-
1
PROgesterone Therapy for Endometrial Cancer prevention in obese
women
(PROTEC) trial: a feasibility study
Abigail E. Derbyshire1, Jennifer L. Allen2, Matthew Gittins3,
Bhavna Lakhiani2, James Bolton4, Joseph
Shaw4, Philip W. Pemberton5, Michelle Needham6, Michelle L.
MacKintosh1, Richard J. Edmondson1,2,
Henry C. Kitchener2, Emma J. Crosbie1,2
1-Division of Gynaecology, Manchester University NHS Foundation
Trust, Manchester Academic Health
Science Centre, Manchester, UK
2-Division of Cancer Sciences, Faculty of Biology, Medicine and
Health, University of Manchester, St
Mary's Hospital, Manchester, M13 9WL, UK
3-Centre for Biostatistics, School of Health Sciences,
University of Manchester, Manchester Academic
Health Science Centre, Manchester, UK
4-Department of Histopathology, Manchester University NHS
Foundation Trust, Manchester Academic
Health Science Centre, Manchester, UK
5-Department of Clinical Biochemistry, Manchester University NHS
Foundation Trust, Manchester
Academic Health Science Centre, Manchester, UK
6-Sleep Apnoea Service, Salford Royal Hospitals NHS Foundation
Trust, Salford, UK
Running title: PROgesterone Therapy for Endometrial Cancer
prevention
Keywords: Endometrial cancer; obesity; levonorgestrel
intrauterine system (LNG-IUS);
chemoprevention; feasibility trial
Correspondence to: Professor Emma Crosbie, Division of Cancer
Sciences, University of Manchester,
School of Medical Sciences, Faculty of Biology, Medicine and
Health, 5th Floor Research, St Mary’s
Hospital, Oxford Road, Manchester M13 9PL. Email:
[email protected]. Phone. +44
(161) 701 6942.
Conflicts of interest: The authors declare no potential
conflicts of interest.
Cancer Research. on July 7, 2021. © 2020 American Association
forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for
publication but have not yet been edited. Author Manuscript
Published OnlineFirst on September 30, 2020; DOI:
10.1158/1940-6207.CAPR-20-0248
mailto:[email protected]://cancerpreventionresearch.aacrjournals.org/
-
2
Abstract
Obesity is the major aetiological driver for endometrial cancer.
The levonorgestrel intrauterine system
(LNG-IUS) reduces the risk of endometrial cancer and its
precursor, atypical hyperplasia. We assessed
feasibility and uptake of the LNG-IUS for primary prevention of
endometrial cancer in high-risk women
and its impact on endometrial tissue biomarkers. Women with
class-III obesity (BMI>40kg/m2) and
histologically normal endometrium were invited to participate in
a clinical trial of the LNG-IUS for
endometrial protection. Recruitment, successful LNG-IUS
insertion and adherence to trial procedures
were recorded. We measured impact of the LNG-IUS on circulating
biomarkers of endometrial cancer
risk, endometrial proliferation (Ki-67, pAKT, PTEN), endometrial
hormone receptor status (ER, PR),
mental wellbeing and menstrual function. At six months, women
chose to keep their LNG-IUS or have
it removed. In total, 103 women were approached, 54 were offered
a participant information sheet, 35
agreed to participate and 25 received a LNG-IUS. Their median
age and BMI were 54 years (IQR 52,57)
and 47kg/m2 (IQR 44,51) respectively. Three women (3/35, 9%)
were ineligible due to atypical
hyperplasia/endometrial cancer on their baseline biopsy. The
LNG-IUS was well tolerated and had a
positive overall effect on bleeding patterns and mental
wellbeing. The LNG-IUS was associated with
endometrial morphological change, reduced Ki-67 and PR
expression but circulating biomarkers of
endometrial cancer risk were unchanged. All but one woman (96%)
kept her LNG-IUS. The LNG-IUS
appears to be acceptable to some women with class-III obesity
for primary prevention of endometrial
cancer, which could provide a strategy for a prevention
trial.
Cancer Research. on July 7, 2021. © 2020 American Association
forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for
publication but have not yet been edited. Author Manuscript
Published OnlineFirst on September 30, 2020; DOI:
10.1158/1940-6207.CAPR-20-0248
http://cancerpreventionresearch.aacrjournals.org/
-
3
Introduction
Endometrial cancer is the sixth most common cancer in women,
with more than 382,000 new
diagnoses and 89,900 deaths recorded globally in 2018 [1]. The
incidence of endometrial cancer is
rising sharply in parallel with escalating obesity rates [2].
Obesity is the strongest risk factor for the
most common histological subtype, endometrioid (type I)
endometrial cancer and its precursor lesion,
atypical hyperplasia [3]. Such is the strength of the
association that approximately 40% of endometrial
cancers are thought to be directly attributable to obesity [4],
and a marked dose-response relationship
bestows higher risk as body mass index (BMI) rises [5]. It has
been estimated that women with obesity
class III (BMI>40kg/m2) have a seven-fold increased risk of
endometrial cancer compared with normal
weight women (BMI 18.5-25kg/m2)[3]. The biological mechanism
responsible for this association
relates to the endometrial stimulatory effect of adipose-derived
estrogen, which is unopposed by
progesterone in anovulatory and postmenopausal women, and
augmented by the negative
consequences of insulin resistance and chronic inflammation [6].
Weight loss achieved and sustained
through bariatric surgery reduces endometrial cancer risk [7,8]
with measurable impact on circulating
biomarkers of adiposity, reproductive hormones and insulin
status, accompanied by down-regulation
of pro-oncogenic signalling pathways in the endometrium [9].
Bariatric surgery is neither available,
appropriate nor acceptable to everyone with an elevated BMI
however, and cannot be recommended
solely for the purpose of primary prevention of endometrial
cancer [10]. Dietary caloric restriction can
facilitate weight loss, particularly if accompanied by increased
levels of physical activity, but the
amount of weight lost and duration of benefit is considerably
lower than following bariatric surgery
[11]. Alternative strategies are therefore urgently needed to
provide protection to women at greatest
risk of endometrial cancer in order to thwart the explosion in
incidence rates predicted by modelling
studies [12,13].
The levonorgestrel intrauterine system (LNG-IUS) delivers
progestin directly to the endometrium,
counteracting the stimulatory effect of estrogen through stromal
decidualisation, down-regulation of
proliferative signalling pathways and glandular atrophy [14].
Epidemiological studies have shown ever-
users of the LNG-IUS have a reduced risk of endometrial cancer
[15,16] and several meta-analyses
have demonstrated its effectiveness as a therapeutic agent for
women with atypical hyperplasia and
low grade cancers confined to the endometrium [17-19]. Despite
strong evidence for its anti-cancer
activity, no previous studies have investigated use of the
LNG-IUS as a chemopreventive agent for the
primary prevention of obesity-driven endometrial cancer. It is
not known whether women with a
raised BMI are aware of their increased risk of endometrial
cancer or whether they would be prepared
to engage in risk reduction with a LNG-IUS. In preparation for a
clinical efficacy study, we measured
feasibility, participation rate and compliance with the LNG-IUS
for endometrial protection in women
Cancer Research. on July 7, 2021. © 2020 American Association
forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for
publication but have not yet been edited. Author Manuscript
Published OnlineFirst on September 30, 2020; DOI:
10.1158/1940-6207.CAPR-20-0248
http://cancerpreventionresearch.aacrjournals.org/
-
4
with class III obesity. We studied its short-term effects on
endometrial morphology, proliferation and
hormone receptor status and on circulating biomarkers of
endometrial cancer risk. Further, we
explored the impact of the LNG-IUS on menstrual bleeding
patterns, as well as mental wellbeing,
through validated questionnaires.
Materials and methods
Study governance
The study was sponsored by Manchester University NHS Foundation
Trust (MFT) and approved by the
Cambridge East Research Ethics Committee – (15/EE/0063),
Medicine and Healthcare Products
Regulatory Authority (MHRA, reference 21387/0234/001-0001) and
local Research and Development
departments. The trial was prospectively registered on the
European (EudraCT number 2014-005610-
37) and UK (ISRCTN40940943) clinical trial databases and
conducted in accordance with Good Clinical
Practice guidelines and the Declaration of Helsinki.
Study design
This was a single arm feasibility study of the LNG-IUS for
endometrial protection in women with class
III obesity. Women attended clinic at baseline (screening visit,
T0), 2 ±1 months (LNG-IUS inserted in
clinic, T1) and 8 ±3 months (final assessment, T2)(Figure 1).
Serial assessment of anthropometric
measures (weight, BMI, waist:hip ratio), serum biomarkers
(hormone status, insulin resistance,
adiposity), endometrial biomarkers (endometrial morphology,
hormone receptor status, Ki-67
proliferation index, pro-proliferation signalling molecules),
menstrual bleeding patterns and mental
wellbeing was performed at all time points.
Feasibility, willingness to receive and compliance with the
LNG-IUS
Willingness to receive the LNG-IUS for endometrial protection
was determined as the proportion of
eligible women who agreed to its insertion. The feasibility of
using the LNG-IUS in women with class III
obesity was calculated as the proportion of successful LNG-IUS
insertions. Complications of insertion,
side effects and adverse events were recorded. At T2 final
visit, women chose whether to keep their
LNG-IUS for ongoing endometrial protection or have it removed.
Adherence with repeated
endometrial sampling and other trial procedures was recorded.
Compliance with the LNG-IUS was
calculated as the proportion of women who chose to keep their
LNG-IUS.
Participants
Cancer Research. on July 7, 2021. © 2020 American Association
forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for
publication but have not yet been edited. Author Manuscript
Published OnlineFirst on September 30, 2020; DOI:
10.1158/1940-6207.CAPR-20-0248
http://cancerpreventionresearch.aacrjournals.org/
-
5
Eligible women were ≥18 years of age with a BMI ≥40kg/m2 and
histologically normal endometrium at
baseline. All participants gave written, informed consent. We
advertised the study on the University of
Manchester and MFT websites, Cancer Research UK and UK ISRCTN
clinical trials databases, on social
media platforms and by word of mouth. We recruited women who
approached the research team for
participation directly and those attending gynaecology and sleep
apnoea outpatient clinics at MFT and
Salford Royal Hospitals NHS Foundation Trust, respectively.
Exclusion criteria included previous
hysterectomy; LNG-IUS or other intrauterine device within the
past 6 months; planning pregnancy,
pregnant or breast feeding; previous endometrial ablation;
congenital or acquired uterine anomaly;
history of pelvic inflammatory disease or genital actinomyces;
breast cancer; overdue cervical
screening or last screen abnormal; immunodeficiency; actively
trying to lose weight; contraindications
to LNG-IUS, including coagulopathy, liver disease, migraine,
raised blood pressure, arterial disease,
postpartum endometritis, infected abortion during the past three
months or recent trophoblastic
disease with persistently elevated hCG levels; and inability to
tolerate endometrial sampling/ LNG-IUS
insertion as an outpatient.
Medical history and baseline safety check
At baseline, we recorded last menstrual period (LMP), menstrual
bleeding pattern and contraceptive
use. Postmenopausal status was defined as LMP occurring >1
year before if FSH, LH and oestradiol
levels were confirmatory; the remaining participants were
considered premenopausal. A urinary
pregnancy test was performed if indicated. Cervical screening
was offered in accordance with the
National Health Service Cervical Screening programme. High
vaginal and endocervical swabs were
taken to exclude active lower genital tract infection. Medical
history was documented. Screening
bloods, including full blood count, urea and electrolytes and
liver function tests were taken to confirm
medical fitness for participation in the trial.
LNG-IUS insertion
The Mirena® LNG-IUS (Bayer plc, Berkshire UK) was inserted in
clinic at T1; women were advised to
take paracetamol and non-steroidal anti-inflammatory drugs one
hour before insertion, if not
contraindicated. The procedure was carried out on a colposcopy
couch using a Winterton speculum
under aseptic conditions, according to the manufacturer’s
instructions. Safety monitoring was by
telephone call at 6, 12 and 18 weeks following LNG-IUS
insertion. Side effects, adverse events and
complications were recorded. Participants were advised to attend
their General Practitioner for a coil
thread check 4 weeks after LNG-IUS insertion.
Anthropometric measurements
Cancer Research. on July 7, 2021. © 2020 American Association
forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for
publication but have not yet been edited. Author Manuscript
Published OnlineFirst on September 30, 2020; DOI:
10.1158/1940-6207.CAPR-20-0248
http://cancerpreventionresearch.aacrjournals.org/
-
6
Height was measured using a stadiometer with shoes removed.
Weight was measured using electronic
scales following removal of bulky clothing and BMI derived using
the formula kg/m2. Waist to hip ratio
was calculated from waist (midpoint between lower margin of last
palpable rib and top of the iliac
crest measured with a tape measure) and hip circumference
(widest portion of the buttocks).
Blood biomarkers
Serum obtained by venepuncture following a 6 hour fast was used
to measure a) reproductive function
(luteinizing hormone, LH; follicle stimulating hormone, FSH; sex
hormone binding globulin, SHBG;
testosterone; free androgen index, FAI; oestradiol;
progesterone), b) insulin resistance (glucose and
insulin to derive Homeostasis Model Assessment: Insulin
Resistance, HOMA-IR [20]; glycosylated
haemoglobin A1c, HbA1c), c) adiposity (adiponectin, leptin) and
d) inflammation (C-reactive protein,
CRP). With the exception of adiponectin and leptin, all analytes
were measured using automated
routine clinical service protocols in the MFT Clinical
Biochemistry Laboratory. Adiponectin and leptin
were measured with a DuoSet ELISA development kit (R&D
Systems, Abingdon, UK).
Endometrial histopathology and tissue biomarkers
Endometrial sampling was performed using a Pipelle© (Carefusion,
UK) or MedGyn Endosampler©
(MedGyn, IL, USA). Premenopausal participants were sampled on
day 12 ±2 of the menstrual cycle,
where possible. Endometrial tissue was formalin-fixed, paraffin
embedded, sectioned and stained with
haematoxylin and eosin. Endometrial morphology was assessed by a
consultant gynaecological
pathologist. In premenopausal participants, endometrial
morphology and reproductive hormone profile
was used alongside LMP to determine menstrual cycle phase.
Abnormalities were confirmed by a
second consultant gynaecological pathologist and classified
according to WHO guidelines [21,22].
Tissue sections (4 µm) were baked for 30 minutes at 70°C. The
automated Ventana BenchMark Ultra
IHC Staining Module (Ventana Co., Tucson, AZ, USA) was used with
the Ultraview 3, 3’
diaminobenzidine (DAB) v3 detection system (Ventana Co.). Tissue
sections were deparaffinised and
incubated in EZPrep Volume Adjust (Ventana Co.). A heat-induced
antigen retrieval protocol was
carried out using a TRIS–ethylenediamine tetracetic acid
(EDTA)–boric acid pH 8 buffer, Cell Conditioner
1(CC1). The sections were incubated with ultraviolet inhibitor
blocking solution for 4 min, followed by
an optimized concentration of antibody (Table S1). Sections were
then incubated with horseradish
peroxidase-linked secondary antibody, DAB chromogen and copper.
Counterstain (Haematoxylin II) was
applied for 12 minutes before a 4-minute incubation with bluing
reagent. Slides were dehydrated
through three steps of 99% IMS and two changes of Xylene.
Sections were coverslipped using ClearVue
Cancer Research. on July 7, 2021. © 2020 American Association
forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for
publication but have not yet been edited. Author Manuscript
Published OnlineFirst on September 30, 2020; DOI:
10.1158/1940-6207.CAPR-20-0248
http://cancerpreventionresearch.aacrjournals.org/
-
7
Mount XYL (Thermo Scientific). Negative (isotype control) and
positive tissue controls were used for
quality assurance.
The Ki-67 score was the proportion of glandular cells with
positive nuclear staining. The Ki-67 score was
determined from >1000 nuclei scored in 3 representative
high-powered fields (x20), chosen by the
study pathologists; scanty samples were scored in their entirety
[23]. Estrogen (ER) and progesterone
receptor (PR) staining was assessed by modified H-score (0-18),
the product of area score (proportion
of positively stained tissue, scored 0-6) and intensity of
staining score (0=none, 1=mild, 2=moderate,
3=strong). Phosphorylated (p)AKT staining was scored using the
percentage of positively stained tissue
[H = (3 x % strong staining) + (2 x % moderate staining) + (%
weak staining)] to account for within tissue
heterogeneity (0-300). PTEN status was scored ‘PTEN null’ if
there were endometrial glands negative
for PTEN adjacent to positive stroma. Slides were scored as
‘PTEN positive’ if all endometrial glands
expressed PTEN [24]. Scoring was performed manually by two
independent scorers who were blinded
to time point. Discrepant scores (>10% or disagreement as to
PTEN status) were reviewed and resolved
by consensus agreement.
Menstrual blood loss and mental wellbeing assessment
Two validated questionnaires, the Hospital Anxiety and
Depression Scale (HADS) [25, 26] and Warwick-
Edinburgh Mental Wellbeing Scale (WEMWBS) [27,28], were
completed at baseline and follow up to
determine whether the LNG-IUS had an impact on mental wellbeing.
For the HADS, different cut-offs
are indicative of a mental health disorder, depending on
clinical context [26], but lower scores indicate
absent or lower severity of symptoms. For the WEMWBS, the mean
score in the general population is
51, with higher scores reflecting improved mental wellbeing
[27]. Premenopausal participants
completed the Menstrual Bleeding Questionnaire [29] at baseline
and follow up.
Sample size considerations
This was a preliminary study designed to inform recruitment
rates, feasibility of and likely adherence to
a clinical efficacy trial of the LNG-IUS for endometrial
protection in women with class III obesity. We
considered that a clinical efficacy trial could be successfully
conducted if >50% of eligible women
agreed to participation, >50% of those eligible had a LNG-IUS
successfully fitted, and >75% of women
kept their LNG-IUS for >6 months. We also measured
LNG-IUS-induced change in circulating and tissue
biomarkers to inform intermediary biomarker endpoints for our
definitive study. We did not perform a
formal sample size calculation and planned the pragmatic
recruitment of 30-40 women over a six to
twelve month recruitment period.
Statistical analysis
Cancer Research. on July 7, 2021. © 2020 American Association
forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for
publication but have not yet been edited. Author Manuscript
Published OnlineFirst on September 30, 2020; DOI:
10.1158/1940-6207.CAPR-20-0248
http://cancerpreventionresearch.aacrjournals.org/
-
8
Statistical analyses were performed using Graphpad Prism 5.0b
for Mac (GraphPad Software, San
Diego, USA) and SPSS 23.0 for Mac (IBM Corp, Armonk, NY, USA).
Descriptive statistics included mean
and standard deviation (SD) for normally distributed, and median
and interquartile range (IQR), for
non-normally distributed data. Within-individual changes over
time were compared using paired t-test
and Wilcoxon signed-rank test for normally distributed and
non-normally distributed data, respectively.
To assess the short-term impact of the LNG-IUS on endometrial
proliferation, a mixed effects
regression model was fitted, with Ki-67 score set as the
dependent variable, time point (baseline set as
reference category) as the predictor of interest and the
covariates baseline Ki-67 score, age,
menopausal status (pre/post), smoking (never, ever, current),
type II diabetes mellitus (yes/no)
baseline BMI, and baseline waist:hip ratio. A further analysis
was performed that included weight at
follow up, to determine if change in weight was responsible for
change in Ki-67 at outcome. To account
for repeated measures within participants, a random effect
intercept was included to account for the
within subject vs between subject variation. To account for
possible departures in normality, a cluster
bootstrapping procedure was employed with 1000 replications. In
an effort to emphasise clinically over
statistically important effects, data are reported in terms of
mean difference effect estimates and 95%
confidence intervals.
Results
Study population
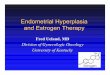
Between October 2015 and September 2016, 103 women were
approached, 54 were offered a
participant information sheet, 35 agreed to participate and 25
received a LNG-IUS (Figure 1). Forty nine
women (48%) were ineligible to receive the participant
information sheet for the following reasons:
LNG-IUS in situ (n=13); previous hysterectomy (n=12); pending
bariatric surgery (n=10); social/ capacity
reasons (n=7); LNG-IUS contraindicated (n=4) or BMI
-
9
46kg/m2) or ethnicity/ race (all except three were White
British). Twelve (48%) were premenopausal
but just 4 had regular menstrual cycles; most were either
amenorrhoeic (5/12) or experienced irregular
menstrual bleeding (3/12). Four (16%) were using hormone
replacement therapy (3/25, 12%) or oral
contraceptives (1/25, 4%) at baseline, which they continued
throughout the trial. All had at least one
comorbidity, most commonly type II diabetes (10/25, 40%),
hypertension (15/25, 60%) or asthma
(8/25, 32%) and 48% had more than three comorbidities.
Compliance with intervention and study procedures
All 25 women received the LNG-IUS in clinic without
complication. There were no insertion failures,
expulsions, uterine perforations or lost devices. One woman (4%)
developed mild symptoms of
endometritis following LNG-IUS insertion, which was treated with
oral antibiotics. One patient
complained of pelvic discomfort/ mild pain following LNG-IUS
insertion that settled with oral analgesia.
Other adverse and serious adverse events, specifically urinary
tract infection (1/25, 4%), vasculitis
(1/25, 4%), sciatica (1/25, 4%) and attempted suicide (1/25, 4%)
were not thought to be related to the
LNG-IUS. All women kept their LNG-IUS until their final
assessment when one woman (4%) chose to
have it removed (“easier now than later”); the remaining 24
women (96%) kept their LNG-IUS for
ongoing endometrial protection. All 25 women were compliant with
study procedures, including
sequential endometrial biopsies (all 3 biopsies taken,
25/25).
Endometrial morphology and biomarkers
Three of 35 participants (9%) had an incidental finding of
atypical hyperplasia or endometrial cancer on
a pre-LNG-IUS biopsy and were excluded from the study. All other
women had histologically normal
endometrium at T0 (baseline) and T1 (time of LNG-IUS insertion).
Many of the samples were scanty.
Morphology was consistent with menopausal status and/or reported
phase of menstrual cycle, as
appropriate. At follow up (T2), all endometrial biopsies showed
stromal decidualisation and glandular
atrophy, consistent with the progesterone effect associated with
LNG-IUS treatment.
The LNG-IUS was associated with a significant decrease in
endometrial proliferation as assessed by Ki-
67 score. The mean Ki-67 score was 27.1% (SD 23.4) at baseline,
21.8% (SD 14.8) at the time of LNG-IUS
insertion and 12.7% (SD 10.9) at follow up. A mixed effects
regression model adjusting for within
participant clustering, potential confounders, and weight change
between time points is shown in
Table 2. Between baseline (T0) and time of LNG-IUS insertion
(T1) and between baseline (T0) and
follow up (T2) the change in Ki-67 score was -5.4% (95% CI
-17.1%, 6.3%) and -14.6% (-25.3%, -3.9%),
respectively. These results were consistent across all three
models, indicating that potential sources of
confounding, including change in weight during follow up, had
little effect on Ki-67 score. Progesterone
Cancer Research. on July 7, 2021. © 2020 American Association
forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for
publication but have not yet been edited. Author Manuscript
Published OnlineFirst on September 30, 2020; DOI:
10.1158/1940-6207.CAPR-20-0248
http://cancerpreventionresearch.aacrjournals.org/
-
10
receptor expression decreased with LNG-IUS treatment (Table 3).
There was no significant change in
expression of the other endometrial biomarkers, estrogen
receptor, PTEN or pAKT. Interestingly, all
three women excluded because of occult endometrial abnormalities
had PTEN null glands and a further
2/25 participants in the study had PTEN null glands before but
not after LNG-IUS insertion.
Anthropometric and circulating biomarkers of endometrial cancer
risk
Overall, women lost weight during the trial, although this was
not clinically significant (median weight
124.4kg (IQR 111, 143), 123.9kg (IQR 111, 142) and 123kg (IQR
111, 144) at T0, T1 and T2, respectively).
There were no clinically significant changes in circulating
biomarkers of reproductive function, insulin
resistance, adiposity or inflammation across the three time
points (Table 3), with the notable exception
of altered serum FSH, LH and progesterone levels over time,
which likely reflect natural reproductive
ageing in our peri-menopausal cohort.
Menstrual bleeding and mental wellbeing
Of the 12 premenopausal participants, 5 (42%) were amenorrhoeic,
4 (33%) had regular and 3 (25%)
irregular menstrual bleeding at baseline. As expected, the 7
women who experienced menstrual
bleeding reported a significant reduction in blood loss with the
LNG-IUS; all but two became
amenorrhoeic according to the Menstrual Bleeding Questionnaire.
Mental wellbeing improved with
the LNG-IUS according to both the WEMWBS and HADS scales (Table
4). A change in score of 2-3
points is clinically significant, but did not reach statistical
significance, most likely because of small
numbers.
Discussion
The PROTEC trial was undertaken to assess the feasibility of a
future clinical efficacy trial of the LNG-
IUS for endometrial protection in women with class III obesity.
In a twelve-month recruitment period,
we approached 103 women, 54 (52%) of whom met the inclusion
criteria, 35 (65%) agreed to
participate and 25 (71%) proceeded to LNG-IUS insertion. There
were no insertion failures and all
women were fully compliant with all study procedures, including
an endometrial biopsy at the final
visit. There were no related serious adverse events but one case
each of endometritis and post-
insertion pain, both recognised complications of LNG-IUS
treatment. We observed no detrimental
impact of the LNG-IUS on mental wellbeing and self-reported
menstrual bleeding profiles improved for
our premenopausal participants. These data suggest that women at
greatest risk of obesity-driven
endometrial cancer are willing to engage in risk reduction with
a LNG-IUS and that a clinical efficacy
trial could be feasible. Roughly a quarter of women approached
for the trial had a LNG-IUS inserted,
Cancer Research. on July 7, 2021. © 2020 American Association
forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for
publication but have not yet been edited. Author Manuscript
Published OnlineFirst on September 30, 2020; DOI:
10.1158/1940-6207.CAPR-20-0248
http://cancerpreventionresearch.aacrjournals.org/
-
11
indicating a relatively high proportion of screen failures and
non-continuation rate. These findings
must be factored in to the design of a clinical efficacy
trial.
To determine the short-term impact of the LNG-IUS on biomarkers
of endometrial cancer risk, we
measured change in anthropometric variables, reproductive
hormones, insulin resistance, endometrial
morphology and glandular proliferation status between baseline,
two months and eight months. As
predicted, we observed stability in these biomarkers prior to
LNG-IUS insertion. Short-term treatment
with the LNG-IUS was associated with changes in endometrial
morphology, reduced proliferation and
progesterone receptor expression; there were no associated
changes to circulating hormone levels,
measures of insulin resistance or adiposity. An unexpected
finding was that women lost an average
2.5kg in weight during the study, however, this was neither
clinically nor statistically significant. Given
our conviction that women with class III obesity are at
sufficiently high risk of endometrial cancer that
they would benefit from risk reducing measures, it is striking
that 3/35 (9%) of our participants had an
incidental finding of atypical endometrial hyperplasia or
endometrioid endometrial cancer at baseline,
requiring hysterectomy. This is consistent with our previous
study that found 10/72 (14%) women with
class III obesity referred for weight loss management had occult
underlying endometrial neoplasia [9].
Endometrial glands are clonal cell populations that frequently
harbour driver mutations in cancer
genes [30]. PTEN null glands confer a proliferative advantage,
predisposing to endometrial
carcinogenesis and have been shown to persist between menstrual
cycles but only a small proportion
progress to endometrial cancer [31]. We found PTEN null glands
in all three women with occult
endometrial abnormalities and in two participants with
histologically normal endometrium before, but
not after, LNG-IUS insertion. This is consistent with the
hypothesis that PTEN null glands in
morphologically normal endometrium represent latent endometrial
cancer precursors that regress
with LNG-IUS treatment [24].
Whilst the endometrial impact of the LNG-IUS is well studied
[32, 33], this is the first trial to offer the
LNG-IUS to women with class III obesity for the primary
prevention of endometrial cancer.
Confirmation that the expected endometrial effects of the
LNG-IUS are observed in this population is
important given their defining characteristics, specifically
their class III obesity and amenorrhoea or
irregular menstrual bleeding, which distinguish them from
regular users of the device. It is known that
Ki-67 score is higher in endometrium harvested from women with
obesity compared to that collected
from normal weight women [34]. We considered that the expected
change in endometrial
morphology, a reduction in glandular proliferation as assessed
by Ki-67 score, and down-regulation of
endometrial progesterone receptors would confirm the utility of
the LNG-IUS at standard doses in this
population. We also quantified the Ki-67 drop at six months
post-LNG-IUS insertion for the purposes of
Cancer Research. on July 7, 2021. © 2020 American Association
forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for
publication but have not yet been edited. Author Manuscript
Published OnlineFirst on September 30, 2020; DOI:
10.1158/1940-6207.CAPR-20-0248
http://cancerpreventionresearch.aacrjournals.org/
-
12
developing an intermediary molecular endpoint for a definitive
trial of the LNG-IUS for endometrial
protection upon which a sample size calculation could be based.
It is interesting that the 15% Ki-67
drop observed after six months treatment with the LNG-IUS was
similar to that observed after an
average bariatric surgery-induced weight loss of 22kg at two
months in women with class III obesity
[9]. Bariatric surgery is known to reduce endometrial cancer
risk [7, 8, 35], and although the
mechanisms underlying risk reduction are not fully understood,
it is thought that down-regulation of
endometrial pro-proliferative signalling pathways could be
important [9, 36]. Ki-67 is only expressed by
proliferating cells, a hallmark of cancer; indeed, Ki-67 is
known to differentiate benign from malignant
endometrium, with higher Ki-67 scores observed in high grade,
advanced stage cancer and correlating
with poor survival outcomes in this group [37]. We considered
that a reduction in glandular
proliferation in benign peri- and postmenopausal endometrium
could reduce the risk of mutational
events that trigger malignant transformation [10].
We have demonstrated proof of principle that some women at high
risk of obesity-driven endometrial
cancer are prepared to engage in risk reduction with a LNG-IUS,
paving the way for a clinical efficacy
trial in this population. Despite concerns that LNG-IUS
insertion would be challenging in the outpatient
setting in postmenopausal women with class III obesity, we had
no insertion failures, consistent with
previous studies [38]. Concerns that uterine instrumentation
would be unacceptable to women who
did not have a gynaecological complaint were also
unsubstantiated, with 32/35 (91%) of participants
consenting to and undergoing three sequential biopsies, without
complication. Further, we found the
LNG-IUS was not associated with a detrimental impact on mental
wellbeing using two validated
questionnaires, with even some suggestion that mental wellbeing
improved during the trial, possibly
due to improved menstrual bleeding profiles and peace of mind
regarding endometrial health; indeed
24/25 (96%) of participants chose to keep their LNG-IUS at the
end of the trial for ongoing endometrial
protection. A short-term study of this kind cannot confirm that
women will be compliant with the LNG-
IUS in the medium to long-term, however. Nor can it help define
the optimal duration of a clinical
efficacy trial. We did not deliberately target peri-menopausal
women for trial participation, although
long-term use of the LNG-IUS in a clinical efficacy trial would
ideally avoid women whose compliance
could be compromised by future pregnancy plans. The single
centre nature of this research is a
limitation of the study, since we cannot necessarily extrapolate
feasibility of our approach to other
centres, countries or healthcare settings. The lack of racial
and ethnic diversity in our study population
precludes any insight into the acceptability and uptake of the
LNG-IUS for uterine protection in non-
White British women. We do not know whether women would consent
to randomisation to a no
intervention arm, which would be the ideal clinical efficacy
trial design, and would certainly impact
feasibility of the definitive study. Furthermore, our biomarker
findings should be interpreted with
Cancer Research. on July 7, 2021. © 2020 American Association
forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for
publication but have not yet been edited. Author Manuscript
Published OnlineFirst on September 30, 2020; DOI:
10.1158/1940-6207.CAPR-20-0248
http://cancerpreventionresearch.aacrjournals.org/
-
13
caution given the small sample size and marked heterogeneity of
participating women with respect to
age, menopausal status and use of exogenous hormones at
baseline.
Whilst invasive, the advantage of the LNG-IUS is that it
releases a continuous supply of levonorgestrel
directly to the endometrium, avoiding the peaks and troughs
observed with oral administration and
eliminating compliance issues [39]. Apart from insertion
problems, there are few contraindications to
its use, at least partly because systemic concentrations of the
drug are much lower than those
achieved with oral administration [40]. Serum levonorgestrel
levels are 20-fold lower in LNG-IUS users
than levonorgestrel-containing combined oral contraceptive pill
users, for example [41]. There is an
inverse correlation between serum levonorgestrel concentrations
and body mass index [42],
suggesting even lower systemic levels in our population. A
further advantage of the LNG-IUS for this
indication is that it would be expected to eradicate or treat
latent endometrial cancer precursors,
atypical hyperplasia and occult obesity-driven endometrial
cancer, as previously demonstrated [24, 17-
19]. Regression of established endometrial abnormalities takes
6-12 months or longer and is more
likely in the case of atypical hyperplasia (approx. 90% complete
response rate) than early stage
endometrial cancer (67% complete response rate)[43]. There are
currently no validated biomarkers
that predict LNG-IUS response to established disease [44],
although some show promise [45, 46],
mandating careful assessment of any new bleeding that develops
following device-induced
amenorrhoea [47] in an endometrial cancer prevention trial.
Overall, we found the LNG-IUS to be safe and well-tolerated,
with no unacceptable side effects in our
study population. This is particularly important if the LNG-IUS
is being used for endometrial protection
rather than an established clinical indication, and should be a
focus of future work. There is no
evidence that the LNG-IUS increases the risk of cardiometabolic
disorders in obese women [48], but a
recent systematic review found LNG-IUS users have a modestly
increased breast cancer risk (odds ratio
=1.16 (95% CI 1.06-1.28, I2 =78%, p
-
14
[51]. Here, we demonstrate that a LNG-IUS is acceptable to some
women with class III obesity and
that a clinical efficacy trial would be feasible. The specifics
of trial design require careful consideration
because a large cohort with sufficient follow up will be
challenging and expensive to achieve.
Minimising trial size, duration of follow up and cost is an
important goal for women, researchers and
funders of such a trial. Whilst endometrial cancer risk is high
in women with class III obesity, absolute
risk is modulated by reproductive, metabolic and genetic factors
[13, 52], as well as competing risks for
death. More sophisticated risk prediction models, calibrated for
clinical use, must now be developed
to establish the optimal prevention trial target population, to
maximise the benefits of participation
and reduce unnecessary harms [53].
Cancer Research. on July 7, 2021. © 2020 American Association
forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for
publication but have not yet been edited. Author Manuscript
Published OnlineFirst on September 30, 2020; DOI:
10.1158/1940-6207.CAPR-20-0248
http://cancerpreventionresearch.aacrjournals.org/
-
15
Acknowledgements
We would like to thank the women who participated in this study.
We are grateful to all the clinical
staff involved in their care who helped facilitate recruitment,
especially Samantha Johnson and Bryan
Wilson. We would particularly like to thank Linsey Nelson, who
contributed to study set up, and Tina
Pritchard, who supported patient recruitment, provided nursing
care and helped with administrative
tasks. We are grateful to the independent members of the Trial
Steering Committee, Professor Sudha
Sundar, Professor Martin Rutter, Professor Steve Roberts and Mrs
Anne Lowry for providing study
oversight.
AED was a Manchester University NHS Foundation Trust Clinical
Research Fellow and EJC an NIHR
Clinician Scientist (NIHR-CS-012-009), and their work was
supported through the NIHR Manchester
Biomedical Research Centre (IS-BRC-1215-20007) and the William
Walter Will Trust. This article
presents independent research funded by the NIHR. The views
expressed are those of the authors and
not necessarily those of the NHS, NIHR, or the Department of
Health.
Author contributions
EJC was Principal Investigator for the study and is its
guarantor. EJC and HCK obtained funding and
designed the study. EJC, MLM and RJE supervised study execution.
MN supported study recruitment.
AED recruited women to the study and carried out trial
procedures. AED, JLA, MG, JB, JS, PWP and EJC
analyzed the results and interpreted the data. AED and EJC wrote
the manuscript. All authors provided
critical comment, edited the manuscript, and approved its final
version.
Cancer Research. on July 7, 2021. © 2020 American Association
forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for
publication but have not yet been edited. Author Manuscript
Published OnlineFirst on September 30, 2020; DOI:
10.1158/1940-6207.CAPR-20-0248
http://cancerpreventionresearch.aacrjournals.org/
-
16
References
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal
A. Global cancer statistics 2018:
GLOBOCAN estimates of incidence and mortality worldwide for 36
cancers in 185 countries. CA
Cancer J Clin. 2018;68(6):394-424.
2. Crosbie EJ, Morrison J. The emerging epidemic of endometrial
cancer: Time to take action.
Cochrane Database Syst Rev. 2014;12:ED000095.
3. Setiawan VW, Yang HP, Pike MC, et al. Type I and II
endometrial cancers: have they different risk
factors? J Clin Oncol 2013;31:2607-2618.
4. Arnold M, Pandeya N, Byrnes G, et al. Global burden of cancer
attributable to high body-mass
index in 2012: a population-based study. Lancet Oncol
2015;16:36–46.
5. Crosbie EJ, Zwahlen M, Kitchener HC, Egger M, Renehan AG.
(2010) Body mass index, sex
hormone-related states and endometrial cancer risk: a
meta-analysis. Cancer Epidemiol
Biomarkers Prev 19:3119-30.
6. Calle EE, Kaaks R. Overweight, obesity and cancer:
epidemiological evidence and proposed
mechanisms. Nat Rev Cancer. 2004;4:579–91.
7. Ward KK, Roncancio AM, Shah NR, et al. Bariatric surgery
decreases the risk of uterine
malignancy. Gynecol Oncol 2014;133:63–6.
8. Anveden A, Taube M, Peltonen M, Jacobson P,
Andersson-Assarsson JC, Sjoholm K, et al. Long-
term incidence of female specific cancer after bariatric surgery
or usual care in the Swedish Obese
Subjects Study. Gynecol Oncol. 2017;145(2):224–9.
9. MacKintosh ML, Derbyshire AE, McVey RJ, et al. (2019). The
impact of obesity and bariatric
surgery on circulating and tissue biomarkers of endometrial
cancer risk. Int J Cancer 144(3):641-
650.
10. MacKintosh ML and Crosbie EJ. (2013). Obesity-driven
endometrial cancer: is weight loss the
answer? BJOG 120: 791-4.
11. Bischoff SC, Damms-Machado A, Betz C, Herpertz S, Legenbauer
T, Löw T, et al. Multicenter
evaluation of an interdisciplinary 52-week weight loss program
for obesity with regard to body
weight, comorbidities and quality of life - A prospective study.
Int J Obes. 2012 Apr;36(4):614–24.
Cancer Research. on July 7, 2021. © 2020 American Association
forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for
publication but have not yet been edited. Author Manuscript
Published OnlineFirst on September 30, 2020; DOI:
10.1158/1940-6207.CAPR-20-0248
http://cancerpreventionresearch.aacrjournals.org/
-
17
12. Rahib L, Smith BD, Aizenberg R, Rosenzweig AB, Fleshman JM,
Matrisian LM. Projecting cancer
incidence and deaths to 2030: the unexpected burden of thyroid,
liver, and pancreas cancers in
the United States. Cancer Res. 2014 Jun 1;74(11):2913-21.
13. Kitson S, Evans DG, Crosbie EJ. (2017). Identifying high
risk women for endometrial cancer
prevention strategies: proposal of endometrial cancer risk
prediction model. Cancer Prevention
Research 10(1):1-13.
14. Bahamondes L, Valeria Bahamondes M, Shulman LP.
Non-contraceptive benefits of hormonal and
intrauterine reversible contraceptive methods. Hum Reprod Update
2015;21:640–51.
15. Jareid M, Thalabard J-C, Aarflot M, Bovelstad HM, Lund E,
Braaten T. Levonorgestrel-releasing
intrauterine system use is associated with a decreased risk of
ovarian and endometrial cancer,
without increased risk of breast cancer. Results from the NOWAC
Study. Gynecol Oncol.
2018;149(1):127–32.
16. Soini T, Hurskainen R, Grenman S, Maenpaa J, Paavonen J,
Pukkala E. Cancer risk in women using
the levonorgestrel-releasing intrauterine system in Finland.
Obstet Gynecol 2014;124:292–9.
17. Wan Y-L, Holland C. The efficacy of levonorgestrel
intrauterine systems for endometrial
protection: a systematic review. Climacteric.
2011;14(6):622–32.
18. Gunderson CC, Fader AN, Carson KA, et al. Oncologic and
reproductive outcomes with progestin
therapy in women with endometrial hyperplasia and grade 1
adenocarcinoma: a systematic
review. Gynecol Oncol 2012;125:477–82.
19. Yuk JS, Song JY, Lee JH, Park WI, Ahn HS, Kim HJ.
Levonorgestrel-Releasing Intrauterine Systems
Versus Oral Cyclic Medroxyprogesterone Acetate in Endometrial
Hyperplasia Therapy: A Meta-
Analysis. Ann Surg Oncol. 2017 May;24(5):1322-1329.
20. Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF,
Turner RC. Homeostasis model
assessment: insulin resistance and beta-cell function from
fasting plasma glucose and insulin
concentrations in man. Diabetologia. 1985 Jul;28(7):412–9.
21. Emons G, Beckmann MW, Schmidt D, Mallmann P, Uterus
commission of the Gynecological
Oncology Working Group (AGO). New WHO Classification of
Endometrial Hyperplasias.
Geburtshilfe Frauenheilkd. 2015 Feb;75(2):135–6.
22. RJ Kurman, Carcangiu M, Herrington CS, Young. WHO
classification of tumours of female
reproductive organs. 4th edition. Lyon: IARC; 2014.
Cancer Research. on July 7, 2021. © 2020 American Association
forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for
publication but have not yet been edited. Author Manuscript
Published OnlineFirst on September 30, 2020; DOI:
10.1158/1940-6207.CAPR-20-0248
http://cancerpreventionresearch.aacrjournals.org/
-
18
23. Dowsett M, Nielsen TO, A’Hern R, Bartlett J, Coombes RC,
Cuzick J, et al. Assessment of Ki67 in
Breast Cancer: Recommendations from the International Ki67 in
Breast Cancer Working Group.
JNCI J Natl Cancer Inst. 2011 Sep 29;103(22):1656–64.
24. Ørbo A, Rise CE, Mutter GL. Regression of latent endometrial
precancers by progestin infiltrated
intrauterine device. Cancer Res. 2006 Jun 1;66(11):5613–7.
25. Zigmond AS, Snaith RP. The hospital anxiety and depression
scale. Acta Psychiatr Scand. 1983
Jun;67(6):361-70.
26. Bjelland, I., Dahl, A. A., Tangen, T. & Neckelmann, D.
The validity of the Hospital Anxiety and
Depression Scale An updated literature review. 52, 69–77
(2002).
27. Tennant R, Hiller L, Fishwick R, Platt S, Joseph S, Weich S,
Parkinson J, Secker J, Stewart-Brown S.
The Warwick-Edinburgh Mental Well-being Scale (WEMWBS):
development and UK validation.
Health Qual Life Outcomes. 2007 Nov 27;5:63.
28. Putz R, O’Hara K, Taggart F, Stewart-Brown S. Using WEMWBS
to measure the impact of your
work on mental wellbeing : A practice-based user guide.
(2012).
29. Matteson KA, Scott DM, Raker CA, Clark MA. The menstrual
bleeding questionnaire: development
and validation of a comprehensive patient-reported outcome
instrument for heavy menstrual
bleeding. BJOG. 2015 Apr;122(5):681-9. doi:
10.1111/1471-0528.13273.
30. Moore L, Leongamornlert D, Coorens THH, et al. The
mutational landscape of normal human
endometrial epithelium. Nature. 2020;580(7805):640-646.
doi:10.1038/s41586-020-2214-z
31. Monte NM, Webster KA, Neuberg D, Dressler GR, Mutter GL.
Joint loss of PAX2 and PTEN
expression in endometrial precancers and cancer. Cancer Res.
2010;70(15):6225-6232.
doi:10.1158/0008-5472.CAN-10-0149
32. Guttinger A, Critchley HO. Endometrial effects of
intrauterine levonorgestrel. Contraception.
2007;75(6 Suppl):S93‐S98.
33. Dinh A, Sriprasert I, Williams AR, Archer DF. A review of
the endometrial histologic effects of
progestins and progesterone receptor modulators in reproductive
age women. Contraception.
2015;91(5):360‐367.
34. Villavicencio A, Aguilar G, Argüello G, Dünner C, Gabler F,
Soto E, et al. The effect of overweight
and obesity on proliferation and activation of AKT and ERK in
human endometria. Gynecol Oncol
2010;117:96–102.
Cancer Research. on July 7, 2021. © 2020 American Association
forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for
publication but have not yet been edited. Author Manuscript
Published OnlineFirst on September 30, 2020; DOI:
10.1158/1940-6207.CAPR-20-0248
http://cancerpreventionresearch.aacrjournals.org/
-
19
35. Zhang K, Luo Y, Dai H, Deng Z. Effects of Bariatric Surgery
on Cancer Risk: Evidence from Meta-
analysis. Obes Surg. 2020;30(4):1265‐1272.
36. Argenta P, Svendsen C, Elishaev E, et al. Hormone receptor
expression patterns in the
endometrium of asymptomatic morbidly obese women before and
after bariatric
surgery. Gynecol Oncol. 2014;133(1):78‐82.
37. Kitson S, Sivalingam VN, Bolton J, McVey R, Nickkho-Amiry M,
Powell ME et al. Ki-67 in
endometrial cancer: scoring optimization and prognostic
relevance for window studies. Mod
Pathol 2017;30:459–68.
38. Saito-Tom LY, Soon RA, Harris SC, Salcedo J, Kaneshiro BE.
Levonorgestrel Intrauterine Device Use
in Overweight and Obese Women. Hawaii J Med Public Health.
2015;74(11):369‐374.
39. Nilsson CG. Tissue concentrations of levonorgestrel in women
using a levonorgestrel-releasing
IUD. Clinical Endocrinology 1982;529–36.
40. Apter D, Gemzell-Danielsson K, Hauck B, Rosen K, Zurth C.
Pharmacokinetics of two low-dose
levonorgestrel-releasing intrauterine systems and effects on
ovulation rate and cervical function:
Pooled analyses of phase II and III studies. Fertil Steril
2014;101(6):1656–62.e4.
41. Mirena Annotated CCDS 2014, Bayer AG, Berlin, Germany, 11th
February 2014.
42. Seeber B, Ziehr SC, Gschlieβer A, Moser C, Mattle V, Seger
C, et al. Quantitative levonorgestrel
plasma level measurements in patients with regular and prolonged
use of the levonorgestrel-
releasing intrauterine system. Contraception
2012;86(4):345‐349.
43. Westin SN, Fellman B, Sun CC, et al. Prospective Phase II
Trial of Levonorgestrel Intrauterine
Device: Non-Surgical Approach for Complex Atypical Hyperplasia
and Early Endometrial
Cancer. Am J Obstet Gynecol. 2020;S0002-9378(20)30861-9.
doi:10.1016/j.ajog.2020.08.032
44. Derbyshire AE, Ryan N, Crosbie EJ. Biomarkers needed to
predict progestin response in
endometrial cancer. BJOG. 2017;124(10):1584.
doi:10.1111/1471-0528.14490
45. Travaglino A, Raffone A, Saccone G, et al.
Immunohistochemical predictive markers of response to
conservative treatment of endometrial hyperplasia and early
endometrial cancer: A systematic
review. Acta Obstet Gynecol Scand. 2019;98(9):1086-1099.
doi:10.1111/aogs.13587
46. Behrouzi R, Ryan NAJ, Barr CE, et al. Baseline Serum HE4 But
Not Tissue HE4 Expression Predicts
Response to the Levonorgestrel-Releasing Intrauterine System in
Atypical Hyperplasia and Early
Stage Endometrial Cancer. Cancers (Basel). 2020;12(2):276.
doi:10.3390/cancers12020276
Cancer Research. on July 7, 2021. © 2020 American Association
forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for
publication but have not yet been edited. Author Manuscript
Published OnlineFirst on September 30, 2020; DOI:
10.1158/1940-6207.CAPR-20-0248
http://cancerpreventionresearch.aacrjournals.org/
-
20
47. Barr CE, Crosbie EJ. The Mirena coil is a suitable treatment
of early-stage endometrial cancer in
obese women: FOR: Careful selection and monitoring is key. BJOG.
2020;127(8):1001.
doi:10.1111/1471-0528.16224
48. Bender NM, Segall-Gutierrez P, Najera SO, Stanczyk FZ,
Montoro M, Mishell DR Jr. Effects of
progestin-only long-acting contraception on metabolic markers in
obese women. Contraception.
2013;88(3):418‐425. doi:10.1016/j.contraception.2012.12.007
49. Conz L, Mota BS, Bahamondes L, et al.
Levonorgestrel-releasing intrauterine system and breast
cancer risk: A systematic review and meta-analysis. Acta Obstet
Gynecol Scand.
2020;10.1111/aogs.13817. doi:10.1111/aogs.13817
50. Wan YL, Beverley-Stevenson R, Carlisle D, Clarke S,
Edmondson RJ, Glover S, et al. Working
together to shape the endometrial cancer research agenda: The
top ten unanswered research
questions. Gynecol Oncol. 2016;143(2):287‐293.
51. Dottino JA, Hasselblad V, Secord AA, Myers ER, Chino J,
Havrilesky LJ. Levonorgestrel Intrauterine
Device as an Endometrial Cancer Prevention Strategy in Obese
Women: A Cost-Effectiveness
Analysis. Obstet Gynecol. 2016;128(4):747-753.
52. Bafligil C, Thompson DJ, Lophatananon A, et al. Association
between genetic polymorphisms and
endometrial cancer risk: a systematic review. J Med Genet.
2020;jmedgenet-2019-106529.
53. O'Mara TA, Crosbie EJ. Polygenic risk score opportunities
for early detection and prevention
strategies in endometrial cancer. Br J Cancer.
2020;10.1038/s41416-020-0959-7.
Cancer Research. on July 7, 2021. © 2020 American Association
forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for
publication but have not yet been edited. Author Manuscript
Published OnlineFirst on September 30, 2020; DOI:
10.1158/1940-6207.CAPR-20-0248
http://cancerpreventionresearch.aacrjournals.org/
-
21
Table 1: Baseline characteristics of the study population
Median age (IQR), years 54 (52, 57)
White British, n (%) 24 (96)
Median weight (IQR), kg 124 (111, 143)
Median BMI (IQR), kg/m2 47 (44, 51)
Median waist:hip ratio (IQR) 0.87 (0.83, 0.93)
Menopausal status, n (%)
Pre-menopausal 9 (36)
Post-menopausal 16 (64)
Menstrual cycle, n (%)
Amenorrhoeic 5 (20)
Regular 4 (16)
Irregular 3 (12)
Parity, n (%)
0 1 (4)
1 6 (24)
2 10 (40)
3+ 8 (32)
Exogenous hormones, n (%) 4 (16)
Polycystic ovary syndrome (PCOS), n (%) 6 (24)
Comorbidities, n (%)
Hypertension 15 (60)
Type II diabetes mellitus 10 (40)
Hypercholesterolaemia 5 (20)
Gallbladder/ liver disease 5 (20)
Thromboembolic disease 3 (12)
Asthma/ COPD 8 (32)
Sleep apnoea 9 (36)
Osteoarthritis 15 (60)
Depression/ anxiety 8 (32)
Cancer Research. on July 7, 2021. © 2020 American Association
forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for
publication but have not yet been edited. Author Manuscript
Published OnlineFirst on September 30, 2020; DOI:
10.1158/1940-6207.CAPR-20-0248
http://cancerpreventionresearch.aacrjournals.org/
-
22
Table 2: Mixed effects regression model reporting change in
Ki-67 score over time
Ki-67 score (No. observations = 71)
Factor Category Coef (95% C.I.)a Coef (95% C.I.)b Coef (95%
C.I.)c
Time point T0 - Baseline (Ref) - - -
T1 - LNG-IUS -5.27(-16.9,6.39) -5.37(-17.1,6.33)
-5.76(-17.5,5.99)
T2 - Follow up -14.4(-25.1,-3.62) -14.6(-25.3,-3.91)
-15.3(-25.9,-4.58)
Baseline age - 0.69(-0.50,1.85) 0.77(-0.49,2.04)
Baseline weight - -0.26(-0.90,0.38) -0.32(-0.98,0.33)
Baseline BMI - 0.94(-1.00,2.82) 1.09(-0.84,3.03)
Smoker Never (Ref) - -
Ever - 3.54(-7.70,14.8) 3.21(-8.02,14.4)
Yes - 7.34(-4.80,19.5) 7.92(-4.28,20.1)
Type II diabetes mellitus No (Ref) - -
Yes - -2.73(-10.9,5.49) -2.23(-10.8,6.30)
Menopause status Post (Ref) - -
Pre - 5.56(-3.80,14.9) 5.42(-4.16,15.0)
Change in weight - - -0.41(-1.50,0.68)
Constant 27.1(17.8,36.4) -23.82(-107,58.9) -28.5(-117,560.0)
Random Effects (Bootstrapped)
Variance constant 7.17E-12 2.38E-11 2.69E-11
Variance residuals 285.4 290.3 290.8
Intra-class correlation 1.47E-13 8.20E-14 9.25E-14
a. Mixed model with time of assessment only adjusted for within
participant clustering b. Mixed model with time of assessment
adjusted for within participant clustering and baseline
screening characteristics c. Mixed model with time of assessment
adjusted for within participant clustering, baseline
screening characteristics and change in weight from baseline
Cancer Research. on July 7, 2021. © 2020 American Association
forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for
publication but have not yet been edited. Author Manuscript
Published OnlineFirst on September 30, 2020; DOI:
10.1158/1940-6207.CAPR-20-0248
http://cancerpreventionresearch.aacrjournals.org/
-
23
Table 3: Changes in anthropometric, blood and endometrial tissue
biomarkers over time
T0 - baseline n=25
T1 - LNG-IUS n=25
T2 - follow up n=25
Anthropometric measures, mean (SD)
Weight, kg 129.1 (19.2) 128.3 (19.4) 126.7 (19.2)
BMI, kg/m2 48.3 (6.3) 48.0 (6.4) 47.5 (6.7)
Waist:hip ratio 0.9 (0.07) 0.88 (0.07) 0.87 (0.07)
Blood biomarkers of reproductive function, mean (SD)
Estradiol, pmol/L 11.8 (6.6) 9.7 (5.5) 10.1 (6.0)
Progesterone, ng/ml 3.1 (2.8) 3.8 (3.8) 1.4 (1.0)
Testosterone, nmol/L 7.1 (3.6) 6.3 (3.4) 6.8 (3.7)
SHBG, nmol/L 43.6 (28.8) 44.6 (24.7) 41.6 (21.9)
FAI 3.1 (2.7) 2.5 (2.2) 2.6 (1.8)
LH, IU/L 18.5 (13.1) 17.1 (12.8) 23.3 (16.1)
FSH, IU/L 28.8 (23.0) 27.9 (21.7) 35.1 (23.8)
Blood biomarkers of insulin resistance, mean (SD)
Glucose, mmol/L 5.5 (0.8) 5.5 (1.0) 5.5 (0.9)
Insulin, mU/L 139.0 (122.6) 123.1 (78.8) 124.9 (110.8)
HOMA 12.5 (7.1) 28.0 (24.3) 33.8 (34.9)
HbA1c, mmol/mol 41.9 (8.2) 41.7 (9.3) 42.2 (9.5)
Blood biomarkers of adiposity, mean (SD)
Adiponectin, mg/L 5.6 (13.4) 3.6 (3.7) 3.2 (4.1)
Leptin, ng/mL 77.3 (35.2) 82.9 (46.0) 83.4 (41.4)
Blood biomarkers of inflammation, mean (SD)
CRP, mg/L 9.0 (4.1) 6.2 (3.3) 7.3 (4.0)
Tissue biomarkers, mean (SD)
Ki-67 score (%) 27.1 (23.4) 21.8 (14.8) 12.7 (10.9)
pAKT H-score 105.5 (49.9) 89.4 (38.3) 93.1 (40.6)
Estrogen receptor (ER) H-score 0.8 (0.1) 0.9 (0.1) 0.8 (0.1)
Progesterone receptor (PR) H-score 0.8 (0.2) 0.9 (0.1) 0.4
(0.2)
Any PTEN-null glands (n, % participants) 2 (8%) 2 (8%) 0
(0%)
Cancer Research. on July 7, 2021. © 2020 American Association
forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for
publication but have not yet been edited. Author Manuscript
Published OnlineFirst on September 30, 2020; DOI:
10.1158/1940-6207.CAPR-20-0248
http://cancerpreventionresearch.aacrjournals.org/
-
24
Table 4: Changes in mental wellbeing and quality of life over
time
WEMWBS HADS
All participants
n=25
Subset of participants*
n=17
All participants n=25
Subset of participants*
n=17
Baseline (T0) Mean score (SD)
45.4 (10.6) 47.3 (10.9) 17.1 (10.4) 12.3 (9.3)
Follow up (T2) Mean score (SD)
47.9 (9.1) 52 (10.9) 14.9 (9.5) 11.4 (8.8)
*After excluding women with known depression/ anxiety
disorder
Cancer Research. on July 7, 2021. © 2020 American Association
forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for
publication but have not yet been edited. Author Manuscript
Published OnlineFirst on September 30, 2020; DOI:
10.1158/1940-6207.CAPR-20-0248
http://cancerpreventionresearch.aacrjournals.org/
-
25
Figure legend
Figure 1: Study flow chart showing accrual and retention of
participants
Cancer Research. on July 7, 2021. © 2020 American Association
forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for
publication but have not yet been edited. Author Manuscript
Published OnlineFirst on September 30, 2020; DOI:
10.1158/1940-6207.CAPR-20-0248
http://cancerpreventionresearch.aacrjournals.org/
-
Cancer Research. on July 7, 2021. © 2020 American Association
forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for
publication but have not yet been edited. Author Manuscript
Published OnlineFirst on September 30, 2020; DOI:
10.1158/1940-6207.CAPR-20-0248
http://cancerpreventionresearch.aacrjournals.org/
-
Published OnlineFirst September 30, 2020.Cancer Prev Res Abigail
E Derbyshire, Jennifer L Allen, Matthew Gittins, et al. obese women
(PROTEC) trial: a feasibility studyPROgesterone Therapy for
Endometrial Cancer prevention in
Updated version
10.1158/1940-6207.CAPR-20-0248doi:
Access the most recent version of this article at:
Material
Supplementary
0-0248.DC1
http://cancerpreventionresearch.aacrjournals.org/content/suppl/2020/09/30/1940-6207.CAPR-2Access
the most recent supplemental material at:
Manuscript
Authorbeen edited. Author manuscripts have been peer reviewed
and accepted for publication but have not yet
E-mail alerts related to this article or journal.Sign up to
receive free email-alerts
Subscriptions
Reprints and
[email protected] at
To order reprints of this article or to subscribe to the
journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take
you to the Copyright Clearance Center's (CCC)
.-0248http://cancerpreventionresearch.aacrjournals.org/content/early/2020/12/11/1940-6207.CAPR-20To
request permission to re-use all or part of this article, use this
link
Cancer Research. on July 7, 2021. © 2020 American Association
forcancerpreventionresearch.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for
publication but have not yet been edited. Author Manuscript
Published OnlineFirst on September 30, 2020; DOI:
10.1158/1940-6207.CAPR-20-0248
http://cancerpreventionresearch.aacrjournals.org/lookup/doi/10.1158/1940-6207.CAPR-20-0248http://cancerpreventionresearch.aacrjournals.org/content/suppl/2020/09/30/1940-6207.CAPR-20-0248.DC1http://cancerpreventionresearch.aacrjournals.org/content/suppl/2020/09/30/1940-6207.CAPR-20-0248.DC1http://cancerpreventionresearch.aacrjournals.org/cgi/alertsmailto:[email protected]://cancerpreventionresearch.aacrjournals.org/content/early/2020/12/11/1940-6207.CAPR-20-0248http://cancerpreventionresearch.aacrjournals.org/content/early/2020/12/11/1940-6207.CAPR-20-0248http://cancerpreventionresearch.aacrjournals.org/
Article FileFigure 1