Embed Size (px)
DESCRIPTION
Â
Citation preview
Journal of Counseling Psychology1990, Vol. 37, No. 1,3-9
Copyright 1990 by the American Psychological Association, Inc.0022-0167/90/S00.75
The (Mis)Treatment of Men: Effects of Client GenderRole and Life-Style on Diagnosis and Attribution
of Pathology
John RobertsonGraduate School of Education
University of California, Santa Barbara
Louise F. FitzgeraldDepartment of Educational Psychology
University of Illinois at Urbana-Champaign
Practicing counselors and therapists (N = 47) were randomly assigned to view one of two versionsof a videotaped simulation of a depressed White male client, portrayed by a professional actor.The tapes were identical except for the client's occupational and family roles, which wereportrayed as either gender-traditional or nontraditional. During specified pauses in the videotape,the therapists responded verbally as if they were conducting a counseling session with a client,and their responses were recorded. After the completion of the viewing session, the subjectsevaluated the client on various dimensions, assigned a diagnosis, and outlined a proposedtreatment plan. The results suggest that the client's gender role affected several aspects of thetherapists' behavior, including the attribution of pathology and problem etiology.
For nearly 2 decades scholars have examined the hypothesisthat counseling and psychotherapy function to support thestatus quo and to inhibit change in the social and vocationalroles of women. Although disagreement about this proposi-tion still exists (see Richardson & Johnson, 1984, for a reviewand critique), numerous studies have appeared to documentthe existence of what is generally known as sex or gender biasin the process of counseling and psychotherapy. Given thepossibility that clinicians have suggested and reinforced thatnarrow segment of psychological and vocational options re-'flected by the traditional female role, research has long doc-umented the existence of negative therapist attitudes towardwomen as well as toward nontraditional roles for women(Abramowitz, Abramowitz, Jackson, & Gomes, 1973; Amer-ican Psychological Association Task Force, 1975; Broverman,Broverman, Clarkson, Rosenkrantz, & Vogel, 1970). Theclassic work in this area is that of Chesler (1972), who waspossibly the first to suggest that therapy functioned in manyways as an agent of social control through which women wererewarded for passivity and punished for social deviance bybeing labeled as sick.
One interesting outgrowth of this research has been thesmall but growing body of literature that focuses on the effectof such gender stereotyping on the psychological developmentand behavior of men. Although Abramowitz et al. (1973)early suggested that men are allowed a wider latitude ofnormal behaviors than are women, research suggests that thislatitude does not extend to behaviors traditionally associated
Portions of this article were presented at the 1987 meeting of theWestern Psychological Association, Long Beach, California.
We wish to thank Brandt Bergerlain and Mary Manlon for theirextensive assistance with data collection and coding.
Correspondence concerning this article should be addressed toJohn Robertson, who is now at University Counseling Services,Kansas State University, Manhattan, Kansas 66S06 or to Louise F.Fitzgerald, Department of Educational Psychology, University ofIllinois, 1310 South Sixth Street, Champaign, Illinois 61820.
with women. For example, Fitzgerald and Cherpas (1985)noted that some evidence indicates that sex-inappropriatebehavior evokes even greater parental concern when exhibitedby boys than by girls (Fling & Manosevitz, 1972; Good-enough, 1957; Lansky, 1967), and Costrich, Feinstein, Kidder,Marcek, and Pascale (1975) reported that college studentsubjects rated sex role-incongruent men as less popular andmore in need of psychotherapy. Similarly, Silverberg (1986)reviewed studies that indicated that sex role-deviant behavioris punished more severely in men than in women in variousways.
One area where the effects of such stereotyping have beenshown to be particularly strong has been that of vocationalbehavior. O'Neil (1982) pointed out that men have beensocialized and expected to work outside the home, with suchemployment as their chief source of status and self-definition.Several books in recent years have explored the power andmeaning of this expectation (e. g., Farrell & Rosenberg, 1981;Goldberg, 1976). The intensity of this societal demand thatmen work (i.e., engage in paid employment) has also beennoted, as has the assumption that men learn that work is theprimary way to define personal worth (Morgan, Skovholt, &Orr, 1979; O'Neil, 1980; Pleck & Sawyer, 1974; Skovholt,1978).
The notion that sex role expectations are at least equally asstrong for men as they are for women and that men experiencesimilar pressures to conform their behavior, particularly theirwork behavior, to these expectations has led some writers tosuggest that counseling and psychotherapy may also functionto reinforce a traditional role for men, much as they havebeen thought to do for women. Initial empirical support forthis suggestion was provided by Fitzgerald and Cherpas(1985), who reported that their sample of counselors-in-train-ing demonstrated negative reactions to a male client whodiscussed and ultimately selected a gender-nontraditional oc-cupational role. Although this work raises interesting issues,it can be criticized not only for its sample of relativelyinexperienced trainees (whose reactions might be related to

JOHN ROBERTSON AND LOUISE F. FITZGERALD
their lack of experience and incomplete training) but also forits use of a relatively weak analogue (audiotape and paper-and-pencil rating scales), in which both the independent anddependent variables bore little resemblance to actual counsel-ing process or counselor behavior. The present study attemptsto improve on that work through examining practicing ther-apists with a more powerful interactive analogue, one thatuses actual counselor behaviors as outcome measures.
The following hypotheses were tested: (a) Counselors re-spond differently to nontraditional male clients than to tra-ditional ones, and specifically, they are more directive in theirresponses; (b) counselors view nontraditional male clients assuffering from more severe problems and pathology thanotherwise identical men; (c) counselors implicate differentetiological factors in the problems of nontraditional maleclients; specifically, when a man has major domestic respon-sibilities, counselors are likely to attribute any psychologicaldifficulties to this situation; and (d) counselors view the non-traditional client as more feminine and less masculine thanhis gender-traditional counterpart.
Method
Overview
Forty-seven practicing counselors-therapists were randomly as-signed to one of two versions of a videotaped simulation of a depressedWhite male client, portrayed by a professional actor. During specifiedpauses in the videotape, the therapists responded verbally as if theywere conducting a counseling session with the client, and theirresponses were recorded by means of a lapel microphone. Aftercompleting the simulated interview, the subjects evaluated the clienton various dimensions, assigned a diagnosis, and outlined a proposedtreatment plan.
Subjects
The subjects were 47 licensed marriage and family therapists (18men and 29 women) engaged in private practice in a prosperouscounty of a large west coast state. The names of prospective subjectswere obtained from a state-provided list organized by county, and alltherapists who practice in the designated county were contacted bymail and invited to participate in a project to study "the informationthat therapists use to make assessments of their clients' problems."After the subjects had received the letter, each was contacted byphone and personally invited to take part in the study. A total of 47therapists agreed to participate, which provided a 41% sample of thecounselors in the area. Although less than optimal, this participationrate seems reasonable, given that the study required more than 2 hrof the subjects' professional time, with no remuneration. The subjectsranged in age from 28 to 71 (M = 44.9, SD - 12.2) and averagedapproximately 12 years of professional experience (SD = 7.3). Toobtain the state license that allows them to practice, all subjects hadbeen required to complete a master's level counseling training pro-gram; 5 subjects also had doctoral degrees. The subject-therapistsidentified a wide range of preferred therapeutic orientations, with noone predominant system.
Experimental Materials
Two parallel versions of a color videotape were prepared, eachportraying close-up scenes of a young male client in his mid-20s. No
counselor was visible on the videotape; instead, the client, filmedagainst the backdrop of a therapist's office, looked directly into thecamera and spoke as if addressing his therapist. This client, portrayedby a dramatic arts student and professional actor, discussed hisdepression in a series of nine segments taken from counseling sessionsthat spanned 6 weeks. Each segment featured the client's talkingabout a particular aspect of his problem. After each of the ninesegments, the screen went silent for 15 s, during which time thesubjects verbally responded to the client as if they were in thecounseling room with him. In effect, they talked to the televisionmonitor as though it were the actual client, and their responses wererecorded on a separate audiotape system.
Two versions of the videotape were produced, with the same actorin both. In one version the client was portrayed as having the majorresponsibility for domestic matters, including child care, whereas hiswife was the main breadwinner and was employed in a nontraditional,professional-level occupation (engineering). In the second version hetook the traditional role and indicated that he himself was an engineerand his spouse a homemaker and mother. This information wasembedded in the first videotaped segment, during which the clientbriefly described his life situation. In each version the client specifi-cally indicated that his marital arrangement was satisfactory (i.e.,"That's not the problem. My wife's not the problem. My kids . . .they aren't the problem either. I'm the problem."). Otherwise, thetwo versions of the videotape were virtually identical, with the excep-tion of matched references to his daily activities. The client describedvarious symptoms of his depression (poor appetite, boredom, sleep-lessness, guilt, etc.) and illustrated his concerns by referring to variousexperiences and incidents in his life. The original scripts for thevideotape were written by John Robertson, who had extensive expe-rience in television production and script writing. They were thenedited by both the authors and the actor who played the client, toensure smoothness, believability, and compatibility with the actor'sstyle.
Procedure
The subjects were randomly assigned, within sex, to view one ofthe two versions of the videotape. All experimental sessions were heldat the psychological clinic of the university where the study wasconducted. On arrival at the clinic, the subject was met by anexperimenter and ushered into the family therapy room, where he orshe was connected to a lapel microphone and given preliminaryinstructions. The experimenter then switched on the videotape andleft the room. All instructions were given by John Robertson andLouise F. Fitzgerald, who appeared on the videotape, welcomed thesubject, and then explained that the study was an examination of theinformation that therapists use in making decisions about theirclients. The subjects were told that they would be viewing a videotapeof a client over several therapy sessions and were instructed how torespond to the client when he fell silent. They were then given severalpractice trials, during which they responded to a practice tape of awoman client portrayed by a counseling psychology graduate student.They were instructed how to signal the experimenter if they neededassistance. After an opportunity to stop the tape and ask questions,the experimental portion of the tape began. After completing thetape, each subject responded to several questionnaires and ratingforms about the client as well as a biographical data sheet. They werethen thanked for their participation, escorted to the lobby, anddismissed. Debriefing took place through a letter sent to each partic-ipant, that also included the results of the study. No subject indicatedin any way that they believed gender roles to be the focus of thestudy.

EFFECT OF CLIENT GENDER ROLE ON DIAGNOSIS
Dependent Variables
Counselor Verbal Response Category System. Developed by Hill(1978), this classification system defines 14 different counselor re-sponse modes and collapses these 14 categories into five hierarchicalgroups: (a) minimal responses (minimal encouragers, silence); (b)directives (approval/reassurance, information, direct guidance); (c)questions (closed question, open question); (d) complex counselorresponses (restatement, reflection, interpretation, confrontation); and(e) strange bedfellows (nonverbal referent, self-disclosure, and other).In developing the system, Hill et al. used three judges to classify eachcounselor response into one of the 14 categories and obtained averageagreement levels for all pairs of the three judges (K = .79). Hill et al.reported other studies that showed agreement levels of K = .71 (Hill,Thames, & Rardin, 1979) and K = .79 (Hill, Charles, & Reed, 1981).In our study four judges were used, which thus predictably loweredthe average agreement (« = .63 for all pairs of judges over the 14categories). Because this figure was below .70, the responses werecombined into their hierarchical categories and the reliability recom-puted. At this level of analysis, K = .84 over all pairs of raters, on atotal of 1,114 response units.
Diagnostic questionnaire. A questionnaire was developed togather information about the dependent variables: diagnosis, problemseverity, and etiological factors. After completing a biographical datasheet, the subjects were requested to characterize the presentingproblem, that is, to assign a diagnosis. A copy of the Diagnostic andStatistical Manual of Mental Disorders (DSM-III; American Psychi-atric Association, 1980) was available to the subjects for reference.The revised version of the DSM-III (DSM-III-R; American Psychi-atric Association, 1987) was only recently published when this studywas conducted. The subjects used DSM-III and their diagnoses werelater converted to DSM-III-R terminology, which in this case requiredonly minor word changes. Next, the subjects were presented with alist of eight factors that might reasonably be thought to be contributingto the client's problem: his marriage, his children, his financialsituation, his occupational situation, his physical health, intrapsychicfactors (e.g., conflict, self-image, identity issues, ego integrity, etc.),poor coping skills, and biological factors, including family of origin.The subjects were instructed to check all that applied and then in aseparate item were asked to rank order those same areas in terms ofthe degree to which they would want to explore them further withthis client, if they had the opportunity to actually interact with him.The subjects were also asked to rate on 7-point Likert scales theseverity of the client's problem and their willingness to work withhim. Finally, they were asked to indicate the minimum number oftherapy sessions that would be required to effect therapeutic change:10 or less, 10-20, or up to a year.
Bern Sex Role Inventory (BSRI). The BSRI is a 60-item inventorythat consists of two 20-item scales—designated as Masculinity andFemininity—and 20 neutral items. These 60 items are personalitycharacteristics previously scaled as desirable for men (the Masculinityitems), desirable for women (Femininity items), or desirable for bothmen and women (the neutral items). The subjects were instructed toindicate on a 7-point scale the degree to which each characteristicwas descriptive or true of the client they had just observed on thevideotape. Bern (1978) reported acceptable internal consistency andstability coefficients for the BSRI. In addition, Masculinity andFemininity scores from the inventory have been shown to be uncor-related (Bern, 1978). Spence (1984) noted that the BSRI Masculinityand Femininity scales appear to be essentially measures of assertiveand interpersonal orientation, respectively.
Results
The first hypothesis predicted that counselors who viewedthe client in the nontraditional role would be more directive
than those who viewed the traditional role, that is, they woulduse more directive responses (approval-reassurance, infor-mation, and direct guidance). The data relevant to this hy-pothesis were examined from both a statistical and qualitativeperspective. Chi-square analysis on the hierarchical combi-nations of counselor responses did not support the hypothesis;in fact, as can be seen from Table 1, the distribution ofresponse modes across the two conditions were very similar.However, when the actual content of the subjects' responseswas examined, some fairly pronounced differences appeared.Among the subjects who viewed the nontraditional client,10% of all response units referred in some way to the marriageagreement. Typical comments included "What messages doyou have from your childhood about what a man is?" "Youprobably need to renegotiate this contract that (you've) got athome," and "Maybe we need to take a look at the bargain,and see if it's still what you and Judy want." By contrast, nocounselors who viewed the traditional client made suggestionsabout changing the domestic arrangements and agreementthat he had made with his wife. Thus, this first hypothesisreceived moderate support.
The second hypothesis predicted that the client's problemwould be viewed as more severe when he was portrayed in anontraditional role than when he appeared in a traditionalone. Three measures of severity were obtained: DSM-IIIdiagnosis, Likert severity ratings, and estimates of treatmentlength. Means and standard deviations of all rated variablesappear in Table 2. Table 3 contains summaries of all statisticalanalyses. The data indicate partial support for the secondhypothesis. With respect to direct severity ratings and esti-mated length of treatment, t tests of the group ratings indi-cated that there were no differences between the two condi-tions. To examine the diagnostic codes, they were first classi-fied into one of three categories: severe mood disorder (bipolar
Table 1Percentage of Total Responses by Hill Counselor VerbalResponse Category
Condition
Response type Traditional Nontraditional
Minimal responsesMinimal encourager 2Silence 1
DirectivesApproval-reassurance 7Information 16Direct guidance 8
QuestionsClosed question 12Open question 29
Complex counselor responsesRestatement 4Reflection 3Interpretation 14Confrontation 1
Strange bedfellowsNonverbal referent 1Self-disclosure 1Unclassifiable —
21
9159
827
36
171
Note. N = 1,114 responses. Dashes represent percentages less than
JOHN ROBERTSON AND LOUISE F. FITZGERALD
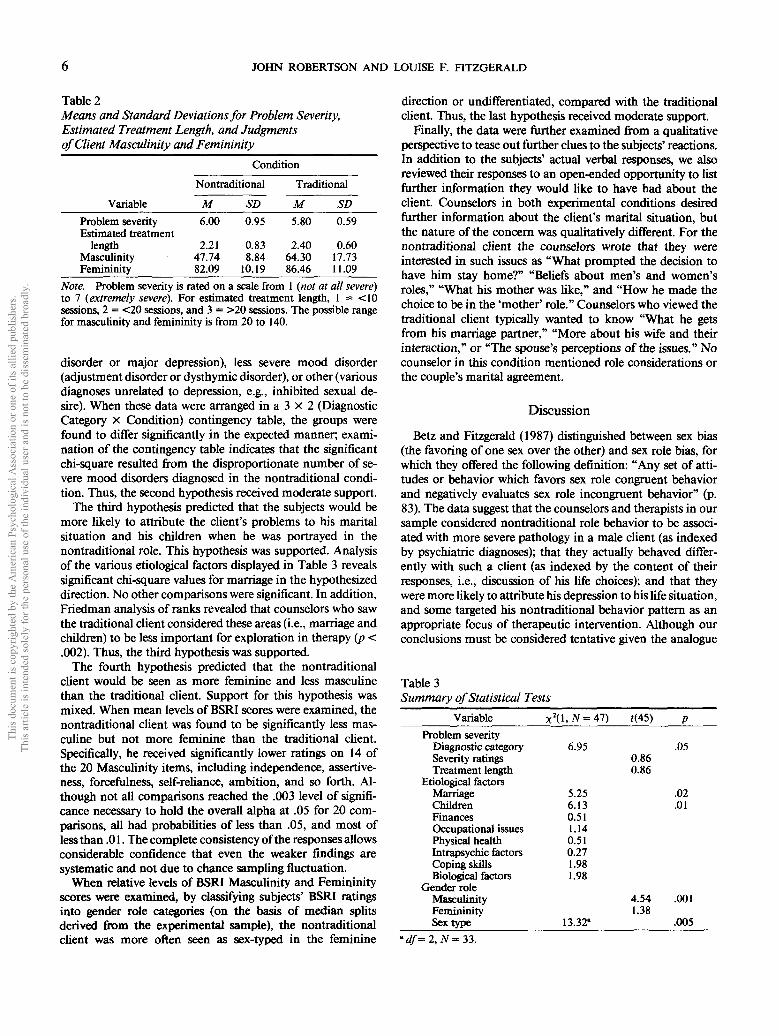
Table 2Means and Standard Deviations for Problem Severity,Estimated Treatment Length, and Judgmentsof Client Masculinity and Femininity
Condition
Nontraditional Traditional
Variable M SD M SDProblem severityEstimated treatment
lengthMasculinityFemininity
6.00
2.2147.7482.09
0.95
0.838.84
10.19
5.80
2.4064.3086.46
0.59
0.6017.7311.09
Note. Problem severity is rated on a scale from 1 (not at all severe)to 7 (extremely severe). For estimated treatment length, 1 = <10sessions, 2 = <20 sessions, and 3 = >20 sessions. The possible rangefor masculinity and femininity is from 20 to 140.
disorder or major depression), less severe mood disorder(adjustment disorder or dysthymic disorder), or other (variousdiagnoses unrelated to depression, e.g., inhibited sexual de-sire). When these data were arranged in a 3 x 2 (DiagnosticCategory x Condition) contingency table, the groups werefound to differ significantly in the expected manner, exami-nation of the contingency table indicates that the significantchi-square resulted from the disproportionate number of se-vere mood disorders diagnosed in the nontraditional condi-tion. Thus, the second hypothesis received moderate support.
The third hypothesis predicted that the subjects would bemore likely to attribute the client's problems to his maritalsituation and his children when he was portrayed in thenontraditional role. This hypothesis was supported. Analysisof the various etiological factors displayed in Table 3 revealssignificant chi-square values for marriage in the hypothesizeddirection. No other comparisons were significant. In addition,Friedman analysis of ranks revealed that counselors who sawthe traditional client considered these areas (i.e., marriage andchildren) to be less important for exploration in therapy (p <.002). Thus, the third hypothesis was supported.
The fourth hypothesis predicted that the nontraditionalclient would be seen as more feminine and less masculinethan the traditional client. Support for this hypothesis wasmixed. When mean levels of BSRI scores were examined, thenontraditional client was found to be significantly less mas-culine but not more feminine than the traditional client.Specifically, he received significantly lower ratings on 14 ofthe 20 Masculinity items, including independence, assertive-ness, forcefulness, self-reliance, ambition, and so forth. Al-though not all comparisons reached the .003 level of signifi-cance necessary to hold the overall alpha at .05 for 20 com-parisons, all had probabilities of less than .05, and most ofless than .01. The complete consistency of the responses allowsconsiderable confidence that even the weaker findings aresystematic and not due to chance sampling fluctuation.
When relative levels of BSRI Masculinity and Femininityscores were examined, by classifying subjects' BSRI ratingsinto gender role categories (on the basis of median splitsderived from the experimental sample), the nontraditionalclient was more often seen as sex-typed in the feminine
direction or undifferentiated, compared with the traditionalclient. Thus, the last hypothesis received moderate support.
Finally, the data were further examined from a qualitativeperspective to tease out further clues to the subjects' reactions.In addition to the subjects' actual verbal responses, we alsoreviewed their responses to an open-ended opportunity to listfurther information they would like to have had about theclient. Counselors in both experimental conditions desiredfurther information about the client's marital situation, butthe nature of the concern was qualitatively different. For thenontraditional client the counselors wrote that they wereinterested in such issues as "What prompted the decision tohave him stay home?" "Beliefs about men's and women'sroles," "What his mother was like," and "How he made thechoice to be in the 'mother' role." Counselors who viewed thetraditional client typically wanted to know "What he getsfrom his marriage partner," "More about his wife and theirinteraction," or "The spouse's perceptions of the issues." Nocounselor in this condition mentioned role considerations orthe couple's marital agreement.
Discussion
Betz and Fitzgerald (1987) distinguished between sex bias(the favoring of one sex over the other) and sex role bias, forwhich they offered the following definition: "Any set of atti-tudes or behavior which favors sex role congruent behaviorand negatively evaluates sex role incongruent behavior" (p.83). The data suggest that the counselors and therapists in oursample considered nontraditional role behavior to be associ-ated with more severe pathology in a male client (as indexedby psychiatric diagnoses); that they actually behaved differ-ently with such a client (as indexed by the content of theirresponses, i.e., discussion of his life choices); and that theywere more likely to attribute his depression to his life situation,and some targeted his nontraditional behavior pattern as anappropriate focus of therapeutic intervention. Although ourconclusions must be considered tentative given the analogue
Table 3Summary of Statistical Tests
Variable x2
Problem severityDiagnostic categorySeverity ratingsTreatment length
Etiological factorsMarriageChildrenFinancesOccupational issuesPhysical healthIntrapsychic factorsCoping skillsBiological factors
Gender roleMasculinityFemininitySex type
(\,N=41)
6.95
5.256.130.511.140.510.271.981.98
13.32"
f(45) p
.050.860.86
.02
.01
4.54 .0011.38
.005
'df=2, AT =33.
EFFECT OF CLIENT GENDER ROLE ON DIAGNOSIS
nature of the study, we believe that this pattern of resultsmeets the criteria for gender role bias suggested by Betz andFitzgerald and provides initial support for the contention thatsuch bias may influence the psychotherapeutic treatment ofnontraditional men. Although it is obviously true that thenumber of men who actually take major responsibility forhomemaking and child care is relatively small and likely toremain so, it is also true that more men than ever before areinvolving themselves in these activities to some degree and inother ways attempting to break out of rigidly stereotypicmasculine behaviors. Our findings suggest that psychotherapy,as an essentially conservative social institution, may be asunprepared to deal effectively with such men as it was withnontraditional women a generation ago.
Limitations of the Study
Before exploring the implications of the findings, theirlimitations must be assessed. These are discussed with respectto internal and external validity considerations as well asalternative interpretations of the results.
Our investigation suffers from the usual limitations ofanalogue research. The primary one is, of course, just that:This is an analogue investigation. Several factors suggest,however, that such limitations may be of less concern than issometimes the case. With respect to external validity (i.e.,generalization), the present investigation examined a largesample of experienced, practicing counselors and psychother-apists who were professionally engaged in the day-to-dayactivities of counseling. It is, of course, important to note thatthe size of our sample and its sex composition did not allowus to analyze the data for possible gender effects, effects thathave sometimes been shown to occur in studies of reactionsto female clients. Our inferences are also limited to Whitetherapists who are responding to a White male client. Thepossible influence of alternative racial or cultural back-grounds, of either counselor or client, is unknown.
Although some paper-and-pencil measures were used (atraditional criticism of analogue studies), the major dependentvariables were other, extremely powerful ones, in that theywere actual counselor behaviors, that is, verbal responses(albeit in a simulated session), diagnosis, evaluation of possi-ble etiological factors, treatment planning, and so forth. It isinteresting to note that it was these variables, rather than thepaper-and-pencil Likert scales such as those traditionally em-ployed in counseling analogues, that were sensitive to theexperimental intervention.
With respect to internal validity, one limitation in thedesign of the study may be noted. Due to practical constraints,no parallel experimental videotapes that used a female clientwere constructed and tested, which thus results in an incom-plete design. Such a design, with four experimental conditions,would allow an even more powerful test of the present hy-potheses; however, the data seem clear that the subjects wereresponding to the nontraditional nature of the client's familyinvolvement, that is, to the interaction of his sex with hischosen role. Examination of the areas that subjects wished toprobe with the client make this point quite clearly, for ex-ample, "What made him choose the 'mother' role?" "What
messages did he get about what it means to be a male?" andso forth. Thus, although comparable data on reactions tofemale clients that would allow formal examination of maineffects and interactions for gender and role are certainlydesirable, the differential therapist responses to the traditionaland nontraditional male clients in the present study providestrong inference that it is indeed the Gender x Role interac-tion to which they were responding. Future research ought toattempt to examine this more formally.
Finally, it is necessary to consider alternative interpretationsof the results. First, it is possible that the therapists sawthrough the manipulation and that this in some way influ-enced their responses. This does not seem likely for severalreasons, primarily because there is no reason to suspect thatthe subjects perceived that gender role was the focus of thestudy. Although the subjects were not directly asked then-perceptions of the study's purpose, none of them indicated(during postexperimental discussions) any doubts that theinvestigation was a straightforward examination of counselordiagnosis and decision making. Possibly more important,even if "demand" or social desirability characteristics wereoperating, it is logical to suppose that they would influencethe results in the opposite direction. Thus, this does not seema likely explanation for the results.
A more powerful alternative hypothesis has to do with thetherapists' level of training. Because they were mostly mas-ter's-level counselors, licensed under a state law that allowspersons to practice with 2 years of academic training and 1year of internship, plus an examination, it is possible to arguethat (a) they were not appropriately trained in diagnosis and(b) they did not receive sufficient training in gender issues tocounteract the effects of traditional cultural stereotypes. Withrespect to the first argument, it is important to note that onlysubjects who indicated that they regularly used DSM-III di-agnoses responded to this question. Although this somewhatdiminished the number of responses available for examination(see Table 3), it also ensured that only those knowledgeablein diagnosis were involved in this portion of the analysis. Inaddition, all of the subjects were in private practice and eligibleto receive third-party payments from insurance companies,which payments undoubtedly constituted the majority of theirprofessional income. To receive insurance remuneration, it is(almost inevitably) necessary to assign a diagnosis. Althoughwe have no way of assessing the subjects' diagnostic facility,there is no reason to suspect that they are any more or lesscompetent than any other sample of experienced practition-ers. It seems unlikely that any diagnostic inexperience thatdid exist would interact with the client's gender role behaviorto produce the pattern of results described here.
It does indeed appear likely that this sample lacked appro-priate training in gender role issues, and that is in some waysexactly the point. Clearly these therapists were not sufficientlytrained or aware that gender role reversals neither imply nornecessarily exacerbate psychological problems. Whether theyhad received less training in these issues than their doctoral-level colleagues and whether the same results would be ob-tained with such a sample of doctoral-level psychologists isan open question; it seems prudent at this point not togeneralize these results to this population without further

8 JOHN ROBERTSON AND LOUISE F. FITZGERALD
research. For the present, we suggest that our data haveimplications for counseling psychology training programs, ifnot direct applications.
One final alternative hypothesis about the subjects' focuson the nontraditional client's marital arrangement deservesexamination. It is possible to argue that exactly because theclient's life-style is nontraditional, because society generally isnot supportive of such choices, it is important to explorewhether this may be contributing to the client's distress.Although opinions likely differ on this point, it is relativelyclear that the data do not arise from such considerations.First, the client clearly stated that his marital and occupationalarrangements were not the issue. Second, our subjects werenot exactly exploring the client's life-style. As their responsesto him make explicit, many of them believed he ought tochange it and directly said so (e.g., "You probably need torenegotiate this contract that you've got at home"). Thishypothesis, that therapist attention to the client's nontradi-tional life-style is not a question of values, but rather a reality-based issue, is addressed by Pleck (1987), who pointed outthat "some might interpret the [data] as suggesting that menexperience increased stress because of the ways that they arechanging their role" (p. 20). As he noted, however, the exactopposite appears to be true: "Increased discomfort occursprimarily among the men whose own role (as reflected bytheir family behavior) is not changing. Current research sug-gests that having a nontraditional role . . . is good for men'smental health" (p. 20).
Implications and Suggestions for Researchand Training
As discussed earlier, disapprobation of boys and men whotransgress gender role norms has been widely documentedamong various groups. Our investigation attempted to extendsuch research to the examination of counseling and psycho-therapy. Although our conclusions are limited to master's-level therapists (albeit experienced ones), it is still somewhatstartling to find that a group of experienced mental healthprofessionals are likely to diagnose severe psychopathologyessentially on the basis that a client has chosen not to engagein the good provider role (Bernard, 1981). Such data provideempirical emphasis to statements such as that of Gilbert(1987), who wrote, "therapists who are opposed to or ambi-valent about women pursuing careers, men being involved infamily work, or changes in the traditional sex-role division oflabor are not very likely to be able to work effectively withindividuals in a (nontraditional) family relationship" (p. 288).Although Gilbert was writing specifically about dual-careerrelationships, her remarks are more broadly applicable to allforms of nontraditional families.
If our results can be replicated and generalized, it appearsthat the next step is the examination of the psychologicalmechanisms that support the operation of gender role bias incounseling. A construct that may prove promising here is thatof gender schema (Bern, 1981; Markus, Crane, Bernstein, &Siladi, 1982); these writers have suggested that men andwomen develop an extensive framework of gender-related
associations that serves to organize and influence the mannerin which they process information about themselves andothers. Persons for whom such frameworks are particularlyextensive and salient are said to be gender schematic or topossess well-developed gender schemas. For such personsgender is an extremely relevant organizing concept, one thatinfluences the way in which they respond in a variety ofsituations. Dobbins, Cardy, and Truxillo (1988) were recently,successful in applying this concept to gender bias in perform-ance appraisal; future research in counseling psychology mayfind it a promising variable as well, not only to predict genderrole bias, but possibly to help explain it.
In summary, in this article we attempt to offer an empiricalcontribution to the emerging dialogue about counseling andpsychotherapy with men. Our results suggest that it is essentialfor attention to be paid to the norms and values that operateto keep men, as Goldberg (1976) stated, "in harness" (p. 1),if therapists are to avoid repeating the errors made whenwomen began to enlarge their social and vocational rolesmore than 20 years ago. Although we are not in any waysuggesting that such problems have been eliminated, they areat least now a legitimate focus of discussion, education andtraining, and professional policy. It is our contention, and ourdata support it, that counselors must also be trained in theproblems and possibilities of male gender role transcendence,in a more self-conscious manner than has previously been thecase.
References
Abramowitz, S. I., Abramowitz, C., Jackson, C., & Gomes, B. (1973).The politics of clinical judgment: What nonliberal examiners inferabout women who do not stifle themselves. Journal of Consultingand Clinical Psychology, 41, 385-391.
American Psychiatric Association. (1980). Diagnostic and statisticalmanual of mental disorders (3rd ed.). Washington, DC: Author.
American Psychiatric Association. (1987). Diagnostic and statisticalmanual of mental disorders (Rev. 3rd ed.). Washington, DC: Au-thor.
American Psychological Association Task Force. (1975). Report ofthe task force on sex bias and sex-role stereotyping in psychother-apeutic practice. American Psychologist, 30, 1169-1175.
Bern, S. L. (1978). Bern Sex-Role Inventory: Professional manual.Palo Alto, CA: Consulting Psychologists Press.
Bern, S. L. (1981). Gender schema theory: A cognitive account of sextyping. Psychological Review, 88, 354-364.
Bernard, J. (1981). The good provider role: Its rise and fall. AmericanPsychologist, 36, 1-12.
Betz, N. E., & Fitzgerald, L. F. (1987). The career psychology ofwomen. New York: Academic Press.
Broverman, I. K., Broverman, D. M., Clarkson, F. E., Rosenkrantz,P., & Vogel, S. R. (1970). Sex-role stereotypes and clinical judg-ments of mental health. Journal of Consulting and Clinical Psy-chology, 34, 1-7.
Chesler, P. (1972). Women and madness. Garden City, NY: Double-day.
Costrich, N., Feinstein, J., Kidder, L., Marcek, J., & Pascale, L.(1975). When stereotypes hurt: Three studies of penalties for sex-role reversals. Journal of Experimental Social Psychology, 11, 520-530.
Dobbins, G. H., Cardy, R. L., & Truxillo, D. M. (1988). The effects
EFFECT OF CLIENT GENDER ROLE ON DIAGNOSIS
of purpose of appraisal and individual differences in stereotypes ofwomen on sex differences in performance ratings: A laboratory andfield study. Journal of Applied Psychology, 73, 551-558.
Farrell, M. P., & Rosenberg, S. D. (1981). Men at midlife. Boston:Auburn House.
Fitzgerald, L. F., & Cherpas, C. C. (1985). On the reciprocal relation-ship between gender and occupation: Rethinking the assumptionsconcerning masculine career development. Journal of VocationalBehavior, 27, 109-122.
Fling, S., & Manosevitz, M. (1972). Sex typing in nursery schoolchildren's play interests. Developmental Psychology, 7, 146-152.
Gilbert, L. A. (1987). Women and men together but equal: Issues formen in dual-career marriages. In M. Scher (Ed.), Handbook ofcounseling and psychotherapy with men (pp. 278-294). BeverlyHills, CA: Sage.
Goldberg, H. (1976). The hazards of being male: Surviving the mythof masculine privilege. New York: Signet.
Goodenough, E. W. (1957). Interest in persons as an aspect of sexdifferences in early years. Genetic Psychology Monographs, 55,287-323.
Hill, C. E. (1978). Development of a counselor verbal responsecategory system. Journal of Counseling Psychology, 25, 461-468.
Hill, C. E., Charles, D., & Reed, K. G. (1981). A longitudinal analysisof changes in counseling skills during doctoral training in counsel-ing psychology. Journal of Counseling Psychology, 28, 428-436.
Hill, C. E., Thames, T. B., & Rardin, D. K. (1979). Comparison ofRogers, Perls, and Ellis on the Hill Counselor Verbal ResponseCategory System. Journal of Counseling Psychology, 26, 198-203.
Lansky, L. M. (1967). The family structure also affects the model:Sex-role attitudes in parents of preschool children. Merrill-PalmerQuarterly, 13, 139-150.
Markus, H., Crane, M., Bernstein, S., & Siladi, M. (1982). Self-
schemas and gender. Journal of Personality and Social Psychology,42,38-50.
Morgan, J. I., Skovholt, T. M., & Orr, J. M., Jr. (1979). Careercounseling with men: The shifting focus. In S. G. Weinrach (Ed.),Career counseling: Theoretical and practical perspectives (pp. 260-266). New York: McGraw-Hill.
O'Neil, J. M. (1980). Male sex role conflicts, sexism, and masculinity:Psychological implications for men, women, and the counselingpsychologist. The Counseling Psychologist, 9(2), 61-80.
O'Neil, J. M. (1982). Gender-role conflict and strain in men's lives.In K. Solomon & N. B. Levy (Eds.), Men in transition (pp. 5-44).New York: Plenum.
Pleck, J. (1987). The contemporary man. In M. Scher (Ed.), Hand-book of counseling and psychotherapy with men (pp. 16-27). Bev-erly Hills, CA: Sage.
Pleck, J. H., & Sawyer, J, (1974). Men and masculinity. EnglewoodCliffs, NJ: Prentice-Hall.
Richardson, M. S., & Johnson, M. (1984). Counseling women. In S.Brown & R. Lent (Eds.), Handbook of counseling psychology. NewYork: Wiley.
Silverberg, R. A. (1986). Psychotherapy for men: Transcending themasculine mystique. Springfield, IL: Charles C Thomas.
Skovholt, T. M. (1978). Feminism and men's lives. The CounselingPsychologist, 7(4), 3-10.
Spence, J. T. (1984). Masculinity, femininity and gender-related traits:A conceptual analysis and critique of current research. Progress inExperimental Personality Research, 13, 1-97.
Received December 5, 1988Revision received May 2, 1989
Accepted May 4, 1989 •