee 17
Is peroxisome proliferator-activated receptor gamma (PPAR) a therapeutic target for the treatment of pulmonary hypertension?
David E. Green, Roy L. Sutliff , C. Michael Hart 33
Functional ion channels in human pulmonary artery smooth muscle cells: Voltage-dependent cation channels
Amy L. Firth, Carmelle V. Remillard, Oleksandr Platoshyn, Ivana Fantozzi, Eun A. Ko, Jason X.-J. Yuan 48
Research Articles
Oxidative injury is a common consequence of BMPR2 mutationsKirk L. Lane, Megha Talati, Eric Austin, Anna R. Hemnes, Jennifer A. Johnson, Joshua P. Fessel, Tom Blackwell, Ray L. Mernaugh, Linda Robinson, Candice Fike, L. Jackson Roberts II, James West 72
STIM2 contributes to enhanced store-operated Ca2+ entry in pulmonary artery smooth muscle cells from patients with idiopathic pulmonary arterial hypertension
Michael Y. Song, Ayako Makino, Jason X.-J. Yuan 84
Doppler-defined pulmonary hypertension in medical intensive care unit patients: Retrospective investigation of risk factors and impact on mortality
Jason A. Stamm, Bryan J. McVerry, Michael A. Mathier, Michael P. Donahoe, Melissa I. Saul, Mark T. Gladwin 95
Expression of mutant BMPR-II in pulmonary endothelial cells promotes apoptosis and a release of factors that stimulate proliferation of pulmonary arterial smooth muscle cells
Xudong Yang, Lu Long, Paul N. Reynolds, Nicholas W. Morrell 103
Short Research Report
Combination use of sildenafil and simvastatin increases BMPR-II signal transduction in rats with monocrotaline-mediated pulmonary hypertension
Tuguang Kuang, Jun Wang, Amy Zeifman, Baosen Pang, Xiuxia Huang, Elyssa D. Burg, Jason X.-J. Yuan, Chen Wang 111
Case Reports
Severe pulmonary artery hypertension following intracardiac repair of tetralogy of Fallot: An unusual finding
Bhupesh Kumar, Goverdhan D. Puri, RohitManoj, Kirti Gupta, Shyam K. S. 115
Clinical demonstration of efficiency and reversibility of hypoxic pulmonary vasoconstriction in a patient presenting with unilateral incomplete bronchial occlusion
Syeda Jafri, Pasupathy Sivasothy, Francis Wells, Nicholas W. Morrell 119
Snapshot
Diagnostic and therapeutic algorithm for pulmonary arterial hypertensionAnkit A. Desai, Roberto F. Machado 122
Announcement
The PVM History Initiative of the PVRIGhazwan Butrous 125
Contributions to Pulmonary Circulation 127
Printed and published by Medknow Publications and Media Pvt. Ltd on behalf of Pulmonary Vascular Research Institute (PVRI), London, UK and printed at ???, Mumbai, and published at B5-12, Kanara Business Centre, Ghatkopar, Mumbai, India.