Embed Size (px)
Citation preview

mA(
MG(aaGrbpws
hwpcym
d
cf�5iwc(
ACc
8
Prolonged Remission of Severe Cushing Syndrome without Adrenalectomyin an Infant with McCune-Albright Syndrome
DAVID GILLIS, MD, ARIEL RÖSLER, MD, TAMARA S. HANNON, MD, BENJAMIN Z. KOPLEWITZ, MD, AND HARRY J. HIRSCH, MD
A 4 month-old girl presented with severe Cushing syndrome caused by McCune-Albright syndrome. After undergoing 19onths of pharmacologic suppression of cortisol production, she has been in clinical remission for more than 6 years.drenalectomy may be avoidable even in severe cases of Cushing syndrome associated with McCune-Albright syndrome.J Pediatr 2008;152:882-4)
cCune-Albright syndrome (MAS) is characterized by the classic triad of gonadotropin-independent precociouspuberty, cafe au lait skin pigmentation, and fibrous dysplasia of bone. There is, however, a broad spectrum of diseaseseverity, and multiple endocrinopathies may be present.1 MAS is caused by a postzygotic activating mutation of
NAS1, the gene encoding the stimulatory-alpha subunit of the signal-transducing guanosine nucleotide-binding proteinGs-alpha). The most common mutation, Arg201Cys,2,3 inhibits guanosine triphosphatase activity, leading to constitutivectivation of adenyl cyclase. Consequently, there is increased production of cyclic-adenosine monophosphate (c-AMP) andctivation of protein kinase A in affected cells, thereby causing increased cellular proliferation and hormone secretion.4,5
lucocorticoid hypersecretion caused by adrenocorticotropin (ACTH)-independent activation of adrenocortical cells has beeneported in infancy as an early manifestation of MAS.6-8 Severe cases have been treated with bilateral adrenalectomy followedy lifelong glucocorticoid and mineralocorticoid replacement. The natural history of this condition if adrenalectomy is noterformed is unknown. Several cases of MAS presenting with mild forms of Cushing syndrome in which morning cortisol levelsere normal6,7 or mildly elevated8 resolved spontaneously.6-8 We report the clinical course of a child with severe Cushing
yndrome associated with MAS for whom the family declined surgery.
CASE REPORT AND LABORATORY RESULTSThis infant girl was born after a normal term pregnancy and delivery. Birth weight was 3040 g. Three older siblings were
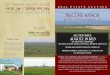
ealthy. At 4 months she presented with rapid weight gain, severe facial (Figure 1) and abdominal (Figure 2; available atww.jpeds.com) obesity, and hypotonia. Her weight was 6.35 kg (SDS: �0.60), length was 56 cm, (SDS: �2.59), and bloodressure was 129/60 mm Hg (above 95th percentile). There was no hirsutism. Two faintafé au lait lesions were seen on the neck and left thigh (Figure 3, neck lesion at age 3ears). At 3 years, both lesions had irregular borders and were of similar size, withaximal diameter about 12 cm.
At presentation, 8 a.m. serum cortisol was 41.8 �g/dL. After administration of oralexamethasone 0.5 mg at midnight, the 8 a.m. serum cortisol was 50.0 �g/dL.
At age 4.5 months, on admission to the hospital, the patient’s morning serumortisol was 39.2 �g/dL and 42.9 �g/dL from 2 different samples. Blood glucose beforeeeding was 83 mg/dL and was thereafter repeatedly normal. Urinary-free cortisol was 114g/24 h, i.e. 362.7 �g/m2/24 h (normal � 70 �g/m2/24 h). Serum DHEA-s level was52 �g/dL (normal infant: 4.3-111 �g/dL) and androstenedione 314.6 ng/dL (normalnfant: 12-77.8 ng/dL). An intravenous dexamethasone suppression test was performed ase have previously described9 (Table I; available at www.jpeds.com). Intravenous human
orticotropin–releasing hormone (CRH) stimulation was performed with 0.1 �g/kg CRHFerring, Kiel, Germany) (Table II; available at www.jpeds.com). Both test results
CTH AdrenocorticotropinRH Corticotropin-releasing hormone-AMP Cyclic-adenosine monophosphate
Gs-alpha Stimulatory -alpha subunit of the signal-transducing guanosine nucleotide-bindingprotein
From the Department of Pediatrics, Pedi-atric Endocrine Unit (D.G.), Department ofEndocrinology and Metabolism (A.R.), andthe Department of Medical Imaging (B.K.),Hadassah-Hebrew University Medical Cen-ter, and the Department of Pediatrics,Shaare-Zedek Medical Center (H.H.),Jerusalem, Israel, and the Department ofPediatrics, Division of Endocrinology, Chil-dren’s Hospital of Pittsburgh (T.H.), Pitts-burgh, PA.
Submitted for publication Oct 8, 2007; lastrevision received Dec 14, 2007; acceptedJan 25, 2008.
Reprint requests: David Gillis, MD, Depart-ment of Pediatrics, Hadassah Medical Cen-ter, Ein-Kerem, Jerusalem 91120, Israel. E-mail: [email protected].
0022-3476/$ - see front matter
Copyright © 2008 Mosby Inc. All rightsreserved.
MAS McCune-Albright syndrome
82
10.1016/j.jpeds.2008.01.037

isafpsw
emdapCadgod(mTape2ssrct(�b
usogp5mt5mis
CiiaeptcwaihGr
F
FAi
P
ndicated autonomous production of cortisol. Adrenal ultra-ound scanning revealed bilateral enlargement (Table III;vailable at www.jpeds.com). A skeletal survey was negativeor fibrous dysplasia of bone. At age 7 years 9 months, theatient has never had a fracture or other clinical evidence ofkeletal lesions. An arg201cys-activating GNAS1 mutationas identified in peripheral blood leukocytes.
Bilateral adrenalectomy was recommended, but the par-nts declined surgery. Therefore the patient was treated withetyrapone and aminoglutethimide, both at 500 mg daily in
ivided doses. The metyrapone was poorly tolerated and wasdministered via nasogastric tube in combination with theotent antiemetic ondansetron. Despite poor compliance,ushingoid features gradually resolved (Figures 3 and 4;
vailable at www.jpeds.com). The patient’s weight for ageecreased and height for age increased appropriately (seerowth chart, Figure 5; available at www.jpeds.com). The sizef the adrenal glands on repeat ultrasound scanning showed aecline in size until they became, appropriately, barely visibleTable III). Treatment was terminated completely at age 19onths, at which time morning cortisol was 19.7 �g/dL.wo months later, morning cortisol levels were 9.1 �g/dL
nd 14.3 �g/dL on 2 separate days. At age 3.5 years theatient presented with thelarche (Figures 3 and 4) and anpisode of vaginal bleeding. At the time, plasma estradiol was9 ng/dL (normal for age � 0.3 ng/dL, the level demon-trated was within the range of a midcycle peak). GnRHtimulated peak LH and FSH were 0.26 IU/L and 0.19 IU/L,espectively, consistent with gonadotropin-independent pre-ocious puberty. Serum cortisol before and 1 hour after in-ravenous injection of 250 �g/m2 synthetic aqueous ACTHSynacthene, tetracosactide, Novartis, France) were 4.94g/dL and 18.3 �g/dL, respectively, i.e., a borderline low
igure 1. Face at presentation.
aseline but normal response to stimulation. Transabdominal c
rolonged Remission of Severe Cushing Syndrome without Adrenalecto
ltrasound scanning revealed an enlarged right ovary with aingle 40- � 32-mm ovarian cyst, and a normal-sized leftvary. Anastrozole, a third-generation aromatase inhibitor,iven orally at 1 mg daily, halted clinical progression ofuberty and reduced serum estradiol to prepubertal levels. Atyears, secondary central puberty began and monthly intra-uscular GnRH superagonist injections (3.75 mg depot trip-
orelin) were added. The patient has currently reached the0th percentile for height and weight. At age 7 years 9onths, baseline morning cortisol was 13.1 �g/dL, decreas-
ng to 5.8 �g/dL after 1 mg midnight dexamethasone (normaluppression � �5 �g/dL).10
DISCUSSIONThis child underwent clinical remission of infantile
ushing syndrome with dramatic resolution of disease man-festations. Concomitantly, morning cortisol levels normal-zed, some dexamethasone suppressibility appeared, and thedrenal glands decreased in size. These phenomena can bexplained by 4 possible mechanisms, all of which could ex-lain a decrease in the amount of abnormally hypersecretingissue: 1. cAMP inhibits apoptosis in most cells11 but in-reases apoptosis in others,12 and the effect might changeithin the life cycle of the same cell type. 2. There might bedose-response effect, as described in steroid producing ovar-
an cells, whereby low levels of cAMP are anti-apoptotic butigher levels are pro-apoptotic.13 3. Prolonged activation ofs-alpha can increase phosphodiesterase activity and could
educe production of cAMP.14 4. A second-site mutation
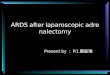
igure 3. Torso at age 3.5 years shows Tanner 3 breast enlargement.rrows delineate a typical café au lait lesion at the base of the neck. There
s no truncal obesity
ould possibly remove the constitutive activation of Gs-al-
my in an Infant with McCune-Albright Syndrome 883

pwric
1u2aE3IJ4e5G26b1
7h8AA9d111AC1abl1am1as1s
8
ha.15 Better understanding of this process might help predicthether there is ongoing risk of either adrenal insufficiency or
ecurrent hypercortisolism. In conclusion, this case shows thatt might be possible to avoid adrenalectomy, even in severeases of MAS-associated Cushing syndrome.
REFERENCES. Lee PA, Van Dop C, Migeon CJ. McCune-Albright syndrome: long-term follow-p. JAMA 1986;256:2980-4.. Lumbroso S, Paris F, Sultan C; European Collaborative Study. Activating Gs-lpha mutations: analysis of 113 patients with signs of McCune-Albright syndrome—auropean Collaborative Study. J Clin Endocrinol Metab 2004;89:2107-13.. Hannon TS, Noonan K, Steinmetz R, Eugster EA, Levine MA, Pescovitz OH.s McCune-Albright syndrome overlooked in subjects with fibrous dysplasia of bone?Pediatr 2003;142:532-8.. Glaser B, Hirsch HJ. McCune-Albright syndrome. In: Glaser B, Hirsch HJ,ditors. Genetics for endocrinologists. London: Remedica Publishing; 2003. p. 12-5.. Weinstein LS, Yu S, Warner DR, Liu J. Endocrine manifestations of stimulatory
protein alpha-subunit mutations and the role of genomic imprinting. Endocr Rev002;22:675-705.. Kirk JMW, Brain CE, Carson DJ, Hyde JC, Grant DB. Cushing syndrome caused
y nodular adrenal hyperplasia in children with McCune-Albright syndrome. J Pediatr999;134:789-92.sB
84 Gillis et al
. Volkl TM, Dorr HG. McCune-Albright syndrome: clinical picture and naturalistory in children and adolescents. J Pediatr Endocrinol Metab 2006;19(suppl 2):551-9.. Halioui-Louhaichi S, Azzabi O, Nefzi L, Ben Hariz ML, Ben Mrad N, Benmmar B, et al. Treatment with metyrapone of Cushing syndrome revealing McCune-lbright syndrome. Arch Pediatr 2005;12:1120-23.
. Shilo S, Rösler A. Single intravenous bolus of dexamethasone for the differentialiagnosis of Cushing syndrome. J Pediatr Endocrinol Metab 1995;8:27-33.0. Orth DN. Medical progress: Cushing syndrome. N Engl J Med995;332:791-803.1. Abramovitch R, Tavor E, Jacob-Hirsch J, Zeira E, Amariglio N, Pappo O, et al.
pivotal role of cyclic AMP-responsive element binding protein in tumor progression.ancer Res 2004; 64;1338-46.
2. Lanotte M, Riviere JB, Hermouet S, Houge G, Vintermyr OK, Gjertsen BT, etl. Programmed cell death (apoptosis) is induced rapidly and with positive cooperativityy activation of cyclic adenosine monophosphate-kinase I in a myeloid leukemia celline. Cell Physiol 1991;146:73-80.3. Yong EL, Baird DT, Hiller SG. Mediation of gonadotrophin-stimulated growthnd differentiation of human granulose cells by adenosine-3’, 5’-monophosphate: oneolecule, two messages. Clin Endocrinol (Oxf) 1992;37:51-8.
4. Lania A, Persani I, Ballare E, Mantovani S, Lossa M, Spada A. Constitutivelyctive Gs alpha is associated with increased phosphodiesterase activity in human GGH-ecreting adenomas. J Clin Endocrinol Metab 1998;83:1624-8.5. Ooms LS, Koster MJ, Mitchell JR, Pals-Rylaarsdam R. Identification of a second-ite suppressor mutation of the GTPase defect associated with McCune-Albright
yndrome: a model using the yeast heterotrimeric G protein, GPA1. Arch Physioliochem 2006;112:166-73.The Journal of Pediatrics • June 2008

F
Tt
24 60.4 45.8
P
igure 2. Back at presentation.
rolonged Remission of Severe Cushing Syndrome without Adrenalecto
able I. Intravenous dexamethasone suppressionest showing no suppression of hypercortisolemia
Time(h)
Cortisol(�g/dL)
ACTHpg/mL
�0.25 69.60 56.9 33.41 542 48.9 38.83 48.44 38.15 51.056 55.2 457 52.038 56.2
23 53.8
my in an Infant with McCune-Albright Syndrome 884.e1

Tde
To
8
able II. CRF stimulation test at the time ofiagnosis showing no effect of CRF on levels ofither ACTH or cortisol
Time(min)
Cortisol(�g/dL)
ACTH(pg/mL)
�15 61.0 32.00 57.0 40.15 52.4 32.0
15 52.7 29.330 52.3 30.245 52.8 40.160 56.6 35.6
his indicates independent cortisol secretion by the adrenal glands causing suppression
f ACTH production.84.e2 Gillis et al The Journal of Pediatrics • June 2008

T
41
1
5
M*†
F
P
able III. Ultrasound evaluation of the adrenal glands
Age
Left adrenal–axes* Right adrenal–axes*
Long Axial (AP) Transverse Long Axial (AP) Transverse
months 21 13 9 18 14 12year 19 10 8 11 7 6
year & 10 months 9† 6† 4† Barely visible†
years & 5 months Barely visible†
easurements of the adrenal glands by ultrasound from diagnosis until after clinical resolution of Cushing syndrome showing decrease in size.
All measurements are in mm.Adrenal glands were barely visible—this is normal for age.igure 4. Face at age 3.5 years, with no Cushingoid features
rolonged Remission of Severe Cushing Syndrome without Adrenalectomy in an Infant with McCune-Albright Syndrome 884.e3

F
8
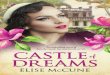
igure 5. Growth chart during infancy demonstrating resolution of Cushingoid anthropometric characteristics.
84.e4 Gillis et al The Journal of Pediatrics • June 2008