Embed Size (px)
Citation preview

1/77
Project Plan to Support the Transformative Redesign of the Mental Health and Addiction Services for the Future in the South East Region by 2015/16 March 31st 2013

2
Table of Contents
Introduction 4
Part I: Need for Change 6
Global and National Context 7
Provincial Context 7
South East LHIN Context: Mental Health and Addiction Sector 9
Vision for the Mental Health and Addiction System 22
System Outcome Goals 24
Summary: Need for Change 25
Part II: Project Plan 27
A. Overview of the Project Plan 28
B. Project Planning Leading Practices 29
C. Planning Principles 30
D. Project Plan 31
Appendices 54

3
Appendix 1: Change Management Considerations 55
Appendix 2: Stakeholder Management Considerations 55
Appendix 3: Risk Assessment and Mitigation 65
Appendix 4: Summary of Stakeholder Engagement 67
Appendix 5: Project Manager Role Description 74
Appendix 6: Examples of Planning Commitees 76

4
Introduction The South East LHIN will lead the redesign of the Mental Health and Addictions services in collaboration with the Mental Health and Addictions providers This document is presented in two parts. Part I: “Need for Change” provides an overview at a global, provincial and LHIN level as to why the LHIN and the providers are going to focus on the redesign of services for the future. Part II: “Project Plan” provides a detailed plan which will be used by the LHIN to provide a structured process to support the transformative redesign and implementation of the services for the future. Both Part I and Part II can be separated and used as standalone documents. Overview of Phases and Timing The Project Plan will be launched April 1st 2013. The work of determining the redesign itself will take place over FY 2013/14 (redesign to be completed by December 2013), with implementation set to occur during the subsequent two fiscal years (2014/15 and 2015/16). Each phase is described with the estimated timeframes in the figure below:
The Project Plan is included in this document, in Part II.
Implementation of the redesigned
Mental Health and Addiction SystemPlan for the redesign of the Mental
Health and Addiction sector
Redesign of the Mental Health and
Addiction sector
Phase
Process
Timing
South East LHIN and Mental Health
and Addiction providers work
collaboratively to implement the new
model for the system
Develop Project Plan through review
of existing work and stakeholder
engagement (KPMG)
South East LHIN and Mental Health
and Addiction providers work
collaboratively to redesign the sector
using the Project Plan as guidance
FY 2014/15 - 2015/16Complete by December 2013 Complete by FY 2013/14
IMPLEMENTPLAN REDESIGN
Transform from a Sector to a System where we plan, work and collaborate together for the purpose of our
residents

5
Scope of System Redesign
The South East LHIN is leading the redesign and implementation phase of this project. The LHIN has conducted multiple community and stakeholder engagement processes and heard from the clients/patients/users/residents/providers that there are opportunities for improvement. This feedback is driving the redesign, in particular the focus on the development of a “system”. The ideal health care system is described in the Drummond Report (2012)1, “It would be patient-centric and would feature co-ordination along the complete continuum of care that a patient might need.” The role of each LHIN is to provide leadership to move the sector towards system integration. Section 24 of the Local Health System Integration Act notes that, “Each local health integration network and each health service provider shall separately and in conjunction with each other identify opportunities to integrate the services of the local health system to provide appropriate, coordinated, effective and efficient services.” To achieve this and the vision of an ideal health system the South East LHIN will be the lead and work collaboratively with the providers to develop the Mental Health and Addiction system for the future. In scope for the system redesign is: LHIN funded Mental Health and Addiction Providers and services/programs across the
continuum Redesign of structures, processes, leadership and service configurations within the current
resources.
As far as possible, the intent is to collaborate in the development and to gather input and feedback on potential options with all Mental Health and Addiction providers and services. For those services not funded by the South East LHIN, the plan needs to incorporate opportunities for engagement and assessment for alignment with the redesign. The following section, “Need for Change” provides the global, provincial and LHIN context for the redesign project.
1 Commission on the Reform of Ontario's Public Services

6
Part I: Need for Change How to read Part I: Need for Change The South East LHIN and Mental Health and Addiction providers and users will step into the future to determine what a high-performing, integrated, patient-centered system could look like. Part I: “Need for Change” provides the rationale for why the change/redesign will be undertaken. Context is provided on the thinking around Mental Health and Addiction systems within Canada (federally and provincially) and internationally. Current state information is also provided on the South East LHIN region’s Mental Health and Addiction services and how the partners are currently working together. To provide parameters for future state discussions, the provincial and LHIN vision and system outcome goals are included. In closing this section, a summary is provided of the “Need for Change” for the transformative redesign of the Mental Health and Addiction sector.

7
Global and National Context The Mental Health and Addiction sectors are on the precipice of transformational change. Key reports and strategies have been released challenging both governments and providers to look at Mental Health and Addiction services in a different way. Rather than relegating addictions and mental health and those it affects to the shadows, there are new strategies emerging that recognize the importance of mental health as essential to our quality of life. In the recently released “Changing Directions, Changing Lives – The Mental Health Strategy for Canada” the Mental Health Commission of Canada acknowledged the truth of the statement “there cannot be health without mental health”. Further, it is acknowledged that mental health problems and illnesses are prevalent in our country. It is a well cited statistic that more than one in three Canadians will suffer from some form of mental illness, with a cost to the economy of Canada well in excess of $50 billion2. Mental health and substance use disorders co-occur in approximately 20 percent – or one in five – of people treated for mental disorders in Ontario’s hospitals and mental health clinics. Within specific groups the rates are even higher: younger adults (55%), people receiving specialty inpatient care (28%), and those with personality disorders (34%). Therefore, it is important that risk management strategies be included in treatment and support models for ALL clients – those with mental health problems and illnesses, those with addiction disorders and those with both. Throughout Canada and beyond, the trend is for mental health providers and addiction providers to collaborate and provide coordinated patient care while respecting the individual needs of each client/patient type. The UK government, jointly with a range of providers/think tank organizations, released a mental health implementation framework – “No health without mental health: implementation framework3.” This framework provides direction to local organizations to implement the mental health strategy. The overriding message in the document is that “It is local leaders who can take action to ensure a range of services work together to promote wellbeing, to tackle the causes of mental ill health, and to act quickly and effectively when people seek the support they need to make their lives better.”
Provincial Context The Ontario government has developed a new strategy for the Mental Health and Addiction sector. "Open Minds, Healthy Minds: Ontario's Comprehensive Mental Health and Addictions Strategy." This follows Ontario's previous mental health strategy, "Making It Happen." The new Mental Health and Addiction strategy focuses on a person-centred approach, across the life span. The strategy is intersectoral and inter-ministerial in scope and is intended to align with various other Ontario initiatives, including new strategies arising from the Excellent Care Act for All
2 Smetanin, 2011
3 July 2012

8
Act, the Poverty Reduction Strategy, Early Learning Strategy and the Long-Term Affordable Housing Strategy.
Ontario's new Mental Health and Addiction strategy has four guiding goals:
Improve mental health and well-being for all Ontarians
Create healthy, resilient, inclusive communities
Identify Mental Health and Addictions problems early and intervene
Provide timely, high quality, integrated, person-centred health and other human services. 4
This strategy is currently being implemented. Twelve of the 14 Ontario LHINs have Mental Health and Addiction as a core priority of their Integrated Health Service Plans. To various extents, these LHINs will be embarking on a transformative journey similar to the South East LHIN.
Key Takeaways: Globally and across Canada, the literature and practices underscore the need for
cooperation and collaboration at a system level between Mental Health and Addiction providers.
Local leaders are in the right position to focus on the patient’s perspectives and to create
a system that meets the needs of the patient.
Mental Health and Addiction is a priority for the Ontario government. The South East LHIN is operationalizing this priority for the South East LHIN region’s residents which was highlighted in their Integrated Health Services Plan 3: Better Integration, Better Health Care.
4 http://www.ontario.cmha.ca/policy_and_research.asp?cID=199259
9
South East LHIN Context: Mental Health and Addiction Sector Overview There are 22 community Mental Health and Addiction service providers/programs that are funded by the South East LHIN, providing a range of programs and services. The LHIN may not be the sole funder of these providers/programs. These are listed below and the geographical location of the providers/services/programs is shown in Figure 1. Addictions Centre Hastings and Prince Edward Brockville and Area Centre for Developmentally Handicapped Persons Brockville General Hospital Canadian Mental Health Association, Leeds-Grenville Branch Community Care Access Centre School Services Frontenac Community Mental Health and Addiction Services Hotel Dieu Hospital – Mental Health Kingston Community Health Centres Kingston General Hospital Lanark County Mental Health (Perth Smiths Fall District Hospital) Leeds and Grenville Mental Health Lennox and Addington Addiction and Community Mental Health Services Mental Health Services Hastings and Prince Edward Mental Health Support Network South East Ontario Providence Care Quinte Health Care Salvation Army Habour Light Centre Sexual Assault Centre for Quinte and District Sexual Assault Centre Kingston The Brock Cottage Tri County Addiction Services Youth Habilitation, Quinte This list does not include private service providers (e.g. psychiatrists) and cross-sector providers that also may provide Mental Health and Addiction services (i.e. municipal, housing etc.).

10
Figure 1: Community Mental Health and Addiction Services Providers in the South East LHIN

11
Key Takeaways: There are a range of providers, programs and services offered in the LHIN region. The
South East LHIN may not be the only funder of these organizations. In the redesign, the LHIN and the providers will need to be cognizant of the difference in payment structures and service provision/relationships within the health sector and external to the health sector.
The geographic span of the South East LHIN is large and includes both urban and rural areas. The system redesign must consider both urban and rural models and opportunities for the use of technology.
Collaboration: Planning and networking There is considerable inter-sectoral networking and collaborating in the South East LHIN between Mental Health and Addiction providers. Within the LHIN region, there are three sub-regional groups that meet at least quarterly. These include: The Frontenac, Lennox and Addington Addiction and Mental Health Coalition Hastings and Prince Edward Addiction and Mental Health Coalition Lanark, Leeds and Grenville Addiction and Mental Health Coalition
Additionally, there are three Clinical Services Roadmap Mental Health and Addiction working groups – Emergency Department, Health Human Resources and Coordinated Access. Members on these groups are senior staff/clinicians from a range of hospital and community providers. The Addictions and Mental Health Network meets on a quarterly basis. In total, there are approximately 45 planning groups in the South East LHIN focused on a range of mental health and addiction issues. These are listed in Appendix 6. Key Takeaways:
There is existing collaboration in the LHIN region. There is an opportunity to harness the momentum and collaboration for the purpose of a system wide redesign, to more effectively achieve improved outcomes.
There are a number of Mental Health and Addiction planning groups. Though these meetings may have different objectives, there may be an opportunity to streamline the planning groups which will allow for more capacity (both administrative and service) in the system.

12
Collaboration: Regional initiatives Within the sector, providers are working together on a number of regional initiatives, for example providers have service agreements with other provider organizations which support the development of integrated treatment plans. The sector has and continues to work together on a number of initiatives. A list is provided in the table below – this is not an exclusive list but is included to provide an overview of the collaboration within the LHIN:
Current Initiatives:
Description:
Health Links Health Links will encourage greater collaboration between local health care providers, including family care providers, specialists, hospitals, long-term care, home care and other community supports. With improved coordination and information sharing, patients will receive faster care, will spend less time waiting for services and will be supported by a team of health care providers at all levels of the health care system. There are 7 Health Links to be implemented in the South East LHIN. These are still in the planning stages, but several have been identified Mental Health and Addictions as a priority.
Clinical Services Roadmap: Mental Health and Addictions
Health Human Resources Plan: The HHR leadership group is tasked with developing a health human resource plan for mental health and addictions to ensure that SE LHIN providers can align with the intent of the provincial Mental Health and Addiction strategy. The outcome will support quality care and improved access to Mental Health and Addiction services across the continuum of care. Current Tasks Include:
The development of a competency framework and training toolkit to be implemented across the Mental Health and Addiction sector. This will enable the workforce to deliver consistent, quality mental health and addictions treatment, supports and services
The development of a psychiatry human resource plan for the South East LHIN system of Mental Health and Addiction
A comprehensive HR strategy focusing on, Chronic Disease/Community Model of Care and Recovery approach
The development of Anti-Stigma training (building upon existing tools) to be implemented in each HSP interacting with Mental Health and Addiction clients (e.g. hospitals, primary care etc.)
Emergency Departments: The Emergency Department leadership

13
group is tasked with improving service response time and access to care for Mental Health and Addiction patients, as well as patients presenting with challenging behaviors. Current Tasks Include:
The design and implementation of a Transitional Intensive Therapy Outpatient Program for Mental Health and Addictions clients (from both ER and community).
The development of a Memorandum of Understanding: Privacy and Consent
The development of a shared care plan process and data sharing of care plans
The completion of LEAD protocol agreements
Coordinated Access: The Coordinate Access leadership group is tasked with enhancing various forms of coordinate access and referral (CAR) for consumers requiring Mental Health and Addiction services across the region. Coordinated Access focuses on a single point of entry (such as a 310-Line) with geographical points of access that have standardized referral forms and assessment tools, that will be shared with other healthcare providers in a timely manner. Current Tasks Include:
Development of a common ‘preliminary screener’ intake form
Development of a common referral form
Implementation of a 310-OPEN crisis line, allowing for 24/7 access to crisis support
Focus on improving transitional support for youth to adult services
HSRC (Tier III)
Implementing the Health Service Restructuring Commission (HSRC) Directives in the South East LHIN includes Tier III or a hospital to community transfer of patients or services. The South East LHIN and its partners continue to implement Tier III directives (transfer of patients from ROHCG to appropriate community settings and from Providence Care to appropriate community settings). Continued implementation of Tier III Directives for Providence Care and BMHS
Transfer of approximately 50 patients to community services.
Closure of approximately 50 beds within 5 years
Transitional Aged Youth The South East LHIN provides funding to Youth Habilitation Quinte
14
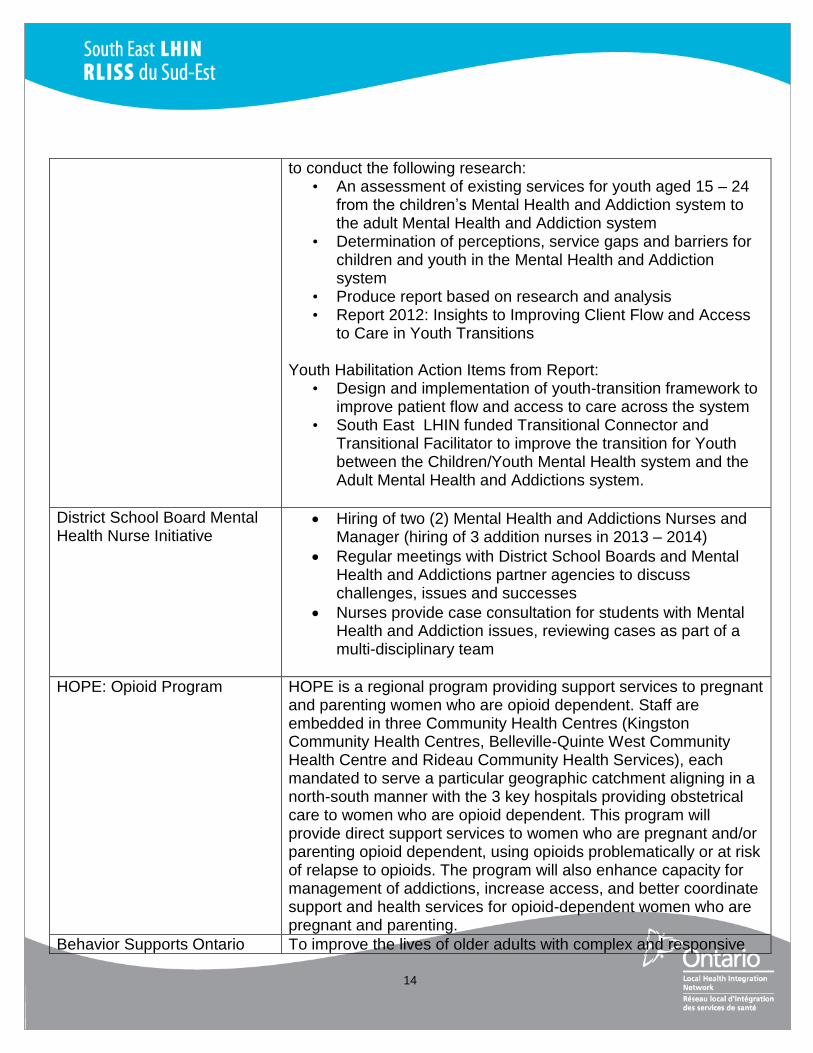
to conduct the following research: • An assessment of existing services for youth aged 15 – 24
from the children’s Mental Health and Addiction system to the adult Mental Health and Addiction system
• Determination of perceptions, service gaps and barriers for children and youth in the Mental Health and Addiction system
• Produce report based on research and analysis • Report 2012: Insights to Improving Client Flow and Access
to Care in Youth Transitions Youth Habilitation Action Items from Report:
• Design and implementation of youth-transition framework to improve patient flow and access to care across the system
• South East LHIN funded Transitional Connector and Transitional Facilitator to improve the transition for Youth between the Children/Youth Mental Health system and the Adult Mental Health and Addictions system.
District School Board Mental Health Nurse Initiative
Hiring of two (2) Mental Health and Addictions Nurses and Manager (hiring of 3 addition nurses in 2013 – 2014)
Regular meetings with District School Boards and Mental Health and Addictions partner agencies to discuss challenges, issues and successes
Nurses provide case consultation for students with Mental Health and Addiction issues, reviewing cases as part of a multi-disciplinary team
HOPE: Opioid Program HOPE is a regional program providing support services to pregnant and parenting women who are opioid dependent. Staff are embedded in three Community Health Centres (Kingston Community Health Centres, Belleville-Quinte West Community Health Centre and Rideau Community Health Services), each mandated to serve a particular geographic catchment aligning in a north-south manner with the 3 key hospitals providing obstetrical care to women who are opioid dependent. This program will provide direct support services to women who are pregnant and/or parenting opioid dependent, using opioids problematically or at risk of relapse to opioids. The program will also enhance capacity for management of addictions, increase access, and better coordinate support and health services for opioid-dependent women who are pregnant and parenting.
Behavior Supports Ontario To improve the lives of older adults with complex and responsive

15
behaviours associated with cognitive impairments due to complex mental health, addictions, dementia, or other neurological conditions, people at risk of the same and their caregivers. Components include:
Enhance coordination among existing behavioural services
Develop new care pathways and clinical tools
Identify/translate best practices
Provide coaching/mentoring/knowledge transfer
Evaluate outcomes for province-wide implementation and
dissemination
Concurrent Disorder Project: Phase II
The Concurrent Disorder Project focuses on creating an inventory of health human resources, skills, competencies, and identification of required skills and competencies. The next steps are the development of a training plan for staff within the South East region. Stakeholders view this project as an example of a successful collaboration and a foundational project so support the continuing redesign of the sector.
Key Takeaways
As part of the redesign phase, each existing regional initiative should be reviewed to assess alignment with the system outcome goals and the options for the redesign. In particular there will need to be a process to ensure that the work of Health Links is considered in the redesign phase.
Data A number of data sources were reviewed to identify information to support the “Need for Change”: The Regional Capacity Project Data Analysis Update provides a snapshot of the utilization in the
South East LHIN The LHIN Mental Health and Addiction profile report The LHIN Quarterly Performance Review A summary of the relevant information is provided in the table below: Data Snapshot of the South East LHIN Region
Regional Capacity Project Data Analysis Update

16
o The number of individuals treated for substance abuse in the SE LHIN has increased by 72% in the period 2007 to 2011
o The SE LHIN has the 3rd highest rate per 1000 population in Ontario for new referrals in 2011 and is rated 4th highest for number of individuals served (per 1000 population).
o The South East LHIN has the 3rd highest rate per 1,000 population in Ontario for inpatient / resident days in 2011 and is rated 5th highest for number of face-to-face patient visits (per 1,000 population).
The table below shows the number of patients, by service type from 2009-2011. There has been a 4% increase in the volume of patients from 2009-2010 and 7% increase from 2010-2011. The largest increase by service type is in crisis intervention, clinic visits and and supports within housing.
LHIN Mental Health and Addiction Profile Report (draft): Analysis was conducted on substance abuse utilization of services. The graphic included shows that there is variation in the different services used during the period of 2004-2011. For new substance abuse cases (new relates to service received for a new case. If a client has been discharged and returns for services the new category will apply) the utilization of community treatments has increased from 2009-2011 and there is a steady increase in the utilization of withdrawal management services (new cases). Carry over utilization rates appear to have decreased during 2004-2011 for many services, except residential treatment and withdrawal services which have stayed steady – carry over relates to services carried over into the next fiscal year for any client.

17
Number of Open Admissions for Substance Abuse by Program Service Category, Fiscal 2004-2011
LHIN Quarterly Performance Review: Repeat unplanned Emergency Visits for Mental Health
o Current performance for repeat unplanned emergency visits within 30 days for mental health conditions is 18.6% o The LHIN is performing well against FY12/13 target (SE LHIN target 12/13 is 18.9%, with an
acceptable performance range of 21.0%) however there is significant opportunity for improvement
o There has been a drop in repeats within 30 days for Mental Health clients between FY11/12 Q3 and Q4; but performance has plateaued from FY11/12 Q4 to FY12/13 Q1
18
o Repeat unplanned Emergency Visits for Substance Abuse Current performance for repeat
unplanned emergency visits within 30 days for substance abuse conditions is 23.2% o The LHIN is not performing well against FY12/13 target (SE LHIN Target 12/13 is 16.5%,
with an acceptable performance range of 18.2%) o There has been an increase in repeats within 30 days for addictions clients between FY11/12
and FY12/13 (~18.7% in FY 11/12 and 23.2% in FY12/13)
Key Takeaways: Number of individuals requiring Mental Health and Addiction Services has increased as
well as the number of repeat visits for these individuals has increased. We know we have to work within the resources we have available in the South East. Given that fact, the impact on the sector of an increase in volume is pressure on the existing capacity. Working together collaboratively across the system should result in increased capacity through standardization, sharing of resources, reduction of duplication and increased knowledge of the services and programs that are available.
The number of unplanned ED visits for Mental Health patients is within LHIN target but for Addiction clients is above target. There are opportunities for both groups to redesign client pathways to further reduce unplanned ED visits.
Community/Stakeholder Engagement The South East LHIN has conducted a number of community engagement sessions which has led to the development of the Clinical Services Roadmap (July, 2010) and the third Integrated Health Services Plan: Better Integration, Better Health Care, 2013-2016 (February, 2013). Analysis of community feedback identified that, to a large extent, the services provided to Mental Health and Addiction clients/patients are of a good quality. Areas for improvement were identified in: Access to care (e.g. lack of 24 hour access, inequitable access to psychiatric care based on
geography) Inconsistencies between services Multiple assessments and duplication Insufficient volumes of services Stigma often faced in accessing Mental Health and Addiction services. As is consistent across other sectors and in health services across the globe, the main area for improvement was the transition between providers across the region and the coordination of care across the continuum of care. Additionally, there are gaps in health human resources as identified in the Clinical Services Roadmap. Stakeholders identified demand for case managers, counseling and psychiatry. In March 2013, KPMG (consultants) conducted a focus group session with 10 individuals with a range of mental health and addiction experience. These individuals were the consumer

19
representatives for the Mental Health Support Centres across the South East Region. Representatives were present from Belleville, Madoc, Picton, Trenton, Bancroft, Napanee and Kingston. Their perceptions and thoughts on the current and future of the Mental Health and Addiction system are provided here. What is working well……. Peer support is very valuable. Resources, that are available such as nurse practioner clinics, hospital liaison services and
outreach programs, are great. On one occasion I called the crisis line at the hospital and the crisis worker and doctor met me at
the hospital to help guide me to the right service. This was seen as excellent. Opportunities for improvement….. I feel lost when I am in the system, I don’t get told the information I need to know and the
coordination between the hospital and community doesn’t exist. I was left with no support. There are fewer resources in smaller rural communities and if you are without transport there is
no way to access services in other parts of the region. Many expressed that they were not aware of many services, such as Mental Health and
Addictions centres. There is insufficient access and availability of alternative treatments. There is an issue with access to services which is why the ED is used as the last resort as it is
always open. However, we sometimes feel stigma going to the ED (security guards are not always welcoming).
What would you like your experience in the mental health and addiction sector/services to look like in the future? I want there to be increased awareness for people with mental health and addiction issues.
There needs to be less labeling. I would also like to know more about available services and programs.
I would like more proactive care and there to be more responsibility for people with mental health and addictions. Stop “dumping” us.
It would be great if we could have someone to support us on our journey through the system. No matter where you live, I would like everyone to have equal access to support. There needs to be more access to services, to psychiatrists and to medication. We go to the ED
as there is no other accessible service. I would like there to be more dignity for us in the system.

20
What else would you like to share with us?
In the mental health and addiction sector, people have different levels of comfort and it will be difficult to develop solutions that meet all needs. Therefore there should be a variety of programs and services in a variety of settings to meet many needs
The current focus is too much on “fixing” people Peer Support Networks are great places to “use” as an access point, for example providing
counseling or a nurse. We are comfortable coming here. We like choices, i.e. traditional medicine, alternative therapies etc. We want to help spread the word about programs and services and gather feedback and input
for the purpose of the redesign Four personal stories are included which support the need for change……
Key Takeaways: Residents in the South East LHIN have expressed a number of opportunities for
improvement in the Mental Health and Addiction sector – it is the LHIN’s and the providers responsibility to work together to create one integrated system for these patients/clients.
Leon went for many years to his family doctor
but they dismissed his anxiousness and he felt like they “laughed” at him. When they realized
he had a mental health issue, they did not know
the services out there or where to refer. He found support and guidance in the local Support
Network.
Claire is dual diagnosis. She moved into the South East region and was referred from her previous
psychiatrist to the local Mental Health and
Addiction centre. She was told at the pharmacy
(when she went to pick up her medication) that she
did not have a doctor at the centre and therefore could not pick up her medication. She tried to self -
refer to the centre but was not able to and as a
result had to “come off” her medication. She has
since managed to self-refer to a doctor at the local
hospital.
Francis was put on a wait list to see a
psychiatrist. It was communicated to him that he would have to wait for some time. He was
unhappy with waiting especially as no one could
tell him when he might have an appointment. He has not had a diagnosis for his mental health
issue and cannot receive disability allowance. This impacts his quality of life.
Many members of Dave’s family have mental
health and addiction issues. He has depression, his son is an addict and has bipolar and his
daughter has mood issues. He has had both
negative and positive experiences in the system. His son’ experience in the hospital was very
scary for him, e.g.- they would leave needles in his room. Further there was no community
support when he was discharged. He has had
positive experience with the Nurse Practitioner model
21
Community engagement has highlighted the need to improve the transitions of care between providers (the quality of care was in most cases great but the journey was difficult)
Community engagement has highlighted that there is an opportunity to “bring” services to where clients/patients feel more accepted and comfortable, such as in Peer Support Network Centres and that there is a lack of awareness of how to access services in the Mental Health and Addictions sector.
Wider sector redesign initiatives Within the South East region, there are further collaboration and redesign initiatives that are being pursued which impact the Mental Health and Addiction sector. For example, the development of Service Collaboratives which are being led by the Ministry for Children and Youth Services. This initiative, which crosses six ministries, is being implemented by CAMH. As the project moves forward, CAMH will engage in discussions around how the Service Collaboratives will engage with children’s planning tables, ‘Working Together’ communities, and existing youth justice community tables.5 At a ministerial level, there is a concerted effort to coordinate the mental health strategies for children and youth. Key Takeaways: The LHIN and providers must be cognizant of other cross-sector initiatives and consider
the impact of these in the design of the new system and ensure on-going communication to inform other sector initiatives.
5 http://everykid.on.ca/camh-set-service-collaboratives/
22
Vision for the Mental Health and Addiction System Vision statements are included to provide guidance on the future state for the South East region’s Mental Health and Addiction services: Provincial Vision An Ontario where every person enjoys good mental health and well-being throughout their
lifetime, and where all Ontarians with mental illness or addictions can recover and participate in welcoming, supportive communities. (Open Minds, Health Minds, Ontario’s Comprehensive Mental Health and Addictions Strategy)
South East LHIN Vision Ensure patients receive the right care at the right time in the right place, enhance capacity of
providers and the system, and reduce stigma. (South East LHIN Integrated Health Services Plan: Better Integration, Better Health Care, 2013-2016)
In September 2011, a number of providers of Mental Health and Addiction Services in Southeastern Ontario came together to host a conversation regarding the transformation of Mental Health and Addiction services in Southeastern Ontario. As part of this session, the providers described the components and characteristics necessary to achieve the vision for Mental Health and Addiction system in Southeastern Ontario:
Improving pathways for people to navigate the system of services Transforming models of service delivery to enable an integrated system of services and
supports Creating multi-level care and support that keeps people connected with their communities Building a welcoming community Creating services and supports that address broad determinants of health Supporting people to live their lives as citizens of the community New collaborative/integrated leadership models Mainstream employment for people with Mental Health and Addiction issues.
(From the document – Partnerships Working Together For Change – Walk out/ Walk on retreat, 2011)

23
Commonalities: Patient centric
Focuses on continuum of care
Focuses on patients “whole” experience and role in community(not just quality of health care provided at one point in time)
The vision statements of the Province and South East LHIN should be key statements that drive the continuing design of the Mental Health and Addiction services. The characteristics and components discussed by a number of providers will also be key information used to guide the redesign efforts. When deciding on changes to system configuration or programs/services, the extent to which these changes will support the vision must be considered.

24
System Outcome Goals
System outcome goals describe the attributes of the future system that are to be realized. System outcome goals are included to provide guidance on the future goals and measures for the South East LHIN’s Mental Health and Addiction system.
System Outcome Goals
Measurable Outcomes
1. Access to equitable, consistent and quality care across the South East LHIN
Reducing or eliminating barriers to access (E.g. translation, transportation, childcare etc.)
Same basket of services offered across the LHIN
Standardized process for accessing services
Reduction in waitlist for Mental Health and Addiction clients
2. Improved patient experience - The system is reflective and responsive to the legitimate expectations and needs of the population
System responsiveness to meet client need at the initial point of contact with the sector
Coordination of services and knowledge exchange among care/service providers
Client satisfaction with their journey to access system and with care provision
Reduction in Stigma –social acceptability
Minimizing gaps in transition or issues with transition
3. Health Outcomes – The health of the Mental Health and Addiction population is improved
Reduction in 30-day repeat Emergency Department visits (both Mental Health and substance abuse clients)
Reduction in 30 day readmits for Mental Health and Addiction issues
Reduction in patients designated as ALC due to challenging behaviours
Reduction of unnecessary hospitalization related to lack of service coordination or provision
Reduction in crisis intervention needed for existing Mental Health clients
4. Sustainability of the system - Accountability at an organizational level shifts to accountability at a regional level
Improved capacity within the system with the resources currently available (e.g. reducing duplication of services, improving processes and patient flow improvement, etc.)
Accountability agreements include regional perspective.
The system outcome goals should be referred to throughout the design of the Mental Health and Addiction services. As part of the redesign phase, specific measure will need to be identified with targets for the system.

25
Summary: Need for Change The context, the current state overview and the future vision and system outcome goals provides a strong case to support the redesign of the Mental Health and Addiction services with the interest of the patient as the key driver and through building on the strengths of each of the providers. A summary of the need for change is provided: 1 Residents in the South East LHIN have expressed a number of opportunities for change in
the Mental Health and Addiction sector – it is the LHIN’s and the providers responsibility to work together to create one integrated system for these patients/clients.
2 Community engagement has highlighted the need to improve the transitions of care between providers (the quality of care was in most cases great, but the journey was difficult).
3 Number of individuals requiring Mental Health and Addiction Services has increased as well as the number of repeat visits for these individuals has increased. We know we have to work within the resources we have available in the South East. Given that fact, the impact on the sector of an increase in volume is pressure on the existing capacity. Working together collaboratively across the system should result in increased capacity through standardization, sharing of resources, reduction of duplication and increased knowledge of the services and programs that are available.
4 There is existing collaboration in the LHIN region. There is an opportunity to harness the momentum and collaboration for the purpose of a system wide redesign, to more effectively achieve improved outcomes.
5 Local leaders are in the right position with which to focus on the patient’s perspectives and to create a system that meets the needs of the patient.
6 Globally, and within Canada, the literature and practices underscore the need for cooperation and collaboration at a system level between Mental Health and Addiction providers.
7 Mental Health and Addiction is a priority for the Ontario government. The South East LHIN is operationalizing this priority for the South East LHIN region’s residents which was highlighted in their Integrated Health Services Plan 3: Better Integration, Better Health Care.

26
To fulfill the provincial and LHIN vision and to achieve the system outcome goals, the sector will need to look to the future, determine what the attributes of the future system are and then identify how to get there – this Project Plan is the roadmap of how to get there. Figure 2 provides a visual of the three phases of this work and the influence the redesign and implementation phases will have on ultimately achieving the system outcome goals and vision for the South East LHIN. Figure 2: Visual of the three phases of the Project Plan and how they will support the system outcome goals and vision of the Mental Health and Addiction system for the South East LHIN.
Part II: “Project Plan” of this document is included in the next section. This provides a step by step reference for the development and implementation of the future redesign for the Mental Health and Addiction sector in the South East LHIN.
Implementation of the redesigned
Mental Health and Addiction SystemPlan for the redesign of the Mental
Health and Addiction sector
Redesign of the Mental Health and
Addiction sector
Phase
Process
Timing
South East LHIN and Mental Health
and Addiction providers work
collaboratively to implement the new
model for the system
Develop Project Plan through review
of existing work and stakeholder
engagement (KPMG)
South East LHIN and Mental Health
and Addiction providers work
collaboratively to redesign the sector
using the Project Plan as guidance
FY 2014/15 - 2015/16Complete by December 2013 Complete by FY 2013/14
IMPLEMENTPLAN REDESIGN
Transform from a Sector to a System where we plan, work and collaborate together for the purpose of our
residents
Ensure patients receive the right care at the right time in the right place, enhance capacity of providers and the
system, and reduce stigma
LHIN vision
(aligns with
Province and
Providers)
System
Outcome
Goals
Access to equitable,
consistent and quality care
Improved patient
experience
The health of the
population is improved
Sustainability of the
system
27
Part II: Project Plan How to read Part II: Project Plan The South East LHIN, together with the Mental Health and Addiction providers and clients/patients will step into the future to determine what a high-performing, integrated, patient-centered system will look like. Part II: “Project Plan” provides structured guidance to lead the redesign and implementation phases of the work. Key sections are listed below: A. Overview of Project Plan: Information is provided on how the Project Plan was developed and
how it should be used. B. Project Planning Leading Practices: A summary of project planning leading practices as
related to design and implementation is provided. C. Planning Principles: Principles to guide the project planning, redesign and implementation
phases are provided. These are NOT the principles that should be used to develop the redesign of the sector (these should be patient/client centric). These are to be used by the Project Manager and the provider representatives to guide the planning processes.
D. Project Plan: For each of the two phases – redesign and implementation – a description of each phase is provided with tasks, responsibilities, timelines and additional information to support each of these phases.
A number of Appendices are also included: Appendix 1: Change Management Considerations Appendix 2: Stakeholder Engagement Considerations Appendix 3: Potential Risks and Mitigations Appendix 4: Summary of Stakeholder Engagement (information is included but stakeholder
engagement is on-going) Appendix 5: Project Management Job Description Appendix 6: Examples of Planning Commitees

28
A. Overview of the Project Plan The South East LHIN will lead the redesign of the Mental Health and Addictions services in collaboration with the Mental Health and Addictions providers. This document is a Project Plan to be used by the South East LHIN and Mental Health and Addiction providers to redesign the sector with the objective of developing a seamless experience for clients/patients.
A project plan includes: a task list, resource allocation, cost estimates, and timeline (or schedule). These four variables make up the overall project plan, which details the actual work to be performed in order to create the deliverables or meet an objective. Project plans are the work plans for ultimately creating deliverables.
It is recommended that a Project Manager be identified by the South East LHIN to manage the implementation of the project plan. This Project Manager would be one FTE whose only responsibility is the execution of the project plan for the redesign and implementation phase. An example job description is provided in Appendix 5. Purpose of Project Plan To be used by a Project Manager to guide the redesign of the Mental Health and Addiction
Services To be used by the LHIN and Mental Health and Addiction providers as a reference document to
guide the redesign of the Mental Health and Addiction Services. Development of the Project Plan A consultancy firm (KPMG) was engaged by the South East LHIN to develop the project plan. The firm conducted the following steps to develop this plan: 1. Document Review A document review was completed on the current state of the sector to determine the initial structure of the project plan. See Part I: Need for Change for summary of findings. 2. Stakeholder Engagement Stakeholder engagement was completed with representatives from each of the Mental Health and Addiction provider sub-regions, the regional psychiatry group and with a sample of individuals with a range of mental health and addiction experience – see Appendix 4 for a list of providers interviewed. The engagement sessions were used to gather insight into what has worked and what has not worked related to planning, redesign and implementation initiatives. Further opinion was gathered on how stakeholders would like to be engaged in the development of the project plan, the redesign and implementation phases. Appendix 4 includes a summary of the messages heard from the stakeholders and, where relevant to the project plan, is included within this document. Feedback gathered will be relevant for the redesign and implementation phases – the Project Manager is responsible for ensuring insights gathered are considered during each phase. 3. Leading Practices Review (see Section B: Project Planning Leading Practices)

29
B. Project Planning Leading Practices Leading practices related to redesign and implementation were also considered and included in the development of this Project Plan. These are summarized below:
Leading Practices: Redesign Leading Practices: Implementation
Development of a committee/group to inform the redesign with diverse representation to ensure that once developed, key stakeholders feel they have had their influence and impact. The committee/group should have a clear Terms of Reference with details of expected deliverables.
Provide sufficient time and resources for planning, implementation, and stabilization. (Amy D. Bentona; Michael J. Austin, 2010)
Share coordinated and consistent Information - ensure objectives, timings and progress is reported to stakeholders
Demonstrate a commitment that the purpose and intent of the redesign is the increase in capacity to deliver integrated services
Appoint an individual to manage the project, hold this person accountable for successful implementation of tasks and timings
Senior management needs to be a champion of change by expressing support for a redesign and framing it as an opportunity rather than a threat (Deetz et al., 2001; Marks & Mirvis, 2000).
Senior management needs to be a champion of change by expressing support for implementation of the new redesign and framing it as an opportunity rather than a threat
Successful and sufficient communication can reduce stress and anxiety as well as increase trust and respect (Bartels, Douwes, de Jong, & Pruyn, 2006; Basinger & Peterson, 2008).
A clear roadmap must be developed – key milestones, clear accountabilities, roles and responsibilities
Appoint an individual to manage the project, hold this person accountable for successful implementation of tasks and timings
Conduct scheduled reviews of the redesign to ensure that the design still works in the context of the current system (formative review)

30
C. Planning Principles
These principles are listed to guide the redesign and implementation of the Mental Health and Addiction services. These are suggestions that should be reviewed and updated/changed as the redesign and implementation phases are undertaken. A clear and shared sense of purpose - Stakeholders should be united by a clear and shared
sense of purpose. The planning process should foster a sense of belonging among the Mental Health and Addiction stakeholders.
Active communications and collaboration – Planning steps should be organized to maximize the flow of information as well as the creation and transfer of knowledge; openness and transparency through regular communication of project status. Systems and structures should be available for the patients/clients, service users and staff to influence decisions.
Transcend barriers between various stakeholders and leverage diversity - Where possible, the redesign planning phase should include and involve a wide range of diverse stakeholders such as: patients, primary care, social services, housing, South East Region Children and Youth Regional Office, municipal government etc.
Realistic activities and timelines – The activities and timelines should reflect both existing constraints as well as the pressing need to achieve the desired outcomes.
Equal opportunity to influence – Consideration must be given to all stakeholders (including clients and patients) so that community agencies and residents feel that they have had the same capability to influence decisions as larger organizations.
Respect: The planning processes should be designed with the utmost respect for and be sensitive to needs of individuals who are most affected by any proposed changes.
Clients, patients and residents: The planning and implementation phases should identify and execute processes through which to engage clients, patients and residents to ensure their perspectives are gathered and that their feedback and input is gathered on options for the redesign.
Note separate principles to guide the redesign and implementation process will need to be developed – see Project Plan.

31
D. Project Plan Introduction
Within this section we describe the Project Plan to guide the redesign of the Mental Health and Addiction services in the South East LHIN. The described Project Plan provides a detailed approach to the redesign phase and a high-level approach to the implementation phase. This is because the tasks supporting the implementation phase will be driven by the new service design. Once the Project Plan has been fully approved by the South East LHIN Senior Management Team, the work of determining the redesign itself will take place over FY 2013/14 (to be completed by December 2013), with implementation set to occur during the subsequent two fiscal years (2014/15 and 2015/16). Each phase is described with the estimated timeframes in the figure below:
1. Develop Implementation Plan for the
redesign of the system2. Implement redesign of the system
IMPLEMENT
January – March 2014
April 2014 –2015/16
1. Visioning
REDESIGN
2. Options
Development
3. LHIN Board
approval of
redesign Model
April – June 2013
July -November
2013 December 2013
Phase 1 Phase 2
Each Phase will be supported by the Project Plan

32
Accountability and Responsibility for the successful execution of the Project Plan The South East LHIN’s Senior Management Team is accountable for the approval and execution of the Project Plan. The LHIN will identify a Project Manager who will be responsible for implementing each step of the Project Plan and who will report to the LHIN’s Senior Management Team. The LHIN will identify 3-4 external advisors, forming an Expert Panel, to advise on leading practices and models. Their role is to advise, inform and assist in the redesign phase. The Project Manager will work with the South East LHIN Management, the Expert Panel and a Redesign Task Force to design and implement the new model for the Mental Health and Addiction Sector. The South East LHIN Board will provide approval on the redesign model. Figure 3 shows the relationship between the various parties involved in the execution of the Project Plan Figure 3: Redesign team structure and relationships
South East LHIN
Board
South East LHIN
Management
Project ManagerExpert Panel
Redesign Task
Force
Line of Reporting
Collaborative working
relationship
Expert Panel provides advice to
Project Manager
and Redesign Task force

33
The LHIN will provide the resources to support the tasks of the Expert Panel and the Project Manager. The following table provides an overview of the accountabilities and responsibilities for the: South East LHIN Board South East LHIN Senior Management Team Expert Panel South East LHIN Project Manager Redesign Task Force.
Accountabilities Responsibilities
South East LHIN Board Accountable for ensuring the redesign, when implemented, will meet the vision as stated in the LHIN’s IHSP - Ensure patients receive the right care at the right time in the right place, enhance capacity of providers and the system, and reduce stigma
Responsible for informal communication of the need for change and progress against Project Plan to other governors
Reviews and provides final approval of the new design of the Mental Health and Addiction services
South East LHIN Senior Management Team
Accountable for the successful execution of the Project Plan
Provides oversight to the Project Manager, Expert Panel and Redesign Task Force
Approves and authorizes key milestones, such as the membership on the Expert Panel and the options for the redesign phase
The Project Manager reports to the LHIN’s Senior Management Team
South East LHIN Project Manager (job description provided in Appendix 5)
Accountable for the successful execution of each task within the Project Plan
Responsible for managing the redesign and implementation project The goal of the Project Manager is to organize and manage resources and tasks in an effective way to meet the project’s defined scope,

34
quality, time and cost requirements, and ultimately to achieve the project’s objectives. Specifically: Responsible for the Project Plan
and each task – brings direction, drive, focus and tempo
Prepares performance reports
against the Plan and presents these to the South East LHIN Senior Management Team and the Redesign Task Force
Works collaboratively with the Expert Panel and the Redesign Task Force
Expert Panel They are a panel to advise, inform and assist in the evaluation of the redesign phase
Responsible for working collaboratively with the Project Manager and the Redesign Task Force.
Responsible for sharing leading practices related to system design and multiple models in the Mental Health and Addiction sector to the Redesign task Force
Responsible for advising and
engaging with the Project Manager and the Redesign Task Force at critical points
Meets the requirements of the Expert Panel Terms of Reference (example provided)

35
Redesign Task Force Accountable for developing options that support the LHIN’s vision, system outcome goals and for placing the user of the system at the heart of all discussions
Works collaboratively with the Project Manager and Expert Panel
Responsible for identifying a number of options for the redesign through liaison with the Expert Panel who will bring forward multiple models and leading practices
Meets the requirements of the Redesign Task Force’s Terms of Reference (example provided)

36
A draft Terms of Reference is provided for the Expert Panel – this document will have to be approved with the Expert Panel, once established.
*Expert Panel: Terms of Reference
Purpose The Expert Panel will share leading practices and multiple models with the Redesign Task Force.
Mandate
Provides advice (including sharing leading practices and multiple models) to develop the redesign of the Mental Health and Addiction services with the Project Manager and Redesign Task Force
Mandate does not include the authority to select the redesign model
Membership
Includes 3-4 members
Members are seen as “leaders of system thinking” in the Mental Health and Addiction sector
Members have a strong understanding of the Provincial Mental Health and Addiction strategy
Members have had experience with redesign at a system level
Project Manager of the redesign project will attend all meetings. Term
The term of membership of the Expert Panel can be up to and until the completion of the implementation phase (end of fiscal 15/16)
Meetings
To be determined by Project Manager Coordination and Administration
The Project Manager will provide administrative support and coordination of the Expert Panel
37
A draft Terms of Reference is provided for the Redesign Task Force – this document will have to be reviewed with the Task Force, once established.
*Redesign Task Force: Terms of Reference
Purpose The Redesign Task Force will receive advise from the Expert Panel and will work with the Project Manager to develop a number of options for the redesign and and prepare for implementation of a new service model for the Mental Health and Addiction services in the South East LHIN region.
Mandate
Involved in gathering input and feedback on options from the wider sector. Answers questions on why changes have been made and how they support the vision and system outcome goals
Supports the need for change, the vision and system outcome goals in internal and external communications
Represents the diversity of Mental Health and Addiction patient/client perspectives on the redesign discussions
Provides insight, guidance for development of options for redesign
Communicates progress and decisions made to respective organizations (including Boards of Governors)
Provides guidance and support to the Project Manager to enable successful implementation of Project Plan tasks
The design options identified by the Task Force will be reviewed by the LHIN Board. The LHIN Board will select the redesign model for the future.
Membership
Represents the diversity of Mental Health and Addiction sector (8-12 members):
Includes fair representation of both Mental Health and Addiction providers (at least 4 representatives from hospitals (schedule 1 hospital and specialty hospital), mental health community provider and addiction community provider). Geographical representation must be considered. (Note: more than one category may be applicable to one individual)

38
Project Manager of the redesign project will attend all meetings
Includes at least three hospital representatives
Includes at least three Executive Directors
Includes at least two patient/client/user/consumer representatives
Includes at least two clinicians (at least one psychiatrist)
Includes at least two front-line staff members involved in the direct provision of service
Expert Panel members will be invited to attend Redesign Task Force meetings.
Members to be identified through a nominations process. Organizations are invited to put
forward two names as possible candidates to be on the Redesign Task Force. The South East LHIN will use the membership criteria (see above) to create the committee.
Term
The term of membership of the committee will be from April 1st 2013 – December 31st 2013
Option to extend term and mandate of committee to the Implementation phase. Evaluation of the taskforce will be conducted by the LHIN at the end of the redesign phase to determine option to extend.
Meetings
Bi-weekly meetings from April – December 2013; all meetings to be face-to-face.
Coordination and Administration
The Project Manager will provide administrative support and coordination of the Committee’s business.
An overview of the approach to the redesign phase now follows; this includes a detailed Project Plan.
39
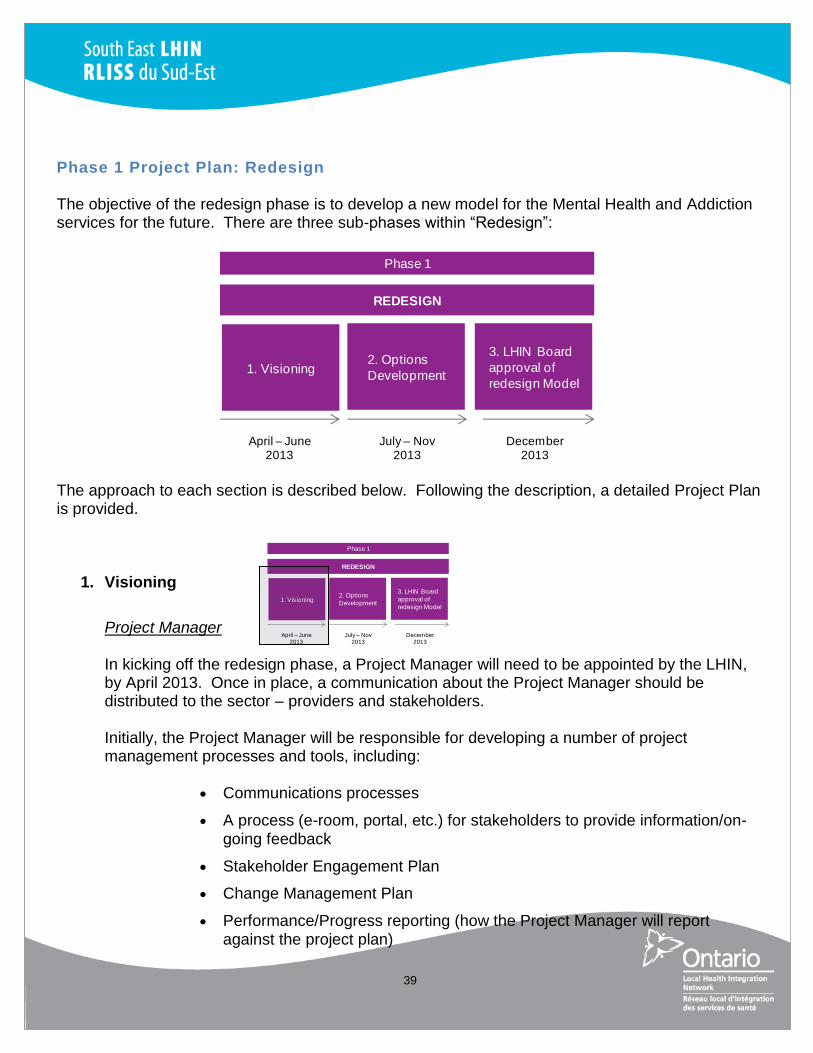
Phase 1 Project Plan: Redesign
The objective of the redesign phase is to develop a new model for the Mental Health and Addiction services for the future. There are three sub-phases within “Redesign”:
The approach to each section is described below. Following the description, a detailed Project Plan is provided.
1. Visioning
Project Manager
In kicking off the redesign phase, a Project Manager will need to be appointed by the LHIN, by April 2013. Once in place, a communication about the Project Manager should be distributed to the sector – providers and stakeholders. Initially, the Project Manager will be responsible for developing a number of project management processes and tools, including:
Communications processes
A process (e-room, portal, etc.) for stakeholders to provide information/on-going feedback
Stakeholder Engagement Plan
Change Management Plan
Performance/Progress reporting (how the Project Manager will report against the project plan)
1. Visioning
REDESIGN
2. Options
Development
3. LHIN Board
approval of
redesign Model
April – June 2013
July – Nov2013
December 2013
Phase 1
1. Visioning
REDESIGN
2. Options
Development
3. LHIN Board
approval of
redesign Model
April – June 2013
July – Nov2013
December 2013
Phase 1

40
Risk Mitigation Plan
Start nominations process for Redesign Task Force (see Terms of Reference)
Examples for many of these tools and processes are included in the Appendix to this Project Plan. For each of these plans, the Project Manager is responsible for execution and progress reporting. The Project Manager will also have to ensure that they have a strong understanding of the stakeholder engagement feedback collected by the consultants – see Appendix 4. Visioning Session The South East LHIN will lead the redesign of the Mental Health and Addiction services in collaboration with the Mental Health and Addiction providers. To do this, it is necessary to have a strong understanding of the current state which will enable the sector to be able to look to the future, determine what the attributes are of the future and to identify how to get there. To do this it is necessary to ensure:
Early agreement to principles of working together and aims of the work – including a realistic understanding of the possible implications;
Shared understanding of the Need for Change, ‘myth-busting’ and gaining realization that the worst case is ‘lose-lose’ for the Mental Health and Addiction sector, and that status quo is not an option
Understanding of the programs, services, patient flows, clinical and financial viability factors across the sector; and,
Consideration of international best practice on service configuration, interactions and the future of health services.
To this end, the first key deliverable for the Project Manager will be to plan, develop and facilitate a full-day Visioning session with all Providers. The objective of the session will be to:
Ensure consistent understanding of the “Need for Change” (see Part I) Ensure high-level understanding of the current state of programs and services To discuss and start to determine – “What do we want to be true about the South
East LHIN Mental Health and Addiction sector in 2020? What will the journey look like for our patients?” (Refer to the consumer engagement feedback in Part 1: Need for Change and stakeholder engagement feedback, Appendix 4, for an overview of stakeholder perspectives that can be referred to when setting the stage for these questions)

41
Attendees would include the Provider’s senior team members, front-line service workers, representatives from the Board, as well as patient/client representatives. Option to also invite external sector participants – police sector, not for profit, social services etc. The Project Manager will work with the Expert Panel to plan and develop the format of the Visioning session. Tasks related to the Visioning session are summarized below:
Schedule a date in June 2013 to hold the networking session
Refine the high-level current state assessment of the programs and services (build on the map and data provided in the “Need for Change”, Part I)
Plan for the full-day session – identify location, timing and develop agenda (an example agenda is provided below)
Coordinate the invitation of a speaker, to present leading practices in the Mental Health and Addiction sector - to prompt innovative thinking and “thinking outside of the box”.
Example Agenda for Visioning Session 09.00 – 09.30: Launch and celebration of redesign initiative (LHIN CEO)
Present members of the Expert Panel and Redesign Task Force Have a client/consumer present “their” journey
09.30 – 10.30: Speaker presentation and questions 10.30 – 11.00: Break 11.00 – 12.00: Overview of current services and programs 12.00 – 12.45: Lunch and networking 12.45 – 13.30: Leading practices related to system redesign 13.30 – 14.30: Facilitated small group discussions on the value of collaboration
Present back to larger group 14.30 – 15.00: Break 15.00 – 16.00: Facilitated small group discussion on what do we want to be true of the Mental Health and Addiction service sector in 2020? Create early options.
Present back to larger group 16.00 – 16.15: Summarize next steps 16.15 – 16.30: Wrap up!
The Project Manager will be responsible for the facilitation of the session.

42
The outcomes of this sub-phase will be: Providers and LHIN have shared understanding of the need for change and the roadmap
for redesign and implementation
Providers and LHIN are excited for the redesign project
Providers have an increased understanding of the services and programs offered by partners
Sector has started to work together to think about options for the future design.
2. Option Development
The Expert Panel will share with the Redesign Task Force leading practice thinking for the redesign. The Redesign Task Force will select a number of options that are best aligned with the vision for the South East LHIN region. The Project Manager will facilitate discussions on these options. At the end of this sub-phase, two to four options for the redesign must be developed, as well as information on each option (i.e. what will this mean for our clients/patients, what are the key attributes and what are the steps necessary to achieve this option). Once options are developed, they should be discussed with the sector’s stakeholders to gather feedback and input. The Project Manager should identify a process through which to gather input from Providers (including Board members), clinicians, patients, clients and external sector stakeholders. A few examples are provided through which to gather feedback from providers (including Board members) Planning and facilitating a number of stakeholder engagement sessions where options are
presented and feedback is gathered through small group sessions Options with details could be presented on an e-portal with questions for
providers/stakeholders to consider; there could be an OTN supported meeting to allow for stakeholders to provide real time feedback
Members of the Redesign Task Force would be responsible for presenting the options in each of their sub-sectors/sub-regions/with patients/clients etc and bringing the information back to the South East LHIN Senior Management, Expert Panel and Redesign Task Force.
KPMG conducted a focus group session with consumer representatives from across the South East Region. They provided feedback that they would appreciate a number of different options to provide input and feedback. These included face to face sessions, opportunities for anonymous surveys, skype/OTN meetings and through social media
1. Visioning
REDESIGN
2. Options
Development
3. LHIN Board
approval of
redesign Model
April – June 2013
July – Nov2013
December 2013
Phase 1

43
portals (such as facebook). They also suggested that they would be happy, as the representatives for a number of consumers, to gather feedback from a wide range of consumers and to share this with the LHIN, Expert Panel and Redesign Task Force.
Six meetings have been identified as required to support the development of two to four options for the redesign. It is estimated each meeting will require at two to three hours. The objective of each meeting is shown in the table:
Meeting Objective
1 To establish and commence the option development phase: A draft Terms of Reference has been developed for the Expert Panel
and the Redesign Task Force. The first task for both groups will be the agreement and update of the Terms of Reference.
To confirm scheduled meetings and objectives: Per the Terms of Reference, the groups will meet six times between
August – November 2013 for the purpose of options development. Project Manager to present the Project Plan (e.g. tasks and timings) and to
communicate decision making points. To conduct a “coming together in a new way for a new purpose” exercise (as
this is the first time the group is meeting – for example, each person to share their individual and organizational hopes for this project and/or their journey in the Mental Health and Addiction sector).
2 To discuss outcomes from the visioning session and to agree and finalize the planning steps for the redesign project.
Expert Panel members to present leading practice thinking on system design and their thoughts on the application of these ideas to the South East LHIN. The Project Manager to facilitate these discussions.
3 The group to discuss options for the design of the Mental Health and Addiction services (consider the future vision and system outcome goals).
To identify all current initiatives and determine against the system outcome goals how these should be prioritised going forward. To determine how to collaborate with the development of Health Links.
4 To determine two to four options for the redesign. To gather feedback and input on each of these options with the sector
(including Board governors).
5 To “flush” out each of the options - what will this mean for our clients/patients; what are the key attributes and what are the steps necessary to achieve these options;what are the possible financial, legal impacts?
6 To develop a case for each of the options. To gather feedback and input on these options with the sector (including Board
governors).

44
The outcomes of this sub-phase will be: Two to four options for the redesign of the Mental Health and Addiction system in the
South East LHIN (note: status quo is not an option)
On-going communication with the sector
Stakeholder, client, resident and consumer feedback and input on the models.
3. LHIN Board Approval of Redesign Model
By this stage, a number of options will have been developed for the design of the Mental Health and Addiction system. These will be presented to the LHIN Board for selection of an approved Mental Health and Addiction system design for implementation
The outcomes of this sub-phase will be: Approved Mental Health and Addiction system design for implementation
The tasks for each sub-phase of the redesign phase are shown in the following table, which also identifies responsibility for each task as well as the date of expected completion. This table can be used to track progress against the execution of the Project Plan. Detailed Project Plan for each sub-phase of Redesign Visioning Tasks Responsibility Decision
Required? Completed By
Status
1. Assign
Project
Manager
1.1 South East LHIN to identify
Project Manager (PM)
1.2 South East LHIN to identify
and recruit for Expert Panel
(EP)
1.3 Communication about Project
Manager including
accountabilities and
South East LHIN South East LHIN Project Manager
Y: LHIN approves PM
Y:LHIN appoints AG
April 2013
1. Visioning
REDESIGN
2. Options
Development
3. LHIN Board
approval of
redesign Model
April – June 2013
July – Nov2013
December 2013
Phase 1

45
responsibilities to be
communicated to the
providers
1.4 Project Manager establishes
weekly communication
process (newsletter, e-mail,
document on a portal,
teleconference) with the
providers.
1.5 Project Manager sets up e-
room/web link and allows
option for on-going feedback
and insight from providers,
governors, staff, clinicians,
patients and residents related
to the redesign
1.6 Project Manager develops
Stakeholder Engagement
Plan, Change Management
Plan and Risk Mitigation Plan
(see example in Appendix)
1.7 Project Manager implements
nomination process for
Redesign Task Force (RTF).
Providers nominate members
for consideration for the RTF.
LHIN selects RTF members
Y :LHIN selects RTF members from nominations
2. Plan and
develop
full-day
Visioning
Session
2.1 Work with Expert Panel to
develop format for Visioning
session (gather feedback on
agenda and speakers)
2.2 Refine the high-level current
state assessment of the
Mental Health and Addiction
sector
2.3 Plan for the full day working
session – identify location,
timing and develop agenda*
(see example)
Project Manager
Y-LHIN approves agenda
Tasks to be completed during April and May Session to be in June

46
2.4 Secure a keynote speaker
and consumer/client/patient
speaker
2.5 Develop current state
presentation
2.6 Develop leading practices
presentation
2.7 Develop final presentation for
Visioning session.
2.8 Facilitate successful
Visioning session
Option Development
1. Meeting 1:
Establish
redesign
Task Force
1.1. Schedule half-day meetings
(twice a month from August
to November) with the RTF
and Expert Panel
1.2. Project Manager to prepare
standard agenda for all
meetings
1.3. Project Manager to present
Project Plan
1.4. Project Manager to facilitate
relationship building exercise
Project Manager/LHIN
July
2. Meeting 2:
Planning
Meeting
2.1. Present outcomes from
Visioning session
2.2. Finalize planning steps for
the redesign phase
2.3. Expert Panel members share
leading practice thinking on
system design and
application of these ideas to
the South East LHIN
2.4. Develop principles related to
the redesign process
2.5. Communicate overview of
meeting to all stakeholders
Project Manager, Expert Panel and RTF
August

47
3. Meeting 3:
Blue Sky
Meeting
3.1. The group to discuss options
for the design of the Mental
Health and Addiction
services (consider the future
vision and system outcome
goals)
3.2. Project Manager to facilitate
discussion on option designs
– “If we stepped into the
future, in 2020, what would
we want the system to look
like?”; “What are the
attributes of the future
system”?; “Imagine there
were no restrictions to the
future, what could we
achieve as a system?”
3.3. To identify all current
initiatives and determine
against the system outcome
goals how these should be
prioritized going forward
3.4. To determine how to
collaborate with the
development of Health Links.
3.5. Communicate overview of
meeting to all stakeholders
Project Manager and RTF
September
4. Meeting 4:
Options
Meeting
4.1. Facilitate discussions on a
number of system designs
4.2. Facilitate a prioritization
exercise - determine
alignment of options
4.3. Determine two to four options
for the system design
4.4. Project Manager to present
two to four options to the
LHIN
4.5. Project Manager to present
feedback and input
Project Manager, Expert Panel and RTF
Y:LHIN approves 2-4 options
First two weeks of October

48
processes to the LHIN
4.6. Feedback and input
processes rolled out to the
sector (including Board
governors)
4.7. Communicate overview of
meeting to all stakeholders
Y: LHIN approves feedback and input processes
5. Meeting 5:
Develop
options for
redesign
5.1. Develop each of the options -
what will this mean for our
clients/patients, what are the
key attributes and what are
the steps necessary to
achieve these options - What
are the possible financial,
legal impacts?
5.2. Communicate overview of
meeting to all stakeholders
Project Manager, Expert Panel and RTF
Latter two weeks of October
6. Meeting 6:
Refine
redesign
options
6.1. Develop a case for each of
the options – determine the
high-level steps necessary to
achieve the objectives of
each option
6.2. Project Manager to present
each case to the LHIN Senior
Management Team
6.3. Gather feedback and input
on the the detailed options
with the sector (including
Board governors)
6.4. Communicate overview of
meeting to all stakeholders
Project Manager and RTF
Y:LHIN approves each case for validation
First two weeks of November
7. Build the
redesign
options
7.1. Develop a business case for
each of the options – this
should include overview,
expected benefits to
residents, challenges and
risks and potential
financial/legal impacts
Project Manager
Y: LHIN approves business case for each of the options
Latter two weeks of November

49
LHIN Board Approval of Redesign Model
1. LHIN Board
approval
1.1. LHIN Board to review each
option in detail and select
one option for
implementation
1.2. Present new design for
Mental Health and Addiction
services with governors,
providers, clinicians, patients,
clients, external stakeholders
(housing, children and
youth). Consider a second
“visioning” session to focus
on how to implement the
chosen redesign for the
sector
1.3. Update the model for
relevant feedback
1.4. Develop a visual of the
design and distribute to all
stakeholders
LHIN Board/Senior Team and Project Manager
December
By January 2014, a design for the Mental Health and Addiction services sector should be agreed and approved. All stakeholders should have an intimate knowledge of this new model. The next phase is the implementation of the new model.

50
Phase 2 Project Plan: Implementation
The objective of the implementation phase is to implement the new model for the Mental Health and Addiction services. There are two sub-phases within “Implementation”:
The approach to each section is described below. Following the description is a high-level project plan for the implementation phase. A detailed project plan is not provided as the tasks will depend on the extent of change from the current service model. Following the approved redesign model, the Project Manager will develop an implementation plan. This plan will guide the implementation process – outlining what tasks are needed to implement the new design and who will be responsible for each task. The plan should include the following sections: Contents of Implementation Plan
Part A: Overview
Description of the current state
Include any principles/joint values that are guiding the planning process (refer to “Project Plan”)
Part B: Overview of Planning Committee
Provide high-level overview of the committee/Task Force developed to manage the implementation process.
Part C: Overview of new service model
Describe the new service model
o Need for Change - provide a full explanation of key objectives, issues being addressed and how the redesign will meet the province’s and SE LHIN’s vision
1. Develop Implementation Plan for the
redesign of the system2. Implement redesign of the system
IMPLEMENT
January – March 2014 April 2014 –2015/16
Phase 2

51
o Provide a geographical map of the new model
o Describe key changes from the current state (shared resources, integrations, amalgamations, new clinical pathways, co-locations, etc.)
o Provide a description of the service arrangements
o Provide an overview of the types of programs and services to be provided
o Describe the patient/client journey for three to five complex/high-user patients/clients
o Provide overview of the following:
Service agreements
Shared services
Centralized teams vs. decentralized teams
Community planning tables/committees.
Part D: Governance and Management Support Governance
Demonstrate how the Mental Health and Addiction governors will:
o Collaborate during the implementation process
o Provide governance oversight, as required. Management
Demonstrate how the provider management will:
o Provide leadership for service changes and reconfigurations. Part E: Programs and Services
Provide an overview of the types of programs and services to be offered (information to be provided at a high-level, not to include sub-programs/services)
Demonstrate how the new design will:
Ensure patients receive the right care, at the right time, in the right place, enhance capacity of providers and the system and reduce stigma.
Part F: Resource Management
Provide an overview if there are to be changes to the following functions across the sector: o Human Resource function
o Locations
o Information Technology
o Premises and Facilities.
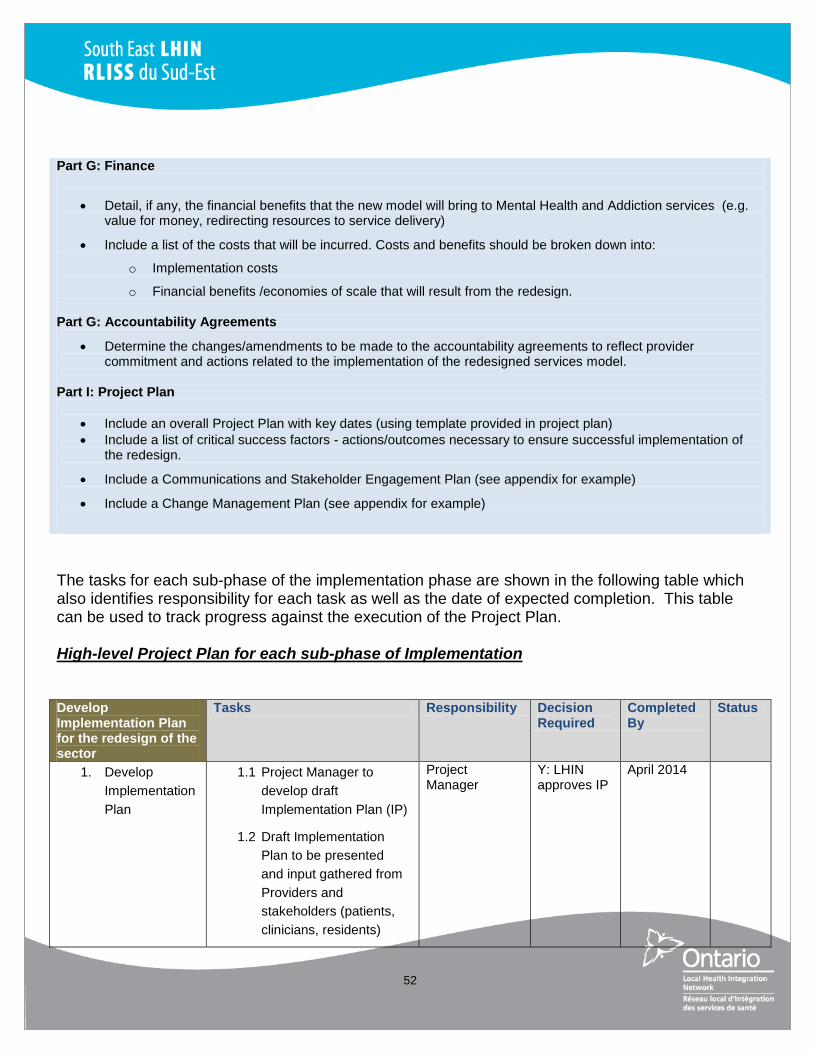
52
Part G: Finance
Detail, if any, the financial benefits that the new model will bring to Mental Health and Addiction services (e.g. value for money, redirecting resources to service delivery)
Include a list of the costs that will be incurred. Costs and benefits should be broken down into:
o Implementation costs
o Financial benefits /economies of scale that will result from the redesign.
Part G: Accountability Agreements
Determine the changes/amendments to be made to the accountability agreements to reflect provider commitment and actions related to the implementation of the redesigned services model.
Part I: Project Plan
Include an overall Project Plan with key dates (using template provided in project plan)
Include a list of critical success factors - actions/outcomes necessary to ensure successful implementation of the redesign.
Include a Communications and Stakeholder Engagement Plan (see appendix for example)
Include a Change Management Plan (see appendix for example)
The tasks for each sub-phase of the implementation phase are shown in the following table which also identifies responsibility for each task as well as the date of expected completion. This table can be used to track progress against the execution of the Project Plan. High-level Project Plan for each sub-phase of Implementation Develop Implementation Plan for the redesign of the sector
Tasks Responsibility Decision Required
Completed By
Status
1. Develop
Implementation
Plan
1.1 Project Manager to
develop draft
Implementation Plan (IP)
1.2 Draft Implementation
Plan to be presented
and input gathered from
Providers and
stakeholders (patients,
clinicians, residents)
Project Manager
Y: LHIN approves IP
April 2014

53
2. Continue
Project
Management
tasks from
redesign phase
2.1 To update
communications on
Implementation Plan
2.2 Update change
management plan,
stakeholder management
plan and other key
documents
Project Manager
On-Going
Implement Redesign of Sector
2. Execute
Implementation
Plan
2.1. Implement tasks as
identified in the
Implementation Plan
2.2. Measure progress
against Implementation
Plan
2.3. New design to be
operational by FY
2015/16.
Project Manager
Completed by April 2016
As noted, this table will be expanded once the new design has been approved. Once the Implementation Plan has been executed, the new design for the Mental Health and Addiction providers will be operational.

54
Appendices
Appendix 1: Change Management Considerations Appendix 2: Stakeholder Engagement Considerations Appendix 3: Potential Risks and Mitigations Appendix 4: Summary of Stakeholder Engagement Appendix 5: Project Manager Role Description Appendix 6: Examples of Planning Commitees
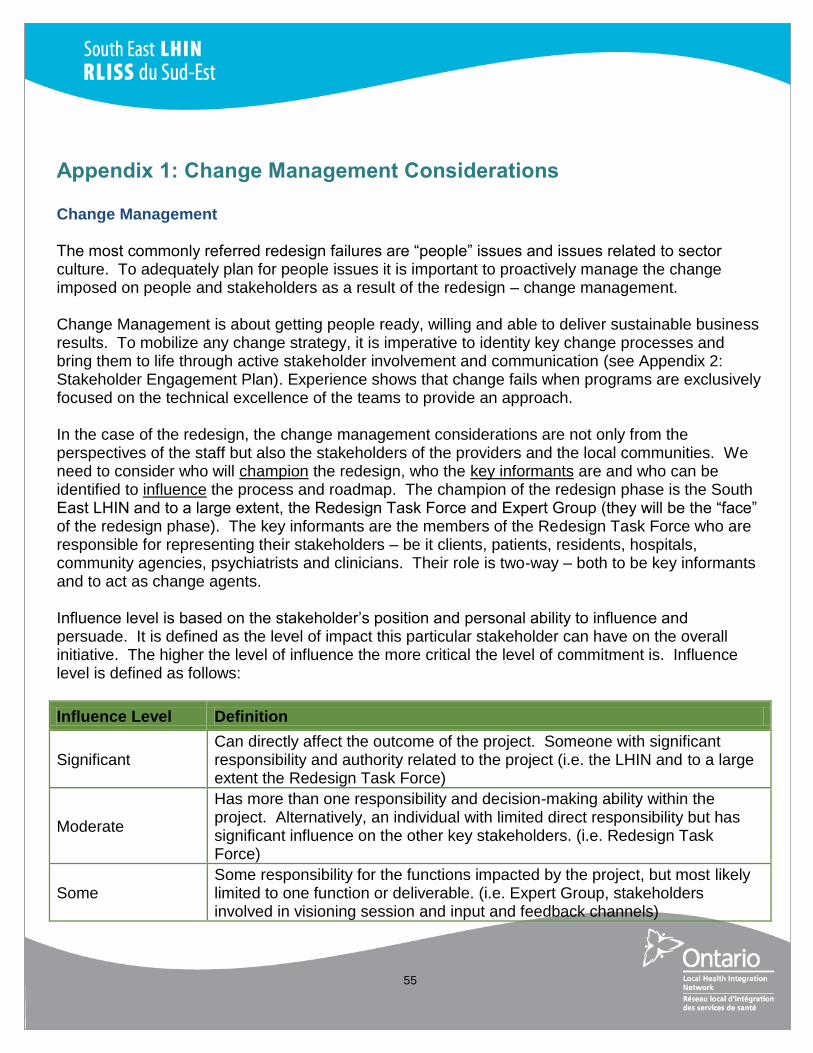
55
Appendix 1: Change Management Considerations Change Management The most commonly referred redesign failures are “people” issues and issues related to sector culture. To adequately plan for people issues it is important to proactively manage the change imposed on people and stakeholders as a result of the redesign – change management. Change Management is about getting people ready, willing and able to deliver sustainable business results. To mobilize any change strategy, it is imperative to identity key change processes and bring them to life through active stakeholder involvement and communication (see Appendix 2: Stakeholder Engagement Plan). Experience shows that change fails when programs are exclusively focused on the technical excellence of the teams to provide an approach. In the case of the redesign, the change management considerations are not only from the perspectives of the staff but also the stakeholders of the providers and the local communities. We need to consider who will champion the redesign, who the key informants are and who can be identified to influence the process and roadmap. The champion of the redesign phase is the South East LHIN and to a large extent, the Redesign Task Force and Expert Group (they will be the “face” of the redesign phase). The key informants are the members of the Redesign Task Force who are responsible for representing their stakeholders – be it clients, patients, residents, hospitals, community agencies, psychiatrists and clinicians. Their role is two-way – both to be key informants and to act as change agents. Influence level is based on the stakeholder’s position and personal ability to influence and persuade. It is defined as the level of impact this particular stakeholder can have on the overall initiative. The higher the level of influence the more critical the level of commitment is. Influence level is defined as follows:
Influence Level Definition
Significant Can directly affect the outcome of the project. Someone with significant responsibility and authority related to the project (i.e. the LHIN and to a large extent the Redesign Task Force)
Moderate
Has more than one responsibility and decision-making ability within the project. Alternatively, an individual with limited direct responsibility but has significant influence on the other key stakeholders. (i.e. Redesign Task Force)
Some Some responsibility for the functions impacted by the project, but most likely limited to one function or deliverable. (i.e. Expert Group, stakeholders involved in visioning session and input and feedback channels)

56
Limited Aware of the project, but peripherally involved, therefore only marginal ability to impact the project. (Possible external sector organizations such as housing and social services)
None No influence on the project.
Once the redesign phase has begun, the Project Manager can determine the levels of influence and how to target changing behaviors or communications to ensure that those with the highest levels of influence are communicating a consistent message and demonstrating behaviors that will ensure the redesign phase will be successful. Underpinning Principles for Achieving Change There are a number of principles which are crucial to achieve successful change. These are noted in the table below and next to each, the action that the LHIN and the sector will take to achieve these principles are also included.
Underpinning Principles for Achieving Change
Action to Achieve Principles
Rigorous compelling case for change
Refer to Part I: Need for Change. To be shared and referred to throughout the redesign phase.
Transformational leadership
Transformational leadership will drive the redesign phase and will come from the LHIN, the Expert Group, the Redesign Task Force and the majority of stakeholders who through the engagement process stated support for the vision and transformation of the Mental Health and Addiction sector for the benefit of the consumer/client/resident/patient.
Top Down - Bottom up
The LHIN Board will approve the final redesign but the options for the design will largely be developed by the Redesign Task Force who will comprise of management, front-line staff, clinicians and clients/patients/consumers.
Alignment of activities to drive and sustain required behaviors
Refer to the change management and stakeholder engagement plan.
Involvement of people to generate ownership to support the change
See Terms of Reference of Expert Group and Redesign Task Force as well as the detailed project plan which described a number of opportunities to provide input and feedback into the redesign phase.
Use existing management processes where possible to implement and sustain
Not as relevant to the redesign phase but the Project Manager will be an employee of the LHIN and therefore
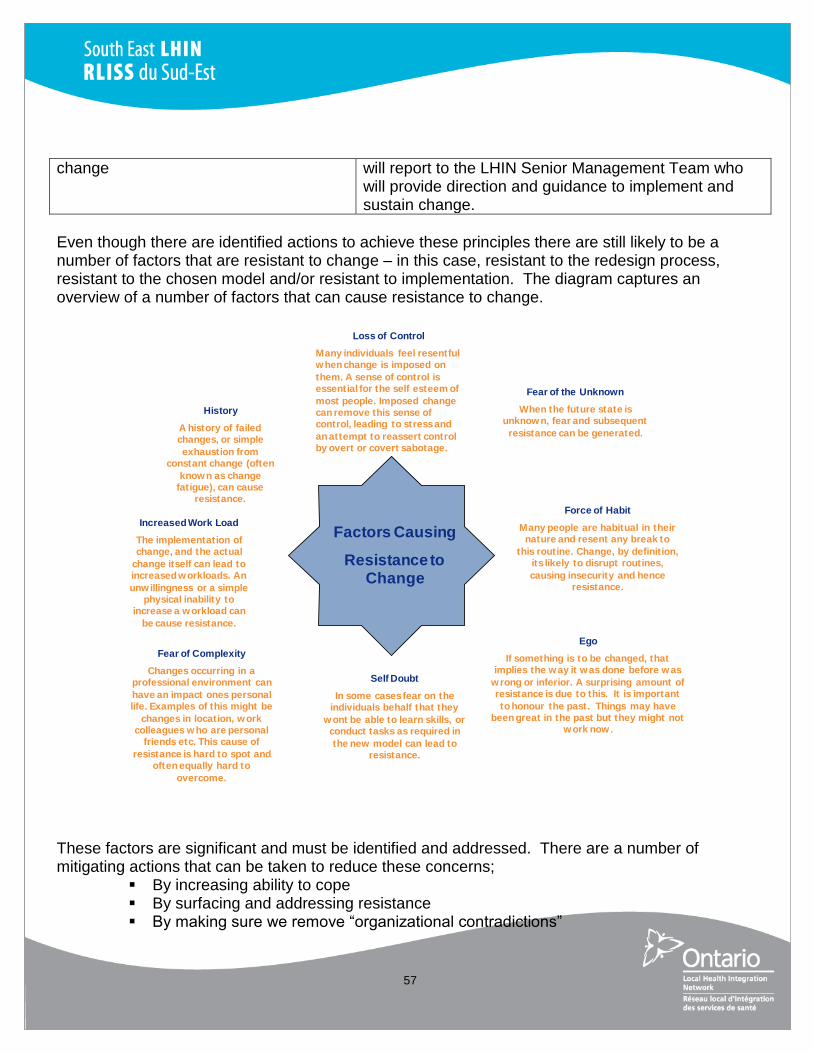
57
change
will report to the LHIN Senior Management Team who will provide direction and guidance to implement and sustain change.
Even though there are identified actions to achieve these principles there are still likely to be a number of factors that are resistant to change – in this case, resistant to the redesign process, resistant to the chosen model and/or resistant to implementation. The diagram captures an overview of a number of factors that can cause resistance to change. These factors are significant and must be identified and addressed. There are a number of mitigating actions that can be taken to reduce these concerns;
By increasing ability to cope By surfacing and addressing resistance By making sure we remove “organizational contradictions”
Loss of Control
Many individuals feel resentful when change is imposed on
them. A sense of control is essential for the self esteem of
most people. Imposed change can remove this sense of control, leading to stress and
an attempt to reassert control by overt or covert sabotage.
Fear of the Unknown
When the future state is unknown, fear and subsequent
resistance can be generated.
Force of Habit
Many people are habitual in their nature and resent any break to
this routine. Change, by definition, its likely to disrupt routines,
causing insecurity and hence resistance.
Ego
If something is to be changed, that implies the way it was done before was
wrong or inferior. A surprising amount of resistance is due to this. It is important
to honour the past. Things may have been great in the past but they might not
work now.
Self Doubt
In some cases fear on the individuals behalf that they
wont be able to learn skills, or conduct tasks as required in
the new model can lead to resistance.
Fear of Complexity
Changes occurring in a professional environment can
have an impact ones personal life. Examples of this might be
changes in location, w ork colleagues w ho are personal
friends etc. This cause of
resistance is hard to spot and often equally hard to
overcome.
Increased Work Load
The implementation of change, and the actual
change itself can lead to increased workloads. An
unwillingness or a simple physical inability to
increase a workload can
be cause resistance.
History
A history of failed changes, or simple
exhaustion from constant change (often
known as change fatigue), can cause
resistance.
Factors Causing
Resistance to Change

58
The graph shown provides additional action items that can help mitigate resistance to change. These action items are shown over a period of time and factor in that changing behaviours and feelings takes time but that there are a number of active steps that can be taken to mitigate the resistance.
The messages/strategies in the graph can be used by the Project Manager throughout the redesign and implementation phase to mitigate resistance to change. Creating a change management plan A change management plan can be a simple communication tool that is used by the Redesign Task Force to ensure that the people (including the communities) involved in and impacted by the amalgamation are ready for the change. Moreover, a change management plan ensures that the needs of staff and stakeholders are considered throughout the life of the redesign and implementation – so that staff are involved more than once and through multiple methods. The stakeholder engagement plan provides details on stakeholder communications – Appendix 2.
Neutral Zone/Transition ZoneLead Up
Time
Uncertainty
Anticipate Loss
Accept
reactions
Compensate
for losses
Give information
Define what is
‘over’
Acknowledge
the end
Respect the
past
Keep
communicating
the vision
Provide structure for support
Strengthen
relationship
Promote
creativity

59
A change management plan can include aspects of the following; Communications: Who needs to be communicated with? What do they need to be
communicated? In what format do they need to be communicated in? What is the timing and frequency and who will be responsible for the communication (i.e. newsletters, e-rooms, staff meetings)? (see Appendix 2 for Stakeholder Engagement Plan)
Change Leadership: Who is leading the redesign and implementation phases, what is their approach?
Cultural Alignment: Are the providers aligned culturally? Do clients/staff/stakeholders perceive there to be mutual values and principles?
Involvement Strategies: What are the strategies we will employ to involve all staff/stakeholders in the change? Should there be joint meetings, joint leadership meetings and/or joint social meetings? How will these be structured? When is the appropriate time to host these meetings / events? (see Appendix 2: Stakeholder Engagement Plan)
A draft change management plan is included. This will require updating by the Project Manager.
Action Status Key Objective Vehicle Audience Date (start)
Develop stakeholder engagement plan
Partially complete – see Appendix 2
The Stakeholder Engagement Plan guides the communications with the providers, communities and stakeholders.
Plan LHIN residents, clients, patients, providers, clinicians
April 1, 2013 – on-going process
Senior Team to define Transformational Leadership
To begin Discussion amongst LHIN Senior Management Team on how to approach redesign of the system as the group with significant influence.
Facilitated discussion by Project Manager
LHIN Senior Management Team
April 2013
Leadership Communication
To begin Ensure LHIN Senior Management Team and LHIN Board has what they need to be champions of the redesign (i.e. consistent messages, summary of the Need for Change – 4-5 bullet points)
Facilitated discussion
LHIN Governors and LHIN Senior Management Team
April 1, 2013 – on-going process (consider meeting every 6 months on this topic)
Redesign Task Force to discuss role as significant influencers
To begin Discussion amongst RTF on how to approach the development of a number of options for the redesign of the system as the group with significant – moderate influence.
Facilitated discussion by Project Manager
RTF As part of Meeting 1
Change Management Optional Assess readiness of the Assessment TBD TBD

60
Readiness Assessment* sector for change (included as optional as there is a risk of losing momentum for the redesign phase through focus on additional current state perspectives)
*Change Management Readiness Assessment An assessment used to determine the readiness and capacity of an organization(s), or parts of it, to introduce change and monitor the change effort throughout the project lifecycle. It can be carried out using questionnaire, one to one interviews, focus groups and workshops or a combination of these. An assessment tool can be provided by KPMG.

61
Appendix 2: Stakeholder Management Considerations Creating a stakeholder engagement strategy/plan
The Stakeholder Engagement Strategy/Plan guides the communications with the providers, communities and stakeholders. A Strategy/Plan provides a clear statement of the approach to be used for the development and execution of all communication activity and defines the parameters for delivering key messages to stakeholders (including the community). In developing the stakeholder engagement plan, the first step should be to list all stakeholders and then to prioritize these in order of influence. Once the stakeholders are identified, they engagement plan should be developed. Example Principles to Guide the Development of the Strategy/Plan
The Engagement Strategy must take into account the level of understanding key stakeholders and
sponsors needed for the project throughout its life cycle
The strategy must set realistic targets and define responsibilities
The strategy should address the Who, How, What, and Why
All communications are delivered in line with agreed standards and protocols
Whenever possible communications are delivered face-to-face
All communications are based on agreed key messages to ensure consistency of tone and messaging
The Engagement Plan is fully incorporated into the overall project plan and communication activities are
aligned to project milestones, key events etc.
All communications have a built-in feedback loop to help ensure an assessment can be made as to how it
was received by the stakeholder groups.
Example Stakeholder Engagement Plan Examples of engagement activity have been population – it is the Project Manager’s responsibility to update and report progress against the plan.
Engagement Activity/Tactics
Timing Target Audience Message
Objectives Sender Response Status Action
Project Team
Meetings
Weekly
(ongoing)
Project Team
and
Governance
Provide detailed
updates on
progress and
issues for the
project
Discussion and
agreement on next
steps
Project
Manager

62
Launch session:
Communicate
overview of Project
Plan to sector
April 2013 Providers,
clinicians and
residents
Encourage
understanding of
the redesign
project and role of
different groups in
executing plan
Provide:
Overview of the
Project and fit with
the LHIN’s vision
and strategic
priorities
Benefits for the
stakeholders and
the system
Overview of the
work ahead and
how people will be
involved
LHIN
Communicate Project
Manager
April 2013 Providers,
clinicians and
residents
Introduce Project
Manager
LHIN
Communicate Expert
Panel Membership
April 2013 Providers,
clinicians and
residents
Introduce Expert
Panel
LHIN
Communicate
Redesign Task Force
membership
April 2013 Providers,
clinicians and
residents
Introduce
Redesign Task
Force and share
nomination
process
LHIN
Communicate
stakeholder
communication
schedule/processes
July 2013 Providers,
clinicians and
residents
Provide high-level
communications
schedule to
stakeholders
inform them of key
engagement points
LHIN
Launch dedicated
project mailbox for
Questions and
Answers
July 2013 Providers,
clinicians and
residents
Note:
communication
resource needs to
be assigned to
monitor and
manage the box
LHIN
Communicate
progress on options
development
October
2013
Providers,
clinicians and
residents
Provide high-level
update on options
development to
ensure momentum
through the
redesign process
LHIN
Communicate
approved design
model
December
2013
Providers,
clinicians and
residents
Communicate the
approved design
model as well as
timelines for
Redesign phase
LHIN

63
To supplment the draft stakeholder engagement plan, as presented above, the Project Manager will want to build in further communication tactics to make the plan more robust. Listed below are potential tactics that the Project Manager may want to consider. Potential Tactics for Communication
Channel At its best Potential downsides Think about
Team meetings Can make communication personal
and relevant to the team involved
Opportunity for discussion, feedback,
questioning and ideas
Project Manager can facilitate a lively
and interactive session
Can help build understanding and
involvement
Success depends on skill of Project
Manager
Time commitment for both manager and
audience
Beware of content overload; other
channels are more effective for
information delivery.
Making the best possible use of this
time – it’s valuable
Training Project Manager
Providing notes and discussion tools
to focus on the main points
Having senior leaders follow-up with
Project Manager to reinforce
importance and ensure discussions
happen.
E-mail Can reach mass audiences fast
Cost-effective and simple to use
Consistent and controlled message
Reaches the recipient directly
Good for information/awareness/
instruction.
Not everyone may have access
Impersonal and open to
misinterpretation
Can result quickly in information
overload
Can’t tell if messages have been read
Doesn’t prioritize messages
Can’t generate dialogue/discussion.
Controlling access to mass
distribution lists
Using the subject box to get across
your key message
Keeping it short and simple
Using headings and bullet points for
key messages to break up the text.
Intranet Fast and consistent
Possibilities are endless; can be
entertaining and visually snappy
Good for information store, reference
and awareness raising
Discussion boards good for
involvement and sharing
Webstats show who is reading.
Not everyone may have access
Relies on people seeking out
information
People may not have time to read it
Difficult to police
Can become unwieldy, hard to navigate
and full of outdated information.
Including ‘killer content’ to draw
people in (processes people need to
do their jobs)
Video Creative and entertaining
Can show real people talking about
their experiences
The camera never lies – can show
proof of progress
Makes people and places accessible
for a mass audience
Consistent, controlled message.
Potentially expensive
Not interactive on its own
Can be seen as glossy corporate
propaganda
Talking heads alone are rarely
engaging!
Can be difficult for mobile workforce.
Using as part of a briefing session to
stimulate debate
Using ‘real people’ to talk about their
experiences, not just senior
executives.
Print magazine/
Newsletter
Reach all stakeholders with a
consistent message
Even time-pressured individuals can
read on coffee breaks/on trains
Can address/reflect stakeholders
feedback and respond
Can show how everything fits
together and reinforce key messages.
Can be seen as biased and not credible
Information dates quickly
Challenging to make it relevant to all
audiences
No opportunity for discussion/ checking
understanding.
What will hook people to open it?
(e.g. a competition)
Using a stakeholder editorial board
to test content and ensure articles
address the real issues.
Events/road
shows
Opportunity for key people to reach
mass audiences face to face
Can be one way ‘tell’ sessions
Agenda set by centre may not be what
Involving stakeholders in setting the
agenda and format

64
Flexible and responsive
Can include Q&A sessions, break out
groups and involve people
Can build team spirit and motivate
Can be used to address controversial
issues by the best communicators.
the audience wants
May be expensive
Time consuming for organizers,
presenters and audience.
Involving stakeholders in the event
itself, as hosts or facilitators
Using interactive voting technology
to maximize audience involvement.
Open forums /
Town Hall
discussions
Gives opportunity to raise and
discuss the real issues
Genuine open dialogue
Helps leaders to understand how
things really are
Enables stakeholders to feel heard.
Dismissive or aggressive response to
questions can close down dialogue
Stakeholders can feel disempowered if
their decisions are over-ruled or
contradicted.
Issuing a summary of discussion for
everyone to see
Proactively raising difficult issues or
asking for questions in advance to
prompt the real debate.
Site visits by LHIN
Leaders
Shows leaders are listening and want
to see what the real issues are
Keeps leaders in touch with the real
issues
Promotes dialogue and
understanding.
Leaders won’t experience the real
issues if treated as ‘royal visits’
May do more harm than good if leaders
show that they are out of touch
Time-consuming for senior leaders to
visit multiple sites.
Giving leaders a good brief on site
issues before they visit
Tracking issues raised and reporting
back on actions.
Web-casting &
similar
Opportunity for senior leaders to
reach mass audiences with
consistent message in real time
Can involve Q&A sessions.
May be expensive
Need the right technology in place
Noise levels may be inappropriate in
some offices
May be difficult for all stakeholders to be
available at the same time.
Finding out about new technology
continually emerging in this area.
Pod Casting Good for younger, more sophisticated
remote stakeholders
Effective for information and
instruction
Relies on people choosing to download
and play content
Can be a significant investment to
ensure each member of your audience
has an iPod.
Including a hook that will make
people listen (e.g. a competition, as
above)

65
Appendix 3: Risk Assessment and Mitigation There are a number of risks when redesigning a health system. As such, it is important to clearly identify the critical success factors of a winning system transformation, prior to embarking on the redesign. Below are the critical success factors which should be incorporated within the redesign.
Effective risk management will be an important part of the project plan. Potential risks have been identified and included in the risk assessment and mitigation table below. In addition to the critical success factors listed above, it is expected that for each risk, the Project Manager will develop appropriate mitigation strategies and the risks in this table will be reported against.
Risk Area Potential Risk Likelihood
Assessment Impact
Assessment Mitigation Strategy Responsibility Status
Project Plan Losing support and
commitment of
stakeholders due to slow
project plan
implementation and timing
L H Ensure momentum for
the implementation
project is high through
focused execution of the
project plan.
Project Manager
Program & people
management
Realize value
Critical Success
Factors
Senior
sponsorship
Focus on change
management
Focus on vision & roadmap
Achieving buy-in &
ownership Change agents
leveraged
Participation is essential
Leadership demonstrates commitment to change and depicts why it is necessary
Leadership takes the form of a strong coalition
Magnitude and readiness for change is assessed and customized change management plan is developed
Communication strategy allows for a clear, targeted and timely exchange of information
Major milestones are balanced in a way that creates quick wins
Transformation is built around a clear and concise vision and roadmap
Strict adherence to disciplined project management
HR resources engaged

66
of moving the redesign
forward.
Project Plan Inability to gain support
and commitment of
stakeholders due to a lack
of trust
L H Utilize “Expert Panel”
and project management
leadership which
includes someone with
knowledge and
experience with MH&A
redesign, in order to gain
trust of MH&A
stakeholders (prevent
bias and ensure
credibility)
Project Sponsor/
Project Manager
Project Plan Conflicting priorities for
scarce resources and
interdependencies
between projects.
H H Continuous alignment of
progress with the
direction defined by the
SE LHIN vision for the
MH&A sector.
Project Sponsor
Redesign Lack of balanced input
from ‘Mental Health’ and
‘Addictions’
M M Strong adherence to a
balanced and
participatory focused
engagement process;
Expert Panel to have
both Addiction and
Mental Health
representation.
Project Manager
Redesign Lack of focus on youth
MH&A
M M Strong adherence to a
balanced and
participatory focused
engagement process;
Expert Panel to have
representation from
youth MH&A sector.
Project Manager
H = High likelihood/impact M = Medium likelihood/impact L = Low likelihood/impact
67
Appendix 4: Summary of Stakeholder Engagement A variety of stakeholders were engaged to inform the Project Plan to Support the Redesign of the Mental Health and Addiction Services for the Future in the South East Region. A total of nine (9) group interview sessions were conducted with stakeholders representing the following HSPs/regions: Addictions Centre Hastings and Prince Edward The Brock Cottage Frontenac Community Mental Health and Addiction Services Hotel Dieu Hospital – Mental Health Leeds and Grenville Mental Health Lennox and Addington Addiction and Community Mental Health Services Mental Health Services Hastings and Prince Edward Mental Health Support Network South East Ontario Providence Care Quinte Health Care Youth Habilitation, Quinte Brockville General Hospital Kingston General Hospital South East LHIN Primary Care Lead Psychiatry Group Consumer Representatives Focus Group Primary Care Lead: South East LHIN Dr Le Clair: Partnership and Development Coordinator and Academic Chair of Geriatric
Psychiatry Providence Care - Mental Health Services The following list of interview questions guided the conversations: 1. How would you like to see the sector approach the redesign of services for the future? How
would you like your organization to be involved? How would we include governors? How would we include patients/clients? What could be the LHIN’s role?
2. What principles should guide the redesign? 3. Describe the current state of MH&A services within your area and in the wider SE LHIN region. 4. What are the key strengths in the region? Where are there any opportunities for improvement?
What is the capacity in the system – what are wait times like for patients? 5. How clear and understood is the need of change (redesign)? 6. What are the key documents that should support the redesign? (e.g. insights to improving
client flow and access to care in youth transitions) 7. How do you envisage working together to redesign the sector? What are any challenges?

68
8. How do we work across sectors – housing, children? 9. How can we work together to ensure the redesign project is successful? 10. What do you think the risks are in approaching this redesign project? 11. What is your vision for the SE region’s MH&A services? 12. What will the sector look like for FY 2016/17? 13. What will the experience be like for a patient/client? Key themes:
Current state of Mental Health and Addiction services
There has been a lot of collaboration in the SE LHIN to date related to Mental Health and Addiction service.
Many stakeholders have found the partnerships which have been formed to be extremely valuable.
The level of collaboration between community and hospital varies between regions – some experiences with collaboration are more positive than others.
Thought, some stakeholders have found there to be a lot of pressure to obtain results – which can be challenging for smaller agencies.
There is a lack of standardization of services.
For example, the work of Case Managers is not necessarily the same across the region.
The lack of data related to Mental Health and Addiction is an issue.
Some agencies have implemented more robust data reporting processes to monitor capacity. Though, this is done in silos and so the information is not shared regionally.
Outcomes are not being measured consistently across the region. There is a need for better data on outcomes. It is not enough to say that clients have been served – need to know if health outcomes are improving, as well as what is working and what is not working.
There is a lack of equitable access across regions.
For example, some regions are sending funding back for Psychiatric consults because they cannot access psychiatric services.
Overall, there is a lack of ability to triage access to psychiatry services in an effective way.
Providers are competitive for resources, which is driven by the way the system is set up.
Mental Health and Addiction is poorly resourced in every venue (from community to hospital), which naturally incents organizations to become competitive for resources.
Rather, the system should be set up to incent and reward collaboration.

69
With all of the resources that are available in the SE LHIN region, services should be better.
Need better integration of services and collaboration between providers to make more efficient/effective use of resources.
Stakeholders have a lot of valuable perspective from the patient that the system is disjointed.
Key strengths, opportunities for improvement and capacity in the system
The players in the SE LHIN region are a very committed group.
Many players are working well together, and would like to build on the strengths of the sector. They have many successful examples of working together – including: Clinical Services Roadmap, Concurrent Disorders Initiative, Service Collaboratives.
Though, some players shared that there is a culture of HSPs ‘protecting their territory’ – which at times impedes their openness to integration.
Overall, HSPs greatly appreciate the LHIN’s support for projects – through endorsement and accountability through MSAAs – and many see this as a key strength in driving the redesign.
The Concurrent Disorders Initiative and Health Links have been cited as foundational to the redesign.
Further, the CSR initiative was cited as an initiative in which the resourcing approach was successful (i.e. the LHIN staff supported the Project Management and a lot of the groundwork)
A significant gap, and area for improvement, is the involvement of patients and families in the system design and system planning. Many feel that the services are not representative of the people served.
Providers believe there is a great deal of value in existing networks of family members and people living with Mental Health and Addiction issues (i.e. Early Intervention Psychosis Program, Hotel Dieu)
Patients and families should be engaged in a variety of ways (i.e. surveys, focus groups, etc.) – not just one way. This will ensure that planning is based on concrete data that is validated.
Consultations should be open to all communities – i.e. Aboriginals, gay, lesbian, transsexual, transgender, francophone, dual diagnosis and other diverse populations.
Opportunity to engage people on face-to-face basis would bring tremendous value.
Many stakeholders believe that current planning tables have the capacity to manage the planning component of the redesign – though, some believe there is no capacity.
All stakeholders voice the need to have support for implementation. Need to recognize that resources and remuneration are needed to support the redesign.
Suggested that the redesign consider models such as secondments.

70
Approaching the redesign of the sector
Need to do an inventory of what exists within the sector, so that the redesign does not leave any pieces out.
Need to ensure that there is a clear understanding of the services that HSPs provide, so as to understand how the current services can work better together.
Also, need to understand referral criteria, wait times, etc. (to understand why referrals are not accepted; i.e. referring inappropriately or long wait lists)
Need to be able to look at redesign without looking at job implications and attitude of ‘protecting territory’.
This leads to missed opportunities – prevents the ability to consider the best potential outcomes for the client – because agencies are not forthcoming with information.
Suggested a third-party with knowledge and experience in redesigning mental health services, in order to prevent bias and to ensure credibility.
Everyone needs to be at the table, not just a select few.
Need to include clients, families and representatives. All HSPs should have a say in the redesign; though, does not
mean a veto. To move the system forward everyone needs to have input, but not a “vote”.
Need better communication and sharing of information to let providers know what is going on.
Suggested to publish best practices and guidelines, for all to be accountable to – this is how you design a system.
Currently, standards exist, but there is no accountability to the standards. There needs to be an evidence-based framework to drive the model forward.
The LHIN needs to be clearer about its direction.
Currently, stakeholders see the LHIN communicating a general notion of integration.
Need to be clear about what the redesign means and what the objectives are. It does not need to be prescriptive, but does need to be clearer.
Some stakeholders believe that the LHIN should exercise its integration orders; HSPs should first be invited/encourage to integrate, but when this does not happen, integration orders should be put in place.
Putting definitions around this will be key to the success of the redesign.
LHIN – can be a policy buster. They can be the conduit to the Ministry.
Need to make sure agencies involve their Boards; this needs to be a partnership.
For example, if there needs to be a merger, should have Boards working together.
The redesign should be orchestrated by the LHIN, and

71
directed by the Boards. With the LHIN collaborative governance meetings, this would
seem to be the most likely place to engage Boards. Suggested that by making the redesign part of some
legislation would help to facilitate Board engagement in the process (Board pays attention because there are deliverables that the Board can sign off on)
Suggested to include the work into annual Board plans in order to engage Boards.
Other suggested ideas for approach:
Must take into account regional differences – consideration that local solutions and regional solutions are different. Further, must consider rural and urban mental health.
Need to recognize the Mental Health and Addiction services which are available provincially, and build those integrations more effectively.
Need to have commitment and someone to say this is a must. This should be the LHIN, through M-SAA.
Need to take in to consideration that some organizations in the system are charities; must look at how CRA comes in to the play. This can be a benefit or a barrier, but must be considered.
Need to be open to how providers work together (i.e. governance changes, co-locations, etc.)
Need to plan for growing geriatric population. The redesign must align with the tactics and directions of the
hospitals. Do not need to spend any more time on the “why”; need to
move to the “how”. Suggested to look to other provincial models; i.e. Cancer
Care, Renal Network. Suggested to look at the notion of ‘clustered community
services’ as an option to ensure the redesign aligns all of the services within scope.
Suggested to have a group that brings forward the best evidence – bringing forward integrated care. Essentially instead talking about intake etc., bring forward a mental health worker who is part of the team. The individual would be used for expertise and support and integrated into a FHT – to bring forward new models and evidence.
Need to ensure there is enough resource base and human resources dedicated to the initiative; and skill building and resources for quality improvement.

72
Need a skilled individual – to say to nay-sayers – “Do you really want to stop the system? What do want for this from addictions, what do you want from mental health, what do you want from specialized services?”
In the South East – develop a network of supports to have continuous exchange – that is virtual and face to face. Need a knowledge exchange strategy to allow the exchange of ideas and the ‘whys’ and ‘whats’.
Risks
There is a lack of trust between Addiction and Mental Health.
Addiction services needs to maintain a strong focus, as traditionally Addiction sometimes gets consumed by Mental Health.
There must be recognition that there is a population that requires Addiction services, and a population that requires both. Where there is overlap, need to work closely together.
Need to promote an environment in which Addiction stakeholders feel they can share their opinion and it won’t get lost in the larger picture of Mental Health.
There is a risk of competing priorities and directions.
The LHIN is looking at redesign amongst many other competing priorities. Currently, CSR, Service Collaborative, Health Links, etc. – as well as various other Ministries.
With all rolling out concurrently, must clearly understand how they overlap and how they will be resourced to move forward effectively.
Need to be conscious of the different purposes and timelines, and how the redesign may impact these other initiatives.
Lack of trust regarding who is leading the redesign and those that are providing input.
Stakeholders recommend strongly that a ‘co-lead’ structure be put in place (Administrative and Medical); an Expert Panel is fine, but to address trust there needs to be someone who has operationalized Mental Health.
There exists a strong fear of losing the voice of youth Mental Health and Addiction; must remain focused on transitional aged youth.
There has to be planning between the psychiatry group and the administrators.
Vision for the SE region’s Mental Health and Addiction services
Address gaps in counseling and access to psychiatry. Seamless services with respect to the changing needs of the users; so they don’t have to relive

73
their story. Seamless journey which is easily navigated by the consumer; a simultaneous push and pull of
services (push appropriate services and pull consumer to services so that they do not fall through the cracks)
Consideration that mental illness does not happen during business hours; around the clock response.
Fully integrated Mental Health and Addiction service delivery. Address social determinants (housing, poverty, income, etc.) Based on the ‘right care, for the right person, and the right place’. Client-based, not provider-based. Whole person and whole family. Address the preventative side; need to provide services where they are needed (“when people
show up on their knees, not when they are flat on their face”) Leverage OTN and find ways to share resources. Each region should have access to the same services, and should be some reflection of the
volumes in the communities. Less players in the space. Taking the resources to where the patient is. Standardization of best practices.
Key documents to support the redesign, as identified by stakeholders: Capacity report Physician paper (outlining essential skills for workers) Partnerships that Work (for guiding principles on how to work together across the region)
74
Appendix 5: Project Manager Role Description REVISION: April 1, 2013 JOB TITLE: Project Manager, Mental Health and Addiction Sector Redesign JOB GRADE: LHIN to Determine REPORTS TO (job title): LHIN to Determine JOBS REPORTING (job titles): None DIVISION / DEPARTMENT: LHIN to Determine LOCATION: Belleville
PRIMARY PURPOSE: The Project Manager will be responsible for managing and implementing the detailed Project Plan for the Redesign of the Mental Health and Addiction Services in the South East LHIN. The Project Manager will work with a Redesign Task Force to design and implement the redesign for the Mental Health and Addiction Sector.
The goal of the Project Manager is to organize and manage resources and tasks in an effective way to meet the project’s defined scope, quality, time and cost requirements, and ultimately to achieve the project’s objectives. The Project Manager will be accountable for the successful execution of each task within the Project Plan. KEY ACCOUNTABILITIES:
Maintains ownership of the Project Plan and each task – bringing direction, drive, focus and tempo.
Develops a number of project management processes and tools, including: communications processes, a process (e-room, portal, etc.) for stakeholders to provide information/-on-going feedback, stakeholder engagement plan, change management plan, and risk mitigation plan.
Prepares performance reports against the Project Plan and presents these to the South East LHIN Senior Management Team
Works collaboratively with the Expert Panel and the Redesign Task Force.
Stays informed of provincial and inter-LHIN planning activities related to Mental Health and Addiction redesign.
Stays abreast of best practices and methodologies in healthcare planning and project management in order to identify and recommend best planning and execution approaches.
Escalates roadblocks as well as obstacles to deliverables or changes to timelines on ad hoc basis.
Recommends to Senior Management how to minimize/mitigate roadblocks to progress.
Other duties as assigned. POSITION REQUIREMENTS: Education:
Post-secondary training/degree in health administration, health planning, business administration, research or relevant field. Project Management Professional certification is an asset.
Experience:
Previous experience in carrying out research, analysis and project planning initiatives, preferably in the healthcare sector.
Previous experience in project management, project processes and project technical dimensions.
Good knowledge of and proven ability to apply multiple planning and analysis methodologies and make effective recommendations.
Understanding of the Ontario healthcare system and issues; specifically, within the Mental Health and Addiction sector.
Excellent written communications skills to prepare clear reports and analyses of data which will support effective decision-making and priority-setting.
Excellent oral communications skills and experience with facilitating large groups and senior executives.

75
NATURE AND SCOPE:
Interpersonal Contacts: Internally, the position engages and communicates with key staff and Senior Management to present and discuss information and problems related to undertaking the design and implementation of the new model for the Mental Health and Addiction sector. Externally, the position communicates directly with various stakeholders to obtain and exchange the information required by the Expert Panel and the Redesign Task Force, and gain consensus and agreement on the needs, priorities and model options required for the design and implementation of the new model. The position communicates with key enablers to project successes.
Level of Responsibility: The position provides a project management support role in the design and implementation of the new model for the Mental Health and Addiction sector. The position works closely with various staff and Senior Management Team member to discuss work plans and priorities. The position directs and manages team members with respect to the project charter objectives and work plan.
Decision-Making Authority: The position provides critical analytical work to determine and support key decisions related to the redesign of the Mental Health and Addiction sector. The position also provides direction to project stakeholders.
Travel Required.

76
Appendix 6: Examples of Planning Commitees
There are a number of planning committees in the South East LHIN which focus on Mental Health and Addictions. A list is provided below, this may not be complete but provides an overview of the type of current planning. CSR MHA Health Human Resources CSR MHA Emergency Department CSR MHA Coordinated Access CSR MHA Tier III Lanark, Leeds & Grenville Coalition Kingston, Frontenac, Lennox and Addington Coalition Hastings Prince Edward Coalition Addictions and Mental Health Network Meetings Concurrent Disorders Capacity Group Addictions Ontario (membership) Drug Treatment Funding Project Residential Standards Writing Team Youth Services Collaborative – KFLA KFLA Child & Youth Services Planning Committee Concurrent Disorders Capacity Project Working Group SEO Problem Gambling Network FASD Action Network – KFLA Dual Diagnosis & Substance Misuse Working Group Joint Operational Leadership Team (KFLA) SEO Human Services and Justice Co-ordinating group L&A Human Services and Justice Co-ordinating group (chair) Sexual violence/Domestic Violence Working Group (L&A) LEAD team co-ordinating group (L&A and Kingston) SEO Crisis Psychiatric Services Working Group JOLT
BSO Forum LEAD Conference Planning Forum Leeds Grenville Human Services Justice Coordinating Committee Mental Health Initiatives Working Group – Child and Youth Thousand Island Health link North Grenville South Ottawa Health link CEO Collaboration Group LLG Victims Issues Coordinating Council CPHC Advisory Council HEADS UP Advisory Board Lanark Human Services and Justice Group Specialized Treatment Home Committee Human Services Committee for Police and Mental Health Protocol Development

77
Lanark Drug Strategy Committee Rural Health Sciences Network HPE Health Care Integration Committee Health Links Groups – HPE and Central Hastings Provincial Consumer Survivor LHIN Leads Network System Improvement Service Collaborative KFL&A Coordinating Committee Against Violence