Embed Size (px)
Citation preview
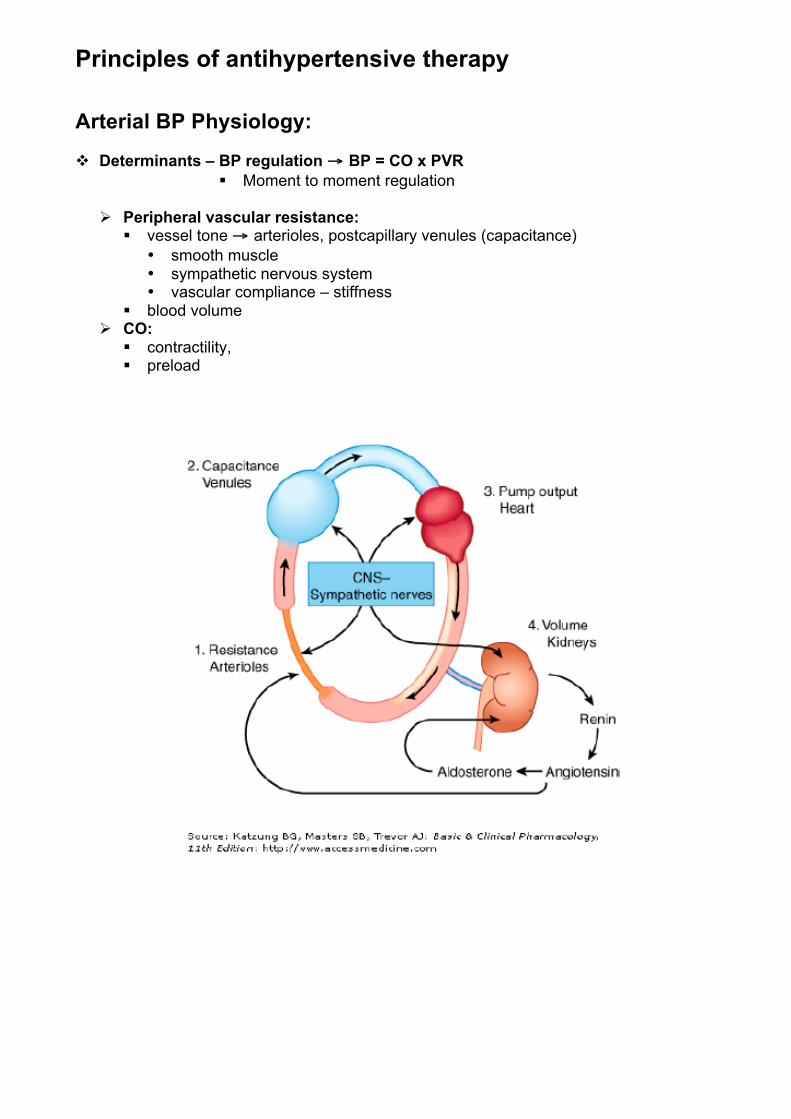
Principles of antihypertensive therapy Arterial BP Physiology: ! Determinants – BP regulation !! BP = CO x PVR
" Moment to moment regulation
# Peripheral vascular resistance: " vessel tone !! arterioles, postcapillary venules (capacitance)
• smooth muscle • sympathetic nervous system • vascular compliance – stiffness
" blood volume # CO:
" contractility, " preload
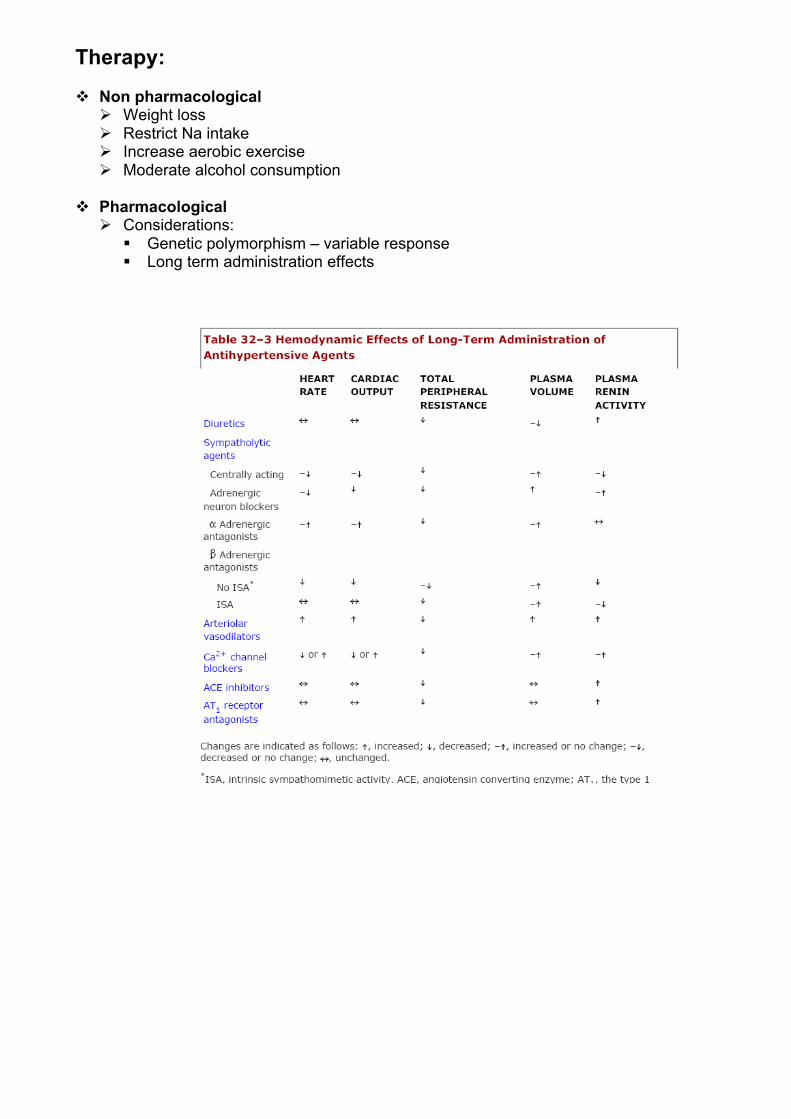
Therapy: ! Non pharmacological
# Weight loss # Restrict Na intake # Increase aerobic exercise # Moderate alcohol consumption
! Pharmacological # Considerations:
" Genetic polymorphism – variable response " Long term administration effects
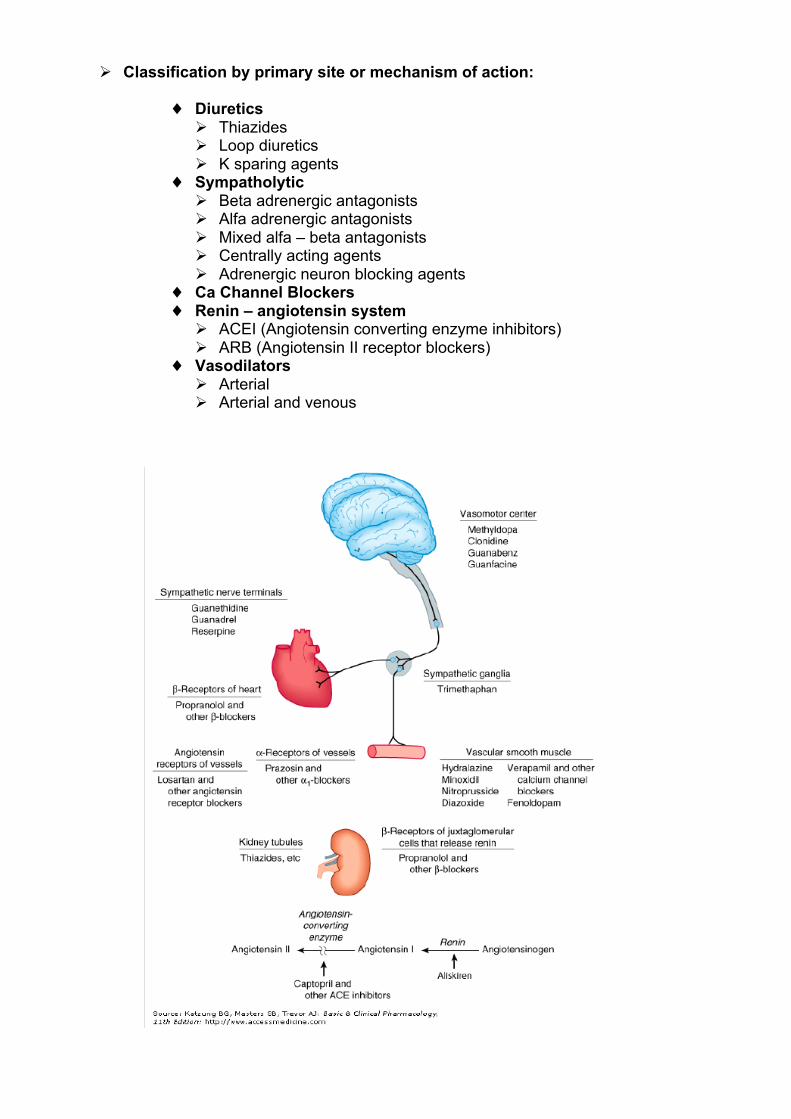
# Classification by primary site or mechanism of action:
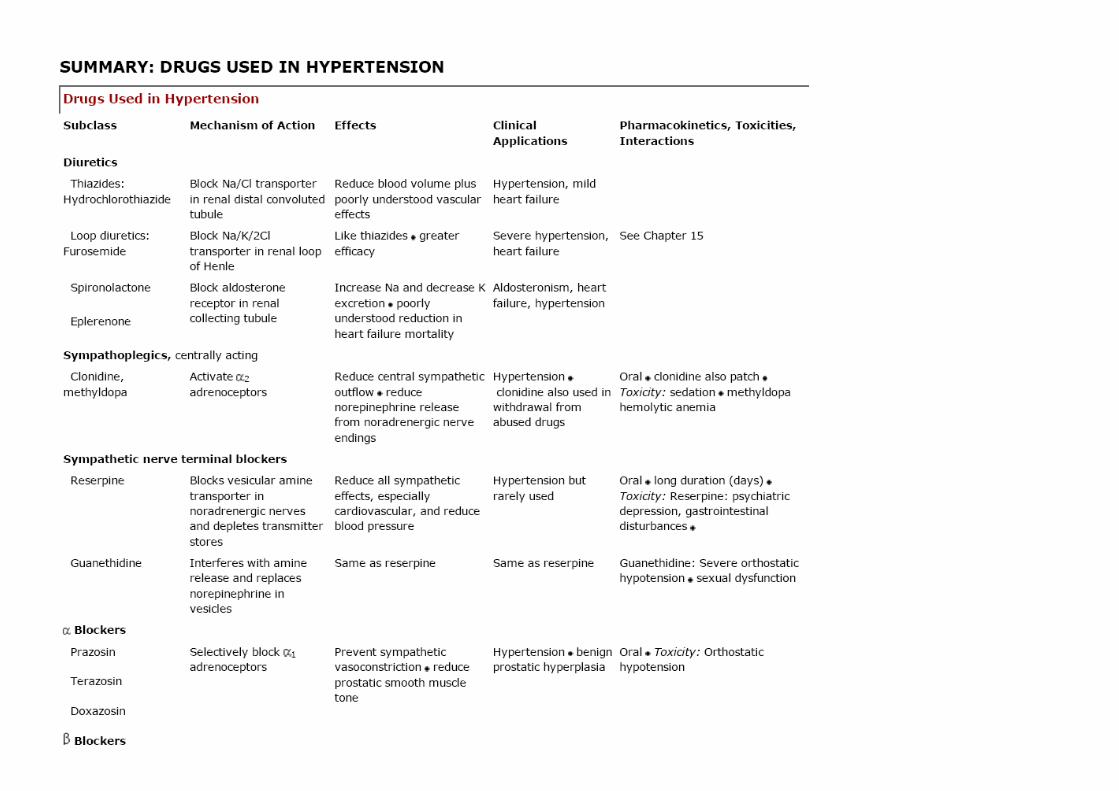
" Diuretics # Thiazides # Loop diuretics # K sparing agents
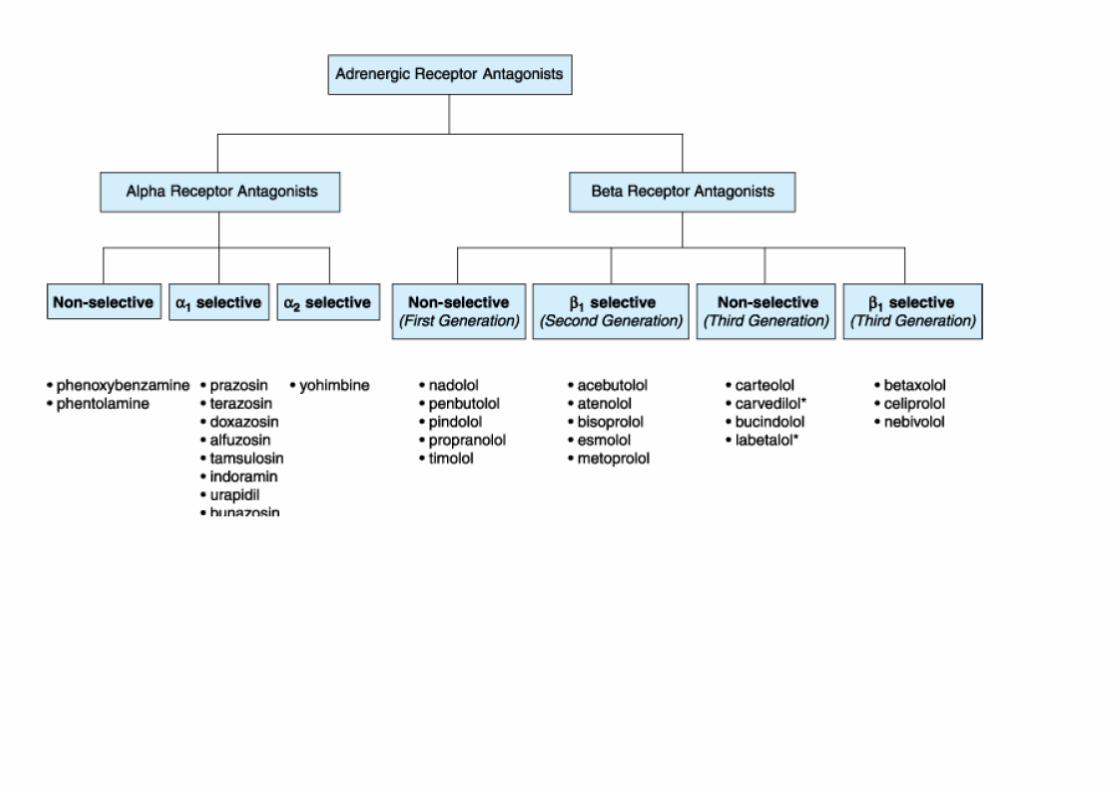
" Sympatholytic # Beta adrenergic antagonists # Alfa adrenergic antagonists # Mixed alfa – beta antagonists # Centrally acting agents # Adrenergic neuron blocking agents
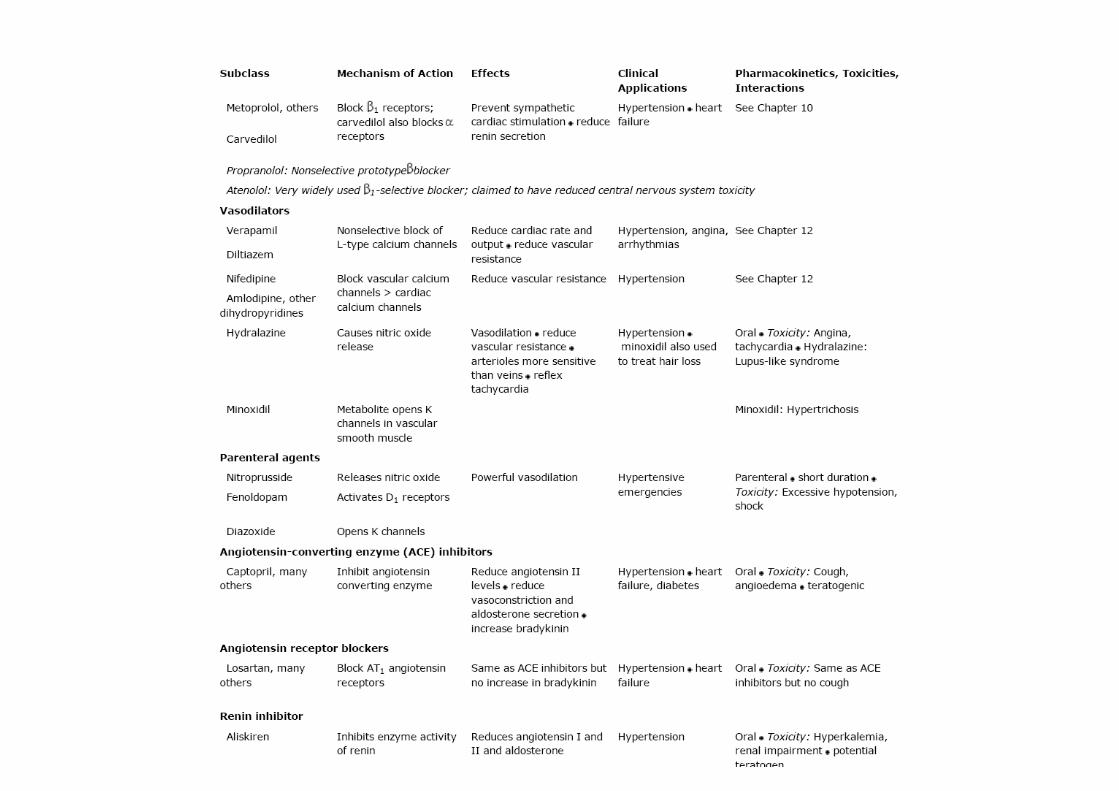
" Ca Channel Blockers " Renin – angiotensin system
# ACEI (Angiotensin converting enzyme inhibitors) # ARB (Angiotensin II receptor blockers)
" Vasodilators # Arterial # Arterial and venous
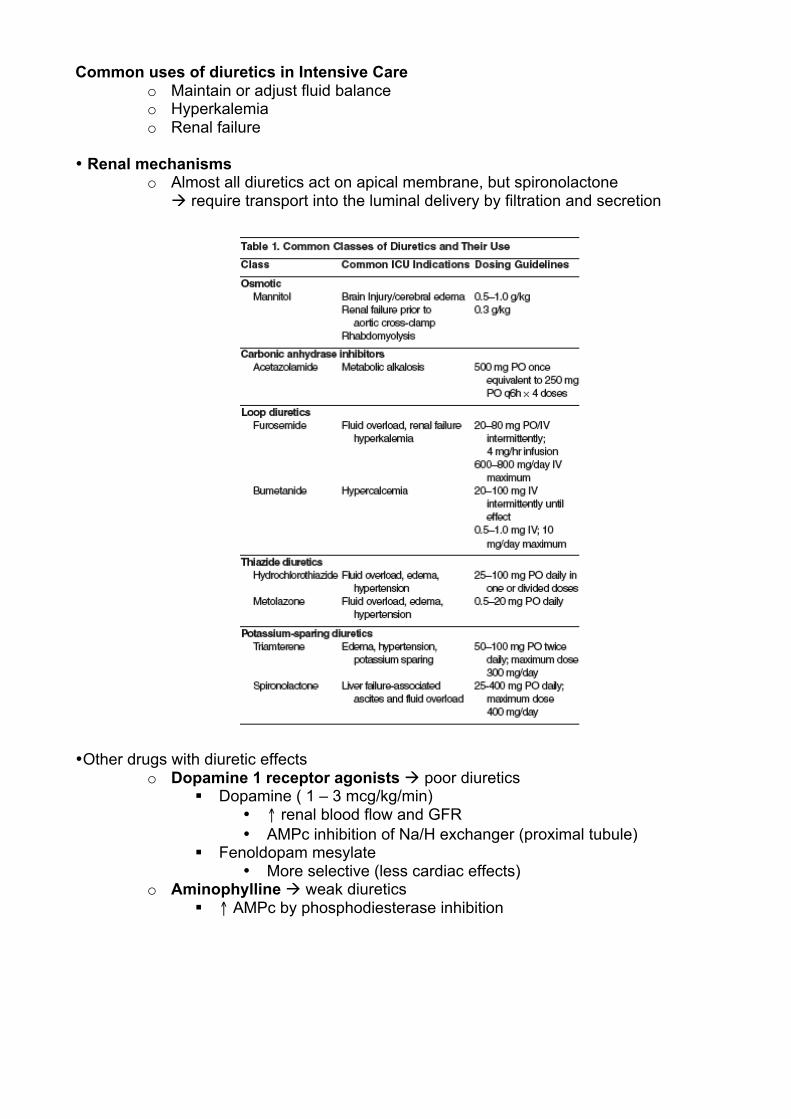
Common uses of diuretics in Intensive Care
o Maintain or adjust fluid balance o Hyperkalemia o Renal failure
• Renal mechanisms o Almost all diuretics act on apical membrane, but spironolactone
$ require transport into the luminal delivery by filtration and secretion
• Other drugs with diuretic effects o Dopamine 1 receptor agonists $ poor diuretics
" Dopamine ( 1 – 3 mcg/kg/min) • # renal blood flow and GFR • AMPc inhibition of Na/H exchanger (proximal tubule)
" Fenoldopam mesylate • More selective (less cardiac effects)
o Aminophylline $ weak diuretics " # AMPc by phosphodiesterase inhibition
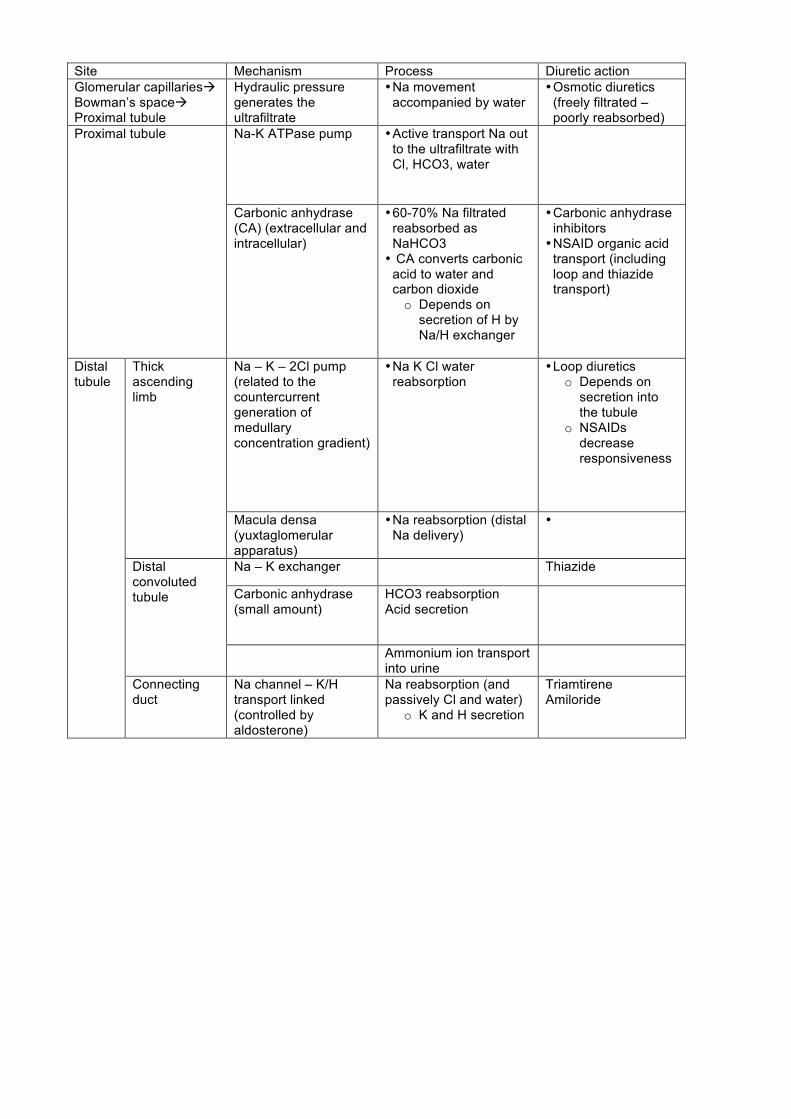
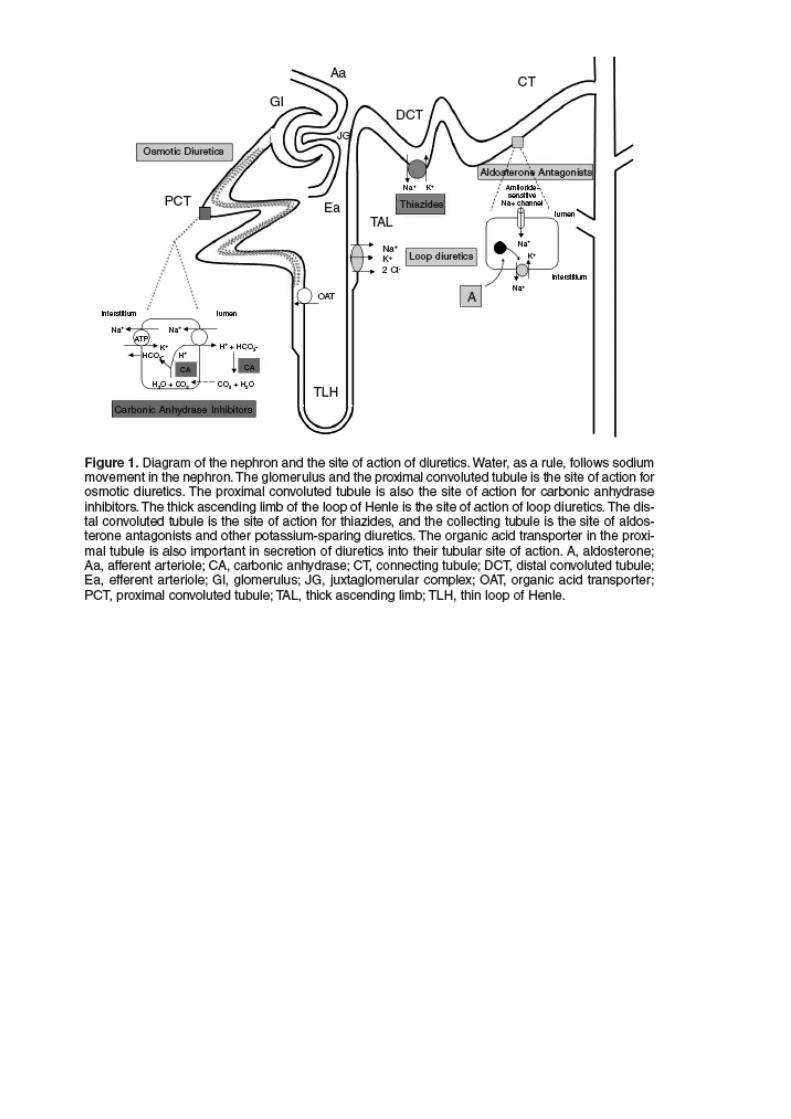
Site Mechanism Process Diuretic action Glomerular capillaries$ Bowman’s space$ Proximal tubule
Hydraulic pressure generates the ultrafiltrate
• Na movement accompanied by water
• Osmotic diuretics (freely filtrated – poorly reabsorbed)
Na-K ATPase pump • Active transport Na out to the ultrafiltrate with Cl, HCO3, water
Proximal tubule
Carbonic anhydrase (CA) (extracellular and intracellular)
• 60-70% Na filtrated reabsorbed as NaHCO3 • CA converts carbonic
acid to water and carbon dioxide o Depends on
secretion of H by Na/H exchanger
• Carbonic anhydrase inhibitors • NSAID organic acid
transport (including loop and thiazide transport)
Na – K – 2Cl pump (related to the countercurrent generation of medullary concentration gradient)
• Na K Cl water reabsorption
• Loop diuretics o Depends on
secretion into the tubule
o NSAIDs decrease responsiveness
Thick ascending limb
Macula densa (yuxtaglomerular apparatus)
• Na reabsorption (distal Na delivery)
•
Na – K exchanger Thiazide
Carbonic anhydrase (small amount)
HCO3 reabsorption Acid secretion
Distal convoluted tubule
Ammonium ion transport into urine
Distal tubule
Connecting duct
Na channel – K/H transport linked (controlled by aldosterone)
Na reabsorption (and passively Cl and water)
o K and H secretion
Triamtirene Amiloride
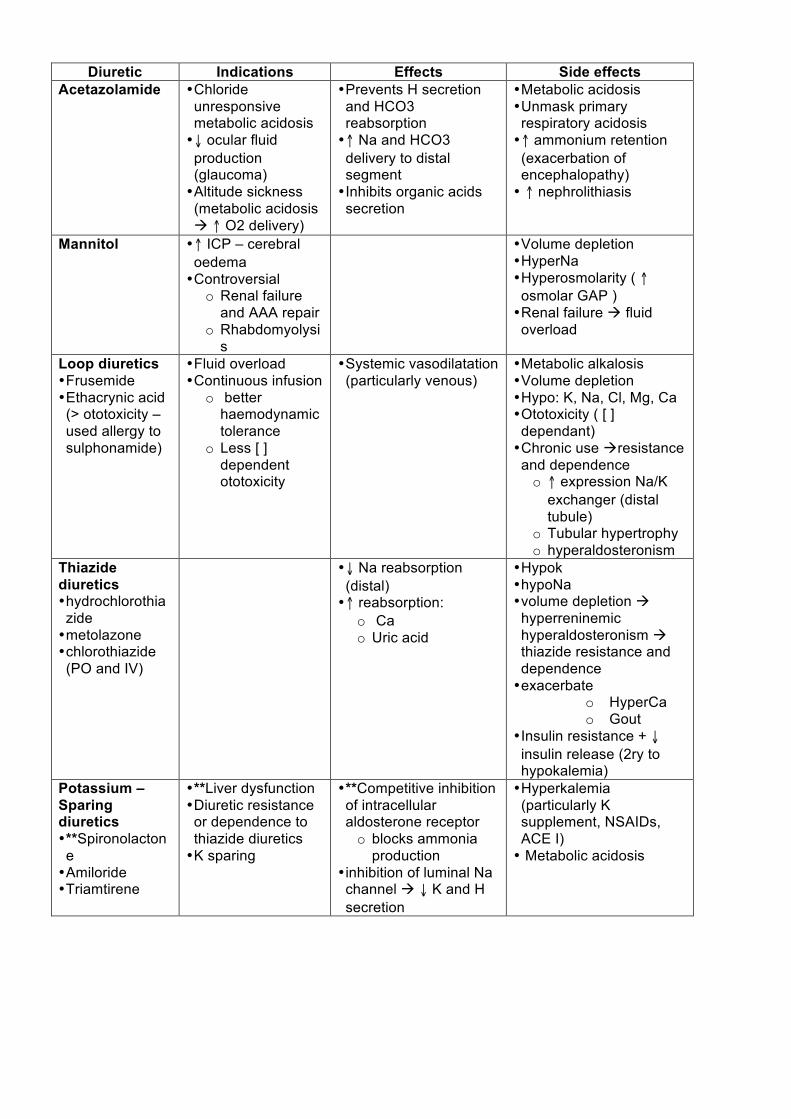
Diuretic Indications Effects Side effects
Acetazolamide • Chloride unresponsive metabolic acidosis • $ ocular fluid production (glaucoma) • Altitude sickness (metabolic acidosis $ # O2 delivery)
• Prevents H secretion and HCO3 reabsorption • # Na and HCO3 delivery to distal segment • Inhibits organic acids secretion
• Metabolic acidosis • Unmask primary respiratory acidosis • # ammonium retention (exacerbation of encephalopathy) • # nephrolithiasis
Mannitol • # ICP – cerebral oedema • Controversial
o Renal failure and AAA repair
o Rhabdomyolysis
• Volume depletion • HyperNa • Hyperosmolarity ( # osmolar GAP ) • Renal failure $ fluid overload
Loop diuretics • Frusemide • Ethacrynic acid (> ototoxicity – used allergy to sulphonamide)
• Fluid overload • Continuous infusion
o better haemodynamic tolerance
o Less [ ] dependent ototoxicity
• Systemic vasodilatation (particularly venous)
• Metabolic alkalosis • Volume depletion • Hypo: K, Na, Cl, Mg, Ca • Ototoxicity ( [ ] dependant) • Chronic use $resistance and dependence o # expression Na/K
exchanger (distal tubule)
o Tubular hypertrophy o hyperaldosteronism
Thiazide diuretics • hydrochlorothiazide • metolazone • chlorothiazide (PO and IV)
• $ Na reabsorption (distal) • # reabsorption:
o Ca o Uric acid
• Hypok • hypoNa • volume depletion $ hyperreninemic hyperaldosteronism $ thiazide resistance and dependence • exacerbate
o HyperCa o Gout
• Insulin resistance + $ insulin release (2ry to hypokalemia)
Potassium – Sparing diuretics • **Spironolactone • Amiloride • Triamtirene
• **Liver dysfunction • Diuretic resistance or dependence to thiazide diuretics • K sparing
• **Competitive inhibition of intracellular aldosterone receptor o blocks ammonia
production • inhibition of luminal Na channel $ $ K and H secretion
• Hyperkalemia (particularly K supplement, NSAIDs, ACE I) • Metabolic acidosis
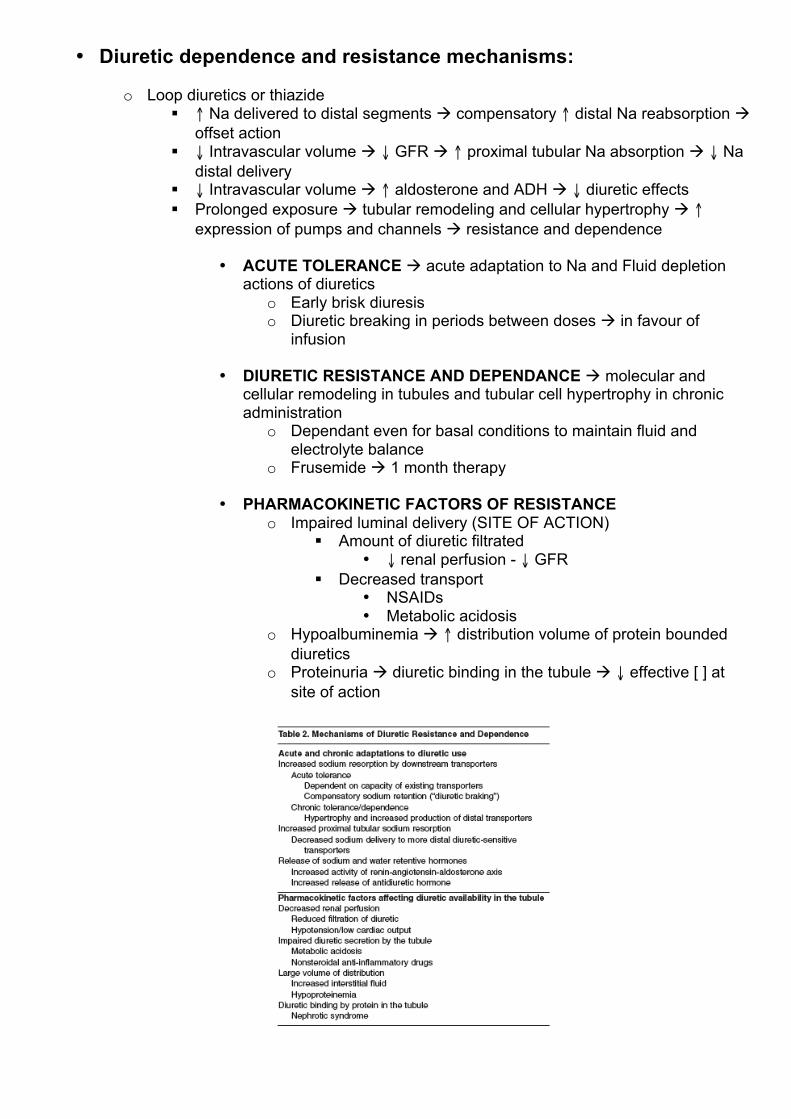
• Diuretic dependence and resistance mechanisms:
o Loop diuretics or thiazide " # Na delivered to distal segments $ compensatory # distal Na reabsorption $
offset action " $ Intravascular volume $ $ GFR $ # proximal tubular Na absorption $ $ Na
distal delivery " $ Intravascular volume $ # aldosterone and ADH $ $ diuretic effects " Prolonged exposure $ tubular remodeling and cellular hypertrophy $ #
expression of pumps and channels $ resistance and dependence
• ACUTE TOLERANCE $ acute adaptation to Na and Fluid depletion actions of diuretics
o Early brisk diuresis o Diuretic breaking in periods between doses $ in favour of
infusion
• DIURETIC RESISTANCE AND DEPENDANCE $ molecular and cellular remodeling in tubules and tubular cell hypertrophy in chronic administration
o Dependant even for basal conditions to maintain fluid and electrolyte balance
o Frusemide $ 1 month therapy
• PHARMACOKINETIC FACTORS OF RESISTANCE o Impaired luminal delivery (SITE OF ACTION)
" Amount of diuretic filtrated • $ renal perfusion - $ GFR
" Decreased transport • NSAIDs • Metabolic acidosis
o Hypoalbuminemia $ # distribution volume of protein bounded diuretics
o Proteinuria $ diuretic binding in the tubule $ $ effective [ ] at site of action
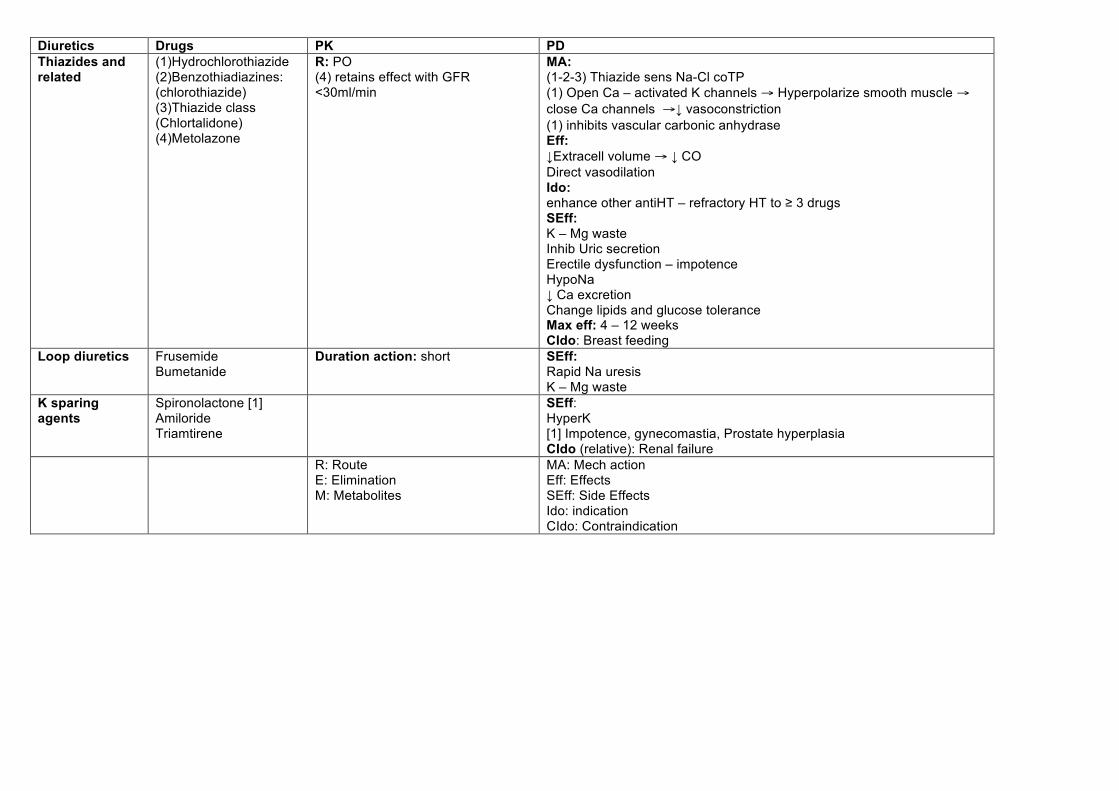
Diuretics Drugs PK PD Thiazides and related
(1)Hydrochlorothiazide (2)Benzothiadiazines: (chlorothiazide) (3)Thiazide class (Chlortalidone) (4)Metolazone
R: PO (4) retains effect with GFR <30ml/min
MA: (1-2-3) Thiazide sens Na-Cl coTP (1) Open Ca – activated K channels ! Hyperpolarize smooth muscle ! close Ca channels !! vasoconstriction (1) inhibits vascular carbonic anhydrase Eff: !Extracell volume ! ! CO Direct vasodilation Ido: enhance other antiHT – refractory HT to " 3 drugs SEff: K – Mg waste Inhib Uric secretion Erectile dysfunction – impotence HypoNa ! Ca excretion Change lipids and glucose tolerance Max eff: 4 – 12 weeks CIdo: Breast feeding
Loop diuretics Frusemide Bumetanide
Duration action: short SEff: Rapid Na uresis K – Mg waste
K sparing agents
Spironolactone [1] Amiloride Triamtirene
SEff: HyperK [1] Impotence, gynecomastia, Prostate hyperplasia CIdo (relative): Renal failure
R: Route E: Elimination M: Metabolites
MA: Mech action Eff: Effects SEff: Side Effects Ido: indication CIdo: Contraindication
PK PD Sympatho
litic Drugs
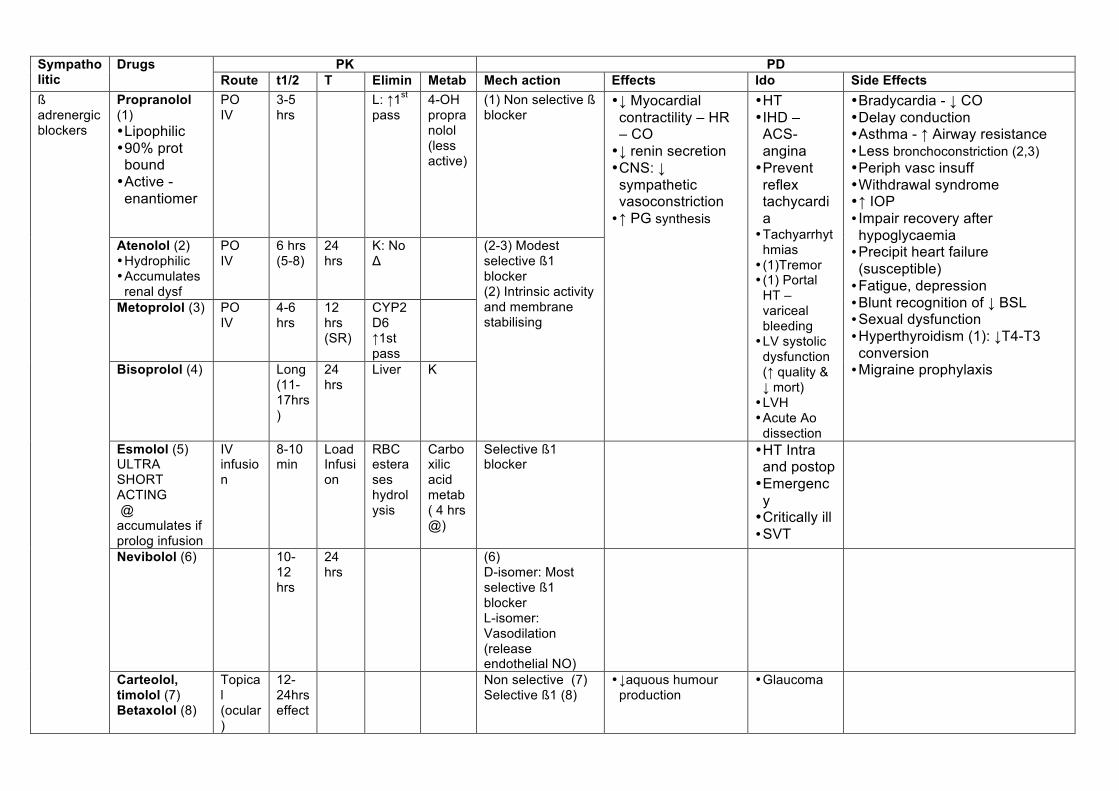
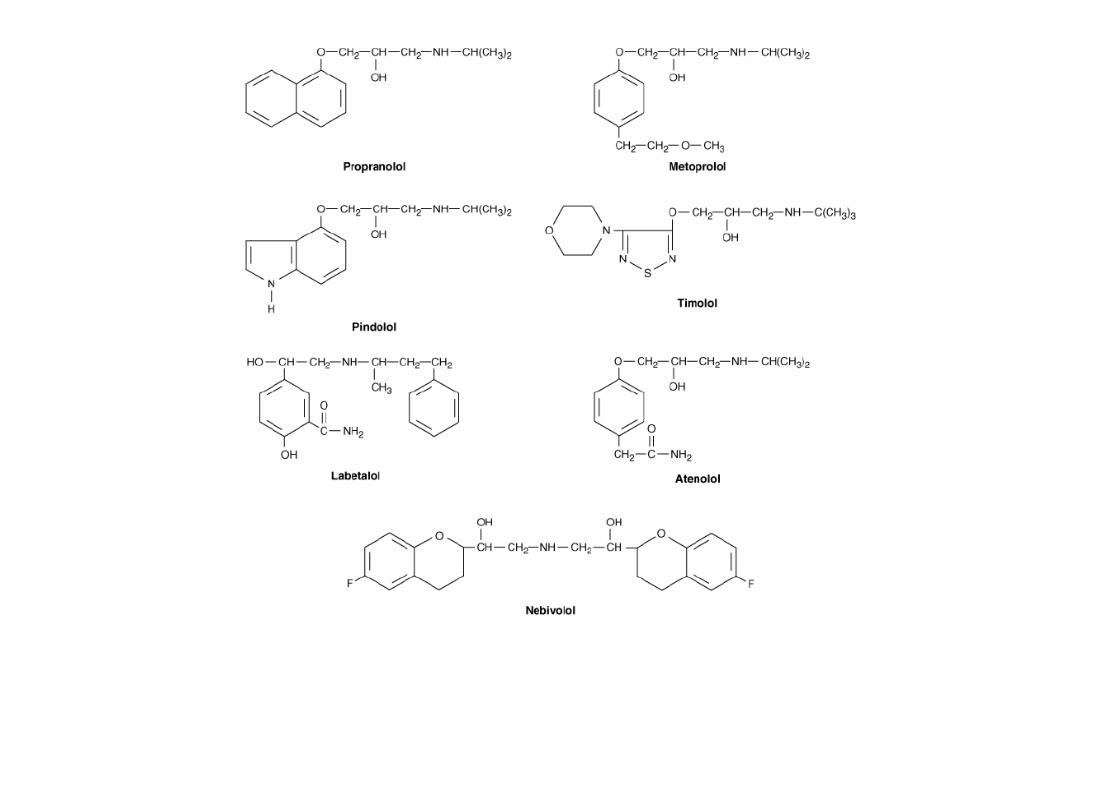
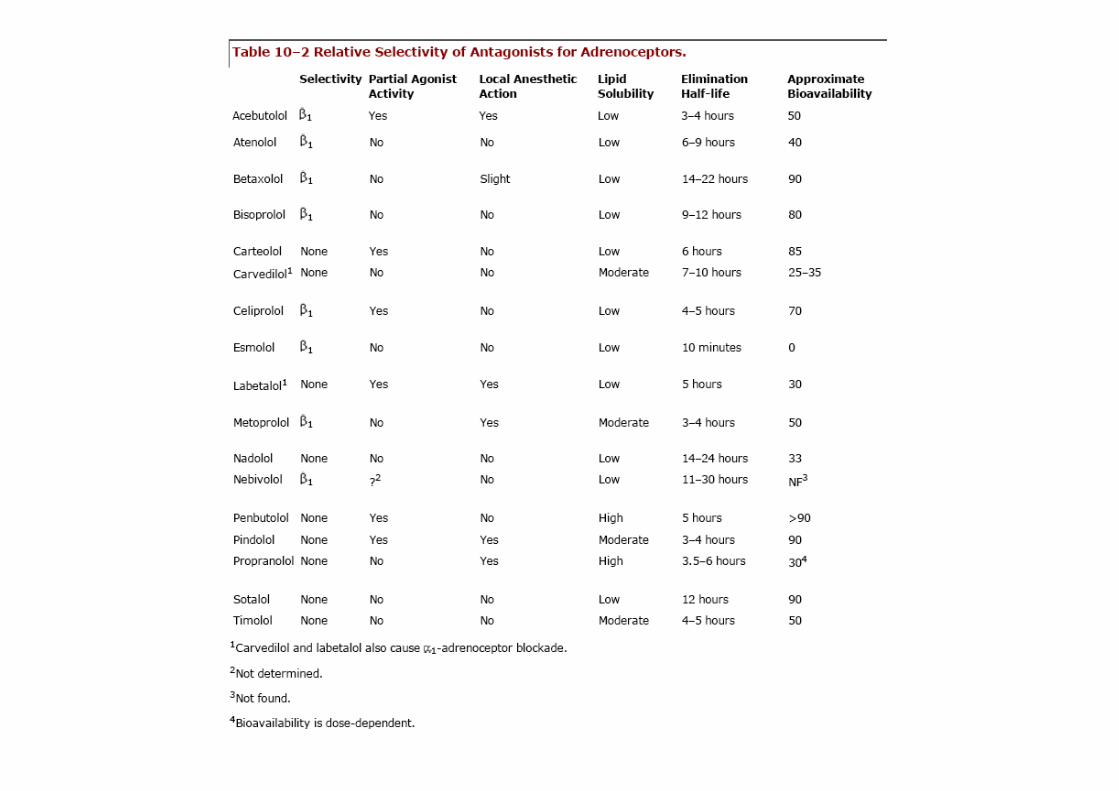
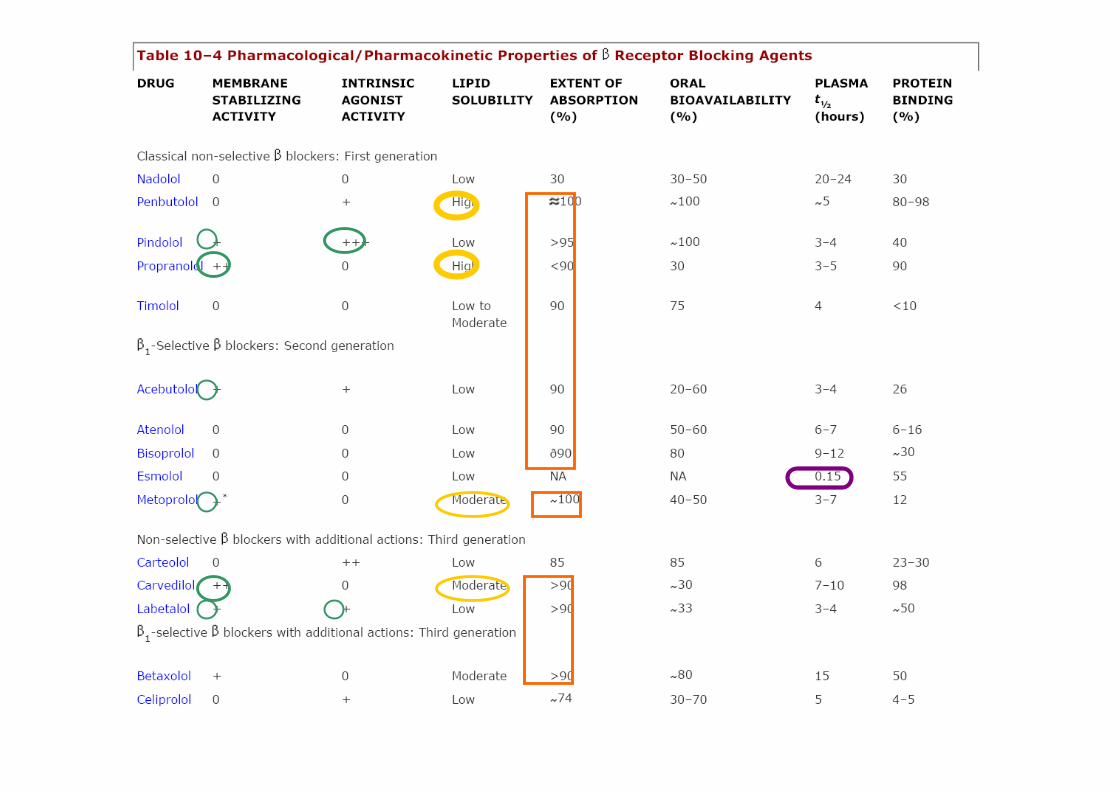
Route t1/2 T Elimin Metab Mech action Effects Ido Side Effects Propranolol (1) • Lipophilic • 90% prot bound • Active - enantiomer
PO IV
3-5 hrs
L: #1st pass
4-OH propranolol (less active)
(1) Non selective ß blocker
Atenolol (2) • Hydrophilic • Accumulates
renal dysf
PO IV
6 hrs (5-8)
24 hrs
K: No $
Metoprolol (3) PO IV
4-6 hrs
12 hrs (SR)
CYP2D6 #1st pass
Bisoprolol (4) Long (11-17hrs)
24 hrs
Liver K
(2-3) Modest selective ß1 blocker (2) Intrinsic activity and membrane stabilising
• ! Myocardial contractility – HR – CO • ! renin secretion • CNS: ! sympathetic vasoconstriction • # PG synthesis
• HT • IHD – ACS- angina • Prevent reflex tachycardia • Tachyarrhyt
hmias • (1)Tremor • (1) Portal
HT – variceal bleeding • LV systolic
dysfunction (# quality & ! mort) • LVH • Acute Ao
dissection
• Bradycardia - ! CO • Delay conduction • Asthma - # Airway resistance • Less bronchoconstriction (2,3) • Periph vasc insuff • Withdrawal syndrome • # IOP • Impair recovery after hypoglycaemia • Precipit heart failure (susceptible) • Fatigue, depression • Blunt recognition of ! BSL • Sexual dysfunction • Hyperthyroidism (1): !T4-T3 conversion • Migraine prophylaxis
Esmolol (5) ULTRA SHORT ACTING @ accumulates if prolog infusion
IV infusion
8-10 min
Load Infusion
RBC esterases hydrolysis
Carboxilic acid metab ( 4 hrs @)
Selective ß1 blocker
• HT Intra and postop • Emergency • Critically ill • SVT
Nevibolol (6) 10-12 hrs
24 hrs
(6) D-isomer: Most selective ß1 blocker L-isomer: Vasodilation (release endothelial NO)
ß adrenergic blockers
Carteolol, timolol (7) Betaxolol (8)
Topical (ocular)
12-24hrs effect
Non selective (7) Selective ß1 (8)
• !aquous humour production
• Glaucoma
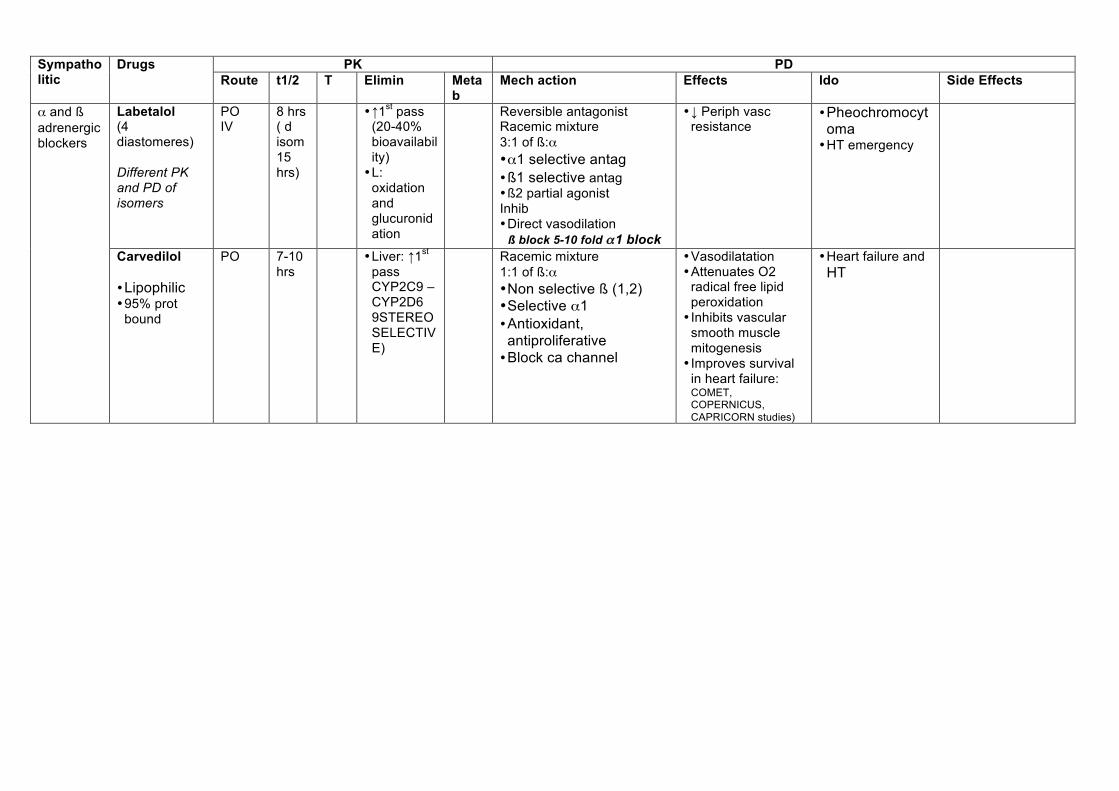
PK PD Sympatho
litic Drugs
Route t1/2 T Elimin Metab
Mech action Effects Ido Side Effects
Labetalol (4 diastomeres) Different PK and PD of isomers
PO IV
8 hrs ( d isom 15 hrs)
• #1st pass (20-40% bioavailability) • L:
oxidation and glucuronidation
Reversible antagonist Racemic mixture 3:1 of ß:" • "1 selective antag • ß1 selective antag • ß2 partial agonist Inhib • Direct vasodilation
ß block 5-10 fold !!1 block
• ! Periph vasc resistance
• Pheochromocytoma • HT emergency
" and ß adrenergic blockers
Carvedilol • Lipophilic • 95% prot
bound
PO 7-10 hrs
• Liver: #1st pass CYP2C9 – CYP2D6 9STEREOSELECTIVE)
Racemic mixture 1:1 of ß:" • Non selective ß (1,2) • Selective "1 • Antioxidant, antiproliferative • Block ca channel
• Vasodilatation • Attenuates O2
radical free lipid peroxidation • Inhibits vascular
smooth muscle mitogenesis • Improves survival
in heart failure: COMET, COPERNICUS, CAPRICORN studies)
• Heart failure and HT
PK PD Sympatho
litic Drugs
Route t1/2 T Elimin
Metab
Mech action Effects Ido Side Effects
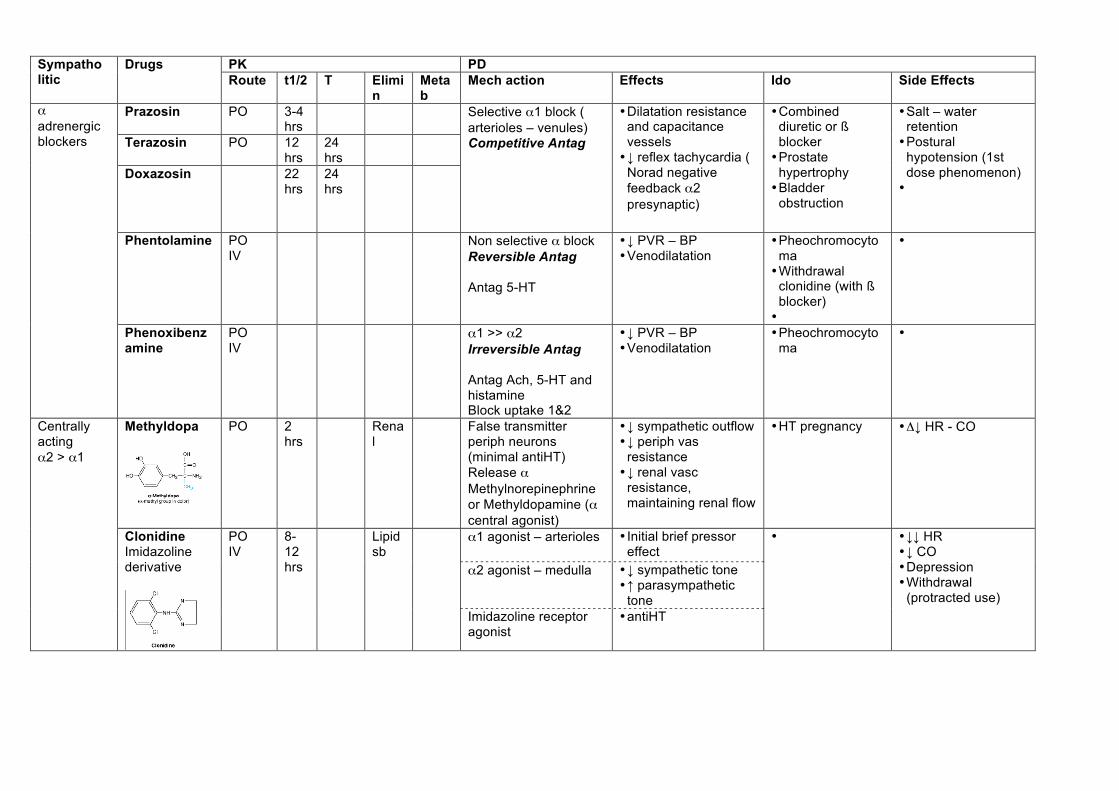
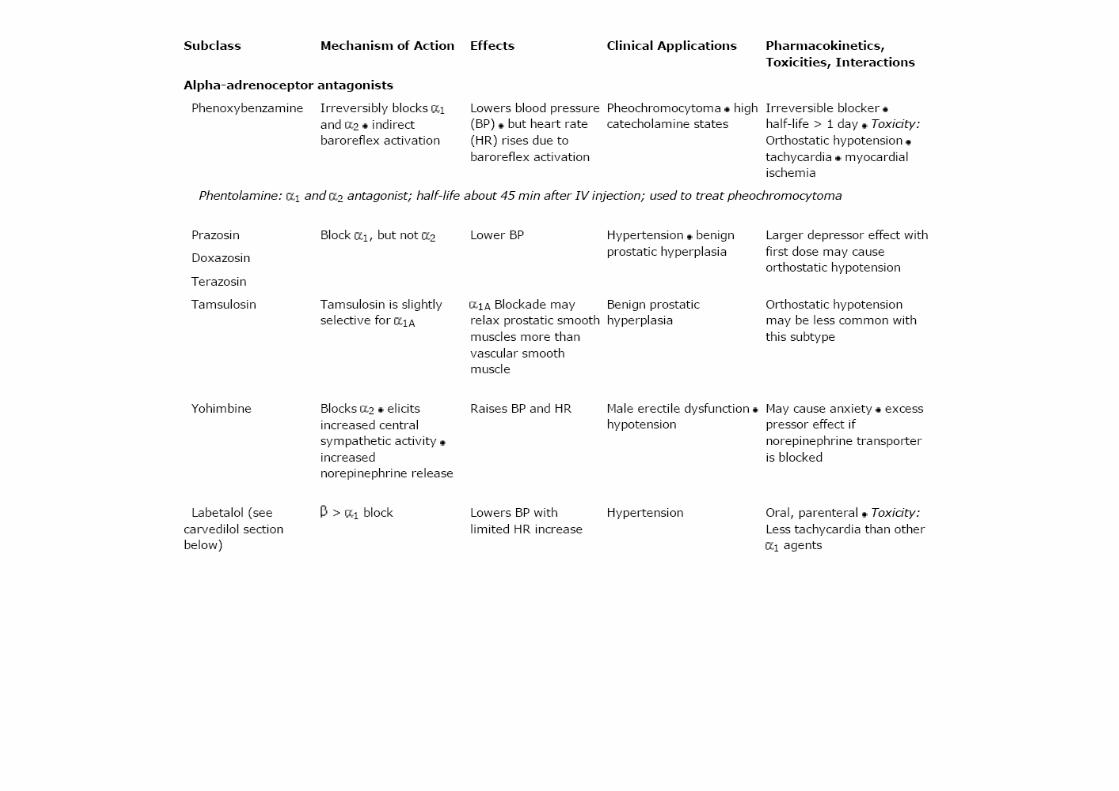
Prazosin PO 3-4 hrs
Terazosin
PO 12 hrs
24 hrs
Doxazosin 22 hrs
24 hrs
Selective "1 block ( arterioles – venules) Competitive Antag
• Dilatation resistance and capacitance vessels • ! reflex tachycardia (
Norad negative feedback "2 presynaptic)
• Combined diuretic or ß blocker • Prostate
hypertrophy • Bladder
obstruction
• Salt – water retention • Postural
hypotension (1st dose phenomenon) •
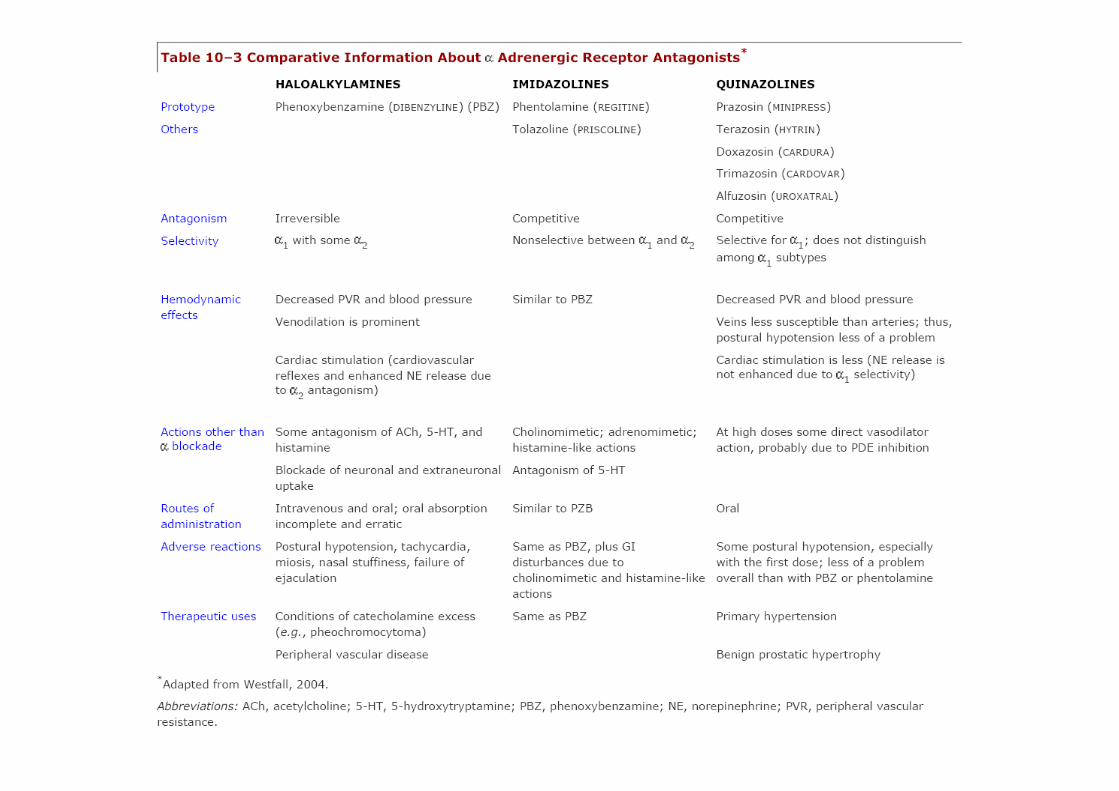
Phentolamine PO IV
Non selective " block Reversible Antag Antag 5-HT
• ! PVR – BP • Venodilatation
• Pheochromocytoma • Withdrawal
clonidine (with ß blocker) •
•
" adrenergic blockers
Phenoxibenzamine
PO IV
"1 >> "2 Irreversible Antag Antag Ach, 5-HT and histamine Block uptake 1&2
• ! PVR – BP • Venodilatation
• Pheochromocytoma
•
Methyldopa
PO 2 hrs
Renal
False transmitter periph neurons (minimal antiHT) Release " Methylnorepinephrine or Methyldopamine (" central agonist)
• ! sympathetic outflow • ! periph vas
resistance • ! renal vasc
resistance, maintaining renal flow
• HT pregnancy • #! HR - CO
"1 agonist – arterioles • Initial brief pressor effect
"2 agonist – medulla • ! sympathetic tone • # parasympathetic
tone
Centrally acting "2 > "1
Clonidine Imidazoline derivative
PO IV
8-12 hrs
Lipid sb
Imidazoline receptor agonist
• antiHT
• • !! HR • ! CO • Depression • Withdrawal
(protracted use)
PK PD Sympatholitic Drugs Route t1/2 T Elimi
n Metab
Mech action Effects Ido CIdo Side Effects
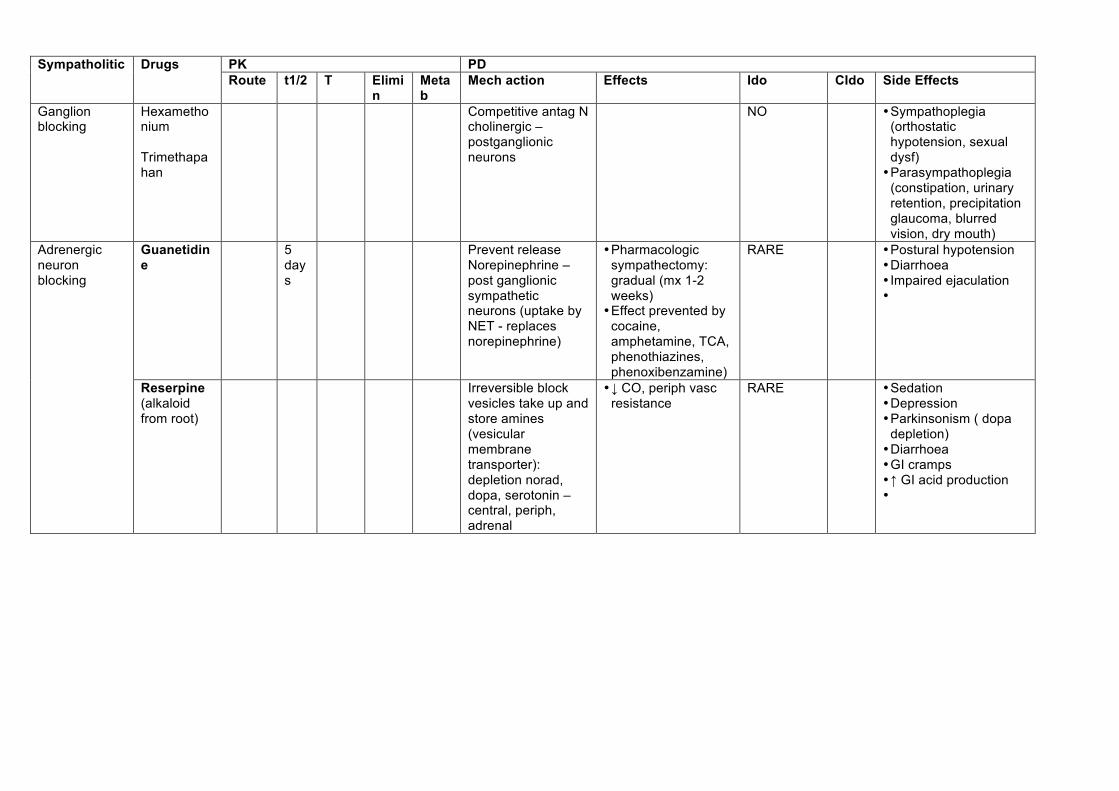
Ganglion blocking
Hexamethonium Trimethapahan
Competitive antag N cholinergic – postganglionic neurons
NO • Sympathoplegia (orthostatic hypotension, sexual dysf) • Parasympathoplegia
(constipation, urinary retention, precipitation glaucoma, blurred vision, dry mouth)
Guanetidine
5 days
Prevent release Norepinephrine – post ganglionic sympathetic neurons (uptake by NET - replaces norepinephrine)
• Pharmacologic sympathectomy: gradual (mx 1-2 weeks) • Effect prevented by
cocaine, amphetamine, TCA, phenothiazines, phenoxibenzamine)
RARE • Postural hypotension • Diarrhoea • Impaired ejaculation •
Adrenergic neuron blocking
Reserpine (alkaloid from root)
Irreversible block vesicles take up and store amines (vesicular membrane transporter): depletion norad, dopa, serotonin – central, periph, adrenal
• ! CO, periph vasc resistance
RARE • Sedation • Depression • Parkinsonism ( dopa
depletion) • Diarrhoea • GI cramps • # GI acid production •
PK PD Vasodilators Drugs Route t1/2 T Elimi
n Metab
Mech action Effects Ido CIdo Side Effects
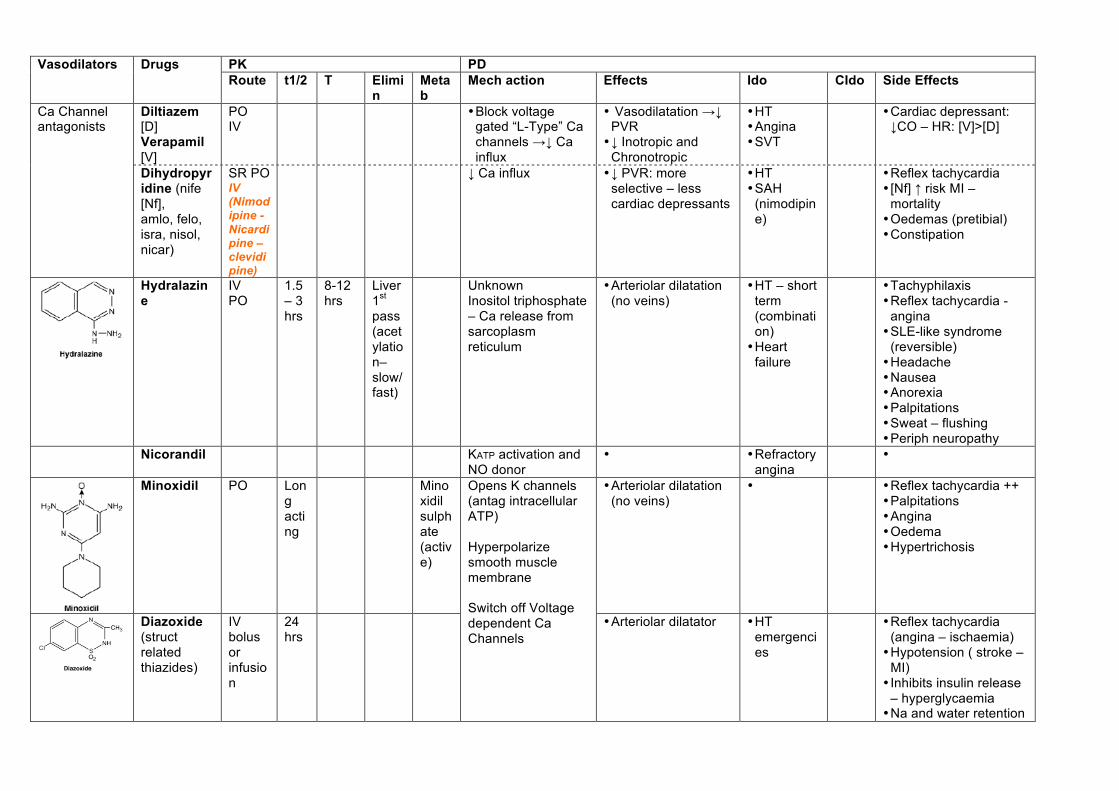
Diltiazem [D] Verapamil [V]
PO IV
• Block voltage gated “L-Type” Ca channels %! Ca influx
• Vasodilatation %! PVR • ! Inotropic and
Chronotropic
• HT • Angina • SVT
• Cardiac depressant: !CO – HR: [V]>[D]
Ca Channel antagonists
Dihydropyridine (nife [Nf], amlo, felo, isra, nisol, nicar)
SR PO IV (Nimodipine - Nicardipine – clevidipine)
! Ca influx • ! PVR: more selective – less cardiac depressants
• HT • SAH
(nimodipine)
• Reflex tachycardia • [Nf] # risk MI –
mortality • Oedemas (pretibial) • Constipation
Hydralazine
IV PO
1.5 – 3 hrs
8-12 hrs
Liver 1st pass (acetylation–slow/fast)
Unknown Inositol triphosphate – Ca release from sarcoplasm reticulum
• Arteriolar dilatation (no veins)
• HT – short term (combination) • Heart
failure
• Tachyphilaxis • Reflex tachycardia -
angina • SLE-like syndrome
(reversible) • Headache • Nausea • Anorexia • Palpitations • Sweat – flushing • Periph neuropathy
Nicorandil KATP activation and NO donor
• • Refractory angina
•
Minoxidil PO Long acting
Minoxidil sulphate (active)
• Arteriolar dilatation (no veins)
• • Reflex tachycardia ++ • Palpitations • Angina • Oedema • Hypertrichosis
Diazoxide (struct related thiazides)
IV bolus or infusion
24 hrs
Opens K channels (antag intracellular ATP) Hyperpolarize smooth muscle membrane Switch off Voltage dependent Ca Channels
• Arteriolar dilatator • HT emergencies
• Reflex tachycardia (angina – ischaemia) • Hypotension ( stroke –
MI) • Inhibits insulin release
– hyperglycaemia • Na and water retention
PK PD Vasodilators Drugs Route
t1/2 T Elimin Metab Mech action Effects Ido CIdo Side Effects
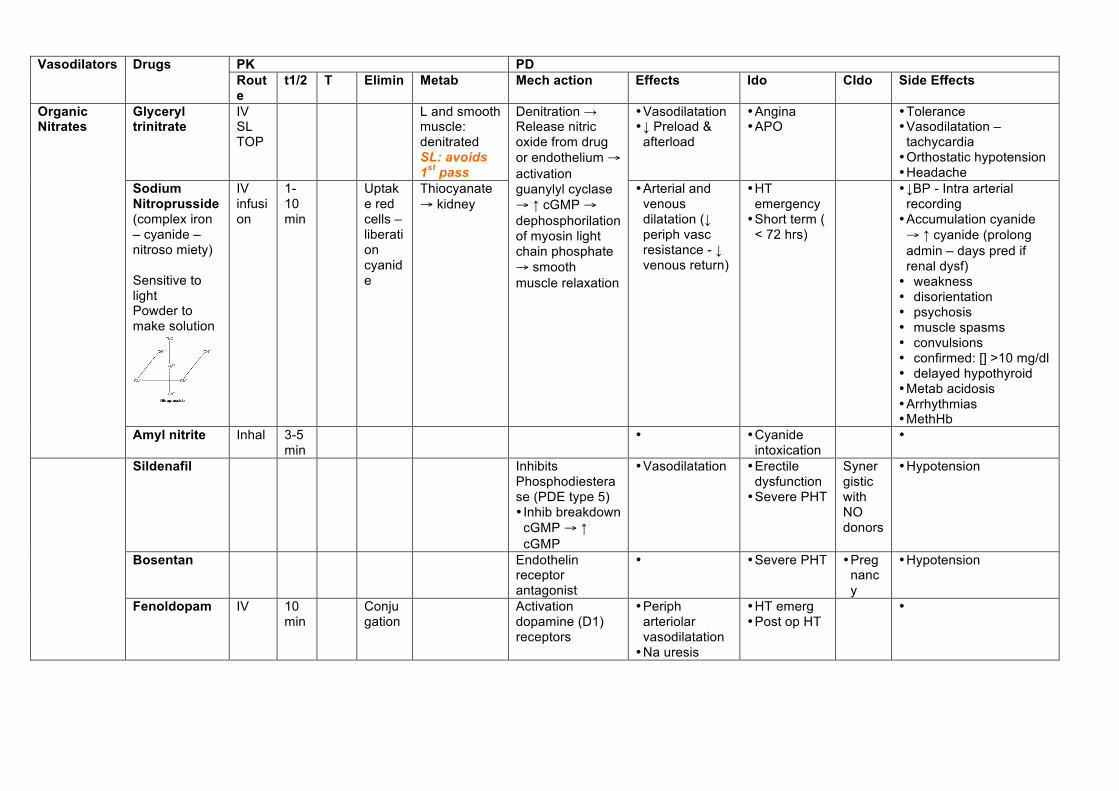
Glyceryl trinitrate
IV SL TOP
L and smooth muscle: denitrated SL: avoids 1st pass
• Vasodilatation • ! Preload &
afterload
• Angina • APO
• Tolerance • Vasodilatation –
tachycardia • Orthostatic hypotension • Headache
Sodium Nitroprusside (complex iron – cyanide – nitroso miety) Sensitive to light Powder to make solution
IV infusion
1-10 min
Uptake red cells – liberation cyanide
Thiocyanate ! kidney
Denitration % Release nitric oxide from drug or endothelium ! activation guanylyl cyclase ! # cGMP ! dephosphorilation of myosin light chain phosphate ! smooth muscle relaxation
• Arterial and venous dilatation (! periph vasc resistance - ! venous return)
• HT emergency • Short term (
< 72 hrs)
• !BP - Intra arterial recording • Accumulation cyanide ! # cyanide (prolong admin – days pred if renal dysf) • weakness • disorientation • psychosis • muscle spasms • convulsions • confirmed: [] >10 mg/dl • delayed hypothyroid • Metab acidosis • Arrhythmias • MethHb
Organic Nitrates
Amyl nitrite Inhal 3-5 min
• • Cyanide intoxication
•
Sildenafil Inhibits Phosphodiesterase (PDE type 5) • Inhib breakdown
cGMP ! # cGMP
• Vasodilatation • Erectile dysfunction • Severe PHT
Synergistic with NO donors
• Hypotension
Bosentan Endothelin receptor antagonist
• • Severe PHT • Pregnancy
• Hypotension
Fenoldopam IV 10 min
Conjugation
Activation dopamine (D1) receptors
• Periph arteriolar vasodilatation • Na uresis
• HT emerg • Post op HT
•
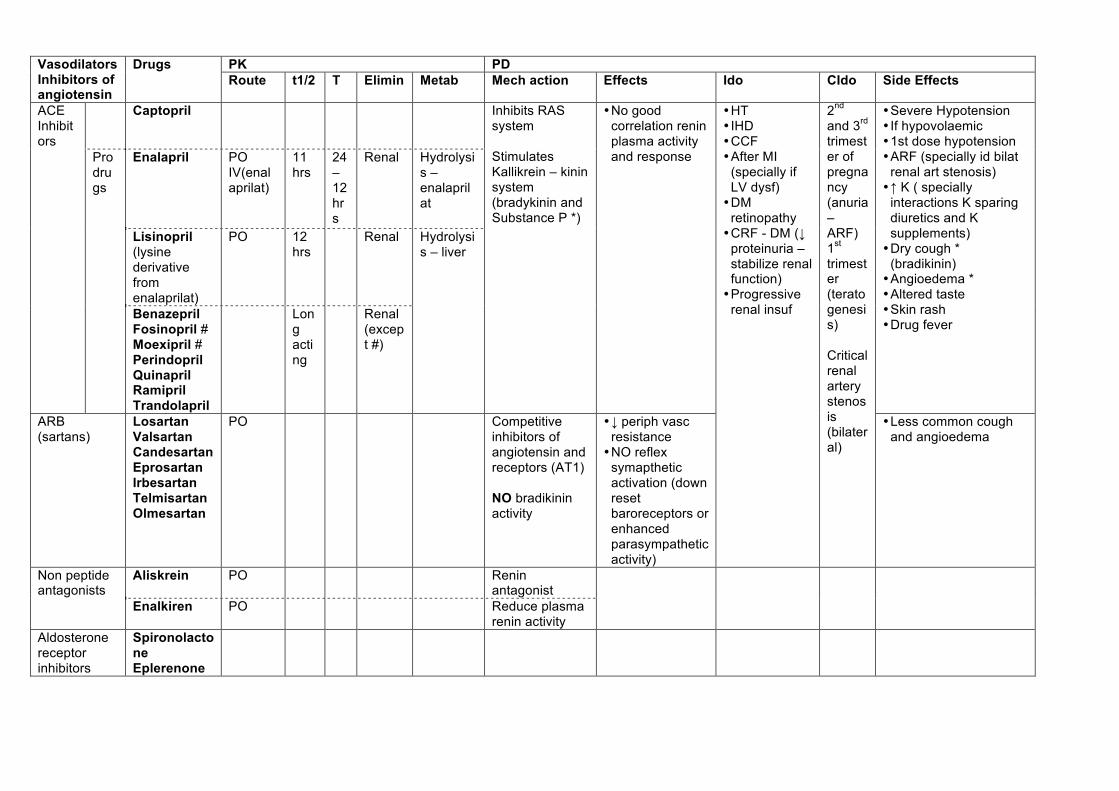
PK PD Vasodilators
Inhibitors of angiotensin
Drugs Route t1/2 T Elimin Metab Mech action Effects Ido CIdo Side Effects
Captopril
Enalapril PO IV(enalaprilat)
11 hrs
24 – 12 hrs
Renal Hydrolysis –enalaprilat
Lisinopril (lysine derivative from enalaprilat)
PO 12 hrs
Renal
ACE Inhibitors
Prodrugs
Benazepril Fosinopril # Moexipril # Perindopril Quinapril Ramipril Trandolapril
Long acting
Renal (except #)
Hydrolysis – liver
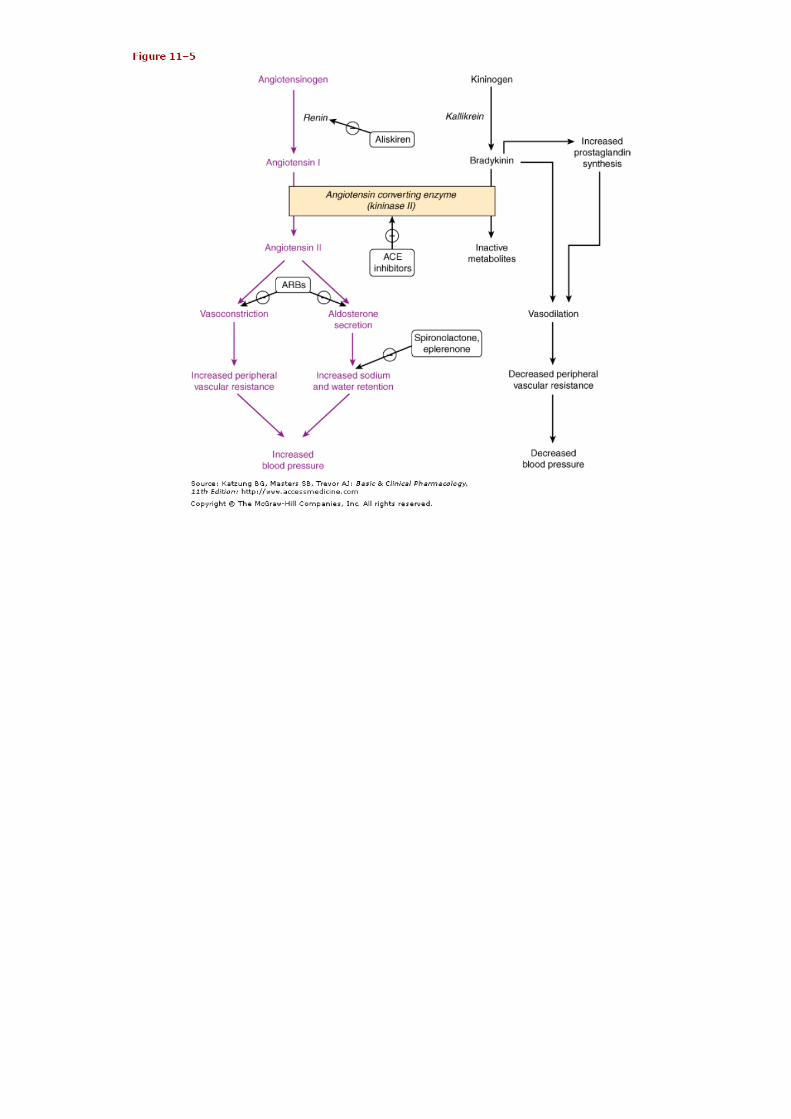
Inhibits RAS system Stimulates Kallikrein – kinin system (bradykinin and Substance P *)
• No good correlation renin plasma activity and response
• Severe Hypotension • If hypovolaemic • 1st dose hypotension • ARF (specially id bilat
renal art stenosis) • # K ( specially
interactions K sparing diuretics and K supplements) • Dry cough *
(bradikinin) • Angioedema * • Altered taste • Skin rash • Drug fever
ARB (sartans)
Losartan Valsartan Candesartan Eprosartan Irbesartan Telmisartan Olmesartan
PO Competitive inhibitors of angiotensin and receptors (AT1) NO bradikinin activity
• ! periph vasc resistance • NO reflex
symapthetic activation (down reset baroreceptors or enhanced parasympathetic activity)
• HT • IHD • CCF • After MI
(specially if LV dysf) • DM
retinopathy • CRF - DM (!
proteinuria – stabilize renal function) • Progressive
renal insuf
2nd and 3rd trimester of pregnancy (anuria – ARF) 1st trimester (teratogenesis) Critical renal artery stenosis (bilateral)
• Less common cough and angioedema
Aliskrein PO Renin antagonist
Non peptide antagonists
Enalkiren PO Reduce plasma renin activity
Aldosterone receptor inhibitors
Spironolactone Eplerenone
! Renal cortex stimulation " Positive feedback:
• ! Renal art perfusion pressure • Sympathetic neural stimulation: ß agonist • PGI2 • ! [Na] distal renal tubule (macula densa)
" Negative feedback: • Angiotensin II
! Renin " Produced by yuxtaglomerular apparatus " Short t1/2 " Proteolysis angiotensinogen (inactive plasma globulin produced by liver) into
angiotensin I (inactive decapeptide – N terminal) " Antagonist: Enalkiren
! ACE " Endothelial ! membrane bound (predominantly rich vascular beds)
• " [ ]lung > heart, brain, striated muscle, kidney " Hydrolysis angiotensin I into angiotensin II (active octapeptide )
• Other enzyme forming angiot II: chymase ( not inhibited by ACEI) " AT 1 Receptors! G protein coupled receptor
# Vasoconstriction ( mostly efferent kidney arterioles) " 40 times more potent than noradrenaline
# " release Norad – sympathetic terminals # Stimulates Na reabsorption ( prox tubule) # Secretion aldosterone ( adrenal cortex) # Cell growth ( heart – arteries)
" AT 2 # Fetal expression # Brain adults # Inhib cardiovasc cell growth
" Inactivates bradykinin (vasodilatator: releases NO and prostacyclin) ! Adrenal gland
" Aminopeptidase A & N " Converts angiotensin II into III and IV
! Angiotensin " II and III ! Stimulate aldosterone release " III ! thirst " IV ! endothelium: release plasminogen activator inhibitor 1
! Parallel systems for angiotensin generation " Heart ! trophic changes – LVH