-
7/29/2019 Process of Motor Development
1/33
Process of motor development
Motor development typically occurs in an orderly sequence from
head to trunk to handsto feet, from midline to extremities, and
from gross to fine muscles. Stable posture
and sensory input facilitate controlled and refined movements
and mobility (Martin,2002).
Motor development occurs:
Gross to fine- Motor skills progress from large muscle use (such
as leg and armmovements for walking, pushing) to small muscle use
(discrete hand movementsfor writing)
Head to toe- Cephalocaudal (see chart below) Center to
extremities- Proximodistal (see chart below)
-
7/29/2019 Process of Motor Development
2/33
Gross Motor Milestones
Atypical Motor Patterns
As noted earlier, motor development may be compromised if there
is damage to thecentral nervous system, to the brain, or to sensory
systems (Allen & Marotz, 1994).
Motor delays that are likely not explained by deafness or
blindness include:
Favoring one hand before 12 months of age (due to weakness or
difficulty usingboth hands)
Crossing midline to pick up a toy (children under 1 years should
reach for
object with hand closest to the object rather than use the
opposite hand,crossing over the midline)
Fisting of the hands beyond 46 months of age Persistent
primitive reflexes beyond 46 months of age Log roll (rather than
segmental roll) Muscle tone (low or high) Scissoring of the legs
(when a child is picked up, the legs should be slightly
apart rather than crossing over each other) Conditions with
deafness that "may" include motor involvement Inner ear
malformations (cochlear dysplasia, mondini deformity)
-
7/29/2019 Process of Motor Development
3/33
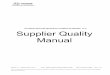
Reprinted with permission from Red flags for disabilities in
children who aredeaf/hard of hearing by S.Wiley and M. P. Moeller.
The ASHA Leader, 12(1),8-9, 28-29. Copyright 2007 by American
Speech-Language-Hearing Association.
-
7/29/2019 Process of Motor Development
4/33
-
7/29/2019 Process of Motor Development
5/33
PATHWAYS AWARENESS FOUNDATION.
Copyright 2006
Reflexes
Reflexes are involuntary responses to specific sensory
stimulithat are generally tactile, proprioceptive, or vestibular in
nature(Colangelo, 1999). Newborns' reflexive behaviors
dominatemovement, allow for survival, and set the stage for
earlyprimitive learning (Allen & Marotz, 1994).
Certain reflexes, such as swallowing, gagging, coughing,
andyawning, remain present throughout a person's lifetime (Allen
&Marotz, 1994). Other reflexes, however, begin to be
integratedinto volitional motor responses by 4 months of age. For
example,the reflexive grasp at birth becomes a voluntary grasp by
4months.
Motor Development and Movement,Carla J. Brown,Tanni
L.Anthony,Susan Shier Lowry, Deborah D. Hatton
-
7/29/2019 Process of Motor Development
6/33
The continued presence of primitive reflexes above the age of
six to twelve monthsand the absence, or under development, of
postural reflexes beyond three and a halfyears of age are reliable
indicators of neurological dysfunction and immature postural,motor,
and visual functioning.
A large majority of children with deafblindness have other
disabilities as well, and mayhave aberrant reflexes that adversely
affect posture and movement.
There are many primitive reflexes but we will consider three
that significantly
affect posture and movement and are seen in many children with
multiple
disabilities.
Moro Reflex: startle reflexes
Emerges at 9 weeks in utero and normally resolves at 2-4 months
of life
The earliest form of "fight or flight"
Stimulus is sudden change in position
The response is extension of the arms and flexion of the legs as
in a protectiveposture.
-
7/29/2019 Process of Motor Development
7/33
Signs of aberrant or retained Moro reflex
Stimulus bound- can't ignore external stimuli
Chronic fatigue; constant hunger; weak immune systems due to
over production ofstress hormones
Hyper-sensitive to change, light, sound or touch
Emotionally inappropriate, impulsive, unable to attend to
tasks
Tonic Labyrinthine Reflex (TLR)
Emerges at birth and is resolved gradually from 6 weeks to 3
years
Position of flexion: the baby's legs are curled up and flexed
into the fetal position
TLR stimulus is a change in head position (forward or
backward)
TLR response is a change in muscle tone (flexion or
extension)
Reflex is needed to help babies through the birth canal.
-
7/29/2019 Process of Motor Development
8/33
Signs of aberrant or unresolved TLR reflex
When retained it can lead to spatial problems, motion sickness,
poor posture, muscletone, and visual perception difficulties.
In supine position, the severely involved child is in stiff
extension and cannot lift head,bring hands to midline or turn
over.
In prone position, the child is in excessive flexion and may not
be able to lift or turnthe head to clear the air passage. For
example, a child sitting and lifting his headwould cause the body
to hyper-extend, causing the child to slip right out of the
chair.Good practice would be to get down on the child's level and
address them eye to eye.This will help avoid posture and muscle
tone change due to unresolved TLR reflex.
Asymmetrical Tonic Neck Reflex (ATNR)
ATNR reflex develops in utero and is strongest at 2 months of
age; usually suppressedby 5-7 months of age.
The ATNR is stimulated by a rotation of the head left or right
and is also refered to asthe "fencing" reflex because of the body
position. The response is an extension of thelimbs on the same side
of the body as the chin is facing; the limbs on the other side
of
the body will curl or flex.
-
7/29/2019 Process of Motor Development
9/33
.
Signs of aberrant or unresolved ATNR
Children with aberrant ATNR are stuck in the positioning until a
head turn releasesthe reflex. With no motivation to turn their
head, a deafblind child can be stuck in thisposition for a very
long time.
Because in this position the muscle tone is different on both
sides on the body, thestudent will have difficulty with bilateral
skills (Balance, running, and jumping are allskills that require
the balanced use of both sides of the body.)
-
7/29/2019 Process of Motor Development
10/33
Development of postural control
"Postural control involves both stability and movement.
Variousfactors influence the development of postural control.
Children with low postural tone (Hypotonia) have
difficultymaintaining a secure posture in which to interact with
theenvironment. They need a point of stability from which to
move.For children with visual impairments, less movement leads
todecreased practice of motor skills, which leads to a
questionablefoundation on which to build more mature movement
patterns.This, in turn, may result in developmental lags in
movement(Norris et al., 1957), atypical movement patterns (Brown
& Bour,1986), and decreased understanding of object and
spatial
concepts (Warren, 1994).
Motor Development and Movement, Carla J. Brown,Tanni
L.Anthony,Susan Shier Lowry, Deborah D. Hatton
Postural reactions
Postural reactions are automatic movements and adjustments
inresponse to, or in anticipation of, changes of position in
relationto the center of gravity. They allow individuals to
maintain aposture against gravity while adjusting to movement
(Alexanderet al., 1993). These reactions develop as the infant's
centralnervous system (CNS) matures and reflexive behaviors
areintegrated and provide the basis for postural stability upon
whichmore mature movement is built (Alexander et al., 1993).
Motor Development and Movement, Carla J. Brown,Tanni
L.Anthony,Susan Shier Lowry, Deborah D. Hatton
Derotational righting- usually appears at 4 to 5 months and
involves the infant's bodyturning to follow the direction of the
head when it turns, helping the child learn to rollover.
Parachute Response:This is a protective response. Beginning at
about 5-6 months, if
the infant falls, he will extend his arms to try and catch
himself.
-
7/29/2019 Process of Motor Development
11/33
Propping- This response helps infants learn to sit.
Anterior propping response begins at 4-5 months and involves the
infant extending hisarms when in sitting position to allow him to
assume a tripod sitting position.
Lateral Propping appears at 6-7 months and causes him to extend
his arm to the side ifhe is tilted.
Posterior propping causes him to extend his arms backwards if he
is tilted backward.
-
7/29/2019 Process of Motor Development
12/33
Goal-directed movement
Goal-directed movement refers to purposeful and self-initiated
movement (Anthony,
1993). Goal directed movement is an important part of
self-determination activities fora child with deafblindness. A
child needs to learn through movement that he caninteract with his
environment. He can move to accomplish a goal like finding a
favoriteperson or toy. Self-initiated movement comes once a child
with deafblindness has hadenough experience with movement that he
feels safe to explore.
In order for a child to want to self-initiate movement, he must
feel safe and must bemotivated to move and explore. To make
exploration functional for a deafblind child,visual, tactile, and
auditory information may need to be supplemented. It is importantto
think about what information the child is missing due to his
sensory impairment and
supplement the information in a motivational way.
Ideas for motivation include:
The use of objects meaningful for childrenfavorite toys,personal
items, caregivers
Tactile reacquaintance with the object just prior to
removal for use as a motivator for movement
-
7/29/2019 Process of Motor Development
13/33
Objects that make use of any residual vision and/or hearingthe
child has
Immediate success assured by:
short distances
opportunity to use well-established motor skills
discreet assistance by the adult
Motor Development and Movement, Carla J. Brown,Tanni
L.Anthony,Susan Shier Lowry, Deborah D. Hatton
Reaching
Reaching for a desired object is the beginning stage of goal
directed movement. A childwith deafblindness will not have the
natural opportunities to see and hear all theinteresting objects
around him that motivate him to reach out and explore. Motivatinga
child with deafblindness to explore beyond himself will take
structured practicesessions with exploration. A communication
partner introduces the child to objectsdirectly, models exploration
of the objects with full or partial assistance, and allowstime to
explore all the sensory qualities of the object. Familiar and
motivating objectsshould then be used in functional ways over and
over again. Is is vital to use a variety offamiliar and motivating
sensory cues to entice the child to self-initiate reaching.
Movement transitions
A child with sensory impairment has a harder time
masteringmovement transitions and rotational skills. Movement
transitions
are the way in which a child moves his body from one position
tothe next. For example: sitting to crawling or stooping to
standing.
"Adelson and Fraiberg (1974) found that although children
whowere blind were able to sit independently and stand within
theage range of sighted children, they did not move into, out of,
orforward from these positions at the same age as did
sightedchildren. While Adelson and Fraiberg (1974) proposed that
lackof vision as a motivator to move was a primary factor in
changingpositions and moving out, Brown and Bour (1986) proposed
that
the lack of crucial movement components (weight shift,
rotation,postural reactions) was responsible for static positions
and
-
7/29/2019 Process of Motor Development
14/33
failure to move. Further, they proposed that facilitating
activemovement transitions assists in the development of weight
shift,rotation, and protective responses, which in turn lead
toincreased mobility in rolling, crawling, and walking.
Also, quick, simple movement transition sequences can be
builtinto common daily events such as:
Diaper changing: At each changing time, the caregiver places
the infant in prone first, then slowly rolls the infant to
supineusing appropriate handling.
Picking up the infant: When picking up the infant from
sitting,
the caregiver helps the infant to weight bear with both hands
toone side, then to roll to all fours just before picking the
infant
up.
Standing position play at sofa: Instead of placing the infant
in
standing each time the infant wants to stand to play, place on
allfours close to the sofa and help the infant reach up with
onehand, move to kneel, then move through half-kneel to
standing.
Motor Development and Movement, Carla J. Brown,Tanni
L.Anthony,Susan Shier Lowry, Deborah D. Hatton
It is important to ask for, and follow, the guidance of the
physical therapist and/oroccupational therapist when it comes to
helping position a child during transitionalmovement. The child's
health, bone health, muscle health and tone will all need to
beconsidered by a professional in developing appropriate movement
patterns.
*Click here to view video on movement transitions
Crawling
"Fraiberg and Freedman (1964) proposed that the act ofreaching
out for an object in the all-fours position is the firstcomponent
of crawling. Maida and McCune (1996) also identifiedthe ability to
reach for an object while on all fours, as well as theability to
move to or from the sitting position, to be the twomost critical
precursors to crawling. In analyzing the componentsof movement
needed to accomplish these skills, postural stability,with the
center of gravity at the hips, which allows for lateral
weight shift to free one hand to reach forward, and
trunkrotation appear to be critical components for crawling
that
-
7/29/2019 Process of Motor Development
15/33
children who are visually impaired may lack.
Some children with visual impairments demonstrate delays
incrawling; others bypass crawling altogether (Adelson &
Fraiberg,
1974; Trster et al., 1994). Infants and young children who
areblind may have difficulty getting into and maintaining an
all-fourscrawling position due to lack of postural stability in the
shouldergirdle (Brown & Bour, 1986). Among children who are
able tomaintain this position, the ability to shift weight and
moveforward on all fours is sometimes absent (Brown & Bour,
1986;Fraiberg, 1968; Trster et al., 1994). As described earlier,
thislack of postural stability may stem from the lack of
activeexperience in the prone progression, the foundation for
crawling(McGraw, 1966). The prone progression consists of: prone
with
head elevated; prone with head and chest elevated; prone
withsupport on forearms; prone with support on forearms
andreaching; prone with extended-arm weight bearing; pivot inprone;
and prone with pushing up to all fours (Bly, 1994).Experience and
play in the prone progression are important fordeveloping the
extensor muscles of the back, shifting children'scenter of gravity
from the head and shoulders down to the hips(Bly, 1994)."
Motor Development and Movement, Carla J. Brown,Tanni L.
Anthony,Susan Shier Lowry, Deborah D. Hatton
-
7/29/2019 Process of Motor Development
16/33
Walking
Cruising is an important functional activity to help children
with sensory need to feelsafe, and gravitationally grounded before
independant walking.
According to Lowry and Hatton (2002), an extended stage
ofcruising may have the following benefits:
Cruising provides varied and repeated hands-on experienceswith
common objects, landmarks, and surfaces, leading tobroader
environmental concepts, a reinforced understanding ofobject
permanence, and goal-directed movement.
Cruising provides opportunities to establish a beginning
mental
map of the area, leading to more confidence and incentives
formovement as independent walking emerges.
Cruising often provides the first means of independent
upright
mobility well before children are posturally ready to walk.
Besides cruising around different obstacles, crawling up,
down,over, and around obstacle such as foam mats, cushions, boxes,
orhills will prepare a child for the depth changes and obstacles
hewill experience walking.
Motor Development and Movement, Carla J. Brown,Tanni
L.Anthony,Susan Shier Lowry, Deborah D. Hatton
A child with deafblindness who is walking independently will
often still benefit from awalking aid such as an adapted cane, a
push toy, stroller or shopping cart. Orientationand Mobility
specialists can be consulted to help find what aids will be most
functionalfor the child. The child can also be taught appropriate
trailing techniques that will helpthe child feel grounded and
receive the spacial information needed for goal
directedmovement.
-
7/29/2019 Process of Motor Development
17/33
Early Gross Motor Skills Intervention Ideas
Mindy Doyle McCall, physical therapist and JC Greeley,
Orientation and MobilitySpecialist, Anchor Center for Blind
Children, 2005
Motor skill milestones that a child with deafblindness may be
currently working to master arelisted below along with ideas for
functional intervention. It is important to consider how tobest use
any residual vision and hearing the child has in order to motivate
movement.
Birth to 4 months (There is no "norm." Ages are for typical
reference only.)
Encourage Prone lying "tummy time"
*Click here for intervention ideas
4 to 6 Months (There is no "norm." Ages are for typical
reference only.)
Encourage hand to foot play
-
7/29/2019 Process of Motor Development
18/33
*Click here for intervention ideas
Encourage rolling
*Click here for intervention ideas
Encourage emerging visual tracking across midline
*Click here for intervention ideas
6 to 8 Months (There is no "norm." Ages are for typical
reference only.)
Encourage mastery of rolling
*Click here for intervention ideas
Encourage the child to pull his legs up under his body
*Click here for intervention ideas
Encourage mastery of trunk control
*Click here for intervention ideas
8-12 months (There is no "norm." Ages are for typical reference
only.)
Encourage exploration
*click here for intervention ideas
12-18 Months (There is no "norm." Ages are for typical reference
only.)
Encourage crawling to standing transition
*Click here for intervention ideas
-
7/29/2019 Process of Motor Development
19/33
Encourage rotation in transitional movement
*Click here for intervention ideas
Encourage spacial and body awareness
*Click here for intervention ideas
Encourage walking with support
*Click here for intervention ideas
18-20 Months (There is no "norm." Ages are for typical reference
only.)
When walking, supported with one hand only
*Click here for intervention ideas
When child is taking steps independently
*click her for intervention ideas
Fine Motor Skill Development
Fine Motor Milestones
Fine motor skills generally refer to the purposeful and
controlledmovements of the small muscles of the fingers and hands.
These
movements are usually coordinated with the larger muscles ofthe
arms and trunk for stability and with the eyes for
eye-handcoordination. Children develop fine motor skills in a step
by stepprogression. Development occurs at an uneven pace, with
periodsof little progression.
These ages are approximate and may vary based on the
child'sdevelopmental process.
Brings hands to mouth and watches the movements of his/her
hands (0 to 3 months)
-
7/29/2019 Process of Motor Development
20/33
Reaches, grasps and brings hands to midline (3 to 6 months)
Transfers objects hand to hand ( 6 to 9 months)
Uses a neat, tip to tip pincer grasp on small, pellet-sized
items(9 to 12 months)
Scribbles with a crayon using whole arm movements (12 to 18
months)
Snips paper with scissors (18 to 24 months)
Imitates a circle and vertical and horizontal lines (2 to 3
years)
Stacks five to seven small blocks (3 to 4 years)
Touches each finger to thumb (4 to 5 years)
Writes first name (5 to 6 years)
Tara Calder, OTR/L,TSBV
As a reminder, typical motor development moves from proximal to
distal (trunk to armsand hands) and general to specific (large body
movements to small body movements).Therefore, whole arm and hand
movement occurs before discrete hand movements.Postural stability
of the head, shoulders, and trunk are necessary for the finer
controlof the hands.
The grasp reflex is evident at birth and occurs when a thin
object is placed in theinfant's hand; the infant's fingers tightly
curl around the object in response. Between1 and 4 months, the
grasp reflex integrates into increasingly voluntary control of
thehand. Over the course of the next 2 years, the infant's hand
skills become more
precise and includes the ability to pick up smaller objects and
to isolate fingers forspecific motions such as poking.
An early and necessary component of fine motor skills is that a
child is aware of hishands and understands that hands can be used
purposefully. Activities that providefirm proprioceptive input into
the hands and that promote hand-to-hand play, hand-to-mouth play,
and hand-to-foot play will facilitate an awareness of the hands and
midlineorientation of the body.
-
7/29/2019 Process of Motor Development
21/33
The first consideration, in preparing a child to participate in
fine motor activities, is toestablish good positioning for the
child. If the child is in a wheelchair the use of a laptray will
help with the support and stability of the arms and shoulders
during finemotor activities. Using the tray may also improve head
control. If the child has use ofonly one extremity, clamp down
paper or materials using a clipboard clamp screwed intothe lap
tray. Velcro strips or tape may also help to stabilize these.
Consulting with anoccupational therapist for the proper and most
functional position for fine motor workwould be of great
benefit.
The service provider will need to adapt for the child's visual
and auditory needs. Some
visual and tactile adaptations for fine motor work could
include:
-
7/29/2019 Process of Motor Development
22/33
Texture on lines with puffy paint or Wikkisticks Use of high
contrast materials (black on white, red on white, or yellow on
black) Reduced complexity (line drawings vs. real pictures) Use of
a light box The use of double lines, a thick marker or enlarged
print Use of playdough to form letters The use of sand or textured
paper in practicing writing
Fine Motor Activities To Encourage Pre-Braille Skills
Intervention Ideas by Debra Sewell, TSBVI
Although not all students with deafblindness will read Braille,
these pre-braille skillscan be beneficial in that they strengthen
hands and fingers, provide proprioceptive
feedback from the fine motor muscles (needed for motor
planning), and increase bodyawareness and tactile sensitivity.
-
7/29/2019 Process of Motor Development
23/33
-
7/29/2019 Process of Motor Development
24/33
-
7/29/2019 Process of Motor Development
25/33
-
7/29/2019 Process of Motor Development
26/33
-
7/29/2019 Process of Motor Development
27/33
-
7/29/2019 Process of Motor Development
28/33
-
7/29/2019 Process of Motor Development
29/33
Assistive Motor Devices
Functional movement is essential for a child with deafblindness
to be able to developconcepts that the the world extends beyond
what they can reach. Therefore, it is important toconsider the
array of specialized mobility equipment which help the child have
more
functional access within daily routines. These aides must be
individualized to the child'svisual, auditory and motor needs. All
equipment should be adapted by a licensedoccupational or physical
therapist. Most equipment will need to be replaced or adjusted
asthe child grows and his motor ability levels change. In fact,
some equipment poses safetyand health concerns if it is not
individualized for the child or is not functioning properly.
Positioning Equipment:
The goal of positioning equipment is to:
Keep children from developing more severe motor problems and/or
deformities
Help the child to function as normally as possible
-
7/29/2019 Process of Motor Development
30/33
Aid in respiration and digestion
Facilitate as much independent movement as possible
Minimize muscle tone issues by strengthening core muscles and
relaxing spastic
muscles
Equipment commonly used for positioning:
Stationary positioning chair provides back support in sitting,
ensuring shoulders areforward and the head is at midline.
Prone Stander provides support in varying angles from horizontal
to vertical and is used forjoint compression (proprioceptive
input), head control, and weight bearing.
Sidelyer provides a good position for encouraging children to
bring and use their hands atmidline. It also is a good position to
help break up excessive muscle tone. Use a motivatingobject, or
model exploration of an object to encourage the child with
deafblindness to use hishands at midline.
Orthoses:
Many children with deafblindness and tone issues use orthoses to
help support joints in afunctional position. Some orthoses are used
only occassionaly to support functionalmovement during a routine,
while others are used daily to keep the joint properly aligned
andto avoid malformation. Orthoses are professionally made and need
to be monitored by theparent and the physical therapist. However,
anyone working with the child can watch for anysign that the
orthoses a renot fitting properly. These signs may include:
redness, blisters or
sores, pain and discomfort, a change in movement pattern from
the child, or signs ofmalfunction (cracked plastic, missing straps,
missing screws). Any of these sign should bebrought to the
immediate attention of the educator in charge, the parent, or
occupational orphysical therapist.
Mobility Aids-
-
7/29/2019 Process of Motor Development
31/33
The purpose of mobility aids is to:
encourage the child to move, explore and participate
increase the child's ability to travel as independently as
possible
facilitate interaction with others
Some common mobility aids include:
Wheelchairs, strollers and scooters- Wheelchairs and scooters
are individually adjustedto ensure proper fit, sitting alignment,
and functional movement. Again, it is the role of theoccupational
and physical therapist to adjust wheelchairs and recommend
supports. Sensoryand cognitive function must be taken into
consideration when determining if a motorize chairis an appropriate
option. Most students with deafblindness who need wheelchair
support willnot be using motorized scooters.
Canes and Walkers- The types of cane and walking aids can vary
as much as theindividuality of the child being served. All service
providers should work together inconsidering vision, hearing, other
sensory (proprioceptive, vestibular), cognitive, and motorissues
before deciding on a functional walking aid with the most potential
benefit. It is onlythrough trial, and sometimes error, that the
child's needs are best met.
-
7/29/2019 Process of Motor Development
32/33
Scooter Boards-Scooter boards, if age appropriate, are a
functional mobility aid that canbe used in either a prone or
sitting position. Children with deafblindness who need fullphysical
support and have limited arm movement can still use a scooter board
while in asupported sitting position and using a switch for
activation.
Adapted Mobility Devices- Many times the most efficient and
inexpensive mobility solutionis "homemade." What can provide the
best support while allowing the child to participate inhis world to
the fullest extent possible, are ideas to consider when thinking
about mobilitysolutions.
-
7/29/2019 Process of Motor Development
33/33