Embed Size (px)
Citation preview
QUANTITATIVE STUDIES OF PULMONARY EMBOLISM
By LEWIS DEXTER, M.D., AND (by invitation) GEORGE T. SMITH, M.D.
BOSTON, MASSACHUTSETTS
For decades there has been suspicion that a single small embolus canproduce sudden death by producing widespread pulmonary vasocon-striction. One of our meimbers, Dr. Gorhamn, has examnined this problemexhaustively.' Many have doubted that such could occur. On the otherhand, it has been recognized since the 1920's2 that the cross-sectionalarea of the main pulmonary artery Imlust be reduced by over 50% beforeany change of pressure or flow in the lungs occurs. Pneumonectomy orballoon occlusion of one main branch of the pulmonary artery or ligationof 3 of the 7 lobar branches has no effect on pressure or flow through thelung. No quantitative information has been obtained regarding the cir-culatory response to emiibolization of smaller arteries and arterioles ex-perimnentally and little information is available regarding the quantityof thrombo-embolic material present in the lungs of patients dying ofembolism. This problemn has been re-investigated in animals and man inthe following fashion.
Polystyrene spheres were passed througlh sieves so as to imatch their(liameter to the diamieter of pulmonary arteries varying in size between5 (lobar arteries) and 0.17 mm (atrial arteries) in dogs weighing approx-imately 8 kg. These spheres were suspended in saline and injected intothe right atrium. The number requiredl to produce a 5 to 10 mm.Hg riseof pressure in the pulinonary artery was recorded, this rise representingthe first sign of circulatory embarrassment. The results are shown inTable 1. It is seen that the number of emboli required was somewhatgreater than the number of vessels of that same size. Small numbers ofeinboli were required for large vessels, large numbers for small arteries.In no instance was the number of emboli strikingly less than the numberof vessels of that same size to suggest reflex constriction. In other words,no evidence of reflex constriction was noted as a result of emibolizingarterial vessels.
Arterioles wviere occluded by injecting lycopodium spores which are
From the Depar-tments of Medicine andl Palthology, Peteir Bent Brighlanm Hospitalan(d Harvard Medical School, Boston, Massachusetts.
Tlhis work was Sul)pOrted in par-t by Grants from the Life Insurance Medical Re-,search Fund, The National Heart Institute, l. S. Publie Healtlh Service (Grants H-450,HTS-5234, HTS-5550, and HE-6370), and the American Heart Association.
71
L. DEXTER AND G. T. SMITH
TABLE 1Number of Emboli Required to Produce Pulmonary Hypertension
Artery
Lobar ..................1st order...............2nd order..............3rd order..............Lobular ................Atrial ..................
Diameter of arteryand emboli mm.
5.04.02.31.00.30.17
Number of arteries
81243
1,02116,00064,000
regularly 28-30 ,u in diameter. These plug the entrance to capillaries atthe exit of arterioles but never pass through capillaries. Estimates of thenumber of capillaries in the lung have varied between 600 million and 277billion3' 4. An average of only 22 million spores was required to produceincipient pulmonary hypertension in these experiments. This discrepancybetween number of emboli and number of vessels suggests a vasocon-
strictive component in response to micro-embolism and confirms thefindings of Bernthal, Horres, & Taylor5 who clearly demonstrated pul-monary vasoconstriction from arteriolar emboli in an isolated perfusedlung.The lungs of patients dying of pulmonary embolism have been studied
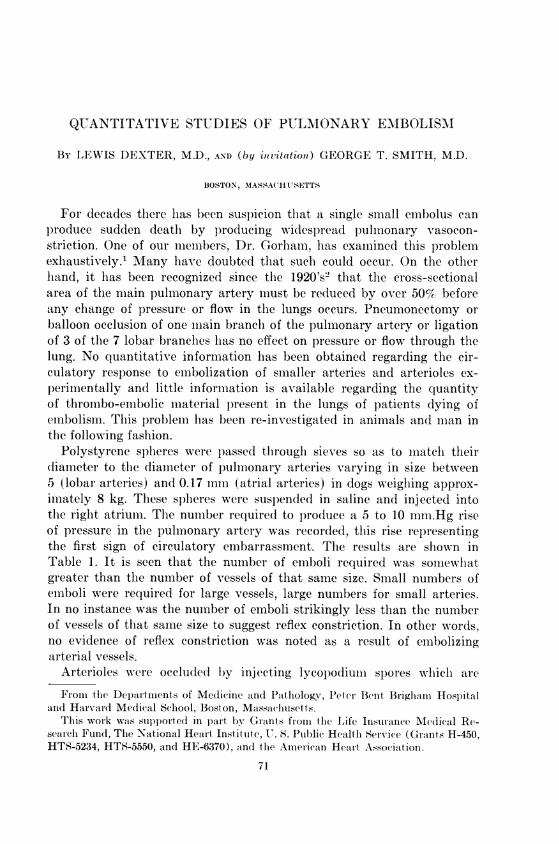
at autopsy. Lungs were excised en bloc, the pulmonary arteries were in-jected with modified Schlessinger mass at a pressure of 30 mm.Hg or more
until the superficial arteries on the surface were filled. This material fillsthe arterial vessels to a diameter of 0.1 mm. but does not enter capil-laries. X-rays of the lung were then taken. Using the x-rays as a road-map to locate emboli, whole lung sections were prepared and examinedhistologically. The distribution of emboli was thus recorded.Table 2 shows the distribution of emboli in the lungs of 34 patients so
studied. It is seen that only 8 lungs had emboli in large elastic arteries.These might have been detected at routine autopsy. Most of the emboliwere found in muscular arteries 0.1 to 1.0 mm. in diameter. These vessels
TABLE 2Location of Emboli in 34 Human Lungs
Arteries
Elastic .................
Muscular ..............
Arterioles ..............
Size, mm. No. of cases Frequency
>1.0 8 Few0.1-1.0 34 Common0.03-0.1 13 Rare
Number of emboli
72860
1,60020,00090,000
72
QUANTITATIVE STUDIES OF PULMONARY EMBOLISM
TABLE 3Arterial Volume of Human Lungs
NormalRight ........................Left ..........................
EmbolizedRight ........................Left .........................
No. of cases
1214
1026
Arterial volume ml/sq. m.
62 i 3.355 4 4.0
21 + 9.822 4i 11.6
cannot be dissected grossly nor can these emboli be recognized with thenaked eye. On routine autopsy these widespread embolic occlusions wouldhave been missed. Only 10% of these occlusions gave rise to infaretshistologically and much fewer clinically. Despite careful search, arteriolarocclusions were rare. Thus, the distribution of emboli was analogous tothe arterial rather than arteriolar embolization in the dog experiments.The volume of embolic material in these lungs was assessed indirectly
by measuring the volume of Schlessinger mass required to fill the arterialtree. The results are shown in Table 3 which shows that arterial volume
FIG. 1. Arteriogram of a normal human lung. Note the long large vessels, extensivebranching, and feathery appearance extending out to the pleural surface.
73
L. DEXTER AND G. T. SMITH
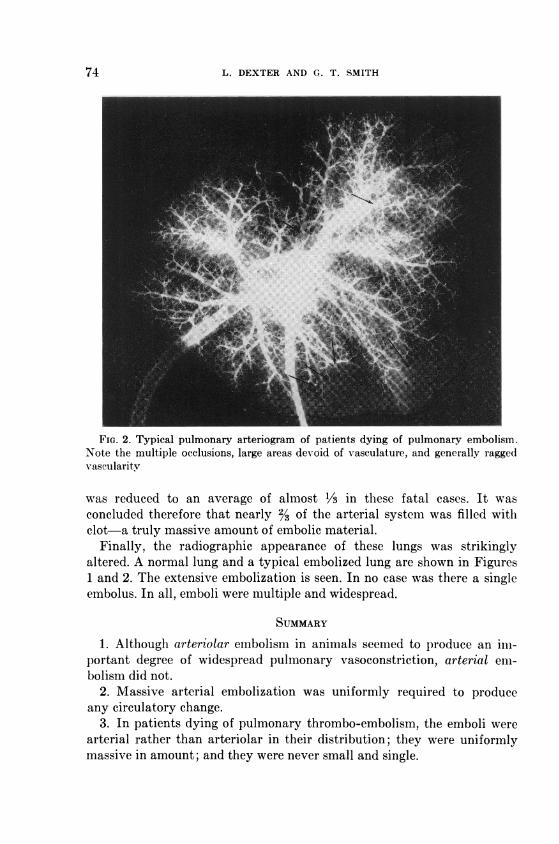
FIG. 2. Typical pulmonary arteriogram of patients dying of pulmonary embolism.Note the multiple occlusions, large areas devoid of vasculature, and generally raggedv-ascularitv
was reduced to an average of almost 1/3 in these fatal cases. It wasconcluded therefore that nearly 23 of the arterial system was filled withclot-a truly massive amount of embolic material.
Finally, the radiographic appearance of these lungs was strikinglyaltered. A normal lung and a typical embolized lung are shown in Figures1 and 2. The extensive embolization is seen. In no case was there a singleembolus. In all, emboli were multiple and widespread.
SUMMARY1. Although arteriolar embolism in animals seemed to produce an im-
portant degree of widespread pulmonary vasoconstriction, arterial em-bolism did not.
2. Massive arterial embolization was uniformly required to produceany circulatory change.
3. In patients dying of pulmonary thrombo-embolism, the emboli werearterial rather than arteriolar in their distribution; they were uniformlymassive in amount; and they were never small and single.
74

QUANTITATIVE STUDIES OF PULMONARY EMBOLISM 75
4. Although one cannot deny the possibility of an element of wide-spread vasoconstriction in human thrombo-embolism, this study does notsupport such a concept. The arterial distribution and massiveness ofembolic occlusion were quite sufficient to attribute death to mechanicalplugging.
REFERENCES
1. GORHAM, L. W.: Arch. Int. Med. 108: 189, 19612. HAGGART, G. E. AND WALKER, A. M.: Arch. Soirg. 6:1, 19233. MILLER, W. S.: J. Morphol. 8: 165, 18934. WEIBEL, E. R. AND GOMEZ, 1). M.: Science 137: 577, 19625. BERNTHAL, T., HORRES, A. 1). AND TAYLOR, J. T. I11: An. J. Physiol. 200: 279, 1961
DISCUSSIONDR. L. WHITTINCTON GORHAM (New York): The mechanism of death in pulmonary
embolism has been a question which has been widely investigated and has evokedmany different theories as to the possible cause.
The mechanical theory is pretty well accepted now for massive embolism when theconus, or the right and left branches of the pulmonary artery are involved. Althoughsome textbooks have said "the larger the embolus, the larger the infarct", nothingcould be further from the truth because there is no infarction in massive embolization.
After a rather prolonged study from the clinical and pathological side at the NewYork Hospital Cornell Medical School I came to approximately the same conclusionthat Dr. Dexter has, that reflex constrictor effects were probably very few in number.If a careful study were made, you would find probably less than 5 per cent of all casesof sudden death in pulmonary embolism, with the major branches free, which mightbe due to vasoconstriction. Some investigators have said there must be either a pul-mono-coronary or a pulmono-pulmonary reflex operating in such cases. The first pos-sibility is pretty well ruled out, because the vagal fibers to the coronary arteries havebeen shown to be dilators and not constrictors. However the second possibility ofvasoconstriction occurring throughi a pulmono-pulmonary reflex cannot be excluded. Itis supported by many investigators, so thiat the importance of this report today cannotbe exaggerated.
Dr. Dexter has introduced a quantitative method of evaluation measuring what thetotal arterial obstruction should be. In the early (lays the pulmonary surgeons werev-ery worried that in removing one lung they would produce a reflex that would causedeath. That was soon proven false because many lungs were removed by operationwithout death. I would like to ask, in closing this discussion, just two questions of Dr.Dexter:
Of these thirty-four patients with minor embolisms in which the main branches werefree, what number of them died suddenly with the clinical symptoms and signs of mas-sive pulmonary embolism? What percentage of them were diagnosed correctly?
And, two, would he say that there still is a possibility that there may be a humoralfactor, such as serotonin, for example, which is known to be a great elevator of thepulmonary pressure, and which may come from blood platelets? (Applause).
DR. DEXTER: Sorry, I can't tell you how many had sudden death. I would have tolook over the protocols.
The number who were diagnosed correctly were about half. I believe that this hasbeen due to the measurement of LDH and SGOT for helping in the diagnosis. These
L. DEXTER AND G. T. SMITH
enzyme changes are now being measured routinely on anyone in whom the slightestsuspicion of embolism exists. This has increased diagnostic acumen considerably at theBrigham. However, there are still many cases that we miss and to me diagnosis stillremains a big problem.You raise the question of humoral factors, particularly serotonin. It has been sug-
gested that serotonin is released by platelets as they lodge in the lungs. I cannot denythe possibility. I do not know of any definitiv-e evidence indicating it to be a factorbut I cannot deny that it may occur. I think it remains to be proven.
In this presentation, I have been referring to thrombo-embolism. Other types ofemboli do indeed occlude arterioles and even traverse the pulmonary capillaries andlodge in brain, kidneys, and other organs. I refer to bone marrow emboli, fat emboli,air emboli, fibrin emboli an(l amniotic fluid emboli. In these, there well may be a power-ful vasoconstrictor response in contradistinction to thrombo-embolism in which v-aso-constriction does not appear to play any significant role.
DR. JOHN T. KING (Baltimore): A number of years ago some of our members hadgotten to the point where they were over-diagnosing pulmonary embolism as againsta diagnosis of pneumonia. That hasn't occurred yet in Baltimore. For some reason wehang on to the diagnosis of pneumonia in some of the acute episodes of the lungs thatI am sure are embolism and lung infarction. Just recently a case came to my attentionin which a gentlemen had had four attacks of broncho-pneumonia in two years. He hadhad antibiotics at home, the disease had run its course, and finally he got into a hos-pital, where difficulty with his left posterior tibial veins, which seem to be a red devilin pulmonary embolism, was perfectly obvious. X-rays of this man's chest showed thathis heart, which had been operated on before, had increased suddenly about 3 centi-meters in transverse diameter. The man recovered, but he had treatment after treat-ment.
It occurred to me that the acute change in heart size might be on the basis of oneof the ideas of the late Aubrey Hampton, who was one of your Boston x-ray specialistsand who was very much interested in this study. He used to say that an acute increasein the transv erse diameter of the heart with sudden prostration was the most reliablex-ray ev-idence of pulmonary embolism. He considered it more reliable than what youlcan see in the lung parenchyma itself. It occurs to me that one of the things that mightenter into this argument about whether a person lives through a pulmonary embolismor not depends on what kind of a heart he has to begin with. The patient that I justquoted to you had had a coronary occlusion some years before.
DR. DEXTER: I understand you to say that one of the problems in making a diag-nosis of pulmonary embolism is that the patients who are particularly prone to haveemboli are those who already have some heart trouble. I agree with you completely.Frequently the only manifestations of the embolism are that they have a little morefailure than they had before. Sometimes it is dramatic as you say. At other times theonly manifestations of embolism are that patients decompensate to a variable extentwithout apparent cause.
Diagnosis of embolism may be positive, probable, or possible. Only occasionally canI make a "positive" diagnosis and if I await definite manifestations, I miss many diag-noses. I over-diagnose the condition if it is at the "possible" level. I try to intervenetherapeutically at the "probable" and "positiv-e" levels rather than at the "possible".
DR. THORNTON SCOTT (Lexington, Kentucky): If I remember correctly, in the latethirties Dr. DeTakats pointed out that in pulmonary embolism there is intense bron-chial as well as arterial spasm. He also demonstrated that this effect, and also fatality,could be blocked by large doses of atropine and papaverine. Secondly, he demonstrated
76
QUANTITATIVE STUDIES OF PULMONARY EMBOLISM 77
that there is a considerable discrepancy between the fatality of embolism in the un-anesthetized and the anesthetized animal. It seems to me that most patients consideredas having pulmonary embolism are not under anesthesia at the time of the attack andthat pulmonary embolism occurring while under general anesthesia is very rare. I won-der if Dr. Dexter could comment on these points.
DR. DEXTER: In our animals we carried out a number of experiments without generalanesthesia. The number of spores and the number of spheres required to produce a riseof pulmonary arterial pressure was identical in the unanesthetized and the anesthetizedanimal.
With respect to embolism in patients with and without anesthesia, I cannot say vervmuch except that most of the manifestations of embolism would be masked by anes-thesia, making diagnosis even more difficult that it ordinarily is.An extremely difficult case with which I was once confronted was a boy with polio
in an iron lung. Respiratory change is one of the most reliable clues to the diagnosisof pulmonary embolism and, of course, his breathing was governed by the iron lung.
The same diagnostic problem would occur in patients during anesthesia. On theother hand, I cannot recall anesthetized patients who had evidence of pulmonary em-bolism on awakening. The usual time for occurrence is 5 to 7 days post-operatively.
I cannot throw any light on Dr. DeTakats' original suggestions. Our experience isnot in accord with his.
DR. CARL MUSCHENHEIM, (New York): I would like to ask Dr. Dexter if he knowsanything about the feasibility of selective angiography in the diagnosis of pulmonaryembolism. Dr. Israel Steinberg has been studying this and I don't think he has studiedenough to arrive at any valid conclusion, but I wondered if you have any experiencewith it.
DR. DEXTER: We have had some experience but not very much. We have been a bitdisappointed. Pulmonary angiography has been carried out by two men, (Dr. O'Connorand Dr. Ryan) in the radiology department at the Brigham. In the upright position,most of the pulmonary blood flow normally goes to the lower lobes and much less tothe upper lobes of the lung. Likewise, emboli lodge preferentially in the lower lobes.You might think that clear pictures similar to the arteriograms I have just shown mightbe obtained. So far we have been rather disappointed using routine angiocardiography.On the other hand, selective angiography, which we are just beginning to use, is muchbetter. However, as I have emphasized, most of these emboli are in the small musculararteries which are very difficult to visualize by current angiographic techniques. On theother hand, embolic obstructions in the larger vessels can be readily detected.
DR. A. MCGEHEE HARVEY, (Baltimore): Dr. H. N. Wagner and Dr. David Sabiston,of Baltimore, have developed a technique now of lung scanning after injecting aggre-gated human serum albumen tagged with I.3. which lodges in the small pulmonaryvessels. In dogs with experimental pulmonary embolism, they outline clearly the oc-cluded areas. This technique has been used in man and they have been able to providethe surgeon with information regarding the exact site of embolic occlusion.



![Fast Food: Regulating Emergency Food Aid in Sudden-Impact ... · 2007] fast food 1131 eruptions can also result in food needs due to widespread destruction of crops.14 Earthquakes](https://img.pdfslide.us/doc/110x75/5f0eb0677e708231d4407405/fast-food-regulating-emergency-food-aid-in-sudden-impact-2007-fast-food-1131.jpg)











![Oliver Strange - Sudden Westerns 06 - Sudden Gold-Seeker(1937)[1]](https://img.pdfslide.us/doc/110x75/54fae2e44a7959575b8b4b9b/oliver-strange-sudden-westerns-06-sudden-gold-seeker19371.jpg)