Embed Size (px)
Citation preview

Ethical committ
*Reprint req
Orthopaedics, R
Trust, Sharoe G
E-mail addre
J Shoulder Elbow Surg (2011) 20, e22-e25
1058-2746/$ - s
doi:10.1016/j.jse
www.elsevier.com/locate/ymse
Propionibacterium acnes infection of the elbow
Morgan Jones, MBChB, BSc*, Mamidi K. Kishore, MBBS, MSc,Daniel Redfern, MBBS, MA, FRCS Orth
Upper Limb Unit, Department of Orthopaedics, Royal Preston Hospital, Preston, Lancashire, UK
Isolated elbow joint infection is very rare, with littleinformation in the literature on the causative organism andclinical sequelae. Propionibacterium acnes is a rare butrecognized cause of osteomyelitis,7 septic arthritis,3 andprosthetic joint infection.6,10 There are no recorded cases ofelbow joint sepsis due to P acnes after a local injection intothe elbow joint. The only previous cases of osteomyelitis ofthe elbow caused by P acnes were described in 1977. Bothindividuals had significant comorbidities, including 70%burns and a puncture wound to the hand.
Case report
A 46-year-old healthy, right handedominant aircraft engineerpresented to the accident and emergency department complainingof a painful swollen left elbow. He had sustained a superficialabrasion to the lateral aspect of the left elbow during a mountainbiking accident 2 weeks previously. A clinical diagnosis ofsuperficial cellulitis (C-reactive protein, 54 mg/L) was made aftera review by a junior casualty officer. Empirical antibiotic therapywas started with flucloxacillin 1 g daily (ie, 250 mg four timesa day for 7 days, with orthopedic follow-up arranged at 1 week.
At the follow-up visit, the patient had symptoms of pain,reduced range of movement, and swelling, which were clinicallysuggestive of septic arthritis of the elbow. There did not appear tobe clinical evidence of olecranon bursitis. An aseptic joint aspi-ration yielded a nonpurulent effusion of clear synovial fluid. Themicrobiologic analysis of the joint aspirate was negative on Gramstain and did not suggest acute intraarticular joint infection, withno white blood cells, no evidence of crystals, and no organisms
ee approval was not required for this case report.
uests: Morgan Jones, MBChB, BSc, ST3 Trauma and
oyal Preston Hospital, Lancashire Teaching Hospitals
reen Lane, PR 2 9HT Lancashire, UK.
ss: [email protected] (M. Jones).
ee front matter � 2011 Journal of Shoulder and Elbow Surgery
.2011.02.016
seen on microscopy. After 3 days of incubation, the aspirate culturewas negative. Inflammatory makers were also within normalreference ranges at that time (C-reactive protein, 2 mg/dL;erythrocyte sedimentation rate, 6 mm/h).
After an initial 48-hour course of intravenous antibiotic treat-ment with flucloxacillin and benzylpenicillin, the patient had a fullpain-free range of movement. An extended course of oral flu-cloxacillin (500 mg daily) was prescribed, and the patient wasdischarged with further outpatient follow-up arranged.
At follow-up 6 weeks later, after a return to normal functionand regular sporting activities, the patient was complaining ofdiscomfort in the region of the lateral epicondyle. There was fullrange of pain-free elbow flexion, extension, pronation, and supi-nation, with localized tenderness over the common extensor originand no evidence of effusion or cellulitis. Pain was reproduced onwrist extension against resistance. Plain elbow radiographs werenormal at that time.
A computed tomography scan of the elbow showed noconvincing evidence of joint effusion, erosive, inflammatory, orseptic features. Inflammatorymarkers (white cell count, 6.7� 109/L;erythrocyte sedimentation rate, 14mm/h) were also not significantlyelevated at this time.
A diagnosis of tennis elbow/lateral epicondylitis was made,and a local steroid injection of 40 mg triamcinolone with 2 mL of0.5% Marcaine (AstraZeneca UK Ltd, Luton, UK) was per-formed. The patient initially reported a significant improvement insymptoms.
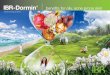
The patient presented 3 months later with pain, limited rangeof motion, deformity, and crepitus on movement of the left elbow.A plain radiograph of the elbow showed gross destruction of thecapitellum and humeroulna joint (Fig. 1). Magnetic resonanceimaging revealed gross destruction of the elbow joint, specificallyof the distal humerus and trochlea, with features suggestive ofosteomyelitis. The patient was referred to the senior author (D.R.)for further management.
An urgent joint aspirate was performed in the operating room,and 25 mL of clear, nonpurulent synovial fluid was aspirated.Aspirate culture at 72 hours was negative for microorganisms,
Board of Trustees.

Figure 1 (A) An anteroposterior radiograph demonstrates destruction of the elbow joint. (B) A l ateral elbow radiograph demonstrateselbow joint destruction.
Propionibacterium acnes infection of the elbow e23
with normal cytology and no evidence of crystal arthropathy.Inflammatory markers were all within normal limits. Washout,sequestrectomy, and bone biopsy was performed by the seniorauthor. Multiple intraoperative bone biopsy specimens of the distalhumerus and proximal ulna grew P acnes. An extended course ofamoxicillin was prescribed after sensitivity testing and discussionwith the resident consultant microbiologist.
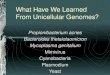
Given the gross joint destruction, a first-stage resectionarthroplasty was performed 3 months later, with insertion ofgentamicin beads at that time. Intraoperative samples taken werenegative on extended enriched culture. A right total elbowreplacement was performed 6 months later because the seniorauthor felt that this would give the patient the best chance ofa satisfactory functional outcome. At 6 months postoperatively,the patient had a satisfactory clinical outcome (Fig. 2), with anexcellent pain-free range of movement.
Discussion
P acnes is a low virulence nonespore-forming anaerobicgram-positive bacillus. P acnes is a major inhabitant ofadult human skin, where it resides within sebaceous folli-cles, usually as a harmless commensal.2
P acnes is a very unusual causative agent in joint or boneinfection. Few detailed clinical descriptions of the clinicalcourse or sequelae of such infections have been reported,with only a few published case reports.3,7,8 Infection (oste-omyelitis/septic arthritis) with Pacnes has been described inpatients with underlying illness,7 recent surgery,1 or in thepresence of prosthetic joint replacement.6 No isolated casesof P acnes osteomyelitis of the distal humerus have beenreported in a healthy individual with no prior orthopedicsurgery. Our patient was otherwise healthy, with no historyof P acnes infection, underlying illness, or immunosup-pressive conditions.
P acnes appears to have a higher rate of infection of theshoulder than any other joint in the body. It is recognized asa common cause of postoperative infection in rotator cuffrepair1 and is known to affect the shoulder joint propor-tionally more than the lower limb.5 P acnes is typicallyimplicated in prosthetic joint replacements of the upperlimb and after invasive procedures rather than as a causativeagent in spontaneous joint or bone infection.
The patient presented in this report initially presentedwith superficial cellulitis, with symptoms a week latersuggestive of septic arthritis. The diagnosis of acute septicarthritis was never confirmed on investigation. Joint aspi-rate, inflammatory markers, and an initial radiographicinvestigation did not point toward acute joint sepsis. It isworth noting that the patient had only moderate pain,inflammatory markers within normal reference rangesthroughout the initial presentation and follow-up (WCC,CRP, and ESR), and did not have a toxic appearance, asmight otherwise be expected in a patient with septicarthritis due to a more virulent bacteria such as Staphylo-coccus aureus. Despite this, the patient received a 6-weekextended course of antibiotic therapy in line with hospitalmicrobiology guidelines.
It appears from our experience and previous descriptionin the literature that P acnes infection runs a more insidiouscourse, with pseudoparalysis of the limb not beinga prominent feature in the early stages.3,7,8 This should beconsidered when confronted with a painful elbow ofunknown etiology where infection may form part of thedifferential diagnosis. The clinical picture may be some-what uncharacteristic for infection, and P acnes should beconsidered as part of this differential diagnosis. In addition,even during washout and drainage, there was no evidenceof a purulent offensive discharge, despite the radiographicchanges that were present.

Figure 2 (A) Postoperative anteroposterior radiograph of the elbow. (B) Postoperative lateral radiograph of the elbow.
e24 M. Jones et al.
It is not possible to state with absolute certainty that thesubsequent elbow joint destruction present in this patient5 months after initial presentation came about as a directconsequence of local corticosteroid injection, given theabsence of definite positive microbiologic or biochemicalinvestigation to suggest an infection. In our opinion, itwould seem a reasonable conclusion that the local steroidinjection after a recent history of possible infection wasinappropriate. The case, however, represents a diagnosticchallenge as well as highlighting the clinical sequelae of anemerging organism more commonly associated with pros-thetic joint infection and not previously described in asso-ciation with massive cartilage destruction.
Typically considered a contaminant in isolated jointaspirate, P acnes is a notoriously slow-growing organism. Itis important to ensure that extended culture of any jointaspirate is performed when a more atypical picture is sus-pected. Average culture time has been reported at11.4 days,6 whereas in the clinical laboratory, P acnes mostfrequently appears in blood cultures as a contaminantduring venepuncture.4 As a slow-growing gram-positiverod, early identification of P acnes as a causative organismin bone and joint infection represents a challenge to tradi-tional diagnostic testing (culture and sensitivity).
Florescence in situ hybridization (FISH) techniques mayoffer a more rapid solution. FISH allows microscopicvisualization of specific bacteria using fluorescently labeledoligonucleotide probes, which bind to unique complimen-tary target sites on ribosomal RNA. Identification time isless than 1 hour, with a reported sensitivity of 95% andspecificity of 100%.9 Accelerated identification of P acnesmay draw early attention to possibly pathogenic nonespore-forming gram-positive rods by quickly identifyingthem as P acnes. At a cost of less than V1 per test, selectiveapplication of this technology represents a powerful andcost-effective tool in early identification of P acnes infec-tion.9 Treatment usually involves an extended course ofantibiotics (the organism is typically penicillin-sensitive)
combined with removal of any infected prostheses andsurgical ablation of affected tissue.6
Conclusion
Although shoulder surgeons may be cognizant of therisks of P acnes, it has not previously been described asa causative organism in the destruction of the elbowjoint. The purpose of this case report is to draw attentionto P acnes as a causative organism in bone and jointinfection as well as to highlight the limited ability oftraditional diagnostic testing in early identification ofseptic arthritis. It should also be recognized that theclinical picture in the presence of P acnes infection maybe far more indolent than would be expected in classicaljoint infection. We suggest an alternative method forearly identification of P acnes when confronted witha painful elbow of unknown etiology. The risk of localcorticosteroid injection in the presence of unrecognizedlocal infection is highlighted.
Disclaimer
The authors, their immediate families, and any researchfoundations with which they are affiliated have notreceived any financial payments or other benefits fromany commercial entity related to the subject of thisarticle.
References
1. Athwal GS, Sperling JW, Rispoli DM, Cofield RH. Deep infection
after rotator cuff repair. J Shoulder Elbow Surg 2007;16:306-11. doi:
10.1016/j.jse.2006.05.013

Propionibacterium acnes infection of the elbow e25
2. Brook I, Frazier E. Infections caused by Propionibacterium acnes
species. Rev Infect Dis 1991;13:819-22.
3. Kooijmans-Coutinho MF, Markusse HM, Dijkmans BA. Infectious
arthritis caused by Propionibacterium acnes: a report of 2 cases. Ann
Rheum Dis 1989;48:851-2.
4. Lee CC, Lin WJ, Shih HI, Wu CJ, Chen PL, Lee HC, et al. Clinical
significance of potential contaminants in blood cultures among patients
in a medical center. J Microbiol Immuno Infect 2007;40:438-44.
5. Levy PY, Fenollar F, Stein A, Borrione F, Cohen E, Lebail B, et al.
Propionibacterium acnes postoperative shoulder arthritis: an emerging
clinical entity. Clin Infect Dis 2008;46:1884-6. doi:10.1086/588477
6. Lutz MF, Berthelot P, Fresard A, Cazorla C, Carricajo A, Vautrin AC,
et al. Arthroplastic and osteosynthetic infections due to Propioni-
bacterium acnes: a retrospective study of 52 cases, 1995-2002. Eur J
Clin Microbiol Infect Dis 2005;24:739-44. doi:10.1007/s10096-005-
0040-8
7. Morrey BF, Fitzgerald RH, Kelly PJ, Dobyns JH, Washington JA.
Diphtheroid osteomyelitis. J Bone Joint Surg Am 1977;59:527-30.
8. Noble RC, Overman SB. Propionibacterium acnes osteomyelitis: case
report and review of the literature. J Clin Microbiol 1987;25:251-4.
9. Poppert S, Riecker M, Essig A. Rapid identification of Propioni-
bacterium acnes from blood cultures by fluorescence in situ hybrid-
ization. Diagn Microbiol Infect Dis 2010;66:214-6. doi:10.1016/j.
diagmicrobio.2009.09.007
10. Zeller V, Ghorbani A, Strady C, Leonard P, Mamoudy P,
Desplaces N. Propionibacterium acnes: an agent of prosthetic joint
infection and colonization. J Infect 2007;55:119-24. doi:10.1016/j.
jinf.2007.02.006