Embed Size (px)
Citation preview

A malignant fibrous histiocytoma (MFH) is a tumorthat occurs most frequently in the lower and upper ex-tremities and in the retroperitoneum. A primary MFHof the mesentery is rare, and few cases have been re-ported (1-4). This case report describes the findings of asonographic image, serial computed tomographic (CT)images, and presents different pathologic diagnoses ofsuch a tumor based on the results of a sono-guided aspi-ration, a laparoscopic biopsy, and an excisional biopsy.A surgical excisional biopsy of the tumor confirmed thepresence of a storiform-pleomorphic MFH in the mesen-tery.
Case Report
A 48-year-old man visited our clinic because of a pain-less palpable mass in the right lower abdomen. The pa-tient detected the mass two weeks prior to the clinic vis-it. The patient had no history of trauma or any previoussurgery. A physical examination of the patient revealedthe presence of a large, firm mass in the right lower ab-domen. The level of serum carbohydrate antigen 19-9was elevated, but the other laboratory findings werenormal. An initial abdominal CT scan showed an ap-proximate 4.5 cm sized heterogeneously enhancingmass with a partially indistinct margin and irregular per-itumoral strands in the mesentery of the right lower ab-domen (Fig. 1A). This mass was causing right hy-dronephrosis. Sonograms showed the presence of an ill-defined low-echoic mass. The presumptive diagnoses in-
J Korean Radiol Soc 2007;57:549-552
─ 549 ─
Primary Malignant Fibrous Histiocytoma of theMesentery: A Case Report1
Jong Heon Park, M.D., Jae Woo Yeon, M.D., Eun Mee Han, M.D.2, Suk Ki Jang, M.D., Su Min Kang, M.D., In Oak Ahn, M.D.
1Department of Radiology, Bundang Jesaeng General Hospital2Department of Pathology, Bundang Jesaeng General HospitalReceived August 13, 2007 ; Accepted October 15, 2007Address reprint requests to : Jae Woo Yeon, M.D., Department ofRadiology, Bundang Jesaeng General Hospital, 255-2, Seohyun-dong,Bundang-gu, Sungnam-si, Gyungki-do 463-774, Korea.Tel. 82-31-779-0051 Fax. 82-31-779-0060 E-mail: [email protected]
A malignant fibrous histiocytoma of the mesentery is rare, and multifocal involve-ment as a primary tumor is very rare. In this report, a case of malignant fibrous histio-cytoma of the mesentery presenting with two masses and multiple peritoneal seedingin a 48-year-old man is described. A physical examination revealed a large, firm, andnon-tender mass in the right lower abdomen of the patient. Computed tomography ofthe lesion revealed a partially, indistinctly marginated and heterogeneously enhancingmass with irregular peritumoral strands in the mesentery of the right lower abdomen,while sonograms of the lesion revealed an ill-defined low-echoic mass. The finalpathology demonstrated the presence of a storiform-pleomorphic malignant fibroushistiocytoma.
Index words : MesenteryMalignant fibrous histiocytomaUltrasonographyComputed tomography (CT)

Jong Heon Park, et al : Primary Malignant Fibrous Histiocytoma of the Mesentery
─ 550 ─
C D
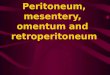
E FFig. 1. A 48-year-old man with a palpable mass in the right lower abdomen.A. Computed tomography shows a partially indistinct and heterogeneously enhancing mass with irregular peritumoral strands(white arrows) in the mesentery of the right lower abdomen.B, C. Three months later, follow-up computed tomography shows an increased size of the known mass (white arrows) in themesentery of the right lower abdomen and another mass (black arrows) with a similar nature in the mesentery of the upper ab-domen.D. A microphotograph shows mononuclear histiocyte-like cells and multinucleated giant cells (H & E staining, × 200).E. Immunohistochemical staining for smooth muscle actin shows a positive reaction in the histiocyte-like cells (smooth muscleactin, × 200).F. Microphotographs show irregular peritumoral strands including infiltrating tumor cells and desmoplastic reaction in the mesen-tery (H & E staining, × 200).
BA

cluded a variety of tumor or tumor-like conditions of themesentery causing a desmoplastic reaction, such as ametastatic tumor, carcinoid tumor and sclerosingmesenteritis. An ultrasound-guided aspiration was per-formed, and the possibility of a benign spindle cell tu-mor was suggested. Three days later, a laparoscopicbiopsy was performed, and the pathologist suggestedthe possibility of fibromatosis or a gastrointestinal stro-mal tumor. A complete excision of the mass was recom-mended for an accurate diagnosis. An excisional biopsywas scheduled, but the biopsy was delayed. Twomonths later, the abdominal pain and distension be-came aggravated. A follow-up abdominal CT scanshowed an increase in the size of the known mass in themesentery of the right lower abdomen, and demonstrat-ed the appearance of a new similar mass in the mesen-tery of the upper abdomen. In retrospect, the initial CTimages revealed the presence of multiple mesentericnodules (Fig. 1B, C). The multiple small, enhancing nod-ules in the mesentery and the omentum had grownwithin the two-month period. An extended right hemi-colectomy with jejunal resection was performed for pal-liative treatment. Macroscopically, the surgical speci-men contained two ill-defined serosal-intramuscularmasses in the mesentery of the jejunum and terminalileum. Neither necrosis nor hemorrhage was present inthe gross specimen. The remaining serosa showed mul-tiple mesenteric nodules, measuring from 0.5 cm to 1.5cm in the longest dimension. A histopathological exami-nation revealed some areas of a storiform pattern, highcellularity, and marked nuclear pleomorphism withmultinucleated giant cells in the tumors of the mesen-tery (Fig. 1D). Immunohistochemical staining was posi-tive for expression of smooth muscle actin and negativefor expression of CD34, C-kit, S-100 protein, desmin,and cytokeratin. These findings were suggestive of astoriform-pleomorphic malignant histiocytoma (Fig. 1E).
Five months have elapsed since the surgery, and thepatient is doing relatively well without any evident tu-mor recurrence or distant metastasis.
Discussion
Primary tumors arising in the mesentery are rare, butthe mesentery is a frequent route for the spread of a ma-lignant neoplasm through the peritoneal cavity and be-tween the peritoneal space and the retroperitoneum (5).Most primary lesions are mesenchymal in origin, andmost are histologically benign. Malignant mesenchymal
lesions include liposarcomas, leiomyosarcomas, malig-nant schwannomas, synovial sarcomas, fibrosarcomasand MFHs. Unfortunately, with the exception of a mi-nority of lesions, such as lipomas, hemangiomas andsubacute hematomas, the radiological appearance ofmost soft-tissue masses remains nonspecific (1).
An MFH in the abdominal cavity represents 16% of allMFHs, and most of these lesions are located in theretroperitoneum. If secondary involvement of the ab-dominal cavity can be ruled out, the presence of an in-tra-abdominal, extra-retroperitoneal MFH could be con-sidered even though multifocal involvement is veryrare. The anatomic distribution of an intra-abdominal,extra-retroperitoneal MFH is as follows: the stomach,the small intestine, the colon, the appendix, the mesen-tery, the liver, and the spleen (1-3).
The pathological diagnosis of MFH can be inaccurateif the whole mass cannot be excised as it is composed ofvariably proportioned histiocytic and fibrous elements.The complete excision of the mass is therefore recom-mended for an accurate diagnosis.
In general, on a CT scan, MFH appears as a relativelywell-defined and homogenous mass, or a mass with in-ternal low attenuation due to necrosis or hemorrhage.The frequency of internal necrosis or hemorrhage in-creases in proportion to the mass size (6). Lee et al. re-ported 13 masses in the abdomen out of seven cases thatwere pathologically confirmed to be MFHs; eight of thelesions (62%) had a peritumoral-vascular-appearingstructure. Previous reports had not mentioned this find-ing (4), and Lee and colleagues first reported this findingbut there was no pathological confirmation of the pres-ence of a peritumoral-vascular-appearing structure.
For MFHs, sonography demonstrates the presence ofthree patterns, including a hypoechoic pattern (the mostfrequent), a mixed pattern with an extensive necroticarea, and a predominantly anechoic pattern with thicksepta (6).
On a CT scan, the MFH appeared as an irregularlymargined, heterogeneously enhancing mass with irregu-lar peritumoral strands in the mesentery, and as an ill-defined low-echoic mass on the ultrasonogram. The ir-regular peritumoral strands in this case are similar to theperitumoral-vascular-appearing structure that Lee andcolleagues have reported. When these findings werecorrelated with the pathological findings, they mainly adesmoplastic reaction that included infiltrating tumorcells (Fig. 1B, F).
The differential diagnoses of soft-tissue masses with ir-
J Korean Radiol Soc 2007;57:549-552
─ 551 ─

regular peritumoral strands in the mesentery includesclerosing mesenteritis, mesenteric edema or hemor-rhage, mesenteric inflammation secondary to pancreati-tis, fibrofatty mesenteric proliferation related to Crohn’sdisease, primary mesenteric neoplasms (e.g., a desmoidor carcinoid tumor), peritoneal mesotheliomas, andmetastatic neoplasms (5, 7). Although rare, a MFHshould be included in these differential diagnoses.
In general, an extra-retroperitoneal abdominal MFHrecurs in 37-51% of all cases and metastases occur in42% of all cases, essentially in the lungs and lymphnodes. The overall two-year and five-year survival ratesfor patients afflicted with MFH have been reported tobe about 60% and 47%, respectively (2). The prognosisof an MFH is unclear, but most of the reports suggestedthat it is poor. One group of investigators reported thatpostoperative chemotherapy increased the survival rate,but another group of investigators has reported thatpostoperative chemotherapy did not achieve curative re-sults. There is a report stating that the tumor was not ra-diosensitive. However, it is clear that complete surgicalexcision in the early phase is essential to improve theprognosis, although the role of adjuvant chemotherapyafter surgery is still unclear (8-10).
In the current case, surgical resection was delayed asthe ultrasound-guided aspiration and laparoscopic biop-sy suggested that the tumor was benign. Unfortunately,this outcome might have influenced the prognosis of thepatient.
In conclusion, if CT scan images reveal a large soft-tis-sue mass with irregular peritumoral strands in themesentery, especially in a middle-aged adult, an MFH
must be included in the differential diagnoses, alongwith other benign or malignant disorders. Furthermore,for an accurate diagnosis of an MFH, the whole massmust be excised.
References
1. Kransdorf MJ. Malignant soft-tissue tumors in a large referral pop-ulation: distribution of diagnoses by age, sex, and location. AJR AmJ Roentgenol 1995;164:129-134
2. Bruneton JN, Drouillard J, Roqopoulos A, Laurent F, Normand F,Balu-Maestro C, et al. Extraretroperitoneal abdominal malignantfibrous histiocytoma. Gastrointest Radiol 1988;13:299-305
3. Ros PR, Viamonte M Jr, Rywlin AM. Malignant fibrous histiocy-toma: mesenchymal tumor of ubiquitous origin. AJR Am JRoentgenol 1984;142:753-759
4. Lee KH, Lee HG, Lee JM, Lee HJ, Ha HK, Baik JH, et al.Radiological findings of primary abdominal malignant fibrous his-tiocytoma: emphasis on CT findings. J Korean Radiol Soc1996;35:559-564
5. Sheth S, Horton KM, Garland MR, Fishman EK. MesenetericNeoplasms: CT appearances of primary and secondary tumors anddifferential diagnosis. Radiographics 2003;23:457-473
6. Goldman SM, Hartman DS, Weiss SW. The varied radiographicmanifestations of retroperitoneal malignant fibrous histiocytomarevealed through 27 cases. J Urol 1986;1352:33-38
7. Horton KM, Lawler LP, Fishman EK. CT findings in sclerosingmesenteritis (panniculitis): spectrum of disease. Radiographics2003;23:1561-1567
8. Levinson MM, Tsang D. Multicentric malignant fibrous fibroushistiocytomas of the colon. Reporto of a case and review of thesubject. Dis Colon Rectum 1982;25:327-331
9. Ekfors TO, Rantakokko V. An analysis of 38 malignant fibrous his-tiocytomas in the extremities. Acta Pathol Microbiol Scand(A)1978;86:25-35
10. King RM, Pairolero PC, Trastek VF, Piehler JM, Payne WS,Bernatz PE. Primary chest wall tumors: factors affecting survival.Ann Thorac Surg 1986;41:597-601
Jong Heon Park, et al : Primary Malignant Fibrous Histiocytoma of the Mesentery
─ 552 ─
대한영상의학회지 2007;57:549-552
장간막의 원발성 악성 섬유성조직구종: 증례 보고1
1분당제생병원 영상의학과2분당제생병원 진단병리과
박종헌·연재우·한은미2·장석기·강수민·안인옥
장간막에 생기는 악성 섬유성조직구종은 드문 원발성 종양이며 다발성으로 생기는 경우는 매우 드물다. 저자들
은 최근 발생한 우하복부에 만져지는 종괴를 주소로 내원한 48세 남자 환자에서 장간막에 발생한 두개의 커다란
종괴와 복막 암종증이 동반된 1예를 경험하였기에 초음파, 컴퓨터단층촬영 및 조직 병리소견을 함께 보고하고자 한
다. 이 종괴는 초음파에서 경계가 불분명한 저에코로 보였고 컴퓨터단층촬영에서는 부분적으로 경계가 불분명한 불
균한 조영증강을 보였으며 주변으로 불규칙한 선상 구조물들이 있었다. 최종 병리 진단은 장간막에서 발생한 다형
성 악성 섬유성조직구종이었다.