Embed Size (px)
Citation preview

PSYCHIATRY AT THE CROSS-ROADS: THE PRESCRIPTION OF MOOD ALTERING DRUGS AND
RELATED ETHICAL OBLIGATIONS
by Natasha Clair Durich
B.A., University of Victoria, 2001
LL.B., University of Victoria, 2005
THESIS SUBMITTED IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE DEGREE OF
MASTER OF ARTS In the School
of Criminology
63 Natasha Clair Durich 2007
SIMON FRASER UNIVERSITY 2007
All rights reserved. This work may not be
reproduced in whole or in part, by photocopy
or other means, without permission of the author.

APPROVAL
Name: Natasha Clair Durich
Degree: Master of Arts (Criminology)
Title of Thesis: Psychiatry at the Cross-Roads: The Prescription of
Mood Altering Drugs and Related Ethical Obligations
Examining Committee: Chair: Margaret A. Jackson, Ph.D.
Date Approved:
Joan Brockman, LL.M.
Senior Supervisor
Professor of Criminology
Jacqueline Faubert, Ph.D.
Supervisor
Adjunct Professor of Criminology
Jessie Horner, LL.M.
External Examiner
Instructor, Criminology
Kwantlen University College

S I M O N FRASER UNIVERSITY L I B R A R Y
Declaration of Partial Copyright Licence The author, whose copyright is declared on the title page of this work, has granted to Simon Fraser University the right to lend this thesis, project or extended essay to users of the Simon Fraser University Library, and to make partial or single copies only for such users or in response to a request from the library of any other university, or other educational institution, on its own behalf or for one of its users.
The author has further granted permission to Simon Fraser University to keep or make a digital copy for use in its circulating collection (currently available to the public at the "Institutional Repository" link of the SFU Library website cwww.lib.sfu.ca> at: chttp:/l[r.lib.sfu.cahandle/l892/11 a) and, without changing the content, to translate the thesisbroject or extended essays, if technically possible, to any medium or format for the purpose of preservation of the digital wwk.
The author has further agreed that permission for multiple copying of this work for scholarly purposes may be granted by either the author or the Dean of Graduate Studies.
It is understood that copying or publication of this work for financial gain shall not be allowed without the author's written permission.
Permission for public performance, or limited permission for private scholarly use, of any multimedia materials forming part of this work, may have been granted by the author. This information may be found on the separately catalogued multimedia material and in the signed Partial Copyright Licence.
While licensing SFU to permit the above uses, the author retains copyright in the thesis, project or extended essays, including the right to change the work for subsequent purposes, including editing and publishing the work in whole a in part, and licensing other parties, as the author may desire.
The original Partial Copyright Licence attesting to these terms, and signed by this author, may be found in the original bound copy of this work, retained in the Simon Fraser University Archive.
Simon Fraser University Library Burnaby, BC, Canada

S I M O N FRASER U N I V E R S I T Y T H I N K I M O O F T H E W O R L D
STATEMENT OF ETHICS APPROVAL
The author, whose name appears on the trtle page of thls work has obtamed, for the researc h described in this work ether
(a)Human research ethics approval from the Simon Fraser University Office of Research Ethics,
(b) Advance approval of the animal care protocol from the University Anlmal Care Committee of Simon Fraser Universw;
or has conducted the research
(c) as a co-investigator, in a research project approved ln advance,
(d) as a member of a course approved in advance for minimal risk human research, by the Office of Research Ethics.
A copy of the approval letter has been filed at the Theses Office of the University Library at the time of submission of this thesis or project.
The orlglnal application for approval and letter of approval are filed wlth the relevant offlces lnquines may be dlrected to those authorities
Bennett Llbrary Slmon Fraser Universrty
Burnaby, BC, Canada

ABSTRACT
Psychiatrists work with potentially harmful mood altering drugs. Wrongful
prescription and conflicts of interest remain as problems despite legal and ethical
remedies. Psychiatrists also work in a context where risk management, the fiction
of the "informed consumer", and questions regarding safety and effectiveness
of pharmaceutical drugs present challenges to the legitimacy and credibility of
the profession. The views of seven psychiatrists are explored, using qualitative
interview methods, on how prescribing impacts "doing psychiatry" and what
ethical obligations are important in prescribing mood drugs. Data analyzed
reveal participant views emerging around active patients, skepticism of the
pharmaceutical industry, and the merits of drug treatment for mood disorders.
Psychiatrists interviewed highlight the importance of an actor's sense of ethical
responsibility and efficacy. However, the willingness and potential to create
dialogue within the profession around ethical prescribing, as well as challenging
the entrenchment of the biomedical model, is largely uncertain.

DEDICATION
For my Grandmother Sarah and my Mother Patty- My first feminist teachers

QUOTATION
In the year 3535 Ain't gonna need to tell the truth, tell no lie
Everything you think, do and say
Is in the pill you took today
Zager and Evans (1969), In the Year 2525

ACKNOWLEDGEMENTS
My supervisor Joan encouraged me to read a book titled Addiction by Prescription. One Woman's Triumph and Fight for Change (2000), by J. E. Gadsby. The book opened
my eyes to the possibility of doing work in this area. I am thankful to Joan and
to Jacqueline for their valuable criticism, insight, and support. To the members of
Criminology 1000: thank-you for your kind words.
I would like to thank the physicians who participated in this study. It is my
hope that I have remained true to the spirit of our discussions.
Last but not least, I have been blessed by the endless love and support of
my partner Lydia, her parents, and my Mother. Thank-you is insufficient.

vii
TABLE OF CONTENTS
APPROVAL.. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ii ABSTRACT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . iii DEDICATION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . iv
QUOTATION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . v
ACKNOWLEDGEMENTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . vi . . TABLE OF CONTENTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .vii
CHAPTER ONE: INTRODUCTION AND LITERATURE REVIEW. . . . . . .1 First Impressions 1
Overview of Study 1
Context of Study 5 Mood Disorders: Some Preliminary Number Crunching 5 ~ a n d ~ D r u ~ W h a t D o e s n ? ~ Y o u W i n M a k e Y m S t r t m p 7 Special Considerations: Gender and Substance Abuse 12
The Psychiatric Profession 13 The Psychiatric Professional and Prescribing Practices 13 The Psychiatric Professional in the Risk Society: The Impact of Risk Management 16 A Managed Form of Professionalism 18
Regulating Prescribing Practices of Psychiatric Professionals 19 Do No Harm: Professional Medical Ethics 20 Government Actions and Regulato y Attempts 24 Righting Wrongs: Legal and Extra-Legal Avenues of Redress for Patients 27
Psychiatry in the 21" Century 28 The Fiction of the "Informed Patient" and Psychiatric Practice 29 Psychiatry Meets the Pharmaceutical Indust y: An Unholy Alliance? 33 A Changing Ethics of Psychiatric Professionalism 37
Speaking Around Drugs, Therapy, & Ethics: Significance of The Study 38
CHAPTER TWO: METHODOLOGICAL CONSIDERATIONS. . . . . . . . .41 The Birth of the Study 41
Mission Questions 41
Data Collection Methods (a) How to best approach the problem (b) Sampling plan, setting, and interviewing

viii
(c) Interview schedule (d) Roles to be assumed
An approach to data analysis Framework Approach Additional Considerations Quality and Value of Research
Ethical Obligations 49
CHAPTER THREE: RESULTS AND DISCUSSION . . . . . . . . . . . . . . .50 Looking Back at the History of Psychiatry: Where are we now? 50
Results 50 Discussion 52
Context Informing Ethical Decision Making Patients as active participants in treatment
Results Discussion
The costs and benefits of using drugs to treat mood disorders Results Discussion
Stigma and medicalizing mood disorders Results Discussion
Other Influences Upon Prescribing Practices Results Discussion
The Pharmaceutical Industry: A Love-Hate Relationship? Results Discussion
Basic Ethics vs. Ethics Plus (+) Preview Results Discussion
The Future of Psychiatry Results Discussion
CHAPTER FOUR: IMPLICATIONS. . . . . . . . . . . . . . . . . . . . . . . . .74
The Re(viewing) the Research Process 74
Re(capturing) Participant Opinions 75

Re(assemb1ing) Insights Patient Characteristics and Drug Treatment Monitoring Patients, Information Keeping, and Aggressive Prescribing The Future of Psychiatry
Farewell Glance 83
Appendix 1: Classes of Antidepressants . . . . . . . . . . . . . . . . . . . . . .84
Appendix 2: Letter of Introduction. . . . . . . . . . . . . . . . . . . . . . . . . .85
Appendix 3: Interview Schedule . . . . . . . . . . . . . . . . . . . . . . . . . . .86
Appendix 4: Conceptual Framework. . . . . . . . . . . . . . . . . . . . . . . . .89
Appendix 5: Framework Method. . . . . . . . . . . . . . . . . . . . . . . . . . .91
Appendix 6: "Doing Psychiatry" (Contextualized) . . . . . . . . . . . . . . . .92
Reference List. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .93

Natasha Durich 1
CHAPTER ONE: INTRODUCTION AND LITERATURE REVIEW
First Impressions
A folded piece of card paper lies before me on the table, resting among a sea of
pamphlets and assorted pens. It looks like a piece of Barbie TM furniture I made
when I was a little girl. Just the right size for a makeshift dinner table. "Take
one-it's origami'; the man in the suit says as he hands me the trinket. I grab it and he gazes back, searching for approval. I look closer and when the object is
flattened, there's a photograph of a young man, smiling, positioned beside the
words Apo-Clozapine (Clozapine). The caption asks you to consider initiating or
switching your patients to Apo-Clozapine. On the other flattened side the online
"risk management program and patient registry" is highlighted, complete with a
screen-shot and the assurance that the company is "fully committed to providing
a reliable, long-term supply of Apo-Clozapine". I walk away from the booth of
Apotex Inc. with a poker face.
This experience I had at the British Columbia Psychopharmacology
Conference (2007) changed my thinking about pharmaceutical companies. I was
aware that these companies provide monies for research and samples, among
other perks, to physicians. I didn't think about the other tools the companies
could provide to physicians. The online risk management system is a means of monitoring patients taking Clozapine, which can cause a serious medical problem
if blood cell counts move beyond the normal range. Is this an example of a
pharmaceutical company making the lives of psychiatrists easier and the world
of patients safer? Is this an instance of a company exerting more control over the
work of physicians and providing a personal shield in case of civil court action?
Can it be both?
Overview of Study
Today's toolkit of psychiatric interventions has expanded to include powerful
drug therapies. In the ever-changing social milieu, psychiatrists negotiate new
challenges to the way they "do psychiatry". The self-regulating profession of
psychiatry has been scrutinized for their relations with the pharmaceutical
industry and the seeming reliance on and promotion of potentially harmful
and unsafe mood altering drugs. Due to this scrutiny, professional legitimacy
and credibility are not guaranteed for psychiatry and for its practitioners. Risk

Natasha Durich 2
management, coupled with micromanaged work, increased access to information
for the "informed patient': and publicized harms caused by drugs to patient
health have unleashed a critique on professional "expertise".
The first objective of my research inquiry is to gain psychiatrist perspectives
on the context in which antidepressant and antianxiety drugs are prescribed.
This includes gathering descriptions on the use of drug-related resources and
information by psychiatrists, interaction with patients as "informed, active"
participants or llconsumers'; and the utility of drug treatments. These reflections
assist us in better understanding how psychiatric practice is shaped by the use of
drug treatment and how "doing psychiatry" is intimately connected with social
factors. Some of those social factors, anticipated from my background reading, are
depicted in a visual map in Appendix 6: "Doing Psychiatry"(contextua1ized). The second objective of my study is to explore and describe the perspectives
of psychiatrists on the ethical obligations that are important in the use of
prescription drugs as treatments for mood disorders. Ethical obligations, in
a medical context, become relevant when they are put into practice and serve
to promote patient health and protect against patient harm. These obligations
can be written in Codes and gleaned from law and policy. However, written
requirements may lose relevance when they ignore the intricacies of a problem or
are not put into practice. The daily actions of psychiatrists not only impact what
treatment for mood disorders means but also what ethical treatment means.
The second objective is framed by turning attention to the problems that
could be, generally, included under the banner of wrongful prescription? The
problems falling under this banner include: failure to monitor for side effects (and
improvements or deterioration), failure to stop medication or change medication
when evidence necessitates, choosing an inappropriate prescription (in dosage
or type of medication), or prescribing a medication that is known to interact
with other medications the patient is taking. The drugs are legally prescribed
but the ways the drugs are prescribed, perhaps along with patient monitoring,
leads to harm. Psychiatrists are not the only physicians who are capable of the
wrongful prescription of mood altering drugs. As noted by Rasmussen (2006,
p.291), research suggests that primary care physicians dispense the majority of all
psychiatric drugs.
My second objective also involves generating discussion with psychiatrists
' Wrongful prescription includes inappropriate prescription, over-medication and over-prescription.

Natasha Durich 3
around the issue of "conflicts of interest" between the pharmaceutical industry
and the psychiatric professional. Schafer (as cited in Brody, 2007, p.34) defines
"conflict of interest" as follows:
A person is in a conflict of interest situation if she is in a relationship with another in which she has an obligation to exercise her judgment in that other's service and, at the same time, she has an interest tending to interfere with the proper exercise of judgment in that relationship.
The pharmaceutical industry contributes monies toward medical research,
drug samples, tools to use in practiceJ2 education and conferences, as well as
other perks such as meals and gifts to physicians (Kassirer, 2005). A reasonable
person might conclude that the relationship between physicians and the
pharmaceutical industry is too close and the influence on patient care is too
great on the part of these businesses. Brody (2007, pp.37-38) suggests that some physicians react with indignation to any suggestion of impropriety, despite the
subtle effects of pharmaceutical company produced advertisements and studies.
Hence, there are two main questions raised by this study. What impact do
these drugs have on the daily practice of psychiatry, according to psychiatrists?
What guidelines or ethical principles do psychiatrists view as important in
treating patients with antidepressants and antianxiety drugs? These questions
have not been sufficiently answered by the research conducted on the topic of
medicating patients. In this thesis, I explore these questions by interviewing
seven psychiatrists and describing my findings, using qualitative methods. This
contextual approach highlights the meanings and experiences of psychiatrists
who treat mood disorders.
The present chapter outlines the important considerations guiding the inquiry. The literature reviewed is engaged in an effort to provide the needed
background insights, scaffolding the questions raised by the thesis. This review
outlines three major areas of concern associated with psychiatrists1 treatment
of mood disorders. First, an overview of mood disorders and mood altering
drugs is provided. This section ends with a brief introduction to some special
considerations: gender and substance abuse and their interaction with the use of
mood altering drugs.
Some of these tools can involve, for example, online monitoring systems, rating scales, diagrams and models.

Natasha Durich 4
Next, the context in which these drugs are prescribed is examined in light
of the changing approach, one that adopts a business-friendly model. Legitimacy
and credibility are essential to the maintenance of power for the psychiatric
profession, a profession given the task of classifying and treating patients with
mental disorders. Psychiatric practice is embedded in a complex social context,
morphing in shape due to the impact of factors associated with the risk society
and the influence of the pharmaceutical industry. Maintenance of power within this social context will be explored.
Third, the issue of regulating psychiatric professionals, and their prescribing
practices, is canvassed, including the special role of self-regulation, medical
ethics, Codes of ethics, case law, and governmental regulatory attempts. Finally,
the specifics of the study at hand are introduced and unique challenges to the
profession in the 21" century are explored.
Chapter Two reflexively discusses the Methodological Considerations. The
place of the researcher in relation to the work (a) in-progress and (b) produced is
highlighted. Reflexivity acknowledges the importance of subjectivity in creating
the study and, later, the re(presentation) of participant views. It becomes integral
that the audience receive sufficient information to judge the trustworthiness of the
work. In Chapter Two, the approach to research, the sampling plan and interview
schedule, along with explanations of the Framework method of data analysis and criteria for evaluation, are outlined. The roles to be assumed and ethical
responsibilities are also noted. Next, the conversations with the seven participants
are explored and described in detail in Chapter Three, the Results and Discussion
section. The Results subsections are meant to provide a description of the views
of participants, while the Discussion subsections provide a deeper level of
interpretation and analy~is .~
Finally, Chapter Four, the Implications section, brings to light some key
reflections gleaned from this qualitative inquiry. In particular, reflections
are presented on the varied, rich discussions around the issues of the active
(informed) patient, the impact of pharmaceutical company involvement, and the
potential utility of drug treatment as a means of treating mood disorders. The
importance of differing ethical concerns and the relationship between social
This distinction reminds me of a song from the animated program The Cat in the Hat (Dr. Seuss, March 10,1971: TV). Karlos K. Krinklebein, the fish, says, "Now to be certain that I have this straight, I'll rerecapitulate". The Results section re-capitulates the views of participants. The Discussion is the re-recapitulation.

Natasha Durich 5
context and ethical action is explored, along with the future directions of the
profession of psychiatry.
This kind of qualitative inquiry serves a number of valuable purposes.
Focusing on how psychiatrists interpret "doing psychiatry1', in relation to
prescribing mood altering drugs, has the potential to open a window into the
world of these professionals, society's experts on mood disorders. Our research
ought to reflect the changes to how we experience our humanity. In these years of
rapid changes in neuroscience and biochemistry, we are faced with the challenges
and promises of the new technologies. In the words of Lewis (2003), "it is not
that medicine is simply wrong or bad, it is more that medicine is too powerful,
too hegemonic, too self-serving, and too unresponsive to alternative points of
view"(p.60).
The insights of psychiatrists are invaluable. For ethicists, the ideas of
psychiatrists are instrumental in shaping our understanding of good prescribing
choices. For the research community, the stories of psychiatrists illuminate the
changing nature of the physician-patient relationship and the matter of how
psychiatrists create their work. For the legal-minded, this inquiry might help
explain the attitudes of psychiatrists when things go wrong.
Context of Study
Mood Disorders: Some Preliminary Number Crunching
It is useful to provide a brief numerical sketch of the problem of mood
disorders in Canada. The intricacies of the statistics cannot be examined here.
Depression and anxiety impact a sizeable portion of the Canadian public. The
Canadian Community Health Survey (2002), conducted by Gravel, Connolly, and
Bedard for Statistics Canada, involved a one-time collection of interview data
from 36,984 persons aged 15 years and older, who lived in private dwelling in
the ten province^.^ Using probability sampling, it was estimated that this group's
data can be used to represent 98% of the population of persons living in private
dwellings in the ten provinces, aged 15 and older. Questions were asked about
mood disorders and substance dependence problems in the twelve months prior
to the interview. Out of 24,996,593 persons in this population, there would be 1,

Natasha Durich 6
195,955 people who meet all the DSM-111 criteria for major depressive epi~ode.~
There would be 239,350 people who meet the criteria for manic episode6 and 375,
973 who meet the criteria for panic di~order.~ These data are simply the result of
translating symptoms into the criteria, based on a single interview and therefore
might not be a true indication of prevalence of depression and anxiety within
the general population. Another indicator measured was life satisfaction. Of the
24,996,593 people in the population, there would be 1,152,720 persons who are
dissatisfied or very dissatisfied with their lives.
The Canadian Community Health Survey (2002) data provides some general
estimates of the overall prevalence of any mood disorder, any anxiety disorder
and substance dependence (alcohol or illicit drugs) in the population described.
In the twelve months prior to the interview, 4.9% of adults (3.8% of the men and
5.9% of the women) aged 15 and over in the population were living with a mood
disorder. In the twelve months prior to the interview, 4.7% of adults (3.6% of the
men and 5.8% of the women) aged 15 and over in the population were living with
an anxiety disorder. In the twelve months prior to the interview, 3.0% of the adults
(4.4% of the men and 1.6% of the women) aged 15 years and over in the population
were living with substance dependence.
The Canadian Community Health Survey (2002) can be useful as a means of
indicating potential needs within the population. Among those surveyed who
reported mental disorders or substance dependencies, 21% reported feeling they
needed help but were not receiving help. In total, 32% of those who reported
mental disorders or substance dependencies received professional help8; 60% of
those persons found the activity to be "a lot useful". From these numbers, one
might speculate that professional help can be deemed useful to a person with a
mental disorder or substance dependency, and a sizeable portion of those persons
with these problems is not receiving help. Coupled with the estimation that over
Defined as at least one episode (2 weeks) with persistent depressed mood, loss of interest or pleasure in normal activities, accompanied by loss of energy, changes in sleep and appetite, impaired concentration and feelings of guilt, hopelessness or suicidal thoughts.
Defined as at least one period (1 week) with exaggerated feelings of wellbeing, energy, confidence or irritable mood during which a person can lose touch with reality. Flight of ideas, racing thoughts, inflated self-esteem, lowered need for sleep, talkativeness and irritability may be present. ' Defined as repeated or unexpected attacks of intense fear and anxiety, followed by one month of persistent concern or worry about having another attack. Usually accompanied by physical manifestations (dizziness, flushing, sweating, palpitations, trembling).
Professional help included a family physician, psychiatrist, medical specialist, nurse or psychologist. Note that social workers are not included as professional helpers in this study. In my view, they play a valuable role in counseling those with mental disorders and addictions.

Natasha Durich 7
1,000,000 persons are dissatisfied or very dissatisfied with their lives, a case can
be made that professional help for mental disorders and substance dependencies
is a growing need. This pool of persons are likely to come into contact with
antianxiety and/or antidepressant medications if they see a psychiatrist as their
health professional of choice.
Antidepressants and Antianxiety Drugs: What Doesn't Kill You Will Make You Stronger
In their classic text The Perspectives of Psychiatry, 2nd ed (1998), McHugh and
Slavney provide a unifying schema for understanding the different orientations
(ways of explaining and treating mental disorder) held by psychiatrists. Four
overarching perspectives (pp. 14-16,289-90) assist in explaining "life under altered
circumstances" (mental disorders):
Life can be altered by what a patient 'has' (diseases), what a patient 'is' (dimensions), what a patient 'does' (behaviours), or what a patient 'encounters' (life stories). (p.17)
The disease perspective involves the use of drug therapies to cure an abnormally
functioning brain. This is but one perspective but many would argue that drug
therapies have become a mainstay in the treatment of depressive and anxiety
disorders. Mood altering drugs are a major focus of modem psychiatric attention.
Given the surges of new drugs on the market, one might be prompted to
ask whether these drugs are making a difference? Van Praag (2003) asked this
question and took "making a difference" to mean altering the suicide rate. Using
World Health Organization statistics for 1980-84, 1985-89, and 1995, he concluded
that "in most countries, the rates of completed suicide seem to be quite stable" (p.184). In particular, he highlights France, Spain, Italy, Germany, Poland, Portugal,
England and Wales, Australia, and the United States. He notes that "[mlany
studies over the past 20 years showed generally modest effect when comparing
placebo and antidepressant drugs" (p.187) and we ought to ask why this might
be the case. Van Praag goes on to provide some speculations (pp. 187-89). The
DSM focuses on symptoms but it is impossible to tell whether an antidepressant
"Making a difference", in the context of this discussion, is focused largely around professional determinations of effectiveness. Patient perceptions of these drugs are likely to be different in some ways, and similar in others. This discussion is beyond the scope of the thesis.

Natasha Durich 8
is preferentially effective in treating a particular symptom. People who are
distressed and worried cannot expect the same results as those with clinical
depression. Furthermore, he argues that monotherapy using drugs might might
be an ineffective therapy for personality disorders, one component of which can
be anxiety and depression, which leads to suicidal behaviour. Residual symptoms
might include maintenance of suicidal thoughts. Finally, SSRIs might influence
auto-aggression but this can be difficult to prove.
Van Praag (2003) encourages a questioning of the capabilities of antidepressant
and antianxiety drugs. These remedies hold promise for the many people
diagnosed with mood disorders. Research behind this treatment is as important
as the treatment itself. How far can these pills go towards helping depressed and
anxious persons move toward life satisfaction? What are the limitations of using
these drugs as a treatment for mood disorders? These are important concerns that
require closer scrutiny.
McHenry (2006) also questions the effectiveness of antidepressants by looking
at the accuracy of the scientific data underlying the presentation of these drugs
to the public. The newest class of antidepressants, the SSRIs, have been presented
to the public as highly effective and safe for the treatment of depression (p.406).
However, the longterm effects of large doses of drugs are not considered. We
also have limited information about the drug trials, especially those that end in
failure or are terminated due to adverse side effects. According to McHenry, the
"industry is marketing the condition and then the lifelong commitment to their
products" (p.407). Control of symptoms becomes the focus, not a true investigation
of the causes of depression (p.406). At one time, benzodiazepines (tranquilizers)
were considered non-addictive; today, that proposition is considered faulty. The
author argues that full disclosure of data, at a minimum, is needed.
It is difficult to accurately describe how effective antidepressant medications
have been in treating patients with depressive disorders. IMS Health Statistics,
an Ottawa-based pharmaceutical tracking agency, provides some numbers as
a reference point?O IMS reports that only 6% of Canadians with depression are
properly diagnosed and treated. It is not clear whether this judgment is based
on a report of being free from depression post-treatment, or whether patients are
judged as being misdiagnosed. Speaking about the Canadian context, IMS Health
Statistics reports that antidepressant prescriptions have increased 64% between
lo www.cbc.ca/news/background/mental-health/depression-mecations.h (October 17,2006)

Nafasha Durich 9
1996 and 2000, with psychotherapeutics being the second most dispensed drug
next to heart disease drugs. Furthermore, Norman (2006, pp.394-95) argues that
although antidepressant medications "remain at the forefront of treatment" there
has been "no quantum leap" seen in treatment effectiveness. He suggests that
it might be inherent in the nature of depressive illness that rapid response to
treatment is unlikely.
As noted by Breggin (1991) and Chetley (1995), mood altering drugs come with
a range of side effects. It has been the aim of psychopharmacology to create better
drugs, with maximum potency for minimum side effects. Some drugs might
be considered extreme experiments, including the use of ketamine. Tucker, in a
Washington Post article (September 26,2006), explains that ketamine is a substance
used as a mild hallucinogen and pet anesthetic. Ketamine works on the electrical
flow between brain cells." Less notorious drugs also raise questions of safety,
including some tranquilizers. For example, in the British Columbia Supreme
Court case of Trueman v. Ripley, [I9981 BCJ 2060 (~ara.20)~ a report provided by Dr.
Rosenbloom, Physician of Pharmacy, evidenced side effects of the tranquilizer
Halcion ranging from memory effects (moving information from short-term
to long-term memory) to loss of control over aggressive impulses. According
to Dr. Rosenbloom, there are at least 58 reported cases of increased hostility or
aggression by users of these drugs. Of these cases, 50% involved physical violence in patients with no prior history of such behaviour.
Sometimes patients agree to take the prescribed drugs but later choose to
abandon the treatment due to experiencing the uncomfortable effects of the
drug. As Penfold and Walker (1983) note, in the physician's office a patient often
does not place her attention "on the impairment of efficiency at work, the dulling
of senses and emotions, the effect on sexual performance, the lack of energy,
and lethargy"(p.188) caused by these drugs. Hence, the impact of the drugs is
felt later, when the patient has been taking the drugs and attempts to resume
regular activities. The full impact of the drugs can come as a surprise, even if the
psychiatrist has briefed the patient. Furthermore, withdrawal can produce equally
difficult symptoms and requires careful monitoring by psychiatrists (Breggin,
1991). The choice of experiencing the painful physiological and psychological
l1 Drugs working on the glutamatergic system are described by Tucker as the wrench-toting plumbers who make house calls; drugs, such as Prozac, that target other systems such as the dopamine and serotonin centres, are more akin to workers who hunt down problems at the water plant.

Natasha Durich 10
changes of withdrawal and continuing to experience the effects of the drugs must
be a difficult decision.
Unfortunately, psychiatrists cannot predict with one hundred percent
certainty which patients will be impacted negatively by antidepressant and
antianxiety drugs. Care in prescribing is vital to a positive outcome for the
patient. Reesal and Lam (2001) comment on the "Principles of Management" and
note that the ideal antidepressant does not exist. An ideal antidepressant would
have rapid onset of action, be effective in short term and longterm treatments,
have a wide therapeutic dose range, show minimum drug-drug interactions, be
safe in overdose, as well as non-addictive, cost-effective and easy to use (p.24S).
Psychiatrists should consider the severity of the episode, patient's age and
ability to comply, suicide risks, history of compliance, tolerance to medications,
presence of comorbid disorders and the use of other medications. According to
Leszcz (2001, p.123), psychiatrists should ask themselves whether prescribing the
medication is (1) a magic that obviates the patient's need to take responsibility,
(2) a means of avoiding the hard work of exploration, and (3) a decision made via
submission and subordination rather than through collaboration. It is not an act of
careful prescribing if these questions are answered in the affirmative.
The ways in which a physician shows concern for the seriousness of drug
treatment can impact a patient's perceptions of the worth of that treatment.
For instance, a physician who shows concern around monitoring treatment is
encouraging patients to take the drugs with caution and to be aware that drug
treatment is not a quick fix for problems. One study that makes this point was
conducted by Barbui, Garattini, and guest Editors (2006). These researchers
argue that qualitative studies suggest that general practitioners are willing to
prescribe drugs without repeated follow-ups (to see if the patient's symptoms
persist). The authors suggest that this behaviour may encourage patients to view
pharmacological means (the "magic bullet") as the only way of getting well. Of
course, this behaviour might be more prevalent among general practitioners,
who are not solely focused on seeing patients with mental disorders. Mann's
(2005) article describes general physician considerations involved in using
drug treatments to manage depression and makes several suggestions for how
physicians can best approach managing these drugs. It is advised that physicians
monitor patients who start drug therapy, assessing progress through interviews
and rating scales, assessing for seven states of response (p.1829). Non-response

Natasha Durich 11
indicates minimal, or less than 25% decrease in the baselineI2 severity of
symptoms. Partial response indicates a response of between 26 and 49% baseline
severity of symptoms. Partial remission indicates that there may be some residual
symptoms, but the patient experiences less than or equal to 50% of initial baseline
symptoms. Remission indicates a return to normal functioning and occurs when
there are no symptoms. While the patient is in remission, they may return to
a fully symptomatic state: relapse. Recovery is the state of extended remission.
An onset of a new depressive episode in a patient who is in recovery is termed
recurrence.
Mann (2005) similarly highlights the uncertainty involved in providing
drugs to treat depression (p.1827). After four to six weeks, treatment is reviewed
and patients with partial response should be reassessed for the diagnosis and
treatment should be "optimized" (higher dosage provided). Alternatively,
inadequate response could mean that a combination of drugs, augmenting
the antidepressant treatment with another drug or hormone treatment, or the
provision of drugs from another class of antidepressants is required. In this
decision-tree, Mann notes that psychotherapy should be considered at any time
and physicians must be alert for special concerns (eg. other illnesses, pregnancy).
This glimpse into physician decision-making shows the inexact science of
providing antidepressants for the treatment of depression. The use of a creative
approach to finding the right fit of treatments for the individual patient is needed.
The biomedical concentration is also apparent, with the focus on the effects of the
brain abnormality and the reduction of symptom severity.
Making sense of side effects and safety concerns can be a time-consuming
venture. Given the rapid evolution of new drugs and public questioning, and
sometimes government restrictions, on available drugs, it has become an
important part of psychiatric practice to remain abreast of new developments in
the pharmaceutical industry. Indeed, instructions can be given to psychiatrists
on how to monitor patients, how best to change medications, and how to keep
informed on drug options. It is more difficult to raise awareness around the
larger issues of drug safety and effectiveness. McHenry (2006) offers the words of
Glenmullen (2005) as a potential means of making sense of how we understand
side effects: it takes 10 years to identify side effects, 20 years to accumulate data to
l2 In this case, "baseline" refers to the initial rating of severity of depression and/or anxiety by the psychiatrist, usually using the aid of standardized rating scales and interviews. The baseline determination occurs before the particular psychiatrist begins a course of treatment.

Natasha Durich 12
make the problem undeniable, and 30 years for agencies to address the problems
caused by those side effects (pp.408-09). This statement is interesting because it
raises the questions of where we are now and whose responsibility it is to become
involved in bettering our drug choices and uses.
Special Considerations: Gender and Substance Abuse
As cited by Copeland (2001, p.9), "a 3:l ratio of women to men exists at every
age group in terms of depressive patients'; which has been attributed to the
help-seeking nature of women, the objective oppression of women, and the
attitudes and behaviours of psychiatrists (p.1). His research raises the question
of whether women are simply diagnosed more often than men, and then
physicians use medication as the first line of treatment regardless of gender.
For a number of reasons, gender is a variable under study when attempting to
understand the regulation of persons labeled as mentally disordered. Dorothy
Smith (1975) argues that psychiatry provides male-generated answers to women-
experienced problems. Psychiatrists, not female patients, have "the privilege
of defining, categorizing, interpreting and assigning value to what they have
said"(p.9).13 Penfold and Walker (1983) have furthered that argument by noting
that psychiatry, along with the rest of the medical profession, has provided "an
even more comprehensive ideology to institutionalize [women's] oppression as an inevitable 'fact of life; and in developing practices that both reflect and enforce
that oppression"(p.243).
How might substance abuse-a comorbid disorder-interact with the
experience of a mood disorder? Mann (2005, p.1829) cautions physicians to be
aware of alcoholism, substance-use disorders and the use of non-psychiatric
medications when making medication changes because these issues can underlie
treatment failures. The World Health Organization report titled Neuroscience of Psychoactive Substance Use and Dependence (2004, pp. 180-183) suggests that there is
a connection between psychoactive substance use and mental i l lne~s?~ The Regier
l3 Smith's 1975 analysis provides one means of approaching this problem. It is important to note that women psychiatrists might be just as likely to medicate. It is possible that today medication is viewed as a first response for both men and women. Further, the category of "women" is broad and needs explication: for instance, how do women of colour, queer women, poor women, role-typical women experience psychiatry? How do categories of oppression overlap? l4 Some of the drugs used to treat depression are also useful in smoking cessation and treating cocaine addiction.

Natasha Durich 13
et al. (1990) study is cited as finding that individuals with an affective disorder are
2.6 times more likely to use psychoactive substances than those without an affective
disorder (p.180). Therefore, there might be something about mental illness-the
physiological workings-that trigger substance abuse, or substances might be
used as self-medication, or simultaneous and complex causal chains might be at
work. Furthermore, it has been suggested that gender differences in emotional
expression in Western culture can impact who is more likely to seek treatment for
mental disorder (Busfield, 1996, p.94). Some people question whether men are more
likely to use alcohol to self-medicate and therefore avoid seeking psychiatric help.
Greenfield and O'Leary (2002, p.473) suggest that a concurrent or lifetime diagnosis
of depression may be correlated with drinking outcomes (p.474).
The Psychiatric Profession
The Psychiatric Professional and Prescribing Practices
Drug treatment decisions in regard to mood disorders made in the office,
within the boundaries of the physician-patient relationship, can mask a
host of related concerns and objectives when viewed as discrete encounters.
The experience of visiting a psychiatrist, discussing a depression and/or
anxiety problem, and being provided with treatment alternatives, including
drug treatment, is not an isolated set of events. This is one level of possible
magnification. Move onto the next level of magnification and one begins to
see an intricate web of social relations, some of which rely on the psychiatrist's
participation as a professional. A magnified view can improve our understanding
of what it means to be a professional, what responsibilities and rewards are
provided to professionals and the changing nature of professionalism. In relation
to the changing nature of professionalism, this section explores the issues of
professional legitimacy, and the emergence of risk management in a shifting
professional context. This section ends with an overview of various means of
regulating the prescribing practices of psychiatric professionals.
What does it mean to be a psychiatric professional? What is a "professional"?
Freidson (1994) suggests that we use the folk concept to answer that question:
how do we accomplish profession and what are the consequences of that
accomplishment (p.25). It is difficult to agree on a set of conditions that define
all professionals. Freidson explains that professional knowledge has a role
in "creating and explaining the officially accepted 'facts' about the social and

Natasha Durich 14
physical world that form our consciousness" (p.44). Although professionals do not
have absolute power, they have formal administrative devices, associations with
links to the state, and specialized knowledge that is given privileged status, all
of which help secure a certain measure of power in organizing social relations
(pp.34-35).
What then is the work of psychiatric professionals? From Busfield's (1996)
viewpoint, psychiatrists participate in the social construction of "mental
disorder1', a construction that varies across time and place. All members of society
participate in the construction when they think about a "mentally disordered
person" and interact with people so labeled (pp.53-60). For Castel, Castel, and
Love11 (1982, p.308), psychiatric professionals treat those people they classify
as being mentally disordered, using various psychiatric interventions which
function as a whole but shift in essence over time and place. Their ideas about
mental disorder are shaped by the world around them and the historical body of
knowledge supporting psychiatry as a discipline.
How might psychiatrists describe the work they do and the people they counsel? Morantls work (2006) involved interviewing sixty mental health
professionals, in London and Paris, including 11 psychiatrists.15 He notes that
psychiatrists are "key players in the network of social constructive processes
through which contemporary social representations of mental illness evolve"
(p.819). They work to bring together the expert and lay bodies of knowledge about
mental illness from policy makers, academic researchers, lay persons, and the
media (p.819). Morant argues that his interviews show that "professionals view
their overall aim as attempting to enhance the quality of people's lives" (pp.827-
28). His participants shared the idea that mental illness is a state of exaggeration
from normal conditions and the belief that the mentally ill are not dangerous or
worthy of rejection (p.833). The theories brought into practice by practitioners
interviewed formed an important part but not the whole part of their information
base when dealing with clients. Professional commonsense was important as well.
Yet, the views of psychiatrists are by no means uniform. Psychiatrists work
toward persuading other psychiatric professionals of their views, thereby
bolstering confidence in the common work that is conducted. Atkinson (1994)
argues that in our oral and literate culture, "medical work is constantly produced
l5 Morant's work did not query how psychiatrists who have mental disorders view mental illness and their work as psychiatrists, which would provide an interesting perspective.

Natasha Durich 15
and reproduced through narrative and other language skills" and that work
"resides in written and spoken rhetorical formats" (p.115). Conversations between
colleagues, the translation of evidence into accounts, writing up cases, and
producing texts including patient charts are all incidences when rhetorical impact
is key (p.114).
Still, psychiatrists are afforded the power to speak as authorities on mental
disorder. Besides sharing common narratives, language and rhetorics, the keeping
of psychiatrists' status has been aided by the ideology of professionalism and
legitimation within the medical establishment. This ideology, Freidson (1975)
argues, is supported by three main propositions asserted by physicians or medical
experts: (1) medical knowledge is complex, detailed and difficult, (2) objective
science underlies medical practice, and (3) physicians will place the welfare of
others above their own (as summarized by Clarke, 2000, p.270). Veatch (1990) puts
it this way: a core presumption in modern medicine is that "there is a medically
best course of action for a given patient in a given situation" and good clinical
skills assist in determining that course of action (p.25). Medical professionalism
and legitimacy are also bolstered for psychiatrists when their patients trust their
decisions (Misztal, 1996, pp.131-33). Misztal argues that patients trust that the
physician is knowledgeable, especially if there have been prior visits, and in a
way this trust serves to obviate the need for a patient to learn about medicine.
Misztal suggests that the reputation of a professional is a complex social opinion
and rests on a code of ethics (values), formal control (discipline), and conformity
to social pressure (p.127). Childress and Siegler (1984, p.139) similarly argue that
one purpose of codes of medical ethics is the fostering of trust by showing where
medical professionals stand and creating a climate of trust. It is possible for "[p]
atients to approach physicians with some trust and confidence in the medical
profession, even though they do not know the physicians before them" (p.139).
The impressions that patients build of psychiatrists and the psychiatric
profession are managed, to a degree, by the actions of psychiatrists.
Professionalism-and professional authority-requires that patients trust in
psychiatrist credibility. Veatch (1990) notes that physicians can persuade in subtle
ways, including tone of voice, phrasing and facial expression (p.37). The rhetorical
capabilities of professionals are also captured by deswaan's (1990, cited in Pilgrim
& Rogers, 2005, p.2549) notion of "protoprofessionalization". The professional
duplicates, to a degree, her learned ideas about a problem by translating them in
a persuasive fashion for a non-professional audience. In this case, psychiatrists re-

Na tasha Durich 16
socialize the public to accept a professional conception of mental health problems.
The matter of persuasion is particularly significant for psychiatrists because their
knowledge resources might be too contested to maintain scientific credibility or
moral authority (Pilgrim & Rogers, 2005, p.2555).
The maintenance of professional legitimacy entails the interplay of ideologies,
actions and a faith in established ethics and regulations. However, scientific
credibility, legitimacy, trustworthiness and professionalism are not static states
but shift along with the position of the profession within a changing society. One
such change involves the increasing focus on risk assessment and management.
The Psychiatric Professional in the Risk Society:
The Impact of Risk Management
As argued above, when the profession is seen as being trustworthy, as providing
credible information, and as serving the diverse needs of the public, then the power
of the profession is more secure. When the profession's ability to deliver on these
promises is questioned, so too is the place of the profession as expert guardians of
knowledge and skill, and for psychiatrists as those who hold the shared monopoly
on mental health care. Societal and professional change can lead to this questioning
of psychiatric expertise. It is worthwhile to explore the impact of some of these changes on the workings of the psychiatric profession.
Kirk and Kutchins (1992) argue that the 1960s and 1970s saw a shift in
psychiatric thinking away from theoretically rich psychoanalytic methods to
ones that moved psychiatry closer to mainstream medical diagnostic methods.
The structured interview helped to limit variance among different psychiatrists
when making a clinical judgment (pp.47-53). The introduction of the Diagnostic
Statistics Manual 111 would further increase validity and reliability by creating
discrete classifications for differing mental illnesses (p.50; pp.116-119). The focus of
attention is not on patient wellness, but on classification of mental disorder so that
a treatment can be provided. Kirk and Kutchins conclude by noting that clinical
judgment will always involve some ambiguity (pp. 229-230). For instance, the
professional will always have some measure of discretion, choosing between client
needs and organizational needs, and the purpose to which the discretion is used.16
Holmes and Warelow (1999) offer a different reading of the current edition
l6 Some purposes include protecting the client from harm, directing the client to various systems, gaining fiscal resources, advancing political goods, and rational decision-making.

Natasha Durich 17
of the DSM-IV7. They see the DSMin terms of risk management. Psychiatrists
provide diagnoses for "disorders", implying a mechanistic view of the body
(p.168). The manual provides "unlimited expansionism" (p.176) into the realm
of classification of behaviour as mental disorder and there is no recognition
of coexisting alternative interpretations of the behaviour (p.171). The manual,
according to Holmes and Warelow, provides the vehicle for psychiatrists to
assess the risk posed by the patient's behaviour and ascribe "mental disorder" where that risk is unacceptable (p.175). Risk is presented as absolute and focus
turns to risk management and the level of acceptable risk, again not on meeting a
definition of wellness.
Scientific credibility is increasingly difficult to muster for psychiatrists due
to these changes in professional thinking, characteristic of the "risk society". For
Ulrich Beck (1994), risk society is a term used to describe a society that focuses on
avoiding unsafe behaviours and states of being. Because danger is a "cognitive
and social construct" (p.6), there is conflict over what is safe and unsafe (p.11).
In the risk society, people challenge authority because the idea of authority is
questionable. The very notions of "safety" and of risk are social constructs and
people are more willing to doubt authority.
How to deal with the various "bads'; including harms from mega
technologies, genetic research, threats to the environment and overmilitarization
(p.6), is a contentious issue. Beck (1994) suggests that cooperation among
individuals, institutions and the state is necessary (p.29-30), lest institutions
become "zombie institutions which have been clinically dead for a long time
but are unable to die" (p.40).18 According to Beck, the state changes through
the process of "withering away plus inventing" (p.38). Psychiatry runs the risk
of becoming a "zombie institution", if Beck's ideas are plausible. Challenges to
credibility in the "risk society" are part of the process of challenging values.
Denney (2005) notes that professionals are facing serious challenges in a society
where ideas of risk and risk assessment are commonplace. The client is more
aware of the option of litigation and aware of the potential risks when consulting
a professional. Information is more accessible for clients and they make demands
I7 The DSM IV was published in 1994 and an update published in 2000 (DSM-IV-TR). A new version of this "gold standard clinician's resource is scheduled for release in 2011 (see www.dsm5.org). This manual is not without its critics, a topic too great to discuss in detail here. l8 For example, government agencies fulfilling a mandate that is already being covered by another group.

Natasha Durich 18
on professionals to justify and explain their actions. Clients are less trusting in
the risk society. The government and managers demand that professionals justify
and explain their actions. Therefore, Denney surmises that professionals are
engaged in a "managed form of professionalism"(p.74). In short, it is "difficult for
professionals to present themselves as the guardians of expert knowledge"(p.80)
when the public is more willing to question professionals and demand
justifications for action.
A Managed Form of Professionalism
Management over the work of professionals is a key change in the work of
psychiatrists. As noted, clients have a greater understanding of risks, through
the proliferation of knowledge and the expansion of litigation; the government
provides more layers of organizational managers; the professionals are pressured to justify and explain their actions (Denney, 2005). The management of persons
with mental disorders within the community has created changes to the client
characteristics of persons who are treated in private practice. In other words,
the independence of psychiatrist decision-making is being questioned. A brief
introduction to the problems associated with professional management follows.
Medical professionals, including psychiatrists, have the power of self-
regulation. Brockman (1998) comments that self-regulation involves a quasi-public
body taking on government regulatory functions, including the prevention of
misconduct and reduction or prevention of incompetence, thereby controlling
quality of service (p.588). Four major intertwined areas of regulation are: (1) entry
requirements, (2) demarcation through licensure, certification and definition of
scope of practice, (3) regulation of process through dealing with competition,
monitoring professionals, and providing continuing education, and (4) corrective
disciplinary system (pp.588-590).
Brockman (1998) also argues that the four areas of regulation have "benefits
to, and drawbacks for, the public" (p.590). Self-regulation is a source of power for
professions. The rationalization is provided that some kind of monopoly over
services is needed so that the organization can "operate effectively to control
incompetence and misconduct"(p.593). As noted by Brockman (p.598), licensing or
certification does not "guarantee[ ] quality of service within the restrictive system"
nor does it guarantee information exchange about services outside the system.
This can be of extreme importance in the medical context, where negligent actions
by a physician could cost a patient her life. Furthermore, Brockman (p.595) states

Natasha Durich 19
that "[p]rofessional socialization, and the resulting professional culture, reinforce
the expertise of the professional and the ignorance and dependency of the
consumer". The divide between lay and expert knowledge might be increasingly
untenable in a world where the consumer has the potential to be more informed.
From a broader historical perspective, it can be argued that patriarchal
ideologies and capitalist interests have played crucial roles in how power within
the medical profession is negotiated. As noted by Witz (1992), women were more
successful in using legislative means as a way to gain entrance into the medical
profession, whereas men could use legislative means as well as credentialism to
secure state sponsorship of male professional projects (p.196). It has been argued
that this power to self-regulate severely limits society's power to control the
deviant behaviour of physicians.
Management from within, in terms of setting entry standards, education
requirements, licensing, and discipline, are also taken as means of securing
psychiatric control over its own work. This form of management is akin to
Freidson's(l994) analytic model for understanding the control of professionals.
Under the analytic model, professionals would have full control over recruitment,
training, work performance and the application of knowledge (pp.67-68): the
occupational principle of organization. The gains in intellectual freedom under
this model come with the complementary obligations to be trustworthy, collegial,
and on guard for possible abuses of power (pp.173-75).
Regulating Prescribing Practices of Psychiatric Professionals
As a means of examining regulatory attempts on psychiatrist prescription of
mood altering drugs, as well as the regulation of the drugs themselves, this
section explores various legal (codes, statues, and case-law) and extra-legal
means of regulation. Ultimately, these regulatory attempts also contribute to the
maintenance of professional legitimacy and credibility.

Natasha Durich 20
Do No Harm: Professional Medical Ethics
On a global scale, medical professionals have turned their attention to the
importance of adhering to a high standard of patient care. The World Psychiatric
Association's Madrid Declaration on Ethical Standards (1996) confirms the right of
patients to be treated as partners by the psychiatrist in the therapeutic process
(#3).19 Furthermore, as an additional guideline (#2) for dealing with conflicts of
interest, the Association insists that psychiatrists must guard against accepting
gifts that could have undue influence on work, disclose financial and contractual
obligations to review boards and research subjects, and gain fully informed
consent from research subjects in drug trials. This Declaration follows the United
Nations adoption of Resolution 46/119 on December 17,1991: Principlesfor the
Protection of Persons with Mental Illness and the Improvement of Mental Health Care.20 Principle 8(2), Standards of Care, cautions that "Every patient should be protected
from harm, including unjustified medication, abuse by other patients, staff or
others or other acts causing mental distress or physical discomfort." The problem
with these sources of guidance is the lack of enforcement in psychiatric practice.
Canadian medical practitioners have multiple sources of ethical guidance.
The College of Physicians and Surgeons is responsible for licensing, ensuring that
standards of practice are met, and establishing those standards. Section 3 of the
Medical Practitioners Act, RSBC 1995, Ch.285, expands on two important duties of
the College:
(d) to establish, monitor and enforce standards of practice to enhance the quality of practice and reduce incompetence, impaired or unethical practice amongst members.. . (g) to establish, monitor and enforce standards of professional ethics amongst members.
The Canadian Medical Association is a voluntary national advocacy association
for physicians and medical students. They have produced a Code of Ethics, which
is the major source of ethical guidance for Canadian physicians. Furthermore, the
Canadian Psychiatric Association, another voluntary association, has produced
clinical guidelines in an effort to encourage the highest standards of professional
practice.

Natasha Durich 2 1
Conflicts of interest between members of the pharmaceutical industry and
physicians have been the topic of regulation in Canada. The Royal College
of Physicians and Surgeons of Canada has produced a Conflicts of Interest
publicationI2l which states:
The best way to manage such conflicts is to either eliminate the conflict or, alternatively, acknowledge that it exists and identify strategies for minimizing the potential effects on medical decision-making.
Physicians are directed to the CMA Code of Ethics and are warned to "be vigilant
in discerning the difference between education and marketing." Likewise,
the College of Physicians and Surgeons of British Columbia, in their Resource
Man~a1,2~ cautions that such conflicts "can occur where a professional or business
arrangement affords a member the opportunity to receive a personal benefit".
Physicians in British Columbia are cautioned to avoid such situations or seek
College direction and/or approval. Alberta physicians are directed by their
College to the relevant CMA Code of Ethics sections, including (1) place the
wellbeing of patients first, (2) do not exploit patients but treat them with respect,
(23) recommend what is beneficial, (49) conduct is open to peer review, and (50)
avoid promotion of treatments for personal gain.23
Ethical considerations around prescribing medications are also included in
some guidelines and policies of the various Colleges of Physicians and Surgeons.
British Columbia, Nova Scotia," Newfoundland, New Brunswick, and Ontario
have various guidelines and policies in place warning against prescribing based
solely on faxed or mailed information (countersigning). Ontario provides the
most clear guideline in Policy #2-05 (May/June 2005).25 Physicians are cautioned
to have a full understanding of the patient's health status prior to prescribing
drugs. The prescription must be done with care and within the scope of their
responsibilities, acknowledging that level of care varies (episodic or well-known
21 See Physicians and industry - conflicts of interest, retrieved from http://rcpsc.medical.org/ publications/index.php 22 See Conflicts of interest, retrieved from https://www.cpsbc.ca/cps/physician~resources/ publications/resource~manual/conflictofinterest 23 See Conflict of interest, retrieved from http://www.cpsa.ab.ca/publicationsreso~~ policies/Conflic t%20oPh20Interest .pdf 24 See Policy regarding prescribing practices/ countersigning prescriptions/ internet prescribing and notice to non-resident physicians concerning cross-border prescribing, retrieved from http://www.cpsns.ns.ca/ publications/polic y-internet-prescribing " See Presoibing practices (Policy #2-05) retrieved from http://www.cpso.on.ca/poliaes/drug_prac.htm

Natasha Durich
patient, minor problem or complex issues). The Resource Manualz6 for British
Columbia's physicians states that there is an obligation to arrange follow-ups and
a responsibility to advise on drug effects, interactions and precautions. Ontario,
in Policy #1-03 (May/June 2003)," and New Brunswick, in a c~mmentary,~~ direct
physicians to alert patients early and fully of any adverse effects. Once again,
Ontario provides a clear statement that harms are "unexpected or normally
avoidable outcome[s] that negatively affects the patient's health and/or quality
of life" and it is part of the fiduciary duty and respect for patient autonomy to
acknowledge such harms and arrange for follow-up care.
The psychiatric profession has the serious responsibility of monitoring the
activity of members and disciplining those who act below the standards set for
psychiatrists. Freidson (2001) considers the place of ethical codes and concludes
that it is important that professional institutions support the professionals by
undertaking "the vigorous investigation of violations and whatever corrective
action is finally deemed appropriate" (p.216). Some violations cannot be easily
placed into codes because they represent violations of trust (p.216). Some
problems are subtle, including showing a lack of respect for the patient, providing
acceptable care but not the best care (when it is possible), and being dismissive
of the patient's desires are difficult to place into Codes or policies and, more
importantly, to monitor.
Furthermore, Freidson (2001) notes that some problems deal with "the
economic, political, social, and ideological circumstances that create many of
the moral problems of work": the institutional ethics (p.216). Codes and policies
that target the activity of individual psychiatrists are needed, but so are larger
solutions that work toward setting-up a work environment that supports good
decision-making and quality patient care. This is not to say that negligent
behavior can be excused for psychiatrists who are struggling with the realities of
modern practice. However, it does point to the fact that ethical practice cannot be
divorced from the social setting in which the actors are embedded.
Psychiatrists are also held to legal standards of conduct, created through
Canadian common law. Harm and causation are key issues in these negligence
26 See Prescribing practices, countersigning prescriptions and internet prescribing, retrieved from https:// www.cpsbc.ca/cps/physician_resources/pubEcations/~so~ce~mnud/presaibhgprac
See Disclosure of Harm (Policy #I-03), retrieved from http:~www.cpso.on.ca/pEcies/discl~~mhhn 28 See Selected Commentaries, Reporting of adverse events, retrieved from http://www.cpsnb.org/english/ Selectedo/020Commentaries/Reporthgo/020oP/02OAdv~seo/02OEvent~.htd

Natasha Durich 23
cases. For instance, Judge Cheverie in the PEI Supreme Court case of Harris v. Beck
Estate, [2007] PEJJ No.11, found against the patient and stated "The question is
whether by the application of those drugs there was a real risk Harris would wind
up in the state which he described (para. 45). Harris, who would accompany
his wife to her appointments, was offered treatment by the psychiatrist. Harris
claimed the medications were unrequested and they caused him to lose contact
with reality. The judge found the evidence provided by Harris to be weak, stating
that the psychiatrist met the standard of care required of psychiatrists at the time
in Prince Edward Island. Further, Harris showed a willingness to take the drugs
by discussing medication changes with the psychiatrist.
Psychiatrists are not expected to achieve perfection. Psychiatrists must disclose
material risks and special or unique risks that a reasonable person in the patient's
situation would want to know (para.41, citing Reibl v. Hughes (1980) and Hopp v. Lepp (1980), Supreme Court of Canada). When a breach of conduct is argued by
the patient, the psychiatrist has an opportunity to justify his actions. To illustrate,
Justice Lang of the Ontario Superior Court of Justice, in the Gallacher v. Jameson
Estate, [2002] OJ No. 2699 case, notes that once the court draws an inference that
harm has been caused by physician negligence, it is up to the physician to lead
evidence to the contrary (para. 15, citing Snell v. Farrell(1990), Supreme Court
of Canada). The patient was unable to prove that but for the prescription of the
antidepressant Anafranil, he would not have had an affair, separated from his
wife, or quit his good job in favour of a risky business venture. It was likely,
according to the judge, that a midlife crisis and subsequent selective memory are
responsible for the account.
Amidst these sources of ethical guidance, the problems with prescribing
medications and drug safety remain. The Atlantic Provinces Medical Peer Review
Programz9 has assessed more than 1200 physicians since 1993. After the first two
years, psychiatrists were added to physicians who could be randomly called for
an in-office review. Some physicians are reviewed off-site. The most common
deficiencies, regardless of practice type or region, are: lack of recording for repeat
prescriptions, outdated drug supplies and samples, lack of allergy flagging,
insufficient documentation in the patient record, and insufficient recording of
prescriptions. It is easy to see how these problems are connected to poor patient
outcomes and adverse drug experiences.

Natasha Durich 24
Government Actions and Regulatory Attempts
Going to the psychiatrist and starting a mood altering medication should not
be a game of Russian roulette. How secure can patients, and psychiatrists, be of
the safety of mood altering drugs in the Canadian setting? Another means of
regulating prescribing practices comes in the form of government regulations
and initiatives. In the Royal College of Physicians and Surgeons submission to the
House of Commons Standing Committee on Health (November 6, 2003),30 it was
stated that post marketing surveillance of drugs is lacking in Canada. It is largely
the responsibility of health care practitioners to record adverse effects, a poor
replacement for a final stage of monitoring. The Canadian government, under the
Food and Drug Regulations, CRC, c.870, C.01.016, requires manufacturers to report
serious adverse drug reactions (including unexpected ones) and provide a concise,
critical analysis of the adverse drug reactions and serious drug reactions on an
annual basis. The government may request from the manufacturer case reports
and a summary report of the drug reactions known to the manufacturer. The
Marketed Health Products Directorate31 assists in the post-market surveillance
of drugs and medical products, aiming to improve Health Canada's ability to
identify drug safety risks and improve response time.
Not only physicians and manufacturers, but also consumers are urged
to report adverse drug effects. The MedEffect online database is a place for
consumers to report adverse reactions and read about warnings for various
medications and medical products.32 As noted on this site, "new or 'unexpected'
side effects" sometimes occur when a product is introduced into the market,
exposed to "real world" conditions. These are "adverse reactions" that have not
been identified in the pre-market testing. Products on the market, according to
this site, have side effects ("expected" and lltolerable") that are outweighed by
the benefits of the product. On October lst, 2007, Health Canada announced that
the adverse effects monitoring program, operating under MedEffect, would be
renamed Canada Vigilan~e.~~ This technological fix for the problem of product
safety, which rests on consumer "vigilance" for monitoring risk, seems to be an
" See Prescription Drugs in Canada: Presentation to House of Commons Standing Committee on Health, retrieved from http://rcpsc.medical.org/publicpolicy/archives-e.php 31 h t t p : / / w w w . h c - s c . g c . c a / a h c - a s c / b r a n c h - 1 32 http://~~~.h~-~~.g~.~a/dhp-mps/medeff/index~e.html 33 h t t p : / w w w . h c - s c . g c . c a / a h c - a s c / b r a n c h - d c annonce-e.html

Natasha Durich 25
"end-of-the-pipe" solution. Longer trial periods for the testing of drugs, under
"real world" conditions would be another means of examining adverse side
effects, without further jeopardizing the health of consumers who are depending
on the medication to improve their condition.
The Health Products and Foods Branch, within Health Canada, is overseeing
the implementation of a project whereby decisions about new drugs and products
will be made The Summary Basis of Decision for novel drug therapies
(New Active Substances) and a subset of Class IV medical devices are public (for
applications for products made after January kt, 2005). The website states:
A Summary Basis of Decision is a document that outlines the scientific and benefit/risk based decisions that factor into Health Canada's decision to grant market authorization for a drug or medical device. The document includes regulatory, safety, efficacy and quality (chemistry and manufacturing) considerations.
Therapeutic product applications and information about those products produced
prior to January lst, 2005 will not be included in this system: one must use the
proper Access to Information protocol to gain that kind of information. There is
no post-market information included, as these decisions are intended to provide
additional information on risks and benefits of the products.
Researchers have also questioned what consequences government-issued
warnings about antidepressants have on prescribing rates. Kurdyak, Juurlink,
and Mamdani (2007) conducted a time series analysis of Ontario computerized
prescription records, for the period of April 1998 through March 2005. During this
time span, five high profile warnings were issued, as follows:
1. June 10,2003: UK warns against the use of paroxetine for patients
under the age of 18;
2. October 27,2003: US FDA warns to use newer antidepressants with
caution for young patients;
3. October 15,2004: US Black Box warning, stating the threat of
suicidal ideation and behaviour in children and adolescents with all
antidepressants;
4. March 22,2004: US FDA warns to closely monitor all patients after the

Natasha Durich 26
initiation of antidepressants or changes to this medication; and,
5. June 3,2004: Health Canada issues a similar advisory as (4).
The UK warning had the effect of decreasing paroxetine prescriptions for younger
patients. The North American warnings showed no impact on any age group. The
researchers speculate that the specific target group and the specific instructions
had an impact, as well as the fact that the UK warning was the first of its kind
(p.754).
The Ontario study represents a statistical examination of trends to try to
produce an explanation for prescribing behaviour. One might ask whether there
is any data that asks physicians to explain their responses to such warnings.
Researchers at the Mayo Clinic conducted an electronic survey (November 2005-
January 2006), which included 24% of available physicians working at the Clinic
at Rochester, Minnesota (Lineberry, 2007), to determine the impact of the October
2004 Black Box warning on physician behaviour. Of the 37 psychiatrists surveyed,
41Y0 made no change in practice; 19% spent more time explaining treatment; 16%
spent more time explaining rationale for treatment; and 11% would see patients
more often for follow-up. The survey was sparked by a concern that over 2 years,
the number of prescriptions filled for antidepressants for children and adolescents
had gone down by 20% in the United States. Similar to the Ontario study,
Lineberry reported a lack of changes in physician prescribing behaviour, which
seems to support the idea that warnings can have little influence on psychiatrist
behaviour.
Physicians, including psychiatrists, are exposed to various warnings
about drug safety and have been encouraged to report any observed adverse drug effects. In terms of in-practice government supports, what is available
to help psychiatrists ensure the safe prescription of mood altering drugs? In
British Columbia, the Ministry of Health has offered an online database called
PharmaNet, since 1995. This tool provides access to patient medication histories
for pharmacists, the College of Pharmacists of British Columbia, the College of
Physicians and Surgeons of British Columbia, and British Columbia physicians. If
a physician wishes to have access to this tool, she must pay a license fee. Patients
can also obtain access to their own medical information. Once accessed by the
medical professional, the information follows the same rules of confidentiality as other medical information. The stated objectives of this program are to prevent
the over consumption of prescription drugs (duplication or fraud), to prevent

Natasha Durich 27
inappropriate therapies (drug interactions), to improve practice standards, to
promote cost effective prescribing, and to streamline claims.35 The fraudulent
obtainment of narcotics has been a serious problem and this database is one
means of curbing this form of abuse. It is an open question whether this database
is proving a useful tool for physicians as a means of assisting in prescribing
medication.
Maynard and Bloor (2003) write from an international perspective about
regulatory interventions aimed at practitioners. They are skeptical of the
effectiveness of such actions and claim "in rare cases where the guidelines affect
clinical practice, there may be a risk of increasing inefficiency by distorting overall
priorities" (p.36). The best interests of the patient and society may be undermined
by problems such as the proliferation of drugs, a refusal to use generic equivalents
and off patent therapies. In France, Germany and the UK, governments have
backed the use of best practice guidelines and three main conclusions can be
drawn about such experiments, according to Maynard and Bloor (p.36). First,
physicians by-and-large were not aware of the regime and found it complicated
to administer. Second, newer and more costly alternatives were used when there
was a list of banned drugs. Third, when it came to antidepressants, pharmacists
were displeased with its impact on choice of drug. These lessons should be taken
into consideration when developing policy alternatives.
Righting Wrongs: Legal and Extra-Legal Avenues of Redress for Patients
There are various possibilities open to remedy the problem of over-medication
and wrongful prescription. Governmental regulation of drug companies is one
possible response (Lexchin, 1990), although the problem of extra-territoriality
is a major stumbling block (Kleefeld & Srivastava, 2005, pp.495-497). Internal
regulation, in terms of guidelines for physicians, is another means of regulation.
New Zealand has a no-fault compensation scheme, which has permitted an open
dialogue with the medical profession regarding standard-setting and patient
rights. However, the system offers minimal remuneration, denies compensation
for the ordinary consequences of treatment and rarely opens the avenue of human
rights litigation (Bismark & Patterson, 2006; Manning, 2004).
Court battles can be waged in the arenas of civil law (mainly negligence)

Natasha Durich 28
or criminal law; yet, these legal means are rarely used, and when used the
plaintiff patient is rarely successful (Jones, 1999, p.121; Cebuliak, 1995; Kaiser,
2002; Liederbach, J., Cullen, F., Sundt, J., & Geis, G., 2001). In the cases of Gadsby
v. MacGillivray, Kroll v. Valiance, and Trueman v. Ripley, the plaintiff patients
were unsuccessful in their claims of negligence against their psychiatrists, for
prescribing various mood altering drugs. The unsuccessful patient in Stewart v. Barry, was told by Judge Morin that the antidepressant was "state of the art" and
acceptable to be given at the upper limit of its dosage (para. 170). In that case,
the patient was switched from one tricyclic to another and claimed to undergo a
period of mania, during which he stole from his client's trust funds. The physician
must be found to be wrong in his prescribing, and he was not, and the injuries
must be proven, which they were not in this case.
Compensation through the judicial system appears to be difficult for patients
to access, possibly due to hurdles in proving harm and causation. Non-legal
responses are aimed at changing the behaviour of those diagnosed with mental
disorder and/or the behaviour of the psychiatrists. The radical notion of anti- psychiatry focuses on removing the label of "mental disorder" and giving people
the opportunity to resolve their problems without medical intervention (Laing,
1985; Burstow, 2005). One major problem with anti-psychiatry, as noted by Ussher
(2005), is its failure to "reconcile a deconstructive critique at the macro-level with
the needs of individuals at a micro-level"(p.31). In other words, how to respond
to the people who feel "ill"? Another set of responses is aimed at the profession
itself: building a feminist psychiatry (Ussher, 2005) or improving the work of
psychiatrists. Change from within requires a sensitive approach, meaning one
that is capable of generating workable solutions for psychiatrists and patients
alike, in terms of practical ethics around the use of psychiatric medication.
Psychiatry in the 21"' Century
In sum, psychiatric professionals are working in a changing context. The
focus on risk management, coupled with a managed form of practice, forces a
spotlight to shine on their performance. Among the watchful eyes are patients,
who have been described as being "informed" participants in the clinical
encounter. The objectivity of psychiatry as a science and the trustworthiness of
psychiatric professionals also come under scrutiny, in part due to the exposure
of conflicts of interest between pharmaceutical companies and psychiatrists. The
pharmaceutical companies manufacture antidepressant and antianxiety drugs

Natasha Durich 29
that have potentially serious, even life-threatening, consequences for users' health.
These drugs are marketed to the general public and to psychiatric professionals
as positive tools for the treatment of mood disorders. The increased scrutiny over
psychiatric work, coupled with its management, raises questions over the ethics
of professionalism for psychiatrists. How does control over one's work impact the
ability to do one's best work as a medical professional? This section aims to provide
a more in-depth review of these issues facing psychiatry in the 21" century.
The Fiction of the "Informed Patient" and Psychiatric Practice
The growth of the internet and direct-to-consumer advertising has impacted our
perception of patient knowledge. The passive patient can now be conceptualized as
an informed consumer of medical treatment. This language has a key place in the
"risk society" because the public is taken as being responsible for monitoring their
risks and addressing them. Henwood, Wyatt, Hart, and Smith (2003, p.604) describe
the "informed patient" by using an ideal type:
Patients take it upon themselves to become informed about their own health conditions and the treatment options available, and doctors agree to listen to patients and negotiate regarding treatments, taking patient's interests and values into account.
The fiction of the "informed patient" creates an image of a level playing field
between doctor and patient (almost equal power dynamics), coupled with a hint of
reverence for the final say of the physician in the health matter.
As with any ideal type, the construct has the power to expose its opposite. The
division between lay and expert knowledge becomes questionable. It is possible for
a patient to see her physician and gain the same information they gathered on their
own time, needing the physician to simply raise the right issue and offer the right
treatment to suit the patient's needs. Morant (2006) suggests that theoretical models
can facilitate communication between professionals, bolster legitimacy and provide
rhetorical aids, and prove useful for professional identity construction (especially for
psychiatrists), but these are only "partial and provisional understandings that must
be used creatively and flexibly in combination with more informal sense-making
processes derived from practical experience with clients" (p.829). More attention
should be paid to compromise solutions, resulting from power relationships
between various social spheres when the material and status inequalities come to
impact the shape of knowledge (p.834).

Natasha Durich 30
Would the psychiatric elite, in charge of research, administration and
education, provide supports for discussion of the differences in values and
information between psychiatrists and patients? One possible response to such
questions is provided by Pilgrim and Rogers' (2005) examination of the Royal
College of Psychiatrists (UK) campaign titled "Changing Minds: Every Family
in the Land (1998). This policy document is.aimed at using psychiatric clinical
categorizations of stigma and related information (p.2549) to help reduce stigma.
It is stressed that mental disorders are common, education by psychiatrists is
necessary to educate around stigma, psychiatry is imprecise as a science, and
people should be "enabled optimally to contribute towards their own recovery"
(p.2548). In this campaign, psychiatrists argue that the technical knowledge of
their discipline, rather than the social sciences, gives them the mandate to deal
with stigma, without considering that seeing a psychiatrist can lead to increased
marginalization (p.2551). Another reading suggested by Pilgrim and Rose is to
situate this campaign within the re-professionalization strategy of psychiatry:
at a time when the biomedical model is being challenged, this report aligns
psychiatry with a biopsychosocial approach (p.2554). Deinstitutionalization
brings the ideas of stigma, social inclusion, citizenship and quality of life to the
forefront. Pilgrim and Rose end by noting that if leaders of the profession express
something different than that which is experienced within the clinical encounter,
then psychiatry's authority will be undermined (p.2555).
The fiction of the "informed patient" has evolved alongside changes to our understanding of patient rights and responsibilities within the doctor-patient
relationship. According to Veatch (1990, pp.26-29), in the late 1960s and early 1970s
the medical problems of euthanasia, abortion, the treatment of serious illnesses,
and genetic engineering raised moral issues for physicians and patients alike. No
longer could medical opinion be considered value neutral: we are faced with "a
ubiquity of values in medical choices" (p.28). This poses problems for physician
authority because "professional expertise cannot determine the relation between
safety and freedom" (p.32). Veatch notes the following (p.30):
Treating a broken arm or a dog bite or a hernia is necessarily contingent on the value system of the one making the choices, and there is no obvious reason why the values of the health-care professional are the appropriate ones.
He considers "medically indicated treatment as being founded on an assumption
that patient's views are similar to the physician's own views (p.32). To decide

Natasha Durich 3 1
that a certain drug is necessary is to decide that the effects are good or bad, how
good or bad they are (p.31) and that the drug produces some acceptable level of
reliability (p.33). Hence, when this decision becomes not simply a pharmacological
choice, the right of the physician to act as drug gatekeeper can come under
question (p.34).
How best to describe the balance of power within the physician-patient
relationship? The negotiation model argues for adequate disclosure, voluntary
actions by patients, accommodation reached by mutually accepted means, and
autonomy as a constraint for action of both physician and patient (Childress and
Siegler, 1984, pp.140-42). It is admitted that sometimes negotiation is not possible,
or is possible in a limited form, and some matters are beyond negotiation. The
negotiation model seems to accept that some limitations to patient involvement
exist: "maintenance, restoration, or promotion of the patient's autonomy may be,
and usually is, one important goal of medical relationships" but the importance of
it is a matter for negotiation between patient and physician (p.141). The impact of
values, conflicting or unclear needs and goals, and the reality of differing power
potentials within the physician-patient relationship are highlighted by the fiction
of the "informed patient". How adequate are such metaphors for capturing the
truth of the relationship? Would it be better to re-work the metaphor to bring
some consumer language into the picture: a barter? How might this look for
psychiatrist-patient relationships?
Lowrey and Anderson (2006) argue that it is too early to say whether exposure
to this information could increase respect for the medical profession and lead to
increased compliance with treatment suggestions (p.130), or whether the overall
effect will be to challenge the authority of physicians (p.126). In a telephone
survey of 406 residents of Baton Rouge, Louisiana, Lowrey and Anderson found
that people who use the internet for health information also tend to believe that
doctors do not have exclusive control over medical knowledge, although they
were more likely to dismiss an individual doctor than the entire profession
(p.129). There was also some evidence to suggest that wealthier individuals and
those who had a positive appreciation for alternative medicine were more likely
to challenge doctors' advice and rely on their own power to obtain medical
information (p.130).
Henwood et al. (2003) conducted qualitative interviews with 32 middle-
aged women in Britain, who were considering taking Hormone Replacement
Therapy. These researchers questioned the impact of relying on the fiction of

Natasha Durich 32
the "informed patient" as a means of understanding patient behavior. Sixteen
of their participants had internet access and fifteen used it to access health
information. The authors express that these women felt it was the doctor's task to
inform patients about their health or the women felt there would be difficulties
with patients working as partners with doctors (p.598). Four women thought
medical sites were more trustworthy than non-medical sites and there was little
understanding of commercial interests behind the online information bp.600-01).
Fourteen of the women had actively searched for information prior to a doctor's
visit, yet they showed "[glreat concern about appearing to over-step the boundary between 'expert' and patient"'(p.601). These women are not the ideal "informed
patients": they display reluctance in taking on the role, although they are capable
of doing so. The information gained did not seem to "empower" these women.
Henwood et al. (2003, pp. 590-94) provide interesting critiques against a
strong defence of the "informed patient" position. Assuming that the responsible,
informed patient will share information with doctors, leading to empowerment,
is questionable. Is there a direct link between empowerment and information? Do patients want this responsibility? Furthermore, is there time within clinical
encounters for this sort of back-and-forth to occur? Is the clinical encounter flexible
enough to mean that information is used by doctors "for choice" and not "for
compliance" (Dixon-Woods, 2001, in Henwood et al.)? Is the information framed by
doctors using their rhetorical strategies to convince patients of their own approach?
For Henwood et al., conflict between lay and expert opinion is part of the clinical
encounter and physicians expect a certain level of compliance (p.605). In their
words, "constraints exist within both practitioner and patient communities and
within the space occupied by both in the medical encounter" (p. 605): the question is
how to create an equitable exchange of knowledge.
There are differences between the choice of taking hormone replacement
therapy to prevent cancer and taking drugs to treat a mood disorder. When the
fiction of the "informed patient" is applied to psychiatry, it appears that people
who consult psychiatrists are not ideal patients under this view. Viewing patients
with mental disorders as being of unsound mind is part of the historical framing
of mental disorders. The real physical and mental impact of mood disorders (the
nature of the illness) on the patient could limit the ability to search for knowledge
and retain it. It is also unclear whether there are differences in social experiences
that would restrict access to resources for persons who suffer from mental
disorders. For instance, if a person is on a disability pension, their limited income
Natasha Durich 33
might restrict easy access to quality information. The power differential within
that relationship is often obscured by the fiction of the "informed patient". Besides
the question of "how knowledgeable" and "how equitable", there is a question
of "how willing". Someone with a mood disorder might also have self-esteem
issues, which may deter a patient from raising concerns and questions with the
psychiatrist.
Psychiatry Meets the Pharmaceutical Industry: An Unholy Alliance?
Alongside the challenge of debunking the concept of the "informed patient",
we must be alert to the ways in which pharmaceutical industry impacts
decision-making in psychiatry. Ties between the psychiatric profession and the
pharmaceutical industry are not new, but have been forged over the past 50 - 100
years. This historical backdrop is a necessary part of the story of psychiatry. The
ties of mutual help and interdependence-drugs to treat disorders and money
to fund drug companies-are part of how psychiatry has become the creature
it is today, with its plentiful took kit of psychiatric interventions. This section
expands on that history and focuses attention on current developments in the
alliance between the psychiatric profession and the pharmaceutical industry. It is
in light of the evolution of psychiatry and its interrelationship with Big Pharma
that we are able to understand, through comparison and critical reflection, what is
happening today.
Castel, Caste1 and Lovell (1982) recount that in the United States, between
1900 and 1930, the mental hygiene movement and the ideas of psychoanalysis
(migrating from Europe) were in vogue. Psychoanalysis provides a way of
reducing social issues into questions of psychology (p.261-62). According to
Castel, Caste1 and Lovell, the idea that psychiatric professionals are necessary to
deal with psychiatric clients took hold around 1944 in the United States (p.258).
The problems of anxiety and psychosis created from World War I1 were creating
government concern (p.2). Castel, Caste1 and Lovell (p.85) state that in May 1954
Chlorpromazine came onto the market (Thorazine) and within eight months it
was provided to over two million patients.
Rasmussen (2006) argues that an alternative reading of antidepressant
history is possible. In the early 1900s through to the late 1920s, drug companies
approached the psychiatrists of the time (neuropsychiatrists) and marketed
amphetamines for depression, drugs initially researched for their antihistamine
properties and stimulating effects (pp.293-99). The company Smith Kline French
Natasha Durich 34
promoted Benzedrine for "mild depression", in the late 1930s and early 1940s,
thereby broadening the condition's definition (pp.315-17). This had the effect of
bolstering Myerson's idea that depression involves apathy (adhedonia), the opposite
of "pep and zeal" (p.318). Rasmussen also contends that early psychoanalysts were
not solely concerned with talking therapy, but were open to using tranquilizers and
electroconvulsive therapy (p.291).
The marketing of drugs to the psychiatric profession, and later to the general
public, expanded the scope of psychiatric therapy beyond the confines of the
prevalent form of treatment at the time-psychoanalysis. According to Kirk and
Kutchins (1992), psychoanalytic methods were critiqued in the 1960s because of their limited appeal: clients were most likely to be young, attractive, verbally articulate,
intelligent and successful (p.19). The 1960s and 1970s was also a time of growth of
experimental talking therapeutic methods beyond drugs and psychoanalysis. As
noted by Castel, Caste1 and Lovell (1982, p.255), "whenever psychiatrization meets
with resistance, it is transformed, and what emerges in each instance is a novel and
more flexible psychiatric model': This flexibility makes the classification system
vulnerable, which lead to changes in the third version of the Diagnostic and Statistics
Manual (Kirk & Kutchins, pp.10-11). This version of the manual is a key point in the
history of psychiatric theorizing because it brings psychiatry closer to mainstream
medicine in terms of how disorders are diagnosed.
As we see from this brief overview of the modern rise of drug therapy, the
treatment options available for psychiatrists are in flux. The tool kit of psychiatric interventions is not locked tightly but is open for new tools, while some rust from
disuse. Castel, Caste1 and Lovell (1982, p.308) note that psychiatric interventions
function as unified whole, although historically and socially different treatments
and theories gain the spotlight at differing times. This spectrum of psychiatric
intervention ranges from the less invasive and less restrictive forms, such as
counselors and outpatient therapies, to the more invasive and restrictive forms, such
as Electroconvulsive Therapy, mandatory confinement in hospital, and forced drug
treatment. Today, the manufacturers of psychiatric drugs offer psychiatrists many
The pharmaceutical industry-Big Pharma-has become quite friendly
with the medical establishment. Drug representatives meeting in the offices
36 For more detailed information on the common classes of antidepressant drugs, refer to Appendix I : Classes of Antiakpressants.

Natasha Durich 35
of physicians, company funds being given to scientists, and even the halls of
medical education are not untouched by drug company dollars (Lexchin, 2001;
Kassirer, 2005). On a small scale-the office-it is unclear how often patients ask
specifically for mood altering drugs (Cebuliak, 1995; Penfold and Walker, 1983),37
as opposed to being given the brand name drug by the physician. It is also
uncertain how patients are positively impacted by the social awareness created
by drug advertisements: depression and anxiety are no longer in the shadows
of public thought. Speaking from a radical social control perspective, Thomas
Szasz (2001) suggests that prescribing practices are fulfilling a number of needs:
the public wishes to take legal drugs, pharmaceutical companies wish to make
large profits, and physicians must diagnose and prescribe in order to keep their
power (p.40).
When drug companies play a crucial role in dictating health care practice,
patient wellbeing is impacted in a serious way. The idea of science, specifically psychiatric science, as being grounded in observation and analysis is challenged
by conflicts of interests. Some thinkers have questioned the impact on democracy
when health care is guided by big business ideals: sell more drugs. McKnight
(1995) argues, "[iln exchange for the power to cope and celebrate, we are offered
chemically managed versions of chemical oblivion"(p.69; Rossides, 1998, p.161;
Szasz, 2001, p.97). Lexchin (2001) argues that psychiatrists are prescribing
"normality" when they dispense "lifestyle and encouraging ignorance of
social injustice and diversification. These "lifestyle drugs" support the notion that
responsible citizens strive for perfect health. Health becomes a consumer's choice.
One ethical question concerns conflict of interest between members of the
medical establishment and the pharmaceutical industry. Brody (2007) argues
for a Divestment Strategy toward the pharmaceutical industry (p.299), aided by
professional repercussions for the violations of these guidelines (p.308). In his
view, information provided by drug representatives is not essential because other
sources (letters and downloads) are available (pp.300-01). The latest drugs might
37 Mintzes et. al. (2002, pp.278-279) conducted a survey of family physicians in Vancouver and Sacramento. These researchers found that in 12% of visits, patients requested drugs (42% of which were advertised directly to consumers). Further, the physicians did not form a strong opinion on the efficacy of the drug for the particular problem in 40-50% of cases; in cases where the patient did not request the drug, physicians were ambivalent in only 12% of cases. This study lends support to the view that patients request drugs despite their potential ineffectiveness. 38 "Lifestyle drugs" include hair-growth drugs and erectile dysfunction drugs. In my view, drugs that produce an upper effect when used to treat mild cases of depression (where other remedies would be equally effective) should be classed as lifestyle drugs.

Natasha Durich 36
not be the best drugs, and even if they were the best drugs, it is questionable
whether physicians can accurately discern whether the information they obtain
is unbiased. Some physicians also wish to obtain free samples (pp.302-05). Brody
claims there is no data to suggest that indigent populations are benefiting from
these samples. Commercial sources have been relied upon to provide gratitude to
physicians and this demoralization must be addressed if physicians are to break
their ties to pharmaceutical companies (pp.305-07). Brody argues for higher levels
of accountability.
Steiman, Bero, Chren and Landefeld (2006) provide an example of a drug
company's (Pfizer Inc., and the subsidiary Warner-Lambert or Parke-Davis)
unethical promotion of their drug (gabapentin, approved in 1993 for the treatment
of partial complex seizures). The authors analyzed 8000 pages of documents
from the litigation, where the company answered charges that it violated federal
regulations by promoting the drug for unapproved uses (spanning from 1994-
1998). The draft promotion budget for the drug (1998) provided the largest single
amount (percentage of total and across categories) for professional education in
terms of speaker's bureaus, advisory boards and dinner meetings: $19,110,000
(p.287). It is easy to see why one business plan stated "Medical education drives
this market!!"(p.284). The single category with the largest amount of dollars
devoted to its needs, surpassing the second category by twice the funds, was
professional education in the area of emerging uses: $11,039,000. By 2000, the
number of prescriptions for the drug for pain and psychiatric disorders was
greater than the amount prescribed for epilepsy, migraines, and other uses. This
great shift was due in part to research improvements and to marketing off-label
uses before getting FDA approval (p.285). In 2004, Warner-Lambert settled the
litigation by paying out $430 million dollars (p.285).
The documentary Little Helpers (2003) also calls for higher levels of
accountability for the drug companies by examining the exposure of drug
safety concerns. These matters include reported suicides while taking certain
antidepressants, unusually high levels of anxiety and anger associated with
taking some medications, and painful withdrawal symptoms. The situation
for physicians was described as difficult because their drug information may
largely be from drug manufacturers. Information about clinical drug trials is
often guarded and seldom comes to light unless mandated by a court. There is a
growing need for accurate information to become public before harm is caused to
patient health. Although the drugs may be safe and effective for many consumers,

Natasha Durich 37
they have had a harmful impact on the lives of many others. The documentary
makes the firm point that this harmful impact could be reduced if accurate
information is released concerning the safety of these drugs. This documentary
did not canvass the questions of how to measure safety and who should set these
standards for antidepressants and antianxiety drugs.
A Changing Ethics of Psychiatric Professionalism
The degree to which professionals can assert control over their work and work
products has been changing rapidly. For Freidson, this administrative control
would stifle innovation and decrease trust. Therefore, it is possible that workers
will rebel against this idea. The desire for administrative control "is related to the
informal attempts of all workers.. . to do their work as they see fit on the basis of
their own sense of knowing how to do it"(p.73-74).
In his updated thesis, Freidson (2001) argues that managerialism (top-down
bureaucratic governance), consumerism (free market rule) and professionalism
are three logics that operate in tandem and it is a policy question of how
to balance them (p.181). Some measure of expert authority and professional
economic privilege (credentialism and monopoly) is warranted in an effort
to nurture specialized knowledge (p.208). According to Freidson, "the most
important problem for the future of professionalism is neither economic nor
structural but cultural and ideological" (p.213). By this he means that a strong
sense of professionalism and a commitment to its highest ideals is needed
if professionalism in its true sense is to survive. In addition, he argues that
"the maximization of profit" is "antithetical" to the ethics of professionalism,
and a political economy that supports it is working against this model of
professionalism (p.218).
Freidsonls (2001) concern about the impact of the profit motive on
professionalism raises the question of what consequences result from health
professionals making profits from the packaging of health as a commodity. In the
growing context of the privatization of health care services, it is of concern that
physicians are able to focus on making profits in the fee-for-service system and
health care becomes big business (Cohen, 1985, p.64). Health care as a commodity
challenges the common notion of the "good physician". In brief, "service is to care
which is to love and love is the universal apolitical value"(McKnight, 1995, p.38).
Why trust the professional if she is no longer above reproach?

Natasha Durich 38
Speaking Around Drugs, Therapy, & Ethics: Significance of The Study
How is psychiatry adapting and changing to accommodate the challenges facing
the profession? The observations of working psychiatrists can provide one means
of answering this question. Likewise, what do they view as being important in
leading up to this particular historical moment? These views can shed light on
what psychiatrists view as critical to their profession and what they are working
towards, or being caught-up in (work environment). For example, Goldbloom
and Garfinkel (2001, p.262) share the views of Frank and Kupfer on challenges
facing psychiatry in the 21" century, based on an integrative and broad approach
to psychiatry. Among those issues are the determination of how life experience
alters gene expression, neurobiological effects of psychotherapy, the creation of
adverse effect-free pharmacotherapies, the investigation of trauma, connecting
physical illness with anxiety and mood regulation and the impact of aging on
affect disorder expression and treatment.
More specially, there are few studies available highlighting the intricacies
of how psychiatrists make treatment choices. In their survey of 273 psychiatric
faculty members in Washington State, Sullivan, Verhulst, Russo, and Roy-
Byrne (1993) report that greater than 75% "would use psychotherapy, consider
its omission inappropriate, and consider it to act upon the cause of the patient's
distress in all three [personality disorder] cases [provided in the surveyl"(p.419).
In another study, Copeland (2001) questioned 90 licensed psychiatrists about their
treatment planning in two hypothetical cases and also gauged their egalitarian
attitudes towards women. His work suggests that the physicians considered
medication as a first choice and did so in a systematic way, regardless of gender
of the patient, gender of the practitioner, or diversity/consciousness training
of the physician. According to this study, older, more experienced physicians
recommended medication less regularly than the younger physicians. This is
an interesting finding bec.ause the psychiatric profession is aging and there is a
high attrition rate due to retirement. Numerous factors motivate psychiatrists to
prescribe certain medications, ranging from expertise, training, personal beliefs,
social norms, and patient satisfaction. The information gleaned from interview
studies can add to our understanding of prescribing practices.
Studying other cultures for a deeper understanding of psychiatrist prescribing
behaviours is another means of shedding light on North American practices. For
example, Slingsby, Motnikoff, Akabayashi, and Mizuno (2007) conducted a novel
qualitative interview study of fifteen psychiatrists in Japan, four had practiced in

Natasha Durich 39
the United States and in Japan. Further interviews were conducted to determine
cultural differences. They explored the various strategies for addressing patient
adherence to psychiatric drug regimes and found that (1) the psychiatrists
recognized that patients had various misconceptions regarding the drugs, such as
their addictive properties, (2) side effects reinforce existing patient misconceptions
and resistance to drug treatment, and (3) psychiatrists intentionally underdose
patients, accept that resistance may be stronger than compliance, and employ
euphemisms (p.243). These researchers state, "Effective care, thus, requires
physician competence to address patients' psychiatric predispositions to the fear
of the use of prescription medications" (p.241).
Slingsby et al. (2007) also reported that the psychiatrists show resignation,
meaning that it is viewed as the patient's choice whether to live with the illness
or take medication, and employ euphemisms, such that a psychiatrist is also
called a mental internist or a neurologist depending on practice setting (p.244).
It was noted that in Japan, the entrusting model predominates. In this model,
patients place a high degree of trust in their physician to make choices for them.
Showing resignation and employing euphemisms might be one means of showing
respect for patients, who are giving psychiatrists the power to make decisions over their health. This respect might be critical in maintaining trust and ensuring
compliance with treatment plans.
More studies like the Slingsby et al. (2007) study could assist us in
understanding psychiatrist prescribing practices. It is more common for social
science researchers to focus their attention on the opinions of those being
regulated, rather than the regulators: "studying up", turning attention to
those who are considered to be the experts, is less c~mrnonplace.~~ Based on
my literature review, it appears that we have less descriptive and analytical
information on how psychiatrists characterize their approach to prescribing
antidepressants and antianxiety drugs and more information focused on
treatment choices and how to prescribe drugs. Qualitative research highlighting
the experiences of psychiatrists with prescribing antidepressants and antianxiety
drugs would provide more much needed insight into how psychiatrists view their
work. In short, it would be beneficial to hear from the psychiatrists themselves.
39 In a comment to the article "Professions of duplexity. A prehistory of ethical codes in anthropology", by Peter Pels, Laura Nader (1999) states that "studying up" is "a term which I coined in the 1960s (Nader, 1969) precisely because I thought the channel within which anthropologists were debating ethics [to be] too narrow. It is still too narrow" b.121).

Natasha Durich 40
Similarly, there is a gap in our understanding of the views of psychiatrists on
the topic of their ethical commitments. Exploring the ethics around prescribing
mood altering drugs has largely been the domain of philosophers and medical
experts. What kinds of ethical problems, both practical and institutional
(Freidson, 2001), do psychiatrists encounter when medicating patients? How
do they feel about the relationship between medical professionals and medical
bodies and the pharmaceutical companies (Brody, 2007)? The physician-patient
relationship is impacted by other social relations, which in turn impact a
psychiatrist's views of his ethical commitments. Qualitative interviews with
psychiatrists are one means of questing for answers to some of these questions.
The descriptive and analytical richness provided by such accounts could
provide information that illuminates what it is like to "do psychiatry" in the 21Bt
century and what attitudes and activities contribute to patient harms due to the
consumption of mood altering drugs.
Natasha Durich 4 1
CHAPTER TWO: METHODOLOGICAL CONSIDERATIONS
The Birth of the Study
My topic of research is psychiatrists' views on prescribing antidepressants and
anti-anxiety medications and the ethical implications. A qualitative examination
of this issue, focusing on the views of psychiatrists, is useful because they are
the professionals who work in the area and are trusted to provide their expertise
(both on drugs and the ethical ramifications of prescribing). Readers have the
opportunity to glimpse into the world of clinical psychiatrists and, hopefully, gain a richer understanding of their ideas on prescribing practices. In brief,
the purposes of this study are exploratory and descriptive. The function of
the research is contextual because it explores the meanings and experiences of
psychiatrists who treat anxiety and depression.
Mission Questions
Chenail (1997) suggests that qualitative researchers should be guided by mission
questions, which are a means of refocusing attention on the salient matters should
confusion arise. Broadly speaking, the two mission questions for my study are as
follows:
1. How do clinical psychiatrists view the impact of prescription drugs
(to treat depression and anxiety) on their practice of psychiatry (use
of drug-related resources, interaction with patients as consumers, and
utility of the drugs)?
2. What ethical obligations are important or need work in the use of
prescription drugs in psychiatric practice (to treat mood disorders)?
Data Collection Methods
(a) How to best approach the problem
In the words of Ritchie (2003), the qualitative approach "offers the opportunity
to 'unpack' issues, to see what they are about or what lies inside, and to explore
how they are understood by those connected with them"(p.27). Psychiatrists
working with depressed and anxious patients are in a good position to discuss
the issues surrounding prescribing antidepressants and anti-anxiety drugs, as
well as the ethical implications. To borrow a metaphor from Rubin and Rubin

Natasha Durich 42
(2005, p.ll), qualitative researchers work "more like a skilled painter than a
photographer, selecting details and creating an image from them". This painting
should be rich in detail. I would add that this painting includes more colours
in part because of the work of feminist social scientists. Atkinson, Coffey and
Delamont (2003, p.83) note, "we [researchers] now have to ask ourselves who
'we' are, who 'they' are, how we represent ourselves and others, and even what
methods we employ".
The preferred method of gathering data is via face-to-face interviews with
psychiatrists. In the words of Arksey and Knight (1999, p.32), "Interviewing is a
powerful way of helping people to make explicit things that have hitherto been
implicit-to articulate their tacit perceptions, feelings and understanding". The
advantages of face-to-face interviewing over questionnaire/survey methods
are many, including the ability to clarify of meanings generated by the subject
(Arksey & Knight, 1999; Palys, 2003, p.160). Furthermore, specialists might provide
"fairly idiosyncratic" perspectives and the subject matter is complex, making the
project suited to interview inquiry (Ritchie, 2003, p.33).
Individual, face-to-face, interviews are ideal because the subject matter is
private (in the sense that it involves individual practices and ethical views) and
detailed accounts are sought (Lewis, 2003, p.56-60). The personal experiences and
views of psychiatrists, which are intermediated by and partially created by the
social factors, are the units of study. I attempt to make sense of their words by
looking at prior literature on the matter and by looking at my own understanding
of what might be impacting their views. I also tried to probe for clarification of
some of these social factors. These ideas speak to the critical realist assumption
that there is a reality and it is tangible/knowable through our views of it (Lewis,
2003, pp.56-60). This study is guided by my belief that "knowledge in the social
sciences is provisional, uneven, complex and contexted"(Arksey & Knight, 1999,
pp.18-19).
(b) Sampling plan, setting, and interviewing
I purposefully chose twenty-four psychiatrists to approach, first via a letter
from my supervisor (Appendix 2: Letter of Introduction) and then following-up with
a phone call or email. I searched the British Columbia College of Physicians and
Surgeons online database and used the search engine Google.ca to determine
whom to contact. When searching with the College database, I selected the listing
of psychiatrists, chose a number to mark an interval, and wrote down the names

Natasha Durich 43
of psychiatrists whose names were in the database at this interval. The chosen
psychiatrists are clinical psychiatrists, licensed to practice in British Columbia,
and have different affiliations. A few psychiatrists were excluded because of
repeat affiliations (i.e. working at the same hospital); when this occurred, I moved to the next name in the database One psychiatrist was removed because
he practiced forensic psychiatry, which is outside of my research focus. Seven
psychiatrists agreed to participate. Seventeen psychiatrists said "no" or did not
answer my follow-up call or email.
The seven psychiatrists "have had the appropriate experience, are
knowledgeable and are able to explain to [me] what they know" (Rubin &
Rubin, 2005, p.70). Three out of seven participants serve in administrative
capacities, two of whom have served in teaching roles. One psychiatrist is
retired from practice. The average number of years in psychiatric practice is
30.5. Four psychiatrists have been practicing between 20 to 30 years. Together,
the psychiatrists are from the geographic areas of New Westminster, Richmond,
Vancouver and Victoria British Columbia. Psychiatrists from Surrey and
Burnaby did not agree to participate.
In addition to accessing the 24 contact names from the British Columbia
College of Physicians and Surgeons website, I used chain referral sampling,
or snowball sampling. According to Palys (2003), "snowball sampling involves
starting with one or two people and then using their connections, and their
connections' connections, to generate a large sample"(p.145). According to Palys,
the technique is less costly and time consuming than attempting to generate a
representative sample from a large geographic area (Palys, 2003, p.140). Atkinson
and Flint (2001, p.2) note that this method is useful when the population is hard
to access (trust is needed to gain access) and can be effective when the aims of the
study are exploratory and descriptive.
However, of the six psychiatrists who were asked to provide referrals, five provided one name each. When the five referrals were contacted (total number
of psychiatrists contacted increased to 29), none of the five referrals agreed to
participate in the study. I did not provide the name of the referring psychiatrist
in an effort to protect confidentiality and anonymity. It is my guess that chain
referral sampling works well when an informant can contact participants and
the personal connection is used to encourage participation. Another tactic,
in retrospect, would be to take the time and network within the psychiatric
community and build personal connections.

Natasha Durich 44
Another potential obstacle to accessing participants is the time commitment
involved. One psychiatrist in particular described his reasons for refusing to
participate in a way that stressed the complexity of the issues and the inability to
offer one hour of time. Perhaps an online survey method would work well with
this group, securing higher participation rates. Yet, the benefits of a face-to-face
interview would be lost in an effort to gain a higher response rate.
It is my belief that these issues can be explored initially through the analysis
of the seven case studies presented here. In order to protect their identities, I assigned the participants the following code names: Peter, Kitta, Dolan, Pearl,
Nelson and mart^.^ Dr. Hoffer insisted that his real name be used in this thesis.
Each face-to-face interview was approximately one hour in length. Peter, Dolan
and Marty's interviews were taped. Kitta, Pearl and Nelson's were not taped.
Notes were taken in all cases. I transcribed the interviews verbatim shortly after
each interview. Each line of text on the printed page was given a number to aid
organization.
The interviews took place at the participants' respective offices. Peter and
Kitta work in hospital settings. Dolan, Pearl and Nelson work at private offices.
Marty works in an office building and does not see clients. Dr. Hoffer works as a
consultant for his orthomolecular medicine business, seeing clients. The feelings
I had as I waited for each interview varied greatly because I dislike hospital
settings. Their smell and sterile feel make me feel sick to my stomach. Dolan's
private office, on the other hand, had a warm and inviting waiting room with
friendly receptionists. Refreshments were also available on the table for those
waiting in Dolan's office. In Marty's office, I did not encounter patients waiting
for their appointment. I did not notice any ways that atmosphere impacted
the interview, in terms of length or quality of responses, or nervousness of
interviewer.
The flexible and emergent nature of qualitative research provided the
opportunity to revise questions. Each interviewee's responses evoked new
images and ideas in my mind, which influenced the way questions were asked of
subsequent participants (Appendix 3: lnterview Schedule). I noticed during the first
couple of interviews that I was giving rather lengthy responses to my participants.
As a remedy, before each interview I asked the following questions: (1) How can I
4a These names are chosen from a book I'm currently reading, as a matter of convenience. The book is Mindplayers by Pat Cadigan (1987, Bantam Books).

Natasha Durich 45
listen more, and (2) How can I turn comments into queries. This helped me focus
my attention on the participant's descriptions of their world.
(c) Interview schedule
The questions I prepared are organized to mimic a natural conversation, with
some less intrusive questions to start and working through toward the more
conceptual and personal (Palys, 2003, pp.190-191). I began with a discussion of my
ethical obligations and background questions in order to help create a comfortable
space. In my opinion, "rapport" is the level of comfortableness between
participant and researcher, built by common dialogue that is not offensive to
either party. It is assumed that there will be a certain level of unfamiliarity
because of a lack of prior encounters and perhaps because of "studying up". Yet,
these are not insurmountable barriers: sensitive interviewing and questioning, as
well as attentive body language and using common terminology are important
factors in building the comfort level. Nelson, in particular, had many questions
about the nature of the research prior to his participation and gave oral consent
only (i.e. did not sign the consent form).
Hathaway and Atkinson (2003) caution that "[ilf the researcher fails to open
up the back regions of a social setting, he or she will only assemble a standard
or public account of the group practices therein"(pp.162-163). Rubin and Rubin
(2005, p.139) suggest that proposing an explanation, providing non-threatening
questions, asking for exceptions to a provided generalization, responding to hints in the speech of interviewee, probing for specific experiences, and concentrating
on the tangible (as opposed to why questions) can be used to help interviewees
open-up.
Understanding that "an informant may be able to generate more than one
frame of reference in his or her accounting"(Atkinson, Coffey & Delamont, 2003,
p.130) is useful to capture the complexity of our personal experiences. In the
words of Becker (1996, p.5), participants "make vague and woolly interpretations
of events and people". It is our task to represent the richness of that complexity,
while alerting our audience to the places where we move from description to
inference (from the ernic to the e t i~)~l . This notion can be illustrated with the
4' The ernic perspective takes the insider's point of view, providing situated meanings; the etic perspective makes comparison across persons in different situations possible, providing a generalized account. These differences highlight the (re)presentation of views that is the work of the researcher.
Natasha Durich 46
phrase "mind the gap". Anyone who has been to the London Underground will be
familiar with the phrase, as it is read on the tiles and heard over the loudspeaker
to alert travelers to watch the gap between the train and the platform. As
interviewers, we must "mind the gap" between describing views and interpreting
them. As a result of our role as re-presenters of views, Becker cautions us that
"the nearer we get to the conditions in which [participants] actually do attribute
meanings to objects and events the more accurate our descriptions of those
meanings are likely to be"(p.4).
(d) Roles to be assumed
As a Criminology student interviewing psychiatrists, I feel as though I am
viewing psychiatry and medical ethics from an outsider's perspective. I wonder
how training in the sciences would influence my point of view. My position might
be comparable to someone studying the prison system, which is both within
society and excluded from it thereby inviting outsider interpretations (Bosworth,
2001, p.437). Building rapport is important, especially as an outsider and as
someone who is studying-up.
Overall, I found the participants to be articulate and eager to answer. I tried
to emphasize that there are no right or wrong answers and I am interested in
gaining participant opinions. For example, a couple of them asked "is this what
you're after" or "did I answer the question". Interviewing the interviewer might
be an explanation for this: psychiatrists conduct clinical interviews. Being aware
of this possible desire to please, I try to be clear when asking the question and use
clarifying probes when needed.
As someone who has family experience with mental illness (depression and
anxiety disorders), I am familiar with psychiatric interviews and the options to
treat these mood disorders. I have felt torn between advocating for medications
in lieu of therapy; torn between advocating for abandoning psychiatry versus
"trying a little harder". These complex emotions surfaced when I had time to
re-read the notes and transcripts. At the end of this project, I am no closer to
reaching a personal conviction on the "goodness" of modern psychiatric practices
for the treatment of depressed and anxious patients. I too hold a "vague and
woolly interpretation" of the work done by psychiatrists.

Natasha Durich
An approach to data analysis-
Framework Approach
In the following section, 1 explore my approach to data analysis. 1 adopted the
Framework method of analysis suggested by Ritchie, Spencer, and OConnor (2003,
pp.219-262; Appendix 5: Framework Method). The first phase is data management. I read
through the transcripts and generated a list of common ideas that emerge through
the various interviews. From this list, I refined these ideas into the following initial
concepts or codes, which are expanded to include sub-ideas (Appendix 4: Conceptual
Framework). This process has its roots earlier in my planning because generating
questions was, in a sense, an initial pondering of codes and possible themes (Basit,
2003, p.145).
Next, I moved from this index of concepts/codes to the process of working with
the transcripts and assigning the codes to the written text. Moving sentence by
sentence with coloured pens for each of the concepts, the transcripts were marked
using the identifying numbers. Then, I created one thematic chart for each of the
concepts (#1 and #2 were placed on one sheet) using the Microsoft Excel program.
Each case (each person interviewed) occupied one row and each sub-idea occupied
one column. I included one column for my own comments as I was working. I included line numbers as I summarized the ideas of each participant, referring back
to the marked transcript. When I felt that an idea was particularly well expressed, I
highlighted it (in a colour to match the pen marking). Once a chart was complete, I
moved to index cards and copied the quotations onto them, along with code name
and concept number. At the end of this process, I had three main products: the
thematic charts, the index cards of quotations, and the marked transcripts. I dealt
with Dr. Hoffer's transcript separately because it allows his voice to dialogue with
the other participants in an interesting way.
The next phase is the descriptive accounts stage. For this I moved away from
Framework, where charts were recommended, and worked by hand scribbling
notes onto paper. This free-form of expression helped me link ideas and detect
more meaningful categories. Regrouping concepts, searching for coherence among
the concepts, and clarifying the most relevant dimensions of the concepts were the
main tasks. I referred back to the index cards as a means of keeping the participant
words and ideas in the forefront of my mind.
The final stage of exploratory analysis calls for a master chart. I did not construct
a master chart because I felt that my small number of participants were easy to

Natasha Durich 48
track with the charts already in place. I moved to the method of rough sketching
to draw out some connections between the concepts. I continued to work with
the index cards. The main tasks are searching for patterns, making sense of the
connections and contradictions, and attempting to draw out the implications and
possible explanations for the findings. Undoubtedly, there are more connections
to be made, even in this small collection of case studies.
As argued by Ritchie and Spencer (1994), the Framework method is
generative (driven by original accounts), dynamic (open to change), systematic,
comprehensive (full review of materials), and accessible (easy retrieval). The
charting allows between and within case comparisons so that every bit of data
can be inspected. They note that the strength is that "it is possible to reconsider
and rework ideas precisely because the analytical process has been documented
and it is accessible" (p.177). Of course, the "creative and conceptual ability of
the analyst to determine meaning, salience and connections" is the ultimate
requirement for good qualitative work (p.177).
Additional Considerations
Throughout the process, I reminded myself of one useful idea introduced by
Weiss (1994), who considered analysis the testing of mini-theories. Weiss stated,
"I do ask myself what I am seeing instances of, what I am learning about, and
what questions the material raises" (p.155). I also attempted to remain sensitive
to the need for reflexivity in my accounting. In this case, the question posed by
Mauthner and Doucet (2003) was of value: in what ways is the knowledge partial,
situated, historical, developmental, modest? (p.424). The value of reflexivity for
qualitative research is the stance that knowledge cannot be separated from context
and source. Ultimately, the account presented is my unique re(presentation) of the
views of the seven participants.
Quality and Value of Research
Marshall and Rossman (1989, pp.144-143) and Atkinson, Coffey, and Delamont
(2003, p.156) discuss Lincoln and Guba's (1985) criteria for evaluating naturalistic
inquiry:
1. Credibility, bolstered through in-depth descriptions,
2. Transferability, testing of the models and concepts you provide,
3. Dependability, considering the world as it is changing,
Natasha Durich 49
4. Confirmability, including questions requiring explanation and elaboration,
possibly corroboration of earlier statements.
The use of the Framework method and careful choice of questions (posed to
interviewees and asked of the data) are ways of approaching the Lincoln and
Guba criteria.
Trustworthiness, which is the central issue, can be improved by a repeated
inspection of "every goblet of relevant dataM(Silverman, 2000, p.180). Uncovering
the many layers of meaning, testing them against what has been recorded, and
explaining anomalies (searching for negative evidence) is part of the process.
Ethical Obligations
It is important to outline my commitment to ethical standards: minimizing the
potential for harm and respecting my participants. I obtained ethics approval
from the SFU Office of Research Ethics and my project is classified as minimal
risk. Prior to asking the interview questions, I informed each participant of
the uses of the data, the security of the data, the voluntary nature of their
participation, and my intention to provide confidentiality and anonymity for their
information. I removed any details that would identify the participant (names,
place names, affiliations) from the transcript. The participants will receive either an abstract or direction to the online copy of the finished thesis, as discussed
individually with the participants at the time of the interviews.

Natasha Durich 50
CHAPTER THREE: RESULTS AND DISCUSSION
The discussion begins with a look at the forces that contribute to the decision
making of psychiatrists. Situating psychiatry historically provides a necessary
backdrop to the conversation. Following that, the situational context, or the
collection of more immediate forces that impact ethical decision making, are
discussed. Providing a rich description of the context is a necessary part of
talking about ethical decision making because it informs professional judgments.
In the words of Dolan, "it's not such a simple thing-what we do in the office"
(133-34). The remainder of the chapter is focused on psychiatrists' opinions on
pharmaceutical companies and ethical obligations when medicating patients.
Finally, the participants' views on the future of psychiatry are discussed. Each
section begins with the Results, a re(presentation) of the words of the participants,
followed by the Discussion, a further interpretation of their words. Participant
quotes and ideas are referenced using line numbers from the transcripts.
Looking Back at the History of Psychiatry: Where are we now?
Results
Participants were asked to fill the shoes of a historian and describe the past 20 or
so years of psychiatry in terms of the major changes to the profession.
One idea shared is in the early days of psychiatry, the focus was on
psychoanalysis and talking therapies. Peter, Pearl and Marty comment on the
shifts in focus throughout the years. According to Peter, the shift was from
psychoanalysis to biological and now it is swinging back to psychosocial and there
is a growing realization that art and science are both part of psychiatry (268-69).
Pearl places the pendulum at the biological stage and hopes that in the future it
shifts toward greater integration of the biological, social and psychological forces
(99-100). Marty takes a historical contextual approach and comments on the
relationship between the zeitgeist of the decades: from the mechanistic 1950s, to the
experimental 1960s, through to the neoconservative approach of brain science in the
1970s until present (306-18). All of the psychiatrists agree that a pure focus on the
biological aspect of psychiatry would do a disservice to patients because it cannot
offer any complete solution to their troubles. For Nelson, it seems impossible to have
a purely technical brand of psychiatry because the honest human relationship is
central to the work (84-88).

Natasha Durich 5 1
The characterization of where psychiatric treatment stands today varies
among these psychiatrists. For Kitta, "we're at a wonderful and scary place" (84)
because we are learning the causes and finding more specific treatments but the
counseling and supportive helps are lacking. Marty explains that psychiatry is
"aiming to be a self-important and detached profession" when it should focus on
population concerns and integration with the other helping professions, such as
social work and nursing (371-75). The needs of patients can get lost when the focus
is only on the medication (338-42). Marty also ponders that "instead of responding
in science [psychiatry] responded with scientism, it sort of looks like science
but it wasn't so much science" (331-33); "it was like the emperor's new clothes"
(335). Similarly, Dolan is not convinced that psychiatry is on a positive pathway: what stands out is the "loss of humanness in the whole thing" (271-72) and the
"physical treatment, physical, physical, physical treatment" (261-62). The focus is
on "the quick fix" (258-64).
Dr. Hoffer advocates the use of orthomolecular medicine42 to treat mental
disorders. He feels that psychiatry has made the wrong choices and "the past 100
years is total tragedy" (474). He feels "awful" about being a psychiatrist and states
that he is "often ashamed to tell people that I was a psychiatrist" (475-76). Those
who treat mental disorders, according to Dr. Hoffer, should look for allergies or
physical causes of the illness and treat those causes (79-83):
Dr. Hoffer: Allergies make up at least 75% of all the people I see with depression. So you have to look at the cause for any physical abnormality. Is it a vitamin problem? Is it a mineral problem? Is it a food problem? Is it a toxins problem? Is it due to a bad relationship? You have to examine why is this person depressed. Natasha: Hrnhm. Dr. Hoffer: Not promptly throw a drug at them.
Ultimately, Dr. Hoffer says he would feel content with psychologists providing
counseling services and general practitioners providing the medication to treat
people with mental disorders (249-60). Psychologists are better at doing those
tasks, according to Dr. Hoffer, "[slo why do we need psychiatrists? It should be
abandoned, abolished" (256-57).
42 Orthom~lecular psychiatry can be defined as "the achievement and preservation of good mental health by the provision of the optimum molecular environment for the mind, especially the optimum concentrations of substances normally present in the human body, such as the vitamins" (http:// orthomolecular.org/library/definition/~

Natasha Durich 52
Mood disorders in particular and mental disorders in general are commonly
discussed using a complex model. Peter describes this "bio-psycho-social-
spiritual framework" as "critical" (231-55). In his words, "psychiatry has also
realized that symptom treatment, getting people back to recovery, is only one
part and a very major part but not the only part" (242-44). Kitta describes the
approach as "multifactorial" (72). Similarly, Dolan doesn't believe that "a relatively
rigid view of the illness model" (154-55) helps because wellbeing involves social,
mental, spiritual and physical development (70-77). The causes of mood disorders
can be far reaching. Nelson notes that personal life experiences need to be
discussed when treating patients with mood disorders (19-22).
Discussion
These ideas echo those of McHugh and Slavney (1998)' who outline
perspectives beyond the disease model. This raises the question of whether the
social, spiritual and psychological aspects of psychiatric care are gaining enough
attention in today's practice settings. As noted by Pilgrim and Rogers (2005),
psychiatry's authority is left open to debate when there is a disconnect between
the promise of a certain approach (i.e.: biopsychosocial) and the experience of
a different reality in the psychiatrist's office (i.e.: biomedical). It seems that the
psychiatrists interviewed agree that such aspects are important for their patient's
treatment. This coincides with Morant's (2006) finding from his interviews with
some psychiatrists and other workers practicing in Paris and London. This author
reports (pp.825-26) hesitancy in answering, coupled with themes of difference,
disruption and distress discussed in relation to how mental illness is understood
by mental health practitioners (82% of cases). Health status of the patient was
judged in connection to social impacts, normative behaviour and expectations for
behaviour.
Thus, the general focus of psychiatry may have expanded in an effort to
integrate the whole person but how well has this translated into psychiatric
treatment planning? The acknowledgement of the importance of the counselling
aspects of treatment was not acknowledged by Dr. Hoffer, who feels that
psychologists are better at it. Dolan, in contrast, fundamentally argues for the link
between art and science.

Natasha Durich
Context Informing Ethical Decision Making
Participants were asked the following questions:
1. What are your thoughts on psychiatrists asking patients to take
greater responsibility for managing their use of antidepressants and
antianxiety drugs?
What sorts of activities would management include?
Do you think this is common?
What are some of the obstacles involved in this approach?
Do you encourage patients to do their own research?
Do you feel this approach is useful?
2. Have your patients requested drugs by name? How do you feel about
these requests?
3. Some patients make the comparison between taking medication for
their mood disorder and other patients with physical illnesses (such
as diabetes) taking medication for their disease (such as insulin). Do
you feel that such comparisons are helpful?
Do you feel that this impacts their sense of responsibility?
Patients as active participants in treatment
Results
All of the participants agreed that most patients are better informed about
mental disorders today than in years past. Drug companies are one possible
source of the information and the aid of the internet is one valuable means of
accessing the information (Peter, 105-07; Dolan, 28-29). Some participants display
concern that the information from the drug companies might be confusing,
incorrect or not useful (Marty, 62-63; Pearl, 22-23; Dolan, 208). In addition, Nelson
argues that some information is not based on science (32-34). Dr. Hoffer is
extremely skeptical of the kind of information available to patients, arguing that
most research is funded by the drug companies who skew results in their favour
(123-29). Therefore, patients have no alternatives and there is no real informed
consent (120-22). Marty queries whether enough information is geared at the
patient audience as opposed to the professional audience (33). Perhaps the general
consensus is summed up by Peter, who states, "you have a population that is a lot
more sophisticated and questions things" (107-08).

Natasha Durich 54
The psychiatrists also agree that patients are often invited to take, and
sometimes arrive at the office willing to take, a more active role in their treatment.
In Dolan1s words, "people are very knowledgeable about what they ask for and
what they want" (29-30). Kitta (18-24) and Marty (13-18) describe some of the
actions that physicians can request of patients: journal their progress, trial a
drug, monitor themselves for side effects, get out of the house, recognize signs
of relapse, investigate existing knowledge, attend self-help and support groups,
and attend psychosocial rehabilitation. Marty feels that the patient is probably
in the best position to avoid problems by doing some of these extra tasks (20-22).
This contrasts from the role of patients as recently as 10-20 years ago, where more
deference was paid to the physician's opinion (Marty, 55-56; Peter, 105-07). Some
patients may even shop around for the opinion they desire (Peter, 136).
There are some difficulties in expecting patients to take a more active role. The
degree of patient involvement, according to Marty, "depends on the individual
condition and the individual situation" (28-29). Furthermore, Marty doesn't
think that educational materials or self-management supports are widely used
in psychiatry (43-48). Dolan is concerned that patients may look for negative
evidence to support their views. If they see "the half empty glass" (47) then they
might ask "why shouldn't I take this and they'll look it up" (48-49).
Collaboration between physicians and patients is viewed by many of the
participants as a positive element to the therapeutic relationship. Pearl (10-13)
and Dolan (304-07) note that the confidential relationship might be the only
place where they can really open up. Pearl argues that this can be empowering
for patients. The willingness to discuss the medications, the patient's feelings
about taking them, and other elements of treatment are important parts of this
collaboration. The "win-win situation" (Dolan, 39) can develop, whereby the
psychiatrist "get[s] the buy-in from the patient" (Kitta, 18-19) and "the helper, if
you will, gets educated as well" (Dolan, 39-40). For Nelson, it is necessary for
the patient to express the choice to take the medication because the patient is
a partner (13). Dr. Hoffer is also clear that he is "not ordering" (115) but "just
advising" (114) patients, who ought to take an active role in their health decisions.
Discussion
Some participants noted the benefits of collaboration with patients, including
the willingness to assist in the treatment, the sharing of information and
the necessity of gaining and informed judgment from a patient. The Madrid

Natasha Durich 55
Declaration (1996) of the World Psychiatric Association encourages psychiatrists to
view their patients as partners. This ethic is echoed by some of the participants.
Concerns were raised around the quality of the information patients area able
to access: sources and motives of companies, accuracy, and understandability.
In general, participants note that patients are viewed as being more open to
questioning doctors. These concerns echo the discussion of constraints and conflicts
that operate within the practitioner and patient communities, and within the space
occupied by both, mentioned by Henwood, Wyatt, Hart and Smith (2003, p.604).
Indeed, the psychiatrist and patient arrive at the interaction with differing levels
of knowledge and there are different expectations placed on each. The lay person
may be informed but that state of being is not judged as sufficient for medical
persons to rely on lay person knowledge to ground a medical opinion. In other
words, the power differential between psychiatrist and patient remains, despite the
"empowerment" that some say flows from the "informed patient" state.
Some participants also mentioned the mood disorder as posing some
challenges to the patient accessing information and understanding it. This seems
like a relevant point for future consideration. How does the psychiatric patient
fit within the ideal type of the "informed patient"? Is it perhaps better to think of
achieving equity within the relationship, and admitting that value conflicts exist
within the medical encounter (Veatch, 1990)? It is difficult to see what this fiction
adds to our understanding of psychiatrist patient relations. Furthermore, the
pharmaceutical industry has been criticized for providing an exaggerated picture
of the effectiveness of the drug treatments (McHenry, 2006). It is clear that the
fiction of the "informed consumer" could benefit drug companies, who are eager
to sell more drugs and supply drug information to patients. Is their aim to supply
relevant, useful information for patients or to increase the potential to sell their
drugs? Could it be both? In addition, an open market for psychiatric treatments
might initiate greater choice of treatments for patients who can pay.
The costs and benefits of using drugs to treat mood disorders
Results
The participants spoke about the utility of using drugs to treat mood
disorders. Kitta (59-61), Nelson (36-37) and Marty (81) mention that there are risks
and benefits to taking any drug arfd the physician is responsible for explaining

Natasha Durich 56
these to the patient. According to Peter, physicians should explain even the rare
side effects to patients (122-24) and can consult the guidelines for the dosage
ranges that might be appropriate in a particular situation (210). Marty questions
the quality of this information, suggesting that many studies downplay the
side effects leading psychiatrists to feel comfortable over dosing patients on the
drugs, often to the patient's detriment (80-81; 221-34). Similarly, Pearl argues that
there seems to be "unwarranted faith" in the medications despite showings of
damaging side effects (54-55). Dolan appears frustrated with the pharmaceutical
industry for recalling good drugs and placing harmful medications on the
market: "what do you do with that?" (212-14). Further, Dolan claims that new
drugs become "amazingly same old, same old" (144-46) once they have been on
the market long enough to realize their full effects.
The utility of antidepressants and antianxiety medications has been greatly
exaggerated, according to Dr. Hoffer. In his view, this research is focused on "a
theory that's never been validated" (331-32). The focus on neurotransmitters "has
been accepted as a holy fact but it's not" and "[t]herers some debate as to whether
they play any role at all" (333-34). Dr. Hoffer would prefer to use substances that
do not cause any harm to heal brain function. These substances include vitamins,
in addition to proper nutrition. The focus on drugs can lead patients, who have
been on numerous drugs, to sit "waiting for this magic moment when they are
going to get their final drug that's going to get them well" (61-62). Dr. Hoffer views
this sort of treatment as unacceptable.
Speaking about the overuse of drugs, Dolan, Pearl and Nelson appeared most
concerned with the loss of other therapeutic outcomes. For Dolan, a patient will
not be able to get over and stay over problems without deeper life changes. In
addition, he questions "What happens when there's no more medication, no more
access"? (77-80). Pearl expresses that medication can be a good catalyst so long as
people are not lost (64), meaning that their needs are being met. Similarly, Nelson
argues that drugs can facilitate the process of change but work is needed on the
deeper psychological issues (25). Dr. Hoffer, likewise, argues that medications
"can be helpful" but they "are being used to the exclusion of anything else" (48- 49). Dr. Hoffer states with disdain that psychiatrists often bounce patients from
drug to drug because of the many permutations, in an effort to find the right
fit for a patient who is becoming increasingly ill (58-63). Only one physician
mentioned the medical services plan as a force of consideration for physicians
when turning to medications. Kitta argues that the medical plan encourages

Natasha Durich 57
short-term solutions, including the use of drugs to treat mental disorders (62-63).
Discussion
The psychiatrists interviewed noted the potential problems with how mood
altering drugs are being prescribed currently. The fast output of drugs by
pharmaceutical companies, without long periods of trial tests, often leads to
recalls once enough people have taken the drug and discovered its long-term
effects. Old drugs, which may have done a good job, are taken off the market
and replaced. This poses questions for the quality of our regulatory schemes,
which have been criticized for their reliance on post-market data and lack of
transparency, especially regarding the setting of acceptable levels of risk.43
There is also the difficulty in encouraging acceptance of changes to prescription
availability (Maynard & Bloor, 2003), where regulation is implemented.
Furthermore, the willingness of some psychiatrists to overdose a patient and/
or to use medications to the exclusion of other treatments is a disturbing reality
expressed by some participants. These actions fail to show concern for the
patient's wellbeing. This might be called a violation of trust (Freidson, 2001,
p.216). Codes of ethics aim to make clear the boundaries of acceptable behaviour,
creating duties for professionals to uphold. Violations of trust pose challenges for
ethicists because of complications in wording and, later, enforcing.
Stigma and medicalizing mood disorders
Results
The stigma of having a mental disorder and taking medication can impact a
patient's choice of treatment, or choice to forgo receiving any treatment. For Peter,
there is "a bit more openness" about having a mood disorder and this is evident
in the willingness of people to discuss it with their neighbours (180-84). It can
comfort patients to know that there is something biochemical happening (191).
Similarly, Kitta says that knowing there is a biological component can "immunize
the stigma" (39-44). Pearl notes that patients can find some comfort knowing that
there is nothing to feel guilty about: someone who experiences a backache should
not feel guilty and someone who has a mood disorder need not feel guilty (37-8).
43 See the Royal College of Physicians and Surgeons submission to the House of Commons Standing Committee on Health (November 6,2003).
Natasha Durich 58
Yet, Kitta argues that we have a long ways to go in accepting people with mental
disorders. Dr. Hoffer agrees, stating that the stigma will not go away "until we
can treat it [schizophrenia] as well as the common cold" (458-59). The same can
be said for any stigma surrounding mental disorder. He notes that because there
are easy medical remedies for tuberculosis and syphilis the stigma has decreased
(453-60). When asked whether it is helpful for patients to compare their mental disorder
with a physical disorder, such as insulin dependent diabetes, the answers
were varied. Peter and Kitta found that analogy to be somewhat helpful. As
noted by Kitta, if your pancreas can go wrong, so can your brain (41-42). This
comparison was troubling for Pearl, who prefers to indicate the range of possible
responses to problems. She uses the analogy of having a broken car: you can fix
it yourself, call a mechanic, see help from friends or let it sit and find alternative
transportation. Marty is also troubled by this analogy, saying "you may be telling a mistruth (84). Whether the medication is as useful to someone with a
mood disorder as insulin is useful for a diabetic is questionable. This analogy is
effective at encouraging people to take their medication without worrying about
dependence: "an antidepressant is not like taking heroin, you are unlikely to
become dependent on these medications" (75-76). Medicalization of the problem
can improve adherence to the regime (70-89). Dolan and Dr. Hoffer find this analogy particularly problematic. For Dolan,
this analogy is upsetting because it is based on the disease model which "takes
away the person's responsibility for getting better and being well" (62-3) by
focusing the attention on someone else or on the medication. For Dr. Hoffer, this
is simply what patients have learned: "It's the idea of one disease one drug. One
disease one drug." (445-46). He notes that it would be nice to simply give one pill
to cure depression but "we don't have these pills yet" (451-52). The need to make
changes beyond taking a pill is a message that is lost when patients are taught to
focus on a drug cure.
Discussion
Having a mood disorder means something different in today's social settings
than it meant fifty years ago, due to changes in psychiatric theorizing, social
attitudes and activism around the issue. Yet, to say that there is no longer any
stigma attached would be na'ive. To be told that one no longer has the capacity to
be reasonable, which is one major focus of psychiatric theorizing (Castel, Castel,

Natasha Durich 59
& Lovell, 1982, p.295), is to invite paternalism in all its forms. To be dependent
on state funds is to admit that one can no longer take care of oneself; one is
dependent on taxpayer money, which is not always willingly given. Persons
diagnosed with mood disorders are still heavily regulated and treatment can
be forced upon them in certain jurisdictions, including British C~ lumbia .~~
Furthermore, contact with psychiatry can have a stigmatizing effect, which is not
accounted for in clinical descriptions of stigma (Pilgrim & Rogers, 2005, p.2549).
It appears that the analogy between having a mood disorder and taking drugs
and having diabetes and taking insulin causes some confusion. When trying
to compare the benefits of the medications for each disorder, the analogy seems
to loose some of its truth value. However, if the aim was to convince patients that taking the drug is a normal part of their treatment, and their illness state
is comparable to others who seek medical attention, then the analogy seems to
fulfill that purpose. Of concern is the inability for this kind of analogy to show
alternatives, which is an important part of the dialogue between a physician
and a patient reluctant to undergo treatment. There should be room for such
sensitivities. Perhaps the image of a car breaking down is superior for this reason.
Other Influences Upon Prescribing Practices
Results
One factor that colours the context in which psychiatrists work is the historical
shift from talking therapy to a more physical type of therapy. As noted by
Marty, psychiatrists may be treating those with more severe mental health issues
and other social problems, such as homelessness (237). More than ever before,
psychiatrists have been turning to medications, resulting in the increased need
to deal with side effects (217-20). However, Marty argues that historically talking
therapy was the mainstay and over time it has shifted to using medications that
require careful physical monitoring (201-20). He concludes that psychiatrists
should be shifting their practices to deal with these changes and if they cannot
provide the monitoring, they should share the duties with other clinical
professionals (238-42).
44 IS the person at serious risk of harming himself or others? An affirmative answer to either can lead to being committed to a hospital for psychiatric care in British Columbia. See Mental Health Act, RSBC 1996, Ch.288, s.22(3).

Natasha Durich 60
Dr. Hoffer, as an advocate for orthomolecular medicine, highlights the
pressure placed on psychiatrists, by those who regulate the practice, to uphold the
same standards of practice. He states most of the orthomolecular physicians in
British Columbia have been "gradually suppressed and thrown out" (246-47). The
changes to the system cannot be made on an individual level (289-90). He states
that modern psychiatry is not a science but a church (357-62):
We have our high priests, our journals45, we have our precepts, we have our things we have to do and pay attention to. And if you are not part of the church what are you? You are an outcast. And if they can, they'll kill you and they can't the way they used to but they can take away your license.
One of the problems is self-regulation. He would prefer a working climate where
the law is in charge of disobedience, not physicians regulating other physicians
(299-301). Another problem is the focus in medical school. He argues that the
"major blame has to go against the medical schools who are turning out a group
of physicians who are slaves to Big Pharma" (400-01).
The spotlight is shining on the individual patient and her mental disorder
when she arrives at the psychiatrist's office. As noted by Marty (342-49), tackling
the complex factors that impact the life of someone with a mental disorder would
take money; money would be needed to refocus on the whole person and take
some of the emphasis away from the defined roles of social workers and nurses. It
would also take a restructuring of how psychiatrists earn their money, according
to Dr. Hoffer, who argues that the "patient per hour business" of psychiatry
means that simply prescribing a drug is the easiest way to make money (367-72).
Pearl also worries that people are "getting lost" when talk gets left to the sidelines;
people getting lost is a trend (60-63). During her years as a psychiatrist, she too
has noticed the increased complexity of cases (92) coupled with greater demands
to justify your professional time to administrators who run the office (88-91).
Discussion
As psychiatric theorizing shifts towards a more complex model of mental
disorders, the emphasis in practice might be gravitating toward physical
treatment. How far one can veer from common practice is a difficult question
45 The Journal of Orthomolecular Medicine is not carried on Medline, according to Dr. Hoffer who is an Editor (353-54).

Natasha Durich 6 1
because psychiatry is accomplished by common actions (Freidson, 1994, p.25).
Furthermore, the power of self-regulation and the tactic of credentialism make
it difficult for the boundaries of psychiatry to be overextended. If you fall too far
outside common practice, you are causing those boundaries to become fuzzy. It is
not surprising, then, that psychiatric professionals who argue for approaches that
are too novel or that are not commonly researched will be disregarded.
Managerialism, as noted by Freidson (2001, p.181), is the top-down approach
to governing professional decision making. By focusing on the individual client's
needs, it becomes easier to monitor the work of physicians. By monitoring the
work of physicians, risk is managed. Work is broken down into manageable units.
This is key under the administrative principle (Freidson, 1994, p.73). Of concern
is the impact on morale of the individual physicians, professionals who are
increasingly under supervision by administrators. How do such demands co-exist
with the daily duties and expectations? What should psychiatrists be driving at
when they "do psychiatry"?
The Pharmaceutical Industry: A Love-Hate Relationship?
Participants were asked the following questions:
1. Some ethical problems resulting from the use of these drugs include
failure to monitor medications, overmedication, conflicts of interest,
and the severity of reactions caused by the medications.
i. What responses are you seeing from your profession in
addressing these ethical concerns?
Some people have suggested that the relationship
between drug companies and the medical profession
is at arm's length.
How would you respond to this statement?
Do you feel that providing education and sample
drugs is good practice or necessary?
Do patients have access to safe alternatives?
ii. Do these ethical concerns receive enough discussion?
Do you feel there's a way to discuss them more?

Natasha Durich 62
2. What other things do you think pharmaceutical companies can do to
help minimize the potentially harmful impacts of their drugs?
For example, the makers of apoclozapine, a drug
requiring careful monitoring, have created an online
tool that allows physicians to track patient blood
levels. Do you feel that this is helpful?
Results
The relationship between the pharmaceutical industry and the psychiatric
profession evokes the feeling of a love-hate relationship. The industry's money
plays a large part in subsidizing medical care. The industry is also aimed at
generating profits for the shareholders of the companies. The participants express
conflicting views on the "goodness" of pharmaceutical industry participation in
advancing psychiatric science. Dr. Hoffer is the most critical claiming that the
industry has lied in producing drug after drug, with the promises of drugs that
are "better," 'safer," and "not addictive" (41-46). All agree that the relationship
between psychiatrists and pharmaceutical companies should be viewed with
caution, meaning ethical concern.
All of the participants, with the exception of Nelson, note that the
psychiatric profession is more aware today than in years past of the potential for
conflicts of interest. Peter, Kitta, Dolan and Marty agree that the days of lavish
trips and extravagant promotions are over. Dolan notes, "the seduction is cut out
of the whole thing" (226). Screening of speakers at conferences and the meetings
between the Colleges and the companies are two other features of this improved
relationship. Peter describes the relationship between the pharmaceutical industry
representatives and the physicians as being "at arm's length" (72). Kitta echoes
this by noting that the relationship is not nearly as intrusive (53). Marty provides a neat summary of what he considers to be the state of
conflicts of interest and psychiatrist awareness today (132-34):
[Tlhere has been a response and the average psychiatrist would certainly probably feel uncomfortable with wholly swallowing information that came from the drug industry and recognizes that there is conflict of interest.
Perhaps it is this awareness that leads to a feeling of moral superiority, the notion
that "I cannot be bought by a company". Peter notes that professional discretion is
key in the minds of some physicians:

Natasha Durich 63
Certainly a number of physicians really take exception to that. Their feeling is that they aren't people who can be bought and they'll prescribe what they want to prescribe. (84-87)
Peter questions whether this can be so. Dr. Hoffer rejects that this can be so: "[w]
e all know that's bull-don't we?" (158). On the other hand, Kitta argues that
physicians are capable of making their own judgments on these matters, for
instance when they listen to a presentation by a "hired gun speaker" (53-54).46
Opinions among participants diverge on whether the relationship between
psychiatrists and the pharmaceutical companies is an "arm's length relationship".
Kitta and Peter are not troubled by the relationship. Peter describes it as an arm's
length relationship (65). For Kitta, a psychiatrist's choice of medications isn't really
influenced by the companies, who are less intrusive today than in the past (53).
Pearl is much more conflicted and says that psychiatrists must ask if there is a vice
placed on them by the pharmaceutical company (80-83). She notes that they have
tried to suppress negative research findings and are in the business of selling
drugs (80-83). Dr. Hoffer expresses similar concerns, asking "[tlo what purpose"
is the drug company money being provided (172-78). He argues that so long as
researchers and physicians don't discuss alternatives, then the money keeps
flowing. Likewise, Marty states that the "problem is there has developed collusion
between psychiatrists in general and Pharma and often with the suspension of
adequate examination of the ethical issues and the concerns that are involved"
(106-09). Dolan (182,161), Marty (137-141), and Dr. Hoffer (419) are comfortable
discussing the lobbies and large political forces behind the industry.
How heavily should psychiatrists rely on pharmaceutical companies for
educational support, research support and free samples or tools? These questions
provoked a range of responses from participants. Not only is the relationship
improving, but according to Kitta (49-56) and Peter (58; 68), pharmaceutical
companies are doing good work by conducting research, promoting more tight
regulations around conflicts of interest, and providing educational opportunities.
Kitta argues that when they provide drug samples for patients to test, they are
often in need of a change and trying out new drugs could be an economic burden
for patients (51-53). For Pearl, the right thing for the companies to do would be to
provide drugs on a compassionate basis (80-101). Unlike his fellow participants,
46 The "hired gun speaker" is one who has received funding from a company in exchange for producing research results that are pleasing to the company.
Natasha Durich 64
Nelson appears not to be bothered by the relations between psychiatrists and
the pharmaceutical industry because the source of good information and good
monitoring technologies is immaterial (65-66). For Nelson, physician evaluation
and opinion, based on science, is the most crucial factor (68-69).
Dolan and Marty are the most vocal about the problems with the
pharmaceutical industry's assistance. The changes encouraged by the
pharmaceutical industry might not be in the best interests of patients, as noted by
Marty in the following statement (269-273):
It's just as likely that they [the pharmaceutical industry] could implement a change that may actually be harmful because more people are getting say antidepressants with mild depression that actually don't need them, are getting ill from the medications they didn't need in the first place and are having many other problems, which is actually a very common, prevalent problem.
Marty also feels that continuing education, if it is set as a priority, should be
funded by the government (145-50); it is "a ridiculous idea" (150) to have drug
companies control this education. According to Dolan, it isn't a question of
implementing minor changes, the very relationship itself ought to be examined
(188-92). The offering of online monitoring tools received mixed reviews from the
psychiatrists, none being surprised at the availability of such technology. It is
most important, according to Peter (162) and Dr. Hoffer (317-21), that a physician
attend to the patient's needs and observe them; a monitoring tool is not needed for
these tasks. Pearl didn't know if she would try it because she would question why
institutions don't use similar technology (74-75). It might just be another selling
gimmick. Dolan sarcastically comments that if he was into giving drugs, he'd love
that tool (156-61). He compares pharmaceutical companies with casino owners:
It's a lot like you can open countless casinos but as long as you have a phone number available for anyone who's got a gambling problem, it's all ok. (188-90)
Dr. Hoffer views it as a terrible compromise, "it's like putting foxes in charge of
the henhouse" (189-90). He recalls that in the United States, Eli Lilly will approach
a State and offer their monitoring of schizophrenic patients on contract, ensuring
that their drugs are used; they will send out instructions to the physicians.

Natasha Durich
Discussion
The willingness of medical professionals to accept the "generosity" of
pharmaceutical companies has received great criticism. For instance, Lexchin
(2001) and Kassirer (2005) have been vocal about the need to curb the alliance
between the pharmaceutical companies and the medical profession. For some
of the participants, relations between the pharmaceutical companies and the
psychiatric profession have been normalized. The relationship can sometimes be
justified by looking at the good that these companies do for the profession and for
patients. For other participants, the relationship is risky because of psychiatrists'
inability to maintain control over research directions and patient care. There was
limited concern with the role of the government in providing leadership in patient
health.
The participants, on various levels, discussed the interests of the
pharmaceutical companies and their feelings as physicians accepting the
"generosity" of these companies. Brody (2007, p.24) argues that medicine has an
internal morality, based on the standards of the medical community, whereas
pharmaceutical companies adhere to a different standard where profit is key.
In his view, the public would not accept an ethic that focuses on profit-making
as being the acceptable standard for medical professionals (p.24). For Brody,
the divestment strategy wouldsee physicians refusing freebies and perks from
pharmaceutical companies, with the relations between journal boards, academics
and medical societies and pharmaceutical companies being regulated based on
acceptable levels of investment (to be determined through careful scrutiny).
Similarly, under Freidson's (2001, p.218) conception of professionalism, "the
maximization of profit" is "antithetical" to its ethics. A political economy that
supports such a motive is working against this model of professionalism. Greater
support for the medical establishment by government and the public would
be needed to ensure that professionals can do the best work they can, without
undue interference from those with profit motives. Of course, this doesn't solve
the problem of "the greedy physician" who would work to bend the rules in her
favour regardless of the payer source.
Brody (2007) also discusses an interesting observation by Leonard Weber
(p.28): pharmaceutical companies are doing good by running successful
businesses that employ many people, providing potentially life saving medicines,
and doing charitable work. The case of ciprofloxacin is cited. In 2001, the United
States courts ruled that the company must provide this antidote to Anthrax

Natasha Durich 66
poisoning even if it means a loss of profits. Why? Anthrax poses a great danger
to public health. Some companies, such as Merck, do seemingly selfless work.
Ivermectin, a cure for river blindness, has been supplied to African nations for
free by this company.
What areas of corporate life demonstrate a caring, and profitable, business
ethics? Green initiatives encourage businesses to care about public health
by taking responsibility for environmental impact. For example, a company
may switch to using a more environmentally sustainable product in their
manufacturing. These changes take time to occur and are sometimes resisted.
However, the connection between profit and responsibility makes green
initiatives more attractive for corporations, coupled with regulatory intiatives
mandating penalties. If businesses can change their behaviour in a way that
serves customers, makes profits, and is gentle on the environment, then perhaps
pharmaceutical companies can bend their practices to reflect patient health and
safety concerns.
Basic Ethics vs. Ethics Plus (+)
Preview
Professional medical ethics could be divided into basic ethics and ethics plus.
The basic ethics is sufficient to fulfill one's legal and professional duties. Ethics
plus (hereinafter "ethics+") is the actor's sense of integrity and perceived ability
to use discretion, and their personal sense of honesty and judgment when doing
their work within the given social and institutional context. Basic ethics is the
codified sources of guidance. Ethics+ refers to a personal experience of doing
one's work with integrity, discretion, honesty and judgment. The context in which
one works has a symbiotic relationship with the actor's sense of ethics and ability
to make such judgments.
The Concise Oxford Dictionary (9th ed.) defines discretion as "(3) the freedom
to act and think as one wishes, usually within legal limits" (p.386). Ethics+ is
the professional's reflections on whether there is freedom to meet the ethical
standards to be best of his/her abilities. It is the professional's own sense of
fulfilling his/her duties. Integrity is also associated with this idea of ethics+. The
same dictionary defines integrity as "(1) moral uprightness; honesty" (p.707).

Natasha Durich 67
Ethics+ includes the professional's sense of honesty in fulfilling ethical duties.
These concerns impact how a person relates to him/herself as "professional".
What I have termed "basic ethics" might be best associated with Freidson's
(2001, pp.216-17) idea of "practice ethics", or those problems of ethics arising
from the work practice. The "ethics+" concerns are more closely connected with
Freidson's (1994) occupational principle, including "the informal attempts of
all workers.. .to do their work as they see fit on the basis of their own sense of
knowing how to do it"(p.73-74). These ethics+ concerns are among the "moral
problems of work" that Freidson (2001, pp.216-17) describes as being created by
"economic, political, social and ideological circumstances". These circumstances
are deemed to be part of "institutional ethics'; by Freidson.
An example might help clarify the difference between basic ethics and ethics+.
If a psychiatrist is working at a busy clinic, with limited resources and little time
available for each patient. Some of these patients have other pressing problems,
such as lack of adequate housing and food. Basic ethics can guide the psychiatrist
during the clinical encounter, creating obligations such as clear explanation of
treatment options and gaining informed consent to treatment. Ethics+ concerns
can easily arise in this case. The psychiatrist forms a perception of her ability to
make good ethical choices in these conditions, due to the social pressures and
limitations imposed by the biomedical model. She is faced with time pressure,
with limited treatment options, and with a small number of issues she can help
with. She may feel capable of doing more, of providing a higher level of care.
These are ethics+ problems.
Results
The participants discussed, in great detail, the concrete actions that
psychiatrists should take when treating patients with medication. Nelson
provided an almost textbook definition of the care involved in prescribing
medications: look for dangers of drug interaction, know your patient's drug
regime, take patient characteristics in to account, be cautious and not too
aggressive (42-46). He was also clear to point out that the patient's informed
consent is needed and the patient can withdraw it at any time (92). If a
patient does not want drugs, then the physician should treat the patient with
psychotherapy (78-81). Making yourself accessible and following-up are tasks
discussed by Kitta (56-59) and Dolan (104-08), who also mentions the necessity of
asking the right questions. Dr. Hoffer puts it simply: "giving patients whatever I

Natasha Durich 68
can following that old medical principle 'do no harm"' (12-13).
Despite an understanding of the ethical obligations, the problems involved
with wrongful prescription continue to impact patients. These problems are huge,
according to Dolan and Marty. For Dolan, the answer is short: "I think this whole
paradigm has to change" (136-37). Pearl mentions that many physicians have a
cavalier attitude towards drugs and giving these drugs has become normalized
(55-57). Indeed, she argues that a pill cannot do everything and when we set it up
as something that does, then problems arise (62-63).
For Marty, two important concerns emerge. First, psychiatrists have not
equipped themselves with the skills to deal with physical examinations of
patients (238-42). Second, "it's still up to the individual's ethical standards to abide
by the guidelines" (128-30). According to Marty (125-28):
The problem with those things [guidelines] that have been instituted is that they are voluntary and people disagree with them and decide that they are not willing to abide by them and there's not likely to be any consequences.
Peter, in contrast, says that psychiatrists "have a lot of what they need" (150) in order
to fulfill their ethical duties. Monitoring tools are available in British Columbia via
the PharmaNet resource, although none of the participants mentioned this tool as
something they were using or something that ought to be used.
One recurring theme in the interviews was individual physician responsibility
for ethical decision making. For Peter, it is a legal responsibility to keep patients
aware of the relevant information, including side effects, and there is sufficient
information and resources around the use of drugs. Dolan argues overmedicating
is "not being responsible" (106-08) and a person should not be allowed to
prescribe if they are irresponsible. Further, Dolan argues that "access to resources
depends on the degree to which the physician himself or herself accesses those
resources" (84-85). Nelson also mentions that the public expects high standards
and the professional must be responsible (48-49). Finally, Pearl mentions "the
individual psychiatrist should hold fast to psychiatry" (83). For instance, it takes
"personal resolution" to resist the drug company lore (52-53).
Dr. Hoffer takes an opposing view-any physician who fails to explore
alternatives is being irresponsible. He argues that "[all1 the double blind control
studies show that the efficacy of antidepressants is maybe 60% compared to
an effect of 50%" (96-98). Dr. Hoffer states, "it's physician ignorance rather
than negligence" (282) that causes problems with treating mood disorders. He
Natasha Durich 69
summarizes his position as follows (99-103):
... if you have any disease which is killing for which there is no treatment, you can try whatever you like so long as it is better than the alternative. But when you have an alternative which is safe and economical and can be used and practical and is not used, in my opinion it is malpractice.
The current state of psychiatric practice ought to change, in his view. Dr. Hoffer
sees "a total disregard for the patient" when physicians are using the drugs as
they are. A psychiatrist must also "be a good internist" (264-66). Dr. Hoffer would like the focus to be on helping patients lead normal lives. He
states, "My only conflict of interest is my desire to get people well" (153-54). He
finds it hard to understand why the word "cure" doesn't appear in the psychiatric
dictionary when he has a simple definition: "free of signs and symptoms, getting
along well with the community, getting along well with their family, and pay
income tax" (407-09). It's a problem that psychiatrists "don't even know when a
person is well or not" (410), according to Dr. Hoffer.
Kitta, Dolan, Pearl and Marty discuss concerns that are best thought of as
ethics+ concerns. Kitta notes that "it's a question of providing the best care
possible or good care for a larger number of people" (68-69). For Dolan, the
problem is doing psychiatry within the narrow confines of the disease model:
"this whole paradigm has to change" (136-37). At the end of the interview, he
describes a "loss of humanness" (271-72) in psychiatry and a longing for the
days when psychiatrists weren't pressured, by society and by the profession, to
prescribe medication or stop seeing a patient who refuses (250-58). He conveys a
sense of longing and grief by stating, "I have a loss in my heart for it [psychiatry]"
(315-16). For Pearl, the practice of psychiatry has become more managed and this
can take away from other important tasks. She questions, where is the bottom
line? Should it be patients, or dollars, or both? (95-96). Marty approaches the
issue from the point of view of one who practices psychopharmacology. These
psychiatrists did not start "necessarily because of the demand but because they
truly believe that this is the way for people to live better lives and to be free from
pain and suffering" (321-26). The participants had varied opinions on whether enough dialogue is
happening within the psychiatric profession around the ethics of prescribing.
For Peter, more dialogue is happening today than ever before, guidelines are
being published, and disclaimers are issued (80-99). Dolan takes the opposing

Natasha Durich 70
view, stating that within the medical profession it is difficult to have this kind of
dialogue (111-14): "the medical model doesn't lend itself to a lot of that". Marty's
views are more on par with Dolan's, stating that trainees have many chances to
discuss ethics but when in practice the opportunities dry up (160-63). He notes
"there is very little discussion of these kinds of issues" (180-81).
If there isn't an adequate dialogue happening now, is there any hope of
changing this situation in the near future? According to Marty, it is possible that
the Royal College of Physicians and Surgeons might set this sort of dialogue as
a priority, perhaps as part of the requirement for continuing education (184-87).
Marty is not hopeful, especially in light of the absence of discussion around
serious issues, such as legal proceedings against local psychiatrists involved
in patient sexual assault (171-76). Dr. Hoffer is even more skeptical, saying that
Canadian psychiatrists would simply ask for more money, claiming that they are
doing the best they can when confronted with allegations of doing an inadequate
job (485-86).
Discussion
Medical ethics are steeped in tradition and the duties of physicians are
relatively well known and articulated in the various Codes of Ethics, Policies and
Guidelines of the Colleges of Physicians and Surgeons and Medical Associations
(see "Regulating Prescribing Practices of Psychiatric Professionals, Do No Harm:
Professional Medical Ethics" above). Gain fully informed consent before treating a patient. Above all, do no harm. When you cannot perform adequately, you should not perform the task but refer the patient to another physician. Each physician is responsible for carrying out these duties, or face internal and sometimes legal consequences. Give the best possible medical care-a physician has a fiduciary, trust-based relationship with the patient. These fall under the purview of basic ethical concerns.
A paradigm change and the need for individual responsibility are two key
points raised by the participants. The control of wrongful prescription and
its accompanying problems are challenging because their roots are in the use
of prescription medications. Perhaps this standard needs closer examination:
are these drugs being overused and are we focusing too much energy in this
direction? Individual physician responsibility is a problem but it seems to be a
truism at first glance. Without personal dedication to high practice standards and
to ethical treatment, a physician will cause harm. Knowing the principles of ethics
does not always translate into good actions.

Natasha Durich 71
The reality of practicing modern western medicine-in this case, psychiatry-
is that physicians are not one wo/man shows. Gone are the days when the
physician arrives at the door of your home, black bag in tow and sometimes
hospital carriage on stand-by. Instead, the physician operates within a larger
system, with administrators, billing agents, research scientists and patient/
consumers making distinct demands. Kitta, Dolan, Pearl and Marty's ethics+
concerns highlight the strains of working within this larger system.
Denney (2003) calls today's professionalism a "managed form of
professionalism" (p.74). For Freidson (2001), reality is a mixture of managerialism,
consumerism and professionalism, the three logics. The personal experience of
the worker can get lost amidst such discussions. Perhaps that is why Freidson
talks of the soul of professionalism as tied to making free choices: what attracts professionals to their work, what motivates them to do good work, and why do
they use their discretion to work in novel ways thereby changing practice for the
better?
Conflicting opinions emerged as to whether there is sufficient dialogue
around the ethical concerns involved in prescribing antidepressants and
antianxiety drugs. Without a priority being set for the discussion of these matters
throughout a physician's career, it is difficult to foresee any changes being made
in this direction. In order to set this as a priority, there must be some level of
agreement that a problem exists and deserves time and attention.
The Future of Psychiatry
Results
The participants were asked to speculate as to what the next fifty years might
hold for the work of psychiatrists. For Kitta (82-89), Pearl (106-08), Nelson (84-
88), and Dolan (279-98), a future where psychiatrists are reduced to the role of
dispensing drugs is bleak and they express discomfort with this prospect. Nelson
and Dolan also express the loss of humanity involved in resorting to the use of
computers in providing psychiatric treatment to patients. The ability to pinpoint
specific causes and offer more targeted treatments, especially for the most serious
mental disorders, was discussed hopefully by Peter (271-81), Pearl (104-05), and
Kitta (82-89). The integration of biological, social and emotional factors, on a larger
scale, was discussed by Pearl (99-105).
Dr. Hoffer is optimistic that orthomolecular medicine will become mainstream

Natasha Durich 72
but it will "be very slow and tedious, with a lot of infighting and bickering with
the drug companies doing their level best to protect this information" (494-96).
He states, "I'm hoping that it [psychiatry] will be a lot more sane" (478). He also
advances an idea of slow change, where people advocate for a better means of
treatment. Dr. Hoffer notes, "I think it's going to take fifteen to one-hundred years
before we become so intelligent that we realize that we mustn't harm our people"
(197-98).
Another changing aspect of the profession, noted by five of the participants,
is the impact of the shrinking number of psychiatrists. This is partially due to
mass retirements and a low number of new recruits. Peter (273-78) and Marty
(375-77) express the view that as the numbers of psychiatrists decreases, other
helping professionals will take their place. Peter speculates that the role of
psychiatrists may become more focused on the medical model, while others will
deal with the psychosocialspiritua1 components of patient care. Marty argues
that the replacement professionals are "less expensive and more valuable". The
young psychiatrists who are entering practice are viewed with a critical eye by some participants. Dolan, who views himself as "a dinosaur in a sense", feels
that the younger professionals are "more into money, technology, the business':
which makes psychiatry "a different sort of animal" (285-89). Pearl hints that
the "younger generation are in touch with different things" (106-07). For Dr.
Hoffer, "[tlradition is so important in medicine" (382-84) and the medical schools
are "letting the drug industry take over the teaching of how to use drugs"
(182). Therefore, Dr. Hoffer does not feel that psychiatrists are taught any new
approaches or alternatives to treating mood disorders.
Speaking for psychiatry in general, Marty and Dolan offer two visions for
the future. Marty comments on the necessity of psychiatry to respond to the real
concerns of the population and work with other professionals in order to solve the
problems at hand. In Marty's words (352-54):
I think that psychiatry is at a kind of cross-roads. It will either respond to the real needs so that the population can survive or it will suffer a lot and will become extinct, or become even less relevant than it is now.
Dolan, in contrast, looks at the quality of treatment being provided at the
physician-patient level. For Dolan, the answer lies in rediscovering the aims of
treating patients (300-02):

Natasha Durich 73
I would love to have nobody to see. Truly. That is what I hope for. I hope that the helpers and healers become real helpers and healers. Which really hasn't got anything to do with pushing buttons and writing prescriptions.
That's what I hope for.
Discussion
Some participants express faith in the power of science to advance such that
better treatments are found, more specific and smarter. There seems to be a
hopefulness on the part of some of the participants that psychiatry can survive
and not deteriorate into a profession where physical science is the only form of
practice. Of course, for Dr. Hoffer, this would be the best case scenario because
physical causes are key to treating our mental problems. For Dolan, this would be
the worst scenario because psychiatrists would not be acting to their full potential
as "healers". Dolan views mental problems as complex, irreducible to purely
physical causes. These questions are real because the death of institutions and
their grizzly afterlife is a probability, as evidenced in Beck 's (1994) conception of
"zombie institutions" (p.40). For Marty, psychiatry is already becoming useless
for many people and a critical direction must be turned. Furthermore, most
participants were not optimistic that the next generation of psychiatrists would
fair any better than the current generation of psychiatrists at proving the value of
the profession to the public.

Natasha Durich
CHAPTER FOUR: IMPLICATIONS
The Re(viewing) the Research Process
For this project, I conducted individual, face-to-face qualitative interviews with
seven psychiatrists from Vancouver, British Columbia and the surrounding area.
In this flexible and emergent process, I was guided by two mission questions.
First, what, in the views of the psychiatrists, is the impact of prescribing mood
altering drugs on their practice of psychiatry? Second, what, in the views of
the psychiatrists, are important or needed ethical obligations when prescribing
these drugs? I opted to use the Framework method of analysis (Ritchie, Spencer,
O'Connor, 2003) as a means of organizing and dissecting the data. The approach
provided a means of making sense of the viewpoints of Kitta, Dolan, Marty,
Nelson, Pearl, Peter, and Dr. Hoffer. I also intended to provide sufficient details for
readers, so that others can draw their own meanings from the data.
This project has various limitations. The seven case studies presented cannot
provide, nor are they intended to provide, a representative view of psychiatrists
in British Columbia, or elsewhere. A researcher who has connections within
the local community, or perhaps using online survey methods which are less
time consuming than interviews, might be able to achieve a higher participation
rate. However, survey methods do not always ensure high participation, as
evidenced by the Mayo Clinic study (Lineberry, 2007). In addition, the aim of
protecting participant confidentiality seemed to limit the workability of the
chain referral sampling technique. Utilizing an informant, who would make
connections and contacts, might be one means of improving on the sampling
for this kind of study. The majority of participants are male. The psychiatrists
are also seasoned to the work, which might impact their views of this problem.
Hence, different psychiatrists in different locations, at different stages of their
careers, might hold differing opinions on the ethics of prescribing. Likewise,
a closer focus on comparing different jurisdictions and their efforts to address
wrongful prescription could assist us in understanding the problem. I also could
not address a number of important concerns, including the impact of gender and
concurrent substance abuse problems.
This study presents the views of a limited number of psychiatrists who
chose to participate in the research. Many psychiatrists contacted declined to
participate. The views of these others might be very different from those of the

Natasha Durich 75
psychiatrist participants. It can be speculated that they have little problems with
the way antidepressant and antianxiety drugs are being used, or that they feel
the administrative and legal bodies responsible for overseeing negligence are the
ones tasked with finding solutions to any concerns. Alternatively, they might have
declined due to time constraints or simply not wanting to be interviewed, yet they
may share similar concerns.
To be of any merit, a qualitative study must be judged to be trustworthy.
Providing varied bases of comparison would be one means of bolstering the
trustworthiness of this study. As noted by Arskey and Knight (1999, p.21), "rather
than just gather[ing] data from one particular group with an interest in the study,
you could seek out the views of several sets of stakeholders and, in that way,
provide a comparative aspect". This is triangulation. Possibly non-psychiatrists,
naturopaths, pharmaceutical industry experts, or patients would have different
points of view. Focus groups with different stakeholders, possibly through an
online venue, would be a start in the direction of opening up dialogue, possibly
representing a form of action research. Observing behaviour in a clinical setting
would also provide validation of the ideas shared by the participants.
Dependability and credibility would be bolstered if participants could be
given a greater opportunity to explain their ideas. One means of clarification
would be for the researcher to do more work at the front-end of the study,
gaining psychiatrist meanings and then drafting appropriate questions. Another
possibility would be to ask participants to create maps of their ideas about ethics, such that the complex ideas are made more understandable to others. The keeping
of an ethics journal might also be one way of receiving a time sensitive account,
one that might be alive with examples and greater detail. The provision of
scenarios for comment might also allow for more in-depth questioning.
Rekapturing) Participant Opinions
Psychiatrists work with patients who are generally more active in the
relationship than their counterparts of fifty years ago. It is generally viewed as
a good thing for patients to be in agreement with the treatment and show an
interest in the treatment plan. The growth of the internet and advertising access
by pharmaceutical companies have expanded the transmission of marketing
information about the newest drugs. Many participants questioned the quality
of the information that patients could access. Dr. Hoffer argues that patients
have been offered the message of "one disease one drug" (445-46). Furthermore,

Natasha Durich 76
patients are able to be active participants to varying degrees, given the severity
of their illness and personal factors. It seems that patients continue to experience
stigma due to their diagnosis, although that stigma might be lessening given the
growth in the number of persons taking mood altering drugs and the biological
approach yielding the ability to medicalize depression and anxiety.
Patients sometimes require convincing by their psychiatrist to take the
prescribed medication. Some psychiatrists worry that the explanations offered to
patients are only somewhat truthful. Whether an antidepressant or mood altering
drug is as effective as insulin is for treating diabetes obscures some important
concerns, namely the social factors involved in mood disorders and the relatively
low success rate of antidepressant drugs over placebos. Relieving self-blame is
also of importance but some care is needed to remain truthful. Another concern
is the relative lack of alternatives and patient-focused information sources. Dolan
questions this, stating that psychiatrists can access other resources but they might
be unwilling to do so (84-85).
There is concern by some that psychiatrists have placed "unwarranted faith"
in medications and have a cavalier attitude when it comes to prescribing (Pearl,
54-57). For Dr. Hoffer, medication can be "helpful" but "it's being used to the
exclusion of everything else" (48-49), namely safe, economical and practical
vitamin and mineral therapies (99-103). This faith in medications might stem from
the growth of science side of psychiatry. Marty argues that psychiatry responded
with "scientism" and "it was like the emperor's new clothes" (331-35). Hence, some
psychiatrists feel comfortable narrowly focusing on prescribing drugs and various
combinations of them, sometimes overdosing patients, because they believe in
that science and feel "they aren't people who can be bought" (84-87). Therefore,
psychiatry is "at a wonderful and scary place" (Kitta, 94). The growth of new
technologies are opening up clues to how the brain functions and this might lead
to more specific remedies for serious disorders. On the other hand, scientism with
a blind faith in medication to the exclusion of other issues can yield a cold brand
of pseudo-psychiatry. A brand that shows psychiatry to be self important and
losing relevance (Marty, 371-75).
The need for individual physician responsibility is a key point made by the
participants. Peter argues that physicians "have a lot of what they need" (150) to
fulfill their duties. The participants also viewed pharmaceutical companies with
skepticism and had mixed reactions about their involvement in medical care. The
research dollars and samples can benefit psychiatrists and their patients, and the

Natasha Durich 77
capacity for conflicts of interest have been discussed and guidelines drafted. On the other hand, the aim of drug companies is to generate dollars, not safeguard
patient wellbeing. Dolan likens this to casinos who are doing good so long as
they open a phone line for problem gamblers (188-90). For Marty, net-widening
is a "very common, prevalent problem": people with low levels of depression are
medicated and they don't necessarily need medication.
Individual psychiatrist responsibility for patient harm due to wrongful
medication is stressed. There was also concern expressed around institutional
ethical concerns-those social and economic factors that impact ethical choices.
This is the point where ethical action meets one's feelings on their ability to meet
those goals, within a given social context: ethics+ concerns. The toss-up between
providing good care for many or the best care for the few (Kitta, 68-69), the
administrative work that surrounds work in some clinics (Pearl), and the push
for providing physical treatment (Dolan) were mentioned as significant concerns.
Individuals too need guidance and speaking about ethical concerns is one
component of generating solutions to the problem of wrongful prescription. There
may be more dialogue happening today about these ethical concerns than years
ago, but is there enough dialogue, what is the subject matter for discussion and at
what stage of the professional career does that occur?
Marty also notes that the individual psychiatrist is largely responsible for
his own ethical commitments because the regulations are voluntary (125-28).
Although regulation on ethical matters may be left up to the individual, Dr.
Hoffer would argue that in the "church of psychiatry", the heretics are quickly
dealt with through excommunication, at great personal and professional peril
(357-60). He notes the rigidity of those rules as they relate to some physicians who
lost their licenses for their practice of orthomolecular medicine. The utility of legal
sanctions and the responsibilities of the government were only mentioned briefly
in a few of the interviews.
The history of psychiatry shows the great malleability of this science.
The chameleon changes its appearance to suit its surroundings as a defense
mechanism. Perhaps the many appearances of psychiatry is also a defense
mechanism for the survival of this profession. For Marty, "psychiatry is at a
kind of cross-roads" (352-54). A greater understanding of the physical factors
involved in depression holds the promise of providing more focused treatment
options. Is it possible to ensure that people don't get lost (Pearl, 54-55) amidst
growing interest in (and some say exclusive use of) the biomedical approach. Will

Natasha Durich 78
psychiatry respond with more than simply some new clothes, holding remedies
out before the public as cure-alls. If, as suggested by Dr. Hoffer, the "foxes [are]
in charge of the henhouse" (188-go), then what might this mean for psychiatry's
future. Will the role of psychiatrists be relegated to distributing medications and
conducting research on the brain? Can it, and should it, aspire to be more?
Re(assemb1ing) Insights
Patient Characteristics and Drug Treatment
The distinction between expert and lay knowledge is problematic (Morant,
2006, p.833) because medical judgments are seen as involving a "ubiquity of
values" (Veatch, 1990). The fiction of the "informed patient" casts further doubt
on the once sacred place of physician opinion. This fiction depends on a patient
who is interested and able to inform themselves, who is articulate and willing to
challenge physician authority, and on a physician who is open to that dialogue
(Henwood, Wyatt, Hart & Smith, 2003, p.164). This fiction is even less believable
when you have a person who is often judged to be of unsound mind, and whose
access to resources and ability to research health matters might be limited. Veatch
(1990) argues that within this context, the practice of writing prescriptions will
"collapse as [a] conceptual muddle" (p.24). If freedom and safety are not matters
for physician judgment (Veatch, 1990, p.32), then the need for equity within the
physician-patient relationship becomes crucial (Henwood et al., 2003, p.604).
Bioethics seems to suggest that psychiatrists ought to be concerned with
patient collaboration, which serves to invite trust on the part of the patient.
The place of power and values within the relationship is not highlighted to the
degree it deserves. How close does the psychiatric clinical encounter approach
a negotiation, with the "maintenance, restoration, or promotion of the patient's
autonomy" being "determined by negotiation" (Childress & Siegler, 1984, p.141)?
If I were entering into negotiations, I would choose a seasoned mediator, armed
with the best information and the best rhetorical skills to represent me. Patients
do not have such an option. The packaging of the partnership metaphor fits
the development of the fiction of the "informed patient", who arrives ready for
mutual participation and a sharing of power in the interdependent interaction.
The compromise and exchange of services, made visible by the rational contractor
model, are largely hidden in the partnership metaphor. Although the therapeutic
goods of having a patient as a partner in their own health care cannot be

Natasha Durich 79
overlooked, a metaphor or model capable of capturing the power dynamics
involved and the conflict inherent in the relationship would be useful.
What kind of a future worth living is being offered to patients with mood
disorders (Mattingly, 2004, p.74)? Are patients encouraged to consider possible
alternatives to accepting drug treatments as remedies for their mood disorders?
Atkinson (1994) argues that "the production, reproduction and use of medical
knowledge" (p.113) is the work of physicians, who use "written and spoken
rhetorical formats" to convey meaning (p.115). The prominence of the disease
model (McHugh & Slavney, 1998, pp.14-16) and weighing of risks creates
challenges for psychiatrists faced with a more questioning patient population. The
perfect patient is one who is aware of the possibilities for treatment, can actively
take part in education, and is capable of self-care (Becker, 2005) and monitoring
to ensure the chosen treatment is carried out. The impact of such regulation on
one's life must be a weighty prospect (Busfield, 1996, p.233), and it is often one that
remains hidden until the patient has accepted treatment and is living with the
label of "mood disorder" (Penfold & Walker, 1983, p.188).
The grand claims of drug manufacturers, without the associated years of
research required to make valid and reliable claims on efficacy of some of the
drugs, seem to encourage anyone feeling sad or worried to ask their physician
about a drug remedy (Van Praag, 2003). Patient illness falls on a spectrum
of severity, as does psychiatrist intervention in terms of invasiveness and
restrictiveness. "Therapy of the normal" (Castel, Castel, & Lovell, 1982, p.263) is
not abstract, living within the pages of a science fiction novel, but seen creeping
into reality with the growth of lifestyle drugs (Lexchin, 2001) and the expanding
base of disorders in the Diagnostic and Statistics Manual (Kirk & Kutchins, 1992,
pp.10-11). Drug companies, with their focus on expanding profits, are providing
new drugs for whatever ailments are seen as "medicate-able". For patients
who arrive at the office of a psychiatrist, the physician provides an important
schema for understanding their problems. Hence, very characterization of a
mood disorder is an important concern, as there is a vast difference between the
analogies of "a broken car" and "taking insulin for diabetes". Therefore, guarding
against "therapy of the normal" is another important concern when discussing
patient sophistication.
The collusion between the pharmaceutical industry and psychiatry casts
an ugly shadow on fiduciary obligations. It is easy for psychiatrists to be
armed with drug company materials, promoting SSRIs (see Appendix 1: Classes

Natasha Durich 80
of Antidepressants) as the best treatments (Brody, 2007, pp.300-04). It takes a responsible psychiatrist to maintain an eye toward providing more. Although
some psychiatrists would take offence to the suggestion that they can be anything
but objective (Brody, 2007, pp.37-38), patients are depending onthe strength of
the convictions of their psychiatrists. This is echoed in the caution provided by
the Royal College of Physicians and Surgeons of Canada to eliminate conflicts
of interest and minimize or eliminate their effects when they cannot be avoided.
Although it seems that many psychiatrists would be aware of the dangers of
conflicts of interest, the more subtle harms created by limited resources and
treatment options are more difficult to create awareness around.
As one of the three logics (Freidson, 2001, p.181), professionalism demands
that the professional remain the bastion of sound information, academic freedom,
and trustworthiness. The further one strays from these ideas, the more open to
questioning professionals become, casting doubt on their claims of exclusivity and power over their field of information and technology (Freidson, 1994, pp.173-75).
Doubt on the part of patients and other members of the public need not paralyze
the growth of psychiatry, but provide a reconsideration of how drug treatments
are related to doing psychiatry (Becker, 1996, p.33). Careful and controlled
prescribing, and a questioning of this approach (Leszcz, 2001), thwarts fears that
psychiatrists are gambling with patient welfare.
Monitoring Patients, Information Keeping, and Aggressive Prescribing
Principles of Management (Reesal & Lam, 2001) and Codes of Ethics (Canadian
Medical Association) put into words the ethical obligations of psychiatrists when
treating patients with mood disorders. An approach that relies on the provision of
antidepressant and antianxiety drugs necessitates the need to physically examine
patients, a task that was remiss with the older talking therapies. The addition of
administrative tasks and managed work (Denney, 2003), the patient-per-hour fee
schedule, and a general partition of each individual health care professional into
separate working units provides further pressure on psychiatrists working within
that context. Problems with record keeping should be red flags (Atlantic Provinces
Medical Peer Review Program). The pharmaceutical companies along with the
government (PharmaNet British Columbia) have tried to step-in in various ways,
to assist in the management of patients with mood disorders.
Drug safety, especially post market surveillance, and aggressive prescribing,
such as over-dosing patients, raise serious concerns for patient welfare (Little

Natasha Durich 81
Helpers, 2003). Despite the ethical language "do no harm", patients are taking a risk
when using drugs that have unknown long-term side effects, at the upper limits
of the acceptable range. The element of prevention of wrongful prescription seems
to be dealt with at the education phase of professional life, where psychiatrists
are learning the fundamentals of using these drug treatments and the associated
ethical approaches. For the practicing psychiatrist, it is unclear what continuing
education happens around wrongful prescription.
When patients do experience physical harms, emotional impacts, and social
repercussions from taking the drugs (Breggin, 1991; Chetley, 1995), where can
they turn for assistance, assuming they can reflect on the source of the harm?
The courts in Canada have not been generous and there is no guarantee that the
Colleges will discipline their members and raise awareness of the misbehaviour.
Ignorance of the harms caused by wrongful prescription weakens psychiatrist
claims to a strong commitment to professionalism, giving credence to those who
prefer the other two logics of managerialism and consumerism (Freidson, 2001,
p.181). The ability of business ethics to account for public safety concerns is a
new territory, especially for pharmaceutical companies (McHenry, 2006). It is
predicted that the percentage of persons with diagnosed mental disorders will
continue to rise. This expanding potential market for drug consumers must be an
attractive prospect for pharmaceutical companies. Growing questions concerning
the goodness of these drugs, coupled with skepticism surrounding the close
relationship between the medical community and the drug industry, might spur
another consideration of commonly held ideas of the best way to market and
sell pharmaceutical drugs. Accountability for drug manufacturers is another
key to changing the ways that drug companies do their business. Examining
the parallels with environmental regulation might expand our notions of the
marriage between profit and care, as well as the importance of setting acceptable
standards of safety and the importance of prevention. Whether we can learn
from these parallels is uncertain because the harms due to wrongful prescription
are often seen as driving from expert opinion, in an effort to help (regulate) sick
people. The larger connection to health and wellbeing are sometimes masked.
The Future of Psychiatry
Psychiatrists and the profession of psychiatry is embedded within an ever-
changing social context (See Appendix 6: "Doing Psychiatry" (Contextualized)). The

Nafasha Durich 82
challenges are, in part, created by interactions with a questioning public and
managers of medical work (Denney, 2005), the doubt cast by the discourse of
risk (Beck, 1994), the questioning within bioethics of the superiority of medical
judgment (Veatch, 1990), and the impact of the pharmaceutical industry on the
shape of medical thought (McHenry, 2006; Brody, 2007) and on the fiction of the
"informed consumer" (Henwood et al., 2003). What is the role of the psychiatric
professional in this changing context? Control over one's work and the importance
of establishing legitimacy and credibility as professionals are key issues to watch
in the future.
The ethics+ concerns discussed by participants seem to be an indication of
the desire for change in how physicians are "doing psychiatry" today. Macro-
level theorizing about the goodness of ethical precepts and the induction of
improved regulatory systems are only a couple of pieces to resolving the problem
of wrongful prescription. The daily efforts of psychiatrists and their sense of
how they make ethic judgments, within the social and institutional context in
which they work, is a crucial part of our understanding of the problem. The
cultivation of self-awareness in terms of the work we do, in relation to the context
in which that work is done, is one step toward encouraging ethical examination
of professional practice. Ethics+ concerns underscore the importance of viewing
ethics not as a static collection of codes coupled with punishments, but as a living
enterprise impacted by the actions of those who do the regulated work. Perhaps
we can borrow a metaphor from Lord Sankey who opined, "the BNA Act planted
in Canada is a living tree capable of growth and expansion within its natural
Our ideas about medical ethics should be equally fluid and open to the
ideas of ethics+, which highlight the symbiotic relationship between social context
and professional integrity and judgment.
I am left with one overpowering conclusion at the end of my research:
"psychiatry is at a kind of cross-roads" (Marty, 352-54). In what direction will
the pendulum shift and what place will patient safety and wellness hold in the
psychiatric toolkit of the future? Speculating on the future of psychiatry allows
us to place our hopes and fears in full view and speak about the essence of
psychiatry. What is necessary to doing psychiatry? What is necessary in order for
professionals to do their best, in terms of patient care and research, and for job
satisfaction to remain high? The actions and (in)actions of individual psychiatrists
47 Eduxlrds v. A-G. CanadaI [I9301 AC. 114,136.

Natasha Durich 83
are key for the scientific breakthroughs projected (targeted treatments, mapping
of the brain, gene therapy), as are they instrumental for preventing horrors
(irrelevant outlook, lack of coordination between disciplines, over-focus on
physical treatment). The battle for the "soul of professionalism" (Freidson,
2001, p.217) is waged not in the public sphere, the legal realm, or even in the
marketplace. It is waged daily by the physicians who practice and create what
we know as psychiatry, within the boundaries created by our social relations
(Busfield, 1996, pp.53-60). Time is needed to witness whether the words of Lewis
(2003) will hold truth for psychiatrists: "it is not that medicine is simply wrong or
bad, it is more that medicine is too powerful, too hegemonic, too self-serving, and
too unresponsive to alternative points of view"(p.60). The question is how long
those harmed by wrongful prescription can wait for answers and solutions to
their problems.
Farewell Glance
The piece of shiny Apo-Clozapine origami sits beside my desk. A gentle reminder
of the many ways the pharmaceutical industry reaches people. Although not
a practicing psychiatrist, their message reaches me. I pick up this feather-
light abstraction and invert it. Inverting their message too. I question how the
world of medical ethics is being transformed by the relationships between the
pharmaceutical industry and the medical profession. I question how many
physicians have folded and unfolded this object's many kin. Perhaps their
questions are not so different from my own.

Natasha Durich 84
APPENDIX 1: CLASSES OF ANTIDEPRESSANTS4*
TRICYCLIC ANTIDEPRESSANTS
First antidepressants (1950s)
Receiving neurons get extra stimulation, helping to regulate the levels of the neurotransmitters norepinephrine and serotonin
Sedating and alerting properties Side effects and hazards include: faintness (falling of blood pressure),
confusion, constipation, difficulty urinating, rapid heart beat, weight gain,
drowsiness
SSRI (SELECTIVE SEROTONIN REUPTAKE INHIBITORS) Selectively raise serotonin levels in the brain
Marketed as being nonaddictive and nonsedating
Pregnant women should use with caution because newborns may
experience adverse effects Side effects and hazards include: may be at risk of harming self or someone
else, vomiting, diarrhea, insomnia, anxiety, tremor, loss of sexual desire
MA0 INHIBITORS Monoamine oxidase inhibitors inactivate an enzyme that normally breaks
down neurotransmitters, leaving more neurotransmitters available for use Atypical symptoms are often treated with this class of drugs
Side effects and hazards include: consumption of tyramine rich foods leads
to adverse effects, faintness, dizziness, headaches, insomnia
OTHER REMEDIES
Lithium (bipolar disorder); St. John's Wort
48 Source: Merck Manual of Medical Information, Home Edition, 17th Edition (2000), from http://www.cbc. ca/news/background/mentd-hedth/depression-medicaito.html (October 17,2006, CBC News)

Natasha Durich
APPENDIX 2: LETTER OF INTRODUCTION
[letter head] School of Criminology
Simon Fraser University
8888 University Drive
Burnaby, British Columbia
V5A IS6
Date
Dear Dr. Xxxxx:
I teach at the School of Criminology at Simon Fraser University, and I am a
member of the Law Societies of British Columbia and Alberta. Natasha
Durich, one of my graduate students, is doing her Master's thesis on the
prescription of antidepressants. She holds both a B.A. (Psychology and
Philosophy) and an LL.B. from the University of Victoria. Natasha is interviewing
local psychiatrists on this topic, and I hope that you would assist her by granting
her an interview.
The focus of Natasha's questions will be psychiatrists' opinions on the
prescription of antidepressant and antianxiety drugs and the ethical
guidelines surrounding such practices. Your opinions would greatly
contribute to an understanding of such matters.
The in-person or telephone interview requires approximately one hour of
your time, to be set at a location of your choice. Your contribution to her
research will be kept confidential and anonymous, through the use of
pseudonyms and removal of identifying information.
If you have any questions or concerns about this project, I can be reached
at by email (XXX) or telephone (XXX). Natasha can be reached at XXX (or XXX). She will be in phone contact within the next week to request an interview. Your
participation would be greatly appreciated.
Sincerely,

Natasha Durich
APPENDIX 3: INTERVIEW SCHEDULE
Introductions
Nature of the research-psychiatrists views on prescription drugs and
their assessment of ethical guidelines around the use of prescription
drugs.
Purpose-to assist in my academic work, forming the basis of my MA
thesis.
Discuss confidentiality, anonymity, and ensure that they voluntarily
wish to participate.
Tell them that they can access my thesis upon completion.
Get permission to tape record the conversation.
(A) Preliminary Questions: Background
1. How long have you been practicing psychiatry?
2. Have you used antidepressants and antianxiety drugs as part of your
treatment plans?
3. Could you describe the work you do briefly? What kinds of mental disorders do you treat?
What brought you to work at XXX?
(B) Questions stemming from mission question #1 (How do clinical
psychiatrists view the impact of prescription drugs on their practice of
psychiatry): Context
1. What are your thoughts on psychiatrists asking patients to take
greater responsibility for managing their use of antidepressants and
antianxiety drugs?
What sorts of activities would management include?
Do you think this is common?
What are some of the obstacles involved in this approach?
Do you encourage patients to do their own research?
Do you feel this approach is useful?
2. Have your patients requested drugs by name? How do you feel about
these requests?
3. Some patients make the comparison between taking medication for
their mood disorder and other patients with physical illnesses (such as

Natasha Durich 87
diabetes) taking medication for their disease (such as insulin). Do you
feel that such comparisons are helpful?
Do you feel that this impacts their sense of responsibility?
(C) Questions stemming from mission question #2 (What guidelines or
ethical principles do clinical psychiatrists view as important in their use of
prescription drugs): Ethical Concerns
1. Some ethical problems resulting from the use of these drugs include
failure to monitor medications, overmedication, conflicts of interest, and
the severity of reactions caused by the medications.
i. What responses are you seeing from your profession in
addressing these ethical concerns?
Some people have suggested that the relationship
between drugcompanies and the medical profession
is at arm's length. Howwould you respond to this
statement?
Do you feel that providing education and sample
drugs is goodpractice or necessary?
Do patients have access to safe alternatives?
ii. Do these ethical concerns receive enough discussion?
Do you feel there's a way to discuss them more?
2. What other things do you think pharmaceutical companies can do to
help minimize the potentially harmful impacts of their drugs? For example, the makers of apo-clozapine, a drug requiring
careful monitoring, have created an online tool that allows
physicians to track patient blood levels. Do you feel that this
is helpful?
(Dl Conclusions
1. There have been many changes to the face of psychiatry within the past
20 years or so. What do you think the historians of the future will note
about this time period for the profession of psychiatry?
2. If you were asked to project 20 or 30 years, even 50 years, into the
future, what do you think the work of psychiatrists will look like?

Natasha Durich 88
(E) Wrap-up Do you have any general comments about our conversation you'd like
to add?
Could you recommend any other psychiatrists who might wish to be
interviewed? (any psychiatrists with diverging opinions?)

Nu t u s h Durich
APPENDIX 4: CONCEPTUAL FRAMEWORK
(1) Personal Details
1.1 Years in practice
1.2 Years as a general practitioner
1.3 Administrative work
1.4 Other
(2) Patients
2.1 Sophistication (information, knowledge, resources)
2.2 Active patient (questioning, researching, requesting)
2.3 Physician-patient collaboration (sharing, educating)
2.4 Other
(3) Drugs
3.1 Utility
3.2 Cost-benefit analysis
3.3 United States drug regulations
(4) Pharmaceutical Companies
4.1 Changes to conflict of interest (the good old days)
4.2 Pharma companies as businesses
4.3 Positive relationships with physicians?
4.4 Skepticism by physicians regarding motives of Pharma companies
4.5 Role in improving patient care
4.6 Other
(5) Ethical Obligations and Concerns
5.1 Responsible physician
5.2 What is needed?
5.3 Sense of integrity

Natasha Durich
5.4 Factors external to professional responsibility 5.5 Dialogue within the profession 5.6 Other
(6) Views on Mental Disorders
6.1 Complex model 6.2 Stigma 6.3 Value to patients of comparing mental disorder with other illness 6.4 Other
(7) Views on Psychiatry
7.1 Art and science relationship within psychiatry 7.2 Feeling on changes 7.3 Hopes for the future Z4 Other
(8) Other key issues not covered
NOTE: Concepts 2,3,5.4 and 6 (not 6.1) are combined to form a meta-concept "Context Informing Ethical Decision Making"
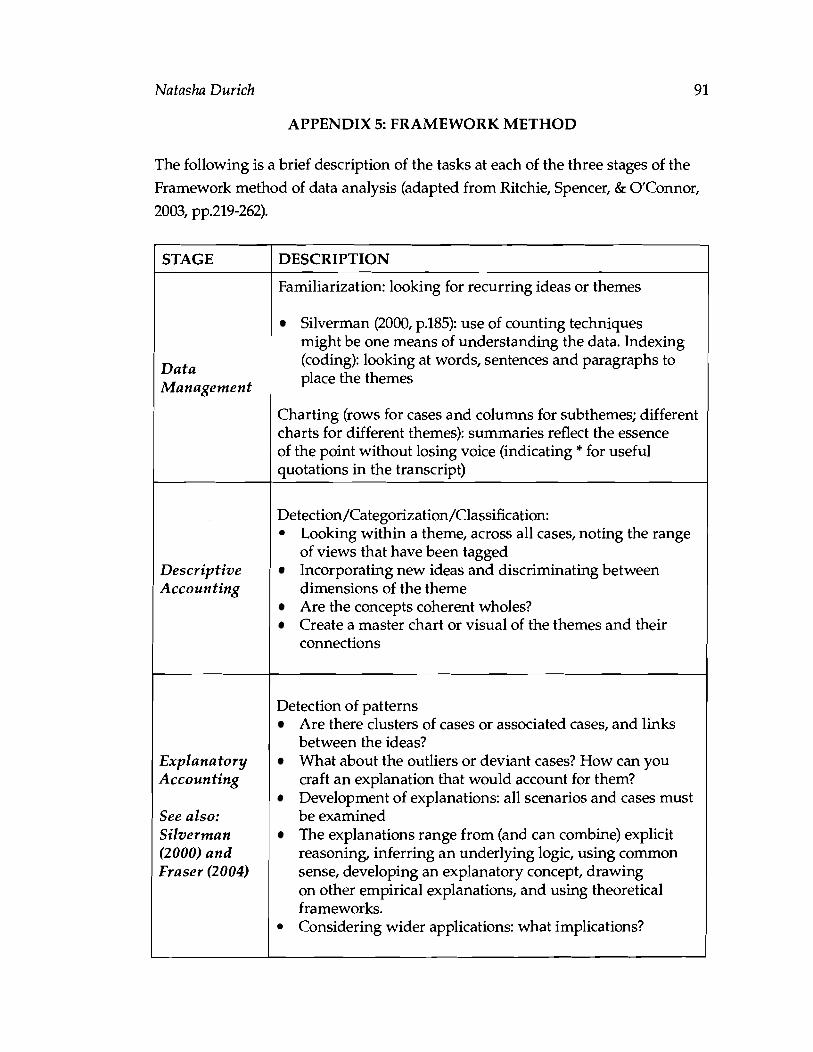
Natasha Durich
APPENDIX 5: FRAMEWORK METHOD
The following is a brief description of the tasks at each of the three stages of the
Framework method of data analysis (adapted from Ritchie, Spencer, & O'Connor,
I STAGE
Data Management
Descriptive Accounting
Explanatory Accounting
See also: Silverman (2000) and Fraser (2004)
DESCRIPTION
Familiarization: looking for recurring ideas or themes
Silverman (2000, p.185): use of counting techniques might be one means of understanding the data. Indexing (coding): looking at words, sentences and paragraphs to place the themes
Charting (rows for cases and columns for subthemes; differen charts for different themes): summaries reflect the essence of the point without losing voice (indicating * for useful quotations in the transcript)
Detection/Categorization/Classification: Looking within a theme, across all cases, noting the range of views that have been tagged Incorporating new ideas and discriminating between dimensions of the theme Are the concepts coherent wholes? Create a master chart or visual of the themes and their connections
Detection of patterns Are there clusters of cases or associated cases, and links between the ideas? What about the outliers or deviant cases? How can you craft an explanation that would account for them? Development of explanations: all scenarios and cases must be examined The explanations range from (and can combine) explicit reasoning, inferring an underlying logic, using common sense, developing an explanatory concept, drawing on other empirical explanations, and using theoretical frameworks. Considering wider applications: what implications?

92 Naiasha Durich
APPENDIX 6: lIDOING PSYCHIATRY" (CONTEXTUALIZED)49
A A a::a: 1&11&1
o oA. o==
A. Y A. yY
>0::
~ :0~ 'i5 v
'15 :r: ~
o/l
c ~ 0
U ~. >- ";:;
'" E .l!! Vl "5>0 c,a: ~
19 Thi s diagram is my own creation, with graphic design assistance from Lydia Del Bianco. It is based on the ideas gleaned from Pilgrim and Rogers (2005, p.2554) and Morant (2006, pp.833-34). I married these insights with my ow n research on the connections between psychiatry, the management of the psychi atric profession, and the relationship between the pharmaceutical industry and the profession (see Chapter One).

Natasha Durich
REFERENCE LIST
Websites:
The Atlantic Provinces Medial Peer Review-Most Common Deficiencies.
Retrieved on November 11,2007, from www.apmpr.ca/Defic.htm
Background Mental Health and Depression. (October 17,2006). Retrieved on July
5,2007, from CBC News Website http://www.cbc.ca/news/background/ mental-health/depression-medicaitons.htm1
Canada Vigilance. Retrieved on November 11,2007, from Health Canada Website,
http://www.hc-sc.gc.ca/ahc-asc/branch-dirgen/hpfb-dgpsa/mhpd-dpsc/ vigilance-announce-annonce-e.html
Marketed Health Products Directorate. Retrieved on November 11,2007, from
Health Canada Website, http://www.hc-sc.gc.ca/ahc-asc/branch-dirgen/
hpfb-dgpsa/mhpd-dpsc/index-e.html
MedEffect Canada. Retrieved on November 11,2007, from Health Canada Website,
http://www.hc-sc.gc.ca/dhp-mps/medeff/index~e~htm1
http://www.orthomolecular.org, accessed on November 11,2002
PharmaNet. Retrieved on November 11,2007, from British Columbia Ministry of
Health Website, http://www.healthservices.gov.bc.ca/pharme/pharmanet.
netindex.htm1
Summary Basis of Decision. Retrieved on November 11,2007, from Health Canada
Website, http://www.hc-sc.gc.ca/dhp-mps/prodph-
Zager and Evans, In the Year 2525. Retrieved on November 11,2007, from http://
www.lyricsondemand.com/z/zagerandevanslyrics/htheyear2525lyrics.htd

Natasha Durich
Television Programs:
Canadian Broadcasting Corporation. Little Helpers. The Fifth Estate (air date
November 12,2003): television, www.cbc.ca/fifth/archives03-04/html
De Patie-Freleng Enterprises. Dr. Seuss teleplay. The Cat in the Hat (air date March
10, 1971): television.
Law (Cases and Statutes):
Drug and Pharmacies Regulation Act: Medicine, RRO 1990, Reg. 548. Retrieved
August 23,2007, from LexisNexis Quicklaw database.
Edwards v. A-G. Canada, [I9301 AC. 114,136. Retrieved August 23,2007, from
LexisNexis Quicklaw database.
Food and Drug Regulations, CRC, c.870 [current to September 15,20061. Retrieved
August 23,2007, from LexisNexis Quicklaw database.
Gadsby v. MacGillivray , [I9971 BCJ No.1564, (BCSC). Retrieved July 5,2006, from
LexisNexis Quicklaw database.
Gallacher v. Jameson Estate, [2002] OJ No.2699, (0.Sup.CJ). Retrieved August 23,2007,
from LexisNexis Quicklaw database.
Harris v. Beck Estate, [2007] PElJ No.11, (PEI.SC). Retrieved August 23,2007, from
LexisNexis Quicklaw database.
Kroll v. Valiance, [I9961 BCJ No.3020, (BCCA). Retrieved July 5,2006, from
LexisNexis Quicklaw database.
Medical Act, Medical Board Regulations, CNLR 1113/96. Retrieved August 23,2007,
from LexisNexis Quicklaw database.
Medical Practitioners Act, RSBC 1995, Ch.285 [updated November 2001.1. Retrieved
August 23,2007, from LexisNexis Quicklaw database.

Natasha Durich 95
Mental Health Act, RSBC 1996, Ch.288, s.22(3). Retrieved August 23,2007, from LexisNexis Quicklaw database.
Stewart v. Barry, [I9941 OJ No.2968, (0.Sup.CJ). Retrieved August 23,2007, from
LexisNexis Quicklaw database.
Trueman v. Ripley, [I9981 BCJ 2060, (BCSC). Retrieved July 5,2006, from LexisNexis
Quicklaw database.
UN Resolution 46/119, Principles for the Protection of Persons with Mental Illness and
the Improvement of Mental Health Care. Retrieved on August 23,2007, from http://www.un.org/documents/ga/res/46/a46rl19.htm
World Psychiatric Association. Madrid Declaration on Ethical Standards. (1996). Retrieved August 23,2007, from http://www.wpanet.org/home.html
Books, Journal Articles, Theses:
Arksey, H., & Knight, P. (1999). Interviewing for the social scientists. An introductory resource with examples. London: Sage Publications.
Atkinson, P., Coffey, A., & Delamont, S. (2003). Key themes in qualitative research. Continuities and changes. New York: Alta Mira Press.
Atkinson, P. (1994). Rhetoric as a skill in a medical setting. In M. Bloor and P. Taraborrelli, (Eds.), Qualitative studies in health and medicine (pp.110-130).
Brookfield, USA: Avebury.
Atkinson, R., & Flint, J. (Summer 2001). Accessing hidden and hard-to-reach
populations: Snowball research strategies. Social Research Update, 33. Retrieved on November 11,2007, from http://sru.soc.surrey.ac.uk/SRU33.
Barbui, C., Garattini, S., & Guest Editors. (2006). Mild depression in general practice: Is the automatism of antidepressant prescribing an evidence-
based approach? Acta Psychiatr Scand, 113,449-451.

Natasha Durich 96
Basit, T.N. (2003). Manual or electronic? The role of coding in qualitative data
analysis. Educational Research, 45(2), 143-154.
Beck, U. (1994). The reinvention of politics: Towards a theory of reflexive
modernization. In U. Beck, A. Giddens, S. Lash, Reflexive modernization.
Politics, tradition and aesthetics in the modern social order (pp. 1-55). Cambridge,
Mass.: Polity Press.
Becker, D. (2005). The myth of empowerment. Women and the therapeutic culture in
America. New York: New York University Press.
Becker, H.S. (1996). The epistemology of qualitative research. In R. Jessor, A. Colby,
& R. Schweder (Eds.), Essays on ethnography and human development (pp.53-
71). Chicago: University of Chicago Press.
Bismark, M., & Paterson, R. (2006). No-fault compensation in New Zealand:
Harmonizing injury compensation, provider accountability, and patient
safety. Health Affairs, 25(1), 278-283.
Bosworth, M. (2001). The past as foreign country: some methodological
implications of doing historical criminology. British Journal of Criminology, 41(3), 431-442.
Breggin, l?R. (1991). Toxic psychiatry. Why therapy, empathy, and love must replace the
drugs, electroshock, and biochemical theories of the "new psychiatry". New York:
St. Martin's Press.
Brockman, J. (1998). "Fortunate enough to obtain and keep the title of profession":
self-regulating organizations and the enforcement of professional
monopolies. Canadian Public Administration, 41(4), 587-621.
Brody, H. (2007). An ethical framework. In H. Brody, Hooked. Ethics, the medical
profession and the pharmaceutical industry (pp.23-54). New York: Rowman &
~ktlefield Publishers Inc.
Natasha Durich 97
Brody, H. (2007). Solutions requiring enhanced professionalism in medicine. In
H. Brody, Hooked. Ethics, the medical profession and the pharmaceutical industry
(pp.299-315). New York: Rowman & Littlefield Publishers Inc.
Burstow, B. (2005). Feminist antipsychiatry praxis-women and the movement(s):
A Canadian perspective In W. Chan, W., D.E. Chunn, & R. Menzies
(Eds.), Women, madness and the law: A feminist reader (pp.245-258). London:
Glasshouse Press.
Busfield, J. (2004). Mental health problems, psychotropic drug technologies and
risk. Health, Risk b Society, 6(4), 361-375.
Busfield, J. (1996). Men, women, and madness. Understanding gender and mental
disorder. New York: New York University Press.
Cadigan, P. (1987). Mindplayers. New York: Bantam Books.
Canadian Psychiatric Association. (n.d.). Position paper: The 1996 CMA code of ethics.
Retrieved on July 5,2006, from http://www.cpaapc.org/Publications/
cjpHome.asp
Castel, R., Castel, F., & Lovell, A. (1982). The Psychiatric Society. New York:
Columbia University Press.
Cebuliak, C. (1995). Life as a blonde: The use of prozac in the '90s. Alta L. Rev., 33,
611-625.
Childress, J.F. & Siegler, M. (1984). Metaphors and models of doctor-patient
relationships: their implications for autonomy. In E.H.W. Kluge (Ed.) (1999),
Readings in biomedical ethics. A Canadian focus (pp.133-44). Scarborough,
Ontario: Prentice Hall Allyn and Bacon Canada.
Chenail, R.J. (1997). Keeping things plumb in qualitative research. The Qualitative
Report, 3(3). Retrieved on January 22,2007, from http://www.nova.edu/ssss/
QR/QR3-3/plumb.html

Natasha Durich
Chetley, A. (1995). Problem drugs. New Jersey: Zed Books, Ltd.
Clarke, J. (2000). The medical profession. In J. Nancarow Clarke, Health, illness, and medicine in Canada (3rd Ed.), (pp. 261-290). Toronto: Oxford University Press.
Cohen, S. (1985). Visions of social control: Crime, punishment, and classification. New York: Polity Press.
College of Physicians and Surgeons of Alberta. (February 2005). Conflict of interest. Retrieved on November 11,2007, from http://www.cpsa.ab.ca/ publicationsresources/attachments~policies/Conflict"/o200f"/o20Interest.pdf
College of Physicians and Surgeons of British Columbia. (n.d.). Conflicts of interest.
In Resource Manual (n.d.). Retrieved on November 11,2007, from https:// www.cpsbc.ca/cps/physician~resources/publications/resource~manual/
conflictofinterest
College of Physicians and Surgeons of British Columbia. (n.d.). Prescribing practices, countersigning prescriptions, and internet prescribing. In Resource Manual (n.d.). Retrieved on November 11,2007, from https://www.cpsbc.ca/cps/ physician~resources/publications/resource~manual/prescribingprac
College of Physicians and Surgeons of New Brunswick (n.d.). Reporting of adverse events. In Selected Commentaries (n.d.). Retrieved on November 11,2007,from See Selected Commentaries, Reporting of adverse events, retrieved from http:// www.cpsnb.org/english/Selected"/020Commentaries/Reporting%20of"/020
Adverse%20Event~.html
College of Physicians and Surgeons of Nova Scotia (March 28,2003). Policy regarding prescribing practices/ countersigning prescriptions/ internet prescribing and notice to non-resident physicians concerning cross-border prescribing. Retrieved on November 11,2007, from http://www.cpsns.ns.ca/ publications/policy-internet-prescribinghtm
College of Physicians and Surgeons of Ontario. (May/June 2005). Prescribing
practices (Policy #2-05). Retrieved on November 11,2007, from http://www.
cpso.on.ca/policies/drug~prac.htm

Natasha Durich 99
College of Physicians and Surgeons of Ontario (May/June 2003). Disclosure of Harm
(Policy #1-03). Retrieved on November 11,2007 from http://www.cpso.
on.ca/policies/disclosure.htm
Copeland, M.B. (2001). The Relationship Among Psychiatrists' Attitudes Toward
Women and Diagnoses and Willingness to Prescribe Antidepressant Medications.
Graduate School of Arts and Sciences, Ph.D. thesis, New York: Columbia
University.
Denney, D. (2005). Professional practice and risk. In D. Denney, Risk and society
(pp. 73-81). Thousand Oaks, California: Sage Publications.
Discretion. In Thompson, D., (Ed). (1995). Concise oxford dictionary (9th ed.), 70%
Oxford: Clarendon Press.
Fraser, H. (2004). Doing narrative research. Analyzing stories line by line.
Qualitative Social Work, 3(2), 179-201.
Freidson, E. (2001). The assault on professionalism. In E. Freidson, Professionalism.
The third logic (pp. 179-196). Chicago: University of Chicago Press.
Freidson, E. (2001). The soul of professionalism. In E. Freidson, Professionalism. The
third logic (pp. 197-222). Chicago: University of Chicago Press.
Freidson, E. (1994). Professionalism reborn: Theory, prophecy, and policy. Oxford: Polity
Press.
Goldbloom, D.S., & Garfinkel, P.E. (2001). The next 50 years. In Q. Rae-Grant
(Ed.), Psychiatry in Canada: 50 years (1951-2001), (pp. 255-264). Canadian
Psychiatric Association.
Gravel, R., Connolly, D., & Bedard, M. (2002). Canadian Community Health Survey.
Mental Health and Well-being. Statistics Canada Catalogue no. 82-617-
XIE. Ottawa. Retrieved August 18,2007, from www.statcan.ca/english/
freepub/82-617-XIE/index.htm

Natasha Durich 100
Greenfield, S. F., & O'Leary, G. (2002). Sex differences in substance use disorders.
In F. L. Hall, et al. (Eds.), Psychiatric illness in women. Emerging treatments and
research. (pp.467-534). Washington, DC: American Psychiatric Publishing,
Inc.
Hathaway, A.D., & Atkinson, M. (2003). Active interview tactics in research on
public deviants: Exploring the two-cop persona. Field Methods, 15(2), 161-186.
Henwood, F., Wyatt, S., Hart, A., & Smith, J. (2003). 'Ignorance is bliss sometimes1:
constraints on the emergence of the 'informed patient' in the changing
landscapes of health information. Soc. Of Health and Illness, 25(6), 589-607.
Holmes, C.A., & Warelow, P. (1999). Implementing psychiatry as risk management:
DSM-IV as a postmodern taxonomy. Health, Risk and Society, 1(2), 167-178.
Integrity. In Thompson, D., (Ed). (1995). Concise oxford dictiona y (9th ed.), 707.
Oxford: Clarendon Press.
Jones, M.A. (1999). Informed consent and other fairy stories. Medical Law Review, 7,
103-134.
Kaiser, H.A. (2002). Mental disability law. In J. Downie, T. Caulfield, & C. Flood
(Eds.), Canadian health law and policy (2nd Ed.) (pp.251-330). Markham, Ont:
Butterworths, LexisNexis Group.
Kassirer, J. (2005). On the take: How america's complicity with big business can endanger
your health. New York: Oxford University Press.
Kirk, S.A. & Kutchins, H. (1992). The selling of the DSM. The rhetoric of science in
psychiatry. New York: Aldine de Gruyter.
Kleefeld, J.C., & Srivastava, A. (2005). Resolving mass wrongs: A command-
consensus perspective. Queen's L.J., 30,449-500.
Kurdyak, RA., Juurlink, D.N., & Mamdani, M.M. (2007). The effect of
antidepressant warnings on prescribing trends in Ontario, Canada.
American Journal of Public Health, 97(4), 750-754.

Natasha Durich 101
Laing, R.D. (1985). Wisdom, madness and folly: The making of a psychiatrist. New York:
McGraw-Hill Book Company.
Leszcz, M. (2001). Psychotherapy in Canada. In Q. Rae-Grant (Ed.), Psychiatry in
Canada: 50 years (1951-2001), (pp. 111-136). Canadian Psychiatric Association.
Lewis, J. (2003). Design issues. In J. Ritchie, & J. Lewis, (Eds.), Qualitative research
practice: A guide for social science students and researchers (pp.47-76). Thousand
Oaks, California: Sage Publications.
Lewis, B.E. (2003). Prozac and the post-human politics of cyborgs. Journal of Medical Humanities, 24(1/2), 49-63.
Lexchin, J. (1990). Drug makers and drug regulators: Too close for comfort. A
study of the Canadian situation. Social Sciences and Medicine, 31(11), 1257-
1263.
Lexchin, J. (2001). Lifestyle drugs: Issues for debate. CMAJ, 164(10), 1449-1452.
Liederbach, J., Cullen, F., Sundt, J., & Geis, G. (2001). The criminalization of
physician violence: Social control in transformation? Justice Quarterly, 18(1),
141-170.
Lineberry, T.W. (April, 2007). Letter to the editor. Impact of FDA black box
warning on physician antidepressant prescribing and practice patterns.
Opening pandora's suicide box. Mayo Clin. Proc., 82(4), 518-520.
Lowrey, W., & Anderson, W.B. (2006). The impact of internet use on the public
perception of physicians: a perspective from the sociology of professions
literature. Health Communications, 19(2), 125-131.
McHenry, L. (2006). Ethical issues in psychopharmacology. J. of Medical Ethics, 32,
405-410.
McHugh, P.R., & Slavney, P.R. (1998). The perspectives of psychiatry. (2nd ed.).
Baltimore: John's Hopkins University Press.

Natasha Durich 102
McKnight, J. (1995). The careless society: Community and its counterfeits. New York:
Basicbooks.
Mann, J.J. (2005). The medical management of depression. New England Journal of
Medicine, 353, 1819-1834.
Manning, J. (2004). Informed consent to medical treatment: The common law and
New Zealand's code of patients' rights. Medical Law Rwiew, 12,181-216.
Marshall, C. & Rossman, G.B. (1989). Designing qualitative research. Newbury Park,
California: Sage Publications Inc.
Mattingly, C. (2004). Performance narratives in the clinical world. In B. Hurwitz,
G. Greenhalgh, & V. Skultans (Eds.), Narrative research in health and illness.
(pp.73-94). Mass: Blackwell Publishing Ltcl: E-book.
Mauthner, N.S., & Doucet, A. (2003). Reflexive accounts and accounts of reflexivity
in qualitative data analysis. Sociology, 37(3), 413-431.
Maynard, A., & Bloor, K. (2003). Dilemmas in regulation of the market for
pharmaceuticals. Health Affairs, 22(3), 31-41.
Mintzes, B., et al. (2002). Influence of direct to consumer pharmaceutical
advertising and patients' requests on prescribing decisions: Two site cross
sectional survey. BMJ, 324,278-279.
Misztal, B.A. (1996). Trust as habitus. In B.A. Misztal, Trust in modern societies.
(pp.102-157). Cambridge, Mass: Polity Press.
Morant, N. (2006). Social representations and professional knowledge: the
representation of mental illness among mental health practitioners. BJ of
Social Psych, 45,817-838.
Nader, L. (1999). Comments. Current Anthropology, 40(2), p.121.
Natasha Durich 1 03
Palys, T. (2003). Quantitative and qualitative perspectives (3rd ed.). Scarborough, Ont:
Thomson Nelson.
Penfold, P. S. & G. A. Walker (1983). Women and the psychiatric paradox. Montreal:
Eden Press.
Penfold, P.S. (2001). Drugged, exploited, labeled and blamed: How psychiatry
oppresses women In D.E. Chunn, R.J. Menzies, & S.C. Boyd (Eds.), (Abhsing power: The canadian experience (pp.174-184). Halifax, NS: Fernwood.
Pilgrim, D., & Rogers, A.E. (2005). Psychiatrists as social engineers: a study of an
anti-stigma campaign. Social Science G. Medicine, 61,2546-2556.
Rasmussen, N. (2006). Making the first antidepressant: Amphetamine in
American medicine, 1929-1950. J. of the Hist. of Medicine and Allied Sciences,
61 (3), 288-323.
Reesal, R.T., & Lam, R.W. (2001). Principles of management. Canadian Journal of
Psychiatry, 46(5) Supplement, 21s-28s.
Ritchie, J. (2003). The applications of qualitative methods to social research. In
J. Ritchie, & J. Lewis, (Eds.), Qualitative research practice: A guide for social science students and researchers (pp.24-46). Thousand Oaks, California: Sage
Publications.
Ritchie, J., & Spencer, L. (1994). Qualitative data analysis for applied policy
research. In A. Bryman, & R.G. Burgess, (Eds.), Analyzing qualitative data
(pp.173-194). New York: Routledge.
Ritchie, J., Spencer, L., & O'Connor, W. (2003). Carrying out qualitative analysis.
In J. Ritchie, & J. Lewis, (Eds.), Qualitative research practice: A guide for social
science students and researchers (pp.219-262). Thousand Oaks, California: Sage
Publications.
Rossides, D. W. (1998). Professions and disciplines: Functional and conflict perspectives.
Upper Saddle River, NJ: Prentice Hall.

Natasha Durich 104
Royal College of Physicians and Surgeons. Prescription Drugs in Canada:
Presentation to House of Commons Standing Committee on Health (November
6,2003). Retrieved on November 11,2007, from http://rcpsc.medical.org/ publicpolicy/archives-e.php
Royal College of Physicians and Surgeons. (n.d.). Physicians and industry - conflicts
of interest. Retrieved November 11,2007, from http://www.rcpsc.medical.org/
publications/index.php
Rubin, H.J., & Rubin, I.S. (2005). Qualitative interviewing. The art of hearing data.
Thousand Oaks, California: Sage Publications.
Silverman, D. (2000). Doing qualitative research: A practical handbook. Thousand
Oaks, California: Sage Publications.
Smith, D.E. (1975). Women and psychiatry. In D.E. Smith & S.J. David (Eds.),
Women look at psychiatry (pp.1-20). Vancouver, British Columbia: Press Gang Publishers.
Slingsby, B.T., Plotnikoff, G.A., Akabayashi, A., & Mizuno, T. (2007). Physician
strategies for addressing patient adherence to prescribed psychotropic
medications in Japan: A qualitative study. J. of Clinical Pharmacy and
Therapeutics, 32, 241-245.
Steiman, M.A., Bero, L.A., Chren, M., & Landefeld, C.S. (2006). Narrative review. The promotion of gabapentin: an analysis of internal individual documents. Annals of Internal Medicine, 145(4), 284-293.
Sullivan, M., Verhulst, J., Russo, J., & Roy-Byrne, P. (1993). Psychotherapy vs. pharmacotherapy: Are psychiatrists polarized?-A survey of academic and
clinical faculty. American Journal of Psychotherapy, 47(3), 411-423.
Szasz, T. (2001). Pharmacracy. Medicine and politics in america. Westport, CT Praeger
Publishers.

Natasha Durich 105
Tucker, N. (Tues, Sept.26,2006). Plumbing the depths of depression. The Washington Post online, C01. Retrieved on October 2,2006, from http://
www.washingtonpost.com/wp-dyn/content/article/2006/09/25/
AR2006092501387-pf.htm1
Ussher, J.M. (2005). Unraveling women's madness: Beyond positivism and
constructivism and towards a material-discursive-intrapsychic approach.
In W. Chan, W., D.E. Chunn, & R. Menzies (Eds.), Women, madness and the law: A feminist reader (pp.19-40). London: Glasshouse Press.
Van Praag, H.M. (2003). A stubborn behaviour: The failure of antidepressants to
reduce suicide rates. World J. Biol. Psychiatry, 4, 184-191.
Veatch, R.M. (1990). Contemporary bioethics and the demise of modern medicine.
In G.L. Ormiston & R. Sassower, (Eds.), Prescriptions. The dissemination of medical authority (pp.23-40). New York, New York: Greenwood Press.
Weiss, R.S. (1994). Learningfi-om strangers. The art and method of qualitative interview studies. New York: The Free Press.
Witz, A. (1992). Professions and patriarchy. London: Routledge.
World Health Organization (2004). Concurrent disorders. In World Health Organization, Neuroscience of Psychoactive Substance Use and Dependence (pp.169-208). Geneva: WHO Retrieved August 23,2007, from http://www.
who.int/substance~abuse/publications/en/Neuroscience.pdf