-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
1/64
PRIMARY SLEEP DISORDERS
Grand RoundsPsychiatry DepartmentSan Fernando General
Hospital
Dr. Shivan A.C. Mahabir
March 01, 2013
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
2/64
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
3/64
Introduction
Sleep is defined behaviorally by four criteria: (1) reduced
motoractivity, (2) decreased response to stimulation, (3)
stereotypicpostures (in humans, for example, lying down with eyes
closed),and (4) relatively easy reversibility (distinguishing it
from coma,hibernation, and estivation).
- Universal Behaviour
- Exact functions unknown
- Prolonged sleep deprivation leads to severe physical and
cognitive
impairment and finally death
- Sleep disturbances occur in virtually all psychiatric
illnesses andare frequently part of the diagnostic criteria for
specific disorders.
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
4/64
Theories of Sleep
- originally thought fatigue causes decrease of sensory
stimulationleading to decrease in brain activity which led to
sleep.
- transection of ascending sensory pathways in brain stem
(therebydecreasing stimulation) did not affect wakefulness or
sleep.
- lesions of reticular formation in the brainstem showed that:
therostral portion of the reticular formation above the
ponscontributes to wakefulness. The caudal part of the
reticularportion below the pons normally inhibits the rostral area
to causesleep. (Moruzzi, 1950s)
-sleep is actively induced and highly organised brain state
withdifferent phases
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
5/64
Regulation of Sleep
- endogenous circadian rhythm
- entrained by light via the retinohypothalamic tract to
thesuprachiasmatic nucleus of the hypothalamus
-Total sleep time remains fairly stable from day to day even
underwidely varying conditions, and is only modestly affected
byvariations in activity and sensory stimulation.
-The only behavioral factor that reliably and substantially
increasessleep is prior sleep loss
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
6/64
Phases of Sleep
- 2 distinct cyclical phases in a highly structured pattern
(Kleitman,Aserinksky, Dement in 1950s)
- non rapid eye movement (NREM)
- rapid eye movement (REM)
- Humans usually fall asleep by entering non-REM sleep, a
phaseaccompanied by characteristic changes in
theelectroencephalogram (EEG). The sleeper next moves into
REMsleep, which is characterized not only by rapid eye movementsbut
also by a surprisingly complete inhibition of skeletal muscle
tone. It is during this phase of sleep that most dreams are
thoughtto occur.
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
7/64
NON-REM Sleep
-Neuronal activity is low, and metabolic rate and brain
temperatureare at their lowest. Sympathetic outflow decreases and
heart rateand blood pressure decline. Parasympathetic activity
increasesand then dominates during the non-REM phase. Muscle tone
and
reflexes are intact.
Non-REM sleep is divided into four characteristic stages.
Stage 1 represents the transition from wakefulness to the onset
ofsleep and lasts several minutes. The EEG shows a
low-voltage,mixed-frequency pattern. In stage 1 and throughout the
non-REM
phase there is some activity of skeletal muscle but no rapid
eyemovements. Rather, the sleeper shows slow, rolling
eyemovements..
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
8/64
NON-REM Sleep
Stage 2 is characterized by bursts of sinusoidal waves called
sleepspindles (12- 14 Hz) and high-voltage biphasic waves calledK
complexes, which occur episodically against a background
ofcontinuing low-voltage EEG activity.
The EEG in stage 3 shows high-amplitude, slow (0.5-2 Hz)
deltawaves.
In stage 4 the slow-wave activity increases and dominates the
EEGrecord.
Stages 3 and 4 in humans are sometimes called slow-wave sleep.
Insome animals all of non-REM sleep is called slow-wave sleep.
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
9/64
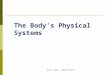
EEG patterns in human sleep
Figure 47-1 Electroencephalogram (EEG) patterns in the stages
ofhuman sleep. Non-REM sleep has four stages. Stage 1
ischaracterized by a slight slowing of the EEG, stage 2 by
high-
amplitude K complexes and spindles (low-amplitude
clusters).Slow, high-amplitude delta waves characterize stages 3
and 4.
REM sleep is characterized by eye movements and loss of
muscletone, in conjunction with a stage 1 EEG. The
higher-voltageactivity in the EOG tracings during stages 3 and 4
reflects high-amplitude EEG activity in prefrontal areas rather
than eyemovements. EOG = electro-oculogram; EMG =
electromyogram.
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
10/64
REM Sleep
In humans the EEG during REM sleep reverts to a
low-voltage,mixed-frequency pattern similar to stage 1 of non-REM
sleep
intense bursts of firing generate high-voltage spike potentials
in theEEG called ponto-geniculo-occipital spikes (PGO spikes),
after thebrain structures in which the spikes appear most
prominently. PGOspikes of REM sleep may be generated by internal
activation ofthe neural circuit for the startle response. PGO
spikes arecorrelated with the bursts of eye movements in REM
sleep.
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
11/64
REM Sleep
Consistent with the overall increase in neural activity during
REMsleep, brain temperature and metabolic rate rise.
In contrast to the waking state, however, almost all skeletal
muscletone is lost (atonia); the skeletal muscles that remain
active arethose controlling the movements of the eyes, middle ear
ossicles,and diaphragm. In addition, some small, phasic twitches
occur.
During REM sleep penile erections occur regularly in men,
andwomen show clitoral engorgement.
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
12/64
REM Sleep
In both sexes the pupils become highly constricted
(miosis),reflecting the high ratio of parasympathetic to
sympathetic outputto the pupil.
Homeostatic mechanisms are attenuated: respiration is
relativelyunresponsive to changes in blood CO2, and responses to
heat andcold are greatly reduced or even absent. As a result,
bodytemperature drifts toward ambient temperatures.
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
13/64
REM/NREM Cycling
The non-REM and REM phases alternate cyclically during
sleep.Human adults usually begin sleep by progressing from stage
1through stage 4 of non-REM sleep.
This progression is intermittently interrupted by body
movements
and partial arousals. After about 70-80 minutes the
sleeperusually returns briefly to stage 3 or stage 2 and then
enters thefirst REM phase of the night, which lasts about 5-10
minutes.
In humans the length of the cycle from the start of non-REM
sleep tothe end of the first REM phase is about 90-110 minutes.
This cycle
of non-REM and REM sleep is typically repeated four to six times
anight. In successive cycles the duration of non-REM stages 3 and
4decreases while the length of REM phases increases.
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
14/64
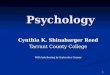
REM/NREM Cycling
The cycling of human sleep stagesat different times of
life.Childhood is broadly defined toinclude early adolescence,
and
old age spans the period fromthe mid 50s to the early 70s.(From
Zepelin 1983, bypermission.)
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
15/64
Classification of SleepDisorders
DSM - IV -TR divides sleep disorders into 1. Primary Sleep
Disorders,2. Sleep disorders related to another mental disorder and
3. Othersleep disorders (due to a medical disorder or substance
induced)
Primary sleep disorders are divided into
1. Dyssomnias:a. Primary Insomniab. Primary Hypersomniac.
Narcolepsyd. Breathing-related sleep disorder
e. Circadian rhythm sleep disorder (sleep-wake schedule
disorder)f. Dyssomnia not otherwise specified.
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
16/64
Classification of SleepDisorders
2. Parasomnias:
a. nightmare disorder (dream anxiety disorder)
b. sleep terror disorder
c. sleepwalking disorderd. parasomnia not otherwise
specified.
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
17/64
Assessment
It is important to determine if another sleep disorder
(seepreliminary questions above), or a physical (such as pain,
heart orlung disease), neurological (such as Parkinsons disease
orcerebrovascular disease) or psychiatric disorder (such
asdepressive illness, anxiety disorder, or substance misuse) is
the
primary diagnosis.
In depression, however, in many cases insomnia should be
regardedas a co-morbid condition, rather than as a secondary
one.
The majority of epidemiological evidence suggests that
insomniatypically predates other psychiatric symptoms and may
represent
an independent risk factor for the development of depression
inparticular
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
18/64
Investigations
Laboratory studies appropriate for those with sleep disorders
includethe following:
Hemoglobin and hematocrit
Arterial blood gases
Thyroid function tests
Drug and alcohol toxicology screening
Oximetry may be performed during sleep to examine blood
oxygenlevels for clinically important desaturations suggestive of
sleepapnea or other forms of sleep-disordered breathing.
Although no imaging studies are directly indicated for the
workup ofinsomnia, underlying medical conditions call for
appropriateinvestigation using suitable studies.
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
19/64
Indices and Scoring Systems
A Beck Depression Index or similar clinical screening tool may
beused to detect an underlying depressive illness as a
contributingfactor in insomnia.
An Epworth Sleepiness Score or another objective measure
ofdaytime sleepiness may lead to clues to the presence of
anotherunderlying sleep disorder. For example, approximately 20%
ofpatients with sleep apnea present with a history of
nighttimeinsomnia; however, patients are excessively sleepy by day
andhave an abnormal score on the Epworth Sleepiness Scale.
Sleep Journal
Subjective measures of sleep are obtained by means of a
sleepjournal. A sleep journal kept for approximately 2 weeks may
helpdetermine the extent of the sleep disturbance. Patients
shouldrecord the total hours slept per night, the frequency of
nighttimeawakenings, and the level of restfulness provided after
sleep.Additional, more objective measures of sleep may be available
if apatient has a sleep partner who keeps a 2-week journal
orprovides a relevant history.
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
20/64
Electroencephalography andPolysomnography
Objective measures of sleep may be obtained by means
ofelectroencephalography (EEG) or polysomnography (PSG).
Thesestudies may be helpful in determining sleep and wakefulness
inthe intensive care unit (ICU) or in the sleep laboratory.
Monitored PSG is the standard for evaluating measures of sleep.
This
study includes measures of multiple channels of
EEG,electrooculography (EOG), chin and leg electromyography
(EMG),nasal and oral airflow, oximetry, abdominal and
chestmovements, and electrocardiography (ECG). Monitored PSG
canhelp the physician discriminate between rapid eye movement(REM)
sleep and non-REM (NREM) sleep, as well as determining
causes of sleep disturbance.Patients with chronic medical
conditions, such as fibromyalgia or
anxiety disorders, often have characteristic alpha
brain-waveactivity that intrudes into the deeper stages of sleep.
This activitycan readily be seen on the EEG during PSG. Patients
with insomniaoften have some degree of sleep-state misperception,
wherein
they perceive and believe that they achieve significantly
lessslee than the actuall do. This can be documented b
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
21/64
Questionnaire to screen forsleep disorders other than
insomnia
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
22/64
Diagnosis Algorithm
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
23/64
Circadian Rhythm Disorders
Circadian rhythm disorders are sleep disorders where there is
amismatch between circadian rhythms and required
sleepwakecycle.
Thus there can be sleeplessness when trying to sleep at a time
notsignalled by the internal clock, and excessive sleepiness
when
needing to be awake.
Some circadian disorders (jetlag and shift-work disorder) are
due toan individual lifestyle, including work and travel schedules,
thatconflicts with the internal clock.
Others are:
delayed sleep-phase syndrome (DSPS), where there is
difficultyfalling asleep before 23 a.m. (sometimes later), and on
dayswithout work/school/college the preferred wake time is after
10a.m., resulting in sleep-onset insomnia and difficulty waking up
inthe morning on days when an early bedtime for an early starttime
is necessary.
free-running sleep disorder, where there is a daily increment
of
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
24/64
DSM-IV-TR Diagnostic Criteria forCircadian Rhythm Sleep
Disorder
A. A persistent or recurrent pattern of sleep disruption leading
toexcessive sleepiness or insomnia that is due to a mismatchbetween
the sleep-wake schedule required by a person'senvironment and his
or her circadian sleep-wake pattern.
B. The sleep disturbance causes clinically significant distress
or
impairment in social, occupational, or other important areas
offunctioning.
C. The disturbance does not occur exclusively during the course
ofanother sleep disorder or other mental disorder.
D. The disturbance is not due to the direct physiological
effects of a
substance (e.g., a drug of abuse, a medication) or a
generalmedical condition.
Specify type:Delayed sleep phase type: a persistent pattern of
late sleep onset and late awakeningtimes, with an inability to fall
asleep and awaken at a desired earlier timeJet lag type: sleepiness
and alertness that occur at an inappropriate time of day relativeto
local time, occurring after repeated travel across more than one
time zone
Shift work type: insomnia during the major sleep period or
excessive sleepiness duringthe major awake period associated with
night shift work or frequently changing shift
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
25/64
Treatment of CircadianRhythm Sleep Disorder
What is known
Melatonin is effective in jet lag disorder (1a), delayed sleep
phasesyndrome (Ib) and free-running disorder (IIa)
Light therapy is effective in delayed sleep-phase syndrome
(III)
What is not known
What are the best efficacy measures subjective versus
objective?
Is there a need to distinguish between adults and adolescents
indelayed sleep-phase disorder, since sleep times are
somewhatdelayed in normal adolescence?
Is there a need to distinguish between sighted and
blindindividuals?
Is melatonin or light therapy more effective for delayed
sleep-phase disorder?
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
26/64
Treatment of CircadianRhythm Sleep Disorder
Recommendations
. Clinical assessment is essential in DSPS and free-running
disorder(A/B).
. Melatonin may be useful in DSPS, free-running disorder and jet
lag(A).
. Other approaches such as behavioural regimes and scheduled
lightexposure (in sighted individuals) can also be used (B/C).
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
27/64
Parasomnias
Parasomnias are unusual episodes or behaviours occurring
duringsleep which disturb the patient or others.
Assessment of parasomnia may be possible with a detailed
historyfrom the patient or a witness but, in general, for an
adequate
diagnosis referral to a specialist sleep centre for
polysomnography(PSG) and video recordingmay be necessary.
Violent or unusual night-time attacks may arise from deep
non-REMsleep (night terrors and sleepwalking) or from REM sleep
(severerecurrent nightmares, REM behaviour disorder),
Treatments depend on which disorder is present.
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
28/64
Night Terrors
Night terrors (also called sleep terrors) are recurrent episodes
ofabrupt awakening from deep non-REM sleep, usually in first
thirdof the night, usually with a scream and signs of intense fear
andautonomic arousal. The patient is unresponsive to
comforting;they may sit up in bed and sometimes engage in
automatic
behaviour associated with fear and escape. There is usually
nodetailed recall, and if the patient wakes from a terror
(notcommon), there is confusion and disorientation and only a
vaguememory of fear.
Night terrors are common in children, with about 3040% having
atleast one episode, and repeated episodes in about 5%. The peakage
for these is at about 27 years, with a gradual diminution upto
early adolescence (DiMario and Emery, 1987).
In some cases night terrors persist into adult life; the
prevalence inadults is unknown. Almost all adult patients have had
night terrorsor sleepwalking as a child (Crisp, 1996).
There is a strong genetic component (Nguyen et al., 2008), and
night
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
29/64
DSM-IV-TR Diagnostic Criteriafor Sleep Terror Disorder
A. Recurrent episodes of abrupt awakening from sleep,
usuallyoccurring during the first third of the major sleep episode
andbeginning with a panicky scream.
B. Intense fear and signs of autonomic arousal, such as
tachycardia,rapid breathing, and sweating, during each episode.
C. Relative unresponsiveness to efforts of others to comfort
theperson during the episode.
D. No detailed dream is recalled and there is amnesia for
theepisode.
E. The episodes cause clinically significant distress or
impairment in
social, occupational, or other important areas of
functioning.
F. The disturbance is not due to the direct physiological
effects of asubstance (e.g., a drug of abuse, a medication) or a
generalmedical condition.
(From American Psychiatric Association. Diagnostic and
Statistical
Manual of Mental Disorders. 4th ed. Text rev. Washington,
DC:
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
30/64
Sonambulism (Sleepwalking)
Sleepwalking alone probably has 1520% lifetime prevalence.
The main symptom is of automatic behaviour at night with
thesufferer unresponsive to surroundings and other people.
Thebehaviour is most commonly walking around, but can include
other behaviours which are highly familiar to the subject such
asdressing, washing, making tea, arranging objects in the
house,etc.
Some cases of sleepwalking seem related to use of certain drugs,
forexample alcohol and hypnotics, especially zolpidem and
triazolam(Pressman, 2007).
It is rare for affected individuals to present for treatment,
except ifthey have injured themselves or a partner, have put
themselvesinto potential danger, or have excessive daytime fatigue
becauseof nighttime disturbance.
Another reason for presentation is anxiety and disruption of
sleep of
partner, family or housemates.
DSM IV TR Di ti C it i f
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
31/64
DSM-IV-TR Diagnostic Criteria forSleepwalking Disorder
A. Repeated episodes of rising from bed during sleep and
walkingabout, usually occurring during the first third of the major
sleepepisode.
B. While sleepwalking, the person has a blank, staring face,
isrelatively unresponsive to the efforts of others to
communicate
with him or her, and can be awakened only with great
difficulty.C. On awakening (either from the sleepwalking episode or
the next
morning), the person has amnesia for the episode.
D. Within several minutes after awakening from the
sleepwalkingepisode, there is no impairment of mental activity or
behavior
(although there may initially be a short period of confusion
ordisorientation).
E. The sleepwalking causes clinically significant distress
orimpairment in social, occupational, or other important areas
offunctioning.
F. The disturbance is not due to the direct physiological
effects of asubstance (e.g., a drug of abuse, a medication) or a
general
T t t f NREM Sl
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
32/64
Treatment of NREM SleepDisordersThere is little high-level
evidence for treatments in these disorders.
There are no controlled trials of treatment of non- REM
parasomniasin adults (see Harris and Grunstein, 2009).
Priorities are to minimize possible trigger factors such as
frighteningfilms, caffeine, alcohol or meals late a night, and to
make surethere is a stable and adequate sleepwake schedule. It
isimportant to safeguard against harm to the patient, such as
bylocking windows, bolting doors, or sleeping on the ground
floor,and safety of the bed partner or nearby children also
requiresattention.
Drug treatment decisions should be based on the frequency
and
severity of events.Clonazepam in doses up to 3mg per night has
been reported to be
effective (case series, n69) (Schenck and Mahowald, 1996).
Smaller case serieshave reported good effects of paroxetine
(Wilsonet al.,1997) and imipramine (Cooper, 1987) (both
effective
immediately), and there is a small case series of hypnotherapy
in
Ni ht /REM Sl
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
33/64
Nightmares/REM SleepBehaviour Disorder
Nightmares and REM sleep behaviour disorder (RBD) are
disordersarising from REM sleep, and the main difference in
presentationfrom the non-REM episodes is that they are normally
recalled bythe patient, who wakes from them and is aware of the
episodeand can describe it.
RBD is a disorder, first described in the late 1980s, with
violentcomplex behaviour at night, which is mostly recalled by
thepatient. There are two sleep abnormalities;lack of atonia during
REM sleep andincreased vividness and/or unpleasant content of
dreams.
The violent behaviour is described as acting out of dreams,
made
possible by the lack of the normal muscle paralysis in REM
sleep.Its incidence is unknown (probably
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
34/64
DSM-IV-TR Diagnostic Criteria forNightmare Disorder
A. Repeated awakenings from the major sleep period or naps
withdetailed recall of extended and extremely frightening
dreams,usually involving threats to survival, security, or
self-esteem. Theawakenings generally occur during the second half
of the sleepperiod.
B. On awakening from the frightening dreams, the person
rapidlybecomes oriented and alert (in contrast to the confusion
anddisorientation seen in sleep terror disorder and some forms
ofepilepsy).
C. The dream experience, or the sleep disturbance resulting from
theawakening, causes clinically significant distress or impairment
in
social, occupational, or other important areas of functioning.D.
The nightmares do not occur exclusively during the course of
another mental disorder (e.g., a delirium, posttraumatic
stressdisorder) and are not due to the direct physiological effects
of asubstance (e.g., a drug of abuse, a medication) or a
generalmedical condition.
(From American Psychiatric Association. Diagnostic and
Statistical Manual of Mental Disorders. 4th
Treatment of REM Sleep
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
35/64
Treatment of REM SleepDisorders
For nightmares, psychological treatments are effective and
thesefocus on exposure writing down dreams or guided
imagery,pleasant images, and changing the ending (Burgess et al.,
1998;Krakow et al., 1995).
There have been a few case series showing beneficial effects of
thealpha-1 adrenergic blocker prazosin in reducing
nightmaresrelated to post-traumatic stress disorder in both
military andcivilian settings (Raskind et al., 2007).
Nightmares have been reported to be triggered or worsened bymany
drug treatments, including cholinesterase inhibitors,
beta-blockers, SSRIs (especially paroxetine levodopa, and
following
withdrawal from antidepressants.
Treatment of REM Sleep
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
36/64
Treatment of REM SleepDisorders
There are no prospective or controlled studies of drug treatment
ofREM behaviour disorder, but case series suggest a good effect
forclonazepam 14mg (Aurora et al., 2010; Boeve et al., 2004)
inreducing the number of episodes and injuries during them,although
it should be used with cautionin patients with dementia,disorders
of gait or balance, or concomitant OSAS.
Smaller beneficial effects have been reported for melatonin 312
mg(Gagnon et al., 2006).
Single case studies and small series have reported beneficial
effectsof clonidine (Nash et al., 2003), donepezil (Massironi et
al., 2003)and sodium oxybate (Kosky et al., 2008).
Drugs which can worsen RBD or provoke its symptoms include
SSRIs,venlafaxine, mirtazapine, bisoprolol, and tramadol (Gagnon et
al.,2006).
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
37/64
Primary Insomnia
Primary insomnia is diagnosed when the chief complaint
isnonrestorative sleep or difficulty in initiating or maintaining
sleep,and the complaint continues for at least a month
The term primary indicates that the insomnia is independent
ofany known physical or mental condition.
Primary insomnia is often characterized both by difficulty
fallingasleep and by repeated awakening.
Increased nighttime physiological or psychological arousal
andnegative conditioning for sleep are frequently evident.
Patients with primary insomnia are generally preoccupied
with
getting enough sleep. The more they try to sleep, the greater
thesense of frustration and distress and the more elusive
sleepbecomes.
DSM IV TR Diagnostic Criteria
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
38/64
DSM-IV-TR Diagnostic Criteriafor Primary Insomnia
A. The predominant complaint is difficulty initiating or
maintainingsleep, or nonrestorative sleep, for at least 1
month.
B. The sleep disturbance (or associated daytime fatigue)
causesclinically significant distress or impairment in social,
occupational,or other important areas of functioning.
C. The sleep disturbance does not occur exclusively during
thecourse of narcolepsy, breathing-related sleep disorder,
circadianrhythm sleep disorder, or a parasomnia.
D. The disturbance does not exclusively occur during the course
ofanother mental disorder (e.g., major depressive disorder,
generalized anxiety disorder, a delirium).E. The disturbance is
not due to the direct physiological effects of a
substance (e.g., a drug of abuse, a medication) or a
generalmedical condition.
(From American Psychiatric Association. Diagnostic and
Statistical Manual of Mental Disorders. 4th
ed. Text rev. Washington, DC: American Psychiatric Association;
copyright 2000, with
Neurotransmitters GABA /
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
39/64
Neurotransmitters GABA /ADENOSINE
The inhibitory effects of GABA are mediated through the
GABAAreceptor, which is a complex of proteins with binding sites
for anumber of sleep-promoting drugs, in particular
benzodiazepines,so-called Z-drugs and barbiturates, all of which
enhance theeffects of GABAs actions at the GABAA receptor
The other main sleep-promoting neurotransmitter is
adenosine.Brain levels of this rise during the day and are thought
to lead tosleepiness, which increases the longer the time since the
lastsleep. The arousing and sleep-impairing effects of caffeine
(Landolt et al., 2004) are thought to be due to blockade
ofadenosine-A2 receptors, so attenuating this natural
process(Porkka-Heiskanen et al., 2002).
Neurotransmitters
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
40/64
Neurotransmitters -MELATONIN
Melatonin is a natural hormone that is produced in the pineal
glandand which has an important role in regulating circadian
rhythms(Cajochen et al., 2003; Dijk and von Schantz, 2005).
The circadian pacemaker in the suprachiasmatic nucleus (SCN)
ofthe hypothalamus drives melatonin synthesis and secretion fromthe
pineal gland. Once melatonin appears in the plasma it enters
the brain and binds to melatonin receptors in the
hypothalamus,forming a feedback loop.
The SCN contains melatonin 1 and melatonin 2 receptors, and
muchresearch is ongoing about their role in sleep/wake regulation
andcircadian rhythms. Melatonin has both phase-shifting effects
(changing the timing of the biological clock), and direct
sleep-facilitating effects.
Neurotransmitters -
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
41/64
Neurotransmitters -MELATONIN
Administering exogenous melatonin or analogues such as
ramelteon(licensed in the USA) can promote sleep onset.
A slow-release formulation of melatonin has been licensed on
thebasis of improved sleep continuity and daytime well-being
inpeople aged over 55 years with insomnia.
Melatonin production is reported to decline with age and to be
lowerin middle-aged and elderly patients with insomnia than in
goodsleepers (Attenburrow et al., 1996; Dowling et al., 2008;
Haimov,2001; Leger et al., 2004).
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
42/64
Treatment Algorithm
l i
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
43/64
Sleep Hygiene
Educating patients in good sleep hygiene is the keystone
oftreatment. The following advice should be given to patients:
Use the bed for sleep and sex only (no television watching or
readingin bed)
Avoid caffeine, especially late in the day; avoid activities
that will getyou stimulated and upset late in the day; practice
relaxationtechniques before bedtime
Exercise each day
Maintain a regular schedule for bedtime and wakening; avoid
naps
Do not watch the clock while in bed; avoid struggling to fall
asleep inbedinstead, get up and spend quiet time out of bed until
sleepcomes
Ph h
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
44/64
Pharmacotherapy
What is known about drug treatments for insomnia
Z-drugs and short-acting benzodiazepines are efficacious
forinsomnia (Ia)
Safety (adverse events and carryover effects) are fewer and
less
serious with decreasing half-lives (Ib)
Prolonged release melatonin improves sleep onset latency
andquality in patients over 55 (Ib)
What is not known Does improvement in insomnia last after
treatment is stopped?
Does treatment reduce risk of subsequent depression?
Ph th
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
45/64
Pharmacotherapy
Recommendation
. It is important to treat insomnia because the condition
causesdecreased quality of life, is associated with impaired
functioning inmany areas, and leads to increased risk of
depression, anxietyand possibly cardiovascular disorders (A).
. Goal of treatment to less suffering and improve daytime
function
. Type of treatment:. Patient-guided. By particular pattern of
problem, i.e. sleep onsetinsomnia,maintenance. By choice of
treatments with an evidence base
. Factors which clinicians need to take into account when
prescribingare efficacy, safety, and duration of action (A).
. Other factors are previous efficacy of the drug or adverse
effects,history of substance abuse or dependence (D).
A tihi t i
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
46/64
Antihistamines
Antihistamines are sedating and are sold as over-the-counter
(OTC)sleeping medications. There is limited evidence that
OTCantihistamines work, although recently some modest benefitshave
been reported after 2 weeks dosing with diphenhydraminein mild
insomnia (Morin et al., 2005b).
Antihistamines are commonly used in alleviation of insomnia in
drugand alcohol withdrawal where traditional hypnotics are
lesssuitable due to the risk of cross-dependence, although there
areno controlled trials in this setting.
Recommendations
. Antihistamines have a limited role in psychiatric and primary
carepractice for the management of insomnia (D).
H ti
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
47/64
Hypnotics
What is known about long-term hypnotic treatment
Insomnia is often long-lasting and is often treated with
hypnoticsfor long periods in clinical practice (Ib)
These studies suggest that dependence (tolerance/withdrawal)
is
not inevitable with hypnotic therapy up to 1year with
eszopiclone,zolpidem, ramelteon (Ib)
There is also evidence that dependence may be more likely
withsome agents or with polysomnography outcome measures ascompared
with self-report measures of outcome
Intermittent dosing may further reduce the risk of tolerance
anddependence (Ib)
H pnotics
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
48/64
Hypnotics
What is not known
How can we predict the needed treatment duration?
How and when should treatment be discontinued?
Should dosing for longer periods be nightly orintermittent? How
do we detect the abuse-prone individual in the clinic?
Does hypnotic therapy affect the course of insomnia or
associated conditions?
Hypnotics
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
49/64
Hypnotics
Recommendations
. Use as clinically indicated (A).
. To stop medication, try intermittent use at first if it makes
sense,then try to stop at regular intervals, say every 36
months
depending on ongoing life circumstances and with patientsconsent
(D).
. CBT during taper improves outcome (A).
Nonbenzodiazepine Hypnotics
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
50/64
Nonbenzodiazepine Hypnotics
Class Summary: These agents are used for the treatment of
acuteand short-term insomnia.
Zolpidem (Ambien)
Zolpidem binds at a benzodiazepine receptor subtype (omega
I).This receptor is found more in the central nervous system
(CNS)
than in the peripheral nervous system, which helps to account
forthe drug's hypnotic effect without significant
muscle-relaxantproperties. Unlike benzodiazepines, zolpidem does
not suppressnormal sleep architecture.
Zolpidem is rapidly absorbed, with a fast onset of action (20-30
min),and thus is a good drug for sleep induction. It decreases
sleeplatency and increases sleep duration.
Nonbenzodiazepine Hypnotics
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
51/64
Nonbenzodiazepine Hypnotics
Zaleplon (Sonata)
Zaleplon is not structurally related to benzodiazepines,
barbiturates,or other drugs with known hypnotic properties. It
interacts withthe GABA-benzodiazepine receptor complex, causing
sedation. Itshould be taken immediately before bedtime.
Zaleplon decreases the time to sleep onset. Its shorter onset
ofaction means that peak serum concentrations are achieved within1
hour of administration. This may account for the lower incidenceof
daytime grogginess and the reduced withdrawal reboundinsomnia.
Nonbenzodiazepine Hypnotics
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
52/64
Nonbenzodiazepine Hypnotics
Eszopiclone (Lunesta)
Eszopiclone is a nonbenzodiazepine hypnotic
pyrrolopyrazinederivative of the cyclopyrrolone class. Its precise
mechanism ofaction is unknown, but it is believed to interact with
GABAreceptors at binding domains close to or allosterically coupled
tobenzodiazepine receptors.
Eszopiclone is indicated for treatment of insomnia by
decreasingsleep latency and improving sleep maintenance. It has a
shorthalf-life (6 h). Higher doses (ie, 2 mg for elderly adults and
3 mgfor nonelderly adults) are more effective for sleep
maintenance,whereas lower doses (ie, 1 mg for elderly adults and 2
mg fornonelderly adults) are suitable for treating difficulty in
falling
asleep.
Ramelteon (Rozerem)
Ramelteon is a melatonin receptor agonist with high selectivity
forhuman melatonin MT1 and MT2 receptors. MT1 and MT2 arethou ht to
romote slee and to be involved in maintenance of
Antidepressants
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
53/64
Antidepressants
What is known
There is limited evidence for efficacy of doxepin,
trimipramine,trazodone, paroxetine in insomnia (Ib)
Antidepressants may affect a wide range of brain receptors
andhave longer-lasting carry-over effects than traditional
hypnotic
drugs antidepressants are associated with increased risks ofroad
accidents especially early in treatment in depression (Ib)
What is not known
Is the effect of antidepressants on insomnia lasting
(particularly asthey are often prescribed for long periods)?
Are they more efficacious than traditional hypnotics?
Do they improve mood or reduce the risk of emergent depressionin
patients?
Antidepressants
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
54/64
Antidepressants
Recommendations
. Use drugs according to a knowledge of pharmacology (A).
. Consider antidepressants when there is coexistent mood
disorderbut then use at therapeutic doses (A).
. Beware toxicity of tricyclic antidepressants in overdose even
when
low unit doses prescribed (A).There are no controlled studies of
hypnotic efficacy of low-dose
amitriptyline in insomnia, and tricyclics are more likely to be
lethalthan licensed hypnotics in overdose (Nutt, 2005a).
The seemingly paradoxical action of paroxetine to improve sleep
is
probably related to its good efficacy in many anxiety
disorders,where it seems to reduce recurrent thinking and
ruminations.
Taking SSRIs, venlafaxine, mianserin or mirtazapine increases
therisk of restless legs syndrome (RLS) and periodic limb
movementsin sleep (PMLS) (Hoque and Chesson, 2010), and SSRIs are
knownto induce or exacerbate sleep bruxism (Wilson and
Argyropoulos,
2005)
Antipsychotics
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
55/64
Antipsychotics
AntipsychoticsWhat is known about use of antipsychotics for
treatment of insomnia
Olanzapine and quetiapine improve sleep in healthy volunteers
(Ib)
Quetiapine improves sleep in primary insomnia (IIb)
Side effects are common because of the pharmacological actionsof
these drugs (I)
What is not known
How do they compare with traditional hypnotic drugs?
RecommendationSide effects are common because of the
pharmacological actions of
these drugs and there are a few reports of abuse.
Together these indicate no indication for use as first-line
treatment(D).
Cognitive Behavioural
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
56/64
Therapy
Psychological treatment of insomnia should be
consideredappropriate for two reasons. First, insomnia is
apsychophysiological disorder, in which mental and
behaviouralfactors play predisposing, precipitating and
perpetuating roles.
Essential features of insomnia are heightened arousal and
learnedsleep-preventing associations. Arousal can reflect a
generalcognitive hypervigilance and many patients describe
racingthoughts as a problem when they are trying to sleep.
A cycle develops in which the more one strives to sleep, the
moreagitated one becomes, and the less able one is to fall asleep.
CBTfor insomnia (CBTi) employs a package of interventions
designed
to encourage poor sleepers to think and behave like
goodsleepers
National Institutes of Health Consensus and State of the
ScienceStatement (NIH, 2005) concluded that a CBT package
containingcognitive and behavioural methods is as effective as
prescriptionmedications are for short-term treatment of chronic
insomnia.
Moreover, there are indications that the beneficial effects of
CBT,
Cognitive Behaviouralh
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
57/64
Therapy
What is known about CBT for insomnia - CBT
CBT is an effective treatment for insomnia delivered
eitherindividually or in small group format (Ia)
CBT has been found to be as effective as prescription
medications
for short-term treatment of chronic insomnia.Moreover, there
areindications that the beneficial effects of CBT may last well
beyondthe termination of active treatment (Ia)
What is not known
Are long-term effects of a short-term course of hypnotics better
or
worse than after CBT?
Long-term effects of CBT versus optimized (e.g. intermittent)
useof hypnotics in the long term
Special Population:M l W
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
58/64
Menopausal Women
Recommendations
. Clinicians should appreciate that there is a rise in incidence
ofsleep-disordered breathing after the menopause and that
clinicalpresentation, often including insomnia, in women is
different thanin men.
. The use of hormone therapy should involve informed
individualizedtreatment of symptoms, looking at risks and benefits
in light ofrecent studies.
. Follow recommendations for insomnia in other sections.
Special Populations: PregnantW
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
59/64
Women
Recommendations
. Good sleep hygiene and lifestyle (D).
. Manage general pregnancy-associated complaints, e.g.
decreasefluid intake, pillow support (D).
. The benefits of CBT in pregnancy have not been published
butapproach would appear sensible (B).
. Recognize RLS by careful history and investigations if
necessary.
. Dopamine agonists are contraindicated (FDA category C or
greater)
Special Populations: PregnantW
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
60/64
Women
Recommendations
. Iron and folic acid supplementation have been shown to
beeffective in RLS. Supplementation is suggested even if levels
arenot low (D)
. Keep caffeine low as it can exacerbate RLS (D)
. Mild to moderate exercise in the early evening, stretching,
massage(D)
. If patient suffers from intractable insomnia and a
pharmacologicalagent is required, zolpidem is preferable as it is
short acting and
does not have anticholinergic side effects.Short-term use is
recommended after discussion on potential risks
and benefits (D).
Special Populations: Elderly
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
61/64
Special Populations: Elderly
Recommendations
. CBT is effective and should be offered as a first line where
available(A).
. When a hypnotic is indicated in patients over 55,
prolonged-release
melatonin should be tried first (B).. If a GABA hypnotic is used
then a shorter half-life will minimize
unwanted hangover (A).
Special Populations: Children
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
62/64
p p
Recommendations
. Behavioural strategies should be tried in children with
disturbedsleep (A).
. Melatonin administration can be used to advance sleep onset
to
normal values in children with ADHD who are not on
stimulantmedication (A).
References
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
63/64
Kaplan & Sadock's Synopsis of Psychiatry, 10th Edition
American Psychiatric Association. Diagnostic and Statistical
Manualof Mental Disorders, 4th ed, Text Revision (DSM
IV-TR).Washington, DC: American Psychiatric Association; 2000.
Normal sleep and sleep disorders. In: Kaplan and Sadock's
Synopsis
of Psychiatry. 10th ed. Baltimore, Md: Williams &
Wilkins;1997:749-772.
Sleep DisordersAuthor: Roy H Lubit, MD, PhD; Chief Editor: Iqbal
Ahmed, MBBS,FRCPsych (UK)
http://emedicine.medscape.com/article/287104-overviewSleep and
Dreaming, Disorders of Sleep and Wakefulness. In:
Principles of Neural Science. 4th Edition. Kandel ER
Wilson SJ, Nutt DJ et al. British Association for
Psychopharmacologyconsensus statement on evidence-basedtreatment of
insomnia,
parasomnias and circadian rhythm disorders; Journal of
Thank You...
http://emedicine.medscape.com/article/287104-overviewhttp://emedicine.medscape.com/article/287104-overview
-
7/28/2019 Psych Grand Rounds- Primary Sleep Disorders
64/64