Embed Size (px)
Citation preview

CentreforAppliedHealthEconomics
Public Investment in Bariatric Surgery
Economics and Evidence
Prof Paul Scuffham FAAHMS
Queensland Clinical Senate23-24th March 2017

CentreforAppliedHealthEconomics
Outline
• Cost-effectiveness• BudgetimpactinQueensland• Publicviews- whomtotreat
• Citizenjuries• Preferencesofthegeneralpublic

CentreforAppliedHealthEconomics
Cost-effectiveness analysis:
AIMS:
• Estimatemostefficientsurgicalapproachforbariatricsurgeryforsevere(BMI>35)andverysevere(BMI>40)obesecomparedtousualcare(UC)
• EstimateimpactonbudgetfromprovidingbariatricsurgeryinQueenslandpublichospitals
3
CentreforAppliedHealthEconomics
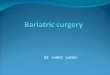
Model structure
4
5BMIweightclasses(healthstates):• normalweight(NW)• overweight(OW)• obese1(OB1)• obese2(OB2)• obese3(OB3)

CentreforAppliedHealthEconomics
Economic evaluation: parametersPerspective PublichealthcaresystemComparator Usualcare(UC)(conventionalpharmacotherapy,diet,exercise)Econeval type Cost-utilityanalysisSourcesofevidence Publishedclinicaltrials,systematic reviewsandmeta-analyses
Cohort 30year oldAustralianfemalewithmoderate(48%)tosevereobesity(52%)
Timehorizon Lifetime(50year duration)Outcomes CostsandQALYs
CostingsourcesQueenslandHealth.Samplecostdata:activitycosting(personalcommunication);AR-DRGsK10A,10B,11A,11B,12Z);MBSandPBSdataforcostsofUC,pre/postsurgery
Utilities•Australianpopulationnorms(SF-6D;Norman2013)•UtilityweightsperBMI classandco-morbidities(Kortt &Clarke2005)
Discountrate 5%forbothcostsandbenefits
5
CentreforAppliedHealthEconomics
Assumptions
• RepeatsurgeryforAGBandRYGB:• Basecasemodel:occurredwithinfirst2years• Scenarioanalysis:usedreoperationratesfromlongterm(>10years)studies.
• Note:nolong-termevidenceforreoperationratesforSG
• Regainofweight:• Basecasemodel:completeweightregainwithAGBbandremoval
• Scenarioanalysis:completeweightregainatdifferenttimeperiods
6

CentreforAppliedHealthEconomics
Results: Base case ICER (50 years / rest of life)
Basecase UC AGB RYGB SG
TotalCosts $118,965 $131,192 $135,043 $140,158
TotalQALYs 11.89 12.39 12.60 12.65
IncrementalCosts - $12,227 $16,078 $21,193
IncrementalQALYs - 0.50 0.71 0.77ICER(inc. cost/QALYgained) - $24,454 $22,645 $27,523
7
0
0
BenefitBenefitCostCostICER
i
i
--
=• QALY = quality-adjusted life year is a
generic measure including both quality and quantity of life lived.
• 1 QALY = one year in perfect health

CentreforAppliedHealthEconomics
Sensitivity analysis - ICERsAGB RYGB SG
ICER:basecase $24,454 $22,645 $27,523SensitivityanalysisAllmalepatients $24,623 $22,638 $27,615TreatOB3only $30,883 $40,067 $31,068TreatOB2only $17,652 $9,437 $24,041Fullweightregainat5years $378,180 $298,628 $487,691Fullweightregainat10years $130,253 $122,077 $158,256Fullweightregainat20years $54,399 $53,492 $65,18910%regainweightfor allbariatricsurgeries
$42,368 $39,571 $47,873
HigherratesforAGBandRYGBreoperations
$30,139 $36,096 $27,624
40yearsold $26,482 $26,355 $31,74150yearsold $30,472 $33,154 $39,42360yearsold $40,374 $48,065 $56,559
8
OB2 = better value for money
Longer weight kept off = better
SG best if repeat surgery for AGB or RYGB > ~20%
Younger = better value for money

CentreforAppliedHealthEconomics
Incremental costs & QALYs for T2 diabetic sub-group
Diabetic cohort
varied by age
AGB vs UC RYGB vs UC SG vs UC
Inc costInc
QALYInc cost Inc QALY Inc cost Inc QALY
Base Case: 30
years-$85,774 0.85 -$105,671 1.22 -$97,930 1.18
40 years -$115,297 0.85 -$134,885 1.18 -$126,925 1.15
50 years -$143,926 0.82 -$159,318 1.09 -$151,041 1.06
60 years -$156,403 0.70 -$164,476 0.90 -$155,748 0.87
9
CentreforAppliedHealthEconomics
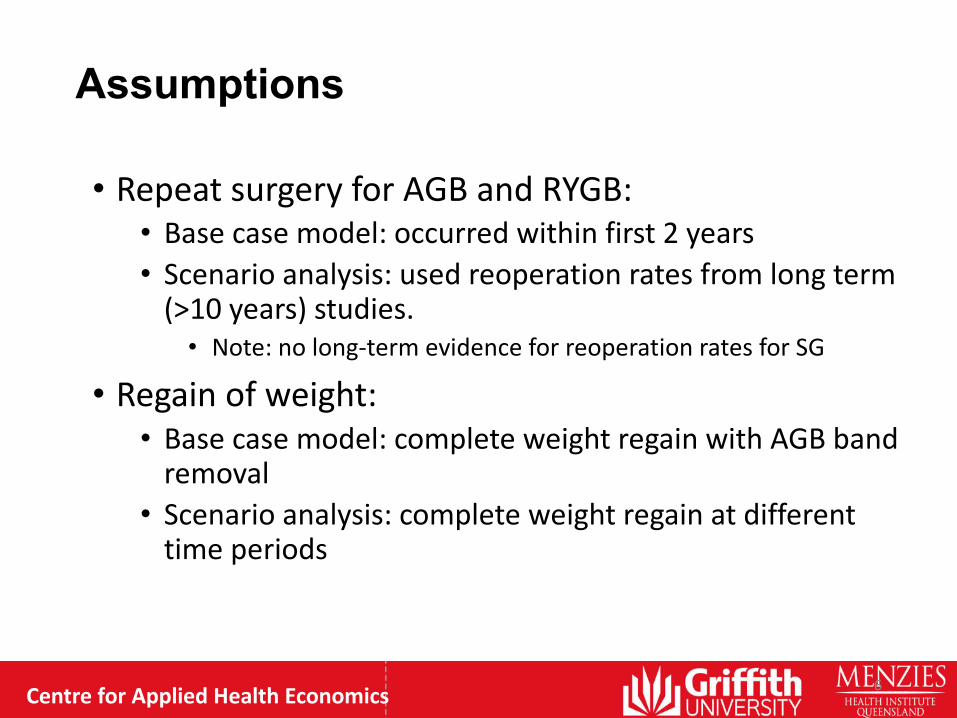
Sensitivity analysis (T2 diabetics): Undiscounted
Diabetic cohort
varied by age
AGB vs UC RYGB vs UC SG vs UC
Inc costInc
QALYInc cost
Inc
QALYInc cost Inc QALY
Base Case: 30
years-$351,734 2.47 -$489,110 3.56 -$485,432 3.47
40 years -$344,731 2.11 -$442,526 2.91 -$437,397 2.84
50 years -$320,285 1.68 -$380,561 2.21 -$374,032 2.16
60 years -$267,409 1.16 -$294,094 1.47 -$286,235 1.44
10

CentreforAppliedHealthEconomics
Conclusions - cost-effectiveness
Bariatric surgery is:• cost-effective option for the management of severe
obesity, relative to usual care• cost saving for diabetic patients with severe obesity
(≥ BMI 35)• Substantial costs for surgery which take years to recoup• RYGB was more cost-effective than AGB and SG, but
results were sensitive to rates of reoperations• Follow-up care is crucial to prevent patients from regaining
their surgical weight loss
11
CentreforAppliedHealthEconomics
Financialestimates

CentreforAppliedHealthEconomics
Financial impact estimation:
Prevalence of obesity in QLD• Used epidemiological approach • Used incremental costs from base case ICER • Queensland 2014: 420,500 adults classified with severe obesity
(OB2/OB3)
Incidence of obesity in Qld• 21% increase over 2007/8 to 2014/15 (3% yearly)
• Used to estimate incidence rate of moderate-to-severe obesity (OB2/3)
• We assumed all patients were eligible for surgery (100% uptake rate over 5 years)
• Financial impact likely overestimated due to prevalence of comorbidities (surgery contraindications)
13

CentreforAppliedHealthEconomics
OB 3 = 33.7%; diabetes = 11.6%
Patient population (OB2/3+)
Year 1 Year 2 Year 3 Year 4 Year 5
Prevalent 426,892
Prevalent treated* 85,378 85,378 85,378 85,378 85,378 Incident (treated annually) 3,232 3,257 3,281 3,306 3,331
Total potential pool for treatment 88,610 88,635 88,659 88,684 88,709
14

CentreforAppliedHealthEconomics
BMI and T2 diabetes subgroups
15
259,876
34,101
132,000
17,321
OB 2 without diabetes OB 2 with diabetes OB 3 without diabetes OB 3 with diabetes

CentreforAppliedHealthEconomics
Cost in year 1 – treat incident population only:
16
Numbers treated Costs ($m)
OB 3+ without diabetes 962 $48.1OB 3+ with diabetes 126 $6.3OB 2 without diabetes 1,895 $94.7OB 2 with diabetes 249 $12.4Total 3,232 $161.6
If treat OB3+ only – minimum cost is $54m
Assumptions:• $50,000 per surgery

CentreforAppliedHealthEconomics
Cost in year 1:Incident population plus 20% of prevalent population
17
Numbers treated Costs ($m)OB 3 without diabetes 26,385 $1,319
OB 3 with diabetes 3,462 $173OB 2 without diabetes 51,946 $2,597OB 2 with diabetes 6,816 $341Total 88,610 $4,430
If treat OB3+ only – minimum cost is $1.5bn (incl 20% prevalent pop)
Assumptions:• $50,000 per surgery

CentreforAppliedHealthEconomics
Long-run financial impact of bariatric surgeries (annual)
18
For diabetic subgroups, RYGB has highest annual cost savings, for OB2 and OB3
For w/o diabetes subgroups, AGB is cheapest, for OB2 and OB3
The proportions in each subgroup will drive the total cost……..

CentreforAppliedHealthEconomics
Implications from treating T2 diabetes patients:
19
• For every 100 T2DM patients treated, can treat some non-diabetic patients and remain cost-neutral:
• AGB: 702• RYGB: 658• SG: 462
• However, cost-neutrality obtained over rest of life
CentreforAppliedHealthEconomics
Financial impact conclusions
20
• Substantial costs initially
• To keep pace with increasing obesity, need to treat at least 3500 patients annually = min of $161 million
• Treat prevalent population?• 45% funded through ABF, remainder has to be found
through State funding• Reduce other services to fund Bariatric surg?• Theatre capacity?

CentreforAppliedHealthEconomics
Views of the public:
1. Citizen Juries

CentreforAppliedHealthEconomics
Citizens’ Juries
• Increasingly used in health policy guidance in the UK (and globally) to seek informed public views (aka “citizen councils”)
• Democratic, deliberative process• Jurors engage with evidence presented by
experts and develop a community-centred focus
• Independent facilitator used

CentreforAppliedHealthEconomics
Citizens’ JuriesAIMS:• Develop criteria for patients to receive bariatric
surgery from a small random sample of the general (tax paying) population
• Make recommendations to Qld Health
---• Naïve sample but presented with evidence for
deliberation• At the end of the process = highly informed sample

CentreforAppliedHealthEconomics
The Process: Recruitment & Methods
Brisbane
• Sampling: Random + purposive
• 17 jurors*
• 3 day jury process
• 2 facilitators
• 6 witness sessions
• 445 mins total deliberation time
Adelaide
• Sampling: Convenience + purposive
• 12 jurors
• 1 day jury process
• (same) 2 facilitators
• 6 (shorter) witness sessions
• 195 mins total deliberation time
*18Brisbanejurors,however1jurorbecameillandcouldnotcompletethejuryprocess

CentreforAppliedHealthEconomics
The Process: Sessions and Expert Witnesses
Brisbane
1. Overview of Overweight and Obesity• Epidemiologist
2. Allied Health Professionals Panel• Exercise physiotherapist• Psychologist• Dietician
3. Surgery: Indications and Outcomes• Bariatric surgeon
4. Consumer Representatives Panel• Consumer who lost weight without surgery• Consumer who recently had surgery• Consumer who had surgery a number of
years ago
5. Bariatric Surgery: Should we do it?• Endocrinologist
Adelaide
1. Overview of Overweight and Obesity• Physician (kidney specialist, diabetes
researcher)
2. Allied Health Professionals Panel• Exercise physiologist• Psychologist• Dietician
3. Surgery Panel: Waitlists, Indications, Prioritisation and Outcomes
• Bariatric Surgery Coordinator• Bariatric Surgeon
4. Consumer Representatives Panel• Consumer on surgery waitlist since 2009• Consumer who recently had surgery• Consumer who had successful surgery

CentreforAppliedHealthEconomics
Outcomes: Criteria for determining access to public funding
Suggested Criteria
Brisbane verdict(All Brisbane criteria subject to a 5 year
review)
Adelaide verdict
Age 30 – 50 years No age restriction (Under 18 years considered in extreme cases)
Body Mass Index (BMI)
BMI ≥35 (Lower for certain (at risk) ethno cultural groups)
BMI ≥35
Comorbidity -Type II diabetes diagnosis-Other comorbidities considered
-Type II diabetes diagnosis in last 5yrs-If BMI ≥50, Comorbidity not required
Behavioural change
-Commitment shown through lifestyle changes over 6 months
-Commitment shown through changing diet and exercise-Opportunity to adopt a healthier lifestyle and demonstrate commitment

CentreforAppliedHealthEconomics
CJ Outcomes: Prioritisation of bariatric surgery in the public health system• Higher BMI• Comorbidities - develop methods to assess seriousness/ level
of risk• Demonstrated commitment to behavioural change • Age and means testing were considered of less importance
• Support programs to assist patients not eligible for public funding
• Brisbane: individually focussed support (from professional staff)
• Adelaide: public health approach

CentreforAppliedHealthEconomics
Views of the public:
2. Discrete Choice Experiments –general public

CentreforAppliedHealthEconomics
Discrete Choice Experiment (DCE)
Aims:• To measure the strength of preferences and
trade-offs for potential prioritisation criteria in a large sample of the general (tax-paying) public
• Derive importance weights for criteria that might be used to prioritise bariatric surgery for adults
CentreforAppliedHealthEconomics
DCE - design and administration• Rigorous scientific approach to elicit preferences
• Designed to identify trade-offs and strength of preferences• NOT an opinion survey
• Attributes and levels – criteria identified from expert focus group and literature
• e.g. Whitty et al., The Patient 2014• Design
• D-efficient design (9 blocks of 18) main + selected 2-way interaction effects, plus a consistency check Q
• Online survey Nov – Dec 2013• Sample – panel (target 2,000)
• quota by state (Qld, SA), age and gender

CentreforAppliedHealthEconomics
DCE– prioritycriteria forsurgeryScenarioThe following two people both need surgical management for their obesity. Surgery is likely to be the only way to reduce their body weight and their health risks. Both people meet the hospital’s clinical criteria for surgery, and the surgery has been recommended by their doctors.However, demand for the surgery is very high, and only one person can have their surgery now. The other person will have to wait at least another 12 months for surgery.
Each person answered 18 choices like this one

CentreforAppliedHealthEconomics
DC
E At
tribu
tes
and
Leve
lsATTRIBUTE LEVELSCurrent level of obesity • Obesity (BMI 30 to less than 40 kg/m2)
• Severe Obesity (BMI 40 to less than 50 kg/m2)• Very Severe Obesity (BMI greater than 50 kg/m2)
Obesity-related conditions • Already has obesity-related conditions• Is at risk of developing obesity-related conditions
Age of person needing surgery
• 20 years• 35 years• 50 years
Family history • At least one parent or sibling is obese, has had weight issues since childhood
• No family history of obesityChance of maintaining a substantial (at least half) reduction in excess weight
• 30%• 50%• 70%
Has shown commitment by responding to prescribed lifestyle intervention (i.e. physical activity and diet)
• Has maintained a healthy lifestyle plan for several months, resulting in some weight loss, however is still in need of surgery
• Has not maintained a healthy lifestyle plan and has had no weight loss
Time already spent on surgery waiting list
• 6 months• 1 year• 2 years

CentreforAppliedHealthEconomics
DCE Participants – Public (n=1,994)CHARACTERISTIC N % AustraliaFemale Female 1038 52.1% 50.2%Age Mean (SD) 46.6 (16.5)
≥50 years 849 42.6% 41.5%State Qld 1484 74.4%ATSI Yes 50 2.5% 2.5%Education (highest) Cert, Dip, Degree 892 44.7% 59% (25-64 yrs)Employment Part/full time 1075 53.9% 60.5% (15yrs+) Income (annual household) >AU$100k 374 21.8% 35.1% (>$104k pa)Private health insurance Hospital cover 945 47.4% 47% (NHS 2004-5)HEALTH N % AustraliaAQoL-8D (utility) Mean (SD) 0.69 (0.21) Mean 0.86BMI ≥25 1171 60.1% 61.4%Perceived weight Overwt/Obese 1052 53.5%HEALTH SERVICE USE N %≥1 hospital admission in last 12 mths 399 20.0%≥4 GP visits last 12 mths 679 34.1%Previous bariatric surgery (self or family) 141 7.1%

CentreforAppliedHealthEconomics
Priority points (Marginal rate of substitution)
79.81
38.81
26.80
10.66
2.03 1.000
20
40
60
80
100
Shown lifestyle
commitment
Very severe obesity
Already has comorbidities
Family history
Wait list per mth
Chance per %
Severe Obesity
Age of person 50yrs
Wei
ght

CentreforAppliedHealthEconomics
Conclusions from Public DCEImportant factors:• Lifestyle commitment very important • Very severe obesity (BMI >50)• Existing comorbidities
Relatively non-important as priority criteria• Age • BMI<50• Time on wait list• Chance of maintaining weight loss

CentreforAppliedHealthEconomics
Keypoints• Surgery is more cost-effective in higher BMI and those
with diabetes • Substantial costs for surgery
• If treat OB3+ and 20% prevalent pop = $1.5bn (annual)• If treat OB3+ incident pop = $54m (annual)
• Benefits accrued over rest of life• Large prevalent population• Public acceptability:
• Must show evidence of lifestyle/behaviour change• Higher BMI takes priority• Greater priority for those with comorbidities

CentreforAppliedHealthEconomics
Acknowledgements
• Contributors:• MrRobbieJames(CAHE)• MsCassandraRanatunga (CAHE)• MrRyanSalton(UK)• DrJoshuaByrnes(CAHE)• ProfJennyWhitty(CAHE/UEA)
• Manyothersinvolvedincitizenjuries,focusgroups,provisionofdataetc
37

CentreforAppliedHealthEconomics
Questions?
Thank you