Embed Size (px)
Citation preview
INTERNATIONAL LECTURE
Prospects and Predictions for theCardiomyopathies
ByJ. F. GOODWIN, M.D., F.R.C.P., F.A.C.C.
Additional Indexing Words:Idiopathic hypertrophic subaortic stenosisCatecholamineLeft ventricular hypertrophyPropranolol Pract4o]
IN THIS LECTURE I shall attempt to surveythe current important problems in the commonest
forms of cardiomyopathies and suggest avenues alongwhich research may profitably proceed in the future.The classification of the cardiomyopathies into
hypertrophic, congestive, obliterative, and restrictivehas the advantage of allowing a study in depth to bemade of the pathological, functional, and clinicalfeatures of these types without prior knowledge oftheir etiology. The classification also assists the iden-tification of various forms of cardiomyopathy in cir-cumstances where causal factors are being sought.'
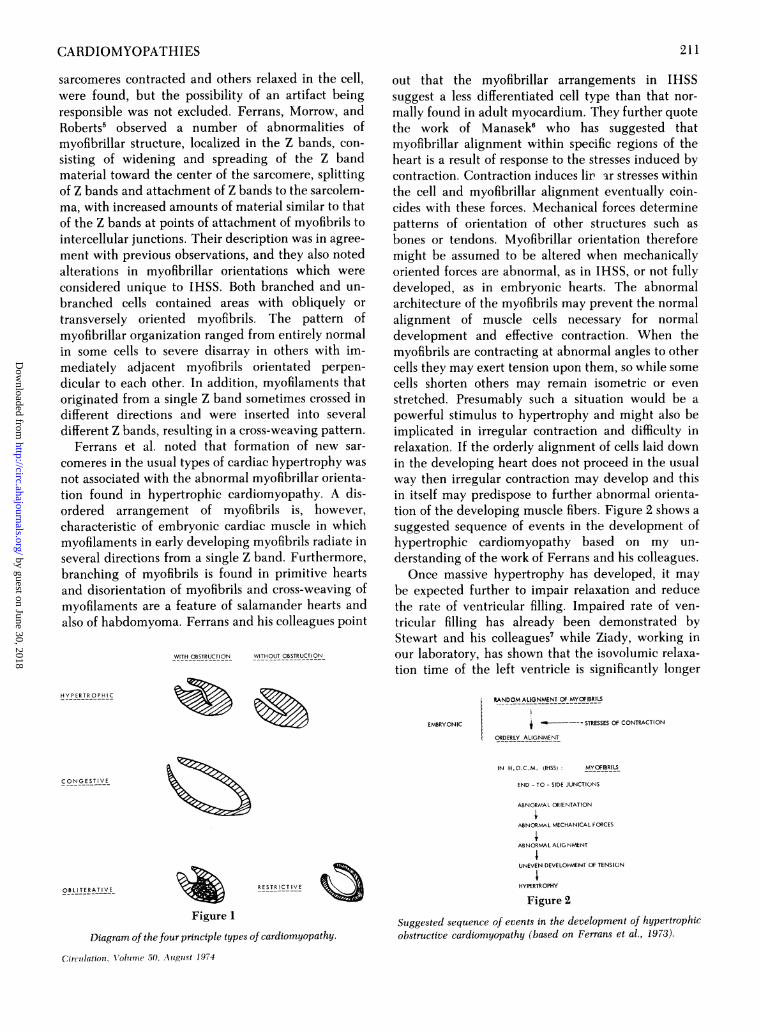
Figure 1 shows the four types in diagrammaticform. The general characteristics of each type are wellknown. In the hypertrophic form there is massive ven-tricular muscle hypertrophy with reduction in end-systolic volume and often a concentration of hyper-trophy in the region of the septum forming theasymmetrical bulge that inspired Teare2 to name thecondition "Asymmetrical hypertrophy of the heart."With this concentration of the disease in the region ofthe septum there is commonly a gradient in systoleacross the outflow tract and the condition is thenusually known as Hypertrophic Obstructive Car-diomyopathy or Idiopathic Hypertrophic SubaorticStenosis (IHSS). In about 10 to 20% of patients,however, no gradient is discernible either at rest or on
From the Division of Cardiovascular Disease (Clinical Car-diology), Department of Medicine, Royal Postgraduate MedicalSchool and Hammersmith Hospital, London, England.
This paper is based on the International Lecture of the AmericanHeart Association, delivered at the 25th Annual Meeting in AtlanticCity, New Jersey, November, 1973.
Address for reprints: Dr. J. F. Goodwin, Clinical Cardiology,Royal Postgraduate Medical School, Hammersmith Hospital, Lon-don W12, England.
210
Beta-adrenergic blockade Beta-adrenergic stimulationFriedreich's ataxia Pompe's disease
Congestive cardiomyopathy Chagas' diseaselol Left ventricular outflow obstruction
provocation and the disorder is then termedNonobstructive Hypertrophic Cardiomyopathy.Opinion is divided as to whether these two conditionsare basically the same disease or whether they aredifferent entities, but in my view the evidence pointsstrongly to their being different facets of the same dis-ease.The congestive type of cardiomyopathy is
characterized by considerable dilatation of the leftventricle but moderate hypertrophy. The contractilefunction of the heart is severely damaged and theheart has very poor pump function. No obstructiveelement is present in this type.The obliterative type embraces Endomyocardial
Fibrosis of humid tropical zones and Loeffler'seosinophilic cardiomyopathy of temperate zones, butit has been suggested that these two conditions arebasically the same disease.3 Here the ventricularcavities, notably the inflow tracts, become obliteratedby fibrous tissue and added thrombus.The restrictive type is characterized by stiff muscle
without marked hypertrophy, as in amyloid disease.
Hypertrophic Cardiomyopathy
The pathology of this condition is now wellrecognized and the characteristic lesion is grosslyhypertrophied, short, thick, fragmented muscle fibersconcentrated in circular arrangements, or whorls, withlarge nuclei and perinuclear spaces. The abnormalmyocardial fibers may be interrupted by fibrous tissuewhich arises within the myocardial fibers and spreadstoward the surface, replacing a variable amount ofmuscle tissue, which results in shortening of the fiberand its termination in collagen tissue.4
In the original observations of our group4 many in-stances of irregular cellular contraction, with some
Circulation, Volinel( .5( utgtst 1.974
by guest on June 30, 2018http://circ.ahajournals.org/
Dow
nloaded from
CARDIOMYOPATHIES
sarcomeres contracted and others relaxed in the cell,were found, but the possibility of an artifact beingresponsible was not excluded. Ferrans, Morrow, andRoberts5 observed a number of abnormalities ofmyofibrillar structure, localized in the Z bands, con-sisting of widening and spreading of the Z bandmaterial toward the center of the sarcomere, splittingof Z bands and attachment of Z bands to the sarcolem-ma, with increased amounts of material similar to thatof the Z bands at points of attachment of myofibrils tointercellular junctions. Their description was in agree-ment with previous observations, and they also notedalterations in myofibrillar orientations which wereconsidered unique to IHSS. Both branched and un-branched cells contained areas with obliquely ortransversely oriented myofibrils. The pattern ofmyofibrillar organization ranged from entirely normalin some cells to severe disarray in others with im-mediately adjacent myofibrils orientated perpen-dicular to each other. In addition, myofilaments thatoriginated from a single Z band sometimes crossed indifferent directions and were inserted into severaldifferent Z bands, resulting in a cross-weaving pattern.
Ferrans et al. noted that formation of new sar-comeres in the usual types of cardiac hypertrophy wasnot associated with the abnormal myofibrillar orienta-tion found in hypertrophic cardiomyopathy. A dis-ordered arrangement of myofibrils is, however,characteristic of embryonic cardiac muscle in whichmyofilaments in early developing myofibrils radiate inseveral directions from a single Z band. Furthermore,branching of myofibrils is found in primitive heartsand disorientation of myofibrils and cross-weaving ofmyofilaments are a feature of salamander hearts andalso of habdomyoma. Ferrans and his colleagues point
WITH OBSTRUCTION WITHOUT OBSTRUCTION
HY P ERTR O PH IC
C ONG E ST IV E
OBLITERATIVE
out that the myofibrillar arrangements in IHSSsuggest a less differentiated cell type than that nor-mally found in adult myocardium. They further quotethe work of Manasek6 who has suggested thatmyofibrillar alignment within specific regions of theheart is a result of response to the stresses induced bycontraction. Contraction induces lip ar stresses withinthe cell and myofibrillar alignment eventually coin-cides with these forces. Mechanical forces determinepatterns of orientation of other structures such asbones or tendons. Myofibrillar orientation thereforemight be assumed to be altered when mechanicallyoriented forces are abnormal, as in IHSS, or not fullydeveloped, as in embryonic hearts. The abnormalarchitecture of the myofibrils may prevent the normalalignment of muscle cells necessary for normaldevelopment and effective contraction. When themyofibrils are contracting at abnormal angles to othercells they may exert tension upon them, so while somecells shorten others may remain isometric or evenstretched. Presumably such a situation would be apowerful stimulus to hypertrophy and might also beimplicated in irregular contraction and difficulty inrelaxation. If the orderly alignment of cells laid downin the developing heart does not proceed in the usualway then irregular contraction may develop and thisin itself may predispose to further abnormal orienta-tion of the developing muscle fibers. Figure 2 shows asuggested sequence of events in the development ofhypertrophic cardiomyopathy based on my un-derstanding of the work of Ferrans and his colleagues.Once massive hypertrophy has developed, it may
be expected further to impair relaxation and reducethe rate of ventricular filling. Impaired rate of ven-tricular filling has already been demonstrated byStewart and his colleagues7 while Ziady, working inour laboratory, has shown that the isovolumic relaxa-tion time of the left ventricle is significantly longer
EMBRYONIC
RESTRICTIVE
Figure 1
Diagram of thefour principle types of cardiomyopathy.
Circulation. vIoluP?e 50. August 1974
RANDOM ALIGNMENT 0F MYOFIBRILS
t ~ - STRESSES OF CONTRACTION
ORDERLY ALIGNMENT
IN H.O.C.M. (IHSS: MYOFIBRILS
END - TO - SIDE JUNCTIONS
ABNORMAL ORIENTATION
ABNORMAL MECHANICAL fORCES
ABNORMAL ALIGNMENT
UNEVEN DEVELOPMENT OF TENSION
HYPERTROPHY
Figure 2
Suggested sequence of events in the development of hypertrophicobstructive cardiomyopathy (based on Ferrans et al., 1973).
211
by guest on June 30, 2018http://circ.ahajournals.org/
Dow
nloaded from
GOODWIN
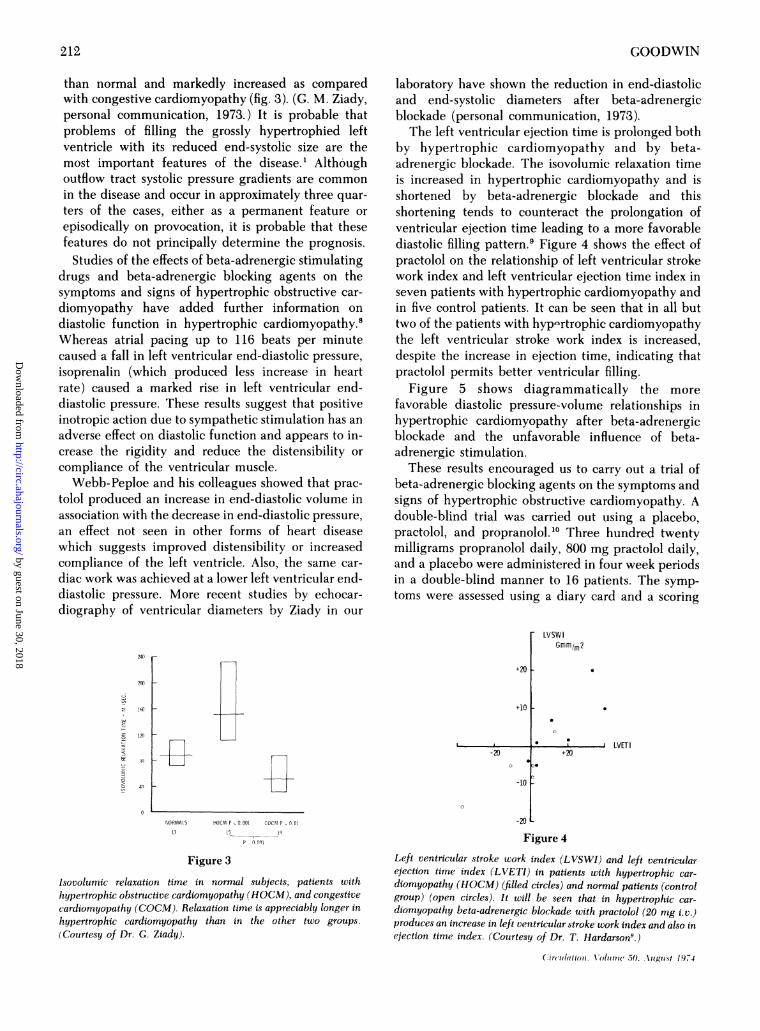
than normal and markedly increased as comparedwith congestive cardiomyopathy (fig. 3). (G. M. Ziady,personal communication, 1973.) It is probable thatproblems of filling the grossly hypertrophied leftventricle with its reduced end-systolic size are themost important features of the disease.' Althoughoutflow tract systolic pressure gradients are commonin the disease and occur in approximately three quar-ters of the cases, either as a permanent feature orepisodically on provocation, it is probable that thesefeatures do not principally determine the prognosis.Studies of the effects of beta-adrenergic stimulating
drugs and beta-adrenergic blocking agents on thesymptoms and signs of hypertrophic obstructive car-diomyopathy have added further information ondiastolic function in hypertrophic cardiomyopathy.8Whereas atrial pacing up to 116 beats per minutecaused a fall in left ventricular end-diastolic pressure,isoprenalin (which produced less increase in heartrate) caused a marked rise in left ventricular end-diastolic pressure. These results suggest that positiveinotropic action due to sympathetic stimulation has anadverse effect on diastolic function and appears to in-crease the rigidity and reduce the distensibility orcompliance of the ventricular muscle.Webb-Peploe and his colleagues showed that prac-
tolol produced an increase in end-diastolic volume inassociation with the decrease in end-diastolic pressure,an effect not seen in other forms of heart diseasewhich suggests improved distensibility or increasedcompliance of the left ventricle. Also, the same car-diac work was achieved at a lower left ventricular end-diastolic pressure. More recent studies by echocar-diography of ventricular diameters by Ziady in our
240 r-
2w
laboratory have shown the reduction in end-diastolicand end-systolic diameters after beta-adrenergicblockade (personal communication, 1973).The left ventricular ejection time is prolonged both
by hypertrophic cardiomyopathy and by beta-adrenergic blockade. The isovolumic relaxation timeis increased in hypertrophic cardiomyopathy and isshortened by beta-adrenergic blockade and thisshortening tends to counteract the prolongation ofventricular ejection time leading to a more favorablediastolic filling pattern.9 Figure 4 shows the effect ofpractolol on the relationship of left ventricular strokework index and left ventricular ejection time index inseven patients with hypertrophic cardiomyopathy andin five control patients. It can be seen that in all buttwo of the patients with hyp-rtrophic cardiomyopathythe left ventricular stroke work index is increased,despite the increase in ejection time, indicating thatpractolol permits better ventricular filling.
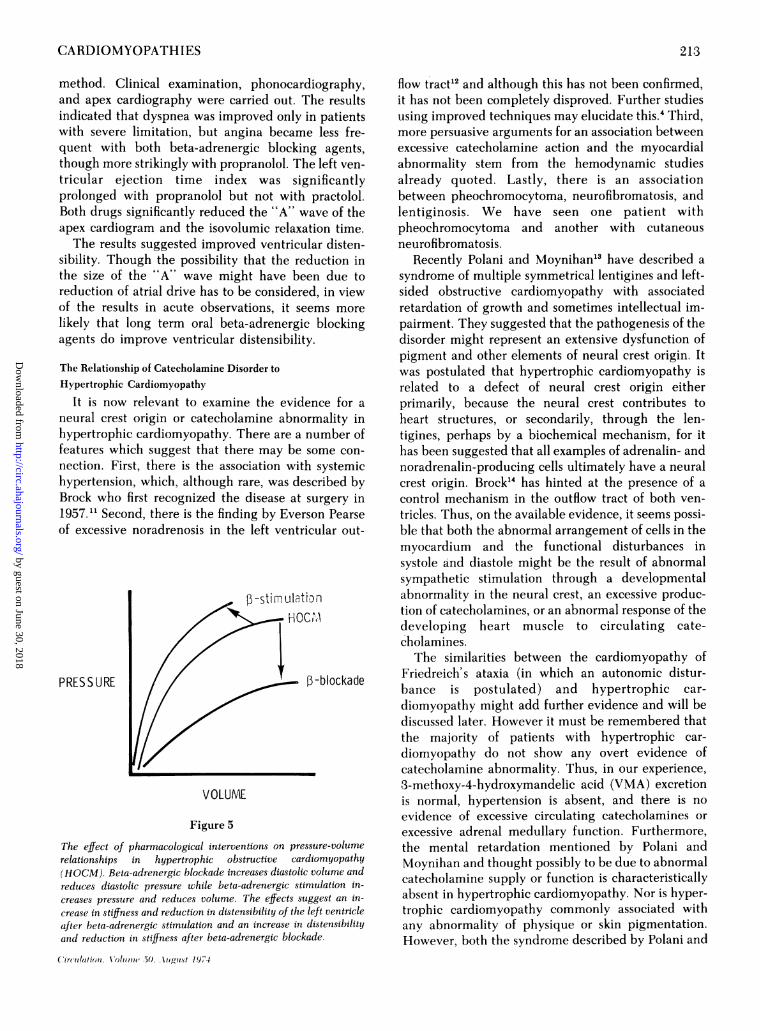
Figure 5 shows diagrammatically the morefavorable diastolic pressure-volume relationships inhypertrophic cardiomyopathy after beta-adrenergicblockade and the unfavorable influence of beta-adrenergic stimulation.
These results encouraged us to carry out a trial ofbeta-adrenergic blocking agents on the symptoms andsigns of hypertrophic obstructive cardiomyopathy. Adouble-blind trial was carried out using a placebo,practolol, and propranolol.'O Three hundred twentymilligrams propranolol daily, 800 mg practolol daily,and a placebo were administered in four week periodsin a double-blind manner to 16 patients. The symp-toms were assessed using a diary card and a scoring
-LVSWIGmmlm2
+20 -
+10 -
1;1
--20
,.
* 0. LVET+20
-10 [
0
NORMALS HOCM P 00,001 COCM P 1 1!01
13 15 1s
Figure 3
Isovolumic relaxation time in normal subjects, patients withhypertrophic obstructive cardiomyopathy (HOCM), and congestivecardiomyopathy (COCM). Relaxation time is appreciably longer inhypertrophic cardiomyopathy than in the other two groups.(Courtesy of Dr. G. Ziady).
20
Figure 4
Left ventricular stroke work index (LVSWI) and left ventricularejection time index (LVETI) in patients with hypertrophic car-diomyopathy (HOCM) (filled circles) and normal patients (controlgroup) (open circles). It will be seen that in hypertrophic car-diomyopathy beta-adrenergic blockade with practolol (20 mg i.v.)produces an increase in left ventricular stroke work index and also inejection time index. (Courtesy of Dr. T. Hardarson9.)
Cir(lulttilon Oluim .50. Xulgtisf 19,74
212
4n
-2
by guest on June 30, 2018http://circ.ahajournals.org/
Dow
nloaded from
CARDIOMYOPATHIES
method. Clinical examination, phonocarand apex cardiography were carried out.indicated that dyspnea was improved onlywith severe limitation, but angina becamquent with both beta-adrenergic blockiithough more strikingly with propranolol. Titricular ejection time index was si}prolonged with propranolol but not withBoth drugs significantly reduced the "A" vapex cardiogram and the isovolumic relax-The results suggested improved ventrict
sibility. Though the possibility that the rethe size of the "A" wave might have bereduction of atrial drive has to be considerof the results in acute observations, it selikely that long term oral beta-adrenergiiagents do improve ventricular distensibilit
The Relationship of Catecholamine Disorder toHypertrophic Cardiomyopathy
It is now relevant to examine the evidneural crest origin or catecholamine abnchypertrophic cardiomyopathy. There are afeatures which suggest that there may benection. First, there is the association withypertension, which, although rare, was deBrock who first recognized the disease at1957." Second, there is the finding by Everof excessive noradrenosis in the left ventr
3-stimulatHOI
PRESSURE
VOLUME
Figure 5
The effect of pharmacological interventions on prerelationships in hypertrophic obstructive car(HOCM). Beta-adrenergic blockade increases diastolireduces diastolic pressure while beta-adrenergic sticreases pressure and reduces volume. The effects Stcrease in stiffness and reduction in distensibility of theafter beta-adrenergic stimulation and an increase inand reduction in stiffness after beta-adrenergic blocA
diography, flow tract12 and although this has not been confirmed,The results it has not been completely disproved. Further studiesin patients using improved techniques may elucidate this.4 Third,ie less fre- more persuasive arguments for an association betweenng agents, excessive catecholamine action and the myocardialhe left ven- abnormality stem from the hemodynamic studiesgnificantly already quoted. Lastly, there is an associationpractolol. between pheochromocytoma, neurofibromatosis, and
vave of the lentiginosis. We have seen one patient withation time. pheochromocytoma and another with cutaneousAar disten- neurofibromatosis.duction in Recently Polani and Moynihan'3 have described a'en due to syndrome of multiple symmetrical lentigines and left-ed, in view sided obstructive cardiomyopathy with associatedeems more retardation of growth and sometimes intellectual im-c blocking pairment. They suggested that the pathogenesis of thety. disorder might represent an extensive dysfunction of
pigment and other elements of neural crest origin. Itwas postulated that hypertrophic cardiomyopathy isrelated to a defect of neural crest origin either
lence for a primarily, because the neural crest contributes to)rmality in heart structures, or secondarily, through the len-number of tigines, perhaps by a biochemical mechanism, for itsome con- has been suggested that all examples of adrenalin- and:h systemic noradrenalin-producing cells ultimately have a neural3scribed by crest origin. Brock'4 has hinted at the presence of asurgery in control mechanism in the outflow tract of both ven-rson Pearse tricles. Thus, on the available evidence, it seems possi-^icular out- ble that both the abnormal arrangement of cells in the
myocardium and the functional disturbances insystole and diastole might be the result of abnormalsympathetic stimulation through a developmental
to3n abnormality in the neural crest, an excessive produc-CM ltion of catecholamines, or an abnormal response of the
developing heart muscle to circulating cate-cholamines.The similarities between the cardiomyopathy of
P-blockade Friedreich's ataxia (in which an autonomic distur-bance is postulated) and hypertrophic car-diomyopathy might add further evidence and will bediscussed later. However it must be remembered thatthe majority of patients with hypertrophic car-diomyopathy do not show any overt evidence of
_ catecholamine abnormality. Thus, in our experience,3-methoxy-4-hydroxymandelic acid (VMA) excretionis normal, hypertension is absent, and there is noevidence of excessive circulating catecholamines orexcessive adrenal medullary function. Furthermore,
,ssure-volume the mental retardation mentioned by Polani andrdiomyopathy Moynihan and thought possibly to be due to abnormalc volume and catecholamine supply or function is characteristicallyimulation in- ctcoaleSpl rrnto SCaatrSlaluggest an in- absent in hypertrophic cardiomyopathy. Nor is hyper-
'left ventricle trophic cardiomyopathy commonly associated withdistensibility any abnormality of physique or skin pigmentation.kade. However, both the syndrome described by Polani and
(irculation. Volume .50. Agust 1.974
213
by guest on June 30, 2018http://circ.ahajournals.org/
Dow
nloaded from

GOODWIN
Moynihan and hypertrophic cardiomyopathy appearto be inherited on a similar genetic basis.
Further work is necessary on the catecholaminecontent of heart muscle in hypertrophic car-diomyopathy and into other aspects of the associationbetween catecholamine excess and the etiology of thedisease.
Does Secondary Hypertrophic Cardiomyopathy Existas an Entity?The first description by Brock of what we now
recognize as hypertrophic obstructive cardio-myopathy was related to a patient with severesystemic hypertension, and he regarded the muscularhypertrophy of the outflow tract of the left ventriclethat produced the obstruction as being secondary tothe hypertension." Since then, speculation that eitherexcessive afterload on the left ventricle or fixed out-flow tract obstruction might produce hypertrophiccardiomyopathy has been rife. The demonstration ofan inappropriate degree of hypertrophy with theclinical and hemodynamic characteristics of hyper-trophic cardiomyopathy in association with a milddegree of fixed outflow tract obstruction in the form ofvalvar aortic stenosis or discrete subvalvar aorticstenosis has been noted in three patients in our ex-perience. Apart from the association with fixed out-flow tract obstruction of the left ventricle or systemichypertension, hypertrophic obstructive cardio-myopathy has been described also in two other ap-parently unrelated conditions associated with severecardiac hypertrophy. These are Friedreich's ataxia15and Pompe's disease.16 Although massive ventricularhypertrophy involving the septum and papillarymuscles, with gross cardiomegaly is recognized inPompe's disease, the histology is typical of glycogenstorage disease with vacuolation of cardiac musclecells due to glycogen infiltration, giving a typical lat-tice work appearance, but no evidence of the typicalhistological and electron microscopic appearances ofhypertrophic cardiomyopathy.A number of descriptions of massive hypertrophy
and obstruction to ventricular outflow have beenreported in patients with Friedreich's ataxia who havecardiac involvement. Outflow tract gradients on bothsides of the heart are well recognized, and Thoren"5has commented on the frequency of systolic murmurs,which tend to disappear as patients become older andtherefore may not be recognized by cardiologists orneurologists dealing only with adult patients.Angiocardiographic studies'7 18 have shown appear-ances very similar to those found in hypertrophicobstructive cardiomyopathy. A large body ofpathological evidence is not available, but histologicalexamination of 16 hearts by Hewer'9 showed con-
siderable muscle hypertrophy with large and bizarremuscle fibers somewhat reminiscent of hypertrophicobstructive cardiomyopathy and often severe in-terstitial fibrosis. Evidence is so far not available onthe distribution and orientation of the muscle fibersand on electron microscope studies. A strikingdifference, however, was the severe though notwidespread narrowing of small coronary arteries,which was considered to be secondary to the cardiacmuscle disease rather than a primary condition. Thisdifference, together with the absence of any evidenceof similar neuromuscular disease in patients withhypertrophic cardiomyopathy, or of the developmentof neuromuscular disease with age in the same condi-tion, suggests that the two are probably separate dis-orders, in spite of interesting similarities. However, itis interesting to postulate a possible common factor inthe form of excessive sympathetic discharge or inap-propriate reaction of the heart muscle to normal sym-pathetic discharge.The Natural History of Hypertrophic Cardiomyopathy
The natural history of hypertrophic cardio-myopathy is, I believe, largely determined by thestiffness of the left ventricle and the filling problems,and the clinical course tends to be related mainly tothe level of the left ventricular end-diastolic pressure,particularly on effort. Most patients appear to havesome degree of obstruction to left ventricular outflowtract, either persistently or on provocation, at sometime during their lifetime, but there is no doubt thatothers in whom evidence of outflow tract obstructiondisappears may develop severe heart failure, oftenassociated with atrial fibrillation and embolism. Thiscourse of the disease however does not appear to occurin more than approximately 10% of patients.20Our original study of the natural history revealed
that most patients maintained a stable course, but thata minority of patients tended either progressively todeteriorate or to apparently improve symptomatically.Sudden death is a well recognized complication and inour experience appears to be slightly more probable inpatients with a particularly high left ventricular end-diastolic pressure and a short history of symptoms ofincreasing severity. Studies by my colleague Dr.Oakley in our patients have suggested that theprognosis may be particularly unfavorable in childrenin whom there may be widespread disease and exten-sive generalized hypertrophy. Our study by Swannand others20 showed that symptoms and theirdeterioration were related to the level of left ven-tricular end-diastolic pressure, as might be expected.There was no relationship between either severity ofsymptoms or tendency to deterioration and the leftventricular systolic gradient, suggesting that this is a
Circulation. Volume 50. AXug2tst 1 974
214
by guest on June 30, 2018http://circ.ahajournals.org/
Dow
nloaded from
CARDIOMYOPATHIES
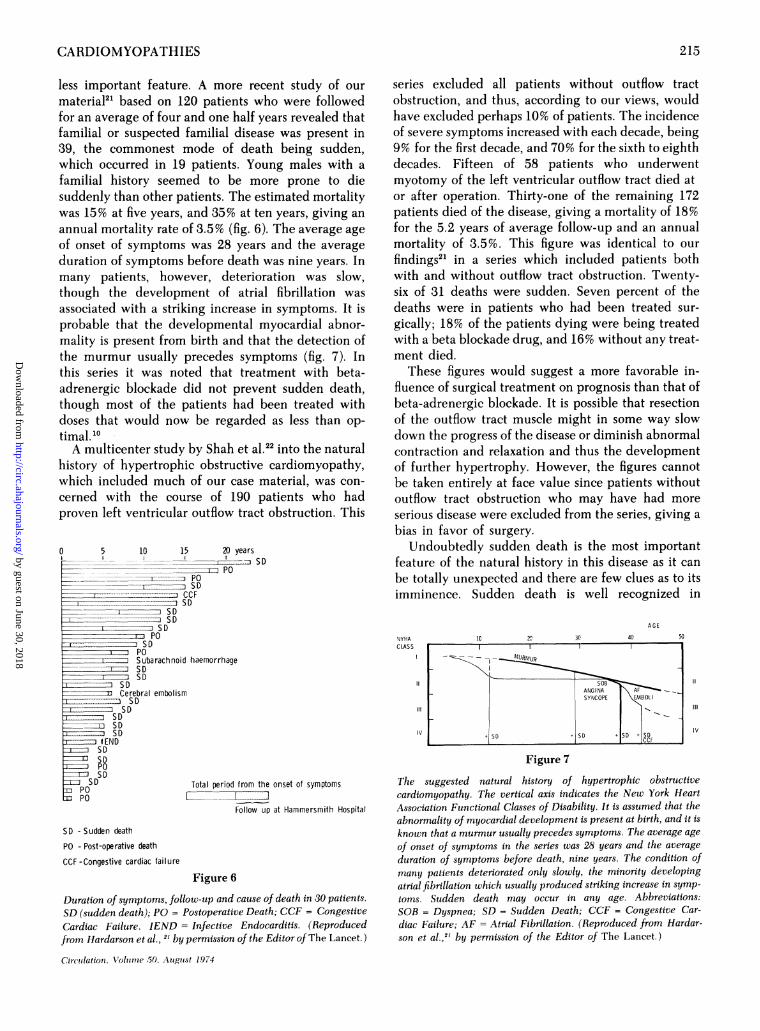
less important feature. A more recent study of ourmaterial2' based on 120 patients who were followedfor an average of four and one half years revealed thatfamilial or suspected familial disease was present in39, the commonest mode of death being sudden,which occurred in 19 patients. Young males with afamilial history seemed to be more prone to diesuddenly than other patients. The estimated mortalitywas 15% at five years, and 35% at ten years, giving anannual mortality rate of 3.5% (fig. 6). The average ageof onset of symptoms was 28 years and the averageduration of symptoms before death was nine years. Inmany patients, however, deterioration was slow,though the development of atrial fibrillation wasassociated with a striking increase in symptoms. It isprobable that the developmental myocardial abnor-mality is present from birth and that the detection ofthe murmur usually precedes symptoms (fig. 7). Inthis series it was noted that treatment with beta-adrenergic blockade did not prevent sudden death,though most of the patients had been treated withdoses that would now be regarded as less than op-timal.'0A multicenter study by Shah et al.22 into the natural
history of hypertrophic obstructive cardiomyopathy,which included much of our case material, was con-cerned with the course of 190 patients who hadproven left ventricular outflow tract obstruction. This
5 10 15 20 yearsxI-zzs SD
.. ._ ~~PO_ PO
'_LZIEI Z SDCCF
- SD
SDSD
SPOPOSD
POSubarachnoid haemorrhageSDSD
SDCerebral embolismSD
SDSDSDSD
lENDSDSDPDSD
SD Total period from the
POFollow up
series excluded all patients without outflow tractobstruction, and thus, according to our views, wouldhave excluded perhaps 10% of patients. The incidenceof severe symptoms increased with each decade, being9% for the first decade, and 70% for the sixth to eighthdecades. Fifteen of 58 patients who underwentmyotomy of the left ventricular outflow tract died ator after operation. Thirty-one of the remaining 172patients died of the disease, giving a mortality of 18%for the 5.2 years of average follow-up and an annualmortality of 3.5%. This figure was identical to ourfindings2` in a series which included patients bothwith and without outflow tract obstruction. Twenty-six of 31 deaths were sudden. Seven percent of thedeaths were in patients who had been treated sur-gically; 18% of the patients dying were being treatedwith a beta blockade drug, and 16% without any treat-ment died.
These figures would suggest a more favorable in-fluence of surgical treatment on prognosis than that ofbeta-adrenergic blockade. It is possible that resectionof the outflow tract muscle might in some way slowdown the progress of the disease or diminish abnormalcontraction and relaxation and thus the developmentof further hypertrophy. However, the figures cannotbe taken entirely at face value since patients withoutoutflow tract obstruction who may have had moreserious disease were excluded from the series, giving abias in favor of surgery.
Undoubtedly sudden death is the most importantfeature of the natural history in this disease as it canbe totally unexpected and there are few clues as to itsimminence. Sudden death is well recognized in
NYHACLASS
11
IVl
!onset of symptoms
)at Hammersmith Hospital
SD -Sudden death
PO - Post-operative death
CCF -Congestive cardiac failure
Figure 6
Duration of symptoms, follow-up and cause of death in 30 patients.
SD (sudden death); PO = Postoperative Death; CCF = CongestiveCardiac Failure. IEND = Infective Endocarditis. (Reproducedfrom Hardarson et al., 2 by permission of the Editor of The Lancet.)
Circulation. Voltunie 50. Auigutst 1974
AGE
IC Y2 3Q 40 51
ANGINA AFSYNCOPE EMBOLI
SD + SD + SD + SDCCF
Figure 7
11
Illi
Iv
The suggested natural history of hypertrophic obstructivecardiomyopathy. The vertical axis indicates the New York HeartAssociation Functional Classes of Disability. It is assumed that theabnormality of myocardial development is present at birth, and it is
known that a murmur usually precedes symptoms. The average ageof onset of symptoms in the series was 28 years and the averageduration of symptoms before death, nine years. The condition ofmany patients deteriorated only slowly, the minority developingatrial fibrillation which usually produced striking increase in symp-toms. Sudden death may occur in any age. Abbreviations:SOB = Dyspnea; SD = Sudden Death; CCF = Congestive Car-diac Failure; AF = Atrial Fibrillation. (Reproduced from Hardar-son et al.,2' by permission of the Editor of The Lancet.)
215
0 by guest on June 30, 2018http://circ.ahajournals.org/
Dow
nloaded from

GOODWIN
children with the disease. Death in 17% of 102children who died suddenly was due to nonobstruc-tive or obstructive cardiomyopathy (E. Lambert, per-sonal communication, 1973).
Progressive Loss of Outflow Tract Obstruction
The progressive disappearance of outflow tractobstruction appears to be associated with progressiveadvance of the disease. Thus the loss of the outflowtract obstructive murmur has been associated in ourexperience with progressive dyspnea and the develop-ment of heart failure.' It appears likely that in theearlier stages of the disease, and throughout thelifetime of many patients, systolic function of the leftventricle remains good though ill-coordinated.Damage to left ventricular muscle, by reducing con-tractile power, diminishes the force of left ventricularcontraction and thus reduces the outflow tractobstruction. This was well documented in a patientwhom I treated in whom the signs of outflow tractobstruction disappeared completely following a largeantero-septal infarct produced by dissection of the leftanterior descending coronary artery. In addition tothe loss of signs of outflow tract obstruction, anginadisappeared and the echocardiogram no longershowed the appearances of outflow tract obstruction.
In a recent report23 myocardium obtained at opera-tion or necropsy from 20 patients (11 with obstructiveand nine with nonobstructive disease) was studied bylight and electron microscopy. All the musclespecimens showed the characteristic greatly hyper-trophied, bizarrely-shaped, and abnormally orientedcardiac muscle cells in the septum. In patients whohad obstruction these abnormalities were either ab-sent or only rarely found in tissue from the left ven-tricular apex, posterior wall, or right ventricle. By con-trast, many areas of abnormal cells were present inboth the left ventricular free wall and right ventriclein seven of the nine patients without obstruction whowere symptomatic. The authors concluded that thecharacteristic cellular abnormalities are always pres-ent in the septum but that the more extensive involve-ment of the free walls of ventricles is limited topatients without obstruction. These findings wouldcertainly harmonize with our views that widespreaddisease with a poor prognosis may be found in theabsence of any obstructive element. It seems likelythat the pattern of the disease is determined largely bythe extent, distribution, and progression of the specificmyocardial lesions.
Progressive deterioration leading to heart failure iscaused by a number of factors: notably, the reducedleft ventricular filling time and increased left ven-tricular filling resistance, and tachycardia, whichlimits filling time, causes further increase in left ven-
tricular end-diastolic pressure and may thusprecipitate heart failure. The development of atrialfibrillation, with consequent loss of atrial drive,together with increasing hypertrophy and extension ofthe disease, completes the picture of deteriorationleading to death in heart failure. It is likely also thatthese factors contribute to, or may be the cause ofsudden death when sudden limitation of fillingcapacity causes a precipitous fall in cardiac output andcoronary blood flow with consequent ventricularfibrillation.
Prospects and Predictions for Hypertrophic Cardiomyopathy
In the light of the known factors and numerousspeculations, it is now appropriate to attempt topredict the paths of investigation that would bedesirable for the further elucidation of this diseaseover the coming years.
First, a follow-up study of patients' relatives todetermine the incidence of the disease and its patternsof progression would clearly be of great value. An in-crease in the ratio of thickness of ventricular septumto posterior wall in patients with hypertrophic car-diomyopathy has been demonstrated in a limitednumber of patients.24 If this initial study proves tohave validity in larger numbers, then serial echocar-diographic examinations would provide a useful,harmless, and subtle way of diagnosing presymp-tomatic stages of the disease and following itsdevelopment in individual patients.
Second, serial examination of patients by nonin-vasive techniques such as echocardiography will beneeded to determine the effect of long term beta-adrenergic blockade on the incidence of suddendeath. The persuasive evidence obtained by acuteobservations and the theoretical considerations in-volved suggest a beneficial role for beta-adrenergicblockade and indicated that further evaluation of theplace of long-term, high dosage regimes is needed.
Third, efforts should be directed to a study of thecatecholamine content of the specific lesions in themyocardium in hypertrophic cardiomyopathy usingnew and refined techniques of fluorescent staining.Attempts should be made to determine whether con-ditions such as Pompe's disease and Friedreich's atax-ia that produce clinical hemodynamic and gross mor-bid anatomical appearances similar to hypertrophiccardiomyopathy also show the characteristic myocar-dial ultrastructural lesions. Further studies ofcatecholamine function and production in conditionsin which abnormality of catecholamine metabolism orresponse may be a common factor are needed.
Finally it should be possible to attempt to create anexperimental model of the disease by determining theeffect of abnormal orientations of developing cardiac
Circulation. Voltinie 50. August 1974
216
by guest on June 30, 2018http://circ.ahajournals.org/
Dow
nloaded from

CARDIOMYOPATHIES
muscle cells grown on tissue culture.In my view it is unlikely that much further study of
the exact dynamics of outflow tract obstruction andmitral regurgitation will yield significant additionalbasic information regarding the disease. Thehemodynamics, clinical features, and prognosis havealready been reasonably accurately delineated.Knowledge of the cause of the disease, its relationshipto other cardiac and noncardiac conditions, and aneffective method of treatment are urgently needed.
Congestive CardiomyopathyI turn now to the enigma of congestive car-
diomyopathy. This is a multifaceted syndromecharacterized by isolated cardiomegaly with dilatedventricles, heart failure, and more extensive hyper-trophy than would be expected from the degree ofdilatation. It is likely that there are many causes andthe definition covers not a single disease but a syn-drome that is a final common path of many differingconditions that insult the ventricular myocardium.
Insults that deserve particular study are those ofalcohol, pregnancy and the puerperium, systemichypertension, and infections, probably of viral nature.These four phenomena may be regarded as "risk fac-tors" if not actual causes, for it is probable that inmany instances it is the combination of more than onefactor that produces the devastating damage to themyocardium.
It is true that other myocardial diseases can producethe clinical and pathological final common pathknown as congestive cardiomyopathy. These areconditions such as endocardial fibroelastosis, Chagas'disease, and many infiltrative diseases of the myo-cardium or granulomatous disorders. There are alsoconnective tissue disorders such as diffuse systemicsclerosis that may involve the myocardium.
I shall not consider alcohol further as it is wellknown that excessive amounts can produce a syn-drome of severe congestive heart failure which is notinfrequently fatal and which tends to improve whenalcohol is discontinued and to recur when drinking isrecommenced. It is likely, however, that some factorother than ingestion of alcohol is implicated since notevery subject who takes large quantities of alcoholdevelops alcoholic cardiomyopathy. Probably in-dividual differences and susceptibilities, and perhapsthe presence of other risk factors, are important.
It has been suggested that systemic hypertensionmay be an important cause of congestive car-diomyopathy. The initial high systemic blood pressureand cardiac output may be succeeded by reduction inthe cardiac output as a result of theligh peripheralvascular resistance and resultant left ventricularsystolic afterload.25 It is true that hypertension andCirctulation, Volutme 50, Atuguzst 1974
cardiomyopathy may coexist in the same population,and Brockington and Eddington25 have argued per-suasively that congestive cardiomyopathy might bethe result of an unusual response of the left ventricleto the persistent afterload. While hypertension maywell be a factor in some patients, or even a cause in afew, it seems improbable that it is a major factor in themajority since incidence of hypertension is uncom-mon and in our experience occurred in only ap-proximately 25% of our patients, and in a number ofthese was probably a reaction to the severe heartfailure.'One of the outstanding problems of the present
time is the possible connection between infectivemyocarditis produced by viruses on the one hand andestablished congestive cardiomyopathy on the other.There is remarkably little data on the transition fromacute myocarditis to chronic congestive car-diomyopathy and almost no evidence to implicate avirus infection in patients with established congestivecardiomyopathy. Nevertheless, such evidence as thereis may be important. Somerville26 described the transi-tion from an acute pyrexial illness with involvement ofthe myocardium to a chronic state of heart failure con-sistent with congestive cardiomyopathy in threepatients. Bengtsson27 described the presence of car-diac abnormalities in 30% of 200 patients five yearsafter acute myocarditis. Obeyesekere and Herman28described the development of congestive car-diomyopathy after arborvirus infection in Ceylon inten patients. So far there is minimal direct evidence ofthe presence of viruses or the hallmarks of virusmyocardial disease in patients with congestive car-diomyopathy, but Kawai29 demonstrated an increasedincidence of complement-fixing antibodies to variousviruses, including poliomyelitis, coxsackie-B, and in-fluenza, in heart muscle cells of patients withidiopathic cardiomyopathy, as compared with con-trols. He also demonstrated positive fluorescence foradeno-virus antigen in the nuclei of myocardial cellsfrom a biopsy from right ventricular myocardium inpatients with cardiomyopathy.
Immunoglobulin-binding in the heart muscle cellsof patients with congestive cardiomyopathy has beendescribed30 but this is not necessarily of etiologicalsignificance and might be the result of an infectiveprocess. The fact that viruses have not so far been im-plicated directly in the causation of congestive car-diomyopathy in no way denies this possibility, andwith better methods of virus detection and improvingtechniques of cardiac biopsy, it should be possible toanswer this important question which assumes evengreater relevance now that we are on the threshold ofdevelopment of antiviral chemotherapy.
I have long been intrigued by the excess of dilata-
217
by guest on June 30, 2018http://circ.ahajournals.org/
Dow
nloaded from

GOODWIN
tion over hypertrophy in congestive cardiomyopathyand have wondered if in some way the normalmechanisms in hypertrophy that compensate formyocardial weakness have been frustrated in con-gestive cardiomyopathy. The dilatation of the leftventricle is diffuse, symmetrical, and akinetic, andthus differs strikingly from the dyskinetic ventricularpattern so commonly seen in occlusive coronary arterydisease. This difference harmonizes with the absenceof significant coronary artery disease in patients withcongestive cardiomyopathy.3' It is possible that theagents that damage the myocardium interfere withcontractile function by preventing calcium-bindingby troponin and that the deficient contractile functionthat follows results in ventricular dilatation, increasedwall tension, and failure of the RNA-DNA responsethat is needed to produce hypertrophy. This is sheerspeculation, but our studies of the relation of hyper-trophy to prognosis in congestive cardiomyopathysuggest that patients with the most hypertrophyappear to have the best prognosis.' Long-term sur-vival was unusual when the end-diastolic volume roseto over two and a quarter times the maximum normalor when the ejection fraction was less than 10%, com-pared to over 60% of the control value.32The failure to discover any characteristic features
on ultrastructural studies or the myocardium in con-gestive cardiomyopathy suggests that the appearancesmay represent little more than a graveyard of deadtissue without revealing the cause of death and thatultrastructure studies are of only limited value. Theinvestigation of the tombstones in a graveyard,however detailed, will not yield clues to the cause ofdeath of the bodies beneath.
It therefore becomes necessary to look beyond theboundaries of structure and ultrastructure to the finerprocesses of myocardial chemistry and cellularbiology. Studies of subcellular organelle enzymes andthe functions of lysosomes, which, on being damaged,rupture and release enzymes that may digest cells,have been started at the Royal Postgraduate MedicalSchool by my colleagues C. M. Oakley and T. Peters.
Prospects and Predictions for Congestive CardiomyopathyThe problems are in many ways much greater than
for hypertrophic cardiomyopathy because we are notdealing with a discrete disease entity but a multifac-torial syndrome producing a final common pathtoward irreversible myocardial damage. The mostfruitful approach is likely to come from improvedtechniques of cardiac biopsy that permit safe andrepeated studies of myocardial function to be made,and from improved studies of cellular biology with ex-amination of enzyme systems and search for virusesand their products.
It should be possible to create an animal model thatsatisfies the hemodynamic and clinical characteristicsof congestive cardiomyopathy by the administrationof such infective or toxic agents that might possibly becausally related in man.
Accurate long-term follow-up studies of cases ofknown acute myocarditis to detect chronic cardiacdamage are essential.
Epidemiological studies of congestive car-diomyopathy should be undertaken to determinewhether other factors, as yet unsuspected, may be in-volved. General agreement on the diagnostic criteriafor congestive cardiomyopathy is vital and mul-ticenter studies could be of great value, provided uni-formity of case material and rigid criteria of diagnosisare insisted upon. Here the Scientific Council on Car-diomyopathies of the International Society of Car-diology might be of crucial importance.
At the present time the prognosis for severe con-gestive cardiomyopathy is so bleak and treatment sounsatisfactory that cardiac transplantation may beconsidered in desperate cases.
Conclusions
I have not attempted to be comprehensive and tocover all aspects of the cardiomyopathies. Rather, Ihave selected those aspects and features that I believeto be of major import and that require further study inthe future and I have not hesitated to be provocativewith hypothesis. As in so many areas of medicine, thestudy of the cardiomyopathies requires the integratedefforts of research workers in many disciplines -clinical, pathological, biochemical, virological, im-munological, epidemiological, and possibly others notas yet considered. The intellectual challenge andstimulation provided by this fascinating and tauntinggroup of diseases may be blunted by the emotionalfrustration arising from the unfortunate prognosis andthe limitations of treatment. But nevertheless weshould never lose our scientific curiosity, which hasbeen compared to "that direct incontinence of thespirit which has a pleasure in it like wrestling with afine woman.
AcknowledgmentI am deeply sensible of the honor done to me by the American
Heart Association in having asked me to deliver the lecture uponwhich this paper is based.
It is a pleasure to acknowledge the work, originality, andstimulating ideas of many colleagues on both sides of the Atlanticand I am profoundly grateful for the help that they have given me.
References
1. GOODWIN JF: The Congestive and HypertrophicCardiomyopathies - A decade of study. Lancet 1: 733, 1970
2. TEARE RD: Asymmetrical Hypertrophy of the Heart in YoungAdults. Br Heart J 20: 1, 1958
Circulation, X*'0iolume 50. Aiigust 1974
218
by guest on June 30, 2018http://circ.ahajournals.org/
Dow
nloaded from
CARDIOMYOPATHIES
3. BRoCKINGTON IF, OLSEN EGJ: Ldeffler's Endocarditis andDavis Endomyocardial Fibrosis. Am Heart J 85: 308, 1973
4. VAN NOORDEN S, OLSEN EGJ, PEARSE AGE: HypertrophicObstructive Cardiomyopathy. A histological, histochemicaland ultrastructural study of biopsy material. Cardiovasc Res5: 118, 1971
5. FERRANS DJ, MORROw AG, ROBERTS WC: Myocardialultrastructure in idiopathic hypertrophic subaortic stenosis.Circulation 45: 769, 1972
6. MANASEK FG: Histogenesis of the embryonic myocardium. AmJ Cardiol 25: 149, 1970
7, STEWART S, MASON DT, BRAUNWALD E: Impaired rate of leftventricular filling in idiopathic hypertrophic subaorticstenosis and valvular aortic stenosis. Circulation 37: 8, 1963
8. WERR-PEPLOE MM: Management of hypertrophic obstructivecardiomyopathy by beta blockade. In HypertrophicObstructive Cardiomyopathy, Ciba Foundation StudyGroup No. 37, edited by WOLSTENHOLME GEW, O'CONNORM. London, Churchill, 1971, p 103
9. HARDARSON T: Systolic time intervals in ischaemic heartdisease, congestive cardiomyopathy and hypertrophicobstructive cardiomyopathy. Ph.D. Thesis, University ofLondon, 1974
10. HUBNER PJB, ZIADY GM, LANE GK, HARDARSON T, SCHALES B,OAKLEY CM, GOODWIN JF: Double-blind trial of Propranololand Practolol in Hypertrophic Cardiomyopathy. Br Heart J35: 1116, 1973
11. BROCK RC: Hypertrophic obstruction of the left ventricularoutflow: clinical recognition of the condition. In Car-diomyopathies, Ciba Foundation Symposium, edited byWOLSTENHOLME GEW, O'CONNOR M. London, Churchill,1964, p 4
12. PEARSE AGE: The histochemistry and electron microscopy ofObstructive Cardiomyopathy. In Ciba Foundation Sym-posium on Cardiomyopathies, edited by WOLSTENHOLMEGEW, O'CONNOR M. London, Churchill, p 132
13. POLANI PE, MOYNIHAN EJ: Progressive cardiomyopathiclentiginosis. Q J Med 41: 205, 1972
14. BROCK RC: Functional Obstruction of the Left Ventricle(Acquired by sub-valvar stenosis). Guys Hosp Rep. 106: 22,1957
15. THOREN C: Cardiomyopathy in Friedreich's Ataxia with studiesof cardiovascular and respiratory function. Acta PaediatrScand 53 (suppl): 153, 1964
16. EHLERS KH, HOGSTROM JWC, LUKAS DS, REDO SF, ENGLE MA:Glycogen storage disease of the myocardium with obstruc-tion to left ventricular outflow. Circulation 25: 96, 1962
17. GACH JV, ANDRIANJ M, FRANK D: Hypertrophic Obstructive
Cardiomyopathy in Friedreich's Ataxia. Am J Cardiol 27:436, 1971
18. RUSHHAUPT DG, SELENIUS OG, CASSELS DE: Friedreich'sAtaxia associated with Idiopathic Subaortic Stenosis. AmHeart J 84: 95, 1972
19. HEWER RL: The heart in Friedreich's Ataxia. Br Heart J 31: 5,1969
20. SWAN DA, BELL B, OAKLEY CM, GOODWIN JF: Analysis of thesymptomatic course and treatment of HypertrophicObstructive Cardiomyopathy. Br Heart J 33: 671, 1971
21. HARDARSON T, DE LA CALZADA CS, CURIEL R, GOODWIN JF:Prognosis and mortality of Hypertrophic Obstructive Car-diomyopathy. Lancet 2: 1462, 1973
22. SHAH PM, ADELMAN AG, WIGLE ED, GOBEL FL, BURCHELL HB,HARDARSON T, CURIEL R, DE LA CALZADA C, OAKLEY CM,GOODWIN JF, Yu PN: The natural and unnatural history ofHypertrophic Obstructive Cardiomyopathy. Circulation 48(suppl IV): IV-5, 1973
23. MARON BJ, FERRANS VJ, HENRY WL, CLARK CE, ROBERTS WC,EPSTEIN SE: Differences in distribution of myocardialcellular abnormalities in asymmetric septal hypertrophy.Circulation 48 (suppl IV): IV-6, 1973
24. HENRY WL, CLARK CE, EPSTEIN SE: Asymmetric septalhypertrophy. Echocardiographic identification of thepathonomonic anatomic abnormality of idiopathic hyper-trophic subaortic stenosis. Circulation 47: 225, 1973
25. BROCKINGTON IF, EDDINGTON GM: Adult heart disease inWestern Nigeria. A clinical pathological synopsis. Am HeartJ 83: 27, 1972
26. SOMERVILLE W: Postcarditic myocardiopathy. In Seminar onCardiomyopathies, edited by SHAPER AG. Postgrad Med J48: 246, 1972
27. BENCTSSON E: Myocarditis and cardiomyopathy. ClinicalAspects. In Introduction to the Cardiomyopathies, edited bySHAPER AG. Cardiologia 52: 108, 1968
28. OBEYESEKERE I, HERMAN Y: Myocarditis after arborvirusinfection. Dengue and Chickengunha fever. Br Heart J 34:821, 1972
29. KAWAI C: Idiopathic Cardiomyopathy. A study on theinfectious immune theory as a cause of the disease. Jap Circ J35: 765, 1971
30. DAS SK, CALLEN JP, DODSON VM, CASSIDY JT: Immunoglobulinbinding in cardiomyopathic hearts. Circulation 44: 612, 1971
31. GAU GT, GOODWIN JF, OAKLEY CM, OLSEN EGJ, RAHIMTOOLASH, RAPHAEL MJ, STEINER RE: Q-waves in coronaryarteriography in cardiomyopathy. Br Heart J 34: 1034, 1972
32. OAKLEY C: Ventricular Hypertrophy in Cardiomyopathy. BrHeart J 33 (suppl): 179, 1971
Circulation, Volune .50. August 1974
219
by guest on June 30, 2018http://circ.ahajournals.org/
Dow
nloaded from
J. F. GOODWINProspects and Predictions for the Cardiomyopathies
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1974 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.50.2.210
1974;50:210-219Circulation.
http://circ.ahajournals.org/content/50/2/210.citationthe World Wide Web at:
The online version of this article, along with updated information and services, is located on
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document.
Permissions and Rights Question and Answer Further information about this process is available in therequested is located, click Request Permissions in the middle column of the Web page under Services.the Editorial Office. Once the online version of the published article for which permission is being
can be obtained via RightsLink, a service of the Copyright Clearance Center, notCirculationpublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on June 30, 2018http://circ.ahajournals.org/
Dow
nloaded from