Embed Size (px)
Citation preview

J. clin. Path. (1961), 14, 219.
A clinicopathological study ofbenign Hodgkin's diseaseP. J. DAWSON1 AND C. V. HARRISON
From the Department ofPathology, Postgraduate Medical School, Ducane Road, London
SYNOPSIS A series of 44 cases of benign Hodgkin's disease is reported. The condition occurs mostcommonly between the ages of 15 and 35 years and affects men more often than women. Thepresenting symptom is painless lymphadenopathy, frequently in the neck, and often confined to a
single group of nodes. The histological features are the presence of Sternberg-Reed cells in a back-ground of mature lymphocytes intermingled with a small number of reticulum cells. Mitoticfigures are usually present only in the Sternberg-Reed cells. The prognosis is good; 93 % of cases
survive five years and 85% 10 years. About one-quarter of the cases show transition to classicalHodgkin's disease after a period of five or more years and die with widely disseminated Hodgkin'sdisease. Biopsy-excision followed by radiotherapy is the treatment of choice.
In 1952 one of us reported six cases of benignHodgkin's disease (Harrison, 1952). We believed thatit was a recognizable histological entity but were thenuncertain as to its behaviour. In particular, we didnot know to what extent the ultimate prognosis wasbetter than that of classical Hodgkin's disease,especially if the latter was seen and treated in anearly stage. Since 1952 we have had the opportunityof studying a considerable number of cases, largelythanks to the kindness of our colleagues. In thepresent paper we have attempted to define thehistological features more closely and to determinewhether the separation of this group is justified interms of ultimate prognosis.
NOMENCLATURE
Jackson and Parker (1944), who first described thecondition, called it 'Hodgkin's paragranuloma';Robb-Smith (1947) described an apparently similarcondition under the name of 'lympho-reticularmedullary reticulosis'. Lumb (1954) has used the title'reticular lymphoma' and Symmers (1958) hassuggested 'indolent Hodgkin's disease'. In the presentpaper we propose to use the name 'benign Hodgkin'sdisease' which we coined in our earlier work. (Theterm 'classical Hodgkin's disease' will be used forpurposes of clarity for the widely recognized and
Received for publication December 1960
'Present address: Department of Pathology, University of CaliforniaMedical Center, San Francisco 22, California, U.S.A.
more usual form of the disease which some callHodgkin's granuloma.)
LITERATURE
Rosenthal (1936) first presented a histologicalclassification of Hodgkin's disease based on theproportion of lymphocytes to reticulum cells. Hefound that a higher proportion of lymphocytescorrelated with a longer survival. Jackson (1937,1939) and Jackson and Parker (1944, 1947) firstdefined the condition which they called para-granuloma and showed that the prognosis wasclearly better than that of ordinary Hodgkin'sdisease. Since then, various workers have describedseries of similar cases (Robb-Smith, 1947; Wright,1956, 1960; Bonenfant, 1954; Lumb, 1954; Traut-mann, 1954, 1959; Marshall, 1956; Symmers, 1958).There is general agreement on the broad definitionof the histology and on the improved prognosis. Inspite of this, the actual cases remain difficult diag-nostic problems. We hope to be able to define thediagnostic criteria a little more closely and to showthat the prognosis is so strikingly better that anaccurate diagnosis is of great clinical importance.
MATERIAL
We have collected all the examples of possiblebenign Hodgkin's disease, both from our ownhospital and from cases sent in by our colleagues.These were examined without any knowledge of the
219
on May 31, 2022 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.14.3.219 on 1 May 1961. D
ownloaded from

P. J. Dawson and C. V. Harrison
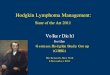
-I = DIEDo BIOPSY/EXCISION SHOWING BENIGN HODGKINS DISEASE* - BIOPSY/EXCISION SHOWING CLASSICAL HODGKINS DISEASE0 - DEEP X-RAY THERAPY
* = CHEMOTHERAPY
_ _8 _ _ _ _
7 81i 2 21 2.2225 24 25
ii-[I-1-1---1-1-1-l-l-l-- 1
2627 2829 30 3132 34 3536 37 M 3940 4142 43 44
C A S E S
FIG. 1. Histogram summarizing the duration, forms of therapy, recurrences, andfollow-up in all 44 patients.
clinical course. Forty-five cases were found which,on purely histological grounds, we considered to beexamples of benign Hodgkin's disease and a follow-up was obtained on these. This was successful in allcases except one, although we have good reason forbelieving the patient to be alive seven years after theonset of the disease. Because of the long course ofthe disease, there seemed little point in consideringcases of very recent onset, so that patients who hadsuffered from the disease for less than three yearswere excluded.There were then 44 cases of benign Hodgkin's
disease selected on morphological grounds with aminimum follow-up period of three years; in fact,all were followed for four years or longer. Fifty-sixbiopsies from these cases were available for study.Multiple biopsies were available in 10 patients;five of these showed transition to classical Hodgkin'sdisease. One further biopsy also showed benignHodgkin's disease, but was too poor technically fordetailed study. We were unable to obtain the firstbiopsy in Case 7; it was reported elsewhere as
Hodgkin's disease and because the second biopsyshowed typical benign Hodgkin's disease we havepresumed that the first was similar and, althoughmarked on Fig. 1, it is not, of course, included in our
analysis. A further four biopsies showed normal
lymphoid tissue only and are not shown in Fig. 1.The cases are numbered and successive biopsies ofthe same patient designated by the letters A, B, andC.Because of the rarity of the condition and because
many of our cases were sent to us for an opinion byother pathologists, only paraffin-blocked materialwas available, and in some cases only a singlehaematoxylin-and-eosin-stained section was obtain-able. Silver-impregnated reticulin preparations were
made wherever possible and a few other specialstains, notably methyl violet for amyloid, were usedto clarify specific points. All histological examina-tions were made without knowledge of the subse-quent course of the patient.
In order to clarify the boundary between benignand classical Hodgkin's disease a control series of43 biopsies from 42 consecutive cases of classicalHodgkin's disease seen in the department from 1950to 1955 were also studied.
CLINICAL FEATURES
Details of the presenting features are summarizedin Table I. The age of onset varied from 6 to 70
272625242322
a 21- 203 19o 18-_ 17- 16o 15- 14
13Ln 12
I?110
w 9
>.8765432
iLj.
6 l0 II 12 13 14u5fv v v v v sxa%Jn%x I * *I y y v v I *I I v
220
4
on May 31, 2022 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.14.3.219 on 1 May 1961. D
ownloaded from

A clinicopathological study of benign Hodgkin's disease
TABLE I
CLINICAL DETAILS
Sex Sites of Disease when First Seen
M
FM
M
M
FFM
M
M
M
'MM
M
F
F
M
M
F
M
M
M
M
M
M
M
M
M
M
M
M
F
M
M
M
F
F
F
F
M
M
F
Neck (R), axillae, groin (L)Neck (L), neck (R)Axillae, groinsNeck (R)NeckNec.k (L)Neck (L)Neck (R)Neck (R)Neck (bilateral), axillaeNeck (L), axillaeNeck (L)Axilla (R)Neck (R)Neck (L)MediastinuiNeckNeckNeck (L), mediastinumNeck (L)Neck (L), groin (R)AxillaeAxilla (R!Neck (R)NeckNeck (R)Neck (R)Neck (L)Neck (L)Neck (R)Neck (L)Neck (L)Neck, neck (L)Axillae, spleenNeckNeck (R), mediastinumAxillaeNeck (L)Groin (R)Neck (L)Neck (R)Axilla (R)Groin (L)Neck (R)
years; in 31 cases the disease began between theages of 15 and 35 years. Thirty-one cases occurredin men and 13 in women, giving a sex ratio of 2-4to 1. In all cases where the patient complained ofsymptoms relevant to the disease the presentingcomplaint was painless enlargement of lymph nodes,and in 36 of the 44 cases these were situated in theneck. The cases were staged when first seen usingthe criteria similar to those of Peters and Middlemiss(1958), except that stage 1I was not subdivided.
Thirty-four cases belonged to stage I, that is tosay, had lymph node involvement confined to onegroup of nodes, six cases belonged to stage II, andfour to stage III. Pain was not a feature. Constitu-tional symptoms were present in two cases in stage Iand in one case in stage II. In one patient the spleenwas enlarged when she was first seen; the liver was
only noted to be enlarged in the terminal stages of
the disease. One patient developed a swelling in onebuttock which responded to radiotherapy; unfor-tunately, it was not biopsied. In one case enlargedtonsils were removed; histologically they are said tohave shown the typical appearances of benignHodgkin's disease. Unfortunately, the sections arenot now available.The interval between the onset of symptoms (or
signs) and the diagnostic biopsy varied from twoweeks to nine years. In six cases the duration ofsymptoms before biopsy was not recorded, or thelymphadenopathy was an incidental finding inpatients attending for other reasons. These casesare recorded as having a biopsy in the first year.In 28 of the remaining 38 cases the interval betweenthe onset of symptoms and biopsy was one year orless, in five cases it was two years, in three cases itwas three years, and in the other two cases sevenand nine years respectively. These intervals are wellsubstantiated and in the nine-year interval is sup-ported by indisputable radiological evidence.Because of this, the duration of the disease has beenmeasured from the first definite lymph node enlarge-ment; in all cases a positive biopsy has subsequentlybeen obtained from the group of nodes first en-larged.
PATHOLOGY
The affected lymph nodes varied in size between3 and 50 mm. in diameter, but the majority werebetween 10 and 30 mm. in diameter. The nodeswere discrete and firm, but not hard. Individualnodes were bound together by loose connectivetissue; their cut surfaces were smooth, homogeneous,and pale pink or light grey. These appearances arenot distinctive and the condition cannot be dis-tinguished from other tumours of lymphoid tissue bynaked-eye examination alone.
Partial involvement of affected nodes was sur-prisingly common, occurring in 16 of 51 biopsies.The uninvolved part of the node was usually smalland usually amounted to several follicles survivingnear the periphery (Figs. 2, 3, and 4). However, infive biopsies7 a substantial part of the node (anestimated 20%) retained its normal structure.
Silver-impregnated preparations were availablein 41 of 51 biopsies and in our experience were ofconsiderable diagnostic value. They always showedthat the normal reticulin pattern in the affected partof the node was completely lost, and incidentallyshowed up by contrast the frequent presence ofsmall unaffected portions. In the affected part thenormal reticulin pattern was replaced by one ofthree abnormal patterns. In 13 biopsies there was adelicate, sometimes incomplete, meshwork of fine
No. ofCase
234567891011121314151617181920212223242526272829303132333435363738394041424344
Age atOnset
2457191215311812331622213396
232029301547182958212528202334836307050171726162238302551
221
on May 31, 2022 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.14.3.219 on 1 May 1961. D
ownloaded from

P. J. Dawson and C. V. Harrison
FIG. 3. Biopsy 14A showing fine reticulin network in themiddle of the node and survival of normal reticulin patternat the two ends. (Silver impregnation x 5-0.)
FIG. 2. Biopsy 8A from a case of benign Hodgkin'sdisease showing incomplete involvement of the node.(Note surviving follicle under capsule at bottom left.)(Haematoxylin and eosin x 100.)
FIG. 4. Biopsy 12B showing lobulation bv reticulin. (Note survivingnormal structure in middle by upper border.) (Silver impregnation x 5 2.)
222
on May 31, 2022 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.14.3.219 on 1 May 1961. D
ownloaded from

A clinicopathological study of benign Hodgkin's disease
FIG. 5. Biopsy 43A showing a folliculat pattern. (Silverimpregnation x 5-2.)
FIG. 6. Biopsy 32A from a case of benign Hodgkin'sdisease, showing the general appearance of massedlymphocytes with a few giant cells. (Haematoxylin andeosin x 100.)
FIG. 7. Same case as Fig. 6, but at a higher magnificationshowing lymphocytes and giant cells. (Note mitosis in aSternberg-Reed cell near bottom margin.) (Haematoxylinand eosin x 380.)
223
on May 31, 2022 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.14.3.219 on 1 May 1961. D
ownloaded from

P. J. Dawson and C. V. Harrison
fibrils, usually less dense than that of a normal node(Fig. 3). In 16 biopsies a similar delicate meshworkwas divided into lobules of variable size by denserbands of reticulin fibrils (Fig. 4). In 10 biopsiesthere was a pattern not unlike that of giant follicularlymphoma. Here the tissue was divided into a seriesof uniform rounded masses 2 to 4 mm. diameter byreticulin bands with very sparse fibrils within the'follicles' (Fig. 5). A heavy increase of reticulin wasunusual and collagenous bands were seen in onlytwo biopsies. Generally the density of the reticulinwas considerably less than in ordinary Hodgkin'sdisease. In many nodes, including those that appearedto be totally involved, part of the peripheral sinuscould still be made out. In ordinary stained sectionslymphocytes comprised the majority of the cells inthe affected nodes (Figs. 6 and 7). They were mor-phologically indistinguishable from the small lym-phocytes seen in normal nodes and did not showmitotic figures. The reticulum cells, which lay freein the pulp among the lymphocytes, were in theminority. They averaged about 10t in diameter andhad a poorly outlined pink cytoplasm. The nucleus,which occupied most of the cell, had a sharplydrawn nuclear membrane, a finely dotted chromatinnet and, sometimes, a small dark nucleolus. Mitoseswere not commonly seen in these cells and were onlypresent in any number in eight biopsies from sevencases. In one of these cases we have histologicalevidence of transition to classical Hodgkin's disease,and a further three died with a clinical diagnosis ofgeneralized Hodgkin's disease. In seven biopsiessarcoid-like aggregates of histiocytes were observed.These cells were larger than those just described,witha smaller nucleus and a brightly eosinophilic cyto-plasm. Of these seven cases two showed histological-ly transition to classical Hodgkin's disease and fourdied, three of generalized Hodgkin's disease.The relative number of lymphocytes and reticulum
cells was found to be of the greatest importance.These were estimated and expressed as a percentageof the total of both types of cell. In 50 biopsies, 80%or more of the cells were lymphocytes and 20% orless reticulum cells. In the remaining biopsy thepercentages were 75 and 25 respectively. In 36biopsies, 90% or more of the background cells werelymphocytes (Fig. 6).
Steinberg-Reed cells were present in all biopsiesand were regarded as essential to the diagnosis.They varied in size from 15, to 45,u in diameter,but the majority lay within the range 15u to 25,u.Transitions between reticulum cells and Stemnberg-Reed cells could be observed fairly readily and forthis reason a minimum diameter of 15,L was acceptedfor the latter (Smetana and Cohen, 1956). Theircytoplasm was poorly outlined, pale pink, and granu-
lar, but often vacuolated so that all that could beseen was a halo around the nucleus. The nucleuswas big in relation to the size of the cell. Sometimesit appeared single and round, sometimes it wasfolded or lobed and sometimes there appeared tobe two or more round, discrete nuclei. The nuclearmembrane was finely drawn, with a few chromatindots upon it. A striking feature was the presence ofone or two large eosinophilic nucleoli measuringfrom l,u to 4,u in diameter. Mitoses, both normaland abnormal, were a constant feature of theSteinberg-Reed cells and in only one case werethey difficult to find. On average, nearly 3 % of allSteinberg-Reed cells were in mitrosis (Fig. 7).There was no apparent correlation between thenumber of mitoses and the liability to transition toclassical Hodgkin's disease. The number ofSteinberg-Reed cells present varied widely bothfrom node to node and in different parts of the samesection. Estimated on a one to four plus system theirdistribution was: one plus in 14 biopsies, two plusin 22 biopsies, and three plus in 15 biopsies. In noinstance were very large numbers of Steinberg-Reed cells seen. In 32 biopsies they were scatteredsingly through the lymphocytic background, in 18biopsies they were aggregated to form small looseclusters, and in one biopsy they formed largeclusters.
Eosinophils were present in small numbers inseven biopsies, but never in the large numberiobserved in some cases of classical Hodgkin'sdisease. Neutrophil polymorphs were present on onebiopsy, and small numbers of plasma cells in four.Amyloid, staining metachromatically with methyl
violet, was present in one biopsy and paramyloid in21.
Caseation and necrosis were not seen, save in onebiopsy where there were a few microscopic areas ofnecrosis. Capsular invasion was not seen.
DIAGNOSTIC CRITERIA
In our experience the following criteria need to befulfilled before a diagnosis of benign Hodgkin'sdisease can be made. The normal architecturalpattern of the node in a reticulin preparation mustbe destroyed in the affected part, and should bereplaced by one of the three patterns describedabove. Steinberg-Reed giant cells must be present.At least 80% of the cells must be small lymphocytesand mitoses in these cells should be absent or rare.Eosinophils should be scanty or absent.
DIFFERENTIAL DIAGNOSIS
Three other malignant lymphomas cause diagnostic
224
on May 31, 2022 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.14.3.219 on 1 May 1961. D
ownloaded from

A clinicopathological study of benign Hodgkin's disease
difficulty: lymphosarcoma, giant follicular lym-phoma, and classical Hodgkin's disease.
In lymphosarcoma the reticulin pattern shows aloose meshwork like that of one of the patterns inbenign Hodgkin's disease. The lymphocytes whichform the great majority of the cells show aniso-cytosis, nuclear variation, and mitotic figures.Small reticulum cells may sometimes be foundamongst the lymphocytes but these should not bemistaken for Steinberg-Reed giant cells which donot occur in lymphosarcoma. Capsular invasion iscommon, a feature which is not seen in benignHodgkin's disease.Giant follicular lymphoma can only be confused
with the type of benign Hodgkin's disease showingan apparent follicular pattern. Two criteria dif-ferentiate these: in giant follicular lymphoma therounded lesions are lymphoid follicles whereas inbenign Hodgkin's disease they are aggregations oflymphocytes without real follicular arrangement.In benign Hodgkin's disease Steinberg-Reed giantcells are present even if scanty: they are absent fromgiant follicular lymphoma. The differential diagnosisfrom classical Hodgkin's disease is less clear becausethe differences are quantitative rather than qualita-tive. In order to define the differences more closelywe compared our 44 cases of benign Hodgkin'sdisease with 43 cases of classical Hodgkin's disease.In the latter partial involvement of the node wasseen only five times. In silver-impregnated prepara-tions the normal architecture was always destroyedand was usually replaced by a tangled network offibres appreciably denser than in the benign form.The total density of the reticulin was excessive inabout two-thirds of cases of classical Hodgkin'sdisease but in the other third it was not appreciablydenser than in the benign form. In seven cases thereticulin showed a fine lobulation like that of onepattern of benign Hodgkin's disease and in anothereight there was a similar but much denser lobulationwith true collagen. In haemalum-and-eosin-stainedsections lymphocytes were always present and theywere not morphologically different from those ofbenign Hodgkin's disease nor did they show mitoticfigures. Reticulum cells were always present inmuch greater numbers than in benign Hodgkin'sdisease and generally they were larger and morepleomorphic. Mitoses could always be found inthem, though they were numerous in only one case.Sarcoid-like aggregates were seen in only five cases.A constant difference was seen in the proportion ofreticulum cells to lymphocytes. Whereas in benignHodgkin's disease reticulum cells did not exceed20%, they always exceeded 35% in the classicaldisease (Fig. 9). Steinberg-Reed giant cells werepresent by definition in both conditions but they
were generally more numerous in the classicaldisease. Using the same grading as we used inbenign Hodgkin's disease, we found 1 plus in onlyfive cases, 2 plus in 19, and 3 or 4 plus in the other19.In all cases mitoses were observed in the Sternberg-
Reed cells and on average they were present in 5 %.In 13 cases Stemnberg-Reed cells were present inlarge closely packed groups.
Eosinophils were present in 38 of 43 biopsies andin 29 of these they were present in moderate orlarge numbers. Neutrophil polymorphs were presentin 18 biopsies, in half of them in moderate or largenumbers, while plasma cells were present in 21biopsies, in seven in moderate or large numbers.Amyloid was not seen but paramyloid was pre-
sent in 19 biopsies. Caseation was not seen butnecrosis was present in nine biopsies and capsularinvasion was present in four.
It was originally felt that it might be necessaryto create an intermediate group of cases lying mid-way between benign and classical Hodgkin's disease.Initially, about eight cases fell into this group.Later, after the distinguishing criteria were betterestablished these were re-examined, when they allseemed to fall quite definitely either into the benignor classical group.
COURSE OF BENIGN HODGKIN'S DISEASE
This is summarized in Fig. 1. Characteristically it isslow, and after radiotherapy most patients enjoy along period of remission during which, althoughsmall shotty nodes may still be palpable at theoriginal site, they usually feel quite well. After avarying period many cases relapse. In our series, thelongest survival was 26 years from the onset of thedisease: another patient who died in the nineteenthyear of her illness never received any specific treat-ment and was only incapacitated by her illness in thelast year of her life. The shortest survival was of apatient who died after an illness lasting 15 months.She had widespread lymphadenopathy and apalpable spleen when first seen, so that there is somedoubt as to whether the biopsy was truly representa-tive. A total of nine out of our 44 patients havedied after periods lasting from 15 months to 19years, four after more than 10 years. In three of thepatients who died there was histological evidence oftransition to classical Hodgkin's disease, and thiswas suggested by the clinical course in another four.We have histological evidence of this transition intwo other patients, both of whom are alive and wellfive and 15 years later respectively (Figs. 8 and 9).The intervals between successive biopsies showingbenign and classical Hodgkin's disease in the cases
225
on May 31, 2022 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.14.3.219 on 1 May 1961. D
ownloaded from

P. J. Dawson and C. V. Harrison
FIG. 8. Biopsy 3A, the original biopsy from a case of FIG. 9. Biopsy 3B, six years after biopsy, 3A, now showingbenign Hodgkin's disease. classical Hodgkin's disease. The majority of the cells are(Haematoxylin and eosin x 380.) now reticulum cells and lymphoc.ytes are scanty.
in which transition occurred varied from four to 13years.
In the other two fatal cases post-mortem examina-tion revealed generalized amyloidosis, and in bothdeath was due to uraemia consequent upon renalvein thrombosis. In one case the benign Hodgkin'sdisease was confined to a single group of nodes in theneck. In the other there was no trace of Hodgkin'sdisease and, although the clinical course was punctu-ated by frequent recurrences, three biopsies takenover a period of nine years all showed benignHodgkin's disease. Intercurrent illnesses were notprominent in our series and none of the deathscould be ascribed to them apart from the abovecases of amyloid which were considered to besecondary to benign Hodgkin's disease.
Treatment was by local excision, radiotherapy, ornitrogen mustard, either singly or in combination.
Local excision was the only form of initial treatmentin 15 cases and in only one of these was a radicaldissection attempted. In 10 of these the diseaserecurred at the same site after intervals varying fromone to 13 years, and in one case residual enlargednodes have remained unchanged. The remainder arefree from recurrence, one, four, four, and 20 yearslater respectively.
Thirty-four patients received one or more coursesof radiotherapy; another patient also receivedradiotherapy but only after transition to classicalHodgkin's disease had occurred. Details of the doseand method are not generally available. A singlecourse of treatment was followed, in 24 patients, bya remission lasting from three to 10 years; only fiveof these have had recurrences. In five patientsseveral courses of treatment were required beforeremissions lasting from five to 22 years were induced.
226
on May 31, 2022 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.14.3.219 on 1 May 1961. D
ownloaded from

A clinicopathological study of benign Hodgkin's disease
In four cases the disease was never satisfactorilycontrolled and ran a relentless course with deathafter illness lasting from 15 months to 12 years. Theremaining patient has been observed for less thanone year since radiotherapy; he is free from recur-rence.Chemotherapy was only employed as the initial
treatment in two cases.The period of follow-up has varied from a mini-
mum of four years in all cases to a maximum of26 years. Of 41 patients followed for five years,three died, giving a crude five-year survival rate of93 %. Of 19 patients followed for 10 years, five died,giving a crude 10-year survival rate of 74%. A betterestimate of the survival rate is given by the lifetable (Table IL); calculated by this method, thefive-year survival rate is 93% (standard error= 3-8 %)and the 10-year survival rate is 85% (standarderror- 65 %).
DISCUSSION
INCIDENCE OF BENIGN HODGKIN'S DISEASE Becauseof the way in which the present series was collected,it was impossible to determine from our figures theincidence of benign Hodgkin's disease. Of 2,127cases of tumours of lymphoid tissue reported in theliterature (Jackson and Parker, 1947; Lumb, 1954;Symmers, 1958), 925 (44%) were examples ofHodgkin's disease. Of these 113 were cases ofbenign Hodgkin's disease. The incidence of benignHodgkin's disease is thus approximately 12% of allcases of Hodgkin's disease and 5% of all tumours oflymphoid tissue. Wright (1960) found that of 339cases of Hodgkin's disease 26 (8 %) were examples ofthe benign form.
CLINICAL FEATURES The published series of benignHodgkin's disease are summarized in Table III. The
TABLE IILIFE TABLE OF SURVIVAL RATES IN BENIGN HODGKIN'S DISEASE
Time No. of Casesin Alive atYears Beginning of
Each Year
No. of CasesAlive butFalling out ofFollow-up
No. of CasesDying inGiven Year
No. at Risk Probability of Probability ofin Given Year Dying in Given Surviving through
Year Given Year
1 44 0 0 44 0 1 1002 44 0 1 44 0-02273 0-97727 9773 43 0 0 43 0 1 9774 43 0 1 43 0-02326 0-97674 9555 42 3 1 405 0-02469 007531 93-16 38 8 0 34 0 1 93-17 30 4 0 28 0 1 93 18 26 3 1 24 5 0-04082 0-95918 89-39 22 2 1 21 0-04762 0-95238 85-010 19 5 0 16 5 0 1 85-0
TABLE IIISEX AND AGE INCIDENCE OF BENIGN HODGKIN'S DISEASE
Author(s) Decade
Ist 2nd 3rd 4th 5th 6th 7th 8th
Jackson and Parker (1947)1
Jelliffe and Thomson (1955)'
Wright (1956)2
Lumb and Newton (1957)2
Symmers (1958)'
Wright (1960)2
Totals
Present series'
M 30F 11M 6F 2
M 8F 2
M 33F 3
M 44F 7
M 21F 3
M 142F 28M 31F 13
2 5 5 6 1
- 2 _- _
3 3 _
- 6 15 5 3 4 3 -
1 8 19 12 5 3 3 -
- 2 11 2 7 2 - -
3 24 60 30 21 19 12 1
11 15 9 1 4 1
'Age at onset. 'Age at diagnosis.Lumb and Newton decades are from 0 to 10 years, 10 to 20 years, etc., whereas in the other series they are from 0 to 9 years, 10 to 19 years, etc.
3
227
Survival Rate(%)
on May 31, 2022 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.14.3.219 on 1 May 1961. D
ownloaded from

P. J. Dawson and C. V. Harrison
combined ratio men to women is 15-1 to 1 comparedwith that in the present series of 2-4 to 1, but someof the published series may be biased because of theauthors' connexions with the Armed Forces. Ourpresent figures correspond closely with those ofJackson and Parker, and with those for Hodgkin'sas a whole (1-8 to 1 in favour of males; collectedseries quoted by Hoster, Dratman, Craver, andRolnick, 1948). Benign Hodgkin's disease is rareunder the age of 10 years and has not been reportedunder the age of 5 years. It is most common betweenthe ages of 15 and 35 years.
SITE OF ONSET AND CLINICAL STAGE Approximatelythree-quarters of all the cases reported in the litera-ture initially involved only a single group of nodes,generally in the neck; our findings are similar. Theexistence of benign Hodgkin's disease outside lymphnodes is still uncertain. Jackson and Parker (1947),Marshall (1956) and Lumb and Newton (1957), allnoted occasional involvement of the spleen and bonemarrow clinically and Symmers (1958) stated thatleukaemia could occur. Wright (1960) observed atnecropsy infiltration of the liver and spleen bycollections of lymphocytes and Sternberg-Reed cells,although elsewhere in the body the picture was thatof classical Hodgkin's disease. In the present seriesthe disease appeared to have involved bone marrow,spleen, spine, breast, and soft tissues of the buttock.In none of these was the involvement confirmedhistologically, so that it is uncertain whether or nottransition to the classical form had occurred; in somecases it appeared likely that it had. Cases showingsplenomegaly or other evidence of spread beyondlymph nodes usually do badly.
Jackson and Parker (1947) state that constitutionalsymptoms do not occur. Three of our patients com-plained of weight loss and fever; in two of these thedisease was apparently confined to a single group ofnodes. One patient remained well for eight yearsfollowing radiotherapy before transition to classicalHodgkin's disease occurred, and one remained wellfor four years following her initial course of treat-ment, before developing enlarged lymph nodes in theabdomen. The remaining patient ran a progressivecourse, dying three years after the onset of thedisease. Four patients have been, or are, pregnant.Hartvigsen (1955) and Southam, Diamond, andCraver (1956) found that in patients with Hodgkin'sdisease who became pregnant the survival time wassignificantly reduced. Patients did badly particularlyif their pregnancy coincided with an active phase ofthe disease. All the pregnancies in our series occurredduring quiescent periods of the disease and, so far,no ill effects have been observed.Two of our patients died from amyloidosis
secondary to benign Hodgkin's disease. Castleman(1949) reports a similar case and Jackson and Parker(1947) report a case in which a transition from benignto classical Hodgkin's disease had occurred. Theassociation of amyloidosis with classical Hodgkin'sdisease is fairly well recognized, although the numberof cases in the literature is only 63 (Dawson, 1960).
HISTOPATHOLOGICAL FEATURES While broadly fol-lowing the description of Jackson and Parker (1947),subsequent descriptions (Harrison, 1952; Lumb,1954; Smetana and Cohen, 1956; Wright, 1956;Lumb and Newton, 1957; Symmers, 1958; Pitcock,Bauer, and McGavran, 1959; Wright, 1960) havediffered in detail and emphasis, and new facts haveemerged.
Partial involvement of affected lymph nodes wasfirst described by Jackson and Parker and stressedby Harrison, although Wright and Symmers believeit to be infrequent. The present series has shown itto be surprisingly frequent and the retention of afew surviving follicles to one side of the node in noway militates against the diagnosis.The reticulin pattern varies widely. Harrison first
drew attention to the reticulin and collagenouslobulation, an observation since confirmed by Lumband Wright as well as by the present findings.Rappaport, Winter, and Hicks (1956) described afollicular lymphoma of Hodgkin's type of whichthey wrote 'were the background not follicular ornodular, one would not hesitate to classify most ofthese as Hodgkin's paragranuloma'. These authorsshowed that the presence of a follicular pattern inany type of tumour of lymphoid tissue was associatedwith an improved diagnosis. In our series, a finenetwork with or without superadded lobular andfollicular pattern was observed. There is thus nosingle characteristic reticulin pattern in this disease,although a gross increase in the amount of reticulinis against the diagnosis and in favour of classicalHodgkin's disease.
All authors stress that the bulk of the node iscomposed of small mature lymphocytes, whichcannot be distinguished morphologically from thoseseen in normal nodes. Mitotic figures are not seenin these cells. The importance of the number oflymphocytes was first realized by Rosenthal (1936)and was the basis of his attempt to correlate histo-logical appearances and prognosis; this has recentlybeen emphasized by Pitcock et al. (1959), who statethat 'the length of survival correlated at the 5%level of probability with the amount of lymphoidbackground'. As a result of the present study, it isnow possible to lay down a lower limit of 75% forthe lymphocytes in the background. In most nodesthey will total 90% or more of the background cells.
228
on May 31, 2022 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.14.3.219 on 1 May 1961. D
ownloaded from

A clinicopathological study of benign Hodgkin's disease
Jackson and Parker stated that reticulum cellswere present in varying numbers. Harrison com-mented on their virtual absence and Lumb thoughtthat an increase in proliferating reticulum cells wasassociated with a liability to malignant change.The present study has shown that the number ofreticulum cells is inversely proportional to thenumber of lymphocytes and is usually less than 10%of the total background cells. A percentage greaterthan 25%, to our mind, precludes a diagnosis ofbenign Hodgkin's disease. The presence of mitoticfigures in these cells has been shown to be of badprognostic significance, and indeed we pay moreattention to the number of reticulum cells and thepresence of mitoses in them than to the lymphocytes.Sarcoid-like lesions have been reported in classicalHodgkin's disease by Smetana and Cohen (1956)and in benign Hodgkin's disease by Jackson andParker (1947). These lesions were observed in sevenbiopsies in the present series and appear to beassociated with a poor prognosis, although this wasnot the experience of Smetana and Cohen. Sternberg-Reed cells are considered by all authors to beessential for the diagnosis of benign Hodgkin'sdisease, although Wright (1960) calls them 'reticulumcells'. They vary widely in number and are indis-tinguishable from those found in other forms ofHodgkin's disease. Lumb makes the reservation thatgiant forms are not common and Symmers thinksthat the presence of bizarre forms forebodestransition to the classical form. On the whole theyare present in small or moderate numbers only andare characteristically scattered singly or in looseclusters through the predominantly lymphocyticbackground. Harrison first drew attention to theconstancy of mitotic figures in these cells, and nearly3% of all Sternberg-Reed cells observed in thepresent series were in mitosis. Both normal andabnormal mitotic figures were observed. There is nodirect correlation between mitotic activity andprognosis.
Jackson and Parker observed small numbers ofeosinophils and plasma cells, a feature confirmed bylater authors and ourselves. Caseation, necrosis, andcapsular invasion do not occur. Paramyloid was afrequent finding in the present study.
Transition from benign to classical or sarcomatousHodgkin's disease has been observed by mostauthors (Jackson and Parker, 1947; Custer andBernhard, 1948; Lumb and Newton, 1957; Symmers,1958; Wright, 1960), although the frequency withwhich this occurred has varied from series to series.Jackson and Parker estimated the frequency atabout 20%, and 10 of Lumb and Newton's 36 casesunderwent this change. We were able to confirmthis transition histologically in five cases, and its
occurrence was suggested by the clinical course in afurther four. Although Smetana and Cohen (1956)felt that this transition was more apparent than realand was due at least in part to misdiagnosis ofthe original biopsy, it now seems established as adefinite occurrence in perhaps 25% of cases, and asthe major cause of death. We believe that thischange represents a phase in the natural history ofthe disease and is evidence for a close aetiologicalrelationship between the two forms. It is impossiblewith the present state of knowledge to predict whichcases will undergo this transition, but in ourexperience the presence of mitotic figures in reticulumcells and sarcoid-like areas are associated with arelatively poor prognosis. In most cases transitionoccurs between the fifth and fifteenth year of thedisease, although Jackson and Parker (1947)describe a case in which it occurred in the twenty-fourth year.
SURVIVAL RATES IN BENIGN HODGKIN S DISEASE Thecomparative survival rates reported in the literaturefor the various types of Hodgkin's disease are givenin Table IV. There seems some doubt as to the
TABLE IVFIVE-YEAR SURVIVAL RATES AND HISTOLOGICAL
CLASSIFICATION IN HODGKIN'S DISEASE
A uthor(s) Classification No. No. ofif CasesCases Surviving at
Five-yearFollow-up
Jackson and Parker(1947)'
Peters (1950)'
Jelliffe and Thomson(1955)1
Smetana and Cohen(1956)2
Lumb and Newton(1957)'Wright (1960)2
ParagranulomaGranulomaSarcoma
EarlyClassicalLateAtypicalGrade IGrade IIGrade III
ParagranulomaGranulomaSarcomaReticular lymphomaHodgkin's diseaseParagranulomaOrdinary Hodgkin'sHodgkin's sarcoma
281363220492420S
15610
35308
52919419
15710
15 (55',)18 (13%)Nil15 (75'%)25 (57%)11 (50%)5 (25 %)5 (100%)
45 (29%)Nil
(77% net)(28% net)Nil27 (93 %)67 (35 %)18 (95%)43 (27%)1 (10%)
'Survival period calculated from onset of symptoms2Survival period calculated from biopsy or treatment
diagnosis in Hall and Olson's (1956) small series offive cases so these are excluded. From these figuresit is readily apparent that these results are muchbetter than the figures generally reported forHodgkin's disease.
229
on May 31, 2022 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.14.3.219 on 1 May 1961. D
ownloaded from

P. J. Dawson and C. V. Harrison
This difference becomes much more significant ifthe 10-year survival rates of benign and classicalHodgkin's disease are compared. Twenty-one of thecases reported by Jackson and Parker (1947) werefollowed for 10 years; 10 (48%) were alive at theend of this time. Smetana and Cohen (1956) re-ported a 55% 10-year survival rate. Wright (1956)followed five cases for 10 years with no deaths; butin a later series (1960) of 11 cases followed for thesame period three died. Fourteen of 19 of our casesfollowed for 10 years survived this period. Theseresults are very different from those quoted forHodgkin's disease as a whole (see Table V) which
TABLE V10-YEAR SURVIVAL IN HODGKIN'S DISEASE
Author(s)
Unselected for histological typeUddstromer (1934)Slaughter and Craver (1942)Merner and Stenstrom (1947)Healy, Amory, and Friedman (1955)Peters and Middlemiss (1958)
Excluding cases of benign Hodgkin's diseaseJackson and Parker (1947)Lumb (1954)
No. of Cases at10-year Follow-up
494 (Nil)265 (3 %)185 (8%)216 (6%)139 (29%)
136 (1%.)123 (2%)
vary between nil and 29 %. In the series of Jacksonand Parker, and of Lumb, where cases of benignHodgkin's disease are excluded, only one of 136 andtwo of 123 cases respectively survived 10 years.The results of Peters and Middlemiss (1958) are
much better than average and must be attributed toa better technique of treatment. It is their practiceto irradiate prophylactically the lymph node regionsadjacent to those actually affected. In the presentseries treatment was undertaken at many centres sothat the results cannot be a reflection of a singletechnical advance in radiotherapy.
It is, however, difficult in a disease with such aslow remittent course to assess accurately the effectof treatment in the individual case. The strikingdifference in the recurrence rates after surgery alone,and after radiotherapy, observed by both Wrightand ourselves suggests that radiotherapy does infact influence the course of the disease. For thisreason we advise biopsy-excision followed byradiotherapy.
Peters (1950) first showed a correlation inHodgkin's disease between the extent of the diseasewhen the patient was first seen and the survival rate.Because of the frequency with which benignHodgkin's disease is initially localized to a singlegroup of nodes, it has been suggested that theimproved prognosis is merely a reflection of thelocalization of the disease. If the present series is
combined with that of Wright (1956) and the otherslisted in Table IV, a total of 151 cases is obtained;of these 127 survived five years. This gives a crudefive-year survival rate of 84%. Two hundred andfifty-nine cases of Hodgkin's disease, clinicallylocalized to a single lymphatic region, mostlyunselected for histological type, are listed in TableVI. (Lumb and Newton exclude cases of what they
TABLE VIFIVE-YEAR SURVIVAL IN HODGKIN'S DISEASE
ACCORDING TO CLINICAL STAGE
Author(s) Clinical No. ofStage Cases
Jelliffe and Thomson (1955) 1IIIII
Sellers (1957)
Lumb and Newton (1957)
Peters and Middlemiss (1958)
IIIII
IIIIIIIIIII
324792100141174676760607091
Five-yearSurvival:No. of Cases
19 (59%.)28 (60%)3 (3%)
57 (57 Y.)49 (35 %)20 (12%)35 (52%)27 (40%)5 (7%.)
43 (71%)39 (56%)14 (15%Y,)
call 'reticular lymphoma'.) Of these, 154 survivedfive years, giving a crude five-year survival rate of59%. There is thus a considerable difference inprognosis between cases of Hodgkin's diseaselocalized to one site and cases of benign Hodgkin'sdisease, irrespective of the extent of the disease whenfirst seen. These arguments in no way invalidatePeters' conclusions and it appears to be an esta-blished fact that the prognosis in classical Hodgkin'sdisease is much better when the condition is localizedto a single group lymphatic region.As far as the individual patient is concerned, it
is extremely difficult to state dogmatically whether acure has been effected in benign Hodgkin's disease.Certainly recurrences and death after a quiescentperiod of 10 years or longer are not uncommon.Jackson and Parker (1947) report a patient who diedin the twenty-seventh year of his illness; followinghis initial course of treatment he had remainedwell for 24 years. The same authors also report apatient surviving 35 years with recurrences in theseventh and twenty-seventh years. We believe thatprogression is ultimately inevitable in the absenceof treatment but that with energetic radiotherapya permanent cure is possible.
This work was made possible by the many colleagueswho sent us cases and helped us so generously with thefollow-up; to them we are deeply grateful. We shouldalso like to thank Professor I. Doniach for much helpfuladvice.
230
on May 31, 2022 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.14.3.219 on 1 May 1961. D
ownloaded from

A clinicopathological study of benign Hodgkin's disease
REFERENCES
Bonenfant, J.-L. (1954). La lympho-reticulose m6dullaire chroniquemaligne avec syndrome Hodgkinien (paragranulome). Bull.Ass. franf. Cancer, 41, 296.
Castleman, B. (1949). Pathological discussion on Cabot case 35391of the Massachusetts General Hospital. New Engl. J. Med.,241, 499.
Custer, R. P., and Bernhard, W. G. (1948). The interrelationship ofHodgkin's disease and other lymphatic tumors. Amer. J. med.Sci., 216, 625.
Dawson, P. J. (1960). Benign Hodgkin's Disease. M.D. Thesis,Cambridge.
Hall, C. A., and Olson, K. B. (1956). Prognosis of the malignantlymphomas. Ann. intern. Med., 44, 687.
Harrison, C. V. (1952). Benign Hodgkin's disease (Hodgkin's para-granuloma). J. Path. Bact., 64, 513.
Hartvigsen, F. B. (1955). Hodgkin's disease and pregnancy. Actaradiol. (Stockh.), 44, 317.
Healy, R. J., Amory, H. I., and Friedman, M. (1955). Hodgkin'sdisease: a review of 216 cases. Radiology, 64, 51.
Hoster, H. A., Dratman, Mary B., Craver, L. F., and Rolnick, H.A. (1948). Hodgkin's disease, 1832-1947. Cancer Res., 8, 1.
Jackson, H. (1937). The classification and prognosis of Hodgkin'sdisease and allied disorders. Surg. Gynec. Obstet., 64, 465.
(1939). Hodgkin's disease and allied disorders. New Engl. J.Med., 220, 26.
,and Parker, F. (1944). Hodgkin's disease. Ibid, 230, 1; 231, 35and 639.
(1947). Hodgkin's Disease and Allied Disorders, Ch. 1,p. 3. Oxford University Press, New York.
Jelliffe, A. M., and Thomson, A. D. (1955). The prognosis in Hodgkin'sdisease. Brit. J. Cancer, 9, 21.
Lumb, G. (1954). Tumours of Lymphoid Tissue, Ch. 7, p. 58.Livingstone, Edinburgh.and Newton, K. A. (1957). Prognosis in tumors of lymphoidtissue: an analysis of 602 cases. Cancer (Philad.), 10, 976.
Marshall, A. H. E. (1956). An Outline of the Cytology and Pathology,of the Reticular Tissue, Ch. 4, p. 164. Oliver and Boyd,Edinburgh.
Merner, T. B., and Stenstrom, K. W. (1947). Roentgen therapy inHodgkin's disease. Radiology, 48, 355.
Peters, M. Vera (1950). A study of survivals in Hodgkin's diseasetreated radiologically. Amer. J. Roentgenol., 63, 299.
-, and Middlemiss, K. C. H. (1958). A study of Hodgkin's diseasetreated by irradiation. Ibid, 79, 114.
Pitcock, J. A., Bauer, W. C., and McGavran, M. H. (1959). Hodgkin'sdisease in children: a clinicopathological study of 46 cases.Cancer (Philad.), 12, 1043.
Rappaport, H., Winter, W. J., and Hicks, Ethel B. (1956). Folli-cular lymphoma: a re-evaluation of its position in the schemeof malignant lymphoma, based on a survey of 253 cases.Ibid, 9, 792.
Robb-Smith, A. H. T. (1947). In S. C. Dyke (Ed.) Recent Advancesin Clinical Pathology, Ch. 34, pp. 360 and 367. Churchill,London.
Rosenthal, S. R. (1936). Significance of tissue lymphocytes in theprognosis of lymphogranulomatosis. Arch. Path. (Chicago),21, 628.
Sellers, A. H. (1957). A Statistical Review of Hodgkin's Disease.Ontario Department of Health.
Slaughter, D. P., and Craver, L. F. (1942). Hodgkin's disease: five-year survival rate; value of early surgical treatment; notes onfour cases of long duration. Amer. J. Roentgenol., 47, 596.
Smetana, H. F., and Cohen, B. M. (1956). Mortality in relation tohistologic type in Hodgkin's disease. Blood, 11, 211.
Southam, C. M., Diamond, H. D., and Craver, L. F. (1956). Pregnancyduring Hodgkin's disease. Cancer (Philad.), 9, 1141.
Symmers, W. St. C. (1958). In R. W. Raven (Ed.) Cancer, Vol. 2,Ch. 24, p. 478. Butterworth, London.
Trautmann, F. (1954). Benigne chronische Lymphomatose. Artzl.Wschr., 9, 1093 and 1113.
(1959). Benign chronische Lymphomatose. Ther. d. Gegenw.,98, 112.
Uddstromer, M. (1934). On the occurrence of lymphogranulomatosis(Sternberg) in Sweden 1915-31 and some considerations as toits relation to tuberculosis. Acta tuberc. scand., Suppl. I.
Wright, C. J. E. (1956). Hodgkin's paragranuloma. Cancer (Philad.),9, 773.(1960). The 'benign' form of Hodgkin's disease (Hodgkin'sparagranuloma). J. Path. Bact., 80, 157.
231
on May 31, 2022 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.14.3.219 on 1 May 1961. D
ownloaded from
























![Benign Breast Disease[1]](https://img.pdfslide.us/doc/110x75/5571f7b649795991698bd982/benign-breast-disease1.jpg)


