Embed Size (px)
Citation preview

Public Perception of the Scope of Practice of
Oral & Maxillofacial Surgeons in Ontario
by
Oscar Dalmao
A thesis submitted in conformity with the requirements
for the degree of Master of Science in Oral and Maxillofacial Surgery
Discipline of Oral and Maxillofacial Surgery
Faculty of Dentistry
University of Toronto
© Copyright by Oscar Dalmao 2020

ii
Public Perception of the Scope of Practice of
Oral & Maxillofacial Surgeons in Ontario
Oscar Dalmao
Master of Science in Oral and Maxillofacial Surgery
Discipline of Oral and Maxillofacial Surgery
Faculty of Dentistry University of Toronto
2020
Abstract
Purpose: Investigate and compare the General Public’s, General Dentists’ and Primary Care Physicians’
level of knowledge of the scope of practice of Oral and Maxillofacial Surgeons (OMS). Materials and Methods: A mail-out survey of the General Public, General Dentists and Primary Care Physicians in
Ontario, Canada. Survey consisted of a screener along with 24 clinical scenarios. Responses
between groups were compared to identify any significant differences between subjects with P
value set at 0.05. Results: The majority of Dentists (100%) and Primary Care Physicians (95.5%) have heard of OMS, in
contrast only 73.7% of the General Public (p < 0.001). A general lack of awareness of OMS
scope of practice by all groups exists. Conclusion: A proportion of the General Public are unaware of OMS. More concerning, the General Public
and health professionals as a whole are unfamiliar with the full scope of practice of OMS.

iii
Acknowledgments
This work was supported by a Canadian Association of Oral and Maxillofacial Surgeons
Research Grant. I would like to thank my supervisor Dr. David Lam who provided me with the
mentorship and tremendous support throughout this master’s process. My sincerest gratitude also
goes to my committee members, Dr. Laura Dempster and Dr. Marco Caminiti for their guidance
and encouragement over the course of the project. Finally, thank you to my family and friends,
especially my girlfriend Dr. Lexi Corrigan for their love and support over the entire course of my
education!

iv
Table of Contents
Abstract……………………………………………………………………………………………ii
Acknowledgments………………………………………………………………………………..iii
Table of Contents…………………………………………………………………………………iv
List of Tables.…………………………………………………………………………………….vi
List of Figures……………………………………………………………………………………vii
List of Abbreviations……………………………………………………………………………viii
List of Appendices ……………………………………………………………………………….ix
Chapter 1. Introduction…………………………………………………………………………1
1.1. An Overview of Oral and Maxillofacial Surgery….....................................................1
1.2. Oral and Maxillofacial Practice vs Reality Gap...........................................................2
1.3. Perceptions of OMS Internationally……….................................................................2
1.4. Value of the Study........................................................................................................4
1.5. Purpose of the Study.....................................................................................................4
Chapter 2. Statement of Objectives and Hypothesis..................................................................6
2.1. Objectives....................................................................................................................6
2.2. Hypothesis....................................................................................................................6
Chapter 3. Public Perception of the Scope of Practice of
Oral & Maxillofacial Surgeons………………………………………………………………....7
3.1 Abstract………………………………………………………………………………..8
3.2 Introduction……………………………………………………………………………9
3.3 Materials and Methods………………………………………………………………10
3.4 Results………………………………………………………………………………..12
3.5 Discussion……………………………………………………………………………14
3.6 Conclusion…………………………………………………………………………...16
3.7 Acknowledgments…………………………………………………………………...16
3.8 References…………………………………………………………………………...17
3.9 Table/Figure Legends..………………………………………………………………21
Chapter 4. Discussion…………………………………………………………………………..48
6.1. Limitations …………………………………………..……………………………………..48
6.2. Implications, Future Directions………... ………………………………………………….49
References……………………………………………………………………………………….51
v
Appendices…………………………………………………………………………………….56
vi
List of Tables
Table 1 Clinical Scenario Questionnaire..……………………………...……………………….18
Table 2 Demographics.………………………………………………………………………….60
Table 3 OMS % selected per condition/scenario by all groups.………………………………...63
Table 4 OMS % selected per condition/scenario Family Physicians vs. General Dentists.…….64
Table 5 OMS % selected per condition/scenario General Public vs. General Dentists.………...65
Table 6 OMS % selected per condition/scenario Family Physicians vs. General Public……….66

vii
List of Figures
Figure 1. Awareness of Specialists……………………………………………………………23
Figure 2A. Fracture of the Upper Jaw……………………………………………………..……24
Figure 2B. Fracture of the Lower Jaw………………………………………………………..…25
Figure 2C. Fracture of the Nose……………………………………………………………...…26
Figure 2D. Fracture of the Eye……………………………………………………………….…27
Figure 2E. Fracture of the Cheek…………………………………………………………..……28
Figure 2F. Fracture of the Skull…………………………………………………………………29
Figure 2G. Cut on the face…………………………………………………………………….…30
Figure 3A. Cancer of the mouth, tongue or lip……………………………………………..……31
Figure 3B. Non-cancerous lesion of the mouth, tongue or lip……………………………...……32
Figure 3C. Non-cancerous tumor/cyst of the upper or lower Jaw…………………………….…33
Figure 3D. Removal of TMJ lesion………………………………………………………...……34
Figure 3E. Salivary Gland Removal………………………………………………………..……35
Figure 3F. Infection/swelling around the mouth/neck……………………….………………..…36
Figure 3G. Infection/swelling around the Eye………………………………….……………..…37
Figure 4A. Child with cleft lip…………………………………………………………….….….38
Figure 4B. Child with cleft palate……………………………………………………………..…39
Figure 4C. Soft tissue grafts for oral reconstruction…………………………………………..…40
Figure 4D. Hard tissue grafts for oral reconstruction……………………………………………41
Figure 5A. Removal of Wisdom teeth………………………………………………………...…42
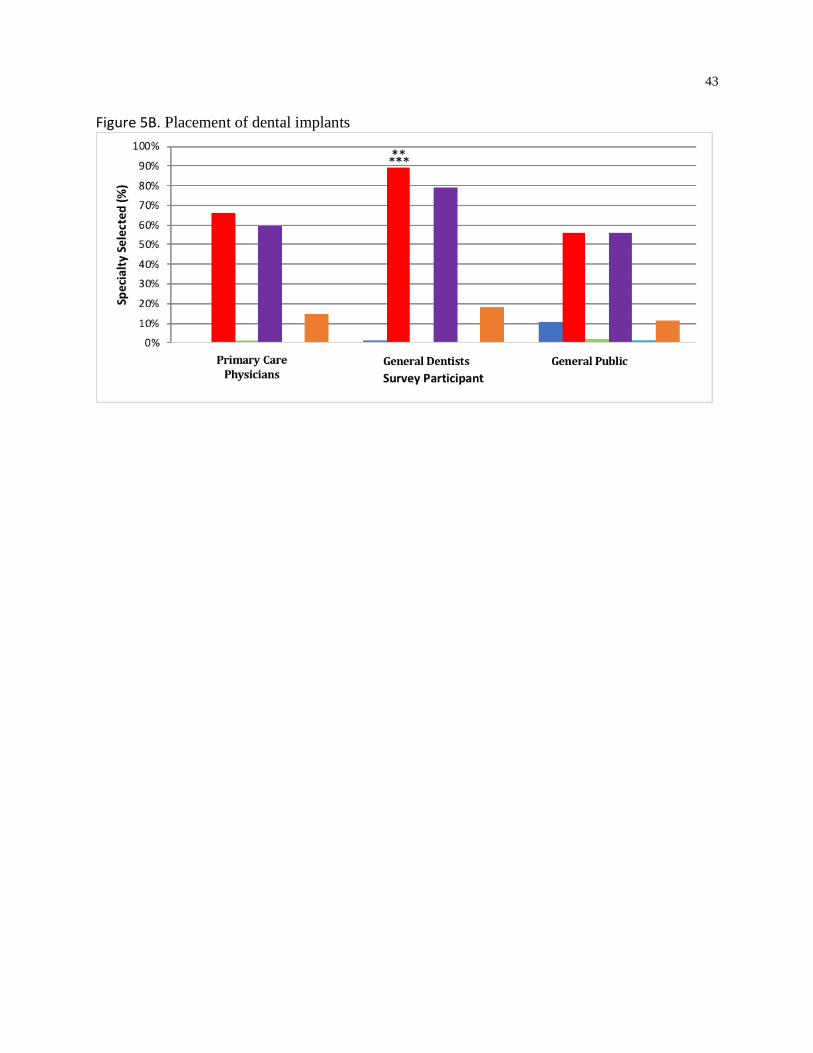
Figure 5B. Placement of dental implants………………………………...………………………43
Figure 5C. Providing general/deep sedation……………………………………..………………44
Figure 6A. Corrective Jaw surgery………………………………………………..…………..…45
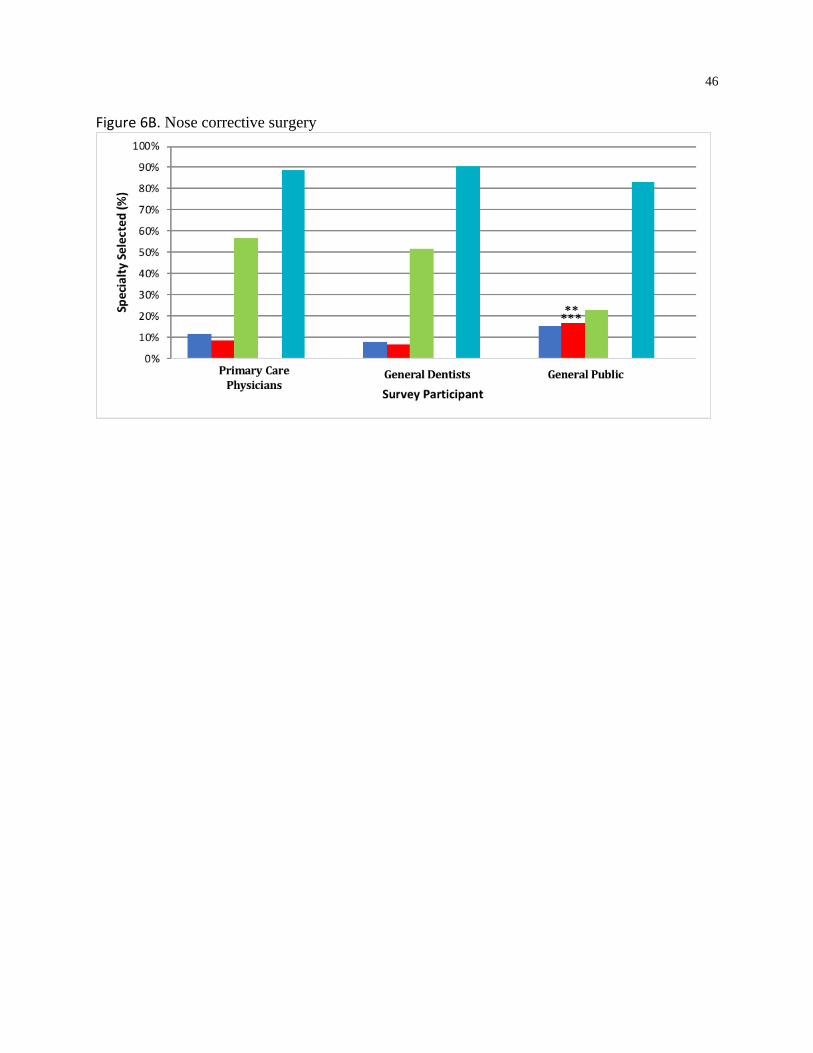
Figure 6B. Nose corrective surgery…………………………………………………..……….…46
Figure 6C. Facial appearance procedures…………………………………………………..……47

viii
List of Abbreviations
AAOMS American Association of Oral and Maxillofacial Surgeons
CAOMS Canadian Association of Oral and Maxillofacial Surgeons
CPSO College of Physicians and Surgeons of Ontario
DDS Doctor of Dental Surgery
ENT Otolaryngologist
GP General Public
GS General Surgeon
MD Doctor of Medicine
OMS Oral and Maxillofacial Surgeons
P Periodontist
PS Plastic Surgeon
RCDSO Royal College of Dental Surgeons of Ontario
UK United Kingdom
US United States of America

ix
List of Appendices
Appendix A. Additional Detailed Methodology……………………………………….………56
Appendix B. Additional Detailed Results………………………………………………..……..59
Appendix C. Initial Contact Letter……………………………………………………....……..67
Appendix D. Invitation to study participation…………………………………………………68
Appendix E. Information and Consent for Participation…………………………………..…69
Appendix F. Study Survey……………………………………………………...……………….71
1
1. Introduction
1. Oral and Maxillofacial Surgery
1.1. An Overview of Oral and Maxillofacial Surgery
Oral and Maxillofacial Surgery is a specialty of dentistry responsible for the diagnosis and
treatment of disorders, diseases, injuries, and defects involving the oral and maxillofacial
regions1, 2 In Canada, Oral and Maxillofacial Surgery can date its origins as far back as the early
20th century where W.G Beers limited his practice to exodontia and is often regarded as the first
Oral and Maxillofacial Surgeon (OMS) in Canada3. The profession continued to evolve and saw
rapid progression during the Second World War where Oral and Maxillofacial Surgery’s
importance as a specialty emerged4. Following this, in the mid-1950s the first three-year training
program in Oral and Maxillofacial Surgery was established at Toronto General Hospital5.
While the profession initially centered around the dentoalveolar complex, it has increasingly
been expanding its scope beyond that to complex facial surgeries6. Oral and Maxillofacial
Surgery training has become more specialized and skilled in a diverse range of treatments in the
maxillofacial anatomical region. This ranges from dentoalveolar procedures, to facial fractures,
craniofacial injuries, dental and skeletal deformities, salivary gland diseases, temporomandibular
disorders and oral and facial cancers with reconstruction by flaps and microvascular tissue
transfer7. The complex surgical procedures performed today follow extensive training that varies
worldwide8. In some countries, as it is in Canada, a dental degree only is required prior to further
Oral and Maxillofacial Surgery training. Once accepted into a Canadian Oral and Maxillofacial
Surgery training program, either a four-year single degree (DDS) or six-year dual degree (DDS/
MD) pathway are available. As in the United States these pathways are program-dependent and
not geographically-dependent. In contrast, in France and Spain, OMS applicants complete a
medical degree without any or little dental training. A combination of both medical and dental
training is required in other countries such as Australia and the United Kingdom (UK). In the
UK, OMS complete dental training prior to medical training in perhaps the lengthiest time to
graduate, taking approximately 18 years to qualify.
2
1.2. Oral and Maxillofacial Surgery Practice vs Reality Gap
The profession has continued to evolve; however, even with the extensive training in major
surgeries of the maxillofacial complex, until as recently as 1982 the Joint Commission on
Accreditation of Healthcare Organizations (a private sector US based non-profit organization
which accredits most US hospitals) still interfered with OMS practice in the hospital. OMS had
difficulty admitting or discharging their own patients or operating in a hospital setting unless
they were overseen by a medical colleague9. Due to Oral and Maxillofacial Surgery bridging the
fields of dentistry and medicine, confusion about the scope of practice has been present since its
inception10,11. Adding to the public’s confusion is the apparent overlap in the OMS scope of
practice with that of more routinely recognized medical specialties such as Plastic Surgery and
Otolaryngology12, 13. OMS require different credentials depending on where the degree is
obtained with countries such as Canada and the United states offering both four-year single
(DDS) and six-year dual (DDS/MD) degree programs, whereas most countries in Europe only
offer dual degree options8. This adds to lack of awareness not only by the public but the medical
community as well, with regards to the level of training that is required to obtain an Oral and
Maxillofacial Surgery degree. To add to that, the scope of Oral and Maxillofacial Surgery within
each individual country may vary by region, as is the case in Canada where cosmetic surgery
such as facelifts is practiced in Alberta but not in Ontario. In Ontario, which has the largest
number of practicing OMS in Canada, guidelines have been set through the Royal College of
Dental Surgeons of Ontario (RCDSO) to determine what procedures fall under the Oral and
Maxillofacial Surgery scope of practice in Ontario.
Even with the progressive steps made by the Oral and Maxillofacial Surgery profession in
education of the public in relation to its place in health care, there is a gap between the perceived
and actual scope of practice of OMS. Most studies completed internationally highlight the
ongoing limited perception by the public1, 7, 10, 12-16.
1.3. Perceptions of OMS Internationally
Geographic variations with respect to the awareness of OMS scope of practice exist.
Unfortunately, most studies suggest there is a lack of awareness of the Oral and Maxillofacial
Surgery specialty1, 10. An Australian survey found that most Family Physicians appropriately
referred cases to OMS when involving fractures of the maxilla, mandible or dentoalveolar

3
complex (75.5 to 92.2%). This drastically decreased with nasal fractures, frontal bone, zygomatic
fractures and lacerations to the face2.
In the UK, a questionnaire determined that out of its 200 General Public citizens, an astonishing
79% had not heard of Oral and Maxillofacial Surgery, compared to 17% that had not heard of
Plastic Surgery, or 46% of ENT. When asked what OMS do, 74% of the General Public
answered ‘Don’t Know’ with only 12% reporting that they work in the mouth. Both medical and
dental professionals showed better awareness of what the profession does; yet still lacked in
awareness of its scope in nasal and cleft lip and palate surgeries1. Ten years later, investigators
conducted a new study to compare their prior results. They found a slight improvement, yet
similar to before, only 34 of 100 people heard of OMS and none surveyed felt OMS could treat
patients unhappy with their facial appearance14.
In contrast, study participants in Florida showed greater recognition of OMS compared to those
in the UK6. Out of 300 General Public participants, 66% had heard of OMS. Similarly, a survey
conducted in India, that focused on the perceptions of medical workers and what OMS do
showed that all dental students and professionals had heard of Oral and Maxillofacial Surgery10
and that 41% of medical students, 76% of medical practitioners and 58% of paramedical workers
had heard of Oral and Maxillofacial Surgery10. However even with greater recognition, still less
than 15% of medical practitioners believed the OMS role included cleft lip and palate (14%),
cosmetic surgeries of the face (11%) and craniofacial anomalies (9%)10.
Even among undergraduate medical and dental students, which one would imagine would have
significant insight into Oral and Maxillofacial Surgery, exposure to a career in Oral and
Maxillofacial Surgery is limited17, 18. A review of the literature, found that a varied knowledge
base of Oral and Maxillofacial Surgery existed from limited in the UK and US to good in Brazil
among medical and dental students19 . Undergraduate medical students in the UK demonstrated a
lack of awareness of the OMS role in aesthetic facial surgeries and felt that certain conditions
such as face and neck infections, were better managed by specialties other than OMS17.
Interestingly in 1975, the American Society of the Oral and Maxillofacial Surgery profession
changed its name from ‘oral surgery’ to ‘oral and maxillofacial surgery20. The change was made
in an effort to more accurately describe the scope and to increase perception of the scope among
dental students. However, some suggest that the more recent name is unfamiliar to the General

4
Public and reported a reduced awareness of the scope of OMS among less-educated respondents
when compared to other specialties21.
1.4. Purpose of the Study
Public perceptions of OMS have only been studied in other geographic areas and have never
been investigated in Canada. Therefore, the purpose of this study was to examine this within
Ontario and see if perceptions held elsewhere also apply to the Canadian population.
The specific aims of the study were 1) to investigate the level of awareness of OMS in Ontario
by the General Public, General Dentists and Family Physicians and 2) to determine the level of
knowledge of the scope of practice of OMS throughout the Ontario population. We hypothesize
that there is a generalized lack of awareness of Oral and Maxillofacial Surgery and limited
knowledge of the scope of practice of OMS throughout the Ontario population, with the General
Public being the least informed and the General Dentists the most informed.
1.5. Value of the Study
It is imperative that the General Public have an awareness of OMS so that in time of need,
patients know where to seek treatment. With General Dentists and Family Physicians holding
key positions as gatekeepers for both appropriate dental and medical referrals, their
understanding is invaluable14. Having all parties adequately informed may allow for better access
to treatment and decrease wait times for patients. If all specialists who can perform a treatment
are recognized, more options will be available for patients and referring physicians to ensure the
population is able to receive care in the shortest possible time.
The results of this study have potential value to the specialty of Oral and Maxillofacial Surgery
and patients alike. Based on the results of this study, important information regarding the
public’s and health care professionals’ perception of OMS in Ontario will be gathered; this may
then be used to address areas where the OMS scope of practice perception is lacking so that
educational or promotional campaigns can be targeted. Beginning in 2014, American
Association of Oral and Maxillofacial Surgeons (AAOMS) created informational campaigns
costing approximately $4 million with goals to increase OMS awareness, inform and to convey
Oral and Maxillofacial Surgery's contributions to the general public22, 23. Using social media,

5
AAOMS made great strives to reach the public24. A website was developed with the patient in
mind using search engine optimization and providing informational videos on various common
procedures in Oral and Maxillofacial Surgery. AAOMS has received awards for this campaign
and effectively reached consumers. The Canadian Association of Oral and Maxillofacial
Surgeons (CAOMS) in contrast is lagging behind their American counterparts on this front. In
January 2019 the CAOMS executive committee along with the OMS resident representative met
and had discussions about creating a task force to determine the feasibility of undertaking a
national rebranding and educational campaign such as the one conducted by AAOMS. At that
time, only discussions were held and no definitive plans were put in place. Similarly, the Ontario
Society of Oral and Maxillofacial Surgeons is currently establishing a scope of practice steering
committee but has not finalized anything yet 25. Results from our study may elucidate areas in
which the specialty of Oral and Maxillofacial Surgery can focus on to enhance its importance as
a specialty in the public eye before these campaigns are put into effect. Identifying gaps in
awareness of scope will continue to help determine areas to focus on, to optimize the pathway to
care and prioritize complex treatments for patients. This may also help or alter government
funding where appropriate.
As well, further expansion of the Oral and Maxillofacial Surgery profession depends on ensuring
the referral pathways are consolidated to support this expansion. The majority of referral bases
continue to come from dentists, which may help explain the vast proportion of dentoalveolar
work. If a disconnect is identified in participant groups with respect to oral vs extraoral
procedures for OMS, steps can be made to highlight OMS expertise in procedures of the facial
complex, not just the dentoalveolar one. This may help increase referrals from both medical and
dental professionals and promote continued expansion of treatment beyond just the dental
complex, which is what OMS are truly trained for.
6
Chapter 2 Statement of Objectives and Hypothesis
2. Statement of Objectives and Hypothesis
2.1. Objectives
1) To determine the level of awareness of the specialty of Oral and Maxillofacial Surgery by
the General Public, General Dentists and Family Physicians in Ontario.
2) To investigate the level of knowledge of the scope of practice of Oral and Maxillofacial
Surgeons (OMS) throughout the Ontario population, including the General Public, General
Dentists and Family Physicians, and determine if there is a significant difference between
these groups.
2.2. Hypotheses
1) Health care professionals (General Dentists and Family Physicians) are more aware of the
Oral and Maxillofacial Surgery specialty than the General Public.
2) There is a generalized lack of knowledge of the scope of practice of OMS throughout the
Ontario population and the level will vary with the General Dentists being the most
informed and the General Public the least.

7
Chapter 3
3. Public and Professional Perceptions of the Scope of
Practice of Oral & Maxillofacial Surgeons Manuscript submitted to Journal of Oral and Maxillofacial Surgery
Oscar E. Dalmao DDS,a Laura J. Dempster BSc. D (DH), MSc, PhD,b Marco F. Caminiti DDS,
MEd, FRCD(C),c Nick Blanas DDS, FRCD(C)1,d David K. Lam MD, DDS, PhD, FRCD(C).e
a Chief Resident, Oral & Maxillofacial Surgery, Faculty of Dentistry, University of Toronto, 124
Edward Street, Toronto, Ontario, Canada M5G 1G6
b Associate Professor, Dental Public Health, Faculty of Dentistry, University of Toronto, 124
Edward Street, Toronto, Ontario, Canada M5G
c Program Director, Oral & Maxillofacial Surgery, University of Toronto, 124 Edward Street,
Toronto, Ontario, Canada M5G 1G6
d Assistant Professor, Oral & Maxillofacial Surgery, University of Toronto, 124 Edward Street,
Toronto, Ontario, Canada M5G 1G6
e Professor & Chairman, Departments of Surgery and Oral & Maxillofacial Surgery, Stony Brook
Medicine, Stony Brook, NY
Corresponding Author: Oscar Dalmao
Oral & Maxillofacial Surgery, University of Toronto, 124 Edward Street, Room 143, Toronto,
Ontario, Canada M5G 1G6
Telephone: 416-979-4922 Ext 4329
Fax: (416) 979-4936
Email: [email protected]

8
3.1 Abstract
Purpose:
To investigate and compare the General Public’s, General Dentists’ and Primary Care Physicians’
level of knowledge of the scope of practice of Oral and Maxillofacial Surgeons (OMS). We
hypothesized that there is a generalized lack of knowledge of the scope of practice of OMS, with the
General Public being the least informed and the General Dentists the most informed.
Materials and Methods:
A cross-sectional survey study was conducted, via a mail-out survey that was delivered to a
random sample of the General Public, General Dentists and Primary Care Physicians in Ontario,
Canada. A total of 1800 participants were selected. The survey consisted of a demographic
screener along with 24 clinical scenarios in which the participants could select all the specialists
they thought were capable of completing the treatment. Inferential statistics were computed
using a chi-square test to compare responses between the groups and identified any significant
differences between participants for each of the 24 scenarios with P value set at 0.05.
Results:
Total response rate of 50.1% (n=902) was achieved. The majority of health professionals (100%
Dentists, 95.5% Primary Care Physicians) have heard of OMS, in contrast to only 73.7% of the
General Public (p < 0.001). There was a general lack of awareness of OMS scope of practice by
all groups wherein OMS were selected less than 50% of the time in 10 (General Dentists), 14
(Primary Care Physicians) and 16 (General Public) of 24 clinical scenarios.
Conclusion:
Greater than 25% of the General Public are unaware of OMS. More concerning, the General
Public and health professionals as a whole are unfamiliar with the full scope of practice of
OMS. To enhance access to care by qualified specialists, educational programs highlighting key
aspects of OMS should be developed and distributed to all populations.

9
3.2 Introduction
Oral and Maxillofacial Surgery is a specialty of dentistry responsible for the diagnosis and
treatment of disorders, diseases, injuries, and defects involving the oral and maxillofacial
regions1,2. In Canada, Oral and Maxillofacial Surgery can date its origins as far back as the early
20th century3. The profession has continued to evolve; however due to it bridging the fields of
dentistry and medicine, confusion about Oral and Maxillofacial Surgeons (OMS) scope of practice
has been present since its inception4. Adding to the public’s confusion is the apparent overlap in
the OMS scope of practice with that of more routinely recognized medical specialties such as
Plastic Surgery and Otolaryngology5,6. Even with the progressive steps made by the Oral and
Maxillofacial Surgery profession in education of the public in relation to its place in health care,
most studies completed internationally highlight the ongoing lack of knowledge of the scope of
practice by the public1,4-9.
The level of knowledge of the scope of OMS has only been studied in other geographic areas
but not in Canada, therefore the aim of this study was to examine the level of knowledge within
Ontario, Canada. The purpose of the study was to investigate the level of awareness of Oral and
Maxillofacial Surgery as a profession and the level of knowledge of the scope of practice of OMS
among the General Public, General Dentists and Primary Care Physicians.

10
3.3 Materials and Methods
A mail-out survey was delivered to a random sample of the General Public, General Dentists and
Primary Care Physicians in Ontario. Primary Care Physicians and General Dentists are usually
the ones who will be consulted first for a head, neck or oral complaint and thus have the
responsibility of making the appropriate referral8,10. They act as potential gatekeepers to
OMS, which is why these two groups along with the General Public who may request their
own referral were surveyed. Ethics approval was obtained from the University of Toronto
Research Ethics Boards (34462). A total of 1800 participants were selected, with 600 per group.
Inclusion criteria:
1. General Public (GP): Adults over the age of 18 who are neither medical nor dental
professionals and living in Ontario.
2. General Dentist (DDS): Any general dentist with a valid provincial dental license
(RCDSO).
3. Primary Care Physician (MD): Any primary care physician with a valid provincial
medical license (CPSO).
Survey Questionnaire
The survey consisted of demographic questions including gender, age and whether participants
were physicians, dentists, or members of the public. Survey participants were asked if they had
heard of, or been treated by specific specialists (General surgeon, ENT (Otolaryngologist), OMS,
Plastic Surgeon, and Periodontist), along with 24 clinical scenarios in which the participants could
select all the above specialists, along with an “Other” option, they thought were capable of
completing the described treatment (Table 3.1). The 24 clinical scenarios where chosen to
encompass the full scope of Oral and Maxillofacial Surgery and similar to previous studies, were
grouped into five categories; Trauma, Pathology, Reconstructive Surgery, Oral Procedures and
Cosmetics5,8.
Data Collection
To maximize participant response rate, an initial contact letter was sent out to inform potential
participants of their selection to partake in our study. This was done to prime participants for the

11
upcoming survey. In addition, surveys were sent out in three separate waves along with follow up
reminder phone calls to all non-responders.
Data Analysis
Descriptive statistics reported demographic data. Inferential statistics via a chi-square test
compared responses between the General Public, Primary Care Physicians, and General Dentists
to identify any significant differences between subjects. Subsequent chi- square tests were
completed between individual groups when significant differences were identified between the 3
groups. To account for type 1 error, a Bonferroni correction was completed and the level of
significance was set at p < 0.0167.

12
3.4 Results
An overall response rate of 50.1% (n=902) was achieved: 259 (43.1%) General Public, 332
(55.3%) General Dentists, and 311 (51.8%) Primary Care Physicians. The average age of the entire
survey population was 49.4±13.5 years with no significant difference between groups. A
significant difference in gender composition (p< 0.01) was evident with the General Dentist
population (67.5%) having a higher male percentage compared to both for Primary Care
Physicians (57.9%) and the General Public (54.1%). Most health care professionals (95.5%
Primary Care Physicians, 100% General Dentists) were aware of OMS, in contrast to 73.7% of the
General Public (p<0.001, Figure 1). Primary Care Physicians and the General Public selected
General Surgeons as the specialty that had treated them the most with 25.4% and 30.9%,
respectively, while General Dentists selected OMS with 26.5%.
In the broad scope of practice encompassed by the 24 clinical scenarios, OMS were selected 42.3%
by the General Public, 42.8% by Primary Care Physicians, and 60.8% by General Dentists
(p<0.001).
Trauma Scenarios
The majority of participants selected OMS for treatment of maxillary (74.9-99.1%, Figure 2A) and
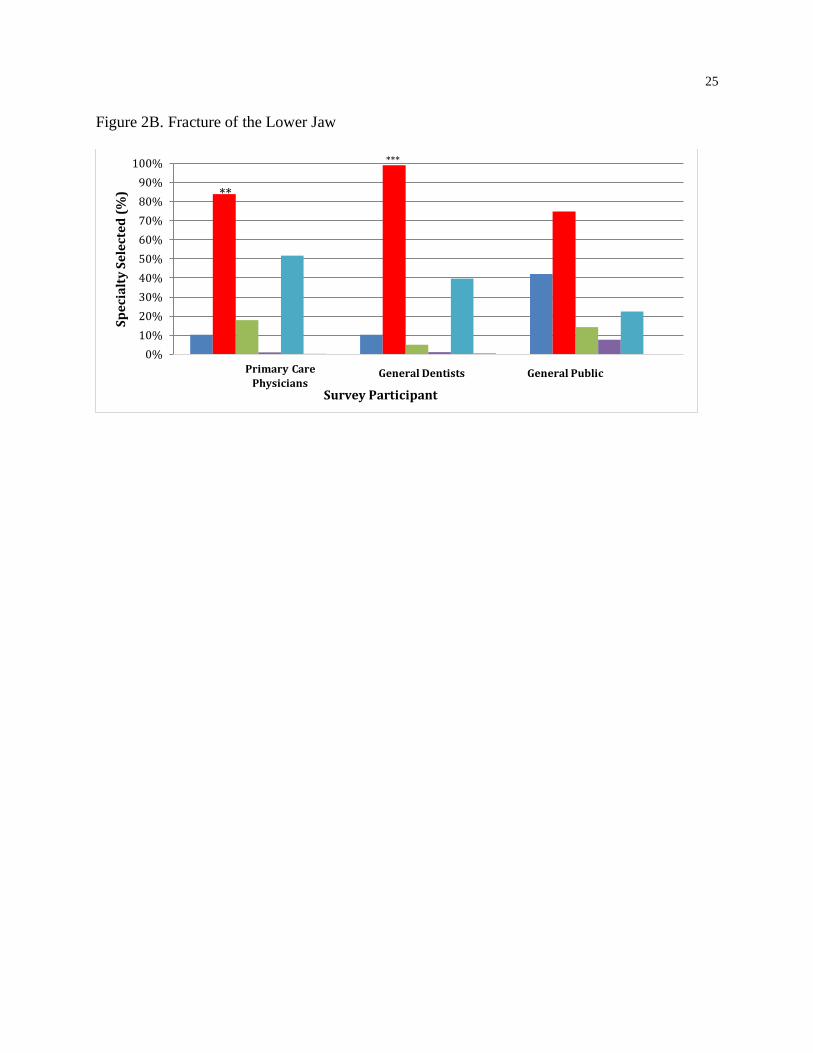
mandibular fractures (65.5-77.4%, Figure 2B). With regards to the remainder of maxillofacial
trauma scenarios, Plastic Surgeons were the dominant selection for treatment of facial lacerations
(81-94.5%, Figure 2G), as well as nasal (63.2-77.5%, Figure 2C), orbital (45.7-78.8%, Figure 2D),
and zygomatic fractures (48.8-78.5%, Figure 2E).
Pathology Scenarios
For clinical situations involving pathology of the head and neck, ENT was the dominant selection
for cancerous lesions (43.0-86.8%, Figure 3A). OMS were the primary selection for noncancerous
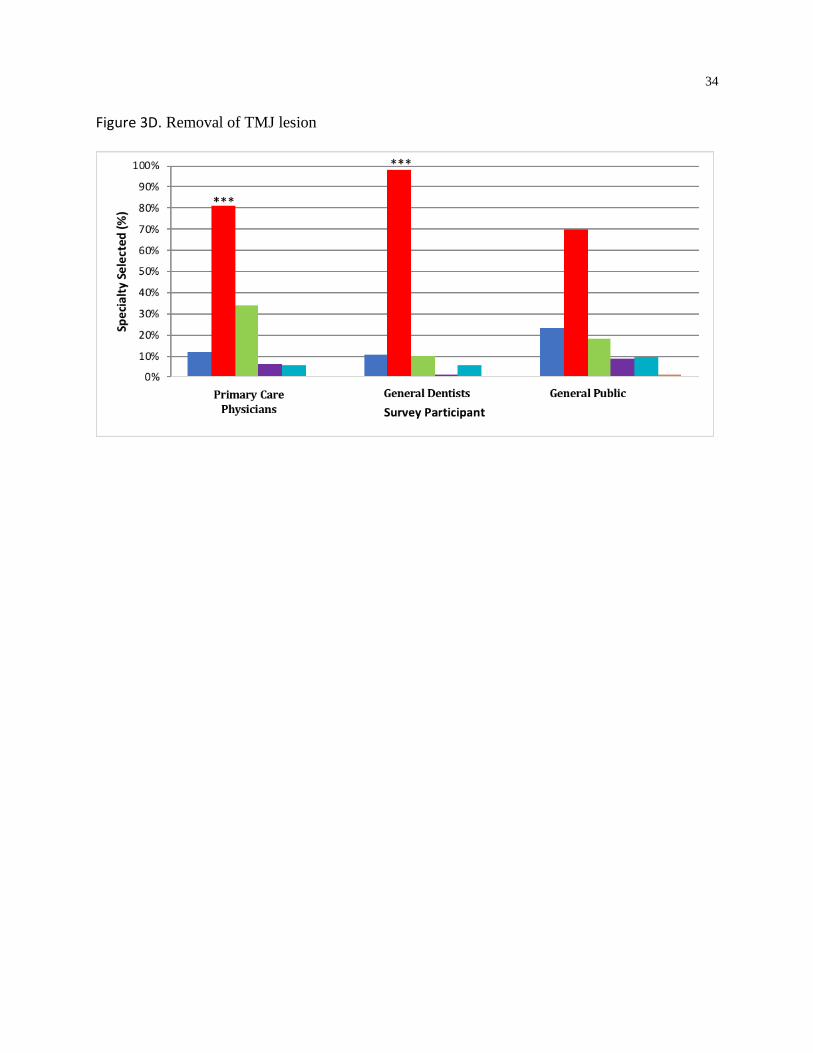
lesions (52.3-94.3%, Figure 3B), noncancerous cysts/tumors (60.5-97.0%, Figure 3C) and TMJ
pathology (69.5-98.2%, Figure 3D). Salivary gland pathology and infections/swellings around the
neck/mouth had mixed results with OMS selected the most by General Dentists (71.1%, Figure 3E
and 46.7%, Figure 3F, respectively) and the General Public (93.7%, Figure 3E and 45.2% Figure
3F, respectively), while the Primary Care Physicians selected ENT the most for both scenarios
13
(81.4%, Figure 3E and 75.2%, Figure 3F respectively). General Surgeons were selected the most
for infections/swellings around the eye by all survey participant groups (65.9-72.6%, Figure 3F).
Reconstructive Surgery Scenarios
All survey participant groups selected Plastic Surgeons the most for reconstructive surgery
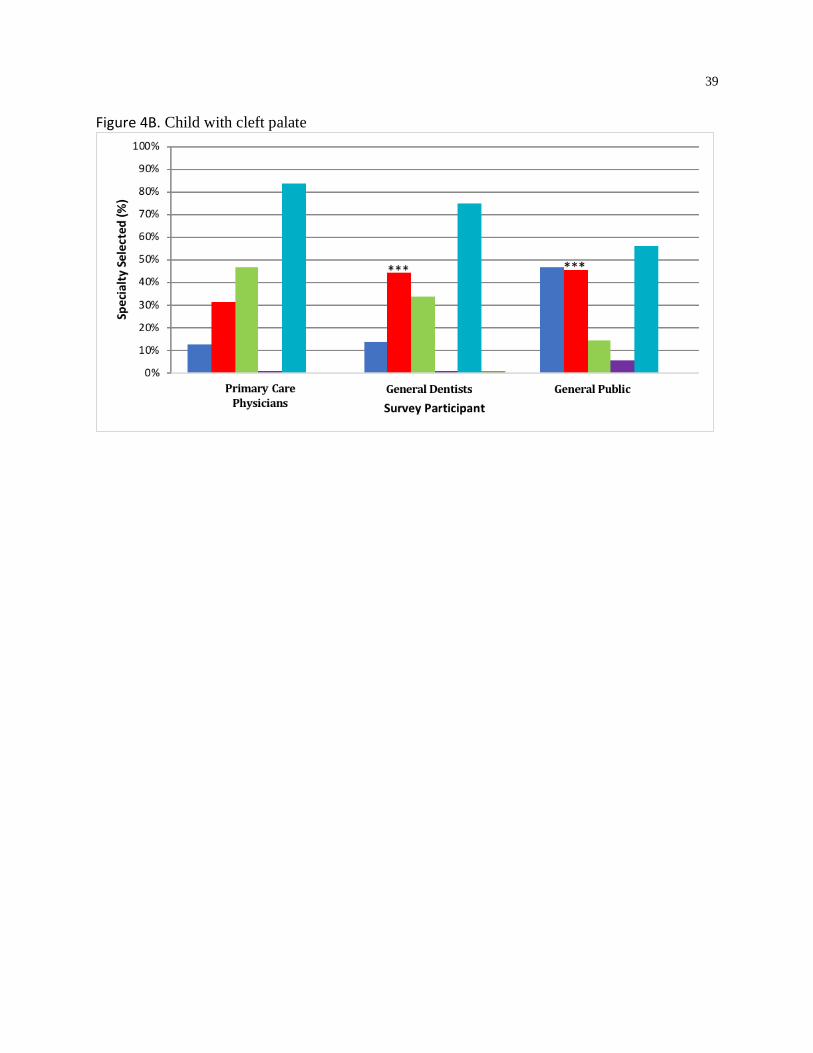
scenarios involving cleft lip (64.5-89.1%, Figure 4A) or cleft palate (56.0-89.1%, Figure 4B).
Primary Care Physicians also selected Plastic Surgeons the most for reconstruction of oral
structures with soft or hard tissue (66.9%, Figure 4C and 62.4%, Figure 4D, respectively). General
Dentists selected Plastic Surgeons for soft tissue procedures (66.3%, Figure 4C) and OMS for hard
tissue procedures (59.0%, Figure 4D). The General Public selected OMS the most for both soft
and hard tissue procedures (48.2%, Figure 4C and 44.8%, Figure 4D, respectively).
Oral Procedure Scenarios
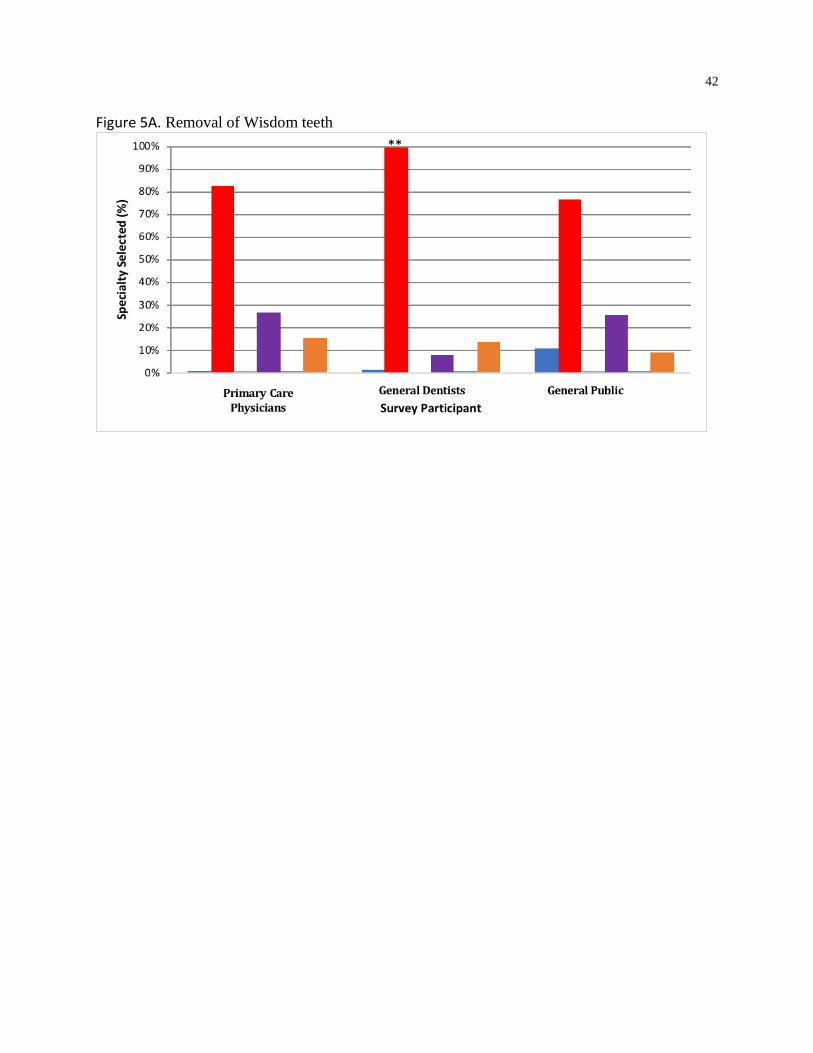
Oral procedures such as wisdom teeth extractions (76.4-99.4%, Figure 5A) and dental implants
(56.4-88.9%, Figure 5B) had a predominantly OMS selection. OMS were selected to provide
anaesthesia by both Primary Care Physicians (50.8%) and General Dentists (86.4%) but not
by the General Public who selected General Surgery the most (54.4%) (Figure 5C).
Cosmetic Scenarios
Jaw corrective surgery was the only cosmetic scenario, which had OMS as the primary selection
(58.3-97.0%) by all survey participant groups (Figure 6A). Nose corrective procedures (83.4-
90.7%, Figure 6B) and facial cosmetic procedures (92.7-98.8%, Figure 6C) had Plastic Surgery as
the highest selection by all survey participant groups

14
3.5 Discussion
The goal of health care is to provide optimal care for patients, including providing patients with
access to care by all surgical specialties capable of providing them care. This ensures that patients
can make the most educated decision. For this to occur, there must be a sound understanding of
the Oral and Maxillofacial Surgery specialty by medical and dental professionals, and the public
so that appropriate referrals are made, leading to effective and efficient treatment for the public1,5.
In our study, the level of awareness of Oral and Maxillofacial Surgery by the General Public
(73.7%) is on the higher end compared to similar international studies that range from 15-83%1,4-
9. Yet, this is significantly lower than health professionals in this study (100% of General Dentists
and 95.5% of Primary Care Physicians). Of greater clinical importance is the limited familiarity
with Oral and Maxillofacial Surgery's full scope of practice, even by General Dentists. This was
demonstrated by the fact that for the majority of the 24 clinical scenarios, OMS were selected less
than 50% of the time and were the highest selection in only 33%, 50% and 42% of the 24 clinical
scenarios by the Primary Care Physicians, General Dentists and General Public groups,
respectively. As anticipated, General Dentists had higher selection than both the Primary Care
Physicians and the General Public for OMS. Our findings suggest there is a lack of awareness of
the full scope of practice of OMS with a distinction occurring between scenarios limited to the oral
cavity versus those occurring outside of it.
Our study was able to highlight recognition of OMS in providing treatment for maxillary and
mandibular trauma, pathology (involving benign lesions and TMJ conditions), cosmetic treatment
via jaw corrective surgery, and oral procedures (such as wisdom teeth extractions and implants).
All of the conditions that had a high OMS selection were related to the dentoalveolar complex.
This is in keeping with previous studies conducted internationally both in the UK, Kuwait and
India.4,7,9
On the other hand, scenarios within the head and neck that fell outside the oral complex usually
had a diminished OMS selection, with one of the medical specialties ENT, Plastic Surgery or
General Surgery favoured. Similar to prior studies by Rocha and colleagues in Brazil, and Hunter
and colleagues in the USA, Plastic Surgeons were selected for treatment of facial lacerations over
OMS5,8. Rocha and colleagues, and Hunter and colleagues had OMS as the primary selection for
zygomatic fractures, however in our study orbital and zygomatic fractures had Plastic Surgery as

15
the most favoured selection 5,8. In keeping with prior studies, ENT was selected for malignant and
salivary gland pathologies, and Plastic Surgery was selected for cosmetic procedures 4,5,8,9.
Various reasons for this lack of awareness have been proposed in the past. Ameerally and
colleagues felt that the name, “OMFS” is confusing for the lay person1. Hunter and colleagues
reasoned that the lack of awareness stems from the fact that the foundation of Oral and
Maxillofacial Surgery is in dentistry and not medicine5. Since referrals in Canada are largely from
General Dentists, oral-related procedures such as wisdom tooth extractions, represent a significant
proportion of work for OMS. Perhaps, it therefore makes sense that the perception by the General
Public in Ontario, of the scope of OMS, is misconstrued to largely oral-related procedures. We
suspect that this also contributes to a diminished awareness of the scope of OMS in a hospital
setting or procedures beyond the mouth. There is also significant overlap among specialties of
Plastic Surgery, ENT and Oral and Maxillofacial Surgery. In addition, regional variations in the
scope of practice exist in Canada as they do in the rest of the world. In certain locations or certain
hospitals, one discipline may take the responsibility for a condition over another and this may
change in another location. This only adds to the confusion of the scope of OMS.
Regardless of why this diminished perception of the scope of practice is present, the aim must be
to have these perceptions changed. Informational campaigns such as the one conducted by
AAOMS which had the goals to increase the public perception of the OMS scope of practice,
inform prospective patients of OMS education and training, and convey the specialty’s
contributions to public health should be carried out in Canada13. Educational videos, consumer
website and public service announcements were all used to address the issues and resulted in very
positive feedback as evident by the 26 awards that were granted to AAOMS for this campaign13.
In addition, implementing teaching that illustrates what OMS can do into both dentists
and physicians’ curriculum during their training would be beneficial. This would allow the
establishment of knowledge at the grass roots level, when practitioners are most receptive to new
ideas. If physicians and dentists exit their training programs with this knowledge in place, all future
campaigns will only reinforce what they have already been taught, instead of being the initial
exposure to this information.

16
Study Strengths and Limitations
Mailed surveys, as all surveys must address the issue of inadequate response rate, however
strategies to enhance this were used resulting in an overall favorable response rate of 50.1%11,12.
The random selection of participants also ensured equal representation among the participant
groups. A mailed survey was also beneficial in our study as email directories where either too
costly or not expansive enough for our chosen subject groups.
The study was restricted to participants in Ontario; therefore the results cannot be generalized to
awareness of OMS across Canada. However, since Ontario is the largest province with the greatest
number of Oral and Maxillofacial Surgeons, one could expect that the awareness reported in
Ontario represents the greatest potential recognition and exposure that would be reported
nationally.
3.6 Conclusion
The results of this study suggest a low level of awareness among the General Public, General
Dentists and Primary Care Physicians in Ontario of OMS full scope of practice. Although
varying levels of awareness have been reported previously in international studies, the theme
remains that people don’t know what the full OMS scope entails. Greater progress needs to be
made in the education of Primary Care Physicians, General Dentists and the General Public, if
the specialty of Oral and Maxillofacial Surgery is to be practiced to its full potential and patients
are to benefit from access to care by highly qualified specialists5,10. Future steps should include
advocacy efforts at all levels including the OMS individual, institutional and association levels.
Focus needs to be placed on key areas such as trauma and pathology where patient care is crucial
and may be expedited if all those involved are aware of what OMS can perform. In addition
procedures that were selected the least based on survey results including facial lacerations,
salivary gland pathology, cleft lip and palate reconstruction and facial cosmetic procedures
should also be highlighted. Ongoing education and advocacy is imperative for increased
awareness of the scope of OMS and therefore improved patient care, access to care and
efficiency of care
3.7 Acknowledgements
This study was supported by a Canadian Association of Oral and Maxillofacial Surgeons
Research Grant.

17
3.8 References
1. Ameerally P, Fordyce AM., Martin, IC: So you think they know what we do? The public and
professional perception of oral and maxillofacial surgery. Br J Oral Maxillofac Surg 32:142,
1994
2. Lababidi E, Breik O, Subramaniam S: Perceptions of oral and maxillofacial surgery amongst
Australian medical general practitioners. Oral Maxillofac Surg Oral Med Oral Pathol 30:229–
232, 2018
3. Weinberg S. (2003, May 1) The End of an Era. Retrieved from
https://www.oralhealthgroup.com/features/the-end-of-an-era
4. Subhashraj K, Subramaniam B: Awareness of the specialty of oral and maxillofacial surgery
among health care professionals in Pondicherry, India. J Maxillofac Oral Surg 66:2330–4,
2008
5. Hunter MJ, Rubeiz T, Rose L: Recognition of the scope of oral and maxillofacial surgery by
the public and health care professionals. J Oral Maxillofac Surg 54:1227, 1996
6. Farook SA, Rihal K, Abullakutty A, Coombes D: Lost tribe? Awareness of oral and
maxillofacial surgery (OMFS) among the general public. Br J Oral Maxillofac Surg 51:e4–e5,
2013
7. Ifeacho SN, Malhi GK, James G: Perception by the public and medical profession of oral and
maxillofacial surgery—Has it changed after 10 years? Br J Oral Maxillofac Surg 43:289, 2005
8. Rocha NS, Laureano Filho JR, Silva ED, Almeida RC. Perception of oral maxillofacial surgery
by healthcare professionals. Int J Oral Maxillofac Surg 37:41– 46, 2008
9. Haron, IM, Sabti MY, Andersson L, Sharma PN. Perception of oral and maxillofacial surgery
by medical and dental health care professionals in Kuwait. J Oral Maxillofac Surg Med Oral
Pathol 25:5–11, 2013
10. Vadepally AK, Sinha R, Uppada UK, Rama Krishna Reddy BV, Agarwal A: Oral and
maxillofacial surgery: Perception of its scope among the medical fraternity and general
public. J Cranio Max Dis 4:21-7, 2015
11. Brtnikova M, Crane LA, Allison MA, Hurley LP, Beaty BL, Kempe: A method for achieving
high response rates in national surveys of U.S. primary care physicians. PLoS ONE 13(8),
2018
12. Asch DA, Jedrziewski MK, Christakis NA: Response rate to Mail Surveys Published in
Medical Journals. J Clinic Epidemiol 50:1129-1136, 1997

18
Table 1. Clinical Scenario Questionnaire
Conditions/ Procedures
General Surgeon
Periodontist Plastic Surgeon
Oral and Maxillofacial Surgeon
Otolaryngologist (ENT)
Other (please specify)
Trauma:
1. Fracture of the upper jaw (broken upper jaw)
2. Fracture of the lower jaw (broken lower jaw)
3. Fracture of the nose (broken nose)
4. Fracture of the eye bones
5. Fracture of the cheek bones
6. Fracture of the skull
7. Cut on the face
Pathology:
8. Cancer of the mouth, tongue or lip
9. Non cancerous lesion of the mouth, tongue or lip
10. Non cancerous tumor/cyst of the upper or lower jaw
11. Removal of temporomandibular joint (TMJ) lesions (Jaw Joint lesions)

19
12. Salivary Gland removal
13. Infection/swelling around the mouth/neck
14. Infection/swelling around the eye
Conditions/ Procedures
General Surgeon
Periodontist Plastic Surgeon
Oral and Maxillofacial Surgeon
Otolaryngologist (ENT)
Other (Please specify)
Reconstruction:
15. Child with cleft lip (improperly joined lip)
16. Child with cleft palate (improperly formed/joined roof of the mouth)
17. Soft tissue (skin, fat, muscle) grafts for oral reconstruction (taking soft tissue to rebuild the oral cavity)
18. Hard tissue (hip, tibia and skull bone) grafts, for oral reconstruction (taking bone tissue to rebuild the oral cavity)
Oral Procedures:
19. Removal of wisdom teeth (3rd molars)
20. Placement of Dental implants
20
21. Providing general anesthesia/deep sedation (putting patients to sleep during dental procedures)
Cosmetic
22. Jaw corrective surgery
23. Nose corrective surgery
24. Facial appearance procedures. (facelift, eyebrow lift, Botox, chemical peels etc..)

21
3.9 Table / Figure Legends:
Table 1. Clinical Scenario Questionnaire. Study participants were asked to review all the surgical
conditions/procedures listed in the table below and select which specialist(s) they thought were
competent (capable) of dealing with each condition.
Figure 1. Awareness of Specialists. The percentage that each of the survey participants were aware of
the following specialists: General Surgeon (GS), Oral and Maxillofacial Surgeon (OMS),
Otolaryngologist (ENT), Periodontist (P), and Plastic Surgeon (PS), is displayed. A total of 95.5% of
Primary Care Physicians, 100% of General Dentists, and 73.7% of General Public were aware of OMS
(*** p<0.001, Primary Care Physicians vs General Public; *** p<0.001, General Dentists vs General
Public).
Figure 2. Trauma Scenarios. Survey participants selected all the specialists they thought were
capable of treating each trauma scenario: (A) Fracture of the Upper Jaw (** p<0.01, Primary Care
Physicians vs General Public; ** p<0.01, General Dentists vs General Public), (B) Fracture of the Lower Jaw .
(** p<0.01, Primary Care Physicians vs General Public; *** p<0.001,General Dentists vs Primary Care Physicians;
*** p<0.001, General Dentists vs General Public), (C) Fracture of the Nose, (D) Fracture of the Eye Bones,
(E) Fracture of the Cheek Bones (** p<0.01, General Dentists vs Primary Care Physicians; ** p<0.01, General
Dentists vs General Public; ** p<0.01, General Public vs Primary Care Physicians), (F) Fracture of the Skull ( ***
p<0.001, General Public vs Primary Care Physicians), and (G) Cut on the Face (** p<0.01, Primary Care
Physicians vs General Public; ** p<0.01, General Dentists vs Primary Care Physicians; *** p<0.001, General
Dentists vs General Public). Primary Care Physicians, General Dentists and General Public selected OMS
the most for treating fractures of the upper and lower jaws.
Specialities are represented by the following colors; General Surgeon, Oral and Maxillofacial
Surgeon, Otolaryngologist, Periodontist, Plastic Surgeon.
Figure 3. Pathology Scenarios. Survey participants selected all the specialists they thought were
capable of treating each pathology scenario: (A) Cancer of mouth, tongue, or lip (*** p<0.001, General
Dentists vs Primary Care Physicians; ** p<0.01, General Public vs Primary Care Physicians), (B) Non-Cancerous
lesion of mouth, tongue, or lip ( *** p<0.001, General Dentists vs Primary Care Physicians; *** p<0.001, General
Dentists vs General Public), (C) Non-Cancerous tumor/cyst of the Upper or Lower Jaw (*** p<0.001, Primary
Care Physicians vs General Public; *** p<0.001, General Dentists vs Primary Care Physicians; *** p<0.001, General
Dentists vs General Public), (D) Removal of TMJ Lesions (*** p<0.001, Primary Care Physicians vs General Public;
** p<0.01, General Dentists vs Primary Care Physicians; *** p<0.001, General Dentists vs General Public), (E)
Salivary Gland Removal (*** p<0.001, General Dentists vs Primary Care Physicians; *** p<0.001, General Dentists
vs General Public; ** p<0.01, General Public vs Primary Care Physicians), (F) Infection/Swelling around
Mouth/Neck (** p<0.01, Primary Care Physicians vs General Public; *** p<0.001, General Dentists vs Primary Care
Physicians; *** p<0.001, General Dentists vs General Public), and (G) Infection/Swelling around Eye (***
p<0.001, General Dentists vs Primary Care Physicians; *** p<0.001, General Public vs Primary Care Physicians).
Primary Care Physicians, General Dentists and General Public selected OMS the most for treating
Non-Cancerous tumor/cyst of the Upper or Lower Jaw, and Removal of TMJ Lesions.
Specialities are represented by the following colors; General Surgeon, Oral and Maxillofacial
Surgeon, Otolaryngologist, Periodontist, Plastic Surgeon.

22
Figure 4. Reconstructive Surgery Scenarios. Survey participants selected all the specialists they
thought were capable of performing each reconstructive surgery scenario: (A) Child with Cleft Lip
(*** p<0.001, General Dentists vs Primary Care Physicians; *** p<0.001, General Public vs Primary Care Physicians),
(B) Child with Cleft Palate (*** p<0.001, General Dentists vs Primary Care Physicians; *** p<0.001, General Public
vs Primary Care Physicians), (C) Soft Tissue Grafts for Oral Reconstruction (*** p<0.001, General Dentists vs
Primary Care Physicians; ** p<0.01, General Public vs Primary Care Physicians), and (D) Hard Tissue Grafts for
Oral Reconstruction (** p<0.01, General Dentists vs Primary Care Physicians; ** p<0.01, General Dentists vs
General Public, ** p<0.01, General Public vs Primary Care Physicians). Primary Care Physicians did not select
OMS highly for any reconstruction surgery scenario.
Specialities are represented by the following colors; General Surgeon, Oral and Maxillofacial
Surgeon, Otolaryngologist, Periodontist, Plastic Surgeon.
Figure 5. Oral Procedure Scenarios. Survey participants selected all the specialists they thought
were capable of performing each oral procedure scenario: (A) Removal of Wisdom Teeth ( ** p<0.01,
General Dentists vs General Public), (B) Placement of Dental Implants ( ** p<0.01, General Dentists vs Primary
Care Physicians; *** p<0.001, General Dentists vs General Public), and (C) Providing General/Deep Sedation (*** p<0.001, Primary Care Physicians vs General Public; *** p<0.001, General Dentists vs Primary Care Physicians; ***
p<0.001, General Dentists vs General Public). Primary Care Physicians, General Dentists and General Public
selected OMS the most for removal of wisdom teeth and placement of dental implants.
Specialities are represented by the following colors; General Surgeon, Oral and Maxillofacial
Surgeon, Otolaryngologist, Periodontist, Plastic Surgeon.
Figure 6. Cosmetic Scenarios. Survey participants selected all the specialists they thought were
capable of performing each cosmetic scenario: (A) Jaw Corrective Surgery (*** p<0.001, Primary Care
Physicians vs General Public; * p<0.05, General Dentists vs Primary Care Physicians; *** p<0.001, General Dentists vs
General Public), (B) Nose Corrective Surgery (** p<0.01, General Public vs Primary Care Physicians; *** p<0.001,
General Public vs General Dentists), and (C) Facial Appearance Procedures (*** p<0.001, General Dentists vs
Primary Care Physicians). Primary Care Physicians, General Dentists and General Public selected OMS
the most for performing jaw corrective surgery.
Specialities are represented by the following colors; General Surgeon, Oral and Maxillofacial
Surgeon, Otolaryngologist, Periodontist, Plastic Surgeon.

23
Figure 1. Awareness of Specialists

24
Figure 2A. Fracture of the Upper Jaw
25
Figure 2B. Fracture of the Lower Jaw
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Medical physician General dentist General public
Sp
eci
alt
y S
ele
cte
d (
%)
Survey Participant
***
**
Primary Care
PhysiciansGeneral Dentists General Public

26
Figure 2C. Fracture of the Nose
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Medical physician General dentist General public
Sp
eci
alt
y S
ele
cte
d (
%)
Survey Participant
Primary Care
PhysiciansGeneral Dentists General Public

27
Figure 2D. Fracture of the Eye

28
Figure 2E. Fracture of the Cheek

29
Figure 2F. Fracture of the Skull

30
Figure 2G. Cut on the face

31
Figure 3A. Cancer of the mouth, tongue or lip

32
Figure 3B. Non-cancerous lesion of the mouth, tongue or lip

33
Figure 3C. Non-cancerous tumor/cyst of the upper or lower Jaw
34
Figure 3D. Removal of TMJ lesion

35
Figure 3E. Salivary Gland Removal

36
Figure 3F. Infection/swelling around the mouth/neck

37
Figure 3G. Infection/swelling around the Eye

38
Figure 4A. Child with cleft lip
39
Figure 4B. Child with cleft palate

40
Figure 4C. Soft tissue grafts for oral reconstruction

41
Figure 4D. Hard tissue grafts for oral reconstruction
42
Figure 5A. Removal of Wisdom teeth
43
Figure 5B. Placement of dental implants

44
Figure 5C. Providing general/deep sedation

45
Figure 6A. Corrective Jaw surgery
46
Figure 6B. Nose corrective surgery

47
Figure 6C. Facial appearance procedures

48
Chapter 6 Discussion
6.1 Limitations:
This study is not without limitations. This survey was performed only in Ontario, and therefore
the results may not be applicable throughout Canada. However, Ontario is the largest province
and has the greatest number of Oral and Maxillofacial Surgeons, so one would expect that they
would have the greatest recognition and exposure here. If anything, in provinces where fewer
OMS are present, the results would be expected to show even less awareness of OMS scope.
Another potential limitation in this study was our response rate of 50.1%. It was slightly below
the mean response rate of 54-61% for physicians and 68% for non-physicians obtained in
systematic review of postal questionnaires 26. However other sources have stated values as low
as 6% for health care professional and 48.4% for published academic studies, therefore our
50.1% response rate represents an acceptable result and not a true limitation 27,28. Our approach
was a modification of The Dillman Tailored Design Survey Method, with the use of an initial
invitation letter, a phased distribution and follow up phone calls all done to maximize the
response rate as multiple mail outs and follow-up reminders are known to reduce bias and
optimize response rate 29. Due to the cost of each wave of mail out surveys, no further strategies
such as monetary incentives could be applied. Our budget also did not allow for a larger sample
to be contacted, as it would not have been feasible and would have likely meant that less waves
of the survey would have been sent. Lastly regional variations in scope of practice exist in
Canada as they do in the rest of the world, making it difficult to accurately assess. Procedures
that are taught in training programs and fall within OMS scope of practice may not be practiced
in some parts of the country. This subsequently makes it hard to determine if there is a true lack
of awareness or if the awareness identified is in fact representative of what is practiced in that
region. With this in mind, only a few procedures listed in our Survey are not routinely performed
in Ontario, therefore the majority of procedures are a true representation of what an Ontario
OMS performs.

49
6.2 Implications and Future Directions: Our study is the first of its kind to be performed in Canada. It showed similar results to those
obtained internationally and has the potential to be applied to a variety of areas. There is a global
lack of awareness of the scope of practice of Oral and Maxillofacial Surgeons in Ontario.
General Dentists appear to be the most knowledgeable, with no difference demonstrated between
Family Physicians and the General Public, however all populations underestimated the true
scope of OMS. Our findings have important implications in the areas of public health and public
education. In terms of public health, everyone should be able to obtain the best possible and most
timely treatment. The goal of health care is to provide optimal care for patients, including
providing patients with all the treatment options and surgical specialties capable of providing
them care. This ensures that they can make the most educated decision. For this to occur, there
must be sound understanding of the Oral and Maxillofacial Surgery specialty by medical and
dental professionals, as well as the General Public so that appropriate referrals are made, leading
to effective and efficient treatment for all1, 12. If Oral and Maxillofacial Surgeons are not
recognized as potential treatment providers, patients may in fact be waiting weeks to months for
medical specialist referrals due to the nature of our saturated health care system. Undergraduate
medical students in the UK, who demonstrated a lack of awareness of OMS, also found a
significant delay to consult Oral and Maxillofacial Surgeons compared to other surgical
specialists17. If all specialties that can manage a specific issue are recognized, the public has a
greater amount of options, which likely means a reduced interval from time of referral to
consult/treatment. Previously, it was found that of the General Public that were aware of OMS, a
majority had heard of it from a friend’s or family member’s experience11. This demonstrates that
any awareness of OMS is gained through personal experience more than public knowledge or
social media currently. Family Physicians and General Dentists are, many times, the primary
point of contact for any head, neck or oral complaint by the public. These professionals act as
potential gatekeepers to OMS 30. They may determine the course of patients, thus having them
informed of all options allows them the opportunity to provide the best care. This is why our data
which showed a clear lack of awareness must be applied to the education of health care
professionals30. As such, greater progress needs to be made in the education of Family
Physicians, General Dentists and the General Public, especially in the areas that were grossly
50
underrepresented, if the specialty of Oral and Maxillofacial Surgery is to be practiced to its full
potential and patients are to receive all treatment options7, 12.
The scope of OMS has expanded more and more in recent years, which underscores the
importance of promoting the profession. While overlapping boundaries with plastic surgery and
ENT may cause confusion, some propose that this creates more of a healthy competition31.
O’Keefe suggests that policymakers encourage this growth to promote innovation that would
provide patients more choice and a better quality of care 32. Future studies should be directed
towards analyzing education patterns on OMS scope of practice and improving education
opportunities for health care providers and patients. In addition, conducting similar studies
throughout the rest of Canada would be beneficial to see if perceptions held in Ontario are held
in the rest of the country. Along with this, the specialty of Oral and Maxillofacial Surgery should
aim for the establishment of a national scope of practice that is consistent from province to
province. This would allow the identification of recurrent areas of weakness in the population’s
perception, without regional variations playing a role, so that education campaigns could be
optimized and conducted on a national level.
Future directions should follow our proactive neighbors with AAOMS prioritizing informational
campaigns. AAOMS targeted the public with branding that was easily understood and well
received using slogans such as “Oral and Maxillofacial Surgeons: The Experts in Face, Mouth
and Jaw Surgery”24. A patient-specific website and information videos on common Oral and
Maxillofacial Surgery procedures helped the profession keep up to date with social media and
allow people to use their tech devices to get answers in the comfort of their home. AAOMS had
much success as a result. Another campaign targeted dental students with the “Morning Huddle
Student Edition” providing daily electronic resources to dental students regarding the scope of
OMS. In Ontario, we can make similar steps to help people understand who to turn to: the
experts.

51
References
1. Ameerally P, Fordyce AM., Martin, IC: So you think they know what we do? The public
and professional perception of oral and maxillofacial surgery. Br J Oral Maxillofac Surg
32:142, 1994
2. Lababidi E, Breik O, Subramaniam S: Perceptions of oral and maxillofacial surgery
amongst Australian medical general practitioners. Oral Maxillofac Surg Oral Med Oral
Pathol 30:229–232, 2018
3. Hargreaves, J. Anthony, "Dentistry". In The Canadian Encyclopedia. Historica Canada.
Article published February 07, 2006; Last Edited December 16, 2013.
https://www.thecanadianencyclopedia.ca/en/article/dentistry
4. Thoma KH: The History of Oral Surgery: The oldest specialty of dentistry. Oral Surg
Oral Med Oral Pathol 10:1-10, 1957
5. Weinberg, S. (2003, May 1) The End of an Era. Retrieved from
https://www.oralhealthgroup.com/features/the-end-of-an-era
6. Rangarajan S, Kaltman S, Rangarajan T, Lopez E: The general public’s recognition and
perception of oral and maxillofacial surgery. Oral Surg Oral Med Oral Pathol Radiol
Endod 106:15, 2008

52
7. Vadepally AK, Sinha R, Uppada UK, Rama Krishna Reddy BV, Agarwal A: Oral and
maxillofacial surgery: Perception of its scope among the medical fraternity and general
public. J Cranio Max Dis 4:21-7, 2015
8. Kumar, S. Training Pathways in Oral and Maxillofacial Surgery Across the Globe—A
Mini Review: J Maxillofac Oral Surg 16:269–276, 2017
9. Bagheri, SC, Bell, RB, Khan, HA: Current Therapy in Oral and Maxillofacial Surgery. 1st
Ed. St. Louis, MO, Saunders, 2012, pp 1-5.
10. Subhashraj K, Subramaniam B: Awareness of the specialty of oral and maxillofacial
surgery among health care professionals in Pondicherry, India. J Maxillofac Oral Surg
66:2330–4, 2008
11. Lau SL: Do you think they know about us? Oral and maxillofacial
surgery in Hong Kong. J Dent Health Oral Disord Ther 1:11, 2014
12. Hunter MJ, Rubeiz T, Rose L: Recognition of the scope of oral and maxillofacial surgery
by the public and health care professionals. J Oral Maxillofac Surg 54:1227, 1996

53
13. Farook SA, Rihal K, Abullakutty A, Coombes D: Lost tribe? Awareness of oral and
maxillofacial surgery (OMFS) among the general public. Br J Oral Maxillofac Surg
51:e4–e5, 2013
14. Ifeacho SN, Malhi GK, James G: Perception by the public and medical profession of oral
and maxillofacial surgery—Has it changed after 10 years? Br J Oral Maxillofac Surg
43:289, 2005
15. Rocha NS, Laureano Filho JR, Silva ED, Almeida RC. Perception of oral maxillofacial
surgery by healthcare professionals. Int J Oral Maxillofac Surg 37:41– 46, 2008
16. Haron, IM, Sabti MY, Andersson L, Sharma PN. Perception of oral and maxillofacial
surgery by medical and dental health care professionals in Kuwait. J Oral Maxillofac
Surg Med Oral Pathol 25:5–11, 2013
17. Goodson AM, Payne KFB, Tahim A, Cabot L, Fan K: Awareness of oral and
maxillofacial surgery as a specialty and potential career pathway amongst UK medical
undergraduates. Surgeon 11:92-95, 2013
18. Jarosz KF, Ziccardi VB, Aziz SR, Sue-Jiang S: Dental student perceptions of oral and
maxillofacial surgery as a specialty. J Oral Maxillofac Surg 71:965-973, 2013

54
19. Ologunde R, Sykes M: A review of oral and maxillofacial surgery journals’ contribution
to undergraduate surgical education. Br J Oral Maxillofac Surg 52:894-900, 2014
20. Guerrero AV, Altamirano A, Brown E, Shin CJ, Tajik K, Fu E, Dean J, Herford A: What
is in a name? Oral and maxillofacial surgeon versus oral surgeon. J Oral Maxillofac Surg
72:8-18, 2014
21. Laskin DM, Ellis JA Jr, Best AM: Public recognition of specialty designations. J Oral
Maxillofac Surg 60:1182–1185, 2002
22. Hupp JR: The AAOMS Informational Campaign – Is it Succeeding? J Oral Maxillofac
Surg 74:223-224, 2016
23. American Association of Oral and Maxillofacial Surgeons (2017, Nov 14). Press
Release: AAOMS garners awards for its Informational Campaign. Retrieved from:
https://www.aaoms.org/media/press-releases/aaoms-garners-awards-for-its-informational-
campaign
24. Nelson WJ: AAOMS Informational Campaign Communicates the OMS Story. J Oral
Maxillofac 74:1109-1110, 2016
25. Ontario Society of Oral Maxillofacial Surgeons (2018). Retrieved from:
https://www.osoms.ca/

55
26. Asch DA, Jedrziewski MK, Christakis NA: Response rate to Mail Surveys Published in
Medical Journals. J Clinic Epidemiol 50:1129-1136, 1997
27. Brtnikova M, Crane LA, Allison MA, Hurley LP, Beaty BL, Kempe: A method for
achieving high response rates in national surveys of U.S. primary care physicians. PLoS
ONE 13(8), 2018
28. Baruch Y, Holtom B: Survey response sate levels and trends in organizational research.
Sage Journals 61:1139, 2008
29. Nakash R, Hutton J, Jorstad-Stein E, Gates S, Lamb S: Maximising response to postal
questionnaires – A systematic Review of randomised trials in health research. BMC
Medical Research Methodology 6(5), 2006
30. Cottrell DA, Reebye UN, Blyer SM, Hunter MJ, Mehta N: Referral patterns of general
dental practitioners for oral surgical procedures. J Oral Maxillofac Surg 65:686-690, 2007
31. McArdle PJ, Whitnall M: The referral practice of general medical practitioners to the
surgical specialties: implications for the future. Br J Oral Maxillofac Surg 34:394–399,
1996
32. O’Keefe JP: Is Competition Good for care? Editorial. J Can Dent Assoc: 72, 2006

56
Appendices
Appendix A. Additional Detailed Methodology
Study Design, Population and Questionnaire
A cross-sectional study via a mail-out survey to a random sample of general dentists, family
physicians and the general public in Ontario was performed. Ethics approval was obtained from
the University of Toronto (protocol #: 34462) Research Ethics Boards. The sample size (n)
calculation is based on the population size (N), proportion of population expected to choose 1 of
2 responses (P=0.5 to allow for maximum variance), the assumed sampling error (C=0.05), and
the Z-statistic of 1.96 (for a 95% confidence interval – CI). Ontario population of 13.6 million,
the sample size of 384 was calculated. n = [ (N)(P)(1-P) ] / [ (N-1)(C/Z)2 + (P)(1-P) ] n = 384.
General Dentist Ontario 8019, the sample size of 367 was calculated n = [ (N)(P)(1-P) ] / [ (N-
1)(C/Z)2 + (P)(1-P) ] n = 367. Medical Professionals 40890, the sample size of 381 was
calculated n = [ (N)(P)(1-P) ] / [ (N-1)(C/Z)2 + (P)(1-P) ] n = 381. The sample target was
increased to 600 in each group to ensure adequate number of responses for analysis of the data
with an expected response rate below 50%. Allocated funds only allowed an increase in all
groups to 600.
Study Population The survey population was a representative sample of the General Public,
General Dentists and Family Physicians in Ontario. The source of this sample frame was the
physician registry and general dentist registry via the CPSO and ODA websites from which a
random population was generated by selecting at random every 67th person from the CPSO and
every 13th person from the ODA websites to obtain a total of 600 participants from each of the
two populations. The General Public was similarly drawn by selecting a random sample of 600
from the Ontario telephone directory and cross matching each selection ensuring they were not
either a registered General Dentist or Family Physician.
Inclusion criteria: 1. General Population: Adults over the age of 18 who are neither medical nor
dental professionals and living in Ontario. 2. Family Physician: Any general medical family
57
physician with a valid CPSO number. 3. General Dentist: Any general dentist with a valid
RCDSO number.
Exclusion Criteria: Any subject under the age of 18. Oral and Maxillofacial Surgeons, medical
and dental professionals cannot be included into the General Public sample. In addition, no Oral
and Maxillofacial Surgeon can be included in either the General Dentist or medical professional
population.
Survey Tool: The survey tool (see Appendix F) was designed based on other patient-related
questionnaires in the literature12, 15. The survey tool was pilot tested amongst 15 participants in
each of the 3 population groups in order to evaluate the validity of the design, respondent burden,
time needed to complete the survey, and level of understanding of the survey. Revisions were
made after pilot testing. The survey consisted of a demographic screener along with 24 clinical
scenarios in which the participant could select all the specialists they thought were capable of
completing the treatment. For each of the 24 clinical scenarios, 5 specialties were given as
options (General surgeon, ENT, OMS, Plastic Surgeon and Periodontist) along with an “Other”
option. This protocol was adopted from previous survey studies5-8. It asks participants to identify
which health care professional performs specific treatments, as well as demographic questions,
and for health professionals, the level of training and type of specialty. The specific treatment
situations were selected to include the entire scope of practice that is taught during an oral and
maxillofacial training program and are in line with those used in the current literature related to
OMS scope.
Survey Implementation: The initial mail-out contact was a brief letter informing the selected
participants of their selection to potentially partake in the study. It informed them that they
would receive the full survey package with further details and full instructions within the
following 2 weeks. This initial contact letter was incorporated to try and maximize survey
response rate. The first full mail out package was sent out 2 weeks after the initial contact letter,
it consisted of the study invitation, research cover letter, information sheet for participants, the
questionnaire, as well as a pre-stamped and pre-addressed return envelope. Four weeks after the
initial mail out contact, only the non-responders were mailed a reminder invitation to participate
in the study, as well as a second questionnaire and a pre-stamped return envelope. Four weeks
58
after the reminder letters were sent, the first follow up phone calls were made to all non-
responders. Four weeks after the first follow up phone call, a final package of the questionnaire
and pre-stamped and pre-addressed envelopes were sent to the remaining non-responders again.
Four weeks after the final mail-out contact, the non-responders received a second phone call
follow up. This staggered survey distribution along with periodic phone call follow-ups was
implemented to maximize study response rate. Data collection began with the initial survey
distribution and ceased with the last follow up phone call over the course of a 22-week period.
Statistical Analysis: Questionnaire data from completed and returned questionnaires were input
into a Microsoft Excel (Microsoft Corp, Redmond, WA) file, and the database exported into the
Statistical Package for Social Sciences software 21.0 (Armonk, NY : IBM Corp.) Descriptive
statistics reported demographic data. Inferential statistics via a chi-square test compared
responses between the general population, physicians, and dentists to identify any significant
differences between subjects. Level of significance was set at p < 0.05. If significant differences
between the three groups were identified a second set of chi-square tests were done comparing
General Dentists vs Family Physicians, General Dentists vs General Public and Family
Physicians vs General Public. A Bonferroni correction was completed to account for type 1 error
making the level of significance p< 0.0167.

59
Appendix B. Additional Detailed Results
Patient Demographics
An overall response rate of 50.1% (n=902) was achieved, 311 Family Physicians, 332 General
Dentists and 259 from the General Public. Demographic data of the respondents was analyzed.
Demographic data (Table 1) shows a statistically significant difference in gender composition (p
= .007) and location (p < .001). General Dentists have higher proportion of males (67.5%)
compared to Family Physicians (57.9%) and the General Public (54.1%). Also, the General
Public participants are more likely to reside in large urban areas (94.2%) compared to Family
Physicians (66.9%) and General Dentists (66.5%). No significant difference was found for age (p
= .06) with the mean age of the entire survey population 49.41 +13.5, or for years of practice (p
= .37).

60
Table 1. Demographics
Demographic Total sample
(n = 902)
Family
Physicians
(n = 311)
General
Dentists
(n = 332)
General
Public
(n = 259)
Comparison between
groups
Gender, n (%) Χ²(4) = 14.2, p = .007
Female
357
(39.6%)
131
(42.1%)
107 (32.2%) 119 (45.9%)
Male
544
(60.4%)
180
(57.9%)
225 (67.5%) 140 (54.1%)
Age, mean ± SD
49.4 ±
13.50
50.6 ±
13.50
49.4 ±
11.90
47.9 ±
15.23
F(2.9) = 2.7, p = .06
Years of practice,
mean ± SD
21.5 ±
13.23
21.1 ±
14.27
21.9 ±
12.19
- F(1,639) = 0.8, p =
.37
Location, n (%) Χ²(6) = 75.4, p < .001
Rural 2 (0.2%) 1 (0.3%) 1 (0.3%) 0
Small urban 108(12.0%) 51 (16.4%) 54 (16.3%) 3 (1.2%)
Medium urban 119
(13.2%)
51 (16.4%) 56 (16.9%) 12 (4.6%)
Large urban 672(74.6%) 208
(66.9%)
220 (66.5%) 244(94.2%)

61
Clinical Scenario Selection:
Similarly, to previous studies, the 24 clinical scenarios were grouped into 5 categories; trauma,
pathology, reconstructive surgery, oral procedures and cosmetic surgery15. 13 of 24 scenarios
had a total OMS selection of less than 50% as seen in Table 3. When each population was
examined individually, the General Population had 16, Family Physicians, 14, and General
Dentists, 10 scenarios, where OMS were selected less than 50%. General Dentists had the
highest OMS selection in 20 of the 24 scenarios (Table 2). When the population groups were
compared to each other, General Dentists had statistically significant higher selection of OMS in
19 of 24 scenarios compared to Family Physicians (Table 3) and 16 of 24 when compared to the
General Public (Table 4). Meanwhile, Family Physicians had 8 of 24 and the General Public had
10 of 24 scenarios with a significant higher OMS selection when compared to each other (Table
5).
Trauma:
OMS selection in trauma scenarios 1. maxillary, 2. mandibular, 3. nasal, 4. orbital, 5. cheek and
6. skull fractures and 7. cuts on the face was (table 3, Fig 2): Bold indicates > 50% selection.
1. Total: (73.3%, 86.9%, 20.6%, 22.9%, 37.5%, 14.1%, 36.4%)
2. General Dentists (77.4%, 99.1%, 23.2%, 27.4%, 47.6%, 14.4%, 53.9%)
3. Family Physicians (75.2%, 83.9%, 20.3%, 19.6%, 28.3%, 7.2%, 35.4%)
4. General Public (65.6%, 74.9%, 17.8%, 20.9%, 35.7%, 21.4%, 15.1%)
Pathology:
OMS selection involving pathology of the head and neck, 1. cancerous lesions, 2. non-cancerous
lesions, 3. non-cancerous cyst/tumors, 4. TMJ pathology, 5. salivary gland treatments, 6.
infections of the neck and 7. infections of the eye was (Table 3, Fig 3): Bold indicates > 50%
selection.
1. Total: (42.8%, 71%, 79.1%, 84.1%, 51.7%, 66.6%, 18%)
2. General Dentists (58.7%, 94.3%, 97%, 98.2%, 71.1%, 93.7%, 25%)
3. Family Physicians (20.3%, 61.7%, 75.6%, 81.4%, 35%, 55.6%, 8%)
4. General Public (49.6%, 52.3%, 60.5%, 69.5%, 46.7%, 45.2%, 20.8%)

62
Reconstructive Surgery:
OMS selection in scenarios involving 1. Cleft lip, 2 Cleft palate, reconstruction of oral structures
with 3. hard or 4. soft tissue was (table 3, Fig 4): Bold indicates > 50% selection.
1. Total: (29.8%, 40.0%, 43.4%, 46.2%)
2. General Dentists (34%, 44.3%, 49.4%, 59%)
3. Family Physicians (21.5%, 31.2%, 33.1%, 33.8%)
4. General Public (34.4%, 45.2%, 48.2%, 44.8%)
Oral Procedures:
OMS selection in Oral procedures such as 1. wisdom teeth extractions, 2. dental implants and 3.
providing anesthesia was (Table 3, Fig 5): Bold indicates > 50% selection.
1. Total: (86.9%, 71.6%, 58.3%)
2. General Dentists (99.4%, 88.9%, 86.4%)
3. Family Physicians (82.3%, 65.9%, 50.8%)
4. General Public (76.4%, 56.4%, 31.3%)
Cosmetic Surgery:
OMS selection for cosmetic procedures 1. Nose corrective procedures, 2. Jaw corrective surgery
and 3. facial appearance procedures had an OMS selection of (Table 3, Fig 6): Bold indicates >
50% selection.
1. Total: (10.3%, 81.5% and 8.5%)
2. General Dentists (6.9%, 97%, 13%)
3. Family Physicians ( 8.4%, 84.2%, 4.2%)
4. General Public (17.7%, 58.3%, 7.7%

63
Table 3. OMS % selected per condition/scenario by all groups.
Bold indicates > 50% selection.
Condition /
Scenario
Total
sample
(n = 902)
Family
Physicians
(n = 311)
General
Dentists
(n = 332)
General Public
(n = 259)
Comparison between
three groups
1 73.3% 75.2% 77.4% 65.6% p = .004
2 86.9% 83.9% 99.1% 74.9% p < .001
3 20.6% 20.3% 23.2% 17.8% p = .27 (NS)
4 22.9% 19.6% 27.4% 20.9% p = .043
5 37.5% 28.3% 47.6% 35.7% p < .001
6 14.1% 7.2% 14.4% 21.4% p < .001
7 36.4% 35.4% 53.9% 15.1% p < .001
8 42.8% 20.3% 58.7% 49.6% p < .001
9 71.0% 61.7% 94.3% 52.3% p < .001
10 79.1% 75.6% 97.0% 60.5% p < .001
11 84.1% 81.4% 98.2% 69.5% p < .001
12 51.7% 35.0% 71.1% 46.7% p < .001
13 66.6% 55.6% 93.7% 45.2% p < .001
14 18.0% 8.0% 25.0% 20.8% p < .001
15 29.8% 21.5% 34.0% 34.4% p < .001
16 40.0% 31.2% 44.3% 45.2% p < .001
17 43.4% 33.1% 49.4% 48.2% p < .001
18 46.2% 33.8% 59.0% 44.8% p < .001
19 86.9% 82.3% 99.4% 76.4% p < .001
20 71.6% 65.9% 88.9% 56.4% p < .001
21 58.3% 50.8% 86.4% 31.3% p < .001
22 81.5% 84.2% 97.0% 58.3% p < .001
23 10.3% 8.4% 6.9% 17.0% p < .001
24 8.5% 4.2% 13.0% 7.7% p < .001

64
TOTAL 49.3% 42.8% 60.8% 42.3% p < .001
Table 4. OMS % selected per condition/scenario Family Physicians vs. General Dentists.
Bold indicates > 50% selection.
Condition / Scenario Family Physicians
(n = 311)
General Dentist
(n = 332)
Comparison of groups
1 75.2% 77.4% p = .5 (NS)
2 83.9% 99.1% p < .001
3 20.3% 23.2% p = .3 (NS)
4 19.6% 27.4% p = .02 (NS)
5 28.3% 47.6% p =.004
6 7.2% 14.4% p = .002
7 35.4% 53.9% p = .003
8 20.3% 58.7% p < .001
9 61.7% 94.3% p < .001
10 75.6% 97.0% p < .001
11 81.4% 98.2% p =.003
12 35.0% 71.1% P < .001
13 55.6% 93.7% p <.001
14 8.0% 25.0% p < .001
15 21.5% 34.0% p < .001
16 31.2% 44.3% p < .001
17 33.1% 49.4% p < .001
18 33.8% 59.0% p = .007
19 82.3% 99.4% p = .02 (NS)
20 65.9% 88.9% p = .004
21 50.8% 86.4% p < .001
22 84.2% 97.0% p = .003
23 8.4% 6.9% p = .5 (NS)
24 4.2% 13.0% p < .001

65
TOTAL 42.8% 60.8% p < .001
Table 5. OMS % selected per condition/scenario General Public vs. General Dentists.
Bold indicates > 50% selection.
Condition / Scenario General Public
(n = 259)
General Dentist
(n = 332)
Comparison of groups
1 65.6% 77.4% p = .002
2 74.9% 99.1% p < .001
3 17.8% 23.2% p = .1 (NS)
4 20.9% 27.4% p = .07 (NS)
5 35.7% 47.6% p =.003
6 21.4% 14.4% p = .03 (NS)
7 15.1% 53.9% p < .001
8 49.6% 58.7% p = .02 (NS)
9 52.3% 94.3% p < .001
10 60.5% 97.0% p < .001
11 69.5% 98.2% p < .001
12 46.7% 71.1% P < .001
13 45.2% 93.7% p <.001
14 20.8% 25.0% p < .24 (NS)
15 34.4% 34.0% p < .9 (NS)
16 45.2% 44.3% p < .8 (NS)
17 48.2% 49.4% p < .8 (NS)
18 44.8% 59.0% p =.002
19 76.4% 99.4% p = .007
20 56.4% 88.9% p < .001
21 31.3% 86.4% p < .001
22 58.3% 97.0% p < .001
23 17.0% 6.9% p = .001
24 7.7% 13.0% p = .04 (NS)

66
TOTAL 42.3% 60.8% p < .001
Table 6. OMS % selected per condition/scenario Family Physicians vs. General Public.
Bold indicates > 50% selection.
Condition / Scenario Family physicians
(n = 311)
General Public
(n = 259)
Comparison of groups
1 75.2% 65.6% p = .01
2 83.9% 74.9% p =.008
3 20.3% 17.8% p = .5 (NS)
4 19.6% 20.9% p = .7 (NS)
5 28.3% 35.7% p =.01
6 7.2% 21.4% p < .001
7 35.4% 15.1% p = .007
8 20.3% 49.6% p = .009
9 61.7% 52.3% p = .02 (NS)
10 75.6% 60.5% p < .001
11 81.4% 69.5% p < .001
12 35.0% 46.7% p = .005
13 55.6% 45.2% p =.01
14 8.0% 20.8% p < .001
15 21.5% 34.4% p < .001
16 31.2% 45.2% p < .001
17 33.1% 48.2% p < .001
18 33.8% 44.8% p = .01
19 82.3% 76.4% p = .08 (NS)
20 65.9% 56.4% p = .02 (NS)
21 50.8% 31.3% p < .001
22 84.2% 58.3% p < .001
23 8.4% 17.0% p = .002
24 4.2% 7.7% p = .07 (NS)
67
TOTAL 42.8% 42.3% p = .9 (NS)
Appendix C. Initial Contact Letter
Dear _________________,
My name is Oscar Dalmao and I am a graduate student at the University of Toronto. This invitation letter
is being sent to you as you have been randomly selected. I am inviting you to participate in a research
project studying the perception of Surgeons’ scope of practice. You can expect to receive a survey in the mail in 2 weeks time.
I would appreciate your help by completing the survey you will receive in 2 weeks. The survey will take
approximately 10 minutes to complete and the results will be made available once the study has
concluded. Further details about study participation will be explained in the mailed out survey package.
Thank you for your time. It is only with the help of generous people like you that our research can be
successful.
Sincerely,
Oscar Dalmao, MSc Candidate
University of Toronto.
Room 143, 124 Edward Street, Toronto, ON, M5G 1G6 Email: [email protected]

68
Appendix D. Invitation to study participation
Dear _________________,
My name is Oscar Dalmao and I am a graduate student at the University of Toronto. I am inviting you to participate in a research project studying the perception of Surgeons’ scope of practice.
I would appreciate your help by participating in this survey which will take approximately 10 minutes to complete. There are no right or wrong answers. Your participation is voluntary and you may withdraw from this study at any time, for any reason.
Your privacy is important to us, and this survey is completely confidential. Your responses will not be linked to your name. Although, I am encouraging you to complete this questionnaire, if you choose to not participate in this study, this will in no way affect the care you receive at the University of Toronto Faculty of Dentistry, or at a private dental clinic.
In regards to the survey itself, you can contact me at [email protected]. Kindly ensure your responses are received no later than ###################
Thank you for your time. It is only with the help of generous people like you that our research can be successful.
Sincerely,
Oscar Dalmao, MSc Candidate
University of Toronto.
Room 143, 124 Edward Street, Toronto, ON, M5G 1G6
Email: [email protected]

69
Appendix E - Information and Consent for Participation
How was I selected to be in this Sample? Who will see my answers? Will my answers be confidential?
You were selected at random to be part of this sample being drawn either from the Ontario Dental Association (ODA), the College of Physicians and Surgeons of Ontario (CPSO) or Ontario population registry. During this research project, names and addresses of participants will be stored electronically on a secure and encrypted network, on a password-protected computer. The surveys will be kept in a locked cabinet in the Discipline of Oral and Maxillofacial Surgery. All electronic data will be stored on a password-protected computer in the Discipline of Oral and Maxillofacial Surgery and the primary investigator will be the only individual with access to these data. Each questionnaire is numbered: the number represents your mailing address. The list that identifies your address is stored separately in a locked cabinet at a different location, and will also be destroyed upon completion of this study. As a result, there is little - if any - possibility of linking a returned survey to the individual who completed it. Contact information is only used for survey distribution and tracking responses. At the end of this study, all of the contact information and all of the surveys will be destroyed and shredded.
Your responses are completely confidential. Your name and any personal identifying information will not be stored with your answers, and it will also not be used in any reports or publications from this study. If chosen, (a) representative(s) of the Human Research Ethics Program (HREP) may access study related-data and/or consent materials as part of the review. All information accessed by the HREP will be upheld to the same level of confidentiality that has been stated by the research team.
What happens if I do not participate?
Participation is completely voluntary. It is your right to refuse to answer any questions or participate, and you can withdraw from the study at any time by not completing the survey and not returning it to us, or by contacting us and informing us about your wishes to withdraw from the study. There are no consequences to you if you decline to participate in this study.
Does my participation provide any benefits to myself?
There are no immediate benefits to you. However obtaining an understanding of the population's view of Oral and Maxillofacial Surgeons may encourage the profession to explore areas where the can provide greater service to the overall public.
Are there any risks or harms in participating?
There are no risks or harms in participating in this study.

70
How do you obtain my consent to participate?
Completing this questionnaire and returning it to the primary investigator implies your consent to participate in this study.
Who can I contact for more information?
Further questions about this study can be answered by myself (the principal investigator) at any time. Kindly email me at [email protected]

71
Appendix F - Study Survey
Thank you for taking the time to fill out this survey. Please answer all of the questions.
Once completed, please return only the questionnaire in the prepaid postage envelope included with this package. If you decline to participate in this study, please return the unfilled questionnaire using the pre-stamped envelope attached, so we do not contact you in the future. Thank you
1. Do you agree to participate in this study?
⎕ Yes
⎕ No
2. Current gender identity: (please check one answer)
⎕ Male
⎕ Female
⎕ Transgender
⎕ Do not identify as male, female or transgender
3. Date of birth
4. Are you a Medical physician or Dentist?
⎕ Yes
⎕ No
If so please indicate your specific field of practice and years of practice
⎕ Family physician
⎕ Medical specialist (please specify)
⎕ General dentist
⎕ Dental specialist (please specify)
Years of practice: ______

72
5. Have you ever heard of any of these specialists? (Please check all that apply)
Specialist YES NO
General Surgeon
Periodontist
Plastic Surgeon
Oral and Maxillofacial Surgeon
Otolaryngologist (ENT)
6. Have you ever been treated by any of these specialists? (Please check all that apply)
Specialist YES NO
General Surgeon
Periodontist
Plastic Surgeon
Oral and Maxillofacial Surgeon
Otolaryngologist (ENT)
7. Please review all the surgical conditions/procedures listed below and select which specialists you think are competent (capable) of dealing with each condition. (Please check ALL specialists who apply for EACH of the conditions/procedures listed)
Conditions/ Procedures
General Surgeon
Periodontist Plastic Surgeon
Oral and Maxillofacial Surgeon
Otolaryngologist (ENT)
Other (please specify)
Trauma:
1. Fracture of the upper jaw (broken upper jaw)
73
2. Fracture of the lower jaw (broken lower jaw)
3. Fracture of the nose (broken nose)
4. Fracture of the eye bones
5. Fracture of the cheek bones
6. Fracture of the skull
7. Cut on the face
Pathology:
8. Cancer of the mouth, tongue or lip
9. Non cancerous lesion of the mouth, tongue or lip
10. Non cancerous tumor/cyst of the upper or lower jaw
11. Removal of temporomandibular joint (TMJ) lesions (Jaw Joint lesions)
12. Salivary Gland removal
13. Infection/swelling around the mouth/neck
14. Infection/swelling around the eye

74
Conditions/ Procedures
General Surgeon
Periodontist Plastic Surgeon
Oral and Maxillofacial Surgeon
Otolaryngologist (ENT)
Other (Please specify)
Reconstruction:
15. Child with cleft lip (improperly joined lip)
16. Child with cleft palate (improperly formed/joined roof of the mouth)
17. Soft tissue (skin, fat, muscle) grafts for oral reconstruction (taking soft tissue to rebuild the oral cavity)
18. Hard tissue (hip, tibia and skull bone) grafts, for oral reconstruction (taking bone tissue to rebuild the oral cavity)
Oral Procedures:
19. Removal of wisdom teeth (3rd molars)
20. Placement of Dental implants
21. Providing general anesthesia/deep sedation (putting patients to sleep during dental procedures)
Cosmetic
22. Jaw corrective surgery
23. Nose corrective surgery

75
24. Facial appearance procedures. (facelift, eyebrow lift, Botox, chemical peels etc..)
Thank you for taking the time to participate in this survey!
Please place the filled questionnaire in the enclosed self-addressed and self-stamped envelope, seal it, and return it to us.