Embed Size (px)
Citation preview

359
THE CONSERVATIVE TREATMENT OFHYDRONEPHROSIS
By PROFESSOR V. Dix, F.R.C.S.Surgeon to the London Hospital and Professor of Surgery in the University of London
It is my intention in this paper to discuss theaims of the conservative treatment of hydro-nephrosis; to indicate the results that may beexpected after conservative procedures; and todescribe some operations of which I have personalexperience and the types of hydronephrosis inwhich they can be used with reasonable expecta-tion of permanent cure.
If it is accepted that a man with one kidney hasa normal expectation of life-and there is noevidence to the contrary-it follows that nephrec-tomy for unilateral hydronephrosis will haveuniformly good results. The diseased organ hasbeen removed and can no longer produce symp-toms. It is against this standard of complete curethat we must measure the results of conservativeprocedures. The only other danger-the pos-sibility of injury to the single remaining kidney-is remote, and cannot reasonably be used as anargument for preferring conservative operations tonephrectomy.
Before considering the types of hydronephrosisand conservative operations, it is useful to have aclear conception of the kind of result that may beexpected. Although a rigid classification is im-possible, since one class merges imperceptibly intothe next, the following list covers most of theresults seen in following up a series of cases:
i. The patient is free from symptoms, thefunction of the kidney normal and the shape ofthe pelvis within normal limits. This may beconsidered a perfect result. It is relatively un-common.
z. The patient is free from symptoms and theshape of the pelvis within normal limits, but thefunction is still subnormal. This is a commonresult.
3. The patient is free from symptoms but therenal function is subnormal and the shape of thepelvis abnormal.
4. In addition to subnormal function andpelvic abnormality there is infection or some othercomplication or there is a return of pain.
It must also be remembered that certain con-servative operations are not without risk of im-mediate failure. It is certainly true that in any
operation in which redundant pelvis is excised,with or without detachment and reimplantation ofthe ureter, a persistent urinary fistula may occur,and the nephrectomy that was to have beenavoided will have to be performed before thepatient leaves hospital.On theoretical grounds conservative treatment
would seem to be the method of choice, if thereis a reasonable chance of obtaining a result of thefirst type, or in less favourable circumstances onenot worse than the second type. In results of thethird type there was probably an error ofjudgmentin selecting the case; in the fourth type there canbe little doubt that a primary nephrectomy shouldhave been performed.How is it then possible to select the right case for
conservative treatment ? During the pre-operativeinvestigations, more attention should be paid tothe function of the affected kidney than to itsshape in the pyelogram. This may be tested in anyof the usual ways-urine urea concentration,phenol-sulpho-phthalein, or indigo-carmine--myown preference being for indigo-carniine. Too littleattention is usually given to the normal kidney,which often indicates clearly the degree of per-manent loss of function on the affected side. Aconspicuous hypertrophy of the normal kidney,with a rapid and satisfactory concentration ofindigo-carmine, always indicates a great loss offunction on the affected side, and a condition thatis in many cases irreversible. If the hypertrophiedsound kidney has taken over most of the totalrenal function, the possibility that the hydro-nephrotic kidney will regain its original share ofthis function is small.The final decision must be postponed until the
kidney has been exposed and mobilized, and it isat this stage that it is most important to rememberthe aims of conservative surgery, as set out above.The anatomical conditions may favour one of theconservative procedures to be described later,although the kidney tissue itself may have reachedthe point at which recovery will be minimal. Ifthe bulk and consistency of the renal parenchymaconfirm the indications of the preliminary in-vestigations, that little return of function is to be
Protected by copyright.
on Novem
ber 21, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.25.286.359 on 1 August 1949. D
ownloaded from

POST GRADUATE MEDICAL JOURNAI,
expected, nephrectomy should be performed, evenwhen the type of hydronephrosis is otherwise mostsuitable for conservative treatment. The tempta-tion to perform a technically pleasing conservativeoperation is especially strong at this stage, and itis for this reason that I have stressed the im-portance of a clear conception of the aims ofconservative surgery, and of reaching a tentativedecision from the facts available before the opera-tion.The selection of the right case for conservative
treatment depends on the experience of the sur-geon and his critical judgment in assessing theresults of previous cases. It is impossible to givefigures for any specific test of renal function thatwill indicate the limits of what is practicable. Iwould suggest, however, as a suitable case forconservative treatment, one in which there is afair concentration in the I 5-minute film of anexcretion pyelogram in which the calyces ararecognizable as calyces and not entirely convertedinto rounded or oval cavities, and in which indigo-carmine appears in the excretion within iominutes of an intravenous injection, even thoughits concentration is never very great. The beginnerin this field of surgery would do well to begin byselecting only those cases with a well-markedhydronephrosis and a minimal impairment ofrenal function.
In certain cases of bilateral hydronephrosis itmay be necessary, as a life-saving measure, to runthe risk of performing conservative operationswhen the renal impairment already present doesnot give much -hope of a return to normal. Un-expectedly good results may be obtained in someof these cases.
Infection and the presence of a few smallcalculi-usually in the lower calyces-are not inthemselves contraindications to conservative opera-tions. Infections which would not clear up inthe obstructed kidney may die out or yield totreatment when the obstruction is removed, andthe calculi, in the absence of infection, willprobably not recur when the pelvis is emptyingnormally.
Types of HydronephrosisThe variation in the size of the pelvis in its
diastolic phase is very great, and is not necessarilythe same on the two sides. It is not my intentionto discuss in this paper what degree of dilatationmay, with justification, be called a hydronephrosisrequiring treatment. It is enough to say that inall the cases on which my conclusions are based,there was at least some distortion of the shape ofthe calyces and. some impairment of renal func-tion. In border-line cases I have always preferredto wait for some months, especially if the renal pain
was atypical, in order to see whether the conditionwas progressive. It is most unlikely that the renalimpairment will become so much worse in sixmonths that, a conservative operation is no longerpossible, and in some cases no operation will everbe necessary. I have recently seen a patient whomI advised to have an operation in 1940 for an earlyhydronephrosis, although the pain was not quitetypical. The air raids of that year made herdecide to postpone the operation. She has had nopain during the last nine years, although the pelvicdilatation remains unchanged and the I940 and1949 pyelograms are indistinguishable. It nowseems probable that she will never have to have anoperation, and there can be little doubt that thedilatation is only an unusually large diastolicphase in a normal pelvis.Nor is it my intention to discuss the etiology of
hydronephrosis or those cases in which there isalso a hydro-ureter. It may be mentioned, how-ever, that in some cases of hydronephrosis andhydro-ureter, division of the ureter at its lowerend and re-implantation into the bladder will givegood results.
In cases in which there is only a very smallintrarenal pelvis and in which the calyces showmost of the dilatation, a conservative procedure -isnot usually satisfactory. Most of the conservativeprocedures to be described can be applied -only tocases in which there is a reasonable degree ofpelvic dilatation. In a short paper it is impossibleto describe all the conditions that may be foundwhen the hydronephrotic kidney has been exposed,and I shall describe only three types of lesion inwhich I have found a conservative operation to beof some value:
i. The kidney shows a pelvic hydronephrosis ofmoderate size, and there is some dilatation of thecalyces to be seen in the pyelogram. When thekidney has been exposed and dissected, there is noapparent cause for the hydronephrosis, and nolower pole vessels are present. There are noobstructive fibrous strands surrounding theuretero-pelvic junction, and the uretero-pelvicjunction itself appears to be normal, with nofibrosis in its musculature.
2. Round the uretero-pelvic junction there aremany small fibrous strands that appear to be in-flammatory in origin. These strands kink and dis-tort the junction and have to be dissected awaywith great care before the ureter can be straightenedout. In addition to the peri-ureteric fibrosis thereis often well-marked hardness and narrowing ofthe upper 0.5 cm. of the ureter, extending to theuretero-pelvic junction. The impression given isthat the tube is a fibrous one and no longer entirelymuscular.
3. There is a band of vessels coming to the
36o .Augiist 1949P
rotected by copyright. on N
ovember 21, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.25.286.359 on 1 A
ugust 1949. Dow
nloaded from

DIX : Conservative Treatment of Hydronephrosis
lower pole of the kidney either causing the obstruc-tion or increasing the obstruction already startedby some other factor. After division ofthese vessels,if this is done, it may be found that the end of theureter and the uretero-pelvic junction are normaland the contents of the pelvis can be pressed downinto the ureter without the slightest difficulty. Inother cases, however, there are many fibrousstrands, as in the previous type, and these have tobe dissected away before the upper end of theureter is free from obstruction. In certain cases,that are much less common, there is also an obviousmacroscopic fibrosis of the upper part of theureter and its junction with the pelvis.
It is true that there are other possible com-binations of the above types, and every case inwhich the surgeon is going to perform a conserva-tive operation must be considered as a separateproblem. But I have selected the above types asthose which can be correlated with the operationsI have found to be of value. Before describingthe type of operation to be performed, it will beappropriate to mention again why errors ofjudgment are liable to occur in performing anexcision of the pelvis and re-implantation of theureter. This operation is so pleasing technically,and in suitable cases gives such good results, thatthere must inevitably be a strong bias in its favourat the time of the operation. But it is well toremember that it is technically easy to perform inthose very cases in which a conservative operationis probably of very little value. It is not difficultto excise the pelvis and re-implant the ureter whenthe pelvis is very large and the function of thekidney considerably diminished. The result maybe apparently satisfactory when an instrumentalpyelogram is performed after the operation, but itis really useless to perform an operation of thismagnitude unless there is afterwards a well-marked restoration of function, as well as asatisfactory leoking pelvis.
OperationsThe three operations I have performed are as
follows:i. Ligature and division of lower pole vessels.2. Dilatation of the uretero-pelvic junction and
temporary nephrostomy.3. Excision of the pelvis and re-implantation of
the ureter.For all these operations the kidney may be ex-
posed by any of the usual incisions. It will befound that a larger incision is necessary for anexcision of the pelvis than for the other twooperations.
i. Ligature and division of lower pole vessels.After the kidney has been dissected and
mobilized, it may be considered that the lower pole
vessels are the primary cause of the obstruction, orthat they may have become an important factor inmaintaining the hydronephrosis already initiatedby some other mechanism. In either case, unlessthe vessels are very large, they should be dividedbetween ligatures. If there is no peri-pelvic andperi-ureteric fibrosis, it should then be possible tosqueeze urine from the unopened pelvis into theureter. When this can be done easily, demon-strating the absence of permanent narrowing of thejunction, nothing more need be done. When,however, the uretero-pelvic junction is surroundedby fibrous strands, a careful dissection must beundertaken, freeing both ureter and pelvis andstraightening out kinks caused by the fibrosis. Itwill then usually be found, as in those cases withoutsurrounding fibrosis, that the pelvis communicatesfreely with the upper ureter through a uretero-pelvic junction of normal diameter. It is un-common to find intra-muscular fibrosis in thesecases, and I have only once had to combinedilatation with division of lower pole vessels.
After division of the vessels there is always anarea of infarction at the lower pole of the kidneyand its extent can be seen by an immediate changeof colour in the affected area. In most cases theestimated amount of kidney affected is not morethan one-sixth of the whole, and I have neverseen any serious complications following this localinfarction of the kidney. If the vessels are verylarge, and therefore likely to supply a corres-pondingly large amount of the kidney, It may bepossible to perform an excision of the pelvis withre-implantation of the ureter on the other side ofthe obstructing vessels.The proved association of hypertension with
certain cases of unilateral renal disease has createddoubts about the wisdom of deliberate damage tothe kidney by the ligation of lower pole vessels.There is, however, no certain evidence that, inman, renal infarction causes the type of ischaemiawhich initiates the series of changes resulting inhypertension. For the present we have no reasonto suppose that this simple operation is moredangerous than it was before the consequences ofrenal ischaemia were fully appreciated. The chiefmerit of the operation is that the pelvis and ureterare not opened. Good results may be expected,unless the compression atrophy of the kidney hasadvanced too far; when it has, nephrectomy andnot ligature of the vessels is the right operation.
2. Dilatation of the uretero-pelvic junction andtemporary nephrostomy.
This operation can be used for those cases offibrosis of the upper ureter and uretero-pelvicjunction, in which it is clear that there is a strictureat the pelvic outlet. A complete dissection of anyexternal fibrous strands is necessary, whether they
36xAugust 1949P
rotected by copyright. on N
ovember 21, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.25.286.359 on 1 A
ugust 1949. Dow
nloaded from

362 POST GRADUATE MEDICAL JOURNAL August 1949
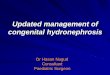
are causing kixiking of the ureter or not. Thepelvis is then opened (preferably on the posteriorsurface, but if necessary on the anterior surface)by an incision in the line of the ureter. The in-cision need not be more than i cm. in length.The smallest gum elastic bougie that will gothrough the stenosed ureteric orifice is then passedinto the ureter. This is followed by a successionof bougies advancing each time by one step on theCharriere scale. In a favourable case it is possibleto dilate to I2 or 13 Charriere. A temporarynephrostomy is then made in the following manner(Fig. I):-
* .
*9-- J
.' $it;. )Ltr *..*h.;jtt81.i.;;;4E~t
A7O'j4 *4. . 1 t a{ 9 - f F ^
FIG. I.-Temporary nephrostomy.
Through the opening in the pelvis a pair offorceps is introduced and the point pushed outthrough the renal substance so that it will emergesomewhere in the lower third of the kidney at itsconvex border and slightly on its posterior surface.A little haemorrhage may follow, but it is nevertroublesome.The end of a whistle-tipped catheter (No. i6
Charriere, with two lateral holes) is then graspedby the forceps and. drawn back into the pelvis,where it is adjusted so that it lies comfortably.When it is in the right position the catheter isheld by the assistant with a pair of forceps whereit emerges from the kidney. A catgut suture ispassed through the catheter, which must be firmlyheld at this stage or it will be pulled out and afurther adjustment will be necessary; the suturepicks up a piece of the capsule of the kidney andthe catheter is fixed. The pelvis is then sutured.Three or four cubic centimetres of fluid can be
introduced through the catheter into the pelvis tosee whether the pelvic suture line is water-tight ornot, and to wash out any small clots.The kidney is now returned to its position, a
perinephric drainage tube inserted and the woundis sewn up. The drainage tube and the catheterdraining the pelvis are allowed to come out of thewound at the most convenient place. This willoften be found (in the case of an oblique incision inthe loin) to be about one-quarter or one-third of thetotal length of the wound away from its anteriorend. The catheter is then attached to the skin bya suture of whatever material is being used for theskin sutures, and it may again be washed outgently to remove small clots.The post-operative management of the catheter
and its removal will be found in the description ofthe next operation.
If the uretero-pelvic stricture is too narrow toadmit even a small bougie, or so tough that dilata-tion is impossible, it may be possible to excise theconstricted uretero-pelvic junction and the dilatedpelvis, and to re-implant the ureter. But it is myexperience, in cases of this type, that the fibrosisextends down the ureter for some distance, oftenso far as to prevent re-implantation withouttension, when the fibrous upper part has beenexcised. In these circumstances a nephrectomyshould be done.During the dilatation, the uretero-pelvicjunction
may split. When this happens a nephrectomy willbe necessary, unless the ureter can be re-implantedafter the stricture and the redundant pelvis havebeen excised. It is uncommon for dilatation tocause splitting, and it is a risk that must be run ifadequate stretching is to be.obtained. As there israrely any other conservative procedure suitablefor cases of this type, a very occasional failure mustbe accepted as a reasonable risk in an attempt tosave the kidney.
3. Excision of the pelvis and re-implantation ofthe ureter (von Lichtenberg).
This operation is suitable for cases with lowerpole vessels that are considered to be too large forligature and division; for cases of stricture inwhich the stricture is limited to the uretero-pelvicjunction and does not encroach upon the ureter;agnd for any cases of hydronephrosis of the pelvictype in which neither of the above simple opera-tions is suitable. When the kidney has been ex-posed, it is freed from the perinephric tissue anda complete dissection of the renal vessels and theupper part of the ureter is made. If it appears thatthe hydronephrosis has been due to kinking of theureter over a vessel, it may be possible to dividethe ureter below this point and to re-implant itinto the reconstructed pelvis on the other sideof the obstructing vessel. When there is any peri-
Protected by copyright.
on Novem
ber 21, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.25.286.359 on 1 August 1949. D
ownloaded from

August I949 DIX: Conservative Treatment of Hydronephrosis 363
... ..
--- -** n| l || l |
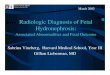
FIG. 3.-B.R. Pre-operative pyelogram (October, 1932).
L
FIG. 4.-B.R. Pyelogram io months after excision ofpelvis and re-implantation of ureter (August, I933).
!'. ..."
................
.::i.:................
FIG. 5.-B.R. Excretion pyelogram (I5-minute film)i6l years after operation (May, I949). Thispatient had a normal pregnancy five years ago.In Mav, 1949, indigo-carmine was excreted in goodconcentration from the kidnev in five minutes.
R .......
FIG. 6.-Q. S. Pre-operative pyelogram.
Protected by copyright.
on Novem
ber 21, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.25.286.359 on 1 August 1949. D
ownloaded from

364 P'OsTr GRADUATE MEDICAL JOURNAL Aug4ust 1)4(
FIG. 7.-Q.S. Pyelogram six years after dilatation ofuretero-pelvic junction and temporary nephros-tomv. Indigo-carmine was excreted in good con-centration from the kidnev in four minutes.
R.::.....
F cG. .-G.1K. Pre-operative pyelogram.
IlIG. 9.-G.K. Pvelogram I5 months after ligatureand division of lower pole vessels. Indigo-carminewas excreted in four minutes, but the concentra-tion was not normal. Although this patient wasfree from symptoms, and the calyces almost normal,the pelvis is still abnormal and the renal functionsubnormal. Time will show wNhether it wouldhave been better to perform nephrectomy.
(This figure, together with Nos. 1, 3, 4 and 8, arereproduced by kind permission of the lEditors of theProceedings of the Royal Society of Medicine.)
1:4:..:
Protected by copyright.
on Novem
ber 21, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.25.286.359 on 1 August 1949. D
ownloaded from

August I949 DIX - Conservative Treatment of Hydronephrosis 365
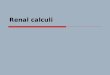
nephritis and peri-ureteritis, the fibrous strandsmust be carefully divided until the pelvis and theureter are completely bare and free from adhesions.The operation itself is performed as follows
(Fig. 2)
r t J -| < i s ai | q* ; -i*
r !X> ''/ SFjLb3A
EL p v f ..i,. U\- j s @ j f , 8.,
FIG. 2.-Excision of pelvis and implantation of ureter.'Maingot's Post Graduate Surgery,' p. 2843 (bypermission of Medical Publications Ltd.). (A) a-Cut edge of pelvis. b-Ureter. c-i6 Ch. catheterin pelvis. d-I2 Ch. catheter sutured into ureter.(B) a, b, c, d, as in (A). e-First suture attachingureter to lower angle of pelvis. ff-Sutures throughcut edge of pelvis (not tied). (C) a, b, c, d, as in (A).e-First suture attaching ureter to lower angle ofpelvis (tied). ff-Sutures through edges of pelvis(tied). g-Extra suture attaching ureter to newpelvis. h-Sutures attaching each catheter separa-tely to renal capsule.
The ureter is divided at its junction with thepelvis or, if there is an obstruction at the uretero-pelvic junction, a little below this point. Eitherbefore or after division of the ureter, the pelvis isopened between two traction sutures by an in-cision running in the line of the ureter towards thekidney. The ureter is held by one suture whichwas inserted before it was divided. The pelvis canat this stage be trimmed and the superflous pelvictissue removed. Most of the anterior and posteriorsurfaces should be removed, leaving enough foreasy suture without tension. A pair of curvedforceps is now inserted through the opened pelvisinto the lower main calyx and out through the
kidney substance, and two whistle-tipped rubbercatheters, a No. i6 and a No. .12 Charriere, aregrasped by the forceps and are drawn back throughthe kidney substance into the pelvis. The smallercatheter is pulled further through and inserted intothe upper end of the ureter for a distance of aboutI.5 cm. A suture is then passed through thecatheter and the ureter, fixing the catheter in thelumen of the ureter. This suture should be some-where in the first centimetre ,f the ureter. As soonas the catheter is fixed it is pulled gently back untilthe upper end of the ureter lies inside the openedpelvis. About i cm. of the ureter should lie in thepelvis at its lowest point, usually in the neighbour-hood of the old uretero-pelvic junction. A sutureis then passed, picking up first one wall of thedivided pelvis, next the wall of the ureter and thenthe other wall ot the divided pelvis. When thissuture is tied on the posterior surface it will beobvious that the ureter is firmly attached to whatwill be the lower angle of the new pelvis. At thisstage the ureter and the pelvis may be rotated andanother suture inserted in the same way. It isimportant that these sutures should pick up onlythe cut edges of the pelvis and the ureteric wall andnot the splinting catheter. The No. i6 catheter isthen aajusted until it lies comfortably in the newpelvis and the latter is reconstructed by suturingtogether the cut edges. The two catheters are nowfixed separately to the capsule of the kidney brpassing one suture through each catheter and thecapsule of the kidney. Care must be taken whenpassing these sutures not to pull the catheters outowing to the resistance of the rubber to the passageof the needle.
If the kidney lies well when replaced in itscavity, and there is no excessive movement onrespiration, nothing further need be done. If,however, the kidney seems to move too freely withrespiration, or if the vessels are long, therebyallowing the kidney a large range of movement, it isbetter to fix it at this stage. This can be done bydecapsulating the upper two-thirds of the kidney,pushing it up under the ribs and fixing it in thisposition, by a simple catgut suture passed throughits lower pole and attached to the upper angle ofthe wound. A -corrugated rubber drain is placedoutside the kidney in contact with the suture linein the reconstructed pelvis. The abdominal walland the skin are then sutured in the ordinary wayand the two catheters fixed at their points of exitfrom the wound. It will be seen that the No. i6catheter, which is the main drainage catheter andon which the success of the operation depends, isattached at two points-at its exit from the kidney,where it is attached to the capsule, and also whereit emerges from the skin incisions. The catheter inthe ureter is fixed at three points; there is one
Protected by copyright.
on Novem
ber 21, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.25.286.359 on 1 August 1949. D
ownloaded from

POST GRADUATE MEDICAL JOURNAL
suture attaching it to the ureter itself, anotherattaching it to the capsule of the kidney where itleaves its posterior border and a third sutureattaching it to the skin. Before the abdominalwall is sutured the reconstructed pelvis should betested in order to see that it is water-tight. This isdone by injecting not more than 3 or 4 cc. ofnormal saline into the pelvis through the largercatheter.The after-treatment is the same as that of any
other kidney operation, with one exception.During the first few days after the operation, andparticularly during the first 24 hours, great caremust be taken to see that the drainage tube doesPot become blocked. There is often a littlebleeding into the pelvis from its cut edges or fromthe hyperaemic mucosa, and small clots may formwhich block the holes of the catheter. If thisobstruction is not removed, the pressure inside thepelvis may become so great that the stitches giveway with the formation ot a urinary fistula. Thecatheter should therefore be examined every hourduring the first 24 hours in order to see that it isdraining freely, and every two hours for the next24 hours. At the end of this time the urine isusually no longer even faintly blood-stained, andno complications are likely to occur. Should thetube become blocked it can easily be cleared bygentle syringing with normal saline, or suctionmay be applied with the syringe. Any amount upto 4 cc. may with safety be injected into the re-constructed pelvis. The corrugated rubber drain
should be removed between the fifth and seventhdays, and the two catheters that are in the kidneyitself may be removed between the tenth andfourteenth days. On the tenth day the skinstitches should be removed and a gentle effortmade to pull out the catheters. If they are loosethey will come out easily, but if they are stillattached to the renal capsule no force should beused, and a further gentle pull should be madeeach day when the dressing is done, until they comeout readily. There is usually no leakage of urineafter the catheters are removed, but should thisoccur it will seldom last for more than two or threedays.
It must not be assumed that the omission ofother operations for restoring function in cases ofhydronephrosis is a condemnation or even animplied criticism of operations different from thoseI have described. In the hands of a surgeonaccustomed to them other operations will doubt-less yield good results. But it is inevitable thateach surgeon should choose certain operationswhich he finds satisfactory and perform theseoperations frequently. If the results of thoseselected are good it is unnecessary to change thetype of operation to another, that will give onlythe same good result. It is my experience thatthe three operations I have described will givegood results and that one of them will be foundsuitable for restoring function in any case ofhydronephrosis in which such restoration ispossible.
August I949366P
rotected by copyright. on N
ovember 21, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.25.286.359 on 1 A
ugust 1949. Dow
nloaded from