Embed Size (px)
Citation preview

Cytometry (Communications in Clinical Cytometry) 26:40-46 (1996)
Prostate Cancer: Flow Cytometric Methods for Detection of Bone Marrow Micrometastases
Maha Hussain, Mark Kukuruga, Sandra Biggar, Wael Sakr, Glenn Cummings, and John Ensley Section of Hematology/Oncology, VA Medical Center, Allen Park (M.H., S.B.); Division of Hematology/Oncology (M.H., G.C.,
J.E.), Department of Pathology (W.S.), Wayne State University; Michigan Cancer Foundation (M.K.), Detroit, Michigan
Up to 60% of patients with clinically localized prostate cancer will relapse despite potentially curative local treatment. Current staging tests have been limited in adequately identifying individual patients who are at a high risk for future relapse. Detection of bone marrow micrometastases may identify individuals destined to develop clinically detectable systemic metastases. Although immunohistochemistry and molecular ap- proaches are being investigated, the most ideal test(s1 are yet to be determined. In this report we describe methods for specific detection and isolation of prostate cancer micrometastases by multi-parameter rare event flow cytometric analysis. A model was developed and validated using three human prostate cancer cell lines, healthy donor marrow, dual marker labeling for cytokeratin (epithelial-specific marker) and CD45 (bone marrow-specific marker). The detection sensitivity of this model was at the level of one prostate cancer cell in 100,000 nucleated bone marrow cells. As a part of an ongoing clinical study, bone marrow aspirates from 15 patients with newly diagnosed prostate cancer have been analyzed. Six patients were found to have cytokeratin positive/CD45 negative cells in their bone marrow aspirates. We conclude that flow cytometric rare event analysis provides a sensitive and specific assay for detection of bone marrow micrometastases in patients with clinically localized prostate cancer. o 1996 Wiley-Liss, tnc.
Key terms: Prostate cancer, bone marrow, micrometastases
Clinically localized prostate cancer accounts for an in- creasing percentage of all diagnosed prostate cancer cases. Patients with localized disease are candidates for a variety of treatment options ranging from radical pros- tatectomy, radiation therapy, primary androgen depriva- tion therapy, or expectant management. Defining the need for treatment and the ideal treatment approach has been hampered by lack of precise prognostic factors that can discriminate between clinically significant and insig- nificant cancers, a crucial distinction for appropriate de- cision making.
Current data indicate that up to 60% of patients with localized prostate cancer will relapse despite potentially curative local treatment (1-7). This suggests that unde- tectable micrometastases must have been present at time of initial diagnosis, thus underscoring the limitations of current staging tests to reliably identify patients who are at high risk for future systemic metastases. By identifying these patients at the time of initial diagnosis, more appro- priate therapy decisions could be made.
Prostate cancer is unique in its preferential pattern of metastases to bone and bone marrow. This, coupled with the ease with which bone marrow may be accessed, al- lows for a unique approach in assessing true pathologic stage. The presence of bone marrow micrometastases has
0 1996 Wiley-Liss, Inc.
been an important prognostic factor in other solid tumors such as breast and gastric carcinoma and the finding of early hematogenous metastases should better our under- standing of the biology of this disease.
Both peripheral blood and bone marrow have been examined for micrometastases. While peripheral blood provides an easier target, the detection of cancer cells in the bone marrow may be a superior indicator of early metastases since the latter is a recognized metastatic site, whereas the former is the conduit for metastases and tumor cells are known to circulate. Proving the superi- ority of either would require a prospective comparison, an approach that is yet to be evaluated.
Early prostate cancer metastases to bone marrow have been sought in a variety of methods. Assaying marrow
Received for publication April 2, 1995; accepted July 5, 1995. This research was supported by the Wayne State University Fund for
Medical Research Education grant 09-62, by grant IRG162F from the American Cancer Society, a grant from DMCIOAD, and by funds from the Analytical Cytometry Facility of Meyer L. Prentis Comprehensive Cancer Center, USDHHS Ca-22453.
Address reprint requests to Maha Hussain, M.D., 111 G, Oncology, VA Medical Center, Allen Park, MI 48101.

FLOW CYTOMETRY FOR DETECTING MICROMETASTASES 41
prostatic acid phosphatase proved to be non-specific (8- 10). Immunohistochemical evaluation of whole marrow aspirates were also investigated and found to be more sensitive than routine hematomorphologic examination with 13% of patients with localized prostate cancer dem- onstrating "abnormal cells" in the bone marrow ( 11 ). This procedure has been limited by its high labor inten- sity, semi-quantitative nature, and moderate objectivity. Efforts at developing methods of greater sensitivity and specificity led to the use of reverse transcriptase poly- merase chain reaction (RT-PCR) to detect PSA mRNA either in peripheral blood or bone marrow (12-16). RT-PCR was found to be more sensitive than immuno- histochemistry in identifying prostate cancer cells ad- mixed with lymphocytes at concentrations of 1 : 1 05-10" (12). The same authors found that 29/55 patients with prostate cancer are marrow-positive for PSA mRNA by RT-PCR Of the 29 positive samples, 24 had evaluable slides and 19/24 samples had identifiable metastatic cells by immunohistochemistry ( 13). While the discrepancy in detection rate is likely to be a function of the extreme sensitivity of RT-PCR as compared with immunohisto- chemistry, recent observations raise concern regarding the specificity of the former with our finding of PSA-RNA in non-prostate cancer cell lines (HLGO and BGl) and in some normal blood (obtained from male and female vol- unteers) using "nested primer" PCR and recent reports on the presence of a Mr33,OOO protein in breast cancer identical to PSA produced by the prostate ( 17-19). These findings impact on the utility of PSA RT-PCR in detecting micrometastatic cells. The lack of selective RNA extrac- tion from the micrometastatic cells introduces the poten- tial for reduced specificity (20). While sensitivity is im- portant, for a particular test to be of clinical value, it must fulfill additional requirements (21). Above all, it must show a high level of specificity and prognostic value in- dependent of other variables. There is currently no single test that is proven to fulfill these requirements com- pletely.
Ideally, isolating metastatic cells is as important as de- tecting their presence. By selectively isolating whole met- astatic cells, further specific and comparative molecular characterization can be performed relative to the primary tumor. In this regard flow cytometry is especially suited for this task. Its ability for multiparameter analysis and sorting provides a unique approach to simultaneously de- tect and selectively isolate micrometastases. The sorting of whole metastatic cells is extremely attractive because coupled with an additional confirmatory test, such as molecular and/or immunocytologic evaluation, it will as- sure a higher level of specificity which is a must for clin- ical decision making. This provides the rationale for our current approach towards detecting micrometastases.
MATERIALS AND METHODS The methods for detecting micrometastatic cells in the
bone marrow were developed using the LNCaP cell line, a human metastatic prostate adenocarcinoma, and mono- clonal antibodies recognizing cytokeratin 8 and 18. Since
prostate cancer is epithelial in origin it expresses cyto- keratin antigens. Normal bone marrow cells do not ex- press cytokeratin and epithelial cells are not found in normal volunteers ( 11 ). The model was then extended to other human prostate cancer cell lines. A negative selec- tion marker, anti-CD45, was added to further enhance rare cancer cell detection.
Human Cell lines LNCaP, PC3, and DU145 prostate cancer cell lines
(American Type Culture Collection, Rockville, MD) were used as positive controls. LNCaP was grown in RPMI medium at 37"C, supplemented with 8% FBS and glu- tamine. PC3 was grown in F12 medium at 37"C, supple- mented with 8% FBS and glutamine. DU145 was grown in MEM medium at 37"C, supplemented with 8% FBS, 1% sodium pyruvate, glutamine, and 1% non-essential amino acids. Cells were obtained by trypsinization at confluence.
Human Bone Marrow Normal marrow was obtained from healthy donors as
part of the Wayne State University transplant program. Heparinized bone marrow is filtered to remove bone fragments and kept at room temperature until processing.
Monoclonal Antibodies The following monoclonal antibodies ( MoAB) were
used: FITC conjugated anti-cytokcratin (Cam 5.2) (Bec- ton-Dickinson, San Jose, CA), FITC conjugated IgG2a neg- ative control (Becton-Dickinson), phycoerythrin (PE) conjugated anti-CD45 (Caltag, So. San Francisco, CA), PE conjugated IgGl negative control (Caltag).
Test Dilutions Serial dilutions were made of the LNCaP cells diluted
in bone marrow cells for a final concentration ranging from lo%, 1%, 0.01%, and 0.001%.
Sample Fixation, Permeabilization, and Staining Cultured prostate cancer cells are trypsinized, washed
once in RPMI + 2% FBS, then resuspended and counted. Bone marrow cells are counted similarly. A standard 1 X
lo6 cells/tube of bone marrow or prostate cancer cells are prepared. Next, 0.2 pgll0' cells of PE-CD45 or PE- IgGl negative control is added to bone marrow samples. Tubes are then vortexed and incubated at room temper- ature for 15 min. Bone marrow and prostate cell samples are then each incubated for 5 min at room temperature with 2 ml/106 cells of FACS lysing solution (Becton-Dick- inson) supplemented with 0.025% Triton X-100 (Sigma, St. Louis, MO). Samples are centrifuged at 1,500 rpm for 5 min and supernate decanted. All tubes are washed with 2 ml Hanks' balanced salt solution (HBSS), vortexed and centrifuged for 5 min at 1,500 rpm, and supernate de- canted. Next, 0.375 p,g/106 cells of FITC-cytokeratin or FITC-IgG2a negative control is added to prostate cancer cells and bone marrow samples. Tubes are incubated for 15 min at room temperature. Then, 1 ml of HBSS is added
42 HUSSAIN ET AL.
to each tube as a wash and tubes are vortexed and cen- trifuged at 1,500 rpm for 5 min. After decanting, all sam- ples are resuspended in 250 p1 of PBS + 4% formalde- hyde and analyzed.
Rare Event Flow Cytometric Analysis A Becton-Dickinson FACStar cell sorter with consort
30 research software is used for analysis and sorting. Some analyses were performed using either a BD FACS 440 cell sorter or a FACScan cytometer. Sheath fluid is filtered through a 0.2 pM membrane filter to reduce background noise, and the fluidics system is flushed thor- oughly with bleach and ethanol prior to analysis, and fre- quently during rare event sorting. Control and compen- sation setup samples are typically analyzed to lo5 events. Admixed samples, depending upon percentage of cancer cells, are acquired to 2 X lo5 events, or a live gate on FITC-cytokeratin positive cells is established, and total counts are accumulated via counters on the FACS con- sole. The higher dilution samples are typically aspirated entirely. Dually labeled cell line samples are used to es- tablish sort windows, and cells are then sorted to micro- scope slides while events are continuously counted. Slides are air-dried and stained for morphologic and PSA confirmation, or sealed with vacuum grease and cover slips for viewing by fluorescence microscopy.
Statistical Analysis The sensitivity of the model was tested using Linear
Regression Procedure in the SAS/Stat Statistical Package (22) for the observed values vs. the expected values based on results of serial dilution mixing experiments. A log transformation was used on all data.
RESULTS Optimization of Permeabilization, Fixation, and Staining Cytokeratin measurement requires adequate cellular
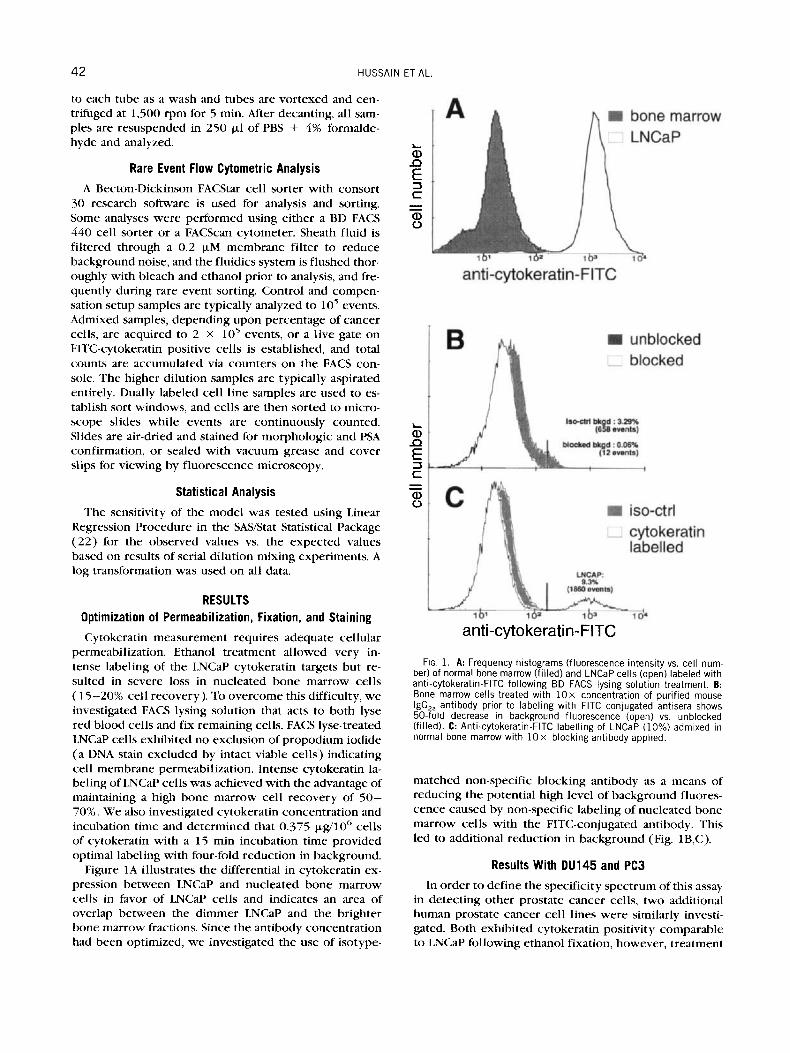
permeabilization. Ethanol treatment allowed very in- tense labeling of the LNCaP cytokeratin targets but re- sulted in severe loss in nucleated bone marrow cells ( 15-20% cell recovery). To overcome this difficulty, we investigated FACS lysing solution that acts to both lyse red blood cells and fix remaining cells. FACS lyse-treated LNCaP cells exhibited no exclusion of propodium iodide (a DNA stain excluded by intact viable cells) indicating cell membrane permeabilization. Intense cytokeratin la- beling of LNCaP cells was achieved with the advantage of maintaining a high bone marrow cell recovery of 50- 70%. We also investigated cytokeratin concentration and incubation time and determined that 0.375 pg/lO" cells of cytokeratin with a 15 min incubation time provided optimal labeling with four-fold reduction in background.
Figure 1A illustrates the differential in cytokeratin ex- pression between LNCaP and nucleated bone marrow cells in favor of LNCaP cells and indicates an area of overlap between the dimmer LNCaP and the brighter bone marrow fractions. Since the antibody concentration had been optimized, we investigated the use of isotype-
L a, 0
3 c a, 0
E
- -
L a, a 3 c a, 0
E
- -
an ti -cyto keratin- Fl TC
FIG. 1. A: Frequency histograms (fluorescence intensity vs. cell num- ber) of normal bone marrow (filled) and LNCaP cells (open) labeled with anti-cytokeratin-FlTC following BD FACS lysing solution treatment. 6: Bone marrow cells treated with l o x concentration of purified mouse IgG,, antibody prior to labeling with FITC conjugated antisera shows 50-fold decrease in background fluorescence (open) vs. unblocked (filled). C: Anti-cytokeratin-FITC labelling of LNCaP (10%) admixed in normal bone marrow with l o x blocking antibody applied.
matched non-specific blocking antibody as a means of reducing the potential high level of background fluores- cence caused by non-specific labeling of nucleated bone marrow cells with the FITC-conjugated antibody. This led to additional reduction in background (Fig. lB,C).
Results With DU145 and PC3 In order to define the specificity spectrum of this assay
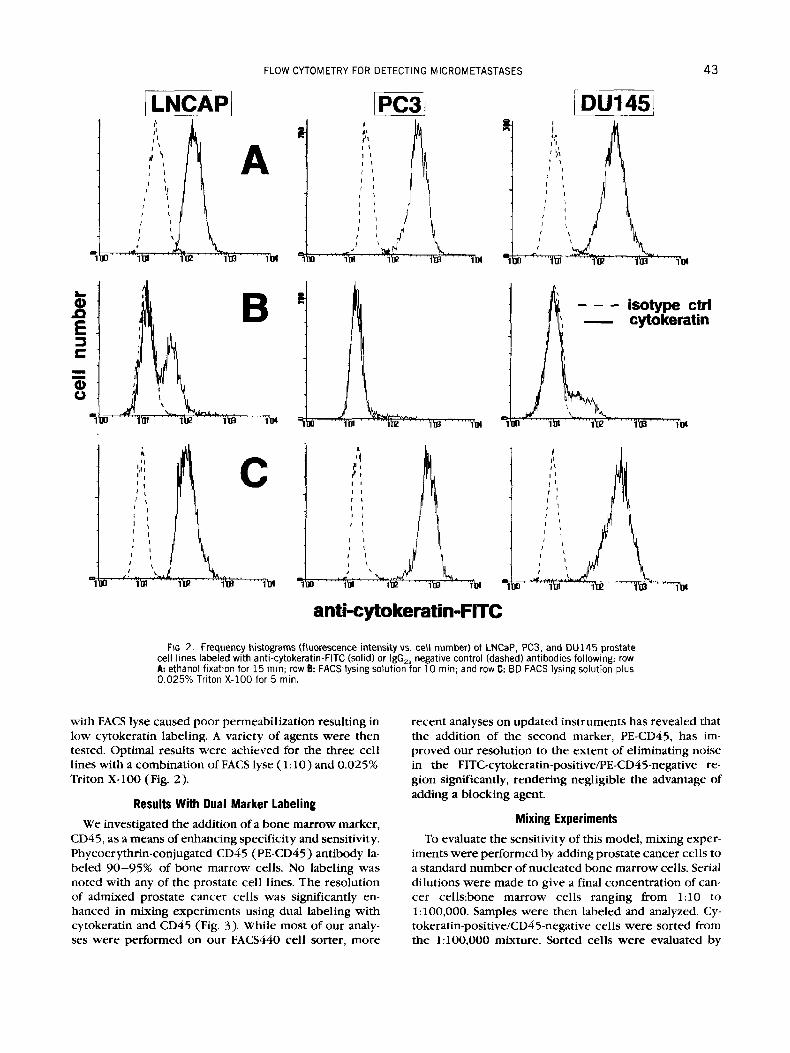
in detecting other prostate cancer cells, two additional human prostate cancer cell lines were similarly investi- gated. Both exhibited cytokeratin positivity comparable to LNCaP following ethanol fixation, however, treatment
FLOW CYTOMETRY FOR DETECTING MICROMETASTASES 43
1 LNCAPI 1 PC3J [DU145/
isotype ctrl -:- cytoketatin
I I ' I' I 1
ant i-cyto kerat i n-FITC
FIG. 2. Frequency histograms (fluorescence intensity vs. cell number) of LNCaP, PC3, and DU145 prostate cell lines labeled with anti-cytokeratin-FlTC (solid) or IgG,, negative control (dashed) antibodies following: row A: ethanol fixation for 15 rnin; row B: FACS lysing solution for 10 rnin; and row C: BD FACS lysing solution plus 0.025% Triton X-100 for 5 rnin.
with FACS lyse caused poor permeabilization resulting in low cytokeratin labeling. A variety of agents were then tested. Optimal results were achieved for the three cell lines with a combination of FACS lyse ( 1 : l O ) and 0.025% Triton X-100 (Fig. 2).
Results With Dual Marker Labeling We investigated the addition of a bone marrow marker,
CD45, as a means of enhancing specificity and sensitivity. Phycoerythrin-conjugated CD45 (PE-CD45) antibody la- beled 90-95% of bone marrow cells. No labeling was noted with any of the prostate cell lines. The resolution of admixed prostate cancer cells was significantly en- hanced in mixing experiments using dual labeling with cytokeratin and CD45 (Fig. 3). While most of our analy- ses were performed on our FACS440 cell sorter, more
recent analyses on updated instruments has revealed that the addition of the second marker, PE-CD45, has im- proved our resolution to the extent of eliminating noise in the FITC-cytokeratin-positive/PE-CD45-negative re- gion significantly, rendering negligible the advantage of adding a blocking agent.
Mixing Experiments To evaluate the sensitivity of this model, mixing exper-
iments were performed by adding prostate cancer cells to a standard number of nucleated bone marrow cells. Serial dilutions were made to give a final concentration of can- cer cel1s:bone marrow cells ranging from 1 : l O to 1 : 100,000. Samples were then labeled and analyzed. Cy- tokeratin-positiveKD45-negative cells were sorted from the 1:100,000 mixture. Sorted cells were evaluated by
HUSSAIN ET AL. 44
W
cu -I LL
a \
. _i h 'a
A
. . B
I
an ti-cytokerati n- FlTC
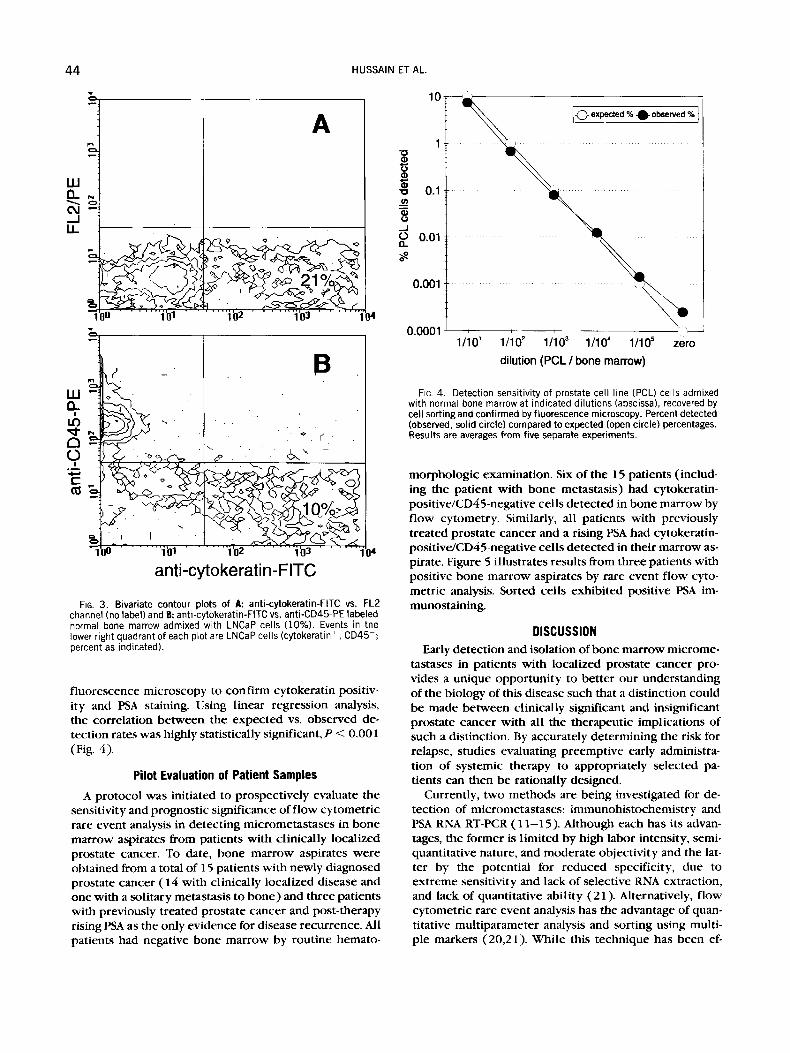
FIG. 3. Bivariate contour plots of A: anti-cytokeratin-FlTC vs. FL2 channel (no label) and B: anti-cytokeratin-FlTC vs. anti-CD45-PE labeled normal bone marrow admixed with LNCaP cells (10%). Eve+nts in the lower right quadrant of each plot are LNCaP cells (cytokeratin , CD45-; percent as indicated).
fluorescence microscopy to confirm cytokeratin positiv- ity and PSA staining. Using linear regression analysis, the correlation between the expected vs. observed de- tection rates was highly statistically significant, P < 0.001 (Fig. 4).
Pilot Evaluation of Patient Samples A protocol was initiated to prospectively evaluate the
sensitivity and prognostic significance of flow cytometric rare event analysis in detecting micrometastases in bone marrow aspirates from patients with clinically localized prostate cancer. To date, bone marrow aspirates were obtained from a total of 15 patients with newly diagnosed prostate cancer (14 with clinically localized disease and one with a solitary metastasis to bone) and three patients with previously treated prostate cancer and post-therapy rising PSA as the only evidence for disease recurrence. All patients had negative bone marrow by routine hemato-
0 expected % * observed % Tr I -J 2 0.01
8
0.001
0.0001 1/10' 1/10' i/i03 1/10' 1110~ zero
dilution (PCL / bone marrow)
FIG. 4. Detection sensitivity of prostate cell line (PCL) cells admixed with normal bone marrow at indicated dilutions (abscissa), recovered by cell sorting and confirmed by f luorescence microscopy. Percent detected (observed, solid circle) compared to expected (open circle) percentages. Results are averages from five separate experiments.
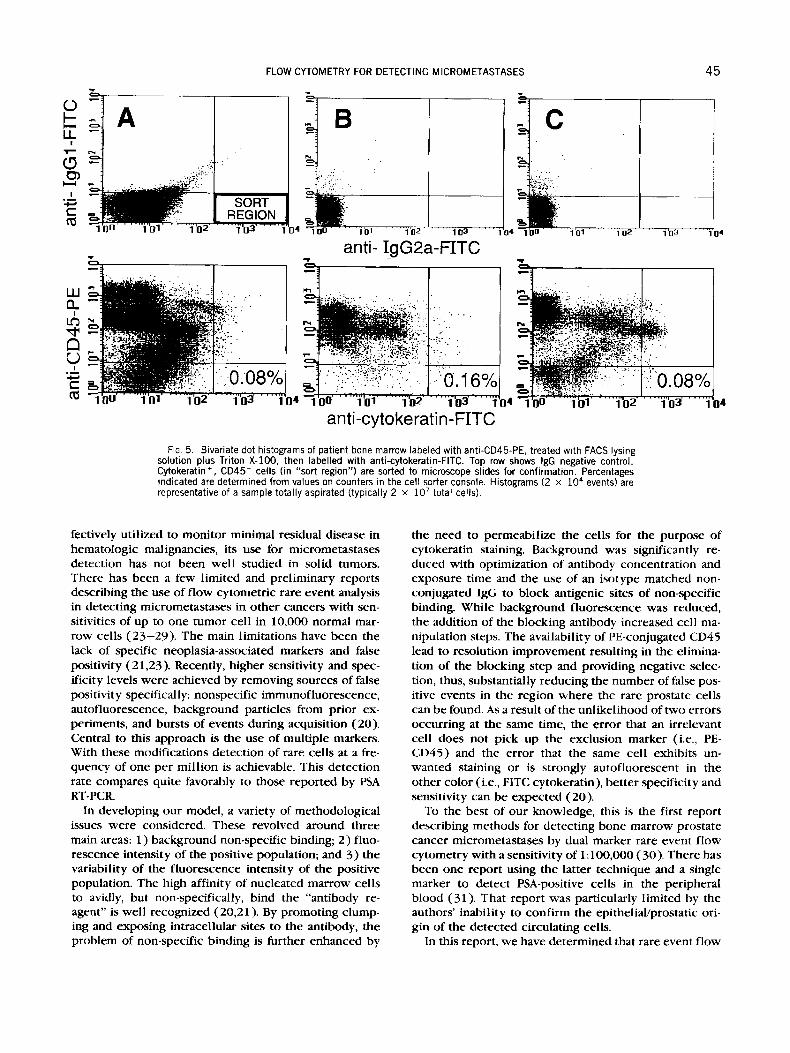
morphologic examination. Six of the 15 patients (includ- ing the patient with bone metastasis) had cytokeratin- positiveKD45-negative cells detected in bone marrow by flow cytometry. Similarly, all patients with previously treated prostate cancer and a rising PSA had cytokeratin- positive/CD45-negative cells detected in their marrow as- pirate. Figure 5 illustrates results from three patients with positive bone marrow aspirates by rare event flow cyto- metric analysis. Sorted cells exhibited positive PSA im- munostaining.
DISCUSSION Early detection and isolation of bone marrow microme-
tastases in patients with localized prostate cancer pro- vides a unique opportunity to better our understanding of the biology of this disease such that a distinction could be made between clinically significant and insignificant prostate cancer with all the therapeutic implications of such a distinction. By accurately determining the risk for relapse, studies evaluating preemptive early administra- tion of systemic therapy to appropriately selected pa- tients can then be rationally designed.
Currently, two methods are being investigated for de- tection of micrometastases: immunohistochemistry and PSA RNA RT-PCR ( 1 1-1 5). Although each has its advan- tages, the former is limited by high labor intensity, semi- quantitative nature, and moderate objectivity and the lat- ter by the potential for reduced specificity, due to extreme sensitivity and lack of selective KNA extraction, and lack of quantitative ability ( 2 1 ). Alternatively, flow cytometric rare event analysis has the advantage of quan- titative multiparameter analysis and sorting using multi- ple markers (20,2 1). While this technique has been ef-
FLOW CYTOMETRY FOR DETECTING MICROMETASTASES 45
w a IA * u n .- + C (II 4
an ti-cyto kerat i n -FITC
FIG 5. Bivariate dot histograms of patient bone marrow labeled with anti-CD45-PE, treated with FACS lyslng solution PI”,” Triton X-100, then labelled with anti-cytokeratin-FlTC. Top row shows IgG negative control. Cytokeratin , CD45- cells (in “sort region”) are sorted to microscope slides for confirmation. Percentages indicated are determined from values on counters in the cell sorter console. Histograms (2 x lo4 events) are representative of a sample totally aspirated (typically 2 x lo7 total cells).
fectively utilized to monitor minimal residual disease in hematologic malignancies, its use for micrometastases detection has not been well studied in solid tumors. There has been a few limited and preliminary reports describing the use of flow cytometric rare event analysis in detecting micrometastases in other cancers with sen- sitivities of up to one tumor cell in 10,000 normal mar- row cells (23-29). The main limitations have been the lack of specific neoplasia-associated markers and false positivity ( 2 1,23). Recently, higher sensitivity and spec- ificity levels were achieved by removing sources of false positivity specifically: nonspecific immunofluorescence, autofluorescence, background particles Erom prior ex- periments, and bursts of events during acquisition (20). Central to this approach is the use of multiple markers. With these modifications detection of rare cells at a fre- quency of one per million is achievable. This detection rate compares quite favorably to those reported by PSA
In developing our model, a variety of methodological issues were considered. These revolved around three main areas: 1) background non-specific binding; 2) fluo- rescence intensity of the positive population; and 3) the variability of the fluorescence intensity of the positive population. The high affinity of nucleated marrow cells to avidly, but non-specifically, bind the “antibody re- agent” is well recognized (20,21). By promoting clump- ing and exposing intracellular sites to the antibody, the problem of non-specific binding is further enhanced by
RT-PCR.
the need to permeabilize the cells for the purpose of cytokeratin staining. Background was significantly re- duced with optimization of antibody concentration and exposure time and the use of an isotype matched non- conjugated IgG to block antigenic sites of non-specific binding. While background fluorescence was reduced, the addition of the blocking antibody increased cell ma- nipulation steps. The availability of PE-conjugated CD45 lead to resolution improvement resulting in the elimina- tion of the blocking step and providing negative selec- tion, thus, substantially reducing the number of false pos- itive events in the region where the rare prostate cells can be found. As a result of the unlikelihood of two errors occurring at the same time, the error that an irrelevant cell does not pick up the exclusion marker (i.e., PE- C D 4 5 ) and the error that the same cell exhibits un- wanted staining or is strongly autofluorescent in the other color (i.e., FITC cytokeratin), better specificity and sensitivity can be expected (20).
To the best of our knowledge, this is the first report describing methods for detecting bone marrow prostate cancer micrometastases by dual marker rare event flow cytometry with a sensitivity of 1:100,000 (30). There has been one report using the latter technique and a single marker to detect PSA-positive cells in the peripheral blood (31). That report was particularly limited by the authors’ inability to confirm the epitheliaVprostatic ori- gin of the detected circulating cells.
In this report, we have determined that rare event flow
46 HUSSAIN ET AL.
cytometric analysis can be used to detect cytokeratin- positiveKD45-negative cells admixed with bone marrow with a sensitivity of 1:100,000 using dual markers. While preliminary, this was successfully applied to patients with localized prostate cancer. Sorted cells exhibited PSA positivity. Whereas PSA positivity coupled with cytoker- atin positivity provides a reasonable assurance of the cells prostatic origin, they are not a confirmation of ma- lignancy. In the absence of neoplasia-associated markers, adequate follow-up observations on relapse and survival will be necessary for the confirmation of the malignant nature of the isolated “micrometastatic cells.”
LITERATURE CITED 1. Partin AW, Pound CR, Clemens JQ, Epstein JI, Walsh PC: Serum PSA
after anatomic radical prostatectomy: the Johns Hopkins experience after 10 years. Urol Clin North Am 20:713-725, 1993.
2. Schroeder FH, Belt E: Carcinoma of the prostate: a study of 213 patients with stage C tumors treated by total perineal prostatectomy. J Urol 114:257-260, 1975.
3. Paulson DF, Lin GH, Hinshaw W, Stephani S, and The Uro-Oncology
15. Katz AE, Olsson CA, Raffo AJ, C m a C, Perlman H, Seaman E, O’Toole KM, McMahon D, Benson MC, Buttydn R: Molecular staging of pros- tate cancer with the use of an enhanced reverse transcriptase-PCR assay. Urology 43:765-775, 1994.
16. Seiden MV, Kantoff PW, fiithivd K, Propert y Bryant M, Haltom E, Gaynes L, Bubley ti, DeWolf W, and Sklar J: Detection of circulating mmor cells in men with localized prostate cancer. J Clin Oncol 122634-2639, 1994.
17. Smith MR, Biggar S, Hussain M: Nested PCR detects prostate specific antigen RNA in non-prostate cells [ abstr]. Proc Am Assoc Cancer Res 35:abst 1174, 1994.
18. Smith RM, Biggar S. Hussain M: Prostate specific antigen mRNA is expressed in non-prostate cells: implications for detection of mi- crometastases. Cancer Res 1994, 55:2640-2644, 1995.
19. Monne M, Croce CM, Yu H, Diamandis EP: Molecular chxacteriza- tion of prostate specific antigen messenger RNA expressed in breast tumors. Cancer Res 54:6344-6347, 1994.
20. Gross HJ. Verwer B, Houck D, Recktenwald D: Detection of rare cells at a frequency of one per million by flow cytometry. Cytometry
21. Ryan DH: Detection of minimal residual disease by flow cytometry. In: Clinical Flow Cytometry Principles and Application, Bauer KD, Duque RE, Shanky IT (eds). Williams and Wilkins. Baltimore, 1993,
22. SAS Institute: The REG Procedure. In: SAS/STAT User’s Guide, Ver- sion 6, Fourth Edition, Volume 2. Sk’ Institute, Cary, NC, 1990, pp
14:519-526, 1993.
pp 479-496.
~~ . , Research Group: Radical surgery versus radiotherapy for adenoc&- cinoma of the prostate. J Urol 128:502-504, 1982.
4. Gibbons RP, Correa RJ, Brannen GE, Weissman RM: Total prostatec-
135 1-1 456. 23. Dantas ME, Brown JP, Thomas MR, Robinson WA, Glode LM: Detec-
tion of melanoma cells in bone marrow using monoclonal antibod- tomy for localized prostate cancer: long term results. J Urol 141: 564-566, 1989.
5. Barzell W. Bean MA. Hiallaris BS. Whitmore WF Tr: Total oerinral
ics. A comparison of fluorescence activated cell sorting (FACS) and conventional immunofluorescence. Cancer 52:949-953, 1983.
24. Leslie DS, Johnston W, Daly L, Ring DB, Shpall EJ, Peters WP, Bast prostatectomy for carcinoma of the prostate. J Uiol 118:2%3-282, 1977.
6. Paulson DF, Moul JW, Walther PJ: Radical prostatectomy for clinical stage TI-2NOMO prostate adenocarcinorna: long-term results. J Urol 144:1180-1184, 1990.
7. I.erner SP, Seal-Hawkins C, Carlton CE Jr, Scardino PT: The risk of dying of prostate cancer in patients with clinically localited disease. J Urol 146:1040-1045, 1991.
8. Pontes JE, Choe B, Rose N, Pierce JM: Reliability of bone marrow acid phosphatax. as a parameter of metastatic prostate cancer. J Urol
9. Bellville WD, Mahan De, Sepulveda RA, Bruce AW, Miller CF: Bone marrow acid phosphatase by radioimmunoassay: 3 years of experi- ence. J Urol 125:809-811, 1981.
10. Cooper JF, Foti AG, Shank PW: Radioimmunochemical measurement of bone marrow acid phosphatase. J Urol 119392495. 1978.
11. Mansi JL, Berger U, Wilson R, Shearer R, Coombes RC: Detection of tumor cells in bone marrow of patients with prostatic carcinoma by immunochemical techniques. J Urol 139545-548, 1988.
12. Wood DR Jr, Banks ER, Humphreys S, Rangnekar VM: Sensitivity of immunohistochemistry and polymerase chain reaction in detecting prostate cancer cells in bone marrow. J Histochem Cytochem 42:
13. Wood DP, Banks ER, Humphreys S, McRoberts JW, Rangnekar VM: Identification of bone marrow micrometastases in paticnts with prostate cancer. Cancer 74:2533-2540, 1994.
14. Moreno JG, Croce MC, Fischer R, Monne M, Vihko P, Mulholland SG, Gomella LG Detection of hematogenous micrometastasis in patients with prostate cancer. Cdnccr Res 52:6110-6112, 1992.
1 22: 1 78 - 1 79, 1979.
505-51 1, 1994.
RC J r Detection of breast carcinoma cells in human bone marrow using fluorescence-activated cell sorting and conventional cytology. Am J Win Pathol 94:s-13, 1990.
25. Gazitt Y, Lee C, Gross S: A rapid F A G method with 3 log accuracy for detection of neuroblastoma cells in purged marrow labstr]. Proc Am Soc Clin Oncol 9.A1155, 1990.
26. Vredenburgh JJ, Davis B, Ball ED: The detection of low percentages of small cell carcinoma of the lung or breast cancer cells in the bone marrow by two-color flow cytometry [abstrl. Proc Am Soc Clin Oncol YA23, 1990.
27. Mansi JL. Mesker WE, McDonnell T, Van Driel-Kulker AM, Ploem JS, Coombes RC: Automated screening for micrometastases in bone marrow smears. J Immunol Methods 112:105-111, 1988.
28. Miglierina R, Aubree B, Pancino G, Calvo F, Roseto A: Detection of rare metastatic breast cancer cells in the bone marrow by flow cytometry using monoclonal antibody 7810 in an experimental model. J Tumor Marker Oncol4:45-53, 1989.
29. M o h o A, Colombatti M, Bonetti F, Zardini M, Pasini F, Perini A, Pelosi G, Tridente G, Veneri D, Cetto GL A comparative analysis of three different techniques for the detection of breast cancer cells in bone marrow. Cancer 671033-1036, 1991.
30. Hussain M, Ensley J, Maciorowski 2. Pieuaszkiewicz H: Sensitivity of flow cytometric rare event analysis in detection of prostate cancer in human bone marrow [abstr]. Proc Am Assoc Cancer Kes 32A162. 1991.
31. Hamdy FC, Iawry J, Anderson JB, Parsons MA, Rees RC, Williams J L Circulating prostate specific antigen-positive cells correlatc with metastatic prostate cancer. Br J Urol 69392-396, 1992.