Embed Size (px)
Citation preview

ESSENTIAL
PSYCHOPHARMACOLOGY
2011: GERIATRIC
PSYCHOPHARMACOLOGY
Carl Salzman MD
Key Largo, Florida

LECTURE OUTLINE
• Depression
• Bipolar disorder
• Alzheimers Disease
– Treatment of agitation/psychosis
– Treatment of cognitive impairment

DEPRESSION

LATE ONSET DEPRESSION
• First depression after 60
• Less robust response to antidepressants
• May be associated with elevated
homocysteine levels
• May be associated with MRI
hyperintensities
Chen, 2005

ROLE OF MEDICAL
COMORBIDITY• Overall, medical comorbidity decreases rate of
response to antidepressants in the elderly although overall response percentage is not affected by illness– Response rate is particularly slow in chronic
pulmonary disease
– Rate is faster patients with atrial fibrillation
• Prostate cancer increases risk of suicide
• Depression is associated with poor medication adherence in diabetics
Kilbourne;LlorenteBogner;
2005





EFFECT OF MEDICAL
ILLNESS IN ELDERLY• Increases risk for depression
• Increases risk of polypharmacy, drug
interactions
– Increases risk for further depression, anxiety,
insomnia, agitation, and side effects
• Medical illness is a leading cause of
suicide in the elderly

RISK OF SUICIDE IN
ELDERLY• Major risk factor is medical illness
• Associated risk factors:
– Loss of function
– Loss of loved ones, friends
– Loss of purpose
– Move from lifelong home
• Associated risk factors:
– Alcohol
– Presence of a gun at home

VASCULAR DEPRESSION
• Characteristics:– Onset after 65 or change in course after onset;
– Persistent symptoms;
– Association with vascular disease or risk factors;
– Associated with white matter hyperintensities
• Symptoms:– Executive dysfunction
– Psychomotor retardation
– Poor insight
– Impaired motivation
– Poor concentration
• Highly prevalent in hypertension, diabetes, coronary artery disease, severe atherosclerosis
Alexopolous 2002; Kales, 2005; Nebes, 2001

DEMENTIA SYNDROME OF
DEPRESSION (DOD)
• Previously called “pseudodementia”
– Is a true dementia, but is reversible
• Four essential diagnostic criteria:
– Evidence of a primary depression with intellectual
impairment
– Clinically, must resemble degenerative dementia
– Intellectual impairment reverses with treatment
– No evidence of primary degenerative process causing
the dementia

DEPRESSION-EXECUTIVE
DYSFUNCTION SYNDROME• Due to frontostriatal dysfunctions
• Characterized by depressed mood and:– Psychomotor retardation and reduced interest
– Less pronounced vegetative symptoms than in major depression
– Fatigue
– Sense of worthlessness
– Cognitive dysfunction
• Poorer response to antidepressants
Sneed 2011; Am J Geriatr Psychiatry 19:99

STROKE RELATED
DEPRESSION• Very high incidence of post-stroke
depression
• Almost all antidepressants are effective
treatments after depression onset
• Escitalopram may prevent onset of
depression after stroke
Robinson, JAMA 2008; 299:2391

SSRIs IN THE ELDERLY
• As effective as TCAs for mild/moderate
depressions
• No anticholinergic or cardiac side effects
• Equal efficacy among all drugs
• Inhibit cytochrome enzymes:
– Fluoxetine (2D6; 3A4)
– Paroxetine (2D6)

Β-BLOCKERS AND DEPRESSION
IN THE ELDERLY
• Β-blockers do not cause depression in the
elderly
• However, highly lipid-soluble Β-blockers
(e.g. propranolol) may increase depressive
symptoms during the first 3 months of
treatment
Luijendijk 2011; J Clin Psychopharmacology 31:45

METHYLPHENIDATE
• Enhances antidepressant response
– (average dose: 10mg/d)
– Response by 3 weeks
• Enhances social performance
• Side effects: anxiety, nausea, urinary
hesitancy
» Lavretsky, 2004

BIPOLAR DISORDER

Sajatovic,2005
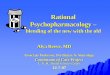
LITHIUM VS. LAMOTRIGINE FOR BP I

DEMENTIA

CHARACTERISTICS OF
DEMENTIA RELATED
PSYCHOSIS• Psychotic symptoms present in 30-50% of AD patients
• 4 year cumulative incidence: 50% of AD patients develop psychosis
• Delusions persist for years
• Associated with behavioral disruption
• Causes great distress in families, caregivers
• Commonly results in institutionalization
• Suggests a distinct syndrome: “Dementia Related Psychosis”
• Lewy-body dementia characterized by visual hallucinations and agitation
Jeste & Finkel, 2000

PREVENTING DEMENTIA?
• Statins do not influence onset of AD or
influence cognition in AD
• NSAIDs may influence onset of AD,
especially ibuprofen.
• Vitamin E does not prevent dementia
Arvanitakis; Neurol 2008; 70:1795;
Vlad; Ibid, 2008; 70:1672

VASCULAR DEMENTIA
• Previously called “Multi-Infarct” dementia
or “arteriorsclerotic dementia”
• Defined as: “a clinical syndrome of
acquired intellectual and functional
impairment resulting from the effects of
cerebrovascular disease”
• May be due to stroke or risk factors for
stroke

DEMENTIA WITH LEWY BODIES
(DLB)
• Dementia syndrome like AD with 3 characteristics:– Fluctuating cognition (day to day)
– Visual hallucinations (people, animals)
– Parkinsonism
• Accounts for 15% of all dementias
• More severe cholinergic deficit than AD
• Very sensitive to conventional neuroleptics
• Better response to cholinergic treatments and SSRIs than AD patients

ALZHEIMERS’S DISEASE:
TREATMENT OF AGITATION
• All neuroleptics are moderately effective– Atypical NLs are first choice, using low doses
• Risperidone: 0.25-1mg/d
– Higher doses are effective but more side effects
• Olanazpine: 2.5-15 mg/d
• Seroquel: 25-200mg/d
– Typicals are still very useful• Haloperidol 0.25 mg-1 ng/d
• Use liquid preparations to get low doses

TYPICAL NEUROLEPTICS
• Overdosed and underdosed
• Modestly effective
• No differential efficacy
• Drug selection based on side effect profile
• “Start low and go slow”

ATYPICAL NEUROLEPTICS:
RISPERIDONE
• 0.5-2mg effective
• Increased EPS with higher doses
• 1.0 mg/d optimum dose for agitation
• Side effects:
– EPS
– Activation
– Recent data on increased risk of stroke

ATYPICAL NEUROLEPTICS:
OLANZAPINE
• 2.5-15 mg effective dose
• Good mood stabilizing properties
• Side effects:
– Sedation
– Weight gain, hyperlipidemia, diabetes

ATYPICAL NEUROLEPTICS:
QUETIAPINE
25-200 mg effective dose; average dose 100-
200mg/d (200 superior for Alzheimer’s
patients)
Side effects:
hypotension
decreased renal clearance
No cerebrovascular events
Zhong, 2004

NEW ATYPICAL NEUROLEPTICS
• Ziprasidone
• Aripiprazole
» Both are effective
» Both are activating

De Deyn 2005
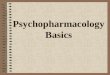
ARIPIPRAZOLE TREATMENT OF PSYCHOSIS IN AD

CATIE-AD
• No overall difference among drugs in dropout; slightly better for olanzapine;
• Lower drop out rate with placebo due to safety or tolerability problems;
• Small statistical improvement for active medications; evidence for efficacy is not seen consistently
• No difference in costs among drugs; extra drug costs for PBO group equalized all

DO ANTIPSYCHOTICS CAUSE
STROKES IN THE ELDERLY?
• FDA now requires black-box warning on
all antipsychotics:
– Death rate in dementia patients receiving
atypical antipsychotic was 1.6-l.7 times that of
PBO
– Sample of 1130 cases >65
– Increased odds ratio suggest increased risk of
cardio- or cerebrovascular events by 20-50%

DO ANTIPSCHOTICS CAUSE
STROKES IN ELDERLY?
• Canadian database: no difference in risk of ischemic stroke between atypical and conventional antipsychotics
• Modest increase risk with all antipsychotics but not statistically significant (Gill, 2005)
• No statistically significantly increased risk of stroke with any antipsychotic (Hermann, 2004)

COGNITIVE EFFECTS OF
ATYPICAL ANTIPSYCHOTICS IN
ALZHEIMER’S• Data from CATIE-AD trial
• Drugs taken: olanzapine, quetiapine,
risperidone, placebo
• Steady, significant declines over 26 weeks
in most cognitive areas
– Declines worse when doses were high
Vigen, 2011; AJP 168:831

MOOD STABILIZERS FOR
AGITATION IN DEMENTIA - I
• VPA and carbamazepine useful for treatment of dementia associated aggression1
• Gabapentin useful for agitation in chronic, severely and persistently mentally ill patients and for dementia associated agitation2
• Gabapentin added to donepzil for treatment of evening agitation3
1Tariot, 1994; Salzman, 19982Megna, 2002; Regan, 1997; Hermann, 2000

VALPROATE TREATMENT OF
AGITATION IN DEMENTIA
• Modest efficacy in controlling agitated behavior
– Dose: 750/d
– Recent study: not different from placebo (Tariot, 2006)
• May exert neuroprotective effects by inhibiting glycogen synthase kinase 3
• Effective when added to antipsychotic drug

CARBAMAZEPINE FOR
AGGRESSION IN DEMENTIA
Tariot,1998

LAMOTRIGINE FOR AGITATION
• Study sample: demented patients in an
acute care hospital unit (N=26)
• Dose: Initial 50mg/d, titrated to 400mg/d
– (mean dose 190mg/d)
• Dramatic antiaggressive effects
• Main side effects: mild tremor, ataxia,
sedation

AGITATION: SEROTONERGIC
DRUGS AND MOOD
STABILIZERS
• Trazodone (25-100mg/d) best second
choice
• Buspirone (60-100mg/d) effective in about
50% of demented patients

ALZHEIMER’S DISEASE
TREATMENT OF COGNITION

MEMORY LOSS
• Age-associated memory impairment (AAMI) is normal
• Memory loss correlates with decline in acetylcholine functioning. Cholinergic treatments include:– Donepzil (Aricept)
– Rivastigmine (Exelon)
– Galantamine (Reminyl)
• Each can modestly improve memory or slow its decline; no drugs reverse true dementia

RELATIONSHIP BETWEEN
DEPRESSION AND DEMENTIA
• Late-life depression is a risk for becoming
demented
– Approximately 20% become demented over a
7 year period
– Early life depression did not increase the risk
• Late-life depression may be an early
manifestation of dementia rather than
increasing the risk for dementia
Li, 2011; ArchGenPsychiat 68:970

TREATMENT OF COGNITION IN
ALZHEIMER’S
• Cholinesterase inhibitors
– Modest efficacy in mild/moderate dementias
– May have mild therapeutic effects on agitation as well
as on cognition
• Rivastigmine (Exelon)
– Butyrlcholinesterase as well as acetylcholinesterase
inhibitor
• Galantamine
– Most recent AChE (Reminyl)
– Affects nicotine and cholinergic receptors

RIVASTIGMINE (EXELON)
• Inhibits acetylcholinesterase and
butyrlcholinesterase
• 5 year metaanalysis of studies: treated
patients were 3-5X better on cognitive
measures
• Dose: 6-12mg/d
• Demonstrated excellent response in DLB

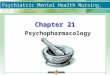
EFFECT OF GALANTAMINE
Lyketsos, 2005

EFFECT OF GALANTAMINE -2
Lyketsos, 2005

TREATMENT OF ALZHEIMER’S:
MEMANTINE (NAMENDA)• Not a cholinesterase inhibitor
• Non-competitive NMDA receptor antagonist
• Dose: 10-20mg/d
• Efficacy in slowing progress of late-stage Alzheimers Disease
• Also has efficacy in mild/moderate Vascular Dementia
• Commonly combined with a cholinesterase inhibitor: significantly decreased behavioral symptoms when combined with donepezil
»
• Cummings, 2004


NEW DRUG FOR DEMENTIA-II
• Rivastigmine (Exelon) is now available as
a patch
• Starting dose: 4.6 mg
– Increase after 4 weeks to 9.5 mg
• Side effects: nausea, vomiting, diarrheaq,
skin irritation