-
7/28/2019 20459323 Pulmonary Circulation
1/36
The Pulmonary Circulation
-
7/28/2019 20459323 Pulmonary Circulation
2/36
Importance
Separate pulmonary and systemic circulationsare optimal for
facilitating gas exchange
The anatomy and physiology of the pulmonarycirculation are
markedly different from thesystemic circulation
Abnormalities in pulmonary blood flow affect theoxygenating
function of the lung
Anaesthesia and surgery may have importanteffects on the
pulmonary circulation, especially indisease states
The pulmonary circulation may be alteredtherapeutically to
improve V/Q ratios
-
7/28/2019 20459323 Pulmonary Circulation
3/36
Overview
Functional anatomy
Determinants of: Pulmonary blood flow
Pulmonary blood volume Pulmonary haemodynamics
pressures
vascular resistance
Measurement of pulmonary blood flow
-
7/28/2019 20459323 Pulmonary Circulation
4/36
Pulmonary Vascular Anatomy
Arteries Pulmonary blood flow ~ systemic
PVR only 1 / 6 SVR
Media thickness ~ 1/2 systemic
Lie close to corresponding air passages Arterioles
Transition at 100 (ID)
Virtually no muscular tissue*
Thin media of elastic tissue
Structurally similar to venules
-
7/28/2019 20459323 Pulmonary Circulation
5/36
pulmonary vascular anatomy
Pulmonary endothelial cells Exposed to entire cardiac output
Link pulmonary and systemic circulations
Regulate vascular smooth muscle tone
Capillaries Dense network over alveolar walls
More than one alveolus per capillary network
Cross- sectional area influenced by alveolar inflation
Venules and veins Venules ~ arterioles (gas exchange possible
with reverse flow)
Veins do not accompany arteries (via intersegmental septae)
-
7/28/2019 20459323 Pulmonary Circulation
6/36
The Bronchial Circulation
Arises from arch of aorta
1% of cardiac output
Nutrient down to terminal bronchioles
Humidifies / warms inspired air Some flow returns to systemic
circulation (azygos
to SVC)
~ normal systemic flow
Some flow returns to pulmonary veins
= venous admixture
-
7/28/2019 20459323 Pulmonary Circulation
7/36
Pulmonary Blood Flow
Slightly less than systemic flow Bronchial and thebesian venous
admixture
From 5 l/m at rest to 25 l/m with exercise
Increased PBF minimally affects PVR
Limited ability to control flow distribution PBF is markedly
affected by gravity:
dependent perfusion > nondependent
Maldistribution of pulmonary flow affects gasexchange
-
7/28/2019 20459323 Pulmonary Circulation
8/36
Pulmonary Blood Volume
Influenced by:
Posture Falls by 27% on standing from lying (due to systemic
pooling)
Drugs Due to greater vasomotor activity of systemic
circulation
Increased by vasopressors / MAST suit
Decreased by vasodilators / lumbar sympathectomy
Left heart failure
-
7/28/2019 20459323 Pulmonary Circulation
9/36
Pulmonary Vascular Pressures
Small pressure drop cf. systemic circulation PAP = 25/10mmHg
Concept ofdriving pressure rather than simpleintravascular
pressure (cf atmospheric) is useful..
Pulmonary driving pressure = mPAP - mLAP
Driving pressure is unaffected by IPPV as PAP and PVPare both
increased
PBF = driving pressure / PVR
-
7/28/2019 20459323 Pulmonary Circulation
10/36
Effect of gravity on alveolar andvascular pressures
ZONE 1
pA >pa >pV
ZONE 2Pa >pA >pV
ZONE 3
Pa >pV >pA
No flow
Flow Pa -pA
Flow Pa -pV
-
7/28/2019 20459323 Pulmonary Circulation
11/36
pulmonary vascular pressure
Transmural pressure = pressure gradientfrom inside to outside of
vessel
For larger vessels, extravascular pressure
= intrathoracic pressure Transmural pressure gradients are
highest in dependent parts of lung Site of pulmonary oedema
-
7/28/2019 20459323 Pulmonary Circulation
12/36
Effect of changes in intra-alveolarpressure on intrathoracic and
pulmonaryvascular pressures
Intrathoracic P = alveolar P - alveolar transmural P
Alveolar transmural pressure depends on lungvolume
IPPV: Intrathoracic pressure increases by lessthan 1/2 the
inflating pressure
Less if poor lung compliance
Increased intra-alveolar pressure directlyincreases SAP (early
valsalva) and PAP
spont.vent.produces higher PAP with expiration
-
7/28/2019 20459323 Pulmonary Circulation
13/36
Pulmonary Vascular Resistance
Pulmonary driving pressure
PVR = Cardiac output
But: Assumes laminar blood flow PVR falls as flow increases due
to low vasomotor
tone Blood is a non - Newtonian fluid (viscosity varies
with linear velocity) Units: usually 50-150 dyne.s.cm-5
-
7/28/2019 20459323 Pulmonary Circulation
14/36
Factors Affecting PVR -passive
Cardiac output
Increased CO produces minimal impact on PAPdue to dilation /
recruitment of collapsed vessels
Recruitment mainly in non-dependent lung Usually all of lung is
perfused during spont.vent
Distension occurs in all pulmonary vessels Especially with
pneumonectomy / ASD / VSD
Lung inflation
Minimum at FRC...
-
7/28/2019 20459323 Pulmonary Circulation
15/36
Relationship Between PVR and LungVolume
Pulmonaryvasc
ularresistance
Lung Volume
RV FRC TLC
compression of alveolar vessels
compression of corner vessels*
/ HPV of collapsed lung units
*lie at junctions between 3 or more alveoli
-
7/28/2019 20459323 Pulmonary Circulation
16/36
Active Control of PulmonaryVascular Resistance
Usual state = active vasodilatation
Many receptors / agonists implicated in vitro,relative
importance in humans is unknown
Many of the basic control mechanisms probably
act directly on smooth muscle Endothelium acts to modulate the
smooth muscle
response
-
7/28/2019 20459323 Pulmonary Circulation
17/36
...active control of pulmonary vascularresistance
Endothelial / smooth muscle receptors... Many types
Agonists:
from nerve endings (eg. Noradrenaline / Ach)
Produced locally (eicosanoids) Via blood (peptides)
Some similar / identical agonists may produceopposite effects at
different receptors
Eg. Noradrenaline at 1and
2receptors
-
7/28/2019 20459323 Pulmonary Circulation
18/36
Role of the endothelium and NO
Many pulmonary vasodilators (eg. Ach /vasopressin) are
endothelium-dependent
Common pathway mainly via NO
Basal production of NO helps maintain a low
PVR
-
7/28/2019 20459323 Pulmonary Circulation
19/36
Activation and Action of NO in the Pulmonary Vasculature
Vascular endothelium
Receptor activation
L-arginine L-citrulline
Ca++
NO synthase
Guanylate cyclase
GTP
Cyclic GMP G Kinase
Ca++ RELAXATION
Vascular muscle
NO
-
7/28/2019 20459323 Pulmonary Circulation
20/36
Respiratory effects on PVR
Hypoxia
Induces HPV Unique to pulmonary vasculature
Mediated by both mixed venous (20%) and alveolar
hypoxaemia (80%) Overall response is nonlinear
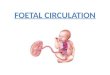
HPV diverts blood from poorly perfused areas Optimises V/Q
Diverts blood from foetal lungs
If chronic: produces pulmonary hypertension
-
7/28/2019 20459323 Pulmonary Circulation
21/36
Mechanism of HPV
Mediated via small arterioles (30-30m)Distal to lobar arteries,
proximal to capillaries
Non-neural (occurs in transplanted lung)
Biphasic responseInitial phase:
Seconds - maximal at 5-10 minutes
Returns almost to baseline
Second phase:
Slow, sustained vasoconstriction, plateau at ~ 40 min.
Mechanism Inhibition of O
2sensitive K+ channels
Inhibits K+ efflux, producing depolarisation and Ca++ entry
through
voltage -dependent Ca++
channels
-
7/28/2019 20459323 Pulmonary Circulation
22/36
100
80
60
40
20
0
0 20 40 60 80
Alveolar PO2
Pressor
response(% max.)
The Effect of Changes in Mixed Venous and Alveolar PO2 on
Pulmonary Vasoconstriction
10mmHg
20mmHg
30mmHg
40mmHg
60mmHg
Mixed venous PO2
-
7/28/2019 20459323 Pulmonary Circulation
23/36
Effect of pCO2 and pH on HPV
Hypercapnia and acidosis Both respiratory and metabolic acidosis
augment HPV
Slight vasoconstriction
Hypocapnia and alkalosis Metabolic and respiratory alkalosis
both inhibit / abolish
HPV
Vasodilation
-
7/28/2019 20459323 Pulmonary Circulation
24/36
Anaesthesia and PVR
Intravenous Minimal effect on HPV, vascualar tone or
oxygenation
Exceptketamine (increases PVR)
Volatile anaesthetics Minimal effect on PVR, decrease PAP
PAP effect: sevoflurane > isoflurane
Effect on PBF due to negative inotropy Halothane reduces PBF, no
effect on PVR
Isoflurane
No effect on HPV at 1-1.2 MAC
N20 increases PVR / attenuates HPV
Reduced / no effect if chronically elevated PVR
-
7/28/2019 20459323 Pulmonary Circulation
25/36
Neural Control of PulmonaryBlood Flow
1. Adrenergic Thoracic sympathetic fibers
Smooth muscle of pulmonary arteries / arterioles
Both constrictor (1-norad.) and dilator (
2-circulating adren.)
2- vasodilatation
Presynaptic: inhibition of NA release Postsynaptic: increase NO
production in endothelium
Dominant effect is 1:
sympathetic stimulation PVR
-
7/28/2019 20459323 Pulmonary Circulation
26/36
neural control of pulmonaryblood flow
2. Cholinergic Vagal stimulation produces vasodilatation
ACh release stimulates M3receptors
Endothelium and NO dependent
AChis constrictor if no endothelium
? Significance of cholinergic control in humans
3. Non- adrenergic / non- cholinergic (NANC) Anatomically
related to ANS
Different neurotransmitters
Mostly inhibitory in lung, vasodilatation via NO release
? Functional significance
-
7/28/2019 20459323 Pulmonary Circulation
27/36
Humoral Control of PulmonaryBlood Flow
*Probably minimal role in control ofnormalPBF Involved in
pulmonary vascular diseases
Catecholamines Adrenaline / dopamine:
and effects
Mainly vasoconstrictor Eicosonoids
Pulmonary vessels metabolise arachadonic acid to PGs/TXA2
Mainly constrictor except PGI2
May be involved in pulmonary hypertension in sepsis / CHD /
reperfusion injury
-
7/28/2019 20459323 Pulmonary Circulation
28/36
humoral control of pulmonaryblood flow
Amines Histamine: variable, constricts resting smooth muscle
5-HT (serotonin): released from activated platelets
Constrictor
May aggravate pulmonary hypertension due to PE
Peptides Diverse responses
Mainly vasodilatation via endothelial receptors
Mainly vasoconstriction via direct smooth muscle action
Purine nucleosides Variable responses
Adenosine is a vasodilator
Receptors and agonists involved in active control of pulmonary
vascular tone
-
7/28/2019 20459323 Pulmonary Circulation
29/36
Receptor Subtypes Principle Responses Endothelium
Group agonists dependent?
Adrenergic 1 noradrenaline constriction No
2 noradrenaline constriction Yes 2 adrenaline dilatation Yes
Cholinergic M3 acetylcholine dilatation Yes
Amines H1 histamine variable Yes
H2 histamine dilatation No
5-HT1 5-HT variable variable
Purines P2x ATP constriction No
P2y ATP dilatation Yes
A1 adenosine constriction No
A2 adenosine dilatation No
Eicosanoids TP thromboxane A2 constriction No
? Prostacyclin (PGI2) dilatation ?
Peptides NK1 Substance P dilatation Yes
NK2 Neurokinin A constriction NoAT angiotensinogen constriction
No
ANP ANP dilatation No
B2 bradykinin dilatation Yes
ETA, ETB endothelin const.A, dil.B NoA, YesBV1 vaso ressin
dilatation Yes
-
7/28/2019 20459323 Pulmonary Circulation
30/36
Measurement of the pulmonarycirculation
Pulmonary blood volume Dye - dilution: PA to PV or LA
Usually 10-20% of blood volume
Pulmonary vascular pressure
PAP: Swan - Ganz catheter / echocardiography PVP: PCWP / LA
catheter
Pulmonary blood flow... Fick principle
Dye / thermal dilution
2-D ultrasound of PA + Doppler flow velocity
-
7/28/2019 20459323 Pulmonary Circulation
31/36
pulmonary blood flow
Fick principleO2 extraction = amount added to blood flowing
though lungs
VO2 = Q (Ca O2- CvO2)
Q =
Ca O2- CvO2
Limitations:
Does not include extrapulmonary shunt flow
Does not include oxygen consumption by the lung
May be large if lungs are infected
VO2
-
7/28/2019 20459323 Pulmonary Circulation
32/36
Modified Fick Method
Soluble, inert tracer gas (15% N2O,freon / argon)
Short sampling period (single breath) Mixed venous concentration
~ 0
tracer gas uptakeQ = art. tracer gas concentration*
* ~ PET. ALVtracer gas X blood solubility coefficient
Noninvasive Limited if large alveolar dead space or shunt
-
7/28/2019 20459323 Pulmonary Circulation
33/36
Thermodilution Measurement of Cardiac Output
SVC
PA
injectate at
known T
thermistor
temp
time
Higher blood flow lower temperature rise in PA
-
7/28/2019 20459323 Pulmonary Circulation
34/36
Echocardiographic Measurement ofPulmonary Blood Flow
Diameter of PA measured PA cross -sectional area calculated
Mean flow in PA measured / beat Velocity. time integral
(VTI)
Stroke volume = PA area X VTI
Cardiac output = SV X HR
DPaVel.
time
VTI
= area under curve
-
7/28/2019 20459323 Pulmonary Circulation
35/36
Summary
The pulmonary circulation differs markedly inanatomy and
function to the systemic circulation
Large changes in cardiac output produce littlechange in PAP due
to distension and recruitment
Pulmonary arteries are low pressure and lessinfluenced by neural
control than are systemic
The pulmonary circulation has limited ability tocontrol blood
flow distribution through the lung
-
7/28/2019 20459323 Pulmonary Circulation
36/36
summary
Pulmonary vascular resistance is influencedpassively by factors
such as cardiac output,posture and lung volume
Pulmonary vascular resistance is actively
influenced by cellular, respiratory, neural andhumeral
factors