Embed Size (px)
Citation preview

Private and Nongovernment Providers:Private and Nongovernment Providers:Partners for Public Health in AfricaPartners for Public Health in Africa
Conference ReportNovember 28 - December 1, 1994Nairobi, Kenya
Gerald Hursh-CésarGerald Hursh-César
With:With:
Peter BermanPeter Berman
Kara HansonKara Hanson
Ravi Rannan-EliyaRavi Rannan-Eliya
Joseph RittmannJoseph Rittmann

Data for Decision Making Project i
Table of Contents
AAcknowledgementscknowledgements ........................................................................................................................................................................ 11
BackgroundBackground .............................................................................................................................................................................................. 22
Summary of Implications ...................................................................................... 2
Conference Setting ............................................................................................... 3
Case Study Findings ............................................................................................. 5
DiscussionDiscussion .............................................................................................................................................................................................. 1111
Barriers to Public/Private Collaboration .................................................................. 12
Policy Issues..................................................................................................... 15
ImplicationsImplications ........................................................................................................................................................................................ 1818
ConclusionConclusion ............................................................................................................................................................................................ 2424
ReferencesReferences .............................................................................................................................................................................................. 2727
Participant ListParticipant List .............................................................................................................................................................................. 2828

ii Peter Berman, Kara Hanson, Ravindra Rannan-Eliya, and Joseph Rittmann

Data for Decision Making Project 1
Acknowledgements
This conference was supported by theUnited States Agency for InternationalDevelopment (USAID) Washington throughthe AFR/SD/Health and Human Resourcesfor Africa (HHRAA) Project (Project No.689-0483), under the Health Care Financ-ing and Private Sector Developmentportfolio, whose senior technical advisor isAbraham Bekele.
We would like to express our appreciationto Kate Colson and Gary Newton atUSAID/Nairobi and Ray Kirkland at REDSO/ESA for all their support. Peter Bermanprovided overall direction for the confer-ence and for the writing of the report.Special thanks to Joseph Rittman andGerald-Hursh-Cesar of Intercultural Com-munication, Inc for coordinating the
logistics of the conference and for writingthis report. Hope Sukin and AbrahamBekele of the HHRAA project at the AfricaBureau reviewed and gave technical inputto the report.
The background papers for the 4 casestudies which provided background for theconference were researched and writtenby DDM and Abt Associates.
Finally, we are especially grateful for thesupport given to us by all the staff ofDDM/Harvard, Ravi Rannan-Eliya, KaraHanson, Kasirim Nwuke, Chris Hale,Catherine Haskell, Kristen Purdy andChristina Oltmer, without whose supportthis conference report could not have beencompleted.

2 Peter Berman, Kara Hanson, Ravindra Rannan-Eliya, and Joseph Rittmann
Background
The Data for Decision Making Project(DDM) (Cooperative Agreement No. DPE-5991-A-00-1052-00), sponsored by theUSAID Africa Bureau’s Health and HumanResource Analysis (HHRAA) Project(Project No. 689-0483), convened aninternational conference on “Private andNon-government Providers: Partners forPublic Health in Africa,” November 28-December 1, 1994, in Nairobi, Kenya. Thepurpose of the conference was to addressthe major policy question:
How can countries make better use ofpublic and private health resources tofurther national health goals?
Underlying this major question is thepremise on which the conference wasbased and which was affirmed by theconference participants: that privateproviders can make and are already makingsignificant contributions to enhancing thecoverage and impact of important publichealth interventions.
The conference produced six implicationsor steps that have to be taken on a coun-try-by-country basis to build a more con-clusive, pragmatic, and empirical base ofknowledge, shared understandings, anduseful information exchanges for thepurpose of health policy decision-making.In brief, those implications are as follows:
Summary of Implications
1. Be Country-Specific
Each country needs to determine which
actions are necessary, possible, anddesirable to build the public/private part-nership in health care provision. The natureof the partnership will vary from country tocountry as political, economic, geographic,and cultural circumstances vary.
2. Build Trust
To overcome mutual suspicions, all of themany perspectives involved in public healthcare—including providers, governmentpolicy-makers, donors, researchers, suppli-ers, and, not least, consumers or healthcare clients—need to participate in thereview and deliberations of relevant datafor policy.
3. Agree on Definitions
Shared understandings and agreements ondefinitions are necessary to promoteeffective communication and information-sharing within and across countries.However, any typology (or other analyticdevice) must be tested for its appropriate-ness to each unique country setting beforebeing applied to the region.
4. Develop a Flexible Approach
The conferees debated a suggested meth-odology for describing and assessing theprivate sector and for undertaking researchstudies to create a reliable informationbase. The methodological guidelinespresented to the conference are a startingplace for work within countries on identify-ing specific strategies to increase the

Data for Decision Making Project 3
private contribution to national healthgoals.
5. Build a Database
Data on private providers should be devel-oped specific to each country. The datashould lead to a common understanding ofwhat are public health priorities, the typesof providers and their roles, their costs andopportunities, and the national policies andresources that affect those providers andthe public health.
6. Develop Communication Strategies
Participants urged that several activities beundertaken in following up the conference.These include improving data capturewithin countries, promoting networkingamong countries with regional clearing-houses, and communicating informationinternationally through such means as
newsletters, videotapes, and similarconferences.
Conference Setting
The conference drew representatives from14 African countries in addition to selectedrepresentatives from the United States andEurope.
Part icipants
The participants included 77 private andnon-government health care providers,government health policy-makers, healthcare researchers, and representatives ofAmerican and European donor agenciesand other international agencies andNGOs. Among the participants were suchprivate providers as physicians, pharma-cists, and traditional healers.

4 Peter Berman, Kara Hanson, Ravindra Rannan-Eliya, and Joseph Rittmann
Some 14 African countries were repre-sented: Burkina Faso, Cote d’Ivoire,Ethiopia, Ghana, Kenya, Malawi,Mozambique, Niger, Senegal, South Africa,Tanzania, Uganda, Zambia, and Zimbabwe.
Object ives
Focusing on the policies and issues affect-ing private and non-government healthcare provision in Africa, the overall pur-pose of the conference was to reviewexisting and new research data from theperspective of participants’ own experi-ences, and draw from their discussions anaction agenda for building an Africanpartnership of private and non-governmentproviders in public health. The specificconference objectives were:
1. To review and discuss the findings ofnew research, particularly recent casestudies on private and non-governmenthealth care provision in Kenya,Senegal, Zambia, and Tanzania, whichincluded assessments of:
• The size, scope, and distribution ofprivate providers.
• The current and potential role ofprivate providers in promoting thepublic health agenda.
• The conditions of consumers’ demandfor health services and the economicand regulatory factors that determinethe supply of privately provided healthcare.
• Existing linkages and opportunities forprivate/public partnerships.
2. To discuss the implications of thesecase studies and other data for policiesrelated to private and non-government
health care provision.
3. To generate ideas and recommendations foran action agenda for private and non-government health care provision in Africa.
4. To prepare an action agenda for policy-makers, international donors, andresearchers.
5. To plan the dissemination of back-ground materials and concept develop-ment on policies and experiences ofprivate and non-government providersin African health care.
Participants discussed the results of thecase studies of public/private provision ofhealth care in Kenya, Tanzania, Senegal,and Zambia conducted prior to the confer-ence in 1994. These case studies weresummarized and described in a conferencepaper, Summary: Private Providers’Contributions to Public Health in FourAfrican Countries. The case studies wereconducted largely on the basis of DDM’sAssessing the Private Sector: Using Non-Government Resources to StrengthenPublic Health Goals -- MethodologicalGuidelines. Both documents were distrib-uted in the Conference Workbook. (NOTE:These and other conference documents areavailable through the DDM Project of theHarvard School of Public Health.)
The case studies were presented asexamples of country analyses for discus-sion and for follow-up disseminationthroughout the African region.
Format
The four-day conference was organizedinto 15 discussion and implications ses-sions.

Data for Decision Making Project 5
DiscussionsDiscussions
The Conference Workbook provided the focus foreach discussion (Forum) session. Theseincluded the characteristics, services, determi-nants, linkages, and opportunities of privateprovision of health care. Usually, these Forumdiscussion sessions focused on specific themeswith formal presentations from the case studiesand related research.
ImplicationsImplications
The conference synthesis of proceedings re-ported here is mostly based on informal partici-pant discussions during the implicationssessions. For the purpose of this report, allbackground papers, notes from discussion andimplication sessions, and many hours ofvideotape were reviewed for main themes. Thiskind of thematic content analysis is qualitative,and does not give firm statistical statements.
Other ActivitiesOther Activities
Among other activities, participants visited localprivate health care facilities and joined in asimulation exercise of building a partnership forpublic health.
Different participants served the agenda indifferent ways. For example, policy-makersand donors presented their perspectives onsuch issues as financing and policy re-forms; while private providers presentedtheir perspectives on such issues asgovernment regulation, service quality,training, and credit requirements.
In addition to the formal case study pre-sentations, researchers from other institu-tions contributed their findings from studies ofprivate providers in Eritrea, South Africa, andThailand.
Contributing Agencies
The U.S. Agency for International Developmentwas represented by officers or other representa-tives of: the USAID Missions in Kenya and 13other countries; A.I.D.’s Regional EconomicDevelopment Services Organization; as well asthe Africa Regional Bureau and the A.I.D. Officeof Health in Washington. The conference wasalso attended by three World Health Organiza-tion representatives.
Private groups included the Harvard School ofPublic Health, which was the lead agency indeveloping the conference; Abt Associates,which contributed two of the case studies;Management Sciences for Health representingthe Kenya Health Care Financing Project, theLondon School of Hygiene and Tropical Medi-cine; the World Council of Churches; andIntercultural Communication, Inc. (ICI), a DDM/Harvard subcontractor, which organized thecommunication and logistical requirements ofthe conference.
Case Study Findings
The principal information made available to theparticipants as a basis for discussion was thepaper, Summary: Private Providers’ Contribu-tions to Public Health in Four African Countries.Both the summary and the individual case studypapers were included in the Conference Work-book. The major findings of these studiesincluded the following points:
Characteristics: Who are the Private
Providers?
Each country has a diverse mix of differenttypes of private providers, ranging fromtraditional to modern practitioners andfrom individual and ambulatory practices to

6 Peter Berman, Kara Hanson, Ravindra Rannan-Eliya, and Joseph Rittmann
large hospitals. For the study, providers wereclassified by their for-profit/non-profit commer-cial orientation and by their type of ownership—for example, individual/group-owned practices,mission/charitable clinics, employer-providedclinics, and others.
While countries vary, there is a general picture ofweakened economic conditions, over-burdenedand unevenly distributed public health systems,slowing or stagnating improvement in healthstatus indicators, and increasing governmentinterest in contributions the private sector mightmake to national health goals. Overall, theflagging economic conditions and thegeneral slump in public health servicesmake it all the more urgent that appropri-ate policies be developed for public/privatecollaboration in health services delivery.
It is widely perceived that the number ofprivate providers and the variety of theirservices are growing. The growth ofprivate providers may reflect the move-ment in each nation’s economy, with thenumber and type of providers increasing aspublic health funds and services deterio-rated. In the 1980s-90s, in particular,governments tended to relax licensing andregulation of private providers and to relaxthe prohibition of public-sector personnelworking in private practice. Today, it is notunusual to find, say, a private dispensaryowned by a MOH physician that is run bya nurse or medical assistant, with thedoctor keeping part-time and eveninghours.
Services: What Do Private
Providers Do?
While the government is the largest healthprovider, the size and distribution of theprivate health sector make it an important
part of national health care. The distribution ofboth public and private services tends mostly tofavor urban areas with larger populations, higheremployment, and better ability to pay. Both thesupply of and the demand for services are morefor curative than preventive health.
• Missions:Missions: Of all private providers, excepttraditional healers, only missions concen-trate in rural areas to serve the poor andunderserved. Their relationship with govern-ment is not uniform. Yet, whatever therelationship, church-based providers areimportant in all four countries for reachingrural areas with preventive as well ascurative services. However, while missionservices are typically not expanding, the for-profits are expanding rapidly.
• Employer-Based Services:Employer-Based Services: Somecountries require that large employersprovide health services or reimbursehealth expenses for their employees.Such services, including governmentparastatals, are often among the bestin the country but are usually availableonly to employees and their families.They provide all types of services, butmostly outpatient care through clinics,pharmacies, and specialty laboratories.Like the for-profit providers, companiesand parastatals tend to concentratetheir services in urban areas.
• For-Profit Providers:For-Profit Providers: The “modern” for-profit providers are the fastest growingsegment of the private health sector,although growth has been uneven andpoorly documented. They are mostly inurban areas, where there is a concen-trated market, higher ability to pay,and better access to supplies andtransportation. They provide a range ofhospital and ambulatory services, and
“The pharmacies are like
the modern clinics ...
most are urban-based,
while the greatest need
for them is in the rural
areas .... Today, they’ve
changed, and their role
is much different from
the past. They give
more services than just
medicines ... more
consultancy, more
counseling, even basic
diagnostics .... Their
one-stop services are
meeting greater patient
demand.”

Data for Decision Making Project 7
the latter are significant in all countries.They are less likely to provide preventiveservices than are the non-profit NGOs orchurch-affiliated facilities.
• Pharmacists/Drug Stores: Pharmacists/Drug Stores: In all fourcountries, pharmacies are the largestsuppliers of over-the-counter, prescrip-tion, and non-prescription medicines.They tend to concentrate in urbanareas and are more closely regulatedby the government than are otherproviders. Their role is expandingbeyond dispensing medicines. It is notunusual to find “one-stop” pharmaciesthat provide medical diagnosis, patientcounseling, and treatment in additionto dispensing drugs.
• Traditional Practitioners: Traditional Practitioners: Healers,charismatics, and birth attendants areoften the most accessible and mostimportant source of rural health care.They, too, tend to be “one-stop”sources of care—diagnosis, medicines,and treatment. There is new interest inthe potential contribution that tradi-tional healers, with modern training,could make to the nations’ health.
• Community-Based Services: Community-Based Services: In linewith governments’ efforts to increaserural health services, more community-based and community-owned clinics andpharmacies are emerging in rural places.They may be managed by a village commit-tee and provide such services as medicines,medical supplies and health education;support immunization programs forchildren’s communicable diseases; and treatmalaria, diarrhoea, worms, and skin andeye infections. Some include a form ofhealth insurance whereby communityresources are pooled to help familiesthrough catastrophic illnesses.
In summary, there is little information on privateservices in any country. The growth of theprivate, especially for-profit, sector has been asuneven as it has been rapid. In the absence ofgood monitoring systems, it is difficult to tracknew facilities and the type and quality of theirservices. There is some evidence that malprac-tice is growing.
Determinants: What Things Affect Private
Services?
The most important demand factors affectingpeople’s use of private services are income andurban/rural place of residence. And the mostconstraining supply factors are lack of access tocapital and high taxes on imported drugs,medical supplies, and equipment.
• Demand-side Determinants:Demand-side Determinants: Thedemand for private services is high—insome countries 40 percent or more ofconsumers use private and missionservices and over-the-counter drugpurchases. Household income is thegreatest constraint on use of privateservices, with lower-income groupsmaking more use of drug sellers, smallproviders, traditional healers, and missionand mosque services. Other importantfactors related to use of private services areeducation, residence, quality of services(government services are often rated loweras compared with private services), avail-ability of health insurance, and government“user fees”—which may lead to greaterdemand for private modern services.
• Supply-side Determinants: Supply-side Determinants: MOHservices have deteriorated with fallingreal government funding—drug short-ages, lack of essential supplies, over-crowding, and long delays. Despite prob-lems getting credit, the economic and
“Health policy is wrong
(to) ignore the traditional
healers and
charismatics. For many
rural, poor people, the
traditionals are the only
accessible source of
medicines and
treatments - no matter
how good .... People
believe in them and they
are everywhere ....
Public education is a
problem. Why should
people travel to the far-
away city, when they
believe in the healing
powers of the
traditionals?”

8 Peter Berman, Kara Hanson, Ravindra Rannan-Eliya, and Joseph Rittmann
political climate in the four countries favorsthe growth of private health services.Governments’ legalization or reducedrestrictions on private providers havecontributed to their expansion. Now, thegreatest constraints on providers are lack ofaccess to capital and credit, high taxes onimported drugs and medical equipment andsupplies, and lack of trained medicalpersonnel.
Overall, government policies, regulations, andlicensing procedures have not constrainedprivate sector growth, but have encouragedurban concentration.
Linkages: What Links Exist Between the
Public and Private Sectors?
Three main linkages between the public andprivate health sectors are (a) laws and regu-laws and regu-lationslations, which tend to be weakly enforced andshow large gaps in their application; (b) com-com-munication and coordinationmunication and coordination, which oftenfalls short of intentions and provide few fora forpolicy dialogues; and (c) service deliveryservice deliveryand financingand financing, which tends in both sectors tobe curative, thus resulting in service duplication.The public/private relationships are not alwaysclear, but their collaboration is not new. Inparticular, the non-profit mission sectorhas existed for many years, with a gener-ally sound relationship with government.Governments’ relations with for-profitproviders typically have been less thansound.
A major linkage in service delivery hasbeen public financing of private providers.This can be direct payment, as in directpayments in cash or kind for service(Kenya NHIF pays private hospitals as wellas public hospitals, most countries providesome supplies, like vaccines or ORS to
private doctors and pharmacies free or lowcost.) And it also can be partial, as insubsidizing inputs (low taxes on drugs,medical equipment) or giving incentivepayments for certain actions. This hasbeen an important area of public actionaffecting private providers.
For family planning services and contracep-tive supply, private providers make a majorcontribution in some countries. For otherpublic health problems, private providersmake varying contributions by, for ex-ample, treating common childhood dis-eases such as diarrhoea and respiratoryinfections, giving immunizations, assistingdeliveries, treating malaria, treating sexu-ally-transmitted diseases and tuberculosis.Their clientele and their services vary bytype of provider (say, missions vs. anurse’s outpatient practice vs. drug sellers)and their urban/rural locations.
Implications: What are Opportunities for
Improving Public Health and Private
Provision?
All the case studies recommended thatgovernments and donors recognize thecurrent and potential importance of privateproviders in health care delivery. While thelack of information limits the assessmentof private providers and their potential forimproving public health, it is known thatthey are not homogeneous in structure,fees, composition, output, location, orsusceptibility to government leverage.Because of the wide variety of privateproviders, policies to enhance support fornational health goals must be tailored tothe needs of each type of provider.
The improvement of health service deliv-ery, reach, and impact will require a more
“...private providers
can make important
contributions to public
health care .... we
have seen good models
of collaboration in
numerous African
countries (and)
substantial scope for
developing ... new
public/private linkages
to improve coverage,
quality, and
affordability of
essential services ....
including joint efforts in
provision and financing
as well as ....
incentives and
subsidies for private
providers, better
monitoring and
regulation, and sharing
of training and
information.”

Data for Decision Making Project 9
inclusive and higher level of policy dialogue thanexists at present, as well as programmingcollaboration with private providers directed at(a) increasing available health resources; (b)increasing efficiency of resource use; (c) increas-ing equity of access; and (d) increasing effective-ness of services.
To increase private providers’ contributions topublic health requires that governments reduceconstraints on private services and improvemonitoring and coordination of those services.Steps might include continued decentralizationof health decision-making, improved informa-tion-sharing, improved modern medical training,relaxed restrictions on public health profession-als working in the private sector, and such otherreforms as setting achievable standards forquality and appropriate use of services andproviding direct material or financial assistancethrough incentives and subsidies.
The central problem for governments is torecognize people’s demand for health servicesand to attempt to meet that demand throughany conventional or unconventional means—pharmacies, traditional healers, birth atten-dants, community-based services—that effec-tively reaches and appeals to people where theylive and that provides higher-quality, affordableservices than people have access to now.
In short, in the views of the participants, theimprovement of national health status requiresgovernments to use more effectively the healthservices that are already in place. To do so,national planners must develop specific modelsof public/private collaboration based on specifichealth problems, types of providers, geographiclocations, target populations, fees paid, insur-ance coverage, and types of services—diseasetreatment, referral, preventive care, and healthinformation. Such models should make explicitthe costs and benefits of improved integration of
private and public delivery of services aimed atimproving the public’s health.
Of course, there already are a number of modelsin various African nations of successful public/private collaboration, especially in immunizationprograms, family planning efforts, and treat-ment of children’s illnesses. But the models thusfar have not been developed comprehensivelynor disseminated widely. Moreover, in the viewof some participants, the efficacy and cost-effectiveness of the models have not yet beensufficiently evaluated.
Yet, the consensus view of the conferenceparticipants was that private providers canmake substantial, positive contributions topublic health care. And, as such, there isgreat scope for developing a wide varietyof new public/private linkages to enhancecoverage, quality, and affordability ofessential services. These could includejoint efforts in provision and financing aswell as programs of public support (incen-tives, subsidies) for private providers,better monitoring and regulation, andsharing of training information.
In opening the conference, its convener, Dr.Peter Berman of the Harvard School of PublicHealth, identified two strands of policy actionthat have become clear in the last decade. Thefirst policy reform activity has been the studyand debate on how to expand the role of privateagents in financing health care which may beadditional to, or partially a substitute for, publicsector spending. This has been the main focusof interest in the private sector in health inAfrica.
The second, more qualitative strand of policyreform, has been efforts to enhance the role ofprivate provision of health services. This secondissue is more recent and very little is known

10 Peter Berman, Kara Hanson, Ravindra Rannan-Eliya, and Joseph Rittmann
about the actual or potential public/privaterelationship; this was the focus of this confer-ence.
However, for their deliberations, conferees werecautioned:
“....that the evidence is not yet availableto support or discount many of the asser-tions that are frequently made about thequality and efficiency of the private sector.Instead, we have sought to identify themerits and weaknesses of different parts ofthe private sector.” (Berman, 1994, p.7).

Data for Decision Making Project 11
Rather than to try to produce a technical agendaof specific policy and program actions to take infollowing up the Nairobi meeting, it was theconsensus of participants that certain, prelimi-nary steps have to be taken first to informpolicy-makers.
While the conference aimed to prepare an actionagenda for building the partnership for publichealth in Africa, the combination of perspectivesand country experiences resulted in a universalsense among participants: (1) that such apartnership would need to be built country by
country; and (2) that not enough is known withcertainty about private providers to makeinformed policy decisions on their future roleand potential in serving national health goals.
As such, rather than arriving at recommenda-tions for technical approaches to the partner-ship, participants sought to discover consisten-cies in themes and issues across countries.Establishing commonalities was in the partici-pants’ view a first step that has to be taken asa basis for developing an action agenda.
Discussion “At a political level,
Governments are
beginning to adopt ...
‘The New Order’
towards the private
sector. In (my country)
this has meant the effort
to harness new
resources in support of
national health goals:
We have focused
primarily on (the) mining
and mission sectors, but
now are also looking
towards the private for-
profit sector in our
search for new partners.
We are promoting a freer
exchange of information,
the opportunity for
dialogue, the formation
of shared values and
ideals, and looking for
win-win solutions to
shared problems .... We
want to be a ‘listening
government.’ ”

12 Peter Berman, Kara Hanson, Ravindra Rannan-Eliya, and Joseph Rittmann
Typically, countries also lack a uniform policyframework for prescribing specific steps toimprove the public/private partnership. Eachcountry’s legal and regulatory framework shouldbe in place as a basis for defining and resolvingproblems of private and public health provision.This is not always the case. And some of thepolicies that are in place, such as prohibitionson public health professionals working in privatepractices and high taxes on imported drugs andmedical equipment, act as constraints onprivate sector development.
Limited Resources Affect Research Priorities
While each country situation is unique, generallyAfrican nations are facing difficult economictimes. Governments are strapped for healthfunding to address problems of lack of trainedpersonnel, lack of health facilities, lack ofmedical schools and professional training, lackof equipment and supplies, and others. Oneproblem common to all countries is thatresource limitations seriously inhibit nationalefforts to monitor and regulate private providerseffectively.
Against the backdrop of other critical needs forfunding, research on the nature and potential ofprivate- and public-sector collaboration iscurrently a rather low priority. While participantsgenerally felt that more conferences such as thisone would be useful, they see the greatest needfor improving the data base and improving thedissemination of data as preconditions toelevating the priority for research.
However, participants recognize that thepresence of data alone is not enough toimprove communication and use of re-search findings. There is not enoughexisting, trustworthy information on public/private health services across African countriesto give reliable guidance for action steps. It is
Accordingly, this report presents the principalthemes and issues identified at the conference.Certain implications are drawn from thesethemes. The first result is a list of barriers thatwere identified as obstructing efforts to developspecific strategies to increase the privatecontribution to national health goals. In brief,those barriers include the following:
Barriers to Public/Private
Collaboration
African Nations are Highly
Heterogeneous
There is significant variability within andacross countries—in languages, geography,customs, behavioral patterns. Each countryhas its unique colonial history, which hasaffected its social, economic, and politicalinstitutional development, its provision ofhealth services, and the relationships ofpublic and private health providers. And,indeed, the four case studies found impor-tant differences in the type of privateproviders in each country and in the rolesthey play in health service delivery.
Accordingly, the participants’ view is thateach country situation is unique, to theextent that actions must be developedcountry-by-country instead of through aregional approach. And, from country tocountry, the problems and the solutionsrelated to private- and public-health provi-sion are different. Until more is knownabout the similarities and differences ofhealth systems among countries, partici-pants felt that discussions of developing acommon core of data and a common studyapproach will be inconclusive. Theircaution to donor agencies is that theremay not be a pan-African policy agenda orapproach.
“The aim of the
conference was to foster
exchange among policy
makers in governments
and international
organizations,
researchers, and private
and non-government
providers on the
partnerships for
improving the public’s
health in Africa .... Three
important points that
emerged (are) suspicion
between the actors ...
(which can, through
conferences like this, be)
largely overcome;
challenges to medical
orthodoxy ... (such as)
pharmacists expanding
their role in health
service delivery (and)
how this challenge plays
out will depend on the
relative strength of the
different professional
bodies; and the need to
start early in developing
an appropriate legal and
regulatory framework for
private providers.”

Data for Decision Making Project 13
healers, manufacturers and suppliers, insurancecompanies, and consumers/recipients of healthservices.
On the other hand, not all relevant parties maybe willing to join the policy discussion. Tradi-tionally, relationships between governmentproviders and mission (charitable) providerstend to be quite good, as the missions arerecognized for serving areas and peopleunderserved by public services. Generally,however, competitiveness rather than coopera-tion marks the public/private relationship. Thesense of competition will not abate until more isknown about the actual and potential roles thatdifferent types of providers may serve in further-ing national health objectives.
Communication Among Parties is Poor
There is generally such little interaction betweenpublic and private health providers that partici-pants on both sides are not sure of the groundon which they stand with respect to possiblecollaboration.
Public and private providers are rarely involvedtogether in mutually supporting front-line servicedelivery. While there is some collaboration at thelevel of the district, it is usually not within thescope of mutually agreed programs and objec-tives. Rather, each group goes its own way. Theprincipal mode of sharing experiences is thepresence of public practitioners working inprivate clinics. Yet, in some countries, suchmoonlighting is illegal.
In situations in which there is low awareness,limited interaction, and little shared experience,it is almost axiomatic that there is poor commu-nication between members of the public sectorand the private sector. Until communicationimproves, stereotyping and suspicion willpersist.
debatable how much of a common core of datacould be obtained in different countries. Thereare a few country-specific studies, but none hasbeen undertaken for regional guidance.
Similarly, there is no uniform methodologicalapproach to the study of public/private relation-ships across countries. The guidelines forassessing the private sector that were offered byHarvard for conference consideration werethought to be a good “starting place.” However,the consensus was that each country shouldstudy its own situation in its own way. But, inthis light, one concern voiced is that country-specific studies will not add up to a region-widedata base if they are greatly different. Further,technical agreements on methodology would beneeded to implement a regional approach—e.g.,common methodology, sampling frames,analysis plan, reporting criteria. Such agree-ments may be difficult to obtain.
Distrust Affects the Public and Private
Relationship
There is much suspicion between membersof the private and public health sectors.Much of the problem of low trust is due tolittle awareness of the private sector’scomposition and health contribution aswell as due to the lack of involvement ofall concerned parties in policy debates.Providers on each side suspect the motivesof the other side. Ignorance andmisperception thrive in the absence ofdata.
One problem that creates distrust is thelack of representation of relevant parties.That is, not everyone who would be partyto building a public/private partnership forhealth delivery is invited to the table todiscuss the issues and problems. Notablymissing from such discussions are traditional

14 Peter Berman, Kara Hanson, Ravindra Rannan-Eliya, and Joseph Rittmann
Parties Lack Agreement on
Roles and Objectives
There is little agreement about the natureand potential of the public/private healthrelationship. Little attention has been paidto the nature of the private sector. Little isknown about its composition, services, oractual or potential roles in advancing thenational public health agenda in anycountry in the region.
Given the lack of data, there is littleagreement on who are private providersand where to start in trying to betterunderstand their health roles. And there islittle agreement about the role they play inambulatory and inpatient curative care orin other public health services such asprevention and health education. There is,however, strong agreement that traditionalpractitioners (healers, spiritualists, birthattendants, bone-setters, herbalists,roadside providers/”kiosk” clinics, shops,pharmacies, and others) are importantprivate providers.
Thus, given the lack of data, lack ofdefinitions, and lack of assessment meth-odology, it is not surprising that there islittle firm agreement on the nature of theproblem or, indeed, whether there is aproblem or what to do about it. Manypublic providers do not see the contribu-tions of private providers as necessary forachieving public health goals.
Information Exchange and Dissemination are
Weak
There is no strategy in place in the region’scountries for systematic dissemination ofinformation on the private sector and on itsrelationships with the public health sector.
Among specific avenues for communication,there is no evidence that education about theprivate sector has yet achieved any place in thecurriculum in public medical schools andtraining centers.
Similarly, there are few learning opportunities orpublic fora for sharing views or for exchanginghard data between public and private providers.It is not a subject that is widely taken up atdonor- or government-sponsored medicalconferences or workshops.
Summary
The above are the major conclusions of confer-ence discussions of barriers to public andprivate health service coordination. In additionto the problem of little information and lowawareness, it is notable that two themes thatrun through these barriers are closely relatedproblems of human relations. The first is lowtrust between members of the public sector andthe private sector, and the second is poorcommunication between them.
When related issues are combined, the list ofbarriers gives six actions (next page) thatconference participants believe have to be takento strengthen the elements of policy reformaimed at improving the public/private relation-ship in health provision.
Presuming resources would be available, thesix-step prescription principally calls for moreand better information and more and betterinformation exchange as a basis for creating apolicy-and-action dialogue. In this respect, theconference produced an action agenda forimproving intelligence rather than an actionagenda of specific policy alternatives (see figure1 below).

Data for Decision Making Project 15
Policy Issues
Of course, numerous policy and programmingissues were discussed among the participants.But no firm consensus emerged from thesediscussions as to specific actions to be taken.Some of the major policy questions discussedwere:
• Incentives:Incentives: The need for more creativeuse of public incentives and fiscal tools(e.g., taxes, subsidies, in-kind contribu-tions) to increase private provision ofservices of national priority (e.g.,treatment of major childhood diseases,reproductive health) and to reachunderserved populations in both urbanand rural areas. Special considerationis needed to encourage private provid-ers to serve urban poor and rural areasthrough, perhaps, sharing investmentcosts for equipment, facilities, importduties, and others.
• Monitoring: Monitoring: Without making licensingor regulation more restrictive, the needfor strengthening government monitor-ing and regulatory capacities to providepossible improvements in the qualityand accountability of private healthcareprovision.
• Program Models:Program Models: The need for devel-oping “new models” of collaborationbetween the public and private sectors toincrease private providers’ contributions tothe national health agenda. This includesmore involvement of private practitioners inpublic health debates and legislative acts—including their participation in discussionsof rate-setting, credentials, service typesand locations, incentives, and other issues.
• Service Coverage: Service Coverage: The need for extend-
ing coverage to the poorest populationsthrough, for example, national insuranceschemes, employer-based services, socialsecurity mechanisms, specialized creditinstitutions, and the like.
• Awareness: Awareness: The need for improvingconsumer knowledge and behaviorthrough public education and motiva-tion; in particular, to educate consum-ers in preventive health measures andreduce the demand burden on curativeservices.
• Education/Training: Education/Training: The need forproducing more well-trained medicalprofessionals and strengthening na-tional capacities (e.g., facilities, appli-cant selection, curricula) for higher qualitymedical education and training; and theneed for incorporating private healthprovision into the public health curricu-lum—thus, to recognize the potential rolesand contributions of the private sector tonational health. This includes new attentionin the formal medical curriculum to tradi-tional health-care systems and practices.
• Credentials: Credentials: The need for the develop-ment and application of country-specific standards for evaluating,certifying, licensing, and regulatingprivate health providers (e.g., physi-cians, clinicians, technicians, pharma-cists).
• Traditional Practitioners:Traditional Practitioners: The need forre-evaluating the certification of, andthe contributing roles played by,traditional healers and practitioners forthe purpose of bringing them into thepublic health debate and for employingtheir services - such as carriers ofmodern health messages—where such
“Privatization of public
health services and
increasing ... private
health care provision are
strategies (receiving)
growing amounts of
attention over the past
decade. They have
arisen out of a number
of concerns and
developments (including)
the shortcomings of the
public sector action
(and) shortfalls in
performance and
outcomes from highly
centralized, top-down
service strategies ....
Another factor (is) the
fiscal crisis faced by
many states (with)
dramatically reduced
economic growth, or
even reductions in
national income .... A
third factor of
importance has been the
growing recognition
that, whatever the
strengths and
weaknesses of public
action, the private health
sector exists and is
sizable in many
countries.”

16 Peter Berman, Kara Hanson, Ravindra Rannan-Eliya, and Joseph Rittmann
services complement and extend coverageof the modern health system. This includesefforts to capture the treatment knowledgeof healers and charismatics, which may belost to modernization.
While these and other policy issues were raised,specific action recommendations were notmade. That is, while many agreed that bettermonitoring and accountability are necessary,there was no real agreement on how to achievea better system. Rather, the conference empha-sized that the first, follow-up step is to improveintelligence as a prerequisite for sound policy-making.
The following are the prevailing views of theconference regarding six steps to be taken indeveloping an information base for policy-makers.
Country-Specific Approaches
African countries are highly heterogeneous. Eachcountry presents a unique context for developinga partnership. The size, composition, and roleof private providers, as well as the extent of thelinkages with the government and amongproviders, vary greatly among countries and
within countries. The circumstances of eachcountry’s development shapes the partnershipfor public health in that country. Moreover, themanagement capacity of the government and ofprivate providers to strengthen the base fordeveloping partnerships is different from onecountry to the next.
The conference demonstrated that, in trying tofind regional solutions, the uniqueness of eachcountry’s own circumstances should not beunderestimated. There can be no regional orsub-regional approach to analyzing public andprivate health provision until it is known withcertainty whether and how the conditions ineach country are similar to or different fromneighboring countries. The participants felt thatuniform approaches, standardized typologies, orother analytic devices should first be tested forappropriate “fit” within countries as a basis fordetermining the fit across countries.
For example, to use standardized categories ofa typology of private providers that wouldpromote a uniform approach to the privatesector in all countries, some of the elementsthat participants felt have to be considered foreach country include: the terminology used andits different meanings; the cultural context in
Six Steps Toward Policy Decisions
1. Conduct data collection and research on a country-specific basis.
2. Attack the problem of trust—bring everyone concerned to the policy table.
3. Agree on definitions of private providers and their services.
4. Agree on the methodology for creating an appropriate data base.
5. Build the data base.
6. Take actions to communicate data implications to all concerned parties.
figure 1: The six step prescription
“In the immediate term,
policy changes in public/
private financing or
provision arrangements
(could be) introduction
of paybeds in selected
hospitals (which) may
stimulate interest in
voluntary health
insurance ....
introduction of partial
payments for drugs at
health clinics and
centers .... Contracting
of some non-clinical
services in hospitals ....
Encouraging new NGO
groups to act as service
implementers (and
putting) private
practices under closely
monitored public
regulations.”

Data for Decision Making Project 17
which health services are delivered; the varyingsocial and economic systems and issues ineach country; the government’s historicalrelationship to the private sector and the level ofinvolvement of both public and private provid-ers; and others.
Also at issue are such questions as, who woulddefine the typology—the public sector or theprivate providers themselves? Would it clarifyownership and control of services? Would it besufficiently flexible to accommodate unantici-pated cases or future conditions? And would itspurpose be well understood by all parties

18 Peter Berman, Kara Hanson, Ravindra Rannan-Eliya, and Joseph Rittmann
affected?
It was the consensus of the conference that atypology of providers is necessary, but thetypology should be adapted to each country’sspecific circumstances: “Typologies are useful... but we need to have typologies withincontexts.”
Developing partnerships is an evolving process.Once started, each country must continue todevelop partnerships, strengthen linkages, andfoster collaboration within its specific circum-stances. Most countries represented have verylimited development of public/private linkages,particularly in areas such as legal and regulatorypolicy, financing, and information. There are a
few experiences of collaboration—both withinthe represented countries as well as in othercountries—that can be used as background forstrengthening collaboration within countries.
Although there is a need for more informationon the private sector, there are a number ofareas where countries are already taking actionto strengthen public-private partnerships. Theseinclude financing private providers to deliverservices of public interest, improving laws,registration and quality monitoring, and intro-ducing collaborative local planning in cities,towns, and rural districts with not-for-profit andfor-profit providers. Since experience needs to begained, action can begin whenever public and
Implicat ions“Collaboration in some
of the countries is at an
embryonic stage. In the
past, some distrust and
lack of understanding
prevented further
collaboration (and
created) some confusion
on the (role) of the
private sector. In most
instances, collaboration
with the MOH (was)
only in terms of
licensing. An exception
was Burkina. A new
program is in place to
provide training support
for the private sector,
provision of commodities
(contraceptives) at
subsidized prices ....
access to medical
equipment. The private
sector, in turn, is
allowing inspections and
providing statistical
information.”

Data for Decision Making Project 19
private sector collaborators are ready.
In sum, the first action in any country is to buildcommon understandings among all relevantconstituencies of, for example, what is publichealth and what is private provision. Thesecond action is to acquire data on the actorsand agencies of public and private healthprovision and on their existing links and poten-tial role in contributing to national public healthgoals.
Build Trust
Any actions to build public/private partnershipsin health care provision will require that trust-worthy data are available and that all actorsand agencies involved in health services bebrought together at the decision-making table.
To-date, private providers have tended to beignored during the process of governments’policy deliberations. In particular, the groupsmost poorly represented are traditional healers,health manufacturers/suppliers, and the citizenconsumers. Also, it is felt that insurancecompanies should be represented as well. Toreduce suspicion, all groups must be involved indeliberations; they have to share the sameperspectives; and they have to contributefinancial, human, and material resources tothe problem.
In the views of the conferees, suspicionbetween private providers and govern-ments has resulted from lack of consistentinformation on the characteristics, ser-vices, and determinants of private provid-ers, as well as confusion about what ispublic health and the role of government,private providers, and consumers in obtain-ing better health. Most countries repre-sented reported having inadequate knowl-edge about the size and composition of the
private sector, what private providers can anddo contribute to national health priorities, andthe dynamics of public/private linkages.
According to one senior participant, VincentMusowe of the Zambia Ministry of Health, partof the suspicion and antipathy of public healthofficials toward private providers derives fromviews that the private sector unduly absorbshealth care personnel; that providers are tooconcentrated in urban areas; that they servemainly upper-income consumers; that they getunfair tax concessions; that they use inappropri-ate and expensive technology; that they focuson clinical services to the detriment of preventivehealth; and that their motives are commercialand exploitative. To what extent these negativeperceptions are based in fact is unclear, as thedata do not exist to support this.
It was the prevailing view of the conferees thatdiscussions based on reliable data and ex-change of perspectives can bridge the suspicionsthat separate providers and government. In fact,one view expressed several times at the confer-ence was that participants were surprised thattheir viewpoints had so much in common bothacross countries and across sectors:
“(A major problem is) suspicion betweenactors—government and private providers.Participants were able to talk freely, shareperspectives, and to discover that they arenot so far apart. In some measure, thestereotypes we in the public sector carry ofprivate providers have been largely over-come” (Musowe, 1994, p.2).
This type of reaction among participants speakswell to the value of conferences and other forafor the exchange of views. However, morediverse views are needed. That is, to seizeopportunities for improving the partnership forpublic health, trust must be built among thebroad base of partners involved—namely

20 Peter Berman, Kara Hanson, Ravindra Rannan-Eliya, and Joseph Rittmann
government policy-makers (not only theministries of health), private providers from thewhole range of orthodox and nonorthodoxproviders, donors, and researchers, and not theleast, the consumer or client of health care.
Create Shared Understandings
Effective public/private partnerships requirecommon agreements and understanding ofthe many issues affecting private provisionand public health specific to each country,including what is public health, the types ofprivate providers and their roles, and nationalpolicies and resources affecting those providersand the public health. Information-sharing willnot help the partnerships much if differentparticipants have different meanings for what isshared. And, indeed, the four case studiesfound different private-sector componentsplaying different roles in the variouscountries.
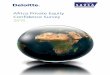
For the problem of varying definitions, andas one part of its methodological guide-lines, Harvard presented to the conferencea possible “typology” for classifying privateand public providers in different countries.
As it was applied in the case study ofZambia, the typology addresses the ques-tion of “Who are the private providers?” Itclassifies providers along three dimensions:(a) commercial orientation—whetherprivate services operate mostly for-profit ornon-profit; (b) complexity of organization—relating to the level of services provided,size of organization, and other factors; and(c) the type of healing system involved—whether “modern” or “traditional” or somecombination. See the typology in figure 2.
One of the reasons for developing thetypology of providers was to help distin-
guish and clarify the relationships of theinformal/traditional providers and other “mod-ern” providers. This the participants felt is animportant distinction to make and it will helpensure that further data collection and analysesof health systems do not ignore the traditional/informal sector.
The typology sparked considerable debate aboutits meanings and applications to individualcountries. It was agreed that each countrywould have to determine for itself the appropri-ateness of the “fit” of the typology within itsown borders.
Develop a Flexible Methodology
For discussion at the conference, the Harvardpublication, Assessing the Private Sector: UsingNon-Government Resources to StrengthenPublic Health Goals -- Methodological Guide-lines was introduced as a “starting place” forparticipants to judge whether and how auniform analytic approach could be developedfor country-to-country assessment of thecontribution of private health care providers tonational health goals. The purpose was togenerate discussion with a view to improvingthe guidelines so that they could be used fromone country to the next for the analysis ofexisting data and, as necessary, for thecollection of new data for efforts toidentify specific strategies to increase theprivate contribution to national healthgoals:
“On the one hand, to try to get privateproviders to do more in support ofprograms of public health interest orincrease access to good qualityservices for populations in need; and,on the other, to reassess the publicsubsidies—both explicit and implicit—to the private sector and, where

Data for Decision Making Project 21
appropriate, to ensure that public fundsare not being used to subsidize servicesthat are not contributing to nationalobjectives” (Berman, 1994, pp.6-7).
Again, the consensus was that each countrywould have to determine for itself the appropri-ateness of such an approach. However, likestandard definitions, it was agreed generallythat a common methodology is necessary bothto describe and to assess the private sectorwithin and across nations. As such, the guide-lines, developed by the DDM project, were feltto be useful as a tool for structuring datacollection and analysis. The guidelines addressthree basic questions:
1. Who are private providers?
As discussed above, a typology of providerswould be useful in order to organize andanalyze strategies. The suggested typology hasthree dimensions: commercial orientation,complexity of organization, and type of modern/traditional healing system.
2. What are the linkages between the publicand private sectors?
To encourage effective public/private partner-ships, we have to know the linkage betweensectors, for example, sources of financing, typeof public or private provision, regulations andlicensing, taxes and subsidies and incentives,supply and demand conditions influencingprovision, and monitoring and reporting activi-ties.
3. What do private providers do?3. What do private providers do?
In order to increase and improve private-sectorcontributions to public health goals, we need toidentify, quantify, and assess the role of privateproviders in ambulatory and inpatient curativecare and in other public health services, such as
prevention programs.
Addressing these kinds of questions will aidgovernment policy-makers in deciding onwhether to increase or reduce public subsidiesto private providers; whether to increase ordecrease services for different populations thatare subsidized with public funds; or whether tosubstitute private for public provision byknowing the circumstances under which it mayor may not be feasible and may or may notproduce more equitable and efficient services.
Of course, all other relevant parties—privateproviders, insurance providers, donors, healthassociations, researchers, and others—wouldbenefit from new knowledge of who the privateproviders are in any country; the roles they playin curative and preventive health services; andwhere and how their services are available andwhere they overlap, compete with, complement,or supplement public services.
As the participants discussed, the private healthsector is highly diverse. It is not a single,monolithic entity. Rather, different parts of theprivate sector tend to be important for differentpopulation groups and for different types ofcurative and preventive services.
Because of the unknown type and amount ofdiversity within each country, we need data-based conclusions. As a starting place forcollecting and analyzing data, it was suggestedthat public and private services be assessedalong at least the two dimensions of: (a) Type:The type of public or private service provision;and (b) Resources: The public or privatesources of finances and other human andmaterial resources committed to the differenttypes of service provision.
Both the methodological guidelines and itstypology of providers sparked considerabledebate, with the eventual conclusion of
“We agree that
governments have to
take action, with new
policies and new
programs, to bring the
public sector and the
private providers
together and in harmony
... and to get the best
and the most benefit
from each. But, first,
our policy makers (need)
more information to
make informed decisions
on which policies and
which programs to
implement.”

22 Peter Berman, Kara Hanson, Ravindra Rannan-Eliya, and Joseph Rittmann
participants that both would have to be adaptedto each country’s own situation.
Build a Database
The conference emphasized the need to identify,recover, and analyze all existing relevant data ineach country before undertaking to collect newdata through field studies. While it was felt thatmany useful data may be found in countries,there was no clear identification of data hold-ings in any of the countries represented at theconference.
The conference itself is testimony to the value ofnew or unknown information for stimulating theexchange of views and experiences even amongthose whose views are radically different andopposed. Many participants found greater
congeniality of views than they anticipated. Thiskind of dynamic, which was simulated by theconference, is likely to function as well in theworkaday world, as policy-makers are given anincreasingly useful information base for theirdecisions.
Field studies undertaken in advance of commonagreements are likely to be wasteful. Thepartnership should be built on a firm base oftrustworthy data that are representative ofpublic- and private-sector conditions in urbanand rural areas as well as for different types ofcommunities and income and ethnic groups. Asa result of the data and the common under-standings obtained from the review by allparties’ perspectives, each country mustdetermine its own action agenda and the means
Non-Profit Providers For-Profit Providers
Employer Provided
• Parastatals
• Mines
• Large Employers(Over 350 Employees)
• Other Employers
Non-Government
Organizations
• Missions/Christian Churches
• Islamic Organizations
• Other Non-profit services(e.g., Flying Doctors)
• Local Non-governmentOrganizations
• Foreign Non-governmentOrganizations
Modern Formal Sector
• Private Clinics
• Private Hospitals
Pharmaceutical Retailers
• Pharmacies
• Drug Stores
• Market Vendors
Traditional Practitioners
• Birth Attendants
• Other Traditionals(e.g., Diviners, Bone-setters,Herbalists, Spiritualists,Healers)

Data for Decision Making Project 23
to implement the agenda, and begin the processof implementing changes, as required.
By building on the common understandingobtained from the data and the resultingdiscussion, each country must define foritself what are its priorities for publichealth, the types and roles of providersincluded in the partnership, and the na-tional policies and resources affecting thepartnership for public health.
Develop Communication Strategies
The conference on private and non-govern-ment health providers drew participantsfrom 14 African countries. It was veryfavorably evaluated by the participants,who typically said that the conference wasa “very useful opportunity” for providers,policy-makers, donors, and researchers toaffirm the importance of building partner-ships for public health in many Africancountries.
The wide consensus was that the commu-nication of the research findings andmethodology discussed at the conferenceneeds to be followed-up by regional andcountry-level dissemination activities. Atpresent, plans for such dissemination donot exist, but the DDM project will explorehow the use of its resources may promotesystematic dissemination as a follow-onactivity.
The participants urged that disseminateddata should be broad-based, including allorthodox and non-orthodox health careproviders ranging from the highest level ofspecialist care to the front-line care giver inthe remotest of situations, from privateentrepreneurs to complex, institutional provid-ers. The data should include policy issues, such
as, financing, training, legal and regulatoryaspects, service quality and equity, monitoringand reporting, and information needs.
For specific dissemination activities, the partici-pants offered three recommendations based onthe spirit of the conference.
Country ResearchCountry Research
With the leadership of each government,participating donors, researchers, andproviders should collaborate to fund initialresearch and data collection on privateproviders specific to each country. Thedata from this research are essential forsuccessful development of a partnershipfor public health.
Regional CentersRegional Centers
In both the francophone and anglophoneregions, regional clearinghouses should beestablished with donor assistance, govern-ment participation, and provider support.Each clearinghouse would serve as a focalpoint for bridging international researchactivities with on-going country-specificactivities, networking among countries,intra-regional study tours and workshops,and supporting country-specific activities.
International DisseminationInternational Dissemination
The international network, fostered by theconference, should be reinforced bycontinuous communication and intellectualsupport. A newsletter should be estab-lished to continue communication amongthe participants and to foster their activi-ties in each country. The newsletter wouldfurther disseminate the methodologiesreviewed in the conference as well asprovide a continuing resource for inter-country exchange of data, tools, experi-

24 Peter Berman, Kara Hanson, Ravindra Rannan-Eliya, and Joseph Rittmann
ence, and progress. A brief video presentationshould be prepared from the extensive videofootage from the conference to be used byparticipants in support of their country-specificdissemination activities.
Conclusion
Participants agreed widely that the Nairobiconference was a valuable impetus tofurthering the public/private dialogue. Forsome of the participants, the conferencewas the first opportunity for public- andprivate-health providers to discuss theissues involved in a health delivery partner-ship. The frank and constructive ex-changes of the Senegal representativeswere a particularly good example toothers. It was evident that many participantsleft the conference eager to continue the dia-logue back home. And, indeed, the conferencedid motivate some immediate follow-up actions.In Zambia, for example, a national conferencehas since been designed based on the Nairobiconference to continue and to make morespecific the dialogue on the nature and require-ments of a public/private partnership.
Although there was a strong consensus on theneed for better information and dialogue,conference participants noted that much wasalready going on and that much more could bedone immediately.
• Many countries already have in place avariety of “models of collaboration”involving central, provincial and localgovernments, social insurance organi-zations, and a wide variety of for-profitand not-for-profit providers. These modelsrange from health financing methods tospecific disease control and family planningcollaborations. Successful models can be
replicated and expanded.
• Countries in different parts of Africa mayhave similar legal systems and experiencewith regulation of private providers. Coun-tries could begin to collaborate on issuessuch as registration, the structure of public-private commissions, drafting of legislationand regulations, and processes for qualitymonitoring and improvement.
• User fees and insurance schemes areexpanding in many African countries.What effect will public sector feeshave on private provision and onpatient welfare? Will private servicesbe covered by insurance? How shouldproviders be paid? What effect willinsurance expansion have on public andprivate provision? Such important policyquestions need to be answered, mainly byexperimentation.
• The significance of traditional practitionersand the informal health sector was stronglyemphasized. The consensus was that thepotential contributions of the informalsector to public health goals must beexamined with an open mind.
In summary, as this report has shown, themajor implications that participants saw asactions for following up the conference areto enhance each country’s data base,improve communication and interactionamong relevant parties, ensure representa-tion of all parties at the policy table, andbuild trust among parties through improvedinformation exchange and more public/private fora.
Abt Associates, Private Sector Delivery of HealthCare in Tanzania, Major Applied Research PaperNo. 14, Health Financing and SustainabilityProject, Bethesda, Maryland Abt AssociatesInc., November 1994.

Data for Decision Making Project 25
Abt Associates, Private Sector Delivery of HealthCare in Senegal, Major Applied Research PaperNo. 15, Health Financing and SustainabilityProject, Bethesda, Maryland Abt AssociatesInc., November 1994.
Bennett, Sara and Ellias Ngalande-Banda,Public and Private Roles in Health: A Reviewand Analysis of Experience in sub-SaharanAfrica, Geneva: Current Concerns Paper No. 6,World Health Organization, March 1994.
Berman, Peter, et al., Zambia: Non-GovernmentHealth Care Provision, Boston, Massachusetts:Data for Decision Making, Harvard School ofPublic Health, October, 1994.
Berman, Peter, et al., Kenya: Non-Governmen-tal Health Care Provision, Boston, Massachu-setts: Data for Decision Making, Harvard Schoolof Public Health, November, 1994.
Berman, Peter and Kara Hanson, Methodologi-
cal Guidelines for Assessing the Private Sector:Using Non-Government Resources to StrengthenPublic Health Goals, Boston, Massachusetts:Data for Decision Making, Harvard School ofPublic Health, February 1994.
Hanson, Kara and Peter Berman, Non-Govern-ment Financing and Provision of Health Servicesin Africa: A Background Paper, Boston, Massa-chusetts: Data for Decision Making, HarvardSchool of Public Health, July 1994.
Hursh-César, Gerald, Summary: Private Provid-ers Contributions to Public Health in FourAfrican Countries, Boston, Massachusetts: Datafor Decision Making, Harvard School of PublicHealth, April 1995.
Rittmann, Joseph, Conference Workbook:Private and Non-Government Providers forPublic Health in Africa, Boston, Massachusetts:Data for Decision Making, Harvard School ofPublic Health, November 1994.
“Our primary policy
question has been ‘How
can countries make
better use of both public
and private health
resources to further
national health goals.
(Our) perspective ... to
guide our discussions ...
implies: That we see
both public and private
health care as
instrumental to achieving
some goals .... that we
be pragmatic in our
approach ... in further
efforts towards these
goals (and) that we be
empirical — seeking
‘data-based’ conclusions
on which to develop
policy and program
strategies.”

26 Peter Berman, Kara Hanson, Ravindra Rannan-Eliya, and Joseph Rittmann
Dr. Alarou AboubacarDirecteur de la Promotion de la Santec/o USAID/Niger MissionS/PHNONiamey, NigerPhone: 227-73-35-08Fax: 227-72-39-18
Dr. Saidi AboudAdministratorCrescent Medical Aid KenyaJamia Plaza, Kigali StreetP.O. Box 33041Nairobi, KenyaPhone: 254-2-220811Fax: 254-2-230748
Mr. Dennis D. AfandePermanent SecretaryMinistry of HealthNairobi, Kenya
Dr. Akin AkinyemiProgram Coordination ManagerUSAID/Nigeria Mission1601, Adeola Hopewell StreetP.M.B. 53373, Falomo P.O.Lagos, NigeriaPhone: 234-1-2619952Fax: 234-1-2615592
Dr. Sako AmadouLecturerFaculty of Health SciencesUniversity of Niameyc/o USAID/Niger MissionS/PHNONiamey, NigerPhone: 227-73-35-08Fax: 227-72-39-18
Dr. R.K.O. AsanteExecutive SecretaryWorld Council of Churches150, route de Ferney -- P.O. Box 21001211 Geneva 2, SwitzerlandPhone: 41-22-791-61-11Fax: 41-22-791-03-61
Felix AwantangHPN OfficerAID Affairs OfficeUSAID/Nigeria Mission1601, Adeola HopewellVictoria IslandLagos, NigeriaPhone: 234-1-614412, 2614621/3825Fax: 234-1-614698/412

Data for Decision Making Project 27
Dr. Bineta BaHealth Care Financing AdvisorREDSO/WCA/HHRUSAID/Abidjan Missionc/o American Embassy01 B.P. 1712Abidjan 01, Cote d’IvoirePhone: 225-41-45-28 to 32Fax: 225-41-35-44
Dr. Ardo Bac/o USAID/Senegal MissionSDIHPlace de l’IndependenceDakar, SenegalPhone: 221-228585Fax: 221-222223
Dr. Sandra BaldwinRegional Projects OfficerRegional Office for East and Southern AfricaInternational Development Research Centre (IDRC)Liaison House State House AvenueP.O. Box 62084Nairobi, KenyaPhone: 254-2-713160Fax: 254-2-177063
Dr. Mazuwa BandaGeneral SecretaryChurches Medical Association of Zambia (CMAZ)Ben Bella RoadP.O. Box 34511Lusaka, ZambiaPhone: 260-1-229702Fax: 260-1-223297
References

28 Peter Berman, Kara Hanson, Ravindra Rannan-Eliya, and Joseph Rittmann
Dr. Chris BarrattUSAID/Senegal Missionc/o American EmbassyB.P. 49Avenue Jean XXIII et Rue KleberDakar, SenegalPhone: 221-23-70-37Fax: 221-232965
Dr. Abraham BekeleSenior Health Economic and Financing AdvisorBureau for AfricaUSAID/AFR/SD/HRD1111 N. 19th Street, Suite 300Arlington, VA 22209-0089 USAPhone: 703-235-5424Fax: 703-235-4466
Dr. Peter BermanDirectorData for Decision Making ProjectHarvard School of Public HealthDepartment of Population and InternationalHealth665 Huntington Avenue, Room 1210Boston, MA 02115 USAPhone: 617-432-4616Fax: 617-432-2181
Dr. Daniel BlumhagenUSAID/Niger MissionS/PHNONiamey, NigerPhone: 227-73-35-08/73-43-63 (his ext.)Fax: 227-72-39-18
Dr. Constance CarrinoDivision DirectorOffice of Health and NutritionUSAIDG/PHN/HN/HPR SA-18, Suite 1200Washington, DC 20523-1817 USAPhone: 703-875-4519Fax: 703-875-4693
Dr. Paul O. ChukeWorld Health Organization (WHO)P.O. Box 45335Nairobi, KenyaPhone: 254-2-723069, 724818Fax: 254-2-720050
Dr. John Paul ClarkUSAID/AFR/ARTS/HRD1111 N. 19th Street, Suite 300Arlington, VA 22209-0089 USAPhone: 703-235-9100
Ms. Kate ColsonUSAID/Kenya MissionNairobi Moi-Haile Selassie AvenueP.O. Box 30137 Unit 64100Nairobi, KenyaPhone: 254-2-749590Fax: 254-2-337304Dr. Perle CombaryProject Manager of Health Financing ActivitiesUSAID/Burkina Faso Missionc/o American EmbassyB.P. 3501 Ouagadougou, Burkina FasoPhone: 226-30-67-23Fax: 226-30-89-03
Dr. Humberto CossaNational DirectorDirectorate of Planning and National Coopera-tionMinistry of HealthP.O. Box 265Maputo, Mozambique
Participant List

Data for Decision Making Project 29
Mr. Mbaye DiagneDoctor PharmacistOrdre des PharmaciensPharmacie RufisquoiseB.P. 74Rufisque, SenegalPhone: 221-363311Fax:
Mr. Fred FischerDirectorREDSO/ESAP.O. Box 30621Nairobi, KenyaPhone: 254-2-331160Fax: 254-2-330945
Dr. Jean-Jacques FrereBASICS ProjectJohn Snow, Inc.1600 Wilson Boulevard, Suite 300Arlington, VA 22209 USAPhone: 703-312-6800Fax: 703-312-6900
Mr. Ibrahim HusseinHealth Care Financing SecretariatMinistry of HealthNairobi, KenyaPhone: 254-2-716760Fax: 254-2-719-308
Dr. Muthoni KariukiAfrican Medical and Research Foundation(AMREF)P.O. Box 30125Nairobi, KenyaPhone: 254-2-501-301,2,3Fax: 254-2-506112
Mr. David KielemMinistry of HealthOuagadougou, Burkina FasoPhone: 226-315389
Mr. James Ray KirklandChiefPopulation and Health DivisionUSAID/REDSO/East and Southern AfricaP.O. Box 30621Nairobi, KenyaPhone: 254-2-749590 x2321Fax: 254-2-330945
Dr. Daniel KraushaarChief of PartyKenya Health Care Financing ProjectUSAID/Kenya MissionP.O. Box 41869Nairobi, KenyaPhone: 254-2-719308Fax: 254-2-719308
Dr. E. LamboHFA UnitWHO/AFROB.P. 06Brazzaville, CongoPhone: 242-8-39356, 8-39354Fax: 242-8-39400
Dr. Charlotte LeightonTechnical Director, HFS ProjectPartnerships for Health ReformAbt Associates, Inc.4800 Montgomery LaneHampden Square, Suite 600Bethesda, MD 20814-5341 USAPhone: 301-913-0500Fax: 301-652-3916
Dr. Denise LionettiDeputy Director for AdministrationHealth Financing Sustainability (HFS)Abt Associates, Inc.4800 Montgomery Lane, Suite 600Bethesda, MD 20814-5341 USAPhone: 301-913-0500Fax: 301-652-3916

30 Peter Berman, Kara Hanson, Ravindra Rannan-Eliya, and Joseph Rittmann
Mr. P.A. LlomoEconomistMinistry of Health/USAIDSamora AvenueP.O. Box 9083Dar es Salaam, TanzaniaPhone: 255-51-46221Fax: 255-51-39951
Professor William LoreKenya Medical Association (KMA)Chyulu RoadBox 48502Nairobi, KenyaPhone: 254-2-724617
Dr. Karanja MbuguaAfrican Medical and Research Foundation(AMREF)P.O. Box 30125Nairobi, KenyaPhone: 254-2-510-301,2,3Fax: 254-2-506112,502699
Dr. E.N. MensahDirector of Institutional Care DivisionMinistry of Healthc/o USAID/Ghana MissonRing Road EastP.O. Box 194Accra, GhanaPhone: 233-21-22-8440, 228467Fax: 233-21-77-34-65
Dr. Ann MillsHeadHealth Policy Unit, Department of Public Health& PolicyLondon School of Hygiene and TropicalMedicineKeppel StreetLondon, WC1E 7HT United KingdomPhone: 44-71-636-8636/071-927-2354Fax: 44-71-637-5391
Dr. MulingeDirectorDivision of Family HealthMinistry of HealthNairobi, Kenya
Dr. Gasper K. MunishiAssociate Professor and DeanFaculty of Arts and Social SciencesUniversity of Dar es SalaamP.O. Box 35051Dar es Salaam, TanzaniaPhone: 255-51-43395, 43500/8 ext. 2294Fax: 255-51-43395
Dr. Jeffrey MuschellNational Health Systems and PoliciesDivision of Strengthening of Health ServicesWorld Health Organization20, Avenue AppiaCH-1211 Geneva 27, SwitzerlandPhone: 41-22-791-2111/2566 (direct)Fax: 41-22-791-0746
Dr. F.D. MusetaP.O. Box 2548Bulawayo, ZimbabwePhone: 263-9-79684Fax: 263-9-77996
Mr. Vincent MusoweChief Health PlannerMinistry of HealthWoodgate HouseP.O. Box 30205Lusaka, ZambiaPhone: 221186, 282959Fax: 223435
Dr. R.J. MuyaMember, Executive CouncilAssociation of Private Hospitals in TanzaniaNew Bagamoyo RoadP.O. Box 6369Dar es Salaam, TanzaniaPhone: 255-51-66050/1Fax: 255-51-44162

Data for Decision Making Project 31
Dr. Allast MwanzaDepartment of EconomicsUniversity of ZambiaSchool of Humanities and Social SciencesBox 32379Lusaka, ZambiaPhone: 252198/158/520, 251565 x1713Fax: c/o AID 260-1-254-532
Dr. R.F. MwesigyeHealth PlannerMinistry of HealthP.O. Box 8Entebbe, UgandaPhone: 256-42-20992Fax: 256-42-20996
Mr. Godwin MzengeFamily Planning Association of Kenya (FPAK)Nairobi, KenyaPhone: 254-2-215676
Mrs. NderituMedical Services CoordinatorKenya Catholic SecretariatWaumini HouseWestlandP.O. Box 48062Nairobi, KenyaPhone: 254-2-443-133Fax: 254-2-442-910
Dr. Daniel K. NdigoHerbalistP.O. Box 11642Nairobi, Kenya
Mr. Raymond NdongConseiller Technique, No. 1Ministere de la Sante et de l’Action Sociale auSenegalDakar, SenegalPhone: 221-216-713Fax: 221-232-965
Dr. Gary NewtonHPN OfficerUSAID/Kenya MissionNairobi Moi-Haille Selassie AvenueP.O. Box 30137 Unit 64100Nairobi, KenyaPhone: 254-2-749590Fax: 254-2-337304
Dr. Henock A.M. NgonyaniHead and Registrar -- Private HospitalsMinistry of HealthHospital Services DepartmentNon-Government and Private HospitalsBox 9083Dar es Salaam, TanzaniaPhone: 255-51-26633Fax: 255-51-39951
Dr. NjugunaTraditional Health PractionerP.O. 23531Nairobi, Kenya
Dr. Sam L. NyaywaDDMS (DEC)/Team LeaderHealth Reform Implementation Team (HRIT)Ministry of HealthP.O. Box 30205Ndeke House AnnexLusaka, ZambiaPhone: 253180/1/2Fax: 253173
Dr. Norman OlemboDirectorChristian Health Association of Kenya (CHAK)P.O. Box 30690Nairobi, Kenya
Dr. Charles OliverOffice of Health and NutritionUSAIDG/PHN/HN/EH, Room 1200, SA-18Washington, DC 20523-1817 USAPhone: 703-875-4507Fax: 703-875-4686

32 Peter Berman, Kara Hanson, Ravindra Rannan-Eliya, and Joseph Rittmann
Dr. Julius O. OmbogoPresidentPharmaceutical Society of KenyaP.O. Box 18288Dakar RoadNairobi, KenyaPhone: 254-2-532-461Fax: 254-2-542689
Dr. F. Osafo-MensahSociety of Private Medical and DentalPractionersP.O. Box 6831Accra, GhanaPhone: 233-21-228-440/467Fax: 233-1-773465
Ms. Joy OworiProject DirectorFamily Planning Private SectorP.O. Box 46042Nairobi, KenyaPhone: 254-2-224646Fax: 254-2-230392
Dr. David ParirenyatwaPresidentCollege of Primary Health Care PhysiciansP.O. Box 66222Kopje HouseHarare, ZimbabwePhone: 263-4-720757, 728282, 721106Fax: 263-4-722418, 720722
Dr. Oscar F. PicazoHealth Finance AdvisorUSAID/REDSO/ESANairobi, KenyaPhone: 254-2-751613Fax: 254-2-749590
Dr. Max PriceDean, Faculty of Health SciencesUniversity of the Witwatersrand7 York RoadParktownJohannesburg, 2193, South AfricaPhone: 27-11-647-2010Fax: 27-11-642-3533
Dr. Joseph RittmannConsultantIntercultural Communication, Inc.109 19th Street, N.E., Apt. 11Watertown, SD 57201 USAPhone: 605-882-0130Fax: 605-882-0130
Dr. Judith Robb-McCordPrivate Sector Family Planning ProjectUSAID/Kenya MissionNairobi Moi-Haile Selassi AvenueP.O. Box 30137 Unit 64100Nairobi, KenyaPhone: 254-2-749590Fax: 254-2-719308
Ms. Roxana RogersUSAID/Zimbabwe MissionP.O. Box 6988Harare, ZimbabwePhone: 263-4-720757, 728282, 721106Fax: 263-4-722418, 720722
Mr. Alex RossUSAIDAFR/SD/HRD1111 North 19th Street, Suite 300Arlington, VA 22209 USAPhone: 703-235-4453Fax: 703-235-4466
Ms. Laura SlobeyGeneral Development OfficerUSAID/Mozambique MissionRue Faria de Sousa, 107Caixa Postal, 783Maputo, MozambiquePhone: 490726, 491689, 7444844Fax: 492098
Dr. Hope SukinHHRAA Project DirectorAfrica BureauUSAIDDepartment of StateWashington, DC 20523 USAPhone: 202-647-8907Fax: 202-647-7430

Data for Decision Making Project 33
Ms. Fatimata SyUSAID/Senegal Missionc/o American EmbassyBP 49Avenue Jean XXIII et Rue KleberDakar, SenegalPhone: 221-23-70-37Fax: 221-232965
Mr. Daniel TylerRegional RepresentativeChurch World Service and WitnessP.O. Box 14176Nairobi, KenyaPhone: 254-2-442204Fax: 254-2-443241
Sister UdokaVice ChairpersonChristian Health Association of Malawi (CHAM)c/o USAID/Malawi MissionP.O. Box 30455Lilongwe 3, MalawiPhone: 265-782-455, 378, 694Fax: 265-783-181
Ms. Dana VogelPopulation OfficerUSAID/Tanzania MissionAir Tanzania Building, 3rd FloorOhio Street and Garden AvenueP.O. Box 9130Dar Es Salaam, TanzaniaPhone: 255-51-464-29/329-22/77Fax: 255-51-46431
Dr. Jerome WolginDirectorOffice of Sustained Development/Bureau for AfricaUSAID320 21st Street N.W.Room 2744Washington, DC 20523-0087 USAPhone: 202-647-8907Fax: 202-647-7430
Dr. Zina YacoubaPermanent SecretaryMinistry of Health03 B.P. 700903 Ouagadougou, Burkina FasoPhone: 226-306654, 305950Fax: 226-306654, 305950
Dr. Paul Zeitzc/o Office of Health and NutritionUSAIDG/PHN/HN SA-18 Suite 1200Washington, DC 20523-1817 USAPhone: 703-875-4551Fax: 703-875-4686