Embed Size (px)
Citation preview

Kidney International, Vol. 66 (2004), pp. 806–810
Pulmonary calcification in hemodialysis patients:Correlation with pulmonary artery pressure values
MORDECHAI YIGLA, ZOHAR KEIDAR, ISRA SAFADI, NAVEH TOV, SHIMON A. REISNER,and FARID NAKHOUL
Division of Pulmonary Medicine; Department of Nuclear Medicine; Department of Cardiology; and Department of Nephrology,Rambam Medical Center and Faculty of Medicine, Technion-Israel Institute of Technology, Haifa, Israel
Pulmonary calcification in hemodialysis patients: Correlationwith pulmonary artery pressure values.
Background. End-stage renal disease (ESRD) patients re-ceiving chronic hemodialysis (HD) via an arteriovenous (A-V) access often develop unexplained pulmonary hypertension(PHT). This study evaluated the role of pulmonary calcification(PC) in this phenomenon.
Methods. The clinical manifestations, systolic pulmonaryartery pressure (PAP) values measured by Doppler echocar-diography and the presence and the extent of PC expressed bylung uptake of 99mTc-MDP bone scintigraphy, were studied in49 patients with ESRD receiving chronic HD therapy via A-Vaccess. The correlation between PC and PHT was investigated.
Results. There were 36 men and 13 women with a mean age of61.7 ± 13.2 years receiving HD therapy for 38.2 ± 43.7 months.Twenty (40.8%) patients had PC expressed by increased lunguptake of 99mTc- MDP and 28 (57.1%) patients had PHT with amean systolic PAP of 46 ± 11 mm Hg. No correlation was foundbetween PC and PHT.
Conclusion. The data suggest that PC expressed by lung up-take of 99mTc-MDP has no role in the pathogenesis of PHTamong ESRD patients undergoing HD therapy via A-V access.
Extraosseous pulmonary calcification (PC) is foundmost commonly in end-stage renal disease (ESRD) pa-tients on chronic hemodialysis (HD) therapy [1–3]. Calci-fications can occur in any tissue of the body but are foundmost commonly in the heart, lungs, kidney, and stomach.In the lungs, calcium deposits have been found in the in-terstitium of the alveolar septum, bronchiole walls, in thelarge airways, and even in the walls of the pulmonary ves-sels [4–6]. The clinical manifestations of PC are usuallyminimal. Occasionally, PC may cause profound respira-tory disturbances [1, 2].
Key words: end-stage renal disease, hemodialysis, pulmonary calcifica-tion, pulmonary hypertension.
Received for publication April 1, 2003and in revised form December 6, 2003Accepted for publication February 20, 2004
C© 2004 by the International Society of Nephrology
In a recently published study [7], we evaluated the in-cidence of pulmonary hypertension (PHT) in ESRD pa-tients using Doppler echocardiography. Almost 40% ofHD patients had systolic PAP above 35 mm Hg, and theircardiac-output (CO) was significantly higher comparedwith HD patients without PHT. Because the study pop-ulation had no obvious cause for PHT, we assumed thatboth ESRD and HD therapy via arteriovenous (A-V)access might be involved in the pathogenesis of this syn-drome. Increased CO per se does not cause PHT unlessthe capacity of the pulmonary circulation is diminished.Pulmonary calcification in the vascular compartment ofHD patients is a possible explanation.
X-ray film and computerized tomography (CT) of thechest, high resolution computed tomography scan withmediastinal images, technetium 99m–labeled [99mTc]–MDP bone scanning, and magnetic resonance imaging(MRI) have all shown variable diagnostic values in de-tecting PC [8–15]. 99mTc-MDP bone scintigraphy is con-sidered to be a sensitive measure of PC in ESRD, and, inaddition, enables semiquantitative evaluation of the PC[11].
This study evaluated the extent of pulmonary uptake of99mTc-MDP bone scintigraphy in a group of HD patientsand correlated this uptake to the occurrence of PHT.
METHODS
Patients
Our local institutional clinical research ethics reviewboard approved the research protocol. All participantssigned an informed consent before entering the study.
Patient selection
A total cohort of 110 ambulatory patients with ESRDreceiving chronic HD therapy via a surgically created A-V access in our institution was reviewed. Patients withknown cardiac (N = 37), pulmonary (N = 6), and sys-temic diseases (N = 4) were excluded from the study. Anadditional 14 patients refused to participate in the study.
806

Yigla et al: Pulmonary calcification in hemodialysis patients 807
110 patients receiving HD
via A-V access
Exclusion criteria
Patient evaluation
Presence ofCardiac disease (N = 37)Lung diseases (N = 6)Systemic diseases (N = 4)
Pulmonary uptake of99mTc -MDP bone scintigraphyDoppler echocardiography
Clinical variables
14refused
Study group49 patients
Analysis
Prevalence & extent of lung uptake of 99mTc-MDPPrevalence of PHT
ComparisonsIncreased vs. normal uptakeCorrelation between PHT & lung uptake
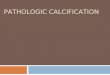
Fig. 1. Study flowchart.
The remaining 49 patients comprised the study popula-tion (Fig. 1).
The study group underwent evaluation that includedphysical examination, chest radiography, and blood testsfor calcium, phosphorus, and parathyroid hormone level.Age, sex, comorbidity, medications used, etiology of kid-ney disease, age at onset, and duration of HD therapywere recorded from patient files.
Hemodialysis patients with systolic PAP above 35 mmHg underwent further evaluation by a specialist pul-monologist that included computed tomography of thechest, complete pulmonary function tests, measurementof blood gases and O2 saturation while breathing roomair, and ventilatory perfusion radioisotope lung scan in-tended to disclose other causes of PHT. None of the pa-tients was excluded from the study after this work-up.
Echocardiography
To avoid overestimation of PAP due to volume over-load, all the Doppler measurements were performedwithin one hour after completion of dialysis. One experi-enced operator, masked with regard to the clinical statusof the patient, performed all echocardiography studiesusing an Acuson Sequoia, Aspen, or 128 XP (MountainView, CA, USA) and GE Vivid 3 (Milwaukee, WI, USA)ultrasound machine. Every patient underwent a com-plete two-dimensional, M-mode, and Doppler echocar-diography study. A tricuspid regurgitation systolic jet wasrecorded from the parasternal or apical window with thecontinuous-wave Doppler probe. Systolic right ventricu-lar (or pulmonary artery) pressure was calculated using
0102030405060708090
Sys
tolic
PA
P
0 1 2 3 4Pulmonary uptake
Fig. 2. Distribution of systolic pulmonary artery pressure (SPAP) ac-cording to degree of 99mTc-MDP pulmonary uptake.
the modified Bernoulli equation given by: PAP = 4 × (tri-cuspid systolic jet)2 + 10 mm Hg (estimated right atrialpressure). PHT was defined as a systolic PAP ≥35 mmHg. Cardiac output was estimated from the left ventricu-lar outflow tract velocity time integral × diameter.
99mTc-MDP pulmonary uptake
All patients underwent bone scintigraphy two hoursafter intravenous injection of 740 MBq of 99mTc-MDP.Whole skeleton planner scintigraphy was performed us-ing a dual- or a single-head digital gamma camera. The99mTc-MDP uptake in the lungs was evaluated for eachpatient from the planar view of the chest. The degree oflung uptake was determined by a nuclear medicine spe-cialist, who was not aware of the patient’s clinical andlaboratory data. The uptake was graded according to thefollowing scale: 0 = no uptake, 1 = mild uptake, inten-sity less than bone uptake, 2 = lung uptake similar tobone uptake, 3 = lung uptake greater than bone uptake.Grade 0–1 uptakes were considered as normal (Fig. 3A),and grade 2–3 lung uptake of 99mTc-MDP (Fig. 3B) wereconsidered as elevated [11–13].
Data analysis
The incidence and the degree of PC were comparedbetween HD patients with and without PHT. The corre-lation between the extent of PC, systolic PAP, and clini-cal variables was evaluated using the two-tailed unpairedStudent t test for continuous data and chi-square analy-sis for discrete data. Continuous data were expressed asthe mean values ± standard deviation (SD). Statisticalsignificance was set as P < 0.05.
RESULTS
Demographic and clinical data of the 49 HD patientsstudied are presented in Table 1. There were 36 menand 13 women with a mean age of 61.7 ± 13.2 years(range 29 to 82 years). Mean duration of HD was 38.2 ±43.7 months (range 7 to 234). The three most com-mon etiologies of renal failure were diabetes mellitus

808 Yigla et al: Pulmonary calcification in hemodialysis patients
A
B
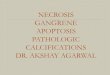
Fig. 3. Grade 3 lung uptake of 99mTc-MDP. (A) Planar bone scintig-raphy (anterior view-left, posterior view-right) of a 42-year-old womanwith ESRD who had been receiving hemodialysis for the last eight yearsdemonstrates abnormal diffuse lung uptake of the tracer, more promi-nent at the bases. Grade 0 lung uptake of 99mTc-MDP. (B) Planar bonescintigraphy (anterior view-left, posterior view-right) of a 34-year-oldmale with ESRD who had been receiving hemodialysis for the last sixyears demonstrates normal distribution of the tracer with no evidencefor lung uptake.
(28.6%), arterial hypertension (22.4%), and glomeru-lopathy (18.4%).
Pulmonary calcification
Increased lung uptake of 99mTc-MDP (grade 2–3) wasfound in 20 (40.8%) patients. Seventeen patients had
Table 1. Data on 49 patients with ESRD on hemodialysis via surgicalA-V shunt
Age yearsMean age 61.7 ± 13.2Range 29–82
SexMale 36 (73.5%)Female 13 (26.5%)
M/F ratio 2.8Etiology of renal failure
Diabetes mellitus 14 (28.6%)Hypertension 11 (22.4%)Glomerulonephritis 9 (18.4%)Chronic pyelonephritis 5 (10.2%)Nephrolithiasis 5 (10.2%)Polycystic kidney 3 (5.1%)Unknown 2 (4.1%)
Duration of dialysis monthsMean 38.2 ± 43.7Range 7–234
Systolic PAPa values mm HgNo. of patients with SPAPa >35 28 (57.1%)Mean SPAPa 46 ± 11
Pulmonary calcificationGrade 0 and 1 normal uptake 30 (59.2%)Grade 2–3 elevated uptake 19 (40.8%)Equal to bone (grade 2) 17More than bone (grade 3) 3
aPAP, pulmonary artery pressure.
Table 2. Distribution of systolic PAP among HD patients withnormal and elevated 99mTc-MDP pulmonary uptake
99mTc- MDP pulmonary uptake
0–1 2–3
SPAP <35 11 10SPAP >34 18 10
grade 2 uptake (equal to the bone), and 3 had grade 3(higher than the bone). Twenty-nine patients had normaluptake (grade 0–1). Review of the chest x-ray films of allthe patients and computerized tomography of the chestof 35 patients (including all patients with PHT who un-derwent CT as a part of the work-up to disclose etiologyfor the PHT) revealed diffuse PC in only one patient withgrade 2 lung uptake and elevated PAP.
Pulmonary artery pressure studies
Systolic PAP of 28 (57.1%) patients was elevated. Theirmean systolic PAP was 46 ± 11 (range 35 to 85). Twenty-one patients had normal systolic PAP (Table 1).
Correlations between increased uptake and PHT
Data on the distribution of systolic PAP values accord-ing to the degree of 99mTc-MDP lung uptake are pre-sented in Figure 2 and Table 2. Note the proportion ofPHT (18/29 vs. 10/20, respectively; P = 0.842) and themean systolic PAP (37 ± 11 vs. 40 ± 15, respectively; P =0.335) did not differ significantly between patients withand without elevated 99mTc-MDP lung uptake.
The data of 20 patients with and 29 patients with-out elevated 99mTc-MDP were compared (Table 3). Age

Yigla et al: Pulmonary calcification in hemodialysis patients 809
Table 3. Clinical and laboratory data between patients with andwithout elevated pulmonary 99mTc-MDP uptake
Normal uptake Elevated uptake P value
No. of patients 29 (59.2%) 20 (40.8%)Gender
Males/females 22/7 14/6 0.898SPAPa >35 mm Hg 18/29 10/20 0.842
(% of patients)SPAPa values mm Hg
Mean 37 ± 11 40 ± 15 0.335Range 20–65 20–85
Age yearsMean 62.4 ± 140 60.8 ± 12.2 0.567Range 29–80 36–82
Cardiac output L/minMean 6.05 ± 1.1 5.75 ± .9 0.231Range 4.8–8.4 3.6–8
Time interval monthsc
Mean 42.2 ± 53.5 32.4 ± 0.5 0.353Range 17–234 7–84
MedicationsAntihypertensive 24 17 0.878
therapyBeta blockers 15 15 0.573
VasodilatorsCa channel blockers 17 12 0.85ACE inhibitors 9 6 0.807
Hemoglobin 10.9 ± 1.8 11.3 ± 1.3 0.311(mean ± SD)
Hematocrit % 34.3 ± 5.8 32.4.2 ± 6.3 0.196PTHb level ng/L
Mean value 343 ± 266 267 ± 165 0.179Range 11–1313 50–602
Ca-P product mg/dLMean value 44.2 ± 11 46 ± 13 0.532Range 29.25–76 25–71
aSPAP, systolic pulmonary artery pressure; bPTH, parathyroid hormone;cfrom onset of HD therapy to detection of pulmonary hypertension.
and gender distribution were similar for both subgroups,as well as comorbid conditions and medications used.Both groups had elevated cardiac output that did not dif-fer significantly (6.05 ± 1.1 vs. 5.75 ± 0.9, respectively;P = 0.231). The mean duration of HD was nonsignifi-cantly higher in the normal uptake group (42.2 ± 53.5 vs.32.4 ± 20.5, respectively; P = 0.353). Both subgroups hadreduced hemoglobin and hematocrit values, but the dif-ferences between these values did not reach statisticalsignificance.
DISCUSSION
Vascular involvement is one of the most striking formsof extraosseous calcification in chronic renal failure [14–16]. The aorta and the coronary arteries [17] are mainlyaffected, but peripheral small vessels in the systemic andthe pulmonary circulation are also affected [5]. Affectedvessels become stiffer independent of age or hyperten-sion. The impact of this phenomenon on the pulmonarycirculation has not been studied previously.
Autopsy studies of HD patients [5–7] have shown thatpulmonary vascular calcification occurs frequently. Of 15patients studied [5], nine (66%) had evidence of vascu-
lar calcification; in its mild form, fine linear and granu-lar deposits along the alveolar capillary wall were noted,while the more severe cases had linear calcification of theelastic laminae and muscle fibers that in some cases wasaccompanied by loose intimal fibrosis with narrowing ofthe vessel lumens. Another study of 56 HD patients [6]found PC in 75% of the cases (severe −48.2%), and notedthat in general the vascular and the parenchymal changeswere parallel. Contrary to pathologic studies, PC is sel-dom recognized clinically. This discrepancy is explainedby the relatively minor tissue reaction evoked by the smallsize of deposited crystals.
Pulmonary hypertension is a new entity in HD patients[7]. Its occurrence in patients with elevated cardiac outputsuggests failure of the pulmonary vasculture to maintainthe A-V access–mediated elevated CO. Increased stiff-ness of pulmonary vasculture due to vascular calcifica-tion is a possible mechanism. This notion is supported by astudy [18] of two subgroups of a dog model of ESRD, onewith an intact parathyroid and the other parathyroidec-tomized. This study showed increased PTH activity, lungcalcium content, and PAP values in the dogs with intactparathyroid glands, thus suggesting a link between PC toPHT through the parathyoid hormone.
In this study, PC expressed by lung uptake of 99mTc-MDP bone scintigraphy was present in 40% of the pa-tients, but was not correlated to PAP values. Fifty percentof the patients with increased uptake had no PHT, while62% of the patients with normal uptake had PHT. Thisstudy does not find a role for PC expressed by lung uptakeof 99mTc-MDP bone scintigraphy in the pathogenesis ofPHT in HD patients.
In other words, the high prevalence of lung uptake of99mTc-MDP reflects scinigraphic findings without hemo-dynamic significance. A possible explanation is thatthe lung uptake of the tracer used reflects pulmonaryparenchymal rather than vascular calcification. Alter-nately, it could reflect the presence of nonsignificant vas-cular calcification. Two autopsy studies [5, 6] support thelatter notion.
As the marker used, 99mTc-MDP is taken up only wherecalcium is actively deposited, and does not simply cor-relate with its anatomic presence [12]; its yield for thedetection of vascular calcification is questionable. Othershave limited its use in the population of HD patients be-cause it has a relatively low uptake by amorphous white-lockite type mineral ([CaMg]3[PO4]2), the predominantcalcium salt in ESRD-associated metastatic calcification[2].
99mTc-MDP bone scan is considered a sensitive butnot specific measure for the detection of PC. Of 23 HDpatients with normal chest radiograph, 14 (61%) hadincreased 99mTc-MDP lung uptake [11]. Another studydemonstrated markedly increased 99mTc-MDP lung up-take confirmed by histology in only 1 of 30 HD patients[13]. Although elevated chest-to-spine ratio was found

810 Yigla et al: Pulmonary calcification in hemodialysis patients
in 66% of the patients, it was considered inconclusivefor the presence of PC due to lack of histologic proof.The present study shows similar data: 40% prevalence of99mTc-MDP lung uptake without corresponding findingsin x-ray films or CT of the chest.
Because histologic lung studies are not always avail-able, there is a need for noninvasive measures for thepresence and the extent of PC. The standard chest x-ray is relatively insensitive for the detection of diffusePC. Conger [5] reported abnormal chest x-ray in only1/15 HD patients with microscopic PC. High-resolutionCT of the chest occupying a mediastinal window withor without densitometry measurements provides betterresults; however, false-negatives may result from themicroscopic size of calcium salt crystals or from signal-averaging from a relative large soft tissue component [8–10]. Electron beam CT and spiral CT are highly sensitivetechniques for detecting coronary artery calcification,and are being used with increasing frequency for screen-ing asymptomatic individuals at risk for the developmentof coronary artery disease [19]. MRI is relatively insen-sitive for detecting PC because neither calcium nor airin the lung typically transmits a signal, thereby failing toproduce a contrast [20].
Our previous observation [7] of reversibility of PHTamong HD patients who underwent successful kidneytransplantation, although their A-V access remainedpatent, indicates a role for a humoral factor in thissyndrome. In a more recent study [21], we noted thatdecreased NO production under basal and stimulatoryconditions in the population of patients with PHT con-firms this observation. It appears that HD therapy is as-sociated with reversible endothelial dysfunction.
Coexistence of PC and PHT in the population of ESRDpatients raises several points of interest. Pulmonary vas-cular calcification and even arteriosclerosis have been de-scribed in several conditions characterized by increasedvessel wall shear stress, such as increased pulmonaryblood flow and PHT caused by congenital left-to-rightshunt [22, 23]. The population of HD patients shares sim-ilar hemodynamic features that might contribute furtherto the development of PC.
CONCLUSION
Based on our observations, we conclude that an insub-stantial number of ESRD patients receiving HD therapyhave increased lung uptake of 99mTc-MDP on bone scan,not correlated to PAP values.
ACKNOWLEDGMENT
The authors thank Mrs. M. Perlmutter for her help in the preparationof this paper.
Reprint requests to Dr. M. Yigla, Division of Pulmonary Medicine,Rambam Medical Center, POB 9602, Haifa 31096, Israel.E-mail: m [email protected]
REFERENCES
1. BENDAYAN D, BARZIV Y, KRAMER MR: Pulmonary calcifications: Areview. Respir Med 94:190–193, 2000
2. CHAN ED, MORALES DV, WELSH CH, et al: Calcium deposition withor without bone formation in the lung. Am J Respir Crit Care Med165:1654–1669, 2002
3. KERR DNS: Hypercalcemia and metastatic calcification. CardiovascRes 36:293–297, 1997
4. WANG N-S, STEELE AA: Pulmonary calcification: Scanning electronmicroscopic and X-ray energy-dispersive analysis. Arch Pathol LabMed 103:252–253, 1979
5. CONGER JD, HAMMOND WS, ALFREY AC, et al: Pulmonary calcifi-cation in chronic dialysis patients: Clinical and pathologic studies.Ann Intern Med 83:330–336, 1975
6. KUZELA DC, HUFFER WE, CONGER JD, et al: Soft tissue calcificationin chronic dialysis patients. Am J Pathol 86:403–424, 1977
7. YIGLA M, NAKHOUL F, SABAG A, et al: Pulmonary hypertension inend-stage renal disease patients. Chest 123:1577–1582, 2003
8. BROWN K, MUND DF, ABERLE DR, et al: Intra-thoracic calcifica-tions: Radiographic features and differential diagnosis. Radiograph-ics 14:1247–1261, 1994
9. LINGAM RK, TEH J, SHARMA A, FRIEDMAN E: Metastatic pulmonarycalcification in renal failure: A new HRCT pattern. Br J Radiol75:74–77, 2002
10. JOHOKOH T, IKEZOE J, NAGAREDA T, et al: Metastatic pulmonarycalcification: Early detection by high-resolution CT. J ComputedAssist Tomogr 17:471–473, 1993
11. FAUBERT PF, SHAPIRO WB, PORUSH JG, et al: Pulmonary calcificationin hemo-dialyzed patients detected by technetium-99m diphospho-nate scanning. Kidney Int 18:95–102, 1980
12. KOK M, CASE D, BILLINGSLY J: The use of bone scintigraphy to eval-uate metastatic calcification caused by end-stage renal disease andsecondary hyperparathyroidism. Clin Nucl Med 28:144–145, 2003
13. DE-GRAFF P, SCHICUT IM, PAUWELS EKJ, et al: Bone scinitigraphyin uremic pulmonary calcification. J Nucl Med 20:201–206, 1979
14. QUINIBI WY, NOLAN CA, AYUS JC: Cardiovascular calcification inpatients with end-stage renal disease: A century-old phenomenon.Kidney Int 82:s73–s80, 2002
15. DAVIES MR, HRUSKA KA: Pathophysiological mechanisms of vas-cular calcification in end-stage renal disease. Kidney Int 60:472–479,2001
16. NITTA K, AKIBA T, UCHIDA K, et al: The progression of vascularcalcification and serum osteoprotegrin levels in patients on long-term hemodialysis. Am J Kidney Dis 42:303–309, 2003
17. GOODMAN WG, GOLDIN J, KUIZON BD, et al: Coronary artery cal-cification in young adults with end-stage renal disease who are un-dergoing hemodialysis. N Engl J Med 342:1478–1483, 2000
18. AKMAL M, BARNATT RR, ANSARI AN, et al: Excess PTH in CRFinduces pulmonary calcification, pulmonary hypertension and rightventricular hypertrophy. Kidney Int 47:158–163, 1995
19. ACHENBACH S, MOSHAGE W, ROPERS D, et al: Value of electron-beamcomputed tomography for the non-invasive detection of high-gradecoronary artery stenosis and occlusion. N Engl J Med 339:1964–1971, 1998
20. TAGUHCI Y, FUYUNO G, SHIOYA S, et al: MR appearance of pul-monary metastatic calcification. J Computed Assist Tomogr 20:38–41, 1996
21. NAKHOUL F, YIGLA M, GELMAN R, et al: The pathogenesis of pul-monary hypertension in hemodialysis patients via arterial-venousaccess. Chest, submitted for publication
22. COHEN BA, GALE JT, MENDELSON DS, MITTY HA: Computerized to-mography demonstration of pulmonary artery calcification in Eisen-menger’s syndrome. J Comput Tomogr 99:153–156, 1985
23. STEINBERG I: Calcification of pulmonary artery and enlargementof right ventricle: A sign of congenital heart disease, Eisenmengersyndrome, pulmonary hypertension, increased pulmonary artery re-sistance and reversal of blood flow. Am J Roentgenol 98:369–377,1966