Embed Size (px)
Citation preview

20
and the following facts elucidated. Two years agoshe had suffered from a severe attack of influenzawhen at Sheffield, at the time when this disease wasmanifesting a pandemic spread, during which she hadrun a high temperature for two to three weeks, accom-panied by severe vomiting and haemorrhages from thenose and mouth. Altogether she was in bed for fiveweeks, and had felt somewhat weak for a year after-wards. Last Christmas, when away in the countrystaying with her sister, who had returned from Indiaafter a prolonged attack of sprue, she had had anotherattack of fever, likewise diagnosed as influenza, startingwith a high temperature and vomiting, which persistedfor three or four days. A week after her recovery shewas attacked with abdominal pain followed by diarrhoeawith the passage of blood and mucus, which continuedfor nearly ten days before finally passing off ; duringthis time the patient continued up and about, thoughfeeling very weak. Since then she has had a
slight degree of debility, and has been unable to takeany violent exercise. It was thought possible that thepatient might have been infected with an organism ofthe dysentery group from her sister, though the latterapparently never had anything to do with the prepara-tion of the food in the house. To test this the serumof the patient was put up on Oct. 4th, the 16th dayof her illness, against emulsions of B. dyse2teric,Flexner, V, , X, Y, Z, and against one of B. !/s6?eWtB,Shiga, but the agglutinations were all negative in adilution of 1-50.There yet remains the possibility that her sister may
have been infected with the B. ente1’itidis, and from herMiss X had become infected with the resulting illnessmarked by abdominal pain and diarrhoea. Failing torid herself entirely of the organism she had remained acarrier, and her recent illness might have been due toan exacerbation of the activity of this organismoccurring while the patient was in a debilitated con-dition. Unfortunately, as her sister does not live inLondon it has not been possible as yet to procure asample of her blood for examination, but if occasionoffers this will certainly be done.
<S’:MKMKt)’7/.(1) A case is reported of a patient suffering from
pyrexia which simulated closely a typhoid course, butwhich was probably due to infection with the B. ente1’i-t’idis of Gaertner. The case, moreover, was of a purelysporadic nature, and was unconnected with any co-
existing outbreak of food-poisoning.(2) It is suggested that it would be advisable in view
of this case to test the sera of patients suffering fromenteric-like infections against a more extended seriesof antigens than are commonly employed, in order toascertain whether sporadic infections with organisms ofthe enteric group other than B. typhos1Ls, B. pa1’a-typhosus A, and B. pa7cttyphosis B are more than merepathological entities.
It is with pleasure that we record our gratitude firstof all to Dr. Fenton for his kind permission in allowingus to publish the case ; secondly to Dr. W. W. C. Topley,director of the Institute of Pathology, Charing CrossHospital Medical School, for giving us advice from hisextensive bacteriological experience of cases of entericinfections; and, thirdly, to the clinical staff of thehospital for the help and facilities they afforded us.
Refere7zces.-1. W. G. Savage : Report to the L.G.B. on BacterialFood-poisoning and Food Infection, Food Reports No. 18, 1913.2. F. A. Bainbridge: Milroy Lectures on Paratyphoid Fever andMeat-poisoning, THE LANCET, 1912, i., p. 849. 3. G. Dean : Journ.Hygiene, 1911, xi., p. 259. 4. G. S. Buchanan : Report on an Out-break of Illness at Mansfield caused by Eating Potted Meat,Report of M.O. to L.G.B., 1896-97, p. 115. 5. W. G. Savage : Reportupon the Presence of Paratyphoid Bacilli in Man, Report of 1VL0.to L.G.B., 1908-09. p. 316. 6. W. G. Savage : Food-poisoning andFood Infections, Camb. Univ. Press, 1920, p. 66. 7. Ibid., p. 48.8. R. P. Garrow : The Myth of Atypical Enteric Infections,THE LANCET, 1920, ii., p. 886. 9. W. W. C. Topley, S. G. Platts,and C. G. Imrie: A Report on the Probable Proportion ofEnteric Infections among Undiagnosed Febrile Cases Invalidedfrom the Western Front since October, 1916, Special Report Series,No. 48, Medical Research Committee, 1920. 10. Zwick, 1909 : Uberdas Vorkommen von Enteritisbazillen in der Milch, Centralb. f.Bakt., xliv., ref. Beiheft, p. 132. 11. Mohler and Buckley, 1902:Report on an Enzootic Among Cattle caused by a Bacillus of theEnteritidis Group, Nineteenth Annual Report of the Bureau ofAnnual Industry.
PSEUDO-COXALGIA:OSTEO-CHONDRITIS DEFORMANS JUVENILIS.
BY H. A. T. FAIRBANK, D.S.O., O.B.E., M.S.LOND.,F.R.C.S. ENG.,
SENIOR ORTHOPÆDIC SURGEON TO KING’S COLLEGE HOSPITAL;SURGEON TO THE HOSPITAL FOR SICK CHILDREN,
GREAT ORMOND-STREET, LONDON.
So little attention has been paid to the above affectionin this country, except by orthopaedic surgeons, that abrief description of what is known of the disease maybe of interest, and may result in greater numbers ofthese cases being recognised and recorded. Since theappearance some ten years ago of the original papersdealing with the subject, by A. T. Legg in America,J. Calve in France, and Perthes in Germany, little hasbeen written on the subject in-this country. Caseshave been reported by R. C. Elmslie, D. P. D.Wilkie, H. H. Platt, E. M. Little, and the writer,while Mr. Muirhead Little published a short paperon this subject in the Clinical Journal in 1915. Anexhaustive paper by Legg on the facts and theoriesto date may be found in Surgery, Gynaecology, andObstetrics of the following year. The chief importancein recognising this condition lies in the differencebetween its prognosis and that of tuberculous hipdisease, for which it is not uncommonly mistaken.Juvenile osteo-chondritis, which is by no means rare,affects children from 3 to about 12 years of age, andmales more commonly than females ; it is usuallyunilateral, but may be bilateral.
Description of a Typical Case.A healthy-looking child of, say, 6 years of age, of an
active disposition and fond of games, begins to limp on
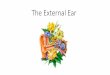
FiG. l.-Tracing of skiagram of unilateralcase of pseudo-coxalgia. Boy aged 5 years.
one leg ; perhapsthere is a history ofsome antecedentfall on the hip, butnot such as wouldraise a suspicionof f any serious
injury; the limppersists, and isaccompanied bylittle or no pain.
Eventually advice is sought, and examination revealsthe following facts.The position of the limb at rest is usually normal.
There is slight wasting of the thigh and buttock, withresulting apparent prominence of the trochanter; sor4ethickening of the neck of the femur, particularly on theinner side, may occasionally be felt; abduction of thehip is markedly limited or obliterated, while flexionremains free, almost, if not quite, to the normal limit ;internal rotation and extension may be somewhatlimited; at this stage there is no shortening, and rarelydoes the shortening amount to much. Trendelenburg’ssign is usually positive. There is no pain on jarring thetrochanter or heel. Skiagraphic examination revealscnaractensuic
appearances; theepiphysis of thehead of the femuris flattened fromabove down-
wards, irregular Bin outline and
density, or evenbroken up into
fragments ; the
epiphyseal line isless distinct than
FIG. 2.-Tracing of skiagram of bilateral caseof pseudo-coxalgia. Boy aged 6 years.(Seen with Mr. 0. Addison.)
it should be, as if invaded by calcified tissue from bothepiphysis and neck; the juxta-epiphyseal region of theneck is irregular and fluffy, and there may be clearsemi-transparent areas adjacent to the epiphyseal line,more commonly at the upper angle of the neck ; on thelower side the neck is thickened ; the joint space is notdiminished, showing that the cartilaginous head is
little, if at all, distorted, but that the changes are

21
rather in the ossific centre inside it; the pelvis may beasymmetrical, the affected side being slightly thesmaller of the two ; the acetabulum may show changesin the way of fluffiness and want of definition.
Progress, Treatment, and Etiology.The progress of the case is always towards recovery.
Abscess formation and other complications seen in truehip disease never occur. Most writers agree in statingthat treatment, or entire absence of treatment, haslittle, if any, effect on the ultimate result. Radiogramstaken at intervals for one, two, or even three yearsshow that after a time the ossification of the epiphysisreturns to the normal, until at last the hemispherical-shape of the ossific centre is restored. Finally, theremay be some mushrooming of the head of the femur,so that the appearance would justify the diagnosis ofone form of juvenile osteo-arthritis. The limp, usuallyslow in disappearing, is eventually lost. Spasm ofmuscles may occasionally be a feature in the earlystages, when the diagnosis may be difficult. As a rulethe diagnosis is easy.Although treatment is said to have no effect, it is
wiser to order a walking calliper splint to take theweight off the femur, while cases with an unusualamount of pain or spasm must be treated with completerest and extension for a time. Muirhead Little advisesabduction under anaesthesia and fixation in plaster, sothat changes in the shape of the head that might limitabduction may be avoided.As to the nature of the affection nothing definite is
known. The theory which receives the greatest amountof support is that trauma produces damage to the blood-supply of the head of the femur, and that the changesin the ossification of the bone are secondary to thisdamage. Developmental error-as a predisposing ifnot the sole cause-local infection, and rickets haveall been suggested in explanation of the appearances.Tubercle and -yphilis can undoubtedly be ruled out ofcourt. Suffice it to say that there are difficulties in theway of accepting the traumatic theory, but the dis-cussion of this subject must be left for a subsequentpublication elsewhere. Similar radiographic changesin an epiphysis are met with in other regions ofthe body.
______________
A NOTE ON
SPIROCHÆTES IN THE ÆTIOLOGY OFCERTAIN PARALYSES.
BY G. SCHUSTER, M.D.,ASSISTANT PROFESSOR AT THE PSYCHOLOGICAL AND NEUROLOGICAL
CLINIC OF THE ROYAL HUNGARIAN UNIVERSITY OF BUDAPEST.
AT the suggestion of Professor E. E. Moravcsik, M.D.,I started research in the parasitology and pathologicaltissues of general paralysis of the insane, at the Psycho-logical and Neurological Clinic of the Royal HungarianUniversity of Budapest, soon after the publication ofNoguchi’s researches. The outbreak of war preventedme continuing this work, but I was able to resume itat the end of 1918. I include in this short contribution
s my more important observations on the presence ofspirochaetes in the central nervous system, beforepublishing a longer description of the cases treated inthis clinic in view of their parasitological, clinical, andtherapeutical applications. I also take the opportunityof reporting an interesting diagnosis in a case ofdisseminated sclerosis.
Levaditi, Marie, Bunkowsky, Moore before Jahnel, laterHauptmann have shown the presence of spirochsetes inlarge quantities in the cortex of patients suffering fromG.P.I. with paroxysms ; they regarded the paroxysms as dueto mechanical and toxic effects of the sudden increase ofspirochaetea. During my researches I have noticed thatthe spirochsetes are situated chiefly in the lower strataof the cortex, sometimes in such quantity as to showalmost a pure culture. This was noticed not onlyin cases of G.P.I. with paroxysms, but also in thosewithout. In eight cases of G.P.I. the main colonies werein the boundary of the cortex and the medullary substance,and in the lowest strata of the cortex; this was so, notonly when the spirochsetes were localised, but when
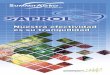
diffused over the whole area of the cortex. It is difficult tosay without further research whether the spirochastes arepermanently localised in these strata, because their dis-semination is prevented by some means, or because the circu-latory or microchemical environment is favourable. Someobservations convinced me of the pathological and clinicalimportance of the boundary of the cortex and the medullarysubstance. In certain cases of disseminated sclerosis thesclerotic spots are mostly on this boundary. I found, as didSiemerling, in an acute and in a chronic case that the dis-integration of the medullary sheath was situated underneaththe cortex and in the lower boundary of the cortex. In cases ofdiffuse sclerosis and peraxial sclerosis (Rossolimo, Angyan,
FIG. 1.—Heterotopia, in disseminated sclerosis.
Schilder) the spots of disintegration of the medullary sheathwere immediately underneath the cortex, also overspreadingsome areas of the cortex; disintegration of the medullarysheath in the cases of G.P.I. (which were similar to thosein disseminated sclerosis) was also to be seen on theboundary of the cortex and medulla, as was shown bySiemerling, Spielmeyer, Borda, and Fischer. These observa-tions show that there are certain places in the centralnervous system which have microchemical properties ofimportance in the aetiology of G.P.I. ; in regard to the para-sitological aspect the lower strata of the cortex seems tohave microchemical affinity with the spirochsetes.The spirochaetes appear in largest quantity in this place,
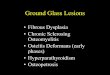
and the so-called degenerative forms are mostly in the upperstrata of the cortex. In an interesting case of disseminatedsclerosis I found fine spirochsetes diffusely spread in theupper strata of the cortex., (Figs. 1 and 2.) This diagnosis
Fie. 2.—Spirochsetes in the cortex of a case of disseminatedsclerosis.
shows an affinity between disseminated sclerosis and G.P.I.in regard to aetiology; the gold sol reaction of the cerebro-spinal fluid is similar in disseminated sclerosis, in G.P.I., andin cerebral syphilis ; it is probable that the spirochaetes foundby Kuhn and Steiner are a similar kind to the S. pallida. Itwas impossible to show spiroohsetes in the brain of patientssuffering from G.P.I. in those cases when 10 per cent.formalin was injected into the brain through the carotidstwo hours after death. I thought I should be able in thisway to fix the spirochsetes thoroughly and instantaneouslyaround the veins, but either the formalin stream carried offthe spiroch2etes or they did not happen to be present in thatpart of the tissue examined. If, indeed, the formalin streamcarries off the spirochsetes this would be a favourable factfrom the therapeutic point of view. We cannot yet judgethe results of the carotid injections made by Knauer. It is













![Veterans Benefits: Compensation & · PDF file[VETERANS BENEFITS: COMPENSATION & PENSION] ... Osteitis deformans (Paget’s disease). Osteomalacia. Palsy, bulbar. Paralysis agitans](https://img.pdfslide.us/doc/110x75/5a7353817f8b9aa2538e908e/veterans-benefits-compensation-pensioncymcdncomsites-veterans-benefits.jpg)


![The Impact of Subungual Osteochondroma Deformans on ... · phyton rubrum, causes most of the superficial fungal infections[4]. Kemna et al. found that dermatophytes had caused 94.7%](https://img.pdfslide.us/doc/110x75/5f449bf610b3724522676a00/the-impact-of-subungual-osteochondroma-deformans-on-phyton-rubrum-causes-most.jpg)









