Embed Size (px)
Citation preview
Psychosocial Aspects of Living with Gaucher Disease
Wendy Packman, JD, PhDProfessor
Director, Pediatric Psychology
and JD-PhD Program in Psychology and LawPacific Graduate School of Psychology at Palo Alto University
Gaucher Patient Meeting: 2014
Outline
Psychosocial issues in inborn errors (IEM): general concepts
Research: Gaucher disease (GD) Quantitative findings Qualitative findings
Coping strategies Psychosocial and neurocognitive
issues in GD: Pediatric patients
Psychosocial Issues
IEM are chronic diseases Infancy through adulthood Affect family system
Clinical presentations of IEM are variable: Metabolic decompensation Neurological symptoms Multi-system organ involvement Developmental delays Behavioral problems
Sources of Psychological Stress For Patients:
Secondary to disease pathology and toxicity
From stressors inherent in living with chronic illness
For Parents and Families: Having a loved one with an inborn error
(Emotional & financial stress, loss of friends, lack of freedom, medication management)
From: Weber S, Segal S, & Packman W (2012), Molec Genet Metab 105: 537-541
Focus of Our Research
What are the psychosocial stressors in a given inborn error?
What are the reactions to the stressors in a given disorder?
Disorders Studied in Our Research
MSUD Galactosemia PKU Hunter syndrome [MPS II] Niemann-Pick B Fabry disease Gaucher disease
Psychological Complications of Patients with Gaucher Disease
W. Packman, T. Crosbie, A. Riesner,C. Fairley, & S. Packman
J Inherit Metab Dis 2006; 29(1):99-105.
Psychological Aspects of Patients with GD: Research Questions
1. Is there a typical psychological profile associated with GD?
2. How does this compare with profiles of other patients with chronic illnesses?
3. Are psychological profiles different for individuals related to severity of symptoms and length of time on ERT?
4. What is the psychological impact of GD on psychosocial functioning?
Psychological Aspects of Patients with GD
Demographic questionnaire Minnesota Multiphasic Personality Inventory
(MMPI-2 ) 567 true-false items to assess personality features Used in chronic illness and chronic pain populations to
assess psychological functioning Semi-structured interview
Initial reaction to diagnosis of GD Daily hardships as a result of their condition Perceived quality of life Relationships with family and friends, stressors
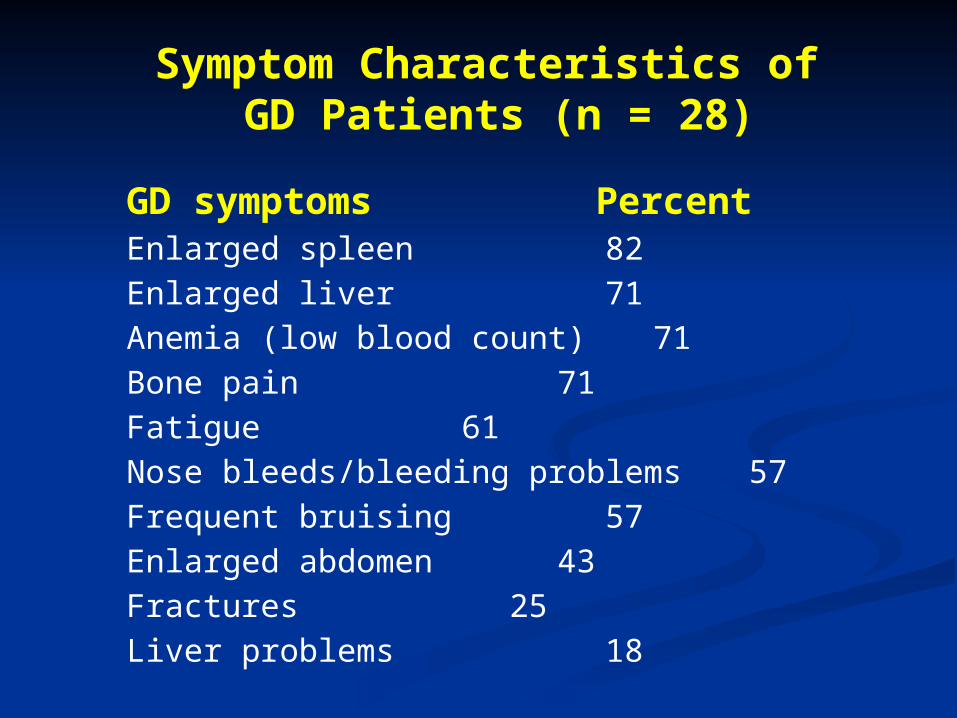
GD symptoms Percent Enlarged spleen 82
Enlarged liver 71
Anemia (low blood count) 71
Bone pain 71
Fatigue 61
Nose bleeds/bleeding problems 57
Frequent bruising 57
Enlarged abdomen 43
Fractures 25
Liver problems 18
Symptom Characteristics of GD Patients (n = 28)
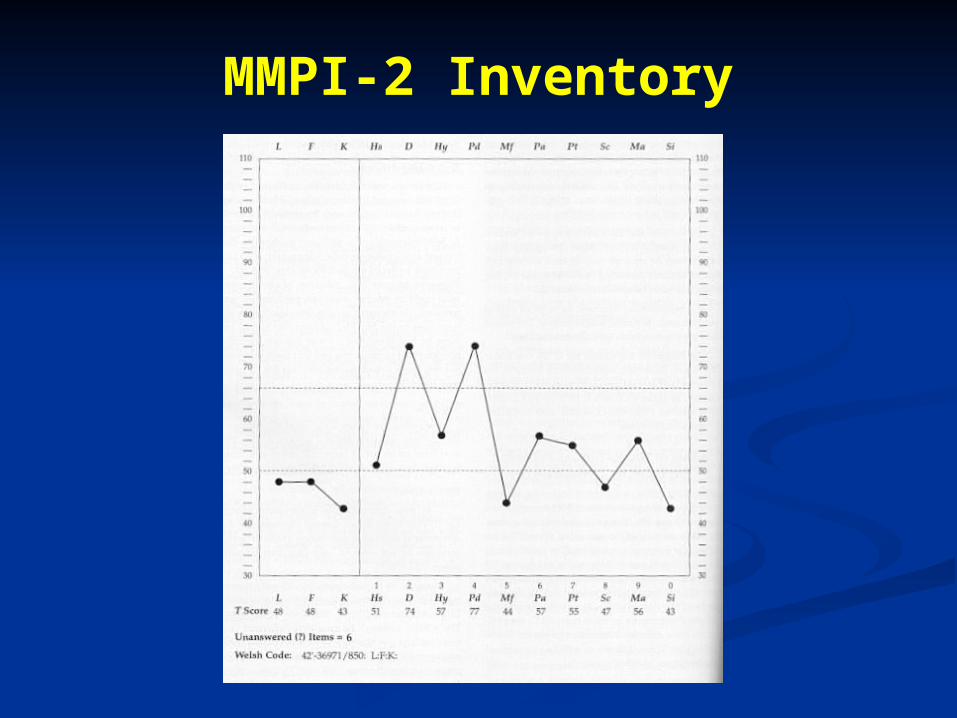
MMPI-2 Inventory
MMPI: Validity Scales
The validity scales include: Lie scale (L), which measures the tendency
to present oneself in a positive light Infrequency (F) scale, which detects unusual
or atypical responses to the test questions Correction (K) scale, which measures test
defensiveness and problem denial
MMPI: Clinical Scales
1 (Hs) Hypochondriasis 2 (D) Depression 3 (Hy) Hysteria4 (Pd) Psychopathic deviate5 (Mf) Masculinity-femininity6 (Pa) Paranoia 7 (Pt) Psychasthenia 8 (Sc) Schizophrenia 9 (Ma) Hypomania 0 (Si) Social introversion
Findings from MMPI-2
Comparison of Psychological Profiles Between GD Participants and Normative Sample
Patients with GD scored significantly higher than MMPI-2 normative sample on MMPI-2 scales Validity (K) Hypochondriasis (Hs) Depression (D) Hysteria (Hy) Psychasthenia (Pt) Schizophrenia (Sc)
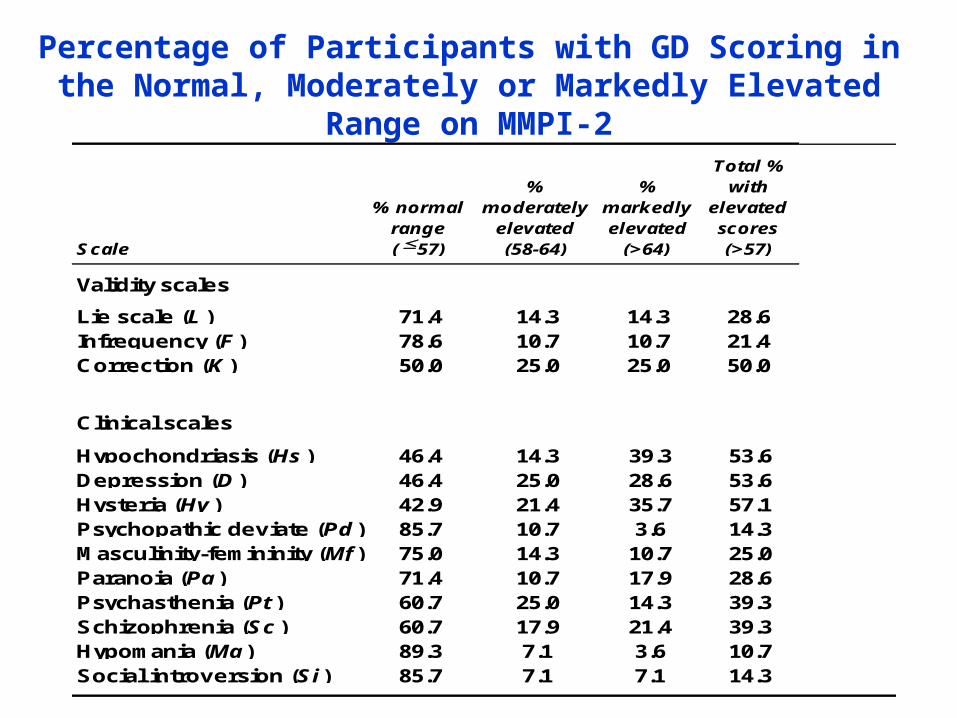
Percentage of Participants with GD Scoring in the Normal, Moderately or Markedly Elevated Range on MMPI-2
Scale
% normalrange(57)
% moderately
elevated(58-64)
% markedlyelevated
(>64)
Total % with
elevatedscores (>57)
Validity scales
Lie scale (L ) 71.4 14.3 14.3 28.6Infrequency (F ) 78.6 10.7 10.7 21.4Correction (K ) 50.0 25.0 25.0 50.0
Clinical scales
Hypochondriasis (Hs ) 46.4 14.3 39.3 53.6Depression (D ) 46.4 25.0 28.6 53.6Hysteria (Hy ) 42.9 21.4 35.7 57.1Psychopathic deviate (Pd ) 85.7 10.7 3.6 14.3Masculinity-femininity (Mf ) 75.0 14.3 10.7 25.0Paranoia (Pa ) 71.4 10.7 17.9 28.6Psychasthenia (Pt ) 60.7 25.0 14.3 39.3Schizophrenia (Sc ) 60.7 17.9 21.4 39.3Hypomania (Ma ) 89.3 7.1 3.6 10.7Social introversion (Si ) 85.7 7.1 7.1 14.3
MMPI-2 Findings
Clinical scales (Hs, D, Hy) suggest reactions that are common among chronically ill individuals: Somatic concerns, sadness Emotional distress, tension Under stressful situations -- increase in
physical symptoms and suffering Comparable to scores of patients with
other IEM and chronic disorders
Findings from Interviews
From: Packman, Crosbie, Behnken, Eudy, & Packman (2010). Am J Medical Genetics 152A, 2002-2010.
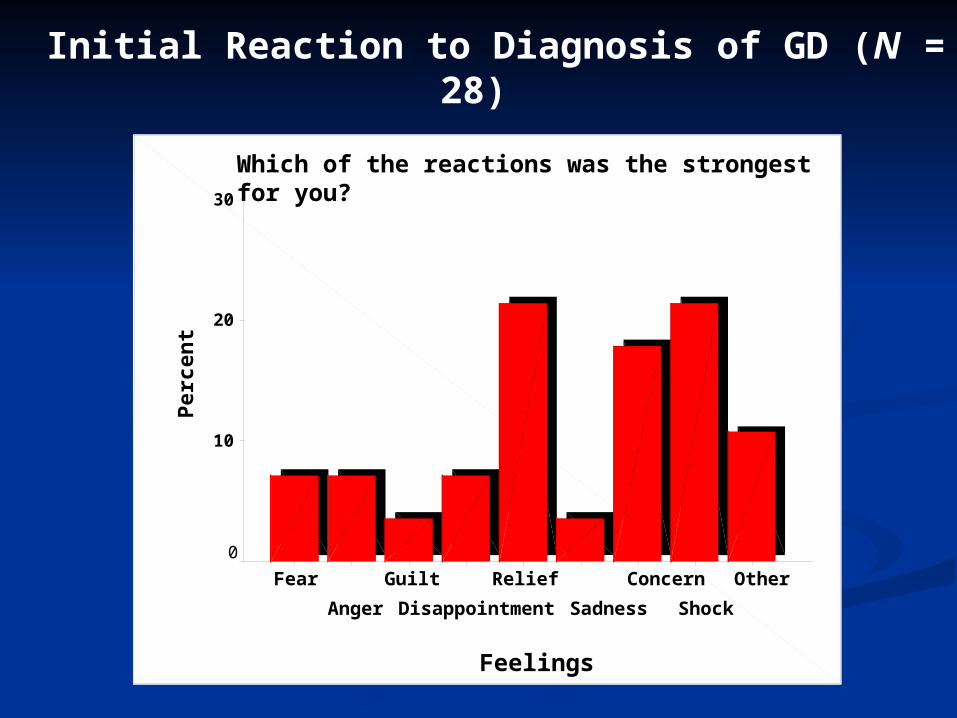
Initial Reaction to Diagnosis of GD (N = 28)
Which of the reactions was the strongest for you?
Feelings
Other
Shock
Concern
Sadness
Relief
Disappointment
Guilt
Anger
Fear
Per
cen
t30
20
10
0
Coping with the Diagnosis
Feelings of relief -- the naming of the illness finally put an end to the frightening and ambiguous questions that surrounded their physical health. Several participants stated:
“it was good to have an answer.’’ The diagnosis of GD also helped to rule out
potentially more fatal illnesses such as leukemia and lymphoma.
Concern or shock were also prominent reactions.
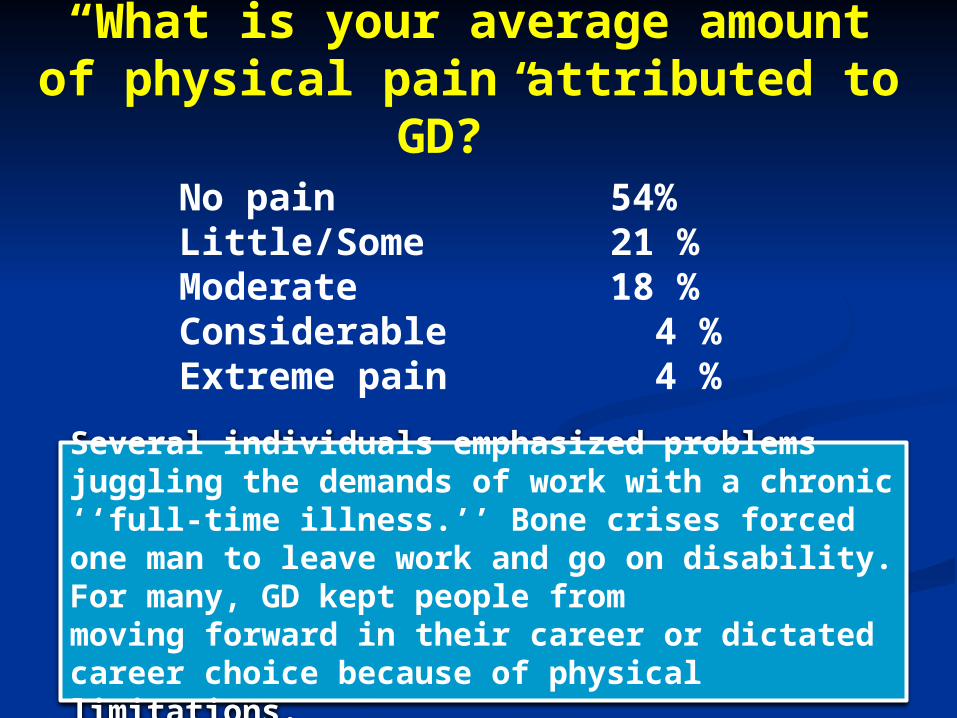
“What is your average amount of physical pain attributed to GD?”
Several individuals emphasized problems juggling the demands of work with a chronic ‘‘full-time illness.’’ Bone crises forced one man to leave work and go on disability. For many, GD kept people frommoving forward in their career or dictated career choice because of physical limitations.
No pain 54%Little/Some 21 %Moderate 18 %Considerable 4 %Extreme pain 4 %
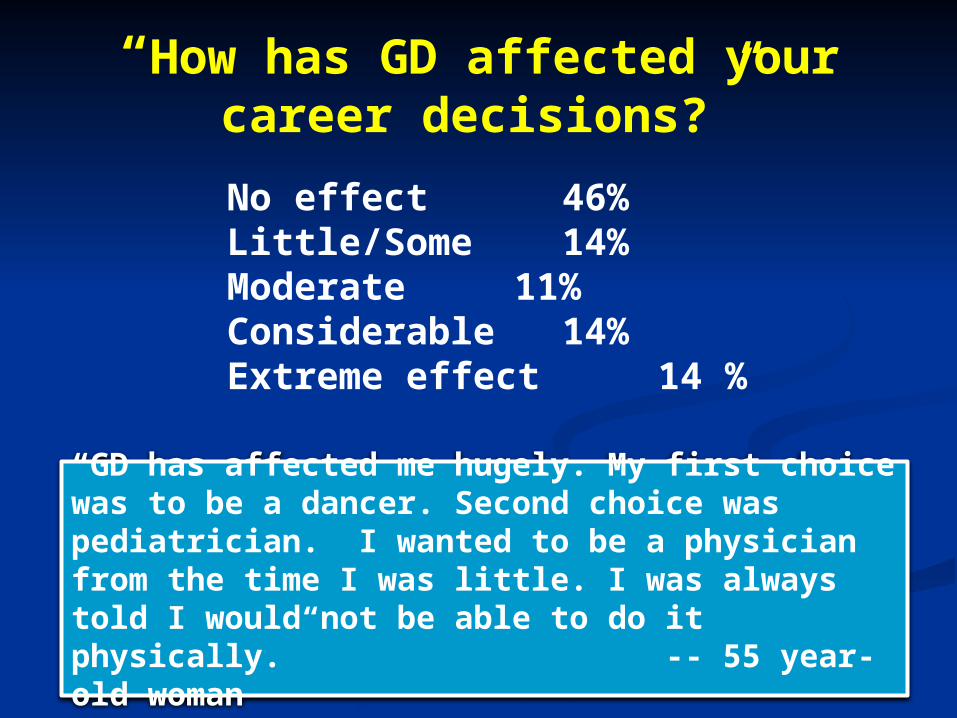
“How has GD affected your career decisions?”
“GD has affected me hugely. My first choice was to be a dancer. Second choice was pediatrician. I wanted to be a physician from the time I was little. I was always told I would not be able to do it physically.” -- 55 year- old woman
No effect 46%Little/Some 14%Moderate 11%Considerable 14%Extreme effect 14 %
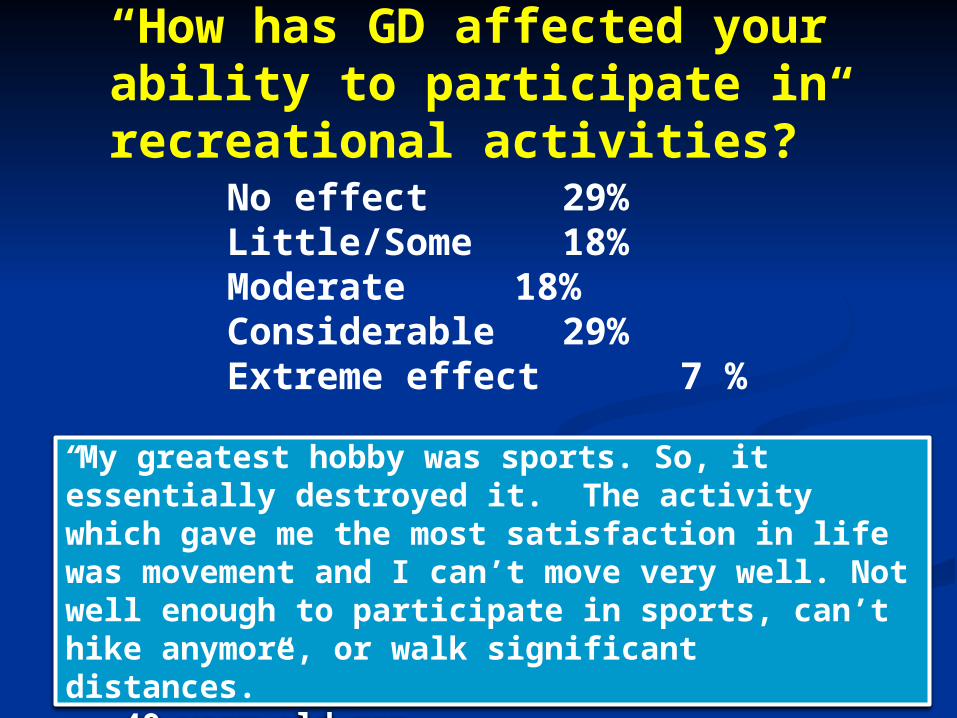
“How has GD affected your ability to participate in recreational activities?”
“My greatest hobby was sports. So, it essentially destroyed it. The activity which gave me the most satisfaction in life was movement and I can’t move very well. Not well enough to participate in sports, can’t hike anymore, or walk significant distances.” -- 49 year-old man
No effect 29%Little/Some 18%Moderate 18%Considerable 29%Extreme effect 7 %
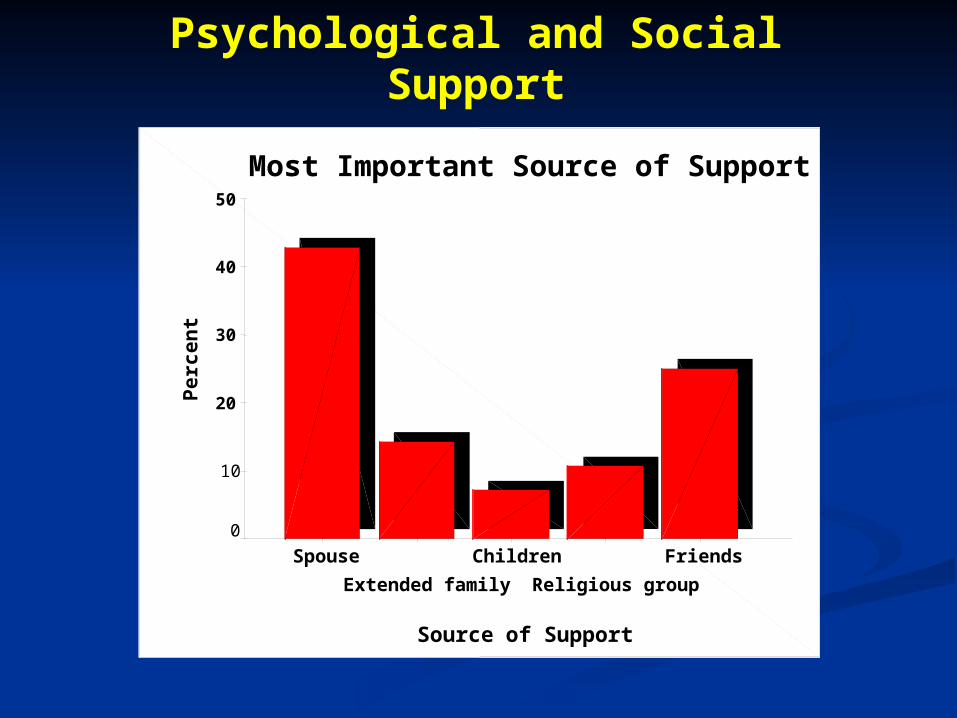
Psychological and Social Support
Most Important Source of Support
Source of Support
Friends
Religious group
Children
Extended family
Spouse
Pe
rce
nt
50
40
30
20
10
0
“How has GD affected your relationships with your immediate family?”
Participants indicated that having GD deepened their family relationships, improved communication between family members, and that the family felt protective. Participants also described friends as supportive and understanding.
No effect 54%Little/Some 21%Moderate 4%Considerable 18%Extreme effect 4%
Quality of Life
Currently on ERT: 82% (range 1 to 13 ys) 65% on ERT for 9+ ys Quality of life since beginning ERT
Extreme improvement 35% Considerable 26% Moderate 9% Some 17% No improvement 13%
“How does your outlook on life compare with that of other people you know?”
“I’m very optimistic. I think I appreciate life more than other people because of my experience with illness.” –20 year-old man
7% Much better outlook 26% A little better19% About the same48% Quite a bit worse
Suggestions: Improving the Care of Individuals with GD
“Listen, feel like I’m being listened to. I think it would be helpful if the health profession didn’t project what they think they know about the disease.” –55 year-old woman
“I struggle with how do you have healthcare providers help with the frustrations of dealing with chronic illness? I guess I’m looking for empathy and acknowledgement of how frustrating it is to be sick so often.” – 59 year-old woman
Stressors
Major stressors include psychological turmoil: Coping with uncertainties of a chronic
illness Coping with insurance Impact of GD on career and
recreational activities Finances
Reactions
Anxiety, worries, increased stress (35%)
Sadness and depression (25%) Somatic concerns as noted on
MMPI-2 Pain and Physical injury Existential fears
Stress-related Growth
GD had a positive influence on lives (70%) Strong relationships with family and
friends Positive outlook on life More empathic and compassionate Optimistic Able to see the bigger picture more
than others Happy with their own life
Coping Strategies
You are not your illness –What gives your life meaning?
Self-nurturing Exercise Stress-reducing Practices (Meditation,
hypnosis) Changing Thoughts and Feelings Therapies (psychotherapy, complementary
medicine [acupuncture]) Support Groups
You Are Not Your Illness
Tendency to become so identified with the disease and its treatment that we forget who we are.
We are not out illnesses – we are still ourselves.
Separate yourself from GD -- begin to have control over it instead of being totally controlled by it.
Self Nurturing
Rest -- Give yourself permission to rest Pleasant Activities – Engage in experiences and
relationships that you value.
“Sit down next to your joy. Find the people that bring out the best in you and listen to their talk and watch their walk. They live quietly among us, in our own families and circles of friends.” (Rumi)
Exercise within your limits
Activity, Rest, and Pacing Pain leads to reduced mobility which leads to
reduced fitness Find a personal balance Choose an activity you want to do and
construct a realistic schedule (walking, cycling, chores)
Stress-reducing Practices
Imagery, Meditation, Self-Hypnosis Change from passive treatment
approach to an active process of taking control and being in charge
Use as diversion, to lower stress, filter hurt out of pain
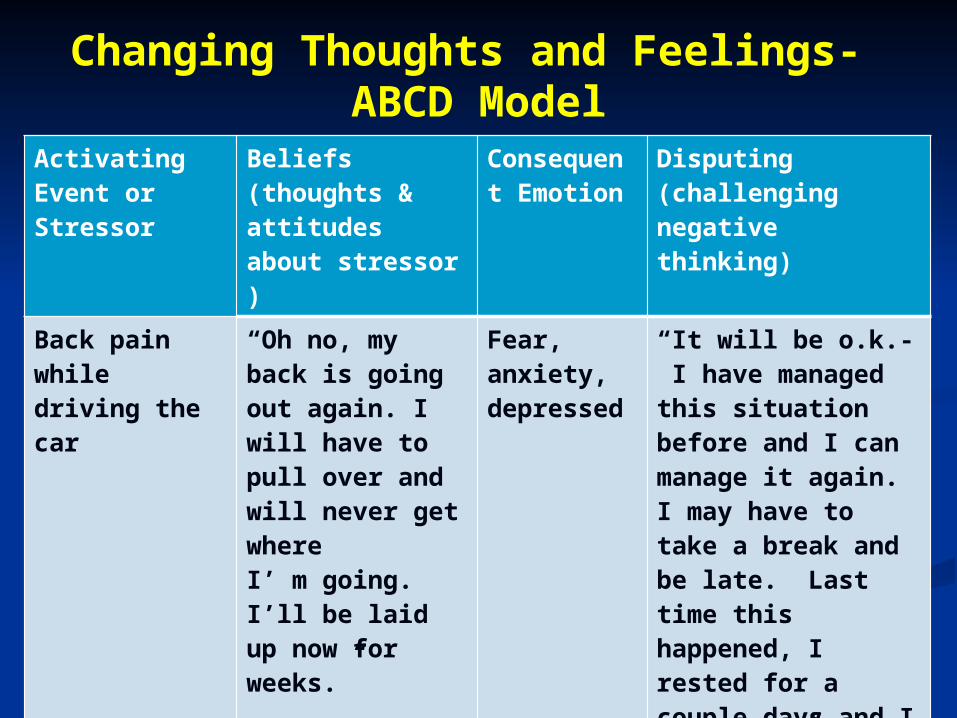
Changing Thoughts and Feelings- ABCD Model
Activating Event or Stressor
Beliefs (thoughts & attitudes about stressor )
Consequent Emotion
Disputing (challenging negative thinking)
Back pain while driving the car
“Oh no, my back is going out again. I will have to pull over and will never get where I’ m going. I’ll be laid up now for weeks.”
Fear, anxiety, depressed
“It will be o.k.- I have managed this situation before and I can manage it again. I may have to take a break and be late. Last time this happened, I rested for a couple days and I was fine.”
Boss yelled at me “How could I be so stupid. He probably wants to fire me. I can’t take much more of this. “
Shame, anger, crying, heart racing
“I feel bad that he yelled at me. He’s probably having a really bad day. I’ll talk to him when we are both less stressed. Tonight, I will go to a movie with a friend.”
Therapies and Support Groups
Psychotherapy Cognitive-Behavioral Therapy (CBT) –
emphasizes the role of thinking in how we feel and what we do
Psychodynamic or insight-oriented therapy: focuses on unconscious processes as they are manifested in a person’s present behavior
Complementary medicine Acupuncture
Support Groups
The Psychosocial and Neurocognitive Impact of Gaucher Disease, Type 1 on Pediatric
Patients and their Families
Andrea Alioto and
Wendy Packman, JD, PhD
Palo Alto University
Psychosocial and Neurocognitive Impact of Gaucher Disease, Type 1 on Pediatric Patients and their Families
Previous Research: Hayes et al. (1998)
Health Related Quality of Life in 16 GD, Type 1 patients (8-67 ys)
Symptoms of bone pain and chronic fatigue interfered with academic, occupational, and social activities.
Caregivers gave similar responses about impact of symptoms and ERT on functioning
No study has independently examined psychosocial or cognitive effects in children.
No study has examined psychological well-being of parents or implications on family unit.
Study Goals:
To examine: Health-Related quality of life Psychological and neurocognitive
functioning Effect of ERT on symptoms and functioning Psychological well-being of parent Impact on family unit
Develop recommendations to improve quality of care.
Participants
Children ages 5-18 diagnosed with GD, Type 1 and their parent(s).
Recruitment: 2015 National Gaucher Conference National Gaucher Care Foundation Gaucher’s Association (UK)
Assessment Measures
Pediatric Quality of Life Inventory PedsQL Pediatric Pain Questionnaire Behavior Assessment System for Children Behavior Rating Inventory of Executive Function PedsQL Cognitive Functioning Scale Profile of Mood States- 2nd Edition PedsQL Family Impact Module Pediatric Inventory for Parents
Self-report measures (in person, mail, via Skype)