Embed Size (px)
Citation preview

Substance Use & Misuse, Early Online:1–13, 2013Copyright C© 2013 Informa Healthcare USA, Inc.ISSN: 1082-6084 print / 1532-2491 onlineDOI: 10.3109/10826084.2013.800118
ORIGINAL ARTICLE
Promoting Abstinence From Alcohol During Pregnancy: ImplicationsFrom Formative Research
Kathryn E. France1, Robert J. Donovan2, Nadine Henley1, Carol Bower3, Elizabeth J. Elliott4,Janet M. Payne3, Heather D’Antoine3 and Anne E. Bartu5
1School of Marketing, Tourism and Leisure, Edith Cowan University, Joondalup, Australia; 2Centre for BehaviouralResearch in Cancer Control, Curtin University, Perth, Australia; 3Centre for Child Health Research, Telethon Institutefor Child Health Research, University of Western Australia, Perth, Australia; 4Discipline of Paediatrics and ChildHealth, University of Sydney, Westmead, Australia; 5School of Nursing and Midwifery, Curtin University, Perth,Australia
This research developed messages to promote absti-nence from alcohol during pregnancy and identifiedelements that enhance message persuasiveness. An ex-ploratory phase was conducted in 2009 that comprisedfour focus groups with 23 women inWestern Australiaand elicited beliefs and attitudes on alcohol use duringpregnancy and motivations for behavior change. Fourtelevision concepts were subsequently developed andappraised in five focus groups with 31 participantsusing standard advertising pretesting questions.The implications for campaigns addressing prenatalalcohol exposure and further research are noted andlimitations discussed. Funding was received fromHealthway and the National Health and MedicalResearch Council.
Keywords: alcohol, pregnancy, FASD, formative, messages,prevention, campaign
INTRODUCTION
Prenatal alcohol exposure is related to a range of physicaland neurodevelopmental effects on the fetus. Theseeffects are collectively known as Fetal Alcohol SpectrumDisorders (FASD). These disorders are estimated toaffect approximately 2%–5% of live-births in the UnitedStates and some Western European countries (Mayet al., 2009), and the effects have lifelong implicationsfor the affected individuals, their families, and theircommunities (Lupton, Burd, & Harwood, 2004; Olson,Oti, Gelo, & Beck, 2009; Streissguth, Barr, Kogan, &Bookstein, 1997). Strategies to prevent prenatal alcoholexposure include broad awareness-raising initiatives thattarget individuals’ knowledge, beliefs, and attitudes, and
Address correspondence to Kathryn E. France, School of Marketing, Tourism and Leisure, Edith Cowan University, 270 Joondalup Drive, Joondalup6027, Australia; E-mail: [email protected].
seek to create and reinforce a social context conduciveto alcohol abstinence (Deshpande et al., 2005). Thesecampaigns also serve to support tailored and clinicalinterventions addressing prenatal alcohol exposure suchas brief interventions in primary care settings, alcoholscreening, and specialized support for pregnant womenwith alcohol-related problems (Hankin, 2002; Poole,2008; Stratton, Howe, & Battaglia, 1996).
Though a large number of communication campaignsaddressing alcohol use during pregnancy have beenconducted, predominantly in North America, campaignsare rarely evaluated beyond measures of campaign recalland general awareness of the topic (Elliott, Coleman,Subebwongpat, & Norris, 2008; Saskatchewan Preven-tion Institute, 2009). Furthermore, recommendationsfor messaging are seldom related to theory or based onformative research, and hence there is little evidence toinform the design of effective messages (Cismaru, Desh-pande, Thurmeier, Lavack, & Agrey, 2010; SaskatchewanPrevention Institute, 2009). This lack of published infor-mation on the development and evaluation of campaignsmakes it difficult to determine what campaign elementsare most effective with respect to the desired targetaudiences’ behavioral intentions and behavior change.
Formative research is necessary for developing persua-sive, population-based messaging for a sensitive and com-plex issue such as alcohol use during pregnancy. Suchresearch often involves a number of phases, with a firstexploratory phase providing insight into the individualand social contexts into which the messages will be de-livered and received. Using qualitative research methods,the exploratory phase can elucidate the knowledge, atti-tudes, beliefs, and practices of the intendedmessage recip-ients with regard to their behavior, along with perceived
1
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Yal
e D
erm
atol
ogic
Sur
gery
on
08/0
2/13
For
pers
onal
use
onl
y.

2 K. E. FRANCE ET AL.
and actual barriers and facilitators of positive behaviorchange (Eitel & Delaney, 2004). These data are then usedto develop the communication objectives and overall mes-sage strategy, that is, to “get the right message” (Egger,Donovan, & Spark, 1993). A second concept developmentphase utilizes further research to identify specific con-tent and to ensure that execution elements have credibility,relevance, and appeal, that is, to “get the message right”(Egger et al., 1993). Formative research can also identifyexecution elements which inhibit acceptance of the mes-sage, as well as potential unintended messages that couldlead to maladaptive responses (Donovan, Jalleh, Fielder,& Ouschan, 2008).
The potential effectiveness of communication cam-paigns is also enhanced if message strategies areunderpinned by behavioral theory (Maibach & Parrott,1995). Social cognition models such as the HealthBelief Model (Becker, 1974; Rosenstock, 1974), SocialCognitive Theory (Bandura, 1977), Protection MotivationTheory (Rogers, 1975), and the Theory of ReasonedAction (Fishbein & Ajzen, 1975) describe constructs im-portant for instigating and maintaining behavior change,and are widely used in health promotion and healthcommunication. By profiling the context of the behavior,and the knowledge, attitudes, beliefs, expectancies, andmotivations of the target audience in terms of theoreticalconstructs, the effectiveness of message strategies canbe strengthened. Although a number of qualitative andquantitative studies have provided insights into women’sknowledge, beliefs, and attitudes with regards to alcoholuse during pregnancy (Balachova, Bonner, Isurina, &Tsvetkova, 2007; Baxter, Hirokawa, Lowe, Nathan, &Pearce, 2004; Kesmodel & Kesmodel, 2002; Raymond,Beer, Glazebrook, & Sayal, 2009; Toutain, 2010), fewdescribe formative research with the target audience thatwas used to develop message strategies aimed at prevent-ing prenatal alcohol exposure (Branco & Kaskutas, 2001;Glik, Prelip, Myerson, & Eilers, 2008; Mengel, Ulione,Wedding, Jones, & Shurn, 2005). Furthermore, otherthan a post hoc allusion to Protection Motivation Theory(Cismaru et al., 2010), we could find no systematic useof theoretical frameworks to develop such campaigns.
This study sought to develop messages that would pro-mote abstinence from alcohol during pregnancy amongstpregnant women and women of childbearing age. A rec-ommendation for abstinence aligns with the Australianalcohol guideline for women who are pregnant or plan-ning a pregnancy, that recommends that “not drinkingis the safest option” (National Health and Medical Re-search Council, 2009, p. 5). The study was consideredtimely for a number of reasons. First, data showed thatalmost 60% of Western Australian women consume al-cohol during pregnancy, with most consuming low tomoderate amounts (Colvin, Payne, Parsons, Kurinczuk, &Bower, 2007); second, many women lack specific knowl-edge about the potential consequences of prenatal alcoholexposure (Peadon et al., 2010); third, the study follows asuccessful intervention in the state of Western Australiathat supported health professionals’ knowledge and prac-
tice with their clients with regards to alcohol use duringpregnancy (Payne et al., 2011); and fourth there had notbefore been any mass media campaigns targeting alcoholand pregnancy in Western Australia.
STUDY OBJECTIVES
The objectives of this study were to:
• identify message strategies that could be effective inpopulation-based communications aimed at preventingprenatal alcohol exposure;
• develop several advertising concept executions based onthese message strategies; and
• test the efficacy of the concept executions with a sampleof the target audience to identify:
1. content and execution factors that enhance mes-sage effectiveness; and
2. the content execution with the most potential foruse in amassmedia campaign aimed at preventingprenatal alcohol exposure.
STUDY DESIGN
The qualitative, formative research comprised focusgroups (FG) with the target audience and was conductedin Perth, Western Australia during 2009. Guided bysocial cognition models (Bandura, 1977; Becker, 1974;Fishbein & Ajzen, 1975; Rogers, 1975) a first exploratoryphase identified motivations for healthy choices duringpregnancy; women’s knowledge, beliefs and practiceregarding alcohol use during pregnancy; and barriersand facilitators for abstinence from alcohol. From thesedata, a series of communication and modeling objectivesand four television concept executions were developedin story-board format. A second phase exposed theconcept executions to a sample of the target audience toidentify which concept had most desired impact overall,and to identify specific copy and execution elementsthat enhanced or detracted from the effectiveness of themessages. The methodology and results for each of thetwo phases are presented sequentially.
Consumer and Community ParticipationA community reference group comprising six women ofchildbearing age advised on all aspects of the study designand implementation.
Ethics ApprovalApproval for this study was granted by the Edith CowanUniversity Human Research Ethics Committee.
EXPLORATORY PHASE—METHOD
Sampling and RecruitmentThe exploratory phase consisted of four FG with 23women of childbearing age: two groups with women whohad been pregnant within the last three years (FG 1 and 4);one with pregnant women (FG 2); and one with womenwithout children who thought they might have children in
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Yal
e D
erm
atol
ogic
Sur
gery
on
08/0
2/13
For
pers
onal
use
onl
y.

PROMOTING ABSTINENCE FROM ALCOHOL DURING PREGNANCY 3
the near future (FG 3). This maximum variation samplingmethod (Patton, 2002) was used to enable insight into abroad range of perspectives while allowing for the iden-tification of ways that groups with certain characteristicsmay vary from each other. The aim was to include womenat different reproductive stages in order to gain insight intothe experience of pregnancy and motivations for behav-ior change that may be relevant before, during, and af-ter pregnancy. To enhance group interactivity, the groupswere homogeneous with respect to socioeconomic statusand alcohol consumption. To be eligible, all participants–-except those who were pregnant—had to screen positiveto alcohol use in the previous month. Based on Australianethical guidelines for research (National Health and Med-ical Research Council, 2007), pregnant women who wereconsuming alcohol were not eligible to participate in thisresearch given the exploratory nature of the data collectionand the potential for discomfort or harm that may resultfrom participation.
Pregnant women and women who had recently beenpregnant were recruited from community-based groupsand events. Women were screened for eligibility overthe phone using a short questionnaire prior to being in-vited to participate. A market research company was con-tracted to recruit women without children from an exist-ing research panel database. Participants who were notpregnant were advised that they were attending a FG on“women’s health” to prevent priming the participants withthe topic of interest. For ethical reasons, the topic of al-cohol use during pregnancy was fully disclosed to preg-nant women prior to seeking their consent to participate.Approximately half the participants were aged less than30 years and half were over 30 years. The majority had
a tertiary qualification and were married or in a de-factorelationship.
Setting and ProcedureThe FGs were held at a centrally located market researchorganization, they lasted one and a half hours, and partic-ipants were provided with a cash reimbursement to covertheir costs of attending. Signed informed consent wasgained prior to each group. The groups were led by thesame moderator (K.F.) and were observed by researcherswho were positioned behind a one-way mirror.
A semistructured topic guide sought information onparticipants’ knowledge, beliefs, and experiences regard-ing pregnancy in general as well as alcohol use duringpregnancy, and motivations for any behavior change dur-ing or prior to pregnancy. Data were transcribed verbatimand analyzed thematically by the primary author. To buildanalytical rigor and theoretical relevance, themes and cat-egories were generated with specific reference to con-structs within social cognition models (Bandura, 1977;Becker, 1974; Fishbein & Ajzen, 1975; Rogers, 1975).Expert checking of the themes and categories against thedata was conducted with two researchers expert in behav-ioral science theory (R.D and N.H.). Quotes which suc-cinctly captured the meaning of categories were sourcedand are identified below by the FG number.
EXPLORATORY PHASE—RESULTS
Knowledge, Beliefs, and PracticeTable 1 summarizes the key themes for women’s knowl-edge, beliefs, and practice about alcohol use duringpregnancy, and describes the potential implications
TABLE 1. Women’s beliefs, attitudes and practice about alcohol use during pregnancy and the implications for messaging
Beliefs, attitudes, and practice Implications for messaging
A reduction in alcohol consumption during pregnancy is a salientbehavior change and abstinence from alcohol during pregnancyis known to be recommended.
Messaging can go beyond a “do not drink alcohol in pregnancy”communication objective as this is already known amongst the targetaudience.
Binge drinking and getting drunk is understood to pose a risk topregnancy and the unborn child; however, there is confusionand skepticism about the risk of low to moderate exposure, andtherefore, skepticism about whether the risk applies to thepattern of drinking that the target audience engages in.
Messaging should focus on decreasing the ambiguity surrounding therisk of low to moderate patterns of drinking alcohol during pregnancy.
Messaging should address a drinking pattern that the target audiencesees as relevant to them such as “a couple of drinks every now andthen.”
The specific consequences of prenatal alcohol exposure for thefetus are not salient.
There may be the potential to fill a knowledge gap and strengthen therationale for an abstinence message through the provision ofinformation regarding the potential effects of alcohol on the fetus.
A change in alcohol consumption is one of a range of behaviorchanges that women make during pregnancy. Other behaviorchanges include diet, exercise, and tobacco use.
Increase the salience of abstaining from or reducing alcoholconsumption during pregnancy by linking to other behavior changeswhich are regularly adopted.
A barrier to abstinence from alcohol is advice from healthprofessionals that it is alright to drink some alcohol duringpregnancy.
Health professionals’ advice has the potential to undermine apopulation-based abstinence message. Use a health professionalwithin messaging and position them as a unquestionable expert whohas the most current information.
Health professionals are a respected source of information duringpregnancy.
Messaging could use a health professional as an expert source to deliverinformation.
Women often do not want to disclose their pregnancy in the earlystages, and this is a barrier to abstinence from alcohol duringsocial situations.
Providing strategies for avoiding alcohol during social situations,without disclosing pregnancy, may be useful.
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Yal
e D
erm
atol
ogic
Sur
gery
on
08/0
2/13
For
pers
onal
use
onl
y.

4 K. E. FRANCE ET AL.
for messaging to prevent prenatal alcohol exposure.A reduction in alcohol consumption during pregnancywas a salient behavior change in all groups. Womenknew that abstinence from alcohol during pregnancyis recommended over consuming some alcohol duringpregnancy: “a lot of things say none is best but an occa-sional one is not so bad” (FG 4). Women also knew thatbinge drinking or “get(ting) plastered” (FG 3) is harmfulduring pregnancy indicating an understanding betweenquantity and pattern of consumption, and risk. However,there was skepticism and confusion regarding the riskrelated to low or moderate alcohol use, such as “a glasshere and there” (FG 2). Despite the high education levelamongst the majority of participants, there did not appearto be a high level of specific knowledge regarding thepotential consequences for the fetus of alcohol use duringpregnancy, and the rationale behind the recommendationfor reducing alcohol intake during pregnancy was notsalient.
Women spoke of different reasons for continuing toconsume alcohol during pregnancy even though they be-lieved they would be better off not drinking. These canalso be viewed as barriers to abstinence from alcohol andincluded feeling social pressure to drink: “I sometimes feltpressured into it sometimes, you know (they would say)‘it’s OK to have one’” (FG 1), receiving conflicting infor-mation about the risks of drinking alcohol during preg-nancy, and being told by a health professional that it wasalright to drink some alcohol during pregnancy.
Women who had had more than one pregnancy spokeabout becoming lax about behavior change in pregnanciessubsequent to the first, and there was a perception thatwomen became more lax toward the final stage of theirpregnancy. While participants were not asked about theirown alcohol use during pregnancy, some participants re-
flected on consuming alcohol during pregnancy, particu-larly with reference to the amount that they had drunk: “Iwasn’t going out and getting hammered or anything likethat” (FG 1), and in regards to consumption before theyknew they were pregnant: “I didn’t intentionally drink, Iremember I had a bottle of wine when I was pregnant with(a friend), and I didn’t know I was pregnant, anyway thatdoesn’t count” (FG 1).
Participants described an important social situationearly in pregnancy which can undermine decisions toavoid alcohol; namely, when women are not ready to di-vulge to others that they are pregnant, but the refusal ofalcohol may indicate to friends, family, or colleagues thatthey are: “I wasn’t going to tell anyone. . . but it was so ob-vious because they knew I was a drinker” (FG 4). For somewomen, it was important to keep pregnancy a secret dur-ing the early stages, and while their intentions may havebeen to avoid alcohol during this time, they found them-selves in a conflicted position within social situations.
Motivations for Reducing or Abstaining from AlcoholDuring PregnancyTable 2 summarizes women’s motivations for reducing orabstaining from alcohol during pregnancy, and the associ-ated emotions and implications for messaging. These im-plications for messaging use Rossiter and Percy’s (1987)basic motivation and emotions (extended by Donovan(1995)) as a framework for categorizing the motivations.
Women described avoiding negative outcomes andreducing fear or worry about these as key motivators foradaptive or healthy behavior change during pregnancy.This feeling was often described as being “paranoid”(FG 2 and FG 4). Other negative motivations includedwanting to avoid the feelings of guilt, regret, andresponsibility if something went wrong with the
TABLE 2. Results from exploratory phase: Negative and positive motivations∗ for modifying alcohol consumption for pregnancy,associated feelings, and the implications for message strategy
Motivation Associated feelings Implications for message strategy
NegativeReduce fear and worryAvoid poor pregnancy and fetal outcomes
Fear, worry, and “being paranoid” Emphasize that these negative outcomes,experiences, and feelings can bereduced or avoided if women abstainfrom alcohol during pregnancy.
Avoid feeling responsible for poorpregnancy or fetal outcomes
Guilt and regret
Avoid social disapproval Shame and embarrassmentPositive
Feel efficacious by avoiding threats thatare within personal control
Feeling “in control” and having “peace of mind” Emphasize that these positiveexperiences and feelings can beobtained or maintained if womenabstain from alcohol during pregnancy.
Gain self approval Feeling that you are “doing the best that you can”Gain social approval Pride and respectFeel socially accepted Belonging and “fitting in”Feel doing “the right thing” by complyingwith professional advice
Virtuous and good
∗Drawing from Rossiter and Percy’s (Rossiter & Percy, 1987) hypothesized relationship linking emotions to motivations in advertising;extended by Donovan (1995).
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Yal
e D
erm
atol
ogic
Sur
gery
on
08/0
2/13
For
pers
onal
use
onl
y.

PROMOTING ABSTINENCE FROM ALCOHOL DURING PREGNANCY 5
pregnancy or child: “imagine the guilt you would feel ifit was through your own carelessness or selfishness thatyour child now has to deal with that for the rest of theirlife” (FG 3).
Along with avoiding fear and worry, women were alsomotivated toward the arousal of certain positive emotionalstates or feelings. These included a desire to feel “in con-trol” (FG 1) and doing the best that they could to supportthe health of the pregnancy and fetus. Having or givingoneself reassurance or peace of mind was another positivemotivation: “I’d like to think that I tried to do everythingpossible to make the baby as healthy as possible” (FG 3).
Another strong motivation for modifying alcohol usewas the avoidance of social disapproval. Women spoke ofbeing “looked down on” (FG 2) by others if they drank al-cohol during pregnancy, and many thought that there wasa strong expectation from others for a pregnant women toabstain from alcohol: “I wouldn’t (drink alcohol) becauseI think, I think people’s opinions of you. . . I think a lotof people think that you shouldn’t drink” (FG 2). The re-verse of this was also relevant: as a positive motivation inthe sense of seeking social approval and wanting to fit inwith the perceived social norm of abstaining from alcoholor drinking only small amounts.
Women also reported that advice from health profes-sionals was a factor that strongly influenced their choicesand behavior during pregnancy. Hence, another positivemotivation was to comply with professional advice. Thosewho had received information from a health professionalthat it was alright to consume some alcohol during preg-nancy, used it as a rationale for their continued con-sumption. For those who had received advice to abstain,this strengthened their decision to avoid alcohol duringpregnancy.
MESSAGE STRATEGY AND CONCEPT DEVELOPMENT
Based on the results of the exploratory phase, the messagestrategy objectives were to create and reinforce healthybeliefs and social norms with regards to abstinence fromalcohol use during pregnancy. The specific communica-tion and modeling objectives are outlined in Table 3.
The rationale for the development of each of the fourconcept executions (Appendices 1–5) is described below.
• Partner. This concept is based on the constructs of self-efficacy and social norms, and seeks to appeal to thepositive motivations of feeling in control, efficacious,and socially accepted. It models the support of a malepartner in helping a woman to abstain during pregnancythrough modifying his own alcohol use. It also modelsa strategy for overcoming a social barrier to avoidingalcohol without disclosing pregnancy.
• Best Friend. Like the Partner concept, Best Friendis based on the constructs of self-efficacy and socialnorms, and seeks to appeal to the positive motivationsof feeling in control, efficacious, and socially accepted.Instead of showing the support of a partner, this con-cept models the support of a female friend in avoid-ing alcohol during a social situation, as a facilitator ofabstinence. It simultaneously shows social inclusion of
TABLE 3. Communication and modeling objectives
Communication objectivesCreate and reinforce the beliefs that:
• if you are pregnant you should reduce your alcohol intake,with abstinence as the primary goal;
• alcohol consumption is something that (most) pregnantwomen can control and that reduction or abstinence fromalcohol will support the health of the pregnancy and baby;
• no alcohol during pregnancy is the safest option;• the risk to the fetus increases with increasing amount andincreasing frequency and there is risk even when a woman isnot “drunk”;
• alcohol consumption is related to short-term and long-termnegative consequences for the pregnancy and fetus; and
• challenge the belief that “a couple of drinks every now andthen” are risk free.
Modeling objectives• Align abstaining from alcohol to other positive behaviorchanges for pregnancy such as “being on a health-kick,”eating healthy foods, or taking folic acid.
• Show a significant person (i.e., partner or friend) supporting awoman to modify her alcohol consumption when pregnant.
• Demonstrate a way of dealing with social situations whenwomen want to abstain from alcohol but do not want others toknow that they are trying to get pregnant or are pregnant.
the pregnant woman, and addresses the social barrier ofavoiding alcohol without disclosing pregnancy by pro-viding an excuse of “being on a health-kick.”
• Woman. This concept focuses on the positive motiva-tions of self-approval, self-efficacy, and control. It seeksto appeal to the notion of a woman “doing everythingthat she can” to support the health of the fetus, and hencegive herself “peace of mind.” As with the other conceptexecutions, this concept shows a woman who is in theearly stages of pregnancy and demonstrates choosing analternative beverage to alcohol at a work-related event.
• Obstetrician. This concept appeals to the motivationsof avoiding fear, worry, and negative consequences forthe fetus. This threat appeal addresses a key questionregarding the risk of low to moderate exposure and fea-tures an expert source of information. To assess theimpact of including specific information on the poten-tial consequences of prenatal alcohol exposure on thefetus, two versions of the Obstetrician concept weredeveloped:
• Obstetrician—risk. This version provides specificinformation pertaining to the nature of the risk of pre-natal alcohol exposure and related specifically to thetheoretical construct of susceptibility to the risk.
• Obstetrician—consequences. This version explic-itly details some of the potential consequences ofprenatal alcohol exposure for the fetus, and relatedspecifically to the theoretical construct of severity ofthe outcomes.
CONCEPT TESTING PHASE–-METHOD
Sampling and RecruitmentFive FGs of 31 participants representing all intended tar-get audiences took part in the concept testing phase: one
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Yal
e D
erm
atol
ogic
Sur
gery
on
08/0
2/13
For
pers
onal
use
onl
y.

6 K. E. FRANCE ET AL.
FG of women recently pregnant (within the last threeyears) (FG 5); one of male partners of women recentlypregnant (FG 6); one of women without children whothought they might soon be pregnant (FG 7); one ofwomen who were pregnant for the first time (FG 8);and one of women who were pregnant with their sec-ond or later child (FG 9). Women were recruited usingthe same strategy and eligibility criteria as for the ex-ploratory phase.Menwere recruited through partners whohad previously participated or registered their interest inthe project. To be eligible, men had to have a child agedthree years or younger, currently drink alcohol, and livein a middle socio-economic area. The majority of partic-ipants were aged between 30 and 34 years and had a ter-tiary qualification. All of the participants were married orin a de-facto relationship. Of the 12 pregnant participants,one was in the first trimester, six were in the second, andfive were in the third trimester of pregnancy.
Setting and ProcedureFGs lasted 2 hours and were conducted at the samevenue and times as those described for the exploratoryphase. Groups were led by the same moderator (K.F).Each participant received a booklet in which the fourconcept executions were provided in story-board formatand presented in rotating order to counter against order-ing effects. Each concept was followed by a question-naire comprising open and closed-ended standard copytesting questions. Half of the participants in each groupreceived Obstetrician—risk and the other half receivedObstetrician—consequences.
Open-ended written responses were sought on the per-ceived main message in each concept (What is the adver-tisement trying to tell you, or telling you to do?). Struc-tured feedback was also gained using the following mea-sures through a five-item response scale comprising theresponse options not at all, only a little, small amount,fair amount, great amount:
• intention to adopt the recommended behavior as a resultof viewing the concept.To what extent does the advertisement make you want todrink less alcohol or not at all during pregnancy? (fe-males)/make you want to do things to help your partneravoid alcohol during pregnancy? (males):
• Engagement with the issueTo what extent does the advertisement make you thinkabout alcohol use during pregnancy?:
• RelevanceHow relevant is the advertisement to you personally?;
• BelievabilityHow believable is the situation shown in the advertise-ment?; and
• AppealHow much do you like the advertisement?
After completing the above questions for all conceptexecutions, participants were asked to rank the executionsin terms of which one was most motivating, that is, mostmade themwant to abstain from alcohol during pregnancy(females) or do things to help their partner avoid alco-
hol during pregnancy (males). A group discussion thenasked participants to elaborate on their reasons for choos-ing their top ranking and the content and execution ele-ments that they found to be effective.
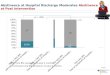
AnalysisThe data from all five FGs were compiled and are pre-sented together below. The open-ended written responsesand group discussion data were thematically analyzed.For the close-ended response data, the proportion of allparticipants nominating the top two positive responses(fair amount or great amount) for each measure wascalculated (see Figure 1). For the analysis of the openand close-ended responses, the two variations of theObstetrician concept were combined to allow compar-ison across the four concept executions. However thegroup discussion data for each were analyzed separatelyin order to identify any key differences resulting fromthe content variation between Obstetrician—risk andObstetrician—consequences.
CONCEPT TESTING PHASE—RESULTS
The concept testing phase results comprise individual,structured feedback and group discussion data. The struc-tured feedback cannot be equated with quantitative data,but rather, is used in combination with the group discus-sion data to allow a clear and comprehensive assessmentof which concept was most effective amongst the targetaudience and why.
Main MessagesThe main messages perceived by participants within allconcept executions closely matched the intended commu-nication and behavior objectives. For all executions exceptObstetrician the main message perceived by participantswas “don’t drink alcohol when you are pregnant.” ForObstetrician, the main message was similar but wordeddifferently: “the safest choice when you are pregnant isno alcohol at all.” Furthermore, Obstetrician had a rangeof secondary messages that were stronger than for theother concept executions and related to the reasons for notdrinking during pregnancy, such as “any alcohol poses arisk to the baby” and “alcohol can disturb the developmentof the fetus.”Best Friend and Partner both successfully conveyed
the message that a friend or partner can support a womanto avoid alcohol during pregnancy, and that this supportis important. Participants who saw Woman perceived astrong main message of “there is risk to the baby if youdrink alcohol during pregnancy, and the risk is loweredif you avoid alcohol,” indicating that it was successful indemonstrating the efficacy of personal action to avert thethreat.
Individual Structured FeedbackIndividual structured feedback was gained on the follow-ing measures: intention to adopt the recommended behav-ior, engagement with the issue, relevance, believability,
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Yal
e D
erm
atol
ogic
Sur
gery
on
08/0
2/13
For
pers
onal
use
onl
y.

PROMOTING ABSTINENCE FROM ALCOHOL DURING PREGNANCY 7
FIGURE 1. Proportion of participants selecting top two responses on each measure for each of the concepts.
and appeal. Figure 1 shows the proportion of participantswho selected the top two responses on each measure foreach of the concept executions.
The Obstetrician concept outperformed all other con-cept executions on all measures except relevance. Theseratings also show that all concept executions scored rea-sonably well on most measures, including the key behav-ioral intention measure, thus confirming the validity of theconclusions derived from the exploratory phase.
Most Motivating Concept and Effective Contentand Execution ElementsObstetrician was the concept considered most likely topromote alcohol abstinence during pregnancy: 58% ofparticipants chose this concept as most motivating. Theensuing group discussion revealed that in terms of content,the Obstetrician concept was favored as it provided infor-mation that participants wanted to know, and included aclear recommendation for abstinence from alcohol duringpregnancy. Participants appreciated thatObstetrician pro-vided a reason as to why abstinence from alcohol was ad-vised. Posing and answering the question: “Is a couple ofglasses of wine every now and then OK?” appeared to bea good execution device to engage attention. The answerprovided by the obstetrician—“We just don’t know howmuch alcohol it takes to do damage”—was perceived ashonest and participants reported that it enhanced the cred-ibility of the overall recommendation of abstinence fromalcohol, “it was honest. . . that they just don’t know andthat is why they say that nothing is better than having oneglass. That they just don’t know how much it takes to dodamage and it is different for every person” (FG 8). Over-
all, two powerful execution elements ofObstetricianwerethe use of the obstetrician as an expert source and the de-livery of information in a clear, direct, and factual way.Obstetrician was also said to be “harder hitting” than
the other concept executions “because it says your babycould be harmed” (FG 8). A greater proportion of the par-ticipants who saw Obstetrician—consequences selectedit as most motivating compared to those who saw andselected Obstetrician—risk and discussion indicated thatparticipants were motivated by the provision of specificinformation about the negative potential consequences forthe fetus of alcohol use during pregnancy.
Those who rated Best Friend as the most motivatingconcept valued the display of friendship and support ofthe pregnant woman by her friend. Similarly, the mostmotivating aspect of Partner was the display of supportfor a pregnant woman by her partner. However, severalmale and female participants thought that the latter sce-nario was unrealistic because they thought it unlikely thata male partner would abstain from alcohol in support ofa pregnant woman: “it’s unrealistic; most guys I knoware like ‘woohoo! I have two years where I don’t have todrive” (FG 5). For both Best Friend and Partner, partic-ipants responded positively to the provision of a strategyfor abstaining from alcohol without disclosing pregnancyduring the early stages.
When probed, none of the participants indicated thatthe concept executions triggered any discomfort abouttheir own drinking during current or previous pregnancies.There were also no negative comments with respect to thetone of the concept executions; that is, participants did notfeel they were being judged or lectured to.
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Yal
e D
erm
atol
ogic
Sur
gery
on
08/0
2/13
For
pers
onal
use
onl
y.

8 K. E. FRANCE ET AL.
DISCUSSION
This study demonstrates the value of formative researchand theoretical frameworks in the development of effec-tive messages to promote abstinence from alcohol dur-ing pregnancy. Research identified insights into women’sknowledge, attitudes, beliefs, and motivations and the im-plications for message strategy. Women knew that absti-nence from alcohol was recommended during pregnancy,but were skeptical about the risk associated with low tomoderate amounts. The reduction of ambivalence is un-derstood to be a precursor to behavior change (Miller &Rollnick, 1991) and hence the communication objectivessought to decrease women’s ambivalence with regards tosmall amounts of alcohol, and to challenge the belief that“a couple of drinks every now and then” are risk free.
Pregnancy is a known “window of opportunity” (Di-Clemente, Dolan-Mullen, & Windsor, 2000, p. iii16) forbehavior change given the intrinsic motivation of havinga healthy baby. However, an assumption that motivationbegins and ends with the baby would preclude many pow-erful motivations that can be used in creating persuasivecommunication. This study identified both positive andnegative motivations for women to abstain from alcoholduring pregnancy. These included wanting to minimizea generalized fear that something could go wrong, andwanting to believe they were in control and doing the bestthat they could to support the health of the pregnancy andthe fetus. The implications drawn were that messagescould either aim to emphasize that the negative outcomes,experiences, or feelings could be reduced or avoidedand/or that positive outcomes, experiences, or feelingscould be obtained or maintained if women abstained fromalcohol during pregnancy. The results clearly indicatedthat the concept appealing to negative motivations,Obstetrician, was most effective at promoting women’sintentions to abstain from alcohol during pregnancy. Thissuggests that the avoidance of negative feelings and out-comes for the pregnancy and fetus are greater motivatorsfor abstinence than positive motivators. This is consistentwith much research around the efficacy of fear (or threat)appeals (Sutton, 1982; Witte & Allen, 2000) which showsthat, provided the promoted response is under volitionalcontrol, the negative motivation of avoiding the threat isa powerful instigator of behavior change.
Some authors have noted the potential risk of us-ing threat appeals within alcohol and pregnancy com-munication (Burgoyne, Willet, & Armstrong, 2006;Saskatchewan Prevention Institute, 2009). However, evena positive message strategy may carry an implicit threat.Furthermore, the provision of information about the risksand consequences of prenatal alcohol exposure may beparticularly important for campaigns in Australia giventhe relative lack of public awareness around this (Peadonet al., 2010). The concern is if threat-based messages areseen by the audience to be overstating the risk or sensa-tionalizing the severity of the consequences, then they arelikely to be rejected and argued against, and this couldwork to promote maladaptive responses. What this studyshows is that if a threat appeal is delivered in a way that is
perceived to be honest, factual, and supportive of womenmaking informed choices about their health behavior dur-ing pregnancy, it is likely to be accepted and persuasive.Several execution elements were identified that appear tobe important to this. Credibility of the message was en-hanced by acknowledging uncertainty about the risk to thefetus with low to moderate alcohol exposure. Rather thanundermine an abstinence-based message, this informationserved as a clear rationale for the recommendation. Anhonest and scientific framing of the message and deliveryby an expert source were also shown to minimize counter-argument and strengthen the message’s persuasiveness.
While the concept executions appealing to positivemotivations were not as persuasive as the concept basedon negative motivation, the data indicate potential forpositive messaging to be used in conjunction with athreat-based message. As identified by Cismaru and col-leagues (Cismaru et al., 2010), messages targeting alcoholuse during pregnancy often focus on increasing perceivedseverity of the threat, and the audiences’ perceivedsusceptibility to the effects of prenatal alcohol exposure,without adequate attention given to perceived self-efficacy as important for instigating protection motivation(Rogers, 1975) or a danger control process (Witte, 1992).In this study, a display of social support and acceptancefor a pregnant women abstaining from alcohol was well-received by participants, as were specific strategies foravoiding alcohol during social situations. Elements suchas these may be used to promote feelings of self-efficacy,and further support the effectiveness of threat-based mes-saging that appeal to fear and other negative motivations.
Study LimitationsIt is important to recognize that these messages were de-signed to target those who drink alcohol, but generally notto excess. It is unlikely that women with alcohol prob-lems would respond to these concept executions with re-spect to abstinence. Further testing with this group maybe important to ensure that there are no maladaptive out-comes of the messaging for women who cannot considerabstinence from alcohol during pregnancy. The sampleof participants was skewed towards an educated, middle-socioeconomic sample of women (and men). While wewould expect the same motivations for abstinence duringpregnancy for women of lower socioeconomic status, itwould be necessary to test any further concept develop-ment with such women to ensure that the language andterminology were at an understandable level.
As with any advertising creation there are numerousways to execute particular message strategies. There maywell be more effective ways to execute these messages.Importantly though, this study demonstrates the applica-tion of insights from exploratory research and social cog-nitive theory within creative concept development.
Summary and Future ResearchThis study is one of the first to report results fromformative research development and testing of persuasivemessages to prevent prenatal alcohol exposure. The study
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Yal
e D
erm
atol
ogic
Sur
gery
on
08/0
2/13
For
pers
onal
use
onl
y.

PROMOTING ABSTINENCE FROM ALCOHOL DURING PREGNANCY 9
provides an assessment of several potentially efficaciousadvertising concept executions that, subject to furtherconfirmatory quantitative assessment and refinement forparticular target audience characteristics, could be usedin a communication campaign to persuade women toabstain from alcohol during pregnancy.
AcknowledgementsThe authors would like to thank the study’s CommunityReference Group members Jocelyn Boylen, Kelly Jef-fries, Sheree Lawson, Josie Maxted, Stacy Maxted andJulie Whitlock and investigators Gary Kirby and HeatherMonteiro for their guidance on project design andimplementation. Also, Lynda Fielder for her assistancewith data collection. Our sincere thanks also to thosewomen and men who participated in the project, andthose organisations and coordinators that assisted withrecruitment of participants.
Declaration of Interest
The authors report no conflicts of interest. The authorsalone are responsible for the content and writing of thearticle.
This work was supported by Healthway [ResearchProject Grant #18044] and the National Health and Medi-cal Research Council [Public Health Postgraduate Schol-arship #480109 to K.F.].
RESUME
Promouvoir l’abstinence d’alcool pendant la grossesse:les implications de la recherche formative
Cette recherche a developpe des messages a promouvoirl’abstinence d’alcool pendant la grossesse et elementsidentifies qui ameliorent un message persuasif. Une phaseexploratoire a ete menee en 2009, qui comprenait qua-tre groupes de discussion avec 23 femmes en Australie-Occidentale et suscite croyances et attitudes sur la con-sommation d’alcool pendant la grossesse et motivationspour le changement de comportement. Quatre concepts detelevision ont ensuite ete developpes et evalues dans cinqgroupes de discussion avec 31 participants utilisant pretestdes questions de publicite standard. Les implications pourles campagnes portant sur l’exposition prenatale a l’alcoolet d’autres recherches sont notes et limitations discutees.Le financement a ete obtenu a partir de Healthway et laNational Health and Medical Research Council.
RESUMEN
Promover la abstinencia de alcohol durante elembarazo: implicaciones de la investigacion formativa
Esta investigacion desarrollada mensajes para promoverla abstinencia de alcohol durante el embarazo y los el-ementos identificados que mejoran mensaje persuasivo.Una fase de exploracion se llevo a cabo en 2009, que con-staba de cuatro grupos focales con 23mujeres enAustralia
occidental y provoco creencias y actitudes sobre el con-sumo de alcohol durante el embarazo y las motivacionespara el cambio de comportamiento. Cuatro conceptos tele-vision fueron posteriormente desarrollados y evaluados encinco grupos de enfoque con 31 participantes con pregun-tas pruebas preliminares de publicidad estandar. Las im-plicaciones para las campanas que abordan la exposicionprenatal al alcohol y una mayor investigacion se observany las limitaciones discutidas. La financiacion se recibioHealthway y la National Health and Medical ResearchCouncil.
THE AUTHORSKathryn E. France has a Ph.D.from Edith Cowan University.This paper reports results fromher Ph.D. study which focusedon the development and testingof advertising concepts for acampaign to promote abstinencefrom alcohol during pregnancy.Kathryn’s research interestsinclude the promotion of healthypregnancies and using formativeresearch to develop persuasivehealth promotion and health
communication..
Robert J. Donovan is Professorof Behavioral Research in theFaculty of Health Sciences,Adjunct Professor of SocialMarketing in the Schoolof Marketing and principal ofMentally Healthy WA’s Act-Belong-Commit campaign atCurtin University. After a careerin commercial marketing hereturned to academia in the early1990s. He has a broad rangeof interests, including alcohol,
tobacco and drugs, child abuse, domestic violence, racism, dopingin sport, suicide prevention and mental health. He is currentlyVice-president of the Board of Relationships Australia WA, aboard member of Mates in Construction (WA), and Chair of theWorld Anti-Doping Agency’s Ad Hoc Social Sciences ResearchSub-Committee.
Professor Nadine Henley hasa Ph.D. from the Universityof Western Australia. She isProfessor of Social Marketingat Edith Cowan University andis coauthor of Principles andpractice of social marketing:An international perspective(2010). Her research focuses onhealth issues in social marketing,specifically investigating whatpersuades people to adopthealthy behaviors.
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Yal
e D
erm
atol
ogic
Sur
gery
on
08/0
2/13
For
pers
onal
use
onl
y.

10 K. E. FRANCE ET AL.
Carol Bower, Ph.D., is agraduate of the Medical Schoolat University of WesternAustralia, has a Ph.D. fromUWA, M.Sc. in epidemiologyfrom University of London, andis a Fellow of the AustralianFaculty of Public HealthMedicine. She is MedicalSpecialist for the Register ofDevelopmental Anomalies,Senior Principal ResearchFellow at the Telethon Institute
for Child Health Research and Winthrop Research Professor in theCentre for Child Health Research at the University of WesternAustralia. Her research focuses on the epidemiology of birthdefects and their prevention.
Elizabeth J. Elliott AM isProfessor of Pediatrics andChild Health, University ofSydney; Consultant Pediatricianat the Sydney Children’sHospitals Network; and NationalHealth and Medical ResearchCouncil (NHMRC) PractitionerFellow. She runs a FASDdiagnostic clinic in Sydneyand is Chief Investigator fora FASD prevalence study inAboriginal communities in
remote Australia. Elizabeth was a member of the committees todevelop: NHMRC guidelines to prevent harm from alcohol use inAustralia; a national action plan for FASD; and to is on the WHOGuideline Development Group for Identification and treatment ofalcohol use in pregnancy. She is on the WHO Advisory Groupon FASD for the WHO International Collaborative ResearchProject on FASD; the NSW Health FASD Working Group;and the Alcohol Policy Committee of the Royal AustralasianCollege Physicians (2013). Elizabeth has published and presentedinternationally on alcohol in pregnancy and FASD and is onthe Expert Advisory Committees for the International FASDCongress in Canada (2011/13/15) and the International Congressfor Adolescents and Adults with FASD (2012/2014). In 2008,she was made a Member of the Order of Australia (AM) 2008 for“service to pediatrics and child health as an academic, researcher,and educator and through the establishment of the AustralianPediatric Surveillance Unit.”
Dr Janet M. Payne hasqualifications in Nursing,Midwifery, Child Health,Health administration, a M.Sc.(Public Health) from CurtinUniversity and a Ph.D. fromThe University of WesternAustralia. She is employed asa Research Program Managerat the Telethon Institute forChild Health Research in Perth,Western Australia. Her researchinterest is the prevention of
prenatal alcohol exposure and fetal alcohol spectrum disorders;and ensuring health professionals receive professional and
workforce development and education on alcohol consumptionin pregnancy and FASD, and FASD diagnosis.
Heather D’Antoine trainedas a registered nurse and amidwife and has extensiveexperience in health services.She completed a Bachelor ofApplied Science and Masters inHealth Economics (Aboriginalhealth) at Curtin University ofTechnology. Heather is currentlyemployed as the Division Leaderand Associate Director forAboriginal Programs at theMenzies School of Health
Research. Her research focus is on prevention in Aboriginal childhealth.
Professor Anne E. Bartuhas a Ph.D. and a MastersDegree of Public Health fromCurtin University, an HonorsDegree (Anthropology) from theUniversity of Western Australia.Previously she was the PrincipalResearch Officer at the Drugand Alcohol Office, Perth.Anne is an Adjunct Professorat the School of Nursing andMidwifery, Curtin Universityand an Honorary Research
Fellow at the Women and Infants Research Foundation, Universityof Western Australia. Her research interests include drugs inpregnancy, transmission of drugs in breast milk and the earlydevelopment of children of substance misusing parents.
GLOSSARY
Concept executions: A concept is an idea upon which anadvertisement is based and a concept execution is thematerial that represents, conveys, or communicates thatconcept.
FASD: Fetal Alcohol Spectrum DisordersFormative research: Research that aims to inform the de-
velopment of interventions, products, and communica-tion materials.
Self-efficacy: An individually held belief that one pos-sesses the ability to perform a specific behavior or be-havior change. As such, messages that seek to promoteself-efficacy seek to promote this belief amongst therecipients of the message.
Thematic analysis: A process whereby descriptive datais sorted and grouped into themes and categories. Thethemes and categories may be dictated by the topic ofinterest or area of inquiry, or may “emerge” and be-come apparent through analysis of the data.
Threat appeal: A message containing a threat that aimsto elicit a response of threat-avoidance in the recipientof the message. A recipient’s perception of the threat issaid to comprise the level to which they feel susceptibleto the threat (perceived susceptibility) and the extent to
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Yal
e D
erm
atol
ogic
Sur
gery
on
08/0
2/13
For
pers
onal
use
onl
y.

PROMOTING ABSTINENCE FROM ALCOHOL DURING PREGNANCY 11
which they feel the threat would affect them (perceivedseverity).
REFERENCES
Balachova, T., Bonner, B., Isurina, G., & Tsvetkova, L. (2007). Useof focus groups in developing FAS/FASD prevention in Russia.Substance Use and Misuse, 42, 881–894.
Bandura, A. (1977). Social learning theory. Englewood Cliffs:Prentice Hall.
Baxter, L. A., Hirokawa, R., Lowe, J. B., Nathan, P., & Pearce, L.(2004). Dialogic voices in talk about drinking and pregnancy.Journal of Applied Communication Research, 32(3), 224–248.
Becker, M. (1974). The health belief model and personal health be-haviour. Health Education Monographs, 2, 324–473.
Branco, E. I., &Kaskutas, L. A. (2001). “If it burns going down. . .”:How focus groups can shape fetal alcohol syndrome (FAS) pre-vention. Substance Use and Misuse, 36(3), 333–345.
Burgoyne,W.,Willet, B., &Armstrong, J. (2006). Reaching womenof childbearing age with information about alcohol and preg-nancy through a multi-level health communication campaign.Journal of FAS International, 4(e17).
Cismaru, M., Deshpande, S., Thurmeier, R., Lavack, A. M., &Agrey, N. (2010). Preventing fetal alcohol spectrum disorders:The role of protection motivation theory. Health MarketingQuarterly, 27(1), 66–85.
Colvin, L., Payne, J., Parsons, D. E., Kurinczuk, J. J., & Bower,C. (2007). Alcohol consumption during pregnancy in non-Indigenous West Australian women. Alcoholism: Clinical andExperimental Research, 31(2), 276–284.
Deshpande, S., Basil, M., Basford, L., Thorpe, K., Piquette-Tomei,N., Droessler, J., et al. (2005). Promoting alcohol abstinenceamong pregnant women: Potential social change strategies.Health Marketing Quarterly, 23(2), 45–67.
DiClemente, C. C., Dolan-Mullen, P., & Windsor, R. A. (2000).The process of pregnancy smoking cessation: Implications forinterventions. Tobacco Control, 9(Suppl. 3), iii16–iii21. doi:10.1136/tc.9.suppl 3.iii16
Donovan, R. J. (1995). The role of emotion in advertising. In R.J. Donovan, N. Henley, G. Jalleh & C. Slater (Eds.), Roadsafety advertising: An empirical study and literature review (pp.84–91). Canberra: Federal Office of Road Safety.
Donovan, R. J., Jalleh, G., Fielder, L., & Ouschan, R. (2008). Whenconfrontational images may be counter productive: Reinforc-ing the case for pre-testing communications in sensitive areas.Health Promotion Journal of Australia, 19(2), 132–136.
Egger, G. J., Donovan, R. J., & Spark, R. (1993). Health and themedia: Principles and practices for health promotion. Sydney:McGraw-Hill Book Company.
Eitel, T., & Delaney, T. (2004). The role of formative research in amass media social marketing campaign. Social Marketing Quar-terly, 10(2), 28–33.
Elliott, L., Coleman, K., Subebwongpat, A., & Norris, S. (2008).Fetal Alcohol Spectrum Disorders (FASD): Systematic reviewsof prevention, diagnosis and managment. HSAC Report, 1(9).
Fishbein, M., & Ajzen, I. (1975). Belief, attitude, intention andbehaviour: An introduction to theory and research. Reading:Addison-Wesley.
Glik, D., Prelip, M., Myerson, A., & Eilers, K. (2008). Fetal Alco-hol Syndrome prevention using community-based narrowcast-ing campaigns. Health Promotion Practice, 9(1), 93–103.
Hankin, J. R. (2002). Fetal alcohol syndrome prevention research.Alcohol Research and Health, 26(1), 58–65.
Kesmodel, U., & Kesmodel, P. S. (2002). Drinking during preg-nancy: Attitudes and knowledge amongst Danish women,
1998. Alcoholism, Clinical and Experimental Research, 26(10),1553–1560.
Lupton, C., Burd, L., & Harwood, R. (2004). Cost of fetal alco-hol spectrum disorders. American Journal of Medical Genetics,127(1), 42–50.
Maibach, E. W., & Parrott, R. L. (Eds.). (1995). Designing healthmessages: Approaches from communication theory and publichealth practice. Thousand Oaks: Sage Publications.
May, P. A., Gossage, J. P., Kalberg, W. O., Robinson, L. K., Buck-ley, D., Manning, M., et al. (2009). Prevalence and epidemio-logic characteristics of FASD from various research methodswith an emphasisi on recent in-school studies. DevelopmentalDisabilities Research Reviews, 15, 176–192.
Mengel, M., Ulione, M., Wedding, D., Jones, E. T., & Shurn, D.(2005). Increasing FASD knowledge by a targeted media cam-paign: Outcome determined by message frequency. Journal ofFAS International, 3(e13), 1–14.
Miller, W. R., & Rollnick, S. (1991). Motivational interviewing:Preparing people to change addictive behaviour. New York:Guilford Press.
National Health and Medical Research Council. (2007). Nationalstatement on ethical conduct in human research. Common-wealth of Australia. Canberra: Author.
National Health and Medical Research Council. (2009). Australianguidelines to reduce health risks from drinking alcohol. Com-monwealth of Australia. Canberra: Author.
Olson, H. C., Oti, R., Gelo, J., & Beck, S. (2009). “Family mat-ters:” Fetal alcohol spectrum disorders and the family. Devel-opmental Disabilities Research Reviews, 15(3), 235–249. doi:10.1002/ddrr.65
Patton, M. Q. (2002). Qualitative research and evaluation methods(3rd ed.). Thousand Oaks: Sage Publications.
Payne, J., France, K., Henley, N., D’Antoine, H., Bartu, A.,O’Leary, C, et al. (2011). Changes in health professionals’knowledge, attitudes and practice following provision of educa-tional resources about prevention of prenatal alcohol exposureand Fetal Alcohol Spectrum Disorder. Paediatric and PerinatalEpidemiology, 25(4), 316–327.
Peadon, E., Payne, J., Henley, N., D’Antoine, H., Bartu, A.,O’Leary, C., et al. (2010). Women’s knowledge and attitudesregarding alcohol consumption in pregnancy: A national survey.BMC Public Health, 10, 510.
Poole, N. (2008). Fetal Alcohol Spectrum Disorder (FASD) pre-vention: Canadian perspectives. Retrieved May 13, 2013,from http://www.phac-aspc.gc.ca/hp-ps/dca-dea/prog-ini/fasd-etcaf/publications/cp-pc/index-eng.php
Raymond, N., Beer, C., Glazebrook, C., & Sayal, K. (2009). Preg-nant women’s attitudes towards alcohol consumption. BMCPublic Health, 9(175).
Rogers, R. W. (1975). A protection motivation theory of fear ap-peals and attitude change. Journal of Psychology, 91, 93–114.
Rosenstock, I. M. (1974). The health belief model and preven-tive health behaviour. Health Education Monographs, 2(4),354–386.
Rossiter, J. R., & Percy, L. (1987). Advertising and promotion man-agement. New York: McGraw-Hill.
Saskatchewan Prevention Institute. (2009). Creating effectiveprimary prevention FASD resources: Evaluation processesin health promotion. Saskatoon: Saskatchewan PreventionInstitute.
Stratton, K., Howe, C., & Battaglia, F. (Eds.). (1996). Fetal Alco-hol Syndrome: Diagnosis, Epidemiology, Prevention, and Treat-ment. Washington, DC: National Academy Press.
Streissguth, A., Barr, H. M., Kogan, J., & Bookstein, F. L. (1997).Primary and secondary disabilities in Foetal Alcohol Syndrome.
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Yal
e D
erm
atol
ogic
Sur
gery
on
08/0
2/13
For
pers
onal
use
onl
y.

12 K. E. FRANCE ET AL.
In A. Streissguth & J. Kanter (Eds.), The challenge of fetal alco-hol syndrome: Overcoming secondary disabilities (p. 250). Seat-tle: University of Washington Press.
Sutton, S. R. (1982). Fear-arousing communications: A critical ex-amination of theory and research. In J. R. Eiser (Ed.), Socialpsychology and behavioural medicine. New York: John Wiley.
Toutain, S. (2010). What women in France say about alcohol ab-stinence during pregnancy. Drug and Alcohol Review, 29(2),184–188. doi: 10.1111/j.1465-3362.2009.00136.x
Witte, K. (1992). Putting the fear back into fear appeals: The ex-tended parallel process model. Communication Monographs,59(4), 329–349.
Witte, K., & Allen, M. (2000). A meta-analysis of fear appeals: Im-plications for effective public health campaigns. Health Educa-tion and Behavior, 27(5), 591–615.
APPENDIX 1
PartnerScene One
A woman aged approximately 30 years comes out ofthe bathroom, she is holding a pregnancy test stick. Shesays to her partner “Two lines. I think we are pregnant!”
He says, “Are you sure?”She says, “I think so!”They look at each other with excitement as the news
“sinks in.”Scene TwoA party scene, and the same couple have just arrived.The woman gets offered a glass of wine by a host, and
she shakes her head.She says, “No thanks, just two orange juices, we’re on
a health-kick.”Her partner is standing next to her and he holds up a
bottle of orange juice that they have brought with them.The host says, “Good on ya, I should be too.”The woman looks at her partner and they smile at each
other.
APPENDIX 2
Best FriendScene One
A woman aged approximately 30 years walking alongthe beach with her friend. The woman says with a smile,“Can you keep a secret?”
Her friend replies, “Of course I can! Why?” She slowsdown her walk.
The woman says, “You have to promise you won’t tellanyone, yet. . .”
The friend stops walking, nods, and looks at her withexcitement.
The woman stops walking and says “I’m pregnant!”They scream and laugh and the friend gives the woman
a big hug.Scene TwoIt is a “girls night out” party scene and the same woman
and her friend are arriving together.
The woman gets offered a glass of wine by the host,and the woman says “No thanks, just an orange juice forme.”
The host says “What? That’s not like you!”The friend is standing next to the woman and says “Oh,
we are on a health-kick, I’ll have an OJ too.”The host says with a roll of her eyes “Good on you, I
should be too!”The woman and her friend smile at each other while the
host turns away to get them the drinks.
APPENDIX 3
WomanScene One
A woman aged approximately 30 years is gazing downat a take-home pregnancy test stick.
There is a voice-over of her thoughts. She says to her-self, “Two lines. I’m pregnant!” (Happy, excited).
She pokes out her tummy in the mirror and laughs atherself.
She then rubs her stomach gazing down with a look oflove and nurturingScene TwoThe same woman is at a work-function and standing
with a small group of colleagues.One of her colleagues finishes off a sentence, he says
“. . . sowhile there aremany things you can’t control, thereare some things you can do to lower the risk and put your-self in the best position.”
A waiter approaches and offers the group drinks. Thereare glasses of red wine, white wine, water, and orangejuice.
The woman picks up an orange juice.There is a voice-over of her thoughts “Just an OJ
for me thanks. I’m doing what I can to lower the riskand put myself in the best position to have a healthypregnancy!”
APPENDIX 4
Obstetrician—RiskScene One
A woman and her partner are in a clinic room with anobstetrician. The obstetrician hands to the woman an ul-trasound picture that she has been looking at.
The obstetrician says, “So you are doing really well,everything is looking very good. Is there anything else youwould like to ask?”
The woman says, “And how about alcohol? I’ve hearddifferent things.”
The obstetrician says, “We recommend that you don’tdrink any alcohol during pregnancy. If you do drink alco-hol, the more you drink, and the more often you drink, thegreater the risk that your baby could be harmed.”
The woman asks, “Is a couple of glasses of wine everynow and then OK?”
The obstetrician says, “We just don’t know how muchalcohol it takes to do damage. No amount of alcohol has
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Yal
e D
erm
atol
ogic
Sur
gery
on
08/0
2/13
For
pers
onal
use
onl
y.

PROMOTING ABSTINENCE FROM ALCOHOL DURING PREGNANCY 13
been proven safe for the fetus. No alcohol is the safestchoice.”
APPENDIX 5
Obstetrician—ConsequencesScene One
A woman (who is not visibly pregnant) and her part-ner are in a clinic room with an obstetrician. The obste-trician hands to the woman an ultrasound picture that shehas been looking at.
The obstetrician says, “So you are doing really well,everything is looking very good. Is there anything else youwould like to ask?”
The woman says, “And how about alcohol? I’ve hearddifferent things.”
The obstetrician says, “Alcohol can disturb the devel-opment of the fetus. The baby could be born with braindamage, birth defects, low IQ, and possibly behavioralproblems which become more obvious as the child grows.We recommend that you don’t drink any alcohol duringpregnancy.”
The woman asks, “Is a glass of wine every now andthen OK?”
The obstetrician says, “We just don’t know how muchalcohol it takes to do damage. It is different for differentwomen and different babies. And that is why we say noalcohol is the safest choice.”
Notice of CorrectionAcknowledgments and funding information have been added to this article since its original online publication dateof 2 July, 2013.
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Yal
e D
erm
atol
ogic
Sur
gery
on
08/0
2/13
For
pers
onal
use
onl
y.