Embed Size (px)
Citation preview

CLINICAL REPORT
aFaculty, DepbFaculty, DepcPrivate pracdProfessor aneAssistant PrfProfessor an
THE JOURNA
Prosthodontic rehabilitation with monolithic, multichromaticCAD-CAM complete overdentures in an adolescent patient with
ectodermal dysplasia: A clinical report
Hussain D. Alsayed, BDS, MSD,a Nasser M. Alqahtani, BDS, MSD,b Yasmin M. Alzayer, BDS, MSD,cDean Morton, BDS, MS,d John A. Levon, DDS, MS,e and Nadim Z. Baba, DMD, MSDf
ABSTRACTEctodermal dysplasia is a rare, hereditary, congenital disease that affects the normal developmentof certain tissues and structures of ectodermal origin. The disease is manifested to different degreesof severity and may involve the nose, eyes, hair, nails, sweat glands, and enamel. This report de-scribes a 14-year-old boy with ectodermal dysplasia, rehabilitated with monolithic, multichromaticmaxillary and mandibular computer-aided design and computer-aided manufacturing (CAD-CAM)acrylic resin complete overdentures. (J Prosthet Dent 2017;-:---)
Ectodermal dysplasia (ED) is arare, hereditary, congenital dis-ease characterized by abnormaldevelopment of certain tissuesand structures of ectodermalorigin. Disturbances in tissuesderived from other embryologiclayers are not uncommon. The
ectodermal germ layer gives rise to different organs andstructures, including the nose, eyes, hair, nails, sweatglands, and enamel.1 The prevalence of hypohidrotic ED inthe general population has been estimated between1:10 000 and 1:100 000 male live births.2,3 Individuals withthis disease generally exhibit a triad of symptoms: hypo-dontia, hypotrichosis, and hypohidrosis.4Dental abnormalities can range from anodontia tohypodontia, which is the more common form.5 Bothdeciduous and permanent dentitions seem to be affected,and conical or peg-shaped teeth predominate.5 In theabsence of teeth, the alveolar process is poorly devel-oped, decreasing the occlusal vertical dimension (OVD)and giving the child’s face an aged appearance, similar tothat of a patient with edentulism. The growth anddevelopment of the child, however, is normal.6,7
Dental treatment should start early in the life of thepatient. Function, psychology, and esthetics are primaryreasons behind such an early approach.8,9 Facial
artment of Prosthetic Dental Sciences, King Saud University College of Deartment of Prosthetic Dental Sciences, King Khalid University College of Dtice, Dammam, Saudi Arabia.d Chair, Department of Prosthodontics, Indiana University School of Dentofessor and Director, Department of Prosthodontics, Indiana University Schd Director, Hugh Love Center for Research and Education in Technology,
L OF PROSTHETIC DENTISTRY
Downloaded for Anonymous User (n/a) at Indiana University - Ruth Lilly MeFor personal use only. No other uses without permission.
appearance can create an inadequate self-image, leadingto social withdrawal and difficulty integrating into soci-ety9,10; the dental appearance of these young patients,therefore, is of the utmost importance. Treatment timingand sequence should be determined in conjunction withthe patient’s parents and may include fixed, removable,or implant-supported fixed partial dentures.9-12
Removable prosthodontics is the most frequentlyused treatment for ED.13 When teeth are present forsupport, overdentures have been successful.14 In additionto being straightforward and inexpensive, removableprosthodontics are a reversible and conservative treat-ment that will leave the teeth of the young patient intactand preserve the alveolar bone.13-15 Mini-implants canbe considered as a viable reversible treatment option for agrowing child with ED.3 Subsequently, the adult patientcan be provided with more definitive treatment,including implant-supported prostheses, withoutdamaging their few remaining teeth. Overdentures help
ntistry, Riyadh, Saudi Arabia.entistry, Abha, Saudi Arabia.
istry, Indianapolis, Ind.ool of Dentistry, Indianapolis, Ind.Loma Linda University School of Dentistry, Loma Linda, Calif.
1
dical Library from ClinicalKey.com by Elsevier on November 16, 2017. Copyright ©2017. Elsevier Inc. All rights reserved.

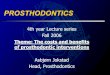
Figure 1. Pretreatment intraoral views. A, Right view. B. Frontal view.C, Left view.
2 Volume - Issue -
to achieve better function, esthetics, and phonetics, alongwith improved self-image.13 Limitations of this optionwith very young patients include the patient’s failure tocomply with oral hygiene, which requires several recallvisits (3 to 4 months), daily application of stannousfluoride to minimize dental caries, and periodic replace-ment of the overdenture because of the child’s normalgrowth.16
Removable complete overdenture prostheses(RCOPs) have been used successfully for patients withED who present with hypodontia, especially young pa-tients who have not yet stopped growing.17 Monolithic,multichromatic computer-aided design and computer-aided manufacturing (CAD-CAM) has been developedto fabricate removal complete dental prostheses(RCDPs).18 Compared with conventionally processeddentures, CAD-CAM RCDPs show several advantages,including a reduction of residual monomer, improvedphysical properties of the acrylic resin base, reduction inpolymerization shrinkage, and reduced adhesion ofCandida albicans organisms to the denture base.19 Inaddition, CAD-CAM RCDPs can be provided over fewerpatient visits, the digital files permit easier remakes, anddenture base adaptation and retention are improved.20,21
This clinical report describes the treatment of anadolescent patient with ectodermal dysplasia, usingmonolithic, multichromatic CAD-CAM RCOPs.
CLINICAL REPORT
A 14-year-old white boy presented with his parents tothe graduate prosthodontic clinic at Indiana UniversitySchool of Dentistry complaining of an unpleasant smileand the inability to masticate properly. His parents statedthat he is socially shy and aware of his condition, espe-cially when his classmates are around him. Their wishwas to replace the missing teeth to improve their son’sesthetics and mastication. His medical history included adiagnosis of ED; and he had no history of allergic re-actions to medications, local anesthetics, or food. Hisdental history disclosed that he visited his dentist regu-larly and had not exfoliated his primary teeth.
He exhibited a reduced lower face height and saddlenose. He presented with a dolichofacial face type and aconcave lateral profile. In addition, he had a low smileline, with less than 75% of the maxillary central incisorshowing at maximum smile. Intraoral screening wasnegative for cancer, generalized microdontia, hypo-dontia, and diastemas. The patient presented with mixeddentition with primary teeth (maxillary right secondmolar, maxillary first molars, maxillary canines, maxillarylateral and central incisors, mandibular lateral incisors,and mandibular canines) in addition to some eruptedpermanent teeth (maxillary first molars, maxillary leftsecond premolar, mandibular first molars, and
THE JOURNAL OF PROSTHETIC DENTISTRY
Downloaded for Anonymous User (n/a) at Indiana University - Ruth Lilly MeFor personal use only. No other uses without permission.
mandibular first and second premolars). The rest of theteeth were clinically missing. A unilateral segmentalreverse articulation of the left side was noted, with slightdental wear of the primary teeth on the same side.Moreover, he presented with signs of generalized slightgingival inflammation with bleeding on probing and nosign of clinical attachment loss. The patient showedacceptable oral hygiene and no dental caries was detec-ted (Fig. 1).
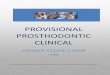
The panoramic radiograph showed congenitallymissing permanent teeth (maxillary third molars,
Alsayed et al
dical Library from ClinicalKey.com by Elsevier on November 16, 2017. Copyright ©2017. Elsevier Inc. All rights reserved.

Figure 2. Pretreatment panoramic radiograph. Figure 3. Polyvinyl siloxane putty index used to identify smile line,anterior occlusal plane, and maxillary anterior tooth width and height.
Figure 4. Digital design. A, Putty index scanned and digitally superimposed on maxillary digital casts. B, RCOPs, design and virtual tooth arrangement.RCOPs, removable complete overdenture prostheses.
- 2017 3
maxillary second molars, maxillary first and second pre-molars, maxillary canines, maxillary incisors, mandibularsecond and third molars, mandibular canines, andmandibular incisors). Complete mouth radiographsshowed no dental caries (Fig. 2). His condition wasdiagnosed by using American College of Prosthodontistsclass IV partial edentulism,22 a low smile line, anabnormal posterior cusp-to-fossa relationship with uni-lateral segmental reverse articulation of the left side, andlocalized mild attrition with wear of left maxillary centralincisor, maxillary lateral incisor, and maxillary canine.Moreover, his diagnosis included generalized, slightplaque-induced gingivitis. The patient’s teeth weremildly microdontic, and some of the primary and per-manent teeth were congenitally missing. Furthermore,the patient showed signs of reduced OVD.
Due to his incomplete growth, the treatment of choicewas to fabricate monolithic, multichromatic CAD-CAMacrylic resin RCOPs by using the AvaDent system(Global Dental Science LLC) to retain the remaining pri-mary and permanent teeth and to restore esthetics, pho-netics, and function. After the risks, benefits, and
Alsayed et al
Downloaded for Anonymous User (n/a) at Indiana University - Ruth Lilly MeFor personal use only. No other uses without permission.
alternatives were discussed with the parents, the treat-ment plan was agreed. The parents were warned that theirson might refuse to wear the RCOPs, which could add tothe complexity of the treatment and affect the outcome.
Maxillary and mandibular preliminary impressionswere made with alginate impression material (Jeltrate;Dentsply Sirona). Maxillary and mandibular custom trayswere fabricated with light-activated acrylic resin materials(Triad; Dentsply Sirona). Tray adhesive material (Ava-Dent Tray Adhesive; Global Dental Science LLC) wasapplied to the borders of the custom trays. Maxillary andmandibular border molds were made of medium bodypolyvinyl siloxane (PVS) border molding materials(AvaDent Border Molding Material; Global Dental Sci-ence LLC). The definitive impressions were made ofmedium- and light-body PVS impression materials(AvaDent Impression Material; Global Dental ScienceLLC). Stabilizing occlusal records were made of light-activated acrylic resin material (Triad; Dentsply Sirona)and type III baseplate wax (TruWax; Dentsply Sirona) tore-established the OVD. A PVS occlusal relation regis-tration material (AvaDent Registration Material; Global
THE JOURNAL OF PROSTHETIC DENTISTRY
dical Library from ClinicalKey.com by Elsevier on November 16, 2017. Copyright ©2017. Elsevier Inc. All rights reserved.

Figure 6. Milled monolithic, multichromatic RCOPs. A, Maxillary RCOP. B, Mandibular RCOP. RCOPs, removable complete overdenture prostheses.
Figure 5. Clinical evaluation of monolithic RCOPs. A, Intraoral frontal view. B, Smile view with marks to correct central incisor length. RCOPs, removablecomplete overdenture prostheses.
Figure 7. Definitive monolithic, multichromatic RCOPs, intraoral frontalview. RCOPs, removable complete overdenture prostheses.
4 Volume - Issue -
Dental Science LLC) was used to record the centricrelation at the re-established OVD. An index was madeusing PVS putty impression material (EXAFLEX Putty;GC America, Inc) to identify the smile line, anteriorocclusal plane, and maxillary anterior tooth width andheight (Fig. 3).
THE JOURNAL OF PROSTHETIC DENTISTRY
Downloaded for Anonymous User (n/a) at Indiana University - Ruth Lilly MeFor personal use only. No other uses without permission.
Definitive casts were scanned with a laboratoryscanner (Dental Wings iSeries; Dental Wings Inc) andarticulated digitally with the help of the centric relationrecord. The putty index was also scanned and digitallysuperimposed on the maxillary digital casts. Maxillaryand mandibular RCOPs were digitally designed, and aprototype was milled from tooth-colored monolithicpoly(methyl methacrylate) (PMMA) material (FunctionalBTI; Global Dental Science LLC) (Fig. 4). The RCOPsprototype was used to verify the OVD, function, occlu-sion, phonetics, and esthetics. The parents had somecomments regarding the length of the maxillary anteriorteeth, and their suggested length was marked on theRCOPs prototype (Fig. 5). The RCOPs prototype wasscanned again to record the occlusal modification andmodify the length of the maxillary teeth according to themarks. The RCOPs were then milled from monolithic,multichromatic cross-linked PMMA material (AvaDentXCL-1; Global Dental Science LLC) (Fig. 6). During thedelivery visit, the existing teeth were not modifiedbecause a relief of 0.5 mm was added over the existingteeth in the design of the prostheses. Minor adjustments
Alsayed et al
dical Library from ClinicalKey.com by Elsevier on November 16, 2017. Copyright ©2017. Elsevier Inc. All rights reserved.

Figure 8. A, Pretreatment smile. B, Post-treatment smile.
- 2017 5
were made to the intaglio surface after applyingpressure-indicating paste (PIP; Mizzy). Both of theRCOPs were then placed in the patient’s mouth, and theocclusion was adjusted (Figs. 7, 8).
Oral hygiene instructions were given, and the patientwas instructed to remove the prostheses at night andclean his teeth and both the maxillary and mandibularRCOPs with a nonabrasive paste and soft-bristle brush.Daily applications of a nonaqueous solution of topical0.4% stannous fluoride gel (Colgate Gel-Kam; Colgate-Palmolive Co) were prescribed, and the patient wasscheduled for a 3-month follow-up for more adjustmentto compensate for his skeletal and dental growth. At the2-year recall appointment, new maxillary and mandibularRCOPs will be made. When the patient attains finalskeletal growth, a definitive treatment can beimplemented.
DISCUSSION
A tentative diagnosis of ED was based on the followingclinical signs and symptoms: sparse hair, eyebrows, andeyelashes; dry skin with periorbital hyperkeratosis; dys-morphic facial features; impaired function of the exocrineglands; and a family history of ED.5 Early dental treat-ment of ED is important for a young patient’s quality oflife. Function, psychology, and esthetics can be improveddramatically by using such an approach.8,9 Moreover, theskeletal growth of young patients should be consideredand can dictate treatment. Long-term provisional treat-ment can prepare such patients for definitive treatmentoptions, including implant-supported prostheses aftercessation of skeletal growth without jeopardizing func-tion and esthetics.13
Osseointegrated implants have been widely used withhigh success rates in the management of patients withED.23 In addition, implant-supported restorations seemto positively affect the quality of life of young patients.24
Dental implants also play an important role in the
Alsayed et al
Downloaded for Anonymous User (n/a) at Indiana University - Ruth Lilly MeFor personal use only. No other uses without permission.
preservation of the alveolar bone, which is already scarcebecause of lack of teeth.25 However, several reports haveraised concerns regarding the placement of endostealimplants in young patients with growing jaws.26,27 Cro-nin et al28 described mandibular jaw growth and theconsequences of placing an implant in such a growingjaw.
Although different treatment approaches have beendescribed to treat patients with ED, a removable dentalprosthesis is considered a viable alternative, especially foryoung individuals.17 RCOPs have been successfullyimplemented as one form of treatment for patients withED who present with hypodontia and microdontia.11,13 Itis a reversible treatment that retains the remaining teethto preserve the alveolar bone.11,12 However, the inabilityof very young patients to comply with oral hygiene re-quires several recall visits and a daily application ofstannous fluoride to minimize dental caries and a peri-odic adjustment and replacement of the overdenturebecause of the child’s normal growth.11,16 Reinforcementof oral hygiene instruction for patients with ED is a keyfactor for a successful treatment outcome.29
Digital designing and milling of the RCDP providedsignificant benefits.18 Although fabricating conventionalRCDPs can be technique-sensitive, especially during thedelivery visit, these complications can be minimized withmonolithic, multichromatic CAD-CAM RCDPs.19,30 Theyrequire fewer patient visits and less chairside time,31
which benefitted a patient of his age and reduced hischances of missing classes. Using monolithic cross-linkedPMMA material (AvaDent XCL-1; Global Dental ScienceLLC) will reduce the incidence of acrylic tooth debond-ing, especially considering the minimum availability ofrestorative space and the physical activities of youngindividuals. The cost of CAD-CAM RCDPs, which ishigher than that of conventional RCDPs, is one of thelimitations of this technique.
In this clinical scenario, the centric relation record wasobtained during the jaw relations visit. The patient
THE JOURNAL OF PROSTHETIC DENTISTRY
dical Library from ClinicalKey.com by Elsevier on November 16, 2017. Copyright ©2017. Elsevier Inc. All rights reserved.

6 Volume - Issue -
exhibited good neuromuscular control, making thecentric relation record more predictable. At the clinicalevaluation visit, the RCOPs prototype was used to verifythe centric relation, and the option of trying the proto-type at home for few days was given. However, the pa-tient felt comfortable with the overall result and wasexcited to move forward with the definitive prostheses.
Clinical challenges may exist with a very young pa-tients with ED, such as a 4- to 6-year-old child. The childshould try the prototype for a few days so that theclinician can evaluate the patient’s cooperation and otherprosthetic parameters such as centric relation and OVD.The prototype should then be examined for wear facetsand any slide from centric relation that might exist shouldbe removed.
SUMMARY
This clinical report is presented to demonstrate thatmonolithic, multichromatic CAD-CAM acrylic resin(RCOPs) can be used to treat adolescent patients withED. Good oral hygiene is a key factor in the overallsuccess of the treatment. This patient tolerated his newOVD well and followed every instruction, which shouldpredict an acceptable long-term outcome and prognosis.Although special care and more experience are needed totreat these types of patients with CAD-CAM RCOPs, thisreport shows that a promising outcome can be achieved.
REFERENCES
1. Berg D, Weingold DH, Abson KG, Olsen EA. Sweating in ectodermaldysplasia syndromes. A review. Arch Dermatol 1990;126:1075-9.
2. Blattner RJ. Hereditary ectodermal dysplasia. J Pediatr 1968;73:444-7.3. Kilic S, Altintas SH, Yilmaz Altintas N, Ozkaynak O, Bayram M, Kusgoz A,
et al. Six-year survival of a mini dental implant-retained overdenture in achild with ectodermal dysplasia. J Prosthodont 2017;26:70-4.
4. Bartlett RC, Eversole LR, Adkins RS. Autosomal recessive hypohidroticectodermal dysplasia: dental manifestations. Oral Surg Oral Med Oral Pathol1972;33:736-42.
5. Kupietzky A, Houpt M. Hypohidrotic ectodermal dysplasia: characteristicsand treatment. Quintessence Int 1995;26:285-91.
6. Deshmukh S, Prashanth S. Ectodermal dysplasia: a genetic review. Int J ClinPediatr Dent 2012;5:197-202.
7. Crawford PJ, Aldred MJ, Clarke A. Clinical and radiographic dental findingsin X linked hypohidrotic ectodermal dysplasia. J Med Genet 1991;28:181-5.
8. Nakata M, Koshiba H, Eto K, Nance WE. A genetic study of anodontia in X-linked hypohidrotic ectodermal dysplasia. Am J Hum Genet 1980;32:908-19.
9. Till MJ, Marques AP. Ectodermal dysplasia: treatment considerations andcase reports. Northwest Dent 1992;71:25-8.
10. Nussbaum B, Carrel R. The behaviour modification of a dentally disabledchild. ASDC J Dent Child 1976;43:225-61.
11. Nowak A. Dental treatment for patients with ectodermal dysplasias. BirthDefects Orig Artic Ser 1987;24:243-52.
THE JOURNAL OF PROSTHETIC DENTISTRY
Downloaded for Anonymous User (n/a) at Indiana University - Ruth Lilly MeFor personal use only. No other uses without permission.
12. Tape M, Tye E. Ectodermal dysplasia: literature review and a case report.Compend Contin Educ Dent 1995;16:524-8.
13. Esposito SJ, Cowper TR. Overdentures in partial anodontia: simple solutionsfor complex problems. Compend Contin Educ Dent 1991;12:172-7.
14. Renner R, Kleinerman V. Overdenture techniques in the management ofoligodontiada case report. Quintessence Int 1980;11:57-65.
15. Goepferd SJ, Carroll CE. Hypohidrotic ectodermal dysplasia: a uniqueapproach to esthetic and prosthetic management. J Am Dent Assoc 1981;102:867-9.
16. Nomura S, Hasegawa S, Noda T, Ishioka K. Longitudinal study of jaw growthand prosthetic management in a patient with ectodermal dysplasia andanodontia. Int J Paediatr Dent 1993;3:29-38.
17. Bajraktarova Valjakova E, Misevska C, Korunoska Stevkovska V, Gigovski N,Sotirovska Ivkovska A, Bajraktarova B, et al. Prosthodontic management ofhypohidrotic ectodermal dysplasia: a case report. South Eur J Orthod Den-tofac Res 2015;2:20-6.
18. Baba NZ, AlRumaih HS, Goodacre BJ, Goodacre CJ. Current techniques inCAD/CAM denture fabrication. Gen Dent 2016;64:23-8.
19. Kattadiyil MT, Jekki R, Goodacre CJ, Baba NZ. Comparison of treatmentoutcomes in digital and conventional complete removable dental prosthesisfabrications in a predoctoral setting. J Prosthet Dent 2015;114:818-25.
20. Goodacre CJ, Garbacea A, Naylor WP, Daher T, Marchack CB, Lowry J. CAD/CAM fabricated complete dentures: concepts and clinical methods ofobtaining required morphological data. J Prosthet Dent 2012;107:34-46.
21. Kattadiyil MT, AlHelal A. An update on computer-engineered completedentures: a systematic review on clinical outcomes. J Prosthet Dent 2017;117:478-85.
22. McGarry TJ, Nimmo A, Skiba JF, Ahlstrom RH, Smith CR, Koumjian JH,et al. Classification system for partial edentulism. J Prosthodont 2002;11:181-93.
23. Wang Y, He J, Decker AM, Hu JC, Zou D. Clinical outcomes of implanttherapy in ectodermal dysplasia patients: a systematic review. Int J OralMaxillofac Surg 2016;45:1035-43.
24. Kent G, Johns R. Controlled longitudinal study on the psychological effects ofosseointegrated dental implants. Int J Oral Maxillofac Implants 1991;6:470-4.
25. Murphy WM. Clinical and experimental bone changes after intraosseousimplantation. J Prosthet Dent 1995;73:31-5.
26. Oesterle LJ, Cronin RJ Jr, Ranly DM. Maxillary implants and the growingpatient. Int J Oral Maxillofac Implants 1993;8:377-87.
27. Mankani N, Chowdhary R, Patil BA, Nagaraj E, Madalli P. Osseointegrateddental implants in growing children: a literature review. J Oral Implantol2014;40:627-31.
28. Cronin RJ Jr, Oesterle LJ, Ranly DM. Mandibular implants and the growingpatient. Int J Oral Maxillofac Implants 1994;9:55-62.
29. Baskan Z, Yavuz I, Ulku R, Kaya S, Yavuz Y, Basaran G, et al. Evaluation ofectodermal dysplasia. Kaohsiung J Med Sci 2006;22:171-6.
30. Bidra AS, Taylor TD, Agar JR. Computer-aided technology for fabricatingcomplete dentures: systematic review of historical background, current status,and future perspectives. J Prosthet Dent 2013;109:361-6.
31. Bidra AS, Farrell K, Burnham D, Dhingra A, Taylor TD, Kuo C-L. Prospectivecohort pilot study of 2-visit CAD/CAM monolithic complete dentures andimplant-retained overdentures: clinical and patient-centered outcomes.J Prosthet Dent 2016;115:578-86.
Corresponding author:Dr Hussain D. AlsayedDepartment of Prosthetic Dental SciencesCollege of Dentistry, King Saud UniversityPO Box 60169 Riyadh, 11545SAUDI ARABIAEmail: [email protected]
AcknowledgmentsThe authors thank Robert Kreyer, CDT, Director of Manufacturing, at AvaDent forlaboratory expertise and assistance in the fabrication of RCOPs.
Copyright © 2017 by the Editorial Council for The Journal of Prosthetic Dentistry.
Alsayed et al
dical Library from ClinicalKey.com by Elsevier on November 16, 2017. Copyright ©2017. Elsevier Inc. All rights reserved.