Embed Size (px)
Citation preview
ProtocolMedicationTherapyAdherenceClinicHEPATITIS
Pharmaceutical Services DivisionMinistry of Health Malaysia
Lot 36, Jalan Universiti,46350 Petaling Jaya, Selangor.
Tel: 03-78413200 Fax: 03-79682222/79682268
Book. Hepatitis MTAC_1.1.indd 1 11/9/15 7:22 PM
First Edition, 2015Pharmaceutical Services DivisionMinistry of Health Malaysia
ALL RIGHTS RESERVEDNo part of this publication may be reproduced, stored or transmitted in any form or by any means whether electronic, mechanical, photocopying, tape recording or others without prior written permission from the Senior Director of Pharmaceutical Services Ministry of Health Malaysia
Perpustakaan Negara MalaysiaCataloguing-in-Publication Data
Book. Hepatitis MTAC_1.1.indd 2 11/9/15 7:22 PM

i
PREFACE
Hepatitis is a disease which needs serious attention as long-term complications lead to high health and economic burden. The seriousness of the problem is being addressed through a national strategic plan and pharmacists should be together with other healthcare professionals in managing patients with this disease, thus minimising complications.
Adherence to treatment with interferon and nucleoside analogues is among the critical factors which determine the success of hepatitis treatment. Medication counselling and assessment of adherence are thus indispensable to ensure patients’ adherence to therapy. Pharmacists who are trained in the management of hepatitis are expected to play this role. Apart from that, the ability to identify and solve drug-related problems is the basic skill of a pharmacist through which he or she can contribute effectively as part of the hepatitis care team.
This protocol is meant for pharmacists in the Ministry of Health (MOH) who provide Hepatitis Medication Therapy Adherence Clinic service. The protocol will guide pharmacists who plan to initiate such a service and ensure standardisation of practice throughout all MOH facilities.
I would like to congratulate all contributors for their effort in developing this protocol.
ABIDA HAQ BINTI SYED M. HAQDIRECTORPharmacy Practice and DevelopmentPharmaceutical Services DivisionMinistry of Health Malaysia
Book. Hepatitis MTAC_1.1.indd 3 11/9/15 7:22 PM
ii
AdvisorsAbida Haq binti Syed M. Haq
Director of Pharmacy Practice and DevelopmentPharmaceutical Services Division, MOH
ContributorsPoh Wei Yoon
Hospital Selayang
Law Bee KengHospital Queen Elizabeth 1, Kota Kinabalu
Loh Sze YanHospital Sultanah Bahiyah, Alor Setar
Nurul Nadiah binti Abd. RahimHospital Melaka
ReviewersRosminah binti Mohd. Din
Deputy DirectorPharmaceutical Services Division, MOH
Noraini binti MohamadSenior Principal Assistant Director
Pharmaceutical Services Division, MOH
Hazimah binti HashimSenior Principal Assistant Director
Pharmaceutical Services Division, MOH
AcknowledgementPharmacy Department
Hospital Selayang
Book. Hepatitis MTAC_1.1.indd 4 11/9/15 7:22 PM
iii
CONTENTS PAGE A. INTRODUCTION ................................................................................... 1 B. OBJECTIVES ........................................................................................ 2 C. SCOPE OF SERVICE .............................................................................. 2 D. MANPOWER REQUIREMENT ................................................................. 2 E. APPOINTMENT ..................................................................................... 2 F. PROCEDURES
1. PATIENT SELECTION .................................................................................. 3 2. INITIAL VISIT (PATIENT ASSESSMENT AND EDUCATION) ......................... 3 3. SUBSEQUENT VISITS (ASSESSMENT, MONITORING AND COUNSELLING) ..... 4 4. COMPLETION AND MISSED VISIT .............................................................. 4 5. PHARMACEUTICAL REVIEW ....................................................................... 5 6. DOCUMENTATION...................................................................................... 6
G. REFERENCES ....................................................................................... 6 H. APPENDICES
1. Appendix Ia: HEPATITIS MTAC WORKFLOW (INITIAL VISIT)................... 8 2. Appendix Ib: HEPATITIS MTAC WORKFLOW (SUBSEQUENT VISITS) ..... 93. Appendix II: PATIENT’S AGREEMENT FORM ......................................... 10 4. Appendix III: PATIENT’S PROFILE AND ASSESSMENT FORM ............... 11 5. Appendix IVa: PATIENT’S MEDICATION DIARY ..................................... 13 6. Appendix IVb: DIARI UBAT-UBATAN PESAKIT ......................................... 16 7. Appendix Va: HEPATITIS C KNOWLEDGE PRE/POST-ASSESSMENT TEST ..... 19 8. Appendix Vb: UJIAN PENGETAHUAN HEPATITIS C SEBELUM/SELEPAS
KAUNSELING .......................................................................................... 20 9. Appendix VI: PRETREATMENT COUNSELLING CHECKLIST ................. 21 10. Appendix VII: TREATMENT DOSING AND DURATION TABLE ................ 22 11. Appendix VIII: SCHEDULE OF PERIODIC TESTS ................................... 24 12. Appendix IX: DOSAGE ADJUSTMENT TABLE ........................................ 25
Book. Hepatitis MTAC_1.1.indd 5 11/9/15 7:22 PM
iv
13. Appendix Xa: RESPONSE-GUIDED THERAPY FOR CHRONIC HEPATITIS C: GENOTYPE 1 ..................................................................... 27
14. Appendix Xb: RESPONSE-GUIDED THERAPY FOR CHRONIC HEPATITIS C: GENOTYPE 2 AND 3 .......................................................... 28
Book. Hepatitis MTAC_1.1.indd 6 11/9/15 7:22 PM
15. Appendix XI: TREATMENT RESPONSE: DEFINITION OF TERMS .......... 29 16. Appendix XII: CRITERIA FOR MAJOR DEPRESSIVE EPISODE: DSM-5 ............. 30
19. Appendix XIVc: SELF- INJECTION TECNIQUE CHECKLIST: S/C Standard Interferon α-2b (Intron-A®)
....................................................... 31
18. Appendix XIVb: SELF-INJECTION TECNIQUE CHECKLIST: S/C Pegylated IFN α-2b (Peg-Intron®) ..................................................32
.................................................. 34
17. Appendix XIVa: SELF-INJECTION TECNIQUE CHECKLIST: S/C Pegylated IFN α-2a (Pegasys®)
1
A. INTRODUCTION Hepatitis B (HBV) and hepatitis C virus (HCV) infections are global health problems. The latest WHO data suggest that more than 185 million people are infected with HCV worldwide, of whom 350,000 die each year. The estimated prevalence of hepatitis C infection in Malaysia is around 2% of the population.1
Chronic hepatitis C has been associated with serious clinical sequelae, such as development of hepatic fibrosis, cirrhosis of the liver and hepatocellular carcinoma.
Studies have shown that participation of clinical pharmacists in medication therapy management of patients brings a lot of benefits by facilitating patients’ adherence to their therapy, improving outcomes of drug therapy and increasing the cost-effectiveness of treatment. These promising results were shown in the pharmacist-managed clinics of chronic disease states such as diabetes mellitus, hyperlipidaemia and asthma.2,3,4,5,6
Studies have shown that pharmacists were able to identify and respond to potential opportunities for improvements in medication use. In Hepatitis Clinics, pharmacists assist patients with drug adherence, management of drug adverse effects and disease state, provision of medication information and achievement of overall treatment goals which increased the probability of HCV treatment success. 7,8,9,10
Book. Hepatitis MTAC_1.1.indd 1 11/9/15 7:22 PM
2
B. OBJECTIVES 1. To maximise the benefits of medication therapy in hepatitis patients. 2. To provide in-depth education for caregivers and patients regarding
their disease(s) including appropriate use of their medications and how to engage in wellness and preventive precautions.
3. To collaborate with healthcare teams and provide consultative services on hepatitis medication-related issues including adverse effects or complications.
4. To assist patients in achieving treatment goals by increasing adherence to medications and their engagement in the process.
5. To customise counselling for specific medication(s) and follow-up with the aim to provide individualised medication therapy management.
C. SCOPE OF SERVICE 1. The Hepatitis MTAC service will operate in the clinic area during clinic
days or in the ward when necessary. 2. The Hepatitis MTAC pharmacist will perform a multitude of duties
throughout the day: assessing patients and addressing their needs, documenting interventions and plans, providing appropriate education to patients/caregivers and completing follow-ups.
3. Activities at the clinic should be structured according to the suggested workflow (refer Procedures).
D. MANPOWER REQUIREMENTOn Hepatitis MTAC days, at least one (1) pharmacist should be placed in the clinic.
E. APPOINTMENTAll appointments will be scheduled by the pharmacist or other healthcare provider participating in the clinic/ward.
Book. Hepatitis MTAC_1.1.indd 2 11/9/15 7:22 PM
3
F. PROCEDURES1. PATIENT SELECTION
Hepatitis (B/C) patients who are planned for treatment with interferon.
2. INITIAL VISIT (PATIENT ASSESSMENT AND EDUCATION) 2.1 The pharmacist will perform an interview with the patient and/or
the caregiver and perform initial assessment on the patient. The initial evaluation will involve:A. Patient informationB. Medical and medication historiesC. Medication knowledge and adherence (for other diseases)D. Diet and lifestyleE. Risk factors (social and family histories)F. Relevant radiology and laboratory investigations (FBC, BUSE/
creatinine, LFT, UPT, thyroid function test etc.)
2.2 Hepatitis C education and pretreatment counselling (refer Appendix VI) will be delivered to the patient.
2.3 Hepatitis C knowledge preassessment test (refer Appendix V) will be conducted to assess patient’s understanding.
2.4 Pharmaceutical care issues (if any) should be determined.
2.5 Documentations should be made on related forms (refer Appendix III and IVa/b).
2.6 Patient’s Agreement Form (refer Appendix II) should be filled up during this visit.
2.7 The pharmacist will follow the next clinic appointment date as decided by the prescriber.
Book. Hepatitis MTAC_1.1.indd 3 11/9/15 7:22 PM
4
3. SUBSEQUENT VISITS (ASSESSMENT, MONITORING AND COUNSELLING) 3.1 Patient’s subsequent appointments should be based on the patient’s
next clinic appointment date. However, the MTAC pharmacist may contact patient to reschedule appointment date based on the following criteria:A. Poor adherence B. Poor self–injection technique C. Other reasons as determined by the MTAC pharmacist
3.2 During follow-up visits, the pharmacist will review the patient and conduct: A. Counselling on medication and treatment goals (refer Education
Material) B. Reassessment on injection technique (refer Appendix XIVa/b/c) C. Adherence assessment for oral pills (refer Appendix XIII) D. Adverse drug reaction monitoring (refer Appendix III) E. Monitoring of virological response and other relevant laboratory
investigationsF. Post-assessment test at fifth visit (refer Appendix Va/b) to
reassess patient’s understanding
3.3 The next appointment date should be assigned and documentations should be made accordingly (refer Appendix IVa/b).
4. COMPLETION AND MISSED VISITS 4.1 A patient is considered as having completed Hepatitis MTAC
programme upon completion of his/her treatment course OR upon treatment discontinuation by physician due to clinical reasons.
4.2 Patient will be contacted on the review date if he/she misses a Hepatitis MTAC visit to reschedule the appointment.
Book. Hepatitis MTAC_1.1.indd 4 11/9/15 7:22 PM
5
5. PHARMACEUTICAL REVIEW 5.1 To be done by Hepatitis MTAC pharmacist at the earliest opportunity
based on patient selection criteria, or after referral by prescribers/other healthcare professionals.
5.2 Identify medication-related problems: • e.g.ADRs,renaladjustmentdose,interactions,contraindicationsetc.
5.3 Solve medication-related problems: • Considernon-pharmacologicaltherapythatmayhelp• Identifythemostsuitablepharmacologicaltherapythatmayhelp
to prevent or solve the problem (consider the pros and cons of each therapeutic alternative)
• Formulatepatient-specificactionplanwithpatientandprescriberusing holistic approach (i.e. consider the patient’s medical, social and financial needs)
5.4 Drug therapy monitoring: • Monitorpatient’sadherencetothepharmacotherapyplan• Follow-up patient’s disease progression (e.g. laboratory
investigations etc.). Discuss with patient and prescribers to ensure the achievement of desired outcomes; modify the existing plan if necessary
• Assessandcounselonproperuseofmedications• MonitorADRsanddeterminetheactionplanwheneverneeded
5.5 Education on disease (hepatitis): • e.g.prevention,transmission,progressionetc.
5.6 Pharmacist’s recommendation: • Offerfeedbackandevidence–basedrecommendationstopatient
and prescriber
Book. Hepatitis MTAC_1.1.indd 5 11/9/15 7:22 PM
6
6. DOCUMENTATION All relevant data and recommendations/interventions shall be recorded in designated forms and patient’s case note accordingly (refer Appendix III and IVa/b).
G. REFERENCES1. World Health Organization. Guidelines for the screening, care and
treatment of persons with hepatitis infection. [Accessed 19th August 2014].
2. Borenstein JE, Graber G, Saltiel E, Wallace J, Ryu S, Archi J et al. Physician-pharmacist co-management of hypertension: a randomized, comparative trial. Pharmacotherapy. 2003; 23(2):209-16.
3. Yanchick JK. Implementation of a drug therapy monitoring clinic in a primary-care setting. Am J Health Syst Pharm. 2000; 57 Suppl 4: S30-4.
4. Bozovich M, Rubino CM, Edmunds J. Effect of a clinical pharmacist-managed lipid clinic on achieving National Cholesterol Education Program low-density lipoprotein goals. Pharmacotherapy. 2000; 20(11): 1375-83.
5. Dolder NM, Wilhardt MS, Morreale AP. Justifying a multidisciplinary high-intensity hepatitis C clinic by using decision analysis. Am J Health Syst Pharm. 2002; 59(9): 867-71.
6. Snella KA, Sachdev GP. A primer for developing pharmacist-managed clinics in the outpatient setting. Pharmacotherapy. 2003; 23(9):1153-66.
7. Mariño EL, Alvarez-Rubio L, Miró S, Modamio P, Banos F, Lastra CF, et al. Pharmacist intervention in treatment of patients with genotype 1 chronic hepatitis C. J Manag Care Pharm. 2009; 15(2):147-50.
8. Smith JP, Dong MH, Kaunitz JD. Evaluation of a pharmacist-managed hepatitis C care clinic. Am J Health Syst Pharm. 2007; 64(6):632-36.
Book. Hepatitis MTAC_1.1.indd 6 11/9/15 7:22 PM

7
9. Kolor B. Patient education and treatment strategies implemented at a pharmacist-managed hepatitis C virus clinic. Pharmacotherapy. 2005; 25(9):1230-41.
10. Rodis JL, Kibbe P. Development of a hepatitis C support group. Am J Health Syst Pharm. 2006; 63(17):1594-96.
Book. Hepatitis MTAC_1.1.indd 7 11/9/15 7:22 PM
8
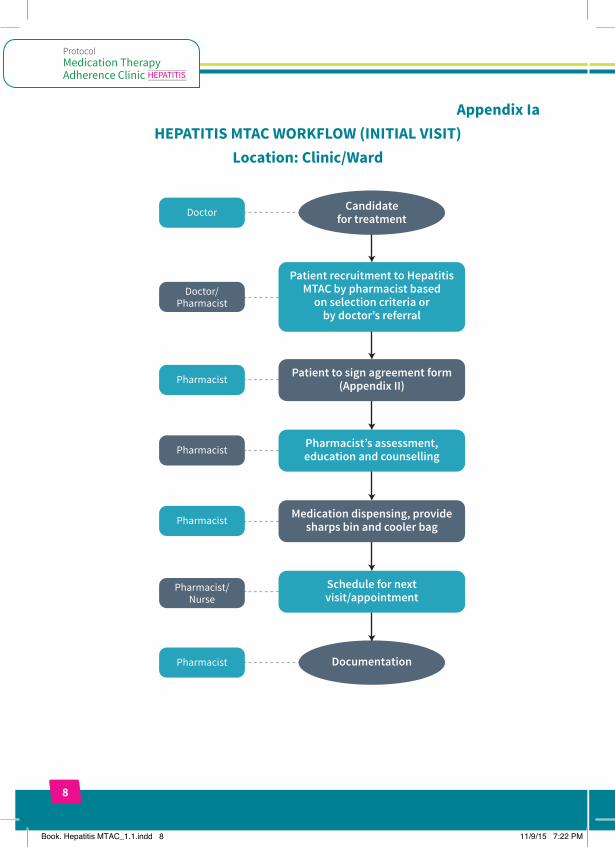
Appendix IaHEPATITIS MTAC WORKFLOW (INITIAL VISIT)
Location: Clinic/Ward
Documentation
Candidatefor treatment
Patient recruitment to Hepatitis MTAC by pharmacist based
on selection criteria orby doctor’s referral
Patient to sign agreement form (Appendix II)
Doctor
Doctor/Pharmacist
Pharmacist/ Nurse
Pharmacist
Pharmacist
Pharmacist
Pharmacist
Pharmacist’s assessment, education and counselling
Medication dispensing, provide sharps bin and cooler bag
Schedule for next visit/appointment
Book. Hepatitis MTAC_1.1.indd 8 11/9/15 7:22 PM
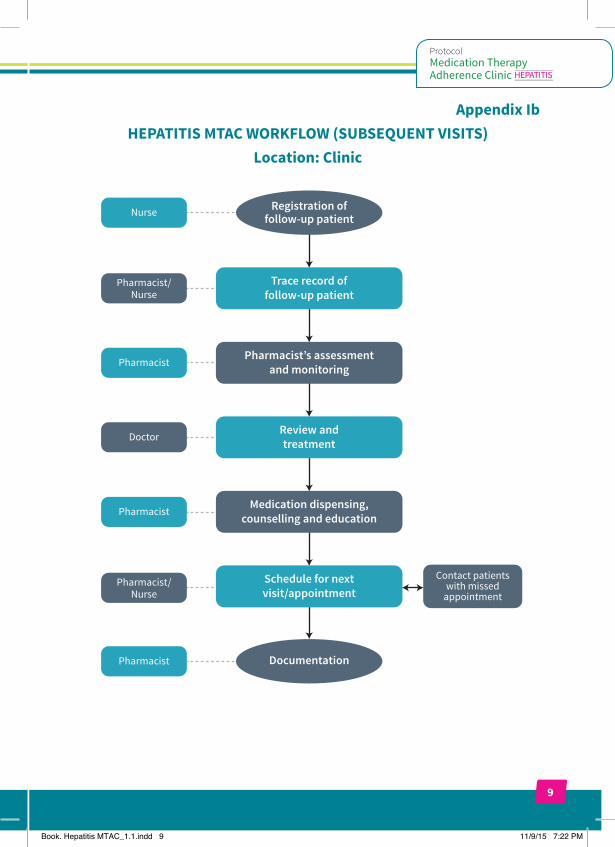
9
Appendix IbHEPATITIS MTAC WORKFLOW (SUBSEQUENT VISITS)
Location: Clinic
Nurse
Pharmacist/Nurse
Pharmacist/ Nurse
Pharmacist
Doctor
Pharmacist
Pharmacist
Registration offollow-up patient
Documentation
Pharmacist’s assessmentand monitoring
Review andtreatment
Trace record offollow-up patient
Medication dispensing,counselling and education
Schedule for nextvisit/appointment
Contact patients with missed
appointment
Book. Hepatitis MTAC_1.1.indd 9 11/9/15 7:22 PM
10
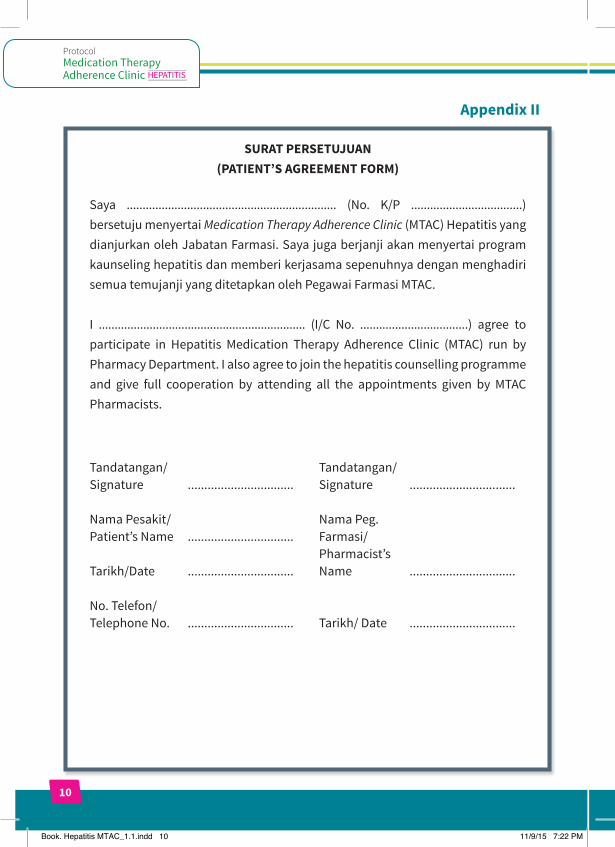
Appendix II
SURAT PERSETUJUAN (PATIENT’S AGREEMENT FORM)
Saya .................................................................. (No. K/P ...................................) bersetuju menyertai Medication Therapy Adherence Clinic (MTAC) Hepatitis yang dianjurkan oleh Jabatan Farmasi. Saya juga berjanji akan menyertai program kaunseling hepatitis dan memberi kerjasama sepenuhnya dengan menghadiri semua temujanji yang ditetapkan oleh Pegawai Farmasi MTAC.
I ................................................................. (I/C No. ..................................) agree to participate in Hepatitis Medication Therapy Adherence Clinic (MTAC) run by Pharmacy Department. I also agree to join the hepatitis counselling programme and give full cooperation by attending all the appointments given by MTAC Pharmacists.
Tandatangan/ Signature
Nama Pesakit/ Patient’s Name
Tarikh/Date
No. Telefon/ Telephone No.
................................
................................
................................
................................
Tandatangan/ Signature
Nama Peg. Farmasi/ Pharmacist’s Name
Tarikh/ Date
................................
................................
................................
Book. Hepatitis MTAC_1.1.indd 10 11/9/15 7:22 PM
11
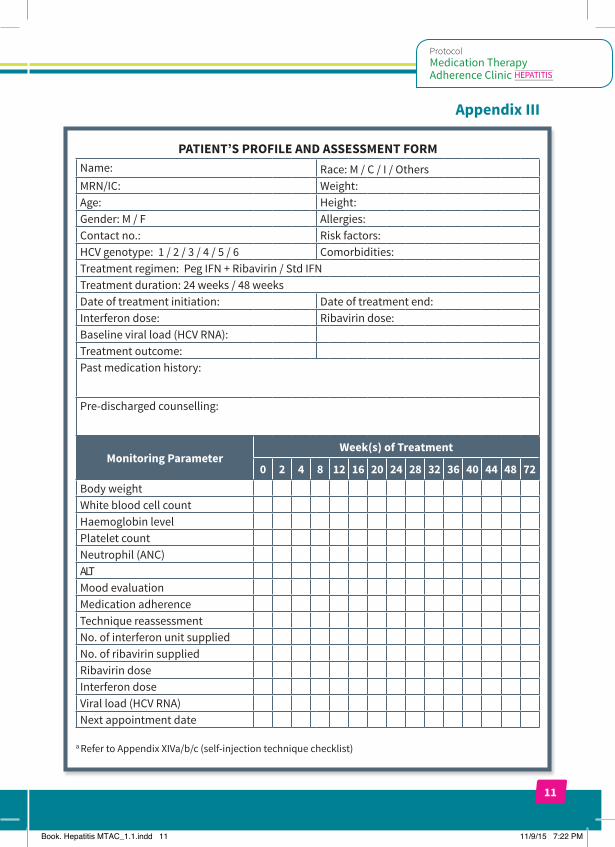
Appendix III
PATIENT’S PROFILE AND ASSESSMENT FORMName: Race: M / C / I / OthersMRN/IC: Weight:Age: Height:Gender: M / F Allergies:Contact no.: Risk factors:HCV genotype: 1 / 2 / 3 / 4 / 5 / 6 Comorbidities:Treatment regimen: Peg IFN + Ribavirin / Std IFN Treatment duration: 24 weeks / 48 weeksDate of treatment initiation: Date of treatment end:Interferon dose: Ribavirin dose:Baseline viral load (HCV RNA):Treatment outcome: Past medication history:
Pre-discharged counselling:
Monitoring Parameter Week(s) of Treatment
0 2 4 8 12 16 20 24 28 32 36 40 44 48 72
No. of interferon unit suppliedNo. of ribavirin suppliedRibavirin doseInterferon doseViral load (HCV RNA)Next appointment date
Book. Hepatitis MTAC_1.1.indd 11 11/9/15 7:22 PM
a Refer to Appendix XIVa/b/c (self-injection technique checklist)
Body weightWhite blood cell count Haemoglobin levelPlatelet countNeutrophil (ANC)ALTMood evaluationMedication adherenceTechnique reassessment
12
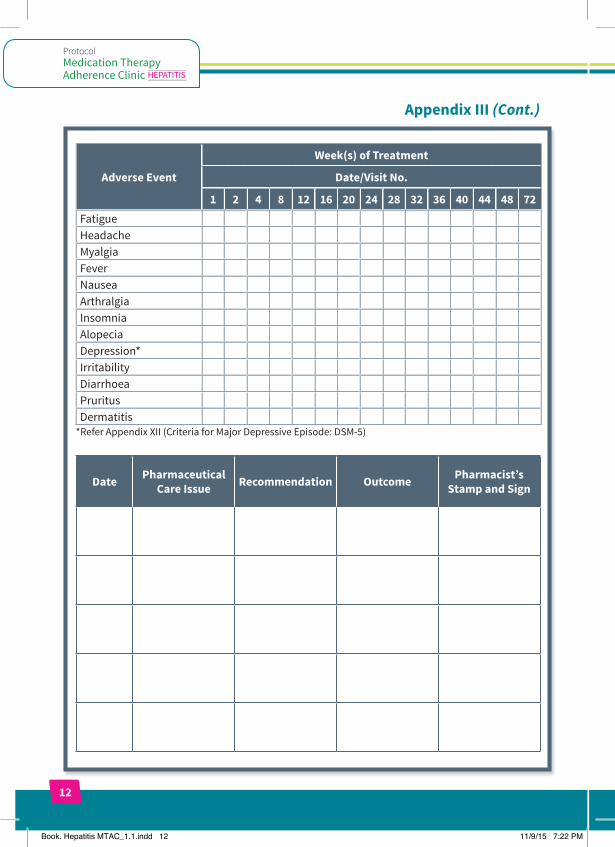
Appendix III (Cont.)
Adverse Event
Week(s) of Treatment
Date/Visit No.
1 2 4 8 12 16 20 24 28 32 36 40 44 48 72FatigueHeadacheMyalgiaFeverNauseaArthralgiaInsomniaAlopeciaDepression*IrritabilityDiarrhoeaPruritusDermatitis
*Refer Appendix XII (Criteria for Major Depressive Episode: DSM-5)
Date Pharmaceutical Care Issue Recommendation Outcome Pharmacist’s
Stamp and Sign
Book. Hepatitis MTAC_1.1.indd 12 11/9/15 7:22 PM
13
Appendix IVa
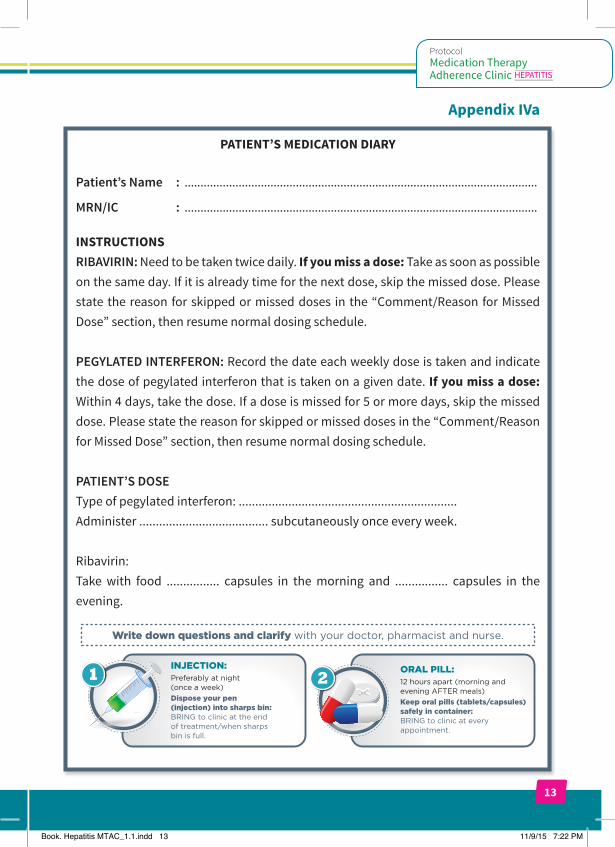
PATIENT’S MEDICATION DIARY
Patient’s Name : ...............................................................................................................
MRN/IC : ...............................................................................................................
INSTRUCTIONSRIBAVIRIN: Need to be taken twice daily. If you miss a dose: Take as soon as possible on the same day. If it is already time for the next dose, skip the missed dose. Please state the reason for skipped or missed doses in the “Comment/Reason for Missed Dose” section, then resume normal dosing schedule.
PEGYLATED INTERFERON: Record the date each weekly dose is taken and indicate the dose of pegylated interferon that is taken on a given date. If you miss a dose: Within 4 days, take the dose. If a dose is missed for 5 or more days, skip the missed dose. Please state the reason for skipped or missed doses in the “Comment/Reason for Missed Dose” section, then resume normal dosing schedule.
PATIENT’S DOSEType of pegylated interferon: ..................................................................Administer ....................................... subcutaneously once every week.
Ribavirin: Take with food ................ capsules in the morning and ................ capsules in the evening.
ORAL PILL:12 hours apart (morning andevening AFTER meals)Keep oral pills (tablets/capsules)safely in container:BRING to clinic at everyappointment.
2INJECTION:Preferably at night(once a week)Dispose your pen(injection) into sharps bin:BRING to clinic at the endof treatment/when sharpsbin is full.
1
Write down questions and clarify with your doctor, pharmacist and nurse.
Book. Hepatitis MTAC_1.1.indd 13 11/9/15 7:22 PM
14
Wee
k
Date
Body
Wei
ght
WBC Hb Pl
t
ANC
ALT
Peg I
FN D
ose
Inje
cted
(Y/N
)
Inje
ctio
n Si
te(L
/R)
Com
men
t /
Reas
on fo
r M
issed
Dos
e
123456789
1011121314151617181920212223242526272829303132
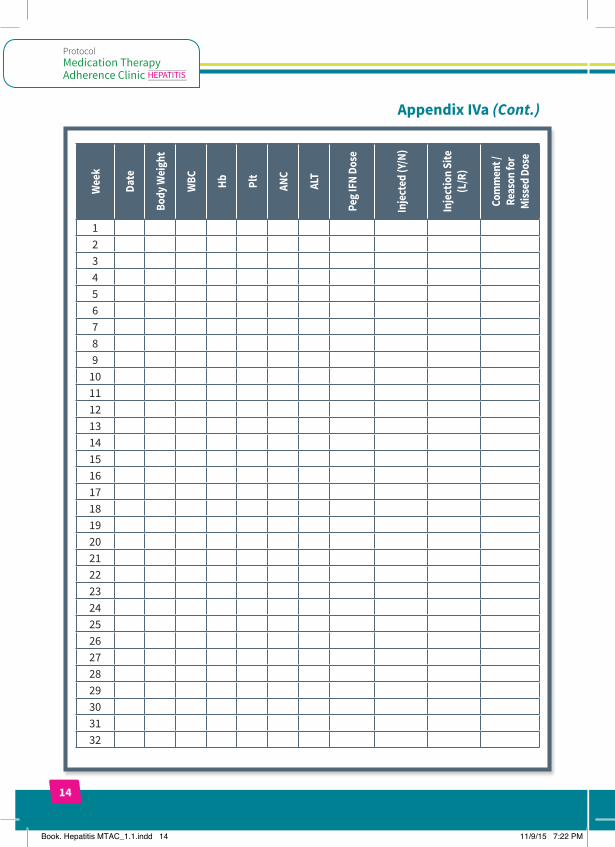
Appendix IVa (Cont.)
Book. Hepatitis MTAC_1.1.indd 14 11/9/15 7:22 PM
15
Wee
k
Date
Body
Wei
ght
WBC Hb Pl
t
ANC
ALT
Peg I
FN D
ose
Inje
cted
(Y/N
)
Inje
ctio
n Si
te(L
/R)
Com
men
t /
Reas
on fo
r M
issed
Dos
e
33343536373839404142434445464748
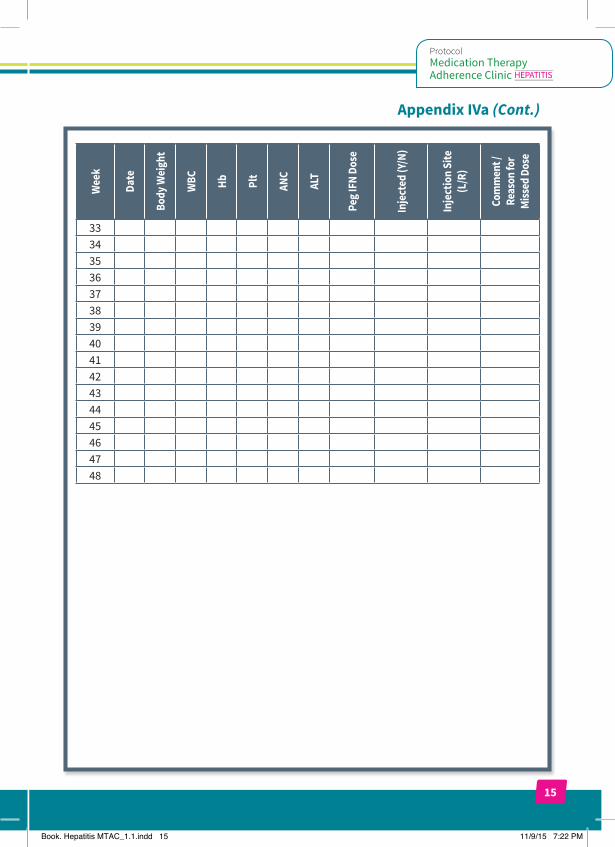
Appendix IVa (Cont.)
Book. Hepatitis MTAC_1.1.indd 15 11/9/15 7:22 PM

16
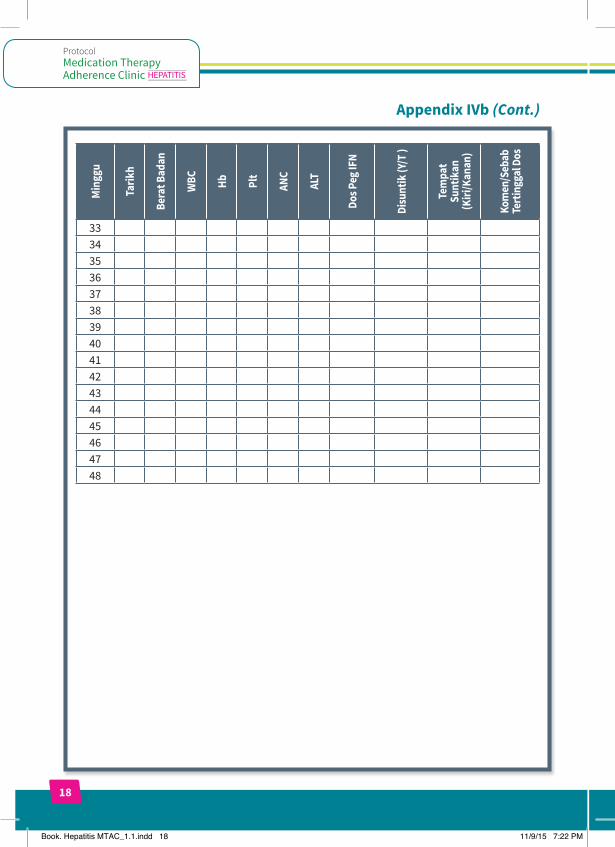
Appendix IVb
DIARI UBAT-UBATAN PESAKIT
Nama Pesakit : ...............................................................................................................
MRN/KP : ...............................................................................................................
ARAHANRIBAVIRIN: Perlu dimakan dua kali sehari. Jika anda tertinggal satu dos: Makan ubat secepat yang mungkin pada hari yang sama. Jika sudah tiba masa untuk dos yang seterusnya, lupakan dos yang tertinggal. Sila dokumenkan sebab dos ubat tidak diambil pada bahagian “Komen/Sebab Tertinggal Dos”, kemudian teruskan dengan jadual pengedosan yang biasa.
PEGYLATED INTERFERON: Rekodkan tarikh setiap dos mingguan disuntik. Nyatakan dos pegylated interferon yang disuntik bagi setiap tarikh. Jika anda tertinggal satu dos: Dalam masa 4 hari, suntik dos itu. Jika 5 hari atau lebih sudah berlalu, lupakan dos yang tertinggal. Sila dokumenkan sebab dos tersebut tidak disuntik pada bahagian “Komen/Sebab Tertinggal Dos”, kemudian teruskan dengan jadual pengedosan yang biasa.
DOS PESAKITJenis pegylated interferon: ..................................................................Suntik ....................................... secara subkutaneus seminggu sekali.
Ribavirin: Makan ................ kapsul pada waktu pagi dan ................ kapsul pada waktu malam bersama makanan.
2SUNTIKAN:Sebaik-baiknya pada waktumalam (seminggu sekali)Buangkan jarum suntikandalam bekas kalis tembus:BAWA ke klinik pada akhirrawatan/setelah bekas penuh diisi.
1
Catatkan jika ada sebarang persoalan dan dapatkan penerangandaripada Doktor, Pegawai Farmasi dan Jururawat.
PIL ORAL:Setiap 12 jam (pagi danpetang selepas makan)Simpan pil oral (tablet/kapsul)dalam bekas yang selamat:BAWA ke klinik setiap kalimenghadiri temujanji.
Book. Hepatitis MTAC_1.1.indd 16 11/9/15 7:22 PM
17
Min
ggu
Tarik
h
Bera
t Bad
an
WBC Hb Pl
t
ANC
ALT
Dos P
eg IF
N
Disu
ntik
(Y/T
)
Tem
pat
Sunt
ikan
(Kiri
/Kan
an)
Kom
en/S
ebab
Te
rting
gal D
os
123456789
1011121314151617181920212223242526272829303132
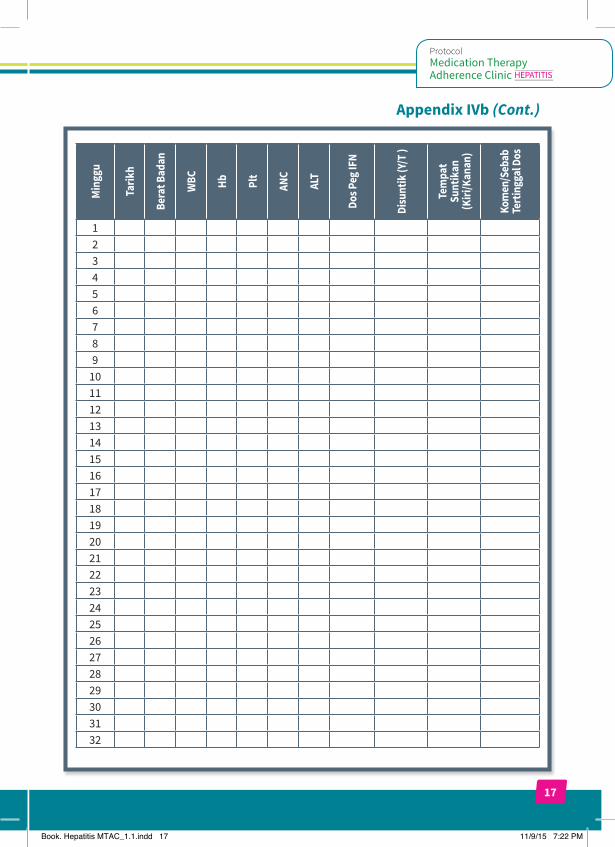
Appendix IVb (Cont.)
Book. Hepatitis MTAC_1.1.indd 17 11/9/15 7:22 PM
18
Appendix IVb (Cont.)M
ingg
u
Tarik
h
Bera
t Bad
an
WBC Hb Pl
t
ANC
ALT
Dos P
eg IF
N
Disu
ntik
(Y/T
)
Tem
pat
Sunt
ikan
(Kiri
/Kan
an)
Kom
en/S
ebab
Te
rting
gal D
os
33343536373839404142434445464748
Book. Hepatitis MTAC_1.1.indd 18 11/9/15 7:22 PM
19
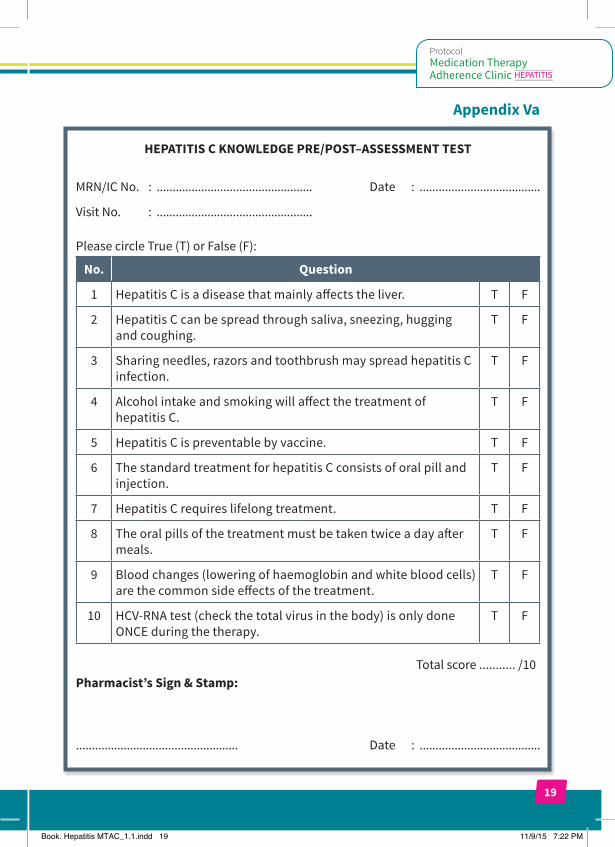
Appendix Va
HEPATITIS C KNOWLEDGE PRE/POST–ASSESSMENT TEST
MRN/IC No. : ................................................. Date : ......................................
Visit No. : .................................................
Please circle True (T) or False (F):
No. Question
1 Hepatitis C is a disease that mainly affects the liver. T F
2 Hepatitis C can be spread through saliva, sneezing, hugging and coughing.
T F
3 Sharing needles, razors and toothbrush may spread hepatitis C infection.
T F
4 Alcohol intake and smoking will affect the treatment of hepatitis C.
T F
5 Hepatitis C is preventable by vaccine. T F
6 The standard treatment for hepatitis C consists of oral pill and injection.
T F
7 Hepatitis C requires lifelong treatment. T F
8 The oral pills of the treatment must be taken twice a day after meals.
T F
9 Blood changes (lowering of haemoglobin and white blood cells) are the common side effects of the treatment.
T F
10 HCV-RNA test (check the total virus in the body) is only done ONCE during the therapy.
T F
Total score ........... /10Pharmacist’s Sign & Stamp:
................................................... Date : ......................................
Book. Hepatitis MTAC_1.1.indd 19 11/9/15 7:22 PM
20
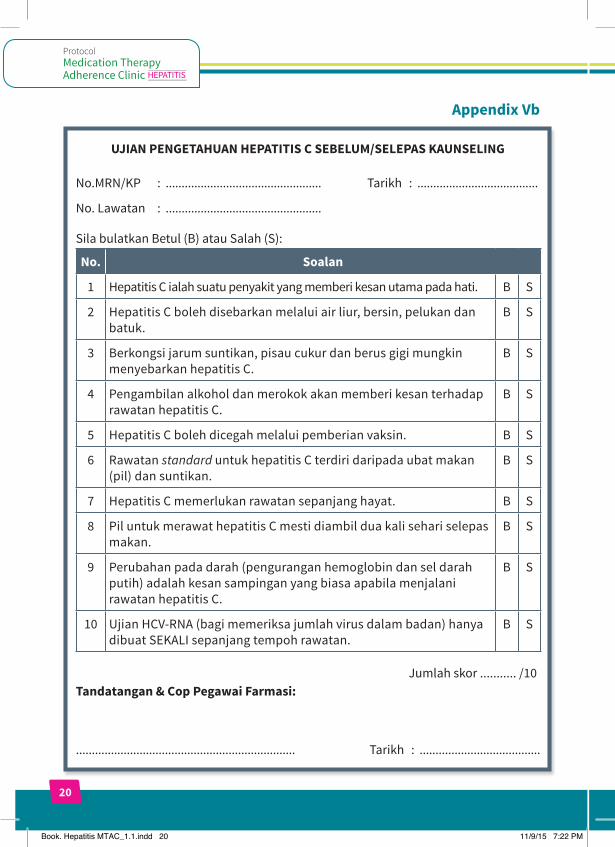
Appendix Vb
UJIAN PENGETAHUAN HEPATITIS C SEBELUM/SELEPAS KAUNSELING
No.MRN/KP : ................................................. Tarikh : ......................................
No. Lawatan : .................................................
Sila bulatkan Betul (B) atau Salah (S):
No. Soalan
1 Hepatitis C ialah suatu penyakit yang memberi kesan utama pada hati. B S
2 Hepatitis C boleh disebarkan melalui air liur, bersin, pelukan dan batuk.
B S
3 Berkongsi jarum suntikan, pisau cukur dan berus gigi mungkin menyebarkan hepatitis C.
B S
4 Pengambilan alkohol dan merokok akan memberi kesan terhadap rawatan hepatitis C.
B S
5 Hepatitis C boleh dicegah melalui pemberian vaksin. B S
6 Rawatan standard untuk hepatitis C terdiri daripada ubat makan (pil) dan suntikan.
B S
7 Hepatitis C memerlukan rawatan sepanjang hayat. B S
8 Pil untuk merawat hepatitis C mesti diambil dua kali sehari selepas makan.
B S
9 Perubahan pada darah (pengurangan hemoglobin dan sel darah putih) adalah kesan sampingan yang biasa apabila menjalani rawatan hepatitis C.
B S
10 Ujian HCV-RNA (bagi memeriksa jumlah virus dalam badan) hanya dibuat SEKALI sepanjang tempoh rawatan.
B S
Jumlah skor ........... /10Tandatangan & Cop Pegawai Farmasi:
..................................................................... Tarikh : ......................................
Book. Hepatitis MTAC_1.1.indd 20 11/9/15 7:22 PM
21
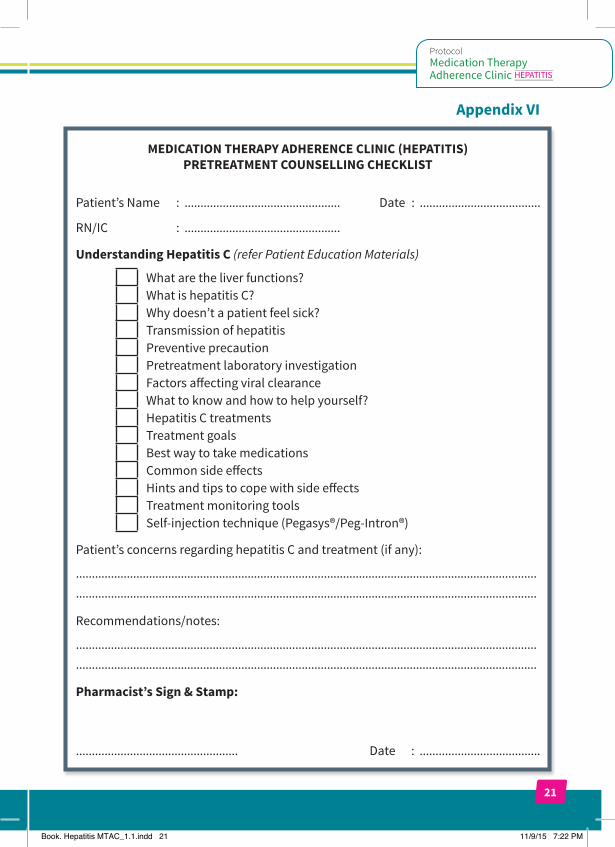
Appendix VI
MEDICATION THERAPY ADHERENCE CLINIC (HEPATITIS) PRETREATMENT COUNSELLING CHECKLIST
Patient’s Name : ................................................. Date : ......................................
RN/IC : .................................................
Understanding Hepatitis C (refer Patient Education Materials)
What are the liver functions? What is hepatitis C? Why doesn’t a patient feel sick? Transmission of hepatitis Preventive precaution Pretreatment laboratory investigation Factors affecting viral clearance What to know and how to help yourself? Hepatitis C treatments Treatment goals Best way to take medications Common side effects Hints and tips to cope with side effects Treatment monitoring tools Self-injection technique (Pegasys®/Peg-Intron®)
Patient’s concerns regarding hepatitis C and treatment (if any):
.................................................................................................................................................
.................................................................................................................................................
Recommendations/notes:
.................................................................................................................................................
.................................................................................................................................................
Pharmacist’s Sign & Stamp:
................................................... Date : ......................................
Book. Hepatitis MTAC_1.1.indd 21 11/9/15 7:22 PM
22
Appendix VII
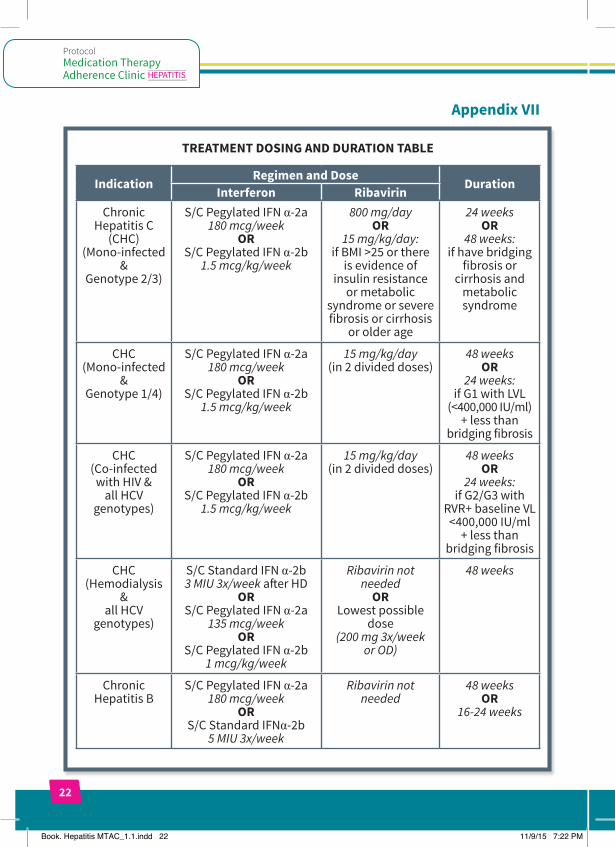
TREATMENT DOSING AND DURATION TABLE
IndicationRegimen and Dose
DurationInterferon Ribavirin
Chronic Hepatitis C
(CHC) (Mono-infected
& Genotype 2/3)
S/C Pegylated IFN α-2a 180 mcg/week
OR S/C Pegylated IFN α-2b
1.5 mcg/kg/week
800 mg/day OR
15 mg/kg/day: if BMI >25 or there
is evidence of insulin resistance
or metabolic syndrome or severe fibrosis or cirrhosis
or older age
24 weeks OR
48 weeks: if have bridging
fibrosis or cirrhosis and
metabolic syndrome
CHC (Mono-infected
& Genotype 1/4)
S/C Pegylated IFN α-2a 180 mcg/week
OR S/C Pegylated IFN α-2b
1.5 mcg/kg/week
15 mg/kg/day (in 2 divided doses)
48 weeks OR
24 weeks: if G1 with LVL
(<400,000 IU/ml) + less than
bridging fibrosis
CHC (Co-infected
with HIV & all HCV
genotypes)
S/C Pegylated IFN α-2a 180 mcg/week
OR S/C Pegylated IFN α-2b
1.5 mcg/kg/week
15 mg/kg/day (in 2 divided doses)
48 weeks OR
24 weeks: if G2/G3 with
RVR+ baseline VL <400,000 IU/ml
+ less than bridging fibrosis
CHC (Hemodialysis
& all HCV
genotypes)
S/C Standard IFN α-2b 3 MIU 3x/week after HD
OR S/C Pegylated IFN α-2a
135 mcg/week OR
S/C Pegylated IFN α-2b 1 mcg/kg/week
Ribavirin not needed
OR Lowest possible
dose (200 mg 3x/week
or OD)
48 weeks
Chronic Hepatitis B
S/C Pegylated IFN α-2a 180 mcg/week
OR S/C Standard IFNα-2b
5 MIU 3x/week
Ribavirin not needed
48 weeks OR
16-24 weeks
Book. Hepatitis MTAC_1.1.indd 22 11/9/15 7:22 PM
23
Appendix VII (Cont.)
Notes:1. The recommended dose of ribavirin is 800 to 1,400mg per day orally based on
patient’s body weight. Ribavirin should be taken with food. Ribavirin should not be used in patients with creatinine clearance less than 50 ml/min.
2. Ribavirin may cause birth defects and death of the unborn child. Extreme care must be taken to avoid pregnancy in female patients and in female partners of male patients. Ribavirin causes haemolytic anaemia. The anaemia associated with ribavirin therapy may result in a worsening of cardiac disease.
3. The Peg-Intron® dose of 1.5 mcg/kg/week should be calculated based on the individual’s weight. Use standard rounding procedures: for 0.1 to 0.4 kg, round down and for 0.5 to 0.9 kg, round up. The volume of Peg-Intron® to be injected depends on the strength of Peg-Intron® and patient’s body weight.
Book. Hepatitis MTAC_1.1.indd 23 11/9/15 7:22 PM
24
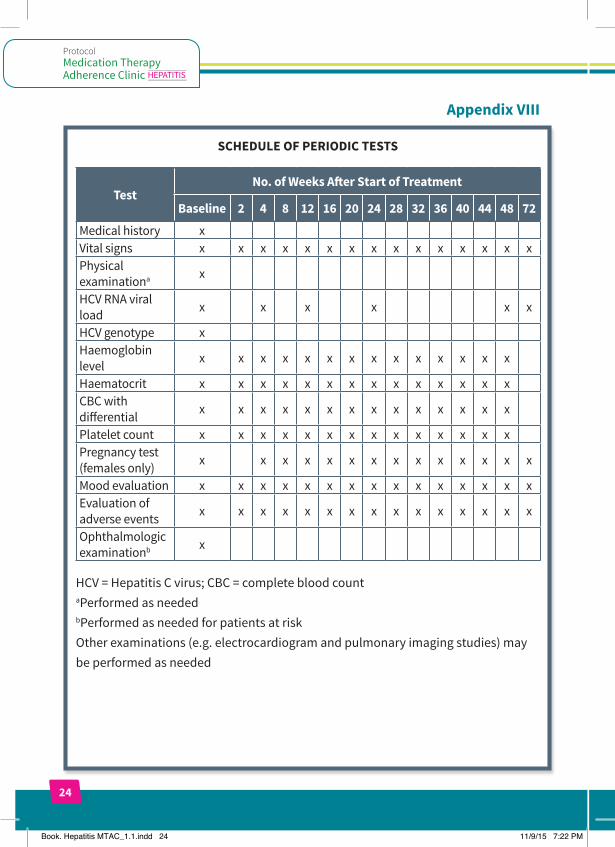
Appendix VIII
SCHEDULE OF PERIODIC TESTS
TestNo. of Weeks After Start of Treatment
Baseline 2 4 8 12 16 20 24 28 32 36 40 44 48 72
Medical history xVital signs x x x x x x x x x x x x x x xPhysical examinationa x
HCV RNA viral load x x x x x x
HCV genotype xHaemoglobin level x x x x x x x x x x x x x x
Haematocrit x x x x x x x x x x x x x xCBC with differential x x x x x x x x x x x x x x
Platelet count x x x x x x x x x x x x x xPregnancy test (females only) x x x x x x x x x x x x x x
Mood evaluation x x x x x x x x x x x x x x xEvaluation of adverse events x x x x x x x x x x x x x x x
Ophthalmologic examinationb x
HCV = Hepatitis C virus; CBC = complete blood count aPerformed as needed bPerformed as needed for patients at risk Other examinations (e.g. electrocardiogram and pulmonary imaging studies) may be performed as needed
Book. Hepatitis MTAC_1.1.indd 24 11/9/15 7:22 PM
25
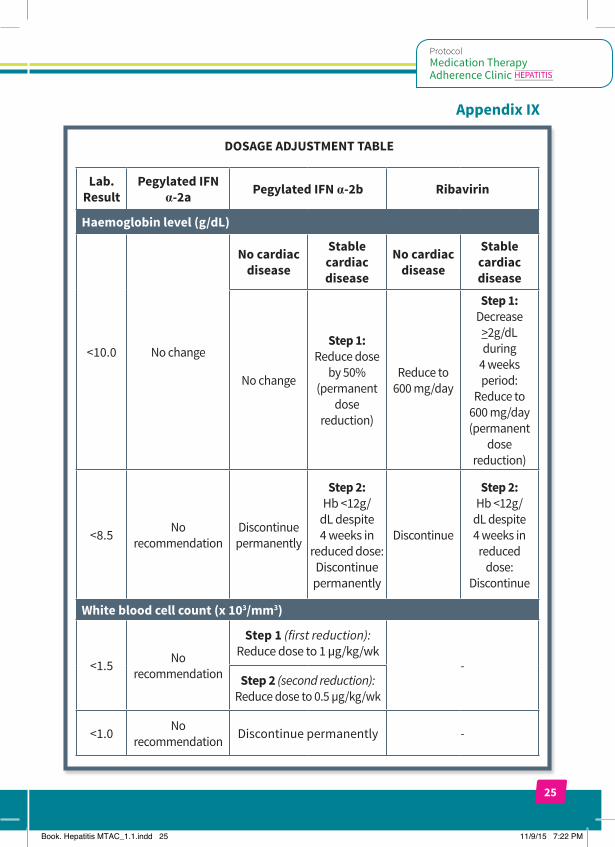
Appendix IX
DOSAGE ADJUSTMENT TABLE
Lab. Result
Pegylated IFN α-2a Pegylated IFN α-2b Ribavirin
Haemoglobin level (g/dL)
<10.0 No change
No cardiac disease
Stable cardiac disease
No cardiac disease
Stable cardiac disease
No change
Step 1: Reduce dose
by 50%(permanent
dose reduction)
Reduce to 600 mg/day
Step 1: Decrease
>2g/dL during
4 weeks period:
Reduce to 600 mg/day (permanent
dose reduction)
<8.5 No recommendation
Discontinue permanently
Step 2:Hb <12g/
dL despite 4 weeks in
reduced dose: Discontinue
permanently
Discontinue
Step 2:Hb <12g/
dL despite 4 weeks in
reduced dose:
Discontinue
White blood cell count (x 103/mm3)
<1.5 No recommendation
Step 1 (first reduction): Reduce dose to 1 µg/kg/wk
-Step 2 (second reduction):
Reduce dose to 0.5 µg/kg/wk
<1.0 No recommendation Discontinue permanently -
Book. Hepatitis MTAC_1.1.indd 25 11/9/15 7:22 PM
26
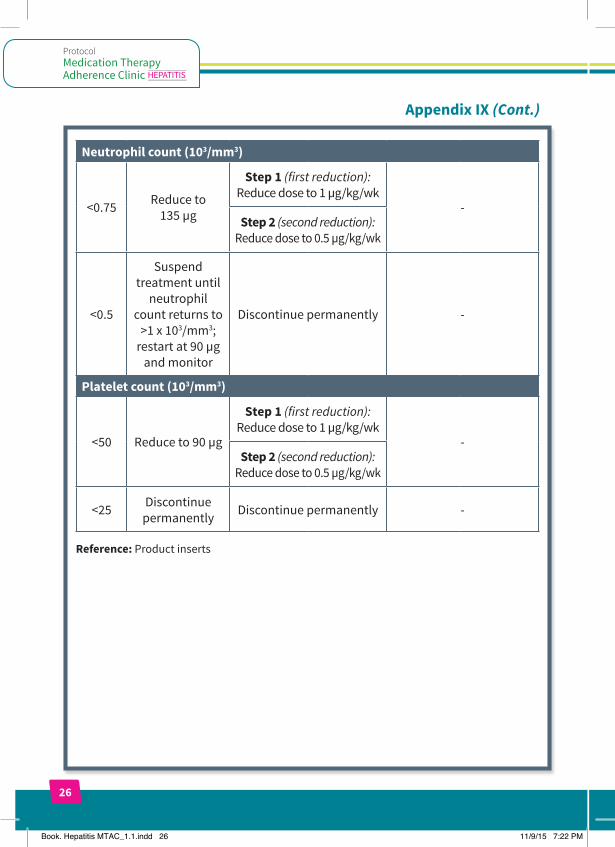
Appendix IX (Cont.)
Neutrophil count (103/mm3)
<0.75 Reduce to 135 µg
Step 1 (first reduction): Reduce dose to 1 µg/kg/wk
-Step 2 (second reduction):
Reduce dose to 0.5 µg/kg/wk
<0.5
Suspend treatment until
neutrophil count returns to
>1 x 103/mm3; restart at 90 µg
and monitor
Discontinue permanently -
Platelet count (103/mm3)
<50 Reduce to 90 µg
Step 1 (first reduction): Reduce dose to 1 µg/kg/wk
-Step 2 (second reduction):
Reduce dose to 0.5 µg/kg/wk
<25 Discontinue permanently Discontinue permanently -
Reference: Product inserts
Book. Hepatitis MTAC_1.1.indd 26 11/9/15 7:22 PM
27
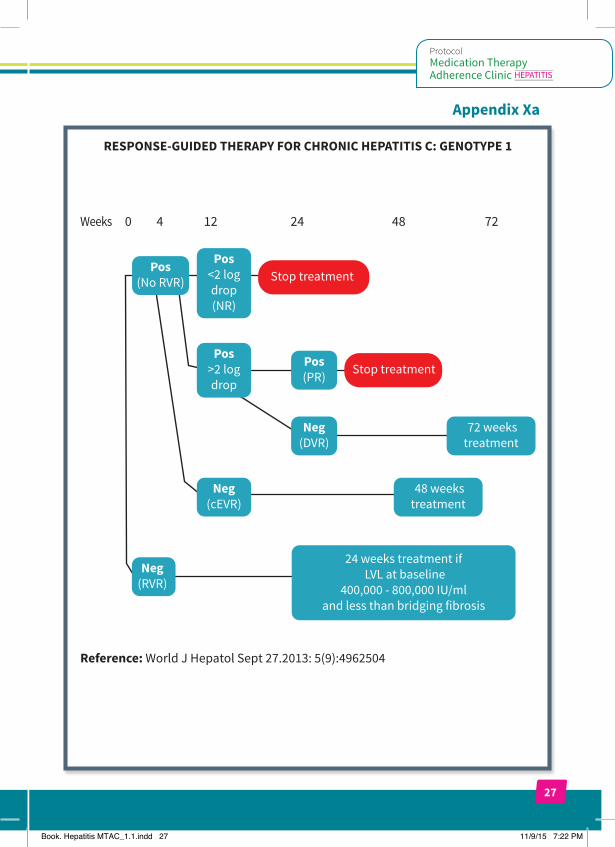
Appendix Xa
RESPONSE-GUIDED THERAPY FOR CHRONIC HEPATITIS C: GENOTYPE 1
Reference: World J Hepatol Sept 27.2013: 5(9):4962504
Weeks 0 4 12 24 48 72
Neg(RVR)
24 weeks treatment if LVL at baseline
400,000 - 800,000 IU/ml and less than bridging fibrosis
Neg(cEVR)
Pos>2 log drop
Pos (No RVR)
Pos <2 log drop(NR)
Pos (PR)
Neg(DVR)
72 weekstreatment
48 weekstreatment
Stop treatment
Stop treatment
Book. Hepatitis MTAC_1.1.indd 27 11/9/15 7:22 PM
28
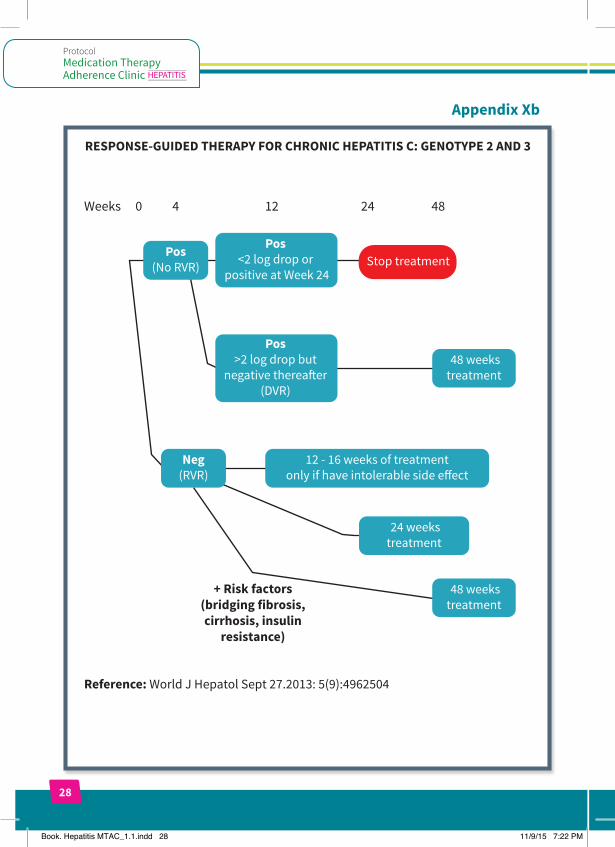
Appendix Xb
RESPONSE-GUIDED THERAPY FOR CHRONIC HEPATITIS C: GENOTYPE 2 AND 3
Reference: World J Hepatol Sept 27.2013: 5(9):4962504
+ Risk factors(bridging fibrosis,cirrhosis, insulin
resistance)
Weeks 0 4 12 24 48
Neg(RVR)
12 - 16 weeks of treatmentonly if have intolerable side e�ect
Pos (No RVR)
Pos <2 log drop or
positive at Week 24
Pos >2 log drop but
negative therea�er(DVR)
Stop treatment
48 weekstreatment
24 weekstreatment
48 weekstreatment
Book. Hepatitis MTAC_1.1.indd 28 11/9/15 7:22 PM
29
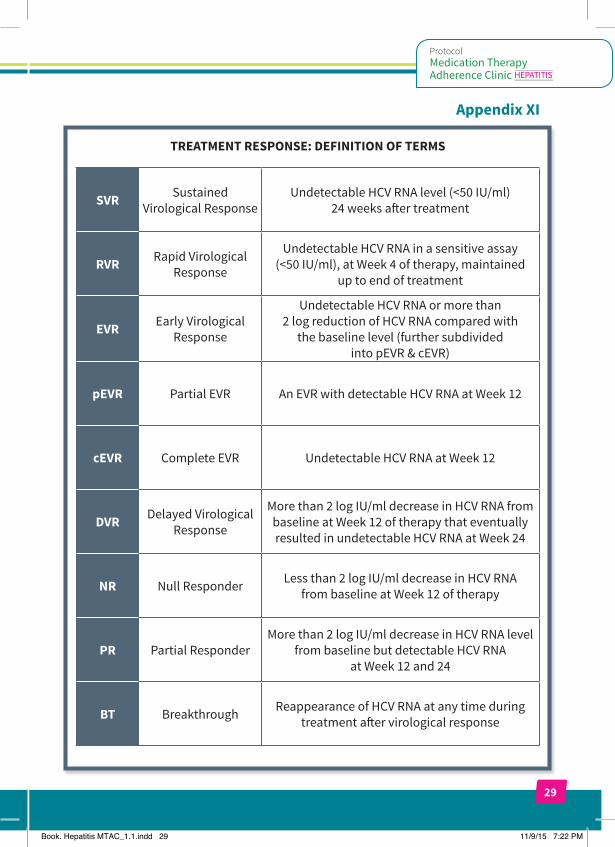
Appendix XI
TREATMENT RESPONSE: DEFINITION OF TERMS
SVR Sustained Virological Response
Undetectable HCV RNA level (<50 IU/ml) 24 weeks after treatment
RVR Rapid Virological Response
Undetectable HCV RNA in a sensitive assay (<50 IU/ml), at Week 4 of therapy, maintained
up to end of treatment
EVR Early Virological Response
Undetectable HCV RNA or more than 2 log reduction of HCV RNA compared with
the baseline level (further subdivided into pEVR & cEVR)
pEVR Partial EVR An EVR with detectable HCV RNA at Week 12
cEVR Complete EVR Undetectable HCV RNA at Week 12
DVR Delayed Virological Response
More than 2 log IU/ml decrease in HCV RNA from baseline at Week 12 of therapy that eventually resulted in undetectable HCV RNA at Week 24
NR Null Responder Less than 2 log IU/ml decrease in HCV RNA from baseline at Week 12 of therapy
PR Partial ResponderMore than 2 log IU/ml decrease in HCV RNA level
from baseline but detectable HCV RNA at Week 12 and 24
BT Breakthrough Reappearance of HCV RNA at any time during treatment after virological response
Book. Hepatitis MTAC_1.1.indd 29 11/9/15 7:22 PM
30
Appendix XII
CRITERIA FOR MAJOR DEPRESSIVE EPISODE: DSM-5
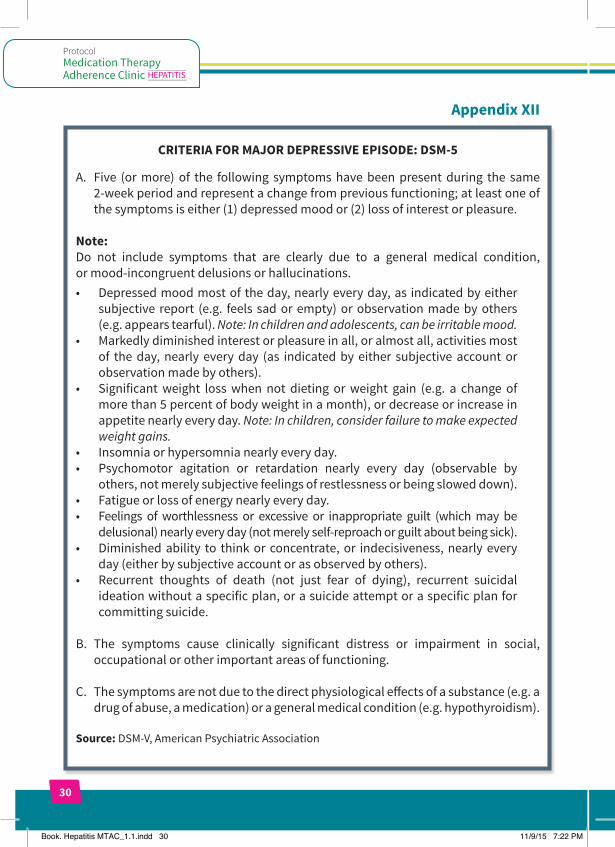
A. Five (or more) of the following symptoms have been present during the same 2-week period and represent a change from previous functioning; at least one of the symptoms is either (1) depressed mood or (2) loss of interest or pleasure.
Note:Do not include symptoms that are clearly due to a general medical condition, or mood-incongruent delusions or hallucinations.• Depressedmoodmostof theday,nearlyeveryday,as indicatedbyeither
subjective report (e.g. feels sad or empty) or observation made by others (e.g. appears tearful). Note: In children and adolescents, can be irritable mood.
• Markedlydiminishedinterestorpleasureinall,oralmostall,activitiesmostof the day, nearly every day (as indicated by either subjective account or observation made by others).
• Significantweight losswhen not dieting orweight gain (e.g. a change ofmore than 5 percent of body weight in a month), or decrease or increase in appetite nearly every day. Note: In children, consider failure to make expected weight gains.
• Insomniaorhypersomnianearlyeveryday.• Psychomotor agitation or retardation nearly every day (observable by
others, not merely subjective feelings of restlessness or being slowed down).• Fatigueorlossofenergynearlyeveryday.• Feelings of worthlessness or excessive or inappropriate guilt (whichmay be
delusional) nearly every day (not merely self-reproach or guilt about being sick).• Diminishedability to thinkor concentrate,or indecisiveness,nearlyevery
day (either by subjective account or as observed by others).• Recurrent thoughts of death (not just fear of dying), recurrent suicidal
ideation without a specific plan, or a suicide attempt or a specific plan for committing suicide.
B. The symptoms cause clinically significant distress or impairment in social, occupational or other important areas of functioning.
C. The symptoms are not due to the direct physiological effects of a substance (e.g. a drug of abuse, a medication) or a general medical condition (e.g. hypothyroidism).
Source: DSM-V, American Psychiatric Association
Book. Hepatitis MTAC_1.1.indd 30 11/9/15 7:22 PM
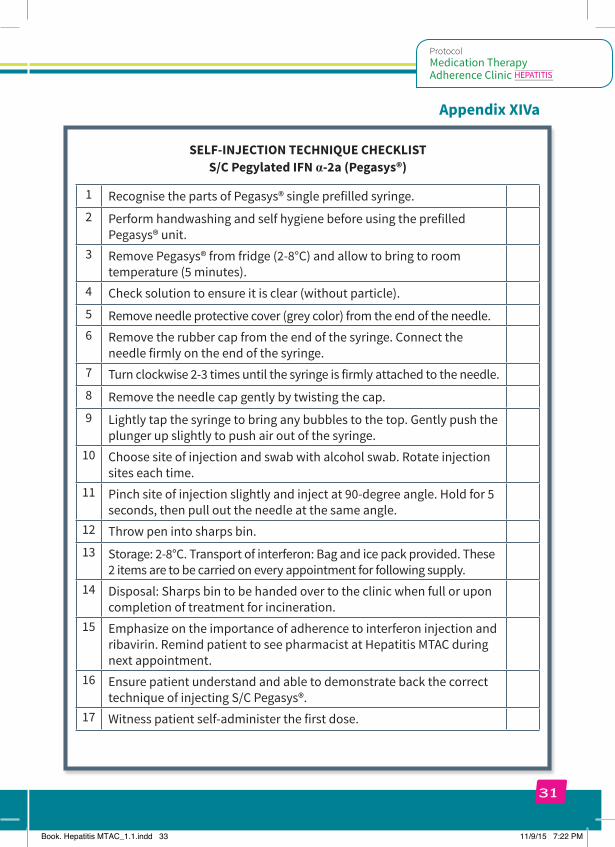
Appendix XIVa
SELF-INJECTION TECHNIQUE CHECKLIST S/C Pegylated IFN α-2a (Pegasys®)
1 Recognise the parts of Pegasys® single prefilled syringe.2 Perform handwashing and self hygiene before using the prefilled
Pegasys® unit.3 Remove Pegasys® from fridge (2-8°C) and allow to bring to room
temperature (5 minutes).4 Check solution to ensure it is clear (without particle). 5 Remove needle protective cover (grey color) from the end of the needle.6 Remove the rubber cap from the end of the syringe. Connect the
needle firmly on the end of the syringe. 7 Turn clockwise 2-3 times until the syringe is firmly attached to the needle.8 Remove the needle cap gently by twisting the cap.9 Lightly tap the syringe to bring any bubbles to the top. Gently push the
plunger up slightly to push air out of the syringe.10 Choose site of injection and swab with alcohol swab. Rotate injection
sites each time.11 Pinch site of injection slightly and inject at 90-degree angle. Hold for 5
seconds, then pull out the needle at the same angle.12 Throw pen into sharps bin.13 Storage: 2-8°C. Transport of interferon: Bag and ice pack provided. These
2 items are to be carried on every appointment for following supply.14 Disposal: Sharps bin to be handed over to the clinic when full or upon
completion of treatment for incineration.15 Emphasize on the importance of adherence to interferon injection and
ribavirin. Remind patient to see pharmacist at Hepatitis MTAC during next appointment.
16 Ensure patient understand and able to demonstrate back the correct technique of injecting S/C Pegasys®.
17 Witness patient self-administer the first dose.
Book. Hepatitis MTAC_1.1.indd 33 11/9/15 7:22 PM
31
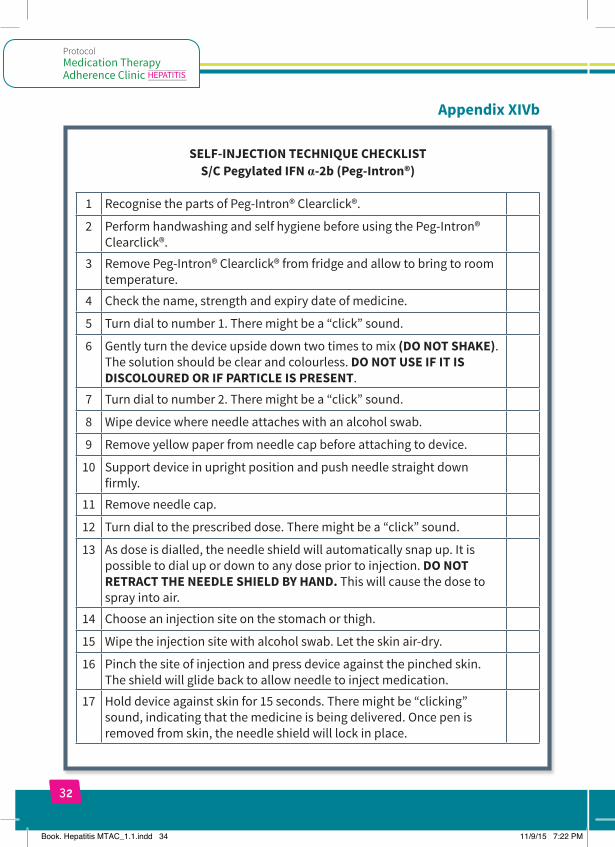
Appendix XIVb
SELF-INJECTION TECHNIQUE CHECKLIST S/C Pegylated IFN α-2b (Peg-Intron®)
1 Recognise the parts of Peg-Intron® Clearclick®.
2 Perform handwashing and self hygiene before using the Peg-Intron® Clearclick®.
3 Remove Peg-Intron® Clearclick® from fridge and allow to bring to room temperature.
4 Check the name, strength and expiry date of medicine.
5 Turn dial to number 1. There might be a “click” sound.
6 Gently turn the device upside down two times to mix (DO NOT SHAKE). The solution should be clear and colourless. DO NOT USE IF IT IS DISCOLOURED OR IF PARTICLE IS PRESENT.
7 Turn dial to number 2. There might be a “click” sound.
8 Wipe device where needle attaches with an alcohol swab.
9 Remove yellow paper from needle cap before attaching to device.
10 Support device in upright position and push needle straight down firmly.
11 Remove needle cap.
12 Turn dial to the prescribed dose. There might be a “click” sound.
13 As dose is dialled, the needle shield will automatically snap up. It is possible to dial up or down to any dose prior to injection. DO NOT RETRACT THE NEEDLE SHIELD BY HAND. This will cause the dose to spray into air.
14 Choose an injection site on the stomach or thigh.
15 Wipe the injection site with alcohol swab. Let the skin air-dry.
16 Pinch the site of injection and press device against the pinched skin. The shield will glide back to allow needle to inject medication.
17 Hold device against skin for 15 seconds. There might be “clicking” sound, indicating that the medicine is being delivered. Once pen is removed from skin, the needle shield will lock in place.
Book. Hepatitis MTAC_1.1.indd 34 11/9/15 7:22 PM
32
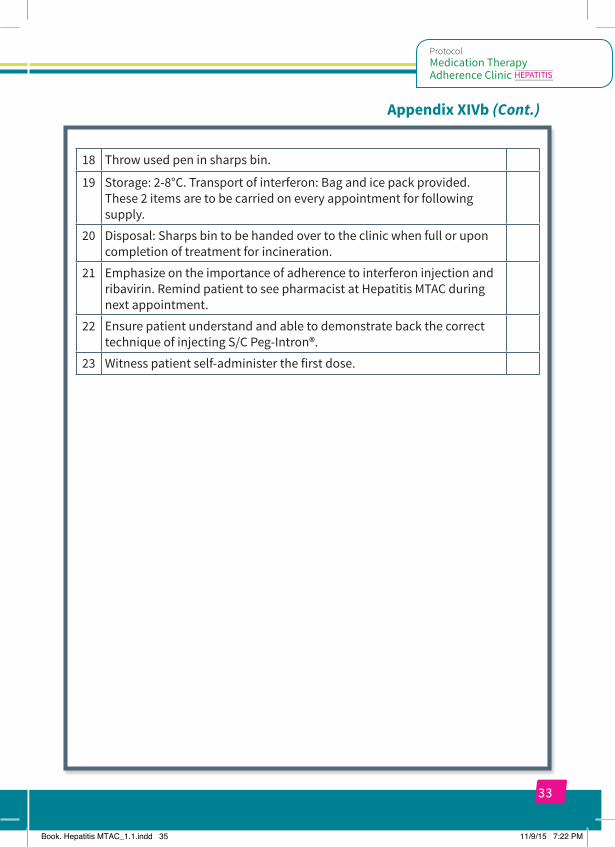
Appendix XIVb (Cont.)
18 Throw used pen in sharps bin.
19 Storage: 2-8°C. Transport of interferon: Bag and ice pack provided. These 2 items are to be carried on every appointment for following supply.
20 Disposal: Sharps bin to be handed over to the clinic when full or upon completion of treatment for incineration.
21 Emphasize on the importance of adherence to interferon injection and ribavirin. Remind patient to see pharmacist at Hepatitis MTAC during next appointment.
22 Ensure patient understand and able to demonstrate back the correct technique of injecting S/C Peg-Intron®.
23 Witness patient self-administer the first dose.
Book. Hepatitis MTAC_1.1.indd 35 11/9/15 7:22 PM
33
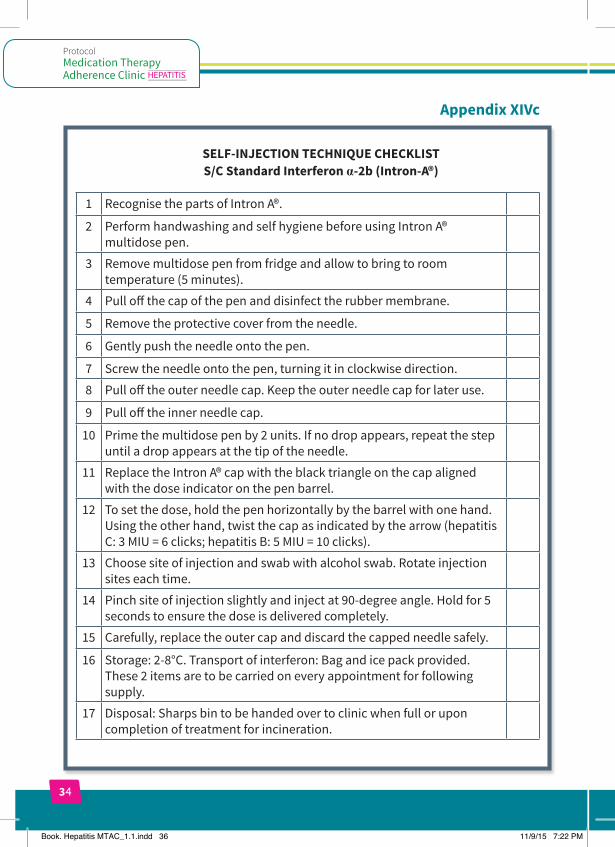
Appendix XIVc
SELF-INJECTION TECHNIQUE CHECKLIST S/C Standard Interferon α-2b (Intron-A®)
1 Recognise the parts of Intron A®.
2 Perform handwashing and self hygiene before using Intron A® multidose pen.
3 Remove multidose pen from fridge and allow to bring to room temperature (5 minutes).
4 Pull off the cap of the pen and disinfect the rubber membrane.
5 Remove the protective cover from the needle.
6 Gently push the needle onto the pen.
7 Screw the needle onto the pen, turning it in clockwise direction.
8 Pull off the outer needle cap. Keep the outer needle cap for later use.
9 Pull off the inner needle cap.
10 Prime the multidose pen by 2 units. If no drop appears, repeat the step until a drop appears at the tip of the needle.
11 Replace the Intron A® cap with the black triangle on the cap aligned with the dose indicator on the pen barrel.
12 To set the dose, hold the pen horizontally by the barrel with one hand. Using the other hand, twist the cap as indicated by the arrow (hepatitis C: 3 MIU = 6 clicks; hepatitis B: 5 MIU = 10 clicks).
13 Choose site of injection and swab with alcohol swab. Rotate injection sites each time.
14 Pinch site of injection slightly and inject at 90-degree angle. Hold for 5 seconds to ensure the dose is delivered completely.
15 Carefully, replace the outer cap and discard the capped needle safely.
16 Storage: 2-8°C. Transport of interferon: Bag and ice pack provided. These 2 items are to be carried on every appointment for following supply.
17 Disposal: Sharps bin to be handed over to clinic when full or upon completion of treatment for incineration.
Book. Hepatitis MTAC_1.1.indd 36 11/9/15 7:22 PM
34
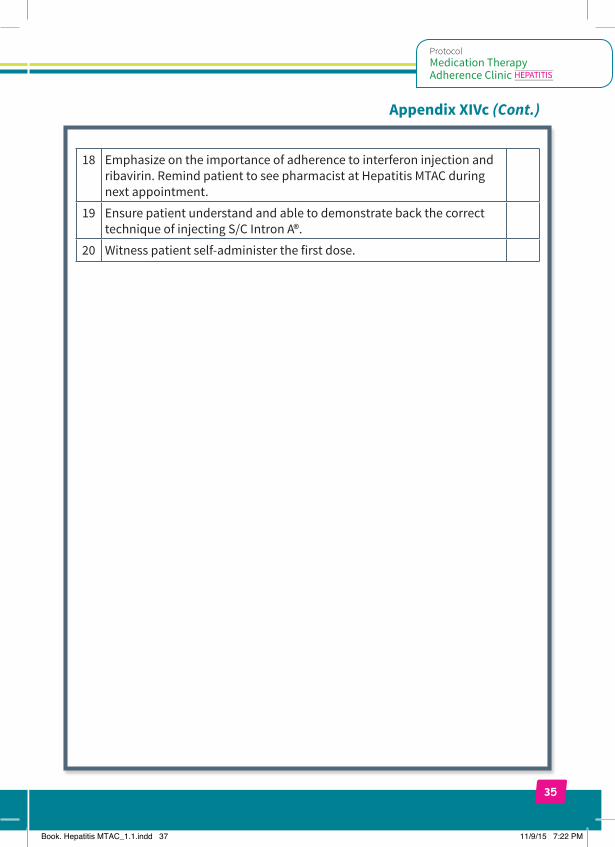
Appendix XIVc (Cont.)
18 Emphasize on the importance of adherence to interferon injection and ribavirin. Remind patient to see pharmacist at Hepatitis MTAC during next appointment.
19 Ensure patient understand and able to demonstrate back the correct technique of injecting S/C Intron A®.
20 Witness patient self-administer the first dose.
Book. Hepatitis MTAC_1.1.indd 37 11/9/15 7:22 PM
35

Book. Hepatitis MTAC_1.1.indd 38 11/9/15 7:22 PM





























