Embed Size (px)
Citation preview

Pulmonary Arterial Hypertension (PAH):Approach and ManagementDemos Papamatheakis, MDAssociate Clinical Professor of MedicinePulmonary, Critical Care and Sleep MedicineUC San Diego Health
Jan 11th 2020

What is Pulmonary Hypertension?
Capillaries

Are there different Pulmonary Hypertension groups?
WHO Group Etiology
1 PAH: idiopathic, heritable, drugs/toxins, associated (liver disease, HIV, CHD, CTD, Schistosoma)
2 Due to left heart disease (post-capillary PH)
3 Due to lung disease and/or hypoxemia
4 CTEPH
5 Other (hematologic disorders, sarcoid, LAM, glycogen storage, fibrosing mediastinitis)

• Similarities within groups • Pathophysiology, pathology, clinical progression
• Different management between groups• Group 1 (PAH): Highly specialized/specific medications• Group 2 (Left heart): Treat HFpEF, HFrEF, etc.• Group 3 (Lung disease): Treat COPD, ILD, OSA• Group 4 (CTEPH): surgical cure (PTE)
Is the classification that important?

What is the likelihood that my patient with PH has PAH?

Why is it important to recognize PAH (group 1 PH)?
Sitbon et. al JACC 2002; D’Alonzo et. al. AIM 1991, McLaughlin et. al. Chest 2004; Hurdman et. al. ERJ 2012, Humbert et. al. ERJ 2010
Treatment EraNo Treatment Era
1
Chronic, progressive disease without a cure and poor prognosis!

7
What do you mean “progressive disease”?

• Other disease processes may have worse prognosis once PH develops
• COPD, ILD, HFrEF or HFpEF
• But: most PH is not PAH
• PAH has very specific/targeted therapies
• Trialed in non-PAH PH (i.e. group 2 or 3 PH)• Either no change or negative studies!
• IV Epoprostenol (Flolan) in HFrEF (FIRST trial)
If PAH is that bad, why not treat all PH as PAH?
8

• Before diagnosing PAH, one needs to at least think of PAH
• High index of suspicion is key!
• Typical patient with PAH
• Younger (<65 y/o)
• Female (70-80%)
• No significant heart or lung disease, no prior VTE
• Possible PAH risks are present (CTD, CHD, stimulant use, anorexigen use, HIV, cirrhosis)
• Non-specific symptoms• DOE, fatigue/poor stamina, lightheadedness; edema, chest pain and syncope if later-stage disease
How do I diagnose PAH?
9

• Findings on physical exam are non-specific and can be subtle• Prominent S2 that can be pathologically split (enhanced and/or delayed P2)
• Cardiac murmur: TR most commonly
• RV heave or lift (due to RVH)
• Elevated jugular venous pulse and/or positive hepatojugular reflux
• S3 or S4 gallop
• Right heart failure findings in late stage PAH
• LEx edema, ascites, hepatomegaly, JVD, etc.
• CXR, ECG, standard lab-work (CBC, CMP)
• Either subtle findings or not particularly specific
Is a physical exam and routine testing helpful?
10

• Assess RVSP and RV/RA + rule out left heart disease
• Echo, ECG (LHC?)
• Rule out parenchymal lung disease or OSA
• PFTs, CXR, chest CT scan, PSG
• Rule out CTEPH
• VQ scan
• Confirm diagnosis, assess left filling pressures and vasoreactivity
• RHC
• Assess PAH etiology/subgroup with lab tests
• HIV, LFTs, ANA, TSH, drug screen
What is a practical approach to PAH diagnosis?
11
Echo
PFT/CXRCT/PSG
VQ scan
RHC


13
RHC

• PAOP/PCWP accuracy is key!
• Difference between PAH and group 2 PH
• Erroneous measurement can lead to poor management decisions
• Measure at end-expiration (avoid mean)
• CO/CI have to be calculated/measured both via indirect Fick and TD methodology
• Required to calculate PVR
• “Vasoreactivity challenge” is required
• Administer rapid-acting vasodilator and assess effect on pressures and CO
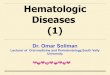
Is this your every-day RHC?
14
Eur Respir Rev 2015; 24: 642
Confirmed Vasoreactivity: a mean PA pressure drop by 10mmHg and to <40mmHg. These patients (~ 5-10%) have improved prognosis and can be treated with CCBs in addition to PAH specific therapies.

• Activity• Active within symptom limits: avoid excessive activity or deconditioning• Supervised Rehab
• Pregnancy• High-risk & teratogenic meds: avoid (2 contraceptive methods recommended)
• Elective surgery• Avoid if possible (GA induction is high risk for circulatory complications)
• Vaccinate for influenza, pneumococcus• Support groups and Genetic counseling for hereditary forms
PAH Therapy – General measures
EHJ 2016;37:67-119

PAH Therapy – Supportive measures
• Diuretics (RV failure)• O2 (no data)• Anticoagulation (controversial)
• Used in iPAH, fPAH and anorexigen related PAH• Digoxin (poor data)
• Can increase CO in PAH acutely (Chest 1998;114:787)• Anemia (common in PAH; poor data)
• Avoid blood transfusions (? Transplant); iron supplementation• No CCBs unless vasoreactive PAH (5-10%)
EHJ 2016;37:67-119

PAH-specific medications
NEJM 2004;351:1425
sGC
sGC activator
+

Endothelin Pathway
• Endothelin receptor antagonists (ERAs)• Bosentan (Tracleer); BID• Ambrisentan (Letairis); daily• Macitentan (Opsumit); daily
• Common SEs• LFT changes (mostly Bosentan)• Fetal toxicity• Anemia• Edema• Headache• Nasal congestion

NO pathway
• Phosphodiesterase type5 inhibitors (PDE5i)• Sildenafil (TID)• Tadalafil (daily or BID)
• Watch for Headache, flushing, epistaxis, myalgia
• Do not use with nitrates or Riociguat
• Soluble guanylate cyclase stimulator• Riociguat (TID, titrating to max dose)
• Similar SEs, + more systemic hypotension/syncope
• Do not use in pregnancy

Prostanoid pathway• IV and SQ
• Epoprostenol IV (synthetic prostacyclin)• Flolan (heat intolerance) and Veletri (more heat resistant)• Only PAH medication to have shown a mortality benefit in RCTs
• Treprostinil IV and SQ• Remodulin: more stable at room temperature (longer half-life/higher concentration)
• Inhaled• Iloprost (Ventavis): 6-9 treatments per day• Treprostinil (Tyvaso): QID
• Oral• Selexipag: prostanoid analogue, BID dosing• Treprostinil: TID dosing
Selexipag 0.8-2.5hmetabolite 6.2-13.5h


Basics of PAH/RV failure acute management
• Optimize fluid balance to decrease RV preload• Diuresis (almost always)
• Commonly hypotensive and tachycardic: NO IVF resuscitation
• Decrease RV afterload• PAH specific Rx: emergent IV prostanoid initiation if needed
• Pulmonary vasodilators: can cause systemic hypotension and VQ mismatch (hypoxia)
• Increase CO/CI:• Inotropes (dopamine or dobutamine)
• Avoid CCBs and BBs
• Maintain systemic BP to improve/maintain RV wall perfusion• Pressors (phenylephrine or norepinephrine)