Embed Size (px)
Citation preview

Prior to the start of the program, please check your syllabus to ensure you have the following printed program materials:• Pre-activity Survey
– Located at the front of your syllabus
• CME Evaluation with Post-activity Survey– Located at the back of your syllabus
Prior to the start of the program, please check your syllabus to ensure you have the following printed program materials:• Pre-activity Survey
– Located at the front of your syllabus
• CME Evaluation with Post-activity Survey– Located at the back of your syllabus

Disclosures
• The relevant financial relationships reported by faculty that they or their spouse/partner have with commercial interests are located on page 5 of your syllabus
• The relevant financial relationships reported by the steering committee that they or their spouse/partner have with commercial interests are provided on page 5 of your syllabus
• The relevant financial relationships reported by the non-faculty content contributors and/or reviewers that they or their spouse/partner have with commercial interests are located on page 5 of your syllabus

Off-label Discussion Disclosure
This educational activity may contain discussion of published and/or investigational uses of agents that are not indicated by the Food and Drug Administration. PCME does not recommend the use of any agent outside of the labeled indications. Please refer to the official prescribing information for each product for discussion of approved indications, contraindications and warnings. The opinions expressed are those of the presenters and are not to be construed as those of the publisher or grantors.

Learning Objectives
• Identify lapses in COPD care that led to the Centers for Medicare and Medicaid Services (CMS) quality measures, and identify opportunities to improve the quality of that care across the healthcare continuum
• Apply current clinical evidence and guidelines to develop a comprehensive care plan that addresses common reasons for repeat exacerbations and hospital readmissions
• Apply quality-of-care models and develop programs to foster effective transitions of care and ongoing maintenance treatments for patients with COPD

What percentage of your COPD patients who present for management of exacerbations do you refer for pulmonary rehabilitation?
A. All of my COPD patients
B. 51%-75% of my COPD patients
C. 25%-50% of my COPD patients
D. <25% of my COPD patients
Polling QuestionPre-activity Survey

In what percentage of your patients presenting for management of COPD exacerbations do you evaluate and manage comorbidities?
A. All of my COPD patients
B. 51%-75% of my COPD patients
C. 25%-50% of my COPD patients
D. <25% of my COPD patients
Polling QuestionPre-activity Survey
Please rate your level of familiarity with the CMS Core Measures for COPD:
1 2 3 4 5
Not at all familiar Expert
Polling QuestionPre-activity Survey

Please rate your level of confidence in your ability to implement strategies to ensure continuity of care for COPD patients based on the CMS Core Measures for COPD:
1 2 3 4 5
Not at all confident Expert
Polling QuestionPre-activity Survey
What is the most common cause of mortality in COPD patients?
A. COPD
B. Depression
C. Cardiovascular disease
D. Diabetes
Polling QuestionPre-activity Survey

A 72-year-old woman is released after management of COPD exacerbation. She has type 2 diabetes, hypertension, hypothyroidism, and rheumatoid arthritis. She is not at the goal for hemoglobin A1C nor blood pressure. She also has mild depression, for which she is successfully managed with trazodone. What is her greatest risk for frequent exacerbations going forward?
A. Her age
B. Age at onset of COPD
C. Her uncontrolled diabetes
D. Her history of exacerbations
Polling QuestionPre-activity Survey

Based on the GOLD 2014 recommendations, which of the following criteria should be present before hospital discharge following COPD exacerbation?
A. Patient has been clinically stable for 12-24 hours
B. Patient is able to walk around the block (if previously ambulatory)
C. Patient requires inhaled short-acting beta2-agonist therapy every 2-4 hours
D. Patient had stable arterial blood gases for 24-48 hours
Polling QuestionPre-activity Survey

Which of the following non-pharmacologic interventions has been shown to decrease readmissions for COPD exacerbation?
A. Vitamin D supplementation
B. Decreased physical activity
C. Yearly influenza vaccination
D. None of the above
Polling QuestionPre-activity Survey

So far, the only therapy documented to reduce COPD disease progression is:
A. Physical activity
B. Influenza vaccination
C. Smoking cessation
D. Good nutrition
Polling QuestionPre-activity Survey
Which of the following outcomes may be seen when enrolling patients in an integrated disease management plan for COPD?
A. Decreased frequency of viral infection
B. Weight gain
C. Decreased readmissions and lengths of stay
D. Significantly increased health care costs
Polling QuestionPre-activity Survey

When selecting a medication delivery system for your COPD patient, which is your most important criteria?
A. Amount of medication deposited in the lungs
B. Cost
C. Disease severity
D. Hand-breath coordination
E. Presence of support system to help administer the medication
Polling QuestionPre-activity Survey

Opportunities to Improve COPD Care
Focus on the CMS Quality Measures

The Impact of COPD
• ~15 million people diagnosed (additional 12M are undiagnosed)– 2nd leading leading cause of disability– 3rd leading cause of 30-day readmissions – 3rd leading cause of death (2nd to CV disease and cancer)
• Mortality rate predicted to increase by 30% over the next decade• Exacerbations
– ~800,000 hospitalizations (+ 3.5 million COPD 2nd dx)– 1.5 million ER visits/year
• Costs for COPD in the United States, 2010 = $50 billion and rising
CDC. http://www.cdc.gov/copd/. Accessed Dec. 2, 2014. The COPD Foundation. www.copd.org. Accessed Nov. 10, 2014.
National Heart, Lung and Blood Institute (NHLBI). COPD – Learn More, Breath Better. https://www.nhlbi.nih.gov/health/educational/copd/index.htm. Accessed Nov. 10, 2014.
Guarascio AJ et al. Clinicoecon Outcomes Res. 2013;5:235-245.

Exacerbation (70%)
New Clinic Visit (1%) Emergency
(7%)
Hospitalization (92%)
30-day readmission rates for COPD are ~25%
Most COPD Costs are Hospital-related
Miravitlles M et al. Chest. 2002;121:1449-1455. Jencks SF et al. N Engl J Med. 2009; 360:1418-1428.

COPD Readmissions are Common and Costly
Condition Types of Hospital
Admission
# of Admits with
Readmission*
Readmission Rate
Avg. Medicare Payment for Readmission
Total Spending on
Readmissions Heart Failure Medical 90,273 12.5% $6,531 $590,000,000COPD Medical 52,327 10.7% $6,587 $345,000,000
Pneumonia Medical 74,419 9.5% $7,165 $533,000,000
Acute MI Surgical 20,866 13.4% $6,535 $136,000,000
CABG Surgical 18,554 13.5% $8,136 $151,000,000
PTCA Surgical 44,293 10.0% $8,109 $359,000,000
Other Vascular
Surgical 18,029 11.7% $10,091 $182,000,000
Total for 7 Conditions
318,760 $2,296,000,000
Total DRGs (% of Total)
1,134,483 (28.1%)
$7,980,000,000 (28.8%)
CABG = coronary artery bypass graft; MI = myocardial infarction; PTCA = percutaneous transluminal coronary angioplasty*Readmissions within 15 days of discharge of the initial inpatient stay
MedPAC (Medicare Payment Advisory Commission), Report to Congress. 2007.

Hospital Readmissions and the Affordable Care Act (ACA): CMS Performance Report
• Hospital readmissions have been singled out for improvement by CMS National Strategy for Quality Improvement in Health Care
• The goal of the CMS strategy is a 20% reduction in hospital readmission rates, potentially preventing 1.6 million hospitalizations and saving an estimated $15 billion
• CMS will publicly report COPD measures on Hospital Compare beginning in 2014 as part of the Hospital Inpatient Quality Reporting (IQR) program
• Data reported in the 2013 Chartbook (1/2009 – 12/2011) summarize “dry run” results shared with hospitals
• COPD readmission measure will be included in the Fiscal Year 2015 Hospital Readmissions Reduction Program (HRRP)
Centers for Medicaid and Medicare Services. Medicare Hospital Quality Chartbook. Performance Report on Outcome Measures (September 2014). Available at:http://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/HospitalQualityInits/Downloads/Medicare-Hospital-Quality-Chartbook-2014.pdf. Accessed Nov. 14, 2014.

Benefits of Guideline-based Treatment
• Improved lung function1,2
• Improved symptoms1,2
• Improved exercise tolerance1,2
• Improved QoL1,2
• Prolonged life and better QoL with smoking cessation1,2
• Delayed time to first exacerbation1,2
• Fewer exacerbations1,2
• Fewer hospitalizations1,2
• Cost savings3
1. Restrepo RD et al. Int J COPD. 2008;3:371-384. 2. Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2014. www.goldcopd.org. Accessed 3/10/14. 3. Asche CV et al. Int J Chron Obstruct Pulmon Dis. 2012;7:201-209.

Management of Acute Exacerbations

Patient Case Study (1 of 4)
• JS is a 58-year-old white male who presents to his primary care physician with painful right inguinal hernia
• Past medical history– Lack of routine health care x 20 years– Considers himself to be active, works outside as a
construction supervisor and teaches horseback-riding lessons – Denies other significant medical conditions other than punctured lung in
his early 30s due to a horseback-riding accident– Smokes 1½ to 2 PPD x 39 years
• Successfully underwent 2 open hernia repairs 3 months apart– Never screened for COPD on pre-operative evaluation and no chest
x-ray performed

Patient Case Study (2 of 4)
• JS underwent his 2nd open hernia repair • Post-operative course after 2nd surgery was
complicated by episode of bronchitis for which he presented to his PCP and was treated with azithromycin x 5 days
• PCP also prescribed:– Albuterol nebulizer solution– Ipratropium nebulizer solution– Advair inhaler BID– Albuterol inhaler prn– Prednisone 5 mg po q day– Roflumilast 500 mcg po q day
• No follow-up appointment or referral to pulmonologist

Impact of Exacerbations in COPD
Patients With Frequent Exacerbations
Higher Mortality
Faster Declinein Lung Function
Poorer Qualityof Life
Greater AirwayInflammation
COPD Foundation.

Patient Case Study (3 of 4)
• JS had 2 episodes of bronchitis over the next 3 months characterized by shortness of breath limiting activity and copious sputum production
• The first episode he received a breathing treatment in the office, chronic medications were continued and he was given levofloxacin x 10 days
• The 2nd episode he self-treated with levaquin leftover from his previous episode and refill of prednisone
• 3 months later JS presents to the emergency department with acute bronchitis, shortness of breath, copious sputum production
– Treated with IV corticosteroids, nebulizers, supplemental oxygen, cefuroxime IV
– Spirometry performed on hospital day 3 confirmed a diagnosis of COPD , FEV1 65% predicted

Management of Severe (Not Life-Threatening)
Exacerbations Requiring Hospitalization• Assess severity of symptoms, blood gases, chest radiograph • Supplemental oxygen therapy • Bronchodilators:
– Increase doses and/or frequency of short-acting bronchodilators – Combine short-acting beta2-agonists and anticholinergics– Use spacers or air-driven nebulizers
• Add oral or intravenous corticosteroids • Consider antibiotics (oral or intravenous) when signs of bacterial infection • Consider noninvasive mechanical ventilation • Monitor fluid balance and nutrition• Consider subcutaneous heparin or low molecular weight heparin• Identify and treat associated conditions (e.g. heart failure, arrhythmias)
Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2014. www.goldcopd.org. Accessed 11/10/14.

Indications for ICU Admission
• Severe dyspnea that responds inadequately to initial emergency therapy
• Changes in mental status (confusion, lethargy, coma) • Persistent or worsening hypoxemia (PaO2 <5.3 kPa, 40 mmHg)
and/or • Severe/worsening respiratory acidosis (pH <7.25) despite
supplemental • Oxygen and noninvasive ventilation • Need for invasive mechanical ventilation • Hemodynamic instability – need for vasopressors
Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2014. www.goldcopd.org. Accessed 11/10/14.

Stage 1: Initial Management Pathway for Hospitalized Patients
Slide provided by Thomashow B. NewYork-Presbyterian Hospital Clinical Pathway.

A 5-day Course of Oral CS May Be Appropriate after COPD Exacerbations Re-exacerbations in the REDUCE Trial
ITT = intention to treat; REDUCE = Reduction in the Use of Corticosteroids in Exacerbated COPD Lueppi JD et al. JAMA. 2013;309:2223-2231.
Proportion of patients without re-exacerbationITT analysisHR, 0.95 (90% CI, 0.70-1.29)P for noninferiority = 0.006
Proportion of patients without re-exacerbationPer-protocol analysis HR, 0.93 (90% CI, 0.68-1.26)P for noninferiority = 0.005
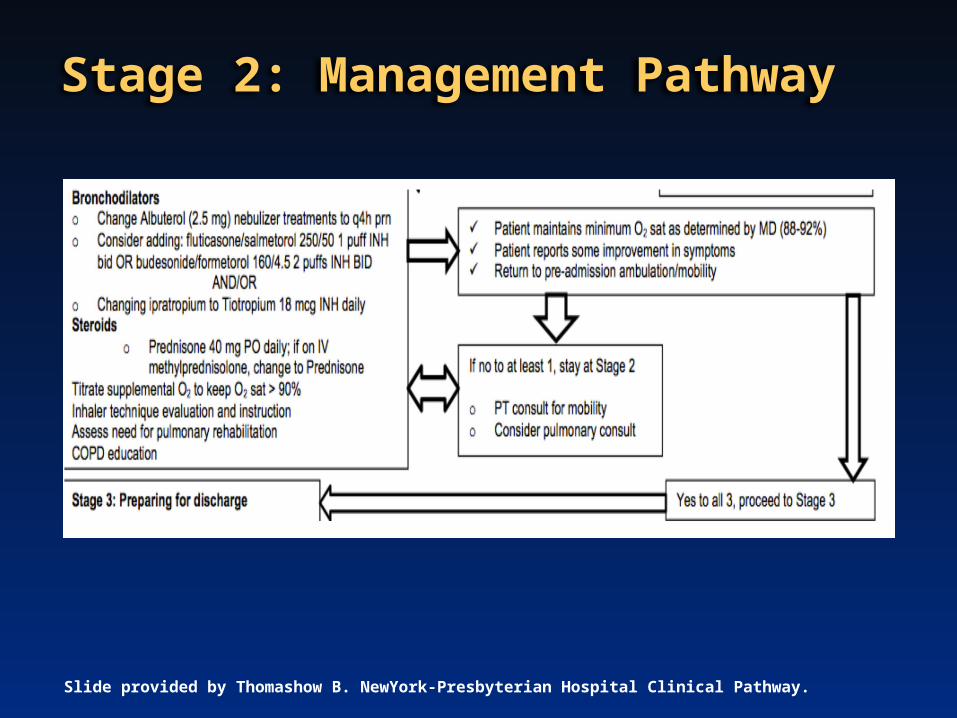
Stage 2: Management Pathway
Slide provided by Thomashow B. NewYork-Presbyterian Hospital Clinical Pathway.

Strategies for Improving COPD Across the Continuum

SYMPTOMS RISK FACTORS
High Index of Suspicion for COPD Screening and Diagnosis
Consider COPD in patients with any symptoms and history of exposure to risk factors
SYMPTOMSPersistent shortness of breath
Chronic coughChronic sputum production
Wheezing
RISK FACTORSTobacco smoke
Indoor/outdoor air pollutionOccupational pollutants
Family historyAge >40 years
Spirometry is required to make diagnosisPost-bronchodilator FEV1/FVC <0.70 confirms presence of
persistent airflow limitation*
*Post-bronchodilator FEV1/FVC measured 10-15 min after 2-4 puffs of a short-acting bronchodilatorFEV1, forced expired volume in 1 second; FVC, forced vital capacity
Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2014. www.goldcopd.org. Accessed 11/10/14.
Facilitate Discharge Transitions of Care
Patient can be discharged when he/she: Is able to use long-acting bronchodilators, either beta2-agonists
and/ or anticholinergics with or without inhaled corticosteroids Does not require inhaled short-acting beta2-agonist therapy
more frequently than every 4 hours Is able to walk across room, if previously ambulatory Is able to eat and sleep without frequent awakening by dyspnea Has been clinically stable for 12-24 hours Has stable arterial blood gases for 12-24 hours
Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2014. www.goldcopd.org. Accessed 11/10/14.

Stage 3: Discharge Planning
Slide provided by Thomashow B. NewYork-Presbyterian Hospital Clinical Pathway.

COPD ExacerbationsPreventative Measures
• Spirometry to confirm diagnosis and determine severity of COPD
• Improve guideline-based non-pharmacologic treatment
• Improve guideline-based pharmacologic treatment• Manage comorbidities• Identify and address social issues• Engage in continuous care

Prevention: The Ultimate Way to Prevent Readmissions for COPD
• Smoking cessation– Like home oxygen therapy, smoking cessation is the only
intervention that has been shown to decrease mortality at all levels of COPD
– Effective at primary, secondary, and tertiary levels of care
• Pulmonary rehabilitation• Physical activity• Good nutrition• Immunizations (influenza vaccine)

Smoking Cessation is The Most Important Thing to Slow Progression of COPD
• Quitting is challenging but achievable• Many options are available to help patients quit smoking
– Gums– Patches– Prescription medicine
• More information at: www.smokefree.gov
COPD Foundation. Quitting Smoking. Available at: http://www.copdfoundation.org/What-is-COPD/Living-with-COPD/Quitting-Smoking.aspx. Accessed Nov. 10, 2014.

Pulmonary Rehabilitation Decreases Readmissions
• Physiology of acute COPD exacerbations1
– Decline in quadriceps muscle strength of 5% between day 3 and 8 of hospital admission
– Quadriceps force continues to decline for up to 3 months after hospital discharge
– Hospitalized patients spend <10 minutes per day walking and remain inactive for up to 1 month after discharge vs those with stable COPD and similar disease severity
NNT = number needed to treat1. Suh ES et al. BMC Medicine. 2013;11:247. 2. Puhan MA et al. Cochrane Database Syst Rev. 2011:5;CD005305. doi: 10.1002/14651858.CD005305.pub3.
• High re-exacerbation and readmission risk in early recovery phase
• Cochrane Review of 9 in 432 patients
• Pulmonary rehabilitation significantly reduced ─ Hospital admissions (pooled OR 0.22,
95% CI 0.08 to 0.58), NNT = 4 (95% CI 3 to 8) over 25 weeks
─ Mortality (OR 0.28; 95% CI 0.10 to 0.84), NNT = 6 (95% CI 5 to 30) over 107 weeks

Advances in Pulmonary Rehabilitation
• Exercise training includes: endurance training, strength training, upper-limb training, and transcutaneous neuromuscular electrical stimulation
• Can be home-based
• Exercise training reduces anxiety and depression
• Exercise rehab started during acute or critical illness reduces the extent of functional decline and speeds recovery
• Pulmonary rehab started after a hospitalization for COPD exacerbation is effective, safe, and leads to a reduction in subsequent hospital admissions
• Symptomatic patients with lesser degrees of airflow limitation derive similar benefits as those with severe disease
Spruit MA et al. Am J Respir Crit Care Med. 2013;188:e13–e64.

Increased Physical Activity Prevents Readmissions for COPD
Mean Minutes Per Day of Higher Level Physical ActivityWithout 30-day ReadmissionMean n
With 30-day ReadmissionMean n
P Value
Week 1 114 ± 19 26 42 ± 14 12 0.02
Week 2 126 ± 20 25 46 ± 13 10 0.02
Week 3 139 ± 25 23 35 ± 09 9 0.20
Week 4+ 131 ± 27 17 1312 ± 10 2 0.16
Chawla H et al. Ann Am Thorac Soc. 2014;11:1203-1209.
Those with lower physical activity (<60 mins/day) over week 1 after discharge were more likely to have 30-day all-cause readmissions than those with higher activity: odds ratio = 6.7; P=0.02.

Oral Nutritional Supplements Decrease LOS and Prevent Readmissions for COPD
Outcome Unit Length of Stay(Days)
Episode Cost(US Dollars)
Readmission Within 30-days (Probability)
Effect of any ONS use (Standard error)
-1.88**(0.71)
-$1,570**(41.8)
-0.0439**(0.0162)
Predicted Outcome w/o ONS 8.75 12,523 0.335
Predicted Outcome With ONS 6.87 10,953 0.291
% Change due to ONS Use -21.5% -12.5% -13.1%
# of Observations 14,326 14,326 11,712
1. Thornton SJ et al. Chest. 2014; doi: 10.1378/chest.14-1368. [Epub ahead of print]. 2. Schols AM et al. Eur Respir J. 2014; in press | DOI: 10.1183/09031936.00070914.
*Medicare patients age 65+ out of 10,322 ONS hospitalizations and 368,097 non-ONS hospitalizations **Indicates significance at the 1% level
Effect of ONS use on length of stay (LOS) and 30-day Readmissions*1
A well-balanced diet is beneficial to all COPD patients for pulmonary benefits and benefits in metabolic and cardiovascular risk2

Recommended Vaccines for Patients with COPD
• 2014 GOLD Guidelines recommend:1
– Pneumococcal vaccine• May reduce mortality2-4
• Newer conjugated vaccines may have greater efficacy
– Influenza vaccine2,5-8
• May decrease risk for acute COPD exacerbations 1. Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2014. www.goldcopd.org. Accessed 11/10/14.2. Osthoff M et al. Swiss Med Weekly. 2013;143:213777. 3. Schembri S et al. Thorax. 2009;64:567-572. 4. Pitsiur GG et al. Respir Med. 2011;105:1776-1783. 5. Poole PJ et al. Cochrane Database Syst Rev. 2006;(1):CD002733. 6. Michiels B et al. Vaccine. 2011;29:9159-9170. 7. Walters JA et al. Cochrane Database Syst Rev. 2010;(11):CD001390. 8. Vila-Corcoles A et al. Expert Rev Vaccines. 2012;11:221-236.

Outcomes of Noninvasive Ventilation (NIPPV) for Acute Exacerbations of COPD in US1998-2008
• >4-fold increase in NIPPV use• 5% NIV required invasive mechanical support (IMV)• Those transitioning from NIPPV to IMV had a 61% greater chance of
death (30% in-hospital mortality) compared to those only treated with IMV alone (more than 20% mortality)
• Clearly defines need for– Close observation and potentially earlier intubation in some
– Alternative to IMV
Chandra D et al. Am J Respir Crit Care Med. 2012;185;2;152-159.

Long-term NPPV Targeted to Reduce Hypercapnea Improves Survival in Stable COPD
• Randomized to NPPV (n=102) or control (n=93)– Stable GOLD stage IV COPD
– Partial PaCO2 of ≥7 kPa (51.9 mm Hg) or pH >7.35
• NPPV to baseline PaCO2 by ≥20% or PaCO2 <6.5 kPa (48.1 mm Hg)
• Only ADE: rash in 14% - change type of mask
HR = hazard ratio; NPPV = non-invasive positive pressure ventilation; PaCO2 = carbon dioxide pressure
Köhnlein T et al. Lancet Respir Med. 2014;2:698-705.
1-year mortality12% NPPV vs 33% control
HR 0.24 (95% CI 0.11-0.49; P=0.0004)

COPD ExacerbationsPreventative Measures: Non-pharmacologic
• Spirometry to confirm diagnosis and determine severity of COPD
• Improve guideline-based non-pharmacologic treatment• Improve guideline-based pharmacologic treatment
• Manage comorbidities• Identify and address social issues• Engage in continuous care


GOLD 2014 Categories of COPD Severity and Suggested Therapies
Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2014. www.goldcopd.org. Accessed 11/10/14.
LABA + LAMA

COPD Foundation Guidelines Spirometry Grades
• SG 0– Normal spirometry does not rule out emphysema, chronic bronchitis,
asthma, or risk of developing either exacerbations or COPD• SG 1 (Mild)
– FEV1/FVC ratio <0.7, FEV1 >60% predicted• SG 2 (Moderate)
– FEV1/FVC ratio <0.7, 30%-60% predicted• SG 3 (Severe)
– FEV1/FVC ratio <0.7, FEV1 <30% predicted• SG U (Undefined)
– FEV1/FVC ratio >0.7, FEV1 <80% predicted– Consistent with restriction, muscle weakness, and other pathologies
COPD Foundation. COPD Treatment. www.copdfoundation.org/Learn-More/For-Medical-Professionals/Treatment.aspx. Accessed 11/8/14.

COPD Foundation Guide for COPD Treatment
*Indicated if chronic bronchitis, high exacerbation risk, and spirometry grades 2/3 all present**Suggest regular exercise program for all with COPD; those with SG2/3 should be considered for pulmonary rehab+Recommended in select cases with upper lobe predominant emphysema++Off label, consider potential cardiac risks and resistance concerns
COPD Foundation. COPD Treatment. www.copdfoundation.org/Learn-More/For-Medical-Professionals/Treatment.aspx. Accessed 2/8/14.

Consider Switching from LABA/ICS TO LABA Only if Low Risk
• Moderate COPD and no exacerbations in previous year • 26-week, randomized double-blind, double-dummy, parallel-group study
– 581 patients with moderate COPD who were receiving salmeterol/fluticasone (SFC) for ≥ months
– Randomized to indacaterol 150 μg once daily or SFC 50/500 μg twice daily • Non-inferiority achieved based on trough FEV1 after 12 weeks• No significant differences for
– Breathlessness (transition dyspnea index) – Health status (Saint George's Respiratory Questionnaire) – Rescue medication use or COPD exacerbation rates over 26 weeks
ICS = inhaled corticosteroids; LABA = long-acting beta2 agonist
Rossi A et al. Eur Respir J. 2014. pii: erj01268-2014. [Epub ahead of print].
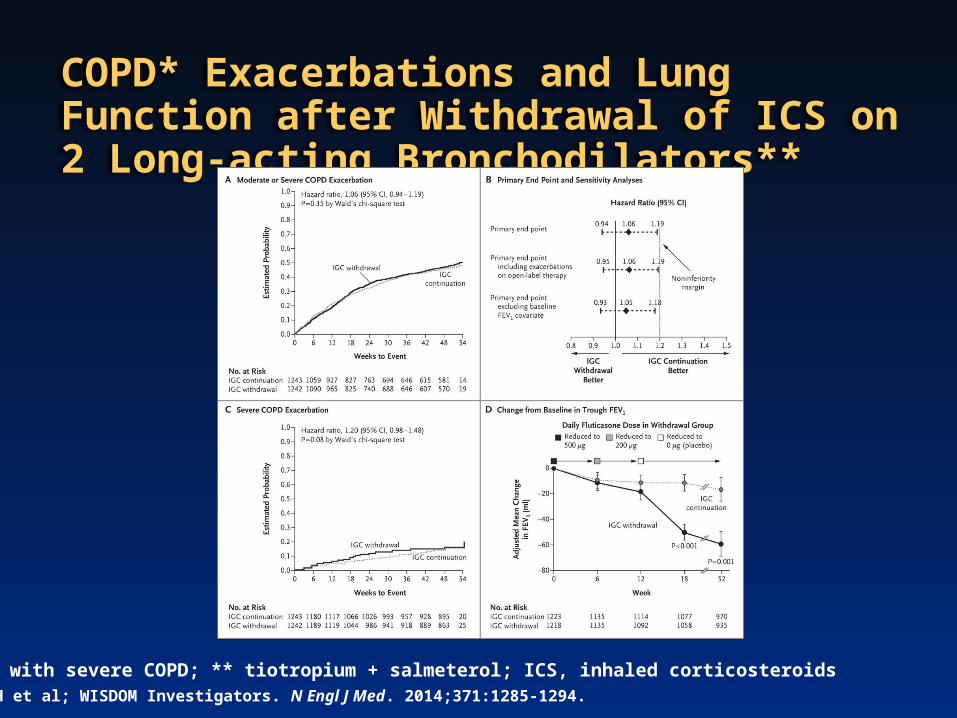
COPD* Exacerbations and Lung Function after Withdrawal of ICS on 2 Long-acting Bronchodilators**
*Patients with severe COPD; ** tiotropium + salmeterol; ICS, inhaled corticosteroids Magnussen H et al; WISDOM Investigators. N Engl J Med. 2014;371:1285-1294.

There are Many Inhaler Devices Available in the United States – Choice is Important
Diskus®
Flexhaler®
Handihaler®
Pressair®
SMI
Neohaler™
Aerolizer™ Twisthaler®
Breo Ellipta®
Neohaler™ Respimat® Soft Mist™
MDI

Strategies for Individualizing Inhaler Choice
• Good hand-breath coordination is required for meter-dose inhalers (MDIs) – May not be suitable for elderly, confused, or those with hand
conditions (e.g. arthritis)
• Dry-powder inhalers (DPIs) do not require coordination of actuation and inhalation and are easier to use than MDIs– Breath actuation may be difficult in patients with poor inspiratory
effort
• Avoid changing inhaler types for individual patients
Vincken W et al. Prim Care Respir J. 2010;19:10-20.De Coster DA et al. Cur Respir Care Rep. 2014;;3:121-132.

Nebulizers May be Beneficial for Some Patients with COPD
• Effective drug delivery requires less intensive patient training vs pMDIs and DPIs1
• Newer portable and efficient models available1 • Efficacy of long-term nebulizer therapy is similar or
superior to pMDI/DPIs in moderate-to-severe COPD, including during exacerbations1
• Consider maintenance nebulizers in1
– Elderly patients– Severe COPD– Frequent exacerbations– Physical and/or cognitive limitations
• Patient/caregiver satisfaction is high2
Small-Volume Nebulizers
1. Dhand R et al. COPD. 2012;9:58-72. 2. Sharafkhaneh A et al. COPD. 2013;10:482-492.

Medications Available via Nebulizer
Medication (Class)1 NotesAlbuterol (SABA)Formoterol (LABA) Significantly improved FEV(1) and dyspnea, decreased rescue medication
use, and a lower incidence of AEs and COPD exacerbations when added to maintenance tiotropium in patients with moderate to severe COPD2
Arformoterol (LABA) ∼40% lower risk of respiratory death or COPD exacerbation-related hospitalization over 1 year versus placebo in patients with COPD and FEV1 ≤ 65% predicted3
Ipratropium bromide (Short-acting anticholinergic)
Beclomethasone dipropionate, flunisolide, fluticasone propionate, budesonide
Valid alternative to inhalers in acute exacerbations of COPD with similar efficacy as oral or ICS and good tolerability4
ICS = inhaled corticosteroid; SABA = short-acting beta2 agonist; LABA = long-acting beta2 agonist
1. Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2014. www.goldcopd.org. Accessed 3/10/14. 2. Tashkin DP et al. Adv Ther. 2009; 26:1024-1034. 3. Donohue JF et al. Chest. 2014. doi:10.1378/chest.14-0117. 4. Melani AS. Respiratory Care. 2012;57:1161-1174.

Identify and Address Poor Adherence
Barriers to adherence Inadequate education about
COPD and therapy1 Perceived burden of
medication regimen1,2
Device is difficult to use3
Depressed mood3
Medication-related cost3
Adverse effects3
1. LaForest L et al. Prim Care Resp J. 2010;19:148-154.
2. George J et al. Chest. 2005;128:3198-3204.
3. Restrepo RD et al. Int J COPD. 2008;3:371-384.
Red Flags for non-adherence
• Failure to refill prescriptions• Excessive use of rescue
medication• Frequent exacerbations• Rapid decline in FEV1

Predictors of Exacerbations and Readmissions Opportunities for Improvement in the Inpatient Setting
• Spirometry to confirm diagnosis and determine severity of COPD
• Improve guideline-based pharmacologic treatment• Improve guideline-based non-pharmacologic treatment• Manage comorbidities
• Identify and address social issues• Engage in continuous care

Interplay of Comorbidities in COPD
Barnes PJ et al. Eur Respir J. 2009;33:1165-852. Barnes PJ. PLoS Med 2010;7:e1000220.

Comorbidities Increase the Risk of Readmission
Only 30% of readmission secondary to index cause

First-choice Treatments for Comorbidities in COPD
Comorbidity 1st Choice Treatment IssuesHypertension ACEI or ARB Avoid beta blockers if hypertension the only comorbidityHeart failure Cardioselective beta1-blocker in addition to
ACEI or ARBDiuretics (loop preferred)
If asthmatic component avoid beta blockerOral corticosteroids may worsen HF – use ICS
Ischemic heart disease
Cardioselective beta1-blocker in addition to ACEI (regardless of BP or LV function)
ICS may have protective effect for CV eventsAvoid high dose beta 2 agonists in USA
Atrial fibrillation Non-dihydropyridine CCB (verapamil or diltiazem) or a cardioselective beta-blocker (i.e. bisoprolol)
Avoid beta 2 agonist, nonselective beta blockers, theophylline, oral corticosteroids
Diabetes Metformin at a low dose and gradual titration Consider contraindications: (diarrhea/abdominal cramp- ing/ lactic acidosis risk/ vitamin B12 deficiency/acidosis/hypoxia/dehydration/unstable heart failure)
Metabolic syndrome MetforminStatins ACE or ARB
Consider drug interactions and contraindications for statins, niacin
Osteoporosis Vitamin D 800 IU/day and calcium 1 gr/dayBisphosphonates if osteoporosis
Oral bisphosphonates cause significant gastrointestinal effects and dosing requirements
Depression and anxiety
Psychological therapy, benzodiazepines and SSRIs
Choice of antidepressant should be made with consideration of risks, age, previous treatment, interactions, preferences and costs
Tsiligianni IG et al. Curr Drug Targets. 2013;14:158-176.

Considerations for Specific Medications for Comorbidities in COPD
Medication Considerations Cardioselective beta blockers
• Reduce the risk of exacerbations and improve survival in patients with COPD in long term treatment
• Associated with reduced mortality in acute COPD exacerbation and in COPD with atherosclerosis
• No significantly change in FEV1 or respiratory symptoms, no affect on the FEV1 treatment response to beta2-agonists
• Conflicted results in FEV1 improvement in long term treatment studies [146, 147].Suggestions:• Despite benefits they are still underused in COPD• Not a first choice for hypertension• An individualized approach starting at low doses and gradually titrating up is recommended • Caution with cardioselective agents as cardioselectivity decreases with increased doses
Angiotensin converting enzyme inhibitors or Angiotensin receptor blockers
• Chronic lowering of ACE improves pulmonary inflammation, respiratory muscle function, peripheral use of oxygen for long term treatment in COPD
• Reduce hospitalization and mortality in patients with COPDSuggestions:• May be used in hypertension, CVD, metabolic syndrome with hypertension component
Tsiligianni IG et al. Curr Drug Targets. 2013;14:158-176.

Considerations for Specific Medications for Comorbidities in COPD (cont’d)
Medication ConsiderationsStatins • Recent prospective, randomized, double-blind, placebo-controlled trial in moderate to severe COPD
showed no difference in exacerbation rate or mortality• Have anti-inflammatory and anti-oxidant properties in the lungs• Increase exercise time and decrease the levels of high-sensitivity C-reactive protein • Reduce the decline in lung function• Provide protection against the development of lung cancer • Reduce requirement for intubation in exacerbations Suggestions:• May be useful in metabolic syndrome, dyslipidemias, cardiovascular disease
Beta 2 agonists • Beta-blockers may neutralize the b2-agonists’ efficacy and COPD patients may have high tolerance for beta-blockers
• Survival benefit for beta-blockers was not found among patients concurrently using beta-agonists or with severe COPD or asthma after myocardial infarction
Suggestions:• Best to avoid if possible in CVD and concomitant cardioselective beta-blocker use in COPD.
Anticholinergic agents
• Reduction in cardiac adverse events was associated with tiotropium in the UPLIFT study Suggestions:• Start treatment with a long-acting antimuscarinic agent rather than LABA when patients have COPD
with heart failure or when they have other CVD requiring use beta-blockers
1. Tsiligianni IG et al. Curr Drug Targets. 2013;14:158-176. 2. Criner GJ et al; COPD Clinical Research Network; Canadian Institutes of Health Research. N Engl J Med. 2014;370:2201-2210.
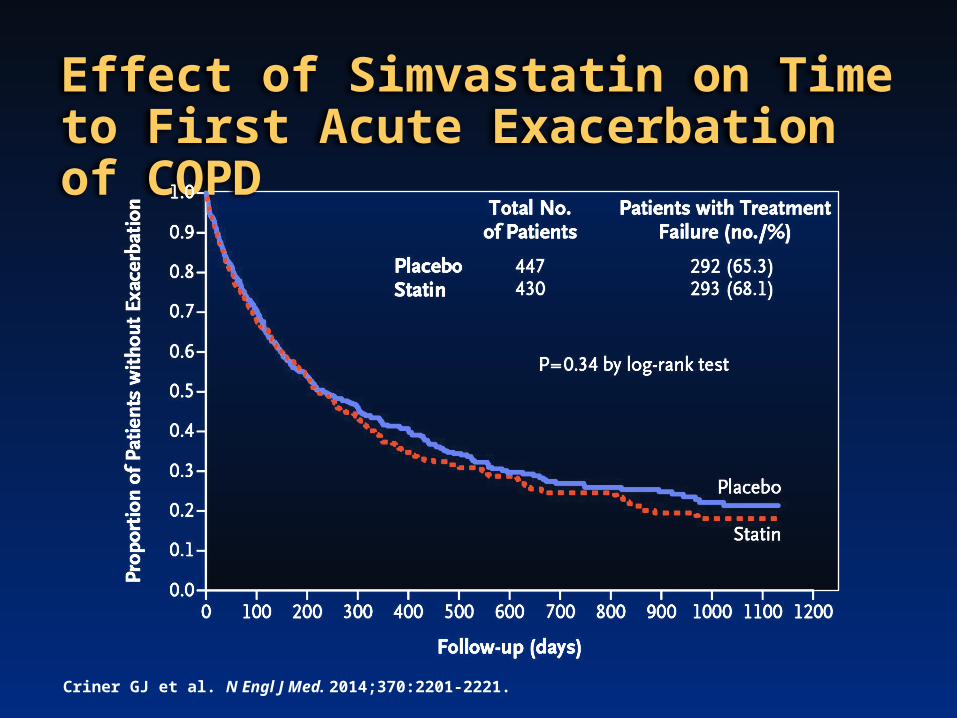
Effect of Simvastatin on Time to First Acute Exacerbation of COPD
Criner GJ et al. N Engl J Med. 2014;370:2201-2221.

Considerations for Specific Medications for Comorbidities in COPD (cont’d)
Medication Considerations Inhaled Corticosteroids
• Possible protective effect against ischemic cardiac events and acute myocardial infarction
Suggestions:• In cases of COPD and DM glucose monitoring and titration of antidiabetic treatment is
required.• Evaluate for increased risk of fractures and loss of bone mineral density• In patients receiving high dose of ICS or low to medium dose ICS with frequent use of
oral CS screening for osteopenia or osteoporosis should be performed Systemic Corticosteroids
• Meta-analysis that included 24 studies suggested high dose oral CS have potentially harmful adverse effects (e.g. diabetes, hypertension, osteoporosis)
• In the case of AECOPD if systemic glucocorticoid steroids used close monitoring of serum glucose is recommended
Suggestions:• If used in COPD close monitoring for diabetes and osteoporosis is recommended.
Specific recommendations for osteoporosis management should be followed if patients take GC>3 months
• GOLD guidelines suggest limited dosage (7-10 days) and avoidance of recurrentcourses of systemic CS for COPD exacerbations
Tsiligianni IG et al. Curr Drug Targets. 2013;14:158-176.

Stable state
THE FREQUENT EXACERBATOR PHENOTYPEHi
gher
exa
cerb
atio
n su
scep
tibilit
y
Pers
isten
t inf
lam
mat
ion/
slowe
r rec
over
y• Greater inflammation• Increases susceptibility to viral infection• Greater bacterial colonization• Faster FEV1 and functional decline• Worse health status • More severe depression• Worsened comorbidity• Increase hospitalization and mortality
INCREASED EXACERBATION SUSCEPTIBILITY
The Frequent Exacerbator Phenotype: Identify and Target (Non-pharmacologic and Pharmacologic)
Wedzicha JA et al. BMC Med. 2013;11:181.
Anti-inflammatory agents can modify the frequent exacerbator phenotype so that patients become infrequent exacerbators
EXACERBATION
Exacerbation triggers-Bacteria-Viruses-Irritants

COPD ExacerbationsPreventative Measures
• Spirometry to confirm diagnosis and determine severity of COPD
• Improve guideline-based non-pharmacologic treatment• Improve guideline-based pharmacologic treatment• Manage comorbidities• Identify and address social issues
• Engage in continuous care

Impact of Social Issues
• Among the countries in the Organization for Economic Development, the United States ranks first in health care spending, but 25th in spending on social services
• Studies have shown the powerful effects that “social determinants” like safe housing, healthful foods, and opportunities for education and employment have on health
• Experts estimate that medical care accounts for only 10% of overall health, with social, environmental, and behavioral factors accounting for the rest
Bradley EH et al. BMJ Qual Saf. 2011;20:826-831.

Social Issues Have a Significant Impact on Readmissions

The “Post-Hospital Syndrome”
• Sleep deprivation• Nutritional issues• Aspiration risks• Deconditioning• Inadequately addressed pain or discomfort• Cognitive issues – sleep/stress/medications• “Marginal clothing”
Krumholz HM. N Engl J Med. 2013;368:100-102.

COPD ExacerbationsPreventative Measures
• Spirometry to confirm diagnosis and determine severity of COPD
• Improve guideline-based non-pharmacologic treatment• Improve guideline-based pharmacologic treatment• Manage comorbidities• Identify and address social issues• Engage in continuous care

Care Transition and Coordination
Models of Care and Strategies for Implementation

Provide a Spectrum of Support for Patients With COPD
Spruit MA et al. Am J Respir Crit Care Med. 2013;188:e13–e64.
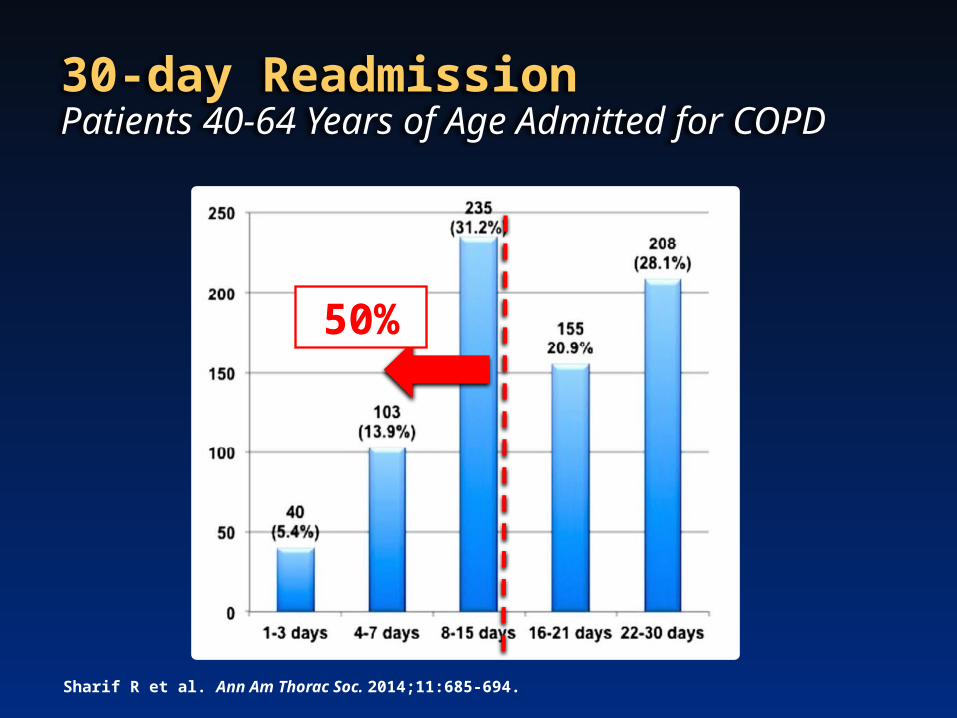
50%
30-day Readmission Patients 40-64 Years of Age Admitted for COPD
Sharif R et al. Ann Am Thorac Soc. 2014;11:685-694.

Transitional Care Management (TCM)
CMS 2013 – 2 new payment codes (99495/99456) to incentivize ambulatory care providers to participate in TCM
CMS will pay provider submitting the claim during 30-day post discharge window
To bill, must provide 3 key services: Must contact patient within 2 days of discharge
Have face-to-face visit within 7-14 days of discharge Provide indicated care-coordinated services during 30 days post
discharge, including review of discharge info, review of pending tests and treatments, education, and arrange referrals and needed community resources
Kangovi S, Grande D. Chest. 2014;145:149-155.

Patient Case Study (4 of 4)
• JS is discharged on hospital day 3 following admission for COPD exacerbation
• He returns for follow-up visit, pulmonary rehabilitation and patient education 1 week later
• He successfully stops smoking after realizing the seriousness of his condition
• He noted: “Nothing has slowed me down like this before… I did not know I had a lung condition, I just thought it was part of getting older and smoking for so long. I know now that it is serious and I have to deal with it.”

Integrated Disease Management (IDM) Programs Work• Aim of IDM: To establish a program of different components of care
(i.e. self-management, exercise, nutrition) in which several health care providers collaborate to provide efficient and good quality of care
• Cochrane review of 26 RCTs – 2997 patients with COPD (mean age 68 years)– Mean FEV1 44% predicted
• Patients in IDM vs controls – Significantly improved quality of life scores – Clinically relevant improvement of 44 m on 6-min walking distance– Fewer patients with ≥1 respiratory related hospital admission
(decreased from 27 to 20 per 100 patients)
– Significantly decreased duration of hospitalization (by nearly 4 days)
Kuis AL et al. Thorax. 2014. doi: 10.1136/thoraxjnl-2013-204974. [Epub ahead of print].

A Multicomponent Disease Management Program Can Be Cost Effective• Intervention
– Single 1.5-h group education session conducted by case manager
– Individualized written action plan that included: (1) a description of the signs and symptoms of an exacerbation that should prompt initiation of self-treatment, (2) refillable prescriptions for prednisone and an oral antibiotic, (3) contact information for a case manager, and (4) the telephone number of the 24-hour VA nursing helpline
– Began action-plan medications for symptoms that were substantially worse than usual
– Case manager made monthly phone calls to each patient
– Patients encouraged to call the case manager during regular working hours if they took action-plan medications or if they had questions relating to their medical care
– No regularly scheduled clinic visits for the remainder of the 1-year follow-up period
• Intervention cost: $241,620 or $650 per patient• The total mean±SD per patient in the DM group was $4491±4678 compared to
$5084±5060 representing a $593 per patient cost savings
Dewan NA et al. COPD. 2011;8:153-159.

Patient and Caregiver Engagement is Important
• Educate, engage patient and family • Develop individualized self-treatment plan for
exacerbations• Follow-up call monthly by a case manager
– Lower hospitalization rate and ED visits
Rice KL et al. Am J Respir Crit Care Med. 2010;182:890-896.

Key Points
• No simple answer to reducing hospital readmissions: – Move away from “disease-centered” to “patient-centered”
care– Optimize medical therapy and address comorbidities– Prevent “post-hospital syndrome”– Address social issues– Coordinate follow-up care (in-hospital care and with PCP) –
communicate with treating physicians– Engage patient (education, phone call reminders, etc.)

FREE iPHONE APP IS NOW AVAILABLE!
The COPD Foundation’s new mobile application includes:
• 7 Severity Domains• Spirometry Grades Chart • COPD Assessment Test (CAT) • Breathlessness Scale (mMRC) • Therapy Chart• COPD Medications• Spirometry Results• And much more!
Scan the QR code on the phone above, or go to:http://www.copdfoundation.org/Learn-More/For-Medical-Professionals/Treatment.aspx

A WEALTH OF RESOURCES FOR YOU AND YOUR PATIENTS
HTTP://COPD.OIONDEMAND.COM
A Wealth of Resources are Available for You and Your PatientsGo to: http://copd.oiondemand.com
Register your Guide at:copdfoundation.org/
PocketGuideRegistration.aspx
copdfoundation.org/Learn-More/Educational-Materials/Brochures.aspxDownloads and Translations

Learn, Connect, and Engage at COPD9USA
COPD9USA EXECUTIVE BOARD• Byron Thomashow, MD• Stephen Rennard, MD• David Mannino, MD• Ravi Kalhan, MD• John Walsh
KEY OPPORTUNITIES• Plenary sessions on hot topics
and 3 dedicated tracks for clinical, research and care delivery topics
• Best practices in readmission reduction, team based care, asthma and COPD overlap, and more
• Young investigator and physician in training development and mentorship programs

Participant CME Evaluation
• Please take out the Participant CME Post-survey and Evaluation Form from the back of your packet and complete to receive credit.
• If you are not seeking credit, we ask that you fill out the information pertaining to your degree and specialty, as well as the few post-activity survey questions measuring the knowledge and competence you have garnered from this program. The post-survey begins on page 1 of the evaluation form.
• Your participation will help shape future CME activities.
Thank you for joining us today!