Embed Size (px)
Citation preview
dr sumer yadav
What is Obesity?
Obesity means excess accumulation of fat in the body
Once it develops it is difficult to ‘cure’ and usually persists throughout life
Obesity is usually diagnosed on the basis of calculation of Body mass indexMeasurement of waist-hip ratio
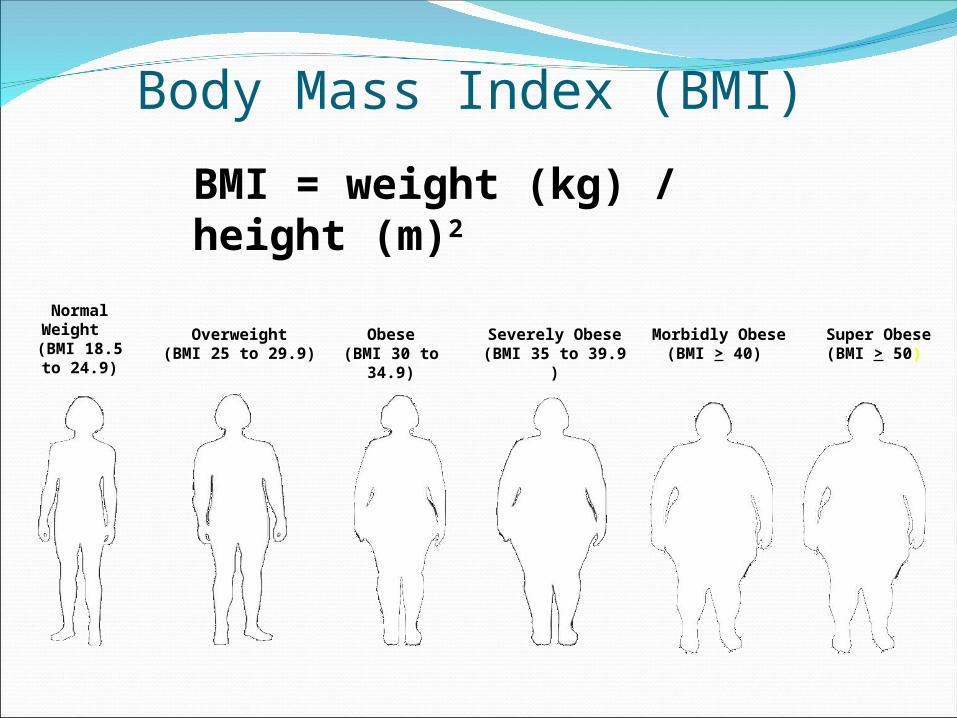
Normal Weight
(BMI 18.5 to 24.9)
Overweight(BMI 25 to 29.9)
Obese(BMI 30 to 34.9)
Severely Obese(BMI 35 to 39.9 )
Morbidly Obese(BMI > 40)
Body Mass Index (BMI)
Super Obese(BMI > 50)
BMI = weight (kg) / height (m)2
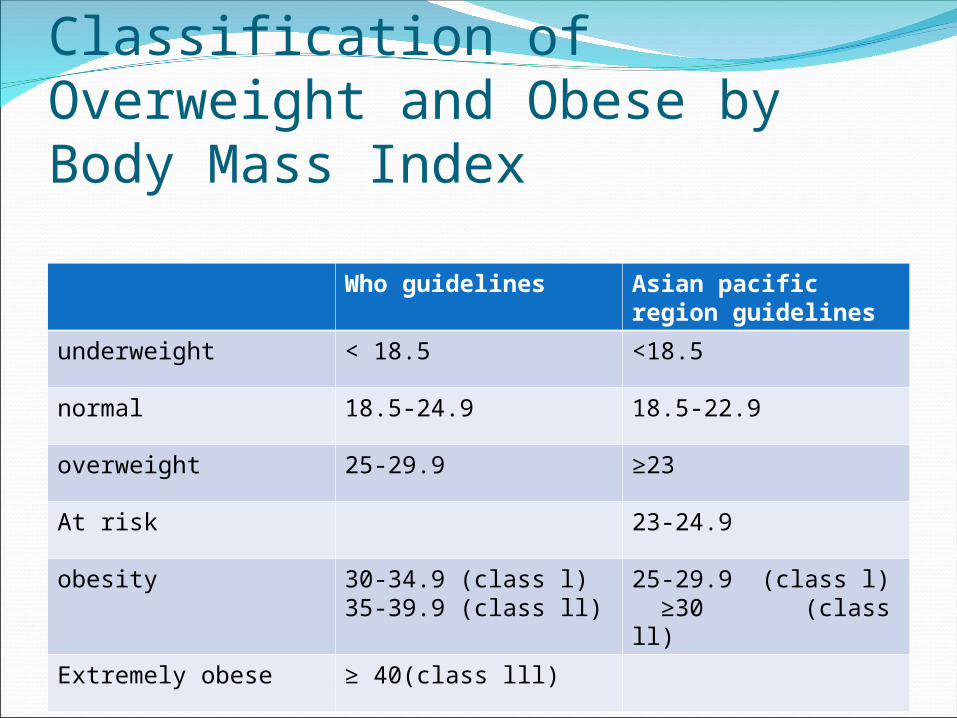
Classification of Overweight and Obese by Body Mass Index
Who guidelines Asian pacific region guidelines
underweight < 18.5 <18.5
normal 18.5-24.9 18.5-22.9
overweight 25-29.9 ≥23
At risk 23-24.9
obesity 30-34.9 (class l)35-39.9 (class ll)
25-29.9 (class l) ≥30 (class ll)
Extremely obese ≥ 40(class lll)
Morbid obesityMorbid obesity is defined as when BMI is more
than 40 kg/ m2 or more than 35 kg/ m2 in the presence of co-morbidities
Waist-to-hip ratio
Risk increase if waist circumference is more than 94 cm in men and > 80 cm in women
Waist : Hip ratiodesired
ratiomen :≤ 1
women :≤0.8
Obesity – An imbalance in energy intake and energy expenditure
The Obesity EpidemicThe weight gain cycle
Eat too muchGain weight
Can’tExercise
GetDepressed
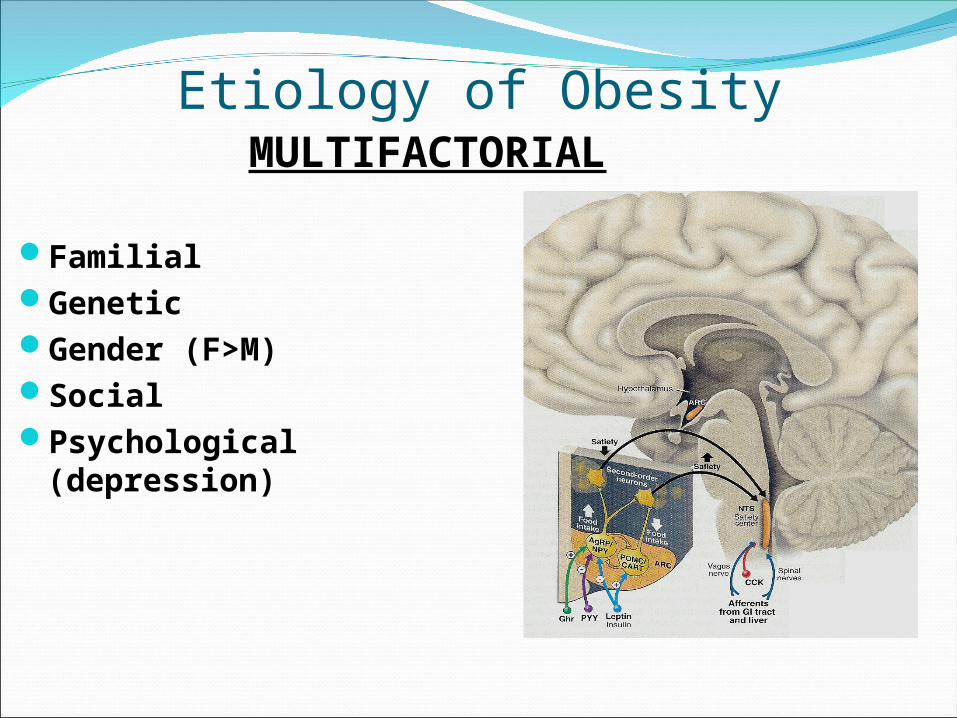
Etiology of Obesity
FamilialGeneticGender (F>M)SocialPsychological (depression)
MULTIFACTORIAL
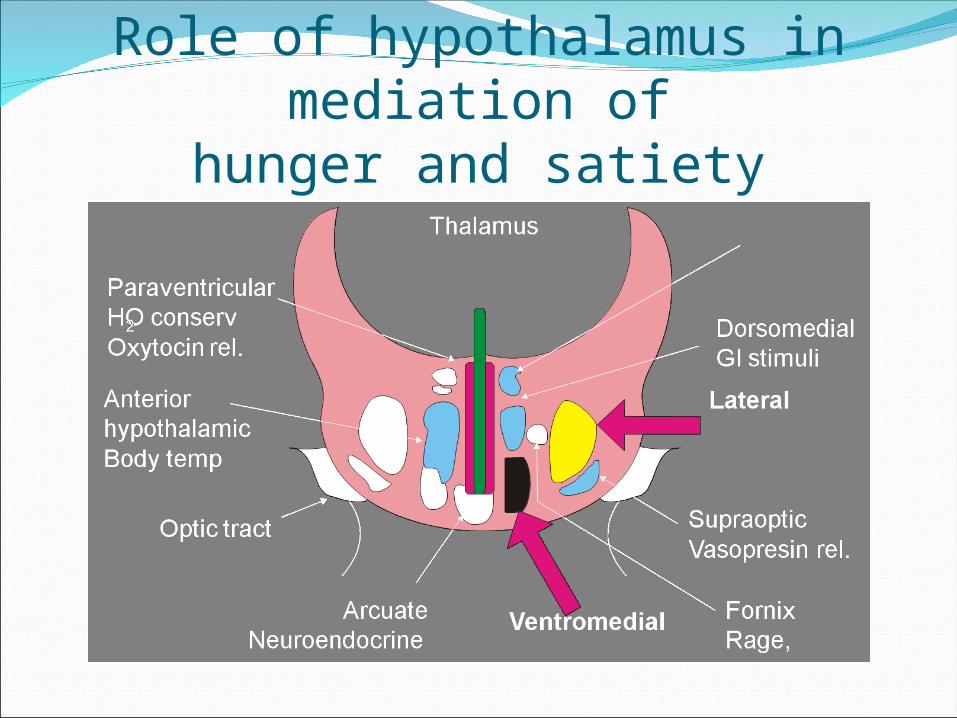
Role of hypothalamus in mediation ofhunger and satiety
2nd only to smoking as the leading cause of
preventable death in the United States.†
> 110,000 deaths/year in the US are associated with
obesity*
Life Expectancy
* Flegal KM et al. JAMA. 2005 Apr 20;293(15):1861-7. † † CDCCDC
Classification of obesity as per fat distribution
Android (or abdominal or central, males)-Collection of fat mostly in the abdomen (above the waist)
-apple-shaped
-Associated with insulin resistance and heart disease
Gynoid (below the waist, females)
• Collection of fat on hips and buttocks
•pear-shaped
-Associated with mechanical problems
Co-morbidities
EndocrineDiabetes
CardiovascularHypertensionHyperlipidemiaHypertriglyceridemiaCoronary and
cerebral vascular disease
Venous stasis
GynecologyInfertilityMenstrual
irregularitiesOrthopedic
DJDArthralgiaLow back pain
DermatologyFungal infection
Co-morbiditiesPulmonary
Sleep apneaAsthmaHypoventilationPulmonary
hypertension
GastrointestinalCholelithiasisGERDFatty liver /dysfunction
Socio-economicDiscrimination
PsychologicalDepressionh/o abuse
CancerEndometrialOvarianbreast
Why do we treat obesity??
• Co-morbidities
• Quality of life
• Survival – Life Expectancy
Advantages of weight loss
Weight loss of 0.5-9 kg (n=43,457) associated with 53% reduction in cancer-deaths, 44% reduction in diabetes-associated mortality and 20% reduction in total mortality
Survival increased 3-4 months for every kilogram of weight loss
Reduced hyperlipidemia, hypertension and insulin resistanceImprovement in severity of diseasesPerson feels ‘fit’ and mentally more active
Treatment goals
Prevention of further weight gainWeight loss to achieve a realistic, target BMILong-term maintenance of a lower body-weight
How much weight loss is significant?
A 5-10% reduction in weight (within 6 months) and weight maintenance should be stressed in any
weightloss program and contributes significantly to
decreased morbidity
Medical TreatmentMedications Dietary ChangesExerciseBehavioral TherapyPsychotherapyHypnosisJaw-wiring
UNSUCCESSFUL AT SIGNIFICANT OR SUSTAINED WEIGHT LOSS!
Drug therapyAppetite suppressants1. Adrenergic agents (e.g. amphetamine, methamphetamine,
phenylpropanol amine, phentermine)2. Serotonergic agents (e.g. fenfluramine, dexfenfluramine,
SSRIs like sertraline, fluoxetine)Thermogenic agents1. ephedrine, 2. caffeineNew ones1. Sibutramine2. Orlistat
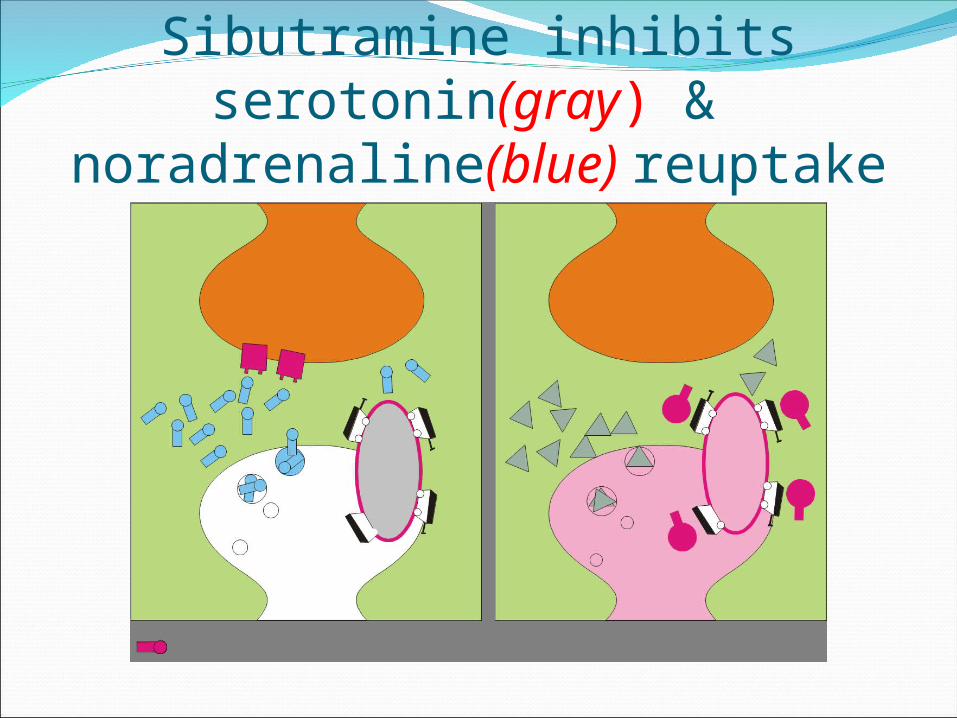
Sibutramine inhibits serotonin(gray) & noradrenaline(blue) reuptake
22
Why Surgery for the Treatment of the Clinically Severe Obese?“Only surgery has proven effective over the long term for most patients with clinically severe obesity.”
- NIH Consensus Conference Statement, 1991
Surgery for the treatment of clinically severe obesity is endorsed by:
The National Institutes of Health
The American Medical Association
The National Institute of Diabetes and Digestive and Kidney Diseases
American Association of Family Practitioners
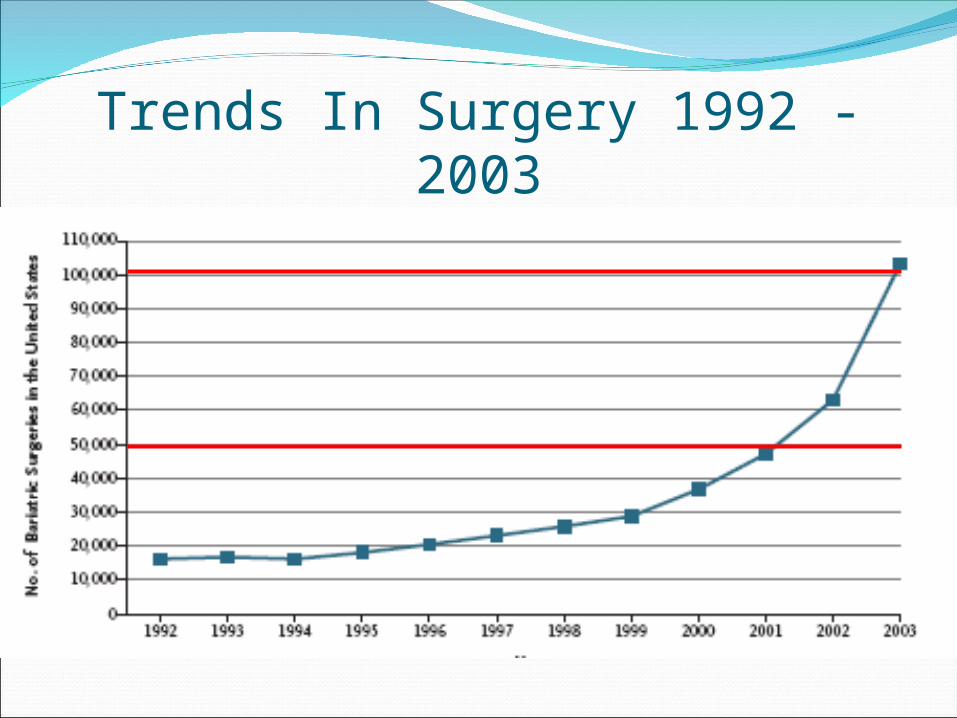
Trends In Surgery 1992 - 2003
Rationale for SurgeryLong Term Outcome Data
Sustained Weight LossImprovement or Resolution of Co-morbiditiesImproved long term survival
Minimally Invasive SurgeryPublic Awareness
Obesity as a diseaseCelebrities
Indications for Surgery
BMI >40 kg/m2, or >35 kg/m2 with significant co-morbid illnesses
Multiple failed weight loss attempts
Acceptable surgical risk
Age 18-60
Demonstrates commitment and understanding of weight loss following bariatric surgery
26
Ineligible PatientsExclusion Criteria:Obesity related to a metabolic or endocrine disorderHistory of substance abuse or untreated major psychiatric
diseaseSurgery contraindicated or high riskWomen who want to become pregnant within the next 18
months
Preoperative Evaluation/EducationStaff evaluation
InternistDietitianPsychologistNurseSurgeonSupport group
•Laboratory evaluation• Blood• ECG, CXR • Stress Test• Sleep study• EGD• PFTs
Consider an IVC filter for any patient with prior history of DVT/PE.
Surgical TreatmentRestrictive
Malabsorptive
•Horizontal gastroplasty•Vertical banded gastroplasty (VBG)•Adjustable gastric band•Sleeve gastrectomy•Roux-en-Y gastric bypass
•Jejunoilial bypass•Biliopancreatic diversion (Scopinaro)•Biliopancreatic diversion w/ duodenal switch
29
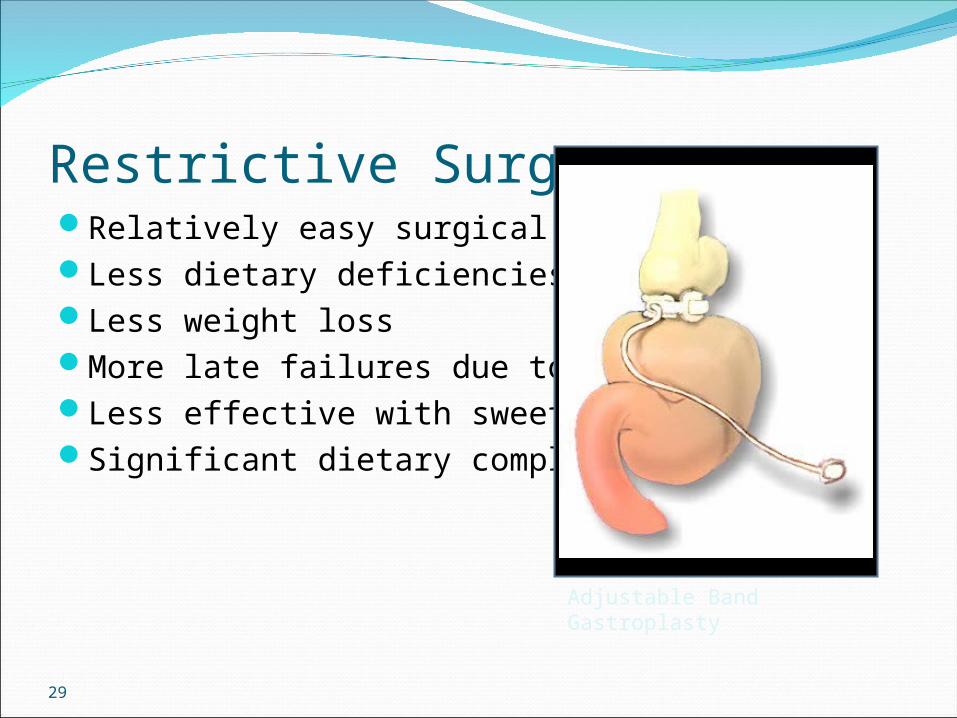
Restrictive SurgeryRelatively easy surgical procedureLess dietary deficienciesLess weight lossMore late failures due to dilationLess effective with sweet eatersSignificant dietary compliance
Adjustable Band Gastroplasty
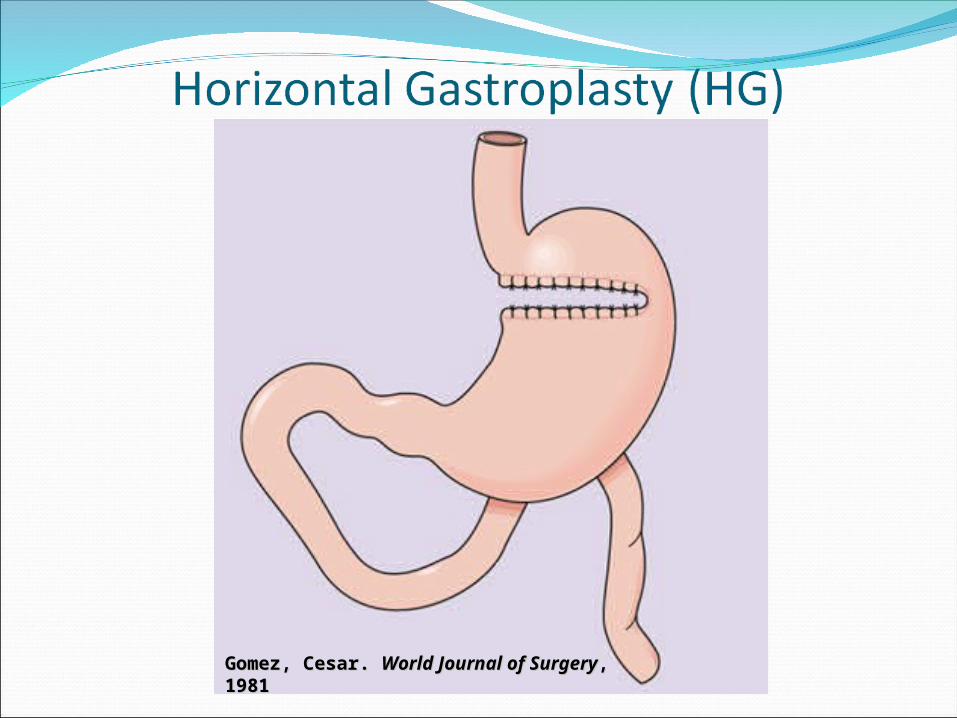
Gomez, Cesar. Gomez, Cesar. World Journal of SurgeryWorld Journal of Surgery, 1981, 1981
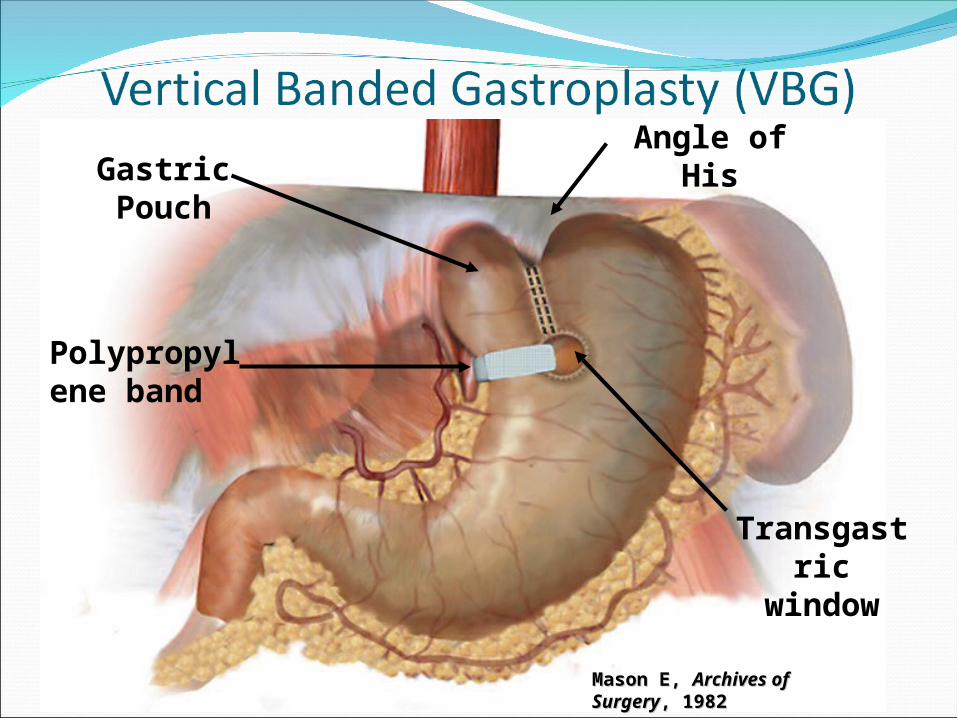
Mason E, Mason E, Archives of SurgeryArchives of Surgery, , 19821982
Polypropylene band
Transgastric window
Angle of HisGastric
Pouch
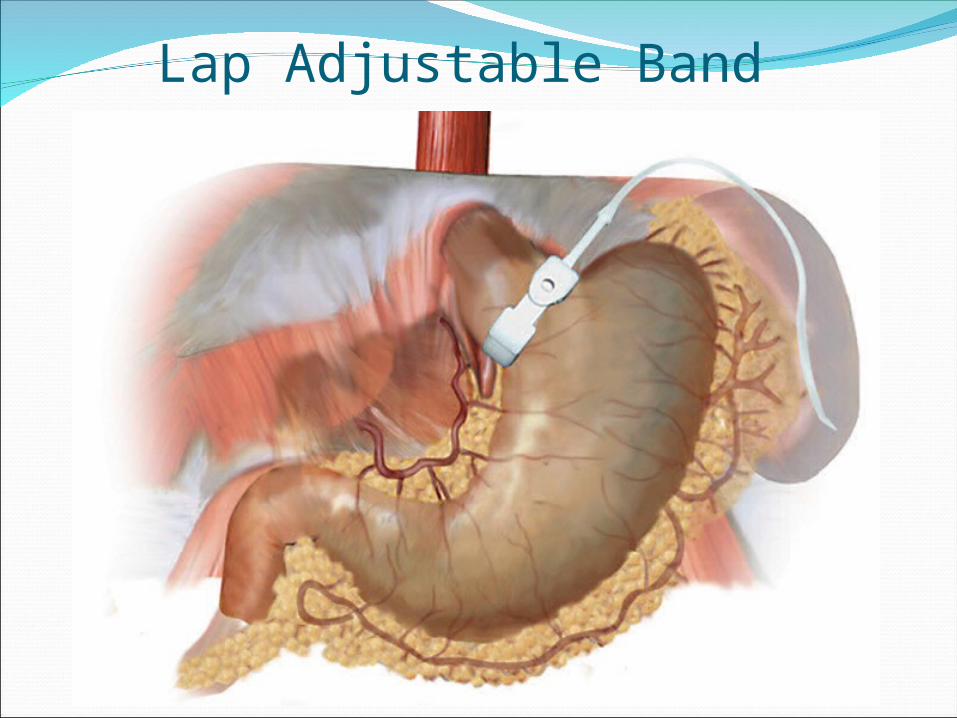
Lap Adjustable Band
• Port displacement/tube break 7%• Wound infection 4%• Stoma obstruction 2%• Slippage 2%• Elective removal 2%• Erosion <1%• Conversion to open <1%• Hemorrhage <1%• Death <0.05%
Complications: Adjustable Gastric Banding
Sleeve gastrectomy Sleeve gastrectomy
It is a surgical weight-loss procedure in which the stomach is reduced to about 15% of its original size, by surgical removal of a large portion of the stomach, following the major curve The open edges are then attached together (often with surgical staples) to form a sleeve or tube with a banana shape. The procedure permanently reduces the size of the stomach. The procedure is performed laparoscopically and is not reversible.
35
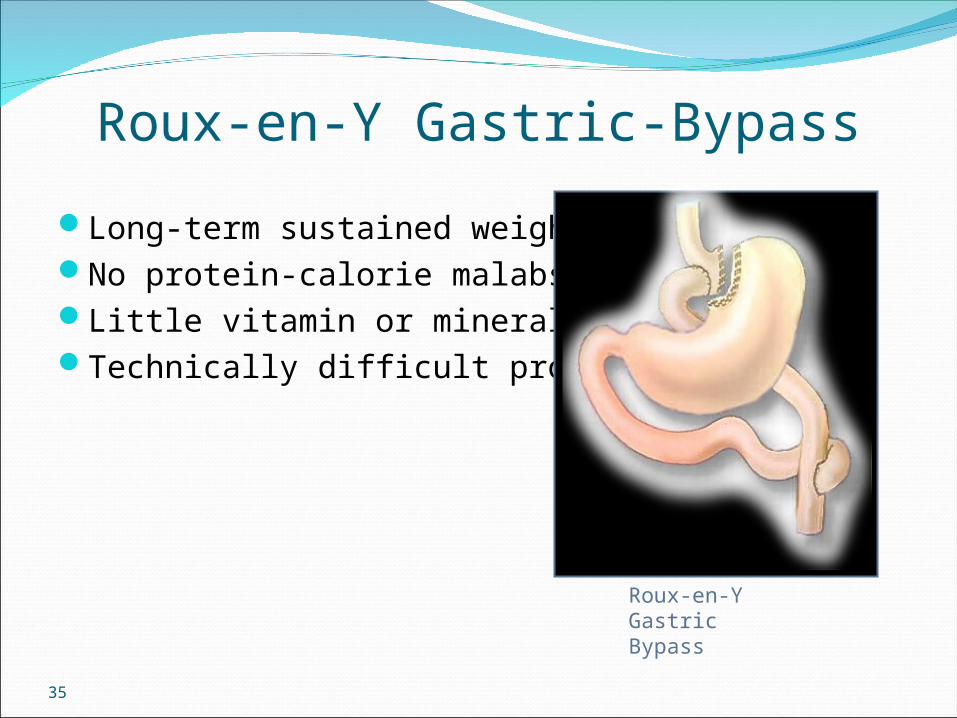
Roux-en-Y Gastric-Bypass
Long-term sustained weight lossNo protein-calorie malabsorptionLittle vitamin or mineral deficienciesTechnically difficult procedure
Roux-en-Y Gastric Bypass
36
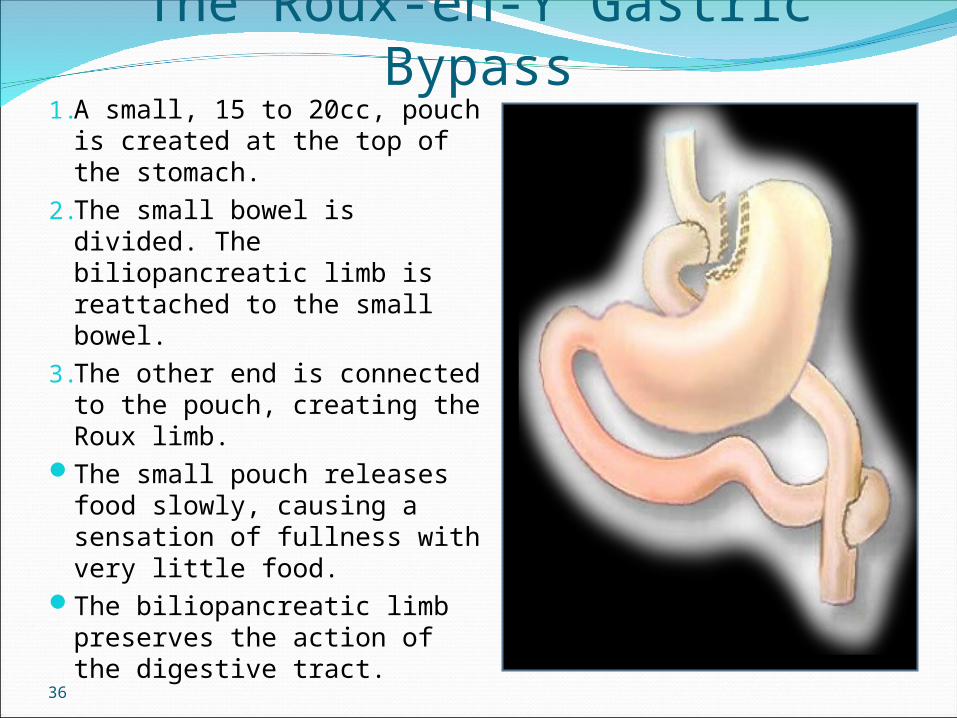
The Roux-en-Y Gastric Bypass1. A small, 15 to 20cc, pouch is
created at the top of the stomach.
2. The small bowel is divided. The biliopancreatic limb is reattached to the small bowel.
3. The other end is connected to the pouch, creating the Roux limb.
The small pouch releases food slowly, causing a sensation of fullness with very little food.
The biliopancreatic limb preserves the action of the digestive tract.
Roux-en-Y Gastric Bypass
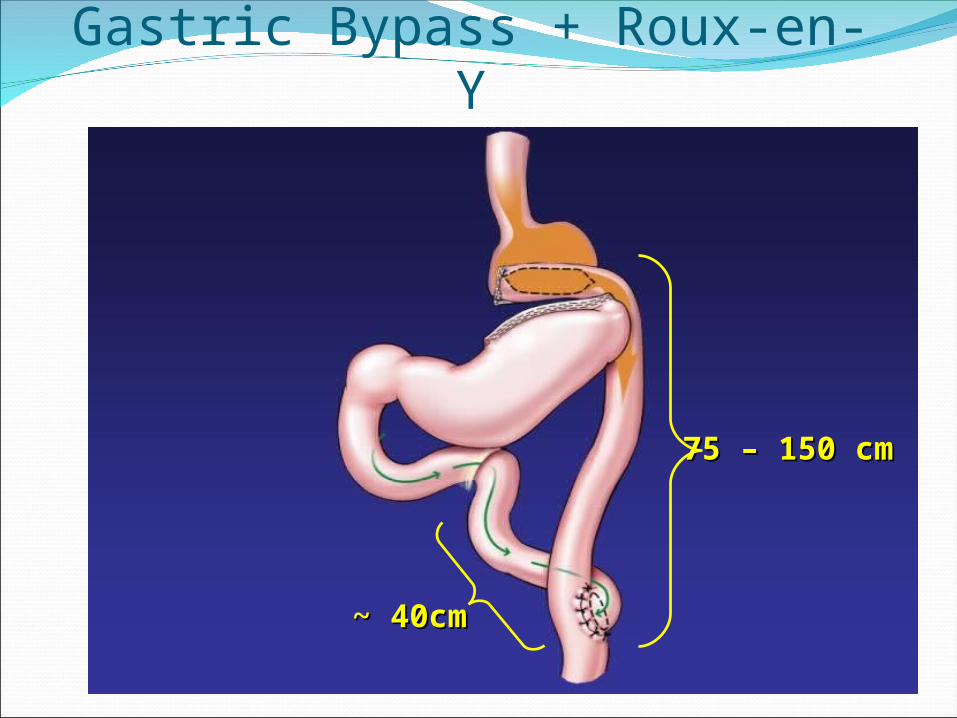
Gastric Bypass + Roux-en-Y
75 – 150 cm75 – 150 cm
~ 40cm~ 40cm
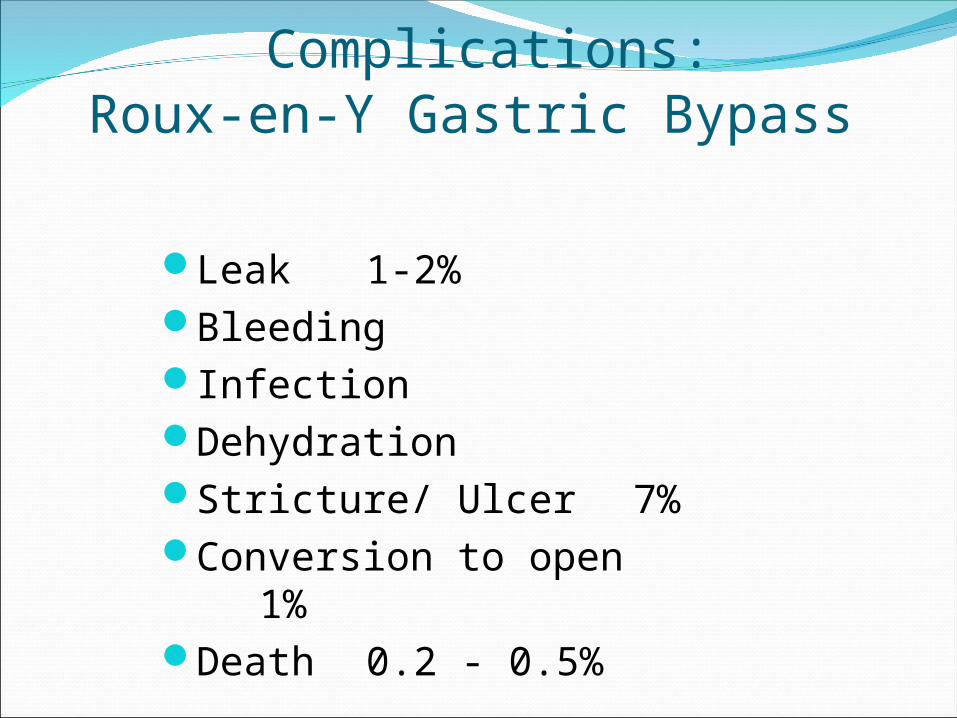
Complications:Roux-en-Y Gastric Bypass
Leak 1-2%BleedingInfectionDehydrationStricture/ Ulcer 7%Conversion to open 1%Death 0.2 - 0.5%
39
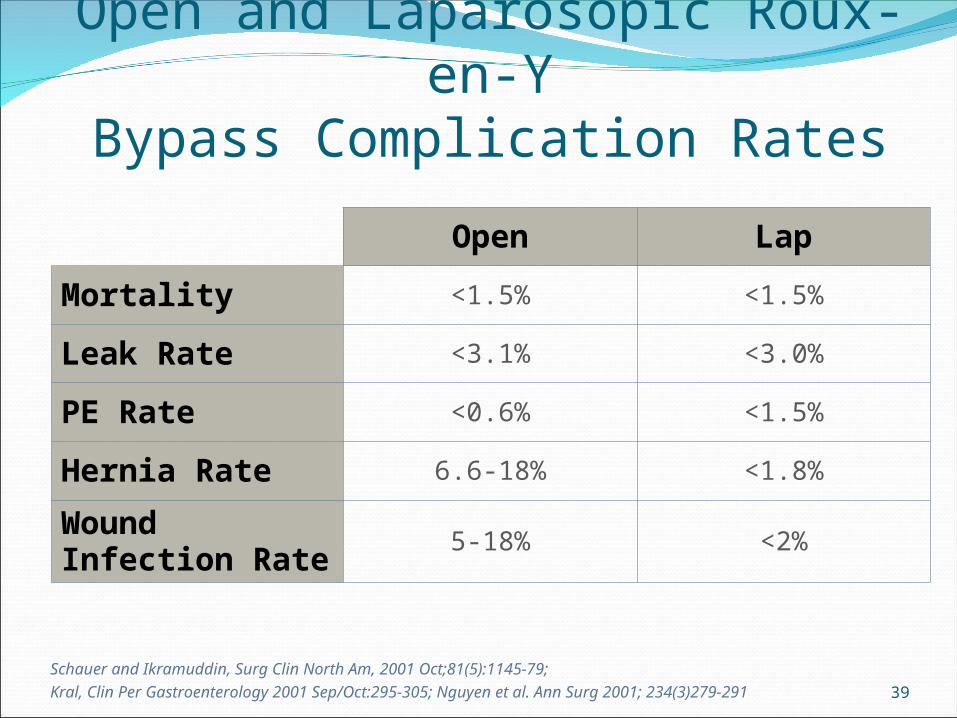
Open and Laparosopic Roux-en-YBypass Complication Rates
Schauer and Ikramuddin, Surg Clin North Am, 2001 Oct;81(5):1145-79; Kral, Clin Per Gastroenterology 2001 Sep/Oct:295-305; Nguyen et al. Ann Surg 2001; 234(3)279-291
Open Lap
Mortality <1.5% <1.5%
Leak Rate <3.1% <3.0%
PE Rate <0.6% <1.5%
Hernia Rate 6.6-18% <1.8%
Wound Infection Rate
5-18% <2%
40
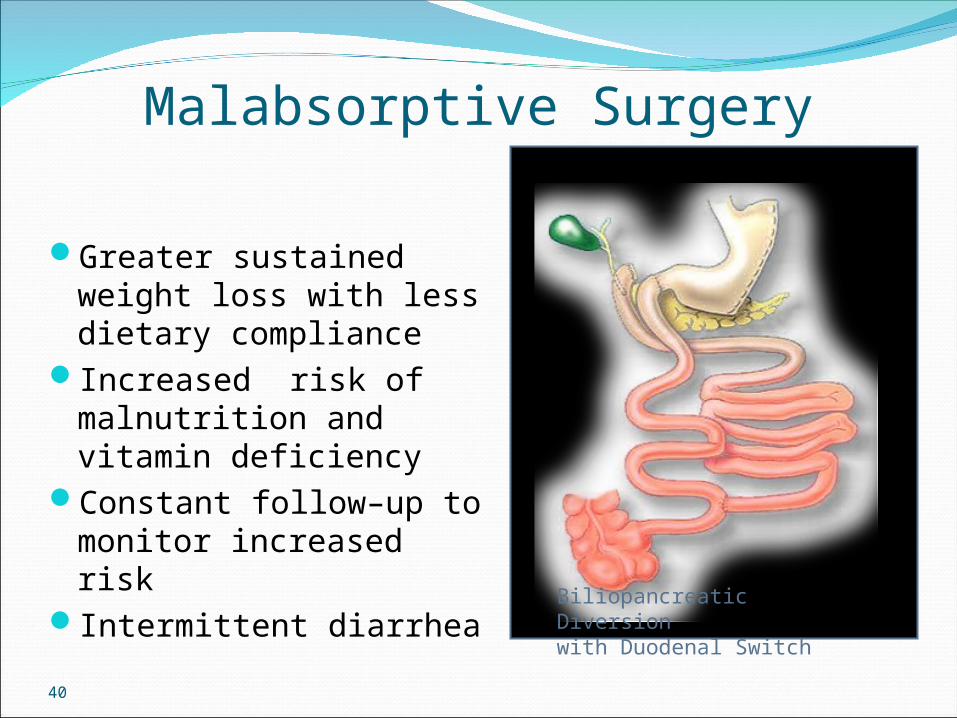
Malabsorptive Surgery
Greater sustained weight loss with less dietary compliance
Increased risk of malnutrition and vitamin deficiency
Constant follow–up to monitor increased risk
Intermittent diarrhea
Biliopancreatic Diversion with Duodenal Switch
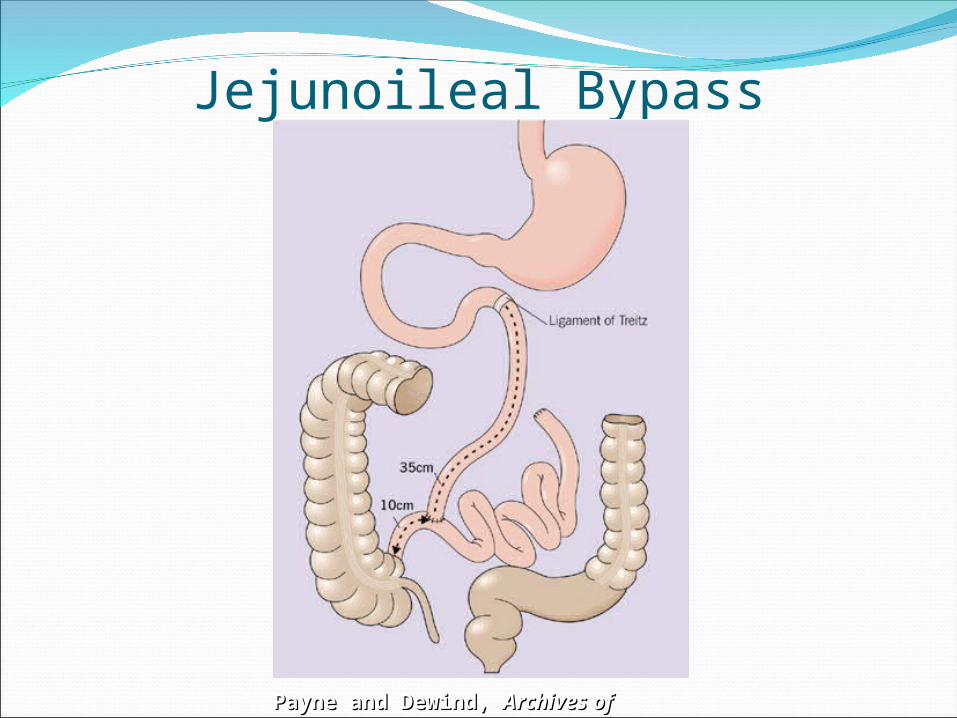
Jejunoileal Bypass
Payne and Dewind, Payne and Dewind, Archives of SurgeryArchives of Surgery, 1973, 1973
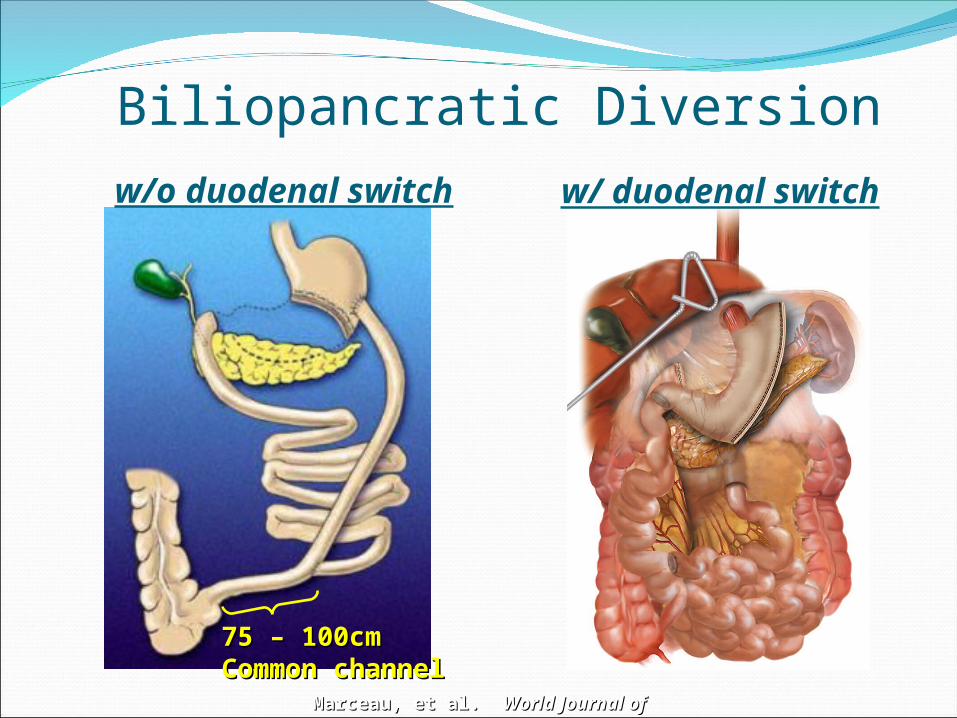
Biliopancratic Diversion
Marceau, et al. Marceau, et al. World Journal of SurgeryWorld Journal of Surgery, 1998, 1998
w/ duodenal switchw/o duodenal switch
75 – 100cm75 – 100cmCommon channelCommon channel
Complications:BPD with Duodenal Switch
Leak 1-2%BleedingInfectionDehydrationMalnutrition 5%Conversion to open 1%Death 0.5 – 1.1%
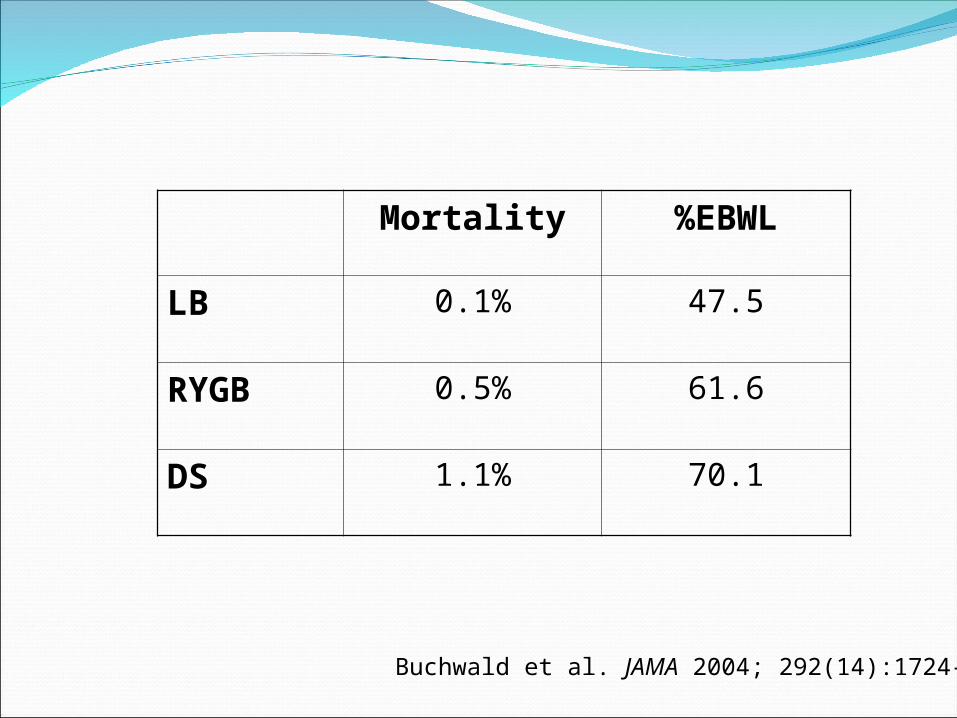
Mortality %EBWL
LB 0.1% 47.5
RYGB 0.5% 61.6
DS 1.1% 70.1
Buchwald et al. JAMA 2004; 292(14):1724-37
45
Open and Laparoscopic Technique in Bariatric Surgery
OpenIncreased post op pain,
longer hospitalizationsIncreased incidence
of wound complications - infections, hernias, seromas
Return to work in 4-8 weeks
Laparoscopic Less post op pain,
early mobilityWound complications
are significantly reduced
2-3 day hospital stayReturn to work in
1-3 weeks
46
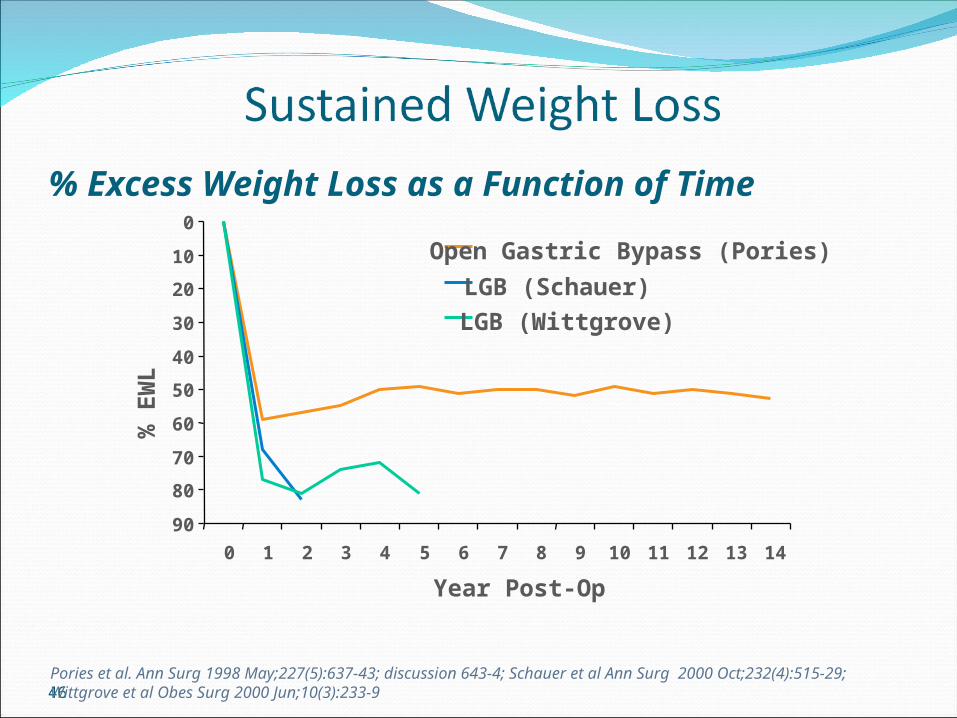
% Excess Weight Loss as a Function of Time
Pories et al. Ann Surg 1998 May;227(5):637-43; discussion 643-4; Schauer et al Ann Surg 2000 Oct;232(4):515-29; Wittgrove et al Obes Surg 2000 Jun;10(3):233-9
0
10
20
30
40
50
60
70
80
90
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
Year Post-Op
% E
WL
Open Gastric Bypass (Pories)LGB (Schauer)LGB (Wittgrove)
47
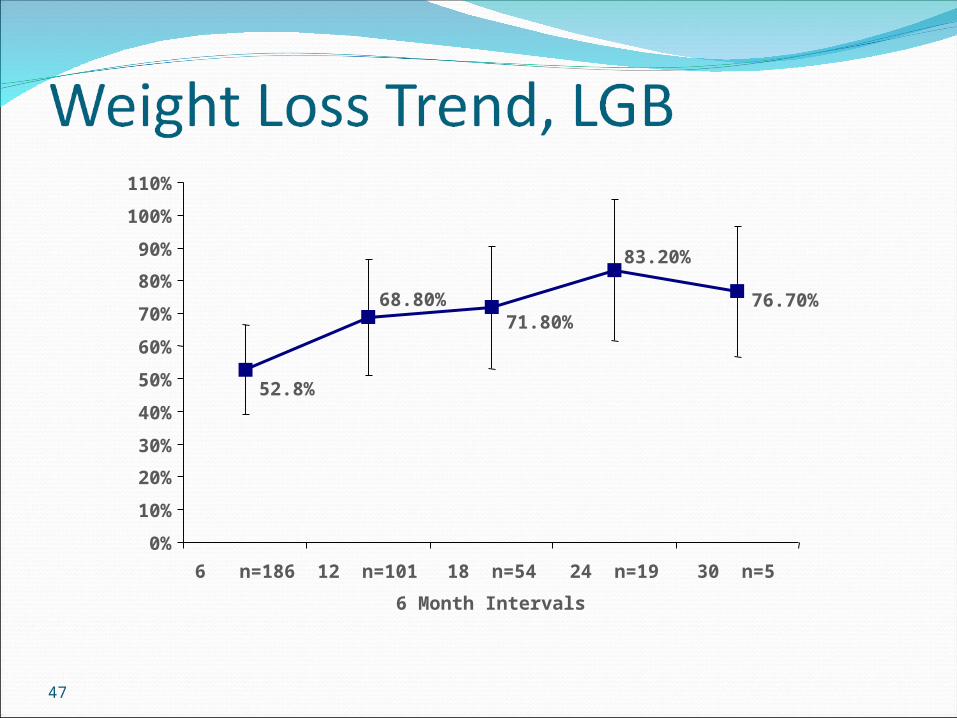
76.70%
83.20%
71.80%68.80%
52.8%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
110%
6 n=186 12 n=101 18 n=54 24 n=19 30 n=5
6 Month Intervals
48Schauer, et al, Ann Surg 2000 Oct;232(4):515-29
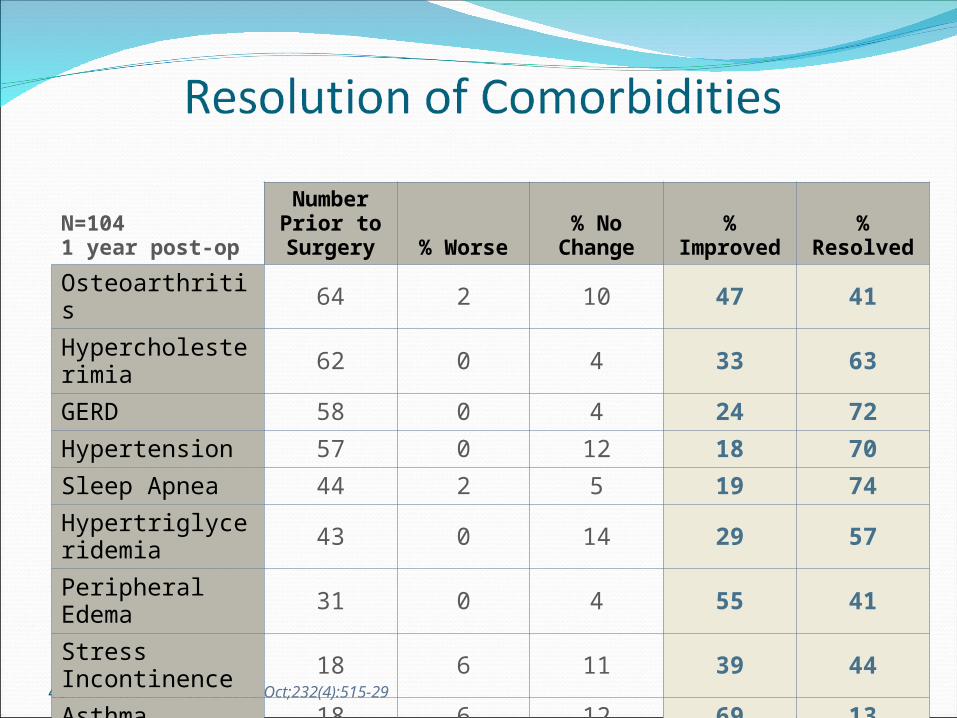
N=1041 year post-op
Number Prior to Surgery % Worse % No Change % Improved % Resolved
Osteoarthritis 64 2 10 47 41
Hypercholesterimia 62 0 4 33 63
GERD 58 0 4 24 72
Hypertension 57 0 12 18 70
Sleep Apnea 44 2 5 19 74
Hypertriglyceridemia 43 0 14 29 57
Peripheral Edema 31 0 4 55 41
Stress Incontinence 18 6 11 39 44
Asthma 18 6 12 69 13
Diabetes 18 0 0 18 82
Average 1.6% 7.8% 35.1% 55.7%
90.8%Improved or Resolved
49
Possible ComplicationsMay Lead to Short or Long-term Hospitalization and/or Re-operationInfection, bleeding or leaking at suture/staple linesBlockage of the intestines or pouchDehydrationBlood clots in legs or lungsVitamin and mineral deficiencyProtein malnutrition Incisional herniaDeath
50
Possible Side EffectsNausea and vomitingGas and bloatingDumping syndromeLactose intoleranceTemporary hair thinningDepression and psychological distressChanges in bowel habits such as diarrhea, constipation,
gas and/or foul smelling stool
51
Post-Operative Summary
On Average, Gastric-bypass Patients…Will find that they have lost 65-80% of their excess
body weight, the majority of it in the first 18 to 24 months after surgery.
May have rapid improvements in the morbid side effects of their obesity, such as type 2 diabetes, high blood pressure, sleep apnea, and high cholesterol levels.
52
53
Bariatric Surgery as a Tool
Bariatric Surgery Will Not Work Alone. Commitment to Diet, Exercise and Support are Intricate Parts of Your Weight Loss Success.

54
Pathway to Bariatric SurgeryPatient ResponsibilitiesHonesty, Responsibility, Cooperation
Bariatric Program ResponsibilitiesHonesty, Responsibility, Cooperation
55
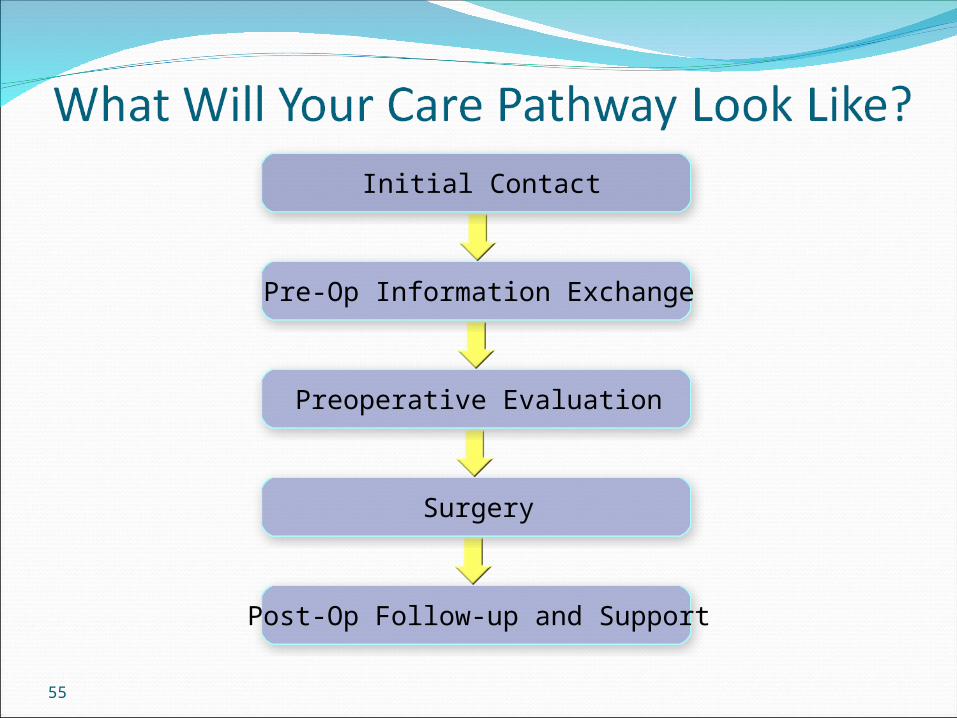
Post-Op Follow-up and Support
Surgery
Preoperative Evaluation
Pre-Op Information Exchange
Initial Contact
56
Who is My Dedicated Team?SurgeonRegistered Nurse CoordinatorRegistered Dietitian Psychologist/Social WorkerExercise SpecialistInsurance CoordinatorAdministrative Assistant
57
Gynecology
Internal Medicine
Anesthesiology
Gastroenterology
Reconstructive Surgery
Pulmonology
Cardiology Endocrinology
Multidisciplinary Approach

58
59
Support Groups – The Heart of the ProgramCreate fellowship through a common bond Provide a source of up-to-date information
about surgery and latest developmentsEducate in nutrition, exercise, and post-op
needsPromote networkingIncrease bariatric surgery successSupport life-style changes
60
61
Pre-operative Diet GoalsBegin Creating Healthy Nutritional
Patterns:Multivitamin and mineral intakeAdequate fluid intakeQuality versus quantityAvoiding the last supper syndrome
62
Diet
Stage I: A low sugar, clear liquid diet,
started two to three days after surgery. It essentially provides hydration during the initial post-operative phase.
Roux-en-Y Gastric Bypass
63
Diet (cont’d)
Stage II: A full liquid diet providing all the essential
requirements for the first post-operative month. Patients go home from the hospital on the stage II diet.
Stage III: A modified solid diet. The surgeon instructs the patient when to
advance to this diet. Introducing semi-solid food or solid diet too early may lead to obstruction and vomiting. It may also unduly stress the anastomosis.
64
Difficult FoodsBread productsCow milk productsPasta products Fatty foods and
fried foodsCandy, chocolate,
any sugary foods and beverages
Bran cereal and other bran products
Corn, whole beans, and peas
Dried fruits and skins of fresh fruit
CoconutCarbonated beverages
65
Fluids
Recommended fluid intake: min. 2 Liters/dayNon-carbonatedNon-calorieNot during mealsContinually sip water throughout the day to
ensure adequate hydrationAvoid caffeinated beveragesAvoid straws
66
Vitamins, Minerals and Supplements Liquid protein supplements required to reach
75 grams of protein per dayMultivitamin with Iron morning and evening1000 mg of folate/dayB-12 supplementations500 mg of Calcium Citrate three times per dayOther supplements on an individual need basisPeriodic blood levels must be taken to ensure
adequate nutrition
67
Dumping Syndrome
Dumping SyndromeEarly: immediately associated with food intake
(GI symptoms)Late: delayed onset, usually 1½ to 2 hours after
food intake (neurological symptoms)Some patients never experience Dumping Syndrome
Some surgeons consider dumping syndrome to be a beneficial effect of Gastric Bypass surgery.
It provides a quick and reliable negative feedback for intake in the “wrong” foods.
68
Long-term Diet Goals
Avoid concentrated sweets due to high calorie content and the possibility of dumping
Low fat, heart healthy dietMaintain adequate water intake
69
70
Your Role Before SurgeryCommit to improving your health
(diet, exercise, mental readiness)Discuss your health history with your surgeonAsk questions and vocalize concerns that you
may have about surgery or your careCommit to following all instructions on nutrition,
activity and other care after surgery
71
Your CommitmentAdhere to dietExercise dailyCommit to lifelong follow-upAttend at least 2 support group meetings pre-op
and participate regularly post-opBuy and take in vitamin and mineral supplements
for the rest of your lifeAvoid tobacco products lifelong and alcohol for
at least 1 year post-op