Embed Size (px)
Citation preview

PROPOSALFORTHEINCLUSIONOFLOWMOLECULARWEIGHTHEPARINSFORTHEPREVENTIONOFVENOUSTHROMBOEMBOLISMINHOSPITALIZEDPATIENTSINTHEWHO
MODELLISTOFESSENTIALMEDICINES
October1st2014
WalterAgenoMarcoDonadini
PantepAngchaisuksiriMarkCrowtherHenryDdunguIsmailElalamy
ZoubidaTaziMezalekPeterVerhammeHenryWatson
ScientificandStandardizationCommitteeonControlofAnticoagulationInternationalSocietyonThrombosisandHaemostasis
DepartmentofClinicalandExperimentalMedicineUniversityofInsubria
Varese,[email protected]
+390332393564
2
Medicinesaffectingcoagulationlistedinthe18thEMLApril2013
Heparinsodium Injection:1000IU/mL;5000IU/mL;20000IU/mLin1‐mL
ampoule
Warfarin Tablet:1mg;2mg;5mg(sodiumsalt)
1. Summarystatementoftheproposalforinclusion
Venousthromboembolism(VTE)isoneoftheleadingcausesofmorbidityand
mortalityinhospitalizedpatientsandpulmonaryembolismisresponsiblefor10%of
overalldeaths.Becausesymptomsofdeepveinthrombosisandpulmonaryembolism
arenon‐specific,atimelydiagnosisremainsdifficultandscreeningtestsforVTEare
notcost‐effective.Thus,carefulselectionofpatientsatincreasedriskandapplication
ofadequateprophylacticstrategiesisnecessarytoreducetheburdenofdisease.There
isalargeamountofevidenceshowingtheefficacyofprophylacticstrategiestoprevent
VTEinat‐riskhospitalizedpatients.Pharmacologicprophylaxiswitheitherlow‐dose
unfractionatedheparin(LDUH)orlowmolecularweightheparin(LMWH)hasbeen
showntoreducetheriskofpulmonaryembolismingeneralsurgicalpatientsby75%.
Becauseoftheirgreatereaseofuse(singledailydose)andtheirimprovedsafety
profile(thefrequencyofheparininducedthrombocytopeniaisthree‐foldlowerwith
LMWHthanwithunfractionatedheparin),LMWHhaswidelybecomethemanagement
ofchoiceforprophylaxisofVTEinthissetting.Inpatientsundergoingmajor
orthopedicsurgery,LMWHhasbeenshowntobethemosteffectiveagentbeforethe
arrivalofthedirectoralanticoagulantdrugs(DOACs)byproducinganapproximately

3
70%riskreductioninVTEandiscurrentlyrecommendedasthetreatmentofchoicein
thissetting(seebelow).Itwasestimatedthatapproximatelytwooutofthreepatients
undergoingsurgicalproceduresshouldbedeemedeligibletoreceiveantithrombotic
prophylaxis.Unfortunately,theresultsofalargeobservationalstudycarriedoutin
severalcountriesthroughouttheworld(ENDORSE)reportedthatonlyabout60%of
at‐risksurgicalpatientsactuallyreceiveadequateprophylacticstrategies.However,
thisratewidelyvariedamongcountries,beinghighestinwesternEuropeancountries
andlowestinlowandmiddleincomeAsiancountries.IncountrieslikeBangladesh,
India,Pakistan,andThailand,prescriptionratesrangedbetween0.2%and16.3%.
TheserateswerehigherinNorthernAfricancountries(Egypt,Tunisia,Algeria)while
noinformationwasavailableforCentralAfricancountries.Insufficientavailabilityof
drugs,butalsoinsufficientawarenessofpost‐surgicalVTEasamajorclinicalissue
remainthemaindriversforthismajorgapbetweenevidencesandclinicalpractice.For
example,theincidenceofpost‐surgicalvenousthrombosishastraditionallybeen
thoughttobelowinAsianethnicpopulations.However,recentstudieshave
challengedthiscommonviewshowingthatthisincidenceissimilartothatreportedin
Westerncountries.Forthesereasons,webelievethatimprovingaccesstodrugswith
thehighesteffectivenessinthepreventionofVTEinsurgicalpatientshasthepotential
toreducetheburdenofdiseaseandthrombosisrelatedcostsalsoinlowandmiddle
incomecountries.However,thisimprovementcanonlybeachievedinconjunction
withanimprovedawarenessofthislife‐threateningdisease.
2. NameofthefocalpointinWHOsubmittingorsupportingtheapplication
DepartmentofEssentialMedicinesandHealthProducts(EMP/PAU)
3. Nameoftheorganizationconsultedandsupportingtheapplication

4
ScientificandStandardizationCommitteeonControlofAnticoagulationofthe
InternationalSocietyonThrombosisandHaemostasis
4. InternationalNonproprietaryName(genericname)ofthemedicine
Lowmolecularweightheparin:enoxaparin,nadroparin,dalteparin,tinzaparin,
reviparin,parnaparin,certoparin,bemiparin
5. Formulationproposedforinclusion
Injectable,subcutaneous.
6. Internationalavailability–sources(manufacturersandtradenames)
Enoxaparin:Clexane/Lovenox(Sanofi‐AventisPharma),Cutenox(GlandChemical),
Dynalix(BioconLimited),Enoxarin(ZuventusHealthCare),Flothin(Ranbaxy
Laboratories),Leeparin(LeeChemBiothecPvt),Lmwx‐PFS(NicholasPiramalIndia),
Lovenox(WatsonPharmaceuticals),enoxaparin(Sandoz),Cardinex(Drug
International),Enoparin(PopularPharmaceuticals),Parinox(InceptaPharma),Novex
(Sothéma),Flumax(Hemolab‐pharma)
Nadroparin:Fraxiparin(Aspen),Seleparina(Italfarmaco),Fraxiparine
(GlaxoSmithKline),Cardioparin(ChandraBhagatPharma),Nadrohep(GlandPharma),
Nadroparin(BharatSerum&Vaccines)
Dalteparin:Fragmin(P.Upjohn),Fragmin(Eisai)
Tinzaparin:Innohep(LeoLaboratories),Innohep(RanbaxyLaboratories)
Reviparin:Clivarin(Abbott),Clivarine(Knoll),Clivarine(Abbott),Clivarina(Abbott),
Lowmorin(BayerYakuhin)
Parnaparin:Fluxum(AlfaWassermann),Fluxum(USV‐Corvette),Lowhepa
(Ajinomoto),Thromboparin(FaranLaboratories)
Certoparin:Sandoparin(Novartis),Sandoparin(Sandoz),Mono‐Embolex(Novartis)
5
Bemiparin:Ivor(Rovi),Ivor(Sigma‐Tau),Ivorat(Gineladius),Zibor(Berlin‐Chemie),
Zibor(Menarini),Hibor(Biotoscana),Hibor(DemIlac),Hibor(Valmor),Hepadren
(Rovi),Badyket(Menarini)
7. Whetherlistingisrequestedasanindividualmedicineorasanexampleofa
therapeuticgroup
Weproposelowmolecularweightheparinasapharmacologicalclass.Althoughsome
pharmacokineticandpharmacodynamicdifferencesexistamongdifferentlow
molecularweightheparins,andalthoughenoxaparinhasthebestevidencefor
effectivenessandsafety,alllowmolecularweightheparinsareapprovedforthe
indicationdiscussedinthisproposalandnooneisconsistentlyavailalblewiththe
lowestpriceinallconsideredcountries.
8. Informationsupportingthepublichealthrelevance(epidemiological
informationondiseaseburden,assessmentofcurrentuse,targetpopulation)
VTEisacommondiseaseandamajorhealthproblem.Theannualincidenceratewas
estimatedtobe131.5(95%CI,130.2‐132.9)per100,000personsinarecentstudy
conductedintheUnitedKingdom(1),104(95%CI95‐114)per100,000personsinthe
UnitedStates(2),and57(95%CI47‐67)per100,000personsinAustralia(3).Case
fatalityratesat28daysafterafirstlifetimeVTEhavebeenestimatedtobe5%(95%CI
1‐9%)afteranidiopathicevent,7%(95%CI2‐13%)afteraVTEprovokedbytrauma,
surgeryorimmobilization,and25%(95%CI15‐36%)inpatientswithcancer(4).
Theincidenceoffirst‐timeVTErisesexponentiallywithage,rangingfromaverylow
rate(0.005%/year)amongchildren15yearsofage,toarateof450to600/100,000
peryear(≈0.5%/year)amongindividualsovertheageof80years(5).Ethnicityis
anothermajordeterminantofVTE.StudiescarriedoutintheUnitedStatesreporteda

6
significantlyhigherincidenceofdeepveinthrombosisandpulmonaryembolismin
whitepersonsandAfrican‐AmericansthaninAsiansandPacificIslanders(6,7).
MorethanhalfofVTEeventsarerelatedtohospitalizationandare,thus,preventable
(8).Surgicalprocedures,inparticularmajororthopedicsurgeryandcancersurgery
arecommonlycomplicatedbyVTE.Studiesassessingthepresenceofasymptomatic
deepveinthrombosisbasedonobjectivediagnosticscreeningwithvenographyin
patientsnotreceivingprophylaxisreportedincidencesbetween40and60%afterhip
orkneearthroplastyandbetween15and40%aftergeneralsurgery(9).Theestimated
rateofsymptomaticVTEatapproximatelyonemonthaftermajororthopedicsurgery
is4.3%(1.5%pulmonaryembolism)inpatientsnotreceivingprophylaxisand1.8%
(PE1.55%)inpatientsreceivingthromboprophylaxiswithLMWH(10).Inalarge
prospectivestudycarriedoutinpatientsundergoingcancersurgery,thereported
incidenceofsymptomaticVTEwas2.8%afterabdominalsurgery,with87%ofthese
patientsreceivingin‐hospitalprophylaxiswithLMWH(11).Theefficacyandsafetyof
pharmacologicprophylaxisinsurgicalpatientshasbeenconsistentlyshownbythe
resultsofseveralrandomizedcontrolledtrialsandmeta‐analysesandclinical
guidelinesrecommendthatallpatientsundergoinghigh‐riskproceduresshould
receiveappropriatetreatment(10,12).LMWHisconsideredthetreatmentofchoice
forpatientsundergoingmajororthopedicsurgery,beingpreferredoverothereffective
alternativessuchasfondaparinux,LDUH,adjusted‐dosevitaminKantagonists(VKA)
ortheDOACs(10).Thispreferenceisduetothefavourableefficacyandsafetyprofile,
tothefavourablecost‐effectiveness,andtotheverylargeexperiencewiththeuseof
theseagentsworldwide.LMWHisalsorecommendedforhigh‐risksurgicalpatients,
withLDUHorfondaparinuxaspotentialalternatives(12).LMWHisinparticular
proposedforpatientsundergoingabdominalorpelviccancersurgery(12).
7
Despiteclear‐cutrecommendations,prescriptionratesofadequate
thromboprophylacticstrategiesremainbelowexpectation.In2008,amultinational,
cross‐sectionalstudy,ENDORSE,reportedtheprevalenceofVTEriskintheacute
hospitalcaresettingandtheratesofat‐riskpatientswhoreceivedeffective
prophylaxisaccordingtorecommendationsfrominternationalguidelines(13).Two‐
thirds(64.4%)ofsurgicalpatientsweredefinedat‐riskforVTE,butonly58.5%of
themreceivedrecommendedVTEprophylaxis.Thestudywascarriedoutinall
continentsandprovidedaninterestingoverviewofdifferencesamongcountries.What
cameoutmoststrikinglyfromthisstudy,albeitnotsurprisingly,wastheverylowrate
ofprescriptionofadequateprophylacticstrategiesdocumentedinsomecountries,
withthelowestratesbeingdocumentedinBangladesh(0.2%),Thailand(0.2%),
Pakistan(10%),India(16%),Venezuela(23%),Russia(26%),SaudiArabia(32%),
Egypt(35%),Turkey(39%),UnitedArabEmirates(43%),Mexico(43%),Colombia
(43%),andBrazil(46%).Reasonsfortheselowprescriptionratesincludelackof
availabilityofrecommendedtherapeuticstrategies,costsofavailabledrugs,concern
aboutbleeding,difficultywithassessingrisklevelofpatients,andlackofawarenessof
VTEasarealprobleminsurgicalpatients.Thislastissuepossiblycontributesto
explainthelowestratesobservedinAsiancountries.Epidemiologicalstudiesfrom
AsiancountriesreportedVTEratesthatarelowerthanthosereportedinWestern
countries(14‐16),althoughayearlyincreasingincidenceandprevalenceofvenous
thrombosiswasconsistentlyshown(14,16),inparticularamonghospitalizedpatients.
Theseincreasingratessuggestedapossibleshiftinperceptionoftheimportanceofthe
disease,ahigherindexofsuspicionandalowerthresholdforperformingdiagnostic
tests(16),buttheuseofthromboprophylaxisremainedextremelylow.Theneedfor
suchashiftisfurthersupportedbyevidencefromprospectiveobservationalstudies

8
thatinAsianpatientstheincidenceofsymptomaticVTEafterhighrisksurgeryisnot
negligible(1.5%atonemonth)(17).Forthisreason,inthe“Asia‐PacificThrombosis
AdvisoryBoardconsensuspaperonpreventionofvenousthromboembolismafter
majororthopaedicsurgery”itwasagreedthatVTErepresentsathreatalsotoAsian
patientsandthatcurrentinternationalguidelinerecommendationsfortheroutineuse
ofpostoperativethromboprophylaxisshouldbeimplementedinAsia.Scant
informationisavailablefromotherlowincomecountriesinAfricaorSouthAmerica,
butitishighlylikelythatprescriptionratesinthesecountriesarenobetterthanthose
reportedfromcountriesparticipatingintheENDORSEstudy,thusleavingmillionof
patientsreceivingsurgicalproceduresatincreasedriskofpulmonaryembolismand,
thus,ofVTErelatedmortality.Forexample,across‐sectionalstudycarriedoutin12
hospitalsinSenegalidentified60.3%surgicalpatientsatriskforVTE,ofwhom37.5%
receivedthromboprophylaxis(18).
Forthisreason,thefirsttargetpopulationforthisproposalisrepresentedbyat‐risk
surgicalpatients(usingdefinitionsproposedbyinternationalguidelines)admittedto
hospitalslocatedinlowandmiddleincomecountriesinallcontinents.
9. Treatmentdetails(dosageregimen,duration;referencetoexistingclinical
guidelines;needfortreatmentmonitoringfacilities)
Enoxaparin2000IUqd(moderaterisksurgicalpatients),4000IUqd(highrisk
surgicalpatients,includingmajororthopedicsurgeryinEurope),3000UIbid(major
orthopedicsurgeryintheUS);nadroparin2850IU(generalsurgerypatientsand
majororthopedicsurgerypatients<50kgbodyweight),3800IUqd(majororthopedic
surgerypatients50‐69kgbodyweight),5700IUqd(majororthopedicsurgery>70
kg);dalteparin2500IU(generalsurgery)and5000IUqd(majororthopedicsurgery);

9
tinzaparin3.500IUqd(generalsurgerypatients)and50IU/Kgqd(majororthopedic
surgery);reviparin1750IUqd(generalsurgerypatients)and4.200IUqd(major
orthopedicsurgery),parnaparin3.200IUqd(generalsurgerypatients)and4250IUqd
(majororthopedicsurgerypatients);certoparin3000IUqd,bemiparin2500IUqd
(generalsurgerypatients)and3500IUqd(majororthopedicsurgerypatients).
Recommendeddurationofprophylaxisvariesaccordingtosurgicalprocedures.
Extendeddurationpharmacologicprophylaxisisrecommendedforhigh‐riskpatients
undergoingabdominalorpelvicsurgeryforcancer(4weeks)(12)andforpatients
undergoingmajororthopedicsurgery(35days)(10).
Plateletcountmonitoringiscurrentlyrecommendedforpatientsreceivingheparinin
whomcliniciansconsidertheriskofheparininducedthrombocytopeniatobehigher
than1%(19).Forthesepatients,plateletcountmonitoringshouldbeperformedevery
2or3daysfromday4today14,oruntilheparinisstopped(19).Basedonavailable
evidence,theincidenceofheparininducedthrombocytopeniainpostoperative
patientsreceivingLDUHrangesbetween1and5%,inpatientsreceivingLMWH
between0.1and1%(19).
Publichealthneedandevidenceappraisalandsynthesis
10. Summaryofcomparativeeffectiveness(identificationofclinicalevidence,
summaryofavailabledata,summaryofavailableestimatesofcomparative
effectiveness)includingsummaryevidencetableswithGradingof
recommendations
LMWHsweretestedagainstvariouscomparatorsinseveralrandomizedcontrolled
trialsindifferentat‐risksurgicalpopulations.Takingintoaccountthatthereare
severaldifferencesbetweenorthopedicandnon‐orthopedicsurgery,especiallywith
10
regardtotheriskofVTE,thesetwogroupsofsurgeriesarepresentedseparately
hereafter.
NonOrthopedicSurgery
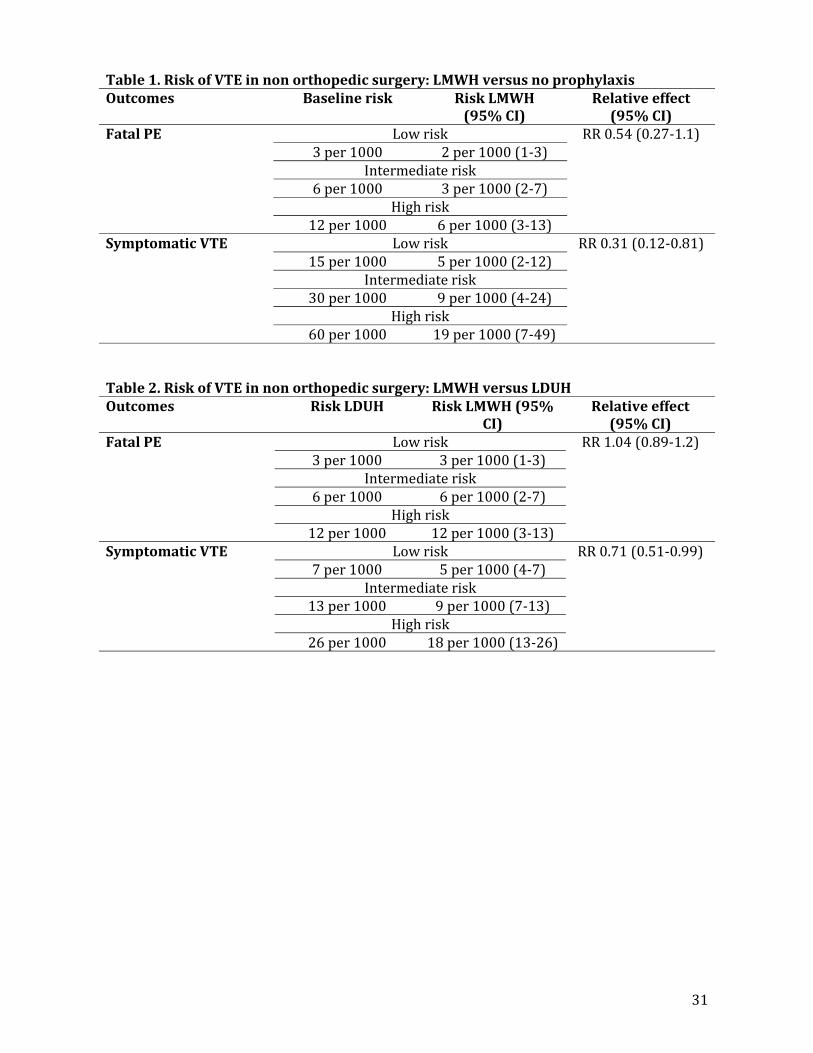
‐LMWHversusnoprophylaxis(Table1)
Ameta‐analysisofeighttrialsconductedingeneralandabdominalsurgeryshoweda
reductionoftheriskofsymptomaticVTEofabout70%(riskratio[RR]0.31,95%CI
0.12‐0.81)inpatientswhoreceivedLMWHascomparedtonoprophylaxis(20).
Furthermore,deathfromanycausewaspossiblyreducedbyabout50%(RR0.54,
95%0.27‐1.10)(20).Thesedatahavebeenmorerecentlyconfirmedinameta‐
analysiswhichincludedstudiesofgastrointestinal,gynecologic,urological,and
thoracicsurgery(21).
‐LMWHversusLDUH(Table2)
Resultsfromameta‐analysisof51trialsonmorethan48000generalandabdominal
surgerypatientsshowedthattheriskofsymptomaticVTEwasreducedbyabout30%
(RR0.71,95%0.51‐0.99)inpatientswhoreceivedLMWHascomparedtoLDUH(20).
Thesedatahavebeenconfirmedinamorerecentmeta‐analysisincluding
gastrointestinal,gynecologic,urological,andthoracicpatients(21).
‐LMWHversusfondaparinux
ArandomizedcontrolledtrialwasconductedinpatientsathighriskofVTEwho
underwentabdominalsurgery(22),comparingfondaparinuxtodalteparin.Theresults
showedthatfondaparinuxwasnon‐inferiortodalteparinatreducingthecomposite
outcomeofdeepveinthrombosisdetectedbybilateralvenographyandsymptomatic,
confirmeddeepveinthrombosisorpulmonaryembolism(relativeriskreduction24.6
percent,95%CI‐9.0to47.9).
‐LMWHversusmechanicalprophylaxis

11
Dataarelimitedtoonestudyontraumapatients(23)andonestudyongynecologic
oncologypatients(24).Inthefirsttrialtherewasnostatisticallysignificantdifference
intherateofasymptomaticandsymptomaticDVTbetweenpatientswhoreceived
LMWHascomparedtointermittentpneumaticcompression(0.5%versus2.7%,
respectively,p=0.122).Intheothertrial,DVTwasdiagnosedin2outof105patients
receivingLMWHandin1outof106patientsreceivingexternalpneumatic
compression,thusleadingtheauthorstoconcludeforasimilareffectofthetested
interventionsinthepostoperativeprophylaxisofthromboembolism.
Asubgroupanalysisofarecentmeta‐analysis(25),thatincludedalltypeofmechanical
compressions(pneumaticcompression,footcompressionandgraduatedcompression
stockings)ascomparedtoLMWHinseveralgroupsofsurgicalpatients,including
orthopedicones,foundasignificantyhigherriskofDVTamongpatientswhoreceived
mechanicalcompressionascomparedtoLMWH(RR1.80,95%1.16‐2.79).
NotrialsareavailableforcomparisonofLMWHwithaspirin,warfarinorneworal
anticoagulantsinnonorthopedicsurgery.
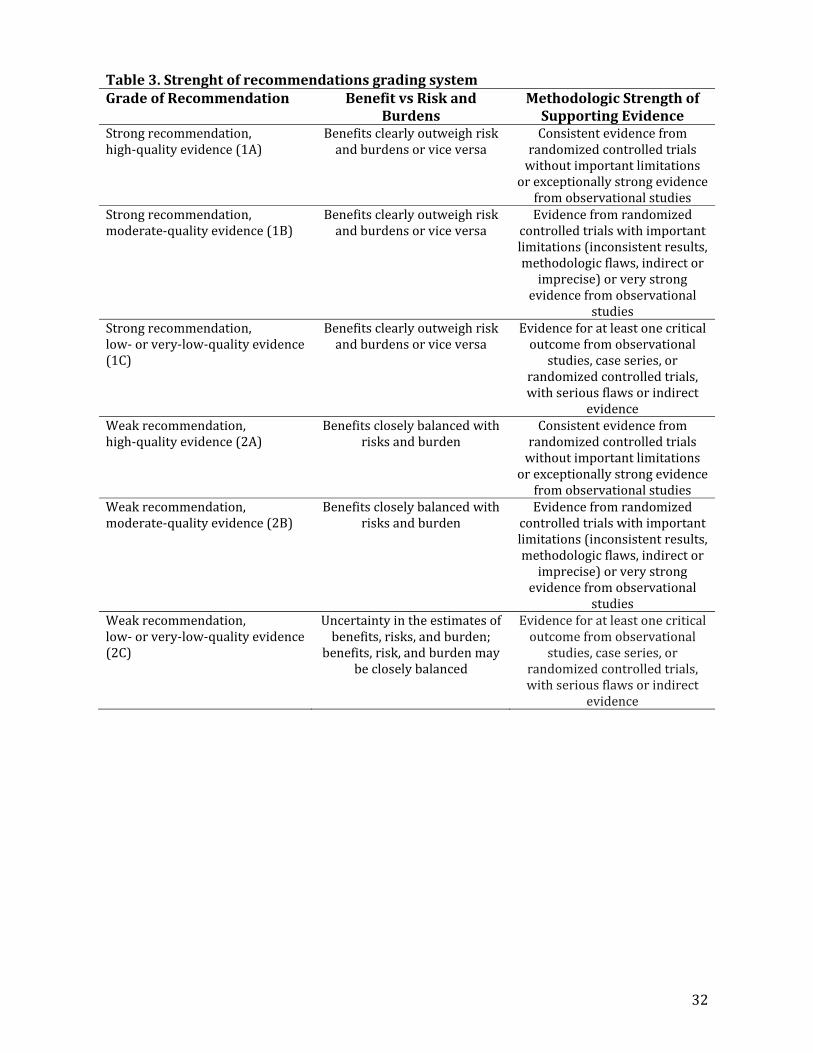
Basedontheavailableevidence,in2012theAmericanCollegeofChestPhysician
providedanupdatedversionoftheevidence‐basedclinicalpracticeguidelinesforthe
preventionofthrombosisinnonorthopedicsurgicalpatients(12).TheGradingof
RecommendationsAssessment,DevelopmentandEvaluation(GRADE)systemwas
usedtoassesstheevidenceandtoformulaterecommendations(Table3)(26).
Inthecontextofnon‐orthopedicsurgery,therecommendationsontheuseof
thromboprophylaxisarebasedonatrade‐offbetweentheriskofVTEandtheriskof
majorbleedingaftersurgery,thatcanbestratifiedaccordingtoseveralpatient‐and

12
surgery‐relatedvariables.TheriskofVTEcanbeconsideredverylow(<0.5%),low
(~1.5%),moderate(~3.0%)andhigh(~6.0%).Ontheotherhand,theriskofmajor
bleedingcanbeconsideredaverage(~1%)orhigh(~2%).Bleedingriskisalso
consideredhighwhenbleedingcomplicationsmayhaveespeciallysevere
consequences(egaftercraniotomy,spinalsurgery,reconstuctiveproceduresinvolving
freeflap).
Recommendationsfortheuseofthromboprophylaxisinnonorthopedicsurgeryare
summarizedinTables4.
OrthopedicSurgery
‐LMWHversusnoprophylaxis(Table5)
Inmajororthopedicsurgery,thatincludestotalhiparthroplasty(THA),totalknee
arthroplasty(TKA)andhipfracturesurgery(HFS),theriskofsymptomaticVTEwas
calculatedfromdataofclinicaltrialsenrollingmorethan16000patients,asfollows:
2.80%(PE1.0%,DVT1.80%)intheinitialpost‐operativeperiod(days0to14)and
1.50%(PE0.50%,DVT1.00%)intheextendedpost‐operativeperiod(days15‐35),for
acumalativepost‐operativeVTEincidenceof4.3%(PE1.50%,DVT1.80%)(10).
Intheinitialpost‐operativeperiod,thebestevidencesuggeststhatLMWHconsistently
reducesDVTbyabout50%afterTHAorTKA(combinedriskratio[RR],0.50,95%CI
0.43‐0.59),withsimilarresultsemergingalsoforHFS.Combiningresultsfromall
relevantstudiesfailedtodemonstrateortoexcludeabeneficialeffectofLMWHonPE
(RR0.58,95%CI0.22‐1.47)(10).
Intheextendedpost‐operativeperiodaftermajororthopedicsurgery,LMWHwas
associatedwithastatisticallysignificantreductionofsymptomaticDVT(RR0.46,95%

13
CI0.26‐0.82),whereasabeneficialeffectonPEwasneitherdemonstratednor
excluded(RR0.24,95%0.04‐1.4)(10).
‐LMWHversusLDUH(Table6)
LMWHandLDUHhavebeencomparedintheinitialprophylaxisaftermajor
orthopedicsurgery.Asubgroupanalysisofasystematicreviewoftrialscomparing
LMWHandUFHincluded2800patientswhounderwentarthroplastyorHFS(27).The
resultsshoweda20%relativeriskreductionofprimarilyasymptomaticDVTinfavor
ofLMWH(RR0.80,95%CI0.73‐0.88)whereastheyfailedtodemonstrateorexcludea
beneficialeffectofLMWHonPE(RR0.78,95%CI0.49‐1.24).
‐LMWHversusVitaminKantagonists(VKAs)(Table7‐8)
LMWHhasbeencomparedtoVKAsinmorethan9000patientsinseveraltrialsforthe
initialpost‐operativeperiodafterTHAandTKA.Thecombinedresultsshoweda
significantlyreducedriskofsymptomaticDVTassociatedwithLMWH(RR0.68,95%
CI0.6‐0.78),whereastheyfailedtoestablishorrefuteadifferenceinPE(RR0.68,95%
CI0.22‐2.1)(10).
Withregardtotheextendedprophylaxis,onlyonetrialenrollingmorethan1200
patientscomparedLMWHwithVKA.TherewerenoPEintheLMWHgroupas
comparedto4outof636intheVKAgroup.Nostatisticallysignificantdifferencewas
foundintherateofasymptomaticDVTintheVKAarmascomparedtoLMWHarm(RR,
1.35;95%CI,0.70‐2.6)(28).
‐LMWHversusaspirin(ASA)(Table9)
Evidenceislimitedforthehead‐to‐headcomparisonbetweenLMWHandASA.The
pooledestimatefromtwotrialsinpatientsundergoingTHAorTKAshowedahigher
incidenceofasymptomaticDVTassociatedwithaspirincomparedtoLMWH(RR1.87,

14
95%CI1.3‐2.7),whereasPEweretoofewtoprovideanaccurateestimateandno
majorbleedingeventswerereported(10,29,30)
‐LMWHversusfondaparinux(Table10)
SeverallargetrialscomparedfondaparinuxwithLMWHfortheinitialVTEprophylaxis
aftermajororthopedicsurgery.Thepooledresultsfailedtodemonstrateorexcludea
beneficialeffectoffondaparinuxonsymptomaticDVT(RR1.31,0.47‐3.7)andPE(RR
1.32,0.37‐4.74)(10).
‐LMWHversusneworalanticoagulants(Table11)
Severaltrialshavebeenconductedmorerecentlytocompareanewgenerationoforal
anticogulantdrugs(twodirectfactor‐Xainhibitors,rivaroxabanandapixaban,andone
directthrombininhibitor,dabigatran)withLMWHafterTKAorTHA.
Morethan10000patientswereenrolledinrandomizedcontrolledtrials(RCTs)
comparingrivaroxabanwithLMWH.Thepooledresultsshowedastatistically
significantreductioninsymptomaticDVTinrivaroxabanarms(RR0.41,95%CI0.2‐
0.83),whereastheyfailedtotodemonstrateorexcludeabeneficialeffectof
rivaroxabanonPE(RR1.34,95%CI0.39‐4.6)(10).
FourRCTscompareddabigatranwithLMWHinpatientsundergoingTHAorTKA,
enrollingmorethan10000patients.Thepooledestimatesfailedtodemonstrateor
excludeadifferenceinthenumberofsymptomaticVTEsforbothdabigatrandose
regimensof220mg(PE:RR1.22,95%CI,0.52‐2.85;DVT:RR0.7,95%CI0.12‐3.91)
and150mg(PE:RR0.31,95%CI0.04‐2.48;DVT:RR1.52,95%CI0.45‐5.05),as
comparedtoLMWH(10).
Finally,apixabanwascomparedtoLMWHinfourRCTsenrollingmorethan12000
patientsundergoingTHAorTKA.Thepooledanalysisfoundthatapixabansignificantly
reducedsymptomaticDVTby59%(RR0.41,95%CI0.18‐0.95),butfailedto

15
demonstrateabeneficialordetrimentaleffectonnonfatalPE(RR1.09,95%CI0.31‐
3.88)(10).
‐LMWHversusmechanicalprophylaxis(Table12)
Pneumaticcompressiondevices(i.e.intermittentpneumaticcompressiondeviceand
venousfootpump)werecomparedwithLMWHinmorethan1000patients
undergoingTHAandTKA.Overall,therewastrendassociatedwithcompression
devicestowardanincreaseinasymptomaticDVT(RR1.38,95%CI0.92‐2.06)andin
nonfatalPE(RR2.92,0.12‐71),evenifnotstatisticallysignificant(10).
Basedontheavailableevidence,in2012theAmericanCollegeofChestPhysician
providedanupdatedversionoftheevidence‐basedclinicalpracticeguidelinesforthe
preventionofthrombosisinorthopedicsurgicalpatients(10).Similarlytothe
methodologyusedfornon‐orthopedicsurgery,theGradingofRecommendations
Assessment,DevelopmentandEvaluation(GRADE)systemwasusedtoassessthe
evidenceandtoformulatetherecommendations(Table3)(26).
Inthecontextoforthopedicsurgery,therecommendationsontheuseof
thromboprophylaxisarebasedonatrade‐offbetweentheriskofVTEandtheriskof
majorbleedingaftersurgery.Formajororthopedicsurgery,differentlyfromnon‐
orthopedicsurgery,thesurgery‐specificriskofVTEfaroutweightsthecontributionof
thepatient‐specificfactors.Indeed,noindividualriskestimationwassufficiently
secureinthisclinicalcontexttomandatedifferentrecommendationsfordifferentrisk
strata.Therefore,recommendationsforthepreventionofVTEinorthopedicsurgery
(summarizedinTable13)arenotbasedonanindividualstratificationoftheriskof
VTEandbleeding.
16
11. Summaryofcomparativeevidenceonsafety(descriptionofadverse
effects/reactions;identificationofvariationinsafetyduetohealthsystemsand
patientfactors;summaryofcomparativesafetyagainstcomparators)including
summaryevidencetableswithGradingofrecommendations
TheevaluationofsafetyrelatedtoLMWHincludeshemorrhagicandnonhemorrhagic
complications.
Hemorrhagiccomplications
Withregardtotheriskofbleedingassociatedwiththeuseofthromboprophylaxis
aftersurgicalintervention,adistinctionbetweenorthopedicandnon‐orthopedic
surgeryismadeandthetwogroupsofsurgeryarepresentedseparatelyhereafter.
NonOrthopedicsurgery
‐LMWHversusnoprophylaxis(Table14)
Ameta‐analysisofeighttrialsconductedingeneralandabdominalsurgeryshowedan
approximatedoublingoftheriskofmajorbleeding(RR2.03,95%CI1.37‐3.01)and
woundhematoma(RR1.88,95%CI1.54‐2.28)associatedwithLMWH,ascomparedto
noprohylaxis(20).Thesedatahavebeenmorerecentlyconfirmedinameta‐analysis
whichincludedstudiesofgastrointestinal,gynecologic,urological,andthoracic
surgery(21).
‐LMWHversusLDUH(Table14)
Resultsfromameta‐analysisof51trialsonmorethan48000generalandabdominal
surgerypatientsfailedtodemonstrateortoexcludeabeneficialeffectofLMWHas
comparedtoLDUHonmajorbleedingandwoundhematoma(RR0.89,95%CI0.75‐
1.05)(20).Thesedatahavebeenconfirmedinamorerecentmeta‐analysisincluding
gastrointestinal,gynecologic,urological,andthoracicpatients(21).

17
‐LMWHversusfondaparinux
Arandomizedcontrolledtrialcomparedfondaparinuxtodalteparininpatientsathigh
riskofVTEwhounderwentabdominalsurgery(22).Theresultsshowedapossible
increaseintheriskofnonfatalmajorbleedingwithfondaparinux(RR1.43,95%CI
0.93‐2.21),butdifferencesintherisksoffatalbleedingandbleedingrequiring
reoperationwereneitherconfirmednorexcluded.
‐LMWHversusmechanicalprophylaxis
Specificdataforthiscomparisonarelimitedtoonestudyontraumapatients(23)and
onestudyongynecologiconcologypatients(24).Inthefirsttrialtherewasno
statisticallysignificantdifferenceintherateofmajorbleedingbetweenpatientswho
receivedLMWHascomparedtointermittentpneumaticcompression(4ineach
group).Intheothertrial,thefrequencyofbleedingcomplications,measuredbythe
numberofrequiredperioperativetransfusions,andestimatedintraoperativeblood
losswassimilarbetweenthetwogroups.
Asubgroupanalysisofarecentmeta‐analysis(25,28),thatcomparedalltypesof
mechanicalcompression(pneumaticcompression,footcompressionandgraduated
compressionstockings)toLMWHinseveralgroupsofsurgicalpatients,including
orthopedicones,foundastatisticallysignificantreductionintheriskofmajorbleeding
withcompressiondevicesascomparedtoLMWH(RR0.51,95%CI0.40,0.64)
‐NotrialsareavailableforcomparisonofLMWHwithaspirin,warfarinorneworal
anticoagulants.
Orthopedicsurgery(Table15)
‐LMWHversusnoprophylaxis

18
Inmajororthopedicsurgery,thebaselineriskofmajorbleedingwasestimatedforthe
initialpost‐operativeperiod(days0to14)fromtheplaceboarmofLMWHtrials,
resultinginamedianrateof1.5%(10).Thisestimateisconsistentwiththatfoundina
systematicreview,rangingfrom1%to2%(27).Theexpectedriskofmajorbleeding
withLMWHhasbeenshowntobeveryclosetothatofplacebo,withalargeCI(RR
0.81,95%CI0.38‐1.72)(10,31).
Similarly,intheextendedpost‐operativeperiod(days15to35),resultsfromameta‐
analysisfailedtodemonstrateorexcludeaneffectofLMWHonmajorbleeding(RR
0.43,95%CI0.11‐1.65)(10).
‐LMWHversusLDUH
LMWHandLDUHhavebeencomparedintheinitialprophylaxisaftermajor
orthopedicsurgery.Asubgroupanalysisofasystematicreviewoftrialscomparing
LMWHandUFHincluded2800patientswhounderwentarthroplastyorHFS(27).The
pooledanalysisfailedtodemonstrateorexcludeabeneficialeffectofLMWHas
comparedtoUFH(RR0.91,95%CI0.75‐1.09).
‐LMWHversusVKAs
LMWHhasbeencomparedtoVKAsinmorethan9000patientsinseveraltrialsforthe
initialpost‐operativeperiodafterTHAandTKA.Thecombinedresultsshowedno
significantdifferenceinmajorbleedingevents(RR1.36,95%CI0.95‐1.96).
Withregardtotheextendedprophylaxis,onlyonetrialenrollingmorethan1200
patientscomparedLMWHwithVKA.Asubstantialincreaseinmajorbleedingwas
foundwithVKAs(RR3.9,95%CI1.9‐8.1)(10).
‐LMWHversusaspirin(ASA)

19
Evidenceislimitedforthehead‐to‐headcomparisonbetweenLMWHandASA.Inthe
twotrialsinpatientsundergoingTHAorTKAnomajorbleedingeventswerereported
inbotharms(29,30).
‐LMWHversusfondaparinux
SeverallargetrialscomparedfondaparinuxwithLMWHfortheinitialVTEprophylaxis
aftermajororthopedicsurgery.Thepooledresultsshowasignificantincreasein
bleedingrequiringre‐operationassociatedwithfondaparinux(RR1.85,95%CI1.1‐
3.11),eveniftherewasnotastatisticallysignificantdifferenceintherateofmajor
bleeding(RR1.35,95%CI0.89‐2.05)(10).
‐LMWHversusneworalanticoagulants
Severaltrialshavebeenrecentlyconductedtocompareanewgenerationoforal
anticogulantdrugs(twodirectfactor‐Xainhibitors,rivaroxabanandapixaban,andone
directthrombininhibitor,dabigatran)withLMWHafterTKAorTHA.
Withregardtorivaroxaban,inapooledanalysisofseventrialsenrollingmorethan
10000patients,therewasatrendtowardincreasedmajorbleedingandbleeding
requiringreoperation,althoughnotstatisticallysignificant(majorbleeding:RR1.58
95%CI,0.84‐2.97;bleedingrequiringreoperation:RR2.095%CI0.86‐4.83;
combined:RR1.73,95%CI,0.94‐3.17)(10).
FourRCTscompareddabigatranwithLMWHinpatientsundergoingTHAorTKA,
enrollingmorethan10000patients.Thepooledestimatesfailedtodemonstrateor
excludeadifferenceinthenumberofmajorbleedingeventsforbothdabigatran
dosageregimensof220mg(RR1.06,95%CI,0.66‐1.72)and150mg(RR0.71,95%CI
0.42‐1.19)(10).

20
Finally,apixabanwascomparedtoLMWHinfourRCTsenrollingmorethan12000
patientsundergoingTHAorTKA.Thepooledanalysisfailedtodemonstrateorexclude
adifferenceinthenumberofmajorbleeding(RR0.76,95%CI0.44‐1.32)(10).
‐LMWHversusmechanicalprophylaxis
Pneumaticcompressiondevices(i.e.intermittentpneumaticcompressiondeviceand
venousfootpump)werecomparedwithLMWHinmorethan1000patients
undergoingTHAandTKA.Thepooledanalysisshowedastatisticallysignificant
reductionoftheriskofmajorbleedingassociatedwithcompressiondevices(RR,0.32,
95%CI0.12‐0.89)(10).
Non‐hemorrhagiccomplications
Heparininducedthrombocytopenia(HIT).Thispotentiallyseverecomplicationis
representedbyafallinplateletcountafterexposuretoheparinandanassociatedpro‐
thromboticsyndrome.Indeed,heparin‐dependentIgGantibodiesbindto
multimolecularcomplexesconsistingofplateletfactor4boundtoheparin,thus
causingplateletsactivation(withreleaseofhighlyprothromboticmicroparticles)and
theirremovalfromthecirculation(withconsequentthrombocytopenia).
SeveralfactorsinfluencetheincidenceofHIT,includingthetypeandpreparationof
heparin(UFHorLMWH)andtheheparin‐exposedpatientpopulation,withthe
postoperativepatientspresentingahigherrisk.
ArecentCochranesystematicreviewandmeta‐analysisspecificallycomparedthe
incidenceofHITafterexposuretoUFHorLMWHafteranysurgicalintervention.The
resultsshowastatisticallysignificantreductionintheriskofHITwithLMWHas
comparedtoUFH(riskratio0.24,95%CI0.07‐0.82)(32).

21
Osteoporosis.Inadditiontoitsanticoagulanteffects,heparinbindstoanumber
ofproteinsandcells,includingosteoblasts,whichthenreleasefactorsthatactivate
osteoclastsandpromoteboneloss.ComparedtoUFH,LWMHhasloweraffinityfor
proteinsandcells,resultingalsoinadecreasedbindingtoosteoblasts.
Long‐termuseofUFHhasbeenassociatedwitha2.2–5%incidenceofheparin‐induced
osteoporoticfracture,butaccuratedataforLMWHdataarescarce.Indeed,arecent
systematicreviewidentifiedonly9casesofLMWH‐inducedosteoporosisfrom13
articles(33).Withregardtothecomparisonoftheriskofosteoporosisbetween
heparins,onlytwosmalltrialshavebeenconducted,bothinpregnantwomenwho
havebeenassignedtoreceiveprophylacticdosesofUFHorLMWHduringpregnancy.
Inthefirsttrial,meanbonedensityofthelumbarspinewassignificantlylowerinthe
UFHgroupthanintheLWMHgroup.Moreover,bonedensitymeasurementsdidnot
differbetweentheLMWHgroupandacontrolgroupofhealthyuntreatedwomen(34).
Inthesecondtrial,oneoutof49women(2.3%)intheLMWHgrouphadsignificant
bonelossatthetotalproximalfemur(definedasadecreaseof>10%),comparedwith
noneofthe40patientsintheUFHgroup(35).Theauthorsoftheabovementioned
systematicreviewconcludethat,untillargeclinicaltrialsaredesignedtoinvestigate
pre‐andpost‐treatmentbonedensityandtocomparedifferentdosagesofLMWH
effectonthebonedensityindifferentpatientgroups,noaccurateconclusionscanbe
madeontheriskofosteoporosisrelatedtoLMWH.
12. Summaryofavailabledataoncomparativecostsandcost‐effectivenesswithin
thepharmacologicalclassortherapeuticgroup(rangeofcostsoftheproposed
medicine;comparativecost‐effectivenesspresentedasrangeofcostperroutine
outcome)

22
CollectingdatafromdifferentcountiesincludingAlgeria,Argentina,Brazil,India,Morocco,
Thailand,Tunisia,andUganda,thecostsofprophylacticdosesofLMWHrangedfrom2.25
to9.5USDperdoseforthe20mgprophylacticdoseofenoxaparin(20mg)to4.75to18.5
USDperdoseforthe40mgprophylacticdoseofenoxaparin,thatisthemostwidelyused
LMWHacrosscountries.BiosimilarLMWHcanbefoundatlowercosts,whereavailable.
Studiesassessingthecost‐effectivenessofVTEprophylaxisinhospitalizedpatientshave
beencarriedoutinWesterncountries.Theuseofpharmacologicprophylaxiswasrecently
confirmedtobeassociatedwithsubstantialcostsavingsinstudiesfromAustralia,Europe
andNorthAmerica(36‐38).ThetotalcostofprophylaxiswithLMWHwaslowerthanthe
costwithUFHinapopulationofhighriskmedicalpatients(39).Nocost‐effectiveness
studiesofVTEprophylaxisareavailablefromdevelopingcountries.However,cost‐
effectivenessstudiescomparingLMWHandUFHforthetreatmentofacuteVTEfrom
ChinaandBrazilfoundlowercostswiththeformerthanwiththelatter(40,41).
Regulatoryinformation
13. Summaryofregulatorystatusofthemedicine(differentcountries)
Inallcountries,LMWHisapprovedforthepreventionofVTEinsurgicalpatientswith
moderateorhighriskforVTE;forthepreventionofVTEinmedicalpatientswith
congestiveheartfailure(NYHAclassIIIorIV),respiratoryfailure,acuteinfectionoracute
rheumatologicdiseasewithatleastoneriskfactorforVTE;forthepreventionofblood
clotintheextra‐corporealcirculationduringhemodialysis;fortreatmentofDVTwithor
withoutPE;forthetreatmentofunstableanginaandnon‐Q‐waveAMI(inconjunction
withaspirin);forthetreatmentofAMIwithST‐segmentelevation.Indicationsmayvary
acrossLMWHs

23
14. Availabilityofpharmacopoeialstandards
BritishPharmacopoeia:Yes
InternationalPharmacopoeia:Yes
UnitedStatesPharmacopoeia:Yes
EuropeanPharmacopoeia:Yes
15. ProposedtextfortheWHOModelFormulary
Basedoncurrentevidence,medicinesinthefollowingtwoclassesofparenteral
anticoagulants(UFHandLWMH)areincludedasessentialmedicinesforthe
preventionofvenousthromboembolisminhospitalizedpatientsundergoinghighrisk
surgicalprocedures(e.g.cancersurgeryandmajororthopedicsurgery).WHO
recommendsandendorsesthelocalimplementationofprotocolsforVTEprevention
andemphasizestheimportanceofusingtheseproductsinaccordancewith
internationalandnationalguidelines.LMWHhaveadvantagesoverUFHandshouldbe
preferredwhereavailable.

24
References
1) MartinezC,CohenAT,BamberL,RietbrockS.Epidemiologyoffirstandrecurrent
venousthromboembolism:Apopulation‐basedcohortstudyinpatientswithoutactive
cancer.ThrombHaemost2014Apr3;112(2)[Epubaheadofprint]
2) SpencerFA,EmeryC,LessardD,AndersonF,EmaniS,AragamJ,BeckerRC,Goldberg
RJ.TheWorcesterVenousThromboembolismStudy.Apopulation‐basedstudyofthe
clinicalepidemiologyofvenousthromboembolism.JGenInternMed2006;21:722‐727
3) HoWK,HankeyGJ,EikelboomJW.Theincidenceofvenousthromboembolism:a
prospective,community‐basedstudyinPerth,WesternAustralia.MedJAustr
2008;189:144‐147
4) CushmanM,TsaiAW,WhiteRH,HeckbertSR,RosamondWD,EnrightP,FolsomAR.
Deepveinthrombosisandpulmonaryembolismmintwocohorts:thelongitudinal
investigationofthromboembolismetiology.AmJMed2004;117:19‐25
5) AgenoW,SquizzatoA,GarciaD,ImbertiD.Epidemiologyandriskfactorsofvenous
thromboembolism.SeminThrombHemost2006;32:651‐658
6) SteinPD,KayaliF,OlsonRE,MilfordCE.Pulmonarythromboembolismin
Asians/PacificIslandersintheUnitedStates:AnalysisofDatafromtheNational
HospitalDischargeSurveyandtheUnitedStatesBureauoftheCensus.AmJMed
2004;116:435‐442
7) WhiteRH,ZhouH,RomanoPS.Incidenceofidiopathicdeepvenousthrombosisand
secondarythromboembolismamongethnicgroupsinCalifornia.AnnInternMed
1998;128:737‐740

25
8) AgenoW,AgnelliG,ImbertiD,MoiaM,PalaretiG,PistelliR,VersoM.Prevalenceofrisk
factorsforvenousthromboembolismintheItalianpopulation:resultsofacross‐
sectionalstudyfromtheMasterRegistry.InternEmergMed2011
9) GeertsWH,BergqvistD,PineoGP,HeitJA,SamamaCM,LassenMR,ColwellCW.
PreventionofVenousThromboembolism:AmericanCollegeofChestPhysicians
Evidence‐BasedClinicalPracticeGuidelines(8thEdition).Chest2004;126(3Suppl):
338S‐400S
10) Falck‐YtterY,FrancisCW,JohansonNA,CurleyC,DahlOE,SchulmanS,OrtelTL,
PaukerSG,ColwellCW.PreventionofVTEinorthopaedicsurgerypatients.
AntithromboticTherapyandPreventionofThrombosis,9thed:AmericanCollegeof
ChestPhysiciansEvidence‐BasedClinicalPracticeGuidelines.Chest
2012;141(2(suppl):e278S‐e325S
11) AgnelliG,BolisG,CapussottiL,ScarpaRM,TonelliF,BonizzoniE,MoiaM,ParazziniF,
RossiR,SonagliaF,ValaraniB,BianchiniC,GussoniG.Aclinicaloutcome‐based
prospectivestudyonvenousthromboembolismaftercancersurgery:the@RISTOS
project.AnnSurg2006;243(1):89‐95
12) GouldMK,GarciaDA,WrenSM,KaranicolasPJ,ArcelusJI,HeitJA,SamamaCM.
PreventionofVTEinNonorthopedicSurgicalPatients.AntithromboticTherapyand
PreventionofThrombosis,9thed:AmericanCollegeofChestPhysiciansEvidence‐
BasedClinicalPracticeGuidelines.Chest2012;141(2(suppl):e227S‐e277S
13) CohenAT,TapsonVF,BergmannJF,GoldhaberSZ,KakkarAK,DeslandesB,HuangW,
ZayaruznyM,EmeryL,AndersonFA.Venousthromboembolismriskandprophylaxis
intheacutehospitalcaresetting(ENDORSEstudy):amultinationalcross‐sectional
study.Lancet2008;371:387‐394

26
14) JangMJ,BangS‐M,OhD.IncidenceofvenousthromboembolisminKorea:fromthe
HealthInsuranceReviewandAssessmentServicedatabase.JThrombHaemost
2011:9:85‐91
15) KishimotoM,LimHY,TokudaY,NaritaM,KitazonoH,ItoH,SetoTB,SumidaKN,
GelberRP.PrevalenceofvenousthromboembolismatateachinghospitalinOkinawa,
Japan.ThrombHaemost2005;93:876‐879
16) NgHJ,LeeLH.Trendsinprevalenceofdeepvenousthrombosisamonghospitalized
patientsinanAsianinstitution.ThrombHaemost2009;101:1095‐1099
17) LeizoroviczA,TurpieAGG,CohenAT,WongL,YooMC,DansA.Epidemiologyof
venousthromboembolisminAsianpatientsundergoingmajororthopaedicsurgery
withoutthromboprophylaxis.TheSMARTStudy.JThrombHaemost2004;2:1‐7
18) BaSA,BadianeSB,DiopSN,DioufFS,FallD,KaMM,KaneA,NdiayeM.Across‐
sectionalevaluationofvenousthromboembolismriskanduseofvenous
thromboembolismprophylaxisinhospitalizedpatientsinSenegal.ArchCardiovascDis
2011;104:493‐501
19) Linkins LA, Dans AL, Moores LK, Bona R, Davidson BL, Schulman S, Crowther M.
Treatment and prevention of heparin‐induced thrombocytopenia. Antithrombotic
TherapyandPreventionofThrombosis,9thed:AmericanCollegeofChestPhysicians
Evidence‐BasedClinicalPracticeGuidelines.Chest2012;141(2(suppl):e495S‐e530S
20) MismettiP,LaporteS,DarmonJY,BuchmullerA,DecoususH.Meta‐analysisoflow
molecularweightheparininthepre‐ventionofvenousthromboembolismingeneral
surgery.BrJSurg.2001;88(7):913‐930.
21) NationalCollaboratingCentreforAcuteCare.VenousThromboembolism:Reducingthe
RiskofVenousThrombo‐embolism(DeepVeinThrombosisAndPulmonary
Embolism)inPatientsAdmittedtoHospital.London,England:NICE;2010

27
22) AgnelliG,BergqvistD,CohenAT,GallusAS,GentM;PEGASUSinvestigators.
Randomizedclinicaltrialofpost‐operativefondaparinuxversusperioperative
dalteparinforpreventionofvenousthromboembolisminhigh‐riskabdominalsurgery.
BrJSurg.2005;92(10):1212‐1220.
23) GinzburgE,CohnSM,LopezJ,JackowskiJ,BrownM,HameedSM.Randomizedclinical
trialofintermittentpneumaticcompressionandlowmolecularweightheparinin
trauma.BrJSurg2003;90:1338–1344
24) MaxwellGL,SynanI,DodgeR,CarrollB,Clarke‐PearsonDL.Pneumaticcompression
versuslowmolecularweighthepariningynecologiconcologysurgery:arandomized
trial.ObstetGynecol2001;98:989–995
25) EppsteinerRW,ShinJJ,JohnsonJ,vanDamRM.Mechanicalcompressionversus
subcutaneousheparintherapyinpost‐operativeandposttraumapatients:a
systematicreviewandmeta‐analysis.WorldJSurg.2010;34(1):10‐19.
26) GuyattGH,NorrisSL,SchulmanS,HirshJ,EckmanMH,AklEA,CrowtherM,Vandvik
PO,EikelboomJW,McDonaghMS,LewisSZ,GuttermanDD,CookDJ,SchünemannHJ;
AmericanCollegeofChestPhysicians.Methodologyforthedevelopmentof
antithrombotictherapyandpreventionofthrombosisguidelines:Antithrombotic
TherapyandPreventionofThrombosis,9thed:AmericanCollegeofChestPhysicians
Evidence‐BasedClinicalPracticeGuidelines.Chest.2012Feb;141(2Suppl):53S‐70S
27) HillJ,TreasureT;NationalClinicalGuidelineCentreforAcuteandChronicConditions.
Reducingtheriskofvenousthromboembolisminpatientsadmittedtohospital:
summaryofNICEguidance.BMJ.2010;340:c95
28) SamamaCM,VrayM,BarreJ,etal;SACREStudyInvestigators.Extendedvenous
thromboembolismprophylaxisaftertotalhipreplacement:acomparisonoflow‐
28
molecular‐weightheparinwithoralanticoagulant.ArchInternMed.
2002;162(19):2191‐2196
29) WestrichGH,BottnerF,WindsorRE,LaskinRS,HaasSB,SculcoTP.VenaFlowplus
LovenoxvsVenaFlowplusaspirinforthromboembolicdiseaseprophylaxisintotal
kneearthroplasty.JArthroplasty.2006;21(6suppl2):139‐143
30) GraorRASJ,LotkePA,DavidsonBL.RDheparin(arde‐parinsodium)vs.aspirinto
preventdeepvenousthrombo‐sisafterhiporkneereplacementsurgery[abstract].
Chest.1992;102(suppl):118S.
31) DahlOE,QuinlanDJ,BergqvistD,EikelboomJW.Acriticalappraisalofbleedingevents
reportedinvenousthromboembolismpreventiontrialsofpatientsundergoinghipand
kneearthroplasty.JThrombHaemost.2010;8(9):1966‐1975.
32) JunqueiraDR,PeriniE,PenholatiRR,CarvalhoMG.Unfractionatedheparinversuslow
molecularweightheparinforavoidingheparin‐inducedthrombocytopeniain
postoperativepatients.CochraneDatabaseSystRev.2012Sep12;9:CD007557
33) LefkouE,KhamashtaM,HampsonG,HuntBJ.Review:Low‐molecular‐weightheparin‐
inducedosteoporosisandosteoporoticfractures:amythoranexistingentity?Lupus
2010;19:3‐12.
34) PettilaV,LeinonenP,MarkkolaA,HiilesmaaV,KaajaR.Postpartumbonemineral
densityinwomentreatedforthromboprophylaxiswithunfractionatedheparinor
LMWheparin.ThrombHaemost.2002;87(2):182‐186
35) CaseleH,HaneyEI, JamesA, Rosene‐MontellaK, CarsonM.Bone density changes in
women who receive thromboprophylaxis in pregnancy. Am J Obstet Gynecol 2006;
195:1109–1113.

29
36) Duff J, Walker K, Omari A, Stratton C. Prevention of venous thromboembolism in
hospitalizedpatients:analysisofreducedcostandimprovedclinicaloutcomes.JVasc
Nurs2013;31:9‐14
37) Gussoni G, Foglia E, Frasson S, Casartelli L, Campanini M, Bonfanti M, Colombo F,
Porazzi E, AgenoW, Vescovo G,Mazzone A. Real‐world economic burden of venous
thromboembolismandantithromboticprophylaxisinmedicalinpatients.ThrombRes
2013;131:17‐23
38) VekemanF,LaMori JC,LalibertèF,NutescuE,DuhMS,BookhartBK,Schein J,DeaK,
OlsonWH,LefebvreP.In‐hospitalriskofvenousthromboembolismandbleedingand
associated costs for patients undergoing total hip or knee arthroplasty. J Med Econ
2012;15:644‐653
39) PineoG,LinJ,SternL,SubrahmanianT,AnnemansL.Economicimpactofenoxaparin
versus unfractionated heparin for venous thromboembolism prophylaxis in patients
with acute ischemic stroke: a hospital perspective of the PREVAIL trial. J HospMed
2012;7:176‐182
40) Chen L, Ying K, HongW, Zhou P. Comparison of lowmolecularweight heparin and
unfractionatedheparinforacutePTE.JZhejiangUnivScienceB2005;6:1195‐1199
41) ArgentaC,PiresFerreiraMA,BeckerSanderG,BeltramiMoreiraL.Short‐termtherapy
with enoxaparin or unfractionated heparin for venous thromboembolism in
hospitalizedpatients:utilizationstudyandcost‐minimizationanalysis.ValueinHealth
2011;14:S89‐S92

30
31
Table1.RiskofVTEinnonorthopedicsurgery:LMWHversusnoprophylaxisOutcomes Baselinerisk RiskLMWH
(95%CI)Relativeeffect(95%CI)
FatalPE Lowrisk RR0.54(0.27‐1.1)3per1000 2per1000(1‐3)
Intermediaterisk6per1000 3per1000 (2‐7)
Highrisk12per1000 6per1000(3‐13)
SymptomaticVTE Lowrisk RR0.31(0.12‐0.81)15per1000 5per1000(2‐12)
Intermediaterisk30per1000 9per1000(4‐24)
Highrisk60per1000 19per1000(7‐49)
Table2.RiskofVTEinnonorthopedicsurgery:LMWHversusLDUHOutcomes RiskLDUH RiskLMWH(95%
CI)Relativeeffect(95%CI)
FatalPE Lowrisk RR1.04(0.89‐1.2)3per1000 3 per1000(1‐3)
Intermediaterisk6per1000 6 per1000(2‐7)
Highrisk12per1000 12 per1000(3‐13)
SymptomaticVTE Lowrisk RR0.71(0.51‐0.99)7per1000 5per1000(4‐7)
Intermediaterisk13per1000 9per1000(7‐13)
Highrisk26per1000 18 per1000(13‐26)
32
Table3.Strenghtofrecommendationsgradingsystem
GradeofRecommendation BenefitvsRiskandBurdens
MethodologicStrengthofSupportingEvidence
Strongrecommendation,high‐qualityevidence(1A)
Benefitsclearlyoutweighriskandburdensorviceversa
Consistentevidence fromrandomizedcontrolledtrialswithoutimportantlimitationsorexceptionallystrongevidencefromobservationalstudies
Strongrecommendation,moderate‐qualityevidence(1B)
Benefitsclearlyoutweighriskandburdensorviceversa
Evidencefromrandomizedcontrolledtrialswithimportantlimitations(inconsistentresults,methodologicflaws,indirectorimprecise)orverystrong
evidencefromobservationalstudies
Strongrecommendation,low‐orvery‐low‐qualityevidence(1C)
Benefitsclearlyoutweighriskandburdensorviceversa
Evidenceforatleastonecriticaloutcomefromobservational
studies,caseseries,orrandomizedcontrolledtrials,withseriousflawsorindirect
evidenceWeakrecommendation,high‐qualityevidence(2A)
Benefitscloselybalancedwithrisksandburden
Consistentevidencefromrandomizedcontrolledtrialswithoutimportantlimitationsorexceptionallystrongevidencefromobservationalstudies
Weakrecommendation,moderate‐qualityevidence(2B)
Benefitscloselybalanced withrisksandburden
Evidencefromrandomizedcontrolledtrialswithimportantlimitations(inconsistentresults,methodologicflaws,indirectorimprecise)orverystrong
evidencefromobservationalstudies
Weakrecommendation,low‐orvery‐low‐qualityevidence(2C)
Uncertaintyintheestimatesofbenefits,risks,andburden;
benefits,risk,andburdenmaybecloselybalanced
Evidenceforatleastonecriticaloutcomefromobservational
studies,caseseries,orrandomizedcontrolledtrials,withseriousflawsorindirect
evidence

33
Table4.Recommendationsforthromboprophylaxisinvariousriskgroupsinnonorthopedicsurgery RiskofmajorbleedingRiskofsymptomaticVTE
Averagerisk(~1%) Highrisk(~2%)orseverecomplications
Verylow(<0.5%) NospecificprophylaxisLow(~1.5%) MechanicalprophylaxisModerate(~3%) LMWH(Grade2B)or
LDUH(Grade2B)orMechanicalprophylaxis(Grade2C)
Mechanicalprophylaxis(Grade2C)
High(~6%) LMWH(Grade1B)or LDUH(Grade1B)plus
Mechanicalpropylaxis(Grade2C)
Mechanicalprophylaxisuntilriskofbleedingdiminishesand
pharmacologicprophylaxiscanbeadded(Grade2C)
Table5.RiskofVTEinmajororthopedicsurgery:LMWHversusnoprophylaxisOutcomes Baselinerisk Riskdifferencewith
LMWH(95%CI)Relativeeffect(95%CI)
NonfatalPE Initialprophylaxis 0.58(0.22‐1.47)10per1000 4fewerper1000
(from8fewerto5more)Extendedprophylaxis 0.24(0.04‐1.4)
5per1000 4fewerper1000(from5fewerto2more)
SymptomaticDVT Initialprophylaxis 0.5(0.43‐0.59)18per1000 9fewer per1000
(from7fewerto10fewer)Extendedprophylaxis 0.46(0.26‐0.82)
10per1000 5fewerper1000(from2fewerto7fewer)
Table6.RiskofVTEinmajororthopedicsurgery:LMWHversusLDUHOutcomes RiskLDUH Riskdifferencewith
LMWH(95%CI)Relativeeffect(95%CI)
PE Initialprophylaxis 0.78(0.49‐1.24)4per1000 1 fewerper1000
(from2fewerto1more)SymptomaticDVT Initialprophylaxis 0.80(0.73‐0.88)
12per1000 2fewer per1000(from2fewerto3fewer)

34
Table7.RiskofVTEinmajororthopedicsurgery:LMWHversusVKAs‐initialprophylaxisOutcomes RiskVKAs Riskdifferencewith
LMWH(95%CI)Relativeeffect(95%CI)
NonfatalPE Initialprophylaxis 0.68(0.22‐2.1)2per1000 1 fewerper1000
(from2fewerto3more)SymptomaticDVT Initialprophylaxis 0.68(0.6‐0.78)
5per1000 2fewer per1000(from1fewerto2fewer)
Table8.RiskofVTEinmajororthopedicsurgery:VKAsversusLMWH‐extendedprophylaxisOutcomes RiskLMWH RiskdifferencewithVKAs
(95%CI)Relativeeffect(95%CI)
NonfatalPE Extended prophylaxis 9.1(0.49‐169)6per1000 45 more per1000
(from5fewerto96more)SymptomaticDVT Extended prophylaxis 1.35(0.7‐2.6)
12per1000 4fewer per1000(from4fewerto20more)
Table9.RiskofVTEinmajororthopedicsurgery:ASAversusLMWHOutcomes RiskLMWH RiskdifferencewithASA
(95%CI)Relativeeffect(95%CI)
SymptomaticDVT Full35‐day prophylaxis 1.87(1.3‐2.7)12per1000 11more per1000
(from4moreto21more)Table10.RiskofVTEinmajororthopedicsurgery:fondaparinuxversusLMWHOutcomes RiskLMWH Riskdifferencewith
fondaparinux(95%CI)Relativeeffect(95%CI)
NonfatalPE Initialprophylaxis 1.32(0.37‐4.74)4per1000 1 more per1000
(from2fewerto13more)SymptomaticDVT Initialprophylaxis 1.31(0.47‐3.7)
8per1000 2more per1000(from4fewerto22more)

35
Table11.RiskofVTEinmajororthopedicsurgery:neworalanticoagulantsversusLMWHOutcomes Relativeeffect
(95%CI)NonfatalPE RiskLMWH Riskdifferencewith
rivaroxaban(95%CI)Full35‐d prophylaxis 1.34(0.39‐4.6)
6per1000 2 more per1000(from3fewerto20more)
RiskLMWH Riskdifferencewithdabigatran220mg(95%CI)
Full35‐d prophylaxis 1.22(0.52‐2.85)6per1000 1moreper1000
(from3fewerto10more)RiskLMWH Riskdifferencewith
dabigatran150mg(95%CI)Full35‐d prophylaxis 0.31(0.04‐2.48)
6per1000 4fewerper1000(from5fewerto8more)
RiskLMWH Riskdifferencewithapixaban(95%CI)
Full35‐d prophylaxis 1.09(0.31‐3.88)6per1000 0 moreper1000
(from4fewerto16more)SymptomaticDVT
RiskLMWH Riskdifferencewithrivaroxaban(95%CI)
Full35‐d prophylaxis 0.41(0.2‐0.83)12per1000 7fewerper1000
(from2fewerto10fewer)RiskLMWH Riskdifferencewith
dabigatran220mg(95%CI)Full35‐d prophylaxis 0.70(0.12‐3.91)
12per1000 4fewerper1000(from11fewerto36more)
RiskLMWH Riskdifferencewithdabigatran150mg(95%CI)
Full35‐d prophylaxis 1.52(0.45‐5.05)12per1000 6moreper1000
(from7fewerto51more)RiskLMWH Riskdifferencewith
apixaban(95%CI)Full35‐d prophylaxis 0.41(0.18‐0.95)
12per1000 7fewerper1000(from1fewerto10fewer)

36
Table12.RiskofVTEinmajororthopedicsurgery:mechanichalcompressionversusLMWHOutcomes RiskLMWH Riskdifferencewith
compressiondevices(95%CI)
Relativeeffect(95%CI)
NonfatalPE Initialprophylaxis 2.92(0.12‐71)4per1000 7moreper1000
(from3fewerto80more)SymptomaticDVT Initialprophylaxis 1.38(0.92‐2.06)
8per1000 3moreper1000(from1fewerto8more)
Table13.Recommendationsforthromboprophylaxisinorthopedicsurgery
THA TKA HFSInitialprophylaxis(minumumof10to14days)
LMWH,fondaparinux,apixaban,dabigatran,rivaroxaban,LDUH,VKA,aspirin(allGrade1B)
orICPD(Grade1C)
LMWH,fondaparinux,LDUH,VKA,aspirin(allGrade2B)
orIPCD(Grade1C)
Extendedprophylaxis(upto35days)Suggestiontoextendthromboprophylaxisupto35days(Grade2B)
IrrespectiveoflenghtoftreatmentorconcomitantIPCDLMWHinpreferencetofondaparinux,apixaban,dabigatran,rivaroxaban,LDUH(allGrade2B),VKA,aspirin(allgrade2C)
LMWHinpreferencetofondaparinux,LDUH
(allGrade2B),VKA,aspirin(allgrade2C)
Table14.Riskofmajorbleedinginnonorthopedicsurgery
Riskofmajorbleeding(95%CI) Relativeeffect(95%CI)Noprophylaxis LMWH RR2.03(1.37‐3.01)
Lowriskpopulation12per1000 24 per1000(16‐36)
Mediumriskpopulation22per1000 45 per1000(30‐66)
LDUH LMWH RR0.89(0.75‐1.05)Lowriskpopulation
19per1000 17 per1000(14‐20)Intermediaterisk
35per1000 31 per1000(26‐37)

37
Table15.RiskofmajorbleedinginmajororthopedicsurgeryRiskofmajorbleeding(95%CI) Relativeeffect
(95%CI)Noprophylaxis RiskdifferencewithLMWH(95%CI)
Initialprophylaxis 0.81(0.38‐1.72)15per1000 3fewerper1000
(from9fewerto11more)Extendedprophylaxis 0.43(0.11‐1.65)
5per1000 3fewer per1000(from4fewerto3more)
RiskLDUH RiskdifferencewithLMWH(95%CI)Initialprophylaxis 0.91(0.75‐1.09)
16per1000 1fewerper1000(from4fewerto1more)
RiskVKAs RiskdifferencewithLMWH(95%CI)Initialprophylaxis 1.36(0.95‐1.96)
11per1000 4moreper1000(from1fewerto11more)
RiskLMWH RiskdifferencewithVKAs (95%CI)Extendedprophylaxis 3.93(1.91‐8.11)
14per1000 41moreper1000(from13moreto100more)
RiskLMWH Riskdifferencewithfondaparinux(95%CI)
Initialprophylaxis 1.35(0.89‐2.05)15per1000 5more per1000
(from2fewerto16more)RiskLMWH Riskdifferencewithrivaroxaban
(95%CI)Full35‐dayprophylaxis 1.58(0.84‐2.97)
15per1000 9more per1000(from2fewerto30more)
RiskLMWH Riskdifferencewithdabigatran220mg(95%CI)
Full35‐dayprophylaxis 1.06(0.66‐1.72)15per1000 1moreper1000
(from5fewerto11more)RiskLMWH Riskdifferencewithdabigatran
150mg(95%CI)Full35‐dayprophylaxis 0.71(0.42‐1.19)
15per1000 4fewerper1000(from9fewerto3more)
RiskLMWH Riskdifferencewithapixaban(95%CI)
Full35‐dayprophylaxis 0.76(0.44‐1.32)15per1000 4fewerper1000
(from8fewerto5more)RiskLMWH Riskdifferencewith
compressiondevices(95%CI)Initialprophylaxis
15per1000 10fewerper1000(from2fewerto13fewer)
0.32(0.12‐0.89)