Embed Size (px)
Citation preview

PRIMARY INTRACEREBRAL HODGKIN’S DISEASE
J. I>. SCHRICKER, JR., LT. COL., M.c., u . s . A . , ~ AND DAVID E. SMITH, M.D.
ODGKIN’S DISEASE arising primarily within the substance of the central nervous sys-
tern and having no demonstrable lesions else- where is unusual. Cases of a sarcomatous form wirh primary lesions in the brain have been reported by Sparling and Adams; Sparling, Adams, and Parker; Berkman, Netsky, and Zimmerman; and Jackson and Parker.6, How- ever, authenticated cases of primary intracere- bra1 granulomatous lesions of Hodgkin’s dis- ease have not been described. Sparling, Adams, and Parker state that there are no proved in- stances of the nonsarcomatous form of Hodg- kin’s disease originating in the cerebral tissue, although they report invasion of the brain. from lesions in the bones of the skull or the in tracranial dura.
The following case is presented because it appears to be a clear-cut example of isolated intracerebral Hodgkin’s granuloma.
CASE REPORT
H. C., a 45-year-old white man, was admitted to the neurosurgical service at Barnes Hospital, September 20, 1951, complaining of severe frontal headache with episodic diz~iness of LWO weeks’ duration.
About December, 1950, his wife noted that he became “less cheerful,” antisocial, insecure, and worried. Without consulting his physician he placed himself on a low salt, reducing diet and lost 40 lb. He felt well until August 3, 1951, when he fainted while at work. This was considered to be due to heat prostration. He was hospitalized locally for seven days and found to be in a state of moderately severe so- dium depletion. He was treated for this condi- tion and discharged after seven days.
There were no further complaints during the ensuing month, but he continued to be moody and depressed. Two weeks prior to ad- mission to Barnes Hospital there was insidious onset of bifrontal headaches of moderate se- verity, relieved somewhat by lying down and associated with occasional nausea and severe
From the departments of Surgery (Division of Neuro- surgery) and Pathology, Washington University Medi- cal School, St. Louis, Missouri.
“Present address: Chief, Neurosurgical Service, De- partment of Surgery, Fitzsimons Army Hospital, Den- ver, Colorado.
Rcceived for publication, January 3, 1955.
episodic vertigo. His family physician noted the presence of papilledema.
The patient, on admission, was a moderately obese white man complaining of headache in- tensified by the upright position. There was bilateral papilIedema, more severe on the right than on the left, with two fresh retinal hemor- rhages close to the disc on the right and a smaller old hemorrhage in the center of the left disc. Blood pressure was 190 mm. of mer- cury systolic and 1 10 mm. diastolic. Neurologi- cal examination was normal except for slight anisocoria, with the right pupil larger than the left, and diminished abdominal reflexes on the right. In the peripheral blood there were 4,680,000 red blood cells per cu. mm., 16,100 white blood cells per cu. mm., and a normal differential leukocytic count.
Ventriculograms were performed September 21, 1951. Twenty cubic centimeters of clear fluid under moderately increased pressure were replaced with air. Films revealed a slight shift of the entire ventricular system to the left. The right temporal horn was found to be markedly elevated, particularly in the posterior and me- dial portions.
Operation, September 21, 1951 (Henry G. Schwartz), consisted of right temporoparietal craniotomy. The surface of the temporal lobe appeared flattened and the sylvian fissure was displaced dorsally. A small core of cortex was excised from the middle temporal convolution. and, at a depth of approximately 2 cm., an area of very soft yellow tissue was encountered. Beyond this tissue was a grayish-yellow, oval- shaped tumor mass. The long axis of the tii- mor was directed medially. The tumor was well demarcated and was shelled out as a sin- gle mass. After removal of the tumor, the infe- rior wall of the defcct consisted of a contin- uous layer of white matter and cortex about 1 cni. in thickness.
The postoperative course of the patient was uneventful except for a mild left hemiparesis that gradually improved prior to discharge. Careful physical examinations for enlarged lymph nodes, liver, or spleen and re-examina- tion of his chest roentgenograms failed to re- veal any evidence of enlargement of lymph nodes or other evidence of systemic Hodgkin’s disease. The blood counts were 4,180,000 red blood cells per cu. mm. and 15,400 white blood cells per cu. mm., with a normal differential count. Although the tumor was completely re- moved, it was thought desirable to give a total
629

630 CANCER May-June 1955 Vol. 8
of 1500 r deep roentgen-ray therapy to the right temporal region, using a 10X10-cm. port a1 a distance of 50 cm. The factors were 200 kvp., 20 ma., with 0.5 mm. copper and 1 mm. aluminum filters.
At the time of his discharge on October 2, 1951, the patient was alert and oriented and had no demonstrable visual field defect. There was evidence of resolution of the papilledema.
The patient has been followed at regular in- tervals by his local physician and has returned here for periodic checkups. His blood pressure has ranged between 130 and 140 mm. of mer- cury systolic and 80 and 90 diastolic. Repeated hematological studies, as well as general and neurological examinations, have failed to re- veal evidence of systemic or locally recurrent Hodgkin’s disease to the date of the present writing, three years after operation.
PATHOLOGICAL FINDINGS
The tissue rcmoved at surgery weighed 9 gm. and consisted of a firm, smoothly locu- lated, 4X2.5XZ-cm., gray-yellow tumor and a
core of overlying white matter and cortex of about equal size. On cross section there was a central pale area that blended with the sur- rounding gray tissue.
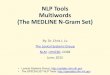
Micr.oscopic Findings. The tissue in micro- scopic sections (Fig. 1) was a pleomorphic mix- ture of cells in a network of small blood ves- sels with thick intima arid broad, loose, fibrous adventitia. The infiltrating cells were small lymphocytes, plasma cells, eosinophils, and large reticulum cells. The latter were dorni- nant throughout and contained a clear nu- cleus with one or two moderate-sized nucleoli and had clear cytoplasm. Among the cells of this type were many large forms with two to five overlapping and notched nuclei 01 the same composition as those of the niononuclear [orins (Fig. 2). These cells were Reed-Sternberg cells. In some parts of the tumor there were small foci of necrosis (Fig. 3). Mitotic figures were present but infrequent, and no sarcoma- tous tissue could be identified. Occasional neu- rons were included in the peripheral portions
FIG. 1. A section of the well-delimited tumor from the right temporal lobe, showing its pleo- morphic cellular composition with reticulum cells, lymphocytes, fibroblasts, and plasma cells. (H. Pe E. X469.)

No. I PRIMARY INTRACEREBRAL HODGKIN’S DISEASE - Schricker Q Smith 63 1
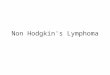
FIG. 2. Fibrosis and pleomorphic cellular content including multinuclcatcd giant cells in the intracerchral tumor. (X266.) Inset: A multiriucleated giant cell with vesicular overlapping nuclei, prominent nucleoli, and heavy nuclear membrane typical of the Reed-Sternberg cell of Hodgkin’s disease. (H. 8c E. X873.)
of the tumor, but the borders of the tumorous tissue were fairly sharply delimited. Vessels in the cerebral substance about the tumor showed dense cuffs of lymphocytic infiltration.
PATHOLOGICAL DIAGNOSIS. The tissue was con- sidered typical of nonsarcomatous Hodgkin’s disease and was comparable in histological ap- pearance to Hodgkin’s tissue as seen in lymph nodes or spleen.
DISCUSSION This case is principally significant in that it
represents the primarily intracerebral occur- rence of the less malignant or granulomatous form of Hodgkin’s disease in contrast to the rare but previously reported examples ol the similar occurrence of Hodgkin’s sarcoma. The histological sections are considered typical 01 Hodgkin’s disease and the clinical course sub- sequent to operation has confirmed both i ts less malignant character and the primary in- tracerebral localization of all recognized mani-
festations of the disease. Even if later systemic lesions should be detected, their discovery will have been antedated three years by the re- moval of the cerebral tumor. From experience with localized Hodgkin’s disease in lymph nodes, the possibility of recurrence of the dis- ease at other sites years after elimination o f the first lesion can not be excluded.
The lesions of Hodgkin’s disease have been variously classified. There is general agreeinen t of its division into a sarconiatous form that closely resembles reticulum-cell sarcoma and a nonsarcomatous or granuloiiiatous type. The latter category has been subdivided7 into Hodgkin’s granuloma and Hodgkin’s para- granuloma and this classification has been used12 in reporting manifestations of the dis- ease in the central nervous system. Sparling, Adams, and Parker state that there are no known cases of involvement ol the central ner- vous system by what they recogni~e as Hodg- kin’s paragranuloma.

632 CANCER May-June 1955 Vol. 8
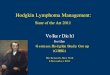
FIG. 3. An area of necrosis in the tumor, illustrating another typical appearance of Hodgkin’s disease. (H. & E. X266.)
The lesion in the present case has the histo- logical characteristics that would apparently satisfy the criteria of Hodgkin’s granuloma in the classification of Sparling, Adams, and Parker. Most of the reports of Hodgkin’s gran- uloma of the central nervous system are con- cerned with neurological involvement second- ary to invasion or compression by epidural lymphogranulomatous tissue arising either from bone lesions of the skull6 or vertebra or from the intracraniall? 9 or intraspinal dura.14 Direct invasion of the spinal canal by granulo- matous tissue may produce mechanical ob- struction and compression of the intrinsic ves- sels of the cord with subsequent anoxic changes.6115 The occurrence of isolated masses within the substance of the brain in associa- tion with lesions in other viscera is much less frequent, but examples such as the case re- ported by von Hecker and Fischer have been described.
I t is significant in the case reported here that the surface of the tumor was found to extend nowhere closer than 1 cm. to the dura and that
evidence of dural reaction could not be dem- ons trated.
Hodgkin’s sarcoma is the most rapidly grow- ing and highly malignant form ok the disease and is thought to arise either primarily or from a pre-existing granulomatous lesion. I t may have a fulminating onset and be rap- idly progressive. Secondary intracranial lesions have been described arising from h i in the tonsils, orbit, and retroperitoneal lymph nodes by Jackson and Parker.6 These authors report some type of involvement of the central nerv- ous system in 16 per cent of the autopsied cases of Hodgkin’s sarcoma, all of which also had widespread involvement of other organs.
While lymphoid tissue is not a normal con- stituent of the brain or spinal cord, other mes- senchymal elements of the reticulo-endothelial system are present that may be the site of origin of primary Hodgkin’s disease of the central nervous system. Ramdn y Cajal and others10 suspected the existence of mesenchymal cells differing from the types of neuroglia recog- nized at that time, and Del Rio-Hortega first

No. 3 PRIMAKY INIXACEREYRAL HODGKIN’S DISEASE . Sckricker Q S m i t h
conclusively demonstrated the existence of mi- croglial cells as mesenchymal intracerebral rep- resentatives of the reticulo-endothelial system. He demonstrated the similarity of these cells to macrophages in their morphology, staining reactions, and property of phagocytosis. Dun- ning and Furth found that microglia and his- tiocytes were morphologically and function- ally identical and constituted progressive steps in the maturation of a single more-primitive cell type. At present it is felt that a primitive reticulum cell gives rise to histiocytes that in turn may mature to form either reticulum cells or microglia. Hodgkin’s disease could there- fore develop intracerebrally from histiocytes of the leptomeninges or the adventitia of the intracer ebral blood vessels,* or from microglia in the white and gray matter.394
SUMMARY
ti33
1. X case is presented of Hodgkin’s granu- loma of the right temporal lobe of the brain, with primary intracerebral manifestations and no recognized involvement of any of the other organs.
2. The tumor was removed and local radia- tion therapy was given. The patient has shown no signs of recurrence after three years.
3. Histologically the tumor had all the char- acteristics of nonsarcomatous Hodgkin’s gran- uloma.
4. The tumor arose in and was confined to the white matter of the right temporal lobe. Microglial cells or perivascular histiocytes are considered as probable sources for the develop- ment of this lesion.
REFERENCES
1. ABBOTT, K. H., and ADSON, A. W.: Primary intra- cranial lymphosarconia; a report of two cases and re- view of literature. Arch. Surg. 47: 147-159, 1943. 2. BERKMAN, J.; NETSKY, M. C., and ZIMMERMAN,
€I. M.: Malignant lymphomas within the central nerv- ous system. [.4bstr.] 1. Neuropath. 6 Exper. Neurol. 10: 100-101; disc. 101-102, 1951.
3. DUNNING, H. S., and FURTH, J.: Studies on the re- lation between microglia, histiocytes and monocytes.
4. GINSBURG, S.: Hodgkin’s disease; with predominant localization in the nervous system: early diagnosis and radiotherapy. Arch. Int . Med. 39: 571-595, 1927.
5. HECH~R, H. v., and FIXHER, W.: Zur Kenntnis der Lymphogranuloinatose. Deutsche med. Wchnschr. 48: 482-484, 1922.
6. JACKSON, H., JR., and PARKFR, F., JR.: Hodgkin’s disease. V. Involvement of certain other organs. New England J. M e d . 233: 369-376, 1945.
7. JACKSON, If., JR., and PARKER, F, JR.: Hodgkin’s Disease and Allied Disorders. New York. Oxford Uni- versity Press. 1947.
8. KINNEY, T. D., and ADAILIS, R. D.: Reticulum cell sarcoma of the brain. Arch. Neurol. & Psychiat. 50:
Am. J . Path. 11: 895-914, P1. 118-120, 1935.
552-564, 1943.
9. MARTIN, H. E., and COURVILLE, C. B.: Hodgkin’s disease with involvement of the cranial dura mater. Bull. Los Angeles Neurol. SOC. 1: 145-148, 1936.
10. RAMON Y CAJAL, S.: Contribucibn a1 conocimien- to de la neuroglia del cerebro humano. Trab. Inst. Cajal d‘invest. biol. 11: 254-315, 1913. Cited by Del Rio- Hortega.
11. RIO-HORTEGA, P. DEL: Microglia. In PENFIELD, W., Ed: Cytology & Cellular Pathology of the Nervous Sys- tem. New York. Paul B. Hoeber, Inc. 1932; Vol. 11, pp. 481-534.
12. SPARLING, H. J., JR., and ADAMS, R. D.: Primary Hodgkin’s sarcoma of the brain. Arch. Path. 42: 338- 344, 1946.
13. SPARLING, H. J., JR.; ADAMS, R. D., and PARKER, F., JR.: Involvement of Lhe nervous system by malignant lymphoma. Medicine 26: 285-332, 1947.
14. WEIL, A.: Spinal cord changes in lymphogranulo- matosis. Arch. h’eurol. 6 Psychiat. 26: 1009-1025; disc. 1026, 1931.
15. WISKELMAN, N. W., and MOORE, M. T.: Lymph0 rrranulomatosis IHod&in’s disease) of the nervous svs- reem. Arch. Neu&l. g p s y c h i a t . 41;: 304-317; disc. 3i7- 318, 1941.