Embed Size (px)
Citation preview

BJUIB J U I N T E R N A T I O N A L
© 2 0 1 2 T H E A U T H O R S
B J U I N T E R N A T I O N A L © 2 0 1 2 B J U I N T E R N A T I O N A L | doi:10.1111/j.1464-410X.2012.11087.x 1
What ’ s known on the subject? and What does the study add? Conventional sonography is the standard imaging technique used in patients with acute renal colic. A decreasing hydronephrosis index (HI) is associated with an increase in obstructive uropathy. Obstructive uropathy leads to an increase in the renal resistive index (RRI).
The present study shows that both the RRI and HI methods are easily practicable in patients presenting with stone-related renal colic. The grade of hydronephrosis correlates positively with the HI but not with the RI.
OBJECTIVE
• To confi rm the reliability of assessements of the renal resistive index (RRI) and the hydronephrosis index (HI) comprising two sonographic techniques providing additional information in patients with acute renal colic.
PATIENTS AND METHODS
• Sonographic measurement of hydronephrosis and assessment of common clinical criteria was performed in 22 consecutive patients presenting with unilateral stone-related renal colic. RRI and HI were separately recorded by two investigators within a prospective study. • Interobserver agreement and comparison of sonographic with computed tomography (CT) fi ndings were assessed with the Cohen ’ s kappa statistic ( κ ) for attributive ordinal characteristics and Spearman ’ s rank correlation/rho ( ρ ) for attributive metric characteristics.
RESULTS
• There was a signifi cant correlation between HI and the sonographically-evaluated grade of hydronephrosis, although not between RRI and the grade of hydronephrosis. • For all procedures (RRI, HI, sonography and CT), signifi cant differences between the symptomatic and the asymptomatic kidney were assessed. • Interobserver agreement was excellent for the grade assessment of hydronephrosis by conventional sonography ( κ = 0.82; P < 0.001), good to very good for HI ( ρ = 0.60; P = 0.003) and acceptable to good for RRI ( ρ = 0.49; P = 0.021).
CONCLUSIONS
• The RRI and HI methods are both easily practicable as stageless examination methods in patients presenting with stone-related renal colic, and both also reliably distinguish between obstruction and non-obstruction. • Exact thresholds for both methods must still be defi ned based on further successive studies. • Additionally, changes of values under medical expulsive therapy and correlation with the functional status of the obstructed kidney remain to be examined.
KEYWORDS
acute hydronephrosis , acute renal colic , hydronephrosis index , interobserver variability , renal resistive index , urolithiasis
Study Type – Diagnosis (reliability) Level of Evidence 2b
Prospective evaluation of interobserver variability of the hydronephrosis index and the renal resistive index as sonographic examination methods for the evaluation of acute hydronephrosis Oleg Rud * , Johannes Moersler † , Julia Peter * , Przemyslaw Waliszewski * ‡ , Christian Gilfrich * , Hannes H ä user † , Maximilian Burger § , Hans-Martin Fritsche § , Wolf F. Wieland § , Ali M. Ahmed * , Sabine Brookman-May § and Matthias May * * Department of Urology and † Institute of Radiology, St Elisabeth-Hospital, Straubing , ‡ Department of Urology, Philipps-University Marburg, Marburg , and § Department of Urology, Caritas-Hospital St Josef, University Regensburg, Regensburg, Germany Accepted for publication 10 November 2011

R U D E T A L .
© 2 0 1 2 T H E A U T H O R S
2 B J U I N T E R N A T I O N A L © 2 0 1 2 B J U I N T E R N A T I O N A L
INTRODUCTION
Assessments of the renal resistive index (RRI) and the hydronephrosis index (HI) comprise two sonographic techniques that can generate useful additional information in patients with acute renal colic in both a primary care setting and during the course of medical expulsive therapy (MET). The RRI represents the reduction in diastolic blood fl ow speed in relation to systolic fl ow speed and can be measured, for example, in the Arteriae arcuatae during an obstruction of the pelvicaliceal system [ 1 – 23 ] . The HI represents the relationship between the entire area of the kidney to the area of the pelvicaliceal system, with increasing obstruction resulting in a reduced HI value [ 24,25 ] .
For a new examination method to become established medical practice, it has to primarily fulfi l two criteria, First, the technique should display and correlate with a clinically relevant endpoint. The detection of an increase in any obstruction or a worsening in kidney function are clinically relevant criteria in cases of stone-related renal colic. Second, the technique must exhibit a high level of reproducibility. This in turn requires studies that can prove good intra-observer agreement (i.e. one investigator observes the same measurements at different points in time), good interobserver agreement (i.e. different investigators observe the same measurements congruently) and good equipment agreement (i.e. one or more investigators observe the same measurements using different examination equipment). The RRI and HI are two diagnostic techniques with high potential. Until now, they have taken no place in the routine evaluation of patients with acute renal colic. Investigations into the value of these techniques in the diagnosis of acute renal colic have previously only given contradictory results for the RRI [ 1 – 23 ] and remain totally absent for the HI. Studies on the reproducibility of both examination methods in this indication have equally not yet been published.
The present prospective study aimed to compare RRI, HI, sonography and native helical CT in the initial diagnostic of acute stone-related renal colic and to investigate the interobsever agreement of the sonography-based techniques.
PATIENTS AND METHODS
The prospective study design, approved by the local ethics committee, was based on the data obtained from all consecutive patients with acute renal colic during the period from January to May 2010 at St Elisabeth-Hospital in Straubing, Germany. Patients were examined ≤ 48 h within the onset of colic pain. Exclusion criteria were the absence of stones in the helical native CT; the presence of only one kidney; evidence of renal co-pathology (known renovascular and/or renoparenchymal diseases, amongst others) ; the unavailability of one of the predetermined observers (two urologists with renosonographic experience, see below); and patient age < 18 years. A run-in phase was conducted before the study, with fi ve patients not being included in the analysis. During this time, both investigators (O.R. and P.W.) agreed on standardized measuring conditions in conjunction with a DEGUM (German Society of Ultrasound in Medicine) certifi ed urologist who was experienced with colour-coded duplex Doppler sonography (M.M.).
Standardized examinations were conducted according to the above listed inclusion and exclusion criteria. To provide comparable conditions for sonography and to render colour-coded duplex Doppler sonography reliably interpretable in the fi rst place, patients had to be low pain (or pain-free). This was normally achieved through the use of metamizole (in a few cases with low-potency opiates). A sonographic examination was conducted once by each investigator within a maximum of 12 min after examination before the other one, and with neither knowing the results of the other ’ s examination. Both investigators then subsequently reached a consensus on the conventional sonographic grade of hydronephrosis. A colour-duplex capable sonographic device with integrated pulse-wave-doppler (Pro Fokus 2202; B-K Medical, Herlev, Denmark) with a 3.5-MHz convex head was used for all scans. A native helical CT scan was performed either immediately before or directly after the examination. CT scans were performed using a 64-line multidetector scanner (Brilliance, Phillips, Eindhoven, the Netherlands). Alongside general patient criteria (age, gender, height, weight, body mass index, fi rst or recurring stone, creatinine serum
value, side of renal colic) the CT gave both stone localization and stone size.
Conventional sonographic and CT graduation of hydronephrosis was conducted separately according to colic side and contralateral kidney using a fi ve-point classifi cation based on the criteria of the Society for Foetal Urology: grade 0 = no hydronephrosis; grade 1 = isolated distension of the renal pelvis; grade 2 = clear distension of renal pelvis with calyx neck recognizable; grade 3 = massive renal pelvic distension with ectasia of neck of the calyx without reduction of the renal parenchyma; grade 4 = as grade 3 but with a reduction of the renal parenchyma [ 26 ] .
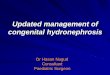
RRI calculations were based on the results of colour-coded duplex Doppler sonographic examinations. Accordingly, the Arteriae arcuatae were identifi ed at the lower, mid- and upper poles of the renal pelvis. During the measurement, the patient was told to hold his/her breath. The RRI was only calculated if four consecutive Doppler curves could be recorded ( Fig. 1 ).
The RRI is calculated according to the formula: (maximum systolic fl ow speed – end-diastolic fl ow speed)/maximum systolic fl ow speed. A mean value was calculated from the three RRI values per side (lower pole, upper pole and mid-pole)
FIG. 1. Image showing the measurement of the renal resistive index using colour-coded duplex sonography in the mid-pole of the kidney. Blood fl ow in the Arteria arcuata is shown graphically in the lower half of the image and analyzed by the scanner software. In total, three measurements are taken: fl ow speed (lower, mid- and upper pole) and a mean of the three computed measurements are shown.

I N T E R O B S E R V E R V A R I A B I L I T Y O F T H E H I A N D T H E R R I
© 2 0 1 2 T H E A U T H O R S
B J U I N T E R N A T I O N A L © 2 0 1 2 B J U I N T E R N A T I O N A L 3
for the corresponding kidney [ 1 – 23 ] . An RRI ≥ 0.70 and a difference in the RRI values ( Δ RRI) between the symptomatic and contralateral kidney > 0.07 are given in the literature as being suggestive of an obstruction [ 1 – 3,5 – 7,11,12,15,16,20,23 ] .
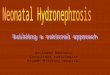
The HI was established both by sonography and CT for the affected and contralateral kidney. Measurements were based on a longitudinal section of the kidney at its
largest extension. The outer contours of the kidney were outlined with the trackball and the sonography device or CT scanner software automatically calculated the kidney area (cm 2 ). This was then repeated for the intrarenal pelvis together with the calyx groups ( Figs 2 and 3 ). The HI (as a percentage) was calculated using the formula: 100 × (total kidney area – intrarenal pyelon and calyx area)/(total kidney area) [ 24,25 ] .
Normally distributed continual variables are given as the mean ( SD ) and non-parametric continual variables are given as the median (interquartile range). The distribution of results between the affected and unaffected kidneys was calculated through statistical analysis of the data using the Student ’ s t -test (or the Mann – Whitney – Wilcoxon U -test for non-normal distribution) and the chi-squared test (categorial distinction). The agreement of both investigators with regard
to the evaluation of hydronephrosis using the three sonographic techniques (conventional sonography, RRI and HI) and a comparison of these values with the CT measurements were verifi ed using Cohen ’ s kappa statistic ( κ ) for attributive-ordinal characteristics and Spearman ’ s rank/rho correlation ( ρ ) (linear association) for attributive-metric characteristics. The coeffi cients were each in the range between – 1 and + 1, where < 0.4 = bad to moderate agreement; 0.40 – 0.59 = acceptable to good; 0.60 – 0.80 = very good; and > 0.80 = excellent agreement. All statistical tests were two-sided. P ≤ 0.05 was considered statistically signifi cant. All analyses were performed using SPSS, version 17.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
The descriptive data from the study group are displayed in Table 1 . The mean ( SD ) age
FIG. 2. Image showing the sonograhic measurement of the hydronephrosis index (HI). Measurements were based on a longitudinal section of the kidney at its largest extension. The outer contours of the kidney (including renal pelvis and calyx groups) were outlined with the trackball and the sonography device or CT scanner software automatically calculated the kidney area (cm 2 ). The HI (as a percentage) is calculated using the formula: 100 × (total kidney area – pyelon and calyx area)/(total kidney area).
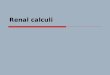
FIG. 3. Imaging showing the CT-generated measurement of the hydronephrosis index (HI). The kidney is shown at its largest extension in coronal mode, the outer contours, and the renal pelvis are outlined with the help of the scanner software and the area of these sections is calculated. The HI (as a percentage) is calculated using the formula: 100 × (total kidney area – pyelon and calyx area)/(total kidney area).
Criteria
Distribution within the study group ( n = 22)
Age (years), mean ( SD ) 50.9 (15.2)Women, n (%) 4 (18.2)BMI (kg/m 2 ), mean ( SD ) 27.3 (4.3)Right stone localization, n (%) 11 (50)Recurrent stone, n (%) 8 (36.4)Colic duration (h), mean ( SD ) 15.0 (12.6)Stone localization, n (%) Upper ureter 3 (13.6) Middle ureter 2 (9.1) Lower ureter 12 (54.5)Many obstructions in various localization, n (%) 5 (22.7)Stone size (imm), mean ( SD ) 5.6 (2.7)Active stone removal, n (%) 17 (77.3)Creatine (mg/dL), mean ( SD ) 1.01 (0.25)Sonography – colic side (Investigator 1), n (%) Grade 0 3 (13.6) Grade 1 14 (63.6) Grade 2 3 (13.6) Grade 3 2 (9.1)Sonography – colic side (Investigator 2), n (%) Grade 0 3 (13.6) Grade 1 16 (72.7) Grade 2 1 (4.5) Grade 3 2 (9.1)CT – colic side ( = I1 & I2 consensus sonography), n (%) Grade 0 3 (13.6) Grade 1 15 (68.2) Grade 2 2 (9.1) Grade 3 2 (9.1)
TABLE 1 Examination criteria

R U D E T A L .
© 2 0 1 2 T H E A U T H O R S
4 B J U I N T E R N A T I O N A L © 2 0 1 2 B J U I N T E R N A T I O N A L
of patients was 50.9 (15.2) years, and patients were predominantly men (82%). Side distribution was equal, with predominantly solitary stones in the lower ureter (55%). Mean ( SD ) stone size was 5.6 (2.7) mm. In total, fi ve (23%) patients passed their stones spontaneously after the study investigations were performed. All patients were confi rmed (both sonographically and by CT) to have an asymptomatic contralateral kidney, free from obstruction or other pathology. The separate evaluations of the colic kidney as carried out by both investigators are detailed in Table 1 . The joint consensus regarding sonographic grade was identical to the CT evaluation. There were three (14%) patients who showed no sonographic or CT obstruction; however, an obstruction was subsequently found when an intervention became necessary; these obstructions could not be displayed image-morphologically as a result of a dichotomic pelvicaliceal system. The descriptive RRI, Δ RRI and HI evaluations of both sonographic investigators and the CT HI are shown in Tables 2 and 3 . No signifi cant correlation was found between RRI, Δ RRI, HI, sonographic obstruction degree and CT obstruction degree with clinical criteria (stone localization, stone size, creatinine level, age, gender, side, body mass index, duration of colic and recurrent stone disease) (all P > 0.05). There was a signifi cant correlation between HI and sonographic consensus grade of hydronephrosis ( = degree of obstruction in CT analysis) at the colic side (Investigator 1: ρ = − 0.47, P = 0.029; Investigator 2: ρ = − 0.56, P = 0.007), although not between RRI and grade of hydronephrosis (Investigator 1:
ρ = – 0.03, P = 0.896; Investigator 2: ρ = – 0.15, P = 0.514).
Table 2 shows the different examination methods (RRI, Δ RRI and HI) together with the degree of obstruction in the sonographic consensus evaluation. Signifi cant differences between the various grades of hydronephrosis were seen in the sonographic HI evaluation (Investigator 2, P = 0.007) and the CT HI ( P < 0.001). Indeed, there was a signifi cant positive correlation between the HI value from Investigator 2 and the HI value given in the CT for the colic side ( ρ = 0.49; P = 0.021).
Table 3 sets out the differences for the respective examination methods between the unaffected and the colic kidney. All methods (RRI, HI, sonographic and CT degree of hydronephrosis) gave signifi cant
differences between both kidneys. Equally, there were differences between the RRI and HI of the colic side compared to the unaffected side in patients without sonographic hydronephrosis (Grade 0, n = 3).
Interobserver agreement (i.e. a comparison of the results obtained by Investigators 1 and 2) over the degrees of hydronephrosis on the colic side was excellent in the conventional sonographic evaluation ( κ = 0.82; P < 0.001); good to very good ( ρ = 0.60; P = 0.003) using the HI; and acceptable to good using the RRI ( ρ = 0.49; P = 0.021). Only 23% of patients (Investigator 1) or 64% of patients (Investigator 2) showed an RRI ≥ 0.7, and Δ RRI was found to be > 0.07 on the colic side in 59% (Investigator 1) and 55% (Investigator 2) of patients ( Table 4 ). Agreement between the two observers was
TABLE 2 Differences in the distribution of renal resistive index (RRI), Δ RRI and hydronephrosis index (HI) for both investigators, as well as between the CT calculated HI at the different sonographic consensus hydronephrosis grades (colic side)
Examination fi ndingsStudy group ( n = 22)
Grade 0 ( n = 3)
Grade 1 ( n = 15)
Grade 2 ( n = 2)
Grade 3( n = 2) P
RRI – Investigator 1 0.68 (0.05) 0.69 (0.05) 0.67 (0.04) 0.64 (0.01) 0.77 (0.09) 0.034RRI – Investigator 2 0.71 (0.04) 0.70 (0.07) 0.71 (0.04) 0.69 (0.01) 0.72 (0.01) 0.910 Δ RRI – Investigator 1 0.09 (0.05) 0.13 (0.05) 0.08 (0.05) 0.05 (0.04) 0.15 (0.09) 0.204 Δ RRI – Investigator 2 0.09 (0.05) 0.07 (0.02) 0.10 (0.06) 0.05 (0.01) 0.05 (0.04) 0.402HI (sonography) – Investigator 1 84.3 (5.6) 88.8 (2.22) 84.4 (5.50) 80.6 (2.97) 80.2 (9.97) 0.296HI (sonography) – Investigator 2 86.1 (6.4) 89.4 (1.10) 87.8 (3.91) 75.8 (8.90) 78.1 (12.09) 0.007HI (CT) 85.7 (5.0) 88.7 (6.34) 87.2 (2.45) 81.5 (2.99) 74.4 (2.09) < 0.001
Data are given as the mean ( SD ).
TABLE 3 Differences in the distribution of renal resistive index (RRI), Δ RRI, hydronephrosis index (HI) (sonography) and HI (CT) between the colic and contralateral unaffected kidney
Examination fi ndings Colic kidneyUnaffected kidney P
RRI – Investigator 1 0.68 (0.05) 0.59 (0.05) < 0.001RRI – Investigator 2 0.71 (0.04) 0.62 (0.05) < 0.001HI (sonography) – Investigator 1 84.3 (5.6) 92.4 (2.9) < 0.001HI (sonography) – Investigator 2 86.1 (6.4) 94.4 (2.5) < 0.001HI (CT) 85.7 (5.0) 96.4 (2.8) < 0.001Degree of hydronephrosis (sonography) – Investigator 1 1.18 (0.79) 0 < 0.001Degree of hydronephrosis (sonography) – Investigator 2 1.09 (0.75) 0 < 0.001Degree of hydronephrosis (sonography – consensus, CT) 1.14 (0.77) 0 < 0.001
Data are given as the mean ( SD ).

I N T E R O B S E R V E R V A R I A B I L I T Y O F T H E H I A N D T H E R R I
© 2 0 1 2 T H E A U T H O R S
B J U I N T E R N A T I O N A L © 2 0 1 2 B J U I N T E R N A T I O N A L 5
insuffi cient at these threshold levels ( κ = 0.29 and κ = – 0.39, respectively).
DISCUSSION
The goal of imaging in patients with acute renal colic is to confi rm initial diagnosis, determine stone size and localization, and to precisely quantify the degree of hydronephrosis, as well as evaluate potential complications [ 4 ] . Conventional sonography may be the standard imaging technique used in kidney examinations and is also ubiquitously available; however, native (contrast-medium free) helical CT has become the gold standard [ 26 – 29 ] . Native helical CT fulfi ls the previously listed requirements for a reliable mainstream clinical diagnostic; nevertheless, four limitations of this technique must also be noted. First, any determination of the extent of hydronephrosis is imprecise and does not allow reliable differentiation between obstructive and non-obstructive expansion of the pelvicaliceal system or between chronic and acute forms. Second, limits in kidney function as a result of the presence of a stone-related obstruction cannot be deduced from the results of the CT scan itself. Third, the imaging technique cannot be freely repeated because of the associated radiation dose, which is particularly important for patients with recurrent stones as a result of the cumulative dose. For this reason, CT imaging lends itself only to initial diagnosis and should not be performed as a part of the ongoing evaluation of patients
who could spontaneously pass their kidney stones (MET). Fourth, CT imaging is not available in all primary or outpatient care settings at all times (e.g. especially not if a patient becomes symptomatic during the night).
The use of colour-coded duplex Doppler sonography to determine the RRI was introduced into obstructive uropathic diagnostics by Platt et al . [ 6,7 ] . This stemmed from the observation that an immediate change in renal haemodynamics occurs during acute ureteric obstruction. This change is caused (amongst other things) by the vasoactive substances thromboxan A2, angiotensin 2 and endothelin [ 3 ] . This in turn leads to an increase in intrarenal resistance, which can be determined by colour-coded duplex Doppler sonography of the Arteriae arcuatae . A RRI value of 0.7 shows a 70% reduction in the sonographically-obtained end-diastolic fl ow speed relative to systolic fl ow speed. In this respect, the RRI correlates with the extent of urinary obstruction, even if this same effect can be observed during renovascular or parenchymal disease and the index can show age-related changes [ 1 – 3,5 ] .
The studies available in the literature have not yet defi ned uniform threshold values for the RRI or Δ RRI results above which a relevant obstructive uropathy can be assumed. The thresholds on which the present study are based ( ≥ 0.7 and > 0.07 respectively) are the values recommended in
the literature [ 1 – 3,5 – 7,11,12,15,16,20,23 ] , despite these not being uniformly identifi ed in all studies [ 19,22 ] . Furthermore, it remains unclear whether the RRI correlates with kidney function and, as such, whether it can be used as a clinical parameter during an expulsive therapy course. To date, indications to abort MET have been based on the development of clinical or laboratorial infection, an increase in creatinine level or analgesia-refractive renal colic [ 27 ] . A non-invasive and readily available indicator that can be calculated with colour-coded duplex Doppler sonography and anatomical – morphological data such as the RRI is highly desirable. However, in addition, any association between RRI and the functional state of the kidney remains to be proven, and this test could still only be sensibly employed if it was shown to exhibit a high level of intra- and interobserver agreement. The available studies on the value of the RRI for stone-related renal colic are summarized in Table 5 [ 1 – 23 ] .
The HI was fi rst described by Shaprio et al . [ 24 ] as a non-invasive, objective and stepless (dimensionless) longitudinal progress monitor in a study group of 46 children (aged 0 – 13 years) with hydronephrosis of various causes [ 24 ] . An HI value approaching 100% indicates normal and obstruction-free urinary function, with a decreasing HI being associated with an increase in obstructive uropathy. According to the defi nition of HI given by Shapiro et al . [ 24 ] , measurements should concentrate exclusively on intrarenal distension of the pelvicaliceal system because of the lower signifi cance of extrarenal system blockage. In another study, Venkatesan et al . [ 25 ] showed a narrow correlation between HI and the sonographically-established grade of hydronephrosis (graded according to the Society of Foetal Urology) using data from 1207 examinations on pelvi-ureteric junction obstruction. Studies of patients with stone-related acute obstruction and investigations into the reproducibility of the HI results remain absent from the literature. The RRI and HI do not compete with the helical native CT in terms of being the standard reference technique in the fi rst diagnostics of acute renal colic; rather, these two sonographic techniques are to be considered as complimentary to the CT and to comprise follow-up care diagnostics during MET.
TABLE 4 Interobserver agreement (Investigator 1 versus Investigator 2) for different diagnostic procedures in the evaluation of hydronephrosis
Examination report Investigator 1 Investigator 2Reliability Agreement ( κ or ρ ); P
RRI – colic, mean ( SD ) 0.68 (0.05) 0.71 (0.04) 0.49 ( ρ ); 0.021RRI – opposite, mean ( SD ) 0.59 (0.05) 0.62 (0.05) 0.25 ( ρ ); 0.269 Δ RRI, mean ( SD ) 0.09 (0.05) 0.09 (0.05) − 0.22 ( ρ ); 0.325HI – colic, mean ( SD ) 84.3 (5.6) 86.1 (6.4) 0.60 ( ρ ); 0.003HI – opposite, mean ( SD ) 92.4 (2.9) 94.4 (2.5) − 0.24 ( ρ ); 0.288Sonography – colic, mean ( SD ) 1.18 (0.79) 1.09 (0.75) 0.82 ( κ ); < 0.001Sonogaphy – opposite, mean ( SD ) 0 0 1.00 ( κ ); < 0.001RRI ≥ 0.7 – colic, n (%) 5 (22.7) 14 (63.6) 0.29 ( κ ); 0.054RRI ≥ 0.7 – opposite, n (%) 0 1 (4.5) No data Δ RRI > 0.07, n (%) 13 (59.1) 12 (54.5) – 0.39 ( κ ); 0.069
HI, hydronephrosis index; RRI, renal resistive index.

R U D E T A L .
© 2 0 1 2 T H E A U T H O R S
6 B J U I N T E R N A T I O N A L © 2 0 1 2 B J U I N T E R N A T I O N A L
In any case, the present study should be considered as the fi rst of many investigations in this area and it is not completely devoid of limitations, which must be considered when interpreting the results. The study group was relatively small and, in this respect, further studies on the interobserver variability of RRI and HI should incorporate a much larger number of patients. Also, the present study did not generate data on intra-observer variability or equipment variability. However, the collection of such data is not without its problems because the close time-spacing required between evaluations could lead to an investigator being infl uenced by the initial fi ndings, and a study design needs to be devised whereby this potential bias could be excluded. The RRI can be affected by various renovascular or renoparenchymal pathologies, and it is also possible that the type of analgesic therapy affects the values
returned by this index, which was not considered in the framework of the present study. Nevertheless, the RRI (as indicated by the records obtained in the present study) only delivers reliable results for low-symptom (symptomless) patients, which meant that regular analgesic medication was necessary. A most important question in this area, namely how RRI and HI progress over the course of acute obstructive uropathy (e.g. during MET), was not addressed by the present study design. Furthermore, it would be equally valuable to establish a correlation between RRI and HI using kidney function data (diuretic dimercaptosuccinic acid scintigraphy/DMSA), ideally obtained over a period of time.
In summary, the present prospective study shows acceptable to good interobserver agreement for the RRI and good to very good interobserver agreement for the HI in
patients with stone-related obstruction of the pelvicaliceal system. Both stepless procedures are simple to perform during the initial sonographic diagnostics and also allow the distinction between an obstructed and obstruction-free pelvicaliceal system, including in those patients with evident obstruction, as well as in those without conventional sonographic kidney obstruction. Because of the reduced interobserver agreement of the RRI in comparison with HI and the inadequate sensitivity of the thresholds for RRI in the present study (RRI ≥ 0.7, Δ RRI > 0.7), as well as several other threshold values described in the literature ( Table 5 ), in our opinion, HI rather than RRI should be explored further. The data obtained from the small patient group in the present study are to be considered primarily as a starting point for further studies. Indeed, further studies should aim to defi ne thresholds for
TABLE 5 Narrative literature review of the available studies on patients with acute hydronephrosis to determine the diagnostic benefi t of renal resistive index (RRI) and Δ RRI
ReferencePatient number
Threshold RRI
Threshold Δ RRI Study limitations Study results
Platt et al . [ 6 ] 21 ≥ 0.7 Not analyzed Few patients only, no reliability RRI can prove acute HN if PCS not dilatedPlatt et al . [ 7 ] 133 ≥ 0.7 Not analyzed RRI measured on different
arteries, no reliabilityRRI increases sonography specifi city
Gottlieb et al . [ 8 ] 8 Undefi ned Not analyzed Few patients only, no reliability HN can lead to increase in RRIRodgers et al . [ 9 ] 48 Undefi ned Not analyzed No reliability, no threshold values RRI can prove acute HN if PCS not dilatedPlatt et al . [ 10 ] 23 Undefi ned Not analyzed Few patients only, no reliability,
no thresholdsHN can lead to RRI increase
Chen et al . [ 11 ] 55 ≥ 0.7 Not analyzed No reliability RRI results can contribute to indication for an active therapy
Shokeir et al [ 16 ] 12 ≥ 0.7 Not analyzed Few patients only, no reliability RRI can prove acute HN if PCS not dilatedOnur et al . [ 5 ] 27 ≥ 0.7 ≥ 0.08 Few patients only, no reliability CCDS can prove acute HN if PCS not dilatedGurel et al . [ 4 ] 65 Undefi ned Not analyzed No reliability, no thresholds RRI is not sensitive for evidence of HNPepe et al . [ 3 ] 100 > 0.7 10% side
differenceNo reliability CCDS improves diagnostic accuracy
Ak ç ar et al . [ 23 ] 28 ≥ 0.7 ≥ 0.1 Few patients only, no reliability RRI und Δ RRI are time dependent parametersHaroun et al . [ 22 ] 88 0.65 0.05 No reliability Δ RRI highly specifi c and sensitive for HNGeavlette et al . [ 1 ] 377 ≥ 0.7 ≥ 0.06 No reliability CCDS and evaluation of urethral jet can
predict spontaneous stone passingKmetec et al . [ 2 ] 31 ≥ 0.7 ≥ 0.07 No reliability CCDS is a reliable method in HN diagnosisShokeir et al . [ 20 ] 117 ≥ 0.7 ≥ 0.06 No reliability CCDS is a reliable method in HN diagnosisGilbert et al . [ 17 ] 56 Undefi ned Not analyzed No thresholds, no reliability RRI is a reliable method in acute HN
diagnosisRoy et al . [ 18 ] 65 Undefi ned Not analyzed No thresholds, no reliability RRI is not sensitive for evidence of HNOpdenakker et al . [ 19 ] 70 ≥ 0.68 ≥ 0.06 No reliability CCDS useful 6 – 48 h after colic startDe Toledo et al . [ 15 ] 191 ≥ 0.7 ≥ 0.06 No reliability CCDS is sensitive for HNTublin et al . [ 12 ] 19 ≥ 0.7 ≥ 0.1 No reliability, few patients only CCDS is not sensitive for HN
CCDS, colour-coded Duplex sonography; HN, hydronephrosis; PCS, pelvicaliceal system.

I N T E R O B S E R V E R V A R I A B I L I T Y O F T H E H I A N D T H E R R I
© 2 0 1 2 T H E A U T H O R S
B J U I N T E R N A T I O N A L © 2 0 1 2 B J U I N T E R N A T I O N A L 7
these techniques (inclusive of RRI), as well as investigate index value changes and their correlation with obstructed kidney function over the course of MET.
ACKNOWLEDGEMENTS
Critical revision: M. Burger, S. Brookman-May, C. Gilfrich, H. H ä user, H.-M. Fritsche, W. F. Wieland, A. M. Ahmed and S. Brookman-May. Study concept and design: S. Brookman-May. Acquisition of data: O. Rud, P. Waliszewski, J. Moersler and S. Brookman-May. Drafting of the manuscript: S. Brookman-May, O. Rud, J. Moersler, J. Peter and H.-M. Fritsche. Statistical analysis: S. Brookman-May and O. Rud.
CONFLICT OF INTEREST
The authors declare that there are no confl icts of interest.
REFERENCES
1 Geavlete P , Georgescu D , Cauni V , Nita G . Value of duplex Doppler ultrasonography in renal colic . Eur Urol 2002 ; 41 : 71 – 8
2 Kmetec A , Peskar-Babnik D , Buturovic-Ponikvar J . Time-dependent changes of resistive index in acute renal obstruction during nonsteroidal drug administration . BJU Int 2002 ; 89 : 847 – 50
3 Pepe P , Motta L , Pennisi M , Aragona F . Functional evaluation of the urinary tract by color-Doppler ultrasonography (CDU) in 100 patients with renal colic . Eur J Radiol 2005 ; 53 : 131 – 5
4 Gurel S , Akata D , Gurel K , Ozmen MN , Akhan O . Correlation between the renal resistive index (RI) and nonenhanced computed tomography in acute renal colic: how reliable is the RI in distinguishing obstruction? J Ultrasound Med 2006 ; 25 : 1113 – 20
5 Onur MR , Cubuk M , Andic C , Kartal M , Arslan G . Role of resistive index in renal colic . Urol Res 2007 ; 35 : 307 – 12
6 Platt JF , Rubin JM , Ellis JH , DiPietro MA . Duplex Doppler US of the kidney: differentiation of obstructive from nonobstructive dilatation . Radiology 1989 ; 171 : 515 – 7
7 Platt JF , Rubin JM , Ellis JH . Distinction between obstructive and nonobstructive pyelocaliectasis with duplex Doppler
sonography . AJR Am J Roentgenol 1989 ; 153 : 997 – 1000
8 Gottlieb RH , Luhmann KIV , Oates RP . Duplex ultrasound evaluation of normal native kidneys and native kidneys with urinary tract obstruction . J Ultrasound Med 1989 ; 8 : 609 – 11
9 Rodgers PM , Bates JA , Irving HC . Intrarenal Doppler ultrasound studies in normal and acutely obstructed kidneys . Br J Radiol 1992 ; 65 : 207 – 12
10 Platt JF , Rubin JM , Ellis JH . Acute renal obstruction: evaluation with intrarenal duplex Doppler and conventional US . Radiology 1993 ; 186 : 685 – 8
11 Chen JH , Pu YS , Liu SP , Chiu TY . Renal hemodynamics in patients with obstructive uropathy evaluated by duplex Doppler sonography . J Urol 1993 ; 150 : 18 – 21
12 Tublin ME , Dodd GD III , Verdile VP . Acute renal colic: diagnosis with duplex Doppler US . Radiology 1994 ; 193 : 697 – 701
13 Cronan JJ , Tublin ME . Role of the resistive index in the evaluation of acute renal obstruction . AJR Am J Roentgenol 1995 ; 164 : 377 – 8
14 Platt JF , Ellis JH , Rubin JM . Role of renal Doppler imaging in the evaluation of acute renal obstruction . AJR Am J Roentgenol 1995 ; 164 : 379 – 80
15 De Toledo LS , Mart í nez-Berganza Asensio T , Cozcolluela Cabrejas R , de Gregorio Ariza MA , Pardina Cortina P , Ripa Saldias L . Doppler-duplex ultrasound in renal colic . Eur J Radiol 1996 ; 23 : 143 – 8
16 Shokeir AA , Provoost AP , Nijman RJ . Resistive index in obstructive uropathy . Br J Urol 1997 ; 80 : 195 – 200
17 Gilbert R , Garra B , Gibbons MD . Renal duplex Doppler ultrasound: an adjunct in the evaluation of hydronephrosis in the child . J Urol 1993 ; 150 : 1192 – 4
18 Roy C , Tuchmann C , Pfl eger D , Guth S , Saussine C , Jacqmin D . Potential role of duplex Doppler sonography in acute renal colic . Clin Ultrasound 1998 ; 26 : 427 – 32
19 Opdenakker L , Oyen R , Vervloessem I et al . Acute obstruction of the renal collecting system: the intrarenal resistive index is a useful yet time-dependent parameter for diagnosis . Eur Radiol 1998 ; 8 : 1429 – 32
20 Shokeir AA , Abdulmaaboud M . Resistive index in renal colic: a
prospective study . BJU Int 1999 ; 83 : 378 – 82
21 Rawashdeh YF , Djurhuus JC , Mortensen J , H ø rlyck A , Frokiaer J . The intrarenal resistive index as a pathophysiological marker of obstructive uropathy . J Urol 2001 ; 165 : 1397 – 404
22 Haroun A . Duplex Doppler sonography in patients with acute renal colic: prospective study and literature review . Int Urol Nephrol 2003 ; 35 : 135 – 40
23 Ak ç ar N , Ozkan IR , Adapinar B , Kaya T . Doppler sonography in the diagnosis of urinary tract obstruction by stone . J Clin Ultrasound 2004 ; 32 : 286 – 93
24 Shapiro SR , Wahl EF , Silberstein MJ , Steinhardt G . Hydronephrosis index: a new method to track patients with hydronephrosis quantitatively . Urology 2008 ; 72 : 536 – 8
25 Venkatesan K , Green J , Shapiro SR , Steinhardt GF . Correlation of hydronephrosis index to society of fetal urology hydronephrosis scale . Adv Urol 2009 ; doi:10.1155/2009/960490
26 Radermacher J . Ultrasonography of the kidney and renal vessels. I. Normal fi ndings, inherited and parenchymal diseases . Urologe A 2005 ; 44 : 1351 – 63
27 Arbeitskreis Harnsteine der Akademie der Deutschen Urologen , Arbeitskreis Endourologie und Steinerkrankung der Ö sterreichischen Gesellschaft f ü r Urologie , Knoll T . S2 guidelines on diagnostic, therapy and metaphylaxis of urolithiasis: part 1: diagnostic and therapy . Urologe A 2009 ; 48 : 917 – 24
28 Taourel P , Thuret R , Hoquet MD , Doyon FC , Merigeaud S , Delabrousse E . Computed tomography in the nontraumatic renal causes of acute fl ank pain . Semin Ultrasound CT MR 2008 ; 29 : 341 – 52
29 Kalb B , Sharma P , Salman K , Ogan K , Pattaras JG , Martin DR . Acute abdominal pain: is there a potential role for MRI in the setting of the emergency department in a patient with renal calculi? J Magn Reson Imaging 2010 ; 32 : 1012 – 23
Correspondence: Oleg Rud, Department of Urology, St Elisabeth Klinikum Straubing, St Elisabeth Street 23, 94315 Straubing, Germany. e-mail: [email protected]
Abbreviations : HI , hydronephrosis index ; RRI , renal resistive index .