-
Progress in Neuro-Psychopharmacology & Biological Psychiatry
58 (2015) 81–88
Contents lists available at ScienceDirect
Progress in Neuro-Psychopharmacology &
BiologicalPsychiatry
Involvement of the dorsolateral prefrontal cortex and superior
temporalsulcus in impaired social perception in schizophrenia
Jung Eun Shin a,b, Soo-Hee Choi c, Hyeongrae Lee d, Young Seok
Shin e, Dong-Pyo Jang e, Jae-Jin Kim a,b,f,⁎a Brain Korea 21 PLUS
Project for Medical Science, Yonsei University College of Medicine,
Seoul, Republic of Koreab Institute of Behavioral Science in
Medicine, Yonsei University College of Medicine, Seoul, Republic of
Koreac Department of Psychiatry, Seoul National University College
of Medicine and Institute of Human Behavioral Medicine, SNU-MRC,
Seoul, Republic of Koread Magnetoencephalography center, Department
of Neurosurgery, Seoul National University Hospital, Seoul,
Republic of Koreae Department of Biomedical Engineering, Hanyang
University, Seoul, Republic of Koreaf Department of Psychiatry,
Yonsei University College of Medicine, Seoul, Republic of Korea
Abbreviations: fMRI, functionalmagnetic resonance imfrontal
cortex; STS, superior temporal sulcus; DMPFC, dortemporo-parietal
junction; DSM-IV-TR, Diagnostic andTest-Revised; RPM, Raven's
progressive matrices; SAS, SPositive and Negative Syndrome Scale;
SC-LFS, Strauss–Scale; TE, echo time; TR, repetition time; BOLD,
blood oxyg⁎ Corresponding author at: Department of Psychiatry
211 Eonju-ro, Gangnam-gu, Seoul, 135–720, Republic offax: +82 2
3462 4304.
E-mail address: [email protected] (J.-J. Kim).
http://dx.doi.org/10.1016/j.pnpbp.2014.12.0060278-5846/© 2014
Elsevier Inc. All rights reserved.
a b s t r a c t
a r t i c l e i n f o
Article history:
Received 12 September 2014Received in revised form 5 December
2014Accepted 19 December 2014Available online 27 December 2014
Keywords:Daily lifeDorsolateral prefrontal
cortexSchizophreniaSocial perceptionSuperior temporal sulcus
Background: Schizophrenia is a mental disorder characterized by
impairments in diverse thinking and emotionalresponses, which are
related to social perception dysfunction. This fMRI study was
designed to investigate aneurobiological basis of social perception
deficits of patients with schizophrenia in various social
situations ofdaily life and their relationship with clinical
symptoms and social dysfunction.Methods: Seventeen patients and 19
controls underwent functional magnetic resonance imaging, during
whichparticipants performed a virtual social perception task,
containing an avatar's speech with positive, negative orneutral
emotion in a virtual reality space. Participants were asked to
determine whether or not the avatar'sspeech was appropriate to each
situation.Results: The significant group × appropriateness
interaction was seen in the left dorsolateral prefrontal
cortex(DLPFC), resulting from lower activity in patients in the
inappropriate condition, and left DLPFC activity wasnegatively
correlated with the severity of negative symptoms and positively
correlated with the level of social
functioning. The significant appropriateness × emotion
interaction observed in the left superior temporal sulcus(STS) was
present in controls, but absent in patients, resulting from the
existence and absence of a differencebetween the inappropriate
positive and negative conditions, respectively.Conclusions: These
findings indicate that dysfunction of the DLPFC-STS networkmay
underlie patients' abnormalsocial perception in various social
situations of daily life. Abnormal functioning of this networkmay
contribute toincreases of negative symptoms and decreases of social
functioning.
© 2014 Elsevier Inc. All rights reserved.
1. Introduction
Schizophrenia is a mental disorder characterized by impairment
inthinking and emotional responses. Clinical symptoms including
posi-tive, negative and disorganized symptoms as well as various
cognitivedeficits lead to social dysfunction, such as ineffective
social interaction,poor social skills and the inability to remain
employed (Boden et al.,
aging; DLPFC, dorsolateral pre-somedial prefrontal cortex;
TPJ,Statistical Manual, 4th Edition,ocial Anhedonia Scale;
PANSS,Carpenter Level of Functioningen level dependent., Gangnam
Severance Hospital,Korea. Tel.: +82 2 2019 3341;
2009; Weinberg et al., 2009). Social dysfunction in
schizophrenia maybe lifelong and predictive of longer
hospitalization (Olfson et al., 2011).In particular, deficits in
social cognition including social perception havebeen linked to
poor functional outcome in schizophrenia (Mancusoet al., 2011).
Social perception involves the ability to identify socialroles,
rules and context and to make inferences about complex or
am-biguous social situations (Green et al., 2008; Penn et al.,
2002). Socialperception is the first step in social cognition, and
it is further involvedin processes of organizing behavioral
responses directly or indirectly(Norman, 2002), suggesting that
abnormal behaviors observed inschizophrenia may be initiated by
impaired social perception.
To understand social perception, previous researchers have
usedvarious stimuli. Human faces are frequently used stimuli
because theyare the basic component of social perception and
provide diverse infor-mation for social communication (Kanwisher et
al., 1997; Marwick andHall, 2008). Patients with schizophrenia have
deficits in both face andfacial affect recognition with less
accurate and slower responses thancontrol participants (Green and
Phillips, 2004; Hooker and Park, 2002),
http://crossmark.crossref.org/dialog/?doi=10.1016/j.pnpbp.2014.12.006&domain=pdfhttp://dx.doi.org/10.1016/j.pnpbp.2014.12.006mailto:[email protected]://dx.doi.org/10.1016/j.pnpbp.2014.12.006http://www.sciencedirect.com/science/journal/02785846
-
82 J.E. Shin et al. / Progress in Neuro-Psychopharmacology &
Biological Psychiatry 58 (2015) 81–88
and they have functional abnormalities in the fusiform gyrus
during thefacial information processing (Quintana et al., 2003).
Another usefulmethod is biological motion. Patients with
schizophrenia have impairedgaze discrimination with longer reaction
time and hyper-perception(Franck et al., 2002; Tso et al., 2012)
and often show difficulties in dis-criminating biological motion
due to abnormalities in the superior tem-poral sulcus (STS) and
inferior parietal lobe (Kim et al., 2011b; Spenceret al., 2013;
Thakkar et al., 2014). In particular, the STS is involved in
un-derstanding other people's actions and intentions (Pelphrey et
al., 2004)and has been considered to be one of the core regions for
the interactionof social perception and emotional processing
(Kramer et al., 2010;Norris et al., 2004).
While perceiving others' behaviors in social situations,
patients withschizophrenia showdysfunction in the intention
network, including thedorsomedial prefrontal cortex (DMPFC) and
temporo-parietal junction(TPJ) (Bara et al., 2011; Walter et al.,
2009). In addition, patients withschizophrenia have shown aberrant
responses in the occipital andtemporal regions while processing
situational pictures as social cues(Bjorkquist and Herbener, 2013),
marked decreases in dorsolateralprefrontal cortex (DLPFC)
activation during audiovisual integration(Szycik et al., 2009), and
ventral premotor dysfunction during video-watching (Ebisch et al.,
2013; Park et al., 2009). Particularly, giventhat the DLPFC plays
an important role in cognitive control in socialsituations
(Weissman et al., 2008), DLPFC hypofunction may be a lead-ing
factor regarding dysfunctional social perception in patients
withschizophrenia.
Despite the accumulation of vast amount of knowledge, social
per-ception remains an actively studied area because of its
complexity anddiversity.More complex social situations have been
increasingly neededto discover how the brain works with a plethora
of stimuli. Since the1990s, several behavioral studies have used
social situations as a stimu-lus. The examples are the social
feature recognition test (Corrigan et al.,1996) and the social cue
recognition videotaped test (Corrigan andNelson, 1998),
demonstrating that patients with schizophrenia areless accurate in
situational feature recognition or social cue recognitionthan
controls. Recently, it has been reported that these deficits in
socialperceptionmay be related to abnormal eye gaze in interactive
social sit-uations (Choi et al., 2010). However, complex social
situations havenever been used in a functional magnetic resonance
imaging (fMRI)study. It therefore remains unclear how the brain
mechanism of deficitsin social perception underlies the experiences
of patients with schizo-phrenia in their daily lives. This unclear
mechanism can be addressedby an fMRI study using a virtual reality
task reflecting social perceptionin daily lives, as virtual reality
provides an immersive environment sim-ulating complex social
situations (Choi et al., 2010; Han et al., 2009). Infact, virtual
reality tasks using avatars have been used to assess
patients'behavioral and emotional characteristics objectively and
to train pa-tients to cope effectivelywith various social
situations (Kim et al., 2008).
This fMRI study was designed to investigate a neurobiological
basisof social perception deficits in schizophrenia using social
situationsthat patients would face in their daily lives. For these
purposes, wedeveloped a virtual social perception task in which
participants wereasked to determine the appropriateness of various
ways of speech indifferent social situations. In this study using
dynamic stimuli and func-tional outcome measures, we hypothesized
that patients with schizo-phrenia would show altered activation in
various social perception-related regions including the prefrontal
cortex and STS, and that thedegree of altered activation would be
correlated with the clinical andsocial functioning scale
scores.
2. Methods
2.1. Participants and clinical measurements
Seventeen patients with schizophrenia and 19 healthy control
sub-jects participated in this study. All patients met the
DSM-IV-TR criteria
for schizophrenia without other comorbid psychiatric disorders
andwere taking antipsychotics with a mean
chlorpromazine-equivalentdosage of 503.3 ± 226.4 mg. The Structural
Clinical Interview forDSM-IV (First et al., 1996) was used for the
diagnosis of schizophreniain patients, who were recruited in the
psychiatric outpatient clinic,and the exclusion of any psychiatric
disorders in controls, whowere re-cruited by poster advertisements.
Any subjects with a past or presenthistory of medical or
neurological illness or with left-handedness wereexcluded. After a
complete description of this study was presented, allsubjects gave
written informed consent to the protocols, which wereapproved by
the local institutional review board.
Participants' general intellectual ability was measured by
theRaven's progressive matrices (RPM) (Raven, 1990), and the
ability toexperience pleasure from social stimuli was measured by
the SocialAnhedonia Scale (SAS) (Chapman et al., 1976). In
addition, the clinicalstatus of each patient was measured using the
Positive and NegativeSyndrome Scale (PANSS) (Kay et al., 1987) for
the severity of schizo-phrenic symptoms and the Strauss–Carpenter
Level of FunctioningScale (SC-LFS) (Strauss and Carpenter, 1972)
for various domains ofsocial functioning such as social contacts,
useful work and fullness oflife.
2.2. Experimental design
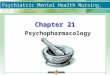
Participants performed the virtual social perception task during
fMRIscanning. As shown in Fig. 1, social situations were created in
a virtualreality space in which an avatar made conversation with
someone. Par-ticipants were asked to determine whether or not the
avatar's speechwas appropriate to the situation by pressing a
corresponding button.The task consisted of 126 experimental trials;
therewere 21 real-life sit-uations that each included six different
conditions. The avatar's speechwas either well or poorly matched to
the situation, in 63 appropriateand 63 inappropriate conditions,
respectively, and was emotionallypositive, negative or neutral, in
42 positive, 42 negative, and 42 neutralconditions, respectively.
The trials were presented randomly in anevent-related design. Each
trial consisted of listening to the avatar'sspeech for 3 s,
followed by 1 s of silence during which participantswere expected
to respond, and seeing a screen with a cross on a blackbackground
for 1 s. Null events were added in varying durations of0.625 to 7.5
s, and the total session time was approximately 14 min.
2.3. MRI acquisition and analysis
The fMRI experiment was conducted on a
research-dedicated,whole-body, 1.5 T MRI system (Sigma Eclipse; GE
Medical Systems,Milwaukee, WI, USA) using a standard quadrature,
bird-cage headcoil. Functional images were obtained using an echo
planar imaging se-quence (matrix size=64× 64, number of slices= 30,
slice thickness=5mm, spatial resolution=3.75 × 3.75 × 5mm3,
TE=22ms, TR=2.5 s,field of view = 240 mm, flip angle = 90°).
High-resolution anatomicalimages were obtained using a gradient
echo sequence (matrix size =256 × 256, number of slices = 115,
slice thickness = 1.5 mm, spatialresolution = 0.94 × 0.94 × 1.5
mm3, TE = 1.8 ms, TR = 8.5 ms, fieldof view = 240 mm, flip angle =
12°) after the functional scans.
Imageswere preprocessed using SPM8 (Welcome Institute of
Cogni-tive Neurology, London, UK; www.fil.ion.ucl.ac.uk/spm), and
bad sliceswere detected and discarded using ArtRepair software
(Mazaika et al.,2005). After correcting for differences in slice
acquisition time andhead motion, the functional images were
co-registered to the T1-weighted image. The co-registered images
were spatially normalizedusing the transformation functions, which
were obtained by normaliz-ing the T1-weighted image to the standard
T1 template using nonlineartransformation. These normalized
imageswere smoothed by a Gaussiankernel of
8mmfull-width-half-maximum.Ahigh-passfilter (128 s)wasapplied on
the image time series to eliminate low frequency signals.
http://www.fil.ion.ucl.ac.uk/spm
-
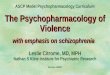
Fig. 1. An example of the experimental stimuli. In a scene of
“at the kiosk,” a woman says something to a storekeeper for 3 s. As
shown on the right side, there are six different trials perscene.
In the appropriate positive condition (APP-POS), her statement
(“Thanks. I hope you to sell a lot!”) is positive and well matched
with the situation. On the other hand, in theinappropriate positive
condition (INA-POS), she says “Help yourself to as much as you
want,” and this statement is positive, but unmatched with the
situation. Four other trials includedthe appropriate negative
(APP-NEG), inappropriate negative (INA-NEG), appropriate neutral
(APP-NEU), and inappropriate neutral (INA-NEU) conditions. Twenty
other scenes with sixconditions were used to express diverse social
situations.
83J.E. Shin et al. / Progress in Neuro-Psychopharmacology &
Biological Psychiatry 58 (2015) 81–88
Functional data were analyzed using a general linear model. To
ex-clude activities related to the processing of neutral emotion,
individualcontrast maps were generated by contrasting positive or
negative emo-tional events with neutral ones at the first-level
analysis. The resultingset of contrast images were then entered
into a second-level analysisusing a flexible factorial model. The
activationmaps for themain effectsand interactionswere analyzed by
a 2 (group: patients and controls) × 2(appropriateness: appropriate
and inappropriate) × 2 (emotion; posi-tive and negative) flexible
factorial model. In addition, the appropriate-ness × emotion
interaction was analyzed in each group. For thecomparison between
trial types, activation was determined by uncor-rected p values of
less than 0.001 with a cluster extent threshold of20 voxels and by
corrected p value of less than 0.05 after the falsediscovery rate
across the entire brain.
Finally, to ascertain the clusters related to task performance,
a regionof interest correlation analysis was performed. Based on
our hypothesisthat patients with schizophrenia would show altered
activation in theprefrontal cortex and STS during social
perception, we selected twoclusters in the DLPFC identified by the
result of the group× appropriate-ness interaction and the STS
identified by the appropriateness ×emotion interaction under each
group. The % BOLD signal changes ofthe clusters were obtained using
MarsBaR version 0.41 (http://marsbar.sourceforge.net/) and then
non-parametric correlation analyses betweencluster activities and
clinical scales in each group were done at a signifi-cance level of
p-values less than 0.05. In these correlation analyses, theduration
of illness and chlorpromazine equivalent dose were used
ascovariates for the patient group.
2.4. Statistical analysis of the behavioral data
Demographic and clinical characteristics were compared
betweengroups with independent-sample t-tests and chi-square tests.
Accuracyand reaction time were analyzed using linear mixed model.
The mainand interaction effects of group, appropriateness, and
emotion wereincluded as fixed effects. In the post hoc analysis the
least squaremeans of 3 emotionswere estimated by theMIXED procedure
at appro-priate or inappropriate.
3. Results
3.1. Participants' characteristics and behavioral
performances
As shown in Table 1, patients and controls did not significantly
differin age, sex and educational level. However, patients showed
lower gen-eral intellectual ability (p b 0.05) and higher social
anhedonia scores(p b 0.05) than controls.
Accuracy and reaction time are shown in Table 2. The main effect
ofaccuracy was found for group (F1,203 = 27.37, p b 0.001), but not
forappropriateness and emotion. Post hoc analyses revealed that
patientsanswered less correctly than controls (p b 0.001). The
interaction effectwas found for the appropriateness × emotion
(F2,203 = 3.26, p b .05).The statistic power for these positive
results was 0.9 and 0.7 (α =0.05) with N95% confidence interval in
the group effect and appropri-ateness × emotion interaction effect
of accuracy, respectively. Themean differences between emotions for
appropriate speech were 0.48(positive and neutral), 13.84 (positive
and negative), and 13.36 (nega-tive and neutral). For inappropriate
speech, however, the mean differ-ences between emotions were
−0.30,−6.76, and −6.46, respectively.No significant interaction
effect was found for group × appropriatenessor group × emotion, and
group × appropriateness × emotion. For reac-tion time, there were
no significant main or interaction effects.
3.2. Imaging findings
Imaging results of the main effects for group, appropriateness,
andemotion are provided in Supplementary Table 1. On an analysis
offunctional neuroimaging, data of three patients and one control
wereexcluded due to a quality problem as bad slices were discarded
usingArtRepair software. The main effect of group was found in a
variety ofthe neocortical and subcortical regions, including the
various prefrontalgyri, various temporal gyri, STS, supramarginal
and angular gyrus,precuneus and cuneus, globus pallidus, and
cerebellum. Themain effectof appropriatenesswas found in the
relatively restricted regions, includ-ing the inferior frontal
gyrus, middle temporal gyrus and precuneus.The main effect of
emotion was also restricted to the precentral gyrus,middle temporal
gyrus, caudate, and cerebellum.
http://marsbar.sourceforge.net/http://marsbar.sourceforge.net/
-
Table 1Demographic information about patients with schizophrenia
and controls.
Patients Controls χ2/t P
(n = 17) (n = 19)
Age (years) 31.0 ± 6.1 28.21 ± 4.2 −1.609 0.117Sex (male/female)
11/6 12/7 0.009 0.923Education level (years) 13.8 ± 1.6 14.6 ± 3.0
1.006 0.321Intelligence quotient 98.7 ± 15 109.1 ± 12 2.270
0.030Social anhedonia scale (0–40) 13.4 ± 6.2 8.8 ± 3.9 −2.581
0.016PANSSPositive 17.1 ± 3.7Negative 17.3 ± 4.5General 32.6 ±
8.4
SC–LFS (0–36) 20.8 ± 5.5Duration of illness 10.9 ±
6.9Chlorpromazine equivalent dosage of antipsychotics (mg)⁎ 503.3 ±
226.4
PANSS, Positive and Negative Syndrome Scale; SC–LFS,
Strauss–Carpenter Level of Functioning Scale.⁎ The medicine was
amisulpride (2), aripiprazole (3), clozapine (3), haloperidol (1),
olanzapine (3), paliperidone (1), quetiapine (1), and risperidone
(4).
84 J.E. Shin et al. / Progress in Neuro-Psychopharmacology &
Biological Psychiatry 58 (2015) 81–88
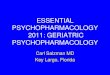
As presented in Table 3, the group× appropriateness
interactionwasexhibited in the left DLPFC, right precentral gyrus
and left supramarginalgyrus. In the post hoc test for the a priori
regions, as shown in Fig. 2, leftDLPFC activity in the appropriate
condition was not significantly differ-ent between the two groups,
whereas left DLPFC activity in the inappro-priate conditionwas
significantly lower in patients than in controls (t=2.6, p b 0.05).
Correlation analysis revealed that left DLPFC activity inthe
inappropriate condition was negatively correlated with the
PANSSnegative scores (r = −0.650, p b 0.05) and positively
correlated withthe SC-LFS scores (r = 0.691, p b 0.05), but not
with any other scalescores. A group × emotion interaction was not
found in any region.
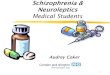
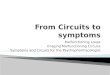
An appropriateness × emotion interaction was observed in
variousbrain regions including the right DMPFC, left DLPFC, left
STS, right supe-rior temporal gyrus, several occipital regions, and
right cerebellum. Anappropriateness × emotion interaction in each
group indicated that dif-ferent regions were involved. In
particular, as shown in Fig. 3, an appro-priateness × emotion
interaction in the left STS was found in controls,but not in
patients. Post hoc analysis revealed that left STS activity in
pa-tients was significantly higher in the appropriate negative
conditionthan in the appropriate positive condition (t = −3.1, p b
0.01), butnot significantly different between the inappropriate
negative andinappropriate positive conditions. Left STS activity in
controls was alsosignificantly higher in the appropriate negative
condition than in theappropriate positive condition (t = −2.1, p b
0.05), but significantlylower in the inappropriate negative
condition than in the inappropriatepositive condition (t = 3.9, p b
0.01).
4. Discussion
In thepresent study,we investigated thebrainmechanisms
involvedin perceiving appropriateness and emotion in social
situations. Usingthe MR-compatible virtual reality system, we
presented diverse socialsituations to participants. Previously, our
research group demonstrated
Table 2The accuracy and reaction time for the virtual social
perception task (mean ± standarddeviation).
Patients (n = 17) Controls (n = 19)
Appropriate Inappropriate Appropriate Inappropriate
Accuracy (%)Positive 71.43 ± 30.91 63.31 ± 37.86 89.72 ± 10.07
82.21 ± 32.06Neutral 69.75 ± 28.02 61.06 ± 33.77 90.48 ± 9.12 84.96
± 30.21Negative 58.82 ± 28.07 67.79 ± 31.25 74.44 ± 28.58 91.23 ±
16.21
Reaction time (ms)Positive 722.88 ± 291.65 704.26 ± 244.07
672.25 ± 324.75 691.77 ± 330.59Neutral 676.69 ± 280.83 722.01 ±
235.16 685.49 ± 336.77 663.87 ± 332.05Negative 784.25 ± 239.88
705.85 ± 286.88 727.74 ± 336.22 655.22 ± 330.45
that such a virtual reality system was useful in assessing
social percep-tion of patients with schizophrenia as well as normal
subjects (Kimet al., 2007). In the diverse social situations of
daily lives, participantsdifferently responded according to the
conditions. Particularly, low ac-curacy in the appropriate negative
condition suggests that both patientsand controls might consider
negative events to be unfamiliar and un-comfortable because bad
news and unlucky events happen less oftenthan ordinary ones and
occur suddenly, and thus both groupsmight per-ceive situationswith
neutral or positive contents as being relativelymorecomfortable and
natural. In contrast, high accuracy for inappropriatenegative
speech suggests that such a condition seems to make bothgroups feel
awkward.
The most characteristic group difference while experiencing the
so-cial situationswas found in the left DLPFC. Significantly
decreased activ-ity in the left DLPFC was found during the
inappropriate condition inpatients compared to controls. Previous
studies have recognized thatthe DLPFC plays an important role in
various cognitive processes (Liuet al., 2004; MacDonald et al.,
2000). Typically, this region is engagedin cognitive
flexibilitywhen people face new and unexpected situationsto
restructure knowledge in multiple ways (Kim et al., 2011a; Gu et
al.,2008) and in abstract thinkingwhen regarding situations in
general andsymbolicmodes (Harrow et al., 1974). The role of
theDLPFC in cognitivecontrol has been shown in social situations of
inconsistent conditions(Weissman et al., 2008). Therefore, our
finding of DLPFC hypoactivityin patients suggests that impairment
in perceiving socially unusualsituations may stem from dysfunction
in cognitive control. This viewis supported by previous findings
that patients with schizophreniaexpressed cognitive rigidity in
real life (Han et al., 2012) and abnormalabstract thinking, which
was associated with impaired DLPFC function(Berman et al.,
1988).
In addition, our study showed that DLPFC activity in patients
had anegative correlation with the severity of negative symptoms
and a pos-itive correlationwith the level of social functioning.
Decreasedmetabol-ic activity in the DLPFC has been considered to be
a core feature relatedto the predominance of negative symptoms in
schizophrenia (Potkinet al., 2002; Wolkin et al., 1992). Cortical
volumetric abnormalities inthe DLPFC and disruption of the white
matter tracts connecting to theDLPFC have also been regarded as a
major feature of deficit schizophre-nia, which is characterized by
the presence of primary and enduringnegative symptoms (Fischer et
al., 2012; Voineskos et al., 2013). Deficitschizophrenia has been
associatedwith greater impairment in cognitiveability and social
cognition (Cohen et al., 2007; Csukly et al., 2014; Volpeet al.,
2012). In particular, negative symptoms include an
inclinationtoward stereotyped thinking (Piskulic and Addington,
2011) and areclosely related to social functioning (Hunter and
Barry, 2012). Therefore,DLPFC hypoactivity-related cognitive
inflexibility may lead to socialdysfunction in patients with
schizophrenia (Carrion et al., 2011; Hunterand Barry, 2012). Taken
together, DLPFC dysfunction in schizophrenia
-
Table 3Brain regions showing the significant interaction effect
of group, appropriateness, and emotion.
Regions (BA) Voxels MNI Coordinates F
x y z
Group × AppropriatenessDorsolateral prefrontal cortex (8)* 25
−22 44 36 15.2Precentral gyrus (6) 80 50 −4 40 22.8Supramarginal
gyrus (40) 23 −58 −40 36 14.4
Group × EmotionNone
Appropriateness × EmotionDorsomedial prefrontal cortex (8)* 79 8
32 48 17.1
58 0 56 30 16.5Dorsolateral prefrontal cortex (9)* 22 −46 8 26
16.5
39 −56 20 28 14.5Superior temporal sulcus (22)* 107 −56 −18 −2
20.0Superior temporal gyrus (22) 21 48 −50 2 14.2Inferior occipital
gyrus (17)* 418 −10 −98 −6 29.7Fusiform gyrus (37)* 651 −52 −64 −18
22.4Cuneus (17) 30 28 −78 10 17.4Cerebellum* 489 36 −66 −22
19.5
Appropriateness × Emotion in patientsCerebellum 60 −44 −50 −22
27.0
Appropriateness × Emotion in controlsSuperior temporal sulcus
(22)* 110 −56 −18 −4 30.2Lingual gyrus (18) 242 −12 −90 −8
23.6Cuneus (17) 61 28 −78 10 20.0Cerebellum 33 10 −82 −32 17.4
Presented regions had a threshold of uncorrected p b 0.001 and
more than 20 voxels. *Regions which survived after false discovery
rate corrected p b 0.05.
85J.E. Shin et al. / Progress in Neuro-Psychopharmacology &
Biological Psychiatry 58 (2015) 81–88
may reflect a deficit in cognitive control during social
perception, whichcontributes to negative symptoms and decreased
social functioning.
Another region showing a noteworthy feature was the left STS,
inwhich the interaction effect between appropriateness and
emotionwas present in controls, but absent in patients. In the
appropriate con-dition, both groups showed significantly higher
left STS activity inresponse to negative speech than to positive
speech. This feature of ac-tivity may be connected to the
behavioral observation that accuracy for
Fig. 2. (A) Dorsolateral prefrontal cortex (DLPFC) activity
showing the interaction of group× appcontrols, and (B) correlations
of DLPFC activity in the inappropriate condition with the
severity
appropriate speech was significantly lower in negative speech
than inpositive speech. The STS is activated by passive viewing of
biologicalmotion (Puce et al., 1998), and is further engaged in
analyzing the inten-tions of observed biological motions
(Lahnakoski et al., 2012; Pelphreyet al., 2004). STS activity tends
to be increased in unexpected comparedto expected situations (Ahmed
andVanderWyk, 2013). In the appropri-ate situations of our
experiment, positive speech appeared to be experi-enced as typical,
in contrast to the perception of negative speech as
ropriateness and the comparison of DLFPC activity in each
condition between patients andof negative symptoms and the level of
social functioning (*p b .05).
-
Fig. 3. Left superior temporal sulcus activity showing the
interaction of appropriateness and emotion that exists only in
controls, and the comparison of signal changes in the
superiortemporal sulcus based on conditions in each group (* p b
.05, ** p b .01).
86 J.E. Shin et al. / Progress in Neuro-Psychopharmacology &
Biological Psychiatry 58 (2015) 81–88
being a relatively uncommon occurrence. This situational
unusualnessof appropriate but negative speech might have led to the
discrepancyin response accuracy and STS activity, with both
patients and controlsacting in a similar fashion under this
appropriate condition. In the inap-propriate condition, however,
controls demonstrated significantlyhigher STS activity in response
to positive speech than to negativespeech, whereas patients showed
no difference between the two condi-tions. This reverse finding in
controls led to an interaction effect be-tween appropriateness and
emotion in the left STS, which is consistentwith the previous
notion that the STS plays a key role in the interactiveprocessing
of social and emotional information (Norris et al., 2004).Given
that STS activity is sensitive to the congruency between
observedaction and emotion (Wyk et al., 2009), the different STS
features be-tween the appropriate and inappropriate conditions in
controls maybe additional evidence for the role of this region in
analyzing the inten-tion of others. Furthermore, the absence of
this conditional difference inpatients seems consistent with their
difficulties in discriminating bio-logical motion (Kim et al.,
2011b; Spencer et al., 2013; Thakkar et al.,2014). Consistently,
our research group has recently reported thatpatients with
schizophrenia did not show normal STS hyperactivity ina socially
interactive situation that was designed to simulate social
re-jection (Lee et al., 2014), supporting the presence of patients'
deficitsin the perception of social acts.
In contrast to our expectations, MPFC activity was not
significantlydifferent between patients and controls in our study.
The MPFC hasbeen regarded as a representative brain region in the
theory of mindnetwork together with the STS (Bosia et al., 2012).
In particular, theMPFC has been implicated in mentalization, such
as making inferencesabout others' intentions andmental states, and
attributions of emotionsto self and others (Frith and Frith, 1999;
Ochsner et al., 2004). The ab-sence of a positive finding in this
region could be attributed to a charac-teristic of our task for
measuring social perception in daily life thatmight recruit
cognitive control or cognitive flexibility rather
thanmentalization. In other words, our social perception task may
provokeactivation of the DLPFC-STS network rather than the
MPFC-STS
network. Dysfunction of theDLPFC-STS network is striking in the
salientstimuli such as inappropriate situations, though there is no
direct evi-dence of connectional dysfunction between these two
regions in ourfindings. However, since abnormal connectivity
between the DLPFCand STS is important in individuals with autism
spectrum disorder(Wicker et al., 2008), it is possible that
impaired connectivity betweenthe two regions may underlie social
perception dysfunction in patientswith schizophrenia. This
interpretation is supported by another reporton schizophrenia,
which demonstrated the inferior frontal gyrus-STSdisconnection
during the processing of metaphoric gestures (Straubeet al.,
2014).
There are some limitations in our study. The generalizability of
ourresults may be limited due to the relatively small sample size.
Becauseall patients in our study were medicated and we did not
evaluate theside effects of the antipsychotic medications, the
effects of the antipsy-chotics could not be excluded from the
results. Further studies includingdrug-naïve patients need to be
done to avoid the confounding effects ofmedication. Another
limitation is that social functioning was assessedonly by the
SC-LFS. Many social functioning scales, which greatly varyin terms
of thenumber and types of domains, have beenused for schizo-phrenia
studies (Burns and Patrick, 2007). The SC-LFS includes domainsof
interpersonal and occupational function but has a weakness in
per-sonal domains. In addition, although cognitive control or
flexibilitywas considered to be an important factor in social
perception, executivefunctions were not evaluated. Given that there
was a significant differ-ence in general intelligence between
patients and controls, executivefunctions would be different
between the two groups and this differ-ence could affect the
performances.
In summary, we investigated the neural basis of social
perceptiondysfunction in daily life of patients with schizophrenia
and its relation-ship with their clinical symptoms and social
functioning. The resultsprovide useful information on the important
role of the DLPFC in socialperception and its relationship with
negative symptoms and socialdysfunction in patients with
schizophrenia. The findings also affirmthe key role of abnormal STS
activity in social perception dysfunction
-
87J.E. Shin et al. / Progress in Neuro-Psychopharmacology &
Biological Psychiatry 58 (2015) 81–88
in schizophrenia. These results suggest the possibility that
dysfunctionof the DLPFC-STS network may underlie patients' abnormal
social per-ception in various social situations of daily life.
Supplementary data to this article can be found online at
http://dx.doi.org/10.1016/j.pnpbp.2014.12.006.
Contributors
SHC and JJK designed the study. SHC, HL and YSS collected the
orig-inal imaging data. JES, YSS and DPJ managed and analyzed the
imagingdata. JES and JJK wrote the first draft of the manuscript.
All authorscontributed to and have approved the final
manuscript.
Acknowledgments
This work was supported by the National Research Foundation
ofKorea (NRF) grant funded by the Korea government (MEST) (No.
NRF-2013R1A2A2A03068342). We would like to thank Dr. Kang Joon
Yoonand Mr. Sang Il Kim for his valuable technical support.
References
Ahmed AA, Vander Wyk BC. Neural processing of intentional
biological motion in unaf-fected siblings of children with autism
spectrum disorder: an fMRI study. BrainCogn 2013;83:297–306.
Bara BG, Ciaramidaro A, Walter H, Adenzato M. Intentional minds:
a philosophical analy-sis of intention tested through fMRI
experiments involving people with schizophre-nia, people with
autism, and healthy individuals. Front Hum Neurosci 2011;5:7.
Berman KF, Illowsky BP, Weinberger DR. Physiological dysfunction
of dorsolateralprefrontal cortex in schizophrenia. IV. Further
evidence for regional and behavioralspecificity. Arch Gen
Psychiatry 1988;45:616–22.
Bjorkquist OA, Herbener ES. Social perception in schizophrenia:
evidence of temporo-occipital and prefrontal dysfunction.
Psychiatry Res 2013;212:175–82.
Boden R, Sundstrom J, Lindstrom E, Lindstrom L. Association
between symptomaticremission and functional outcome in
first-episode schizophrenia. Schizophr Res2009;107:232–7.
Bosia M, Riccaboni R, Poletti S. Neurofunctional correlates of
theory of mind deficits inschizophrenia. Curr Top Med Chem
2012;12:2284–302.
Burns T, Patrick D. Social functioning as an outcome measure in
schizophrenia studies.Acta Psychiatr Scand 2007;116:403–18.
Carrion RE, Goldberg TE, McLaughlin D, Auther AM, Correll CU,
Cornblatt BA. Impact ofneurocognition on social and role
functioning in individuals at clinical high risk forpsychosis. Am J
Psychiatry 2011;168:806–13.
Chapman LJ, Chapman JP, Raulin ML. Scales for physical and
social anhedonia. J AbnormPsychol 1976;85:374–82.
Choi SH, Ku J, Han K, Kim E, Kim SI, Park J, et al. Deficits in
eye gaze during negative socialinteractions in patients with
schizophrenia. J Nerv Ment Dis 2010;198:829–35.
Cohen AS, Saperstein AM, Gold JM, Kirkpatrick B, Carpenter Jr
WT, Buchanan RW. Neuro-psychology of the deficit syndrome: new data
and meta-analysis of findings to date.Schizophr Bull
2007;33:1201–12.
Corrigan PW, Nelson DR. Factors that affect social cue
recognition in schizophrenia.Psychiatry Res 1998;78:189–96.
Corrigan PW, Garman A, Nelson D. Situational feature recognition
in schizophrenic outpa-tients. Psychiatry Res 1996;62:251–7.
Csukly G, Polgár P, Tombor L, Benkovits J, Réthelyi J. Theory of
mind impairments inpatients with deficit schizophrenia. Compr
Psychiatry 2014;55:349–56.
Ebisch SJ, Salone A, Ferri F, De Berardis D, Romani GL, Ferro
FM, et al. Out of touch withreality? Social perception in
first-episode schizophrenia. Soc Cogn Affect
Neurosci2013;8:394–403.
First MB, Gibbon M, Spitzer RL, Williams JBW. Structured
clinical interview for DSM-IVaxis I disorders. New York:
Psychiatric Institute Biometric Research; 1996.
Fischer BA, Keller WR, Arango C, Pearlson GD, McMahon RP, Meyer
WA, et al. Corticalstructural abnormalities in deficit versus
nondeficit schizophrenia. Schizophr Res2012;136:51–4.
Franck N, Montoute T, Labruyere N, Tiberghien G, Marie-Cardine
M, Daléry J, et al. Gazedirection determination in schizophrenia.
Schizophr Res 2002;56:225–34.
Frith CD, Frith U. Interacting minds—a biological basis. Science
1999;286:1692–5.Green MJ, Phillips ML. Social threat perception and
the evolution of paranoia. Neurosci
Biobehav Rev 2004;28:333–42.Green MF, Penn DL, Bentall R,
Carpenter WT, Gaebel W, Gur RC, et al. Social cognition in
schizophrenia: an NIMHworkshop on definitions, assessment, and
research opportu-nities. Schizophr Bull 2008;34:1211–20.
Gu BM, Park JY, Kang DH, Lee SJ, Yoo SY, Jo HJ, et al. Neural
correlates of cognitive inflex-ibility during task-switching in
obsessive-compulsive disorder. Brain 2008;131:155–64.
Han K, Ku J, Kim K, Jang HJ, Park J, Kim JJ, et al. Virtual
reality prototype for measurementof expression characteristics in
emotional situations. Comput Biol Med 2009;39:173–9.
Han K, Kim IY, Kim JJ. Assessment of cognitive flexibility in
real life using virtual reality: acomparison of healthy individuals
and schizophrenia patients. Comput Biol Med2012;42:841–7.
Harrow M, Adler D, Hanf E. Abstract and concrete thinking in
schizophrenia during theprechronic phases. Arch Gen Psychiatry
1974;31:27–33.
Hooker C, Park S. Emotion processing and its relationship to
social functioning in schizo-phrenia patients. Psychiatry Res
2002;112:41–50.
Hunter R, Barry S. Negative symptoms and psychosocial
functioning in schizophrenia:neglected but important targets for
treatment. Eur Psychiatry 2012;27:432–6.
Kanwisher N, McDermott J, Chun MM. The fusiform face area: a
module in humanextrastriate cortex specialized for face perception.
J Neurosci 1997;17:4302–11.
Kay SR, Fiszbein A, Opler LA. The positive and negative syndrome
scale (PANSS) forschizophrenia. Schizophr Bull 1987;13:261–76.
Kim K, Kim JJ, Kim J, Park DE, Jang HJ, Ku J, et al.
Characteristics of social perceptionassessed in schizophrenia using
virtual reality. Cyberpsychol Behav 2007;10:215–9.
Kim SI, Ku J, Han K, Lee H, Park J, Kim JJ, et al. Virtual
reality applications for patients withschizophrenia. J Cyberther
Rehab 2008;1:101–12.
Kim C, Johnson NF, Cilles SE, Gold BT. Common and distinct
mechanisms of cognitiveflexibility in prefrontal cortex. J Neurosci
2011a;31:4771–9.
Kim J, Park S, Blake R. Perception of biological motion in
schizophrenia and healthyindividuals: a behavioral and FMRI study.
PLoS One 2011b;6:e19971.
Kramer UM, Mohammadi B, Donamayor N, Sami A, Munte TF. Emotional
and cognitiveaspects of empathy and their relation to social
cognition - an fMRI study. Brain Res2010;1311:110–20.
Lahnakoski JM, Glerean E, Salmi J, Jaaskelainen I, Sams M, Hari
R, et al. Naturalistic fMRImapping reveals superior temporal sulcus
as the hub for the distributed brainnetwork for social perception.
Front Hum Neurosci 2012;6:233.
Lee H, Ku J, Kim J, Jang DP, Yoon KJ, Kim SI, et al. Aberrant
neural responses to socialrejection in patients with schizophrenia.
Soc Neurosci 2014;9:412–23.
Liu X, Banich MT, Jacobson BL, Tanabe JL. Common and distinct
neural substrates ofattentional control in an integrated Simon and
spatial Stroop task as assessed byevent-related fMRI. Neuroimage
2004;22:1097–106.
MacDonald 3rd AW, Cohen JD, Stenger VA, Carter CS. Dissociating
the role of the dorsolat-eral prefrontal and anterior cingulate
cortex in cognitive control. Science 2000;288:1835–8.
Mancuso F, HoranWP, Kern RS, GreenMF. Social cognition in
psychosis: multidimension-al structure, clinical correlates, and
relationship with functional outcome. SchizophrRes
2011;125:143–51.
Marwick K, Hall J. Social cognition in schizophrenia: a review
of face processing. Br MedBull 2008;88:43–58.
Mazaika PK,Whitfield S, Cooper JC. Detection and repair of
transient artifacts in fMRI data.Neuroimage 2005;26:S36.
Norman J. Two visual systems and two theories of perception: an
attempt to reconcile theconstructivist and ecological approaches.
Behav Brain Sci 2002;25:73–96.
Norris CJ, Chen EE, Zhu DC, Small SL, Cacioppo JT. The
interaction of social and emotionalprocesses in the brain. J Cogn
Neurosci 2004;16:1818–29.
Ochsner KN, Knierim K, Ludlow DH, Hanelin J, Ramachandran T,
Glover G, et al. Reflectingupon feelings: an fMRI study of neural
systems supporting the attribution of emotionto self and other. J
Cogn Neurosci 2004;16:1746–72.
Olfson M, Ascher-Svanum H, Faries DE, Marcus SC. Predicting
psychiatric hospital admis-sion among adults with schizophrenia.
Psychiatr Serv 2011;62:1138–45.
Park KM, Kim JJ, Ku J, Kim SY, Lee HR, Kim SI, et al. Neural
basis of attributional style inschizophrenia. Neurosci Lett
2009;459:35–40.
Pelphrey KA, Morris JP, McCarthy G. Grasping the intentions of
others: the perceivedintentionality of an action influences
activity in the superior temporal sulcus duringsocial perception. J
Cogn Neurosci 2004;16:1706–16.
Penn DL, Ritchie M, Francis J, Combs D, Martin J. Social
perception in schizophrenia: therole of context. Psychiatry Res
2002;109:149–59.
Piskulic D, Addington J. Social cognition and negative symptoms
in psychosis. PsychiatryRes 2011;188:283–5.
Potkin SG, Alva G, Fleming K, Anand R, Keator D, Carreon D, et
al. A PET study of the path-ophysiology of negative symptoms in
schizophrenia. Positron emission tomography.Am J Psychiatry
2002;159:227–37.
Puce A, Allison T, Bentin S, Gore JC, McCarthy G. Temporal
cortex activation in humansviewing eye and mouth movements. J
Neurosci 1998;18:2188–99.
Quintana J, Wong T, Ortiz-Portillo E, Marder SR, Mazziotta JC.
Right lateral fusiform gyrusdysfunction during facial information
processing in schizophrenia. Biol Psychiatry2003;53:1099–112.
Raven J. Standard progressive matrices: sets A, B, C. D & E:
Oxford Psychologists Press;1990.
Spencer JM, Sekuler AB, Bennett PJ, Christensen BK. Contribution
of coherent motion tothe perception of biological motion among
personswith Schizophrenia. Front Psychol2013;4:507.
Straube B, Green A, Sass K, Kircher T. Superior temporal sulcus
disconnectivity duringprocessing of metaphoric gestures in
schizophrenia. Schizophr Bull 2014;40:936–44.
Strauss JS, Carpenter Jr WT. The prediction of outcome in
schizophrenia. I. Characteristicsof outcome. Arch Gen Psychiatry
1972;27:739–46.
Szycik GR, Munte TF, Dillo W, Mohammadi B, Samii A, Emrich HM,
et al. Audiovisualintegration of speech is disturbed in
schizophrenia: an fMRI study. Schizophr Res2009;110:111–8.
Thakkar KN, Peterman JS, Park S. Altered brain activation during
action imitation and ob-servation in schizophrenia: a translational
approach to investigating social dysfunc-tion in schizophrenia. Am
J Psychiatry 2014;171:539–48.
Tso IF, Mui ML, Taylor SF, Deldin PJ. Eye-contact perception in
schizophrenia: relationshipwith symptoms and socioemotional
functioning. J Abnorm Psychol 2012;121:616–27.
http://dx.doi.org/10.1016/j.pnpbp.2014.12.006http://dx.doi.org/10.1016/j.pnpbp.2014.12.006http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0005http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0005http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0005http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0010http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0010http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0010http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0015http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0015http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0015http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0020http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0020http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0025http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0025http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0025http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0030http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0030http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0035http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0035http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0040http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0040http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0040http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0045http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0045http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0050http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0050http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0055http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0055http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0055http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0065http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0065http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0060http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0060http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0070http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0070http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0075http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0075http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0075http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0080http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0080http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0085http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0085http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0085http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0090http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0090http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0095http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0105http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0105http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0100http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0100http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0100http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0110http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0110http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0110http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0115http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0115http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0115http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0120http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0120http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0120http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0125http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0125http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0130http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0130http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0135http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0135http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0140http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0140http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0145http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0145http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0160http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0160http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0165http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0165http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0150http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0150http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0155http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0155http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0170http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0170http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0170http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0175http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0175http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0175http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0180http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0180http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0185http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0185http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0185http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0190http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0190http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0190http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0195http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0195http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0195http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0200http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0200http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0205http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0205http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0210http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0210http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0215http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0215http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0220http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0220http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0220http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0225http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0225http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0230http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0230http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0235http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0235http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0235http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0240http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0240http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0245http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0245http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0250http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0250http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0250http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0255http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0255http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0260http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0260http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0260http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0265http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0265http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0270http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0270http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0270http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0275http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0275http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0280http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0280http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0285http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0285http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0285http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0290http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0290http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0290http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0295http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0295http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0295
-
88 J.E. Shin et al. / Progress in Neuro-Psychopharmacology &
Biological Psychiatry 58 (2015) 81–88
Voineskos AN, Foussias G, Lerch J, Felsky D, Remington G, Rajji
TK, et al. Neuroimagingevidence for the deficit subtype of
schizophrenia. JAMA Psychiatry 2013;70:472–80.
Volpe U,Mucci A, Quarantelli M, Galderisi S, MajM. Dorsolateral
prefrontal cortex volumein patients with deficit or nondeficit
schizophrenia. Prog Neuropsychopharmacol BiolPsychiatry
2012;37:264–9.
Walter H, Ciaramidaro A, Adenzato M, Vasic N, Ardito RB, Erk S,
et al. Dysfunction of thesocial brain in schizophrenia is modulated
by intention type: an fMRI study. Soc CognAffect Neurosci
2009;4:166–76.
Weinberg D, Shahar G, Davidson L, McGlashan TH, Fennig S.
Longitudinal associationsbetween negative symptoms and social
functioning in schizophrenia: themoderatingrole of employment
status and setting. Psychiatry 2009;72:370–81.
Weissman DH, Perkins AS, Woldorff MG. Cognitive control in
social situations: a role forthe dorsolateral prefrontal cortex.
Neuroimage 2008;40:955–62.
Wicker B, Fonlupt P, Hubert B, Tardif C, Gepner B, Deruelle C.
Abnormal cerebral effectiveconnectivity during explicit emotional
processing in adults with autism spectrumdisorder. Soc Cogn Affect
Neurosci 2008;3:135–43.
Wolkin A, Sanfilipo M, Wolf AP, Angrist B, Brodie JD, Rotrosen
J. Negative symptoms andhypofrontality in chronic schizophrenia.
Arch Gen Psychiatry 1992;49:959–65.
Wyk BC, Hudac CM, Carter EJ, Sobel DM, Pelphrey KA. Action
understanding in thesuperior temporal sulcus region. Psychol Sci
2009;20:771–7.
http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0300http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0300http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0305http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0305http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0305http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0310http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0310http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0310http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0315http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0315http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0315http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0320http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0320http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0325http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0325http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0325http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0330http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0330http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0335http://refhub.elsevier.com/S0278-5846(14)00243-7/rf0335
Involvement of the dorsolateral prefrontal cortex and superior
temporal sulcus in impaired social perception in schizophrenia1.
Introduction2. Methods2.1. Participants and clinical
measurements2.2. Experimental design2.3. MRI acquisition and
analysis2.4. Statistical analysis of the behavioral data
3. Results3.1. Participants' characteristics and behavioral
performances3.2. Imaging findings
4. DiscussionContributorsAcknowledgmentsReferences