Embed Size (px)
Citation preview

Brief Clinical Report
Pseudodiastrophic Dysplasia Type Burgio ina Newborn
R. Fischetto,1* F. Causio,3 G. Corso,2 V. Lillo,1 B. Natale,2 and F. Papadia1
1Divisione Malattie Metaboliche-Genetica Medica, Ospedale Regionale Pediatrico ‘‘Giovanni XXIII’’, Bari, Italy2Divisione Centro Immaturi-Nipiologia, Ospedale Regionale Pediatrico ‘‘Giovanni XXIII’’, Bari, Italy3Prima Clinica Ostetrico-Ginecologica dell’Universita degli Studi di Bari, Bari, Italy
Pseudodiastrophic dysplasia is a distinctdisorder that differs from diastrophic dys-plasia on the basis of elbow and proximalinterphalangeal joint dislocations, platy-spondyly, and scoliosis. We report on a newpatient with this rare skeletal dysplasia andtwo previously undescribed major malfor-mations: omphalocele and complex heartdefect. Am. J. Med. Genet. 71:222–225, 1997.© 1997 Wiley-Liss, Inc.
KEY WORDS: pseudodiastrophic dysplasiatype Burgio; diastrophic dys-plasia; failure to thrive; om-phalocele; complex heart de-fect
INTRODUCTIONPseudodiastrophic dysplasia was first described by
Burgio et al. in 1974 as an autosomal recessive condi-tion with clinical manifestations somewhat similar tothose of diastrophic dysplasia, but with distinct roent-genographic and chondro-osseous histological findings.
Additional patients were subsequently reported byCanki et al. [1979], Eteson et al. [1986], Canki-Klain etal. [1990], and Bertrand et al. [1991].
Abnormal findings are: rhizomelic shortness oflimbs, elbow dislocation, interphalangeal joint disloca-tion of the hands, and clubfoot.
We report one additional patient with this rare skel-etal dysplasia, with new findings including omphalo-cele and congenital heart disease.
CLINICAL REPORTThe patient was the second daughter born to a 28-
year-old G2P1A0 healthy mother and her 29-year-oldnon-consanguineous healthy husband. Family history
was negative for genetic disorders. The term pregnancywas complicated by oligohydramnios; no drugs weretaken and there was no history of any illness. Caesariansection was necessary because of breech presentation.
Examination at 1 month of age showed: length 47 cm(<3rd centile), weight 2,650 g (<3rd centile), head cir-cumference 35 cm (<3rd centile), brachycephaly, roundand chubby face, frontal bossing, blue sclerae, nasalbridge with mild hypertelorism, large anteverted nos-
*Correspondence to: Dr. Rita Fischetto, Ospedale Regionale Pe-diatrico ‘‘Giovanni XXIII’’, via Amendola 207, 70126 Bari, Italy.
Received 5 April 1996; Accepted 14 October 1996 Fig. 1. The proposita with small omphalocele..
American Journal of Medical Genetics 71:222–225 (1997)
© 1997 Wiley-Liss, Inc.

trils, small asymmetric chest, omphalocele (Fig. 1),low-set ears with abnormal folding of superior helixand antitragus. Smooth philtrum, micrognathia, shortneck with pterigium colli were also observed (Fig. 2).There was rhizomelic shortness of limbs, dislocated el-bows and knees, clubfoot, interphalangeal joint flexioncontractures with ulnar deviation of the fingers, bilat-eral camptodactyly with hypoplastic nail of the thumb(Fig. 3). A systolic heart murmur could be heard.
Laboratory tests, including routine blood and urineexaminations, chromosomal analysis, thyroid screen,
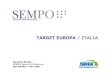
Fig. 2. Frontal bossing, flat nasal bridge, large anteverted nostrils, smooth philtrum, micrognathia, short neck.
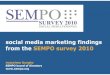
Fig. 3. Camptodactyly, hypoplastic nail of the left thumb. Fig. 4. X-ray of the skull: midface hypoplasia and cervical kyphosis.
Burgio in a Newborn 223

mucopolysaccharides screen were all normal. Echocar-diography showed mitral and tricuspidal valves incom-petence, persistent pulmonary hypertension, perimem-braneous ventricular septal defect with left-rightshunt, anterior leaflet with third-degree incompetence.
Roentgenographic findings were: enlarged bitempo-ral diameter and midface hypoplasia of the skull (Fig.4); normal clavicles and scapulae; short and anteriorlyflared ribs; kyphosis and wedge-shaped cervical spine;platyspondyly and scoliosis of the lumbar region (Fig.5); rhizomelic shortness of upper limbs, dislocated el-bows, short metacarpals, multiple interphalangealjoint dislocations; short femora with mild metaphysealflare (Fig. 6); and clubfeet.
Clinical evolution was marked by ineffectual suck-ing, failure to thrive, vomiting, and mild intermittentfever.
At four months of age the infant suffered from cya-nosis and hyperthermia not responsive to therapy. She
died of cardio-pulmonary failure. Autopsy permissionwas not obtained.
DISCUSSION
Pseudodiastrophic dysplasia is a distinct clinical en-tity, which can mimic diastrophic dysplasia in the new-born. Particular differences between these two entitiesare listed in Table I. The major clinical and roentgeno-graphic findings in our patient are consistent with thediagnosis of pseudodiastrophic dysplasia (Table II).
A severe clinical course was present in all patientspreviously described, except three cases [Eteson et al.,1986; Canki-Klain et al., 1990]. Unexplained hyper-thermia and pulmonary infections are the most com-mon cause of death in these patients; they probablyresult from failure in respiratory dynamics due to ab-normal thorax conformation.Fig. 5. Scoliosis, metaphyseal flared rhizomelic femur.
Fig. 6. Dislocated elbow, multiple interphalangeal joint dislocations.
224 Fischetto et al.

Two major malformations not previously describedwere present in our patient: omphalocele and complexheart defect involving the septal and mitral valve. Themode of inheritance of pseudodiastrophic dysplasia isautosomal recessive, although sporadic occurrence can-not be ruled out in our patient, since the cases reportedso far are still scanty.
ACKNOWLEDGMENTS
We are indebted to Professors Giampiero Beluffi andRoberto Burgio for critically reviewing this case.
REFERENCES
Bertrand JG, Zaoui C, Vandevelde MF, Desmettre C, Ramaherrison P,Cuignet PH, Noel JL, Bertrand J (1991): La dysplasie pseudodiastro-phique. Ann Ped 38 1:19–22.
Burgio GR, Belloni C, Beluffi G (1974): Nanisme pseudodiastrophique.Etude de deux soeurs nouveau-nees. Arch Fr Ped 31:681–696.
Canki N, Sernec-Logar B, Prodan M, Pintar L (1979): Le nanisme pseudo-diastrophique: A propos d’une observation. J Genet Hum 27:247–252.
Canki-Klain N, Stanescu V, Bebler P, Maroteaux P (1990): Pseudodiastro-phic dysplasia evolution with age and management. Report of two newcases and review of the literature. Ann Genet 33:129–136.
Eteson DJ, Beluffi G, Burgio GF, Bellon C, Lachman RS, Rimoin DL(1986): Pseudo-diastrophic dysplasia: A distinct newborn skeletal dys-plasia. J Pediatr 109:635–641.
Qureshi F, Jacques SM, Johnson SF, Johnson MP, Hume RF, Evans MI,Yang SS (1995): Histopathology of fetal diastrophic dysplasia. Am JMed Genet 56:300–303.
TABLE II. Clinical and Roentgenographic Manifestations ofPseudodiastrophic Dysplasia*
Findings Present + previous cases
Reduced birth length 10/10Blue sclerae 6/10Hypertelorism 7/10Large malformed ear lobes 10/10Cleft palate 6/10Congenital heart defect 1/10Omphalocele 1/10Contractures 8/10Rhizomelic shortness of limbs 10/10Dislocated elbows 9/10Interphalangeal joint dislocations 10/10Scoliosis 9/10Clubfeet 9/10Platyspondyly 10/10Horizontal acetabular roof 10/10
*A compilation of this patient and the seven previously reported cases:Burgio et al., [1974], Canki et al. [1979], Eteson et al. [1986], Canki-Klain[1990], and Bertrand et al. [1991].
TABLE I. Differentiating Traits of PseudodiastrophicDysplasia and Diastrophic Dysplasia
Pseudodiastrophicdysplasia
Diastrophicdysplasia
Face Round SquareFlat nasal bridge Narrow nasal bridgeMidface hypoplasia Broad midnoseMicrognathia Micrognathia
Ears Large, malformedlobes
Cystic swelling of thepinnae
Nose Large, antevertednostrils
Flared nostrils
Mouth Narrow Full and broadCleft palate Cleft palate (25%)
Spine PlatyspondylyEarly scoliosis Late scoliosis
Upper Rhizomelic shortness Flare of the inferiorlimbs Elbow dislocation radial metaphysis
Multipleinterphalangealjoint dislocations
Shortness of the firstmetacarpal bone
Camptodactyly Interphalangeal jointcontractures
Proximally placedthumbs
Lower Knee dislocation Hip dysplasialimbs Clubfoot deformities Severe clubfoot
deformitiesHistology of
cartilageIrregular mixoid
degeneration withsmall cystic areas
Fibrous degenerationIrregular
proliferativecolumns
Prognosis Severe during thefirst weeks ormonths of life
Death later in life
Burgio in a Newborn 225