Embed Size (px)
Citation preview
Psychopharmacology of Mood Disorders
Dr. Lisa McMurray6 Jan 2015
Based on a 2014 presentation by Dr. Kate Huntington
Pre-test (true/false)
• All patients with symptoms of major depression should be treated with an antidepressant
• Mirtazapine causes drowsiness through its effects on the benzodiazepine receptor
• SNRIs such as Venlafaxine can cause diastolic hypertension
Pre-test (true/false)
• Trazodone is rarely tolerated at full therapeutic dosages due to significant sedation side effects
• Lithium is rarely tolerated due to multiple side effects and should be reserved only for treatment resistant bipolar patients
• Atypical antipsychotics are indicated as first line monotherapies for bipolar depression, mania and maintenance treatments
Objectives• Describe the neurotransmitter systems and neuroanatomical pathways
that are implicated in mood disorders• List the common classes of antidepressant medications and give one
example of each• Describe first line pharmacologic treatment of major depressive disorder
and bipolar disorder, across the lifespan• Explain the mechanism of action and side effect profile of SSRI’s, SNRI’s
TCA’s , Lithium and Valproic Acid• List the common drug interactions with Lithium• Describe monitoring of SSRI’s and mood stabilizers• Describe the role of antipsychotic medication in the treatment of mood
disorders
A few words on Memory and Mnemonics
Memory
Declarative
Working memory:Rate limiting step
Can only hold 7+/-2 pieces of information
If you cannot hold it in working memory, it
cannot eventually be encoded and stored
Long term memory:Hippocampus
triages and stores in hippocampus,
prefrontal cortex and association
areas
Procedural
A few words on Memory and Mnemonics (2)
• Mnemonics assist learning by reducing/simplifying information
• This reduces the load on working memory, allowing larger pieces of information to be encoded and stored for later retrieval
A few words on Memory and Mnemonics (3)
• Why in psychiatry?– Less anatomical therefore less framework to add
information to– Often looking at systems such as
neurotransmitters with diffuse effects– Use of diagnostic criteria– High prevalence of mental illness and use of
psychiatric meds in the general population necessitates easy access to this knowledge for any type of physician
Criteria for Depressive Disorders
Criteria for MDD (Major Depressive Disorder)
• Five of the following for at least 2 weeks, represents change from baseline , includes at least one of either mood or interest criteria
• Mood depressed (can be subjective or objective)• Sleep changes• Interests decreased with loss of pleasure (subjective or objective)• feelings of Guilt or worthlessness• Energy decreased• Concentration decreased or problems thinking or making
decisions (subjective or objective)• Appetite changes which may be associated with weight loss or
gain• Psychomotor changes (must be objective)• Suicidal thoughts, plans, or recurrent thoughts of death
Criteria for MDD (2)
• Causes distress or impairment in functioning• Is in excess of what would be expected as a response
to a significant loss (differentiate from the loss/emptiness of grief)
• Not due to a substance or another medical condition• Symptoms are not better explained with a diagnosis
of a psychotic disorder• There has NEVER been a manic or hypomanic
episode
What is wrong in Depression?
Part I: Normal Monoamine Neurotransmission
Monoamine neurotransmitters: normal pathways, function and inactivation
• The main monoamine neurotransmitters are serotonin (5HT), norepinephrine (NE) and dopamine (DA)
• All three can be removed from the synapse by specific reuptake pumps and inactivated by monoamine oxidase (MAO).
• Feedback is provided to the neuron via autoreceptors, mostly at the somatodendritic end of the neuron
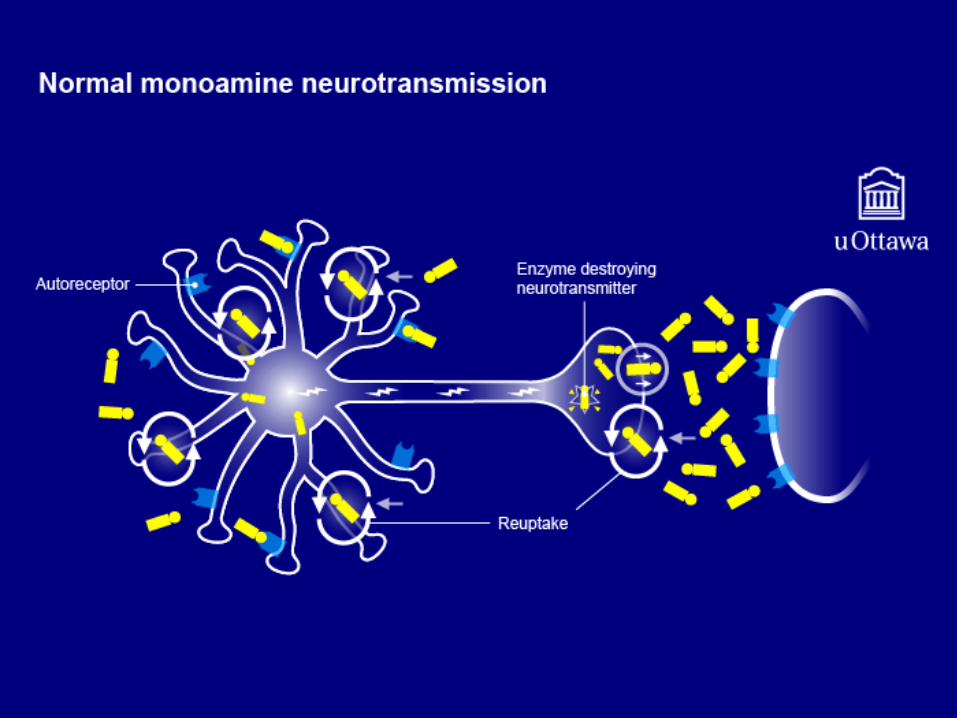
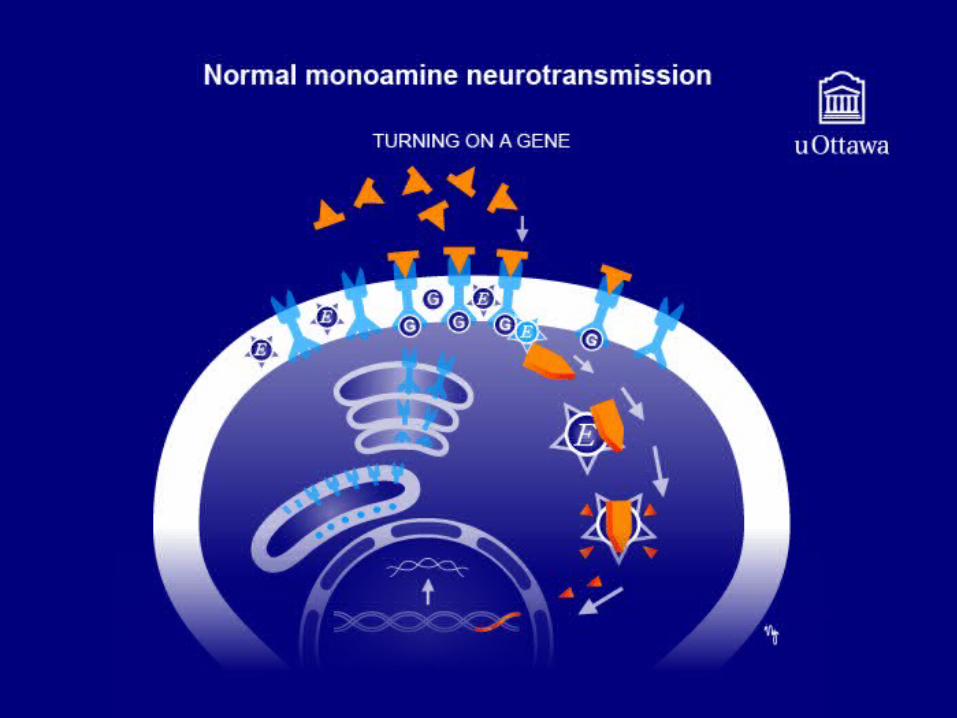
Normal monoamine neurotransmission• Signal • Electrical impulse• Release of neurotransmitter to synapse• 1. Couple with presynaptic receptor, providing feedback• 2. Couple with post synaptic receptor
• Bind with G protein• Activates “2nd messenger system”
• Ultimately activates genes (leading to creation of enzymes, receptors, transcription factors and neurotrophic factors)
• 3. Reuptake and repackaging via reuptake pumps and inactivation via MAO
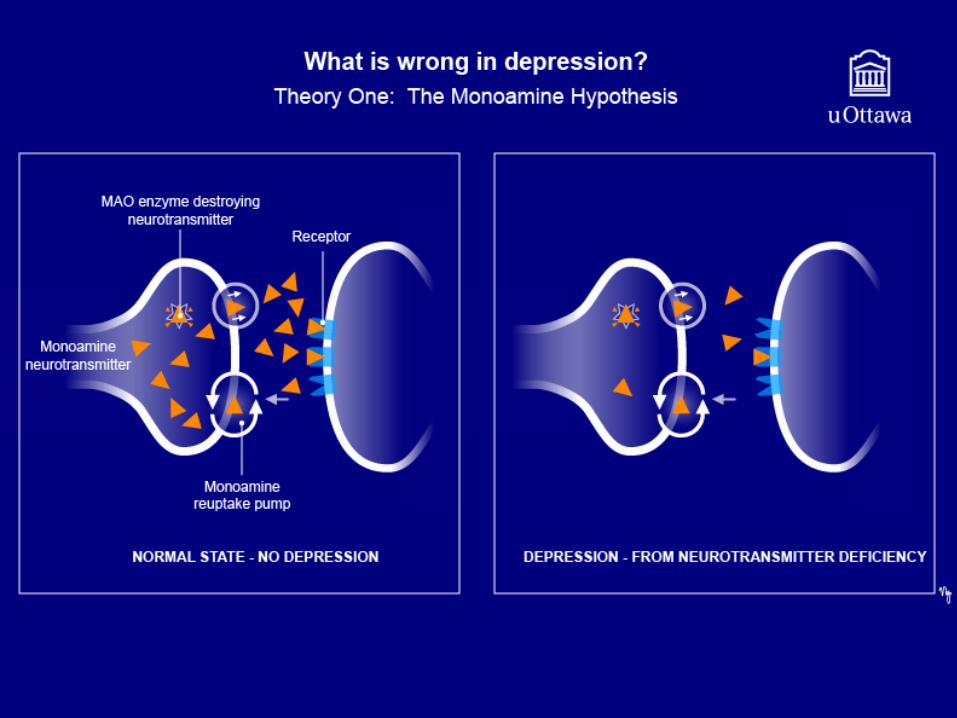
What is wrong in depression?Theory one: The monoamine hypothesis
• There is insufficient amount of the monoamine neurotransmitters; increasing neurotransmitters causes a return to the normal state
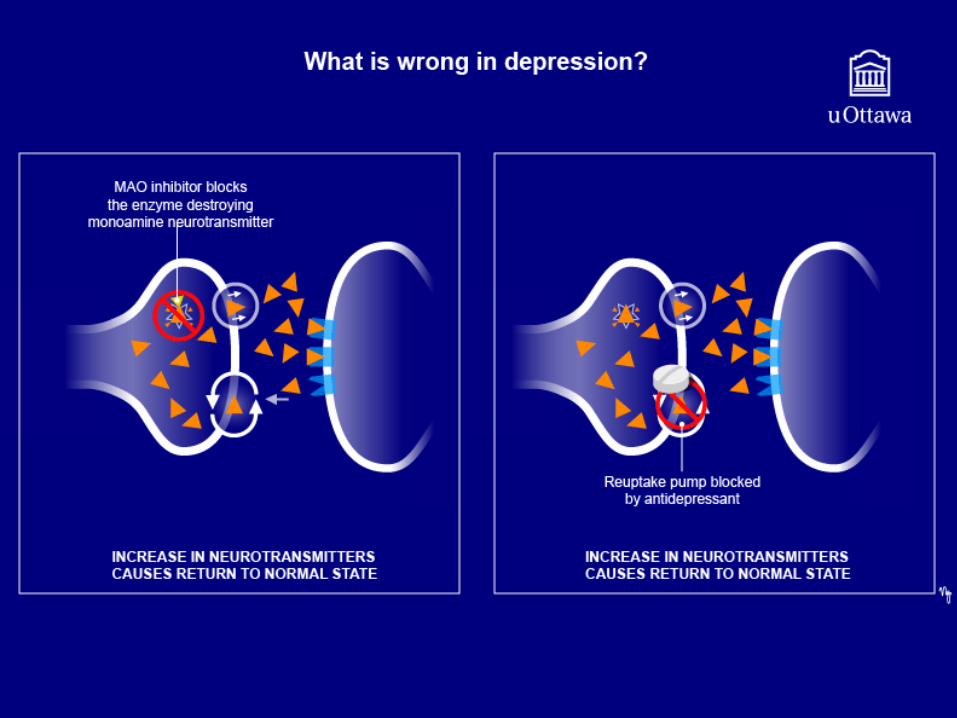
• Evidence:• Drugs that deplete monoamines can cause depression• TCA’s and MAOI’s increase monoamines and are known to treat
depression• Norepinephrine and serotonin metabolites deficient in some
depressed patients• Problems:
• Monoamine levels are boosted immediately with antidepressant medications but the onset of therapeutic effect is delayed by weeks
What is wrong in depression? Theory two: neurotransmitter receptor
hypothesis• Depletion of monoamines causes compensatory up regulation
(increased number and sensitivity) of postsynaptic neurotransmitter receptors; treatment response correlates with down regulation (decreased number and sensitivity) of receptors
• Evidence:• Post mortem studies show increased number of 5HT2 receptors in
the frontal cortex of some patients who commit suicide• Depressed patients have been shown to have abnormal
neurotransmitter receptors in platelets and lymphocytes
What is wrong in depression?Monoamine hypothesis of gene expression
• There are stress induced changes in the Monoamine signal transduction cascade, leading to inappropriate gene expression (eg. Reduced production of brain derived neurotrophic growth factor, and upregulated pre -and post-synaptic receptors)
• antidepressants may be able to reverse this though a cascade which ultimately results in upregulation of genes such as those for BDNF and down regulation of genes such as those for upregulated receptors
• Evidence for abnormally functioning neuronal system/gene expression:• Probing monoamine receptors with agonists leads to deficient
hormone output and neuronal firing rates• Imaging studies show decreased hippocampal volume in
depression
Summary:How do antidepressants work?
• There are three main monoamine neurotransmitters: serotonin, norepinephrine and dopamine
• In depression, the levels of these neurotransmitters is believed to be decreased, and the neurons in the circuits are functioning poorly, upregulating receptors and not producing enough of other proteins, such as BDNF
• Antidepressants work by increasing the amount of monoamines by blocking their reuptake or preventing their breakdown; this leads to a cascade of events which ultimately results in changes in gene products such as receptor proteins and BDNF.
MCQ
• Which of the following is not a monoamine neurotransmitter?A. SerotoninB. GlutamateC. DopamineD. Norepinephrine
Monoamine-regulated CNS circuits

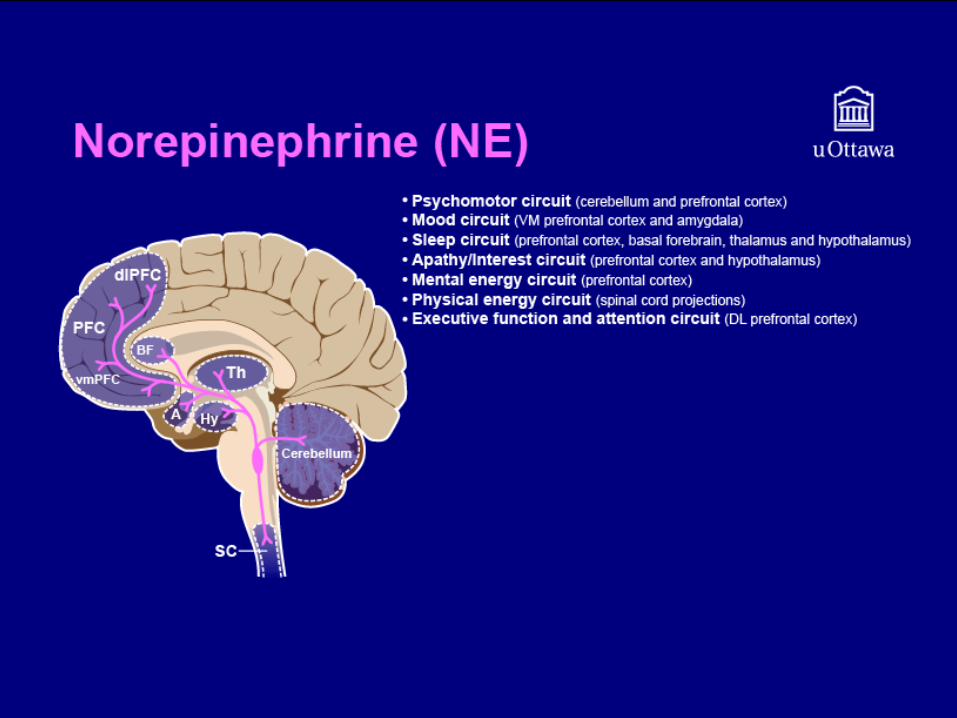
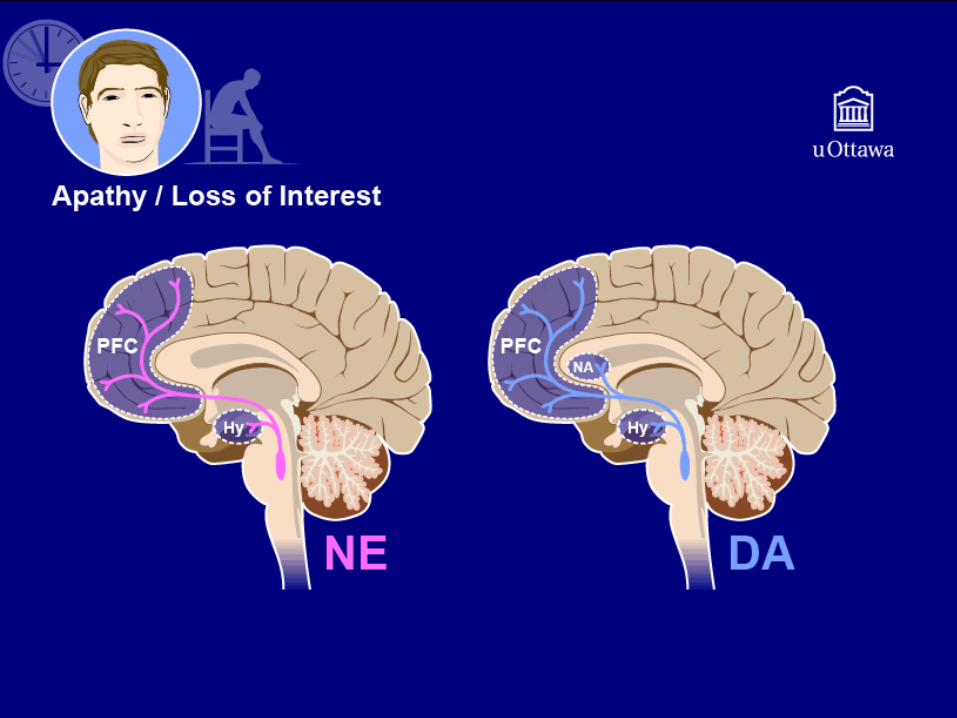
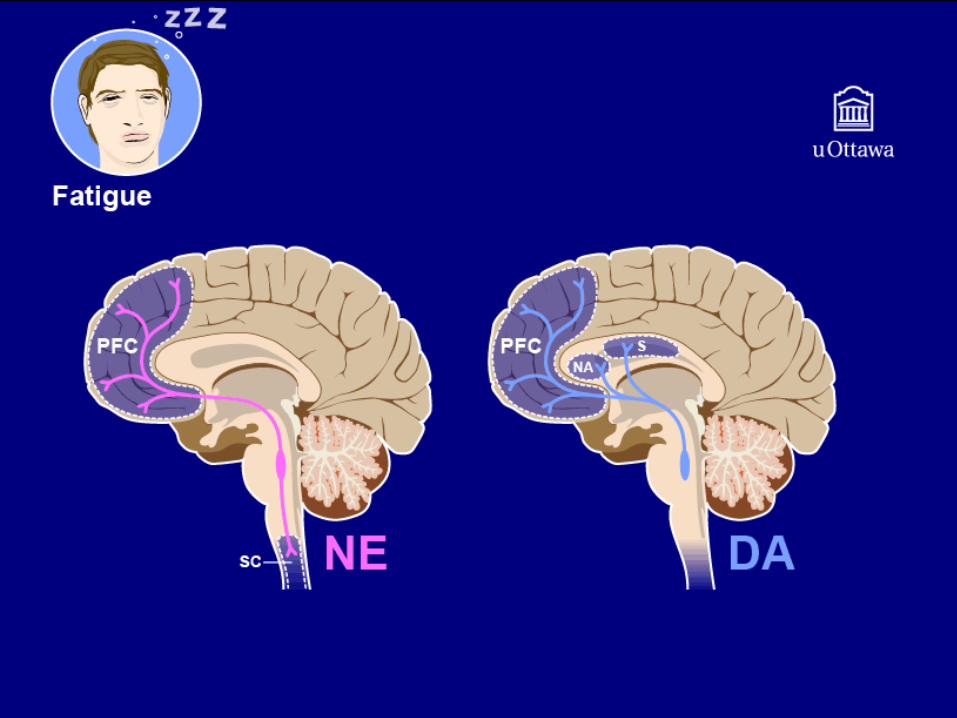
Norepinephrine (NE)• Most of the cell bodies for the noradrenergic neurons are in the locus
coeruleus. This is an important center for priorizing incoming stimuli and focusing attention.
• Noradrenergic projections regulate the following circuits:• Psychomotor circuit (cerebellum and prefrontal cortex) • Mood circuit (VM prefrontal cortex and amygdala)• Sleep circuit (prefrontal cortex, basal forebrain, thalamus and
hypothalamus)• Apathy/Interest circuit (prefrontal cortex and hypothalamus)• Mental energy circuit (prefrontal cortex)• Physical energy circuit (spinal cord projections)• Executive function and attention circuit (DL prefrontal cortex)
• There is also prominent noradrenergic involvement in the SNS and brainstem cardiovascular center
Copyright: <a href='http://www.123rf.com/profile_serezniy'> / 123RF Stock Photo</a>
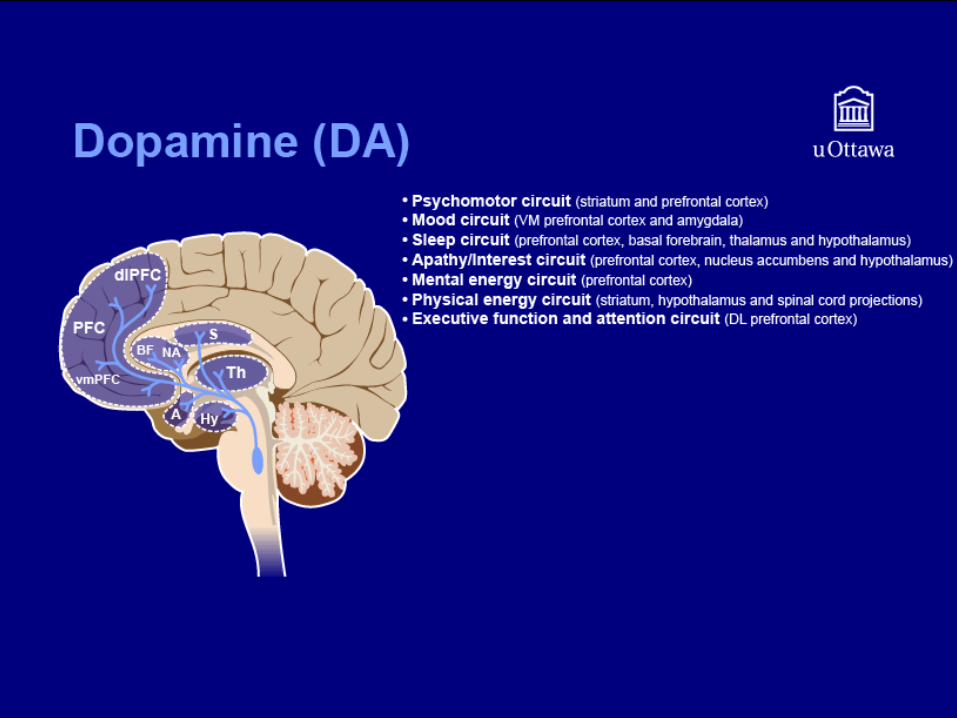
Dopamine (DA)• Dopaminergic cell bodies are located in the substantia nigra and the
ventral tegmental area of the brainstem. • Dopaminergic projections regulate the following circuits:
• Psychomotor circuit (striatum and prefrontal cortex)• Mood circuit (VM prefrontal cortex and amygdala)• Sleep circuit (prefrontal cortex, basal forebrain, thalamus and
hypothalamus)• Apathy/Interest circuit (prefrontal cortex, nucleus accumbens and
hypothalamus)• Mental energy circuit (prefrontal cortex)• Physical energy circuit (striatum, hypothalamus and spinal cord
projections)• Executive function and attention circuit (DL prefrontal cortex)
• Dopamine is the “Goldilocks” monoamine when it comes to treating mood. Too much dopamine leads to abuse; not enough dopamine and the drug is no use.
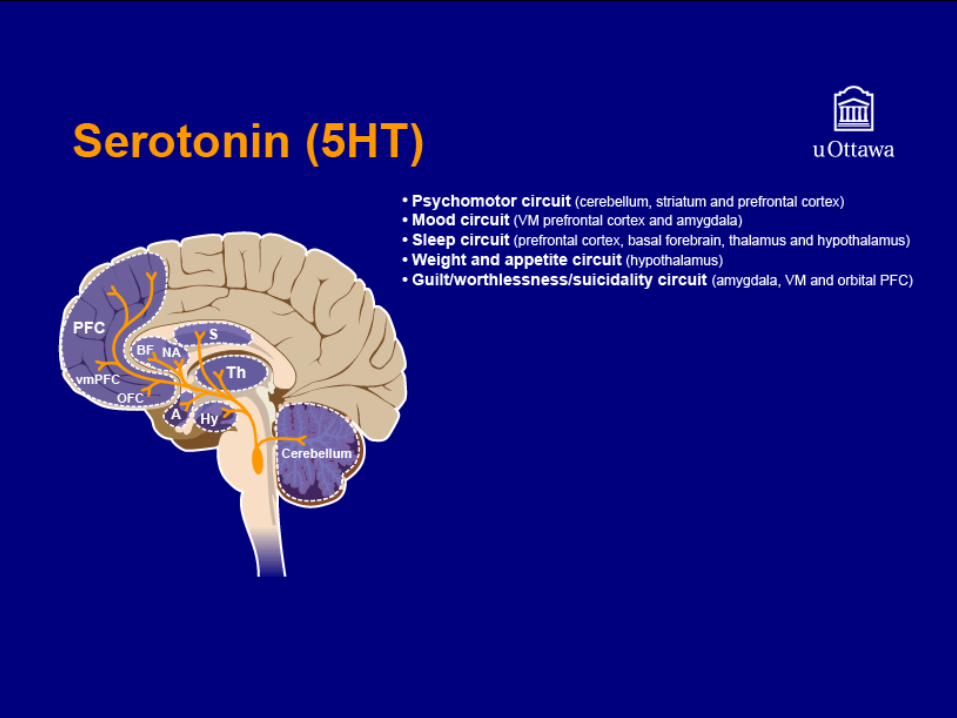
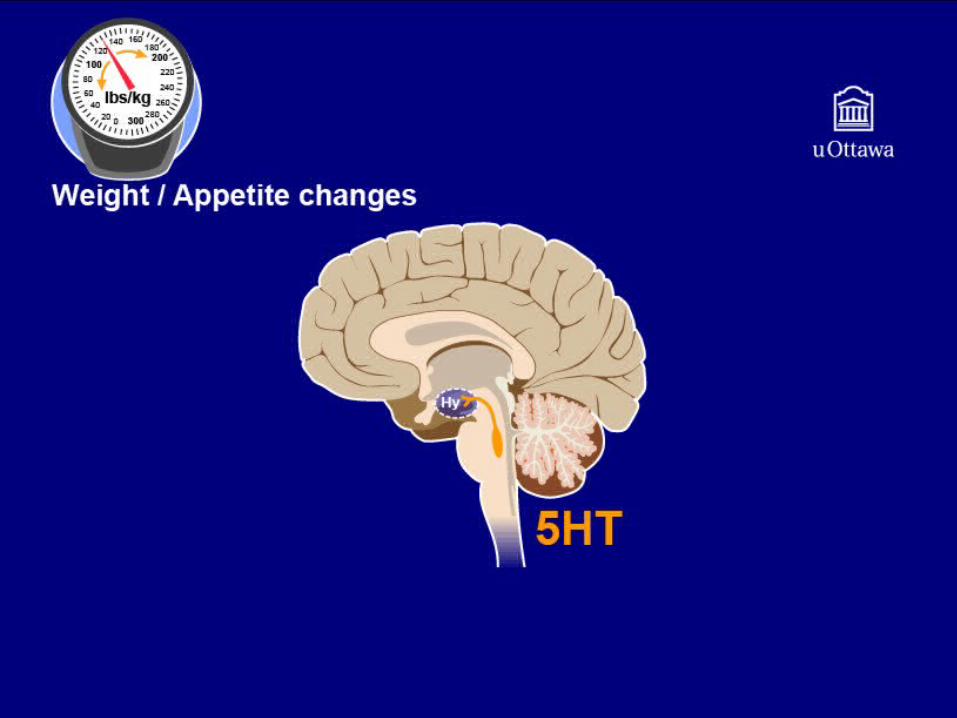
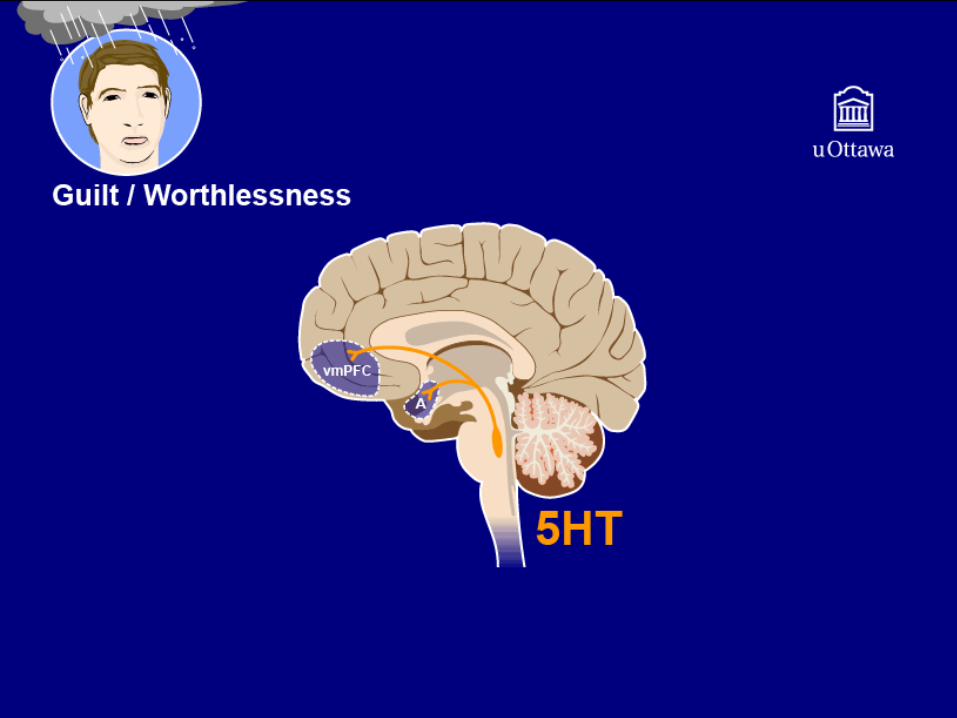
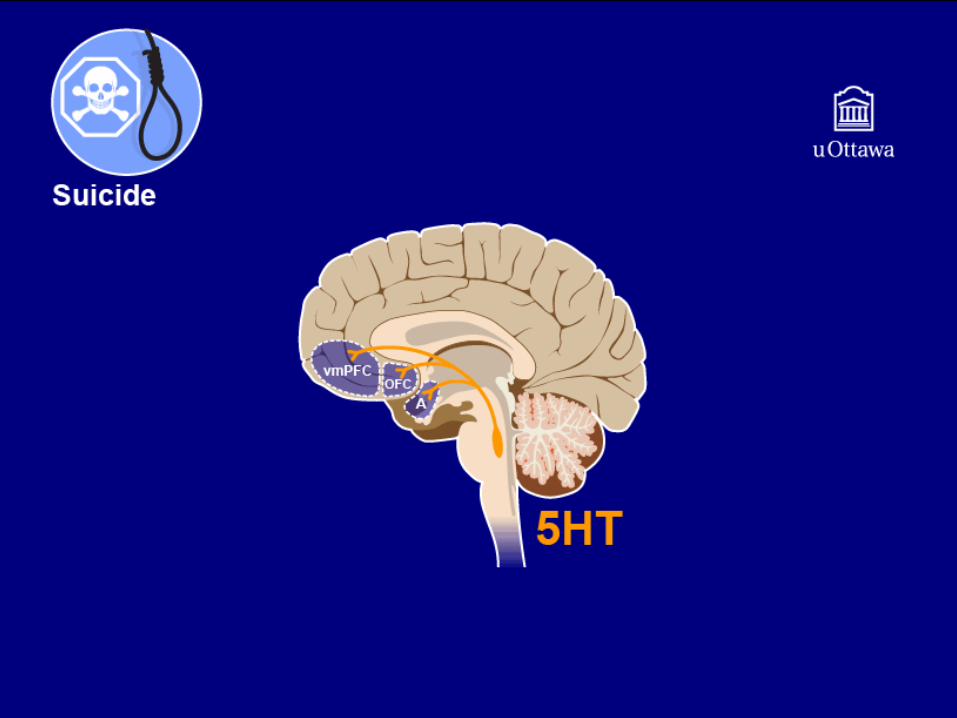
Serotonin (5HT)
• Most of the serotonergic cell bodies are located in the raphe nucleus
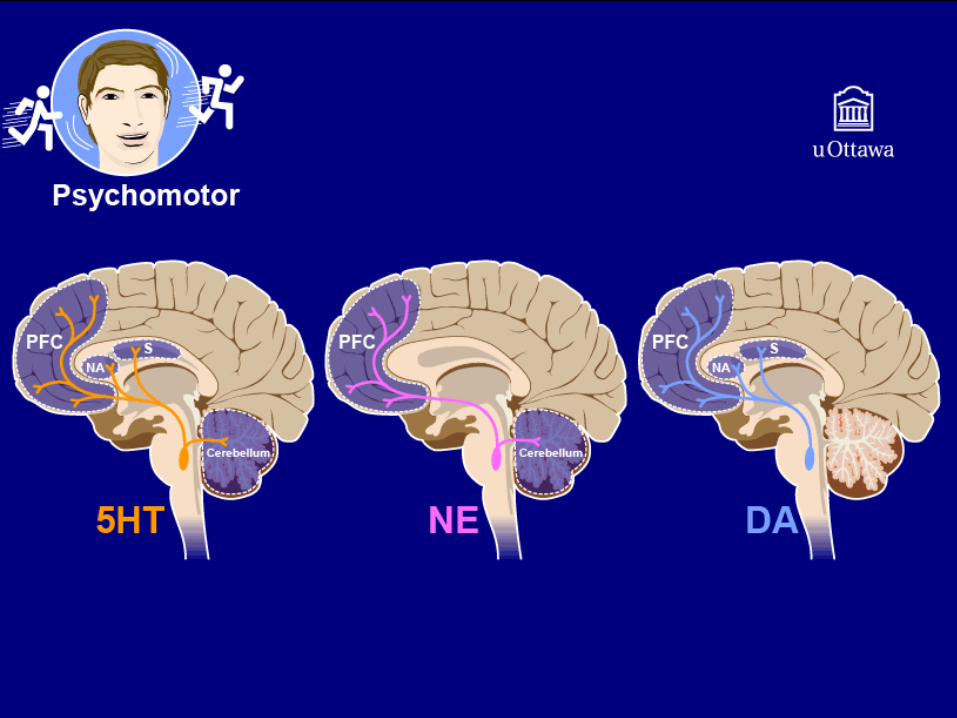
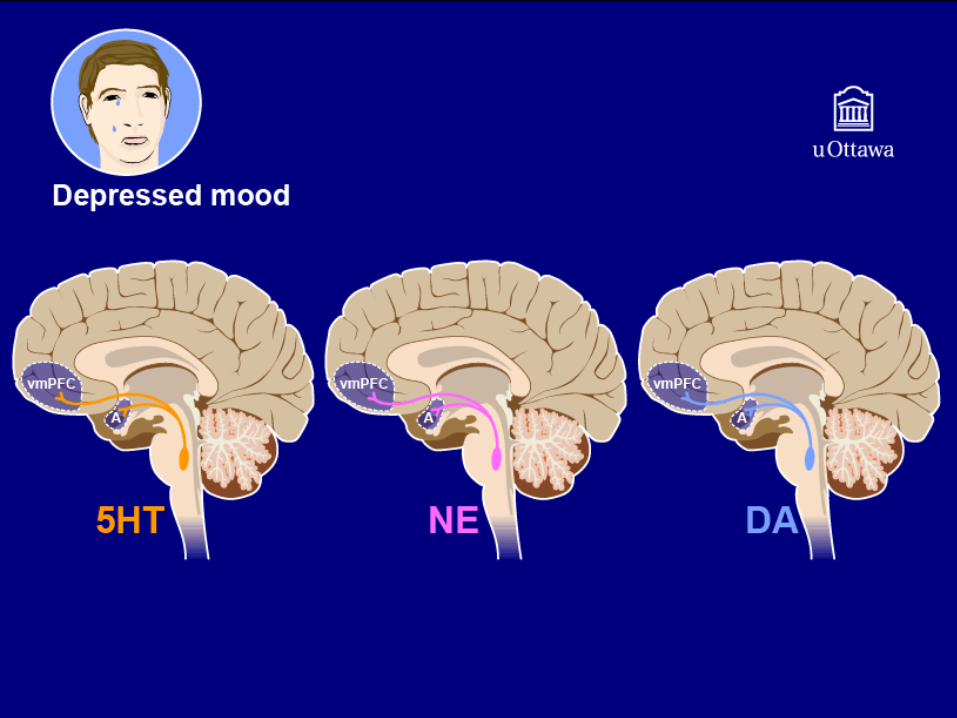
• Serotonergic projections regulate the following circuits:• Psychomotor circuit (cerebellum, striatum and prefrontal cortex)• Mood circuit (VM prefrontal cortex and amygdala, 5HT1A
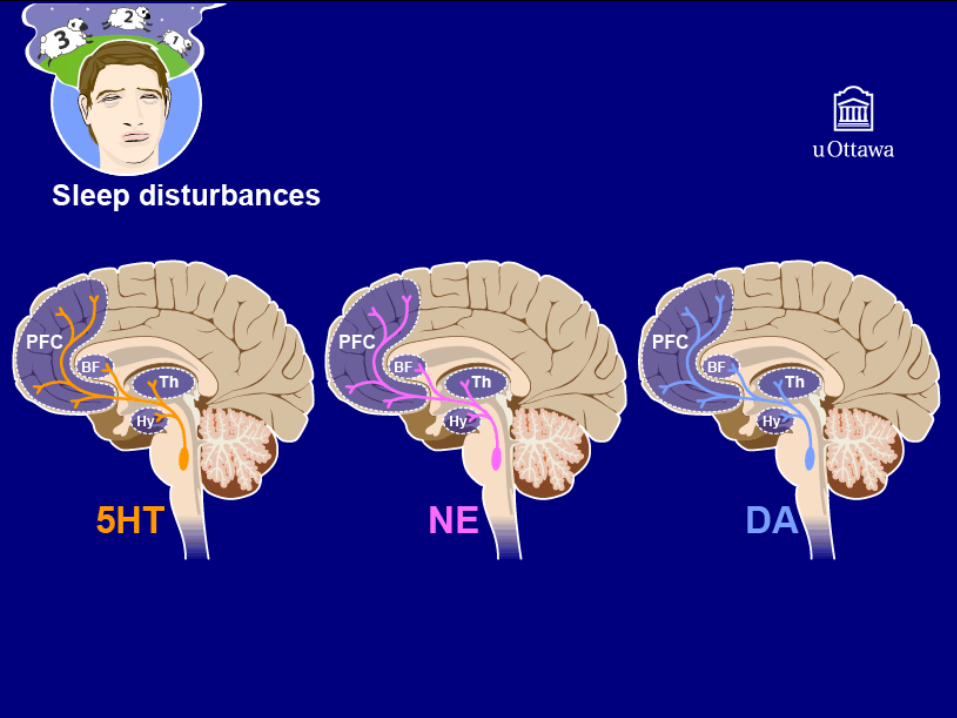
receptors)• Sleep circuit (prefrontal cortex, basal forebrain, thalamus and
hypothalamus, 5HT2 receptors)• Weight and appetite circuit (hypothalamus, 5HT3 receptors)• Guilt/worthlessness/suicidality circuit (amygdala, VM and orbital
PFC)• There are also prominent descending serotonergic spinal cord
projections and 5HT3 receptors in the GI system
MCQ
• Mr. Flynt presents with symptoms of loss of appetite and weight loss, feelings of worthlessness and thoughts of death, psychomotor changes, sleep disturbance, decreased attention, decreased interests and low physical and mental energy. Which neurotransmitters should be targeted in order to treat all of his symptoms?– A: serotonin– B: norepinephrine– C: dopamine– D: A and B– E: A, B and C

Treatment

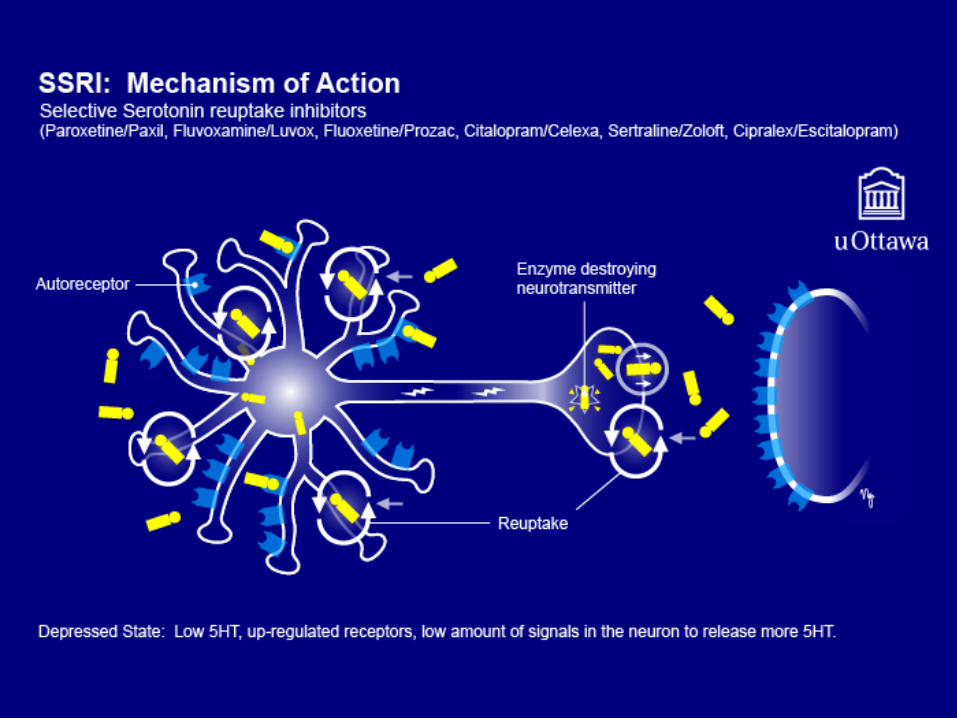
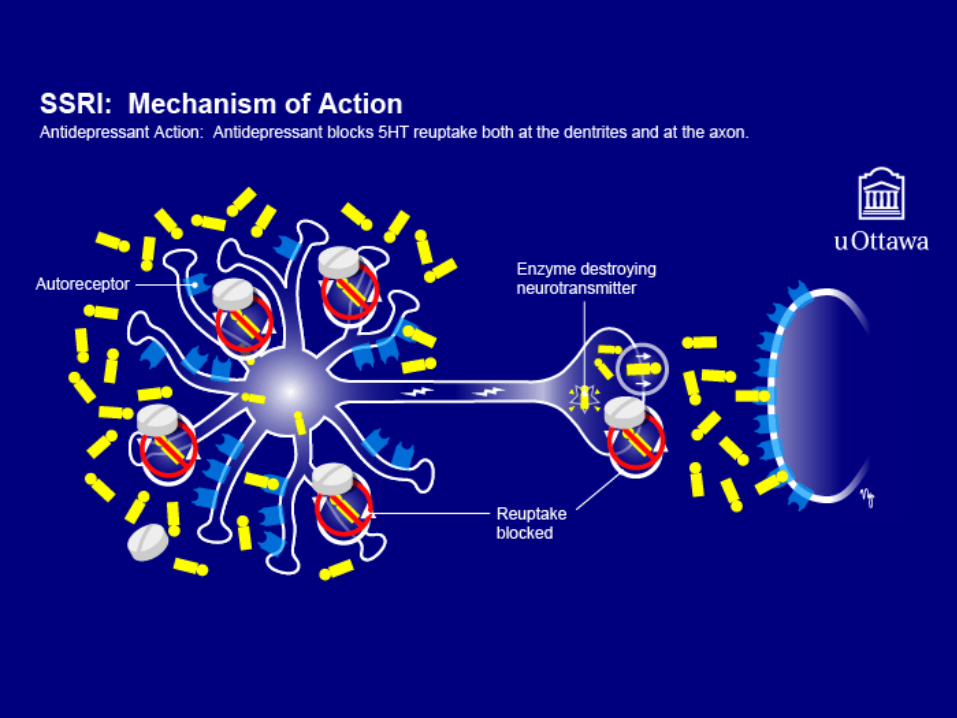
SSRI: Mechanism of Action
• In depression, the serotonin neuron has a relative deficiency of serotonin and the autoreceptors and postsynaptic receptors are malfunctioning and sending faulty signals
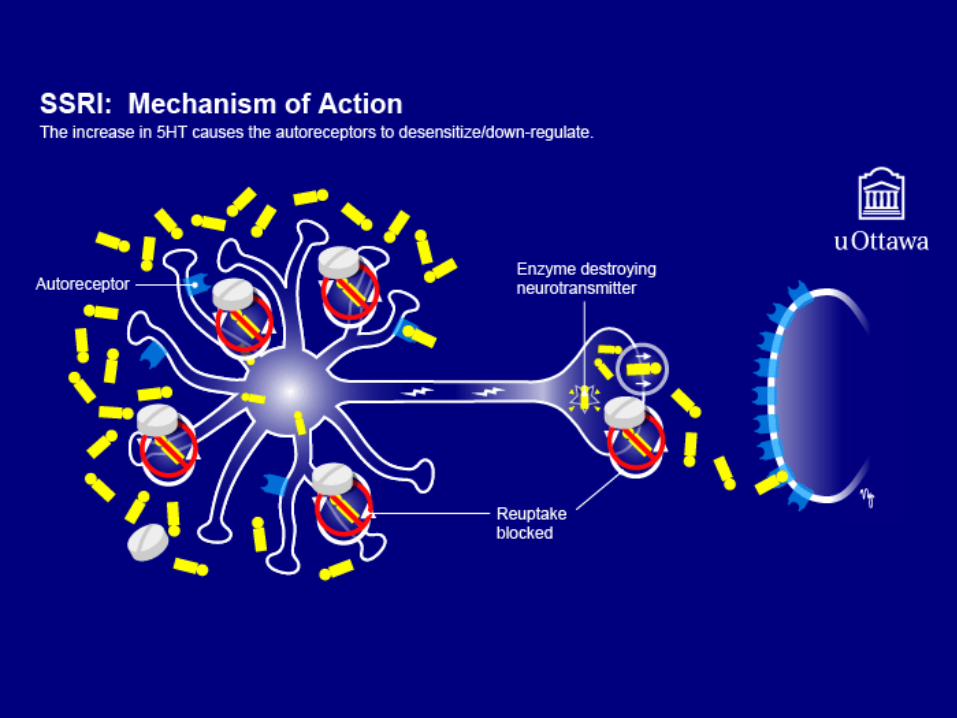
• When the reuptake pump is blocked and the level of serotonin increases in the somatodendritic area, this sends a message to the nucleus to pump up quality control on the production of autoreceptors
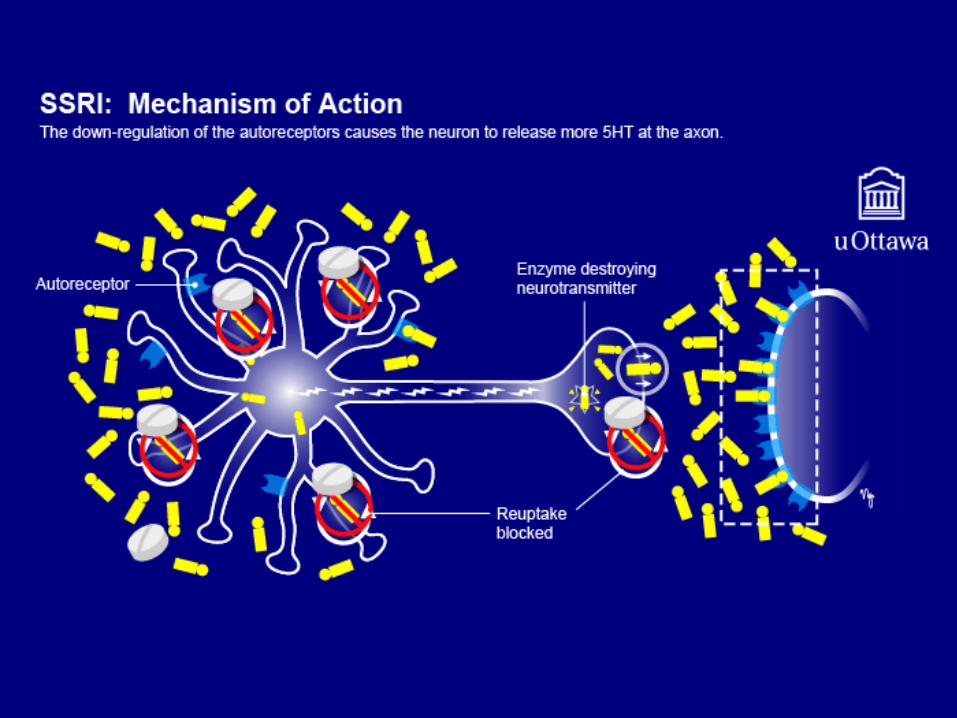
• The new and improved autoreceptors detect a deficiency of serotonin and increase production and release of neurotransmitter to the synapse
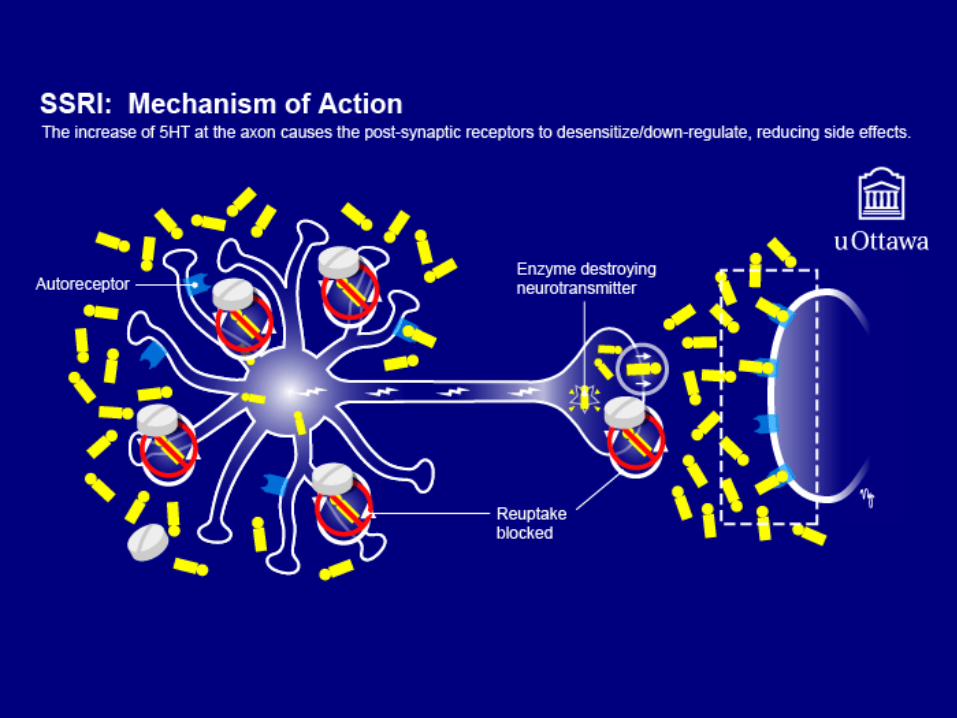
• Increased levels of serotonin in the synapse send a message to the post synaptic neuron to correct the production of its gene products including receptors and neurotrophic growth factors
SSRI: Side Effect Profile
• Headache• Anxiety and Agitation (mood and psychomotor circuits)• Nausea (weight/appetite circuit and GI receptors)• Diarrhea (peripheral GI 5HT3 & 5HT4 receptors)• Sexual dysfunction (spinal projections) and Sleep disruption or
Somnolence (sleep circuit)
SSRIs: Less common but more serious side effects• UGI bleeding (platelet dysfunction), esp. in combo with
NSAID’s or other blood-thinning agents• SIADH• Osteoporosis and fractures in the elderly• Serotonin syndrome• QT prolongation/sudden death• SSRI discontinuation syndrome (slow taper)
• Flu-like symptoms• Insomnia• Nausea• Imbalance• Sensory disturbances• Hyperarousal (agitation/anxiety)
Norepinephrine & Dopamine Reuptake Inhibitor:Mechanism of Action
(Bupropion/Wellbutrin)
• Blockade of norepinephrine and dopamine reuptake pumps, leads to similar cascade as with SSRI’s
NDRI: Side Effect Profile
• Seizures (not with extended release formulations & following correct dosing; contraindicated with Bulimia or electrolyte disturbances)
• Headache, Hypertension (SNS activation)• Agitation (mood and psychomototr circuits) and Anticholinergic (relative
decrease in parasympathetic tone)• Rash• Emesis, decreased appetite and weight loss (SNS activation)• Sleep disruption, Shaking and Sweating (sleep and psychomotor circuits
and SNS activation)
Serotonin & Noradrenergic reuptake Inhibitors: Mechanism of Action
(Venlafaxine/Effexor, Desvenlafaxine/Pristiq, Duloxetine/Cymbalta)
• Blockade of serotonin reuptake at lower dose range
• Blockade of serotonin and norepinephrine reuptake in mid dose range
• Blockade of serotonin, norepinephrine and dopamine reuptake at very high dosages
SNRI: Side Effect Profile
• As with SSRI’s in lower to mid dose range• As with NDRI in mid to high dose range
SNRI: more serious side effects
• Diastolic Hypertension• As with SSRI’s
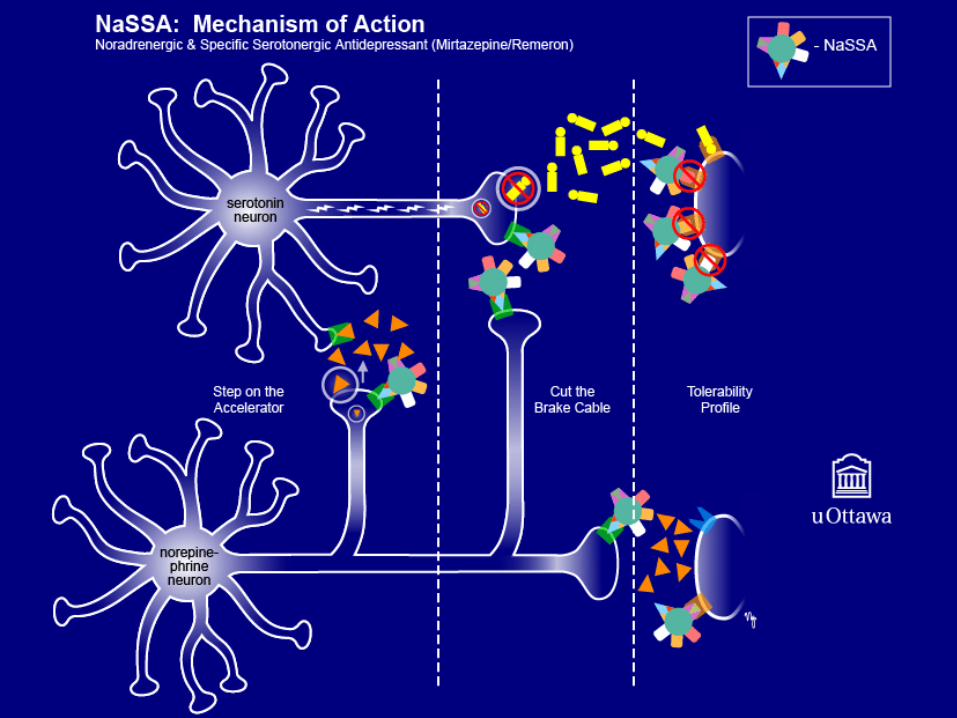
NaSSA: Mechanism of Action
• NaSSA: Noradrenergic and specific serotonergic antidepressant• Blocks Alpha 2 autoreceptors on norepinephrine neurons &
heteroreceptors on Serotonin neurons, causing more NE & 5HT to be released (puts the brakes on the brakes)
• NE neurons from the locus coeruleus innervate midbrain raphe 5HT neurons. Therefore, increased NE causes a further increase in 5HT release
• Blocks 5HT2 receptors, having an anxiolytic effect & blocking sleep & sexual side effects
• Blocks 5HT3, blocking GI side effects from peripheral receptors & from brainstem chemoreceptor trigger zone
• Blocks H1 histamine receptors, causing sedation & weight gain
NaSSA: Side Effect Profile
• Weight gain (H1 blockade)• (Anticholinergic: constipation, urinary retention, dry mouth, blurred vision, drowsiness, sinus tachycardia,
confusion/delirium, fever (red as a beet, dry as a bone, blind as a bat, mad as a hatter, hot as a hare; bowel & bladder lose their tone & the heart goes off alone) – in reality Mirtazapine has very weak and usually clinically insignificant anticholinergic activity
• Drowsiness (H1 blockade)• Equilibrium
NaSSA: Rare but Dangerous Side Effects
• Neutropenia
• Serotonin syndrome
• Hepatotoxicity
• SIADH
• QT prolongation/sudden death
SARI: Mechanism of ActionSerotonin 2A antagonists/reuptake inhibitors (Trazodone/Desyrel)
• Primarily blocks 5HT2A, reducing sexual dysfunction & sleep disruption & increasing effect of 5HT1A stimulation (5HT2A & 5HT1A oppose one another’s actions in several ways)
• Weak 5HT reuptake inhibitor, increasing 5HT stimulation of 5HT1A (therapeutic effects)
• H1 blockade causes sedation
• Alpha One blockade leads to orthostatic hypotension
SARI: Side Effect Profile
• Orthostatic hypotension
• Sedation
SARI: Rare but Dangerous Side Effects
• Serotonin syndrome
MCQ
• The following medication targets primarily the neurotransmitter serotonin:– A: escitalopram– B: mirtazepine– C: venlafaxine– D: Bupropion– E: Duloxetine
TCA: Mechanism of ActionTricyclic antidepressants:
3° amines (eg amitriptyline, imipramine, doxepine) 2° amines (eg nortriptyline, desipramine)
HISTORY Originally developed as treatment for schizophrenia (similar 3-ringed chemical structure); found ineffective for psychosis but helpful for depression.
• Therapeutic effects and side effects from blocking Serotonin, Norepinephrine & Dopamine Reuptake
• Some also have 5HT2 blocking ability (blocks sex & sleep side effects)• Side effects from blocking H1 histamine receptors, muscarinic receptors,
alpha one adrenergic receptors & sodium channels in the heart & brain
TCA: Side Effect Profile
• Antihistamine – weight gain & sedation
• Anticholinergic – (remember toxidrome from NaSSA and NDRI)
• Anti-alpha adrenergic – dizziness, orthostatic hypotension
• Blockade of fast sodium channels – prolongation of QTc (risk of Torsades)
TCA: Rare but Dangerous Side Effects• Torsades de Pointes
• EKG – rule out bradycardia and prolonged QTc• Lytes – rule out electrolyte imbalance• Make sure not on type 1 or 3 antiarrythmic drugs
• SIADH• Serotonin Syndrome
MAOI: Mechanism of ActionMonoamine oxidase inhibitors:
“the classics” (phenylzine/nardil, tranylcypromine/parnate)Reversible inhibitor: (moclobemide/mannerix)
HISTORY: • The first clinically effective antidepressants• Originally, an anti-tuberculosis drug, found to decrease
comorbid depression
• Irreversibly bind MAO (2 wks) & destroy its function, therefore decrease monoamine breakdown, increasing 5HT, NE & DA
MAOI: Side Effect Profile
• Side effects related to increase in serotonin norepinephrine & dopamine (see SSRI’s & NDRI’s)
• Orthostatic hypotension
MAOI: Rare but Dangerous Side Effects• Hyperthermia i.e.Serotonin Syndrome
• even more susceptible than with other serotonergic antidepressants; need to avoid anything that has serotonergic effects such as antidepressants and opioids)
• When you see an MAOI, get a pharmacy consult, the patient should consult their pharmacist about any over - the – counter medications
• Hypertensive crisis• Consult the dietician Re: MAOI diet• Patients need to avoid all foods with tyramine (aged foods such as
aged cheeses and wines or tap beer) and any medications with noradrenergic effects (cold remedies, stimulants etc)
• Hepatotoxicity• Teratogenicity• Blood dyscrasias
Serotonin Syndrome: HARMED
• Hyperthermia• Agitation/Autonomic instability• Rigidity/Reflexes increased• MyoClonus/tremors• Encephalopathy• Diaphoresis
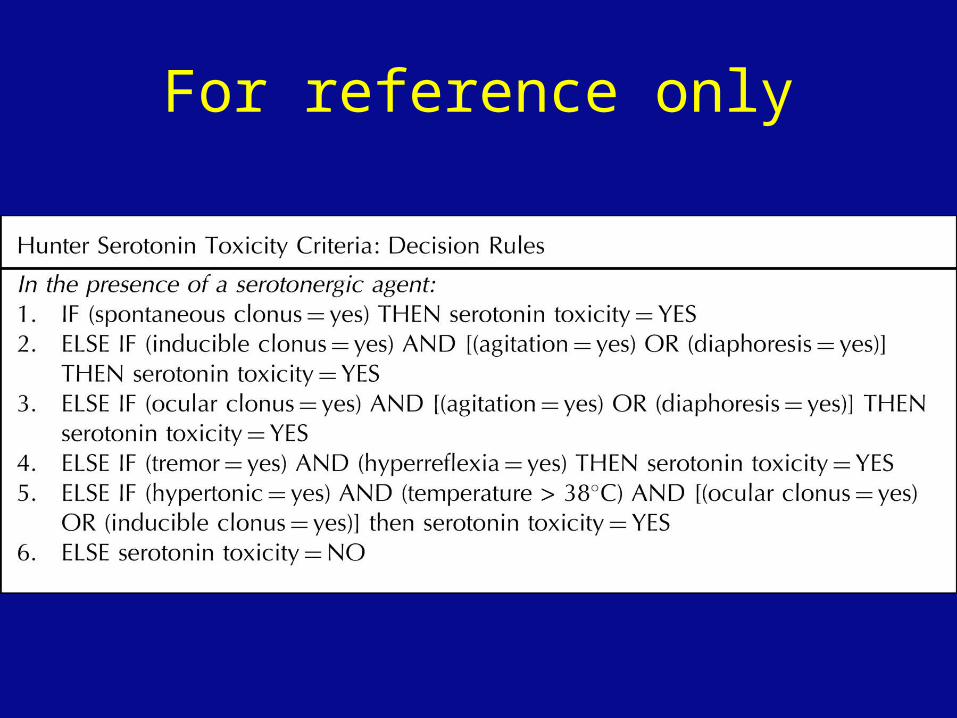
For reference only
MCQ
• Serotonin syndrome is most likely to be caused by the combination of which two medications?
• A: Duloxetine(SNRI) and Mirtazepine (NaSSA)• B: Citalopram (SSRI) and Trazodone (SARI)• C: Bupropion(NDRI) and Fluvoxamine (SSRI)• D: Phenylzine (MAOI)and Fluoxetine(SSRI)• E: Venlafaxine (SNRI) and Lithium
Hypertensive Crisis• Norepinephrine is the amine most closely linked with control of blood
pressure
• MAO normally inactivates norepinepherine
• Tyramine, an amine present in aged foods, causes release of norepinepherine
• In the presence of MAOI, this increased NE cannot be broken down, resulting in a hypertensive crisis
Choice of initial treatment in MDD
• Medication indicated in mild to moderate depression if preferred by patient over psychotherapy
• Medication indicated in moderate to severe depression with or without psychotherapy or ECT (BA has also been shown to be effective even in severe depression)
• Psychotic depression requires either combination antipsychotic and antidepressant or ECT (ECT is gold standard)
Treatment choices in children
• Concerns were raised about the safety of antidepressants (Paroxetine and Venlafaxine) in children and youth in 2004
• Further metaanalyses and epidemiologic studies now confirm that antidepressants in children and youth are safe with close (weekly) monitoring.
• Problems with Venlafaxine and Paroxetine may have been related to poor adherence and discontinuation symptoms
Starting Antidepressants: General Guidelines
• Start with a reuptake inhibitor (SSRI, SNRI, NDRI) or mirtazapine (i.e. not a TCA or MAOI)
• Start at lowest possible dose (half of this with anxiety and in the elderly and medically frail)
• Increase by this increment about every five half lives (or about once a week) until one of the following endpoints:• Intolerable side effects• Full response• Maximum dose
• Continue to monitor regularly (once a week initially) for therapeutic effects, side effects and safety (suicidality)
Choice of Initial Treatment in children/youth
• Mild to moderate depression: – Start with psychotherapy or non-medication interventions
as first line– Second line is to add medication; best evidence is for
Fluoxetine; other SSRI’s could be considered next• Moderate to severe depression:
– First line is to consider medication but depending on patient/family preference, may also start with psychotherapy or monitoring
• Note that the clinical presentation in children and youth can change quickly; they may appear severely depressed one week then by the next week be in a new relationship and everything is better…
Choice of Initial Antidepressant in Adults
• There is comparable efficacy between and within classes of medication, therefore, initial selection is based on:• Symptom profile (i.e. target circuits; see next slide)• Side effect profile in relation to the individual patient• Patient preference• Cost• History of previous response of the patient or family members• Comorbid psychiatric or medical illnesses• Potential drug-drug interaction
• The BEST antidepressant is the one that a patient will actually take acutely and for the long haul
Goals of antidepressant therapy
• REMISSION of symptoms and maintaining that level of improvement in order to prevent relapse and recurrence
• Rate of relapse is significantly less for patients who achieve full remission of symptoms
• Patients who have been ill longer tend to be more treatment resistant; there is also evidence of hippocampal atrophy with prolonged illness, leading to the concept of disease progression and the hope that this can be modified by treating all mood episodes to the point of remission
Bipolar Disorder
DSM5 Criteria
Criteria BPD I (Bipolar Disorder Type I)
• At least one manic episode
Criteria BPAD II(Bipolar Disorder Type II)
• Presence or history of one or more Major Depressive Episode
• Presence or history of at least one hypomanic episode
• There has never been a manic episode
Criteria Manic Episode
• A period of • persistently elevated, expansive, or irritable mood • persistently increased goal directed activity or energy
• Causes impairment in functioning, hospitalization or psychosis
• Present most of the day every day for one week or less if hospitalized
• Not due to substance use of GMC
Criteria Manic Episode (2)• Associated with
• 3 other criteria if mood is elevated or expansive • 4 other criteria if mood is irritable
Grandiosity or inflated self esteem• Sleep (decreased need)• Talkative (speech is increased in rate or pressure)• Pleasurable activities with Painful consequences• Activity increased/Agitation• Ideas (flight of) or experience of “racing thoughts”• Distractible (i.e. attention easily drawn to irrelevant
stimuli)
Criteria Hypomanic Episode
• Same as Mania except:– Only needs to last 4 days– Not hospitalized– Not psychotic– Unequivocal change in function (observable to others) but
no significant impairment in function
Could Mr. Flynt have BPAD?
• A: yes• B: no

Treatment of BPAD
What is a “mood stabilizer”?
• Originally , these medications treated mania and prevented its recurrence, thus treating and stabilizing the manic pole of bipolar disorder
• More recent medications can be thought of as treating one of the following phases:– Acute bipolar depression– Acute bipolar mania– Maintenance
Lithium: Mechanism of Action• MOA is unclear• Thought to be involved in:
• Modulating second messenger systems (ie G protein-coupled receptors, through which most hormones and neurotransmitters mediate their effects) which leads to:
• Increasing GABA activity• Reducing glutamate activity• Stabilizing catecholamine receptors• Blocking the effects of some hormones (eg. ADH and TSH) on end organs
• Works in acute bipolar mania, depression and maintenance phases
• Decreases suicide, deliberate self harm and death from all causes in patients with mood disorders
Lithium: Side Effect Profile
• Lethargy• Insipidis• Tremor/Teratogen (increased risk Ebstein’s anomaly
(0.1% vs 0.005%) in first trimester)• Hypothyroid• Increased weight• Vomitting, nausea, GI• Miscellaneous: EKG changes (T wave flattening or
inversion), acne, hair loss
Lithium: Toxicity
• Narrow therapeutic index!!!
• Anything that affects water and electrolyte imbalance can contribute to Lithium toxicity (CAUTION with flu, dehydation, meds)
• Levels are increased by NSAIDS, thiazide diuretics, ACEI, tetracycline, anticonvulsants
• Levels are decreased by caffeine, salt , osmotic diuretics (mannitol) and carbonic anhydrase inhibitors
Lithium: Toxicity
• There is delayed distribution and elimination in the brain relative to serum therefore early signs are peripheral and later signs are central unless high level is chronic, in which case peripheral and central symptoms will occur simultaneously
• Peripheral symptoms: nausea, vomiting, cramping, diarrhea
• Central symptoms: tremulousness, hyperreflexia, ataxia, mental status changes, coma, seizures
• Can lead to irreversible neurotoxicity including cognitive impairment, peripheral neuropathy and cerebellar dysfunction
• Hospitalize for levels >2.0 or based on clinical symptoms
Lithium: Initial Work-up• Lytes, BUN, Cr (renally excreted)• TSH (5% hypothyroidism)• BhCG (risk of teratogenicity)• Calcium, albumin• CBC
• Also consider:• EKG with rhythm strip (contraindicated with sick sinus syndrome)• Metabolic baseline including baseline weight , BMI, waist circumference ,
BP, fasting glucose and lipid profile• Personal and family history of obesity, dyslipidemia, hypertension and
cardiovascular disease
Lithium: Ongoing Monitoring• Lithium level every five days until steady state is reached then
at 3-6 months, with signs of dehydration or toxicity or with change in medications or salt intake
• Repeat kidney functions, TSH and EKG every 6-12 months
• BMI monthly for three months and then 3x per year• Waist circumference at the umbilicus, BP, fasting glucose and
lipid profile repeat at 3 months and then annually
Lithium : Rx Reference only
• Adult• Dosing 600 – 1500 mg/d (bid dosing)• Level 0.5 – 1.2
• Geriatric• Dosing 150 – 600 mg/d (bid dosing)• Level 0.4 – 0.8
Why Use an Anticonvulsant as a Mood Stabilizer: The Kindling Hypothesis
• Term first coined by Graham Goddard in 1967 while studying learning in rats using low intensity electrical brain stimulation
• Over time the rats became sensitized to this and began to have seizures when they received this low intensity signal
• Likened to kindling in starting a fire in that the stimulus is not enough to cause the event on its own but when repeated enough leads to an episode
Why Use an Anticonvulsant as a Mood Stabilizer: The Kindling Hypothesis
• Robert Post drew the parallel to BPAD where the initial episode is often precipitated by a stressor but when cycles continue untreated, the brain can become “kindled” and future episodes can occur with little or no precipitant
• Dysfunctional cation (Na &Ca) pumps leading to an imbalance between excitatory (glutamate) & inhibitory (GABA) neurotransmitters may contribute to this kindling phenomenon
• Anticonvulsants are thought to prolong inactivation of cation channels during activity, preventing spread of activity & leading to downstream changes in GABA & glutamate
Valproic Acid: treatment effects
• Indicated for bipolar mania and for maintenance phase
• First line for bipolar depression in combination with lithium or SSRI/bupropion
• Second line monotherapy for bipolar depression
Valproic Acid: Acute Side Effect ProfileSTUN
• Sedation (31%)• Tremor (10-29%)• Unsteadiness (dizziness)• Nausea (20%) /GI
• Teratogenic – avoid in women of childbearing age
Valproic Acid:longer term side effect monitoring
• On the surface: – Acne , hair loss
• Under the surface: – weight gain, edema
• Systemic: – blood dyscrasias (esp plt dysfn) – liver dysfunction +/- elevated ammonia levels– reproductive changes incl menstrual irregularities (up to
45%), PCOD, teratogenicity (5-15%)
Valproic Acid: Initial Work-up & Ongoing Monitoring
Initial• CBC + LFT’s, BhCG in women• Epival level q2-4 days until steady state reached• Consider: Metabolic baseline including baseline weight and BMI• Baseline personal and family history of obesity, dyslipidemia,
hypertension and cardiovascular disease• Baseline waist circumference at the umbilicus, BP, fasting glucose and
lipid profileOngoing• Repeat tests monthly x 6 months then Q6mos or if symptoms develop• BMI monthly for three months and then 3x per year• Waist circumference at the umbilicus, BP, fasting glucose and lipid profile
repeat at 3 months and then annually
Valproic Acid: RxReference only
• Starting dose:• 250 qhs (geriatrics)• 250 bid-tid (adults)
• Dose range: 750 – 3000 mg/d (bid dosing)
• Levels: 350 – 800 umol/l
Lamotrigine: Treatment effects
• Treats bipolar depression• First line maintenance treatment
Lamotrigine: Side Effect Profile
• Rash – 0.3% adults / 1% in children. With slow titration risk was reduced to 0.01% comparable to other anticonvulsants.
• Activation (3-8%), Ataxia• Spaced out (cognitive slowing), Sedation, Sleep disturbances• H/A, Hypersensitivity reactions
Lamotrigine: Rx
• Start with 25-50 mg/d
• Increase every 2 weeks by 25-50 mg
• Usual maintenance dose is 200 mg in 2 divided doses
Atypical Antipsychotics
• All atypical antipsychotics (risperidone, olanzapine, quetiapine, aripiprazole, ziprazidone) are indicated to treat bipolar mania
• Quetiapine is first line monotherapy for bipolar depression
• Risperidone LAI, olanzapine and quetiapine are first line maintenance treatments
• Further details on mechanism of action, side effects, initial work up and monitoring to be covered during psychosis week
Choice of Treatment in BPAD (Bipolar Affective Disorder)
• First line for acute mania: • Lithium, • Valproic Acid • atypical antipsychotics (olanzapine, risperidone, quetiapine, ziprasidone,
aripiprazole) • taper and discontinue antidepressants
• First line for acute bipolar depression: • Lithium• lamotrigine • quetiapine
• do not use antidepressant monotherapy
• First line for maintenance therapy: • Lithium• Valproic acid• Lamotrigine• Atypical antipsychotics quetiapine, risperidone LAI and Olanzapine
Goals of treatment in BPAD
• Again, the goal is to treat to complete remission of all mood symptoms
• It has been theorized that under-treated discrete depressive and manic episodes may progress to mixed and dysphoric episodes, rapid cycling and treatment resistance
• The hope is that recognition and full treatment of mood episodes may prevent progression to more difficult mood states
Pre-test (true/false)
• All patients with symptoms of major depression should be treated with an antidepressant – FALSE
• Mirtazapine causes drowsiness through it’s effects on the benzodiazepine receptor – FALSE (antihistaminic)
• SNRIs such as Venlafaxine can cause diastolic hypertension - TRUE
Pre-test (true/false)
• Trazodone is rarely tolerated at full therapeutic dosages due to significant sedation side effects - TRUE
• Lithium is rarely tolerated due to multiple side effects and should be reserved only for treatment resistant bipolar patients - FALSE
• Atypical antipsychotics are indicated as first line monotherapies for bipolar depression, mania and maintenence treatments - TRUE
References• CANMAT Clinical guidelines for the management of major depressive disorder in
adults. III. Pharmacology• CANMAT guidelines for the management of patients with bipolar disorder: update
2009• Stahl’s Essential Psychopharmacology, Third edition, Cambridge University Press,
2008.• Ottawa Review Course of Psychiatry• DSM5• Mnemonics are in part from mnemonics and more for psychiatry, P.I.E.C.E.S
education Initiative & mnemonics in mnutshell, Current psychiatry, Oct 2008• The Hunter Serotonin Toxicity Criteria, QJ Med 2003• Current Concepts: The Serotonin Syndrome, NEJM, 352, 11, 1112-1123• Special thanks to Dr. Michael Cheng for input on child content and to Perry Ng for
preparing images• 2008 Position Paper on Using SSRIs in Children and Adolescents. J Can Acad
Adolesc Psychiatry 18:2 May 2009