Embed Size (px)
Citation preview
Journal of Affective Disorders 136 (2012) e69–e75
Contents lists available at SciVerse ScienceDirect
Journal of Affective Disorders
j ourna l homepage: www.e lsev ie r.com/ locate / j ad
Research report
Principal domains of quantitative anxiety trait in subjects with lifetimehistory of mania
Javier Contreras a,b,⁎, Elizabeth Hare a, Michael Escamilla a, Henriette Raventos b
a South Texas Psychiatric Genetics Research Center, Texas Tech University Health Science Center, El Paso, TX, USAb Centro de Investigación en Biologia Celular y Molecular, University of Costa Rica, San Jose, Costa Rica
a r t i c l e i n f o
⁎ Corresponding author at: Centro de InvestigaciónMolecular, University of Costa Rica, San Jose, Costa R3187; fax: +506 2511 3190.
E-mail address: [email protected] (J. C
0165-0327/$ – see front matter. Published by Elseviedoi:10.1016/j.jad.2011.06.036
a b s t r a c t
Article history:Received 21 November 2010Received in revised form 31 May 2011Accepted 23 June 2011Available online 19 July 2011
Background: High comorbidity rates for anxiety have been documented in subjects withhistory of mania or hypomania. We explored the presence of latent constructs of quantitativeanxiety in subjects who have a history of mania or hypomania.Methods: We conducted an exploratory factor analysis of anxiety trait in 212 subjects who havea lifetime history of at least one manic/hypomanic syndrome. Participants were originallyrecruited for a Costa Rican sibling pair genetic study of Bipolar Disorder. We used principalfactors extraction method with squared multiple correlations (SAS/SAT Professional software)of the STAI (trait subscale).Results: A three-factor solution with a good simple structure and statistical adequacy wasobtained with a KMO of 0.84 (N0.6) and Bartlett's Test of Sphericity of 2.4668E-162 (pb0.05).Items were grouped into anxiety-absent factor and the anxiety-present symptoms in twoadditional factors based on the nature of the symptoms, worry and rumination.Limitations: Comorbid disorders could affect the interaction of anxiety score with manic/hy-pomanic symptoms. Some statistical parameters (mood status independence, score distribu-tion and correlation between trait score and quantitative mania/hypomania) were not takeninto consideration to extract the factors. Because anxiety dimensions were explored onindividuals with history of mania or hypomania and not in healthy subjects, comparison of ourresults with other studies can draw confusing conclusions.Conclusions: Two underlying constructs, worry and rumination may explain anxiety sub-syndromic symptoms in Costa Rican patients with history of mania or hypomania.
Published by Elsevier B.V.
Keywords:ManiaHypomaniaExploratory factor analysisFamily studiesSub-syndromic anxiety
1. Introduction
Current diagnostic systems do not adequately reflect thecomplexity of bipolar disorder (BD) (Akiskal et al., 2000;Akiskal and Pinto, 1999). Categorical diagnosis and globalseverity assessments provide suboptimal information toimprove our knowledge on pathophysiology, diagnostic as-sessment, prognosis, and novel therapies. Insights into BPgenetics, illness course and pharmacological studies increas-
en Biologia Celular yica. Tel.: +506 2511
ontreras).
r B.V.
ingly reinforce this conclusion. Syndromal diagnostic criteriacould also be aided by the reliable convergence of severaldimensional variables, including behavioral domains, illnesscourse and family history (Contreras et al., 2010; Goodwin andJamison, 2007; Vieta and Phillips, 2007).
High comorbidity rates for anxiety have been documentedin bipolar I disorder (MacKinnon et al., 2002; McElroy et al.,2001). However, sub-syndromal levels of anxiety have alsobeen associated with bipolar I patients who did not meetcriteria for a categorical Diagnostic and Statistical Manual ofMental Disorders (DSM-IV) anxiety disorder (Mantere et al.,2008). Research on the underlying variables and factors islimited to individual categorical clinical states (Sato et al.,2002). The above limitations have made it difficult to

e70 J. Contreras et al. / Journal of Affective Disorders 136 (2012) e69–e75
extrapolate results to current clinical practices and to replicatefindings.
Clinical and epidemiologic evidence suggests that majormood disorders form a spectrum from major depressivedisorder to pure mania (Angst et al., 2010). More specifically,transient manic symptoms in children were probed to be arisk factor for eventual conversion to the bipolar spectrumdisorder (Nadkarni and Fristad, 2010). Family studies havealso supported the concept of a spectrum of subthresholdaffective traits or temperaments (e.g. cyclothymia andanxiety) in bipolar pedigrees (Vázquez et al., 2008). Sincethe concept of bipolar spectrum denotes overlapping clinicalexpressions, without necessarily implying underlying genetichomogeneity; we arbitrarily defined bipolar spectrum disor-der as lifetime history of any manic syndrome/episode. Thus,we analyzed subjects who have a history of mania orhypomania (bipolar disorder type I, bipolar disorder type II,bipolar disorder not otherwise specified, schizoaffectivebipolar disorder, schizophrenia with manic syndrome andsubstance related manic syndrome). One of the reasons forusing any manic or hypomanic syndrome as inclusion criteriais the fact that in our previous published work the trait scorewas correlated with lifetime mania (LDPS M-1 duration×se-verity) (pb .0001) after controlling for age and gender. In thatstudy we did not find significant correlation between anxietytrait and depression (Contreras et al., 2010).
The goal of this study was to explore the presence of latentconstructs which contribute to the STAI score in subjects whohave a history ofmania.Weused the anxiety trait (trait subscaleof the STAI) that showed normal distribution in healthysubjects, significant heritability and genetic correlation andindependence to mood clinical state in our multiplex bipolar Ifamilies (Contreras et al., 2010). Also, research has shown thatstate–trait dimensions (from studying the two subscalestogether) may be multidimensional themselves (Virella et al.,1994). The advantage of knowing if there are factors is to betterunderstand the biologic components which make up theglobal STAI score in this group of patients. If this anxiety traitrepresents a biologicalmarker for bipolar I disorder in this CostaRican sample, exploration of its underlying constructs mightprovide a high face and construct validity with respect tomania/hypomania in this Costa Rican sample.
We reasoned that the combination of quantitative anxietytrait and best estimation diagnostic process based on DSM-IVdiagnostic criteria would serve to yield reliable and informa-tive scores on fundamental affect components of subjectswith history of mania/hypomania.
2. Methods
2.1. Participants
Subjects were originally recruited for a multi-site bipolarsibling pair study (Genetics of Bipolar disorder in LatinoPopulations NIMH 1 R01 MH069856-01A2). The study wasexplained to each subject and written informed consent wasobtained. This study was reviewed and approved by theInstitutional Review Boards of the University of Costa Ricaand the University of Texas (UTHSCSA). The sample wascomposed of 212 subjects. Each individual had lifetime historyof at least one manic/hypomanic syndrome.
2.2. Diagnostic assessment
The subjects were diagnosed based on the diagnosticcriteria of DSM-IV through a best estimation process utilizingclinical information obtained from the Diagnostic Interview forGenetic Studies (Nurnberger et al., 1994), a Family Interview forGenetic Studies (Maxwell, 1992) and psychiatric records. Finaldiagnoses were determined through a consensus processwhere two independent psychiatrists reviewed all availableinformation and arrived at independent diagnoses.
2.3. Anxiety assessment
Sub-syndromal anxiety was assessed by means of the STAIto measure anxiety scores in each individual. The STAI is a self-rated instrument that contains two 20-item scales (4 responsechoices per item, higher scores indicate higher anxiety)(Spielberger et al., 1983). One scale measures state anxiety(i.e. the extent to which respondents experience anxietysymptoms at the time ofmeasurement) (Vigneau and Cormier,2008). The second scale measures trait anxiety (i.e. the extentto which respondents generally experience anxiety symp-toms). This instrument has been validated in Spanish (Rodrigoand Lusiardo, 1988).
2.4. Exploratory factor analysis
Exploratory factor analysis was performed using theprincipal factors extraction method with squared multiplecorrelations (SMC) of each variable with all the other variablesfor the prior communality estimates. This is the simplest andcomputationally most efficient method of common factoranalysis. Although maximum likelihood (ML) factor analysishas desirable asymptotic properties and allows to testhypotheses about the number of common factors, it generatesbetter estimates in samples larger than thenumber of subject ofthe current study (Joreskog, 1977).
To determine whether the common factor model isappropriate, we calculated the Kaiser's measure of samplingadequacy (KMO). This measure varies between 0 and 1; avalue greater than 0.6 was considered the minimum acceptedvalue (Kaiser, 1974). Bartlett's Test of Sphericity tests thenull hypothesis: that the correlation matrix is an identitymatrix (matrix in which all of the diagonal elements are 1 andall of diagonal elements are 0). By using the test, the nullhypothesis would be rejected.
Partial correlation (controlling all other variables) wasexplored to evaluate whether the data was appropriate forthe factor model. It is presumed that partial correlation willbe small compared to the original correlations. SMC replacesthe diagonal of the original observed correlation matrix bythese square multiple correlations.
During the extraction, the values indicate the proportionof each variable's variance that can be explained by theretained factors. Variables with high values are well repre-sented in the common factor space, while variables with lowvalues are not well represented. Because the square multiplecorrelations are usually less than one, the resulting correla-tion matrix for factoring is called the reduced correlationmatrix. The Regression Method was used to produce thecoefficients for each item in order to generate the estimated

e71J. Contreras et al. / Journal of Affective Disorders 136 (2012) e69–e75
factor scores for each observation (SAS/SAT Professionalsoftware, SAS Institute, Inc., Cary, NC). The initial eigenvaluesare the variances of the factors. The first factor accounts forthe most variance (and hence have the highest eigenvalue),and the next factor will account for as much of the left overvariance as it can. Thus, each successive factor will account forless and less variance. The percentage of variance contains thepercent of total variance accounted for by each factor (itscumulative contains the cumulative percentage of varianceaccounted for by the current and all preceding factors). Todetermine the optimal number of factors to be extracted, theprotocol required each factor to have at least four items withrotated factor loading scores greater than 0.30. This cut-offscore was chosen because it does not eliminate potentiallysignificant factors and it conforms to traditional exploratoryfactor analysis methodology (Floyd andWidaman, 1995). Thescree plot produces a plot of the eigenvalues that is helpful indeciding how many factors to use (Fabrigar et al., 1999).
The Extraction Sums of Squared Loadings correspond tothe number of factors retained. The rotation sums of squaredloadings represent the distribution of the variance after thevarimax rotation. Varimax rotationmaximizes the variance ofeach of the factors, so the total amount of variance accountedfor is redistributed over the three extracted factors (Kaiser,1960). Rotation of factor pattern is to apply a nonsingularlinear transformation to the unrotated factor pattern matrix.An optimal transformation is usually defined as a minimumor maximum point of a simplicity function. Different rotationmethods are based on different simplicity functionsemployed. Since orthogonal rotation of the extracted factorloadings was conducted we were not able to explore whetherthe obtained factors were correlated.
3. Results
3.1. Sample characteristics
Out of the 212 subjects, 164 (77%) had bipolar disordertype I, 8 (4%) bipolar disorder type II, 18 (8%) bipolar disordernot otherwise specified, 13 (6%) schizoaffective disorderbipolar type, 2 (1%) schizophrenia with manic syndrome, 7(4%) substance induced mood disorder with manic symp-toms. One-hundred and fifteen subjects (54%) were femalesand the average age of the whole sample was 45.3(SD=12.2). The sample of this analysis was composed of68 families (average number of individuals per family 3members, range: 1–9).
3.2. Factor structure
To assess if the common factor model was appropriate forour sample, the correlation matrix of the STAI trait subscale(20 items) was computed. Inspection of the correlationmatrix showed that the correlations were substantial,indicating the presence of a substantial general factor. KMOof 0.845275243 (N0.6) and Bartlett's Test of Sphericity of2.4668E-162 (pb0.05) showed adequacy of data for factoranalysis. Since the aim of this work was exploratory factoranalysis in pedigrees with one or more affected members,factor scores were not computed which are necessary for
heritability estimates as an index of familiarity within thissample.
After computing the prior communality estimates (pro-portion of variance of each of the 20 items shared by allremaining items)we found that item 11 (I am inclined to takethings hard) has the prior communality estimate of 0.26,which means that only 26% of the variance of the item 11 isshared by all other items, indicating that this item issomehow a different construct than the other items. A similarsituation is shownwith item 14 (I try to avoid facing a crisis ordifficulty). Since more common communalities in socialsciences are low to moderate (0.40–0.70) (Velicer and Fava,1998), items with communalities less than 0.40 were notincluded in the current analysis.
As shown in Table 2, the sum of all prior communalityestimates, 9.96 (the estimate of the common variance amongall items) constitutes about 50% of the total variance presentamong all 20 items, current estimate of the common variancewas slightly larger (10.20). According to the proportioncriterion (N0.30) and the scree plot (not shown) three factorscan be retained. For the scree plot, a point below whichfactors explain relatively little variance and above which theyexplain substantially more is shown as an “elbow”. Cattell'sguidelines (Cattell, 1966) call for retaining factors above theelbow and rejecting those below it.
We analyzed the item loading table after rotation to selectthe “cleanest” factor structure: item loadings above 0.30, noitems cross loadings, and no factor with fewer than threeitems.
The off-diagonal elements of the residual correlationmatrix (table not shown) are close to 0.01, indicating thatthe correlations among the 20 items can be accuratelyreproduced from the retained factors. The root mean squaredoff-diagonal residual is 0.03. The inspection of the partialcorrelation matrix yields similar results: the correlationsamong the 20 items after the retained factors are accountedfor are all close to zero. The root mean squared partialcorrelation is 0.06, indicating that four latent factors canaccurately account for the observed correlations among the20 items.
Based on the obtained factor pattern all variables exceptitems 11 and 14 had high loadings on one factor and becameeasier to interpret after rotation. As seen in Table 1, 16 itemshad factor loadings ranging from 0.52 to 0.75. No item hada loading greater than 0.50 on more than one factor. ItemsQ1 (I feel pleasant), Q6 (I feel rested), Q7 (I am calm and cool),Q10 (I am happy), Q13 (I feel secure), Q16 (I am content)and Q19 (I am a steady person) load higher on Factor1. ItemsQ2 (I tire quickly), Q3 (I feel like crying), Q9 (I worry toomuchover something that really doesn't matter) and Q20 (I get in astate of tension or turmoil as I think over my recent concernsand interests) load higher on Factor2. Items Q5 (I am losingout of things because I can't make up my mind soon enough),Q8 (I feel that difficulties are piling up so that I cannotovercome them), Q12 (I lack self-confidence), Q17 (Someunimportant thought runs throughmymind and bothers me)and Q18 (I take disappointments so keenly that I can't putthem out of my mind) load higher on Factor3.
The proportion of variance explained by each factor afterrotation is shown in Table 2. Even though the varianceexplained by the rotated Factor1 is less than that explained by
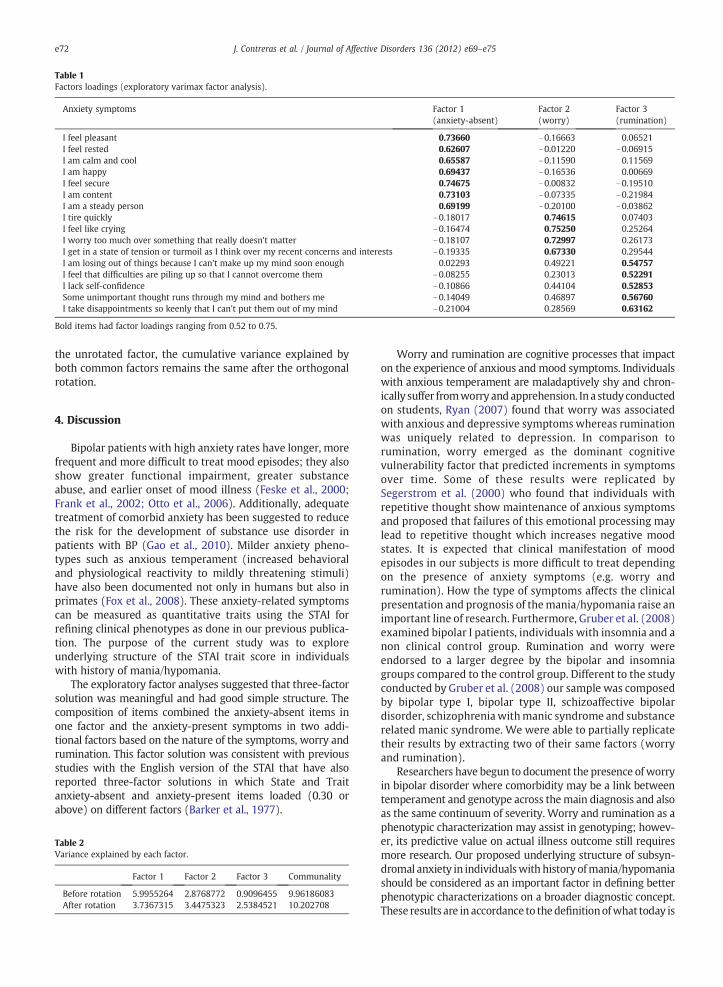
Table 1Factors loadings (exploratory varimax factor analysis).
Anxiety symptoms Factor 1(anxiety-absent)
Factor 2(worry)
Factor 3(rumination)
I feel pleasant 0.73660 −0.16663 0.06521I feel rested 0.62607 −0.01220 −0.06915I am calm and cool 0.65587 −0.11590 0.11569I am happy 0.69437 −0.16536 0.00669I feel secure 0.74675 −0.00832 −0.19510I am content 0.73103 −0.07335 −0.21984I am a steady person 0.69199 −0.20100 −0.03862I tire quickly −0.18017 0.74615 0.07403I feel like crying −0.16474 0.75250 0.25264I worry too much over something that really doesn't matter −0.18107 0.72997 0.26173I get in a state of tension or turmoil as I think over my recent concerns and interests −0.19335 0.67330 0.29544I am losing out of things because I can't make up my mind soon enough 0.02293 0.49221 0.54757I feel that difficulties are piling up so that I cannot overcome them −0.08255 0.23013 0.52291I lack self-confidence −0.10866 0.44104 0.52853Some unimportant thought runs through my mind and bothers me −0.14049 0.46897 0.56760I take disappointments so keenly that I can't put them out of my mind −0.21004 0.28569 0.63162
Bold items had factor loadings ranging from 0.52 to 0.75.
e72 J. Contreras et al. / Journal of Affective Disorders 136 (2012) e69–e75
the unrotated factor, the cumulative variance explained byboth common factors remains the same after the orthogonalrotation.
4. Discussion
Bipolar patients with high anxiety rates have longer, morefrequent and more difficult to treat mood episodes; they alsoshow greater functional impairment, greater substanceabuse, and earlier onset of mood illness (Feske et al., 2000;Frank et al., 2002; Otto et al., 2006). Additionally, adequatetreatment of comorbid anxiety has been suggested to reducethe risk for the development of substance use disorder inpatients with BP (Gao et al., 2010). Milder anxiety pheno-types such as anxious temperament (increased behavioraland physiological reactivity to mildly threatening stimuli)have also been documented not only in humans but also inprimates (Fox et al., 2008). These anxiety-related symptomscan be measured as quantitative traits using the STAI forrefining clinical phenotypes as done in our previous publica-tion. The purpose of the current study was to exploreunderlying structure of the STAI trait score in individualswith history of mania/hypomania.
The exploratory factor analyses suggested that three-factorsolution was meaningful and had good simple structure. Thecomposition of items combined the anxiety-absent items inone factor and the anxiety-present symptoms in two addi-tional factors based on the nature of the symptoms, worry andrumination. This factor solution was consistent with previousstudies with the English version of the STAI that have alsoreported three-factor solutions in which State and Traitanxiety-absent and anxiety-present items loaded (0.30 orabove) on different factors (Barker et al., 1977).
Table 2Variance explained by each factor.
Factor 1 Factor 2 Factor 3 Communality
Before rotation 5.9955264 2.8768772 0.9096455 9.96186083After rotation 3.7367315 3.4475323 2.5384521 10.202708
Worry and rumination are cognitive processes that impacton the experience of anxious and mood symptoms. Individualswith anxious temperament are maladaptively shy and chron-ically suffer fromworry andapprehension. Ina study conductedon students, Ryan (2007) found that worry was associatedwith anxious and depressive symptoms whereas ruminationwas uniquely related to depression. In comparison torumination, worry emerged as the dominant cognitivevulnerability factor that predicted increments in symptomsover time. Some of these results were replicated bySegerstrom et al. (2000) who found that individuals withrepetitive thought show maintenance of anxious symptomsand proposed that failures of this emotional processing maylead to repetitive thought which increases negative moodstates. It is expected that clinical manifestation of moodepisodes in our subjects is more difficult to treat dependingon the presence of anxiety symptoms (e.g. worry andrumination). How the type of symptoms affects the clinicalpresentation and prognosis of themania/hypomania raise animportant line of research. Furthermore, Gruber et al. (2008)examined bipolar I patients, individuals with insomnia and anon clinical control group. Rumination and worry wereendorsed to a larger degree by the bipolar and insomniagroups compared to the control group. Different to the studyconducted by Gruber et al. (2008) our sample was composedby bipolar type I, bipolar type II, schizoaffective bipolardisorder, schizophreniawithmanic syndrome and substancerelated manic syndrome. We were able to partially replicatetheir results by extracting two of their same factors (worryand rumination).
Researchers have begun to document the presence ofworryin bipolar disorder where comorbidity may be a link betweentemperament and genotype across themain diagnosis and alsoas the same continuum of severity. Worry and rumination as aphenotypic characterization may assist in genotyping; howev-er, its predictive value on actual illness outcome still requiresmore research. Our proposed underlying structure of subsyn-dromal anxiety in individualswith history ofmania/hypomaniashould be considered as an important factor in defining betterphenotypic characterizations on a broader diagnostic concept.These results are in accordance to thedefinitionofwhat today is

e73J. Contreras et al. / Journal of Affective Disorders 136 (2012) e69–e75
considered bipolar disorder type II (i.e. cyclothymic reactivity,neurotic features and panic attacks) (Akiskal et al., 2006).
According to Cloninger's seven-factor biosocial model ofpersonality, harm avoidance is a trait leading to behaviorsthat avoid aversive stimuli (Cloninger et al., 1994). The fourharm avoidance subscales include: anticipatory worry, fear ofuncertainty, shyness and fatigability. High harm avoidancehas been the most consistent finding across bipolar studiesand it has been shown to be vulnerable to state effects(Engström et al., 2004) being more associated with thesubsyndromal depression experienced by many patients ininterepisode periods (Judd et al., 2002). On the other hand,research has shown that patients with anxiety disorders havehigher scores on harm avoidance compared with healthyindividuals (Ball et al., 2002). Worriers have less perceivedcontrol over their anxiety, their inner experience of emotions,and less control over the external signs of emotion (Gouldand Edelstein, 2010). In our study the following items wereidentified in factor 2: Q2 I tire quickly, Q3 I feel like crying, Q9I worry too much over something that really doesn't matterand Q20 I get in a state of tension or turmoil as I think overmyrecent concerns and interests. It has been found thatrumination is associated with hypomania scores. Rustingand Nolen-Hoeksema (1998) found that rumination increasesanger and two years later Nolen-Hoeksema (2000) found thatrumination increases anxiety. Additionally, bipolar remittedpatients have reported greater rumination than those in acutemood episode (Thomas et al., 2007). Being these items verysimilar to those of the harm avoidance subscale, our findingssuggest that harm avoidance, as proposed by Cloninger,somehow defines a specific anxiety dimension of our sample.In the specific case of our study, we called this anxietydimension as worry considering it the most appropriate termto define this group of anxiety symptoms.
Comorbid obsessive compulsive disorder in bipolar disor-der is characterized by episodic course, higher rates of certainobsessions (e.g. aggressive/impulsive, sexual, religious, andobsessional doubts) which require more frequent hospitali-zations and complex pharmacological interventions (Perugiet al., 2002). A defining characteristic of OCD is unsuccessfulsuppression of unwanted thoughts. Obsessive symptomshave else been positively associated with rumination andinversely associated with perceived thought control ability(Grisham and Williams, 2009). Rumination involves repeti-tive thought about past events, current mood states, or failureto achieve goals (Martin and Tesser, 1996). Evidence suggeststhat rumination predicts the future occurrence of anxiety inanxious depressed comorbid conditions (Nolen-Hoeksema,2000). In subjects with history of mania/hypomania, rumi-nation may play an important role in triggering depressiveepisodes too. In our study, the following items were groupedin factor 3: Q5 I am losing out of things because I can't makeup my mind soon enough, Q8 I feel that difficulties are pilingup so that I cannot overcome them, Q12 I lack self-confidence,Q17 some unimportant thought runs through my mind andbothers me and Q18 I take disappointments so keenly that Ican't put them out of my mind. Due to the nature of the itemswe called this factor as rumination. One can argue that low-confidence represents a distinct type of anxiety; howeverrumination exhibits a negative effect on individual's decision-making which can ultimately be addressed as low self
confidence. For instance, Van Randenborgh et al. studied theunderlying mechanisms of rumination in dysphoric andnondysphoric subjects. They found that dysphoric subjectsexperience the decisions as more difficult and have lessconfidence in their choices (van Randenborgh et al., 2010).
Our results can help to develop further animal researchmodels to study the underlying etiologies of anxious-relatedprocesses in patients with history of mania/hypomania.Mounting evidence shows some functional genetic variantsassociatedwith anxiety givingnew insights into themoleculargeneticmechanismsunderlying these disorders. Specifically, astudy assessing sustained trait-like brain responses associatedwith anxious temperament rhesus monkeys found significantheritability of the anxious temperament phenotype (usingquantitative genetic analysis) and the metabolic activity inanxious temperament-associated hippocampal regions (usingvoxelwise analyses) (Oler et al., 2010). Recent findings from astudy using a knock-in mouse design suggested that subjectshomozygous for the 66Met allele scored significantly higherthan Val66 allele carriers on anxiety-related facets of theconstruct ‘harm avoidance’ (i.e., ‘anticipatory worry’ and ‘fearof uncertainty’) of the Temperament and Character Inventory(Montag et al., 2010). Somerville et al. (2010) found that bednucleus of the stria terminalis showed greater overallrecruitment and exaggerated tracking of threat proximity inindividuals with greater anxiety. These results suggest thatcontinuous functional magnetic resonance imaging could beused for elucidating the neural circuitries underlying sus-tained anticipatory features that ultimately might be utilizedin individuals with history of mania/hypomania.
In conclusion, our exploration analysis of anxiety subsyn-dromic symptoms has identified two anxiety constructs, worryand rumination. Based on the reviewed literature and on ourresults, it seems that worry and rumination are commonanxiety dimensions across patients with any history ofmania/hypomania and not only in bipolar disorder type I.Both, worry about potential future events and ruminationabout recently past eventsmay play a causal role in the creationof anxious comorbid disorders (as categorical diagnosis) in thisgroup of patients. The exploration of these underlyingconstructs will yield our proposed endophenotype of highface and construct validity with respect to subsyndromicanxiety. Our next step will be based on confirmatory factoranalysis aswell as other latent variablemodeling techniques totest hypotheses via inferential approach. We will test theobtained factors and analyze the variation among variablesusing the few newly created variables (factors) and theirmeaning based on current literature. Further research will testwhether these component factor scores are heritable, whetherthey share the same genetic factors, which (if they are nothighly correlated) may further help define the componentsunderlying bipolar disorder and other psychiatric disorderswith ahistory ofmania/hypomania.Wewill focus on etiologicalvalidity of these factors where quantitative anxiety trait can beused to identify genetic loci and genes which underlie this“portion” of the complex phenotype of patients with history ofmania/hypomania in the isolated Costa Rican sample. Our lineof research intends to improve our understanding on thepathophysiology of affective and anxiety disorders for a betterdiagnostic and pharmacologic treatment of these disablingdisorders.

e74 J. Contreras et al. / Journal of Affective Disorders 136 (2012) e69–e75
Some limitations of the current study are the assumptionof the same statistical parameters from our previouswork (nosignificant differences in the trait score regarding moodcurrent status, normal distribution of trait score and positivecorrelation between trait score and quantitative mania/hy-pomania). Even though the number of individuals are similarand belong to the same original study following identicalrecruitment and diagnostic process, the inclusion criteriadiffers due to specific research question. Previously, weanalyzed 30 bipolar I extended families (300 subjects) and20 healthy unrelated controls to study anxiety as a candidateendophenotype for the Costa Rican bipolar I sample. In thecurrent work we conducted an exploratory factor analysis ofsubjects who have history of mania/hypomania withouttaking into consideration familiarity. Confirmatory factoranalysis is beyond the scope of the current work andtherefore drawing substantive conclusions should be cau-tiously taken. For instance, for a given sample made up ofpedigrees of related individuals, the variance of the traitshould be partied into factors that reflect (depending onmodel specification) additive polygenic effects vs sibshipeffects or nuclear family effects. The effects of those factorscould be assessed after obtaining factor scores with confir-matory factor analysis and estimating heritability as an indexof familiality. Even though this analysis was conducted with asmall sample size, studies have revealed that adequatesample size in factor analysis is determined by the nature ofthe data (MacCallum et al., 1999). Our data showed uniformlyhigh communalities without cross loadings and more thanthree variables loading strongly on each retained factor. Sincemost of the psychometric analyses of this scale have beenconducted on nonclinical sample, comparison of our resultswith other studies becomes an important limitation.
Role of funding sourceFinancial support for this study was provided by Fogarty (TW006152)
training grant and NIMH 1 R01 MH069856-01A2 grant.
Conflict of interestNone of the authors have financial disclosures.
AcknowledgmentsFinancial support for this study was provided by Fogarty (TW006152)
training grant and NIMH 1 R01 MH069856-01A2 grant. The authors wish tothank Evelyn Duran, MD, Luis Roberto Rodriguez, MD, Marcela Barguil, MA,Lara Mora, MA and Adriana Pacheco MA for assistance in data collection andMercedes Ramirez, MD, Salvador Contreras, MD, Juan Zavala MD, ReginaArmas, PhD and Lorena Jimenez, MD for assistance in best estimation. Noneof the authors have financial disclosures. We are also grateful to the familieswho have made this research possible.
References
Akiskal, H.S., Pinto, O., 1999. The evolving bipolar spectrum. Prototypes I, II,III, and IV. Psychiatr. Clin N. Am. 22, 517–534.
Akiskal, H.S., Bourgeois, M.L., Angst, J., Post, R., Möller, H., Hirschfeld, R., 2000.Re-evaluating the prevalence of and diagnostic composition within thebroad clinical spectrum of bipolar disorders. J. Affect. Disord. 59, 5–30.
Akiskal, H.S., Akiskal, K.K., Perugi, G., Toni, C., Ruffolo, G., Tusini, G., 2006.Bipolar II and anxious reactive “comorbidity”: toward better phenotypiccharacterization suitable for genotyping. J. Affect. Disord. 96, 239–247.
Angst, J., Cui, L., Swendsen, J., Rothen, S., Cravchik, A., Kessler, R.C.,Merikangas, K.R., 2010. Major depressive disorder with subthresholdbipolarity in the national comorbidity survey replication. Am. J.Psychiatry 167, 1194–1201.
Ball, S., Smolin, J., Shekhar, A., 2002. A psychobiological approach topersonality: examination within anxious outpatients. J. Psychiatr. Res.36, 97–103.
Barker, B.M., Barker Jr., H.R., Wadsworth Jr., A.P., 1977. Factor analysis of theitems of the state–trait anxiety inventory. J. Clin. Psychol. 33, 450–455.
Cattell, R.B., 1966. The scree test for the number of factors. MultivariateBehav. Res. 1, 245–276.
Cloninger, C.R., Przybeck, T.R., Svrakic, D.M., Wetzel, R.D., 1994. TheTemperament and Character Inventory (TCI): a Guide to its Develop-ment and Use. Washington University Center for Psychobiology ofPersonality, St. Louis.
Contreras, J., Hare, E., Pacheco, A., Escamilla, M., Raventos, H., 2010. Issubclinical anxiety an endophenotype for bipolar I patients? A studyfrom a Costa Rican sample. J. Affect. Disord. 122, 267–272.
Engström, C., Brändström, S., Sigvardsson, S., Cloninger, R., Nylander, P.O.,2004. Bipolar disorder I. Temperament and character. J. Affect. Disord. 82,131–134.
Fabrigar, L.R., Wegener, D.T., MacCallum, R.C., Strahan, E.J., 1999. Evaluatingthe use of exploratory factor analysis in psychological research. Psychol.Meth. 4, 272–299.
Feske, U., Frank, E., Mallinger, A.G., Houck, P.R., Fagiolini, A., Shear, M.K.,Grochocinski, V.J., Kupfer, D.J., 2000. Anxiety as a correlate of response tothe acute treatment of bipolar I disorder. Am. J. Psychiatry 157, 956–962.
Floyd, F.J., Widaman, K.F., 1995. Factor analysis in the development andrefinement of clinical assessment instruments. Psychol. Assess. 7,286–299.
Fox, A.S., Shelton, S.E., Oakes, T.R., Davidson, R.J., Kalin, N.H., 2008. Trait-likebrain activity during adolescence predicts anxious temperament inprimates. PLoS One 3, 2570.
Frank, E., Cyranowski, J.M., Rucci, P., Shear, M.K., Fagiolini, A., Thase, M.E.,Cassano, G.B., Grochocinski, V.J., Kostelnik, B., Kupfer, D.J., 2002. Clinicalsignificance of lifetime panic spectrum symptoms in the treatment ofpatients with bipolar I disorder. Arch. Gen. Psychiatry 59, 905–911.
Gao, K., Chan, P.K., Verduin, M.L., Kemp, D.E., Tolliver, B.K., Ganocy, S.J., Bilali,S., Brady, K.T., Findling, R.L., Calabrese, J.R., 2010. Independent predictorsfor lifetime and recent substance use disorders in patients with rapid-cycling bipolar disorder: focus on anxiety disorders. Am. J. Addict. 19,440–449.
Goodwin, F.K., Jamison, K.R., 2007. Manic–Depressive Illness: BipolarDisorders and Recurrent Depression, Second Edition. Oxford UniversityPress, New York, pp. 29–86.
Gould, C.E., Edelstein, B.A., 2010. Worry, emotion control, and anxiety controlin older and young adults. J. Anxiety Disord. 24, 759–766.
Grisham, J.R., Williams, A.D., 2009. Cognitive control of obsessional thoughts.Behav. Res. Ther. 47, 395–402.
Gruber, J., Eidelman, P., Harvey, A.G., 2008. Transdiagnostic emotionregulation processes in bipolar disorder and insomnia. Behav. Res.Ther. 46, 1096–1100.
Joreskog, K.G., 1977. Factor analysis by least-square and maximum-likelihood method, Statistical Methods for Digital Computers3 ed. JohnWiley and Sons, New York.
Judd, L.L., Akiskal, H.S., Schettler, P.J., Endicott, J., Maser, J., Solomon, D.A.,Leon, A.C., Rice, J.A., Keller, M.B., 2002. The long-term natural history ofthe weekly symptomatic status of bipolar I disorder. Arch. Gen.Psychiatry 59, 530–537.
Kaiser, H.F., 1960. Varimax solution for primary mental abilities. Psychome-trika 25, 153–158.
Kaiser, H.F., 1974. An index of factorial simplicity. Psychometrika 39, 31–36.MacCallum, R.C., Widaman, K.F., Zhang, S.B., Hong, S.H., 1999. Sample size in
factor analysis. Psychol. Meth. 4, 84–99.MacKinnon, D.F., Zandi, P.P., Cooper, J., Potash, J.B., Simpson, S.G., Gershon, E.,
Nurnberger, J., Reich, T., DePaulo, J.R., 2002. Comorbid bipolar disorderand panic disorder in families with a high prevalence of bipolar disorder.Am. J. Psychiatry 159, 30–35.
Mantere, O., Suominen, K., Valtonen, H.M., Arvilommi, P., Isometsä, E., 2008.Only half of bipolar I and II patients report prodromal symptoms.J. Affect. Disord. 111, 366–371.
Martin, L.L., Tesser, A., 1996. Some ruminative thoughts. In: Wyer, R.S. (Ed.),Advances in Social Cognition. Lawrence Erlbaum Associates, Hillsdale, NJ.
Maxwell, M., 1992. Manual for the FIGS. Intramural Research Program,National Institute of Mental Health, Wasington, DC.
McElroy, S.L., Altshuler, L.L., Suppes, T., Keck Jr., P.E., Frye, M.A., Denicoff, K.D.,Nolen, W.A., Kupka, R.W., Leverich, G.S., Rochussen, J.R., Rush, A.J., Post,R.M., 2001. Axis I psychiatric comorbidity and its relationship to historicalillness variables in 288 patients with bipolar disorder. Am. J. Psychiatry158, 420–426.
Montag, C., Basten, U., Stelzel, C., Fiebach, C.J., Reuter, M., 2010. The BDNFVal66Met polymorphism and anxiety: support for animal knock-instudies from a genetic association study in humans. Psychiatry Res. 179,86–90.

e75J. Contreras et al. / Journal of Affective Disorders 136 (2012) e69–e75
Nadkarni, R.B., Fristad, M.A., 2010. Clinical course of children with adepressive spectrum disorder and transient manic symptoms. BipolarDisord. 12, 494–503.
Nolen-Hoeksema, S., 2000. The role of rumination in depressive disordersand mixed anxiety/depressive symptoms. J. Abnorm. Psychol. 109,504–511.
Nurnberger Jr., J.I., Blehar, M.C., Kaufmann, C.A., York-Cooler, C., Simpson,S.G., Harkavy-Friedman, J., Severe, J.B., Malaspina, D., Reich, T., 1994.Diagnostic interview for genetic studies. Rationale, unique features, andtraining. NIMH Genetics Initiative. Arch. Gen. Psychiatry 51, 849–859.
Oler, J.A., Fox, A.S., Shelton, S.E., Rogers, J., Dyer, T.D., Davidson, R.J., Shelledy,W., Oakes, T.R., Blangero, J., Kalin, N.H., 2010. Amygdalar and hippo-campal substrates of anxious temperament differ in their heritability.Nature 466, 864–868.
Otto, M.W., Simon, N.M., Wisniewski, S.R., Miklowitz, D.J., Kogan, J.N., Reilly-Harrington, N.A., Frank, E., Nierenberg, A.A., Marangell, L.B., Sagduyu, K.,Weiss, R.D., Miyahara, S., Thas, M.E., Sachs, G.S., Pollack, M.H., STEP-BDInvestigators., 2006. Prospective 12-month course of bipolar disorder inout-patients with and without comorbid anxiety disorders. Br. J.Psychiatry 189, 20–25.
Perugi, G., Toni, C., Frare, F., Travierso, M.C., Hantouche, E., Akiskal, H.S., 2002.Obsessive–compulsive–bipolar comorbidity: a systematic exploration ofclinical features and treatment outcome. J. Clin. Psychiatry 63,1129–1134.
Rodrigo, G., Lusiardo, M., 1988. Note on the reliability and concurrent validityof the Spanish version of the state–trait anxiety inventory. Percept. Mot.Skills 67, 926.
Rusting, C.L., Nolen-Hoeksema, S., 1998. Regulating responses to anger:effects of rumination and distraction on angry mood. J. Pers. Soc. Psychol.74, 790–803.
Ryan, Y.H., 2007. Worry and rumination: differential associations withanxious and depressive symptoms and coping behavior. Behav. Res.Ther. 45, 277–290.
Sato, T., Bottlender, R., Kleindienst, N., Möller, H.J., 2002. Syndromes andphenomenological subtypes underlying acute mania: a factor analyticstudy of 576 manic patients. Am. J. Psychiatry 159, 968–974.
Segerstrom, S.C., Tsao, Jennie, C.I., Alden, L.E., Craske, M.G., 2000. Worry andrumination: repetitive thought as a concomitant and predictor ofnegative mood. Cogn. Ther. Res. 24, 671–688.
Somerville, L.H., Whalen, P.J., Kelley, W.M., 2010. human bed nucleus of thestria terminalis indexes hypervigilant threat monitoring. Biol. Psychiatry68, 416–424.
Spielberger, C.D., Gorsuch, R.L., Lushene, R., Vagg, P.R., Jacobs, G.A., 1983.Manual for the State–Trait Anxiety Inventory (Form Y). ConsultingPsychologists Press, Palo Alto, CA.
Thomas, J., Knowles, R., Tai, S., Bentall, R.P., 2007. Response styles to depressedmood in bipolar affective disorder. J. Affect. Disord. 100, 249–252.
van Randenborgh, A., de Jong-Meyer, R., Hüffmeier, J., 2010. Ruminationfosters indecision in dysphoria. J. Clin. Psychol. 66, 229–248.
Vázquez, G.H., Kahn, C., Schiavo, C.E., Goldchluk, A., Herbst, L., Piccione, M.,Saidman, N., Ruggeri, H., Silva, A., Leal, J., Bonetto, G.G., Zaratiegui, R.,Padilla, E., Vilapriño, J.J., Calvó, M., Guerrero, G., Strejilevich, S.A.,Cetkovich-Bakmas, M.G., Akiskal, K.K., Akiskal, H.S., 2008. Bipolardisorders and affective temperaments: a national family study testingthe “endophenotype” and “subaffective” theses using the TEMPS-ABuenos Aires. J. Affect. Disord. 108, 25–32.
Velicer, W.F., Fava, J.L., 1998. Effects of variable and subject sampling onfactor pattern recovery. Psychol. Meth. 3, 231–251.
Vieta, E., Phillips, M.L., 2007. Deconstructing bipolar disorder: a criticalreview of its diagnostic validity and a proposal for DSM-V and ICD-11.Schizophr. Bull. 33, 886–892.
Vigneau, F., Cormier, S., 2008. The factor structure of the State–Trait AnxietyInventory: an alternative view. J. Pers. Assess. 90, 280–285.
Virella, B., Arbona, C., Novy, D., 1994. Psychometric properties and factorstructure of the Spanish version of the state–trait anxiety inventory.J. Pers. Assess. 63, 401–412.