Embed Size (px)
Citation preview

280
2 0 0 6 E N D O D O N T I C U P D A T E
© 2 0 0 6 , C O P Y R I G H T T H E A U T H O RJ O U R N A L C O M P I L A T I O N © 2 0 0 6 , B L A C K W E L L M U N K S G A A R D
*Private practice, Tacoma, WA; associate clinical professor, University of Washington School of Graduate Endodontics, Tacoma, WA, USA; and clinical instructor,
Boston University Henry M. Goldman School of Dental Medicine, Boston, MA, USA
Endodontic Update 2006
JOHN WEST, DDS, MSD*
DOI 10.1111/j.1708-8240.2006.00039.x
ABSTRACTThe past 10 years have witnessed more significant changes in the artand science of endodontics than the previous 100 years. This observa-tion is no surprise, given that change is our only constant. The rate ofchange, however, has been anything but constant. The rate has acceler-ated so fast that all clinicians in the field of dentistry need a reliablesource to guide us in what works. What works today in endodontics isthe theme of this update.
The discoveries and advancements in endodontic technology, instru-ments, and materials enable practitioners to achieve treatment outcomesthat were previously considered unattainable. For example, in nonsurgi-cal endodontic treatment, nickel titanium technology consistently canproduce predictable radicular preparations that can be easily obturated.In nonsurgical re-treatment, the previous endodontic obturationattempt frequently can be removed and successfully re-treated largelybecause of enhanced vision and coaxial lighting from the operatingmicroscope. Importantly, careful nonsurgical re-treatment usually canbe accomplished without disruption to the existing restorations andwithout risk to ferrule integrity. In endodontic surgery underfilledforamina, and the isthmi between them, predictably can be connectedand obturated with state-of-the-art miniature instruments.
CLINICAL SIGNIFICANCEThis article reviews the clinical endodontic breakthroughs encounteredduring the last decade and focuses on three primary topics: (1) findingcanals; (2) following canals; and (3) finishing canals. Every day, dentistsare faced with the interdisciplinary treatment planning question of to“save or not to save a tooth?” Dentists must routinely make the deci-sion of whether to remove or restore the tooth based on biology, struc-ture, function, esthetics, and value.1 Occasionally, the endodonticallytreated tooth can be the weakest link in the restorative and estheticsequence. This article examines the current state of endodontic technol-ogy, as well as the fundamentals of endodontic mechanics needed toachieve the most predictable endodontic outcome with the highestdegree of success.
(J Esthet Restor Dent 18:280–300, 2006)
PROFILE
John D. West, DDS, MSD
Current OccupationPrivate practice
Education
University of Washington School of Dentistry, 1967, DDS
Boston University Henry M. Goldman Schoolof Dental Medicine, 1971, Certificate andMSD in Endodontics
Academic Affiliations
Associate clinical professor, University of Washington School of Graduate Endodontics
Clinical instructor, Boston University Henry M. Goldman School of Dental Medicine
Professional Memberships
American Association of EndodonticsInternational College of DentistsAcademy of Microscope Enhanced DentistryNorthwest Network for Dental ExcellenceAmerican Academy of Esthetic Dentistry
Positions Held
Scientific editor, Boston University’sEndodontic Communique
American Academy of Esthetic Dentistry(AAED) Executive Council
Vice-president of AAEDEditorial advisory board for the following
journals:1. Advanced Esthetics and Interdisciplinary
Dentistry;2. Academy of Microscope Enhanced
Dentistry;3. Journal of Esthetic and Restorative
Dentistry;4. Practical Procedures and Aesthetic Dentistry
Honors/Awards
1995 Distinguished Alumnus Award, Henry M.Goldman School of Dental Medicine
Publications
Obturation of the radicular space (with Dr. John Ingle) in Ingle’s 1994 and 2002 editions of Endodontics
Cleaning and shaping the root canal system in Cohen and Burns (senior author) in 1994 and 1998 Pathways of the Pulp
Orthodontic–endodontic treatment planning of traumatized teeth (with Dr. Dave Steiner). Semin Orthod 1997;3(1):39–44
A method to determine the location and shape of an intracoronal bleach barrier (with Dr. Dave Steiner) J Endod 1994;20(6);304–6
Bleaching pulpless teeth (with Dr. Dave Steiner) in Goldstein and Garker’s 1995 edition of Complete Dental Bleaching.
Personal Interests
Boating/skiing, golfing, and being with familyand friends
Notable Contribution(s) to Dentistry
Co-inventor of the ProTaper Endodontic Technology, Dentsply Tulsa Dental, Tulsa,OK, USA

W E S T
V O L U M E 1 8 , N U M B E R 5 , 2 0 0 6 281
F I N D I N G C A N A L S
The rationale for endodonticsstates that “any endodontically
involved tooth can be saved if theroot canal system can be sealednonsurgically or surgically, if theperiodontal condition is healthy orcan be made healthy, and the toothis restorable”2 (Figure 1). Whileendodontic treatment may have a100% “capacity” for healing andsuccess, in reality, the success rate is100–X, where X represents the clin-ician’s endodontic knowledge andskill as well as their “willingness”to stay focused on the desired out-come while there may be pressuresto do otherwise. But, in order tohave success, dentists must first findthe canals. The microscope,
improved access cavities, and ultra-sonics have significantly enhanceddentists’ ability to find the canals inendodontics.
MicroscopeThe early 1990s was a time thatwas highlighted by significant tech-nological advances in endodontics(Figure 2).3,4 It began with theintroduction of the microscope.Not only did the microscope allowdentists to find canals that werepreviously difficult or impossible tofind, but also, it allowed dentists tofind these canals more frequently.The microscope allowed cliniciansto see better, feel better, and thinkbetter. In addition to facilitatingfinding canals, the microscope also
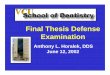
has improved endodontic outcomesin diagnosis, predictability, toothconservation, and location of addi-tional canals.5 The microscopemakes it easier to diagnose hairlinevertical fractures especially in ClassI and II cracked tooth syndromecases, micromovement of loosecrowns, bridges and restorations,detecting internal access microleak-age under restorations and crowns,tracing orifi of sinus tracts, detect-ing Class V apical fractures, discov-ering isthmi between two canals inthe same root, and finding canalorifi that are difficult to see (Figure3A–F). Predictability of the out-come improves because of betteraccess, debridement, shaping, andobturation. The literature suggests
Figure 1. Rationale for endodontics. A, Teeth exist first with a healthy pulp and healthy attachment apparatus. B, Whenpulps die, they become avascular, and viable and nonviable irritants migrate out of the root canal system portals of exit(POE) or foramina. C, Lesions of endodontic origin form adjacent to the POEs. D, The root canal system is cleaned andshaped with the same thoroughness as if the tooth were actually extracted. E, The cleaned and shaped preparation isobturated. F, The lesions of endodontic origin predictably heal.

282
2 0 0 6 E N D O D O N T I C U P D A T E
© 2 0 0 6 , C O P Y R I G H T T H E A U T H O RJ O U R N A L C O M P I L A T I O N © 2 0 0 6 , B L A C K W E L L M U N K S G A A R D
that the use of the microscope incombination with an appropriatecase selection and other currenttechnologies and materials mayresult in improved surgical treat-ment outcomes.6–8
The microscope literally broughtendodontics out of the dark andrepresented a paradigm shift notonly in endodontics, but also inperiodontics9–11 and advancedesthetic and restorative den-tistry.12,13 The use of the micro-scope has been met with bothexcitement and controversy in thepast decade. It is, of course, not apanacea. It is certainly not a reli-gion, as some may have us believe.
It will not make a good dentistgreat. It will, however, make both agood dentist and a great dentist bet-ter because they can see better. Thebenefit is just that simple. Themicroscope also does not definethe standard of care in endodontics,but it can help define the level ofprecision and therefore potentiallythe level of excellence. The micro-scope has clearly advanced from anovelty item and marketing tool toan indispensable instrument.
Beginning in 1997, residents in thefield of endodontics in America andCanada have been required to grad-uate with proficiency in the use of the operating microscope. In
addition, industry insiders estimatethat 76% of all US endodontistscurrently own a microscope in theirpractice. Interestingly, the marketgrowth potential seems to be in thegeneral practitioner arena. The per-centage of general dentists currentlyowning a microscope is estimatedat a mere 1%. Recently, the University of Washington School ofDentistry in Seattle, Washington,was the first dental school in thecountry and the world to providepredoctoral students with the use ofmicroscopes in clinical dentistry.14
Three years from now, in 2009,these dentists will be among thefirst generation of graduates in theworld where the use of the micro-scope to enhance their restorativeprecision will be second nature.They will change dentistry, becausethey will be able to see better.
Access CavitiesThe first step toward successfulcleaning and shaping is a straight-line access cavity.15 This means thatfiles enter the root canal systemunimpeded from the restriction ofenamel or dentin triangles. Thesetriangles act as file fulcrums, bothby deflecting the desired instrumentpath and decreasing the operator’stactile sense and control.
Anterior teeth typically have anincisal enamel triangle (triangle I)and a lingual dentin triangle (trian-gle II) that must be removed inorder to achieve straight-line
Figure 2. Microscope enables both clinician and dental assistant to treat inhealthy posture without tethering to the light source and without often-awkward magnifying glasses.

W E S T
V O L U M E 1 8 , N U M B E R 5 , 2 0 0 6 283
access. Triangle I is most easilyremoved with the same round burused to attain the initial access bypenetrating and alternately flaringincisally until the enamel triangle is removed. A thin tapered diamondis useful for finishing. The dentin
triangle II is most easily removedwith a #1 and #2 Gates Gliddendrill and finished with a thintapered diamond or a ProTaper SXfile (Dentsply Tulsa Dental, Tulsa,OK, USA) in a lingual brushingmotion.
In posterior multirooted teeth, ori-fice dentin triangles frequently pre-vent straight-line access and mustbe removed by a small Gates Glidden or an endodontic rotaryinstrument such as the SX ProTapershaping file (Figure 4A–D).
A B C
D E F
Figure 3. The microscope can bring the dentist closer to reality. A, Pretreatment radiograph of symptomatic tooth #8. B, Surgically beveled root-end with 2.5× magnification. C, At 10× apical Class V, fracture becomes obvious. D, Root-endpreparation of maxillary premolar stained with methylene blue. Note the patent isthmus between the buccal and lingual canal. In order to maximize endodontic success, the isthmus must be prepared with small ultrasonic instruments and sealed. E, Access cavity of maxillary first molar endodontic failure, as seen with low eyewear magnification. F, 15× magnificationreveals a second distobuccal and second mesiobuccal canal entrance (arrows).

284
2 0 0 6 E N D O D O N T I C U P D A T E
© 2 0 0 6 , C O P Y R I G H T T H E A U T H O RJ O U R N A L C O M P I L A T I O N © 2 0 0 6 , B L A C K W E L L M U N K S G A A R D
11 burs (Figure 5A). Second, theProTaper access kit (Dentsply TulsaDental) consists of just six essentialburs, including the new X-GatesGlidden that features a consolida-tion of all six Gates Glidden drillgeometries into one single drill.Space also exists in the kit for theclinician’s addition of his or herpersonal choice of burs (Figure 5B).
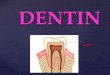
UltrasonicsUltrasonic technology, such asProUltra ultrasonic tips (DentsplyTulsa Dental), has become an indis-pensable part of the endodonticarmamentarium16 (Figure 6A).Ultrasonic instrument use includes removing pulp stones,
denticles, posts, separated instru-ments, silver cones, gutta-percha,Resilon, and carrier-based obtura-tors. Locating MB2 canals, whichexist in over 93% of maxillarymolars and, of which, over 50%are entirely separate canals, is challenging, because the head of thehigh-speed handpiece often blocksthe precision placement of the bureven if using extra-long surgicallength burs.17 The ultrasonic unithas no handpiece head and, there-fore, no line-of-sight barrier. Theclinician can safely control wherethe ultrasonic tip cuts (Figure6B–H). Because canals calcify in acoronal to apical direction, ultrasonics are extremely valuable
A B
C D
Figure 4. Straight-line access for posterior teeth. A, Pretreatment radiograph ofpulpitic tooth #14. B, Dentinal triangle prevents unrestricted access into the MBcanal. C, Dentinal triangle removed. D, Straight-line access is achieved. Cleanedand shaped canal is easily obturated.
A
B
Figure 5. Modern access kits. A, LAAxxess kit. B, ProTaper access kit.
Many errors are made in the selec-tion of access burs. They are oftentoo large in diameter, resulting ingouging the axial walls and pulpalfloor. Smaller burs tend to cutsmoother than larger burs and are,therefore, kinder to the tooth andto restorative materials such asporcelain. Additionally, thesmoother a bur cuts, the more posi-tive the patient experience. Ideally,only new burs should be used in theendodontic access. In an attempt tosimplify access choices, two newsystems have been recently introduced. The LA Axxess kit(SybronEndo, Orange, CA, USA)features both high- and low-speedlatch-grip burs numbering a total of

W E S T
V O L U M E 1 8 , N U M B E R 5 , 2 0 0 6 285
A B C
D E F
G H I
J
Figure 6. The ultrasonic advantage. A, ProUltra ultrasonic tips are one brand of several that enable unprecedented visualaccuracy during their use. B, Pretreatment radiograph of tooth #14 with necrotic pulp and chamber calcific metamorphosis.C, Mesiopalatal canal is palatal to mesiobuccal, but is not patent due to chamber calcification. D, Head of handpiece withlong-shank #2 round bur blocks the view of the bur’s cutting tip. E, Ultrasonic tip allows operator to observe active tip forpinpoint accuracy. F, Mesiopalatal canal conservatively located and cleaned and shaped. G, Both mesiobuccal canals obtu-rated. H, Radiograph shows two distinct canals with separate orifi and separate apical portals or exit. I, Orifice of calcifiedcanal is discovered less than 3 mm from the apex! Note that calcified dentin is darker than the surrounding dentin. Patentcanal entrance is darker yet and in the middle of the ultrasonic penetration. J, Radiograph demonstrates the extraordinary yetsafe depth before the canal could be negotiated.

286
2 0 0 6 E N D O D O N T I C U P D A T E
© 2 0 0 6 , C O P Y R I G H T T H E A U T H O RJ O U R N A L C O M P I L A T I O N © 2 0 0 6 , B L A C K W E L L M U N K S G A A R D
in following “darker-than-dentincolor maps” until the calcified canalbecomes patent and can be followedwith an endodontic file (Figure 6I,J).
Ultrasonic tips should be used in alight brushing motion. When usedto vibrate posts in order to removethem, use water coolant spray toprevent overheating the post, tooth,and periodontal ligament.18 If thetooth is anesthetized, there is noheat warning to the patient whatso-
ever. Ultrasonics also can refine andmarry the access cavity to thecanal’s entrance and subsequentradicular “glide path.”
Finally, finding canals is more suc-cessful today because of endodonticexplorers that are less than half thediameter of traditional endodonticexplorers (CK Dental, Orange, CA,USA). They enable the clinician toaccess the canal entrance withfinesse and without instantly
blocking it with “dentin mud” thatwould typically be entrapped in thecanal orifice using the wider stan-dard endodontic explorer.
F O L L O W I N G C A N A L S
There is perhaps no part ofendodontic treatment that requiresgreater delicacy and greaterrestraint than following the canalfrom the orifice entrance to theradiographic terminus (RT) (Figure7). The RT is the only reproducible
A B
D E
C
Figure 7. Important keys to successful endodontic mechanics. A, #10 file before curving the tip. B, Using cotton pliers withbeaks parallel to the shaft of the file, gently sweep to the file tip while intentionally curving the file. Now the instrument hasthe capacity to slide around denticles, dense collogen, or necrotic debris. C, Maximum tactile sense is achieved by using mini-mal “skin contact.” D, Maximum “skin contact” results in minimal tactile sense. E, Diagram of the four possible reasons a filedoes not go to length during the early stages of cleaning and shaping.

W E S T
V O L U M E 1 8 , N U M B E R 5 , 2 0 0 6 287
landmark that allows patencythroughout cleaning and shapingand is, by definition, slightly pastthe foraminal constriction. The skillrequired in following canals is atthe heart of the art of predictablysuccessful endodontics and repre-sents one of the four intentionalmotions that are key in developinga “glide path.”19 Whenever a den-tist passes a file past the canal ori-fice, he or she must ask, “What ismy intention with this file? What isthe outcome I want from its use?”Most endodontic students learnedto “file for awhile and hope thatsomething good would happen.”Often, it did not! Other motionswere “watch/wind” and“push/pull.” None of these motionsaccurately described how to pro-gressively begin the cleaning andshaping mechanics.
MotionsMasterful cleaning and shapingbegins with understanding the roleof thoughtful and efficient manualfile motions that are used to pavethe way for successful rotary finish-ing. Essentially, there are four criti-cally distinct motions that takeadvantage of the geometries oftoday’s hand files. The motions are follow, smooth, balance, andenvelope.
FollowA good analogy to describe the fol-low motion is a child sliding downa curved playground slide. If the
child simply does not fight the ten-dency to “go with the flow,” he orshe will safely arrive at the bottomof the slide time after time withoutfail. Successful endodontic follow-ing requires a precurved instru-ment, copious irrigation withsodium hypochlorite, and minimaltactile contact with the endodonticfile (Figure 7A,B). The index fingerand thumb should literally be posi-tioned behind the instrument ratherthan to the side (Figure 7C,D). Thispositioning reduces the temptationto direct the instrument, andincreases the desired motion of sim-ply “going along for the ride.” Theminimal finger contact alsoincreases tactile sense.
Anytime an instrument cannot befollowed to the radiographic and/orelectronic terminus, there are fourpossible causes or combination ofcauses (Figure 7E).
1. The apical area is clogged with“dentin mud.” The solution is toirrigate and gently “disrupt” thecoronal fraction of the apicalblock by placing an abrupt api-cal curve on the file and follow-ing with the instrument until ittouches the coronal portion ofthe block. By repeating thesequence, the file will often dis-rupt the dense dentin mud thatis packed at the coronal end ofthe dense plug. Next, follow themore loosely packed dentin mudto the terminus.
2. The curve of the file does notmatch the curve of the canal.The solution is to re-curve thefile with cotton pliers and sys-tematically mimic the possiblecurvatures until the file finds the path to follow to the terminus.
3. The tip diameter of the file istoo wide for the width of thecanal. The solution is to select atip size one or two sizes narrower. In dealing with a calcified canal, the choice shouldbe a #6 or #8 file.
4. The shaft of the file is widerthan the coronal portion of thecanal. This problem is becauseof the restrictive dentin forma-tion and a natural expression ofcanals calcifying from the crowndown. The solution is to widenthe coronal dentin using theremaining three motions.
SmoothOnce the dentist has reached theradiographic terminus with a #10and then a #15 file, for example,the very next step is to reproducethis path and begin the “glidepath,” which represents a smooth,though perhaps narrow, tunnelfrom the orifice to the electronicportal of exit or the radiographicterminus. Then, and only then, arerotary files predictably safe to use.The smoothing motion is an “inand out” vertical movement usingsmall amplitudes of 1mm until theamplitude is naturally and easily

288
2 0 0 6 E N D O D O N T I C U P D A T E
© 2 0 0 6 , C O P Y R I G H T T H E A U T H O RJ O U R N A L C O M P I L A T I O N © 2 0 0 6 , B L A C K W E L L M U N K S G A A R D
increased because of the wearingaway of the dentinal walls. Thisapproach is dissimilar to “circum-ferential filing” in that the file isnot leaned against one wall andthen another wall. Circumferentialfiling only creates the illusion thatall the walls are actually filed. Inreality, the orifice acts as a fulcrumand the canal is indiscriminatelywidened. In addition, becausecurved stainless steel files havememory, circumferential filing risksapical transportation. The desiredmotion is directly in and out untilthe file can enter from the orificeand follow the smooth canal wallsuninterrupted to the terminus.
BalanceIntroduced by Roane20 and furtherpopularized by Buchanan,21 thismotion is especially effective inremoving coronal dentin. Themotion is simple: first turn the han-dle clockwise one-half to one fullrotation. The dentin is “loaded” inthe file’s blades. With slight, and yetenough, apical pressure that pre-vents the file from unscrewing outof the canal, counter-rotate the fileone-half to two or three full rota-tions. The dentin is “cut” and rest-ing in the flutes of the file’s blades.Always use delicate motions and donot screw the file into the canal.The file is removed using the initialclockwise motion while, at thesame time, withdrawing it. Inspec-tion of the blades under magnifica-tion usually reveals small amounts
of dentin. Remember, endodonticsis not a big job, it is a small job. Itis, however, a smart job. After irri-gation, the same or previous-sizefile that did not easily follow to thedesired depth previously will almostalways now follow deeper. Switchto the follow motion or continuewith balance motion until a wideenough, smooth, and reproducibleglide path is made. Usually, thismeans a #10 or #15 file followseasily to length.
EnvelopeThe envelope of motion isextremely efficient for removingrestrictive dentin, and it is a motionthat requires more restraint thanthe balance motion. It is the onlymotion that does not engage dentinwith the “in” stroke. Envelopeactually carves dentin on the “out”stroke. Specifically, a precurved fileis followed short of maximum resis-tance, then removed while rotatingit in a clockwise direction. Witheach pass the file will easily andpredictably advance deeper into the canal as the restrictive dentin ispassively and yet intentionallyremoved. The shape produced inthe canal is actually determined by the envelope of motion createdby the path of the precurved file asit is withdrawn in the clockwisedirection. The resulting preparation shape is a function of the shape of the original instru-ment modified by its curvaturewithin the canal.
Blocks, Ledges, and TransportationsDuring the manual phase of canalpreparations, there are three mainproblems that can be encountered:blocks, ledges, and apical trans-portations (Figure 8).22 Although itis better to prevent these temporarysetbacks, techniques exist to correctthem.
BlocksThe steps for removing a block are:
1. Remember the path is still there.It is temporarily clogged withthe densest dentin coronally(dentin mud). While it mayappear that the clinician is 2 to3mm short, in fact, he or she ismore likely only a fraction of amillimeter away from the morelightly packed dentin, which canbe negotiated easily once the filehas delicately disrupted thedense coronal dentin mud.
2. Shake your fingers loose.3. Relax.4. Irrigate thoroughly.5. Picture in your mind what it will
look like, feel like, and what youwill be thinking after you suc-cessfully ferrite your waythrough the block.
6. Forget the clock. Act like youhave all the time in the world.
7. Be gentle, gentle, gentle.8. Follow the canal in a random-
ized fashion. Do not search forthe canal direction. Let the canaldo the directing.

W E S T
V O L U M E 1 8 , N U M B E R 5 , 2 0 0 6 289
9. Know that with each pass thefile will advance deeper,although you may not perceiveit at first because the distance isso small. Be patient.
LedgesA ledge is one of the most difficultpreparation errors to overcome.Once created, files and subsequentobturation materials do not easily
bypass the ledge. Correctionattempts were previously made byfirst following a precurved #20 hed-strom file past the ledge and thencircumferentially filing the ledgeuntil the edge of the ledge waspartly worn away. The ledge couldrarely be removed completely. Inaddition, unnecessary and indis-criminate dentin was removed.With the advent of nickel-titanian(NiTi), the ledge can be more easilycorrected while, at the same time,cutting the proper apical taper. Forexample, a manual ProTaper F1 canbe precurved using orthodonticbirdbeak pliers and used to easilyremove the ledge (Figure 8A,B).The curved F1 is guided around theledge and then manually rotatedclockwise. As the file is rotated inan apical direction, the ledge is usu-ally removed and the F1 shape ismade (apical size 20 and 7-degreeapical taper). The cone-fit and subsequent obturation is uneventful.
Transportation. If a terminal fora-men is externally torn (inadver-tently enlarged) and if enough toothstructure remains to properly shapethe canal using the new “super-foramen,” then proceed. If bleedingpersists, intracanal calcium hydrox-ide dressings may be useful. If,however, there is not enough toothstructure to shape, or the canal can-not be dried, a barrier of calciumsulfate or CollaPlug (Sultzer Medica, Plainsboro, NJ, USA) must
A B
C D
Figure 8. Ledges and transportations. A, Straight ProTaper F1 usually cannot predictably bypass a ledge. B, Orthodontic birdbeak pliers can easily curve the ProTaper file, which retains the curve even though made of nickel titaniummetal. The file can then manually slide past ledge, rotated, and remove ledgewhile simultaneously carving a proper apical shape. C, Maxillary central incisorwith necrotic pulp and underformed root. D, Apical barrier is placed, MTAcompacted into canal and restored. Treatment is without the need for gutta-per-cha and can be a single-visit procedure.

290
2 0 0 6 E N D O D O N T I C U P D A T E
© 2 0 0 6 , C O P Y R I G H T T H E A U T H O RJ O U R N A L C O M P I L A T I O N © 2 0 0 6 , B L A C K W E L L M U N K S G A A R D
be placed to act as a backstop forvertical obturation of gutta-perchaor mineral trioxide aggregate(MTA) (Figure 8C,D).
Electronic Apex LocatorsThe length of a root canal hasalways been one of the milestonesof root canal preparation. Researchand clinical experience support theclaim that apex locators can assistin accurately determining canallength in the majority of cases.23–26
In the past, manual shaping couldrequire up to an hour per canal.Lengths of curved canals (the short-est distance between two points is astraight line) would shorten slowlyover that hour. Rotary shaping hassignificantly changed the rate andtime of canal shortening. For exam-ple, a single pass with a rotaryinstrument may shorten a long andcurved canal by 2mm or more.Instead of change that previouslytook an hour will now take only a
few minutes! What this means tothe operator is that canal length isdynamic. To say that a canal is 24-mm long, write it down, and bemarried to that length is a big mistake. This situation is where the electronic apex locator (Figure 9A) has tremendous value,because at any time, the apex locator can be attached to a manually placed rotary file and the length can be adjusted accordingly.
A B C
D E F
Figure 9. Adjuncts for “following” and cleaning root canal systems. A, New Root ZX II. B, EndoIrrigator for precise andconvenient delivery of up to six different irrigants. C, Radicular preparation before removal of smear layer. Note dentinaltubules are covered. D, Smear layer removed using combination of sodium hypochlorite followed by MTAD. (Scanning elec-tron microscope [SEM] images compliments of Dr. Mahmoud Torabinejad, Loma Linda University). E, Before digital radi-ographs, doctor and patient had to squint at a film less than an inch in size and attempt to educate about a tooth’s condition.F, Digital images are easily seen by doctor, staff, and patient. In addition, they can be viewed instantly and are significantlysafer for the patient due to the reduction in radiation.

W E S T
V O L U M E 1 8 , N U M B E R 5 , 2 0 0 6 291
In addition, apex locators can iden-tify perforations resulting frominstrument errors or resorptions,root fractures, and lateral portals of exit. Finally, the use of apexlocators is contraindicated inpatients who have cardiac pacemakers.27
IrrigationIrrigation is a key part of both following and finishing. New andinnovative devices such as theEndoIrrigator (Vista Dental Products, Racine, WI, USA) facili-tate irrigation efficiency (Figure9B). Of all endodontic irrigants,sodium hypochlorite is perhaps themost widely used endodontic irri-gating solution. It effectively digestsdetached and necrotic pulpal tissueand possesses excellent antimicro-bial efficacy. Baumgartner andCuenin, in an in vitro study, foundthat sodium hypochlorite com-pletely removed pulpal remnantsand predentin, even in uninstru-mented surfaces of single canal premolars.28 Ethylenediaminete-traacetic acid (EDTA) removes thesmear layer, which may block thecleaning and obturation of poten-tially significant lateral canals.29–30
Both sodium hypochlorite andEDTA should be alternated formaximum effect. Hydrogen perox-ide is useful in combination withsodium hypochlorite when cleaningand shaping mandibular teeth. Theresulting effervescence elevates“dentin mud” coronally and
therefore reduces the chance ofblocking the canal apically.
More recently, a mixture of tetracy-cline acid, and a detergent (MTAD)(Dentsply Tulsa Dental) has beenintroduced as a 5-minute rinse priorto obturation.31 The MTAD isdesigned to remove possibleremaining smear layer and bacteria(Figure 9C,D).
Regardless of the personal irriga-tion preference, several guidelineswill increase their effectiveness:
1. increase volume2. increase temperature3. agitate4. use combinations5. change solution frequently6. increase contact time7. place irrigating needle closer to
canal terminus
Digital RadiographyLike the microscope, the digitalimage allows the dentist, patient,and assistant to see instantly andclearly.32–35 The image on a stan-dard radiograph will typicallybecome more difficult to read withage (Figure 9E). Making the imagethe size of a computer screen is agreat advantage beyond the educa-tional value to the patient, assis-tant, and dentist (Figure 9F). If thepatient cannot see or understandthe problem, they will often notaccept the solution. Another advan-tage is that instead of waiting for a
conventional radiograph for 2 min-utes or more, the treatment imageappears seconds after taking thedigital radiograph. Instant modifi-cations can be made if film place-ment correction is needed and thedentist keeps flowing with the treat-ment instead of having to keepstopping and starting. Digital radiography has made dental radiography better, safer, and moreefficient.
F I N I S H I N G C A N A L S
Cleaning and ShapingFundamental MechanicsMany new endodontic technologiesare described in this article to makeendodontic success easier and tohave a more predictable outcome.All these advancements arefounded, however, on timelessendodontic biologic and mechanicalprinciples (Figure 10A–C). Just asthere are certain mechanicalrequirements that are prerequisitefor the resistance and retentionform of a restorative full crownpreparation, certain mechanicalrequirements are also prerequisitefor optimal endodontic radicularpreparations. In 1974, Schilder sug-gested that “cleaning and shapingmechanics may be viewed as anextension of the principles of coro-nal cavity preparations to the fulllength of the root canal system.”36
Schilder was the first dentist todescribe the desired mechanicaldesign objectives for cleaning andshaping:

292
2 0 0 6 E N D O D O N T I C U P D A T E
© 2 0 0 6 , C O P Y R I G H T T H E A U T H O RJ O U R N A L C O M P I L A T I O N © 2 0 0 6 , B L A C K W E L L M U N K S G A A R D
4. The apical foramen shouldremain in its original spatialrelationship both to the boneand to the root surface. Themovement or transportation ofthe apical opening is a commonerror in root canal preparation,which leads all too frequently tochronic root canal discomfort oroutright failure in treatment(Figure 11H–K).
5. The apical opening should bekept as small as is practical in allcases (Figure 11L–O).
When all five mechanical objectivesare met, the result truly has “thelook” of excellent finishing (Figure11P).
Glide PathAs previously described, the glidepath in endodontics is represented
by a smooth pathway from the ori-fice to the foramen. This path maybe narrow and it may be curved. Itmay be curved gently or abruptly,particularly in the apical 2 to 3mm.The key word is smooth. Then, andonly then, can nickel titanium filespredictably follow.
A glide path must be created manu-ally with hand files. The problem,however, with hand files is theirrapid and inappropriate increase intip size at D1 (1 mm from the tip ofthe instrument). For example, a size#15 has a 50% larger D1 than a#10 file! It is no surprise that whena #10 file follows easily to the RT, a#15 does not easily reach length aswell. In fact, there is substantialrisk that a blockage or a ledge willbe present after its use. After much
A B C
Figure 10. Classic and timeless principles. A, The two most frequently cited references in endodontics are Schilder’s Novem-ber, 1967 Filling Root Canals in Three Dimensions and his April, 1974 Cleaning and Shaping the Root Canal (Dental Clinicsof North America). B and C, Outstanding examples of endodontic obturation from over 30 years ago! The molar and premo-lar are abutment teeth for the same fixed prosthesis and appeared on page 223 in Dr. John Ingle’s first book titled Endodon-tics in 1965. The treatment was accomplished decades before the microscope and rotary endodontics (courtesy of Dr. HerbertSchilder).
1. The root canal preparationshould develop a continuouslytapering funnel from the rootapex to the coronal access cavity(Figure 11A,B).
2. In compliance with the aboveprinciple, the cross-sectionaldiameter of the preparationshould be narrower at everypoint apically, and wider at eachpoint as the access cavity isapproached (Figure 11C).
3. Unlike funnels of simple geomet-ric design, this root canal prepa-ration should occupy not onlythree planes, but as many planesas are presented by the root androot canal under treatment; thatis, the root canal preparationshould have flow with the shapeof the original canal (Figure11D–G).

W E S T
V O L U M E 1 8 , N U M B E R 5 , 2 0 0 6 293
A B C
E F G
H I J
D
Figure 11. Five mechanical objectives. A, Pretreatment radiograph of a gutta-percha cone tracing the sinus tract to the mesialof tooth #9. B, Objective number 1: continuously tapering cone shape allows successful obturation of one canal and a total oftwo portals of exit (foramina.) C, Mechanical objective number 2: mandibular molar demonstrates objective that states eachcross-sectional diameter should become narrower as the preparation moves apically (courtesy of Dr. Jason West). Mechanicalobjective number 2 facilitates the achievement of objective number 1 and together the two objectives create the hydraulicsneeded for predictable obturation. D, Mechanical objective number 3: the root canal preparation should demonstrate the sameflow as the original canal. D through G illustrate that the instruments flow with the ouginal buccal canals to the radiographictermini followed by the cone-fit and the eventual obturation that successfully replicates the original natural flow of the rootcanal system. H, Mechanical objective number 4 states “do not transport the foramen either internally (block) or externally(tear).” This maxillary right first molar demonstrates both errors. The distobuccal is blocked and the mesiobuccal is torn api-cally. I, Apical anatomy of mandibular molar is blocked and the tooth is symptomatic. J and K, Oblique radiographs show re-treatment result. Six canals were discovered and the tooth promptly became asymptomatic (courtesy of Dr. Jason West).

294
2 0 0 6 E N D O D O N T I C U P D A T E
© 2 0 0 6 , C O P Y R I G H T T H E A U T H O RJ O U R N A L C O M P I L A T I O N © 2 0 0 6 , B L A C K W E L L M U N K S G A A R D
K L M
N O P
Figure 11. cont’d L, Mechanical objective number 5 states to keep the foramen as small as is practical. Pretreatment filmshows presence of a periradicular radioluceny. M, If there is enough tooth structure to make a continuously tapering shape, anappropriate cone-fit is possible. N, Posttreatment. O, 9-month healing. P, Radiographic evidence of achieving all five mechani-cal objectives (courtesy of Dr. Jason West).

W E S T
V O L U M E 1 8 , N U M B E R 5 , 2 0 0 6 295
effort, the block or ledge may beremoved, only to have the problemamplified further with a #20 file,which is incontinently 33.3% widerat D1 than a #15 file. It is as if thesystem was sabotaged from thebeginning. In order to solve thisproblem, Dentsply Tulsa Dental,with the late Dr. Herbert Schilder’sguidance, introduced the Series 29.The first three files (#1, #2, and #3)are particularly helpful for develop-ing a smooth glide path in a calci-fied canal. Each tip size has a D1that is 29% larger than the
previous instrument in the series.Clinically, this translates that if a #1 file follows easily to the termi-nus then a #2 and then a #3 file willeasily follow to the terminus. Atthis point, rotary files can confi-dently and safely be introduced.
Recently, a new glide file has beenintroduced, known as the SinseusProFinder glide path file (Maieffer,Ballaigues, Switzerland) (Figure12A). The ProFinder increases inD1 diameter in a logical progres-sion similar to the 29 series, with
the added advantage of reverse progressive geometries similar toProTaper finishers. The resultingglide path preparations reflect theclassical and time-tested Schildercleaning and shaping principles ofprogressive shaping (serial reamingand filing), recapitulation (thesequential re-entry of all previousfiles), and cleaning and shaping tothe RT (patency). The ProFinderhandles are made of silicone, whichincreases tactile sensitivity.
Connecting the DotsWith the aid of an endodonticmicroscope, coaxial light, andknowledge of the root canal systemanatomy, most clinicians can findmost canal orifi. With small pre-curved instruments, irrigation, andthe added ingredient of restraint,most canals can be successfully fol-lowed to their terminus. In actual-ity, dentists can “rough out” thebasic radicular shape. However, thechances of making consistentlysmooth and continuously taperingcanal walls from access to the rootcanal system terminus were slim. Itwas not until viewing the final radi-ographs that the clinician even trulyknew the outline form. It was thenthat the outline form was literally“discovered.” In a multirootedtooth, the chances of making all thewalls smooth was even less. Essen-tially, only one dimension out of apotential 360 degrees of dimensioncan be measured in a two-dimensional radiograph.
A B
C D
Figure 12. New technologies for cleaning and shaping. A, Senseus glide file withsilicone handle. B, Six-pack ProTaper rotary files consisting of three shaping filesand three finishing files. C, System-based ProTaper kit including electric motor,rotary and manual files, and matching gutta-percha cones and obturators. D, SEMdemonstrating critical distinction of efficient cutting blades (below) and laboriousplaning blades (above).

296
2 0 0 6 E N D O D O N T I C U P D A T E
© 2 0 0 6 , C O P Y R I G H T T H E A U T H O RJ O U R N A L C O M P I L A T I O N © 2 0 0 6 , B L A C K W E L L M U N K S G A A R D
Endodontics needed a way to “con-nect the dots” of the “roughed out”canal so that the walls would besmooth and enable good obturationhydraulics throughout the prepara-tion length and width. Because clini-cians cannot crawl into the rootcanals, something was needed to doit for them. If necessity is themother of invention, it is no surprisethat NiTi solved what seemed to bean insurmountable need in shapingmechanics. This remarkably strongand flexible exotic metal has pro-duced positive results that areimpossible with stainless steel.
It is estimated that there are at least18 different rotary file brands in theendodontic marketplace. They varyin tapers, number and types ofblades, tip design, and number offiles in a series. It is paramount tofollow the direction for use of eachseries because they are markedlydifferent. Most breakage of rotaryfiles, regardless of the manufac-turer, is because the dentist failed tofollow the directions for that partic-ular file. It has been said that everydentist is capable of breaking everyrotary file. The greatest variable,therefore, is not the file; it is, asalways, the clinician. To increasesafety, most endodontic teachersand educators emphasize sufficientsupervised training by endodontiststhat have mastered any particularsystem. These skills should bedeveloped using extracted teeth, notlive patients! The following are
strict guidelines to maximize NiTirotary file safety:
1. Always have a “glide path”before rotary instruments areused.
2. Never force a rotary file at anytime.
3. Start each patient treatmentwith new files.
4. Bathe the root canal system inEDTA during rotary radicularcavity preparation.
5. Frequently inspect file flutesunder magnification.
6. Clean flutes each time the file isremoved from the canal.
7. Use an electric torque controlmotor at 220 to 300 rpm and at90% torque.
One rotary concept, the ProTaperEndodontic System, like the GT(greater taper) System (both fromDentsply Tulsa Dental), is a com-prehensive solution built aroundthe exceptional efficiency of theProTaper nickel titanium rotary and manual files (Figure 12B–D).Each element of the system works together to intuitively generate a seamless flow fromcleaning and shaping to three-dimensional obturation. Like theGT system, each ProTaper obturator and ProTaper gutta-percha cone matches the shape created by its corresponding ProTaper finishing file. Each ProTaperabsorbent point matches the corresponding finisher.
NiTi rotary files coupled with theendodontic microscope are the twobiggest and best things to happen toendodontics in the last 100 years.Neither is magic by itself. Skillsmust be developed and thoroughly rehearsed before use.The reward is consistency and arenewed feeling of confidence andcompetence.
Electronic Endodontic MotorsThe introduction of endodonticelectric torque control motors hasincreased rotary safety and pre-dictability. The DTC electric motor(Dentsply Tulsa Dental), for exam-ple, has a lightweight handpieceand is durable.
ObturationIn a survey conducted for the 2002American Association of Endodon-tists national annual meeting, thescientific advisory board for theJournal of Endodontics, the direc-tors of the graduate schools in theUnited States and Canada, and“valued and respected” endodonticclinicians all agreed that the qualityof obturation was the hallmarkdeterminant of endodontic clinicalexcellence.37 Currently, the mosteffective and well-documented,time-tested obturation systems arethe vertical compaction of warmgutta-percha techniques (multiwaveor classic Schilder vertical conden-sation, single-wave or continuous-wave, and carrier-basedobturation). These methods have

W E S T
V O L U M E 1 8 , N U M B E R 5 , 2 0 0 6 297
the capacity to successfully distortsymmetrical gutta-percha intoasymmetrical foraminal constric-tions while at the same time reduc-ing the gutta-percha/dentininterface so that it is as narrow aspossible (Figure 13A,B). New tech-nologies in thermoplastic obtura-tion have made these proceduressafer, easier, and better (Figure13A). Vertical compaction tech-niques use heat sources for boththeir downpack and backpack obu-ration (Figure 13B,C). Gutta-perchatechniques exhibit an extremelyhigh success rate when large patientpopulations are carefully evaluated.
For example, initial nonsurgicalendodontics are reported to have a97% success rate over a period of 8years.38 Gutta-percha also requiresa coronal seal to be successful.39–44
The simple solution to overcomeany coronal to radicular leakageconcern is to place a coronal seal atthe time of obturation. This sealcan easily be achieved by first stop-ping the backpacked gutta-percha 1mm below the chamber floor of thecanal orifice. The gutta-percha andchamber floor then can be restoredwith glass ionomers, flowable com-posites, IRM, zinc phosphate, amal-gam, ZOE, etc.
Recently, dentin bonding technol-ogy has become a possibility forendodontic obturation.45 As withmany new materials or techniques,early literature citations and scien-tific presentations are reportingconflicting results. The inventorsclaim to use a biocompatible resinas a sealer and an obturator of resinfiber creating an intimate bond ofResilon (Pentron Clinical Technolo-gies, Wallingford, CT, USA),sealant, and dentin. Resilon is ahigh-performance industrialpolyurethane. The new obturationproduct consists of a resin conematerial (Resilon), which is
A B
D E
C
Figure 13. New technologies for obturation. A, Arrows point to gap between gutta percha and dentin in horizontal root sec-tion of an endodontic obturation. B, In a different horizontal section, arrows indicate extremely tight gutta percha-dentininterface, which minimizes reliance on endodontic sealer. C, Matching finishing files, paper points, and gutta cones. D, SystemB heat source (SybronEndo) for the continuous wave obturation technique. E, Calamus flow unit (Dentsply Tulsa Dental) forthermoplastic obturation techniques and for backpacking during the vertical compaction of the warm gutta-percha technique.

298
2 0 0 6 E N D O D O N T I C U P D A T E
© 2 0 0 6 , C O P Y R I G H T T H E A U T H O RJ O U R N A L C O M P I L A T I O N © 2 0 0 6 , B L A C K W E L L M U N K S G A A R D
composed of polyester, difunctionalmethacylate resin, bioactive glass,and radiopaque fillers and a resinsealer. Resilon is reported to benontoxic, nonmutagenic, and bio-compatible. Resilon is similar togutta-percha, which is 35% rubberand 65% fillers. Resilon is 35%polyester resin and 65% fillers. Oneof the pioneers of a possible gutta-percha substitute idea is Dr. MartinTrope, who rightfully is also con-cerned about the same bacterialpenetration that a good restorativecoronal seal is designed to solve.Dr. Trope writes,
Although sealers can form closeadhesion to the root canal wall,none is able to bond to the gutta-percha core material. Upon setting,the sealer pulls away from thegutta-percha core, leaving a gapthrough which bacteria may pass.This article describes a new thermo-plastic, synthetic root canal fillingmaterial, whose design is based onpolyester chemistry, that looks andhandles like gutta-percha. It is usedin the same manner as most bond-ing systems. After the usual prepa-ration of the root canal, a self-etchprimer is used to condition thecanal walls and prepare them forbonding to the resin. The resinsealant is introduced in the rootcanal. It bonds to the primer and tothe resin core material; thus, a“monoblock” is formed withoutthe gaps typical in gutta-percha fillings.46
This author is currently recallingover 100 cases of record whereResilon was the obturation mater-ial. Therefore, due to multirootedteeth, approximately 300 canalswill be evaluated over 2 years afterobturation. No further cases havebeen obturated with Resilon untilthe study is complete. As with anynew material, they must be testedand the results measured in clinicalpractice. This retrospective studywill be submitted for publicationafter completion. While the systemresembles gutta-percha and can beplaced using single cone, lateralcondensation, thermoplastic injec-tion, or warm vertical compaction,using Resilon in the “vertical com-paction of warm Resilon” multi-and single-wave approach didrequire modification of technique.Resilon heat wave is shorter inlength and duration.
S U M M A R Y
Instruments, materials, and technol-ogy are in constant change. Manycome and go with time. Principlesare more timeless. In this regard,endodontics is no different fromother dental disciplines. The ethicaland responsible dentist must learnif these changes help attain and exe-cute the fundamental successfulprinciples better, easier, and/orsafer. This article has discussed thekey points of a changing field thatneed to be understood when treat-ing patients who have endodonticdisease.
D I S C L O S U R E A N D
A C K N O W L E D G M E N T S
As a co-inventor, the author has afinancial interest in the ProTaperEndodontic System (Dentsply TulsaDental).
This article is dedicated to the lateDr. Herbert Schilder—mentor andfriend. Most of the state-of-the-arttechnologies reviewed in this 2006Endodontic Update were inspiredby Schilder’s discovery of timelessbiologic principles and his visionfor masterful endodontics.
R E F E R E N C E S
1. Spear F. Facially Generated TreatmentPlanning. Presented at the American Acad-emy of Esthetic Dentistry 16th AnnualMeeting, August 8, 1991, Santa Monica,CA.
2. West J, Roane J. Cleaning and shaping theroot canal system. In: Cohen S, Burns RC, editors. Pathways of the Pulp, 7th ed. St. Louis (MO): Mosby;1998. p. 204.
3. Carr GB. Ultrasonic root end preparation. Dent Clin North Am1997;41:541–61.
4. Ruddle CJ. Micro-endodontic nonsurgicalretreatment. Dent Clin North Am1997;41:429–54.
5. West J. The role of the microscope in 21st century endodontics: visions of anew frontier. Dent Today 2000;19(12):62–9.
6. Rubinstein RA, Kim S. Long-term follow-up of cases considered healed one yearafter apical microsurgery. J Endod2002;28:378–83.
7. Schwarze T, Baethge C, Stecher T, Geurtsen W. Identification of secondcanals in the mesiobuccal root of maxil-lary first and second molars using magni-fying loupes or an operating microscope.Aust Endod J 2002;28(2):57–60.

W E S T
V O L U M E 1 8 , N U M B E R 5 , 2 0 0 6 299
8. Buhrley LJ, Barrows MJ, BeGole EA,Wenckys CS. Effect of magnification onlocating the MB2 canal in maxillarymolars. J Endod 2002;28:324–7.
9. Shanelec D. Anterior esthetic implants:Microsurgical placement in extractionsockets with immediate provisionals. CDAJ 2005(November);33:233–40.
10. Shanelec D. Magnification in periodontics.J Esthet Restor Dent2003;15(7):402–7,discussion 408.
11. Shanelec D. Current trends in soft tissuegrafting. CDA J 1991;20(Decem-ber):57–60.
12. Friedman MJ, Landesman HM. Micro-scope assisted precision dentistry—advanc-ing excellence in restorative dentistry.Contemp Esthet Restor Prac 1997;1(1).
13. Friedman MJ, Landesman HM. Micro-scope assisted precision (MAP) dentistry—a challenge for new knowledge. CDA J1998;26(2):900–5.
14. Dental Alumni News. The University ofWashington Dental Alumni Association2005;31(2):38.
15. Levin H. Access cavities. Dent Clin NorthAm 1967;11:701–10.
16. von Arx T, Walker WA 3rd. Microscopeinstruments for root-end cavity prepara-tion following apicoectomy: a literaturereview. Endod Dent Traumatol2000;16(2):47–62.
17. Stropko J. Canal morphology of maxil-lary molars: clinical observations of canalconfigurations. J Endod1999;25(6):446–50.
18. Budd JC, Gekelman D, White JM. Tem-perature rise of the post and on the rootsurface during ultrasonic post removal. IntEndod J 2005;38:705–11.
19. West JD. Finishing: the essence of excep-tional endodontics. Dent Today2001;20(March):36–41.
20. West JD, Roane JB. Cleaning and shaping the root canal system. In: CohenS, Burns. RC, editors. Pathways of thepulp, 7th ed. St. Louis (MO): Mosby;1998. 244–8.
21. Buchanan LS. Cleaning and shaping theroot canal system: instrument selection
and usage. Dent Today1994;13(March):4–10.
22. West J. Perforations, blocks, ledges, and transportations: overcoming barriers to endodontic finishing. Dent Today 2005;24(January):68–73.
23. Dunlap CA, Remeikis NA, BeGole EA,Rauschenberger CR. An in vivo evaluationof an electronic apex locator that uses theratio method in vital and necrotic canals. J Endod 1998;24(1):48–50.
24. Fouad AF, Krell KV, McKendry DJ, et al.Clinical evaluation of five electronic rootcanal length measuring instruments. J Endod 1990;16(9):446–9.
25. Fouad AF, Reid LC. Effect of using elec-tronic apex locators on selected endodon-tic treatment parameters. J Endod2000;26(6):364–7.
26. Shabahang S, Goon WWY, Gluskin AH.An in vitro evaluation of Root ZX elec-tronic apex locator. J Endod1996;22:616–8.
27. Garofalo RR, Ede EN, Dorn SO, KuttlerS. Effect of electronic apex locators on car-diac pacemaker function. J Endod2002;28(12):831–3.
28. Baumgartner JC, Cuenin PR. Efficacy ofseveral concentrations of sodiumhypochlorite for root canal irrigation. J Endod 1992;18:605–12.
29. Peerez F, Rouqueyrol-Pourcel N. Effect of low-concentration EDTA solution onroot canal walls; a scanning electronmicroscope study. Oral Surg Oral MedOral Pathol Oral Radiol Endod2005;99:383–7.
30. Kokkas AB, Boutsioukis ACH, Vassiliadis LP, et al. The influence of thesmear layer on dentinal tubule penetrationdepth by three different root canal sealers: an in vitro study. J Endod2004;30:100–2.
31. Torabinejad M, Shabahang S, Bahjri K.Effect of MTAD on postoperative discom-fort: a randomized clinical trial. J Endod2005;31:171–6.
32. Hellen-Halme K, Rohlin M, Petersson A.Dental digital radiography: a survey ofquality aspects. Oral Surg Oral Med OralPathol Oral Radio Endod2005;99(4):499–504.
33. Woolhiser GA, Brand JW, Hoen MM, et al. Accuracy of film-based, digital, andenhanced digital images for endodonticlength determination. Quintessence Int2005;36(1):65–70.
34. Erten H, Akarslan ZZ, Topuz O. The effi-ciency of three different films and radio-visiography in detecting approximalcarious lesions. J Am Dent Assoc2004;135(10):1437–9.
35. Farman AG, Farman TT. A comparison ofl8 different x-ray detectors currently usedin dentistry. Oral Surg Oral Med OralPathol Oral Radiol Endod2005;99(4):485–9.
36. Schilder H. Cleaning and shaping the root canal. Dent Clin North Am1974;18:269–96.
37. West J. Finishing: The Essence of Excep-tional Endodontics. Presented at theAnnual AAE Meeting, April 2002, NewOrleans, LA.
38. Salehrabi R, Rotstein I. Endodontic treat-ment outcomes in a large patient popula-tion in the USA: epidemiological study. J Endod 2004;30:846–50.
39. Torabinejad M, Shabahang S, KetteringJD. In vitro bacterial penetration of coro-nally unsealed endodontically treatedteeth. J Endod 1990;16:566–9.
40. Welch JD, Anderson RW, Pashley DH, et al. An assessment of the ability of various materials to seal furcation canals in molar teeth. J Endod1996;22:608–11.
41. Roghanizad N, Jones JJ. Evaluation ofcoronal leakage after endodontic treat-ment. J Endod 1996;22:471–3.
42. Ray H, Trope M. Periapical status ofendodontically treated teeth in relation tothe technical quality of the root filling andthe coronal restoration. Int Endod1995;28:12–18.
43. Pisano DM, DiFiore PM, McClanahan SB,et al. Intraorifice sealing of gutta-percha obturated root canals to prevent coronal leakage. J Endod1998;24:659–62.
44. Torabinejad M, Ung B, Kettering JD. Invitro bacterial penetration of coronallyunsealed endodonically treated teeth. J Endod 1990;16:566–9.

300
2 0 0 6 E N D O D O N T I C U P D A T E
© 2 0 0 6 , C O P Y R I G H T T H E A U T H O RJ O U R N A L C O M P I L A T I O N © 2 0 0 6 , B L A C K W E L L M U N K S G A A R D
45. Johnson WT, Gutmann JL. Obturation ofthe cleaned and shaped root canal systemIn: Hargreaves KM, Cohen S, editors.Pathways of the pulp, 9th ed. St. Louis(MO): Mosby; 2006. p. 372–5.
46. Teixeira FB, Teixeira EC, Thompson J, et al. Dentinal bonding reaches the root canal system. J Esthet Restor Dent 2004;16(6):348–54, discussion 354.
Reprint requests: John West, DDS, MSD,48801 S. 19th Street, Tacoma, WA 98405;email: [email protected]
©2006 Blackwell Publishing, Inc.