Embed Size (px)
Citation preview

BritishJournal ofOphthalmology, 1990, 74, 437-439
Primary orbital liposarcoma: clinical and computedtomographic features
Alan A McNab, Ivan Moseley
AbstractLiposarcoma of the orbit is rare. The clinicaland radiological characteristics of two cases,of myxoid and pleomorphic types, arereported. In neither case was the histologicaldiagnosis evident before surgery.
Primary orbital liposarcoma is extremely rare.Sixteen cases, mostly myxoid and none definitelyidentified as pleomorphic, have been reported indetail in the literature. The two patients des-cribed here are the fourth and fifth to be seen inthe Orbital Clinic at Moorfields Eye Hospitalsince 1982. The preceding patients, all of whomhad myxoid tumours, have been reported onpreviously.' To our knowledge the clinical andradiological features ofpleomorphic liposarcomaarising in the orbit are described for the firsttime.
Case reports
CASE 1A 69-year-old woman complained of progressiveright proptosis over six months. She had verticaldiplopia and difficulty in seeing colours clearlywith the right eye. Her general health wasexcellent.Her best corrected vision was 6/9 in the right
eye and 6/6 left. She made four errors on theIshihara test plates with the right eye, and wasthought to have an afferent pupillary defect. Theglobe was displaced 9 mm forwards and 4 mmdownwards. Ocular motility was restricted,
I
::
40
Figure IB
particularly in elevation. A non-tender mass waspalpable in the upper orbit. General examinationwas normal, as was a chest radiograph.Computed tomography (CT) of the orbits was
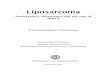
obtained in sagittal and coronal planes afterintravenous injection of iodinated contrastmedium (Fig 1). A well defined, rounded intra-conal mass of low density was shown, lying justabove the globe.The mass was explored via an upper lid skin
incision, the levator palpebrae superiorisand superior rectus muscles being retractedmedially. Anteriorly the tumour was wellcircumscribed, but posteriorly it appeared toblend with the orbital fat. It was pale, yellow-grey, and petechial haemorrhages appeared onits surface as it was touched. The incisionalbiopsy specimen floated in 10% formaldehydesolution.
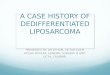
Histological examination revealed a tumourwith numerous rounded spaces which on frozensection contained lipid. Some cells were spindleshaped and lay in a mucinous matrix, whileothers showed a signet ring form. There wasnuclear hyperchromatism, scattered cells havingenlarged, pleomorphic nuclei; some of the nucleiwere vesicular. Numerous capillaries werepresent throughout the mass. The appearanceswere typical of a myxoid liposarcoma (Fig 2).Over the next four weeks the proptosis
increased by 2 mm. Orbital exenteration wasperformed, with removal of the upper lid andadequate clearance beyond the posterior marginof the tumour. There has been no evidence ofrecurrence for more than a year since surgery.
.. ...
Moorfields Eye Hospital,City Road, LondonEC1V 2PDA A McNabI MoseleyCorrespondence to:Dr I Moseley.Accepted for publication25 January 1990
Figure IA
Figure 1: Case 1. CT with intravenous contrast medium.Axial (A) and direct coronal (B) sections show a well defined,rounded, intraconal mass lying above the globe, which is notdistorted. The mass extends posteriorly above the optic nerve(C). The orbit is not enlarged. The radiographic density ofthemass is uniform, being intermediate between that ofthevitreous and that ofnormal orbitalfat - that is, it appears lessdense than water. The more anterior coronal image (B)suggests a capsule ofhigher density.
eI7 ..
Figure IC
437
on Septem
ber 16, 2020 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.74.7.437 on 1 July 1990. Dow
nloaded from

McNab, Moseley438
Figure 2: Case 1. Myxoidliposarcoma with nuclearhyperchromatism andoccasional signet ring cells.The numerous clear spacescontained lipid on frozensection. (Haematoxylin andeosin, x 225.)
,I. A
X- I-, i
X in
~*l
r
A, .. .4;fIrv
1.~~~~~~~~~~~4
-4k
.,=. a,^ .... .t R*.
CASE 2
A 52-year-old man noted blurred vision in theright eye seven months before his presentation to
the orbital clinic, followed two months later byproptosis. His vision corrected to 6/9, but he hadmild disc swelling and 3 mm of proptosis. Thisincreased to 5 mm over 3 months, and he devel-oped diplopia on left lateral gaze. He had no pain.
In the orbital clinic his best correctd acuitywas 6/24 in the right eye and 6/5 left. He read allthe Ishihara plates, but was slower on the right.There was a mild right relative afferent pupildefect. The globe was displaced 5 mm forwards
Figure 3A
Figure3B
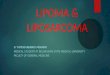
Figure 3: Case 2. CT without intravenous contrast medium. Direct axial (A) and reformattedoblique parasagittal (B) images: a well defined, lobulated mass over 2 cm in diameter lies withinthe muscle cone, superomedial to the optic nerve, slightlyflattening the globe. The mass isgenerally isodense with brain; its less dense posterior portion is still denser than the vitreous. Theroofofthe orbit is very thin, possibly eroded.
use s . .#e 4ls A S2
clear ,:spce als cotane slpdon frze section.
(HaelfatoXylin and eosin preparation, x225.)
and inferolaterally, with limited elevation andadduction. The optic disc was grossly swollen,with engorged retinal veins, but there were nochoroidal folds. The upper lid was full. Generalexamination and chest radiograph were normal.
Plain films of the orbits also showed nothingabnormal, but CT showed a well defined masswithin the muscle cone, containing areas oflowerdensity within it (Fig 3).
At lateral orbitotomy a large, purplish, lobu-lated tumour was found intraconally, abuttingthe globe, the medial rectus muscle, and theupper surface of the optic nerve. It appeared tobe well encapsulated, and was dissected free ofthe surrounding structures. A large artery enter-ing its posterior pole was divided and the masswas removed in one piece.
Histological examination (Fig 4) disclosed aliposarcoma of extremely variable morphology,with numerous thin walled vessels, lipoblasts,and large, deeply eosinophilic giant cells. Mitoticfigures were infrequent, but foci of inflammationand haemorrhage were present. There was notrue capsule. The histological diagnosis wastherefore pleomorphic liposarcoma.The orbit was exenterated, together with the
scar, but the lids were spared. Examination ofthe excised tissue showed a single nodule oftumour, less than 1 mm in diameter, well clear ofthe resection margin. One year later there wasno evidence of local recurrence or distantmetastasis.
DiscussionBecause of its rarity liposarcoma does not usuallyenter into the differential diagnosis in patientswith orbital masses. The 16 primary orbitalliposarcomas reported in detail' 12 affected menand women equally, their ages ranging from 5 to77 years, mean 34.
Reports of the results of imaging are sketchy.Plain radiography commonly shows nothingabnormal, but it may show enlargement of theorbit, sometimes considerable, with thinningand inferior displacement of the floor.' Echo-graphy may indicate a relatively well defined,multiseptate lesion with non-specific areas ofhigh echogenicity. I3 In the few patients who haveundergone CT, none of whom had pleomorphictumours, findings have varied from well defined,homogeneous lesions of soft tissue density, not
on Septem
ber 16, 2020 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.74.7.437 on 1 July 1990. Dow
nloaded from

Primary orbital liposarcoma: clinical and computed tomographicfeatures
evidently fatty," 13 to heterogeneous masses con-taining fat.' In two patients CT failed to reveal anidentifiable mass, and in one of these T2-weighted magnetic resonance imaging (MRI)showed abnormally high signal from part of theorbital fat, indicating its pathological nature.'
In our first patient the clue to the correctdiagnosis was the low radiographic density of thelesion: fat is the only tissue component less densethan the water of the vitreous. Choristomas maycontain fat, but are not characteristically retro-bulbar, and benign lipomas of the orbit are
exceedingly rare. Case 2 showed areas of lowerdensity than brain but no clear evidence of fat.There were no radiological features indicatingthe malignant nature of the tumour in eitherpatient. The short history and documented pro-gression of symptoms and signs are, in retro-spect, more suggestive.
Enziger and Weiss'4 divided primary lipo-sarcomas into myxoid tumours (which formabout half) and round cell, well differentiated,and dedifferentiated forms; a pleomorphic typeis also described. Myxoid tumours usually have a
gelatinous consistency, while poorly differen-tiated tumours are soft and haemorrhagic, withareas of necrosis and cyst formation. Of theprimary orbital lesions reported most were
myxoid; one showed predominantly roundcells,9 while another, described as lipocytic,6might have been categorised as pleomorphic.
Metastasis of liposarcoma to the orbit is alsoreported,'3 '5 the commonest primary sites beingthe deep connective tissue planes of the thigh or
retroperitoneum. In an obese patient like our
case 1 it is possible, though unlikely, that a
primary tumour went undetected.The peak incidence of lipomas outside the
orbit is between 40 and 60 years of age - that is,later than that of orbital lesions, probably reflect-ing their less critical location. Patients withmyxoid tumours tend to be younger, and malesare more commonly affected than females. 'IOf the 16 well documented cases of primary
orbital liposarcoma'-12 six resulted in death. Theconsensus on treatment elsewhere in the body iswide local excision."'" Radiotherapy affordslittle benefit in the better differentiated lipo-sarcomas, but successes have been reported withpoorly differentiated tumours.'6 Chemotherapyhas not generally been helpful, though Gottliebet a120 reported remission in three patients.
Both the tumours described here were welldefined on CT and appeared relatively wellencapsulated at surgery. However, the 'capsule'represents compressed orbital tissues; there is no
true capsule between the neoplastic tissue andthe normal structures. Three patients previouslyoperated upon in this hospital' have now beenfollowed up for from two to five years withoutevidence of tumour recurrence or dissemination.
Prognosis of liposarcomas elsewhere in thebody has been related to histology. Thus in aseries of 77 patients treated by surgical excision,27 of whom also received radiotherapy, the 10-year survival was 12 of 20 with myxoid tumours,but only 1 of 24 with round cell or pleomorphiclesions. Site, size, and adequacy of excision wereall important factors.2' The rational approach toorbital liposarcoma would therefore appear to bewide local excision, which will usually necessi-tate exenteration or even midfacial resection. Inan elderly patient with a mxyoid or well differen-tiated tumour local excision is justifiable.
AA McNab was supported by the OPSM fellowship of the RoyalAustralian College of Ophthalmologists.
1 Lane CM, Wright JE, Garner A. Primary myxoid liposarcomaof the orbit. BrJ Ophthalmol 1988; 72: 912-7.
2 Strauss M. Liposarkom der recten Orbita. Dtsch MedWochenschr 191 1; 37: 239.
3 Stout AP. Liposarcoma - the malignant tumour of lipoblasts.Ann Surg 1944; 119: 86-107.
4 Quer6 MA, Camain R, Baylet R. Liposarcome orbitaire. AnnOculist (Paris) 1963; 1%: 994-1003.
5 Cilotti P. Su di particolare forma di liposarcoma dell'orbitacon conspicue variazioni morfologiche durante la suaevoluzione. Ann Oftal Oculistica 1964; 90: 325-37.
6 Mortada A. Rare primary orbital sarcomas. AmJr Ophthalmol1969; 68: 919-25.
7 Henderson JW. Orbital tumors. Philadelphia: Saunders, 1973:262-7.
8 Schroeder W, Dastendieck H, von Domarus D. Primaresmyxoides Liposarkom der Orbita: klinscher und histopatho-logischer Fallbericht. Ophthalmologica 1976; 172: 337-45.
9 Kimura Y, Nagato M, Yamabe H. A case of orbital lipo-sarcoma. Fol OphthalmolJpn 1978; 29: 983-8.
10 Jakobiec FA, Jones IS. In: Duane TD, ed. Clinical ophthal-mology. Hagerston: Harper and Row, 1982; 2: 17-9.
11 Naeser P, Mostrom U. Liposarcoma of the orbit: a clinico-pathological case report. BrJ7 Ophthalmol 1982; 66: 190-3.
12 Malan P, Baldet P, Arnaud B. Primary orbital liposarcoma.Clinicopathological case report and review of the literature.Orbit 1983; 2: 99-105.
13 Nasr AM, Ossoinig KC, Kersten RF, Blodi FC. Standardizedechographic-histopathologic correlations in liposarcoma.AmJ Ophthalmol 1985; 99: 193-200.
14 Enziger FM, Weiss SW. Soft tissue tumors. St Louis: Mosby,1973.
15 Abdalla MI, Ghaly AF, Hosni F. Liposarcoma with orbitalmetastases. BrJ7 Ophthalmol 1966; 50: 426-8.
16 Enterline HT, Culberson JD, Rochlin DB, Brady LW.Liposarcoma: a clinical and pathological study of 53 cases.Cancer 1960; 13: 932-50.
17 Pack GT, Pierson JC. Liposarcoma: a study of 105 cases.Surgery 1954; 36: 687-712.
18 Spittle ME, Newton KA, McKenzie DH. Liposarcoma. Areview of 60 cases. BrJ7 Cancer 1970; 24: 696-704.
19 Kinne DW, Chu FCH, Huvos AG, Yagoda A, Fortner JG.Treatment of primary and recurrent retroperitoneal lipo-sarcoma. Twenty-five-year experience at MemorialHospital. Cancer 1973; 31: 53-64.
20 Gottlieb JA, Baker LH, Quagliana JM, et al. Chemotherapy ofsarcomas with a combination of adriamycin and dimethyltriazeno imidazole carboxamide. Cancer 1972; 30: 1632-8.
21 Kindblom LG, Angervall L, Svendsen P. Liposarcoma: aclinicopathological, radiographic and prognostic study. ActaPathol Microbiol Immunol Scand (A) 1975: supply 253.
439
on Septem
ber 16, 2020 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.74.7.437 on 1 July 1990. Dow
nloaded from